 Lorena Cudris-Torres1*†
Lorena Cudris-Torres1*† Stefano Vinaccia Alpi2†
Stefano Vinaccia Alpi2† Álvaro Barrios-Núñez3†
Álvaro Barrios-Núñez3† Natali Gaviria Arrieta4†
Natali Gaviria Arrieta4† Jéssica Mejía Gutiérrez1†
Jéssica Mejía Gutiérrez1† Libia Alvis Barranco4†
Libia Alvis Barranco4† Gerson Rios-Carlys4†
Gerson Rios-Carlys4† Silvia E. Cuenca-Calderón1†
Silvia E. Cuenca-Calderón1† Valmore Bermúdez5†
Valmore Bermúdez5† Juan Hernández-Lalinde6†
Juan Hernández-Lalinde6† Carlos Arturo Riveira Zuleta4†
Carlos Arturo Riveira Zuleta4† Marly Johana Bahamón7†
Marly Johana Bahamón7† Juany Sofía Álvarez Herrera3†
Juany Sofía Álvarez Herrera3†- 1Programa de Psicología, Fundación Universitaria del Área Andina, Valledupar, Colombia
- 2Facultad de Ciencias de la Salud, Universidad del Sinú, Montería, Colombia
- 3Clínica General del Norte, Barranquilla, Colombia
- 4Programa de Psicología, Universidad Popular del Cesar, Valledupar, Colombia
- 5Centro de Investigaciones en Ciencias de la Vida, Universidad Simón Bolívar, Barranquilla, Colombia
- 6Universidad Simón Bolívar, Cúcuta, Colombia
- 7Universidad del Sinú, Montería, Colombia
The purpose of the present study was to establish the association between self-efficacy, perception of disease, emotional regulation, and fatigue and the health-related quality of life in older adults living in the departments of Cesar and Atlántico in Colombia and who have been diagnosed with a chronic disease. The participants were 325 older adults of both sexes, with literacy and no presence of cognitive impairment in the Mini-Mental State Examination (MMSE); A non-probabilistic sampling was carried out. We used the MOS-SF-36 questionnaire, the Brief Illness Perception Questionnaire scale for measuring the perception of disease, the Stanford Patient Education Research Center’s Chronic Disease Self self-efficacy questionnaire for chronic patients, the Difficulties in Emotional Regulation Scale, and the Fatigue Severity Questionnaire as measurement instruments. The design was non-experimental cross-sectional with a correlational scope. The results indicate that self-efficacy, disease perception, emotional regulation and severity of fatigue are variables that could impact the physical function of quality of life, confirming that self-efficacy would work as a factor that decreases the probability that a participant score low on this dimension of quality of life. On the other hand, both the perception of the disease and the severity of fatigue were identified as factors that probably negatively influence quality of life.
1. Introduction
Over the past 200 years, average human life expectancy has doubled in most developed and developing countries. Better water quality, nutrition, hygiene, housing, immunization against infectious diseases, antibiotics, and improved medical care reduced mortality for those in the early years of life and then after about 1950, among people in their 70s (Partridge et al., 2018; Mitchell and Walker, 2020). However, the increased longevity and owing to lifestyle changes may have led to a significant increase in the prevalence of noncommunicable diseases (NCDs), also known as chronic diseases—which are medical conditions associated with long duration and slow progression—in the human population. NCDs are non-infectious and are the result of interaction of several factors, including genetic, physiological, behavioral, social, and environmental factors (Martinengo et al., 2019). According to the World Health Organization (2013), NCDs are the leading cause of death worldwide, accounting for 71% of the total number of deaths per year.
The four leading causes of death among NCDs with the highest number of deaths are cardiovascular diseases (17.9 million deaths annually), cancer (9.0 million), respiratory diseases (3.9 million), and diabetes (1.6 million) (World Health Organization, 2019, 2020). Many individuals with chronic diseases do not know how to cope with their disease. They have enormous difficulties in understanding its causes and do not know how to monitor it, i.e., they do not know how the disease should be managed. This leads to deterioration of their well-being and quality of life and emerging negative emotions including anxiety, depression, hopelessness, and stress. This results in inadequate monitoring of their disease and as a consequence over time, to the appearance of episodes of learned hopelessness (Bica et al., 2017). On the contrary, positive self-management of the disease can be associated with self-efficacy which can be defined as an individual’s belief of their ability to control adverse events that may influence their life (Dunke Pereira et al., 2018).
Self-efficacy plays an important role in determining whether actions of self-care are initiated, how much effort is expended, and how long the effort is sustained in the presence of obstacles and failures (Bandura and Freeman, 1997). Patients that have a high level of self-efficacy when faced with their chronic diseases show a perceived ability to cope with the challenges related to their diseases and a sense of control over their lives (Bandura and Freeman, 1997; Cheng et al., 2019; Chan, 2021). In this regard, empirical studies have been developed in the last 20 years based on the favorable influence of self-efficacy in the management of chronic diseases. The diseases include chronic obstructive pulmonary disease (Kar and Zengin, 2020; Selzler et al., 2020; Paneri and Napolitano, 2021; Yi et al., 2021), chronic renal failure (Brioni et al., 2021), chronic diseases in general (Almutary and Tayyib, 2020; Farley, 2020; Yuan et al., 2021), and stroke (Bailey, 2019).
However, in recent years a number of studies have focused on understanding how relevant the mental representation of the disease is in the patient’s perception of the disease. For example, owing to negative emotions, patients perceive that the duration of the disease is much longer and the consequences to be more severe while greater personal and treatment control corresponds to a less severe perception of the consequences of the disease. This is observed in chronic diseases in general (Özkan Tuncay et al., 2018; Cheng et al., 2020; Giuffrida et al., 2021; Szabó-Bartha and Mirnics, 2021) and cases of chronic renal failure (Dantas et al., 2020), multiple sclerosis (Timkova et al., 2021), hepatitis B and C (Ekmen et al., 2021), leukemia (Arrato et al., 2022), and systemic lupus erythematosus (Elefante et al., 2020).
Similarly, some studies refer to the role that fatigue plays in the perception of well-being and quality of life of the chronically ill patients. Fatigue can be defined as the subjective feeling of a lack of physical and mental energy, perceived by a person, which interferes with daily activities (Gregg et al., 2021). Fatigue is a disabling symptom, which often covaries with depressive symptoms, anxiety, and sleep impairment and it is associated with a poor state of subjective health perception and a low level of quality of life (Adamowicz et al., 2022). The studies include those on chronic disease in general (Menting et al., 2018; Torossian and Jacelon, 2021), irritable colon (Nocerino et al., 2020), and renal failure (Swain and Jones, 2020; Gregg et al., 2021); similarly, numerous studies have referred to the impact of different chronic diseases on health-related quality of life (HRQOL).
HRQOL is a multidimensional construct consisting of at least three broad domains (physical, psychological, and social functioning) that are affected by the disease itself and/or its treatment. The associated conditions include chronic low back pain (Járomi et al., 2021), chronic venous insufficiency (Silva et al., 2021), systemic lupus erythematosus (Elefante et al., 2020), renal transplantation (Sawada et al., 2021), globus pharyngeus (Zhang and Liu, 2021), Lyme disease (Hill and Frost, 2022), and chronic respiratory failure (Oga et al., 2018).
Similarly, emotional regulation, i.e., experiencing, processing, and modulating emotional responses, is necessary to manage common emotional stressors in patients with chronic disease. Overwhelming emotional demands deplete the resources needed for the daily management of chronic disease self-care and they contribute to poor health outcomes (Wierenga et al., 2017, 2018; Zarotti et al., 2018; Della Vecchia et al., 2019). Pertinent studies in the past have focused on cases of cardiovascular disease (Roy et al., 2018; Luque et al., 2020) and chronic disease in general (Bramanti et al., 2021).
In spite of the epidemiological projections on the high prevalence of chronic diseases in Colombia (Gallardo-Solarte et al., 2016) and considering the impact of self-efficacy, disease perception, self-regulation, and fatigue on HRQOL, several studies have focused on this subject worldwide. In addition, there is a paucity of empirical studies in Colombia from the field of health (Ardila, 2018). Therefore, the aim of this study was to analyze and compare the relationship that self-efficacy, illness perception, self-regulation, fatigue, and socio-demographic and clinical characteristics have on HRQOL in Colombian patients with chronic diseases.
2. Materials and methods
2.1. Design
This is a quantitative non-experimental, cross-sectional research with a correlational scope and a survey-type data collection model (Hernández et al., 2014).
2.2. Participants
Non-random sample of 325 older adults with a medical diagnosis of a chronic disease of at least 1 year with a mean age and standard deviation of 68.39 and 4.15 years (CV = 6.07%), respectively. Residents of the departments of Cesar and Atlántico, participating voluntarily and provided informed consent. Subjects had no cognitive impairment (Mini-mental State Examination [MMSE] scores of >23) and had reading and writing ability so that they could understand the tests.
The conditions of the population of interest made it impossible to obtain a sampling frame, forcing the researchers to select the participants through a non-probabilistic convenience sampling. Given this situation, the sample size was determined based on the maximum number of participants that could be selected within the limitations of the research.
