
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 29 March 2023
Sec. Neuropsychology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1121251
 Ciro Rosario Ilardi1
Ciro Rosario Ilardi1 Girolamo di Maio2
Girolamo di Maio2 Ines Villano2*
Ines Villano2* Giovanni Messina3
Giovanni Messina3 Vincenzo Monda4
Vincenzo Monda4 Antonietta Messina2
Antonietta Messina2 Chiara Porro3
Chiara Porro3 Maria Antonietta Panaro5Nadia Gamboz6
Maria Antonietta Panaro5Nadia Gamboz6 Alessandro Iavarone7
Alessandro Iavarone7 Marco La Marra2
Marco La Marra2Background: Parkinson’s disease (PD) is a chronic neurodegenerative disorder characterized by motor and non-motor symptoms. The latter mainly include affective, sleep, and cognitive deficits. Non-demented PD patients often demonstrate impairments in several executive domains following neuropsychological evaluation. The current pilot study aims at assessing the discriminatory power of the Frontal Assessment Battery-15 (FAB15) in differentiating (i) non-demented PD patients and healthy controls and (ii) PD patients with more and less pronounced motor symptoms.
Methods: Thirty-nine non-demented early-stage PD patients in the “on” dopamine state (26 females, mean age = 64.51 years, SD = 6.47, mean disease duration = 5.49 years, SD = 2.28) and 39 healthy participants (24 females, mean age = 62.60 years, SD = 5.51) were included in the study. All participants completed the FAB15. Motor symptoms of PD patients were quantified via the Unified Parkinson’s Disease Rating Scale-Part III (UPDRS-Part III) and Hoehn and Yahr staging scale (H&Y).
Results: The FAB15 score, adjusted according to normative data for sex, age, and education, proved to be sufficiently able to discriminate PD patients from healthy controls (AUC = 0.69 [95% CI 0.60–0.75], SE = 0.06, p = 0.04, optimal cutoff = 11.29). Conversely, the battery lacked sufficient discriminative capability to differentiate PD patients based on the severity of motor symptoms.
Conclusion: The FAB15 may be a valid tool for distinguishing PD patients from healthy controls. However, it might be less sensitive in identifying clinical phenotypes characterized by visuospatial impairments resulting from posteroparietal and/or temporal dysfunctions. In line with previous evidence, the battery demonstrated to be not expendable in the clinical practice for monitoring the severity of PD-related motor symptoms.
Parkinson’s disease (PD) is a progressive neurodegenerative disorder whose etiology, resulting from the interaction between environmental and genetic factors, is still unclear (Hirsch et al., 2013; Beitz, 2014; Tysnes and Storstein, 2017; Simon et al., 2020). PD prevalence is about 1–4% (de Lau and Breteler, 2006; Pringsheim et al., 2014; Marras et al., 2018) while incidence is hovering around 16–19/100,000 new cases per year (Tanner and Goldman, 1996; Twelves et al., 2003; Alves et al., 2008).
The pathognomonic clinical manifestations of PD are bradykinesia and/or hypokinesia, rigidity, rest tremor, gait dysfunctions, and postural instability (Jankovic, 2005, 2008; National Collaborating Centre for Chronic Conditions (UK), 2006; Postuma et al., 2015). The pathophysiology of PD is mainly characterized by degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNc) (Rodriguez-Oroz et al., 2009; Dirnberger and Jahanshahi, 2013; Pagonabarraga et al., 2015). This leads to functional alterations within the nigrostriatal pathway connecting the SNc to the dorsal striatum (Deumens et al., 2002; Di Monte, 2003; Herrera et al., 2017). A reduced supply of dopamine to the caudate nucleus affects visuomotor control (Yanagisawa et al., 1989; Owen, 1998; Bloem et al., 2004; Brooks and Piccini, 2006; Chieffi et al., 2014, 2019), making the patient unable to respond to external stimuli with rapid and appropriate intentional motor responses. In addition, decreased dopamine supply to the putamen results in the inability to perform fine sequential movements (Graybiel et al., 1990; Yu et al., 2013; Ilardi et al., 2022a; La Marra et al., 2022d).
Although the clinical management of PD is typically centered on the treatment of the cardinal motor symptoms, these often coexist with non-motor symptoms such as fatigue (Friedman et al., 2007; Herlofson and Kluger, 2017; Siciliano et al., 2018), depression (Cummings, 1992; Schrag, 2006; Reijnders et al., 2008), anxiety (Richard et al., 1996; Richard, 2005; Ray and Agarwal, 2020), apathy (den Brok et al., 2015; Pagonabarraga and Kulisevsky, 2017; D’Iorio et al., 2018), sleep disorders (Comella, 2007; Zhang et al., 2020; Maggi et al., 2021), urological dysfunctions (Blackett et al., 2009; Yeo et al., 2012; Margolesky et al., 2020), and cognitive impairments (Padovani et al., 2006; Litvan et al., 2012; Yang et al., 2016) ranging from mild deficits to overt dementia.
In PD, deficits of executive functions are the most representative expression of cognitive impairment in both demented and non-demented patients (Zgaljardic et al., 2003; Kudlicka et al., 2011; Dirnberger and Jahanshahi, 2013; Mack and Marsh, 2017; O’Callaghan and Lewis, 2017) and are likely due to abnormal activity in the frontostriatal network (Zgaljardic et al., 2003; Mack and Marsh, 2017; Lang et al., 2019). Executive functions are a family of top-down mental processes, such as attention, abstract thinking, planning, cognitive flexibility, inhibitory control and working memory, which are involved in the execution of complex action schemes aimed at adaptively coping with environmental requests in unfamiliar or conflicting contexts (Burgess and Simons, 2005; Diamond, 2013; La Marra et al., 2022b). Besides executive blunting often revealed during formal neuropsychological evaluation, it seems that PD patients are impaired in dual-task performance, i.e., the concurrent execution of two or more attention-demanding tasks, and compensate their difficulties in making simple procedural motor tasks, such as walking, via hypercontrolled movements (Kelly et al., 2012; Raffegeau et al., 2019). These phenomena can be considered indexes of a limited/overloaded executive control system (Ceravolo et al., 2012; Dirnberger and Jahanshahi, 2013). Since executive dysfunctions are associated with inability to perform efficiently daily activities and poor quality of life in non-demented PD patients (Ceravolo et al., 2012), early detection of executive deficits may enable clinicians to predict which patients will develop dementia.
Among the available psychometric tests devoted to the assessment of executive functions, the Frontal Assessment Battery (FAB) (Dubois et al., 2000) is the most widely used screening tool. It is employed internationally for assessing general executive functioning at the bedside and in the outpatient clinical practice. Some studies have found that non-demented PD patients got lower FAB scores than healthy controls (Lima et al., 2008; Kenangil et al., 2010; Koerts et al., 2011; Bezdicek et al., 2017). However, it is unclear whether the battery holds sufficient discriminatory power for distinguishing between non-demented PD patients and cognitively-intact individuals without PD (Hurtado-Pomares et al., 2018b). Furthermore, to the best of our knowledge, no study assessed the extent to which the FAB could differentiate PD patients according to the severity of motor symptoms. The close relationship between executive and motor functions is inherent in the very concept of executive functions and likely justified by shared neural mechanisms involving cortical and subcortical frontal regions (Raz, 1997; Rycroft et al., 2019) as well as basal ganglia (Dubois et al., 2000; Bezdicek et al., 2017) and cerebellum (Koppelmans et al., 2017). Interestingly, according to a recent theoretical model described by Koziol et al. (2012) and Koziol and Lutz (2013), the functional architecture of the brain would evolve from childhood to adulthood for promoting action control, facilitating interactive adaptive behaviors rather than the efficiency of cognitive processes. Hence, the maturation of frontal (and executive) functions may be significantly affected by the sensorimotor interaction with the environment.
