
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychol., 20 April 2023
Sec. Psycho-Oncology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1125545
This article is part of the Research TopicHighlights in Psycho-Oncology: Study ProtocolsView all 8 articles
 Anja Mehnert-Theuerkauf1*†
Anja Mehnert-Theuerkauf1*† Julia Marie Hufeld1†
Julia Marie Hufeld1† Peter Esser1
Peter Esser1 Ute Goerling2
Ute Goerling2 Myriel Hermann2
Myriel Hermann2 Tanja Zimmermann3Hannah Reuter3
Tanja Zimmermann3Hannah Reuter3 Jochen Ernst1
Jochen Ernst1Background: Despite remarkable progress, cancer remains a life-threatening disease for millions of people worldwide, also resulting in significant psychosocial limitations. High-quality, comprehensive cancer care requires patient and family involvement and the provision of needs-based, targeted psychosocial services. Although progress has been made in understanding the occurrence of mental comorbidity and psychosocial distress in cancer patients, comparatively little is known about the course of psychological comorbidity and psychosocial distress in early survivorship among patients and their families. We therefore aim to estimate the prevalence of mental disorders according to the DSM-5, psychosocial distress, perceived needs for psychosocial support and utilization of psychosocial support offers in newly diagnosed cancer patients and their relatives, taking into account potential contributing biopsychosocial factors for the occurrence of psychological comorbidity.
Methods/design: This study follows a prospective multi-center observational cohort design across four measurement time points: within 2 months after cancer diagnosis (t1), and in the follow-up period at 6 months (t2), at 12 months (t3), and at 18 months (t4) after t1. Patients older than 18 years who have a confirmed initial diagnosis of a malignant solid tumor and are scheduled for cancer treatment at one of the participating cancer centers are eligible for study participation. Relatives of eligible patients are also eligible for study participation if they are older than 18 years. Patients are interviewed using the Structured Clinical Interview for DSM-5 Disorders (SCID-5-CV). In addition, patients and relatives receive a set of validated questionnaires at each measurement time point, covering comorbid conditions and functional performance, perceived psychological distress and quality of life, partnership aspects and social relationships, supportive care needs and use of psychosocial support services, health literacy, and health behavior and meaning in life.
Discussion: This prospective multi-center observational cohort study has a major focus on increasing quality of care and quality of life in cancer survivors through providing rigorous longitudinal data for the development and implementation of target group-specific psychosocial support services.
Trial registration: NCT04620564, date of registration 9/11/2020; DKG OnkoZert: Registrier-No.: ST-U134, date of registration 5/11/2021.
Despite remarkable progress in cancer research, diagnostics and treatment, cancer continues to affect millions of people worldwide as a life-threatening disease, associated with invasive interventions and often irreversible impairments (Sung et al., 2021). The increasing incidence of cancer in many countries will lead to a higher prevalence of cancer survivors in the coming years. Survivors in different age generations are affected to varying degrees by pre-existing as well as disease- and treatment-related physical and psychological comorbidities that are significant in their frequency and severity (Singer et al., 2013; Hartung et al., 2017; Götze et al., 2018, 2019; Smitherman et al., 2018; Niedzwiedz et al., 2019; Renzi et al., 2019; Chao et al., 2020). Mental comorbidity is understood as the presence of a mental disorder in addition to cancer that meets the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM) (American Psychiatric Association [APA], 2013) or the International Classification of Diseases (ICD) (World Health Organization [WHO], 2022). The meta-analysis by Mitchell et al. (2011) found pooled prevalence rates of 16.3% for depression, 19.4% for adjustment disorders, and 10.3% for anxiety disorders in over 70 international studies and more than 10,000 cancer patients in oncology and haemato-oncology settings. Combined diagnoses were common; the prevalence for any mood and/or anxiety disorder was 38.2%. Our research group found a 4-week prevalence of 31.8% for any mental disorder in a large epidemiological study in Germany, with anxiety disorders (11.5%) and adjustment disorders (11.1%) being most prevalent (Mehnert et al., 2014). The 12-month prevalence of any mental disorder here was 39.4% and the lifetime prevalence was 56.3% (Kuhnt et al., 2016). Over a 12-month period anxiety disorders and mood disorders were the most frequent mental disorders.
In distinction to the presence of a mental disorder, a large proportion of cancer patients suffer from a high degree of perceived distress, including anxiety and depressive mood (Herschbach et al., 2020; Bach et al., 2022). In a representative sample across all major tumor entities, 52% of patients reported high psychological distress. The highest distress levels were found in patients with female genital cancers or pancreatic cancer (Mehnert et al., 2018). In a sample of 10,153 patients with various types of cancer, Linden et al. (2012) found that 19% of patients suffered from clinical anxiety and further 23% from subclinical anxiety symptoms. In addition, 13% of the patients had clinical symptoms of depression and another 16.5% had subclinical symptoms.
Psychosocial adjustment to cancer varies widely, with some patients improving over time and others deteriorating. Studies on the course of distress, anxiety, and depression symptoms show different trajectories depending on individual coping strategies, long-term and late effects of cancer treatment, and psychosocial stressors before and during the survivorship phase (Lam et al., 2013; Hellstadius et al., 2017; Dionisi-Vici et al., 2021). Lopes et al. (2022) studied the course of anxiety and depressive symptoms in a cohort of 506 breast cancer patients who were followed for 5 years after cancer diagnosis. The authors identified three trajectories of anxiety symptoms and three of depressive symptoms. The trajectories of high anxiety and high depression during the 5 years of follow-up were equally frequent. One in five women was affected by each trajectory. The other two anxiety and two depression trajectories showed a decline in scores over time: one trajectory with mid-range scores and one with low scores for anxiety symptoms, and similarly, one mid-range scores and one low scores trajectory, for depression symptoms.
Higher levels of psychosocial distress have been found to be associated with significantly lower quality of life, higher morbidity and mortality (Russ et al., 2012; Walker et al., 2020, 2021; Varela-Moreno et al., 2022) and higher costs to the health system (Chiu et al., 2017). Correlates of psychological distress and mental comorbidity in cancer populations include female gender, poor physical functioning that is often associated with advanced disease status and more invasive cancer treatments, less social support and socioeconomic status (SES), measured by education, income, and/or occupation (Singer et al., 2013; Syrowatka et al., 2017; Sauer et al., 2019).
In particular, the relationship between SES and health, especially mental health, has been extensively demonstrated for other diseases (Fryers et al., 2003; Mirza and Jenkins, 2004; Hanel et al., 2009; Moreno-Peral et al., 2014; Mackenbach, 2019; Marmot, 2019; Toussaint and Herzog, 2020; Barbek et al., 2022). Research suggests a higher prevalence of psychological comorbidities and health burden in patients with lower SES, but data for cancer populations are insufficient. There are multiple reasons why social inequalities in health lead to different outcomes in terms of morbidity, mortality and quality of life. It is likely that patients with low SES are more likely to be exposed to negative psychosocial factors (Siegrist and Marmot, 2004). Behavioral and lifestyle factors play an important role in relation to tobacco and alcohol consumption, diet and physical activity. Furthermore, SES has an influence on health literacy, access to health information and the use of health services (Mackenbach et al., 2008). Structural aspects of the health system also affect SES-specific utilization behavior, such as access barriers to health services for people with lower SES.
Although progress has been made in understanding the occurrence of mental comorbidity and psychosocial distress in cancer patients, comparatively little is known about the course of psychological comorbidity and psychosocial distress in the early survivorship phase in patients and their relatives. Relatives and informal caregivers experience high levels of emotional distress such as anxiety, helplessness and hopelessness, depressed mood, and impaired quality of life (Sklenarova et al., 2015; Thana et al., 2021; Goodwin et al., 2022). Acute, long-term and late physical and psychosocial impairments due to the partner’s cancer, role changes, difficulties in coping with the disease or impaired family interaction processes are stressors for the relatives (Hagedoorn et al., 2008). Many informal caregivers also face a difficult task: while they are often the main source of emotional and practical support for the sick person and are involved in medical decision-making (Ernst et al., 2017; Laidsaar-Powell et al., 2017; Weissflog et al., 2017; Cincidda et al., 2022), they themselves have a high psychosocial burden that requires support (Zimmermann, 2022).
Hu et al. (2023) showed a higher risk of any mental disorder in spouses of cancer patients compared to spouses of individuals without cancer in a binational study in Denmark and Sweden. The risk of first-onset mental disorders increased by 30% during the first year after cancer diagnosis, especially for depression and stress-related disorders. The risk increase was thus particularly high during the first year following cancer diagnosis and persisted during the entire follow-up.
Therefore, comprehensive cancer carer requires the involvement of the patient’s family and social environment and the provision of needs-based psychosocial services for relatives. Considering biopsychosocial factors such as SES as influencing factors on distress and mental comorbidity according to the new diagnostic criteria (DSM-5) will provide much needed data for more targeted psychosocial care for groups with specific needs. The data will most likely also reveal factors that are important for strengthening resilience and resource orientation.
Our primary study aims are to (i) estimate the prevalence of mental disorders according to the DSM-5 (APA) in newly diagnosed cancer patients a few weeks after cancer diagnosis and over a follow-up period of 18 months; and (ii) to assess the frequency and extent of psychosocial distress, perceived needs for psychosocial support and utilization of psychosocial support offers in newly diagnosed cancer patients and their relatives a few weeks after cancer diagnosis and over a follow-up period of 18 months.
In particular, we take into account demographic factors such as age, sex, SES and cancer-related factors as potential contributing factors for the occurrence of psychosocial distress and supportive care needs in both patients and relatives. We further aim to identify and analyze moderating and mediating as well as associated factors such as dyadic coping, quality of life, fear of recurrence, adherence, and satisfaction with medical and psychosocial care for the occurrence of mental disorders, psychological distress, and supportive care needs.
