
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 23 November 2023
Sec. Movement Science
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1243804
 Sheila Geiger1,2*
Sheila Geiger1,2* Lisa Maria Jahre1,2
Lisa Maria Jahre1,2 Julia Aufderlandwehr1
Julia Aufderlandwehr1 Julia Barbara Krakowczyk1,2
Julia Barbara Krakowczyk1,2 Anna Julia Esser1,2
Anna Julia Esser1,2 Thomas Mühlbauer3
Thomas Mühlbauer3 Eva-Maria Skoda1,2
Eva-Maria Skoda1,2 Martin Teufel1,2
Martin Teufel1,2 Alexander Bäuerle1,2
Alexander Bäuerle1,2Introduction: Elite athletes are exposed to a variety of sport-specific stressors that may put them at particular risk for mental health symptoms and disorders. The aim of the present study was to assess data on mental health of elite athletes and investigate associations and interconnections among different variables using network analysis.
Methods: A cross-sectional study was conducted from December 2021 to December 2022. The sample consisted of 275 German elite athletes (167 females) aged ≥18 years. Next to sociodemographic, medical and sport-related data, psychometric data such as psychological distress, symptoms of generalized anxiety, depression, and somatic symptom disorder have been gathered through questionnaires and analyzed by means of network analysis.
Results: Over 95.0% of the athletes showed elevated distress and 28.6% reported symptoms of depression. Results of the network analysis show, among other findings, that symptoms of somatic symptom disorder were associated with severe injuries and substance use. Moreover, elite athletes who reported a better financial situation reported fewer symptoms of depression, generalized anxiety, and somatic symptom disorder. They also reported a lower incidence of mild to moderate injuries and severe injuries, fewer years spent in elite sports, less substance use, and fewer training sessions per week. Conversely, these athletes reported a higher level of distress. Furthermore, sex, financial situation and number of training units per week emerged as significant predictors for mental health symptoms.
Discussion: Elite athletes showed increased numbers regarding mental health symptoms. Providing appropriate mental health interventions for elite athletes and further analysis of factors that influence the mental health of elite athletes and their interplay seem to be of central importance for the general well-being of elite athletes.
Elite athletes often devote a significant amount of time and resources to their training and compete in events or competitions at national, international or professional levels (APA, 2023). In general, research supports the idea that physical activity has a positive impact on mental health (Daley, 2008; Hamer et al., 2009). Moreover, being involved in elite sports tends to have a beneficial impact on one’s lifespan (Lemez and Baker, 2015). However, on the other hand, some studies show that elite athletes can be particularly vulnerable to mental health symptoms and psychopathological disorders due to the unique stressors they face in competitive sports (Arnold and Fletcher, 2012; Gouttebarge et al., 2019). Intense physical activity at the level of elite sports can have a negative effect on mental wellbeing, potentially increasing anxiety, depression, overtraining, injury, and burnout (Peluso and Andrade, 2005). It is commonly believed that an excessive training load is a vital stimulus to improve athletic performance (Issurin, 2010). Nevertheless, an inadequate balance between training intensity and appropriate recovery periods may give rise to various impairments, such as overtraining syndrome or relative energy deficiency (Stellingwerff et al., 2021; Carrard et al., 2022). In addition to physical stress, elite athletes are also exposed to a range of risk factors such as performance pressure, injuries, competition pressure, risk of financial issues, lack of (social) support (Arnold and Fletcher, 2012), and involuntary retirement due to injuries (Gouttebarge et al., 2019). Female sex, young age, and injuries were found to be risk factors of anxiety symptoms (Rice et al., 2019). Moreover, psychosocial variables such as stress response can increase injury risk of elite athletes (Ivarsson et al., 2017).
Despite the risk factors and mental health symptoms, elite athletes are less likely to seek professional help for mental health symptoms compared to the general population (Watson, 2005). Reasons for this include fear of stigma and a potential impact on performance and career, a perception that seeking help is a sign of weakness as well as a lack of understanding of mental health (Gulliver et al., 2010, 2012). The high levels of training can lead to overexertion, which can manifest in a range of symptoms such as exhaustion, depression, anxiety disorders, hypertension, and a variety of somatic symptoms (Bompa et al., 2020). A systematic review and meta-analysis suggests that the prevalence of mental health symptoms and disorders may be slightly higher in current and former elite athletes (16.0–34.0%) compared to the general population (Gouttebarge et al., 2019). Moreover, one third of elite athletes reported symptoms of anxiety and/or depression, while 19.6% experienced distress (Gouttebarge et al., 2019). Thus, prevalences of mental health symptoms and disorders among elite athletes are comparable to, if not slightly higher than, those of the general population. However, their likelihood of seeking help is low, making them even more vulnerable to more severe and continued mental health symptoms. To date, we have not found any study that has investigated somatic symptom disorder in elite athletes. Given the physical and emotional demands of elite sports, which can both increase the risk of injury and cause mental health symptoms and the fact that competitive athletes need their bodies to perform the sports, an examination of the prevalence and severity of somatic symptom disorder in this population is warranted.
Mental health symptoms can lead to a variety of negative consequences such as decreased quality of life or increased risk for suicide (Evans et al., 2007; Moitra et al., 2021). Going further, there is evidence that mental health symptoms can negatively impact athletic performance (Beedie et al., 2000; Khan et al., 2017). Even though there has been a growing focus on identifying and addressing mental health symptoms among elite athletes in the past decade (Rice et al., 2016), the field of sports psychiatry and its associated research are still in their early stages. As a result, the mental health care currently provided to elite athletes may not consider sport-specific factors that could affect their risk for mental health symptoms or address unique diagnostic or treatment considerations for this group (Reardon and Factor, 2010; Bär and Markser, 2013). Additional information on these factors can be valuable for establishing preventive measures as well as managing acute phases.
To prevent mental health symptoms among athletes, it is important to identify and address potential risk and protective factors, as well as explore possible interconnections between relevant factors. Network analysis (NA) is an innovative way to depict and examine psychopathology and related constructs independent from categorial approaches (Levinson et al., 2018). NA is a method used to study complex systems or concepts by representing them as nodes in a network and examining the relationships between these nodes. The basis for this approach is network theory (Borsboom, 2017). Within the field of psychology, NA has been used to study a variety of topics, including the relationships between different symptoms of mental health disorders (Borsboom and Cramer, 2013). NA can be particularly useful in exploring relationships between complex concepts in an exploratory manner, without making any assumptions or hypotheses about the eventual network configuration (Borsboom and Cramer, 2013). Since psychological variables are assumed to influence each other directly and not to be caused by an unobserved latent entity (Borsboom and Cramer, 2013), NA represents the totality of interrelationships better than looking at partial aspects only. Moreover, NA enables us to examine numerous interrelationships simultaneously and to show how different aspects are interconnected in their entirety. We consider network analysis as a useful method to investigate these relationships in more detail. Levinson et al. suggest that psychological networks can further be used as important evidence base for more targeted treatment options, e.g., by focusing on central nodes in order to weaken the connections within the psychopathological network (Levinson et al., 2018). By uncovering key factors influencing the mental health of elite athletes and considering negative feedback processes between vulnerabilities, supportive and treatment offers can be adapted accordingly, to enhance their effectiveness.
The present study contains two objectives. The first one is to evaluate the prevalences and severity of generalized anxiety symptoms, depression symptoms, somatic symptom disorder symptoms and psychological distress in elite athletes. Similar to previous studies it is expected that there will be higher prevalences in mental health symptoms in elite athletes compared to the general population (Gouttebarge et al., 2019).
The second aim of this study is to identify different factors connected with mental health symptoms using NA and regression analyses. We focused on depressive symptoms, generalized anxiety, distress, financial situation, injuries and trainingload, as these are known risk factors and known mental health symptoms in the research (Gouttebarge et al., 2019; Rice et al., 2019; Stellingwerff et al., 2021; Carrard et al., 2022). Moreover, we included somatic symptom disorder and substance use as further variables because there has been little research to date on substance use among elite athletes and no research on somatic symptom disorder (Exner et al., 2021). Although NA is an exploratory method, it is anticipated that mental health symptoms will be linked to injuries (Gouttebarge et al., 2016; Kiliç et al., 2018). Additionally, there is an expectation that poorer financial circumstances are connected to mental health symptoms (Argabright et al., 2022; Guan et al., 2022).
By examining the potential factors linked to mental health symptoms in elite athletes, our findings could serve as a roadmap for future research that is relevant to clinical practice.
