 Youngmee Kim
Youngmee Kim Charles S. Carver
Charles S. Carver Barry E. Hurwitz
Barry E. Hurwitz
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychol. , 09 February 2023
Sec. Health Psychology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1103081
Concerns pertaining to health and to problems in close relationships are both known to be major stressors, yet existing tools are inadequate to assess individual reactions to such stressors. Thus, we sought to develop and preliminarily validate a stress-inducing task for use in a laboratory setting that pertains to the sorts of health-related concerns people face in close relationships. Heterosexual dating couples (44 individuals: mean age 22) were randomized to be paired with their own partner or a stranger and to play a role of speaker or listener. Participants were asked to imagine a scenario in which one person is hit by a car (listener role) and the partner has no means to provide or seek out help for the victim (speaker role). The session consisted of baseline, speech preparation, stress task, and recovery phases. General linear modeling results revealed that the task induced stress, evidenced in cardiovascular activities and self-reported negative affect. Giving a brief speech about the stressful situation creates physiological and psychological strains, regardless of pairing with one’s own partner or stranger. Furthermore, cardiovascular and negative affect reactivity to the STress Induction Tool for Close relationships and Health (STITCH) task tended to vary by individual characteristics that reflect one’s sensitivity to close relationship-and health-related stress. This tool is intended to be used for testing relationship theory-driven phenomenon and longer-term implications of physiological and affective reactivities in the quality of life and health outcomes of those who experienced a medically stressful circumstance personally or in the family.
Responses to acute laboratory stressors (reactivity and recovery) have long been recognized as reliable markers of variation in development of diseases even years later (Dickerson and Kemeny, 2004; Steptoe et al., 2007; Chida and Hamer, 2008; Pattyn et al., 2010; Dias and Neto, 2016; Ford et al., 2018; Giannakakis et al., 2019). One of the most widely used tasks to induce stress in the laboratory is the Trier Social Stress Task (TSST; Kirschbaum et al., 2004). The TSST involves delivering a speech and performing mental arithmetic in front of an audience or a video camera recording the performance to be evaluated by others. These procedures thus induce social evaluative stress, in the form of judgmental other people (experimenter or audience).
Although such tasks are successful stress inducers, they have important limitations. For example, the TSST provokes one particular sort of stress: social evaluative stress. Although social evaluation is an important source of stress, it differs from many other common kinds of stress that people experience in their lives, such as problems in close relationships and confrontations with medical illnesses. The TSST is also designed to create a stress response in one person at a time. However, many kinds of stress involve more than one person who mutually experience the common stressor, such as concerns pertaining to health and problems in close relationships. Both kinds of stress are known to be major stressors (Slavich, 2016), which have been significant predictors of adverse neuroendocrine and immune responses, poor quality of life, and even the developing of major diseases (Dickerson and Kemeny, 2004; Robles et al., 2014). If each of these two kinds of stressors is problematic in itself, joining them to one another is likely to exacerbate the adverse effect of each. How people react to these sorts of stressors is likely not well captured by the TSST or other existing commonly used lab stressors.
Further, in line with the adult attachment theory (Hazan and Shaver, 1987; Feeney and Kirkpatrick, 1996; Fraley and Shaver, 2000) and the social baseline theory (Beckes and Coan, 2011), adult family relationships are an interdependent system, in which stress and its regulation by one person involves not only that person’s own experience but also that of the partner. Thus, for example, a new medical illness for one family member is a stressor shared by all adult family members. The diagnosis imposes additional and mutual challenges on the relationship, with the introduction of new roles of patient and caregiver. Major medical illnesses also impose repeated or cyclic challenges over a long period of time.
