 Carmen Varela1,2,3*
Carmen Varela1,2,3* Ángela Hoyo3
Ángela Hoyo3 María Eugenia Tapia-Sanz3
María Eugenia Tapia-Sanz3 Ana Isabel Jiménez-González3
Ana Isabel Jiménez-González3 Benito Javier Moral3Paula Rodríguez-Fernández4
Benito Javier Moral3Paula Rodríguez-Fernández4 Yadirnaci Vargas-Hernández4
Yadirnaci Vargas-Hernández4 Luis Jorge Ruiz-Sánchez3
Luis Jorge Ruiz-Sánchez3- 1Universitat de Barcelona, Barcelona, Spain
- 2Departamento de Ciencias de la Salud, Facultad de Ciencias de la Salud, Universidad de Burgos, Burgos, Spain
- 3Área de Psicología, Facultad de Ciencias de la Salud, Universidad Isabel I, Burgos, Spain
- 4Facultad de Humanidades y Ciencias Sociales, Universidad Isabel I, Burgos, Spain
Introduction: Eating disorders (EDs) are serious psychological problems that affect not only the individual, but also their entire environment. The prevalence rates of EDs are higher among the adolescent population. A better understanding of ED risk factors is essential to design effective prevention and intervention programs that focus beyond the areas of weight and appearance.
Methods: The main objective of this systematic review was to identify the risk factors of EDs and provide a comprehensive approach, analyzing the interplay between individuals, their inner circle, and the society characteristics. The Web of Science, Scopus, CENTRAL and PsycInfo databases were searched.
Results: The initial search produced 8,178 references. After removing duplicates and performing the selection process by three independent reviewers, 42 articles were included in the systematic review according to the pre-specified inclusion criteria. The results suggest the relevance of society and the inner circle on the development of EDs.
Discussion: The internalization of the thin ideal, promoted by the current society, and living in an unsupportive, unaffectionate, non-cohesive environment were associated with the onset of EDs symptomatology. Other associated variables with this ED indicator were poor-quality relationships and feeling judged about appearance. These aspects seem to be essential for the development of individual characteristics like self-esteem or adaptative coping during adolescence. This systematic review has shown the complex etiology of EDs and the relevance of the interplay between the different areas involved. Furthermore, this information could be relevant to improve the design of innovative and more effective prevention and intervention programs.
Systematic review registration: PROSPERO, identifier CRD42022320881.
1. Introduction
Eating disorders (EDs) are psychological conditions characterized by specific and severe disturbances in eating behavior, resulting from distressing thoughts and emotions mainly related to weight, body shape. However, some EDs like avoidant/restrictive food intake disorder (ARFID) or Binge Eating Disorder (BED) are more focused on aspects like food or intake (López and Treasure, 2002; Gaete and López, 2020). These are serious and potentially life-threatening disorders that can affect people’s emotional and physical health as well as their social functioning (O’Brien et al., 2017; Gaete and López, 2020). Types of eating disorders include anorexia nervosa (AN), bulimia nervosa (BN), BED, ARFID, and other specified feeding, and eating disorder (OSFED; American Psychiatry Association, 2013).
The prevalence of EDs is variable and complex due to changes in diagnostic criteria and differences between geographical regions. In the last decade, different reviews (Smink et al., 2012; López, 2017) have shown that the countries with the highest prevalence of EDs are Switzerland (12%), Chile (8.3%), and Spain (6.2%), followed by Colombia (4.5%), the United Kingdom (3.7%), and Portugal (3.1%; López, 2017). In countries such as the United States, EDs lifetime prevalence varies between 0.5 and 1.5% (Smink et al., 2012). Prevalence also varies between different age and gender groups, but a common feature is that EDs are more frequent in women than in men, in all countries and at all ages. Concretely, one study showed that the weighted means of lifetime EDs were 2.2% for men and 8.4% for women (Galmiche et al., 2019). Moreover, EDs usually begin in adolescence, a time when major psychological changes related to identity and physical appearance, as well as the development of self-regulation, occur (Smink et al., 2012; Galmiche et al., 2019; Stice et al., 2021).
Considering the above-described evidence, it is not surprising that the World Health Organization (WHO) has considered EDs as a priority problem among adolescents, given the health risk that these disorders imply, and the high rate of comorbidity with other types of disorders (Gibson et al., 2019; Stice et al., 2021). Some of the disorders that show the highest comorbidity in adolescents are the following: depression, anxiety, and obsessive-compulsive disorder (Gaete and López, 2020; Hambleton et al., 2022). They are also associated with personality disorders, substance abuse, and self-harming behaviors (Hambleton et al., 2022). Finally, there is also a high association between EDs and suicidal behavior in adolescents (Gibson et al., 2019). In this regard, during the pandemic a study showed that 65% of female adolescents with EDs had suicidal ideation and 45% had attempted suicide. Although the quarantine situation could increase suicide rates, there is a significant association between suicidal thoughts and behaviors and EDs (Semenova et al., 2022). This makes EDs one of the disorders that require further research in the field of prevention and intervention in adolescence, especially given that the current intervention programs have shown mixed efficacy (Pratt and Woolfenden, 2002; Swanson et al., 2011; Fairburn et al., 2015; Stice et al., 2021).
Understanding the risk factors involved in the onset of EDs is essential for the development of effective prevention and early intervention programs. Research has shown that a variety of risk factors may be involved, such as biological, psychological, familiar, and socio-cultural factors (Stice, 2016; Solmi et al., 2020; Barakat et al., 2023), with psychological-type factors being most associated with eating disorder symptomatology in adolescents (Suarez-Albor et al., 2022). Factors that have shown such an association include body dissatisfaction, (e.g., Fortes et al., 2013; Lazo et al., 2015; Gismero-González, 2020), social difficulties, poor to no support network (Cardi et al., 2018), tendency toward perfectionism (Pamies and Quiles, 2014; Laporta et al., 2020), impulsivity (Nuño-Gutiérrez et al., 2009), low self-esteem in relation to weight and image (Fairburn et al., 2003; Serpell and Troop, 2003), emotional dysregulation (Monell et al., 2018), and family environment (Cerniglia et al., 2017). Despite this evidence, there have been no systematic reviews published in recent years that have specifically identified the psychological risk factors that may predict the onset of EDs in adolescents. Stating the art of this question is essential to design prevention and intervention programs that effectively address the right psychological targets (Stice et al., 2021). The focus on psychological factors is due to improvements in psychological interventions and current eating disorder prevention programs. For that reason, biological and genetic factors have not been included in this systematic review, although their knowledge is relevant to provide a comprehensive approach. A multidisciplinary team must be involved in the development of future proposals Therefore, the aim of the present study is to conduct a systematic review to provide a comprehensive and updated view of the psychological risk factors that predict the onset of EDs in adolescents. This information could be useful to design innovative prevention and intervention programs for adolescent population, highlighting areas beyond weight and appearance.
2. Methods
A systematic review of the literature was conducted. The international prospective register for systematic reviews (PROSPERO) accepted the protocol of this systematic review on 3rd June 2022, registration number CRD42022320881. This systematic review follows the guideline of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021).
2.1. Eligibility criteria
Adapted for a systematic review of association, the Population, Intervention, Comparator, Outcome and Study (PICOS) framework was used to establish the eligibility criteria of this study (Higgins and Green, 2008; Moola et al., 2015). As a result, the following inclusion criteria’s were: (a) population: adolescents between 11 and 19 years old; (b) exposure variables: psychological risk variables related to the onset of an ED (i.e., impulsivity, emotional dysregulation, social network exposure, perfectionism, self-demand, self-esteem, interpersonal relationships -social anxiety or social skills-, fear of maturing, low social or family support, and expressed emotion); (c) outcome: presence of ED symptomatology assessed by self-report or standardized/validated tools; and (d) type of study: observational studies that establish an association between exposure variables and outcome. Thus, adolescents who did not fall within the defined age range were excluded, as well as comorbidity with other serious physical or psychological problems, editorials, and conference abstracts. Table 1 shows the criteria for considering studies.
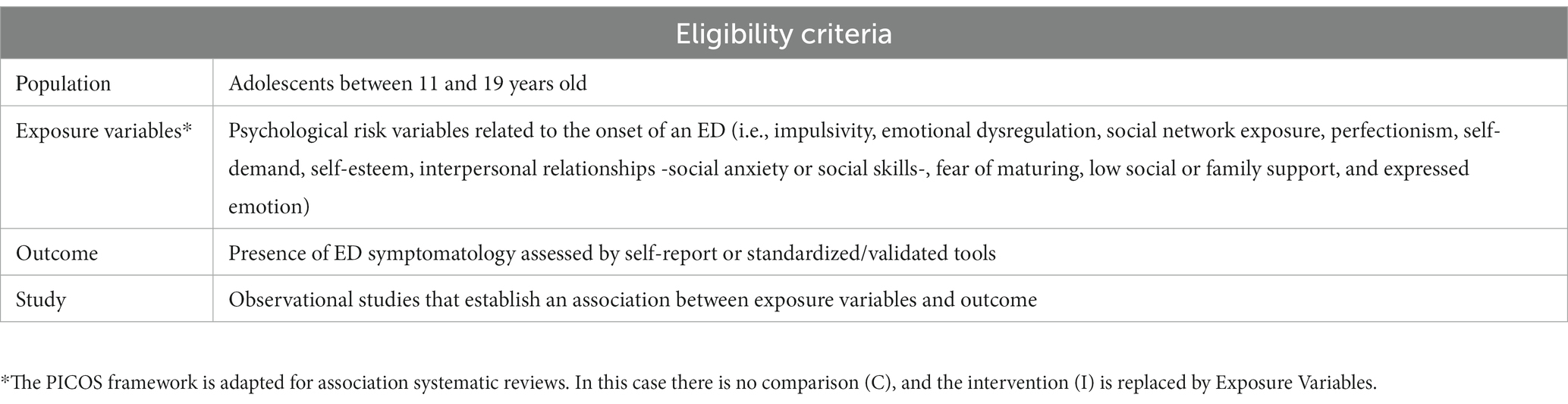
Table 1. Eligibility criteria to select studies for the systematic review.