The present pilot study aims to evaluate the above psychometric dimensions of the FAB’s clinicometric validity, but on a shortened version of the battery, namely, the Frontal Assessment Battery-15 (FAB15) (Ilardi et al., 2022b). The choice of this FAB version stems from its robust psychometric architecture that boasts a solid factorial structure, good internal consistency, excellent interrater and test-retest reliabilities, and regression-based norms extracted –to the best of our knowledge– from the largest normative sample ever recruited in Italy for a neuropsychological tool (Ilardi et al., 2022b). In addition, the FAB15 solves the well-known problem concerning the pronounced ceiling effect typically encountered in both healthy (Asaadi et al., 2016; Bezdicek et al., 2017; Hurtado-Pomares et al., 2018b; Goh et al., 2019; Abrahámová et al., 2022) and clinical populations (Stamelou et al., 2015; Hurtado-Pomares et al., 2018b; Goh et al., 2019) on the sixth and last FAB subtest, which was originally devised to explore one the components of the environmental dependency, i.e., the prehension behavior (Dubois et al., 2000). This makes the FAB15 more valid and severe as compared with the conventional six-item battery.
Retrospective data collection was performed for consecutive patients referred to the Neurology Outpatient Clinic of CTO Hospital (Neurological Unit, AORN “Ospedali dei Colli,” Naples, Italy). Eligible patients satisfied the following inclusion criteria: diagnosis of PD according to MDS-PD Criteria (Postuma et al., 2015), ≤80 years of age, ≥5 years of formal schooling, no visual or hearing impairment, and adjusted scores higher than normative datasets provided for the Mini-Mental State Examination (MMSE). Patients were excluded if affected by atypical or secondary parkinsonism, Mild Cognitive Impairment (MCI) in PD (Litvan et al., 2012) or PD dementia (Goetz et al., 2009). In addition, we excluded patients with current or past history of major depression, bipolar disorder, schizophrenia, epilepsy, transient ischemic attack, stroke, head injury, serious medical illnesses, or alcohol/drug abuse. All PD patients were examined in the “on” dopamine state.
Healthy volunteers were recruited in order to construct a matched-control sample. Inclusion criteria were age ≤80 years, ≥5 years of education, no visual or hearing impairment, and adjusted MMSE score within the normality range. Exclusion criteria were previous or current neurocognitive (mild and major), psychiatric, or psychological disorders, and ongoing intake of psychotropic drugs potentially interfering with the efficiency of cognitive processes.
All participants were administered the MMSE and the FAB15. The latter is a validated shortened version of the conventional FAB, from which the prehension behavior subtest (environmental dependency) was removed following a thorough psychometric investigation on 1,187 healthy individuals (Ilardi et al., 2022b). Thus, the FAB15 consists of five subtests (i.e., similarities, phonological verbal fluency, Luria’s fist-edge-palm test, conflicting instructions, and go-no-go test) assessing as many executive domains (i.e., abstraction ability, cognitive flexibility, planning and executing motor sequences, sensitivity to interference, and inhibitory control). The total FAB15 score ranges from 0 to 15, with a higher score indicating a better executive functioning. The psychometric properties of the new FAB15 are described in detail elsewhere (Ilardi et al., 2022b).
For PD patients, we had available data about disease duration, Levodopa Equivalent Daily Dose (LEDD) and severity of motor symptoms, which was assessed via both the Unified Parkinson’s Disease Rating Scale-Part III (UPDRS-Part III) (Goetz et al., 2008) and Hoehn and Yahr staging (H&Y scale) (Goetz et al., 2004). The UPDRS-Part III is composed of 18 items (response set from 0 = “normal” to 4 = “severe”) exploring motor signs of PD (i.e., speech, facial expression, rigidity, finger taps, hand movements, pronation/supination, toe tapping, leg agility, arising from chair, gait, freezing of gait, postural stability, posture, global spontaneity of movements, postural tremor of hands, kinetic tremor of hands, rest tremor amplitude, constancy of rest tremor). The H&Y scale is a descriptive clinical staging scale for PD and takes into account both functional and motor impairments. According to the H&Y scale, patients can be classified as having from a stage 1 (“unilateral involvement only”) to a stage 5 disease (“wheelchair bound or bedridden unless aided”). For all participants, the neuropsychological examination was conducted by trained neuropsychologists.
All participants gave prior written informed consent to the study which was approved by the ethics committee of the University of Campania “Luigi Vanvitelli” and carried out according to the 1964 Declaration of Helsinki.
For descriptive purposes, between-group comparisons were conducted by means of two-way chi-squared test (χ2) for nominal variables, and univariate analysis of variance (ANOVA), Mann–Whitney (U) Test, or Kruskal–Wallis (H) test for continuous variables, when appropriate. To determine the diagnostic accuracy of FAB15, we firstly adjusted raw scores according to normative correction grids for sex, age, and education (Ilardi et al., 2022b). Then, we ran three non-parametric Receiver Operating Characteristic (ROC) curve analyses (Mandrekar, 2010), where group (PD patients vs. healthy controls) and severity of motor symptoms (PD patients with greater motor symptoms vs. PD patients with minor motor symptoms) entered as state variables. For all ROC curve analyses, the FAB15 corrected score entered as test variable. The Youden index (YI, sensitivity + specificity − 1) was employed in order to identify any optimal cutoffs (Liu, 2012; Unal, 2017). A p-value ≤ 0.05 was considered statistically significant. Analyses were conducted by means of IBM SPSS Statistics for Windows, v. 26 (IBM, Armonk, 204 NY, USA) and easyROC, v. 1.3.1., using R language.
At a nominal alpha level of 0.05, 1–β set to 0.80, expected AUC of 0.80, and allocation ratio = 1, the required total sample size for conducting a ROC curve analysis was 20 sample units (Obuchowski, 2005).
We analyzed data from 39 PD patients (26 females, M age = 64.51 years, SD = 6.47, M education = 9.97 years, SD = 4.25; M disease duration = 5.49 years, SD = 2.28) and 39 healthy participants (24 females, M age = 62.60 years, SD = 5.51, M education = 8.97 years, SD = 3.61). General descriptive statistics are summarized in Table 1. No between-group differences were detected in the frequency of the sex variable’s levels [χ2(1) = 0.233, p = 0.64]. Similarly, patient and control groups were equivalent in terms of years of age [F(1,76) = 1.966, p = 0.165], years of education [F(1,76) = 1.256, p = 0.266], and MMSE score [F(1,76) = 0.02, p = 0.89]. Instead, as expected, healthy subjects outperformed PD patients on general executive functioning [FAB15, F(1, 76) = 4.464, p = 0.03]. Twenty-two patients got an adjusted FAB15 score below the upper limits of the equivalent score 1 (score < 11.12), suggesting a performance on the edge of normality.