Therefore, the study included 390 participants, of whom 65 presented cognitive impairment in the application of the Mini-Mental State Examination (MMSE), this being an exclusion criterion; The final response rate was 83.33%.
2.3. Instruments
The mini-mental scale is a brief psychometric scale to evaluate the cognitive state of people and the Colombian version of this scale has been introduced by Rosselli et al. (2000). This scale was introduced into clinical practice as a practical method to assess the cognitive status of their patients. This instrument is composed of 30 dichotomous items that evaluate six cognitive processes: temporal orientation, spatial orientation, fixation memory, recall memory, attention and calculation, and language; the internal consistency is adequate (Cronbach’s alpha: 0.807).
The Fatigue Intensity scale (FSS) consists of nine items with a Likert-type response of seven possibilities of increasing intensity and scores between 1 and 7. The total is the sum of all the items. The Colombian version of Riveros Munévar et al. (2017) was used for this study.
The Colombian version of the Difficulties in Emotion Regulation Scale (DERS) was prepared by Muñoz-Martínez et al. (2006). This measures emotional dysregulation and consists of 36 items grouped into six factors as follows: (a) non-acceptance of emotional responses (non-acceptance), (b) difficulties in goal-directed behaviors when upset (goals), (c) difficulties in controlling impulsive behaviors when upset (impulsivity), (d) limited access to emotional regulation strategies that are perceived as effective (strategies), (e) lack of emotional awareness (awareness), and (f) lack of emotional clarity (clarity). The analysis of the DERS applied in a sample of Colombians revealed an internal consistency α = 0.90.
The Stanford Patient Education Research Center’s Chronic Disease Self-Efficacy (SEMCD-S) was developed by Ritter and Lorig (2014). This consists of four items on a scale of 1–10, with 1 being “Very Insecure” and 10 being “Very Confident.” This is an instrument for measuring the self-efficacy related to chronic disease management. Research reports a reliability of 0.95 (22) and for this research a Cronbach’s alpha of α = 0.791 was obtained.
MOS SF-36 Health Questionnaire was validated in Colombia by Lugo et al. (2006). This questionnaire consists of 36 items that explore eight dimensions of health status corresponding to physical function, social function, role limitations: physical problems, emotional problems, mental health, vitality, pain, and perception of general health. The reliability of the MOSSF-36 Health Questionnaire is 0.7; the physical role, physical function, and emotional role measurements obtained reliability scores equal to 0.90; in terms of content validity they had high correlations with the physical component (r ≥ 0.74).
Brief Illness Perception Questionnaire (Brief Illness Perception Questionnaire [IPQ-B]). In the Spanish version of Pacheco-Huergo et al. (2012), this questionnaire consists of nine items with Likert-type responses ranging from 0 to 10 points. It comprises eight dimensions and an ordinal open-ended question with three possible answers. These dimensions are as follows: consequences, duration, personal management, treatment management, identity, worry, emotional response and understanding of the disease. Item number 9 is an open-ended question in reference to the factors that caused his or her disease according to the person and organized accordingly of their importance. The questionnaire has adequate internal consistency indices ranging from α = 0.67–0.89.
2.4. Procedure
Before starting the field phase of the research, which included the instrument application, 16 adults aged >60 years were selected and they underwent a pilot test to identify the words or questions that were difficult to understand to identify the respective comprehension in the response system and to establish the time for each of the instruments. At the end of this process, there was clarity and understanding on the part of the participants of the pilot test.
A total of 325 older adults were selected from the departments of Cesar and Atlántico based on the fact that they were older than 60 years, met the characteristics of having a diagnosis of a chronic disease, and voluntarily decided to participate.
At the outset, a brief explanation of the research was performed, explaining the objectives and procedures to be performed. After this, informed consents were signed, so that there was a written agreement with the participants to authorize their voluntary participation; This was followed by the scaling of sociodemographic data in order to find out the characteristics of the population and with these data, the MMSE was applied, which helped to rule out the subjects who presented cognitive impairment, ruling out cognitive impairment in the participants, this was followed by applying the instruments in the following order (FSS, DERS, SEMCD-S, MOS SF-36 and IPQ-B), the whole process lasted approximately 2 h per participant. The data obtained were incorporated into a database and analyzed using the SPSS-27 statistical package.
2.5. Analysis plan
Firstly, an exploratory data analysis (EDA) was conducted in order to evaluate compliance with the assumptions needed to perform parametric tests, as well as to assess whether the use of multiple linear regression (MLR) was an appropriate option. In this regard, the normality of the variables was tested by means of the Shapiro–Wilk (SW) test, also opting for the construction of Q-Q plots as a complementary tool. Equality of variances was examined using Levene’s test, considering each of the sociodemographic characteristics as grouping factors. Independence of observations was inspected at statistical level using the median-based Wald-Wolfowitz cluster test, while the MLR conditions were validated by means of a thorough analysis of the residuals of each model.
In this regard, SW contrast was used again to check whether the residuals conformed to a normal distribution, while homoscedasticity was inspected graphically and analytically through typed scatter plots and by means of the Breusch–Pagan (BP) and White procedures. The residual autocorrelation assumption was evaluated with the Durbin-Watson (DW) statistic, while the presence of multicollinearity was checked using the variance inflation factors (VIF) and the condition index (CI). After this preliminary phase, it was concluded that nonparametric tests and regression options involving less demanding statistical assumptions should be used due to the violation of the aforementioned assumptions.
Once these conjectures were discarded, the research variables were described using basic summary measures. The raw or transformed scores were characterized through the minimum, maximum, range, interquartile range, mean, median, mode, variance, standard deviation, coefficient of variation, lower quartile, and upper quartile.
Furthermore, the sociodemographic characteristics compiled in the study, most of which were attribute variables, were presented in the form of absolute and relative frequencies. To compare the effect of these factors on the variables of interest, the Mann–Whitney U test (MWU) was selected when these characteristics consisted of two groups, choosing the Kruskal–Wallis H test (KWH) when, on the contrary, the number of levels was greater than or equal to three. On this occasion, the post hoc contrasts were conducted with the MWU method; however, the outcomes were corrected for significance via Bonferroni correction.
The dependent variables of the binary logistic regression (BLR) models were set from each of the eight dimensions of quality of life and used as predictors of the scores of the global constructs of self-efficacy, perception of disease, emotional regulation, and fatigue severity. The study was advanced in this way and each dimension was not incorporated as a regressor owing to the multicollinearity found between the factors of each scale, which had a negative impact on the VIF and the CI, increasing their values considerably.
In addition to the abovementioned statistical argument, there are numerous empirical and theoretical evidences to justify the use of global constructs of these instruments for description, classification, and prediction purposes. However, the categorization of the DVs was obtained by defining those scores below the lower quartile and above the upper quartile as low and high levels, which enabled the dichotomous characteristics necessary for the use of the BLR to be obtained. In addition, age, sex, time of disease diagnosis and the patient’s circumstances with respect to whether he/she lives alone or accompanied were introduced to the regression models to obtain adjusted estimates and odds ratios that truly reflected the magnitude of the association between the variables. Linearity between the predictors of the BLR and the logarithm of the odds ratio was checked through the Box-Tidwell procedure without finding relevant inconsistencies, while the existence of outliers and influence points was inspected by means of residuals, Cook’s and Mahalanobis distances. The presence of certain anomalies or influence data was moderate and did not impact the estimates.
Finally, data processing and analysis were performed with the IBM SPSS statistical package (version 27 for Windows 64-bit). Results whose significance was less than 0.05, 0.01 or 0.001 were considered significant.
3. Results
3.1. Sociodemographic characteristics of the participants
The sample consisted of 325 people, of which 46.46% (n = 151) were female and 53.54% (n = 174) were male. Their age ranged from 60 to 78 years, with a mean of 68.39 and standard deviation of 4.15 (CV = 6.07%). In terms of time since disease diagnosis, values ranged from 5 to 60 years, with a mean of 15.79 and variability of 6.96 (CV = 44.08%). Other participant characteristics, such as the municipality of residence, marital status, whether living alone or accompanied, education, socioeconomic status, health system, psychiatric medication intake and treatment for their chronic condition are shown in Table 1.