The study follows a prospective multi-center observational cohort design across four measurement time points: within 2 months after cancer diagnosis (t1), and in the follow-up period at 6 months (t2), at 12 months (t3), and at 18 months (t4) after t1. The study is being conducted at the university cancer centers of the three main German study centers in Leipzig, Berlin and Hannover as well as at cooperating cancer centers in Braunschweig, Dresden, and Göttingen. The study design follows both STROBE statement for observational studies (Vandenbroucke et al., 2007) and Patient-Centered Outcomes Research Institute (PCORI) (Selby et al., 2012) methodology standards, including patient engagement, research questions and methods, data integrity and analysis, preventing and handling of missing data and dissemination of and implementation of study results.
The study is funded by the German Cancer Aid Foundation (Stiftung Deutsche Krebshilfe) (funding numbers: 70113544, 70113611, and 70113613) and additionally financially supported by the Department of Medical Psychology and Medical Sociology at the University Medical Center of Leipzig, by the Charité Comprehensive Cancer Center, Berlin, and the Department of Psychosomatic Medicine and Psychotherapy, Hannover Medical School, Hannover.
Patients older than 18 years who have a confirmed initial diagnosis of a malignant solid tumor according to the medical record and are scheduled for cancer treatment at one of the participating cancer centers are eligible for study participation. Further inclusion criteria are: sufficient knowledge of the German language, physical, psychological, and cognitive ability for study participation, and written informed consent for study participation.
Relatives of eligible patients are also eligible for study participation if they are older than 18 years and provide written informed consent for study participation.
Study enrolment began in April 2020 and ended in July 2022 (t1). Follow-up assessments (t2–t4) are projected to end in January 2024. Patients are consecutively screened by the study staff for inclusion criteria at the participating cancer centers. Eligible patients are contacted personally by trained study staff and receive written educational material describing the study. If it is not possible for the study team to contact the patient at the cancer center, for example due to COVID-19 patient safety restrictions, patients receive a letter sent at their home address. If patients have given their written informed consent to be contacted, they receive all documents and a phone call, in which they are also asked to name a relative. The relative should be from the patient’s immediate living environment, if possible. If the patient has consented, the study team receives the contact details of the relative to invite him/her to participate in the study as well.
Patients fulfilling the inclusion criteria who agreed to participate were interviewed using the German adaptation of the Structured Clinical Interview for DSM-5 Disorders (SCID-5) (First et al., 2015; Beesdo-Baum et al., 2019). The SCID-5 was administered face-to-face by trained study staff during inpatient care or by telephone due to COVID-19 patient safety restrictions (t1). At follow-up (t2–t4), the SCID-5 was performed usually by telephone.
In addition to the SCID-5, participating patients receive a set of validated questionnaires and a stamped return envelope. They are asked to complete the study questionnaires within 10 days and return it to the local study center. Alternatively, patients will be offered to complete the study questionnaires online via an individualized link using the LimeSurvey software (LimeSurvey GmbH, 2015). For the follow-up measurements (t2–t4), patients again receive the study questionnaires with a stamped return envelope by post or an individualized link to LimeSurvey.
Relatives are not interviewed with the SCID-5. They receive a set of validated study questionnaires according to the same data collection scheme at all measurement times (t1–t4) either by post with a prepaid envelope or via an individualized link to LimeSurvey.
Both patients and relatives will systematically receive a telephone reminder from the study team after 14 days and after 3 weeks if they have not completed and returned the questionnaire by then. Patients and relatives are also offered support by the trained study team if they have difficulties completing the study questionnaires.
Table 1 gives an overview over the study measures including the SCID-5 clinical interview and self-report questionnaires that will be completed by patients and relatives.
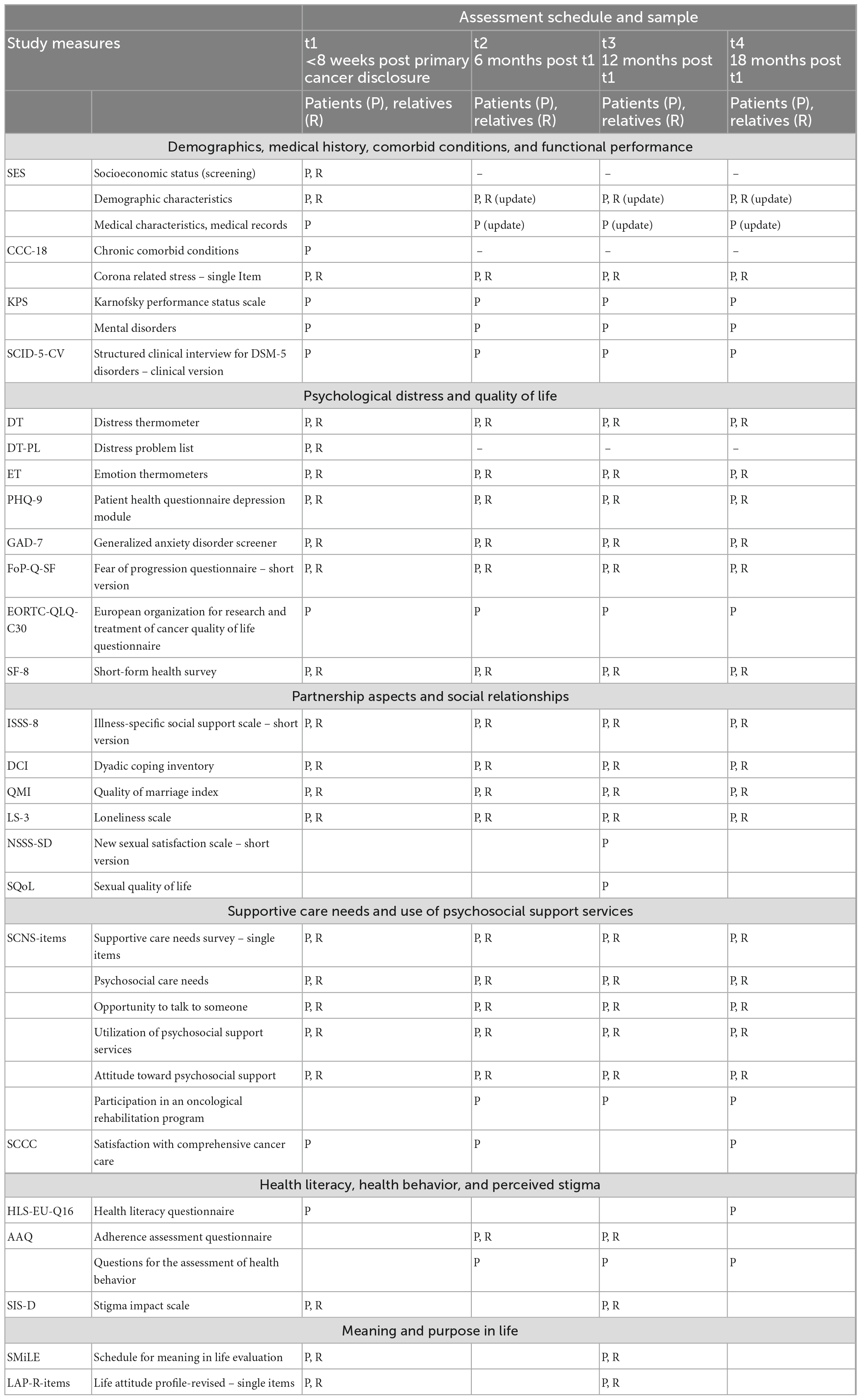
Table 1. Study assessment schedule and study measures.
Sociodemographic data such as age, sex, nationality, religion, marital status and partnership, children, school education, vocational training, monthly household income, employment status, occupational situation, housing situation, and residential area were collected during the SCID-5 telephone interview with the patients. The same demographic characteristics and additionally the relationship to the patient were collected from the relatives using a standardized questionnaire.
Socioeconomic status is determined by indicators including education, income, and/or occupation according to Winkler and Stolzenberg (2000).
Medical information on tumor entity, date of initial diagnosis and time since initial diagnosis, Union for International Cancer Control (UICC) disease stage, information on remission, recurrence and progression of cancer, metastases, and current cancer treatments is collected from medical records and standardized questionnaires.
We assess the number and severity of chronic diseases using a modified version of a self-report instrument developed by Bayliss et al. (2005). The original questionnaire includes a list of 23 common chronic conditions. Validation against the standard criterion of medical record review showed a mean sensitivity of 75% and a mean specificity of 92%. For our study, the specificity of the original scale was reduced by grouping similar disorders together. Two additional comorbidities were added: mental disorders and sensory disturbances. The modified questionnaire contained a final 18 conditions: hypertension, asthma, lung disease, diabetes, thyroid disease, chronic back pain, rheumatism, osteoarthritis, osteoporosis, colon problems, stomach problems, kidney disease, sensory disturbances, heart disease, stroke, neurological disease, eye disorders, and mental disorders. For each condition, respondents indicate whether they currently have the condition and whether the condition affects their daily activities from 1 (“not at all”) to 5 (“very much”). A comorbidity index can be calculated, which represents the degree of morbidity. The total score ranges from 0 to 90 and represents the sum of the conditions weighted by the degree of impairment assigned to each condition (Bayliss et al., 2009).
We use the Karnofsky Performance Status Scale (KPS) (Karnofsky and Burchenal, 1949) to rate the ability of a patient to perform usual activities. A person is evaluated on a score ranging from 0 to 100, where 0 is “dead” and 100 is “normal, no complaints, and no signs of disease.” The lower the Karnofsky score, the worse the survival for most severe diseases such as cancer.
The Structured Clinical Interview for DSM-5 Disorders – Clinical Version (SCID-5-CV) (First et al., 2015) is a semi-structured interview for diagnosing mental disorders according to the DSM-5. Each DSM-5 criterion is assigned corresponding interview questions to assist the interviewer in assessing the criterion. The interview covers the most common DSM-5 diagnoses encountered in the clinical setting. In this study, 7 of the 10 modules were asked: (i) mood episodes and persistent depressive disorder, (ii) differential diagnosis of mood disorders, (iii) substance use disorders, (iv) anxiety disorders, (v) obsessive-compulsive and related disorders and posttraumatic stress disorder (PTSD), (vi) screening questions for other disorders, and (vii) adjustment disorders.
