
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 24 February 2023
Sec. Pediatric Psychology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1130331
 Kaiyi Zhu1,2†
Kaiyi Zhu1,2† Wei Yang3†
Wei Yang3† Zesheng Ying3
Zesheng Ying3 Yingjie Cai3XiaoJiao Peng3
Yingjie Cai3XiaoJiao Peng3 Nijia Zhang3Hailang Sun3Yuanqi Ji3Ming Ge3*
Nijia Zhang3Hailang Sun3Yuanqi Ji3Ming Ge3*Background: To investigate the long-term quality of life (QoL) of children with cerebellar mutism syndrome (CMS) and explore the risk factors for a low QoL.
Procedure: This cross-sectional study investigated children who underwent posterior fossa surgery using an online Pediatric Quality of Life Inventory questionnaire. CMS and non-CMS patients were included to identify QoL predictors.
Results: Sixty-nine patients were included (male, 62.3%), 22 of whom had CMS. The mean follow-up time was 45.2 months. Children with CMS had a significantly lower mean QoL score (65.3 vs. 83.7, p < 0.001) and subdomain mean scores (physical; 57.8 vs. 85.3, p < 0.001; social: 69.5 vs. 85.1, p = 0.001; academic: p = 0.001) than those without CMS, except for the emotional domain (78.0 vs. 83.7, p = 0.062). Multivariable analysis revealed that CMS (coefficient = −14.748.61, p = 0.043), chemotherapy (coefficient = −7.629.82, p = 0.013), ventriculoperitoneal (VP) shunt placement (coefficient = −10.14, p = 0.024), and older age at surgery (coefficient = −1.1830, p = 0.007) were independent predictors of low total QoL scores. Physical scores were independently associated with CMS (coefficient = −27.4815.31, p = 0.005), VP shunt placement (coefficient = −12.86, p = 0.025), and radiotherapy (coefficient = −13.62, p = 0.007). Emotional score was negatively associated with age at surgery (coefficient = −1.92, p = 0.0337) and chemotherapy (coefficient = −9.11, p = 0.003). Social scores were negatively associated with male sex (coefficient = −13.68, p = 0.001) and VP shunt placement (coefficient = −1.36, p = 0.005), whereas academic scores were negatively correlated with chemotherapy (coefficient = −17.45, p < 0.001) and age at surgery (coefficient = −1.92, p = 0.002). Extent of resection (coefficient = 13.16, p = 0.021) was a good predictor of higher academic scores.
Conclusion: CMS results in long-term neurological and neuropsychological deficits, negatively affecting QoL, and warranting early rehabilitation.
Cerebellar mutism syndrome (CMS) is a multifaceted complication after posterior fossa surgery in children. Up to 25% of children with posterior fossa tumors are affected by this clinical condition (Robertson et al., 2006). Transient loss of speech is thought to be the primary symptom of CMS and has been of great concern in previous studies. To date, the mechanism of CMS has been elusive, and most studies have concentrated on revealing its risk factors. Medulloblastoma, midline location, younger age, and male sex were thought to be risk factors of CMS (Gronbaek et al., 2021; Yang et al., 2022a). A consensus on CMS was reached in 2016 that included other symptoms in addition to speech deficits, including emotional liability and cognitive and motor dysfunctions, with these persisting longer (Gudrunardottir et al., 2016). However, few studies have reported the long-term condition of children with CMS. And previous studies indicated that the long-term performance of children remains uncertain (Camara et al., 2020; Grieco et al., 2020; Khan et al., 2021).
With the improved survival rate of children with brain tumors, long-term quality of life (QoL) has become a key concern in clinical practice. Posterior fossa tumors are the most common brain tumors in children (Ostrom et al., 2021), and CMS is the most common complication (Ashida et al., 2021). The impact of CMS on children’s QoL remains unknown. The Pediatric Quality of Life Inventory (PedsQL) is designed to measure the core dimensions of health, which include physical, emotional, and social functions, as well as school performance, well covering the domains related to CMS. The inventory includes self-report and parent-proxy report versions, both of which are highly reliable. Several studies on the QoL of children with brain tumors have been conducted, where PedsQL 4.0 were widely used (Eaton et al., 2020; Li et al., 2021; Peragallo et al., 2021). However, similar studies on CMS are scarce.
Similar with CMS, cerebellar cognitive affective syndrome (CCAS) is another complication after posterior fossa surgery, which stresses executive deficit, visuospatial cognition deficit, speech deficit, and emotional deficit. Thus far, the relationship between CMS and CCAS remains controversial (Argyropoulos et al., 2020). Some researchers regard CMS as one aspect of the larger neuropsychological entity of CCAS; however, this perspective was not widely recognized (Sadeh and Cohen, 2001; Schmahmann, 2020). At present, the Posterior Fossa Society1 still considers CMS and CCAS as two different but related entities; however, the two diseases share similar deficits in cognitive and emotional domains (Schmahmann, 2020).
The emotional impairment can manifest with social–emotional aberrant behaviors, social cognition impairments, and poor self-monitoring of negative emotion (Clausi et al., 2015; Hoche et al., 2016). The initial papers indicate that affective impairments are transient (Argyropoulos et al., 2020), whereas subsequent work has shown that affective changes can be chronic, especially in adult survivors of childhood cerebellar insults (Steinlin et al., 2003). As Schmahmann has mentioned, the affective component is assessed in a less systematized fashion, with many previous studies employing clinical psychiatric assessment, which is based on DSM diagnosis (Argyropoulos et al., 2020). Although a working group in posterior society have been built to develop an easy-to-use scale to quantify the emotional impairments of CMS, no standardized scale has been published so far. Herein, we expect to assess the affective status with emotional domain of PedsQL, and this may provide useful information for future studies.
The cerebellum has been gradually considered to play a role in cognitive and executive function. Studies of CCAS also revealed that the posterior lobe of the cerebellum was associated with cognitive impairment (Stoodley et al., 2016). In addition, radiation to the posterior fossa is expected to impair cognitive function (Mulhern et al., 2005; Conklin et al., 2008; von Hoff et al., 2008; Aarsen et al., 2009; Moxon-Emre et al., 2014). Therefore, the long-term cognitive performance in children with CMS needs to be investigated further.
The school domain of PedsQL assesses behaviors associated with attention, memory, and learning capability. Previous studies have demonstrated that neurocognitive performance is correlated with QoL outcomes (Kuhlthau et al., 2012). Low school scores may reflect impairments in cognitive functioning, processing speed, and attention, at least in part. Considering its accessibility and simplicity, the school domain was used to reflect the cognitive performance in this study.
Above all, in this cross-sectional study, we aimed to investigate the long-term QoL of children with or without CMS and explore the associated factors that have an impact on QoL.
This retrospective study was approved by the Ethics Committee of the Beijing Children’s Hospital (grant number: [2022]-E-076-R). Patients diagnosed with posterior fossa tumors and treated by tumor removal surgery before December 2019 at our hospital were reviewed. The inclusion criteria were (1) diagnosis of posterior fossa tumors by MR and pathology; (2) tumor removal surgery; (3) more than 2 years since surgery date; (4) age 5–18 years at investigation; and (5) consent to participate in this study. The exclusion criteria were as follows: (1) patients who underwent biopsy rather than craniotomy; (2) no survival at follow-up or loss of follow-up; (3) incomplete medical records that influenced the statistical analysis; and (4) CMS status that could not be determined through medical records or phone inquiries. Participants were divided into CMS and non-CMS groups based on their diagnosis of CMS. Figure 1 shows the workflow of patient selection.

Figure 1. Workflow of the patient selection.
Based on the consensus from the Delphi conference, CMS was defined as mutism or notably reduced speech after posterior fossa tumor removal. Hypotonia, behavior change, and dysphagia after surgery during hospital days were also acquired from medical records or telephone interviews to further depict the details of CMS manifestations. Due to the difficulties of assessing ataxia when patients are in a hypotonia status, we did not include this feature. Behavior change was defined as when the patient presented with irritability or apathy. The onset of mutism was defined as days after the surgery date, and the surgery date was set as day 0. The restoration of speech was defined as being able to speak at least one Chinese word, i.e., “Baba” (dad) or “Mama” (mum), rather than a conversational speech. The duration of mutism was the duration between mutism onset and speech restoration. The aforementioned were collected from medical records and a follow-up database.