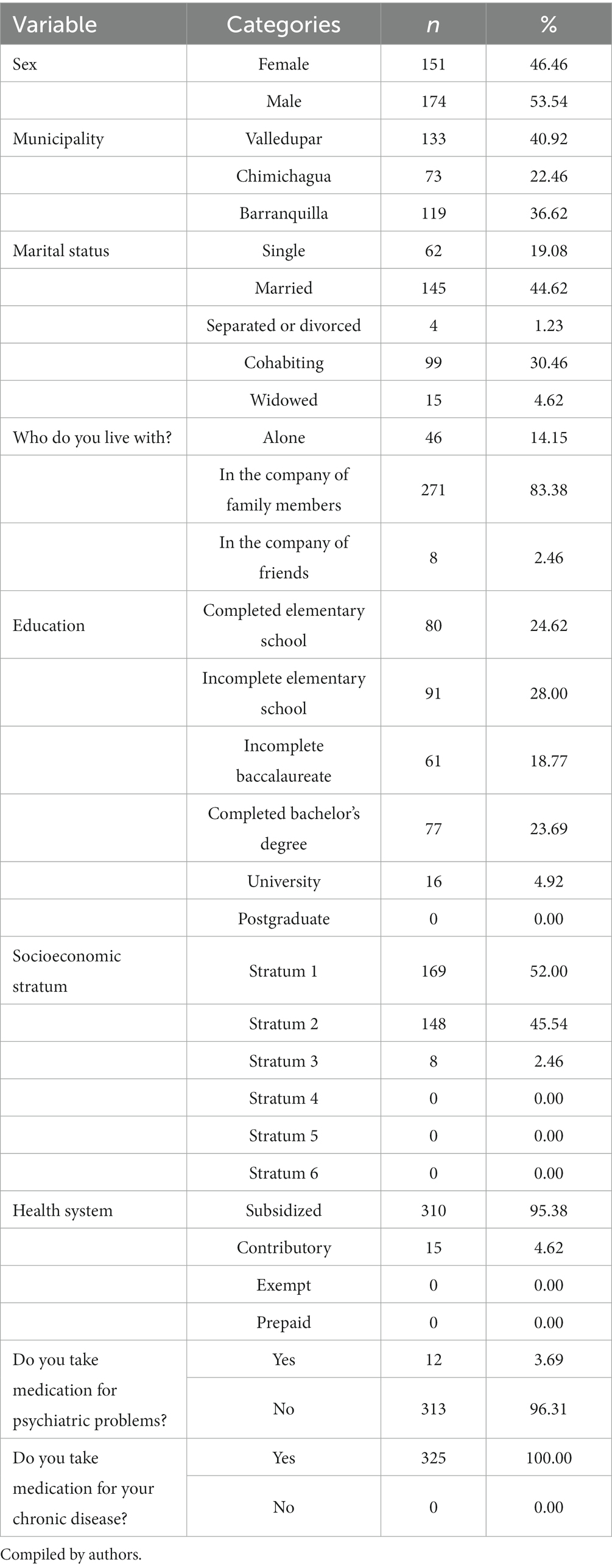
Table1. Sociodemographic characteristics of the participants.
Quality of life, self-efficacy, illness perception, emotional regulation, and fatigue.
The physical function of quality of life will be used as an example to develop this section. As can be seen in Table 2, it was found that the scores in this dimension ranged from 20 to 80 points, involving a range of 60 points. The lower and upper quartiles were 30 and 70, respectively, thus obtaining an interquartile range of 40 points. Regarding the centralization measurements, the scores averaged 49.91 points, with a median of 50 and a mode of 30. Variability was observed around the mean of 21.42 points, thus reflecting a relatively high coefficient of variation of 42.92%. For practicality, the characterization of the rest of the variables is omitted and the reader is referred to the detailed information shown in Table 2.
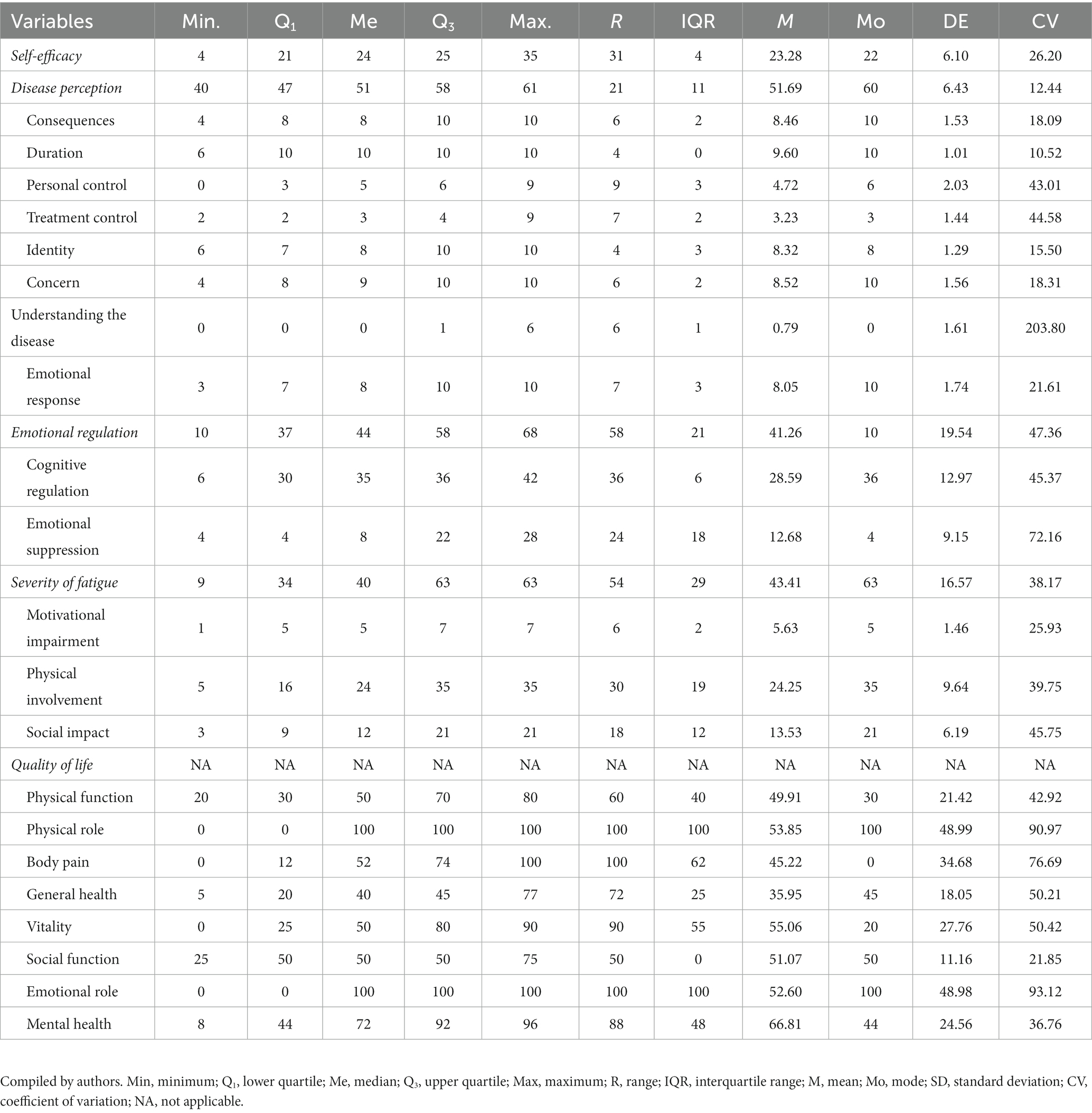
Table 2. Raw or transformed scores of the variables analyzed in the research.
3.2. Comparison by sociodemographic characteristics
Tables 3–5 show the results of assessing the effect of the sociodemographic characteristics on the variables of interest for the study. It is emphasized at this point what was clarified in the statistical analysis section: nonparametric tests were used as a consequence of the non-observance of the postulates under which these tests operate. Thus, the data contrasted in these tables respond to the average assigned ranges, this is a typical transformation applied in these tests and is used to carry out the procedure. Therefore, special care must be taken when interpreting these values since they do not correspond to the raw scores.
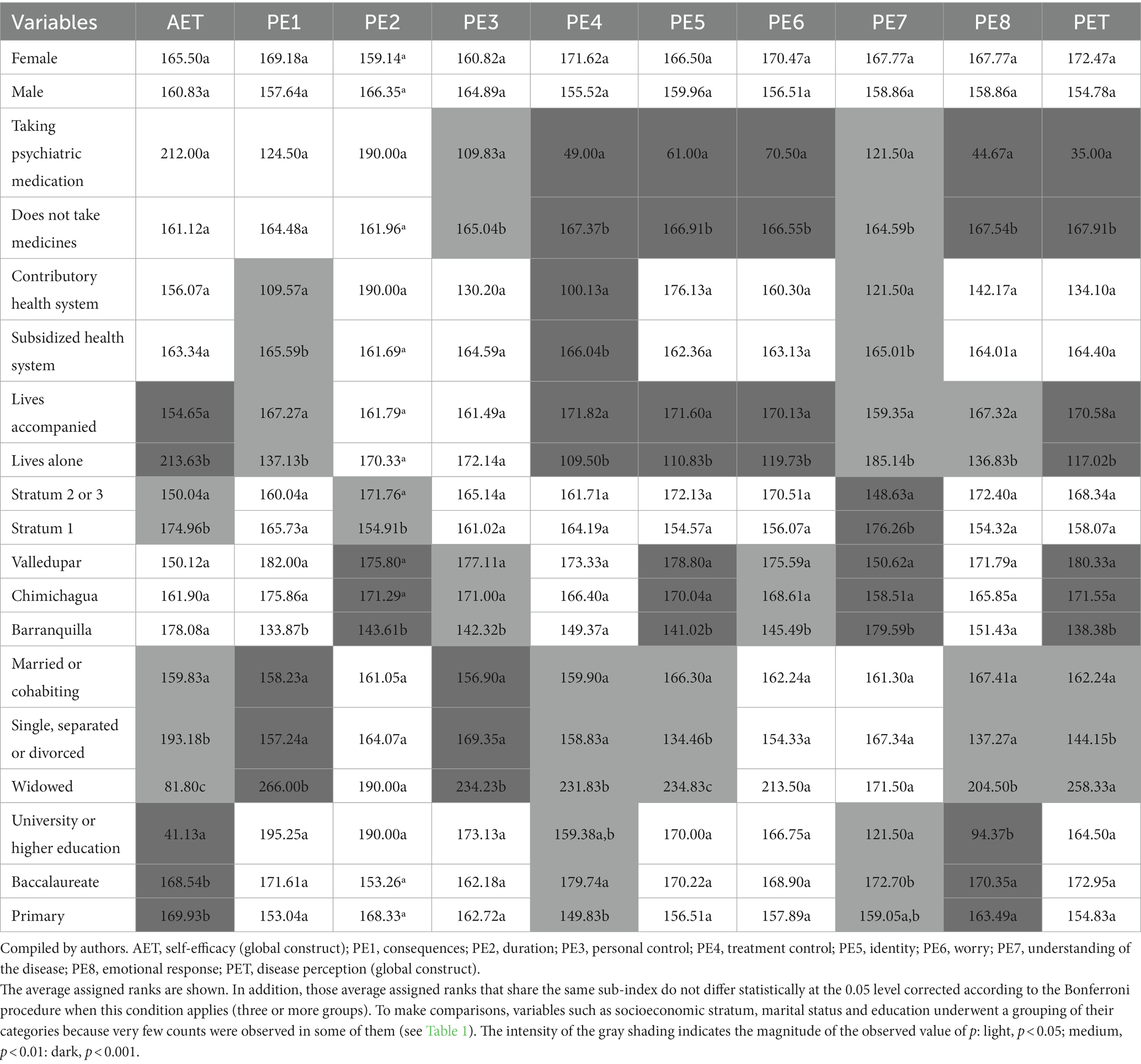
Table 3. Self-efficacy and perception of disease according to sociodemographic characteristics.