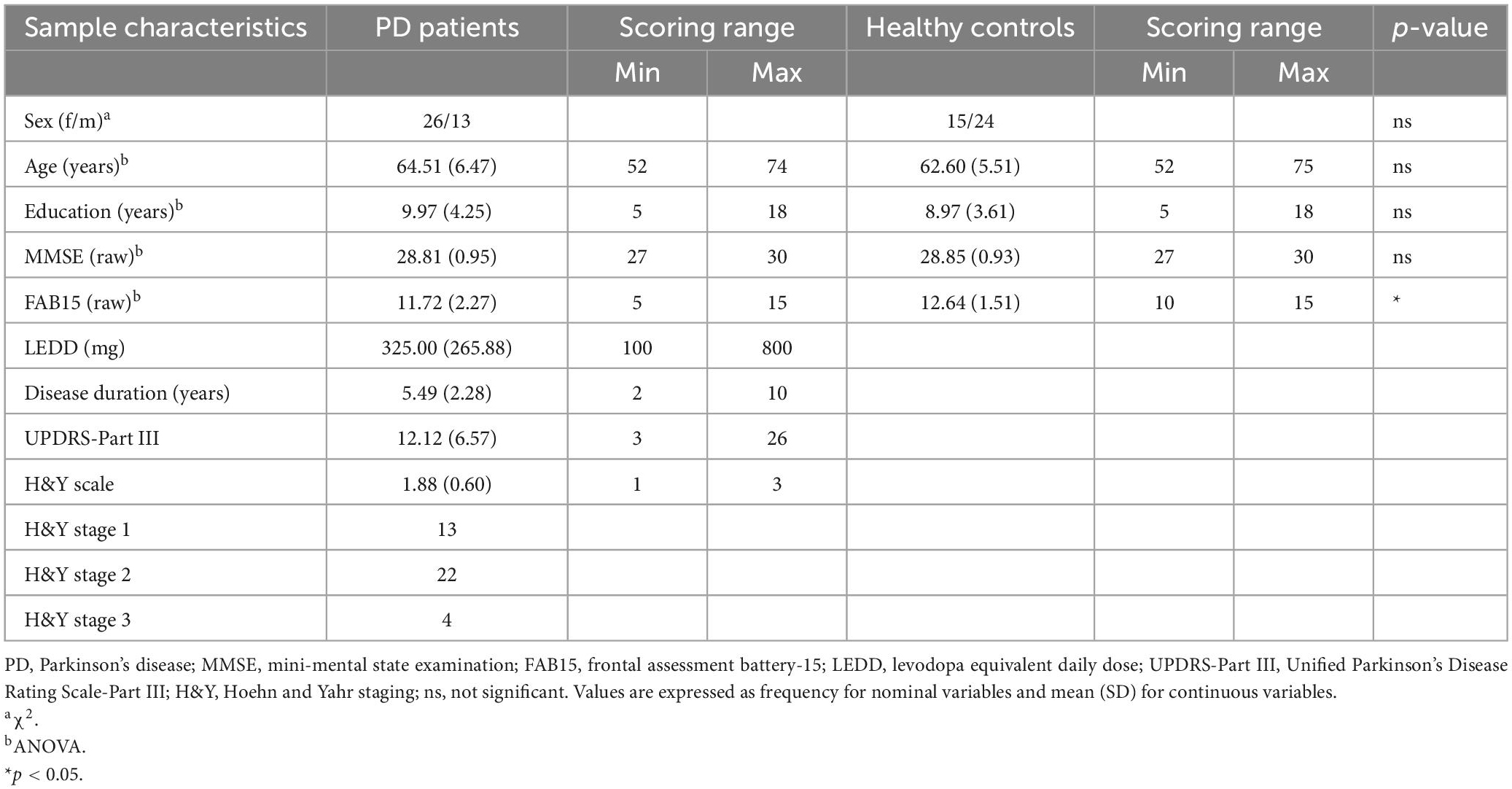
Table 1. Descriptive statistics concerning the patient and control group.
To assess whether the FAB15 was able to differentiate PD patients from healthy controls, a ROC curve analysis was performed, entering the group (patients vs. controls) as state variable and the adjusted FAB15 score as test variable. The FAB15 proved to be sufficiently discriminative (AUC = 0.69 [95% CI 0.60–0.75], SE = 0.06, p = 0.04). Based on a simultaneous assessment of sensitivity and specificity across all the possible cutoff points, the optimal FAB15 cutoff for differentiating PD patients from healthy participants on the adjusted scores distribution was 11.29 (sensitivity = 0.51, specificity = 0.89, YI = 0.28).
To examine the capability of the FAB15 in discriminating between PD patients with more- and less-deep impacting motor symptoms, two ROC curve analyses were performed. Based on tertiles (Ti) calculated along the UPDRS-Part III score distribution (T1 = 8, T2 = 15), patients were divided into three subgroups (see Table 2): slight motor impairment (SMI, 14 patients getting a score ≤ 8), mild motor impairment (MMI, 11 patients getting a score ranging from 9 to 14), and large motor impairment (LMI, 14 patients getting a score ≥ 15). This 3-level ordinal variable was used as state variable while the adjusted FAB15 score entered as test variable. Results suggested that FAB15 lacked sufficient discriminative capability if required to differentiate PD patients based on the severity of motor symptoms evaluated via UPDRS: SMI group vs. MMI group, AUC = 0.50 [95% CI 0.13–0.87], SE = 0.19, p = 0.99; SMI group vs. LMI group, AUC = 0.64 [95% CI 0.31–0.97], SE = 0.17, p = 0.42; MMI group vs. LMI group, AUC = 0.60 [95% CI 0.24–0.95], SE = 0.18, p = 0.58. As concerns the H&Y score, patients were splitted into two subgroups in an attempt to balance the sample size, with all the limits that the overt positive skewness entails: 13 patients with H&Y stage 1 disease and 26 patients with H&Y stage ≥ 2 disease (see Table 3). Similarly, this nominal variable entered the ROC curve analysis as state variable, whereas the adjusted FAB15 score was employed as test variable. Again, results showed that FAB15 was unable to detect the variability of motor impairment in PD patients according to the H&Y classification: AUC = 0.67 [95% CI 0.40–0.99], SE = 0.15, p = 0.23.
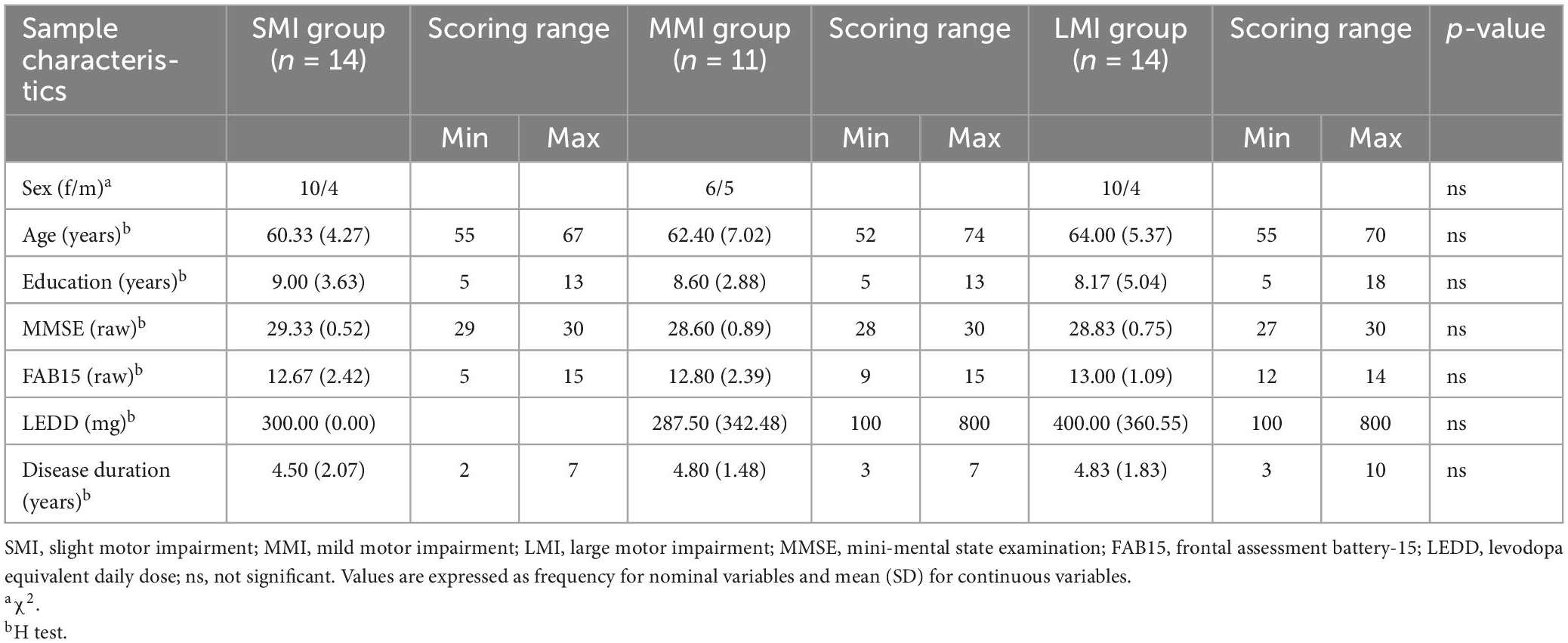
Table 2. Descriptive statistics on UPDRS-based groups.