We measure psychological distress by using the validated German version of the Distress Thermometer (DT) (Roth et al., 1998; Mehnert et al., 2006b). The DT is a valid, reliable, and widely used screening measure. The screening contains a single−item visual analog scale ranging from 0 (“no distress”) to 10 (“extreme distress”) to quantify the global level of distress experienced in the past week including the current day and a standardized problem checklist containing 36 potential causes of distress (yes/no questions) that are grouped into 5 categories including physical problems (21 items), practical (5), family (2), emotional problems (6), and spiritual/religious concerns (2). A score of ≥5 at the visual analog scale is recommended as a cutoff for a clinically significant level of distress (Mehnert et al., 2006b; Donovan et al., 2014).
We measure emotional responses beyond core distress during the past week, including the current day using the validated German version of the Emotion Thermometers (ET) as a multi-domain screening (Mitchell et al., 2010a,b; Hinz et al., 2019). In addition to the general distress screening, the ET consist of four visual analog scales that measure anxiety (AnxT), depression (DepT), anger (AngT), and the need for help (HelpT). Similar to the DT, all dimensions are to be rated on the visual analog scale with the anchors 0 (“none”) and 10 (“extreme”). Higher scores indicate higher emotional distress or need for help.
We additionally assess the current burden of the COVID-19 pandemic using a 5-point Likert scale ranging from 1 (“not distressed at all”) to 5 (“highly distressed”).
We use the validated German version of the Patient Health Questionnaire Depression Module (PHQ-9) (Kroenke et al., 2001; Löwe et al., 2004), the 9-item depression module from the Patient Health Questionnaire (PHQ). It was designed to score each of the DSM-IV (Bell, 1994) criteria of major depression on a 4-point Likert scale from 0 (“not at all”) to 3 (“nearly every day”) over the previous 2 weeks. The PHQ-9 is recommended by the DSM-5 working group of the American Psychiatric Association as an instrument to measure the severity of major depression according to the new DSM-5 criteria. The total score ranges from 0 to 27. The PHQ-9 has excellent reliability, as well as criterion, construct, factorial, and procedural validity (Löwe et al., 2004). A score up to 4 indicates the absence of depression, scores of 5–9 represent mild, scores of 10–14 represent moderate and scores of 15 and higher represent severe depression (Löwe et al., 2004). For the German general population, normative data for the PHQ-9 are available for both genders and different age groups (Kocalevent et al., 2013).
We use the validated German version of the Generalized Anxiety Disorder Scale (GAD-7) (Spitzer et al., 2006; Löwe et al., 2008), the 7-item generalized anxiety module from the PHQ. The GAD-7 is based on the most prominent diagnostic features of the DSM-IV diagnostic criteria for generalized anxiety disorder and has excellent reliability, as well as criterion, construct, factorial, and procedural validity. The 7 items assess frequency of core generalized anxiety disorder symptoms within the past 2 weeks. Items are scored on a 4-point Likert scale ranging from 0 (“not at all”) to 3 (“nearly every day”) with a total score ranging from 0 to 21. A score up to 4 indicates the absence of generalized anxiety disorder, scores of 5–9 represent mild, scores of 10–14 represent moderate and scores of 15 and higher represent severe anxiety symptom levels (Löwe et al., 2008). For the German general population, normative data for the GAD-7 are available for both genders and different age groups (Hinz et al., 2017).
We use the validated German short form of the Fear of Progression Questionnaire (FoP-Q-SF) (Mehnert et al., 2006a) to measure fear of cancer progression and recurrence in patients and relatives (Zimmermann et al., 2011). The 12-item measure is based on the Fear of Progression Questionnaire (FoP-Q) (Herschbach et al., 2005). The FoP-Q-SF encompasses affective reactions, partnership/family, work, loss of autonomy and coping reactions and has a high internal consistency (α = 0.87). The FoP-Q-SF items are scored on a 5-point Likert Scale ranging from 1 (“never”) to 5 (“very often”). The total FoP-Q-SF score ranges from 12 to 60 and a score of 34 and above indicates a clinical level of FoP (Herschbach et al., 2010). Higher values indicate higher levels of fear of progression.
We measure cancer related quality of life (QoL) using the validated German version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC-QLQ-C30) (Aaronson et al., 1993; Schwarz and Hinz, 2001). This instrument is widely used and has excellent reliability and validity. The EORTC-QLQ-C30 contains 30 items, 28 of which are rated on a 4-point Likert scale that ranges from 1 (“not at all”) to 4 (“very much”) and clustered to 5 functioning scales (physical, role, social, cognitive, and emotional functioning); and 3 symptom subscales (fatigue, pain, and nausea and vomiting) and 6 single symptom items (dyspnea, sleeping problems, loss of appetite, constipation, diarrhea, and financial problems). General health and global QoL are rated on 2-items with a 7-point Likert scale that ranges from 1 (“very poor”) to 7 (“excellent”). The raw values are transformed into a range of values from 0 to 100. Higher scores in the functional subscales and global QoL subscale represent better functioning, whereas higher scores in symptom subscales and items reflect a greater extent of symptom distress and worse QoL. For the German general population, normative data for the EORTC-QLQ-C30 are available for both genders and different age groups (Schwarz and Hinz, 2001).
We use the validated German version of the Short-Form Health Survey (SF-8) to measure general health-related QoL (Ware et al., 1999), a questionnaire which was originally a short-form health survey with 36 questions. The SF-8 comprises eight dimensions of QoL: general health (GH), physical functioning (PF), role physical (RP), bodily pain (BP), vitality (VT), social functioning (SF), mental health (MH), role emotional (RE), and two summary scores for physical (PCS) and mental health (MCS). Items are rated on 5-point and 6-point scales. The raw values are transformed into a range of values from 0 to 100. Higher scores indicate better health-related QoL. For the German general population, normative data for the SF-8 are available for both genders and different age groups (Ellert et al., 2005).
To measure positive support and detrimental social interaction we use the short validated German version (ISSS-8) (Ullrich and Mehnert, 2010) of the Illness-specific Social Support Scale (ISSS) originally developed by Revenson and Schiaffino (1990) and adapted to German language by Ramm and Hasenbring (2003). The validated ISSS-8 captures social interactions perceived as positive and supportive (4 items) or as distressing or harmful (4 items). Items are scored on a 5-point Likert scale ranging from 0 (“never”) to 4 (“always”). Internal consistencies are satisfying to very good (Ullrich and Mehnert, 2010). Higher sum scores in both subscales indicate higher characteristic values.
We use the validated Dyadic Coping Inventory (DCI) (Bodenmann, 2008; Ledermann et al., 2010), a 37-item self-reporting instrument designed to measure perceived communication and dyadic coping (support each other, cope together and delegate stress to each other in times of overload) that occurs in close relationships when one or both partners are stressed. All Items are rated on a 5-point Likert scale that ranges from 1 (“very rarely”) to 5 (“very often”). The total DCI score is a sum of items 1 through 35. Items 36 and 37 are evaluation items and not included in this study. A DCI total score <111 represents a dyadic coping below average; DCI between 111–145 a dyadic coping in the normal range and a DCI total score >145 a dyadic coping above average. The evaluation of the German translation of the scale provide evidence of internal consistency for the overall scale (α = 0.91) and the individual subscales (German α range 0.61–0.86) (Bodenmann, 2008; Ledermann et al., 2010).
We use the validated German version of the Quality of Marriage Index (QMI) (Norton, 1983; Zimmermann et al., 2019), a brief self-report instrument, to measure global perceptions of relationship satisfaction. The scale consists of six positively worded items. Five items are rated on a 7-point Likert scale, ranging from 1 (“strong disagreement”) to 7 (“strong agreement”). The final item, a general estimation of the relationship satisfaction, is rated on a 10-point Likert scale, ranging from 1 (“very unhappy”) to 10 (“very happy”). Total scores range from 6 to 45, with higher scores reflecting better overall marital quality. The cutoff score is 34. The German QMI demonstrates good item characteristics and excellent reliability (α = 0.94) (Zimmermann et al., 2019).
To measures perceived feelings of loneliness and social isolation, we use the validated 3-item short version of the Loneliness Scale (LS-3) (Hughes et al., 2004), developed from the revised UCLA Loneliness Scale (Russell et al., 1980). In the German adaptation used in this study, items are scored on a 5-point Likert scale from 0 (“never”) to 4 (“very often”). A higher sum score indicates higher feelings of loneliness.
We use the validated German 12 item short version of the New Sexual Satisfaction Scale (NSSS-SD) (Stulhofer et al., 2010; Hoy et al., 2019), a widely used questionnaire for assessing sexual satisfaction. The questionnaire is originally based on two subscales (ego-centered and partner- and sexual activity-centered sexual satisfaction). For the NSSS-SD a one-dimensional factor structure was confirmed with excellent reliability (α = 0.96) (Hoy et al., 2019). This NSSS-SD measures satisfaction with various aspects of one’s own sexual life. The items are scored on a 5-point Likert scale from 1 (“not at all satisfied”) to 5 (“very satisfied”). The scores of all items are summed up. Higher scores indicate higher sexual satisfaction.
We use the Sexual Quality of Life (SQoL) questionnaire to measure quality of sexual life. The 18-item questionnaire captures sexual self-esteem, emotional wellbeing and relationship issues in women (SQoL-F) (Symonds et al., 2005) and men (SQoL-M) (Abraham et al., 2008). In the present study, the 18 items are used in a binary (male/female) form. Each item is rated on a 6-point Likert scale (“completely agree” to “completely disagree”) either in descending order 6 to 1 (items 1, 5, 9, 13, and 18) or ascending order 1 to 6 (remaining items). The values of the items are added to a sum score, which is then transferred to a standardized scale from 0 to 100. A higher score indicates higher SQoL (Symonds et al., 2005).