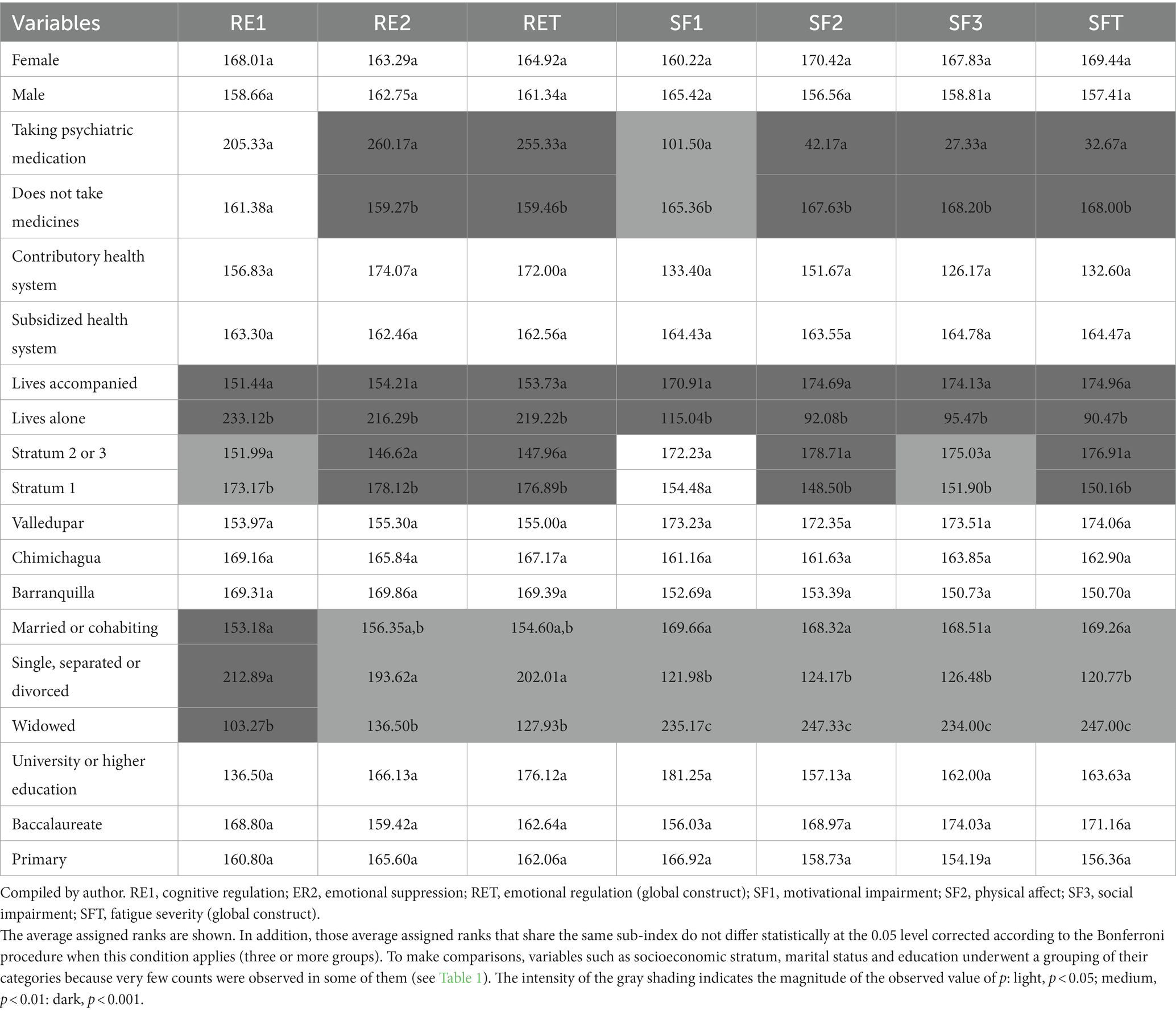
Table 4. Emotional regulation and fatigue severity according to sociodemographic characteristics.
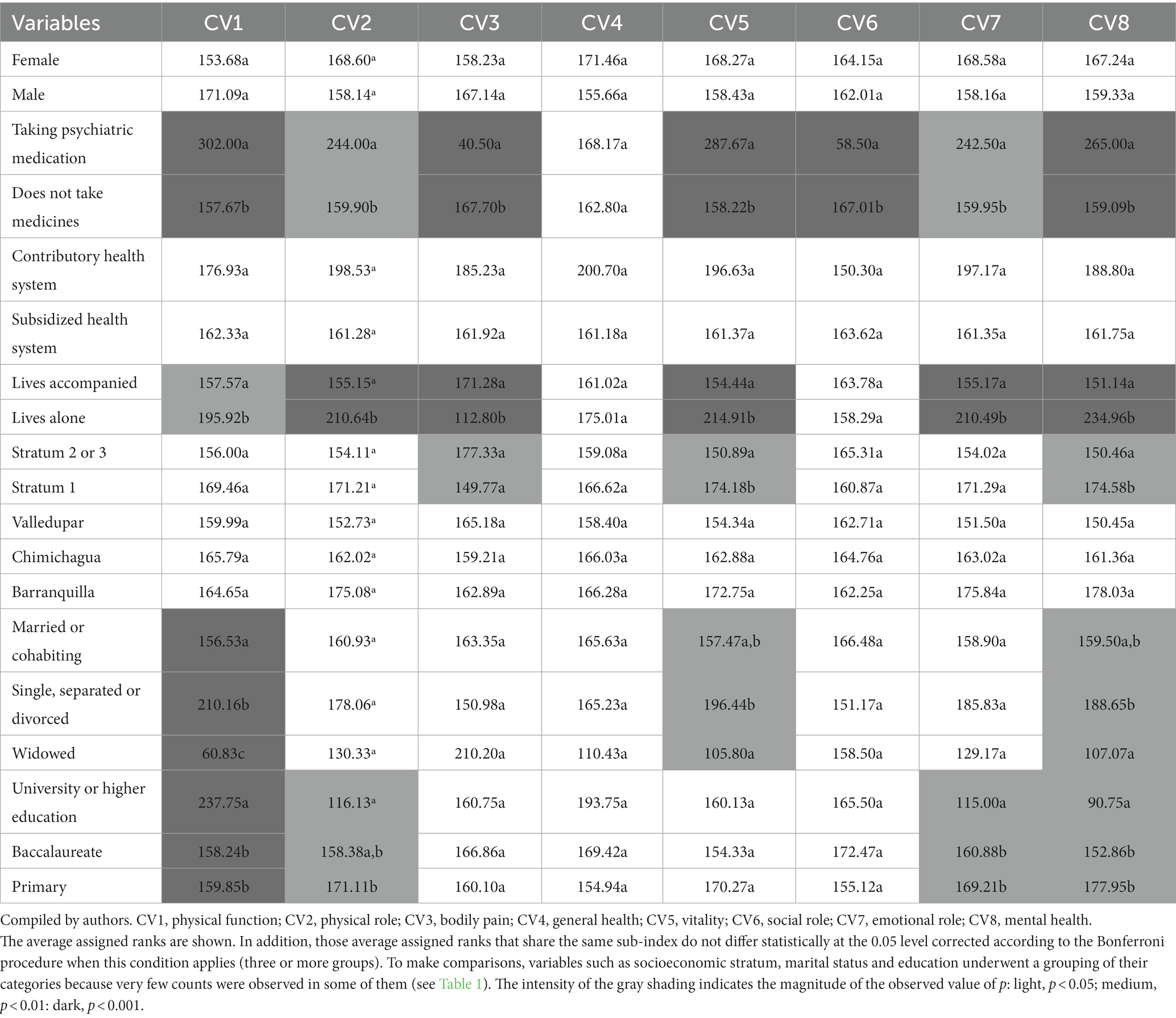
Table 5. Quality of life according to sociodemographic characteristics.