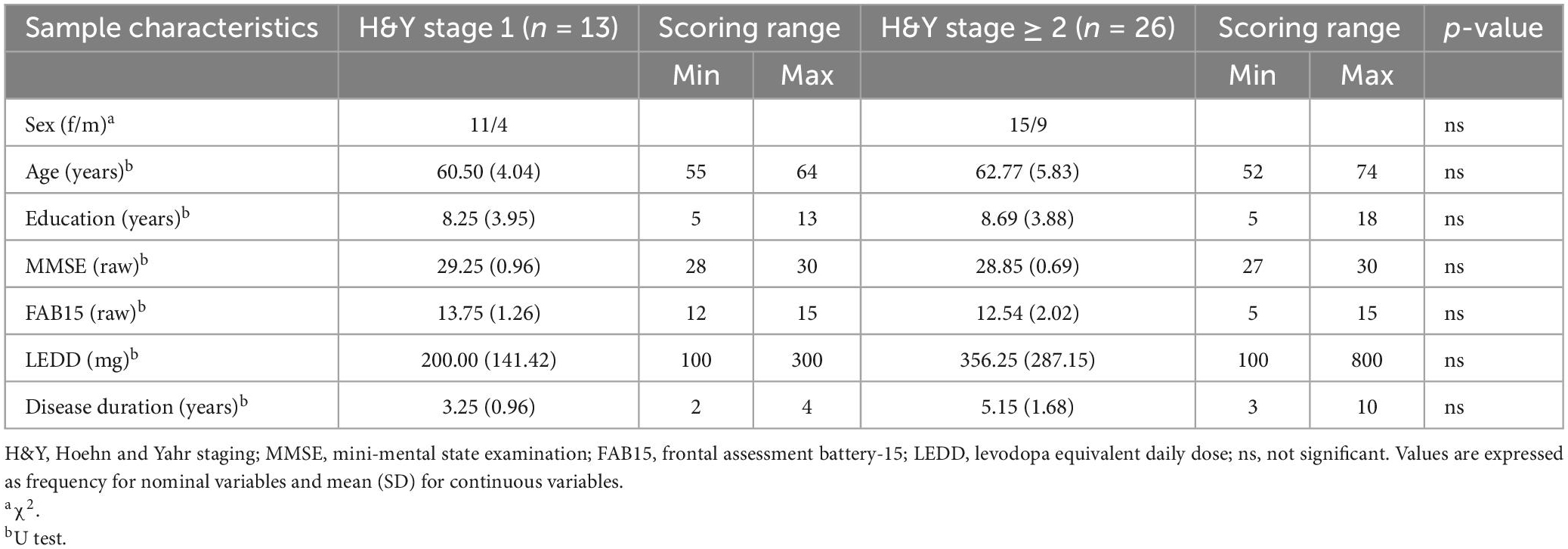
Table 3. Descriptive statistics on H&Y-based groups.
A high proportion of PD patients without MCI/dementia demonstrate executive deficits following neuropsychological evaluation. These mainly involve planning and performing complex goal-directed actions, abstract thinking, inhibitory control, set-shifting, and working memory (Foster and Hershey, 2011; O’Callaghan et al., 2014; D’Iorio et al., 2021).
Dysfunction in the frontostriatal network is likely responsible for the onset of executive deficits in non-demented PD patients. The nigrostriatal pathology results in dopamine depletion in the dorsal striatum, with relative sparing of the ventral striatum. As a consequence, dopamine depletion in the somatosensory cortex –in addition to decreased connectivity within the somatosensory and dorsolateral prefrontal cortices (Tekin and Cummings, 2002; Helmich et al., 2010; Chieffi et al., 2017; Polito et al., 2020a; Villano et al., 2021)– accounts for the emergence of executive deficits in PD (Jellinger, 2001; O’Callaghan et al., 2014; Lang et al., 2019). Since executive functions orchestrate most of our daily activities (Bell-McGinty et al., 2002; Miller and Wallis, 2009; Stuss, 2011; Francavilla et al., 2020; Polito et al., 2020b; La Marra et al., 2022a,e), early identification of executive deficits in PD may help predict patients who will develop dementia.
In the current pilot clinicometric study, we tested the diagnostic properties of the short FAB15 in discriminating between non-demented PD patients and healthy controls. We found that non-demented PD patients showed normal global cognitive functioning but a certain degree of impairment in executive abilities. Furthermore, the FAB15 showed a fair diagnostic capability in differentiating between non-demented PD patients and healthy participants. As a consequence, we argue that FAB15 may be considered a valid tool to support diagnosis of PD, even independently on disease duration or severity of motor symptoms. This result is in line with previous evidence suggesting that (a) non-demented PD patients typically show executive blunting and (b) the FAB score is related to lower gray matter density in cortical regions strictly involved in executive functioning (Bezdicek et al., 2017; Ilardi et al., 2022a).
Nevertheless, in the context of PD, the FAB15 diagnostic capability is disputable but improvable. On the one hand, our small sample size and the patients’ clinical characteristics are to be accounted for (La Marra et al., 2022c); on the other hand, PD patients may also suffer from occipito-temporal dysfunctions determining visuospatial deficits (Watson and Leverenz, 2010; Koerts et al., 2011). From a neurocognitive standpoint and in line with the dual syndrome hypothesis, there would be two kinds of PD neuropsychological profiles: one with executive impairments reflecting neurofunctional abnormalities in the frontostriatal network, and the other one with visuospatial impairments due to posteroparietal (especially along the mesial portion, e.g., precuneus) and temporal dysfunctions (Kehagia et al., 2010, 2013). Since the FAB appears to be mainly sensitive to impairments in the dorsolateral, ventro-, and orbito-medial prefrontal regions, as well as in the basal ganglia (Dubois et al., 2000; Bezdicek et al., 2017; Hurtado-Pomares et al., 2018a), it might be able to identify non-demented PD patients with predominant executive but not visuospatial deficits (Bezdicek et al., 2017).
Our second aim was to check whether the battery was able to discriminate non-demented PD patients with more and less prominent motor marks, which were quantified by the UPDRS-Part III and H&Y scale. In sum, the FAB15 was unable to consistently capture the severity of motor symptoms caused by PD. Results from the present pilot study are supported by previous research finding no difference on the UPDRS score between groups of patients with higher and lower FAB scores (Matsui et al., 2006) and no correlation between motor and executive deficits in PD (Kenangil et al., 2010); in our study: FAB15 vs. UPDRS-Part III, rrho = −0.104, p = 0.691; FAB15 vs. H&Y, rrho = −0.105, p = 0.688.