We use an adapted form of the German version of the Short-form Supportive Care Needs Survey (SCNS-SF34-G) (Sanson-Fisher et al., 2000; Lehmann et al., 2012). The single items cover the five dimensions of the original SCNS-SF34 (psychological support needs, support needs regarding physical problems and coping with daily living, support needs with regard to the health system and information, support needs with regard to patient care and support, and sexuality needs). Items are scored on a 4-point scale from 1 (“no need”) to 4 (“high need”). Higher scores indicate higher supportive care needs.
To assess patients’ perceived supportive care needs, we use single items that had proven suitable in earlier studies (Mehnert and Koch, 2008; Faller et al., 2016). To determine the need for psychosocial support, we ask participants, “Do you have a need for psychosocial support?” Response options were “yes” or “no.” We further ask participants “Would you accept an offer of psychosocial support?” with a yes/no response format to determine the acceptance of psychosocial support offers. In addition, we ask participants to rate the strength of their wish for talking (a) with clinical psychologist and (b) with a closely person: “Do you currently have the wish to talk about the psychological distress because of your cancer?” with the response options 1 (“not at all”), 2 (“somewhat”), 3 (“quite a bit”), 4 (“strongly”), and 5 (“very strongly”).
We ask the participants to rate the possibility of talking (a) with a psycho-oncologist and (b) with a close person: “Do you currently have the possibility to talk about the psychological distress because of your cancer?” with the response options 1 (“not at all”), 2 (“somewhat”), 3 (“quite”), 4 (“strongly”), and 5 (“very strongly”).
Using a 5-point response format ranging from 1 (“not at all”) to 5 (“very well”), we ask participants to evaluate their opportunities of talking about their distress to different persons, including family, friends, physicians, nurses, and psycho-oncologist. We ask patients “How well would you be able to talk to the below-mentioned persons about the psychological distress because of your cancer and cancer treatment?” with response options 1 (“not at all”), 2 (“somewhat”), 3 (“partly”), 4 (“well”), and 5 (“very well”), to be rated for each of the individual persons as indicated above.
To assess patients’ utilization of psychosocial support services, we ask participants “Have you previously utilized psychosocial support offers because of your cancer?” Six items further specified support: “psychological counseling/psychotherapy,” “social legal counseling,” “pastoral care,” “self-help groups,” “web based-support offers,” and “other offers.” Response options were “yes” or “no.” We further ask participants to rate how helpful they perceived the services to be when they had used them with the response options 1 (“not at all”), 2 (“rarely”), 3 (“somewhat”), 4 (“quite”), and 5 (“strongly”). We further asked utilization of cancer rehabilitation offers. Response options were “yes” or “no.”
We further ask participants if they had been advised by their partner or a close person to seek professional psychosocial support. Response options were “yes” or “no.” We further ask participants if they had received a recommendation from their doctor to seek professional psychosocial support. Response options were “yes” or “no.” We ask participants to specify which professional group was recommended to them (clinical psychology, social worker, pastor, and other). We also ask participants to indicate where they had sought professional psychosocial support (hospital, rehabilitation clinic, outpatient psychotherapy, outpatient cancer counseling center, and other). If participants had not sought professional psychosocial support, they were asked to indicate the reasons why they had not done so.
We ask participants to rate their attitude toward professional psychosocial support offers due to cancer on a numerical rating scale ranging from 0 (“negative”) to 10 (“positive”).
We use an adapted version of the validated German Satisfaction with Comprehensive Cancer Care (SCCC) Questionnaire (Esser et al., 2021) to measure satisfaction with medical and psychosocial cancer care. In detail, 32 items address human quality of physicians (interest of physicians toward patient and in his/her psychosocial condition), information (psychosocial support services/alternative possibilities of treatment and their consequences) and accessibility to psychosocial services (psychosocial counseling on supportive care services/psycho-oncological support/legal and financial advice/pastoral support/support in searching for a psychotherapist/support in acquiring coping strategies/support to join self-help or therapeutic groups). Response categories differ between item categories including 1 (“very dissatisfied”) to 5 (“very satisfied”); 1 (“very bad”) to 5 (“excellent”); and 1 (“do not agree at all”) to 5 (“completely agree”). Some items contain the additional response option 0 (“not applicable”). Higher values indicate higher satisfaction.
We measure health literacy using the validated German version of the European Health Literacy Survey Questionnaire (HLS-EU-Q16) (Röthlin et al., 2013), the 16-item short version of the 47-item European Health Literacy Survey Questionnaire (HLS-EU Consortium, 2012). The validated questionnaire has a high internal consistency (Cronbach’s alpha = 0.90). All items are rated on a 4-point Likert scale 1 (“very simple” to 4 (“very difficult”). The answer categories of all items are dichotomized. Answers 1 (“very simple”) and 2 (“fairly simple”) are scored with 0. Answers 3 (“quite difficult”) and 4 (“very difficult”) are scored with 1. The scores are summed up. A sum score ≤8 indicates “insufficient,” 9–12 “problematic,” and ≥13 “sufficient” health literacy.
We use the validated German version of the Adherence Assessment Questionnaire (AAQ) (Mueller et al., 2018), a self-reporting instrument to assess the extent of non-adherence in chronic indications. The 11-item AAQ has excellent reliability (α = 0.84 to α = 0.97) as well as a good validity. Eight items are formulated as statements that are rated on a 4-point Likert-scale from 1 (“strongly agree”) to 4 (“strongly disagree”). One additional item is stated as a visual analog scale to show the percentage of adherent days in the last 2 weeks. Moreover, two items measuring a patient’s tendency to answer in a socially desirable way were added to the AAQ. The scores of all items are summed up. Higher scores indicate higher inflexibility and less adherence.
Patients are asked about their drinking and smoking habits, physical exercise, relaxation techniques, regular intake of medication as well as weight and height for calculating the body mass index (BMI). The questions are adapted from the validated German Questionnaire for the Assessment of Health Behavior (FEG) (Dlugosch and Krieger, 1995) and the report of the Federal Health Monitoring in Germany (Schulze and Lampert, 2006). Items are rated on a 4-point Likert scales from 1 (“never”) to 4 (“daily”) or with the response options “yes” or “no.”
We use the validated German version of the Stigma Impact Scale (SIS) (Fife and Wright, 2000; Eichhorn et al., 2015) to measure perceived experiences of stigmatization. The 24-items measure the effect on patients and their families of negative social attitudes toward the patients’ health or mental health condition. The SIS consists of four subscales: social rejection (9 items), financial insecurity (3 items), internalized shame (5 items), and social isolation (7 items). All items are rated on a 4-point Likert scale that ranges from 0 (“do not agree at all”) to 3 (“fully agree”). Scale means and a total mean score can be calculated. The SIS has a high internal consistency (α = 0.81 to α = 0.89).
We use the validated German language Schedule for Meaning in Life Evaluation (SMiLE) questionnaire to measure meaning in life (Fegg et al., 2008). The SMiLE uses an idiographic approach and allows individuals to choose the life areas that they consider to be important for their own meaning in life. Respondents are first asked to indicate from 3 to 7 areas that actually provide meaning to their lives. In a second step (level of importance), the importance of each area is rated on a 5-point scale, ranging from 1 (“somewhat important”) to 5 (“extremely important”). In a third step (level of satisfaction), the respondents rate their current level of satisfaction with each area on a 7-point Likert scale, ranging from −3 (“very unsatisfied”) to +3 (“very satisfied”). Different indices can be formed, which indicate both the mean weighting of the meaning in life areas and the average satisfaction or dissatisfaction with the individual meaning in life areas.
We use the validated German version of the Life Attitude Profile-Revised (LAP-R) (Reker, 1992; Mehnert et al., 2007), a questionnaire assessing meaning and purpose in life and motivation to find meaning and purpose in life. Here, we use 20 items of the original 48-item questionnaire covering 6 dimensions: purpose (PU), coherence dimension (CO), choice/responsibleness (CR), existential vacuum (EV), and goal seeking (GS). The dimensions of the German validation have satisfactory to high internal consistencies (Cronbach’s alpha between 0.78 and 0.85). All items are rated on a 7-point Likert scale from 1 (“strongly disagree”) to 7 (“strongly agree”). Higher sum scores indicate higher characteristic values in each subscale.
All study interviewers are certified psychologists or physicians familiar with the DSM-5 classification and diagnostic criteria. They complete a mandatory standardized SCID-5 training before the beginning of the study interviews. After the SCID-5-CV training, each study interviewer conducts several test interviews with voluntary subjects, one of which was videotaped and evaluated by a certified psychotherapist responsible for quality assurance at the Leipzig university study center. Evaluation criteria included correct implementation of the SCID-5-CV interview questions, comprehension and interactional factors. Each interviewer received detailed feedback about his/her SCID-5-CV training interviews. Interviewers were not allowed to conduct study interviews until they had ensured that they could conduct the SCID-5-CV correctly.
The university study center Leipzig is responsible for coordinating data collection and ensuring the accuracy of the assessment, data collection, and data input. The study center Leipzig also plays a key role of facilitating communication between collaborating study centers using routine monitoring, meetings, and feedback to ensure that tasks are accomplished and problems are addressed.
Each collaborating center receives regular reports showing how well the site is meeting recruitment goals, in terms of total number of participants recruited and study targets set. All incoming data is entered at the study center Leipzig into the study database (SPSS Vs. 27) in a timely manner. It is verified that the recruited participants meet all eligibility criteria. With regard to missing data, data editing, and entry procedures, we generate routine data quality reports to assess missing data and inconsistencies. A study research assistant follows up with patients and relatives who have missing data at baseline or follow-up. Adverse events such as death of a patient are documented.