Patients eligible for inclusion were contacted via phone or email. Patients who were willing to participate in this study were sent an online version of the PedsQL 4.0 Generic Core Scale (in Chinese). The PedsQL 4.0, assesses four domains of QoL, including physical, social, emotional, and academic functions. The scale consists of self-report and parent–proxy reports. We chose the PedsQL 4.0, Generic Core Scales because of its frequent use in pediatric literature and its specific brain tumor module. It has been demonstrated that self-reported scores correlate well with proxy-reported scores (Varni et al., 2007; Cheng et al., 2015). Here, we used proxy reports to assess the QoL. Items are reverse scored and linearly transformed to a 0–100 scale. The row score was transformed to the 0–100 range according to the guidance of PedsQL manuals. Higher scores mean better function. The items were listed as an appendix in Supplementary Table S1.
Sex, age, tumor size, and ventroperitoneal (VP) placement were obtained from medical records or follow-up information. Ages at surgery and investigation were included in the analysis. Hydrocephalus was defined as Evans index >0.3. The tumor size was defined as the maximum diameter of the three planes. Tumor locations were categorized into midline and lateral. Pathology grades were classified as low grade (World Health Organization [WHO] I–II) and high grade (WHO III–IV). Chemotherapy and radiotherapy treatment information was acquired during the follow-up.
Data analysis was conducted using SPSS (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Descriptive statistics for continuous variables and percentages for categorical variables were calculated. PedsQL total scores and sub-scores are reported as the mean and standard deviation. A two-sample t-test or Chi-squared test was used to test for group differences. The Pearson’s correlation coefficient was calculated for continuous variables. A forward stepwise linear regression was performed in the multivariable analysis, and variables in the univariate analysis were included. Forward stepwise regression is a stepwise regression approach that starts from the null model and adds variables that improves the model the most, one at a time, until the stopping criterion is met.
A total of 69 patients who received posterior fossa tumor resection between 2015 and 2019 were included in this study. Of these, 22 patients were diagnosed with CMS after surgery. All patients with CMS restored their speaking abilities (be able to speak conversational speech) prior to the investigation. The median duration of mutism was 6.29 (range: 1–19.43) weeks (see Table 1). Of the patients with CMS, 28.6% restored their speech within 1 month and 76.2% did so within 3 months.
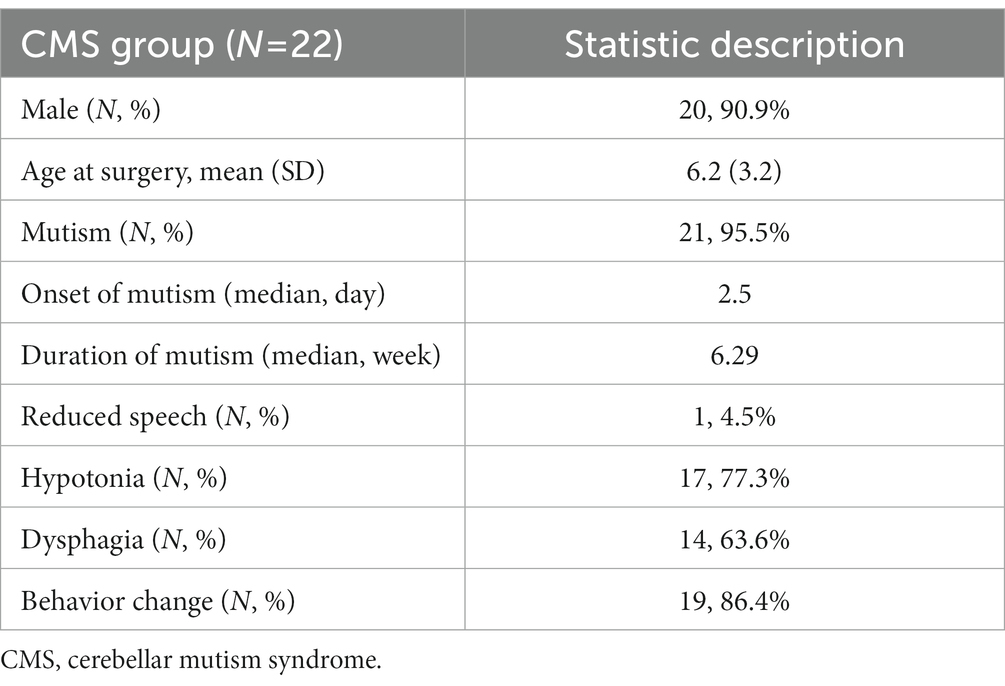
Table 1. CMS patient’s characteristics.
Demographic information and clinical characteristics of the two groups of children are presented in Table 2. The median age at surgery of the cohort was 5.4 [3.0, 8.2] years, and no significant difference was detected between the CMS (5.8 [4.2, 7.7]) and non-CMS groups (5.3 [2.9, 8.6]). Compared with the non-CMS group, the CMS group had a greater proportion of male participants (90.9% vs. 48.9, p = 0.002). The two groups showed significant differences in hydrocephalus, tumor location, presurgical VP shunt, extent of resection, surgical routes, pathology, hypotonia, oropharyngeal dysfunction, and behavioral change (p < 0.05). Tumor size was evenly distributed between the two groups.
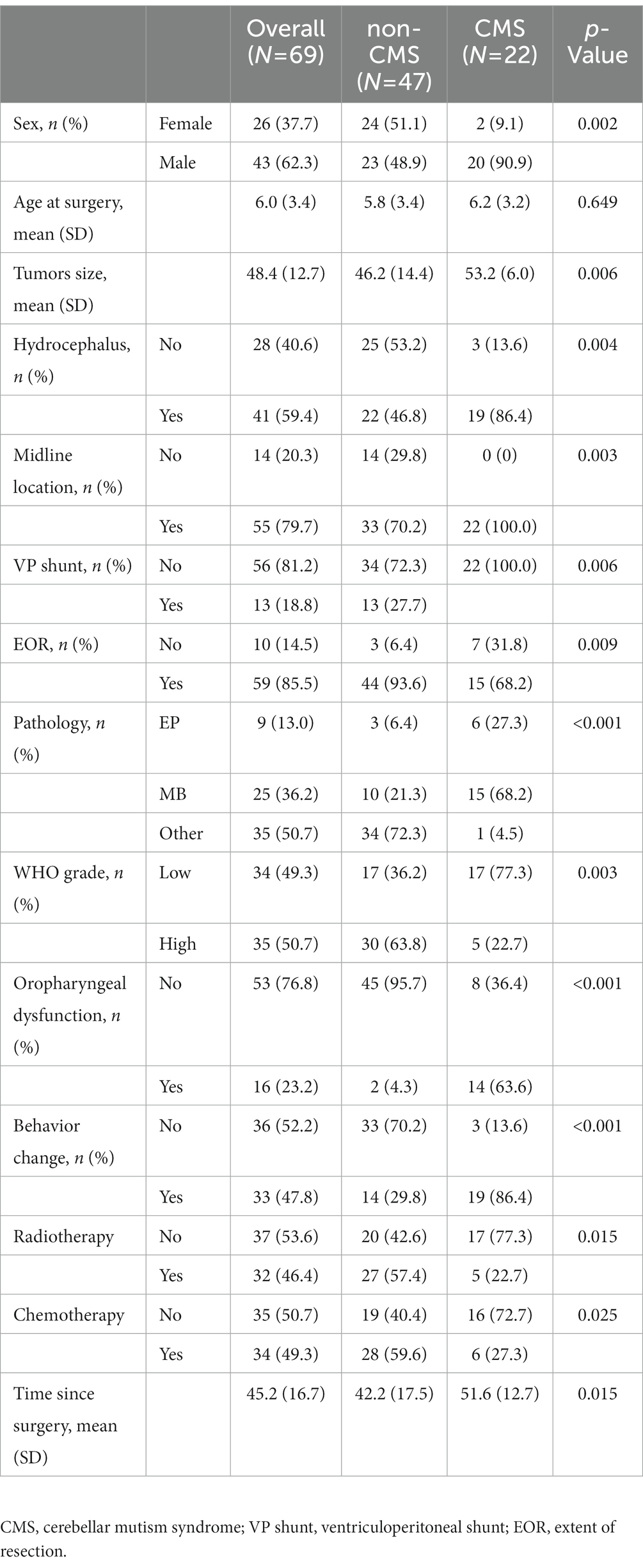
Table 2. Patients clinical characteristics.