By the very nature of pilot studies, there are critical limitations to their epistemological weight and interpretation. The main limitations of the present study have to be attributed to the narrow sample size and to the fact that patients were in the early stage of the disease. However, according to a priori power analysis, our sample appeared to be sufficiently large to test the FAB15 diagnostic accuracy. Moreover, the scientific literature of reference claims that cognitive deficits are typically detected in PD from the early stages after diagnosis (Poletti et al., 2012). However, it is certain that the discriminatory power of the FAB15 in relation to the severity of motor symptoms should be addressed with an ad hoc recruitment also covering an a priori classification of the disease severity levels.
It is important to note that our sample may not be sufficiently representative of the PD population since the occurrence of this pathology appears to be moderated by gender differences, with men affected twice as often as women (Baldereschi et al., 2000). Still, recent findings on PD have suggested that executive impairments are significantly greater in males than females after adjusting for demographic variables and disease severity (Reekes et al., 2020). This result was not replicated in our investigation (males with PD vs. females with PD on FAB15: U = 165.50, SE = 33.12, p = 0.92).
Finally, we included only PD patients in the “on” state. Nevertheless, it has been observed that, unlike PD-related motor symptoms, cognitive blunting may be not significantly affected by antiparkinsonian treatment with intravenous levodopa (Leh et al., 2010).
The FAB15 proved useful in differentiating PD patients without MCI/dementia and healthy controls. Conversely, this neuropsychological battery demonstrated to be not expendable in the clinical practice for monitoring the severity of PD-related motor symptoms. Our results should be taken with caution due to pilot study design. The clinicometric validity of the FAB15 needs to be further assessed in future investigations preferably encompassing a larger –and more differentiated– sample of PD patients.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
All participants gave prior written informed consent to the study which was approved by the Ethics Committee of the University of Campania “Luigi Vanvitelli” and carried out according to the 1964 Declaration of Helsinki. The patients/participants provided their written informed consent to participate in this study.
CRI and MLM: conceptualization, methodology, and formal analysis. CRI: software. AM and IV: validation. CRI, MLM, CP, AI, GdM, and VM: investigation. AM, GdM, IV, NG, and VM: resources. CRI, MP, and GdM: data curation. CRI, MLM, and IV: writing—original draft preparation. CRI, MLM, IV, and AI: writing—review and editing. NG: visualization. CRI, MLM, IV, GM, and AI: supervision and project administration. All authors read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abrahámová, M., Smolejová, E., Dančík, D., Pribišová, K., Heretik, A., and Hajdúk, M. (2022). Normative data for the Slovak version of the frontal assessment battery (FAB). Appl. Neuropsychol. Adult 29, 273–278. doi: 10.1080/23279095.2020.1748031
Alves, G., Forsaa, E. B., Pedersen, K. F., Dreetz Gjerstad, M., and Larsen, J. P. (2008). Epidemiology of Parkinson’s disease. J. Neurol. 255, 18–32.
Asaadi, S., Ashrafi, F., Omidbeigi, M., Nasiri, Z., Pakdaman, H., and Amini-Harandi, A. (2016). Persian version of frontal assessment battery: Correlations with formal measures of executive functioning and providing normative data for Persian population. Iran. J. Neurol. 15, 16–22.
Baldereschi, M., Di Carlo, A., Rocca, W. A., Vanni, P., Maggi, S., Perissinotto, E., et al. (2000). Parkinson’s disease and parkinsonism in a longitudinal study: Two-fold higher incidence in men. Neurology 55, 1358–1363. doi: 10.1212/WNL.55.9.1358
Bell-McGinty, S., Podell, K., Franzen, M., Baird, A. D., and Williams, M. J. (2002). Standard measures of executive function in predicting instrumental activities of daily living in older adults. Int. J. Geriatr. Psychiatry 17, 828–834. doi: 10.1002/gps.646
Bezdicek, O., Růžička, F., Fendrych Mazancova, A., Roth, J., Dušek, P., Mueller, K., et al. (2017). Frontal assessment battery in Parkinson’s disease: Validity and morphological correlates. J. Int. Neuropsychol. Soc. 23, 675–684. doi: 10.1017/S1355617717000522
Blackett, H., Walker, R., and Wood, B. (2009). Urinary dysfunction in Parkinson’s disease: A review. Parkinsonism Relat. Disord. 15, 81–87. doi: 10.1016/j.parkreldis.2007.10.016
Bloem, B. R., Hausdorff, J. M., Visser, J. E., and Giladi, N. (2004). Falls and freezing of gait in Parkinson’s disease: A review of two interconnected, episodic phenomena. Mov. Disord. 19, 871–884. doi: 10.1002/mds.20115
Brooks, D. J., and Piccini, P. (2006). Imaging in Parkinson’s disease: The role of monoamines in behavior. Biol. Psychiatry 59, 908–918. doi: 10.1016/j.biopsych.2005.12.017
Burgess, P. W., and Simons, J. S. (2005). “Theories of frontal lobe executive function: Clinical applications,” in The effectiveness of rehabilitation for cognitive deficits, eds P. W. Halligan and D. T. Wade (Oxford: Oxford University Press), 211–232. doi: 10.1093/acprof:oso/9780198526544.003.0018
Ceravolo, R., Pagni, C., Tognoni, G., and Bonuccelli, U. (2012). The epidemiology and clinical manifestations of dysexecutive syndrome in Parkinson’s disease. Front. Neur. 3:159. doi: 10.3389/fneur.2012.00159
Chieffi, S., Castaldi, C., Di Maio, G., La Marra, M., Messina, A., Monda, V., et al. (2019). Attentional bias in the radial and vertical dimensions of space. C. R. Biol. 342, 97–100. doi: 10.1016/j.crvi.2019.03.003
Chieffi, S., Messina, A., Villano, I., Valenzano, A. A., Nigro, E., La Marra, M., et al. (2017). The use of velocity information in movement reproduction. Front. Psychol. 8:983. doi: 10.3389/fpsyg.2017.00983
Chieffi, S., Messina, G., La Marra, M., Iavarone, A., Viggiano, A., De Luca, V., et al. (2014). “Distractor interference in visual motor tasks,” in Horizon in neuroscience research, eds. A. Costa and E. Villalba (Hauppauge, NY: Nova Science Publishers, Inc.).