Common stressors for patients with a medical illness include dealing with the disease itself and also feeling that their illness (and they themselves) burden their family members in numerous ways (Hagger and Orbell, 2003; Kim et al., 2016). Common stressors for caregivers include attempting to minimize the patient’s suffering and providing diverse types of support to the patient, and carrying out their own existing social roles and roles that have been newly added by the patient’s illness, all while managing their own emotional upheaval brought on by the patient’s illness (Kim and Given, 2008; Northouse et al., 2010; Kent et al., 2016). In addition to attachment relationship orientations, individual differences in stress perception and regulation, such as personality traits, have also been associated with different adjustment outcomes (McCrae et al., 2005).
An important goal is understanding how the shared stress and stress regulation that follow from a serious medical diagnosis affects the mental and physical health of each person in the family, ultimately resulting in long-term poor quality of life and development of morbidities. How to study the stress regulation of families confronting illness presents a real challenge, however. The time surrounding a diagnosis involves demands at an individual, family, and medical system level. There are multiple difficulties in obtaining information about the family’s reactions to these demands. It often is difficult to have patients and family members participate in psychosocial research during the period of a medical crisis, and retrospective information about such experiences is subject to substantial recall bias.
Thus, we sought to develop and validate a stress-inducing task that is pertinent to the sorts of health-related concerns people face in close relationships. In essence, we sought to create an analog of illness-related relationship stress that incorporated a challenge to physical health in a laboratory setting. The task we developed used a standardized event—a hypothetical accident in which one person (representing the patient) is badly injured by an impaired driver who fled the scene, while the partner (representing the caregiver) is left otherwise alone and helpless. Dyads were asked to imagine themselves in this situation as vividly as possible and consider the thoughts and feelings they would have. The caregiver then spoke about those thoughts and feelings while the patient listened.
Using a laboratory analog in which the same context is presented to everyone, rather than trying to assess stress regulation in the medical setting itself has several benefits. First, as noted above, there are both practical and ethical issues involved in trying to assess these responses in real time during the medical crisis itself. Instead, stress regulation between a dyad can be assessed later on, at a time that does not intrude on the medical event. Second, using a standardized event for the lab task reduces variability between individuals and between couples stemming from exposure to different medical systems, different actual medial events, and so on. Standardizing the requirements of the task, and using a context that, although health-related, is not the same medical situation as the patient actually has been dealing with will reduce effects of variations in wishing not to talk about the patient’s medical illness itself while “moving on” after the initial medical treatment.
In the work reported here, the newly developed task in this study was validated by assessment of cardiovascular activity and self-reported negative affect. Cardiovascular activity indicators and self-reported negative affect across various stress induction phases and study conditions were chosen as primary outcomes, as the link from conflict in close relationships to these indicators has been well-documented (Nealey-Moore et al., 2007; Chida and Steptoe, 2010). We hypothesized that cardiovascular activity indicators and self-reported negative affect would peak when the task stress is induced, and that it would be more prominent for the person delivering a speech about the stress experience (as opposed to listening to the speech). We also expected that stress would be greater when the person was paired in the stressful task with his or her own romantic partner (as opposed to being paired with a stranger). For this purpose, we decided to study young dating couples to randomly assign them to either pairing condition, as opposed to old cancer patient-caregiver dyads.
A second approach to validation was to examine individual difference characteristics that are sensitive to close relationship-and health-related stressors. We hypothesized that attachment anxiety and neuroticism would be related to greater cardiovascular activity and negative affect at baseline, reflecting the trait characteristics of hyperarousal to relationship loss or distress. Attachment anxiety and agreeableness were also hypothesized to be sensitive to the onset of the stressor reflecting a threat to close relationship and health (Kim, 2006; Dimsdale, 2008; Schneider et al., 2012; Pietromonaco and Beck, 2019); thus its association with outcomes would vary significantly across study phases.
Young adult couples were recruited for this study from the university campus using flyers and by word of mouth. Eligibility criteria were to be 18 years or older and to have been in a committed relationship for at least 3 months with a heterosexual partner at the time of participation. Individuals participated in the study for course credits or for cash in response to study flyers. A total of 44 individuals (22 couples) participated in this study.