Having said this and taking as a reference whether the patient takes psychiatric medication to cope with his or her condition, it was observed that this factor had an effect on the scores of the “personal control” dimension of the disease perception scale. It is noted that those not taking these medications reported higher assigned ranges than those who do (165.04 vs. 109.83, p < 0.05), which could be interpreted as meaning that the perception of disease is higher among those subjects who do not have the benefit of this palliative. When analyzing the health system and its influence, it can be seen that the participants belonging to the contributory system exhibit lower ratings in the “consequences” aspect of this questionnaire than those in the subsidized regime (109.57 vs. 165.59, p < 0.05), implying that the repercussions of the disease are conceived to be less serious among these individuals. However, it is important to emphasize that previous results should be interpreted cautiously because the sample size in one group is small and very different from that in the other group. As such, the validity of these findings may be questionable.
Regarding the severity of fatigue, it is noted that those using psychiatric medication reached significantly lower figures than those not doing so, this was observed in the dimensions of motivational affectation (101.50 vs. 165.36, p < 0.01), physical (92.08 vs. 174.69, p < 0.001), social (95.47 vs. 174.13, p < 0.001) and in the questionnaire total (90.47 vs. 174.96, p < 0.001).
As regards quality of life, it was found that marital status had a significant effect on the patients’ assessment of this construct. Specifically, widowers reported much lower ratings in the aspect of this variable defined as “physical function” than those who were single, separated or divorced (60.83 vs. 210.16, p < 0.001), but also than those who were married or cohabiting (60.83 vs. 156.53, p < 0.001). In turn, participants cohabiting with their partner reflected lower assigned ranks than those who were separated or single (156.53 vs. 210.16, p < 0.001). A similar situation was observed in vitality and mental health, both subscales of the MOS SF-36 instrument that measures health-related quality of life.
In an effort to avoid an excessive description of the results of this phase, the reader is encouraged to continue with this analysis by carefully reviewing the findings shown in Tables 3–5. In this regard, it should be noted that the APA methodology has been used for identifying whether two or more assigned ranges differ statistically, a procedure that involves assigning different letters as subscripts (a, b, c, etc.,). Furthermore, we have chosen to facilitate the visualization of the table by shading in gray those comparisons that were found to be significant, increasing the intensity of the shading as this property increases. Specifically: if highlighted in light gray, the value of p obtained is less than 0.05; if in medium gray, the significance observed is less than 0.01; and if in dark gray, the difference is statistically significant for values less than 0.001.
3.3. Association between quality of life, self-efficacy, disease perception, regulation, and fatigue
As noted in the statistical analysis section, when establishing the association between the aspects of quality of life (DV: dependent variables) and self-efficacy, disease perception, emotional regulation, and fatigue severity (IV: independent variables), BLR models were used. DVs were categorized from the lower and upper quartiles, while IVs were entered unmodified, in their raw or direct form. To obtain adjusted odds ratios (OR), covariates such as sex, age, disease duration and the patient’s living situation were incorporated into each model. The fit was assessed with Cox-Snell and Nagelkerke coefficients (pseudo R2), while the precision of the estimates was identified by displaying the bilateral confidence interval of the ORs together with their level of significance. All BLR assumptions were tested without any major irregularities or deviations being discovered.
Thus, the results indicate that self-efficacy, disease perception, emotional regulation, and severity of fatigue are variables that could impact physical function and quality of life. Note that each of these regressors reflected statistically significant odds ratios. Specifically, the perception of the disease and the severity of fatigue were identified as factors that probably negatively influence quality of life. It is noted that, if all other factors are held constant, for each point that self-efficacy increases, the probability of this happening is reduced by approximately 12% (OR = 0.88, p = 0.002, 0.81–0.95), a fact also observed under similar conditions, although less marked, in emotional regulation. In this case, if the other variables are not modified, a unit increase in this construct implies a 3% decrease (OR = 0.97, p = 0.027, 0.95–0.99) in the possibility of obtaining low levels of physical function. Conversely, both disease perception and fatigue severity were identified as risk variables. Regarding the former, one-point increases would lead to a 22% increase (OR = 1.22, p < 0.001, 1.11–1.34) in the probability of achieving low ratings in physical function; while, regarding the latter, unit increases in the fatigue severity scale would generate an increase in this risk of 13% (OR = 1.13, p < 0.001, 1.08–1.18). Judging from the pseudo R2s, about 57 to 77% of the variation in physical function would be explained by the model. To understand all the findings of this stage of the research, let us perform a similar description as in the previous paragraph with the rest of the models shown in Table 6.
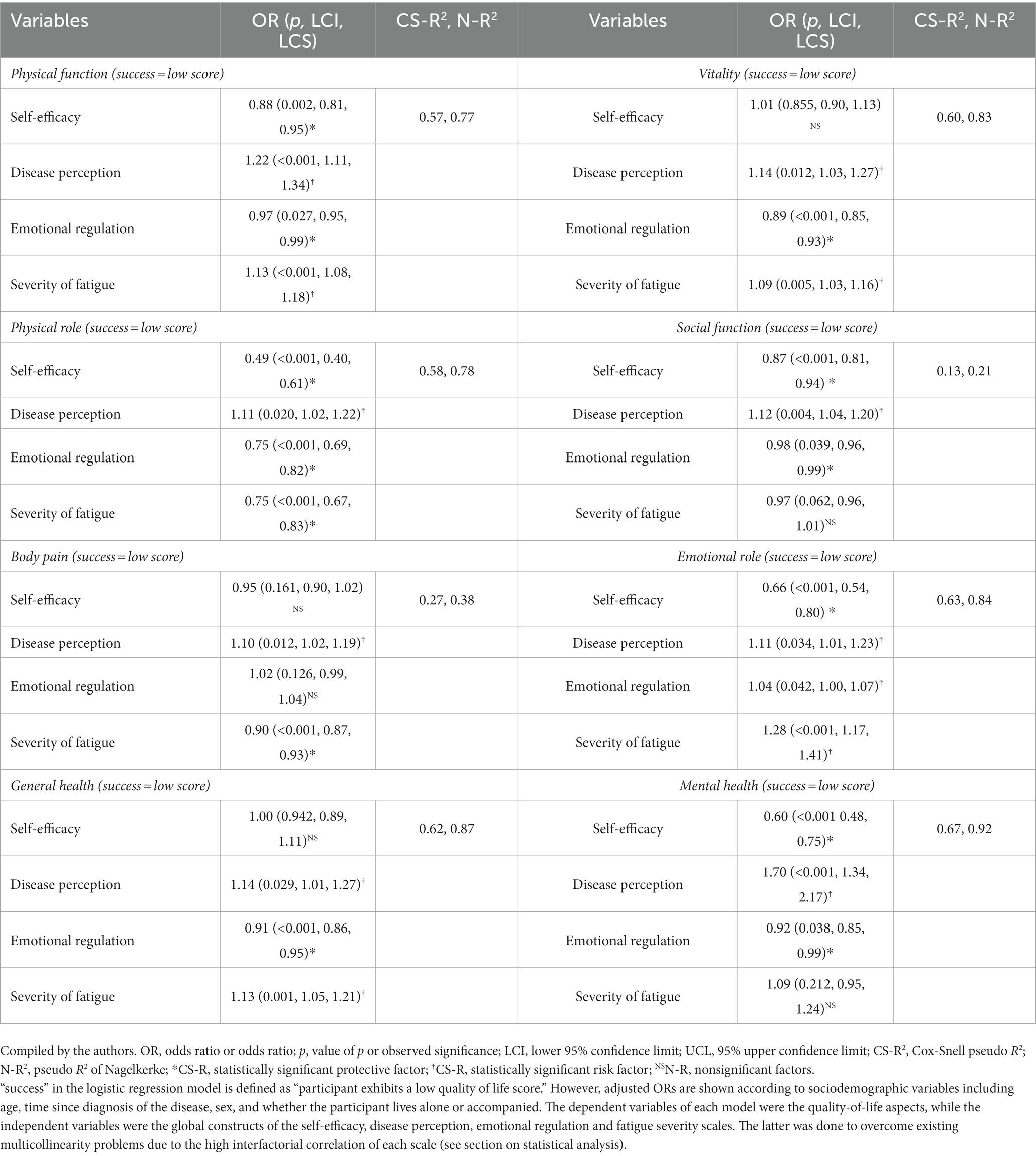
Table 6. Relationship between quality of life, self-efficacy, perception of disease, emotional regulation, and severity of fatigue.