Comella, C. L. (2007). Sleep disorders in Parkinson’s disease: An overview. Mov. Disord. 22, S367–S373. doi: 10.1002/mds.21682
Cummings, J. (1992). Depression and Parkinson’s disease: A review. Am. J. Psychiatry 149, 443–454. doi: 10.1176/ajp.149.4.443
D’Iorio, A., Guida, P., Maggi, G., Redgrave, P., Santangelo, G., and Obeso, I. (2021). Neuropsychological spectrum in early PD: Insights from controlled and automatic behavioural regulation. Neurosci. Biobehav. Rev. 126, 465–480. doi: 10.1016/j.neubiorev.2021.04.003
D’Iorio, A., Maggi, G., Vitale, C., Trojano, L., and Santangelo, G. (2018). “Pure apathy” and cognitive dysfunctions in Parkinson’s disease: A meta-analytic study. Neurosci. Biobehav. Rev. 94, 1–10. doi: 10.1016/j.neubiorev.2018.08.004
de Lau, L. M., and Breteler, M. M. (2006). Epidemiology of Parkinson’s disease. Lancet Neurol. 5, 525–535. doi: 10.1016/S1474-4422(06)70471-9
den Brok, M. G. H. E., van Dalen, J. W., van Gool, W. A., Moll van Charante, E. P., de Bie, R. M. A., and Richard, E. (2015). Apathy in Parkinson’s disease: A systematic review and meta-analysis: Apathy in Parkinson’s disease. Mov. Disord. 30, 759–769. doi: 10.1002/mds.26208
Deumens, R., Blokland, A., and Prickaerts, J. (2002). Modeling Parkinson’s disease in rats: An evaluation of 6-OHDA lesions of the nigrostriatal pathway. Exp. Neurol. 175, 303–317. doi: 10.1006/exnr.2002.7891
Di Monte, D. (2003). The environment and Parkinson’s disease: Is the nigrostriatal system preferentially targeted by neurotoxins? Lancet Neurol. 2, 531–538. doi: 10.1016/S1474-4422(03)00501-5
Diamond, A. (2013). Executive functions. Annu. Rev. Psychol. 64, 135–168. doi: 10.1146/annurev-psych-113011-143750
Dirnberger, G., and Jahanshahi, M. (2013). Executive dysfunction in Parkinson’s disease: A review. J. Neuropsychol. 7, 193–224. doi: 10.1111/jnp.12028
Dubois, B., Slachevsky, A., Litvan, I., and Pillon, B. (2000). The FAB: A frontal assessment battery at bedside. Neurology 55, 1621–1626. doi: 10.1212/WNL.55.11.1621
Foster, E. R., and Hershey, T. (2011). Everyday executive function is associated with activity participation in Parkinson disease without dementia. OTJR Occup. Particip. Health 31, S16–S22. doi: 10.3928/15394492-20101108-04
Francavilla, V. C., Genovesi, F., Asmundo, A., Di Nunno, N. R., Ambrosi, A., Tartaglia, N., et al. (2020). Fascia and movement: The primary link in the prevention of accidents in soccer. Revision and models of intervention. Med. Sport 73, 291–301. doi: 10.23736/S0025-7826.20.03677-7
Friedman, J. H., Brown, R. G., Comella, C., Garber, C. E., Krupp, L. B., Lou, J.-S., et al. (2007). Fatigue in Parkinson’s disease: A review. Mov. Disord. 22, 297–308. doi: 10.1002/mds.21240
Goetz, C. G., Emre, M., and Dubois, B. (2009). Parkinson’s disease dementia: Definitions, guidelines, and research perspectives in diagnosis. Ann. Neurol. 64, S81–S92. doi: 10.1002/ana.21455
Goetz, C. G., Poewe, W., Rascol, O., Sampaio, C., Stebbins, G. T., Counsell, C., et al. (2004). Movement disorder society task force report on the Hoehn and Yahr staging scale: Status and recommendations the Movement disorder society task force on rating scales for Parkinson’s disease. Mov. Disord. 19, 1020–1028. doi: 10.1002/mds.20213
Goetz, C. G., Tilley, B. C., Shaftman, S. R., Stebbins, G. T., Fahn, S., Martinez-Martin, P., et al. (2008). Movement disorder society-sponsored revision of the unified Parkinson’s disease rating scale (MDS-UPDRS): Scale presentation and clinimetric testing results: MDS-UPDRS: Clinimetric assessment. Mov. Disord. 23, 2129–2170. doi: 10.1002/mds.22340
Goh, W. Y., Chan, D., Ali, N. B., Chew, A. P., Chuo, A., Chan, M., et al. (2019). Frontal assessment battery in early cognitive impairment: Psychometric property and factor structure. J. Nutr. Health Aging 23, 966–972. doi: 10.1007/s12603-019-1248-0
Graybiel, A. M., Hirsch, E. C., and Agid, Y. (1990). The nigrostriatal system in Parkinson’s disease. Adv. Neurol. 53, 17–29.
Helmich, R. C., Derikx, L. C., Bakker, M., Scheeringa, R., Bloem, B. R., and Toni, I. (2010). Spatial remapping of cortico-striatal connectivity in Parkinson’s disease. Cereb. Cortex 20, 1175–1186. doi: 10.1093/cercor/bhp178
Herlofson, K., and Kluger, B. M. (2017). Fatigue in Parkinson’s disease. J. Neurol. Sci. 374, 38–41. doi: 10.1016/j.jns.2016.12.061
Herrera, A., Muñoz, P., Steinbusch, H. W. M., and Segura-Aguilar, J. (2017). Are dopamine oxidation metabolites involved in the loss of dopaminergic neurons in the nigrostriatal system in Parkinson’s disease? ACS Chem. Neurosci. 8, 702–711. doi: 10.1021/acschemneuro.7b00034
Hirsch, E. C., Jenner, P., and Przedborski, S. (2013). Pathogenesis of Parkinson’s disease: Pathogenesis of Parkinson’s disease. Mov. Disord. 28, 24–30. doi: 10.1002/mds.25032
Hurtado-Pomares, M., Terol-Cantero, M. C., Sánchez-Pérez, A., Leiva-Santana, C., Peral-Gómez, P., Valera-Gran, D., et al. (2018b). Measuring executive dysfunction in Parkinson’s disease: Reliability and validity of the Spanish version of Frontal Assessment Battery (FAB-E). PLoS One 13:e0207698. doi: 10.1371/journal.pone.0207698
Hurtado-Pomares, M., Carmen Terol-Cantero, M., Sánchez-Pérez, A., Peral-Gómez, P., Valera-Gran, D., and Navarrete-Muñoz, E. M. (2018a). The frontal assessment battery in clinical practice: A systematic review: Clinical practice of the FAB. Int. J. Geriatr. Psychiatry 33, 237–251. doi: 10.1002/gps.4751
Ilardi, C. R., Iavarone, A., La Marra, M., Iachini, T., and Chieffi, S. (2022a). Hand movements in mild cognitive impairment: Clinical implications and insights for future research. J. Integr. Neurosci. 21:067. doi: 10.31083/j.jin2102067
Ilardi, C. R., Chieffi, S., Scuotto, C., Gamboz, N., Galeone, F., Sannino, M., et al. (2022b). The frontal assessment battery 20 years later: Normative data for a shortened version (FAB15). Neurol. Sci. 43, 1709–1719. doi: 10.1007/s10072-021-05544-0
Jankovic, J. (2005). Motor fluctuations and dyskinesias in Parkinson’s disease: Clinical manifestations. Mov. Disord. 20, S11–S16. doi: 10.1002/mds.20458
Jankovic, J. (2008). Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 79, 368–376. doi: 10.1136/jnnp.2007.131045
Kehagia, A. A., Barker, R. A., and Robbins, T. W. (2010). Neuropsychological and clinical heterogeneity of cognitive impairment and dementia in patients with Parkinson’s disease. Lancet Neurol. 9, 1200–1213. doi: 10.1016/S1474-4422(10)70212-X
Kehagia, A. A., Barker, R. A., and Robbins, T. W. (2013). Cognitive impairment in Parkinson’s disease: The dual syndrome hypothesis. Neurodegener. Dis. 11, 79–92. doi: 10.1159/000341998
Kelly, V. E., Eusterbrock, A. J., and Shumway-Cook, A. (2012). A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Parkinsons Dis. 2012:918719. doi: 10.1155/2012/918719