This cross-sectional study was conducted in the form of a digital survey. It was performed within approval guidelines of the Ethics Committee of the Faculty of Medicine of the University of Duisburg-Essen (19-8947-BO). Prior to starting the survey, electronic informed consent was obtained from each participant. Participation was anonymous and voluntary. There was no form of reimbursement. The average time of completing the digital survey was 19:50 min. The standard deviation was 10:45 min and the range of time for completion amounted to 73:45 min. The Unipark software (Tivian XI GmbH) was used, and the survey was distributed from December 2021 to December 2022. The eligibility requirements included adult age (≥18 years), a good command of the German language, internet access, and being an elite athlete. An elite athlete was defined as a person who (1) aligns their life to sports, (2) strives for athletic excellence, and (3) participates in professional or Olympic competitions (Pfaff, 2004; Lämmle, 2011; Reardon et al., 2019). Sports federations (regional and national) and sports clubs (with elite athletes competing in regional and nationwide tournaments) of all sports were contacted via mail and social media. The criteria that had to be fulfilled in order to be considered an elite athlete and to be able to take part in the study were listed here. A total number of 382 participants answered the questionnaire. Out of these, 29 participants had to be excluded at the beginning of the survey because they were younger than 18 years. Another 78 participants were excluded from the study as they did not meet the criteria required for elite athlete status at the time of the survey. The final sample for data analysis consisted of N = 275 athletes.
The survey collected sociodemographic data, including age, sex, family status, housing situation, level of education, financial situation, and occupation. Medical data covered body height, body mass, medications, and injuries within the last 12 months (regardless of type, location, and whether or not it was a contact injury). Since the survey addressed elite athletes, it also covered different sport-related data such as type of sports, years in elite sports, number of training units per week, duration of training units, etc.
Five validated measures were used in the survey to assess aspects of mental health symptoms, namely generalized anxiety symptoms, depressive symptoms, somatic symptom disorder symptoms and psychological distress. First, the Generalized Anxiety Disorder Scale-7 (GAD-7) identifies the severity of generalized anxiety symptoms (Löwe et al., 2008). It consists of seven items assessing symptoms of generalized anxiety disorder over the past 2 weeks. Scores can range from 0 (not at all) to 3 (nearly every day) for each item. The total score ranges from 0 to 21 and can be categorized between minimal (0–4), mild (5–9), moderate (10–14), and severe (15–21) levels of anxiety. The GAD-7 is a reliable and valid tool to evaluate generalized anxiety symptoms (Löwe et al., 2008). Reaching a value of 0.85 for Cronbach’s alpha, this measure showed high internal consistency in our study. Second, the Patient Health Questionnaire-8 (PHQ-8) is a questionnaire to assess depression symptoms (Kroenke et al., 2008). It consists of eight items, each of which can score between 0 (not at all) and 3 (nearly every day), thus yielding a total score from 0 to 24. We used the recommended cut-off score of 10 points for major depression symptoms. The scale reached high internal consistency with Cronbach’s alpha of 0.85. Third, the Patient Health Questionnaire-15 (PHQ-15) and Somatic Symptom Disorder Scale (SSD-12) were used to assess somatic symptom disorder symptoms (Toussaint et al., 2020). The PHQ-15 evaluates the severity of somatic symptoms experienced during the past 4 weeks. Item scores range between 0 (not bothered at all) and 2 (bothered a lot) each, the sum score ranges between 0 and 30. It can be used to assess the A criteria of Somatic Symptom Disorder (SSD) defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The recommend cut-off combined with SSD-12 is ≥9 (Toussaint et al., 2020). In our study, the PHQ-15 reached a value of 0.78 for Cronbach’s alpha, which is considered medium to high. Additionally, the SSD-12 was applied, which comprises 12 items to cover the B criteria of the DSM-5 definition of the SSD (excessive and disproportionate thoughts, feelings, and behaviors associated with somatic symptoms; Falkai et al., 2015). It has proven to be a reliable and valid tool to screen for the B criteria of SSD (Toussaint et al., 2017). Three subgroups containing four items each assess the aforementioned criteria. Item scores range from 0 to 4 with total sum scores ranging from 0 to 48. We used the optimal combined cut-off of ≥9 for the PHQ-15 and ≥23 for the SSD-12 (Toussaint et al., 2020). In our study, the SSD-12 reached a value of 0.90 for Cronbach’s alpha, which is considered excellent. Fourth, the Distress Thermometer (DT) was applied to evaluate psychological distress in the past week on a visual scale from 0 (no distress) to 10 (extreme distress). For the German version of the DT a cut-off of 4 points has been identified to be a sign of relevant distress (Mehnert et al., 2006).
Data analysis was conducted using SPSS Statistics 26 (IBM) and R 4.1.1 (R Core Team). Descriptive statistics were calculated for the participants’ sociodemographic data and scores on various psychometric instruments (GAD-7, PHQ-8, PHQ-15, SSD-12). Linear and multiple regression analyses were conducted to determine predictors of mental health variables. To provide evidence for the construct validity of the applied questionnaires, confirmatory factor analyses (CFA) were conducted. The maximum likelihood method was chosen as the estimation method. Model fit was assessed using a χ2 test and common approximate fit indices (RMSEA, SRMR, CFI, and TLI; Hu and Bentler, 1999). NA was performed using the packages qgraph, igraph, bootnet, and EGAnet (Csardi and Nepusz, 2006; Epskamp et al., 2012; Golino and Epskamp, 2017). Centrality indices were computed and assessment of the network’s stability and accuracy was conducted via bootnet. Missing data was addressed using listwise deletion, with the minimum sample size set to 250–350 participants to ensure sufficient power for the analysis of networks with 20 nodes or fewer (Constantin et al., 2021). The study estimated and visualized the network using a gaussian graphical model (Epskamp and Fried, 2018). Depressive symptoms, somatic symptom disorder, generalized anxiety, distress, mild to moderate injuries, severe injuries, years in elite sports, substance use, financial situation and training units per week were selected as nodes, resulting in a total of 11 nodes in the network. The dependencies among the variables were represented as edges in the network based on partial correlations (Epskamp and Fried, 2018). According to Epskamp and Fried (2018), gLASSO and EBIC (Chen and Chen, 2008; Friedman et al., 2008) methods were applied, with a tuning parameter of 0.5. The tuning parameter of 0.5 was chosen to create a parsimonious network with a higher specificity, as suggested by Epskamp and Fried (2018). The centrality indices were then calculated to determine the importance of each node in the network. These indices included degree centrality, strength, closeness, and betweenness (Hevey, 2018). Degree centrality is the sum of all edges of a node, strength is the sum of the edge weights of all edges of a node, closeness measures the average distance of a node to other nodes, and betweenness identifies the role of a node in connecting other nodes (Hevey, 2018). The centrality indices are intended to provide clues as to which constructs are particularly relevant in the context of – in this case - various mental health and sport-related variables (Epskamp and Fried, 2018). The stability and accuracy of the network were evaluated through different bootstrap procedures, including an edge weight variation analysis (Isvoranu et al., 2021) and a correlation stability analysis. It is recommended that, in order to interpret centrality with confidence, stability coefficients should exceed at least 0.25 and ideally surpass 0.50 (Epskamp et al., 2018). The interpretability of the edge weight, node strength, and centrality indices was also assessed.
Table 1 shows the sample characteristics of the present study. Participants were between 18 and 63 years old (M = 23.67 years, SD = 6.29 years) with 76.5% being 18–25 years old. 60.7% of participants were female and 39.3% were male. The average body height for male athletes was 182.67 cm (SD = 7.44 cm), and their average body mass was 79.60 kg (SD = 11.36 kg). Female athletes had an average body height of 170.75 cm (SD = 7.23 cm) and an average body mass of 65.83 kg (SD = 8.56 kg). A total of 85 athletes took part in team sports only, while 143 were exclusively involved in individual sports, leaving 47 participants who were actively engaged in both. The number of athletes per type of sports is illustrated in Table 1. Most athletes practiced their sport for an average of 9.69 years (SD = 5.25) and, accordingly, began participating in elite sports at school age. Information regarding recent training habits reveals that the average length of each training session was 96.86 (SD = 32.96) minutes, and there were 8.20 (SD = 4.27) training units per week on average. The elite athletes exercised an average of 754.77 (SD = 367.42) minutes per week. No information was provided regarding whether the participants were affiliated with a German national team or if they were college or university students.