The median follow-up period between surgery and this assessment was 2.5 years. Children diagnosed with CMS had significantly lower total and subdomain scores than non-CMS children (p < 0.05), except for emotional scores (p > 0.05) (Table 3).
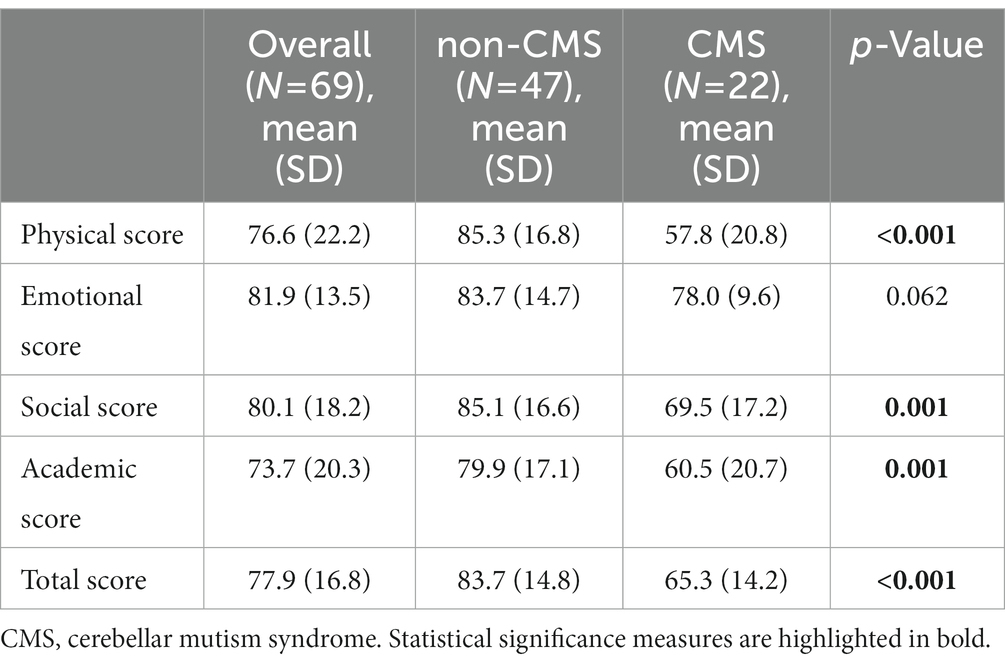
Table 3. comparison of QOL between CMS and non-CMS patients.
The items in each domain were compared between the two groups (Table 4). Among the 23 items, children with CMS scored significantly lower on 15 items than the non-CMS children. In the emotional domain, score of Item E2 was significantly lower in children with CMS than non-CMS children (3.2 ± 0.8 vs. 3.7 ± 0.9, p = 0.023).
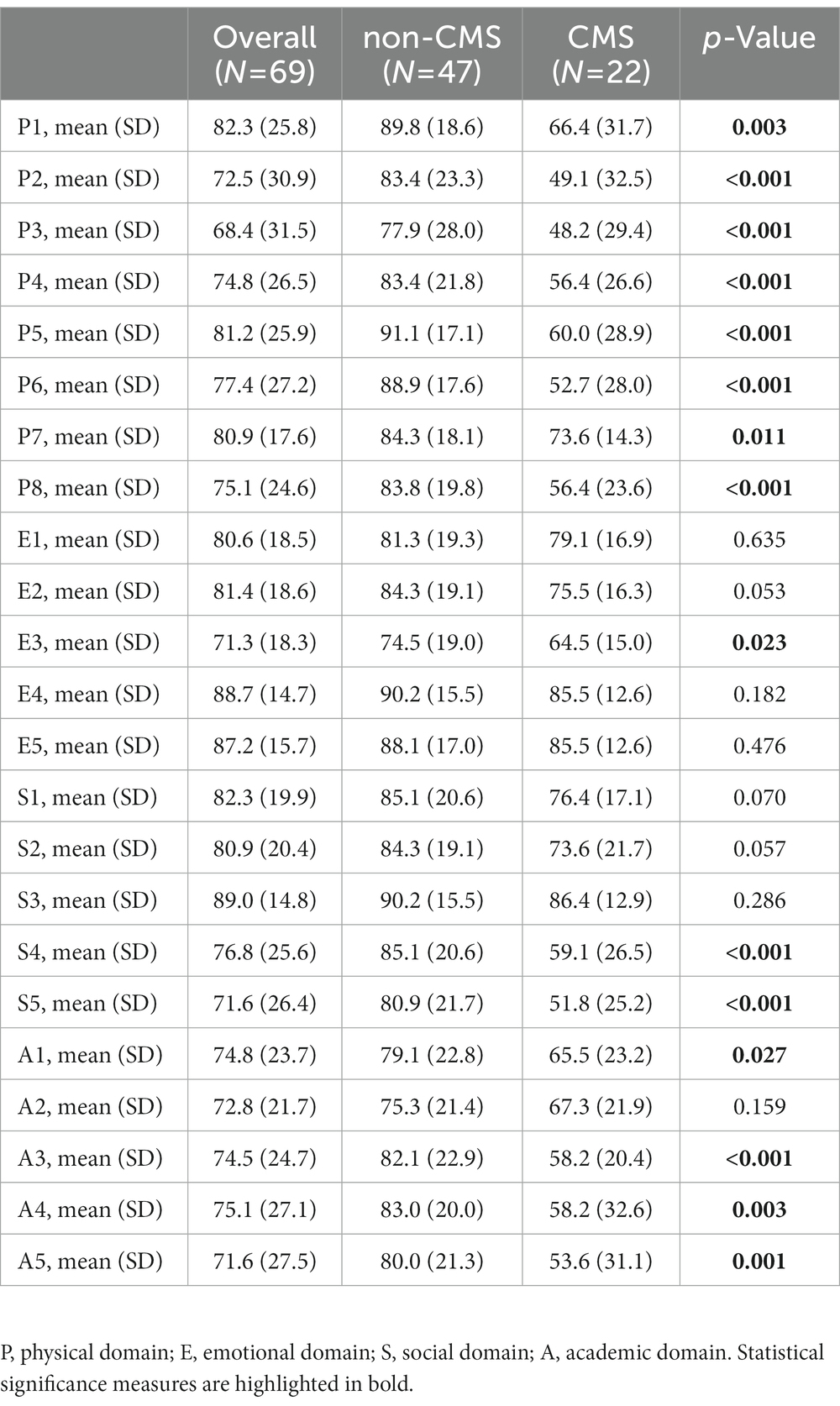
Table 4. Items comparison between CMS and non-CMS patients.
In the univariate analysis, the correlation or association between QoL score and clinical variables was presented with Pearson’s coefficient or difference of the mean values and p values. A weak negative correlation (−0.26 to −0.38, p < 0.05) was observed between age at surgery and QoL total score or its subdomain scores. Diagnosis of CMS, male sex, VP shunt placement, higher WHO tumor grade, radiotherapy, chemotherapy, tumor rest in midline location, and presence with hydrocephalus are associated with lower total score of QoL or sub-score of QoL (range of difference: −6.4 to −26.3, p < 0.05). Tumor size, extend of resection, and time to surgery were not associated with scores of QoL or its subdomains (p > 0.05) (see Table 5).