We aim to estimate possible biases in our sample. Patients who meet the inclusion criteria but decline study participation will be asked to provide information about their sociodemographic and medical characteristics, as well as the reason for declining the study on a voluntary basis. Due to data protection regulations and limited access to patients, data for non-participants are only available for the characteristics sex, date of birth, cancer diagnosis, and reason for non-participation. Other characteristics such as SES, stage of disease or Karnofsky index could not be completely collected. Study participants and eligible non-participants will be analyzed in terms of sociodemographic information including sex, age, and medical characteristics including type of diagnosis and cancer stage. Baseline characteristics and follow-up data between those with and those without missing data will also be compared to estimate bias.
The sample size was calculated based on previous data of 4-week prevalence rates of mental disorders in different strata of patients with cancer, assuming an overall prevalence in this population of 30% (Mehnert et al., 2014). In the study application, our original case number planning was to recruit a total of 2,000 cancer patients and 1,600 relatives. Due to the COVID-19 pandemic, which almost coincided with the start of study recruitment, oncology care, and access in the collaborating cancer centers was significantly restricted over a long period of time, so that recruitment opportunities for the study were also severely limited. Therefore, we had to adjust the sample size to approximately 1,000 patients and 600 relatives. With reference to the relevant literature by Newcombe (1998) and Fleiss et al. (2003), a minimum sample size of N = 300 is required, given the expected prevalence of mental disorders in cancer patients of approximately 30% (Mehnert et al., 2014).
In order to obtain a representative sample, the SES of the patients was screened on the basis of educational level, occupational status, and income. Following the distribution in the German general population, we aimed to stratify the sample in a ratio of 20% (high SES), 60% (medium SES), and 20% (low SES) (Lampert et al., 2013). Stratification also had to be adapted to the limited patient access and recruitment during the COVID-19 pandemic.
Due to the longitudinal design of the study, a failure rate over the measurement time points must also be considered. In a methodologically similar study with cancer patients, a failure rate of 9% was reported (Voigt et al., 2017). However, higher failure rates can be assumed for patients with lower SES (Baekeland and Lundwall, 1975), which is why we conservatively expect a higher failure rate of 25% here.
Prevalence estimates for mental comorbidity (number of patients, %, and SE) are calculated. We present frequencies including their 95% confidence intervals for the main outcome variables. Multiple logistic regression models will be used to calculate and test adjusted differences in age, sex, study center, or tumor entity. In all of the analyses, the quota distribution by SES is taken into account in the form of appropriate weighting factors.
We analyze associations between categorical variables using the Chi-squared test, and between continuous variables using the Pearson correlation coefficient, respectively. Between-group differences are examined using the independent t-test for continuous dependent variables. To identify independent predictors, logistic regression analyses will be performed.
For identifying the function of relatives and mutual dependencies between partner and patient (dyadic coping) actor-partner interdependence models (APIM) are calculated. The APIM takes into account the interdependence between the persons within a dyad with regard to the outcome variables under investigation.
The possible influence of dropouts on the representativeness of the results at later measurement times is investigated through pattern mixture modeling (Little, 1995; Hedeker and Gibbons, 1997).
In view of the demographic change, the increasing cancer prevalence and advances in biomedicine, concepts for the development of high-quality care for cancer patients in all survivorship phases that go beyond the existing aftercare are urgently needed with the aim of improving survival and the management of the physical and psychological long-term and late effects as well as alleviating the occupational and social consequences.
Issues of cancer survivorship and quality of life have been put on the agenda both internationally and nationally by various professional societies and national committees (Nekhlyudov et al., 2019). The American Society of Clinical Oncology (ASCO) published criteria for high-quality cancer survivorship care as early as 2013 (McCabe et al., 2013). In Germany, both the National Decade Against Cancer (NDK), which was proclaimed in 2019 by the Federal Ministry of Education and Research (BMBF) together with the Federal Ministry of Health (BMG) (Bundesministerium für Bildung und Forschung, 2022), and the European Cancer Plan (European Commission, 2021) pursue clear objectives with regard to improving the quality of cancer care and the quality of life of those affected in all survivorship phases.
Psychosocial aspects play an important role in initiatives to improve cancer care; not only from the perspective of patients and those affected, but also from the perspective of health care professionals. Although psycho-oncological interventions significantly reduce psychosocial distress such as anxiety and depression and improve quality of life (Faller et al., 2013; Mulick et al., 2018), many patients face barriers to accessing psychosocial support offers (Faller et al., 2016; Weis et al., 2018). A major barrier to low-threshold access to psycho-oncological support offers are socioeconomic inequalities, but these are not well researched in the cancer population. At the same time, the development and implementation of target group-specific psychosocial support services without rigorous longitudinal empirical data will be a challenge in practice.
The data from our study will provide an opportunity to identify at-risk groups for specific psychosocial needs. While it is likely that the majority of survivors do not need or want intensive psychosocial care, those who are at high risk for psychosocial impairment will require more timely and more intensified care. Data that provide the basis for such a risk-based approach, including the development and implementation of survivorship screening, should help to ensure that survivorship care plans can be tailored to the specific needs of each cancer survivor.
This prospective multi-center observational cohort study has a major focus on increasing quality of care and quality of life in cancer survivors through estimating the prevalence of mental disorders, the frequency and extent of psychosocial distress, perceived needs for psychosocial support and utilization of psychosocial support offers in newly diagnosed cancer patients and their relatives a few weeks after cancer diagnosis and over a follow-up period of 18 months. A strength of the study is the inclusion of relatives, who often face a variety of psychosocial challenges during the cancer diagnosis and survival period (Ernst et al., 2017). They often experience a similar psychosocial burden as the patients (Fujinami et al., 2015). Yet, family members usually receive limited support (Rosenberger et al., 2012). While there are support services for relatives in psycho-oncological care (Kuhnt et al., 2018), these are often limited in time or insufficiently tailored to their needs (Lambert et al., 2012; Sklenarova et al., 2015). In the worst case, this can lead to prolonged stress and maladaptive adjustment within the family system.
Findings on the course of psychological distress and perceived supportive care needs in patients and their relatives in the early survivorship phase, taking into account associated biopsychosocial factors, will promote the target-group-specific development of support offers and cancer survivorship care plans particularly for vulnerable groups.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The local ethics committee of all study centers approved the study protocol (AZ: 207/18-ek, SR-EK-536112020, 8533_BO_K_2019, 14/4/21Ü). All patients willing to participate provide written informed consent.
AM-T, JE, PE, UG, and TZ contributed to the conception and design. All authors contributed to the manuscript writing and approved the submitted version.
This study was funded by grants from the German Cancer Aid Foundation (Stiftung Deutsche Krebshilfe) and financially supported by the Department of Medical Psychology and Medical Sociology at the University Medical Center of Leipzig, by the Charité Comprehensive Cancer Center, Berlin, and the Department of Psychosomatic Medicine and Psychotherapy, Hannover Medical School, Hannover. The funding and sponsoring sources are not involved in any stage of the research process.
The authors would like to acknowledge the cancer patients, their partners and relatives, and study stakeholders, who have contributed significantly to the study design und choice of outcome variables.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aaronson, N. K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull, A., Duez, N. J., et al. (1993). The European organization for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 85, 365–376. doi: 10.1093/jnci/85.5.365
Abraham, L., Symonds, T., and Morris, M. F. (2008). Psychometric validation of a sexual quality of life questionnaire for use in men with premature ejaculation or erectile dysfunction. J. Sex. Med. 5, 595–601. doi: 10.1111/j.1743-6109.2007.00749.x
American Psychiatric Association [APA] (2013). Diagnostic and statistical manual of mental disorders: DSM-5™. Arlington, VA: American Psychiatric Publishing, Inc. doi: 10.1176/appi.books.9780890425596
Bach, A., Knauer, K., Graf, J., Schäffeler, N., and Stengel, A. (2022). Psychiatric comorbidities in cancer survivors across tumor subtypes: A systematic review. World J. Psychiatry 12, 623–635. doi: 10.5498/wjp.v12.i4.623
Baekeland, F., and Lundwall, L. (1975). Dropping out of treatment: A critical review. Psychol. Bull. 85, 738–783. doi: 10.1037/h0077132
Barbek, R. M. E., Makowski, A. C., and von dem Knesebeck, O. (2022). Social inequalities in health anxiety: A systematic review and meta-analysis. J. Psychosom. Res. 153:110706. doi: 10.1016/j.jpsychores.2021.110706
Bayliss, E. A., Ellis, J. L., and Steiner, J. F. (2005). Subjective assessments of comorbidity correlate with quality of life health outcomes: Initial validation of a comorbidity assessment instrument. Health Qual. Life Outcomes 3:51. doi: 10.1186/1477-7525-3-51
Bayliss, E. A., Ellis, J. L., and Steiner, J. F. (2009). Seniors’ self-reported multimorbidity captured biopsychosocial factors not incorporated into two other data-based morbidity measures. J. Clin. Epidemiol. 62, 550–557.e1. doi: 10.1016/j.jclinepi.2008.05.002
Beesdo-Baum, K., Zaudig, M., and Wittchen, H.-U. (2019). “SCID-5-PD: Strukturiertes klinisches interview für DSM-5 - persönlichkeitsstörungen: Deutsche bearbeitung des,” in Structured clinical interview for DSM-5 - personality disorders, eds M. B. First, J. B. W. Williams, L. S. Benjamin, and R. L. Spitzer (Göttingen: Hogrefe Verlag).
Bell, C. C. (1994). DSM-IV: Diagnostic and statistical manual of mental disorders. JAMA 10, 828–829. doi: 10.1001/jama.1994.03520100096046
Bundesministerium für Bildung und Forschung (2022). Projektgruppe nationale dekade gegen Krebs dekade gegen Krebs. Available online at: www.dekade-gegen-krebs.de/ (accessed December 10, 2022).