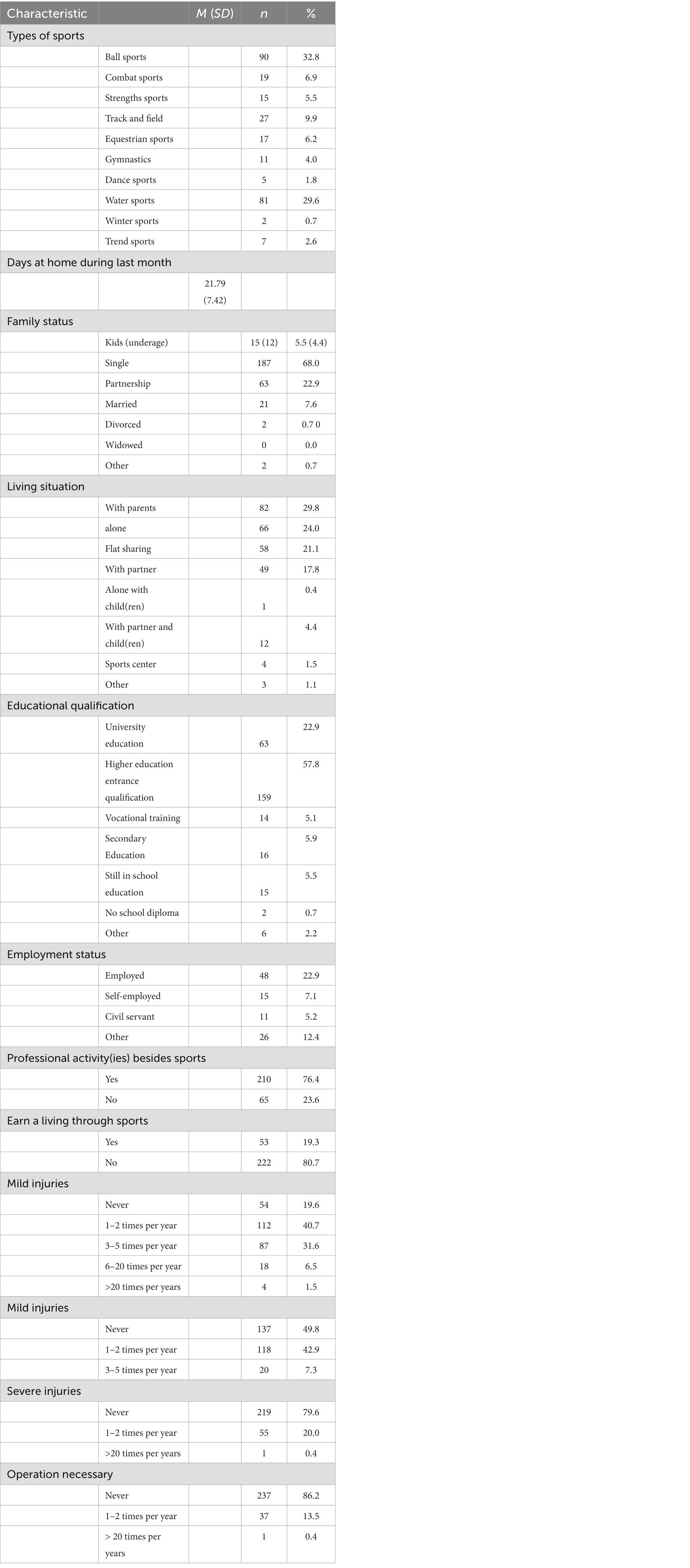
Table 1. Sample characteristics (N = 275).
CFA could only confirm the three factorial structure of the SSD-12. Results of the CFA can be found in the Supplementary Table S6.
The prevalence of psychological distress, depression symptoms, generalized anxiety symptoms, and somatic symptom disorder symptoms, stratified by sex is shown in Table 2. The GAD-7 (M = 5.0, SD = 3.8) measures revealed that 35.6% of participants had mild, 9.1% had moderate, and 2.9% had severe anxiety symptoms. Cut-off scores of PHQ-8 (M = 6.8, SD = 4.6) showed that 28.6% of the participants experienced symptoms of major depression. Using the combined cut-offs for the SSD-12 (≥23; M = 11.1, SD = 7.9) and the PHQ-15 (≥9; M = 7.0, SD = 4.3), 6.5% of participants exceeded the combined criterion, indicating somatic symptom disorder symptoms. The analyses of the DT scores (M = 7.4, SD = 2.0) resulted in 95.3% of participants reaching the cut-off value of 4, showing relevant distress. 95.3% reported any mental health symptoms and 4.7% reported none.
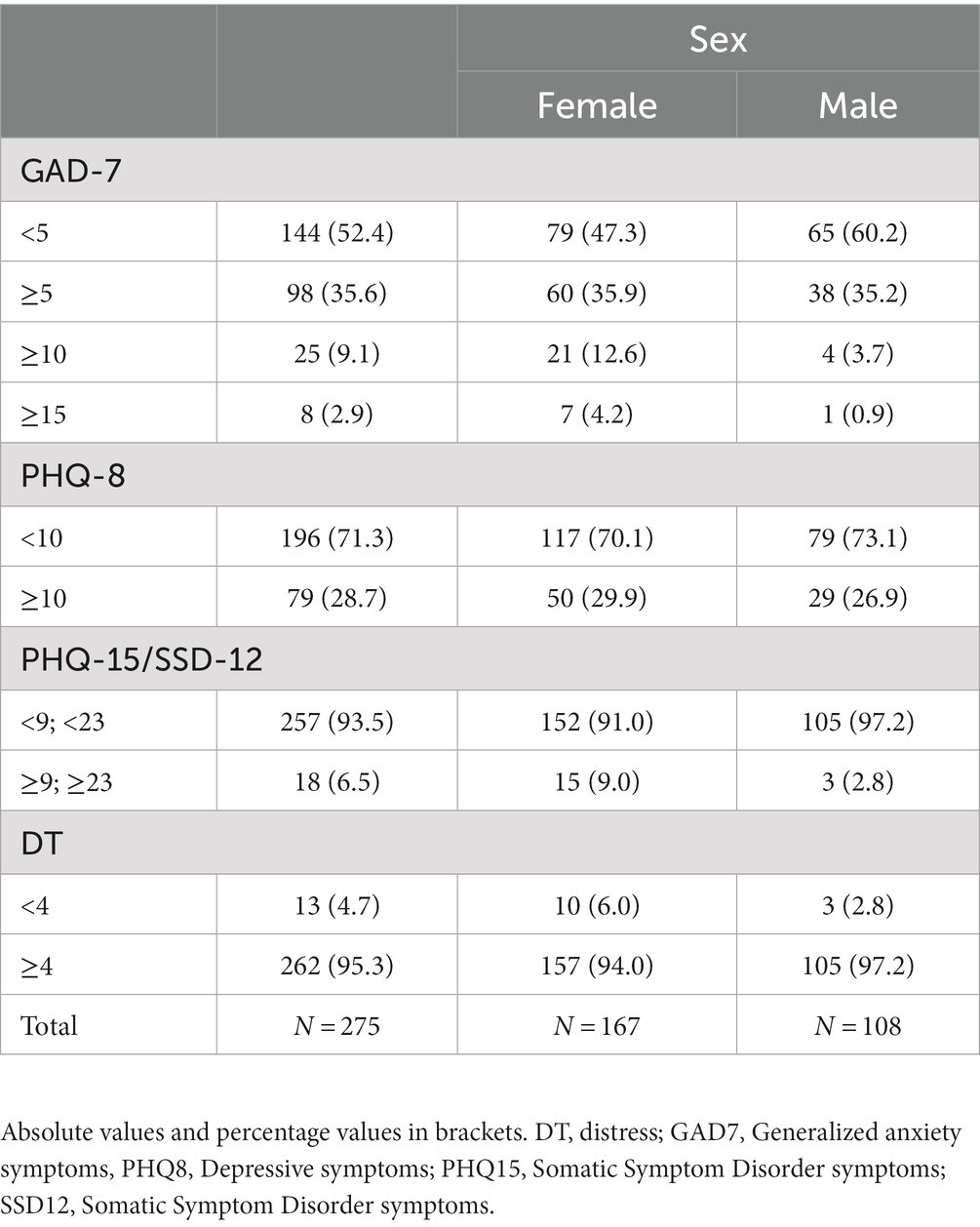
Table 2. Prevalence of generalized anxiety symptoms, depression symptoms, psychological distress and SSD12 stratified by sex.