Kenangil, G., Orken, D. N., Ur, E., and Forta, H. (2010). Frontal assessment battery in patients with Parkinson disease in a Turkish population. Cogn. Behav. Neurol. 23, 26–28. doi: 10.1097/WNN.0b013e3181c5e2b0
Koerts, J., Tucha, L., Leenders, K. L., van Beilen, M., Brouwer, W. H., and Tucha, O. (2011). Subjective and objective assessment of executive functions in Parkinson’s disease. J. Neurol. Sci. 310, 172–175. doi: 10.1016/j.jns.2011.07.009
Koppelmans, V., Hoogendam, Y. Y., Hirsiger, S., Mérillat, S., Jäncke, L., and Seidler, R. D. (2017). Regional cerebellar volumetric correlates of manual motor and cognitive function. Brain Struct. Funct. 222, 1929–1944. doi: 10.1007/s00429-016-1317-7
Koziol, L. F., and Lutz, J. T. (2013). From movement to thought: The development of executive function. Appl. Neuropsychol. Child 2, 104–115. doi: 10.1080/21622965.2013.748386
Koziol, L. F., Budding, D. E., and Chidekel, D. (2012). From movement to thought: Executive function, embodied cognition, and the cerebellum. Cerebellum 11, 505–525. doi: 10.1007/s12311-011-0321-y
Kudlicka, A., Clare, L., and Hindle, J. V. (2011). Executive functions in Parkinson’s disease: Systematic review and meta-analysis. Mov. Disord. 26, 2305–2315. doi: 10.1002/mds.23868
La Marra, M., Messina, A., Ilardi, C. R., Verde, G., Amato, R., Esposito, N., et al. (2022d). The neglected factor in the relationship between executive functioning and obesity: The role of motor control. Healthcare 10:1775. doi: 10.3390/healthcare10091775
La Marra, M., Ilardi, C. R., Villano, I., Polito, R., Sibillo, M. R., Franchetti, M., et al. (2022b). Higher general executive functions predicts lower body mass index by mitigating avoidance behaviors. Front. Endocrinol. 13:1048363. doi: 10.3389/fendo.2022.1048363
La Marra, M., Ilardi, C. R., Villano, I., Carosella, M., Staiano, M., Iavarone, A., et al. (2022a). Functional relationship between inhibitory control, cognitive flexibility, psychomotor speed and obesity. Brain Sci. 12:1080. doi: 10.3390/brainsci12081080
La Marra, M., Villano, I., Ilardi, C. R., Carosella, M., Staiano, M., Iavarone, A., et al. (2022e). Executive functions in overweight and obese treatment-seeking patients: Cross-sectional data and longitudinal perspectives. Brain Sci. 12:777. doi: 10.3390/brainsci12060777
La Marra, M., Messina, A., Ilardi, C. R., Staiano, M., Di Maio, G., Messina, G., et al. (2022c). Factorial model of obese adolescents: The role of body image concerns and selective depersonalization—a pilot study. Int. J. Environ. Res. Public Health 19:11501. doi: 10.3390/ijerph191811501
Lang, S., Hanganu, A., Gan, L. S., Kibreab, M., Auclair-Ouellet, N., Alrazi, T., et al. (2019). Network basis of the dysexecutive and posterior cortical cognitive profiles in Parkinson’s disease. Mov. Disord. 34, 893–902. doi: 10.1002/mds.27674
Leh, S. E., Petrides, M., and Strafella, A. P. (2010). The neural circuitry of executive functions in healthy subjects and Parkinson’s disease. Neuropsychopharmacology 35, 70–85. doi: 10.1038/npp.2009.88
Lima, C. F., Meireles, L. P., Fonseca, R., Castro, S. L., and Garrett, C. (2008). The Frontal Assessment Battery (FAB) in Parkinson’s disease and correlations with formal measures of executive functioning. J. Neurol. 255, 1756–1761. doi: 10.1007/s00415-008-0024-6
Litvan, I., Goldman, J. G., Tröster, A. I., Schmand, B. A., Weintraub, D., Petersen, R. C., et al. (2012). Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement disorder society task force guidelines: PD-MCI diagnostic criteria. Mov. Disord. 27, 349–356. doi: 10.1002/mds.24893
Liu, X. (2012). Classification accuracy and cut point selection. Statist. Med. 31, 2676–2686. doi: 10.1002/sim.4509
Mack, J., and Marsh, L. (2017). Parkinson’s disease: Cognitive impairment. Focus 15, 42–54. doi: 10.1176/appi.focus.20160043
Maggi, G., Trojano, L., Barone, P., and Santangelo, G. (2021). Sleep disorders and cognitive dysfunctions in Parkinson’s disease: A meta-analytic study. Neuropsychol. Rev. 31, 643–682. doi: 10.1007/s11065-020-09473-1
Mandrekar, J. N. (2010). Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 5, 1315–1316. doi: 10.1097/JTO.0b013e3181ec173d
Margolesky, J., Betté, S., and Singer, C. (2020). Management of urologic and sexual dysfunction in Parkinson disease. Clin. Geriatr. Med. 36, 69–80. doi: 10.1016/j.cger.2019.09.011
Marras, C., Beck, J. C., Bower, J. H., Roberts, E., Ritz, B., Ross, G. W., et al. (2018). Prevalence of Parkinson’s disease across North America. NPJ Parkinsons Dis. 4:21. doi: 10.1038/s41531-018-0058-0
Matsui, H., Udaka, F., Miyoshi, T., Hara, N., Tamura, A., Oda, M., et al. (2006). Frontal assessment battery and brain perfusion image in Parkinson’s disease. J. Geriatr. Psychiatry Neurol. 19, 41–45. doi: 10.1177/0891988705284714
Miller, E. K., and Wallis, J. D. (2009). Executive function and higher-order cognition: Definition and neural substrates. Encyc. Neurosci. 4, 99–104. doi: 10.1016/B978-008045046-9.00418-6
National Collaborating Centre for Chronic Conditions (UK) (2006). Parkinson’s disease: National clinical guideline for diagnosis and management in primary and secondary care. London: Royal College of Physicians (UK).
O’Callaghan, C., and Lewis, S. J. G. (2017). Cognition in Parkinson’s disease. Int. Rev. Neurobiol. 133, 557–583. doi: 10.1016/bs.irn.2017.05.002
O’Callaghan, C., Bertoux, M., and Hornberger, M. (2014). Beyond and below the cortex: The contribution of striatal dysfunction to cognition and behaviour in neurodegeneration. J. Neurol. Neurosurg. Psychiatry 85, 371–378. doi: 10.1136/jnnp-2012-304558
Obuchowski, N. A. (2005). ROC analysis. Am. J. Roentgenol. 184, 364–372. doi: 10.2214/ajr.184.2.01840364
Owen, A. (1998). Abnormal basal ganglia outflow in Parkinson’s disease identified with PET. Implications for higher cortical functions. Brain 121, 949–965. doi: 10.1093/brain/121.5.949
Padovani, A., Costanzi, C., Gilberti, N., and Borroni, B. (2006). Parkinson’s disease and dementia. Neurol. Sci. 27, s40–s43. doi: 10.1007/s10072-006-0546-6
Pagonabarraga, J., and Kulisevsky, J. (2017). Apathy in Parkinson’s disease. Int. Rev. Neurobiol. 133, 657–678. doi: 10.1016/bs.irn.2017.05.025
Pagonabarraga, J., Kulisevsky, J., Strafella, A. P., and Krack, P. (2015). Apathy in Parkinson’s disease: Clinical features, neural substrates, diagnosis, and treatment. Lancet Neurol. 14, 518–531. doi: 10.1016/S1474-4422(15)00019-8
Poletti, M., Frosini, D., Pagni, C., Baldacci, F., Nicoletti, V., Tognoni, G., et al. (2012). Mild cognitive impairment and cognitive-motor relationships in newly diagnosed drug-naive patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 83, 601–606. doi: 10.1136/jnnp-2011-301874
