 Huidong Wang
Huidong Wang Md Sakib Ullah Sourav
Md Sakib Ullah Sourav Mengdi Yang
Mengdi Yang- School of Management Science and Engineering, Shandong University of Finance and Engineering, Jinan, China
The most widely used technique for psychiatric diagnosis is a contemporary manual-based procedure based on prevailing culture-bound data for the classification of mental disorders. However, it has several inherent faults, including the misdiagnosis of complex patient phenomena and others. A potential mental patient from a minority culture could present with atypical symptoms that would be missed by the standard approach. Using the three-way decisions (3WD) as a framework, we propose a unified model that represents the subjective approach (CSA) of clinicians (psychiatrists and psychologists) consisting of three components: qualitative analysis, quantitative analysis, and evaluation-based analysis. The results of the qualitative and quantitative investigation are a classification list and a set of numerical weights based on malady severity levels according to the clinician’s highest level of assumptions. Moreover, we construct a comparative classification of diseases into three categories with varying levels of importance; a three-way evaluation-based model is utilized in this study in order to better comprehend and communicate these results. This proposed method enables clinicians to consider identical data-driven individual behavioral symptoms of patients to be integrated with the current manual-based process as a complementary diagnostic instrument to improve the accuracy of mental disorder diagnosis.
1. Introduction
In this modern era, where technology is at its peak, with endless amusement and entertainment scopes, still, a substantial amount of people, mostly young adults, are suffering from depression and other mental disorders (Substance Abuse and Mental Health Services Administration, 2020). Prevalence can be seen as having a lack of motivation to live, losing interest in everything among common people. Hence, they are frequently thriving toward psychiatric diagnosis than in the past days. Therefore, improper diagnosis of mental health disorders may lead to even more vulnerable consequences in a greater sense from an individual to a social perspective (Shen et al., 2018). The traditional form of psychiatric diagnosis is much pretentious nowadays as few recent studies (Wardenaar and de Jonge, 2013; Allsopp et al., 2019) demonstrate several shortcomings within the widely established systems used for classifying mental disorders, namely, bipolar disorder, anxiety disorders, phobias, substance use disorder, mood disorders, and many others. More often these recognized tools, such as DSM-5 (American Psychiatric Association, 2013) and ICD-11 (World Health Organization, 2019/2021), fails to distinguish between the proper and correct disorder diagnosis of a complex phenomenon in individual cases. Patients with the same disorder exhibit diverse symptom profiles during diagnosis (Jacob and Patel, 2014) and comorbidities or co-occurring conditions creating numerous clinical and research challenges as well (Aina and Susman, 2006). In such a situation, the pragmatic and expertise-oriented judgment from the clinicians (psychiatrists and psychologists) should be reinforced to avoid an improper diagnosis of a mental disorder and restrict its consequences. While three-way classification has emerged as a prominent problem-solving and decision-making paradigm, we intend to integrate its theory into the classification process of mental disorders in order to help the clinicians’ diagnosis process in a more accurate and confident manner.
“Psychiatric nosology” or “psychiatric taxonomy” are terms used to describe how mental diseases are classified. There are presently two commonly used instruments or methods for defining mental disorders: the World Health Organization’s (WHO) International Classification of Diseases (ICD-11) and the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders (DSM-5). In contrast to the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders (DSM), Research Domain Criteria (RDoC) was launched in 2009 with the goal of addressing the heterogeneity in current nosology by providing a biologically-based, rather than symptom-based, a framework for understanding mental disorders (Clark et al., 2017). The Chinese Society of Psychiatry (CSP) (Chen, 2002) produced the Chinese Classification of Mental Diseases (CCMD), a clinical reference for diagnosing mental disorders in China. It is now working on the CCMD-3, a third edition was written in both Chinese and English. It is designed to be structurally and categorically identical to the International Classification of Diseases (ICD) and the Diagnostic and Statistical Manual (DSM).
One of the most fundamental flaws in the DSM-5 and other manuals is that they lack culture-specific meaning and do not include the cultural context of a certain nation (for example, Bangladesh). Common people’s habits, tastes, life expectations, social behavior is much more distinct and unique in different parts of the world and these changes rapidly. After the emergence of COVID-19 amidst the imposed restrictions of various sorts, the mental health circumstances is in big threat; the symptoms are relapsing in normal population, university students, clinical workers, patients with pre-psychiatric disorders, and others in such a way that makes the situation more complex (Krammer et al., 2020; Xie et al., 2020; Belz et al., 2022). In addition, these taxonomies or guides are mostly based on various statistical analyses and information theory, with some cultural representations thrown in for good measure yet backfire to provide us a timely, holistic and unified view on a deeper scale. On the other hand, the broadening of diagnostic criteria in DSM-5, according to critics, may increase the number of “mentally ill” people and/or pathologies “normal behavior,” thus exposing millions of additional patients to pharmaceuticals that may do more damage than good (Bolton, 2013). What is more, the different manual-guided psychiatric diagnoses follow approaches like- categorical, dimensional, and others, those also have their controversy in terms of their validity in many cases (Avasthi et al., 2014; Jablensky, 2016).
Prior to the introduction of manual-based diagnostic systems (about 1980), the clinician’s subjective experience was highly regarded (Fuchs, 2010; Pallagrosi et al., 2016). Although the effectiveness of the method may have increased since the DSM/ICD was introduced, the limitations of this technique are now evident (Wardenaar and de Jonge, 2013; Avasthi et al., 2014; Jablensky, 2016; Allsopp et al., 2019). A study (Picardi et al., 2021) on clinician’s subjective experience supports the resurrection of growing potential on clinician’s subjectivity and its promising role in diagnostic process. Other recent studies (Xie et al., 2020; Belz et al., 2022) show evidence that the clinician’s subjective experience might play a useful role in the diagnostic process as well.
The term “diagnosis” refers to both a phrase and a procedure that is closely linked to concerns of classification (Volkmar, 2013). In conventional psychiatric diagnosis process, a doctor or clinician classify among listed mental disorders by referring to the outlined and data-driven manuals (DSM-5/ICD-11) that include descriptions, symptoms, and so forth; and by following other diagnostic criteria. This is an objective approach that implies internal information-based analysis and it has been put much of the importance comparatively. Simultaneously, similar importance should be imposed on practitioners’ external analysis, namely, culture-specific knowledge along with domain knowledge, through attained expertise and experience with a subjective approach during diagnosis process that has been focused on in the current study, this is shown in Figure 1.