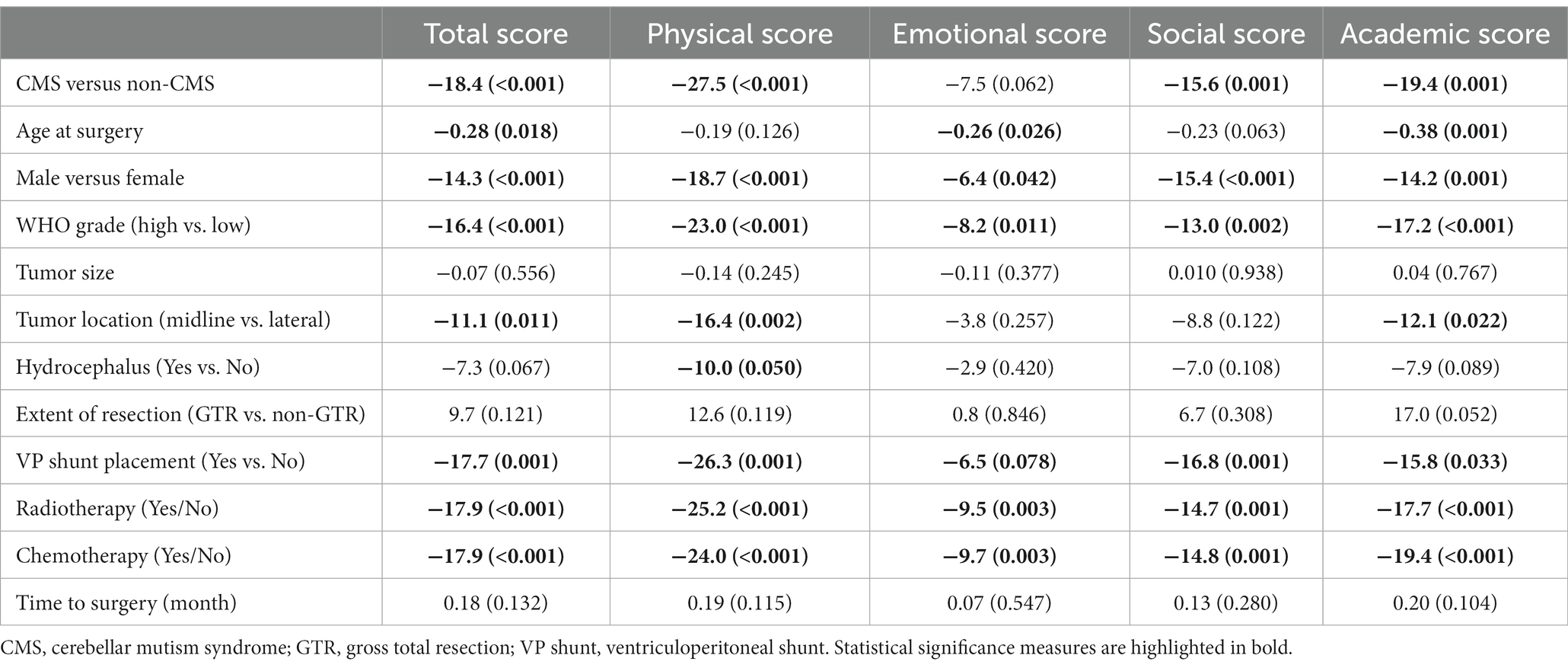
Table 5. Association of QOL and clinical variables.
Forward stepwise multivariable analyses were conducted to investigate independent risk factors of QoL total score and subdomain scores, and all variables in the univariate analysis were included. Diagnosis of CMS (coefficient: −8.61, 95%CI: [−16.95, −0.27], p = 0.043), older age at surgery (coefficient: −1.30, 95%CI: [−2.24, −0.36], p = 0.007), and receiving chemotherapy (coefficient: −9.82, 95%CI: [−17.48, −2.17], p = 0.013) were independently associated with lower total QoL score. CMS (coefficient: −15.31, 95%CI: [−25.77, −4.86]), VP shunt placement (coefficient: −12.86, 95%CI: [−24.07, −1.65], p = 0.025), and radiotherapy (coefficient: −13.63, 95%CI: [−23.32, −3.92], p = 0.007) were independently associated with lower physical scores. Chemotherapy (coefficient: −9.11, 95%CI: [−15.08, −3.14], p = 0.003) and age at surgery (coefficient: −0.96, 95%CI: [−1.85, −0.06], p = 0.037) were associated with emotional scores. Male sex (coefficient: −13.68, 95%CI: [−21.63, −5.75], p = 0.001) and VP shunt placement (coefficient: −14.36, 95%CI: [−24.20, −4.53], p = 0.005) were associated with lower social scores. Chemotherapy (coefficient: −17.45, 95%CI: [−25.28, −9.61], p < 0.001) and older age at surgery (coefficient: −1.92, 95%CI: [−3.10, −0.74], p = 0.002) were associated with lower academic scores, whereas extent of resection (coefficient: 12.16, 95%CI: [2.04, 24.29], p < 0.021) was associated with higher academic scores (Table 6). The multicollinearity diagnosis found no significant dependency among the predicted variables.
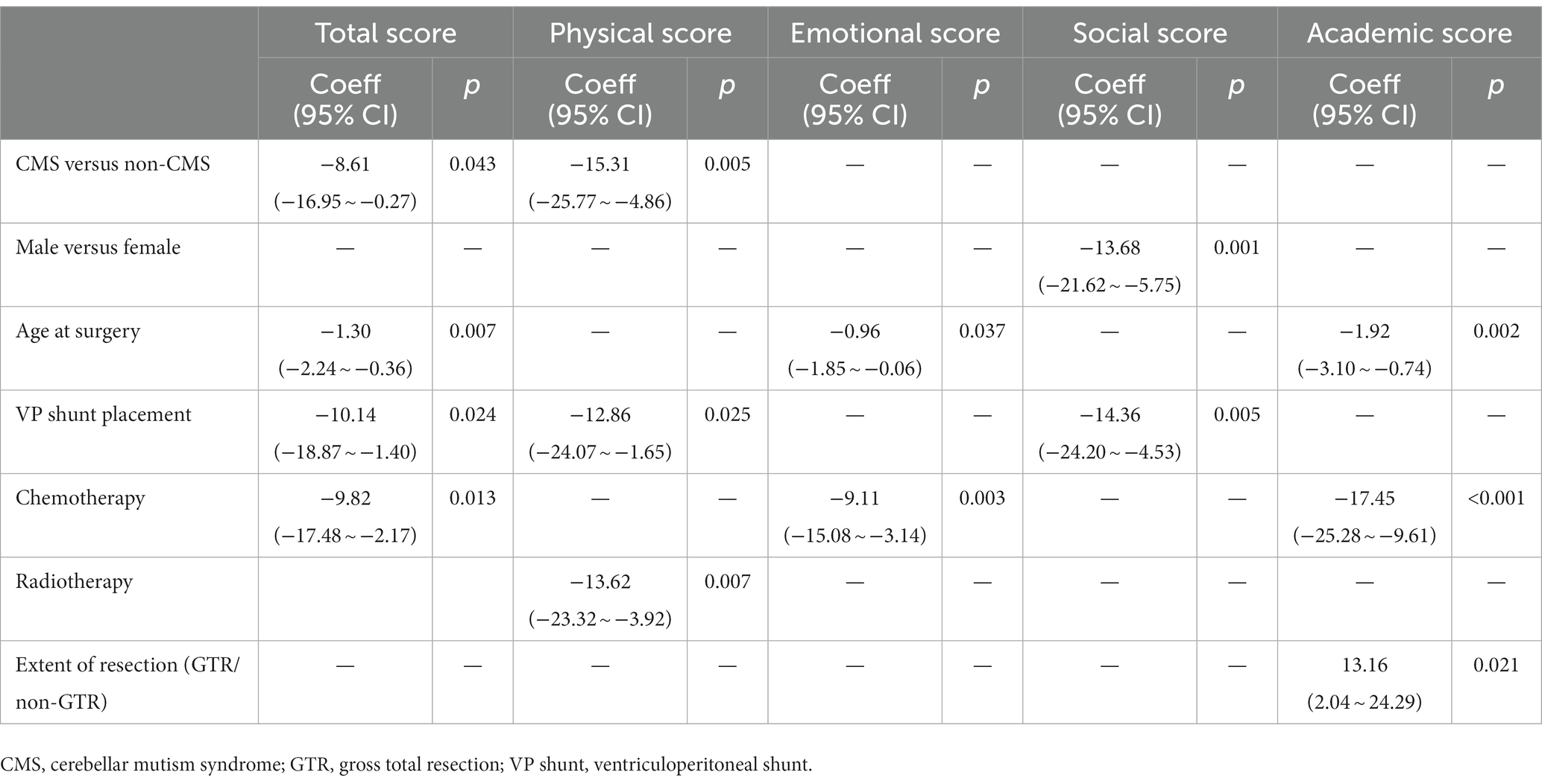
Table 6. Multivariable analysis for risk factors of PedsQL scores.