2.2. Information sources
The search was carried out using the electronic databases Web of Science (WoS), Scopus, Cochrane Central Register of Controlled Trials (CENTRAL) and PsycInfo. The search was closed on 23rd November 2021. An update of the search was conducted on the 4th of October 2023.There were no limits regarding the publication year. The only limitation imposed on the search was the language, including only documents in English or Spanish.
2.3. Search strategy
In consideration of the format of each database, the following keywords in English were used in combination with the Boolean logic operators: (“eating disorders” OR “anorexia” OR “bulimia” OR “binge eating” OR “binge eating disorder” OR “unspecified eating disorder”) AND (impuls* OR “emotional dysregulation” OR “social media exposure” OR “social media misuse” OR “social media use” OR “perfecctio*” OR “self-demand” OR “self-esteem” OR “social support” OR “maturity fear*” OR “expressed emotion”) AND (“high school” OR adoles* OR teen*).
2.4. Data extraction and coding
All identified documents were imported into Rayyan, a research tool designed to work with systematic reviews, to eliminate duplicates. The screening process was performed by three independent reviewers, and disagreements were solved by discussion. If consensus was not achieved, the reviewer with the most experience in the area made the final decision. Data extraction was conducted by the same independent reviewers. The extracted information includes the following: (a) study identification: authorship, year, and country; (b) characteristics of the participants: sample size, gender and age; (c) characteristics of the exposure variables mentioned above, types and measuring instrument; (d) characteristics of the outcome variable: measuring instrument e) characteristics of statistical analysis: type and results.
2.5. Quality and risk of bias assessment
The methodological quality of the selected articles was assessed by four independent reviewers using the tool recommended by Cochrane, Quality in Prognosis Studies (QUIPS; Grooten et al., 2019). To specifically analyze the risk of bias, six main domains were evaluated: (i) study participation; (ii) study attrition; (iii) prognostic factor measurement; (iv) outcome measurement; (v) study confounding; and (vi) statistical analysis and reporting.
Several descriptors are presented in each domain, which were ranked on a three-point scale (high, medium, or low level of risk), according to the tool specification, assess the risk of potential bias in the results (Grooten et al., 2019).
3. Results
The initial number of identified articles was 8,700, including the initial search and the update. After removing duplicates, 5,455 studies were screened by three independent reviewers and 101 were selected for full-text screening. Finally, 47 studies met the pre-specified criteria and were included in the systematic review (Figure 1).
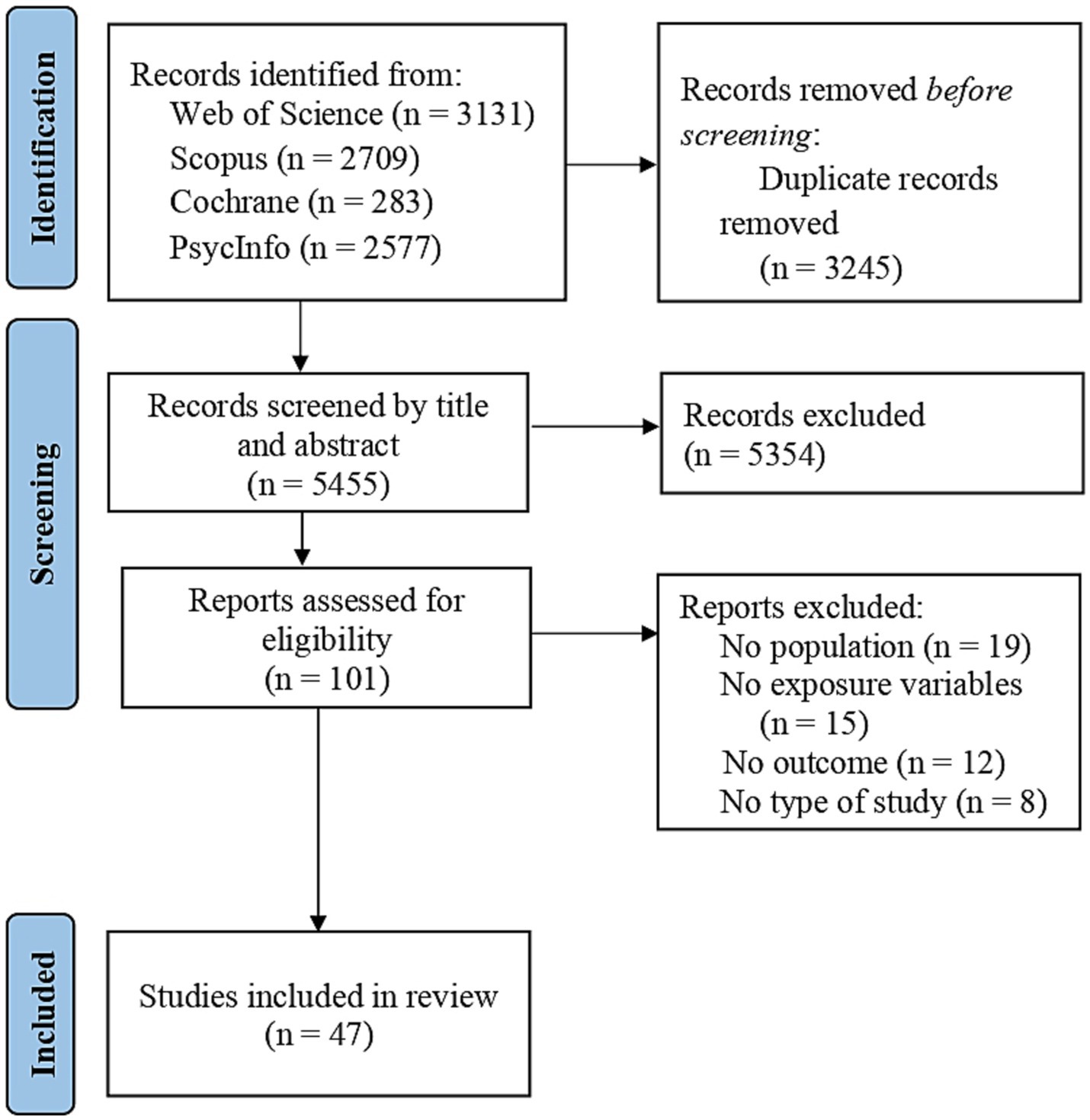
Figure 1. Flow diagram of study selection.
3.1. Descriptive data
A total of 47 studies were finally included in this systematic review after meeting the pre-specified inclusion criteria. These articles were conducted from 1996 to 2023 to cover the widest possible range and provide in-depth analysis of eating disorder predictors. The total sample comprised 41,115 teenagers, mean age = 14.9 years and ranged from 11 to 19 years. Most of the sample were women, 17 studies presented 100% women, 18 studies ≥50% women, 11 studies <50% women and only 1 study 100% men.
The studies were carried out in the United States (n = 6), Australia (n = 4), Spain (n = 5), Italy (n = 3); China, Iran, Belgium, Portugal, Brazil, Mexico, United Kingdom, Greece, Cyprus (each country, n = 2); Chile, Germany, Israel, Canada, Thailand, New Zealand, Malaysia, Netherlands, India, Bosnia Herzegovina and Turkey (each country, n = 1). Almost 70% of the studies (n = 33) were carried out in countries considered Western Societies. However, the risk factors identified in the included studies did not present relevant differences in terms of country or culture. All studies had a cross-sectional design except for eight longitudinal studies (Shomaker and Furman, 2009; Bachar et al., 2010; Boone et al., 2014; Dakanalis et al., 2014; Wade et al., 2015; Pace et al., 2018; Evans et al., 2019; Beckers et al., 2023). Most of the studies used regression and structured equation modeling analysis. The number of participants selected in longitudinal studies were indicated by the authors to carry out the statistical analysis indicated in Table 2.

Table 2. Summary table of the included studies.
3.2. Risk of bias assessment
Table 3 presents results of the estimated risk of bias for each study using QUIPS tool. Further analysis provides the frequency of the six assessed domains and (percentages were presented for each label; see Table 4). Most included studies showed low risk for all domains, except for the confounding variables, where the majority presented medium risk. Not all relevant potential variables were considered in the study design or were not reported by the authors.