Figure 1 illustrates the Visualized Partial Correlation Network. After excluding 7 participants who had missing values on relevant variables, the network consisted of N = 268 participants. Across the network, 11 nodes were connected by 33 out of 55 (60.0%) possible edges. Among these, 27 displayed positive associations and 6 displayed negative ones. A graphical representation of the network with displayed edge weights can be found in the Supplementary Figure S1. The following strongest positive edges have been identified: Depression symptoms and generalized anxiety symptoms (0.55), somatic symptom disorder symptoms and severity of somatic symptoms (0.34), depression symptoms and severity of somatic symptoms (0.33), mild to moderate and severe injuries (0.26), somatic symptom disorder symptoms and generalized anxiety symptoms (0.17), years in elite sports and severe injuries (0.16), distress and depression symptoms (0.15), somatic symptom disorder symptoms and severe injuries (0.15), somatic symptom disorder symptoms and substance use (0.14) and training units per week and depression symptoms (0.13). The strongest negative edge weight was between financial situation and severity of somatic symptoms (−0.12). The edges associated with financial situation were generally all negative except for financial situation and distress (0.04).
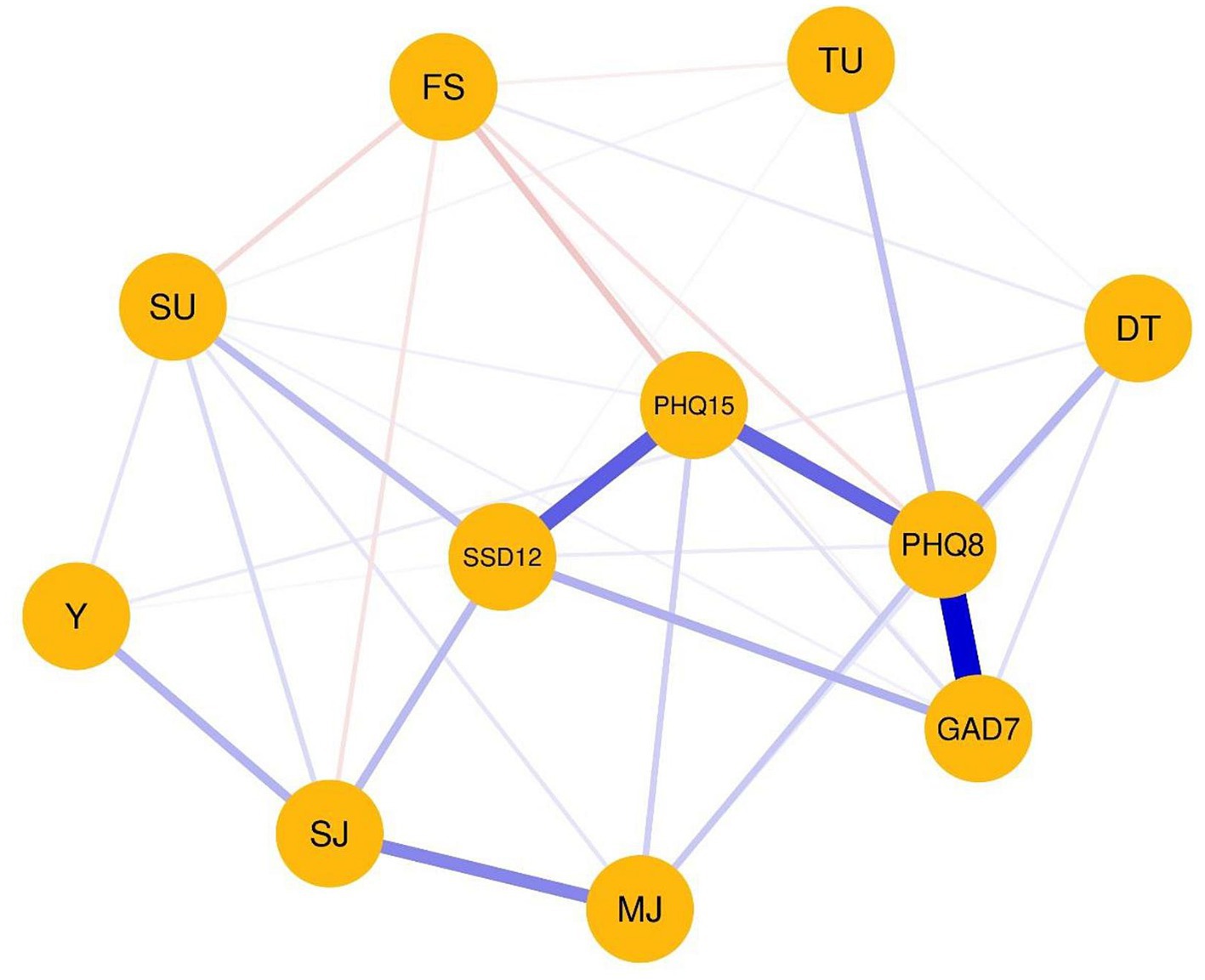
Figure 1. Visualized partial correlation network. The abbreviations within the network display the nodes. The thickness of the edges represents the edge connections between those nodes are referred to as edges. The thickness of the edges represents the edge weight, which is an indication of the strength of the edge. The thicker the edge, the higher the edge weight. Blue edges represent positive associations, whereas red edges represent negative associations. The meanings of the variables’ abbreviations can be seen on the right side of the network display. DT, distress; FS, financial situation; GAD7, Generalized anxiety symptoms; MJ, mild to moderate injuries; PHQ8, Depressive symptoms; PHQ15, Somatic Symptom Disorder symptoms; SSD12, Somatic Symptom Disorder symptoms; SJ, severe injuries to operation necessary; SU, substance use; TU, training units per week; Y, years in elite sports.
Figure 2 displays the centrality strength, closeness, and betweenness. The highest strength centrality was obtained for depression symptoms (1.23), severity of somatic symptoms (0.93), somatic symptom disorder symptoms (0.62), and generalized anxiety symptoms (0.67). The highest closeness index was found for severity of somatic symptoms (1.50), depression symptoms (1.23), somatic symptom disorder (1.20), and generalized anxiety symptoms (0.73). The highest betweenness index was detected for depression symptoms (2.16), severity of somatic symptoms (1.09), somatic symptom disorder (0.63), and severe injuries (0.63).