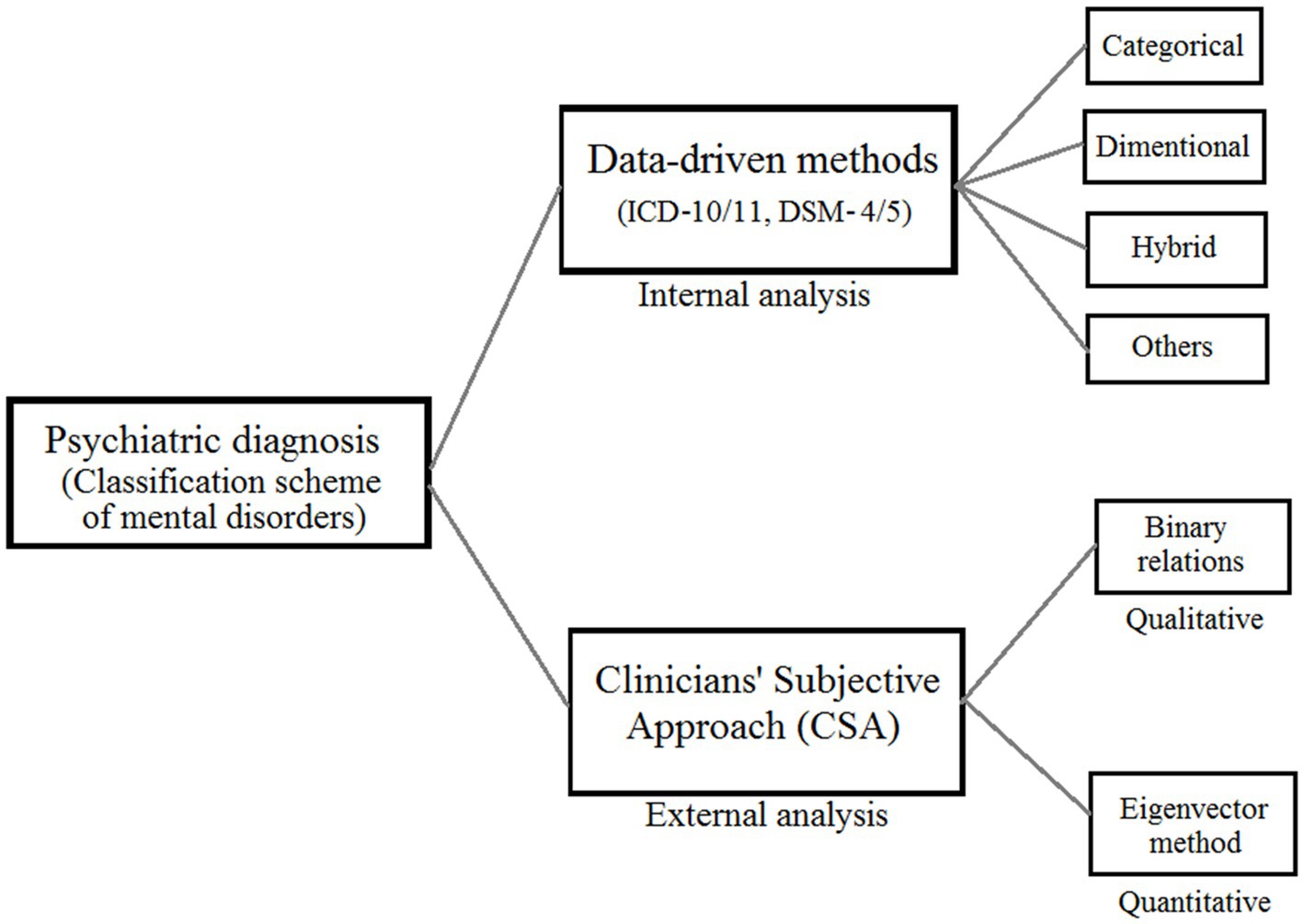
Figure 1. A unified framework of mental disorder classification consisting clinicians’ subjective approach (CSA).
The contributions of this paper are listed as follows:
• The primary purpose of this paper is to provide a general framework and adopt concrete methods to analyze clinicians’ subjective approach (CSA) in mental disorders classification or psychiatric nosology.
• The model proposed in this study to analyze CSA to be integrated with the traditional psychiatric diagnosis that we believe be an effective complimentary tool to make the whole diagnostic process more robust and powerful in future.
• This is the first-ever work that utilized three-way decisions (3WD) theory as the fundamental framework to classify mental disorders in psychiatric diagnosis.
The content of this paper is generally arranged into three parts, qualitative analysis of CSA using binary relations, quantitative analysis of CSA using the eigenvector method, and evaluation-based analysis. Section 2 describes the implications of 3WD in CSA. Section 3 has the qualitative analysis of CSA while quantitative analysis of CSA has been explained in section 4. Evaluation-based CSA analysis is depicted in section 5 and in section 6, discussions and future works are presented. Finally, section 7 has the conclusions of this study.
2. Three-way decision in clinicians’ subjective approach (CSA)
Yao (2018) developed the 3WD theory, which seeks to offer a coherent structure for thinking, problem-solving, and the processing of information in three dimensions. It provides a helpful basis for modeling the difficulties that are encountered in the actual world. 3WD has been implemented in many other domains, such as three-way conflict analysis (Lang et al., 2017; Yao, 2019), three-way clustering (Yu et al., 2016; Zhang and Yao, 2017; Afridi et al., 2018; Wang and Yao, 2018), three-way recommender systems (Zhang and Min, 2016; Huang et al., 2017; Zhang et al., 2017), three-way concept analysis (Ren and Wei, 2016; Yao, 2016), three-way granular computing (Yao, 2018; Yang et al., 2019), three-way face recognition (Li et al., 2016), and many more domains.
In this study, we investigate the subjective approach (CSA) taken by doctors to identify mental diseases during psychiatric diagnosis using 3WD theory as our primary theoretical framework. The Trisecting-Acting-Outcome (TAO) model, the Three-Level Computing Model, and the Evaluation-Based Approach are the three models that are utilized in the research on CSA. As can be seen in Figure 1, we will be doing both a qualitative and quantitative analysis of CSA. In the qualitative research, we evaluate a collection of mental diseases by using CSA. The order correlations between sickness pairs served as the basis for this rating system. We use the TAO mode in three-way options so that we may model the structure and evaluate CSA. Comparing and evaluating the relative preference of each disease in pairs is the first step in our process when considering a clinical perspective. After that, we sort all of these couples into one of three groups: the preferred, the neutral, and the less favored. In the end, we use a binary connection to put diseases and disorders in order from worst to best. When doing quantitative analysis, the eigenvector technique is typically the method of choice for determining disease weights. When the number of things being computed is greater than nine, there is a possibility that a significant error will be made (Saaty and Vargas, 2012). This is one of the drawbacks of the eigenvector approach. The challenge is solved by utilizing the three-level computing paradigm, which is accomplished by the construction of a structure with three levels. The eigenvector method is then applied to the calculation of weights in several iterations, which enables us to obtain a high number of disease weights without compromising an excessive amount of precision.
The conclusions of the qualitative and quantitative study are a ranking list as well as a set of numerical weights based on the severity levels of diseases based on the clinician’s most severe beliefs. The ranking list was created based on the findings of the investigation. In addition, we constructed a comparative categorization of diseases into three groups with varied critical levels. This study makes use of a three-way evaluation-based model with the intention of understanding and expressing these results in a more clear manner.