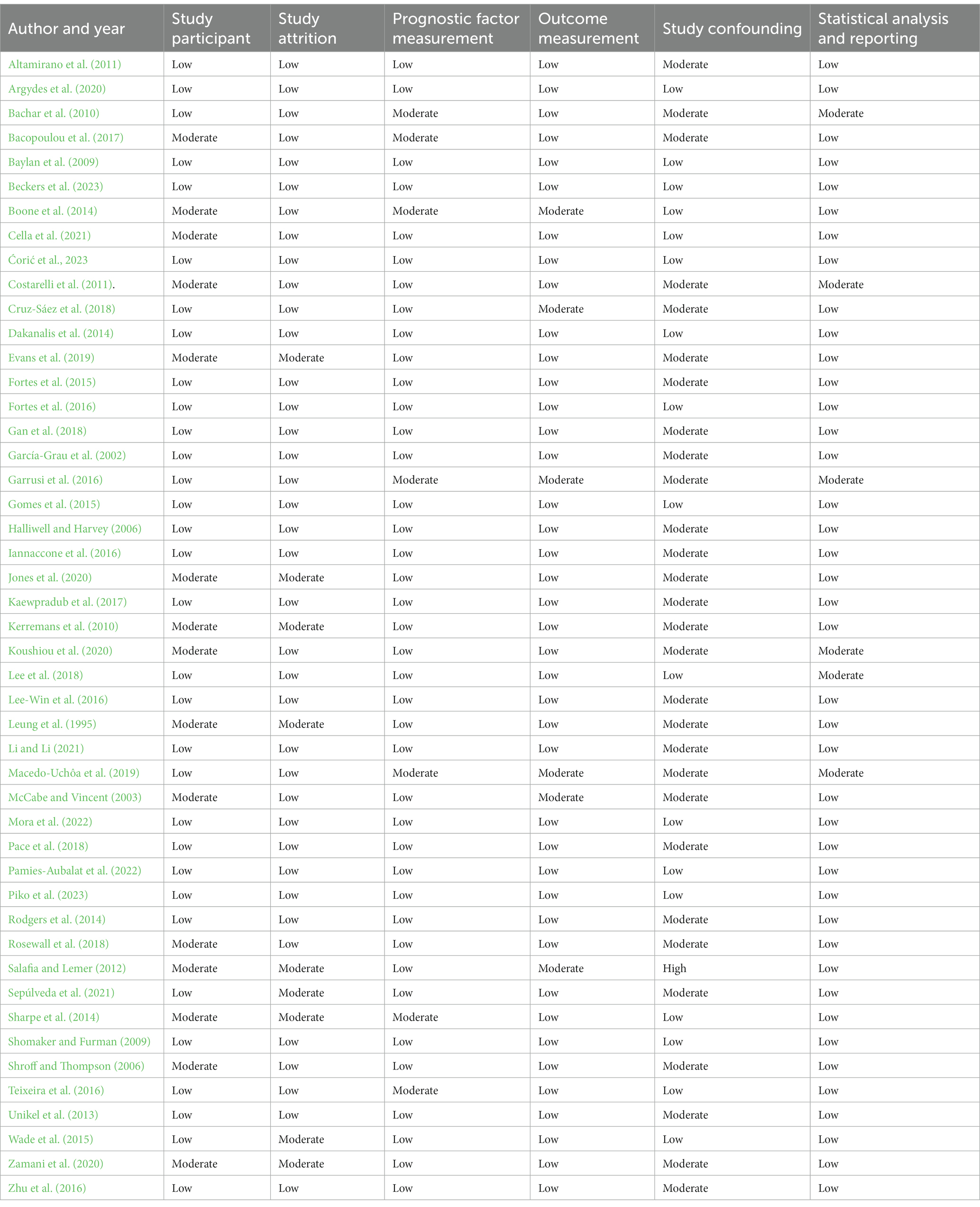
Table 3. Level of risk of bias assessment using QUIPS tool.
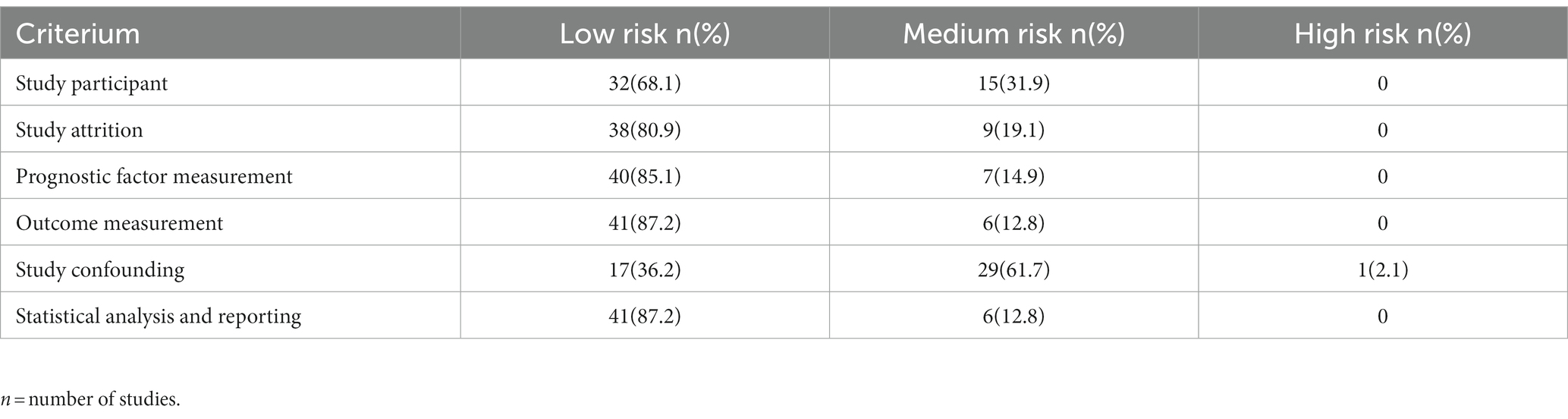
Table 4. Risk of bias summary.
3.3. Synthesis of primary outcomes
3.3.1. Individual variables
3.3.1.1. Self-esteem
Traditionally, low self-esteem has been associated with a greater likelihood of ED symptoms, particularly in adolescents.
Almost half of the included studies, concretely 24, have analyzed this variable and its relationship with disordered eating. Generally, low self-esteem has been identified as a predictive factor of the onset of EDs symptomatology. However, seven studies did not find significant associations between this variable and negative eating behaviors (Shroff and Thompson, 2006; Baylan et al., 2009; Rodgers et al., 2014; Garrusi et al., 2016; Kaewpradub et al., 2017; Argydes et al., 2020; Pamies-Aubalat et al., 2022).
A total of 12 studies showed self-esteem as a predictive factor with a direct influence on EDs symptomatology. Adolescents with lower self-esteem scores were more likely to develop disordered eating behaviors (McCabe and Vincent, 2003; Altamirano et al., 2011; Gomes et al., 2015; Teixeira et al., 2016; Gan et al., 2018; Rosewall et al., 2018; Jones et al., 2020; Zamani et al., 2020; Cella et al., 2021; Mora et al., 2022; Beckers et al., 2023; Ćorić et al., 2023). In two studies analyzing the role of gender, self-esteem was a strong predictor of the onset EDs symptomatology in both women and men (McCabe and Vincent, 2003; Cella et al., 2021).
Some studies found an interaction between self-esteem and different body attitudes. For example, Cella et al. (2021) observed that negative body feelings and body protection mediate the association between self-esteem and binge eating symptoms for both genders. Two more studies found the same effect regarding body shame (Iannaccone et al., 2016) and body dissatisfaction (Fortes et al., 2016). Thus, presenting negative body attitudes is related with low self-esteem scores and, consequently, a greater presence of disordered eating behaviors during adolescence.
Moreover, self-esteem was also related with other characteristics besides body attitudes. Jones et al. (2020) found that perfectionism was significantly associated with concerns about weight and body through self-esteem. Low scores in this variable were associated with higher scores on perfectionism and more concerns about weight in boys. Also, adolescents who perceived less affection presented lower self-esteem and more disordered eating behaviors (Unikel et al., 2013). Self-esteem also mediates the effect of family functioning and family preoccupation on weight and appearance, therefore participants with low self-esteem were more vulnerable to their family situation, and presented more negative eating behaviors (Leung et al., 1995). The association between self-esteem and EDs symptomatology was also mediated by psychological inflexibility, the adolescents with higher scores in this variable are the ones who presented a lower self-esteem and more likely to present disordered eating behaviors (Koushiou et al., 2020).
3.3.1.2. Body dissatisfaction and attitudes toward body
Body dissatisfaction and attitudes toward the body were also variables traditionally related to the onset of EDs symptomatology. Their relationship with self-esteem and the consequences in the presence of disordered eating behaviors has been analyzed (Fortes et al., 2016; Iannaccone et al., 2016; Cella et al., 2021).
Due to its relevance, 11 articles included body dissatisfaction as a variable of interest. It was observed in 8 studies that body dissatisfaction has been commonly associated with the appearance of EDs symptomatology, and that lower body dissatisfaction was related to a greater presence of disordered eating behaviors for both genders (Altamirano et al., 2011; Boone et al., 2014; Fortes et al., 2015; Garrusi et al., 2016; Teixeira et al., 2016; Cruz-Sáez et al., 2018; Macedo-Uchôa et al., 2019; Argydes et al., 2020; Pamies-Aubalat et al., 2022; Ćorić et al., 2023). This association was also significant in the only study with an entire sample of men (Garrusi et al., 2016).
Boone et al. (2014) also observed interaction effects between body dissatisfaction, personal standards perfectionism, and evaluative concerns perfectionism. Adolescents with higher scores on perfectionism variables presented higher scores in body dissatisfaction and, consequently, more overvaluation of their weight and shape, as well as more bulimic symptoms. The same relationship was found for self-oriented perfectionism in another study (Teixeira et al., 2016). Besides, Salafia and Lemer (2012) showed that high scores on body dissatisfaction were related with higher levels of different kinds of stress for women (family, relationship, and performance stress) and for men (performance, relationship, family, financial and educational stress). These participants were more likely to present dieting behaviors, and for women these behaviors could lead to bulimic symptoms. Cruz-Sáez et al. (2018) observed that the association between body dissatisfaction and disordered eating was mediated by negative self-esteem and negative affect for both genders.
Regarding attitudes toward the body, 7 studies found significant associations between these variables and EDs symptomatology. Negative perception of physical appearance (Costarelli et al., 2011), perception of body size (Gan et al., 2018), social physique anxiety (Gomes et al., 2015) and drive for thinness (Sepúlveda et al., 2021) were directly associated with symptoms of EDs. Argydes et al. (2020) found that overweight preoccupation and body dysphoria were risk factors, while body appreciation was identified as a protective factor for both genders. Li and Li (2021) also showed body esteem as a protective factor against the onset of EDs symptoms. One study showed the influence of media-ideal internalization on body shame and appearance anxiety was mediated by self-objectification for both genders, being the participants with higher scores on these variables and more likely to present dietary restraint or binge eating (Dakanalis et al., 2014). Finally, regular exercise was associated with psychological well-being and with a lower propensity for disordered eating behaviors in adolescents (Gomes et al., 2015).
3.3.1.3. Depression, anxiety, and stress
Because of the higher comorbidity between depression and eating disorders, their relationship has been widely studied. Concretely, 12 articles of this systematic review analyzed this association. Except for two studies (Unikel et al., 2013; Cruz-Sáez et al., 2018), depressive symptoms or negative affect presented a significant and strong association with the appearance of EDs symptomatology for both genders (McCabe and Vincent, 2003; Baylan et al., 2009; Kerremans et al., 2010; Rodgers et al., 2014; Fortes et al., 2015, 2016; Wade et al., 2015; Gan et al., 2018; Rosewall et al., 2018; Evans et al., 2019). Moreover, depressive symptoms lead to an easier internalization of esthetic ideal and developing disordered eating behaviors (Unikel et al., 2013). Previously, it has been analyzed as the mediator role of negative effect between body dissatisfaction and eating behaviors for both genders (Cruz-Sáez et al., 2018).