4. Discussion
The aim of this research was to establish the presence of associations between variables such as self-efficacy, perception of disease, emotional regulation, and fatigue and the health-related quality of life in older adults diagnosed with a chronic disease. The results demonstrated that it was possible to identify the existence of different associations between the variables analyzed.
It was found that older adults who had pharmacological treatment with psychiatric medication offered lower scores in personal control and a greater perception of disease. Therefore, it is important to consider that personal control relates to the beliefs that the individual has about monitoring the disease and their state of health and these are attributed to internal or external factors. In this sense, the literature has shown that this perception relates to different aspects, within these are the socioeconomic conditions of the individual and better levels of mental health and subjective well-being (April et al., 2012).
This result on the exposure to psychiatric pharmacological treatment would indicate the need to address aspects relating to the patient’s education concerning their health condition, in order to develop beliefs focused on the fact that, both health and disease are the result of the patient’s own actions, willpower and set of sustained efforts that the patient themselves must make to maintain an optimal state of health according to their conditions and characteristics (Kurtović et al., 2018).
However, the perception of disease as a construct has been widely studied in the field of health, coincident with the fact that patients construct different representations to make sense of the experience of disease to develop coping responses (Hagger and Orbell, 2003). This is a process in which beliefs are formed related to the nature of the disease, the course of time, the consequences or personal impact, possible causes and control/cure relationship, and this approach provides opportunities to help converge the beliefs of the physician and patient in order to achieve significant positive influences including not only the improvement of physical health, but also mental health conditions, since the dissonance between treatment and patient beliefs may increase the symptoms of anxiety and depression undermining their mental health (Broadbent et al., 2009; Morgan et al., 2014).
Among older adults that have psychiatric pharmacological treatment the greater perception of disease suggests a need to inquire about the moderating effect that this condition may have on self-care behaviors, given that although “severity” predicts the presence of self-care behaviors. It has also been identified that a poor emotional state and the belief that the disease is out of control, does not always translate into greater self-management (Riegel et al., 2009; Goodman et al., 2013).
Another relevant characteristic in the results of this research focused on the circumstances of the regime to which the adults belonged. The participants within the contributory regime presented lower scores in severity of disease consequences compared to the older adults benefited from health services corresponding to the subsidized regime. In this sense, it is necessary to contextualize that the subsidized regime is a governmental mechanism aimed at the poorest population of the country that do not have the capacity to pay and access health services through a subsidy offered by the state, while the contributory regime consists of a health system aimed at the population that has the capacity to pay and the monthly income to do so.
This makes sense given that the population belonging to the subsidized regime has lower economic income and socioeconomic characteristics of high vulnerability. Thus, this measure of “severity” of the disease proves that those older adults with better incomes tend to score lower in this dimension perceiving that the consequences of the disease may be less catastrophic compared to the group of adults who are more economically vulnerable and whose consequences may translate into difficulties accessing treatments or an inability to obtain some kind of income for their subsistence, contributing to a cyclical process in which subjective well-being and the perception of mental health are reduced, also undermining their physical health (April et al., 2012).
A fundamental feature in the study of health-disease processes in older adults is associated to the risk and protective factors that contribute to the development of the disease in different directions and in which early intervention could modify the adverse circumstances of the individual. Along these lines, the findings of this study suggest the presence of “fatigue severity” as a probable risk factor for physical function, since as scores of the former increase, so do scores of the latter. These data are consistent with the existing literature, which suggests a significant relationship between the feeling of fatigue often experienced by people diagnosed with a chronic disease and a lower presence of caregiving behaviors (Stadje et al., 2016; Son, 2019).
It is important to emphasize the influence of health- associated quality of life on the “physical function” scores found in this study, an issue that shows a need to discover the multiple ways in which this construct manifests itself and which can be translated into healthy habits and lifestyles that contribute to an optimal state of health for the individual. In general terms, health-related quality of life refers to the subjective evaluation of the interaction between current state of health, care, and promotional activities for maintaining general functioning and according to the data it seems that this assessment of the participants helps by increasing the physical activity among adults, which is linked to habits that promote actions for caring for one’s health (Urzua, 2010).
Finally, evidence was found that self-efficacy and emotional self-regulation positively influence health-related quality of life. Self-efficacy has been studied in the field of health to refer to the perception that people have of their abilities to perform a task, which can lead to people adopting behaviors that care for their health. The results in this field coincide with what has been proposed by different researchers who state that this construct is fundamental to monitoring chronic diseases internally in the long term (Senécal et al., 2000; Fathi et al., 2011).
Conversely, emotional self-regulation suggests that individuals who learn to regulate their emotions have a greater capacity to attenuate, maintain, increase or modify behaviors according to their goals and the conditions of the context in which they are in showing better physical health indicators (Jenaabadi et al., 2015; Hoorelbeke et al., 2016), an issue that coincides with what was found in this study and this highlights the need for carrying out preventive actions related to this variable.
The set of results found, supports the results of different investigations that have found information in the same vein, demonstrating that there is a need to carry out health promotion and prevention strategies aimed at the older adult population that take into consideration factors such as socioeconomic characteristics, beliefs, and perceptions of the disease, as well as individual conditions for the functional coping of chronic disease.
5. Limitations and strengths
We had as a limitation in the study that it was not possible to establish representativeness of the sample, because in Colombia there is no reliable and consolidated information on the exact number of people who suffer from chronic diseases.
This is the first study to be developed in Colombia, evaluating self-efficacy, illness perception, emotional regulation and fatigue on the quality of life associated with the health of older adults. Generating new knowledge for this country.
6. Conclusion
The results of this study show that older adults that have psychiatric medication tend to present lower scores in personal control and a greater perception of disease, which exacerbates their emotional state, and they perceive the disease’s effects to be a large burden, an issue that should be studied in depth considering that the perception of disease is closely associated to the emotional state of the subject.
Furthermore, it was found that socioeconomic status significantly increased the scores in association to the consequences of the disease, which denotes a need for these features to be addressed given that negative perceptions about the disease’s effects contribute to increased depression and anxiety among patients with chronic disease.
Another relevant aspect was to identify the perception of illness and, to a greater extent, the severity of fatigue as factors that could have a negative impact on the physical function of the participants, which contributed significantly to the presence of low scores in physical activity.
Finally, it was found that self-efficacy and emotional self-regulation can increase the positive perception of health-related quality of life.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Comité de Ética de la Clínica General del Norte en Barranquilla-Colombia. The patients/participants provided their written informed consent to participate in this study.
Author contributions
LC-T and SV had full access to all study data and assumed responsibility for the integrity of the data and the accuracy of the analysis. LC-T and SV: concept and design. LC-T, NG, ÁB-N, and JH-L: acquisition, analysis, or interpretation of data. LC-T, SV, MB, and NG: the drafting of the manuscript. LC-T, SV, ÁB-N, NG, JM, LA, GR-C, SC-C, VB, JH-L, CR, MB, and JÁ: critical revision of the manuscript for important intellectual content. JH-L and VB: Statistical analysis. LC-T and VB: acquisition of funding. LC-T, SV, CR, GR-C, SC-C, JM, LA, and JÁ: technical, administrative, or material support. LC-T and SV: supervision. All authors contributed to the article and approved the submitted version.