This study was conducted in compliance with the regulations of the University of Miami Institutional Review Board from February to May 2011. No foods or drinks were allowed for 30 min before arrival to the laboratory. Upon arrival, participants provided informed consent individually. Next, participants were assigned to one of the two study conditions: paired with their own romantic partner or with a stranger. The pair then moved to an experimental room, where a blood pressure cuff and three electrodes were placed on each participant before he/she began filling out questionnaires for the next 30 min, allowing blood pressure to reach a baseline (Baseline Phase).
At the end of the baseline phase, individuals within a dyad were randomly assigned to one of two experimental roles, speaker or listener, in a scenario that was to be read aloud by the experimenter. An eight-minute stress period (3 min of Preparation Phase and 5 min of Stress Task Phase) was followed by 22 min of Recovery. During the recovery phase, participants continued filling out questionnaires with no further tasks. Finally, participants were debriefed about the study and given appropriate incentive of either course credits or having the option to either receive a $30 check or enter their names into a $200 raffle, as a couple. Participants were given an opportunity to revoke their consent to participate in the study after the debriefing.
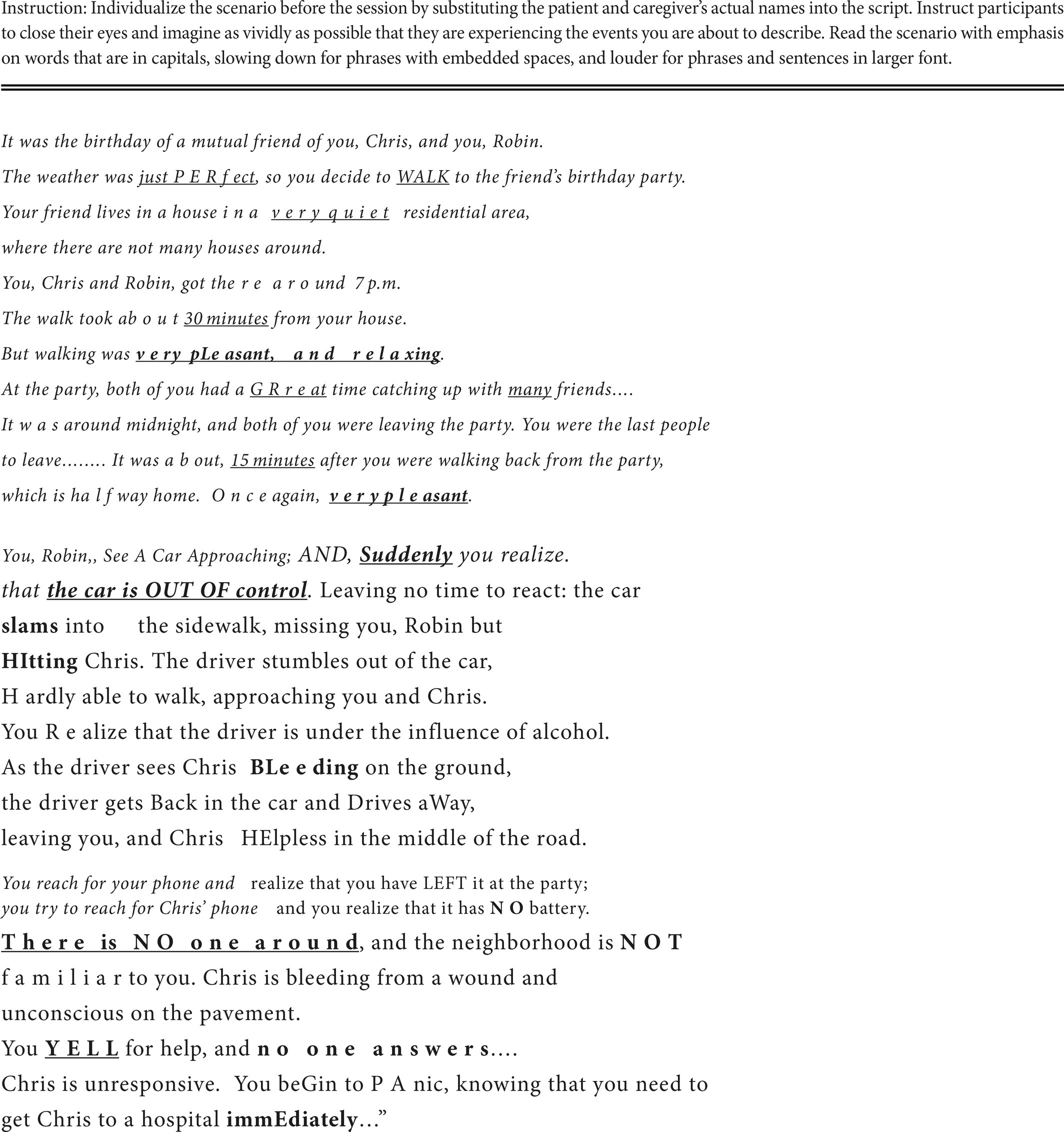
The STress Induction Tool for Close relationships and Health (STITCH) task was developed for this study in order to induce stress that is pertinent to close relationships, and to do so in the context of health issues. The STITCH requires the dyad to imagine being involved in a car accident in which one is hit by a drunk driver who drives away, leaving the partner helpless in the middle of the road late at night in an unfamiliar neighborhood without convenient access to immediate help (see Appendix for full STITCH scenario).
The person randomized to the speaker role at the beginning of the preparation phase was instructed to identify him/herself with the character in the scenario whose partner was injured, as a proxy of caregiver; the listener was instructed to identify him/herself with the character in the scenario who had been injured, as a proxy of the patient. The experimenter then read the scenario to the couple. After