In the previous section, body dissatisfaction was a mediator between different kinds of stress with diet and bulimic symptoms (Salafia and Lemer, 2012). Zhu et al. (2016) also observed a direct association between life stress events and binge eating. Moreover, this relationship was stronger the higher the levels of impulsivity. Regarding anxiety, 3 studies found an influence of this variable on developing eating disorders for both genders (McCabe and Vincent, 2003; Costarelli et al., 2011; Bacopoulou et al., 2017). Concretely, McCabe and Vincent (2003) observed that anxiety was a strong predictor for bulimic symptoms in men and for extreme weight loss in both women and men.
3.3.1.4. Personal characteristics
High levels of perfectionism have been significantly associated with the onset of EDs symptomatology for both genders (McCabe and Vincent, 2003; Fortes et al., 2015; Teixeira et al., 2016). However, it also presented an indirect relation through self-esteem, mood intolerance (Jones et al., 2020) and body dissatisfaction (Boone et al., 2014). Two studies found a relationship between self-oriented perfectionism and disordered eating for girls (Rosewall et al., 2018; Sepúlveda et al., 2021). Rosewall et al. (2018) also observed an association of socially prescribed perfectionism, proving that social pressure could be a stronger predictor of EDs symptoms in women compared to men.
It has also been observed that other personal characteristics, such as high psychological inflexibility (Koushiou et al., 2020), low emotional intelligence (Li and Li, 2021) and interoceptive awareness (Kerremans et al., 2010) are associated with EDs symptomatology for both genders. Ineffectiveness (McCabe and Vincent, 2003) and covert delinquency (Kerremans et al., 2010) were observed only for men, while inhibited behavior and low effortful control were presented only for women (Kerremans et al., 2010). Obsessive compulsive symptoms were found to be a strong predictor for girls in two studies (Baylan et al., 2009; Sepúlveda et al., 2021). Finally, three studies showed an association between impulsivity and the development of disordered eating behavior during adolescence. In two of the studies, it was observed not only as a significant relationship but also a strong interaction with negative affect, and the negative affect reactivity groups presenting more symptoms of eating disorders for both genders (Wade et al., 2015; Evans et al., 2019). Zhu et al. (2016) showed that the relationship between life stress events and early maladaptive schemas in female and male adolescents was stronger when impulsivity was high, increasing the odds of presenting EDs symptoms.
3.3.1.5. Coping strategies
Two studies focused on analyzing the coping strategies of adolescents and their associations with the appearance of disordered eating behaviors Intropunitive avoidance, avoidance of social support (García-Grau et al., 2002) and escape-avoidance (Lee-Win et al., 2016) showed a direct association with EDs symptoms. Concretely, lifetime prevalence of binge eating was 1.13 times higher with escape-avoidance coping strategy (Lee-Win et al., 2016). These results were supported by Unikel et al. (2013), who included criticism in the analysis and found a positive association with internalization of thin ideal. Finally, two studies found that problem solving could be a protective coping strategy for disordered eating, especially for girls (García-Grau et al., 2002; Baylan et al., 2009).
3.3.2. Sociocultural and social media influence
Eleven articles showed significant associations between the exposure to sociocultural or social media and the onset of EDs symptomatology. Four studies, with 100% women, presented a significant relationship between sociocultural influence (Rodgers et al., 2014), media pressure (Fortes et al., 2016; Rosewall et al., 2018) and internalization of aesthetic thin ideal with disordered eating (Unikel et al., 2013).
Another five studies showed significant associations between media pressure and EDs symptoms according to gender. Argydes et al. (2020) found significant relationships between media pressure and EDs symptomatology in both women and men. Dakanalis et al. (2014) showed the influence of media-ideal internalization on body shame and appearance anxiety mediated by self-objectification for both genders. Two studies (Halliwell and Harvey, 2006; Pamies-Aubalat et al., 2022), found a significant indirect association between weight pressure and body dissatisfaction for both genders, mediated by social comparisons, pressure to lose weight and internalization. Concretely, the odds of presenting disordered eating behaviors increase in participants with higher scores on social comparisons. However, Macedo-Uchôa et al. (2019) only found a significant association between media pressure and EDs symptomatology for men (see Table 2).
Finally, Kaewpradub et al. (2017) conducted a study to analyze the influence of internet and social network use in EDs symptomatology. Moreover, Piko et al. (2023) found that adolescents with smartphone addiction presented more probabilities of developing EDs symptoms. Table 1 showed significant associations between these variables with eating problems, binge eating, purging behavior and taking laxatives.
3.3.3. Family and peers’ influence
Eight studies analyzed the influence of family variables on the appearance of EDs symptomatology.
Some protective factors against the appearance of disordered eating were identified, such as maternal care (Iannaccone et al., 2016), affective involvement (Baylan et al., 2009) and family cohesion (Gan et al., 2018). Specifically, Lee et al. (2018) showed family cohesion to be a positive mediator in the associations between tiredness, boredom, and stress with binge eating (see Table 2).
However, family variables such as paternal achievement oriented psychological control (Pace et al., 2018), parental overinvolvement, mother’s anxiety (Sepúlveda et al., 2021) and family stress (Salafia and Lemer, 2012) presented significant associations with EDs symptomatology. The chances of presenting disordered eating behaviors increase in the presence of these variables. In addition, poor family functioning and family concerns about weight and appearance are related, mediated by self-esteem and body dissatisfaction, with negative eating behaviors in adolescents (Leung et al., 1995; Table 2).
Regarding interpersonal relationships, seven studies identified the influence of these variables on eating behaviors. Perceived peer support was identified as a protective moderator in the relationship between paternal achievement oriented psychological control and EDs symptomatology (Pace et al., 2018; Piko et al., 2023). However, characteristics related with low-quality friendships such as conflicts among friends (Beckers et al., 2023), provide less self-validations, feelings of alienation and perception of less helpful friendships are associated with more probabilities of presenting symptoms of EDs (Sharpe et al., 2014). Moreover, peers’ negative attitudes against body and weight, experienced weight, or appearance teasing (Shomaker and Furman, 2009), and poor communication were more likely to lead to bulimia symptomatology (Shroff and Thompson, 2006).
Finally, being in a romantic adolescent relationship has been identified as another source of pressure and was associated with negative eating behaviors (Shomaker and Furman, 2009; Salafia and Lemer, 2012).
4. Discussion
This systematic review aimed to identify the risk factors for EDs symptomatology onset during adolescence, by focusing on both individual and environmental factors.
This study was conducted without limitations for years, in order to provide the most comprehensive overview about EDs risk factors. In fact, the oldest identified article is from almost 30 years ago and was focused on family characteristics and the association with EDs symptoms (Leung et al., 1995). Observations over the past decades, have shown a growing interest in this field, most likely due to the increasing prevalence rates, especially, at early ages (Smink et al., 2012; López, 2017; Galmiche et al., 2019). For that reason, the design of effective prevention and intervention programs has been a priority. However, up to now the proposals in that regard have not shown consistent effective results (Pratt and Woolfenden, 2002; Swanson et al., 2011; Fairburn et al., 2015; Stice et al., 2021).
Consequently, risk factors for EDs should be thoroughly analyzed to identify what is missing from current programs to achieve greater effectiveness, especially in terms of prevention. This systematic review has contributed to fill this gap, as it has identified that, although environmental risk factors (i.e., friends, family and society) were also found to be associated with ED occurrences, prevention programs mainly focus on characteristics like appearance, body weight, and body dissatisfaction, therefore reducing or removing the attention from other relevant areas (Stice et al., 2021). According to this data, the amount of research about the association of peers, family and society characteristics with EDs symptomatology during adolescence are reduced, compared to that of studies about individual characteristics and EDs. For example, from the 47 included studies in this systematic review, only 10 (Halliwell and Harvey, 2006; Unikel et al., 2013; Dakanalis et al., 2014; Rodgers et al., 2014; Fortes et al., 2016; Kaewpradub et al., 2017; Rosewall et al., 2018; Macedo-Uchôa et al., 2019; Argydes et al., 2020; Pamies-Aubalat et al., 2022), eight (Leung et al., 1995; Baylan et al., 2009; Salafia and Lemer, 2012; Iannaccone et al., 2016; Gan et al., 2018; Lee et al., 2018; Pace et al., 2018; Sepúlveda et al., 2021) and six (Shroff and Thompson, 2006; Shomaker and Furman, 2009; Salafia and Lemer, 2012; Sharpe et al., 2014; Pace et al., 2018; Beckers et al., 2023) studied the relationship between society, family and peers with disordered eating behaviors, respectively.
Regarding society, women have always been under more pressure to pursue unrealistic and unattainable appearance ideals. Normally, the standards promoted by current society were based on extreme thinness and looking perfect, and these characteristics were associated with success. The promotion of the thin-ideal and the rejection of other body shapes leaded to a greater body dissatisfaction and the practice of behaviors like dieting, purging or restrictions (Izydorczyk and Sitnik-Warchulska, 2018; Dondzilo et al., 2019). For those reasons, research in this area has focused on women, especially adolescents. In this systematic review, 33 of the included studies had a sample composed entirely or mostly by females. However, in recent years, the investigation with male samples has increased, finding no significant differences compared to women, for the association between sociocultural or media influence with EDs symptomatology (Halliwell and Harvey, 2006; Dakanalis et al., 2014; Kaewpradub et al., 2017; Macedo-Uchôa et al., 2019; Argydes et al., 2020).