Chao, C., Bhatia, S., Xu, L., Cannavale, K. L., Wong, F. L., Huang, P. S., et al. (2020). Chronic comorbidities among survivors of adolescent and young adult cancer. J. Clin. Oncol. 38, 3161–3174. doi: 10.1200/JCO.20.00722
Chiu, M., Lebenbaum, M., Cheng, J., de Oliveira, C., and Kurdyak, P. (2017). The direct healthcare costs associated with psychological distress and major depression: A population-based cohort study in Ontario, Canada. PLoS One 12:e0184268. doi: 10.1371/journal.pone.0184268
Cincidda, C., Oliveri, S., Sanchini, V., and Pravettoni, G. (2022). The role of caregivers in the clinical pathway of patients newly diagnosed with breast and prostate cancer: A study protocol. Front. Psychol. 13:962634. doi: 10.3389/fpsyg.2022.962634
Dionisi-Vici, M., Fantoni, M., Botto, R., Nervo, A., Felicetti, F., Rossetto, R., et al. (2021). Distress, anxiety, depression and unmet needs in thyroid cancer survivors: A longitudinal study. Endocrine 74, 603–610. doi: 10.1007/s12020-021-02786-y
Dlugosch, G. E., and Krieger, W. (1995). [Health behavior questionnaire (FEG)]. Frankfurt: Swetz and Zeitlinger.
Donovan, K. A., Grassi, L., McGinty, H. L., and Jacobsen, P. B. (2014). Validation of the distress thermometer worldwide: State of the science. Psychooncology 23, 241–250. doi: 10.1002/pon.3430
Eichhorn, S., Mehnert, A., and Stephan, M. (2015). [German version of the social impact scale (SIS-D)–Pilot testing of an instrument for measuring experienced stigmatization in a sample of cancer patients]. Psychother. Psychosom. Med. Psychol. 65, 183–190. doi: 10.1055/s-0034-1398523
Ellert, U., Lampert, T., and Ravens-Sieberer, U. (2005). [Measuring health-related quality of life with the SF-8. Normal sample of the German population]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 48, 1330–1337. doi: 10.1007/s00103-005-1168-5
Ernst, J., Hinz, A., Niederwieser, D., Döhner, H., Hönig, K., Vogelhuber, M., et al. (2017). Dyadic coping of patients with hematologic malignancies and their partners and its relation to quality of life - a longitudinal study. Leuk. Lymphoma 58, 655–665. doi: 10.1080/10428194.2016.1194983
Esser, P., Sautier, L., Sarkar, S., Schilling, G., Bokemeyer, C., Koch, U., et al. (2021). Development and preliminary psychometric investigation of the German satisfaction with comprehensive cancer care (SCCC) questionnaire. Health Qual. Life Outcomes 19:147. doi: 10.1186/s12955-021-01784-y
European Commission (2021). Europe’s beating cancer plan. Available online at: https://ec.europa.eu/health/sites/default/files/non_communicable_diseases/docs/eu_cancer-plan_en.pdf (accessed December 6, 2022).
Faller, H., Schuler, M., Richard, M., Heckl, U., Weis, J., and Küffner, R. (2013). Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: Systematic review and meta-analysis. J. Clin. Oncol. 31, 782–793. doi: 10.1200/JCO.2011.40.8922
Faller, H., Weis, J., Koch, U., Brähler, E., Härter, M., Keller, M., et al. (2016). Perceived need for psychosocial support depending on emotional distress and mental comorbidity in men and women with cancer. J. Psychosom. Res. 81, 24–30. doi: 10.1016/j.jpsychores.2015.12.004
Fegg, M., Kramer, M., L’Hoste, S., and Borasio, G. (2008). The schedule for meaning in life evaluation (SMiLE): Validation of a new instrument for meaning-in-life research. J. Pain Symptom Manage. 35, 356–364. doi: 10.1016/j.jpainsymman.2007.05.007
Fife, B. L., and Wright, E. R. (2000). The dimensionality of stigma: A comparison of its impact on the self of persons with HIV/AIDS and cancer. J. Health Soc. Behav. 41, 50–67. doi: 10.2307/2676360
First, M. B., Williams, J. B., Karg, R. S., and Spitzer, R. L. (2015). Structured clinical interview for DSM-5-research version (SCID-5 for DSM-5, research version; SCID-5-RV). Arlington, VA: American Psychiatric Association, Inc.
Fleiss, J., Levin, B., and Paik, M. (2003). Statistical methods for rates and proportions. Hoboken, NJ: John Wiley & Sons, Inc. doi: 10.1002/0471445428
Fryers, T., Melzer, D., and Jenkins, R. (2003). Social inequalities and the common mental disorders: A systematic review of the evidence. Soc. Psychiatry Psychiatr. Epidemiol. 38, 229–237. doi: 10.1007/s00127-003-0627-2
Fujinami, R., Sun, V., Zachariah, F., Uman, G., Grant, M., and Ferrell, B. (2015). Family caregivers’ distress levels related to quality of life, burden, and preparedness. Psychooncology 24, 54–62. doi: 10.1002/pon.3562
Goodwin, B. C., Crawford-Williams, F., Ireland, M., March, S., Chambers, S. K., Aitken, J. F., et al. (2022). The quality of life of regional and remote cancer caregivers in Australia. Eur. J. Cancer Care 31:e13587. doi: 10.1111/ecc.13587
Götze, H., Köhler, N., Taubenheim, S., Lordick, F., and Mehnert, A. (2019). Polypharmacy, limited activity, fatigue and insomnia are the most frequent symptoms and impairments in older hematological cancer survivors (70+): Findings from a register-based study on physical and mental health. J. Geriatr. Oncol. 10, 55–59. doi: 10.1016/j.jgo.2018.05.011
Götze, H., Taubenheim, S., Dietz, A., Lordick, F., and Mehnert, A. (2018). Comorbid conditions and health-related quality of life in long-term cancer survivors-associations with demographic and medical characteristics. J. Cancer Surviv. 12, 712–720. doi: 10.1007/s11764-018-0708-6
Hagedoorn, M., Sanderman, R., Bolks, H. N., Tuinstra, J., and Coyne, J. C. (2008). Distress in couples coping with cancer: A meta-analysis and critical review of role and gender effects. Psychol. Bull. 134, 1–30. doi: 10.1037/0033-2909.134.1.1
Hanel, G., Henningsen, P., Herzog, W., Sauer, N., Schaefert, R., Szecsenyi, J., et al. (2009). Depression, anxiety, and somatoform disorders: Vague or distinct categories in primary care? Results from a large cross-sectional study. J. Psychosom. Res. 67, 189–197. doi: 10.1016/j.jpsychores.2009.04.013
Hartung, T. J., Brähler, E., Faller, H., Härter, M., Hinz, A., Johansen, C., et al. (2017). The risk of being depressed is significantly higher in cancer patients than in the general population: Prevalence and severity of depressive symptoms across major cancer types. Eur. J. Cancer 72, 46–53. doi: 10.1016/j.ejca.2016.11.017
Hedeker, D., and Gibbons, R. D. (1997). Application of random-effects pattern-mixture models for missing data in longitudinal studies. Psychol. Methods 1, 64–78. doi: 10.1037/1082-989X.2.1.64
Hellstadius, Y., Lagergren, J., Zylstra, J., Gossage, J., Davies, A., Hultman, C. M., et al. (2017). A longitudinal assessment of psychological distress after oesophageal cancer surgery. Acta Oncol. 56, 746–752. doi: 10.1080/0284186X.2017.1287945
Herschbach, P., Berg, P., Dankert, A., Duran, G., Engst-Hastreiter, U., Waadt, S., et al. (2005). Fear of progression in chronic diseases: Psychometric properties of the fear of progression questionnaire. J. Psychosom. Res. 58, 505–511. doi: 10.1016/j.jpsychores.2005.02.007
Herschbach, P., Berg, P., Waadt, S., Duran, G., Engst-Hastreiter, U., Henrich, G., et al. (2010). Group psychotherapy of dysfunctional fear of progression in patients with chronic arthritis or cancer. Psychother. Psychosom. 79, 31–38. doi: 10.1159/000254903
Herschbach, P., Britzelmeir, I., Dinkel, A., Giesler, J. M., Herkommer, K., Nest, A., et al. (2020). Distress in cancer patients: Who are the main groups at risk? Psychooncology 29, 703–710. doi: 10.1002/pon.5321
Hinz, A., Klein, A. M., Brähler, E., Glaesmer, H., Luck, T., Riedel-Heller, S. G., et al. (2017). Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. J. Affect. Disord. 210, 338–344. doi: 10.1016/j.jad.2016.12.012
Hinz, A., Mitchell, A. J., Degi, C. L., and Mehnert-Theuerkauf, A. (2019). Normative values for the distress thermometer (DT) and the emotion thermometers (ET), derived from a German general population sample. Qual. Life Res. 28, 277–282. doi: 10.1007/s11136-018-2014-1
HLS-EU Consortium (2012). Comparative report on health literacy in eight EU-member states. The European health literacy survey. Available online at: http://cpme.dyndns.org:591/adopted/2015/Comparative_report_on_health_literacy_in_eight_EU_member_states.pdf (accessed December 14, 2022).
Hoy, M., Strauss, B., Kröger, C., and Brenk-Franz, K. (2019). [Evaluation of the German short version of the “new sexual satisfaction scale” (NSSS-SD) in a representative sample]. Psychother. Psychosom. Med. Psychol. 69, 129–135. doi: 10.1055/a-0620-0002
Hu, K., Liu, Q., Laszlo, K. D., Wei, D., Yang, F., Fall, K., et al. (2023). Risk of psychiatric disorders among spouses of patients with cancer in Denmark and Sweden. JAMA Netw. Open 6:e2249560. doi: 10.1001/jamanetworkopen.2022.49560
Hughes, M. E., Waite, L. J., Hawkley, L. C., and Cacioppo, J. T. (2004). A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 26, 655–672. doi: 10.1177/0164027504268574
Karnofsky, D. A., and Burchenal, J. H. (1949). “The clinical evaluation of chemotherapeutic agents in cancer,” in Evaluation of chemotherapeutic agents, ed. C. M. MacLeod (New York, NY: Columbia University Press).