Polito, R., Francavilla, V. C., Ambrosi, A., Tartaglia, N., Tafuri, D., Monda, M., et al. (2020a). The Orexin-A serum levels are strongly modulated by physical activity intervention in diabetes mellitus patients. J. Hum. Sport Exerc. 15, S244–S251. doi: 10.14198/jhse.2020.15.Proc2.15
Polito, R., Scarinci, A., Ambrosi, A., Tartaglia, N., Tafuri, D., Monda, M., et al. (2020b). The beneficial effects of physical activity and weight loss on human colorectal carcinoma cell lines. J. Human Sport Exerc. 15, S252–S260. doi: 10.14198/jhse.2020.15.Proc2.16
Postuma, R. B., Berg, D., Stern, M., Poewe, W., Olanow, C. W., Oertel, W., et al. (2015). MDS clinical diagnostic criteria for Parkinson’s disease: MDS-PD clinical diagnostic criteria. Mov. Disord. 30, 1591–1601. doi: 10.1002/mds.26424
Pringsheim, T., Jette, N., Frolkis, A., and Steeves, T. D. L. (2014). The prevalence of Parkinson’s disease: A systematic review and meta-analysis: PD prevalence. Mov. Disord. 29, 1583–1590. doi: 10.1002/mds.25945
Raffegeau, T. E., Krehbiel, L. M., Kang, N., Thijs, F. J., Altmann, L. J. P., Cauraugh, J. H., et al. (2019). A meta-analysis: Parkinson’s disease and dual-task walking. Parkinsonism Relat. Disord. 62, 28–35. doi: 10.1016/j.parkreldis.2018.12.012
Ray, S., and Agarwal, P. (2020). Depression and anxiety in Parkinson disease. Clin. Geriatr. Med. 36, 93–104. doi: 10.1016/j.cger.2019.09.012
Raz, N. (1997). Selective aging of the human cerebral cortex observed in vivo: Differential vulnerability of the prefrontal gray matter. Cereb. Cortex 7, 268–282. doi: 10.1093/cercor/7.3.268
Reekes, T. H., Higginson, C. I., Ledbetter, C. R., Sathivadivel, N., Zweig, R. M., and Disbrow, E. A. (2020). Sex specific cognitive differences in Parkinson disease. NPJ Parkinsons Dis. 6:7. doi: 10.1038/s41531-020-0109-1
Reijnders, J. S. A. M., Ehrt, U., Weber, W. E. J., Aarsland, D., and Leentjens, A. F. G. (2008). A systematic review of prevalence studies of depression in Parkinson’s disease: The Prevalence of Depression in PD. Mov. Disord. 23, 183–189. doi: 10.1002/mds.21803
Richard, I., Schiffer, R., and Kurlan, R. (1996). Anxiety and Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 8, 383–392. doi: 10.1176/jnp.8.4.383
Rodriguez-Oroz, M. C., Jahanshahi, M., Krack, P., Litvan, I., Macias, R., Bezard, E., et al. (2009). Initial clinical manifestations of Parkinson’s disease: Features and pathophysiological mechanisms. Lancet Neurol. 8, 1128–1139. doi: 10.1016/S1474-4422(09)70293-5
Rycroft, S. S., Quach, L. T., Ward, R. E., Pedersen, M. M., Grande, L., and Bean, J. F. (2019). The relationship between cognitive impairment and upper extremity function in older primary care patients. J. Gerontol. Series A 74, 568–574. doi: 10.1093/gerona/gly246
Schrag, A. (2006). Quality of life and depression in Parkinson’s disease. J. Neurol. Sci. 248, 151–157. doi: 10.1016/j.jns.2006.05.030
Siciliano, M., Trojano, L., Santangelo, G., De Micco, R., Tedeschi, G., and Tessitore, A. (2018). Fatigue in Parkinson’s disease: A systematic review and meta-analysis: Fatigue in Parkinson’s Disease. Mov. Disord. 33, 1712–1723. doi: 10.1002/mds.27461
Simon, D. K., Tanner, C. M., and Brundin, P. (2020). Parkinson disease epidemiology, pathology, genetics, and pathophysiology. Clin. Geriatr. Med. 36, 1–12. doi: 10.1016/j.cger.2019.08.002
Stamelou, M., Diehl-Schmid, J., Hapfelmeier, A., Kontaxopoulou, D., Stefanis, L., Oertel, W. H., et al. (2015). The frontal assessment battery is not useful to discriminate progressive supranuclear palsy from frontotemporal dementias. Parkinsonism Relat. Disord. 21, 1264–1268. doi: 10.1016/j.parkreldis.2015.08.006
Stuss, D. T. (2011). Functions of the frontal lobes: Relation to executive functions. J. Int. Neuropsychol. Soc. 17, 759–765. doi: 10.1017/S1355617711000695
Tanner, C. M., and Goldman, S. M. (1996). Epidemiology of Parkinson’s disease. Neurol. Clin. 14, 317–335. doi: 10.1016/S0733-8619(05)70259-0
Tekin, S., and Cummings, J. L. (2002). Frontal–subcortical neuronal circuits and clinical neuropsychiatry. J. Psychosom. Res. 53, 647–654. doi: 10.1016/S0022-3999(02)00428-2
Twelves, D., Perkins, K. S. M., and Counsell, C. (2003). Systematic review of incidence studies of Parkinson’s disease. Mov. Disord. 18, 19–31. doi: 10.1002/mds.10305
Tysnes, O.-B., and Storstein, A. (2017). Epidemiology of Parkinson’s disease. J. Neural Transm. 124, 901–905. doi: 10.1007/s00702-017-1686-y
Unal, I. (2017). Defining an optimal cut-point value in ROC analysis: An alternative approach. Comput. Math. Methods Med. 2017:3762651. doi: 10.1155/2017/3762651
Villano, I., Ilardi, C. R., Arena, S., Scuotto, C., Gleijeses, M. G., Messina, G., et al. (2021). Obese subjects without eating disorders experience binge episodes also independently of emotional eating and personality traits among university students of Southern Italy. Brain Sci. 11:1145. doi: 10.3390/brainsci11091145
Watson, G. S., and Leverenz, J. B. (2010). Profile of cognitive impairment in Parkinson’s disease. Brain Pathol. 20, 640–645. doi: 10.1111/j.1750-3639.2010.00373.x
Yanagisawa, N., Fujimoto, S., and Tamaru, F. (1989). Bradykinesia in Parkinson’s disease: Disorders of onset and execution of fast movement. Eur. Neurol. 29, 19–28. doi: 10.1159/000116449
Yang, Y., Tang, B., and Guo, J. (2016). Parkinson’s disease and cognitive impairment. Parkinsons Dis. 2016, 1–8. doi: 10.1155/2016/6734678
Yeo, L., Singh, R., Gundeti, M., Barua, J. M., and Masood, J. (2012). Urinary tract dysfunction in Parkinson’s disease: A review. Int. Urol. Nephrol. 44, 415–424. doi: 10.1007/s11255-011-9969-y
Yu, R., Liu, B., Wang, L., Chen, J., and Liu, X. (2013). Enhanced functional connectivity between putamen and supplementary motor area in Parkinson’s disease patients. PLoS One 8:e59717. doi: 10.1371/journal.pone.0059717
Zgaljardic, D. J., Borod, J. C., Foldi, N. S., and Mattis, P. (2003). A review of the cognitive and behavioral sequelae of Parkinson’s disease: Relationship to frontostriatal circuitry. Cogn. Behav. Neurol. 16, 193–210. doi: 10.1097/00146965-200312000-00001
Keywords: Parkinson’s disease, executive functions, frontal assessment battery-15, diagnosis, motor symptoms
Citation: Ilardi CR, di Maio G, Villano I, Messina G, Monda V, Messina A, Porro C, Panaro MA, Gamboz N, Iavarone A and La Marra M (2023) The assessment of executive functions to test the integrity of the nigrostriatal network: A pilot study. Front. Psychol. 14:1121251. doi: 10.3389/fpsyg.2023.1121251
Received: 17 January 2023; Accepted: 13 March 2023;
Published: 29 March 2023.
Edited by:
Martina Amanzio, University of Turin, ItalyReviewed by:
Fabio Giovannelli, University of Florence, ItalyCopyright © 2023 Ilardi, di Maio, Villano, Messina, Monda, Messina, Porro, Panaro, Gamboz, Iavarone and La Marra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ines Villano, aW5lcy52aWxsYW5vQHVuaWNhbXBhbmlhLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.