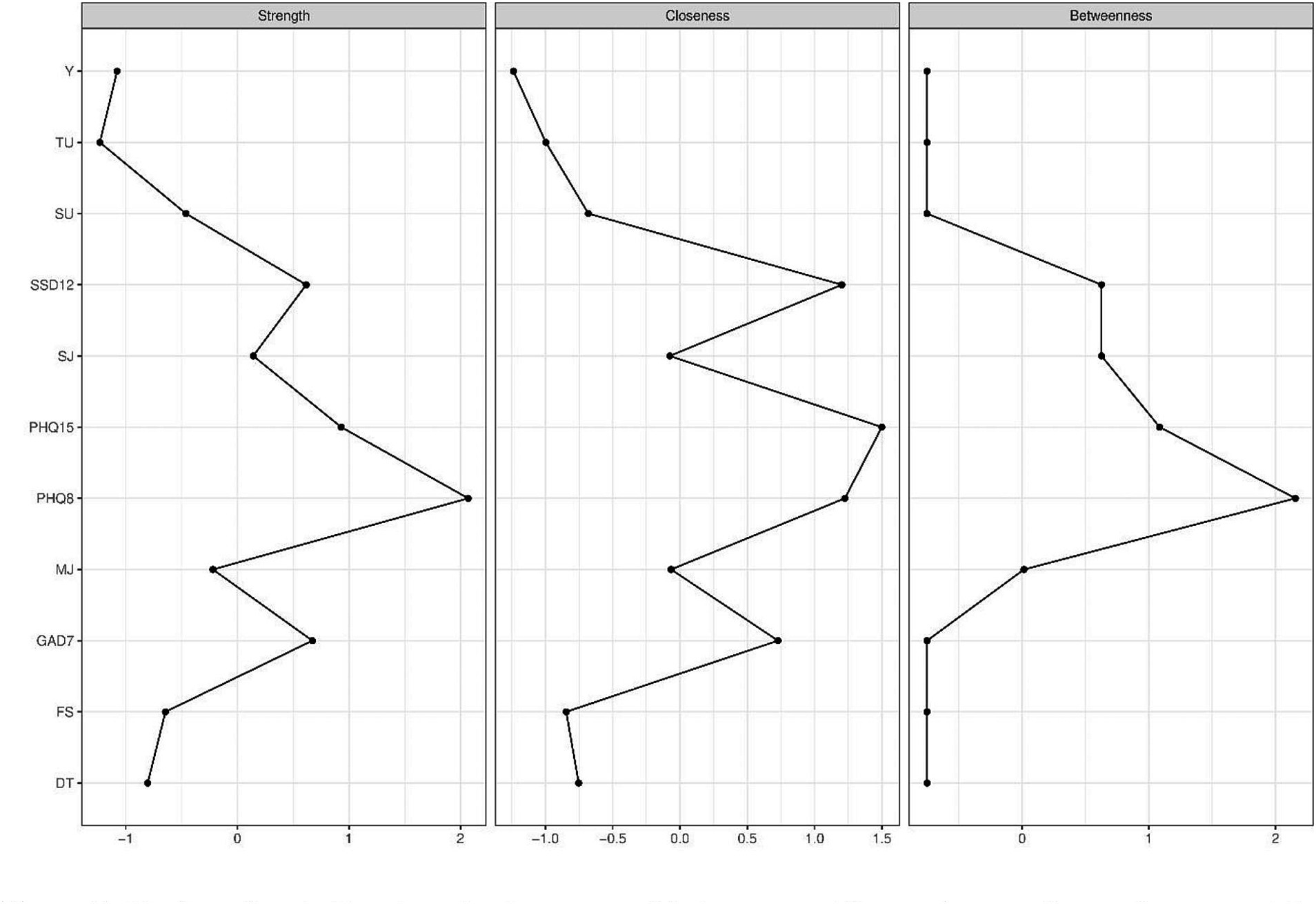
Figure 2. Display of centrality strength, closeness and betweenness. The numbers on the y-axis represent the allocated nodes numbered sequentially. The x-axis represents z-values associated with the centrality indices. The higher the z-value, the higher the centrality index of the respective variable. DT, distress; FS, financial situation; GAD7, Generalized anxiety symptoms; MJ, mild to moderate injuries; PHQ8, Depressive symptoms; PHQ15, Somatic Symptom Disorder symptoms; SSD12, Somatic Symptom Disorder symptoms; SJ, severe injuries to operation necessary; SU, substance use; TU, training units per week; Y, years in elite sports.
To test whether the estimation of the partial correlation network was accurate and stable, bootstrap procedures were conducted for edge weight variation, the significance of edge weight and node strength differences, and the correlation stability of the centrality indices. Stability analysis revealed that the network model was stable. Edge weight stability of the network was good (0.67). The strength centrality coefficient and expected influence coefficient were excellent (0.75 for both). A graphical representation of the edge stabilities can be found in the Supplementary Figure S2.
In the multiple regression analyses, it was shown that the sociodemographic variables and sport related variables significantly predicted depression symptoms (R2 = 0.287; F23,273 = 4.384; p < 0.001). Of the sociodemographic variables female sex (β = 0.183; p = 0.002) and worse financial situation (β = −0.232; p = <0.001) significantly predicted depression symptoms. Of the sports related variables number of training units per week (β = 0.235; p = <0.001) and of the type of sports strength sports (β = 0.157; p = 0.047) significantly predicted depression symptoms.
Regarding the generalized anxiety disorder, sociodemographic variables and sports types represented significant predictors (R2 = 0.246; F23,273 = 3.538; p < 0.001). Older age (β = 0.011; p = <0.001) and worse financial situation (β = −0.243; p = <0.001) as well as the living situations living alone (β = −0.274; p = 0.019) or living with parents (β = −0.290; p = 0.014) significantly predicted generalized anxiety symptoms. Also the type of sports, ball sports (β = 0.304; p = 0.017), strength sports (β = 0.229; p = 0.005) and track and field (β = 0.208; p = 0.024) represented significant predictors.
Only the sociodemographic factors female sex (PHQ-15: β = 0.248; p = <0.001; SSD-12: β = 0.229; p = 0.005) and worse financial situation (PHQ-15: β = −0.293; p = <0.001; SSD-12: β = 0.229; p = 0.005) and the sports related variable number of training units per week (PHQ-15: β = 0.160; p = 0.013; SSD-12: β = 0.229; p = 0.005) were significant predictors for somatic symptoms according to PHQ-15 (R2 = 0.296; F23,273 = 4.568; p < 0.001) and SSD-12 (R2 = 0.191; F23,273 = 2.568; p < 0.001).
There were no significant predictors in the multiple regression analysis of distress. All results of the regression analyses can be found in Supplementary Tables S1–S5.
The present study examined the mental health and related factors of German elite athletes. Specifically, prevalences of generalized anxiety, depression, somatic symptom disorder, and psychological distress have been assessed among this population. An increased prevalence of generalized anxiety, depressive symptoms, and psychological problems in elite athletes has been shown. NA reveals strong associations between mental health symptoms. Somatic symptom disorder symptoms were associated with severe injuries and substance use. Furthermore, athletes who reported a more favorable financial situation reported fewer symptoms of depression, generalized anxiety, and somatic symptom disorder, as well as fewer mild to moderate injuries, severe injuries, years spent in elite sports, substance use, and training sessions per week. Conversely, these athletes reported higher levels of distress. Significant predictors for mental health symptoms were sex, financial situation and training units per week.
In the study sample, 35.6% showed mild symptoms of generalized anxiety disorder. Moderate levels were observed in 9.1% of the participants, three times higher than the average (3.0%) in the German population (Löwe et al., 2008). Severe symptoms were found in 2.9% of the participants, surpassing the rates of 1.0 and 1.2% reported in a normative sample and a population-based study, respectively (Löwe et al., 2008; Hinz et al., 2017). These results are consistent with research showing a 33% prevalence of depression/anxiety (undifferentiated) in elite athletes (Gouttebarge et al., 2019). Moreover, this study found that 28.6% of the participants experience symptoms of major depression, which aligns with current research (Gouttebarge et al., 2019). In a large random comparison sample (N = 198,678), 8.6% of the participants experienced depressive symptoms (Kroenke et al., 2008). Thus, elite athletes report higher prevalences of depressive symptoms than the general population in Germany. Furthermore, 6.5% of participants showed symptoms of somatic symptom disorder, which is in line with the estimated prevalence of 5.0–7.0% in the general population in Germany (Toussaint et al., 2020). This suggests that elite athletes are not necessarily more likely to experience somatic symptom disorder than the general population. One potential reason for this is that in somatic symptom disorder, one source of stress may be the presence of physical symptoms without any clear medical explanation (APA, 2000). In contrast, athletes often have a clear understanding of the physical symptoms they experience and may not face an additional psychological burden as a result. The prevalence of psychological distress was found to be considerably higher (95.3% versus 39.0%), compared to samples from the German population and to those found in the meta-analysis of Gouttebarge and colleagues, in which on average 19.6% of elite athletes reported distress (Gouttebarge et al., 2019; Hinz et al., 2019). One explanation could be that the elite athletes understood distress as purely physical distress and indicated a high level of distress due to the physical stress of the training. Another explanation could be that elite athletes tend to experience a lot of arousal in order to perform best at competition (Raglin, 1992). One must also consider that high between-study heterogeneity was observed in the study of Gouttebarge and colleagues, likely due to measurement-related concerns and differences in the cohorts (Gouttebarge et al., 2019).
Results of the NA reveal close connections between mental health symptoms and injuries due to sports. Specifically, included were symptoms of generalized anxiety, depression, and somatic symptom disorder, as well as injuries. The results are consistent with recent research finding a higher overall risk for mental health symptoms and disorders in elite athletes with severe musculoskeletal injuries and multiple surgeries (Gouttebarge et al., 2016; Kiliç et al., 2018). This suggests that injuries and mental health symptoms are interconnected. Elite athletes are exposed to high levels of physical demands throughout their careers and this cumulative physical load, when combined with inadequate recovery, puts them at risk of developing musculoskeletal injuries (Kenttä and Hassmen, 1998; Chen et al., 2005; Cunniffe et al., 2009). In line with this, NA shows that severe injuries were associated with years in elite sports. Thus, addressing mental health in athletes requires a multifaceted approach that includes both providing support and resources for athletes who have suffered injuries (Putukian, 2016; Rice et al., 2018) and even more important proactively addressing the root causes of mental health symptoms.