3. Three-way qualitative clinicians’ subjective approach analysis
Order relations, which is an intuitive sense of ordering things against one another, are a significant implication of binary relations. For example, given that (x, y) is an ordered pair of two elements, we may derive order relations between x and y, such as x being greater than y, x being poorer than y, or x being a component of y in various instances. Order relations are a frequent representation of user preference in decision theory, we write an order relation as or >. If x ≥ y, we say x is at least as good as y, if x > y, we say x is strictly better than y. We solely focus on the strict order relation of “>” in this study to develop a clinician’s preference-based approach (CPA) later on in a more clear way based on the property of trichotomy.
3.1. Clinicians’ subjective approach and the property of trichotomy
The idea of user preference has been intensively investigated in several user-oriented research domains, such as information retrieval (Kelly and Teevan, 2003; Zhou and Yao, 2010), economics (Evren and Ok, 2011), and social sciences (Hogg, 2010). In qualitative CSA analysis, the concept of user preference theory may be employed, and the feature of trichotomy is crucial. This trait makes order relations useful for modeling a CSA toward a set of illnesses.
Humans are skilled at establishing relative comparisons between numbers, goods, methods, and other things in our daily lives. Given two arbitrary real numbers n and m, we may easily argue that one of nm, n = m, or n > m must hold in number theory; this is known as the trichotomy property of real numbers. Similarly, a person can identify the ordering relation between x and y as one of the following: x is preferred over y, x is indifferent to y, or x is less favored than y by comparing a pair of things x and y under a specified criterion. Obviously, a person’s preferred preference for a pair of things is three. This concept can easily be expanded to include order relations.
If we use an order relation > to represent the meaning “preferred,” the indifference relation ∼ is defined as an absence of >, which is defined as:
Give an ordered pair (x, y), if an order relation > expresses the first element is preferred than the second element. Its converse relation which is written as , is called a less preferred relation, which is defined as:
We usually write as ≺ if it does not cause any ambiguity.
Definition 1. An order relation on a disorder set D is called trichotomous if ∀(x, y), x, y ∈ D, exactly one of x > y, x ~ y, or x ≺ y holds.
The purpose of user preference-related research, from the perspective of a decision-maker, is to identify optimum options by examining the order relations among members of a nonempty set, which is characterized as preference relation. The method of user preference theory may be described as first establishing reasonable axioms based on the decision maker’s preferences, and then assessing a user’s preferring behavior based on those preferences (Evren and Ok, 2011). The mathematical properties of trichotomy and transitivity are used to construct a preference relation.
Definition 2. A preference relation, denoted as >, is a special type of binary relation on the set of elements D that satisfies the following two rationality properties. ∀x, y, z ∈ D,
If we use an order relation > as a preference relation, user preference is represented as:
For a disorder set Ds, we divide all disorder attribute pairs into three classes. Based on this trisection, disorder ranking can be induced. This process is shown in Figure 2:
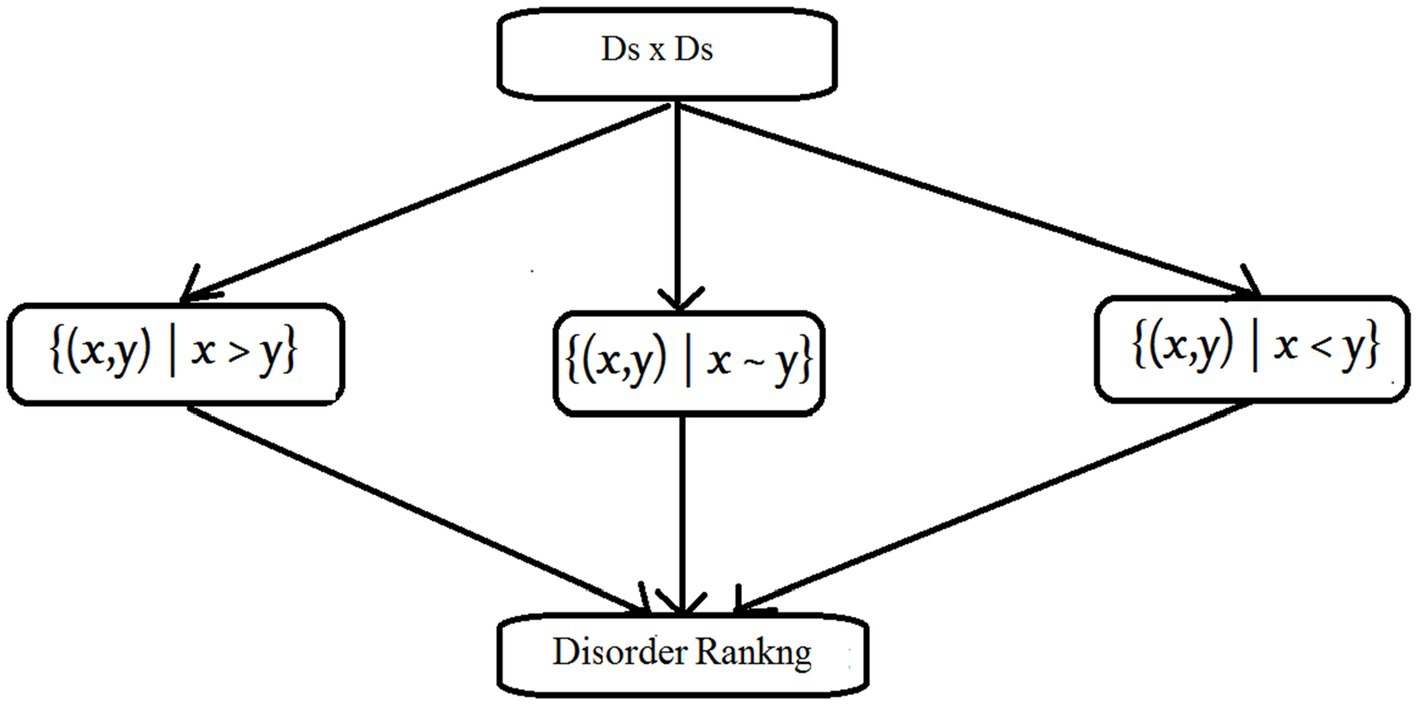
Figure 2. The property of trichotomy.
Linear orders, weak orders, and semiorders are the three types of order relations that all have the properties of trichotomy and transitivity. These three order relations are employed in this article to describe the clinician’s choice for CSA analysis.
3.2. Modeling of CSA as linear order
Given a disorder set Ds, a linear order > enables us to arrange diseases in the form Ds = {d1, d2,.., dn}, such that di > dj if and only if I < j, for this reason, a linear order is also called a chain.
Definition 3. Given a set Ds, a binary relation > is a linear order on Ds, if it satisfies for any x, y, z ∈ Ds:
The asymmetric feature precludes the circumstance in which di is better than dj and dj is better than di at the same time. Reasonable inference may be applied thanks to the transitive property. Weak completeness assures that all illnesses are comparable to one another.
Example 1. Given a set of disorder Ds = {d1, d2, d3, d4, d5}, a clinicians’ preference in accordance of the assumptions on a patient having a potential disorder on Ds is defined by a linear order >. Suppose the ordering between disorders is specified by a clinician as:
Then, disorders are ranked as:
3.3. Modeling of CSA as weak order to illustrate comorbidity in mental disorder
Weak orders are commonly utilized in several disciplines to indicate user preference relations (Kelly and Teevan, 2003; Hogg, 2010; Zhou and Yao, 2010; Evren and Ok, 2011). A weak order enables ties in the ranking results, as opposed to a linear order that places items in a chain, which is quite powerful in representing real-world issues. To put it another way, some properties in a collection may be regarded as indifferent.