Kocalevent, R. D., Hinz, A., and Brähler, E. (2013). Standardization of the depression screener patient health questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 35, 551–555. doi: 10.1016/j.genhosppsych.2013.04.006
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Kuhnt, S., Brähler, E., Faller, H., Härter, M., Keller, M., Schulz, H., et al. (2016). Twelve-month and lifetime prevalence of mental disorders in cancer patients. Psychother. Psychosom. 85, 289–296. doi: 10.1159/000446991
Kuhnt, S., Mehnert, A., Giesler, J. M., Faust, T., Weis, J., and Ernst, J. (2018). [The development of quality standards for the psychosocial outpatient care of cancer patients - results of a Delphi survey]. Gesundheitswesen 80, 113–121. doi: 10.1055/s-0042-100732
Laidsaar-Powell, R., Butow, P., Charles, C., Gafni, A., Entwistle, V., Epstein, R., et al. (2017). The TRIO framework: Conceptual insights into family caregiver involvement and influence throughout cancer treatment decision-making. Patient Educ. Couns. 100, 2035–2046. doi: 10.1016/j.pec.2017.05.014
Lam, W. W., Soong, I., Yau, T. K., Wong, K. Y., Tsang, J., Yeo, W., et al. (2013). The evolution of psychological distress trajectories in women diagnosed with advanced breast cancer: A longitudinal study. Psychooncology 22, 2831–2839. doi: 10.1002/pon.3361
Lambert, S. D., Harrison, J. D., Smith, E., Bonevski, B., Carey, M., Lawsin, C., et al. (2012). The unmet needs of partners and caregivers of adults diagnosed with cancer: A systematic review. BMJ Support. Palliat. Care 2, 224–230. doi: 10.1136/bmjspcare-2012-000226
Lampert, T., Kroll, L. E., Müters, S., and Stolzenberg, H. (2013). Messung des sozioökonomischen status in der studie zur gesundheit erwachsener in deutschland (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56, 631–636. doi: 10.1007/s00103-012-1663-4
Ledermann, T., Bodenmann, G., Gagliardi, S., Charvoz, L., Verardi, S., Rossier, J., et al. (2010). Psychometrics of the dyadic coping inventory in three language groups. Swiss J. Psychol. 69, 201–212. doi: 10.1024/1421-0185/a000024
Lehmann, C., Koch, U., and Mehnert, A. (2012). Psychometric properties of the German version of the short-form supportive care needs survey questionnaire (SCNS-SF34-G). Support. Care Cancer 20, 2415–2424. doi: 10.1007/s00520-011-1351-1
LimeSurvey GmbH (2015). LimeSurvey. Available online at: www.limesurvey.org/de/ (accessed December 14, 2022).
Linden, W., Vodermaier, A., Mackenzie, R., and Greig, D. (2012). Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 141, 343–351. doi: 10.1016/j.jad.2012.03.025
Little, R. J. A. (1995). Modeling the drop-out mechanism in repeated-measures studies. J. Am. Stat. Assoc. 90, 1112–1121. doi: 10.1080/01621459.1995.10476615
Lopes, C., Severo, M., Fontes, F., Lopes-Conceicao, L., Ferreira, A., Pereira, S., et al., (2022). Trajectories of anxiety and depression symptoms over five years since breast cancer diagnosis: Results of the NEON-BC prospective study. Healthcare (Basel) 10:661. doi: 10.3390/healthcare10040661
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., et al. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med. Care 46, 266–274. doi: 10.1097/MLR.0b013e318160d093
Löwe, B., Grafe, K., Zipfel, S., Witte, S., Loerch, B., and Herzog, W. (2004). Diagnosing ICD-10 depressive episodes: Superior criterion validity of the patient health questionnaire. Psychother. Psychosom. 73, 386–390. doi: 10.1159/000080393
Mackenbach, J. P. (2019). Health inequalities: Persistence and change in modern welfare states. New York, NY: Oxford University Press. doi: 10.1093/oso/9780198831419.001.0001
Mackenbach, J. P., Stirbu, I., Roskam, A. J., Schaap, M. M., Menvielle, G., Leinsalu, M., et al. (2008). Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 358, 2468–2481. doi: 10.1056/NEJMsa0707519
McCabe, M., Bhatia, S., Oeffinger, K., Reaman, G., Tyne, C., Wollins, D., et al. (2013). American society of clinical oncology statement: Achieving high-quality cancer survivorship care. J. Clin. Oncol. 31, 631–640. doi: 10.1200/JCO.2012.46.6854
Mehnert, A., Brähler, E., Faller, H., Härter, M., Keller, M., Schulz, H., et al. (2014). Four-week prevalence of mental disorders in patients with cancer across major tumor entities. J. Clin. Oncol. 32, 3540–3546. doi: 10.1200/JCO.2014.56.0086
Mehnert, A., Hartung, T. J., Friedrich, M., Vehling, S., Brähler, E., Härter, M., et al. (2018). One in two cancer patients is significantly distressed: Prevalence and indicators of distress. Psychooncology 27, 75–82. doi: 10.1002/pon.4464
Mehnert, A., Herschbach, P., Berg, P., Henrich, G., and Koch, U. (2006a). [Fear of progression in breast cancer patients–validation of the short form of the fear of progression questionnaire (FoP-Q-SF)]. Z. Psychosom. Med. Psychother. 52, 274–288. doi: 10.13109/zptm.2006.52.3.274
Mehnert, A., Müller, D., Lehmann, C., and Koch, U. (2006b). Die deutsche version des NCCN distress-thermometers. Z. Psychiatr. Psychol. Psychother. 54, 213–223. doi: 10.1024/1661-4747.54.3.213
Mehnert, A., and Koch, U. (2008). Psychological comorbidity and health-related quality of life and its association with awareness, utilization, and need for psychosocial support in a cancer register-based sample of long-term breast cancer survivors. J. Psychosom. Res. 64, 383–391. doi: 10.1016/j.jpsychores.2007.12.005
Mehnert, A., Müller, D., and Koch, U. (2007). [Measuring meaning-based coping and life attitudes. Psychometric evaluation of the German version of the life attitude profile-revised (LAP-R) in a representative sample of breast cancer patient]. Z. Klin. Psychol. Psychother. 36, 176–188. doi: 10.1026/1616-3443.36.3.176
Mirza, I., and Jenkins, R. (2004). Risk factors, prevalence, and treatment of anxiety and depressive disorders in Pakistan: Systematic review. BMJ 328:794. doi: 10.1136/bmj.328.7443.794
Mitchell, A. J., Baker-Glenn, E. A., Granger, L., and Symonds, P. (2010a). Can the distress thermometer be improved by additional mood domains? Part I. Initial validation of the emotion thermometers tool. Psychooncology 19, 125–133. doi: 10.1002/pon.1523
Mitchell, A. J., Baker-Glenn, E. A., Park, B., Granger, L., and Symonds, P. (2010b). Can the distress thermometer be improved by additional mood domains? Part II. What is the optimal combination of emotion thermometers? Psychooncology 19, 134–140. doi: 10.1002/pon.1557
Mitchell, A. J., Chan, M., Bhatti, H., Halton, M., Grassi, L., Johansen, C., et al. (2011). Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 12, 160–174. doi: 10.1016/S1470-2045(11)70002-X
Moreno-Peral, P., Conejo-Ceron, S., Motrico, E., Rodriguez-Morejon, A., Fernandez, A., Garcia-Campayo, J., et al. (2014). Risk factors for the onset of panic and generalised anxiety disorders in the general adult population: A systematic review of cohort studies. J. Affect. Disord. 168, 337–348. doi: 10.1016/j.jad.2014.06.021
Mueller, S., Gorasso, V., Black, K. M., Murnane, K., and Wilke, T. (2018). PRM208 - Validation of the English version of the adherence assessment questionnaire (AAQ). Value Health 21:S392. doi: 10.1016/j.jval.2018.09.2326
Mulick, A., Walker, J., Puntis, S., Burke, K., Symeonides, S., Gourley, C., et al. (2018). Does depression treatment improve the survival of depressed patients with cancer? A long-term follow-up of participants in the SMaRT oncology-2 and 3 trials. Lancet Psychiatry 5, 321–326. doi: 10.1016/S2215-0366(18)30061-0
Nekhlyudov, L., Mollica, M., Jacobsen, P., Mayer, D., Shulman, L., and Geiger, A. (2019). Developing a quality of cancer survivorship care framework: Implications for clinical care, research and policy. J. Natl. Cancer Inst. 111, 1120–1130. doi: 10.1093/jnci/djz089
Newcombe, R. G. (1998). Interval estimation for the difference between independent proportions: Comparison of eleven methods. Stat. Med. 17, 857–872. doi: 10.1002/(SICI)1097-0258(19980430)17:8<857::AID-SIM777>3.0.CO;2-E
Niedzwiedz, C. L., Knifton, L., Robb, K. A., Katikireddi, S. V., and Smith, D. J. (2019). Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 19:943. doi: 10.1186/s12885-019-6181-4
Norton, R. (1983). Measuring marital quality: A critical look at the dependent variable. J. Marriage Fam. 45, 141–151. doi: 10.2307/351302
Ramm, G. C., and Hasenbring, M. (2003). [The German adaptation of the Illness-specific social support scale and the test statistical evaluation on the basis of patients undergoing bone marrow transplantation with the Illness-specific social support scale (ISSS)]. Z. Med. Psychol. 12, 29–38.
Reker, G. T. (1992). Manual of the life attitude profile-revised (LAP-R). Peterborough: Student Psychologist Press.