In the past decades, communication media was the main way to promote the unrealistic aesthetic ideal (Unikel et al., 2013; Rodgers et al., 2014; Fortes et al., 2016; Rosewall et al., 2018; Macedo-Uchôa et al., 2019; Argydes et al., 2020). However, in recent years, internet and social networking sites have increased and intensified the internalization process of the thin-ideal and social comparisons (Halliwell and Harvey, 2006; Kaewpradub et al., 2017; Pamies-Aubalat et al., 2022). The access to the information and unrealistic aesthetic models are easier and faster, based on an immediate reward system. For example, the use of Instagram in the lockdown was associated with an increase of body dissatisfaction and drive for thinness among young people, who followed more appearance-focused accounts (Vall-Roqué et al., 2021). Therefore, it seems that the education to use social networking sites, personal empowerment, and a correct interpretation of the media information with respect to appearance should be pillars in the EDs prevention programs. The inclusion of these factors could prevent the appearance of body dissatisfaction, body shame or self-objectification symptoms, which are commonly associated with the onset of EDs symptoms (Dakanalis et al., 2014; Saunders et al., 2020).
Considering this information, not only the individual is exposed to the current society, but also their closest and most significant circle, family, and peers. Therefore, the relationship and interactions between the adolescent with their family and peers have been identified as another risk factor of EDs symptomatology (Leung et al., 1995; Shroff and Thompson, 2006; Baylan et al., 2009; Shomaker and Furman, 2009; Salafia and Lemer, 2012; Sharpe et al., 2014; Iannaccone et al., 2016; Gan et al., 2018; Lee et al., 2018; Pace et al., 2018; Sepúlveda et al., 2021). For that reason, family concerns about weight and appearance were associated with features such as low self-esteem (Leung et al., 1995). Also, parental characteristics, like mothers’ anxiety, or parenting styles, such as overinvolvement or psychological control, were associated with more presence of disordered eating behaviors (Salafia and Lemer, 2012; Pace et al., 2018; Sepúlveda et al., 2021). However, there is no agreement about the role of family factors for the onset of EDs symptomatology. Evidence supports that these factors are associated with the exacerbation and maintenance of the symptoms (Sepúlveda et al., 2021).
Furthermore, characteristics like maternal care (Iannaccone et al., 2016), affective involvement (Baylan et al., 2009) and family cohesion (Gan et al., 2018; Lee et al., 2018) were identified as protective factors against disordered eating. It appears that more cohesive families are likely to promote a more stable environment, which in turn is associated with characteristics necessary to deal with the influences of current society, such as higher self-esteem.
However, the influence of peers during adolescence could be just as significant as that of the family. In fact, peer support could be a protective factor of the appearance of EDs symptoms for adolescents whose parents own a controlling parenting style. These individuals perceive the positive reinforcement they need in their equal relationships (Pace et al., 2018; Piko et al., 2023). On the contrary, low-quality relationships based on lack of support, feeling alienated or less self-validation have been identified as risk factors of EDs (Sharpe et al., 2014; Beckers et al., 2023). Moreover, adolescents have been identified as a common audience of appearance-focused accounts on social networking sites (Vall-Roqué et al., 2021) which could lead to exacerbate negative attitudes against weight and body, even suffering from appearance teasing and poor communication (Shroff and Thompson, 2006; Shomaker and Furman, 2009).
In addition to friendship relationships, adolescence is also characterized at the beginning of romantic relationships. This has been identified as another source of pressure, as adolescents desire to be liked by others (Shomaker and Furman, 2009; Salafia and Lemer, 2012). When pursuing to fulfill this need, they may take celebrities as reference. Therefore, they could practice negative behaviors, normally related to EDs symptomatology, with the aim of mirroring famous people who promote unrealistic aesthetic ideals (Unikel et al., 2013; Rodgers et al., 2014; Fortes et al., 2016; Rosewall et al., 2018; Macedo-Uchôa et al., 2019; Argydes et al., 2020). Consequently, the development and the maintenance of EDs symptoms could be reduced if relationships and aesthetic ideals were included in prevention programs, together with training strategies oriented to family members and preparing them to cope with the problem (Moreno-Encinas et al., 2021).
Adolescence is a period characterized by identity formation and emerging independence. Many significant constructs like self-esteem, self-concept, or self-efficacy play an important role in this period. For that reason, it is relevant to develop these characteristics, so they are adaptive and useful for managing stressful events and preventing the onset of psychological problems like EDs (Bardone-Cone et al., 2018). The relevance of individual characteristics in the appearance of EDs symptomatology has promoted a great deal of research in this area. However, this systematic review also showed that the inner circle and the society are key risk factors. For example, if parents were trained in emotion-regulation skills, they could teach these abilities to their children in a more adaptive way. Likewise, if family and friends provide a cohesive, supportive, and validating environment, the likelihood of developing ED symptoms will be reduced. The adolescent is more likely to develop protective personal variables such as strong self-esteem and self-concept. Therefore, the influence of society will have less power, having more skills to manage the pressures to achieve an unrealistic and unhealthy ideal of beauty. If adolescents feel safe in their immediate circle, they will have to make less efforts to try to fit into social standards (Lafrance et al., 2015; Moreno-Encinas et al., 2021).
Regarding individual characteristics, self-esteem has been identified as an essential factor in the appearance of EDs symptoms (Shroff and Thompson, 2006; Baylan et al., 2009; Rodgers et al., 2014; Garrusi et al., 2016; Kaewpradub et al., 2017; Argydes et al., 2020; Mora et al., 2022; Beckers et al., 2023). Therefore, low self-esteem during adolescence showed a significant association with EDs for both genders (McCabe and Vincent, 2003; Altamirano et al., 2011; Gomes et al., 2015; Teixeira et al., 2016; Gan et al., 2018; Rosewall et al., 2018; Jones et al., 2020; Zamani et al., 2020; Cella et al., 2021; Ćorić et al., 2023). However, self-esteem was also a moderator between other characteristics and EDs, especially body dissatisfaction or attitudes toward the body. These characteristics also presented a significant association with EDs (Altamirano et al., 2011; Costarelli et al., 2011; Boone et al., 2014; Fortes et al., 2015; Gomes et al., 2015; Garrusi et al., 2016; Teixeira et al., 2016; Cruz-Sáez et al., 2018; Gan et al., 2018; Macedo-Uchôa et al., 2019; Argydes et al., 2020; Ćorić et al., 2023). This systematic review showed how society could lead to pursue unattainable appearance ideals, failure to achieve these unrealistic goals and the comparisons with models or peers could lead to body dissatisfaction or negative attitudes toward the body (Fortes et al., 2016; Iannaccone et al., 2016; Cella et al., 2021). It has been observed that adolescents with higher self-esteem presented less internalization of the thin-ideal and consequently less probabilities of developing disordered eating behaviors (Bardone-Cone et al., 2018). The presence of low self-esteem and poor family functioning has also influenced the onset of EDs symptoms. Adolescents living in an invalidating environment or being victims of appearance teasing tend to present lower self-esteem and more probabilities of developing negative eating behaviors (Leung et al., 1995; Unikel et al., 2013).
Self-esteem (Jones et al., 2020), body dissatisfaction and attitudes toward body (Boone et al., 2014; Teixeira et al., 2016) were also influenced by perfectionism (McCabe and Vincent, 2003; Fortes et al., 2015; Teixeira et al., 2016), psychological inflexibility (Koushiou et al., 2020) or obsessive-compulsive symptoms (Baylan et al., 2009; Sepúlveda et al., 2021). These associations could be related to establishing unrealistic goals or expectations. Moreover, society, family, and peers could be pressuring the adolescent to pursue those goals (Rosewall et al., 2018). This pressure could lead to obsessive-compulsive behaviors to achieve weight and appearance ideals (Baylan et al., 2009; Sepúlveda et al., 2021). Consequently, body dissatisfaction and negative body attitudes increase as well as the probabilities of developing disordered eating behaviors (Boone et al., 2014; Teixeira et al., 2016; Jones et al., 2020; Koushiou et al., 2020).
However, perfectionism was not the only personal characteristic identified as a risk factor of EDs symptomatology. Ineffectiveness and covert delinquency (McCabe and Vincent, 2003; Kerremans et al., 2010) were associated with disordered eating in men, while inhibited behavior and low effortful control were the features observed in women (Kerremans et al., 2010). Low emotional intelligence was identified as a risk factor for both genders, supporting the individuals with non-adaptive emotion-regulation skills are likely to use strategies like maladaptive eating behaviors to cope with stressful situations (Li and Li, 2021). Impulsivity was analyzed in three studies of this systematic review, being a risk factor for both genders. This trait mediated the relationship between life stress and negative affect with disordered eating, the participants with more symptomatology were those in the negative affect reactivity groups (Wade et al., 2015; Zhu et al., 2016; Evans et al., 2019). In fact, negative affect has been associated with EDs symptoms, playing a relevant role in the internalization of the aesthetic ideal and appearing normally after body dissatisfaction. The dissonance generated between the ideal and the failure to achieve it despite the efforts made leads to not only negative affect (McCabe and Vincent, 2003; Baylan et al., 2009; Kerremans et al., 2010; Rodgers et al., 2014; Fortes et al., 2015, 2016; Wade et al., 2015; Gan et al., 2018; Rosewall et al., 2018; Evans et al., 2019), also high levels of anxiety and stress (McCabe and Vincent, 2003; Costarelli et al., 2011; Salafia and Lemer, 2012; Zhu et al., 2016; Bacopoulou et al., 2017). Therefore, if adolescents are in a period of changing, living in a society focused on thinness and feeling the pressure from their closest circle, they should present active and adaptive coping strategies to face this reality. However, growing in an unsupportive environment which tends to judge appearance leads to develop passive coping strategies, normally related to EDs symptomatology. Intropunitive avoidance, criticism, avoidance of social support and escape-avoidance have been associated with the greater presence of disordered eating behaviors (García-Grau et al., 2002; Unikel et al., 2013; Lee-Win et al., 2016).