In mental disorder classifications, comorbidity of psychiatric illnesses is a widespread issue with major consequences for health-care delivery (Aina and Susman, 2006). Depression, anxiety, and drug dependency disorders are the most common comorbid mental illnesses (Swendsen and Merikangas, 2000). Here, we used ∼ to denote comorbidity of mental disorders and weak ordered relation > to denote ranking of clinician’s preference among disorders.
Definition 4. A weak order > is a binary relation on set Ds, if it satisfies for any x, y ∈ Ds:
Example 2. Given a set of disorder Ds = {d1, d2, d3, d4, d5}, a clinician’s preference on Ds is defined by a weak order >. Suppose the ordering between disorders is specified as:
Because the clinician neither preferences d1 to d2, nor prefer d2 to d1, so d1 must be in comorbid condition or indifferent with d2, written d1 ∼ d2. That means the clinician suspects the particular patient has disease d1 and d2 at the same time. Similarly, d4 ∼ d5. By considering the above ordering, we can rank disorder attributes like:
3.4. Modeling of CSA as semiorder
In fact, a transitive indifference relationship is not always the case. A reader may assume that books C and D are equally good, as are books D and E, after reading three novels, yet he can know that he prefers C to E based on his intuition after reading three books. To put it another way, the individual’s preferring attitude cannot discriminate neither between C and D, nor between D and E, but he can distinguish between C and E. To model this type of situation, Luce (1956) proposed semiorders.
Definition 5. A semiorder > on a set Ds is a binary relation which satisfies for any x, x’, x,” y, y’ ∈ Ds:
Example 3. Given a set of disorder Ds = {d1, d2, d3, d4, d5}, a clinician’s preference on Ds is defined by a semiorder . Suppose the ordering between disorders is specified as:
The clinician neither prefers d2 to d3, nor prefer d3 to d2, so d2 ∼ d3, similarly we can get d3 ∼ d4, however, the indifference is intransitive, because d2 d4. So, we cannot rank all disorders in one order but several, like below:
4. Three-way quantitative clinicians’ subjective approach analysis
Mathematically, quantitative CSA analysis can be considered as a process of mapping each disorder to a numerical value,
where Ds is a set of disorders, R is a real number set, and w is a mapping function that calculates or assigns a numerical value to each disorder. For a disorder d ∈ Ds, w(d) represents its weight from the perspective of a clinician.
4.1. Formulating a three-level structure
This study offered two methods for calculating or assigning numerical weights to each ailment. The first is calculating weights using the eigenvector approach, which is covered in section 4.2. The second method is to assign weights. To be more explicit, we first use the eigenvector method to construct an important scale with numerical weights, and then we compare each disease to this scale to determine its weight; this methodology is detailed in section 4.3. Obviously, the eigenvector technique is vital in both approaches; however, it has a limitation in that it is not suitable when the number of objects is greater than 9 since large mistakes in the computation would be introduced (Saaty and Vargas, 2012). We use the 3WD theory to solve this problem. More specifically, the issue is divided into three levels, after which the eigenvector approach is used to calculate weights from top to bottom. The three-level structure allows us to limit the number of items in the computation of the weights to no more than 9, allowing us to compute weights using the eigenvector approach without sacrificing too much precision.
4.2. Three-way quantitative disease weighting based on eigenvector method
Figure 3 depicts the framework of the quantitative illness weighting model. Assume we have a disorder set Ds, where dij denotes a disorder at the lowest level. We create a three-level framework by categorizing illnesses into various groups based on semantic significance.
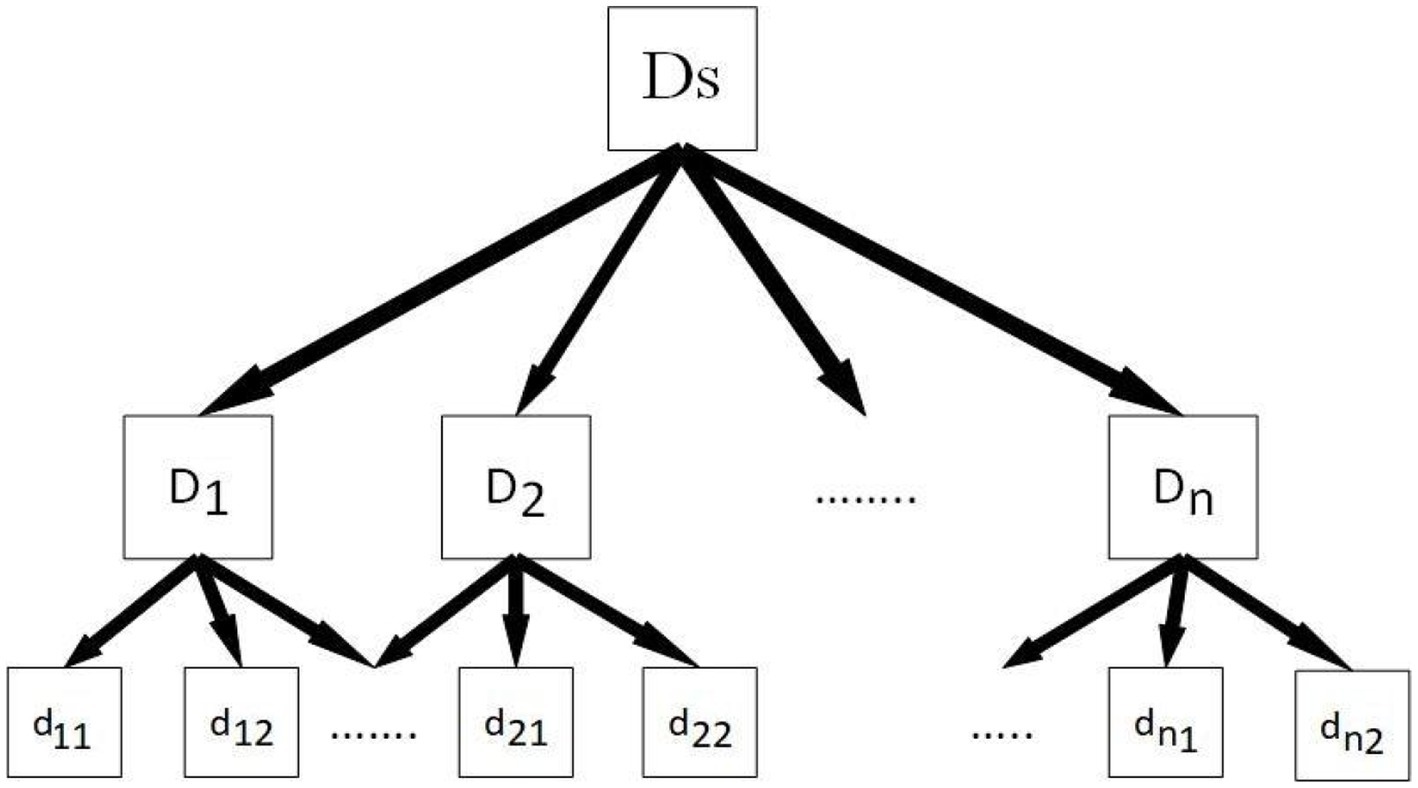
Figure 3. The structure of the three-level disease weighting method.