Funding
The study was funded by the Fundación Universitaria del Área Andina, Universidad del Sinú, Universidad Popular del Cesar, Universidad Simón Bolívar and Clínica General del Norte.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adamowicz, J. L., Velez-Bermudez, M., and Thomas, E. B. K. (2022). Fatigue severity and avoidance among individuals with chronic illness: A meta-analysis. Journal of psychosomatic research 159:110951. doi: 10.1016/j.jpsychores.2022.110951
Almutary, H., and Tayyib, N. (2020). Factors associated with exercise self-efficacy among people with chronic diseases. Appl. Nurs. Res. 54:151275. doi: 10.1016/j.apnr.2020.151275
April, K. A., Dharani, B., and Peters, K. (2012). Impact of locus of control expectancy on level of well-being. Rev. Eur. Stud. 4, 124–137. doi: 10.5539/res.v4n2p124
Ardila, E. (2018). Chronic diseases. Biomedica, 38, 5–6.[date of Consultation July 9, 2022]. ISSN: 0120-4157. Available at: https://www.redalyc.org/articulo.oa?id=84356697001
Arrato, N. A., Valentine, T. R., Byrd, J. C., Jones, J. A., Maddocks, K. J., Woyach, J. A., et al. (2022). Illness representations and psychological outcomes in chronic lymphocytic leukaemia. Br. J. Health Psychol. 27, 553–570. doi: 10.1111/bjhp.12562
Bailey, R. R. (2019). Self-efficacy, self-regulation, social support, and outcomes expectations for daily physical activity in adults with chronic stroke: a descriptive, exploratory study. Occup. Ther. Health Care 33, 129–141. doi: 10.1080/07380577.2018.1558326
Bica, T., Castelló, R., Toussaint, L. L., and Montesó-Curto, P. (2017). Depression as a risk factor of organic diseases:an international integrative review. J. Nurs. Scholarsh. 49, 389–399. doi: 10.1111/jnu.12303
Bramanti, S. M., Trumello, C., Lombardi, L., and Babore, A. (2021). COVID-19 and chronic disease patients: perceived stress, worry, and emotional regulation strategies. Rehabil. Psychol. 66, 380–385. doi: 10.1037/rep0000409
Brioni, E., Delli Zotti, G., Apuzzo, L., Magnaghi, C., Iodice, M., Burrai, F., et al. (2021). Self-efficacy and self-management in patients in hemodialysis: a narrative review of multidisciplinary theories. G. Ital. Nefrol. 38:2021–vol3
Broadbent, E., Ellis, C. J., Thomas, J., Gamble, G., and Petrie, K. J. (2009). Further development of an illness perception intervention for myocardial infarction patients: a randomized controlled trial. J. Psychosom. Res. 67, 17–23. doi: 10.1016/j.jpsychores.2008.12.001
Chan, S. W. (2021). Chronic disease management, self-efficacy and quality of life. J. Nurs. Res. 29:e129. doi: 10.1097/JNR.00000000000000000422
Cheng, Y., Cheng,, et al. (2019). Input and Output Data. United States. doi: 10.25584/data.2020-02.1114/1597292,
Cheng, C., Yang, C. Y., Inder, K., and Chan, S. W. (2020). Illness perceptions, coping strategies, and quality of life in people with multiple chronic conditions. J. Nurs. Scholarsh. 52, 145–154. doi: 10.1111/jnu.12540
Dantas, L. G., Rocha, M. S., and Cruz, C. M. S. (2020). Non-adherence to hemodialysis, perception of the illness, and severity of advanced nephropathy. J. Bras. Nefrol. 42, 413–419. doi: 10.1590/2175-8239-JBN-2019-0147
Della Vecchia, C., Préau, M., Carpentier, C., Viprey, M., Haesebaert, J., Termoz, A., et al. (2019). Illness beliefs and emotional responses in mildly disabled stroke survivors: a qualitative study. PLoS One 14:e0223681. doi: 10.1371/journal.pone.0223681
Dunke Pereira, L., Bellinati, N. V. D. C., and Aparecida Kanan, L. (2018). Self-Efficacy for Managing Chronic Disease 6-Item Scale: avaliação da autoeficácia no gerenciamento da doença crônica. Rev. Cuid. 9, 1–11. doi: 10.15649/cuidarte.v9i3.561
Ekmen, N., Can, G., and Can, H. (2021). Preliminary examination of the relations between disease stage, illness perceptions, coping strategies, and psychological morbidity in chronic hepatitis B and C guided by the common-sense model of illness. Eur. J. Gastroenterol. Hepatol. 33, 932–939. doi: 10.1097/MEG.0000000000002131
Elefante, E., Tani, C., Stagnaro, C., Ferro, F., Parma, A., Carli, L., et al. (2020). Impact of fatigue on health-related quality of life and illness perception in a monocentric cohort of patients with systemic lupus erythematosus. RMD Open 6:e001133. doi: 10.1136/rmdopen-2019-001133
Farley, H. (2020). Promoting self-efficacy in patients with chronic disease beyond traditional education: a literature review. Nurs. Open 7, 30–41. doi: 10.1002/nop2.382
Fathi, A., Kheir, M., and Atigh, M. (2011). The relationship between self-efficacy and quality of life due to the mediating role of resiliency among patients with cardiovascular disease. Psychol. Methods Models 2, 109–122. doi: 10.7508/jnms.2015.02.003
Gallardo-Solarte, K., Benavides-Acosta, F. P., and Rosales-Jiménez, R. (2016). Costos de la enfermedad crónica no transmisible: La realidad colombiana [in English: costs of chronic noncommunicable disease: the Colombian reality]. Rev. Ciencias de la Salud 14, 103–114. doi: 10.12804/revsalud14.01.2016.09
Giuffrida, S., Fiala, S., Barro, L., Pazzi, S., Soldini, E., Levati, S., et al. (2021). Descrizione e analisi delle rappresentazioni di malattia nei pazienti cronici attraverso l'Illnes Perception Questionnaire (IPQ-r): impliczioni per la pratica clinica. Prof. Inferm. 74, 219–226. doi: 10.7429/pi.2021.744226
Gregg, L. P., Bossola, M., Ostrosky-Frid, M., and Hedayati, S. S. (2021). Fatigue in CKD: epidemiology, pathophysiology, and treatment. Clin. J. Am. Soc. Nephrol. 16, 1445–1455. doi: 10.2215/CJN.19891220
Goodman, R. A., Posner, S. F., Huang, E. S., Parekh, A. K., and Koh, H. K. (2013). Defining and measuring chronic conditions: imperatives for research, policy, program, and practice. Prev. Chronic Dis. 10:E66. doi: 10.5888/pcd10.120239
Hagger, M. S., and Orbell, S. (2003). A meta-analytic review of the common-sense model of illness representations. Psychol. Health 18, 141–184. doi: 10.1080/088704403100081321
Hernández Sampieri, R., Fernández Collado, C., and Baptista Lucio, P. (2014). Metodología de la investigación (6th ed.). Mexico D.F.: McGraw-Hill.
Hill, E. M., and Frost, A. (2022). Illness perceptions, coping, and health-related quality of life among individuals experiencing chronic Lyme disease. Chronic Illn. 18, 426–438. doi: 10.1177/1742395320983875
Hoorelbeke, K., Koster, E. H., Demeyer, I., Loeys, T., and Vanderhasselt, M. A. (2016). Effects of cognitive control training on the dynamics of (mal) adaptive emotion regulation in daily life. Emotion 16, 945–956. doi: 10.1037/emo0000169
Járomi, M., Szilágyi, B., Velényi, A., Leidecker, E., Raposa, B. L., Hock, M., et al. (2021). Assessment of health-related quality of life and patient’s knowledge in chronic non-specific low back pain. BMC Public Health 21:1479. doi: 10.1186/s12889-020-09506-7
Jenaabadi, H., Ali-Ahani, M., and Sabaghi, F. (2015). Examining the relationship of optimism and emotion regulation strategies with general health among students of University of Sistan and Baluchestan. Health 07, 865–872. doi: 10.4236/health.2015.77102
Kar, S., and Zengin, N. (2020). The relation between self-efficacy in patients with chronic obstructive pulmonary disease and caregiver burden. Scand. J. Caring Sci. 34, 754–761. doi: 10.1111/scs.12780
Kurtović, A., Vuković, I., and Gajić, M. (2018). The effect of locus of control on university students’ mental health: possible mediation through self-esteem and coping. J. Psychol. 152, 341–357. doi: 10.1080/00223980.2018.1463962
Lugo, L., García, H., and Gómez, C. (2006). Reliability of the SF-36 health quality of life questionnaire in Medellín Colombia. Rev. Fac. Nac. Salud Pública 24, 37–50.
Luque, B., Castillo-Mayén, R., Cuadrado, E., Gutiérrez-Domingo, T., Rubio, S. J., Arenas, A., et al. (2020). The role of emotional regulation and affective balance on health perception in cardiovascular disease patients according to sex differences. J. Clin. Med. 9:3165. doi: 10.3390/jcm9103165
Martinengo, L., Olsson, M., Bajpai, R., Soljak, M., Upton, Z., Schmidtchen, A., et al. (2019). Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies. Ann. Epidemiol. 29, 8–15. doi: 10.1016/j.annepidem.2018.10.005
Menting, T., Tack, C. J, Bleijenberg, G., Donders, R., Droogleever Fortuyn, H. A., and Fransen, J. (2018). Is fatigue a disease-specific or generic symptom in chronic medical conditions? Health psychology: official journal of the Division of Health Psychology, American Psychological Association. 37, 530–543. doi: 10.1037/hea0000598
Mitchell, E., and Walker, R. (2020). Global ageing: successes, challenges and opportunities. Br. J. Hosp. Med. 81, 1–9. doi: 10.12968/hmed.2019.0377
Morgan, K., Villiers-Tuthill, A., Barker, M., and McGee, H. (2014). The contribution of illness perception to psychological distress in heart failure patients. BMC Psychol. 2, 2–9. Available at: http://www.biomedcentral.com/2/1/50
Muñoz-Martínez, A. M., Vargas, R. M., and Hoyos-González, J. S. (2006). Difficulties in emotional regulation scale (DERS): factorial analysis in a Colombian sample. Acta Colomb. de Psicol. 19, 233–244.
Nocerino, R., De Filippis, F., Cecere, G., Marino, A., Micillo, M., Di Scala, C., et al. (2020). The therapeutic efficacy of Bifidobacterium animalis subsp. lactis BB-12® in infant colic: A randomised, double blind, placebo-controlled trial. Aliment. Pharmacol. Ther. 51, 110–120. doi: 10.1111/apt.15561
Oga, T., Windisch, W., Handa, T., Hirai, T., and Chin, K. (2018). Health-related quality of life measurement in patients with chronic respiratory failure. Respir. Investig. 56, 214–221. doi: 10.1016/j.resinv.2018.01.006
Özkan Tuncay, F., Fertelli, T., and Mollaoğlu, M. (2018). Effects of loneliness on illness perception in persons with a chronic disease. J. Clin. Nurs. 27, e1494–e1500. doi: 10.1111/jocn.14273
Pacheco-Huergo, V., Viladrich, C., Pujol-Ribera, E., Cabezas-Peña, C., Núñez, M., Roura-Olmeda, P., et al. (2012). Perception in chronic illnesses: linguistic validation of the revised illness perception questionnaire and the brief illness perception questionnaire for a Spanish population. Aten. Primaria 44, 280–287. doi: 10.1016/j.aprim.2010.11.022
Paneri, G., and Napolitano, F. (2021). Assessing patients’ self-efficacy in chronic obstructive pulmonary disease: translation, content and face validation of the “understanding COPD questionnaire”. Prof. Inferm. 74:271. doi: 10.7429/pi.2021.744271b.