that, the speaker was given 3 min to prepare for a speech describing as vividly as possible how he/she would feel physically and emotionally and what he/she might attempt to do if he/she was in the situation described in the scenario. The listener was instructed writing a paragraph describing the classroom of a class he/she took last week, not to engage in any interaction with the speaker, and also to simulate the unconscious condition of the victim. After the preparation phase, the speaker spoke for 5 min. If he/she stopped before the end of 5 min, the experimenter instructed the speaker to reiterate what had been said. While the speaker presented his/her speech, the listener was asked to simply sit still and listen to the speaker.
Each individual’s systolic blood pressure (SBP, mmHg), diastolic blood pressure (DBP, mmHg), and heart rate (HR, beats per min) were measured using a Critikon Dinamap (model 1846SX) Adult/Pediatric Vital Signs Monitor. The occlusion cuff was placed on the upper portion of the arm. The three indicators of cardiovascular activity were measured at approximately 1.5 min intervals during a given study phase. The two final baseline recordings were used to represent baseline value before the stress task was introduced. In the preparation phase, recordings were made at 1.5 and 3 min (end of that phase). In the 5 min of the Stress Task Phase, recordings were made at 1.5, 3, and 4.5 min. At the start of the recovery phase, three recordings were obtained at 1.5, 3, and 4.5 min, to capture the initial recovery patterns immediately after removal of the stress. The values of each cardiovascular activity indicator within a phase were averaged. Data for each measure thus consisted of one mean for each of the study phases: baseline, preparation, stress task, and recovery.
Each individual’s perceived stress at the moment was measured using three adjectives (stressful, unpleasant, and strained) responding to a question “how do you feel right now?” on a 5-point Likert type scale (1 = not at all; 5 = very much) at the end of each phase. The three items were averaged: higher scores indicating greater self-reported negative affect. Internal consistency during the stress induction phases (preparation, stress task, and recovery phases) was good (αs = 0.85, 0.83, and 0.72, respectively), while that before the stress induction was acceptable (α = 0.59).