The second step is to use the eigenvector approach to calculate from top to bottom after we have this three-level structure. We create cluster weights based on clinician choice, and then we determine the weights of illnesses inside each cluster based on cluster weight.
The following is a description of how to calculate weights using the eigenvector approach. Assume that a disorder collection Ds has been divided into n clusters, n ≤ 9, with no more than 9 illnesses in each cluster. We establish a comparison matrix M as specified in Definition 6. to produce a weight vector w = (w1, w2, ···,wn) for clusters, where element mij reflects the relative significance of a cluster Di compared to a cluster Dj.
Definition 6. A comparison matrix M is a square matrix of order n, whose elements are mij, M is a positive reciprocal matrix if M is:
Where, ∀i, j (i, j = 1, 2… n). M is a comparison matrix that looks like below, and in a perfect situation, m i j should exactly be the weights ratio of a cluster D i compared with D j.
In practice, the values of components in a comparison matrix are determined by the user’s preference and flexibility. We use the 9-point rating scale established by Saaty and Vargas (2012) to precisely determine the weight ratio w1/w2 between two clusters (see Table 1).
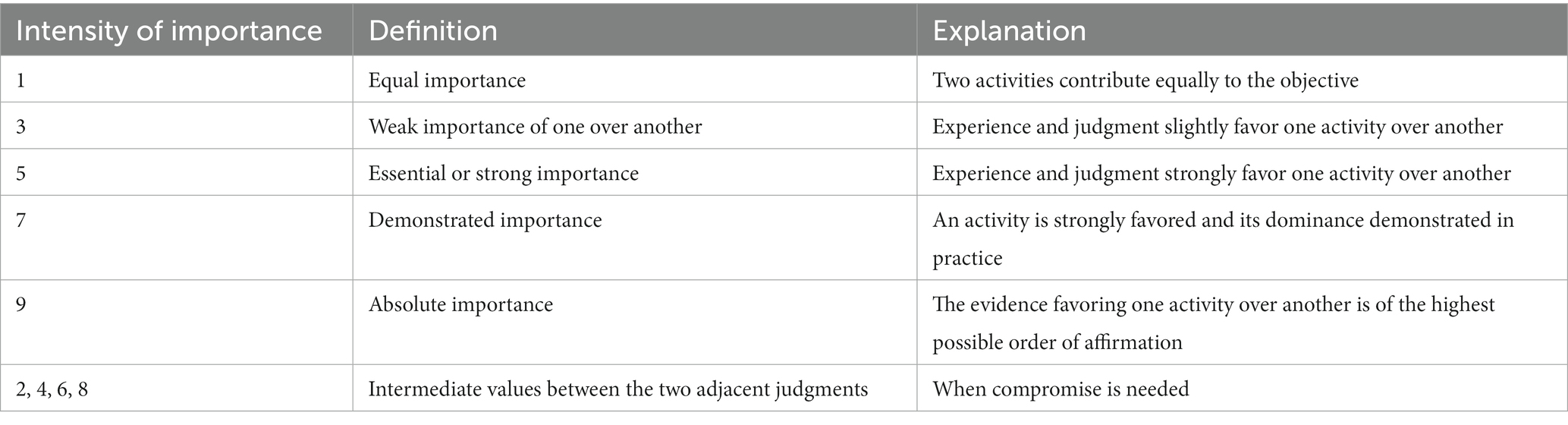
Table 1. The Saaty’s 9-points rating scale (Saaty and Vargas, 2012).
Table 1 shows that the number 1 denotes that two clusters are equally essential. An arbitrary cluster should be equally significant to itself, hence the value mii of the major diagonal in a comparison matrix must be 1. Furthermore, for two clusters a and b, the weight ratio wa/wb should be larger than 1 if an is favored over b, else it should be equal to or less than 1.
We may get the matrix equation as follows under ideal conditions:
where, M is multiplied on the left by the weights vector w, and the result is nw. The issue we are working on has been rewritten as Mw = nw = 0, or (M – n I) w = 0. Ideally, M is consistent if and only if its principle eigenvalue λmax = n (Saaty and Vargas, 2012). Inconsistency is unavoidable since items in a comparison matrix are personal judgments evaluated by a clinician. Precisely because of this, changes in the matrix lead to changes in the eigenvalues. We now have a new challenge to solve:
Where is the perturbed matrix of M = (mi j), is the principal eigenvector and λmax is the principal eigenvalue of. What we want to learn is how good the principal eigenvector represents w. Consistency ratio C.R. is used to determine whether an inconsistency is acceptable:
Table 2 shows the average random consistency index (R.I.). These indices were created using a 9-point rating scale and a sample of randomly generated reciprocal matrices (Saaty and Vargas, 2012).

Table 2. Average random consistency index (R.I.).
Eigenvector w can be used as cluster weights if C.R. is less than 10%; otherwise, the comparison matrix must be changed until C.R. is less than 10%.
Example 4. Assume we have a disorder set Ds that has been divided into six clusters, Ds = {D1, D2, D3, D4, D5, D6}. Based on a clinician’s assessment, a comparison matrix has been created, and the weights calculation procedure is illustrated in Table 3 (Cui et al., 2020):
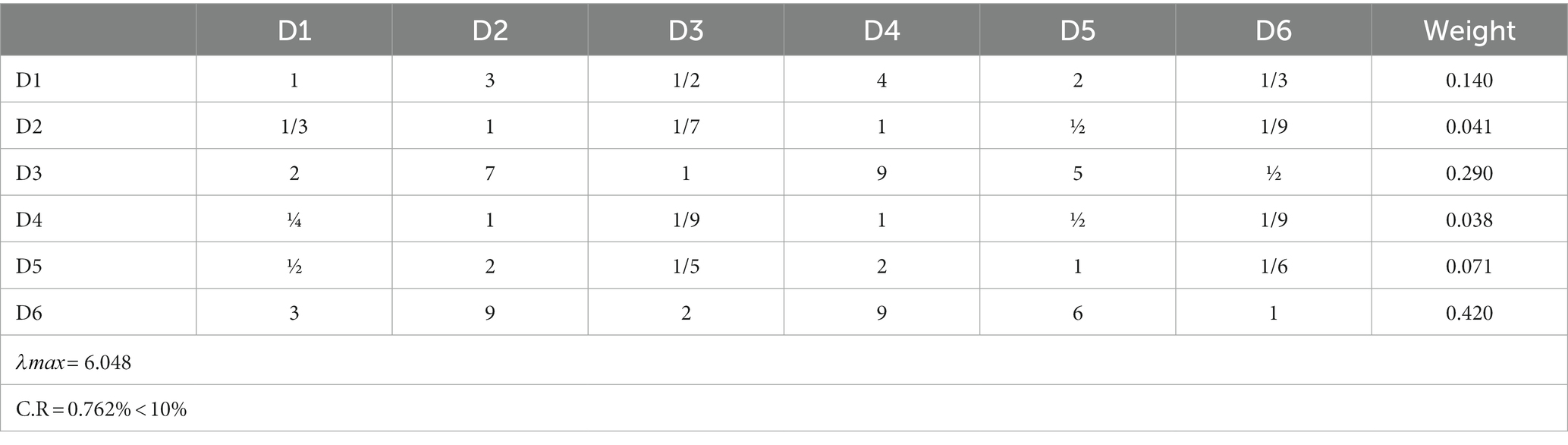
Table 3. Weights calculation of six clusters.