Furthermore, NA demonstrates a strong correlation between depressive symptoms and generalized anxiety, indicating that these conditions are closely intertwined and are likely to occur together. This finding is consistent with previous research that highlights a high comorbidity of depression and anxiety at both the disorder and symptom levels both in the general population and in elite athletes (Jacobson and Newman, 2017; Åkesdotter et al., 2022). This corresponds with the centrality analysis results. In particular, mental health variables show high centrality in the network analysis. The dominance of mental health variables in centrality was expected due to their frequency in the network analysis. Nevertheless, the result confirms our expectations and means that no other variable has a higher degree of centrality. Furthermore, a more favorable financial situation was associated with fewer symptoms of depression, generalized anxiety, and somatic symptom disorder. Less financial burden was further related to fewer mild to moderate injuries, severe injuries, fewer years of involvement in elite sports, and lower levels of substance use and training sessions per week. Conversely, athletes with less financial burden reported higher levels of distress, which is an unexpected finding. Financial stress has been proposed as an economic determinant of depression (Guan et al., 2022) and higher financial worries were significantly associated with higher psychological distress (Ryu and Fan, 2023). In the present study, the results were the opposite. The less financial stress, the more distress was reported by the elite athletes. One explanation could be that athletes who have a better financial situation tend to work more and thus experience more distress.
In the multiple regression analyses sex, financial situation, training units and strength sports were significant predictors of depression symptoms. Female sex, worse financial situation, more training units and engaging in strength sports were associated with more depression symptoms. Moreover, age, financial situation, living alone, living with parents, ball sports, strength sports and track and field were found to significantly predict generalized anxiety symptoms. Financial situation, living alone and living with parents were associated with less generalized anxiety symptoms. Engaging in ball sports, strength sports and track and field was associated with more generalized anxiety symptoms. Fittingly, in a recent study, female sex was found to be a significant predictor of depressive symptoms, while age was not found to have significant predictive value (Wilson et al., 2022). In line with this, a meta-analysis showed that male elite athletes exhibited a 52% lower likelihood of reporting mild or severe depressive symptoms compared to their female counterparts who are also elite athletes (Gorczynski et al., 2017). This association also exists in the general population (Parker and Brotchie, 2010), highlighting the established sex disparity in relation to depressive symptoms. Moreover financial concern was found to be a significant predictor of both depression symptoms and anxiety (Pensgaard et al., 2021). These findings are also consistent with the outcomes from the network analysis. Additionally, financial situation appears to be a predictor of somatic symptom disorder. Worse financial situation was associated with more symptoms somatic symptom disorder. The financial situation, respectively the financial burden, seems to be an important factor regarding the mental health of elite athletes. Unlike our findings, a recent study did not find age and sports type to be significant predictors of generalized anxiety (Li et al., 2021). However, sex was not a significant predictor of generalized anxiety in this study, consistent with our results (Li et al., 2021). Interestingly, both living alone and living with parents were shown to be significant predictors of generalized anxiety. This finding suggests further investigation into the potential factors or dynamics associated with these life situations that might contribute to the experience of generalized anxiety. Furthermore, sex, financial situation, and training units per week emerged to be significant predictors for somatic symptom disorder. Female sex, worse financial situation and more training units were associated with more symptoms of somatic symptom disorder. Thus, training units per week was a significant predictor for both symptoms of depression and somatic symptom disorder. However, although current research shows that physical activity has positive effects on psychological well-being (Daley, 2008; Hamer et al., 2009), one explanation for this result could be overtraining syndrome. Overtraining syndrome refers to a condition characterized by a long-term decline in performance that occurs after a sustained imbalance between exercise-related and non-exercise-related stress and recovery (Meeusen et al., 2013). Insufficient focus on maintaining a proper balance between training intensity and recovery can result in enduring fatigue and unusual training responses (maladaptation) (Fry et al., 1991; Kenttä and Hassmén, 1998; Meeusen et al., 2013). In summary, the complex interplay of various factors such as sex, financial situation, and training units per week, as highlighted in the regression analyses, underscores the importance of considering these elements when understanding the mental health of elite athletes.
The study design was cross-sectional, which precludes causal inference from the data. Additionally, all data was obtained via self-reporting, which makes objective verification of symptoms impossible. The data was collected through an online survey that was distributed via social media, sports clubs, and sports associations and thus selection bias should be taken into consideration when interpreting the findings. Moreover, retest-reliability assessment was not possible; future research should address this limitation to strengthen findings with elite athletes. Another important limitation is the construct validity assessment of the measurement instruments, especially for elite athletes. While we conducted confirmatory factor analyses and reliability assessments, the use of elite athlete-specific validated instruments is a consideration. The contrast between assumed and athlete-observed structures requires careful interpretation. Future studies could develop and validate measurement tools for elite athletes’ unique mental health dynamics. Similarly, the lack of cut-off values specifically validated for elite athletes in the questionnaires used is an additional limitation that needs to be addressed. Again, future research is needed to establish appropriate cut-off values for elite athletes. Consequently, the results can only be interpreted in the context of studies that examined different populations. Furthermore, the present study had a higher proportion of female participants and athletes with higher education levels, which should also be considered in terms of generalizability, as research shows that female elite athletes report performance anxiety, poor concentration, and somatic anxiety to a higher degree than males (Abrahamsen et al., 2008). Although comparative studies utilized highly validated and representative reference values, the differing age and sex distributions in the reference samples represent a limitation. Missing data on elite athletes’ specific sports, regional backgrounds (i.e., East or West Germany) and performance/competition level (e.g., highest level throughout career and current level) leads to uncertainties regarding the scope of the study. Future research should incorporate these variables for a more comprehensive analysis. Furthermore, the scheme used for classifying types of sports in Table 1, while practical for data collection, exhibited limitations due to inconsistent criteria and overlapping categories. Adopting the analytically clear categorization proposed by Emrich et al. (2001) in future studies could offer more precise insights into the relationships between different sport types and mental health symptoms. The timespan in which our data was collected (i.e., December 2021 to December 2022) may also be of consequence, as the fading COVID-19 pandemic may have affected prevalence of mental health symptoms (Dragioti et al., 2022; Robinson et al., 2022). To the best of our knowledge, this study is the first to offer a NA of mental health symptoms in elite athletes. Furthermore, we were able to survey a relatively large sample size.
In conclusion, the results of this study suggest that elite athletes have higher prevalences of mental health symptoms compared to the general population. The findings suggest that elite athletes may face unique challenges related to their sports, such as injuries and financial stressors, which may contribute to their risk for mental health symptoms. The high rates of psychological distress, depression and anxiety highlight the need for increased awareness and the importance of providing access to mental health resources for elite athletes, especially when they are at risk for or recovering from injury. To effectively address mental health symptoms in elite athletes, it is important to focus not only on treating symptoms, but also to explore the underlying causes that contribute to these mental health symptoms. Sex, financial situation, and number of training sessions seem to be essential factors in this context. Since many symptoms are closely related to each other, it is important to respond as soon as some of them occur. Early intervention could include screening programs, education and training for athletes and coaches, access to mental health professionals and to eHealth interventions. Further research is needed to better understand the factors contributing to the high levels of mental health symptoms seen in elite athletes.
The raw data supporting the conclusions of this article will be made available upon reasonable request to the corresponding author.
The studies involving humans were approved by Ethics Committee of the Faculty of Medicine of the University of Duisburg-Essen. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their electronic informed consent to participate in this study.
AB, MT, E-MS, and SG initiated and conceptualized the study. JA and TM were co-responsible for the recruitment of the participants. SG, LJ, and JK performed the statistical analyses and interpretation of the data. SG wrote the first draft of the manuscript. All authors contributed to the further writing of the manuscript and approved the final version.
We thank the Open Access Fund of the University of Duisburg-Essen for supporting the publication of the manuscript.