The qualities of attachment that participants felt with respect to their romantic partner were measured dimensionally, using the Measure of Attachment Qualities, or MAQ (Carver, 1997). MAQ items are statements, answered for extent of agreement on a 4-point Likert-type scale (1 = strongly disagree, 4 = strongly agree). The MAQ has four subscales, one reflecting security (e.g., “It feels relaxing and good to be close to him/her”), one reflecting anxiety related to worry (e.g., “I often worry that he/she does not really love me”), one reflecting anxiety related to desire to merge (e.g., “I have trouble getting others to be as close as I want them to be”), and one reflecting avoidance (e.g., “I prefer not to be too close to him/her”). Each of the four sub-scales had adequate internal consistency: security (3 items, α = 0.69); anxiety-worry (3 items, α = 0.69); anxiety-merger (3 items, α = 0.74); and avoidance (5 items, α = 0.72). Each sub-scale was scored by averaging responses (after appropriate reversals). Security was inversely and fairly substantially related to avoidance, r = −0.62, p < 0.001, but was not significantly related to anxiety-worry and anxiety-merger (rs < −0.18, ps > 0.22); correlations of anxiety-worry with anxiety-merger and avoidance were positive and significant (r = 0.502, p < 0.001; r = 0.374, p = 0.017, respectively); and correlation of anxiety-merger with avoidance was 0.43, p < 0.006.
Individual differences in the five major personality factors (extraversion, agreeableness, conscientiousness, neuroticism, and agreeableness) were assessed using the 25-item NEO-FFI (Costa and McCrae, 1992; McCrae et al., 2005) on a 5-point Likert-type scale. Each factor was scored by averaging corresponding items (after appropriate reversals). Each of the five factors (5 items per factor) had adequate internal consistency (0.64 < αs < 0.81) and represented fairly distinct characteristics to each other (|0.002| < rs < |0.307|, 0.057 < ps < 0.992).
Mean, standard deviation, and frequency of study variables were computed. The primary aim was to validate the stress-inducing task, STITCH, in two ways. First, whether cardiovascular activities and negative affect changed in response to the STITCH task was examined using general linear modeling. Each of the cardiovascular activity and negative affect markers was predicted independently by study phases (repeated measures), experimental role (speaker vs. listener), experimental condition (paired with own partner or a stranger), and the two-way interaction effects with study phases.
The validity of the STITCH task with regard to inducing stress would be supported by the following effects. A significant curvilinear (inverse U-shape with peaks during preparation and stress task phases) time effect would indicate an overall stress response. The interaction of time with experimental role (speaker showing greater stress reaction) would support the predicted role difference. And the interaction of time with experimental condition predicted experimental condition difference.
Regarding the validity of the STITCH task by individual difference characteristics would be supported by attachment anxiety and neuroticism associated with greater cardiovascular activity and negative affect at baseline; and attachment anxiety and agreeableness associated with greater variability in outcomes across study phases. Significance level in all analyses was set at p < 0.05. Significance at p < 0.10 was interpreted with caution.
Study participants were primarily either non-Hispanic or Hispanic White young adults. Their cardiovascular activity indicators were normative for their age during the resting baseline phase (Tables 1, 2). As shown in Table 2, curvilinear time effects, showing increases from baseline to preparation and stress task periods and decreases afterward, of all three cardiovascular activity indicators and negative affect were significant (ps < 0.03). Both SBP and DBP increased to peak at the stress task phase and then subsided at the recovery phase. DBP value at the recovery phase completely returned to the initial resting baseline level [paired t-tests between baseline and recovery values: t(1,43) = 1.05, p = 0.30]; that of SBP remained marginally elevated [paired t(1,43) = 1.86, p = 0.069]. HR peaked equally at the preparation and stress task phases then subsided at the recovery phase, but did not return to baseline [paired t(1,43) = 2.04, p = 0.047]. Self-reported negative affect increased to peak at the preparation phase and then subsided by the end of the recovery phase to be similar to the initial baseline level [paired test between baseline and recovery t(1,43) = 0.53, p = 0.60].