Renzi, C., Kaushal, A., Emery, J., Hamilton, W., Neal, R. D., Rachet, B., et al. (2019). Comorbid chronic diseases and cancer diagnosis: Disease-specific effects and underlying mechanisms. Nat. Rev. Clin. Oncol. 16, 746–761. doi: 10.1038/s41571-019-0249-6
Revenson, T. A., and Schiaffino, K. M. (1990). “Development of a contextual social support measure for use with arthritis population,” in Paper presented at the 1990 convention of the arthritis health professionals association, Seattle.
Rosenberger, C., Hocker, A., Cartus, M., Schulz-Kindermann, F., Härter, M., and Mehnert, A. (2012). [Outpatient psycho-oncological care for family members and patients: Access, psychological distress and supportive care needs]. Psychother. Psychosom. Med. Psychol. 62, 185–194. doi: 10.1055/s-0032-1304994
Roth, A. J., Kornblith, A. B., Batel-Copel, L., Peabody, E., Scher, H. I., and Holland, J. C. (1998). Rapid screening for psychologic distress in men with prostate carcinoma: A pilot study. Cancer 82, 1904–1908. doi: 10.1002/(SICI)1097-0142(19980515)82:10<1904::AID-CNCR13>3.0.CO;2-X
Röthlin, F., Pelikan, J. M., and Ganahl, K. (2013). [The health literacy of 15-year-old adolescents in Austria]. Wien: Association of the Austrian Social Insurance Institutions.
Russ, T. C., Stamatakis, E., Hamer, M., Starr, J. M., Kivimaki, M., and Batty, G. D. (2012). Association between psychological distress and mortality: Individual participant pooled analysis of 10 prospective cohort studies. BMJ 345:e4933. doi: 10.1136/bmj.e4933
Russell, D., Peplau, L. A., and Cutrona, C. E. (1980). The revised UCLA loneliness scale: Concurrent and discriminant validity evidence. J. Pers. Soc. Psychol. 39, 472–480. doi: 10.1037/0022-3514.39.3.472
Sanson-Fisher, R., Girgis, A., Boyes, A., Bonevski, B., Burton, L., and Cook, P. (2000). The unmet supportive care needs of patients with cancer. Supportive care review group. Cancer 88, 226–237. doi: 10.1002/(SICI)1097-0142(20000101)88:1<226::AID-CNCR30>3.0.CO;2-P
Sauer, C., Weis, J., Faller, H., Junne, F., Hönig, K., Bergelt, C., et al. (2019). Impact of social support on psychosocial symptoms and quality of life in cancer patients: Results of a multilevel model approach from a longitudinal multicenter study. Acta Oncol. 58, 1298–1306. doi: 10.1080/0284186X.2019.1631471
Schulze, A., and Lampert, T. (2006). [Federal health survey: Social differences in smoking behavior and exposure to secondhand smoke in Germany]. Berlin: Robert-Koch-Institut.
Schwarz, R., and Hinz, A. (2001). Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur. J. Cancer 37, 1345–1351. doi: 10.1016/S0959-8049(00)00447-0
Selby, J. V., Beal, A. C., and Frank, L. (2012). The patient-centered outcomes research institute (PCORI) national priorities for research and initial research agenda. JAMA 307, 1583–1584. doi: 10.1001/jama.2012.500
Siegrist, J., and Marmot, M. (2004). Health inequalities and the psychosocial environment-two scientific challenges. Soc. Sci. Med. 58, 1463–1473. doi: 10.1016/S0277-9536(03)00349-6
Singer, S., Szalai, C., Briest, S., Brown, A., Dietz, A., Einenkel, J., et al. (2013). Co-morbid mental health conditions in cancer patients at working age–prevalence, risk profiles, and care uptake. Psychooncology 22, 2291–2297. doi: 10.1002/pon.3282
Sklenarova, H., Krümpelmann, A., Haun, M. W., Friederich, H. C., Huber, J., Thomas, M., et al. (2015). When do we need to care about the caregiver? Supportive care needs, anxiety, and depression among informal caregivers of patients with cancer and cancer survivors. Cancer 121, 1513–1519. doi: 10.1002/cncr.29223
Smitherman, A. B., Anderson, C., Lund, J. L., Bensen, J. T., Rosenstein, D. L., and Nichols, H. B. (2018). Frailty and comorbidities among survivors of adolescent and young adult cancer: A cross-sectional examination of a hospital-based survivorship cohort. J. Adolesc. Young Adult Oncol. 7, 374–383. doi: 10.1089/jayao.2017.0103
Spitzer, R. L., Kroenke, K., Williams, J. B., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Stulhofer, A., Busko, V., and Brouillard, P. (2010). Development and bicultural validation of the new sexual satisfaction scale. J. Sex Res. 47, 257–268. doi: 10.1080/00224490903100561
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., et al. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249. doi: 10.3322/caac.21660
Symonds, T., Boolell, M., and Quirk, F. (2005). Development of a questionnaire on sexual quality of life in women. J. Sex Marital Ther. 31, 385–397. doi: 10.1080/00926230591006502
Syrowatka, A., Motulsky, A., Kurteva, S., Hanley, J. A., Dixon, W. G., Meguerditchian, A. N., et al. (2017). Predictors of distress in female breast cancer survivors: A systematic review. Breast Cancer Res. Treat. 165, 229–245. doi: 10.1007/s10549-017-4290-9
Thana, K., Lehto, R., Sikorskii, A., and Wyatt, G. (2021). Informal caregiver burden for solid tumour cancer patients: A review and future directions. Psychol. Health 36, 1514–1535. doi: 10.1080/08870446.2020.1867136
Toussaint, A., and Herzog, A. (2020). Einführung somatoforme störungen, somatische belastungsstörungen. Willmering: UTB GmbH. doi: 10.36198/9783838553498
Ullrich, A., and Mehnert, A. (2010). [Psychometric validation of the 8-Item short-version of the Illness-specific social support scale (ISSS) among cancer patients]. Klin. Diagn. Eval. 3, 359–381.
Vandenbroucke, J. P., von Elm, E., Altman, D. G., Gotzsche, P. C., Mulrow, C. D., Pocock, S. J., et al. (2007). Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. Epidemiology 18, 805–835. doi: 10.1097/EDE.0b013e3181577511
Varela-Moreno, E., Rivas-Ruiz, F., Padilla-Ruiz, M., Alcaide-Garcia, J., Zarcos-Pedrinaci, I., Tellez, T., et al. (2022). Influence of depression on survival of colorectal cancer patients drawn from a large prospective cohort. Psychooncology 31, 1762–1773. doi: 10.1002/pon.6018
Voigt, V., Neufeld, F., Kaste, J., Bühner, M., Sckopke, P., Wuerstlein, R., et al. (2017). Clinically assessed posttraumatic stress in patients with breast cancer during the first year after diagnosis in the prospective, longitudinal, controlled COGNICARES study. Psychooncology 26, 74–80. doi: 10.1002/pon.4102
Walker, J., Magill, N., Mulick, A., Symeonides, S., Gourley, C., Toynbee, M., et al. (2020). Different independent associations of depression and anxiety with survival in patients with cancer. J. Psychosom. Res. 138:110218. doi: 10.1016/j.jpsychores.2020.110218
Walker, J., Mulick, A., Magill, N., Symeonides, S., Gourley, C., Burke, K., et al. (2021). Major depression and survival in people with cancer. Psychosom. Med. 83, 410–416. doi: 10.1097/PSY.0000000000000942
Ware, J. E., Kosinski, M., Dewey, J. E., and Gandek, B. (1999). How to score and interpret single-item health status measures: A manual for users of the SF-8TM health survey. Lincoln, RI: Quality Metric, Inc.
Weis, J., Hönig, K., Bergelt, C., Faller, H., Brechtel, A., Hornemann, B., et al. (2018). Psychosocial distress and utilization of professional psychological care in cancer patients: An observational study in national comprehensive cancer centers (CCCs) in Germany. Psychooncology 27, 2847–2854. doi: 10.1002/pon.4901
Weissflog, G., Hönig, K., Gündel, H., Lang, D., Niederwieser, D., Döhner, H., et al. (2017). Associations between dyadic coping and supportive care needs: Findings from a study with hematologic cancer patients and their partners. Support Care Cancer 25, 1445–1454. doi: 10.1007/s00520-016-3541-3
Winkler, J., and Stolzenberg, H. (2000). [Social class index in the federal health survey]. Gesundheitswesen 61, S178–S183.
World Health Organization [WHO] (2022). International statistical classification of diseases and related health problems (ICD). Available online at: www.who.int/standards/classifications/classification-of-diseases (accessed December 14, 2022).
Zimmermann, T. (2022). [Partnership and family aspects of cancer]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 65, 446–452. doi: 10.1007/s00103-022-03495-1
Zimmermann, T., de Zwaan, M., and Heinrichs, N. (2019). The German version of the quality of marriage index: Psychometric properties in a representative sample and population-based norms. PLoS One 14:e0212758. doi: 10.1371/journal.pone.0212758
Keywords: psychosocial distress, cancer patient, relatives, psychosocial support, psycho-oncology, socioeconomic status, survivorship, mental disorders
Citation: Mehnert-Theuerkauf A, Hufeld JM, Esser P, Goerling U, Hermann M, Zimmermann T, Reuter H and Ernst J (2023) Prevalence of mental disorders, psychosocial distress, and perceived need for psychosocial support in cancer patients and their relatives stratified by biopsychosocial factors: rationale, study design, and methods of a prospective multi-center observational cohort study (LUPE study). Front. Psychol. 14:1125545. doi: 10.3389/fpsyg.2023.1125545
Received: 16 December 2022; Accepted: 31 March 2023;
Published: 20 April 2023.
Edited by:
Simon Dunne, Dublin City University, IrelandReviewed by:
Clizia Cincidda, University of Milan, ItalyCopyright © 2023 Mehnert-Theuerkauf, Hufeld, Esser, Goerling, Hermann, Zimmermann, Reuter and Ernst. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anja Mehnert-Theuerkauf, YW5qYS5tZWhuZXJ0QG1lZGl6aW4udW5pLWxlaXB6aWcuZGU=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.