We are thankful to our colleagues who provided expertise that greatly assisted the research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1243804/full#supplementary-material
Abrahamsen, F. E., Roberts, G. C., and Pensgaard, A. M. (2008). Achievement goals and gender effects on multidimensional anxiety in national elite sport. Psychol. Sport Exerc. 9, 449–464. doi: 10.1016/j.psychsport.2007.06.005
Åkesdotter, C., Kenttä, G., Eloranta, S., Håkansson, A., and Franck, J. (2022). Prevalence and comorbidity of psychiatric disorders among treatment-seeking elite athletes and high-performance coaches. BMJ Open Sport Exerc. Med. 8:e001264. doi: 10.1136/bmjsem-2021-001264
Argabright, S. T., Tran, K. T., Visoki, E., DiDomenico, G. E., Moore, T. M., and Barzilay, R. (2022). COVID-19-related financial strain and adolescent mental health. Lancet Reg. Health Am. 16:100391. doi: 10.1016/j.lana.2022.100391
Arnold, R., and Fletcher, D. (2012). A research synthesis and taxonomic classification of the organizational stressors encountered by sport performers. J. Sport Exerc. Psychol. 34, 397–429. doi: 10.1123/jsep.34.3.397
Bär, K. J., and Markser, V. Z. (2013). Sport specificity of mental disorders: the issue of sport psychiatry. Eur. Arch. Psychiatry Clin. Neurosci. 263, 205–210. doi: 10.1007/s00406-013-0458-4
Beedie, C. J., Terry, P. C., and Lane, A. M. (2000). The profile of mood states and athletic performance: Two meta-analyses. Journal of Applied Sport Psychology, 12, 49–68.
Bompa, T.O., Côté, J., and Haff, G.G. (2020). Periodization: theory and methodology of training. The high levels of training can lead to overexertion, which can manifest in a range of symptoms such as exhaustion, depression, anxiety disorders and a variety of somatic symptoms.
Borsboom, D. (2017). A network theory of mental disorders. World Psychiatry 16, 5–13. doi: 10.1002/wps.20375
Borsboom, D., and Cramer, A. O. (2013). Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 9, 91–121. doi: 10.1146/annurev-clinpsy-050212-185608
Carrard, J., Rigort, A. C., Appenzeller-Herzog, C., Colledge, F., Konigstein, K., Hinrichs, T., et al. (2022). Diagnosing overtraining syndrome: a scoping review. Sports Health 14, 665–673. doi: 10.1177/19417381211044739
Chen, J., and Chen, Z. (2008). Extended Bayesian information criteria for model selection with large model spaces. Biometrika 95, 759–771. doi: 10.1093/biomet/asn034
Chen, S. K., Cheng, Y. M., Lin, Y. C., Hong, Y. J., Huang, P. J., and Chou, P. H. (2005). Investigation of management models in elite athlete injuries. Kaohsiung J. Med. Sci. 21, 220–227. doi: 10.1016/S1607-551X(09)70191-3
Constantin, M.A., Schuurman, N.K., and Vermunt, J. (2021). A General Monte Carlo method for sample size analysis in the context of network models. (Psychol Methods).
Csardi, G., and Nepusz, T. (2006). The Igraph software package for complex network research. Inter J. Complex Systems. 1695, 1–9.
Cunniffe, B., Proctor, W., Baker, J. S., and Davies, B. (2009). An evaluation of the physiological demands of elite rugby union using global positioning system tracking software. J. Strength Cond. Res. 23, 1195–1203. doi: 10.1519/JSC.0b013e3181a3928b
Daley, A. (2008). Exercise and depression: a review of reviews. J. Clin. Psychol. Med. Settings 15, 140–147. doi: 10.1007/s10880-008-9105-z
Dragioti, E., Li, H., Tsitsas, G., Lee, K. H., Choi, J., Kim, J., et al. (2022). A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J. Med. Virol. 94, 1935–1949. doi: 10.1002/jmv.27549
Emrich, E., Pitsch, W., and Papathanassiou, V. (2001). “Ein Versuch auf empirischer Grundlage” in Schriftenreihe des Bundesinstituts für Sportwissenschaft (Schorndorf: Verlag Karl Hofmann)
Epskamp, S., Borsboom, D., and Fried, E. I. (2018). Estimating psychological networks and their accuracy: a tutorial paper. Behav. Res. Methods 50, 195–212. doi: 10.3758/s13428-017-0862-1
Epskamp, S., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D., and Borsboom, D. (2012). Qgraph: network visualizations of relationships in psychometric data. J. Stat. Softw. 48, 1–18. doi: 10.18637/jss.v048.i04
Epskamp, S., and Fried, E. I. (2018). A tutorial on regularized partial correlation networks. Psychol. Methods 23, 617–634. doi: 10.1037/met0000167
Evans, S., Banerjee, S., Leese, M., and Huxley, P. (2007). The impact of mental illness on quality of life: a comparison of severe mental illness, common mental disorder and healthy population samples. Qual. Life Res. 16, 17–29. doi: 10.1007/s11136-006-9002-6
Exner, J., Bitar, R., Berg, X., Pichler, E. M., Herdener, M., Seifritz, E., et al. (2021). Use of psychotropic substances among elite athletes - a narrative review. Swiss Med. Wkly. 151:w20412. doi: 10.4414/smw.2021.20412
Falkai, P., Wittchen, H., and Döpfner, M. (2015). Diagnostisches und statistisches Manual psychischer Störungen DSM-5®. Göttingen: Hogrefe.
Friedman, J., Hastie, T., and Tibshirani, R. (2008). Sparse inverse covariance estimation with the graphical lasso. Biostatistics 9, 432–441. doi: 10.1093/biostatistics/kxm045
Fry, R. W., Morton, A. R., and Keast, D. (1991). Overtraining in athletes. Sports Med 12, 32–65. doi: 10.2165/00007256-199112010-00004
Golino, H. F., and Epskamp, S. (2017). Exploratory graph analysis: a new approach for estimating the number of dimensions in psychological research. PLoS One 12:e0174035. doi: 10.1371/journal.pone.0174035
Gorczynski, P. F., Coyle, M., and Gibson, K. (2017). Depressive symptoms in high-performance athletes and non-athletes: a comparative meta-analysis. Br. J. Sports Med. 51, 1348–1354. doi: 10.1136/bjsports-2016-096455
Gouttebarge, V., Aoki, H., Ekstrand, J., Verhagen, E. A., and Kerkhoffs, G. M. (2016). Are severe musculoskeletal injuries associated with symptoms of common mental disorders among male European professional footballers? Knee Surg. Sports Traumatol. Arthrosc. 24, 3934–3942. doi: 10.1007/s00167-015-3729-y
Gouttebarge, V., Castaldelli-Maia, J. M., Gorczynski, P., Hainline, B., Hitchcock, M. E., Kerkhoffs, G. M., et al. (2019). Occurrence of mental health symptoms and disorders in current and former elite athletes: a systematic review and meta-analysis. Br. J. Sports Med. 53, 700–706. doi: 10.1136/bjsports-2019-100671
Guan, N., Guariglia, A., Moore, P., Xu, F., and Al-Janabi, H. (2022). Financial stress and depression in adults: a systematic review. PLoS One 17:e0264041. doi: 10.1371/journal.pone.0264041
Gulliver, A., Griffiths, K. M., and Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry 10:113. doi: 10.1186/1471-244X-10-113
Gulliver, A., Griffiths, K. M., and Christensen, H. (2012). Barriers and facilitators to mental health help-seeking for young elite athletes: a qualitative study. BMC Psychiatry 12:157. doi: 10.1186/1471-244X-12-157
Hamer, M., Stamatakis, E., and Steptoe, A. (2009). Dose-response relationship between physical activity and mental health: the Scottish health survey. Br. J. Sports Med. 43, 1111–1114. doi: 10.1136/bjsm.2008.046243
Hevey, D. (2018). Network analysis: a brief overview and tutorial. Health Psychol. Behav. Med. 6, 301–328. doi: 10.1080/21642850.2018.1521283
Hinz, A., Klein, A. M., Brahler, E., Glaesmer, H., Luck, T., Riedel-Heller, S. G., et al. (2017). Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. J. Affect. Disord. 210, 338–344. doi: 10.1016/j.jad.2016.12.012
Hinz, A., Mitchell, A. J., Degi, C. L., and Mehnert-Theuerkauf, A. (2019). Normative values for the distress thermometer (DT) and the emotion thermometers (ET), derived from a German general population sample. Qual. Life Res. 28, 277–282. doi: 10.1007/s11136-018-2014-1
Hu, L.-T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. 6, 1–55. doi: 10.1080/10705519909540118
Issurin, V. B. (2010). New horizons for the methodology and physiology of training periodization. Sports Med. 40, 189–206. doi: 10.2165/11319770-000000000-00000
Isvoranu, A. M., Abdin, E., Chong, S. A., Vaingankar, J., Borsboom, D., and Subramaniam, M. (2021). Extended network analysis: from psychopathology to chronic illness. BMC Psychiatry 21:119. doi: 10.1186/s12888-021-03128-y
Ivarsson, A., Johnson, U., Andersen, M. B., Tranaeus, U., Stenling, A., and Lindwall, M. (2017). Psychosocial factors and sport injuries: Meta-analyses for prediction and prevention. Sports Med. 47, 353–365. doi: 10.1007/s40279-016-0578-x
Jacobson, N. C., and Newman, M. G. (2017). Anxiety and depression as bidirectional risk factors for one another: a meta-analysis of longitudinal studies. Psychol. Bull. 143, 1155–1200. doi: 10.1037/bul0000111
Kenttä, G., and Hassmen, P. (1998). Overtraining and recovery. A conceptual model. Sports Med. 26, 1–16. doi: 10.2165/00007256-199826010-00001
Khan, M. K., Khan, A., Khan, S. U., and Khan, S. (2017). Effects of anxiety on athletic performance. Res. Inves. Sports Med. 1, 1–5.