Partridge, L., Deelen, J., and Slagboom, P. E. (2018). Facing up to the global challenges of ageing. Nature 561, 45–56. doi: 10.1038/s41586-018-0457-8
Ritter, P. L., and Lorig, K. (2014). The English and Spanish self-efficacy to manage chronic disease scale measures were validated using multiple studies. J. Clin. Epidemiol. 67, 1265–1273. doi: 10.1016/j.jclinepi.2014.06.009
Riegel, B., Moser, D. K., Anker, S. D., Appel, L. J., Dunbar, S. B., Grady, K. L., et al. (2009). State of the science: promoting self-care in people with heart failure: a scientific statement from the American Heart Association. Circulation 120, 1141–1163. doi: 10.1161/CIRCULATIONAHA.109.192628
Riveros Munévar, F., Bernal Vargas, L., Bohórquez Borda, D., Vinaccia Alpi, S., and and Margarita Quiceno, J. (2017). Psychometric analysis of the Connor-Davidson Resilience Scale (CD-RISC 10) in a Colombian university population. Psicología desde el Caribe, 34, 161–171. doi: 10.14482/psdc.34.3.11140
Rosselli, D., Ardila, A., Pradilla, G., Morillo, L, Bautista, L., Rey, O., et al. (2000). The mini-mental state examination as a selected diagnostic test for dementia: a Colombian population study. GENECO. Rev. Neurol. 30, 428–432.
Roy, B., Riley, C., and Sinha, R. (2018). Emotion regulation moderates the association between chronic stress and cardiovascular disease risk in humans: a cross-sectional study. Stress 21, 548–555. doi: 10.1080/10253890.2018.1490724
Sawada, A., Hiragi, S., Tamura, H., Goto, R., Matsuyama, Y., Sakai, K., et al. (2021). Evaluation of the quality of life and health-related quality of life of patients with end-stage kidney disease resulting from kidney transplantation using the kidney disease quality of life-short form and EuroQOL-5 Dimension-5 level questionnaires. Transplant. Proc. 53, 881–884. doi: 10.1016/j.transproceed.2020.09.018
Selzler, A. M., Habash, R., Robson, L., Lenton, E., Goldstein, R., and Brooks, D. (2020). Self-efficacy and health-related quality of life in chronic obstructive pulmonary disease: a meta-analysis. Patient Educ. Couns. 103, 682–692. doi: 10.1016/j.pec.2019.12.003
Senécal, C., Nouwen, A., and White, D. (2000). Motivation and dietary self-care in adults with diabetes: are self-efficacy and autonomous self-regulation complementary or competing constructs? Health Psychol. 19, 452–457. doi: 10.1037/0278-6133.19.5.452
Silva, W. T., Ávila, M. R., de Oliveira, L. F. F., de Souza, I. N., de Almeida, I. L. G. I., Madureira, F. P., et al. (2021). Differences in health-related quality of life in patients with mild and severe chronic venous insufficiency: a systematic review and meta-analysis. J. Vasc. Nurs. 39, 126–133. doi: 10.1016/j.jvn.2021.09.002
Son, C. G. (2019). Differential diagnosis between “chronic fatigue” and “chronic fatigue syndrome”. Integr. Med. Res. 8, 89–91. doi: 10.1016/j.imr.2019.04.005
Stadje, R., Dornieden, K., Baum, E., Becker, A., Biroga, T., Bösner, S., et al. (2016). The differential diagnosis of tiredness: a systematic review. BMC Fam. Pract. 17:147. doi: 10.1186/s12875-016-0545-5
Szabó-Bartha, A., and Mirnics, Z. (2021). Representations of chronic illness in patients and their partners. Psychiatr. Danub. 33, 432–440.
Timkova, V., Mikula, P., Fedicova, M., Szilasiova, J., and Nagyova, I. (2021). Psychological well-being in people with multiple sclerosis and its association with illness perception and self-esteem. Mult. Scler. Relat. Disord. 54:103114. doi: 10.1016/j.msard.2021.103114
Torossian, M., and Jacelon, C. S. (2021). Chronic illness and fatigue in older individuals: a systematic review. Rehabil. Nurs. 46, 125–136. doi: 10.1097/RNJ.0000000000000278
Urzua, M. A. (2010). Health related quality of life: conceptual elements. Rev. Med. Chil. 138, 358–365.
Wierenga, K. L., Lehto, R. H., and Given, B. (2017). Emotion regulation in chronic disease populations: an integrative review. Res. theory nurs. pract. 31, 247–271. doi: 10.1891/1541-6577.31.3.247
Wierenga, L. M., Sexton, J. A., Laake, P., Giedd, J. N., and Tamnes, C. K. (2018). A key characteristic of sex differences in the developing brain: greater variability in brain structure of boys than girls. Cerebral cortex (New York, NY: 1991), 28, 2741–2751. doi: 10.1093/cercor/bhx154
World Health Organization. Global Action Plan: For the Prevention and Control of Non-Communicable Diseases (2013-2020) (2013). Available at: https://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf (Accessed January 13, 2020).
World Health Organization. Noncommunicable Diseases (Ncd) (2019). Available at: https://www.who.int/gho/ncd/mortality_morbidity/en/ (Accessed January 03, 2020).
World Health Organization. (2020). World Health Organization. Retrieved from World Health Organization: https://www.paho.org/es/temas/enfermedades-no-transmisibles
Yi, Q. F., Yang, G. L., and Yan, J. (2021). Self-efficacy intervention programs in patients with chronic obstructive pulmonary disease: narrative review. Int. J. Chron. Obstruct. Pulmon. Dis. 16, 3397–3403. doi: 10.2147/COPD.S338720
Yuan, Y., Xu, H. W., Zhang, S., Wang, Y., Kitayama, A., Takashi, E., et al. (2021). The mediating effect of self-efficacy on the relationship between family functioning and quality of life among elders with chronic diseases. Nurs. Open 8, 3566–3574. doi: 10.1002/nop2.906
Zarotti, N., Simpson, J., Fletcher, I., Squitieri, F., and Migliore, S. (2018). Exploring emotion regulation and emotion recognition in people with presymptomatic Huntington’s disease: the role of emotional awareness. Neuropsychologia 112, 1–9. doi: 10.1016/j.neuropsychologia.2018.02.030
Keywords: well-being, mental health, skill, personality, emotions
Citation: Cudris-Torres L, Alpi SV, Barrios-Núñez Á, Gaviria Arrieta N, Mejía Gutiérrez J, Alvis Barranco L, Rios-Carlys G, Cuenca-Calderón SE, Bermúdez V, Hernández-Lalinde J, Riveira Zuleta CA, Bahamón MJ and Álvarez Herrera JS (2023) Quality of life in the older adults: The protective role of self-efficacy in adequate coping in patients with chronic diseases. Front. Psychol. 14:1106563. doi: 10.3389/fpsyg.2023.1106563
Edited by:
Nai Peng Tey, University of Malaya, MalaysiaReviewed by:
Yuke Tien Fong, Singapore General Hospital, SingaporePavol Mikula, University of Pavol Jozef Šafárik, Slovakia
Copyright © 2023 Cudris-Torres, Alpi, Barrios-Núñez, Gaviria Arrieta, Mejía Gutiérrez, Alvis Barranco, Rios-Carlys, Cuenca-Calderón, Bermúdez, Hernández-Lalinde, Riveira Zuleta, Bahamón and Álvarez Herrera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorena Cudris-Torres, bGN1ZHJpc0BhcmVhbmRpbmEuZWR1LmNv
†ORCID: Lorena Cudris-Torres, https://orcid.org/0000-0002-3120-4757
Stefano Vinaccia Alpi, https://orcid.org/0000-0001-5169-0871
Álvaro Barrios-Núñez, https://orcid.org/0000-0003-4153-8950
Natali Gaviria Arrieta, https://orcid.org/0000-0002-2401-7662
Jéssica Mejía Gutiérrez, https://orcid.org/0000-0002-7458-9132
Libia Alvis Barranco, https://orcid.org/0000-0002-7723-3385
Gerson Rios-Carlys, https://orcid.org/0000-0002-5029-4268?lang=es
Silvia E. Cuenca-Calderón, https://orcid.org/0000-0002-9749-9359
Valmore Bermúdez, https://orcid.org/0000-0003-1880-8887
Juan Hernández-Lalinde, https://orcid.org/0000-0001-6768-1873
Carlos Arturo Riveira Zuleta, https://orcid.org/0000-0001-5752-2609
Marly Johana Bahamón, https://orcid.org/0000-0003-2528-994X
Juany Sofía Álvarez Herrera, https://orcid.org/0000-0002-5332-5023