Because C.R. ≤ 10%, which satisfies consistency checking, the eigenvector of comparison matrix can be used as the weights of {D1, D2, D3, D4, D5, D6}, that is:
We begin with the weights of clusters and employ the same procedure to compute the weights of diseases within each cluster. The disease weights are then normalized by dividing them by the relevant cluster weights. Lastly, we can compute disease weights.
4.3. A quantitative disease weighting method using an importance scale
It is straightforward for a physician to assign numerical values as weights to ailments based on his or her own perspective. Yet, when the number of probable diseases is extremely high, fluctuations in judgment are inevitable, resulting in a conclusion with low precision. Hence, a critical scale is utilized to resolve the issue (Saaty and Vargas, 2012).
The illness weighting method utilizing an importance scale may be broken down into the following three components. Initially, the doctor groups the intensity of the preferred degree of disease orders into different degrees, such as substantially matched, matched, moderately matched, poorly matched, and not matched. Using the eigenvector technique outlined in section 4.2, we can then calculate weights for each intensity degree. When the intensity degree count surpasses nine, a three-level structure is necessary. As a result, we devise an importance scale to help in our decision-making. With this scale, the weights of diseases are computed.
Example 5. Suppose a clinician sets five intensities of the preferential degree of suspected disorders, which are A: significantly matched, B: matched, C: moderately matched, D: weakly matched, E: not matched. A clinician builds a comparison matrix of these intensities, and the weights calculation of intensities is described as Table 4 (Cui et al., 2020):
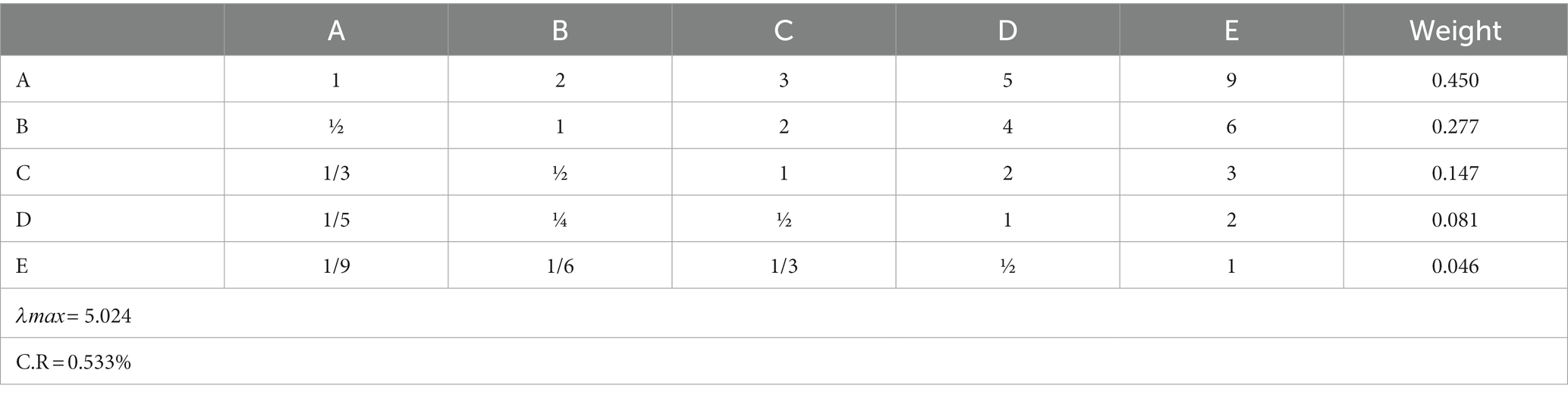
Table 4. A pairwise comparison matrix of intensity levels.
Because the consistency check is complete, the weights of these intensities are used to construct an important scale. Then, using this scale, we compare each property one by one, assigning various weights to each disorder attribute from the clinician’s perspective.
5. Three-way evaluation based CSA analysis
The 3WD (Yao and Gao, 2015) is based on dividing the universe into three zones and employing various tactics in each. The result of a qualitative or quantitative CPA analysis is a ranking list or a set of numerical weights that are significant but difficult for a physician to use in making a choice. These findings will be processed and classified into three pair-wise disjoint classes with varying levels of relevance, namely high importance, medium importance, and low importance, in this part. We’ll refer to these three classes as H, M, and L for the rest of this study. We chose three classes because human cognition and problem-solving rely on a three-way divide, which allows us to convert complexity into simplicity in a variety of scenarios (Yao, 2016).
5.1. Trisecting a disorder set based on thresholds
Research Domain Criteria (RDoC), considering the possibility of increasing need of constructing various thresholds for different purposes, is trying to gather information consistently to set thresholds in diagnostic systems of mental disorder where this is relevant; especially in particular research purpose or applications in clinical settings or in health policymaking (Clark et al., 2017). Our current study acknowledges this concern and suggests insightful paths on formulating thresholds in mental disorder classification while in the diagnosis process.
Using two percentiles is one method for trisecting a disorder set. The first step is to convert a linear order > from a qualitative or quantitative analytical result. This phase can be bypassed if the outcome of the qualitative method is based on linear order. To identify the three areas, the second step is to use a pair of thresholds, based on the percentiles.
There are various methods for linearly transforming qualitative and quantitative findings. The first is topological sorting, which states that an element will not appear in a ranking list until all other items that are preferable to it have been listed (Kahn, 1962). We can generate a decreasing ranking list by utilizing topological sorting. Another option is to use an assessment function to convert qualitative and quantitative analytical results into a set of diseases’ evaluation status values (ESVs). The ESV of disease d is defined as follows:
Illnesses will be sorted in decreasing order depending on their ESVs, with diseases with the same ESV being listed in any order.
Now, we have a list of ESVs, which is in the form of v1, v2.., vn where v1 is the largest value and vn is the smallest value. Using the ranking lists of the above two methods, we then adopt two ESVs at αth and βth percentiles with 0 < β < α < 100 to calculate a pair of thresholds h and l as:
Where the ceiling function gives the smallest integer that is not less than x, and the floor function gives the largest integer that not greater than x. The floor and ceiling functions are necessary for the reason that αn/100 and βn/100 may not be integers (Graham et al., 1989; Yao and Gao, 2015).
Three regions, H, M, and L, may be created using the descending ranking list and two thresholds. Disorders in the H region are of high priority, disorders in the M region are of moderate priority, and disorders in the L zone are of low priority.