CMS has been proposed to involve multiple domains, including speech, motor, emotion, and cognitive functions. Previous studies have concentrated on risk factors for CMS, whereas few studies have been conducted on children’s QoL. It has been suggested that patients with CMS should undergo routine follow-up to monitor emotional, behavioral, and social problems over time (Gora et al., 2017). In this cross-sectional study, we investigated the long-term QoL of children who underwent posterior fossa surgery and compared children with and without CMS. Our data showed that children with CMS had significantly lower QoL and subdomain scores than non-CMS children. No significant association was found between time to surgery and overall QoL scores. These findings stress the long-term negative influence of CMS, which is not only restricted to speech function.
Multivariable analysis was performed to eliminate the interference of other clinical variables, since patients with and without CMS were not evenly distributed with regard to clinical variables in the baseline comparison. This demonstrated that CMS was consistently associated with lower QoL and physical scores in univariable and multivariable analyses in our study. Children with CMS had the lowest score and greatest difference in physical function compared to non-CMS children. The observed weakness in physical function is consistent with previous findings (Hartley et al., 2019; Grieco et al., 2020), and should be given more attention.
The CMS group had significantly lower social score than the non-CMS group in the univariable analysis, despite this losing statistical significance in the multivariable analysis. This has been reported in survivors of other cancers; however, the CMS group seemed to face more difficulty in dealing with social relations (Barrera et al., 2005; Ness and Gurney, 2007; Lund et al., 2011). The cerebellum has been shown to participate in social functions (Cutando et al., 2022). Changes in dopamine D2 receptors levels in cerebellum of male mice during adulthood alter sociability and preference for social novelty (Cutando et al., 2022). Functional MRI studies have revealed three distinct representations for social function in cerebellum. Schmahmann holds that like coordinating the motor, the cerebellum modulates behavior, maintaining it around a homeostatic baseline appropriate to context (Guell et al., 2018). Previous studies based on semi-structured interviews found that survivors of CMS had difficulties maintaining social relations (Camara et al., 2020; Wibroe et al., 2021). In the multivariable analysis, male sex was independently correlated with lower social score. We will discuss this further below. Overall, our results suggest that more attention should be paid to psychological rehabilitation in children with CMS.
Cognitive impairment and physical dysfunction have significant impacts on school scores (Nesayan et al., 2019; Fritz et al., 2020). Processing speed is a cognitive ability reflecting the ability to automatically process information and to process information quickly and outside of conscious awareness. Previous studies have found that patients with CMS exhibit impaired (>2 SD below the mean value) processing speed and below-average intellectual ability at 1 year postoperatively, with scores remaining low over time (Schreiber et al., 2017). In our study, the CMS group had significantly lower school scores in the long-term assessment than the non-CMS group, which is consistent with previous studies, despite losing statistical significance in the multivariate analysis. However, Julia et al. (Grieco et al., 2020) reported that 18 pairs of patients with or without CMS showed no difference in overall intelligence, and expressive and receptive vocabulary (mean follow-up time, 3.26 years). Further studies on this field may provide more compacted evidence.
Persistent emotional and behavioral dysregulation is another concern in children with CMS (Steinbok et al., 2003; Lanier and Abrams, 2017; Schreiber et al., 2017). In our study, no significant difference in emotional scores was found between patients with and without CMS, which is consistent with previous studies (Grieco et al., 2020). However, the analysis of each item of the scale showed that children with CMS were more susceptible to loss of temper than children without CMS. This indicates that emotional dysregulation exists among children after posterior fossa surgery, but its relationship with CMS still needs to be investigated in further research.
Radiotherapy and chemotherapy were not consistently correlated with QoL scores (An et al., 2011; Kuhlthau et al., 2012; Bull et al., 2014). There are studies (Penn et al., 2009; Aukema et al., 2013) that found no significant differences in the QoL of children who received surgery only and those who received surgery with adjuvant therapy. In contrast, a series of studies (Pogorzala et al., 2010; Kuhlthau et al., 2012; Netson et al., 2016) demonstrated the detrimental effects of radiotherapy or chemotherapy on QoL. In our study, chemotherapy and radiotherapy were related to lower QoL score and subdomain scores in both univariate and multivariate analyses. The detrimental effects of chemotherapy or radiotherapy may persist long term (Prabhu et al., 2014; Lawrie et al., 2019).
Male participants had poorer QoL scores across all subdomains than female participants in the univariable analysis in our study. However, in the multivariable analysis, sex was exclusively significantly associated with social scores, rather than QoL total score and other sub-domains. The relationship between sex and QoL in pediatric patients with brain tumors remains controversial (Bell et al., 2018). Previous reports indicated that males had lower school-related QoL score (Bhat et al., 2005; Lipak et al., 2022; Ljungman et al., 2022). However, there were also reports that women had poorer QoL scores than men, or that no significant difference existed between males and females (Bull et al., 2014; Barrera et al., 2017; Quast et al., 2018). No evidence has shown the sex effect for social performance in children with brain tumor (Litzelman et al., 2011). Previous studies have indicated the increased prevalence of CMS in males in contrast to females (Robertson et al., 2006; Gora et al., 2017; Yang et al., 2022a). Considering the male’s predominance in the CMS group, it is reasonable to presume that the lower QoL score and sub-domain scores are associated with CMS. And given the small sample size of our data, the impact of sex on QoL still needs to be validated in future studies.
Age at diagnosis was negatively associated with QoL scores in our results, which means patients receiving surgery at an older age have more deteriorative QoL scores. This was inconsistent with previous studies (Mulhern et al., 1992; Silber et al., 1992; Mulrooney et al., 2019; Sleurs et al., 2022). It was perceived that excessive treatment, including radiotherapy and chemotherapy, had a greater negative effect when children were younger. Mulhern et al. (1992) and Silber et al. (1992) found that Younger age with irradiation treatment was associated with lower intelligent performance. However, a systematic review demonstrated that older age at diagnosis was related to decreased QoL scores (Macartney et al., 2014). Although the harmful effect of radiotherapy and chemotherapy at a younger age is inevitable, the restoration ability of the somatic body decreases with age. With regard to the total QoL score, considering the capacity of compensation of all physical domains decreases gradually with age, younger age is expected to be a favorable predictor of QoL.
Hydrocephalus has been associated with inferior neurocognitive outcomes (Di Pinto et al., 2012; Brinkman et al., 2016). VP shunts are thought to be associated with favorable long-term QoL, since it addresses the increased intracranial pressure (Reimers et al., 2009). However, for children with brain tumors, this association may not hold true. In our study, VP shunt placement is a predictor of lower QoL scores. In our center, the removal of tumors is the highest priority to address the increased cranial pressure, rather than the VP shunt. The various complications associated with VP shunt should never be overlooked, and VP shunt placement should mainly be for patients with recurrent hydrocephalus after tumor resection. Therefore, patients with VP shunt placement may reflect worse medical experiences. Likewise, gross total resection was related to higher academic score, since non-gross total resection always occur when the tumor was infiltrative and malignant, and total resection cannot be easily performed.
No treatment or rehabilitation procedures for CMS have been established at present (Ashida et al., 2021). Treatment and rehabilitation should focus on three domains: language function, behavioral and cognitive function, and motor function. Pharmacological intervention, cognitive rehabilitation, and physical rehabilitation are the three main interventions at present. Several cases reported described mediation therapy such as corticosteroids, fluoxetine, thyrotropin-releasing hormone, bromocriptine and zolpidem, and modafinil, which were used in the acute stage to alleviate the symptoms of CMS (Catsman-Berrevoets, 2017; Molinari et al., 2019; Paquier et al., 2020). However, the results were inconsistent and not proven by larger-scale trials. Besides, speech therapists might help address mutism symptoms. Earlier intervention may provide the opportunity for avoiding the eventual emergence of long-term sequelae (Paquier et al., 2020). As regards behavioral and cognitive deficits, neuropsychological evaluation and the follow-up of long-term treatment are imperative for patients with CMS (Malbari et al., 2022). Studies have found that emotional intervention contributes to understand and manage emotions, and this may relive the emotional irritability in CMS children (Ratliff et al., 2022). This should be given more attention in future. The 2018 posterior fossa society meeting mentioned the opportunity of using transcranial direct current stimulation (tDCS) and transcranial magnetic stimulation (TMS) in the rehabilitation of CMS, which may resolve the diaschisis of the cerebellum and cerebrum. However, there is no direct evidence of the treatment effect of tDCS or TMS in patients with CMS. Future studies should pay more attention to this promising treatment.