This systematic review showed an integrative and comprehensive update on the risk factors that are more likely to lead to EDs symptoms during adolescence. The Supplementary material of this article provides an additional figure to understand the interaction between risk factors. The results presented data from the last 3 decades, from 21 different countries and for both genders, observing non relevant differences by these two variables. Besides, most studies showed a high methodological quality. Although the risk factors for EDs symptomatology have been extensively studied, more research is needed to fully understand the interplay between society, inner circle, and individual characteristics. It has been observed that the etiology of these disorders is complex and involves many factors. However, prevalence rates are still growing, especially at early ages (Smink et al., 2012; López, 2017; Galmiche et al., 2019). Intervention programs have not shown consistent results of long-term effectiveness and up to 80% of people with an ED do not receive an appropriate intervention (Pratt and Woolfenden, 2002; Swanson et al., 2011; Fairburn et al., 2015; Stice et al., 2021). For these reasons, research and constant updating are essential in this area, to identify current gaps and design innovative prevention programs. Knowing the risk factors and the interaction between them, the inclusion of family members in treatments is essential. Training in emotional management and parenting skills is a fundamental point to include in treatments. Furthermore, the integration of these tools in the school dynamics, involving peers and families, could be a measure to take into account from the political sphere. In this way, in addition to information about EDs, practical tools would be provided for adolescents to form their identity in environments where cohesion, support and validation predominate. At the same time, parents could be trained to set limits in a way that is assertive and tolerant, rather than authoritarian and/or overprotective. Moreover, expanding the training offer for healthcare professionals including family and peer therapy would also be a measure to consider. For example, the New Maudsley Method is a novel approach that has demonstrated positive results when administered to parents. This strategy involves training parenting skills in the treatment of disorders. This training method and its extension, including skills for dealing with peers and social pressures, could be a current and innovative solution (Toubøl et al., 2019).
4.1. Implications and limitations
Future directions could focus primarily on prevention. With the provision of psychoeducational information by experts in secondary schools, not only for the adolescents but also for educators and families, and the training to promote a safe environment at both school and home, where adolescents can develop and explore their identities and notice the warning signs of the EDs’ onset as soon as possible. The consideration of biological and genetic risk factors involved in EDs could provide a more comprehensive explanation of the onset of these disorders. In this regard, early identification has been associated with a better prognosis (Le Grange and Loeb, 2007). Thus, improvement is needed in intervention programs, especially regarding prevention, which should include in a relevant way the society, family, and peers’ relationships, as well as individual characteristics beyond weight and appearance. Another gap that should be covered is the inclusion of the adolescents’ environments in these programs, to inform about the risks, management of these situations, and effectively prevent them from homes and schools.
Despite its implications and strengths, this systematic review has some limitations. Firstly, although the included studies have analyzed the risk factors for both genders, there are other studies that have only focused on the female population. It’s true that this population has traditionally been more affected by EDs; however, increasing prevalence rates of these problems are also being observed in men. For this reason, further studies involving both genders are required. Secondly, there are more cross-sectional than longitudinal studies included in this review. This type of studies is needed to understand the onset and progression of EDs, as well as testing the long-term effectiveness of prevention and intervention programs. Longitudinal studies require more resources and time, but this type of analysis is also necessary to capture the relative importance that risk factors have at different stages of adolescence. This information could be very useful to identify the risk factors involved in the onset and early stages of EDs. This early identification would allow an earlier and more effective action in terms of prevention and intervention, with the possibility of customize programs to adapt them to specific needs, providing the most appropriate resources in relation to the age of the participant.
The third limitation is that, biological factors were not included, as we focused on psychological factors with the aim to provide information for designing more effective prevention and intervention programs. However, as this may limit the scope of conclusions of this systematic review, future research could include biological factors. Setting of the reviewed studies was another limitation that could bias interpretation and generalization of results: as there were no country restrictions during the search, the included studies are mostly from Europe. However, significant differences were not found in terms of country or culture. Therefore, it seems that beauty ideals are increasingly similar through diverse societies. Since individual risk factors are similar in all cultures, for example, low self-esteem has been seen as a risk factor in most of the articles included. Studies that have analyzed sociocultural, family and peer influences are mostly located in Western societies. However, this only indicates that these variables have been more studied in these places, and that more research is needed into these factors in a wider range of countries. Finally, most of the studies were focused on one area, namely, society, the inner circle, or individual characteristics. To widen the knowledge on the interplay between these three areas in the etiology of EDs, more studies should be carried out in a more integrative and comprehensive way.
To conclude, in future lines of research, the implementation of randomized controlled and longitudinal trials is recommended, specifically, to test and validate the effectiveness of new treatments and prevention programs for EDs. Primarily, these programs should focus on the psychological variables identified as risk factors, rather than aspects related to food or body shape. Furthermore, the role that parents play as a fundamental part of the treatment must be considered; in accordance, parents can not only provide support, but also act as therapists if trained on emotional and parenting skills. Likewise, the inclusion of the management of social pressures, the media and relationships with peers should be relevant elements within treatment and prevention.
5. Conclusion
In conclusion, adolescence has traditionally been regarded as a period of changing and identity formation. Adolescents are vulnerable to develop psychological problems if they do not feel they are in a safe environment to define a stable self-concept and self-esteem (Bardone-Cone et al., 2018). This systematic review has shown the importance of including society, family, and peers relationships in interventions and also prevention programs. It is essential that adolescents know the current society and the continuous unrealistic information that people receive about having the perfect body or appearance, and the dangerous behaviors promoted to achieve these goals. It has also been identified that the individual needs to feel affection, support, and cohesion in the family. Moreover, adolescents need to learn how to develop healthy romantic relationships characterized by validation and positive reinforcement. Considering these aspects from an early age, it is likely that the adolescent develops a stronger self-esteem with less possibility of showing high body dissatisfaction. Consequently, negative affect, anxiety, stress, and personal associated traits are likely to result in a more adaptive way, using protective coping strategies such as problem solving. Understanding the etiology of EDs in a comprehensive way could not only have scientific implications but also clinical, for designing innovative and integrative prevention and intervention programs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not necessary for the current systematic review as no new participants were recruited for the purpose of the research. However, this study is part of a larger project, approved by the ethical standards of Bioethics Committee of the University Isabel I (Reference: FUI1-014).
Author contributions
CV, ÁH, MT-S, AJ-G, BM, PR-F, YV-H, and LR-S contributed to design the systematic review. CV designed and conducted the search strategy. CV, ÁH, and MT-S carried out independently the title-abstract and full-text screening. Disparities were solved by discussion. All authors contributed to write the manuscript and approved the submitted version.
Funding
This study is part of a larger project with reference FUI1-014. The project was funded by the “la Caixa” Foundation and the “Caja de Burgos” Foundation, under the agreement LCF/PR/PR18/51130008.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1221679/full#supplementary-material
References
Altamirano, M. B., Vizmanos, B., and Unikel, C. (2011). Continuum of risky eating behaviors in Mexican adolescents. Rev. Panam. Salud Publica 30, 401–407. doi: 10.1590/s1020-49892011001100001
American Psychiatry Association (2013). Guía de consulta de los criterios diagnósticos del DSM-5 [Diagnostic and statistical manual of mental disorders: DSM-5]. Washington: American Psychiatry Publishing.
Argydes, M., Anastasiades, E., and Alexiou, E. (2020). Risk and protective factors of disordered eating in adolescents based on gender and body mass index. Int. J. Environ. Res. Public Health 17:9238. doi: 10.3390/ijerph17249238
Bachar, E., Gur, E., Canetti, L., Berry, E., and Stein, D. (2010). Selflessness and perfectionism as predictors of pathological eating attitudes and disorders: a longitudinal study. Eur. Eat. Disorders Rev. 18, 496–506. doi: 10.1002/erv.984
Bacopoulou, F., Foskolos, E., Stefanaki, C., Tsitsami, E., and Vousoura, E. (2017). Disordered eating attitudes and emotional/behavioral adjustment in Greek adolescents. Eat. Weight Disord. 23, 621–628. doi: 10.1007/s40519-017-0466-x
Barakat, S., McLean, S. A., Bryant, E., le, A., and Marks, P., National Eating Disorder Research Consortium (2023). Risk factors for eating disorders: findings from a rapid review. J. Eat. Disord. 11:8. doi: 10.1186/s40337-022-00717-4
Bardone-Cone, A. M., Thompson, K. A., and Miller, A. J. (2018). The self and eating disorders. J. Pers. 88, 59–75.
Baylan, G., Erol, A., and Kilicoglu, A. (2009). Predictors of Anoretic and bulimic symptoms in adolescent girls. Klinik Psikofarmakol. Bülteni. 19, 407–413.