5.2. Trisecting a disease set based on a statistical method
Yao and Gao (2015) examined the statistical procedure of building and evaluating three areas. Mean and standard deviation are statistical methods for examining numerical numbers that may be applied to the findings of a quantitative CPA study. Suppose w(d1),w(d2),..,w(dn) are the weights of disorders in Ds, n is the cardinality of Ds, the mean and standard deviation is calculated by:
We use two non-negative numbers k1 and k2 to represent the position of thresholds away from the mean, then a pair of thresholds is determined as Yao and Gao (2015):
Based on thresholds h and l, three regions of a disorder set can be constructed as:
Disorders can be categorized into three regions H, M, and L considering their weights.
6. Discussion and future directions
We are optimistic that the CSA model will serve as an efficient auxiliary instrument to make the diagnostic process for mental disorders more robust and effective in the years to come. However, we essentially emphasized that the mental symptoms and indicators are passively observed subjects in the paradigm that this research proposes. However, in terms of phenomenological psychopathology, clinicians can also examine patient symptoms and signs using emphatic techniques (Oyebode, 2008). This approach specifically excludes a different method for analyzing symptoms, which is not phenomenological psychiatry but rather an understanding of the disease of mental functioning. Additionally, mental disorders are defined with an operational manner in mainstream diagnostic systems (such as ICD-11 and DSM-5) but are not based on biological indicators. The psychiatric diagnoses therefore correspond to the practical or fuzzy kinds but not the natural kinds. What is more, the operational definitions are relevant to language games in terms of Wittgenstein’s philosophy of language (Travis, 1989). Specifically, the instances with a single diagnosis might be linked by a chain of meanings rather than being supported by a single biological foundation in such disease essentialism. With the addition of psychiatrist-patient interaction (i.e., psychiatrist’s emphatic approach) and/or its influences on the classification as future work or extension of this current study, the proposed classification model of mental disorders through clinicians’ subjective approach on 3WD can be further modified.
Consequently, different paradigms, such as pointing graphs, can be used to develop the disorder ranking procedure. To calculate the weight value of each disorder cluster, analytic hierarchy process can be adopted in lieu of eigenvector method and the results can be compared. The quantification of the weight values for diseases using a three-level structure is required in future by clinicians when the number of intensity degrees exceeds 9. For the time being, this current study is offering the theoretic approach to solve this complex problem related to psychiatric diagnosis. Practical implications in both the qualitative and quantitative perspectives should be explored in further studies to ensure the proposed method is better than other existing methods.
7. Conclusion
Despite having a number of limitations, the data-driven manual-based categorization approach is the way of mental disease classification that is employed the most frequently. Based on the three-way choice, we present a unified model consisting of three parts that may be used for clinicians’ subjective approach (CSA) analysis. In the qualitative research, we employ binary relations and the TAO model to rank mental disorders according to their patients’ preferences based on the criteria that we collect. The three-level computing paradigm is implemented throughout the quantitative analysis, and the eigenvector approach is applied in order to provide numerical weights to the various mental illnesses. In the end, we divide the findings from the qualitative and quantitative research into three distinct categories according to the weight that we place on each of the factors.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
HW: methodology, writing—review, and editing. MS: writing—original draft preparation. MY: qualitative and quantitative analysis. JZ: evaluation-based analysis. All authors read and approved the final manuscript.
Acknowledgments
We acknowledge Md Omar Faruk (clinical psychology researcher) for his suggestions and guidance on clinical psychiatric diagnosis of mental disorders that helps us encounter with this proposed method.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Afridi, M. K., Azam, N., Yao, J. T., and Alanazi, E. (2018). A three-way clustering approach for handling missing data using GTRS. Int. J. Approx. Reason. 98, 11–24. doi: 10.1016/j.ijar.2018.04.001
Aina, Y., and Susman, J. L. (2006). Understanding comorbidity with depression and anxiety disorders. J. Am. Osteopath. Assoc. 106, S9–S14.
Allsopp, K., Read, J., Corcoran, R., and Kinderman, P. (2019). Heterogeneity in psychiatric diagnostic classification. Psychiatry Res. 279, 15–22. doi: 10.1016/j.psychres.2019.07.005
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders. 5th Edn. Washington: American Psychiatric. doi: 10.1176/appi.books.9780890425596
Avasthi, A., Sarkar, S., and Grover, S. (2014). Approaches to psychiatric nosology: a viewpoint. Indian J. Psychiatry 56, 301–304. doi: 10.4103/0019-5545.120560
Belz, M., Hessmann, P., Vogelgsang, J., Schmidt, U., Ruhleder, M., Signerski-Krieger, J., et al. (2022). Evolution of psychosocial burden and psychiatric symptoms in patients with psychiatric disorders during the Covid-19 pandemic. Eur. Arch. Psychiatry Clin. Neurosci. 272, 29–40. doi: 10.1007/s00406-021-01268-6
Bolton, D. (2013). Overdiagnosis problems in the DSM-IV and the new DSM-5: can they be resolved by the distress-impairment criterion? Can. J. Psychiatr. 58, 612–617. doi: 10.1177/070674371305801106
Chen, Y. F. (2002). Chinese classification of mental disorders (CCMD-3): towards integration in international classification. Psychopathology 35, 171–175. doi: 10.1159/000065140
Clark, L. A., Cuthbert, B., Lewis-Fernández, R., Narrow, W. E., and Reed, G. M. (2017). Three approaches to understanding and classifying mental disorder: ICD-11, DSM-5, and the National Institute of Mental Health’s research domain criteria (RDoC). Psychol. Sci. Public Interest 18, 72–145. doi: 10.1177/1529100617727266
Cui, X., Yao, J., and Yao, Y. (2020). “Modeling use-oriented attribute importance with the three-way decision theory” in Rough sets. IJCRS 2020, lecture notes in computer science. eds. R. Bello, D. Miao, R. Falcon, M. Nakata, A. Rosete, and D. Ciucci, vol. 12179 (Cham: Springer), 122–136.
Evren, O., and Ok, E. A. (2011). On the multi-utility representation of preference relations. J. Math. Econ. 47, 554–563. doi: 10.1016/j.jmateco.2011.07.003
Fuchs, T. (2010). Subjectivity and Intersubjectivity in psychiatric diagnosis. Psychopathology 43, 268–274. doi: 10.1159/000315126
Graham, R. L., Knuth, D. E., Patashnik, O., and Liu, S. (1989). Concrete mathematics: a foundation for computer science. Comput. Phys. 3, 106–107. doi: 10.1063/1.4822863
Hogg, T. (2010). Inferring preference correlations from social networks. Electron. Commer. Res. Appl. 9, 29–37. doi: 10.1016/j.elerap.2009.04.006
Huang, J. J., Wang, J., Yao, Y. Y., and Zhong, N. (2017). Cost-sensitive three-way recommendations by learning pair-wise preferences. Int. J. Approx. Reason. 86, 28–40. doi: 10.1016/j.ijar.2017.03.005
Jablensky, A. Psychiatric classifications: validity and utility. World Psychiatry (2016). 15:26–31. doi: 10.1002/wps.20284.