Our study has several limitations. First, our study lacked baseline QoL assessment before surgery. As a result, we could not confirm that QoL scores of the children with CMS were worse than those of non-CMS children at baseline. Second, clinical variables were not evenly distributed between the two groups, especially because there were only two females in the CMS group, which may affect the representation of our results. Thirdly, the lack of information regarding the socioeconomic backgrounds of these families is another limitation of our study. The impact of socioeconomic background on rehabilitation treatment is important for the improvement of QoL score. In this study, we did not discuss the potential discriminative demographic and clinical variables between the groups, as only a proportion of the children with posterior fossa tumors in our center participated in the project, and the statistical analysis may contain sample biases. The small sample size may also result in selection bias. As for the risk factors of CMS, please refer to our previous studies, which enrolled a larger cohort (Yang et al., 2022a, b).
In summary, children with CMS exhibit poorer performance on QoL assessment, and motor dysfunction showed worse outcomes, which should be given more attention. The impact of the CMS on social and school performances cannot be ignored. Long-term neuropsychological assessment with individualized rehabilitation treatment is necessary to help these children return to a normal life. Although no significant difference was detected in the emotional scores, a significant difference in the outbreak of tempers was identified between the CMS and non-CMS groups. A more comprehensive investigation is needed to evaluate the emotional profile of patients after posterior fossa surgery.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of Beijing Children’s Hospital. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
KZ, WY, ZY, YC, XP, NZ, HS, YJ, and MG contributed to the study conception and design. HS and YJ performed the material preparation. NZ, YC, and XP performed the data collection. ZY and WY performed the data analysis. WY and KZ wrote the first draft of the manuscript. MG conducted the funding acquisition and supervision. KZ, WY, ZY, YC, XP, NZ, HS, YJ, and MG commented on previous versions of the manuscript. All authors contributed to the article and approved the submitted version.
This study was funded by Beijing Hospital’s Authority Clinical Medicine Development of Special Funding (code: XMLX202144) and Newborn Young Doctors Scientific Research Fund (Z-2019-41-2101-04).
We would like to thank Beijing Hospital’s Authority Clinical Medicine Development of Special Funding for foundation and Editage (www.editage.cn) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1130331/full#supplementary-material
QoL, Quality of life; CMS, Cerebellar mutism syndrome; VP shunt, Ventroperitoneal shunt; PedsQL, Pediatric Quality of Life Inventory; WHO, World Health Organization.
Aarsen, F. K., Paquier, P. F., Arts, W. F., Van Veelen, M. L., Michiels, E., Lequin, M., et al. (2009). Cognitive deficits and predictors 3 years after diagnosis of a pilocytic astrocytoma in childhood. J. Clin. Oncol. 27, 3526–3532. doi: 10.1200/JCO.2008.19.6303
An, K. J., Song, M. S., Sung, K. W., and Joung, Y. S. (2011). Health-related quality of life, activities of daily living and parenting stress in children with brain tumors. Psychiatry Investig. 8, 250–255. doi: 10.4306/pi.2011.8.3.250
Argyropoulos, G. P. D., van Dun, K., Adamaszek, M., Leggio, M., Manto, M., Masciullo, M., et al. (2020). The cerebellar cognitive affective/Schmahmann syndrome: a task force paper. Cerebellum 19, 102–125. doi: 10.1007/s12311-019-01068-8
Ashida, R., Nazar, N., Edwards, R., and Teo, M. (2021). Cerebellar Mutism syndrome: An overview of the pathophysiology in relation to the Cerebrocerebellar anatomy, risk factors, potential treatments, and outcomes. World Neurosurg. 153, 63–74. doi: 10.1016/j.wneu.2021.06.065
Aukema, E. J., Schouten-van Meeteren, A. Y., Last, B. F., Maurice-Stam, H., and Grootenhuis, M. A. (2013). Childhood brain tumor survivors at risk for impaired health-related quality of life. J. Pediatr. Hematol. Oncol. 35, 603–609. doi: 10.1097/MPH.0b013e31829b7ec6
Barrera, M., Atenafu, E. G., Schulte, F., Bartels, U., Sung, L., Janzen, L., et al. (2017). Determinants of quality of life outcomes for survivors of pediatric brain tumors. Pediatr. Blood Cancer 64:e26481. doi: 10.1002/pbc.26481
Barrera, M., Shaw, A. K., Speechley, K. N., Maunsell, E., and Pogany, L. (2005). Educational and social late effects of childhood cancer and related clinical, personal, and familial characteristics. Cancer 104, 1751–1760. doi: 10.1002/cncr.21390
Bell, H., Ownsworth, T., Lloyd, O., Sheeran, N., and Chambers, S. (2018). A systematic review of factors related to children's quality of life and mental health after brain tumor. Psychooncology 27, 2317–2326. doi: 10.1002/pon.4850
Bhat, S. R., Goodwin, T. L., Burwinkle, T. M., Lansdale, M. F., Dahl, G. V., Huhn, S. L., et al. (2005). Profile of daily life in children with brain tumors: an assessment of health-related quality of life. J. Clin. Oncol. 23, 5493–5500. doi: 10.1200/JCO.2005.10.190
Brinkman, T. M., Krasin, M. J., Liu, W., Armstrong, G. T., Ojha, R. P., Sadighi, Z. S., et al. (2016). Long-term neurocognitive functioning and social attainment in adult survivors of pediatric CNS tumors: results from the St Jude lifetime cohort study. J. Clin. Oncol. 34, 1358–1367. doi: 10.1200/JCO.2015.62.2589
Bull, K. S., Liossi, C., Culliford, D., Peacock, J. L., Kennedy, C. R., Children's, C., et al. (2014). Child-related characteristics predicting subsequent health-related quality of life in 8-to 14-year-old children with and without cerebellar tumors: a prospective longitudinal study. Neurooncol Pract 1, 114–122. doi: 10.1093/nop/npu016
Camara, S., Fournier, M. C., Cordero, P., Melero, J., Robles, F., Esteso, B., et al. (2020). Neuropsychological profile in children with posterior fossa tumors with or without postoperative cerebellar Mutism syndrome (CMS). Cerebellum 19, 78–88. doi: 10.1007/s12311-019-01088-4
Catsman-Berrevoets, C. E. (2017). Cerebellar mutism syndrome: cause and rehabilitation. Curr. Opin. Neurol. 30, 133–139. doi: 10.1097/WCO.0000000000000426
Cheng, C.-P., Luh, W.-M., Yang, A.-L., Su, C.-T., and Lin, C.-Y. (2015). agreement of children and parents scores on Chinese version of pediatric quality of life inventory version 4.0: further psychometric development. Appl. Res. Qual. Life 11, 891–906. doi: 10.1007/s11482-015-9405-z
Clausi, S., Coricelli, G., Pisotta, I., Pavone, E. F., Lauriola, M., Molinari, M., et al. (2015). Cerebellar damage impairs the self-rating of regret feeling in a gambling task. Front. Behav. Neurosci. 9:113. doi: 10.3389/fnbeh.2015.00113
Conklin, H. M., Li, C., Xiong, X., Ogg, R. J., and Merchant, T. E. (2008). Predicting change in academic abilities after conformal radiation therapy for localized ependymoma. J. Clin. Oncol. 26, 3965–3970. doi: 10.1200/JCO.2007.15.9970