Kiliç, Ö., Aoki, H., Goedhart, E., Hagglund, M., Kerkhoffs, G., Kuijer, P., et al. (2018). Severe musculoskeletal time-loss injuries and symptoms of common mental disorders in professional soccer: a longitudinal analysis of 12-month follow-up data. Knee Surg. Sports Traumatol. Arthrosc. 26, 946–954. doi: 10.1007/s00167-017-4644-1
Kroenke, K., Strine, T. W., Spitzer, R. L., Williams, J. B., Berry, J. T., and Mokdad, A. H. (2008). The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 114 (1-3, 163–173. doi: 10.1016/j.jad.2008.06.026
Lämmle, L. (2011). “Theoretische Konzeption, Diagnostik und Bedeutung von Motivation und Selbstregulation im (Hoch-) Leistungssport” in Selbstregulation und Leistungsexzellenz (Münster). Eds. M. Dresel und L. Lämmle (Hrsg.), Motivation, Selbstregulation und Leistungsexzellenz, 91–112.
Lemez, S., and Baker, J. (2015). Do elite athletes live longer? A systematic review of mortality and longevity in elite athletes. Sports Med Open 1:16. doi: 10.1186/s40798-015-0024-x
Levinson, C. A., Vanzhula, I. A., Brosof, L. C., and Forbush, K. T. (2018). Network analysis as an alternative approach to conceptualizing eating disorders: implications for research and treatment. Curr. Psychiatry Rep. 20, 1–15. doi: 10.1007/s11920-018-0930-y
Li, C., Fan, R., Sun, J., and Li, G. (2021). Risk and protective factors of generalized anxiety disorder of elite collegiate athletes: a cross-sectional study. Front. Public Health 9:607800. doi: 10.3389/fpubh.2021.607800
Löwe, B., Decker, O., Muller, S., Brahler, E., Schellberg, D., Herzog, W., et al. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med. Care 46, 266–274. doi: 10.1097/MLR.0b013e318160d093
Meeusen, R., Duclos, M., Foster, C., Fry, A., Gleeson, M., Nieman, D., et al. (2013). Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 45, 186–205. doi: 10.1249/MSS.0b013e318279a10a
Mehnert, A., Müller, D., Lehmann, C., and Koch, U. (2006). Die deutsche Version des NCCN distress-thermometers. Psychiatr. Psychol. und Psychother. 54, 213–223. doi: 10.1024/1661-4747.54.3.213
Moitra, M., Santomauro, D., Degenhardt, L., Collins, P. Y., Whiteford, H., Vos, T., et al. (2021). Estimating the risk of suicide associated with mental disorders: a systematic review and meta-regression analysis. J. Psychiatr. Res. 137, 242–249. doi: 10.1016/j.jpsychires.2021.02.053
Parker, G., and Brotchie, H. (2010). Gender differences in depression. Int. Rev. Psychiatry 22, 429–436. doi: 10.3109/09540261.2010.492391
Peluso, M., and Andrade, L. (2005). Physical activity and mental health: the association between exercise and mood. Clinics 60, 61–70. doi: 10.1590/S1807-59322005000100012
Pensgaard, A. M., Oevreboe, T. H., and Ivarsson, A. (2021). Mental health among elite athletes in Norway during a selected period of the COVID-19 pandemic. BMJ Open Sport Exerc. Med. 7:e001025. doi: 10.1136/bmjsem-2020-001025
Putukian, M. (2016). The psychological response to injury in student athletes: a narrative review with a focus on mental health. Br. J. Sports Med. 50, 145–148. doi: 10.1136/bjsports-2015-095586
Reardon, C. L., and Factor, R. M. (2010). Sport psychiatry: a systematic review of diagnosis and medical treatment of mental illness in athletes. Sports Med. 40, 961–980. doi: 10.2165/11536580-000000000-00000
Reardon, C. L., Hainline, B., Aron, C. M., Baron, D., Baum, A. L., Bindra, A., et al. (2019). Mental health in elite athletes: International Olympic Committee consensus statement (2019). Br. J. Sports Med. 53, 667–699. doi: 10.1136/bjsports-2019-100715
Rice, S. M., Gwyther, K., Santesteban-Echarri, O., Baron, D., Gorczynski, P., Gouttebarge, V., et al. (2019). Determinants of anxiety in elite athletes: a systematic review and meta-analysis. Br. J. Sports Med. 53, 722–730. doi: 10.1136/bjsports-2019-100620
Rice, S. M., Parker, A. G., Rosenbaum, S., Bailey, A., Mawren, D., and Purcell, R. (2018). Sport-related concussion and mental health outcomes in elite athletes: a systematic review. Sports Med. 48, 447–465. doi: 10.1007/s40279-017-0810-3
Rice, S. M., Purcell, R., De Silva, S., Mawren, D., McGorry, P. D., and Parker, A. G. (2016). The mental health of elite athletes: a narrative systematic review. Sports Med. 46, 1333–1353. doi: 10.1007/s40279-016-0492-2
Robinson, E., Sutin, A. R., Daly, M., and Jones, A. (2022). A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 296, 567–576. doi: 10.1016/j.jad.2021.09.098
Ryu, S., and Fan, L. (2023). The relationship between financial worries and psychological distress among U.S. Adults. J Fam Econ Issues 44, 16–33. doi: 10.1007/s10834-022-09820-9
Stellingwerff, T., Heikura, I. A., Meeusen, R., Bermon, S., Seiler, S., Mountjoy, M. L., et al. (2021). Overtraining syndrome (OTS) and relative energy deficiency in sport (RED-S): shared pathways, symptoms and complexities. Sports Med. 51, 2251–2280. doi: 10.1007/s40279-021-01491-0
Toussaint, A., Husing, P., Kohlmann, S., and Löwe, B. (2020). Detecting DSM-5 somatic symptom disorder: criterion validity of the patient health Questionnaire-15 (PHQ-15) and the somatic symptom Scale-8 (SSS-8) in combination with the somatic symptom disorder - B criteria scale (SSD-12). Psychol. Med. 50, 324–333. doi: 10.1017/S003329171900014X
Toussaint, A., Löwe, B., Brahler, E., and Jordan, P. (2017). Normwerte und psychometrische Eigenschaften der, Somatic Symptom Disorder--B Criteria Scale (SSD-12)' in einer repräsentativen Stichprobe der deutschen Bevölkerung. J. Psychosom. Res. 63, 110–112.
Watson, J. C. (2005). College student-Athletes' attitudes toward help-seeking behavior and expectations of counseling services. J. Coll. Stud. Dev. 46, 442–449. doi: 10.1353/csd.2005.0044
Keywords: mental health, sports, distress, depression, anxiety, somatic symptom disorder
Citation: Geiger S, Jahre LM, Aufderlandwehr J, Krakowczyk JB, Esser AJ, Mühlbauer T, Skoda E-M, Teufel M and Bäuerle A (2023) Mental health symptoms in German elite athletes: a network analysis. Front. Psychol. 14:1243804. doi: 10.3389/fpsyg.2023.1243804
Edited by:
Humberto M. Carvalho, Federal University of Santa Catarina, BrazilReviewed by:
Arne Güllich, University of Kaiserslautern, GermanyCopyright © 2023 Geiger, Jahre, Aufderlandwehr, Krakowczyk, Esser, Mühlbauer, Skoda, Teufel and Bäuerle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheila Geiger, c2hlaWxhLmdlaWdlckB1bmktZHVlLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.