Jacob, K. S., and Patel, V. (2014). Classification of mental disorders: a global mental health perspective. Lancet 383, 1433–1435. doi: 10.1016/S0272-7358(99)00026-4
Kelly, D., and Teevan, J. Implicit feedback for inferring user preference: a bibliography. In: Proceedings of the ACM SIGIR Forum. downtown Hilton in Toronto: Canada (2003), 18–28.
Krammer, S., Augstburger, R., Haeck, M., and Maercker, A. (2020). Adjustment disorder, depression, stress symptoms, Corona related anxieties and coping strategies during the Corona pandemic (COVID-19) in Swiss medical staff. Psychother. Psychosom. Med. Psychol. 70, 272–282. doi: 10.1055/a-1192-6608
Lang, G., Miao, D., and Cai, M. (2017). Three-way decision approaches to conflict analysis using decision-theoretic rough set theory. Inf. Sci. 406, 185–207. doi: 10.1016/j.ins.2017.04.030
Li, H. X., Zhang, L. B., Huang, B., and Zhou, X. Z. (2016). Sequential three-way decision and granulation for cost-sensitive face recognition. Knowl.-Based Syst. 91, 241–251. doi: 10.1016/j.knosys.2015.07.040
Luce, R. D. (1956). Semiorders and a theory of utility discrimination. Econometrica 24, 178–191. doi: 10.2307/1905751
Oyebode, F. (2008). Sims' symptoms in the mind: an introduction to descriptive psychopathology Elsevier Health Sciences.
Pallagrosi, M., Fonzi, L., Picardi, A., and Biondi, M. (2016). Association between clinician's subjective experience during patient evaluation and psychiatric diagnosis. Psychopathology 49, 83–94. doi: 10.1159/000444506
Picardi, A., Panunzi, S., Misuraca, S., Di Maggio, C., Maugeri, A., Fonzi, L., et al. (2021). The clinician's subjective experience during the interaction with adolescent psychiatric patients: validity and reliability of the assessment of clinician's subjective experience. Psychopathology 54, 119–126. doi: 10.1159/000513769
Ren, R., and Wei, L. (2016). The attribute reductions of three-way concept lattices. Knowl. Based Syst. 99, 92–102. doi: 10.1016/j.knosys.2016.01.045
Saaty, T. L., and Vargas, L. G.. Models, methods, concepts and applications of the analytic hierarchy process. New York, NY: Springer (2012).
Shen, H., Zhang, L., Xu, C., Zhu, J., Chen, M., and Fang, Y. (2018). Analysis of misdiagnosis of bipolar disorder in an outpatient setting. Shanghai Arch. Psychiatry 30, 93–101. doi: 10.11919/j.issn.1002-0829.217080
Substance Abuse and Mental Health Services Administration . (2020). Key substance use and mental health indicators in the United States: results from the 2019 National Survey on Drug Use and Health (HHS publication no. PEP20-07-01-001, NSDUH series H-55). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Available at: https://www.samhsa.gov/data/.
Swendsen, J. D., and Merikangas, K. R. (2000). The comorbidity of depression and substance use disorders. Clin. Psychol. Rev. 20, 173–189. doi: 10.1016/S0272-7358(99)00026-4
Volkmar, F. R. (2013). “Diagnosis and classification” in Encyclopedia of autism spectrum disorders (New York, NY: Springer), 1–9.
Wang, P. X., and Yao, Y. Y. (2018). CE3: a three-way clustering method based on mathematical morphology. Knowl. Based Syst. 155, 54–65. doi: 10.1016/j.knosys.2018.04.029
Wardenaar, K. J., and de Jonge, P. (2013). Diagnostic heterogeneity in psychiatry: towards an empirical solution. BMC Med. 11:201. doi: 10.1186/1741-7015-11-201
World Health Organization . (2019/2021) International classification of diseases, eleventh revision (ICD-11).
Xie, Q., Fan, F., Fan, X.-P., Wang, X. J., Chen, M. J., Zhong, B. L., et al. (2020). COVID-19 patients managed in psychiatric inpatient settings due to first-episode mental disorders in Wuhan, China: clinical characteristics, treatments, outcomes, and our experiences. Transl. Psychiatry 10:337. doi: 10.1038/s41398-020-01022-x
Yang, X., Li, T. R., Liu, D., and Fujita, H. (2019). A temporal-spatial composite sequential approach of three-way granular computing. Inf. Sci. 486, 171–189. doi: 10.1016/j.ins.2019.02.048
Yao, Y. (2016). Interval sets and three-way concept analysis in incomplete contexts. Int. J. Mach. Learn. Cybernet. 8, 3–20. doi: 10.1007/s13042-016-0568-1
Yao, Y. Y. (2016). Three-way decisions and cognitive computing. Cogn. Comput. 8, 543–554. doi: 10.1007/s12559-016-9397-5
Yao, Y. (2018). Three-way decision and granular computing. Int. J. Approx. Reas. 103, 107–123. doi: 10.1016/j.ijar.2018.09.005
Yao, Y. Y. (2019). Three-way conflict analysis: reformulations and extensions of the Pawlak model. Knowl. Based Syst. 180, 26–37. doi: 10.1016/j.knosys.2019.05.016
Yao, Y., and Gao, C. (2015). “Statistical interpretations of three-way decisions” in RSKT 2015. LNCS (LNAI). eds. D. Ciucci, G. Wang, S. Mitra, and W.-Z. Wu, vol. 9436 (Cham: Springer), 309–320.
Yu, H., Zhang, C., and Wang, G. (2016). A tree-based incremental overlapping clustering method using the three-way decision theory. Knowl. Based Syst. 91, 189–203. doi: 10.1016/j.knosys.2015.05.028
Zhang, H. R., and Min, F. (2016). Three-way recommender systems based on random forests. Knowl. Based Syst. 91, 275–286. doi: 10.1016/j.knosys.2015.06.019
Zhang, H. R., Min, F., and Shi, B. (2017). Regression-based three-way recommendation. Inf. Sci. 378, 444–461. doi: 10.1016/j.ins.2016.03.019
Zhang, Y., and Yao, J. T. (2017). Gini objective functions for three-way classifications. Int. J. Approx. Reason. 81, 103–114. doi: 10.1016/j.ijar.2016.11.005
Keywords: data-driven decision making, mental disorder classification, psychiatric diagnosis, three-way decisions, the Trisecting-Acting-Outcome (TAO) model
Citation: Wang H, Sourav MSU, Yang M and Zhang J (2023) Classifying mental disorders through clinicians’ subjective approach based on three-way decisions. Front. Psychol. 14:1144826. doi: 10.3389/fpsyg.2023.1144826
Edited by:
Yuan-Wei Du, Yunnan University, ChinaReviewed by:
Surapati Pramanik, Nandalal Ghosh B.T. College, IndiaRachele Mariani, Sapienza University of Rome, Italy
Susu Wang, Ocean University of China, China
Copyright © 2023 Wang, Sourav, Yang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huidong Wang, aHVpZG9uZy53YW5nQGlhLmFjLmNu
†These authors have contributed equally to this work and share first authorship