Beckers, D., Laresen, J. L., and Burk, W. J. (2023). Self-esteem and negative affectivity as mediators of the prospective links between adolescent interpersonal peer problems and disordered eating behaviors. Appetite 186:106558. doi: 10.1016/j.appet.2023.106558
Boone, L., Soenens, B., and Luyten, P. (2014). When or why does perfectionism translate into eating disorder pathology? A longitudinal examination of the moderating and mediation role of body dissatisfaction. J. Abnorm. Psychol. 123, 412–418. doi: 10.1037/a0036254
Cardi, V., Mallorqui-Bague, N., Albano, G., Monteleone, A. M., Fernandez-Aranda, F., and Treasure, J. (2018). Social difficulties as risk and maintaining factors in anorexia nervosa: a mixed-method investigation. Front. Psych. 9:e0012. doi: 10.3389/fpsyt.2018.00012
Cella, S., Cipriano, A., Aprea, C., and Cotrufo, P. (2021). Self-esteem and binge eating among adolescent boys and girls: the role of body disinvestment. Int. J. Environ. Res. Public Health 18:7496. doi: 10.3390/ijeph18147496
Cerniglia, L., Cimino, S., Tafà, M., Marzilli, E., Ballarotto, G., and Bracaglia, F. (2017). Family profiles in eating disorders: family functioning and psychopathology. Psychol. Res. Behav. Manag. 10, 305–312. doi: 10.2147/PRBM.S145463
Ćorić, M. K., Graovac, M., Pravdić, N., Raguž, A. B., and Kaštelan, A. (2023). Predictive factors of disordered eating among adolescents in Bosnia and Herzegovina. J. Educ. Health Promot. 12:258. doi: 10.4103/jehp.jehp_1560_22
Costarelli, V., Antonopoulou, K., and Mavrovounioti, C. (2011). Psychosocial characteristics in relation to disordered eating attitudes in Greek adolescents. Eur. Eat. Disorders Rev. 19, 322–330. doi: 10.1002/erv.1030
Cruz-Sáez, S., Pascual, A., Wlodarczyk, A., and Echeburúa, E. (2018). The effect of body dissatisfaction on disordered eating: the mediating role of self-esteem and negative affect in male and female. J. Health Psychol. 25, 1098–1108. doi: 10.1177/1359105317748734
Dakanalis, A., Carrà, G., Calogero, R. M., Fida, R., Clerici, M., Zanetti, M. A., et al. (2014). The developmental effects of media-ideal internalization and self-objectification processes on adolescents’ negative body-feelings, dietary restraint, and binge eating. Eur. Child Adolesc. Psychiatry 24, 997–1010. doi: 10.1007/s00787-014-0649-1
Dondzilo, L., Rieger, E., Jayawarden, N., and Bell, J. (2019). Drive for thinness versus fear of fat: approach and avoidance motivation regarding thin and non-thin images in women. Cognit. Ther. Res. 43, 585–593. doi: 10.1007/s10608-018-9989-3
Evans, B. C., Felton, J. W., Lagacey, M. A., Manasse, S. M., Lejuez, C. W., and Juarascio, A. S. (2019). Impulsivity and affect reactivity prospectively predict disordered eating attitudes in adolescents: a 6-year longitudinal study. Eur. Child Adolesc. Psychiatry 28, 1193–1202. doi: 10.1007/s00787-018-01267-4
Fairburn, C., Bailey-Straebler, S., Basden, S., Doll, H., Jones, R., Murphy, R., et al. (2015). A transdiagnostic comparison of enhanced cognitive behaviour therapy (CBT-E) and interpersonal psychotherapy in the treatment of eating disorders. Behav. Res. Ther. 70, 64–71. doi: 10.1016/j.brat.2015.04.010
Fairburn, C. G., Cooper, Z., and Shafran, R. (2003). Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behav. Res. and Ther. 41, 509–528. doi: 10.1016/s0005-7967(02)00088-8
Fortes, L. S., Amaral, A. C. S., Almeida, S. S., and Ferreira, M. E. C. (2013). Efeitos de variáveis psicológicas, morfológicas e sociodemográficas sobre comportmento alimentar de adolescentes. Rev. Paul. Ped. 31, 182–188. doi: 10.1590/S0103-05822013000200008
Fortes, L. S., Filgueiras, J. F., Oliveria, F. C., Almieda, S. S., and Ferreira, M. E. C. (2016). Etiological model of disordered eating behaviors in Brazilian adolescent girls. Cad. Saude Publica 32: e000024115. doi: 10.1590/0102-311X00024115
Fortes, L. S., Meireles, J. F. F., Neves, C. M., Almeida, S. S., and Ferreira, M. E. C. (2015). Disordered eating, body dissatisfaction perfectionism, and mood state in female adolescents. Rev. Nutri. Campinas. 28, 371–383. doi: 10.1590/1415-52732015000400004
Gaete, V., and López, C. (2020). Trastornos de la conducta alimentaria en adolescentes. Una mirada integral [Eating disorders in adolescents. A comprehensive approach]. Rev. Chil. Pediatr. 91, 784–793. doi: 10.32641/rchped.vi91i5.1534
Galmiche, M., Déchelotte, P., Lambert, G., and Tavolacci, M. P. (2019). Prevalence of eating disorders over the 2000-2018 period: a systematic literature review. Am. J. Clin. Nutr. 109, 1402–1413. doi: 10.1093/ajcn/nqy342
Gan, W. Y., Mohamad, N., and Law, L. S. (2018). Factors associated with binge eating behavior among Malaysian adolescents. Nutrients 10:66. doi: 10.3390/nu1001006
García-Grau, E., Fusté, A., Miró, A., Saldaña, C., and Bados, A. (2002). Coping style and Distrubed eating attitudes in adolescent girls. Int. J. Eat. Disord. 32, 116–120. doi: 10.1002/eat.10060
Garrusi, B., Baneshi, M. R., and Pakgohar, M. (2016). Eating disorders among Iranian male adolescents. Iran J. Pyschiatry Behav. Sci. 10:e5352. doi: 10.17785/ijpbs-5352
Gibson, D., Workman, C., and Mehler, P. S. (2019). Medical complications of anorexia nervosa and bulimia nervosa. Psychiatr. Clin. N. Am. 42, 263–274. doi: 10.1016/j.amjmed.2015.06.031
Gismero-González, M. E. (2020). Factores de riesgo psicosociales en los Trastornos de la Conducta Alimentaria: Una revisión y algunas consideraciones Para la prevención y la intervención [psychosocial risk factors for eating disorders: a review and some considerations for prevention and intervention]. Revista de Psicoterapia. 31, 33–47. doi: 10.33898/rdp.v31i115.354
Gomes, R., Gonçalves, S., and Costa, J. (2015). Exercise, eating disordered behaviors and psychological well-being: a study with Portuguese adolescents. Rev. Latinoam. Psicol. 47, 66–74. doi: 10.1016/S0120-0534(15)30008-X
Grooten, W. J. A., Tseli, E., Äng, B. O., Boersma, K., Stånacke, B. M., Gerdle, B., et al. (2019). Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS-aspects of interrater agreement. Diagn. Progn. Res. 3, 5–11. doi: 10.1186/s41512-019-0050-0
Halliwell, E., and Harvey, M. (2006). Examination of a sociocultural model of disordered eating among male and female adolescents. Br. J. Health Psychol. 11, 235–248. doi: 10.1348/1359070X39214
Hambleton, A., Pepin, G., Le, A., Maloney, D., Touyz, S., and Maguire, S. (2022). Psychiatric and medical comorbidities of eating disorders: findings from a rapid review of the literature. J. Eat. Disord. 10, 132–123. doi: 10.1186/s40337-022-00654-2
Higgins, J., and Green, S. (2008). Cochrane handbook for systematic reviews of interventions. The Cochrane collaboration. Chichester: John Wiley & Sons.
Iannaccone, M., D’Olimpio, F., Cella, S., and Cotrufo, P. (2016). Self-esteem, body shame and eating disorder risk in obese and normal weigth adolescents: a mediation model. Eat. Behav. 21, 80–83. doi: 10.1016/j.eatbeh.2015.12.010
Izydorczyk, B., and Sitnik-Warchulska, K. (2018). Sociocultural appearance standards and risk factors for eating disorders in adolescents and women of various ages. Front. Psychol. 9:e00429. doi: 10.3389/fpsyg.2018.00429
Jones, E. J., Egan, S. J., Howell, J. A., Hoiles, K. J., and Mazzucchelli, T. G. (2020). An examination of the transdiagnostic cognitive-behavioural model of eating eating disorders in adolescents. Eat. Behav. 39:101445. doi: 10.1016/j.eatbeh.2020.101445
Kaewpradub, N., Kiatrungrit, K., Hongsanguansri, S., and Pavasuthipaisit, C. (2017). Association among internet usage, body image and eating behaviors of secondary school students. Shanghai Arch. Psychiatry 29, 208–217. doi: 10.11919/j.issn.1002-0829.216092
Kerremans, A., Claes, L., and Bitjttebier, P. (2010). Disordered eating in adolescent males and females: associations with temperament, emotional and behavioral problems and perceived self-competence. Pers. Individ. Differ. 49, 955–960. doi: 10.1016/j.paid.2010.08.003
Koushiou, M., Loutsiou, A., and Karekla, M. (2020). Eating disorders among middle-school students: the role of psychological inflexibility and self-esteem. J. Sch. Educ. Psychol. 9, S58–S68. doi: 10.1080/21683603.2020.1742259
Lafrance, A., Dolhanty, J., and Greenberg, L. (2015). Emotion-focused family therapy for eating disorders in children and adolescents. Clin. Psychol. Psychother. 22, 75–82. doi: 10.1002/cpp.1861
Laporta, I., Delgado, M., Reboyar, S., and Lahuerta, C. (2020). Perfectionism in adolescents with eating disorders. Eur J Health Research. 6, 97–107. doi: 10.30552/ejhr.v6i1.205
Lazo, Y., Quenaya, A., and Mayta-Tristán, P. (2015). Influencia de los medios de comunicación y el riesgo de padecer trastornos de la conducta alimentaria en escolares mujeres en Lima, Perú. Arch. Argent. Pediatr. 113, 519–525. doi: 10.5546/aap.2015.519
Le Grange, D., and Loeb, K. (2007). Early identification and treatment of eating disorders: prodrome to syndrome. Early Interv. Psychiatry 1, 27–39. doi: 10.1111/j.1751-7893.2007.00007.x
Lee, A. Y., Reynolds, K. D., Stacy, A., Niu, Z., and Xie, B. (2018). Family functioning, moods, and binge eating among urban adolescents. J. Behav. Med. 42, 511–521. doi: 10.1007/s10865-018-9994-8
Lee-Win, A. E., Townsend, L., Reinblatt, S. P., and Mendelson, T. (2016). Associations of neuroticism-impulsivity and coping with binge eating in a nationally representative sample of adolescents in the United States. Eat. Behav. 22, 133–140. doi: 10.1016/j.eatbeh.2016.06.009
Leung, F., Schwartzman, A., and Steiger, H. (1995). Testing a dual-process family model in understanding the development of eating pathology: a structural equation modeling analysis. Int. J. Eat. Disord. 20, 367–375. doi: 10.1002/(SICI)1098-108X(199612)20:4<367::AID-EAT4>3.0.CO;2-L
Li, Y., and Li, J. (2021). The boundary conditions by which body-esteem leads to eating disorders risk among adolescents. J. Gen. Psychol. 149, 97–115. doi: 10.1080/00221309.2021.1915741
López, A. P. S. (2017). Prevalencia de trastornos de la conducta alimentaria en seis países europeos. Metas de enfermería [Prevalence of eating behaviour disorders in six European countries]. 20:9. doi: 10.35667/MetasEnf.2019.20.1003081094
López, C., and Treasure, J. (2002). Eating disorders in adolescents: description and management. Rev. Méd. Clín. Las Condes. 22, 85–97. doi: 10.1016/S0716-8640(11)70396-0
Macedo-Uchôa, F. N., Macêdo-Uchôa, N., Medeiros da Costa-Daniele, T., Pinheiro-Lustosa, R., Domingos-Garrido, N., Figueiredo-Deana, N., et al. (2019). Influence of the mass media and body dissatisfaction on the risk in adolescents of developing eating disorders. Int. J. Environ. Res. Public Health 16:1508. doi: 10.3390/ijerph16091508
McCabe, M. P., and Vincent, M. A. (2003). The role of biodevelopmental and psychological factors in disordered eating among adolescent males and females. Eur. Eat. Disorders. Rev. 11, 315–328. doi: 10.1002/erv.500
Monell, E., Clinton, D., and Bigegard, A. (2018). Emotion dysregulation and eating disorders- associations with diagnostic presentation and key symptoms. Int. J. Eat. Disord. 51, 921–930. doi: 10.1002/eat.22925
Moola, S., Munn, Z., Sears, K., Sfetcu, R., Currie, M., Lisy, K., et al. (2015). Conducting systematic reviews of association (etiology): the Joanna Briggs Institute’s approach. Int. J. Evid. Based Healthc. 13, 163–169. doi: 10.1097/XEB.0000000000000064
Mora, F., Álvarez-Mon, M. A., Fernández-Rojo, S., Ortega, M. A., Félix-Alcántara, M. P., Morales-Gil, I., et al. (2022). Psychosocial factors in adolescence and risk of development of eating disorders. Nutrients 14:1481. doi: 10.3390/nu14071481
Moreno-Encinas, A., Graell, M., Martínez-Huertas, M. F., Treasure, J., and Sepúlveda, A. R. (2021). Adding maintaning factors to develpmental models of anorexia nervosa: an emprical examination in adolescents. Eur. Eat. Disorders. Res. 29, 548–558. doi: 10.1002/erv.2826
Nuño-Gutiérrez, B. L., Celis-de la Rosa, A., and Unikel-Santoncini, C. (2009). Prevalence and associated factors related to disordered eating in student adolescents of Guadalajara across sex. Rev. Investig. Clin. 61, 286–293.