Cutando, L., Puighermanal, E., Castell, L., Tarot, P., Belle, M., Bertaso, F., et al. (2022). Cerebellar dopamine D2 receptors regulate social behaviors. Nat. Neurosci. 25, 900–911. doi: 10.1038/s41593-022-01092-8
Di Pinto, M., Conklin, H. M., Li, C., and Merchant, T. E. (2012). Learning and memory following conformal radiation therapy for pediatric craniopharyngioma and low-grade glioma. Int. J. Radiat. Oncol. Biol. Phys. 84, e363–e369. doi: 10.1016/j.ijrobp.2012.03.066
Eaton, B. R., Goldberg, S., Tarbell, N. J., Lawell, M. P., Gallotto, S. L., Weyman, E. A., et al. (2020). Long-term health-related quality of life in pediatric brain tumor survivors receiving proton radiotherapy at <4 years of age. Neuro-Oncology 22, 1379–1387. doi: 10.1093/neuonc/noaa042
Fritz, J., Cöster, M. E., Rosengren, B. E., Karlsson, C., and Karlsson, M. K. (2020). Daily school physical activity improves academic performance. Sports (Basel) 8:83. doi: 10.3390/sports8060083
Gora, N. K., Gupta, A., and Sinha, V. D. (2017). Cerebellar Mutism syndrome following midline posterior fossa tumor resection in children: An institutional experience. J. Pediatr. Neurosci. 12, 313–319. doi: 10.4103/jpn.JPN_23_17
Grieco, J. A., Abrams, A. N., Evans, C. L., Yock, T. I., and Pulsifer, M. B. (2020). A comparison study assessing neuropsychological outcome of patients with post-operative pediatric cerebellar mutism syndrome and matched controls after proton radiation therapy. Childs Nerv. Syst. 36, 305–313. doi: 10.1007/s00381-019-04299-6
Gronbaek, J. K., Wibroe, M., Toescu, S., Fric, R., Thomsen, B. L., Moller, L. N., et al. (2021). Group: postoperative speech impairment and surgical approach to posterior fossa tumours in children: a prospective European multicentre cohort study. Lancet child Adolesc. Health 5, 814–824. doi: 10.1016/S2352-4642(21)00274-1
Gudrunardottir, T., Morgan, A. T., Lux, A. L., Walker, D. A., Walsh, K. S., Wells, E. M., et al. (2016). Consensus paper on post-operative pediatric cerebellar mutism syndrome: the Iceland Delphi results. Childs Nerv. Syst. 32, 1195–1203. doi: 10.1007/s00381-016-3093-3
Guell, X., Gabrieli, J. D. E., and Schmahmann, J. D. (2018). Triple representation of language, working memory, social and emotion processing in the cerebellum: convergent evidence from task and seed-based resting-state fMRI analyses in a single large cohort. NeuroImage 172, 437–449. doi: 10.1016/j.neuroimage.2018.01.082
Hartley, H., Pizer, B., Lane, S., Sneade, C., Williams, R., Mallucci, C., et al. (2019). Incidence and prognostic factors of ataxia in children with posterior fossa tumors. Neurooncol Pract 6, 185–193. doi: 10.1093/nop/npy033
Hoche, F., Guell, X., Sherman, J. C., Vangel, M. G., and Schmahmann, J. D. (2016). Cerebellar contribution to social cognition. Cerebellum 15, 732–743. doi: 10.1007/s12311-015-0746-9
Khan, R. B., Patay, Z., Klimo, P., Huang, J., Kumar, R., Boop, F. A., et al. (2021). Clinical features, neurologic recovery, and risk factors of postoperative posterior fossa syndrome and delayed recovery: a prospective study. Neuro-Oncology 23, 1586–1596. doi: 10.1093/neuonc/noab030
Kuhlthau, K. A., Pulsifer, M. B., Yeap, B. Y., Rivera Morales, D., Delahaye, J., Hill, K. S., et al. (2012). Prospective study of health-related quality of life for children with brain tumors treated with proton radiotherapy. J. Clin. Oncol. 30, 2079–2086. doi: 10.1200/JCO.2011.37.0577
Lanier, J. C., and Abrams, A. N. (2017). Posterior fossa syndrome: review of the behavioral and emotional aspects in pediatric cancer patients. Cancer 123, 551–559. doi: 10.1002/cncr.30238
Lawrie, T. A., Gillespie, D., Dowswell, T., Evans, J., Erridge, S., Vale, L., et al. (2019). Long-term neurocognitive and other side effects of radiotherapy, with or without chemotherapy, for glioma. Cochrane Database Syst Rev 8:CD013047. doi: 10.1002/14651858.CD013047.pub2
Li, B., Feng, J., Chen, L., Li, Y., Wang, J., Lv, W., et al. (2021). Relapse pattern and quality of life in patients with localized basal ganglia germinoma receiving focal radiotherapy, whole-brain radiotherapy, or craniospinal irradiation. Radiother. Oncol. 158, 90–96. doi: 10.1016/j.radonc.2021.02.009
Lipak, K. G., Rausch, J. R., Fisher, R. S., Prussien, K. V., Clark, O. E., Kenney, A. E., et al. (2022). The impact of CNS-directed treatment on quality of life in childhood cancer survivors. Qual. Life Res. 31, 817–829. doi: 10.1007/s11136-021-02984-1
Litzelman, K., Catrine, K., Gangnon, R., and Witt, W. P. (2011). Quality of life among parents of children with cancer or brain tumors: the impact of child characteristics and parental psychosocial factors. Qual. Life Res. 20, 1261–1269. doi: 10.1007/s11136-011-9854-2
Ljungman, L., Remes, T., Westin, E., Huittinen, A., Lonnqvist, T., Sirkia, K., et al. (2022). Health-related quality of life in long-term survivors of childhood brain tumors: a population-based cohort study. Support Care Cancer 30, 5157–5166. doi: 10.1007/s00520-022-06905-x
Lund, L. W., Schmiegelow, K., Rechnitzer, C., and Johansen, C. (2011). A systematic review of studies on psychosocial late effects of childhood cancer: structures of society and methodological pitfalls may challenge the conclusions. Pediatr. Blood Cancer 56, 532–543. doi: 10.1002/pbc.22883
Macartney, G., Harrison, M. B., VanDenKerkhof, E., Stacey, D., and McCarthy, P. (2014). Quality of life and symptoms in pediatric brain tumor survivors: a systematic review. J. Pediatr. Oncol. Nurs. 31, 65–77. doi: 10.1177/1043454213520191
Malbari, F., Gill, J., Daigle, A., Rodriguez, L. L., Raghubar, K. P., Davis, K. C., et al. (2022). Cerebellar Mutism syndrome in pediatric Neuro-oncology: A multidisciplinary perspective and call for research priorities. Pediatr. Neurol. 132, 4–10. doi: 10.1016/j.pediatrneurol.2022.04.014
Molinari, E., Oto, M., Waterston, A., and Fullerton, N. (2019). Modafinil in the rehabilitation of a patient with post-surgical posterior fossa syndrome: a lesson to be learned? Cerebellum Ataxias 6:11. doi: 10.1186/s40673-019-0105-6
Moxon-Emre, I., Bouffet, E., Taylor, M. D., Laperriere, N., Scantlebury, N., Law, N., et al. (2014). Impact of craniospinal dose, boost volume, and neurologic complications on intellectual outcome in patients with medulloblastoma. J. Clin. Oncol. 32, 1760–1768. doi: 10.1200/JCO.2013.52.3290
Mulhern, R. K., Hancock, J., Fairclough, D., and Kun, L. (1992). Neuropsychological status of children treated for brain tumors: a critical review and integrative analysis. Med. Pediatr. Oncol. 20, 181–191. doi: 10.1002/mpo.2950200302
Mulhern, R. K., Palmer, S. L., Merchant, T. E., Wallace, D., Kocak, M., Brouwers, P., et al. (2005). Neurocognitive consequences of risk-adapted therapy for childhood medulloblastoma. J. Clin. Oncol. 23, 5511–5519. doi: 10.1200/JCO.2005.00.703
Mulrooney, D. A., Hyun, G., Ness, K. K., Bhakta, N., Pui, C. H., Ehrhardt, M. J., et al. (2019). The changing burden of long-term health outcomes in survivors of childhood acute lymphoblastic leukaemia: a retrospective analysis of the St Jude lifetime cohort study. Lancet Haematol 6, e306–e316. doi: 10.1016/S2352-3026(19)30050-X
Nesayan, A., Amani, M., and Gandomani, R. A. (2019). Cognitive profile of children and its relationship with academic performance. Basic Clin. Neurosci. 10, 165–174. doi: 10.32598/bcn.9.10.230
Ness, K. K., and Gurney, J. G. (2007). Adverse late effects of childhood cancer and its treatment on health and performance. Annu. Rev. Public Health 28, 279–302. doi: 10.1146/annurev.publhealth.28.021406.144049
Netson, K. L., Ashford, J. M., Skinner, T., Carty, L., Wu, S., Merchant, T. E., et al. (2016). Executive dysfunction is associated with poorer health-related quality of life in pediatric brain tumor survivors. J. Neuro-Oncol. 128, 313–321. doi: 10.1007/s11060-016-2113-1
Ostrom, Q. T., Cioffi, G., Waite, K., Kruchko, C., and Barnholtz-Sloan, J. S. (2021). CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2014–2018. Neuro Oncol. 23, iii1–iii105. doi: 10.1093/neuonc/noab200
Paquier, P. F., Walsh, K. S., Docking, K. M., Hartley, H., Kumar, R., and Catsman-Berrevoets, C. E. (2020). Post-operative cerebellar mutism syndrome: rehabilitation issues. Childs Nerv. Syst. 36, 1215–1222. doi: 10.1007/s00381-019-04229-6
Penn, A., Lowis, S. P., Stevens, M. C., Hunt, L. P., Shortman, R. I., McCarter, R. J., et al. (2009). Family, demographic and illness-related determinants of HRQL in children with brain tumours in the first year after diagnosis. Pediatr. Blood Cancer 53, 1092–1099. doi: 10.1002/pbc.22157
Peragallo, J. H., Bruce, B. B., Vasseneix, C., Jariyakosol, S., Janss, A. J., Newman, N. J., et al. (2021). Vision-related quality-of-life in pediatric primary brain tumor patients. J. Neuro-Oncol. 154, 365–373. doi: 10.1007/s11060-021-03835-2
Pogorzala, M., Styczynski, J., Kurylak, A., Debski, R., Wojtkiewicz, M., and Wysocki, M. (2010). Health-related quality of life among paediatric survivors of primary brain tumours and acute leukaemia. Qual. Life Res. 19, 191–198. doi: 10.1007/s11136-009-9580-1
Prabhu, R. S., Won, M., Shaw, E. G., Hu, C., Brachman, D. G., Buckner, J. C., et al. (2014). Effect of the addition of chemotherapy to radiotherapy on cognitive function in patients with low-grade glioma: secondary analysis of RTOG 98-02. J Clin Oncol 32, 535–541. doi: 10.1200/JCO.2013.53.1830
Quast, L. F., Phillips, P. C., Li, Y., Kazak, A. E., Barakat, L. P., and Hocking, M. C. (2018). A prospective study of family predictors of health-related quality of life in pediatric brain tumor survivors. Pediatr. Blood Cancer 65:e26976. doi: 10.1002/pbc.26976
Ratliff, E. L., Kerr, K. L., Cosgrove, K. T., Simmons, W. K., and Morris, A. S. (2022). The role of neurobiological bases of dyadic emotion regulation in the development of psychopathology: cross-brain associations between parents and children. Clin. Child. Fam. Psychol. Rev. 25, 5–18. doi: 10.1007/s10567-022-00380-w
Reimers, T. S., Mortensen, E. L., Nysom, K., and Schmiegelow, K. (2009). Health-related quality of life in long-term survivors of childhood brain tumors. Pediatr. Blood Cancer 53, 1086–1091. doi: 10.1002/pbc.22122
Robertson, P. L., Muraszko, K. M., Holmes, E. J., Sposto, R., Packer, R. J., Gajjar, A., et al. (2006). Children's oncology: incidence and severity of postoperative cerebellar mutism syndrome in children with medulloblastoma: a prospective study by the Children's oncology group. J. Neurosurg. 105, 444–451. doi: 10.3171/ped.2006.105.6.444
Sadeh, M., and Cohen, I. (2001). Transient loss of speech after removal of posterior fossa tumors-one aspect of a larger neuropsychological entity: the cerebellar cognitive affective syndrome. Pediatr. Hematol. Oncol. 18, 423–426. doi: 10.1080/088800101750476005
Schmahmann, J. D. (2020). Pediatric post-operative cerebellar mutism syndrome, cerebellar cognitive affective syndrome, and posterior fossa syndrome: historical review and proposed resolution to guide future study. Childs Nerv. Syst. 36, 1205–1214. doi: 10.1007/s00381-019-04253-6
Schreiber, J. E., Palmer, S. L., Conklin, H. M., Mabbott, D. J., Swain, M. A., Bonner, M. J., et al. (2017). Posterior fossa syndrome and long-term neuropsychological outcomes among children treated for medulloblastoma on a multi-institutional, prospective study. Neuro-Oncology 19, 1673–1682. doi: 10.1093/neuonc/nox135
Silber, J. H., Radcliffe, J., Peckham, V., Perilongo, G., Kishnani, P., Fridman, M., et al. (1992). Whole-brain irradiation and decline in intelligence: the influence of dose and age on IQ score. J. Clin. Oncol. 10, 1390–1396. doi: 10.1200/JCO.1992.10.9.1390
Sleurs, C., Lemiere, J., Bullens, K., and Jacobs, S. (2022). QOL-08. Visual memory and potential clinical risk factors in long-term survivors of a childhood brain tumor. Neuro Oncol 24, i134–i135. doi: 10.1093/neuonc/noac079.491
Steinbok, P., Cochrane, D. D., Perrin, R., and Price, A. (2003). Mutism after posterior fossa tumour resection in children: incomplete recovery on long-term follow-up. Pediatr. Neurosurg. 39, 179–183. doi: 10.1159/000072468
Steinlin, M., Imfeld, S., Zulauf, P., Boltshauser, E., Lovblad, K. O., Ridolfi Luthy, A., et al. (2003). Neuropsychological long-term sequelae after posterior fossa tumour resection during childhood. Brain 126, 1998–2008. doi: 10.1093/brain/awg195
Stoodley, C. J., MacMore, J. P., Makris, N., Sherman, J. C., and Schmahmann, J. D. (2016). location of lesion determines motor vs. cognitive consequences in patients with cerebellar stroke. Neuroimage Clin 12, 765–775. doi: 10.1016/j.nicl.2016.10.013
Varni, J. W., Limbers, C. A., and Burwinkle, T. M. (2007). Parent proxy-report of their children's health-related quality of life: an analysis of 13, 878 parents' reliability and validity across age subgroups using the Peds QL 4.0 generic Core scales. Health Qual. Life Outcomes 5:2. doi: 10.1186/1477-7525-5-2
von Hoff, K., Kieffer, V., Habrand, J. L., Kalifa, C., Dellatolas, G., and Grill, J. (2008). Impairment of intellectual functions after surgery and posterior fossa irradiation in children with ependymoma is related to age and neurologic complications. BMC Cancer 8:15. doi: 10.1186/1471-2407-8-15
Wibroe, M., Ingersgaard, M. V., Larsen, H. B., Juhler, M., and Piil, K. (2021). Living with the cerebellar mutism syndrome: long-term challenges of the diagnosis. Acta Neurochir. 163, 1291–1298. doi: 10.1007/s00701-020-04479-3
Yang, W., Ge, M., Zhu, K., Chen, J., Yang, P., Cai, Y., et al. (2022a). Male predisposition in cerebellar Mutism syndrome: a cohort study. Cerebellum. doi: 10.1007/s12311-022-01449-6
Keywords: cerebellar mutism syndrome, quality of life, PedsQL, risk factors, long-term
Citation: Zhu K, Yang W, Ying Z, Cai Y, Peng X, Zhang N, Sun H, Ji Y and Ge M (2023) Long-term postoperative quality of life in childhood survivors with cerebellar mutism syndrome. Front. Psychol. 14:1130331. doi: 10.3389/fpsyg.2023.1130331
Edited by:
Marta Tremolada, University of Padua, ItalyReviewed by:
Geraldina Poggi, Eugenio Medea (IRCCS), ItalyCopyright © 2023 Zhu, Yang, Ying, Cai, Peng, Zhang, Sun, Ji and Ge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming Ge, bWluZ19nZUAxMjYuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.