O’Brien, K. M., Whelan, D. R., Sandler, D. P., Hall, J. E., and Weinberg, C. R. (2017). Predictors and long-term health outcomes of eating disorders. PLoS One 12:e0181104. doi: 10.1371/journal.pone.0181104
Pace, U., D’Urso, G., and Zappulla, C. (2018). Negative eating attitudes and behaviors among adolescents: the role of parental control and perceived peer support. Appetite 121, 77–82. doi: 10.1016/j.appet.2017.11.001
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. Brit. Med. J. 372:n160. doi: 10.1136/bmj.n160
Pamies, L., and Quiles, Y. (2014). Perfectionism and risk factors for the development of eating disorders in Spanish adolescents of both genders. An. de Psicol. 30, 620–626. doi: 10.6018/analesps.30.2.158441
Pamies-Aubalat, L., Quiles, Y., and Torregrosa, M. L. (2022). Psychosocial profle related to disordered eating attitudes in Spanish adolescents. Curr. Psychol. 42, 20193–20202. doi: 10.1007/s12144-022-03164-1
Piko, B. F., Patel, K., and Kiss, H. (2023). Risk of disordered eating among a sample of Indian adolescents: the role of online activity. Soc. Anx. Soc. Supp. 18, 315–321. doi: 10.1177/09731342231163391
Pratt, B. M., and Woolfenden, S. (2002). Interventions for preventing eating disorders in children and adolescents. Cochrane Database Syst. Rev. 2002. doi: 10.1002/14651858.CD002891
Rodgers, R. F., Paxton, S. J., and McLean, S. A. (2014). A biopsychosocial model of body image concerns in early adolescent girls. J. Youth Adolesc. 43, 814–823. doi: 10.1007/s10964-013-0013-7
Rosewall, J. K., Gleaves, D. H., and Latner, J. D. (2018). An examination of risk factors that moderate the body dissatisfaction-eating pathology relationship among New Zealand adolescent girls. J. Eat. Disord. 6:38. doi: 10.1186/s40337-018-0225-z
Salafia, E. H., and Lemer, J. L. (2012). Associations between multiple types of stress and disordered eating among girls and boys in middle school. J. Child Fam. Stud. 21, 148–157. doi: 10.1007/s10826-011-9458-z
Saunders, J. F., Eaton, A. A., and Aguilar, S. (2020). From self(ie)-objectification to self-empowerment: the meaning of selfies on social media in eating disorder recovery. Comput. Hum. Behav. 111:106420. doi: 10.1016/j.chb.2020.106420
Semenova, N., Slobodskaya, H., and Rezun, E. (2022). Suicidal behavior in adolescent girls with eating disorders. Eur. Psychiatry 64, S32–S38. doi: 10.3109/08039480903265751
Sepúlveda, A. R., Moreno-Encinas, A., Martínez-Huertas, J. A., Anastasiadou, D., Nova, E., Marcos, A., et al. (2021). Toward a biological, psychological and familial approach of eating disorders at onset: case-control ANOBAS study. Front. Psychol. 12:714414. doi: 10.3389/fpsyg.2021.714414
Serpell, L., and Troop, N. (2003). “Psychological factors” in The handbook of eating disorders. eds. J. Treasure, U. Schmidt, and E. V. Furth (Chichester: John Wiley & Sons), 151–168.
Sharpe, H., Schober, I., Treasure, J., and Schmidt, U. (2014). The role of high-quality friendships in female adolescents’ eating pathology and body dissatisfaction. Eat. Weight Disord. 19, 159–168. doi: 10.1007/s40519-014-0113-8
Shomaker, L. B., and Furman, W. (2009). Interpersonal influences on late adolescent girls’ and boys’ disordered eating. Eat. Behav. 10, 97–106. doi: 10.1016/j.eatbeh2009.02.003
Shroff, H., and Thompson, K. (2006). Peer influences body-image dissatisfaction, eating dysfunction and self-esteem in adolescent girls. J. Health Psychol. 11, 533–551. doi: 10.1177/1359105306065015
Smink, F. R., Van Hoeken, D., and Hoek, H. W. (2012). Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 14, 406–414. doi: 10.1007/s11920-012-0282-y
Solmi, M., Radua, J., Stubbs, B., Ricca, V., Moretti, D., Busatta, D., et al. (2020). Risk factors for eating disorders: an umbrella review of published meta-analyses. Braz. J. Psych. 43, 314–323. doi: 10.1590/1516-4446-2020-1099
Stice, E. (2016). Interactive and mediational etiologic models of eating disorder onset: evidence from prospective studies. Annu. Rev. Clin. Psychol. 12, 359–381. doi: 10.1146/annurev-clinpsy-021815-093317
Stice, E., Onipede, Z. A., and Marti, G. (2021). A meta-analytic review of trials that tested whether eating disorder prevention programs prevent eating disorder onset. Clin. Psychol. Rev. 87:102046. doi: 10.1016/j.cpr.2021.102046
Suarez-Albor, C. L., Galletta, M., and Gómez-Bustamante, E. M. (2022). Factors associated with eating disorders in adolescents: a systematic review. Acta Biomed 93:e2022253. doi: 10.23750/abm.v93i3.13140
Swanson, S. A., Crow, S. J., Le Grange, D., Swendsen, J., and Merikangas, K. R. (2011). Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch Gen Psychiatry, 68, 714–723. doi: 10.1001/archgenpsychiatry.2011.22
Teixeira, M. D., Pereira, A. T., Marques, M. V., Saraiva, J. M., and Macedo, A. F. (2016). Eating behaviors, body image, perfectionism, and self-esteem in a sample of Portuguese girls. Rev. Bras. de Psiquiatr. 38, 135–140. doi: 10.1590/1516-4446-2015-1723
Toubøl, A., Koch-Christensen, H., Bruun, P., and Nielsen, D. S. (2019). Parenting skills after participation in skills-based training inspired by the new Maudsley method: a qualitative study in an outpatient eating disorder setting. Scand. J. Caring Sci. 33, 959–968. doi: 10.1111/scs.12694
Unikel, C., Martín, V., Juárez, F., González-Fortaleza, C., and Nuño, B. (2013). Disordered eating behavior and body weight and shape relatives’ criticism in overweight and obese 15- to 19-year-old females. J. Healht. Pyschol. 18, 75–85. doi: 10.1177/1359105311435945
Vall-Roqué, H., Andrés, A., and Saldaña, C. (2021). The impact of COVID-19 lockdown on social network sites use, body image disturbances and self-esteem among adolescent and young women. Prog. Neuropsychopaharmacol. Biol. Psychiatry. 110:110293. doi: 10.1016/j.pnpbp.2021.110293
Wade, T. D., Wilksch, S. M., Paxton, S. J., Byrne, S. M., and Austin, S. B. (2015). How perfectionism and ineffectiveness influence growth of eating disorder risk in young adolescent girls. Behav. Res. Ther. 66, 56–63. doi: 10.1016/j.brat.2015.01.007
Zamani, S. H., Fathirezaie, Z., Gerber, M., Pühse, U., Bahamani, D. S., and Bashiri, M. (2020). Self-esteem and symptoms of eating disordered behavior among female adolescents. Psychol. Rep. doi: 10.1177/00332948226
Keywords: eating disorders, adolescence, prevention, risk factors, protective factors
Citation: Varela C, Hoyo Á, Tapia-Sanz ME, Jiménez-González AI, Moral BJ, Rodríguez-Fernández P, Vargas-Hernández Y and Ruiz-Sánchez LJ (2023) An update on the underlying risk factors of eating disorders onset during adolescence: a systematic review. Front. Psychol. 14:1221679. doi: 10.3389/fpsyg.2023.1221679
Edited by:
Nicholas T. Bello, Rutgers, The State University of New Jersey, United StatesReviewed by:
Gemma Sharp, Monash University, AustraliaArlette Setiawan, Padjadjaran University, Indonesia
Copyright © 2023 Varela, Hoyo, Tapia-Sanz, Jiménez-González, Moral, Rodríguez-Fernández, Vargas-Hernández and Ruiz-Sánchez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carmen Varela, Y2FybWVudmFyZWxhQHViLmVkdQ==