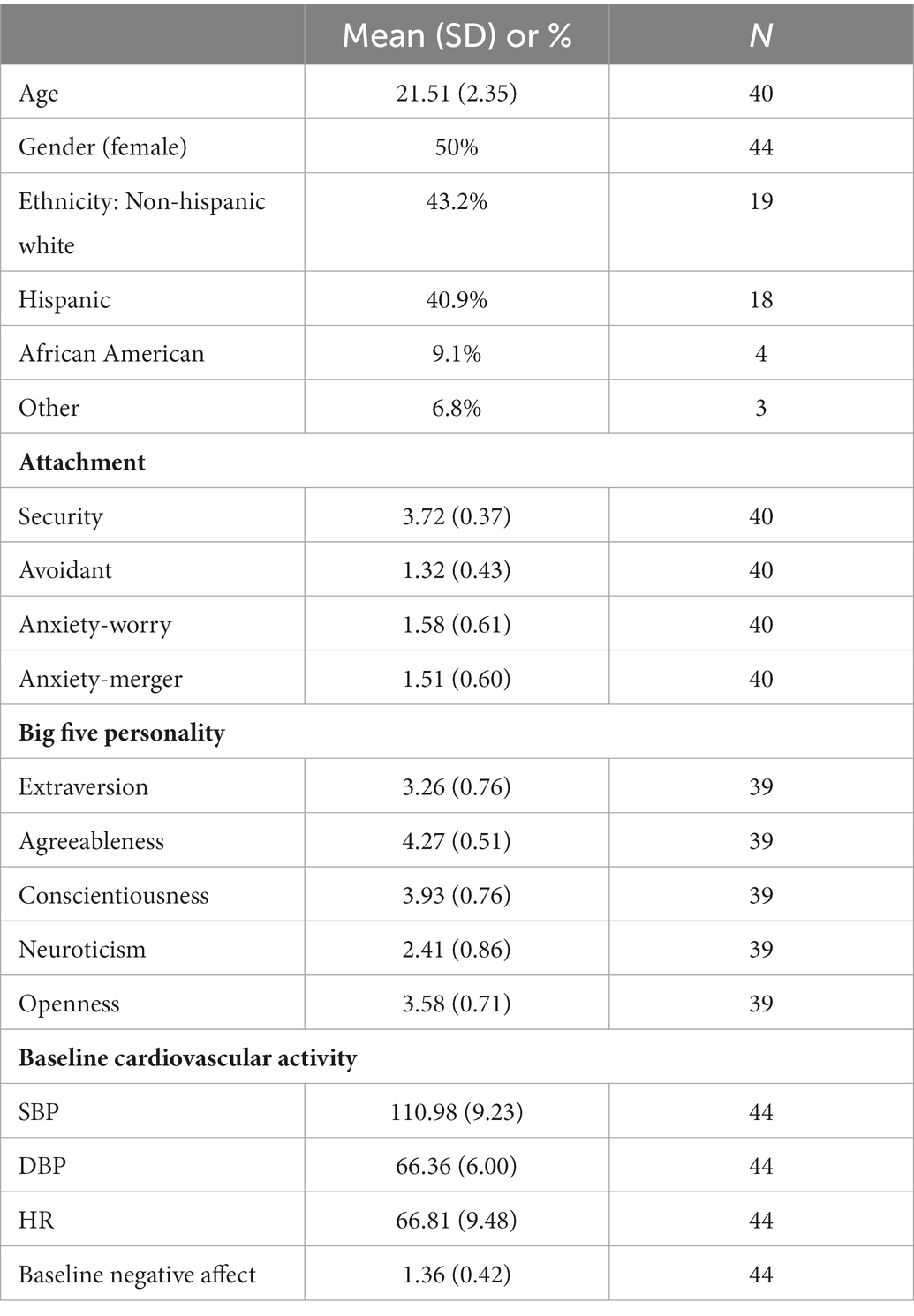
Table 1. Sample characteristics and descriptive statistics for study variables.
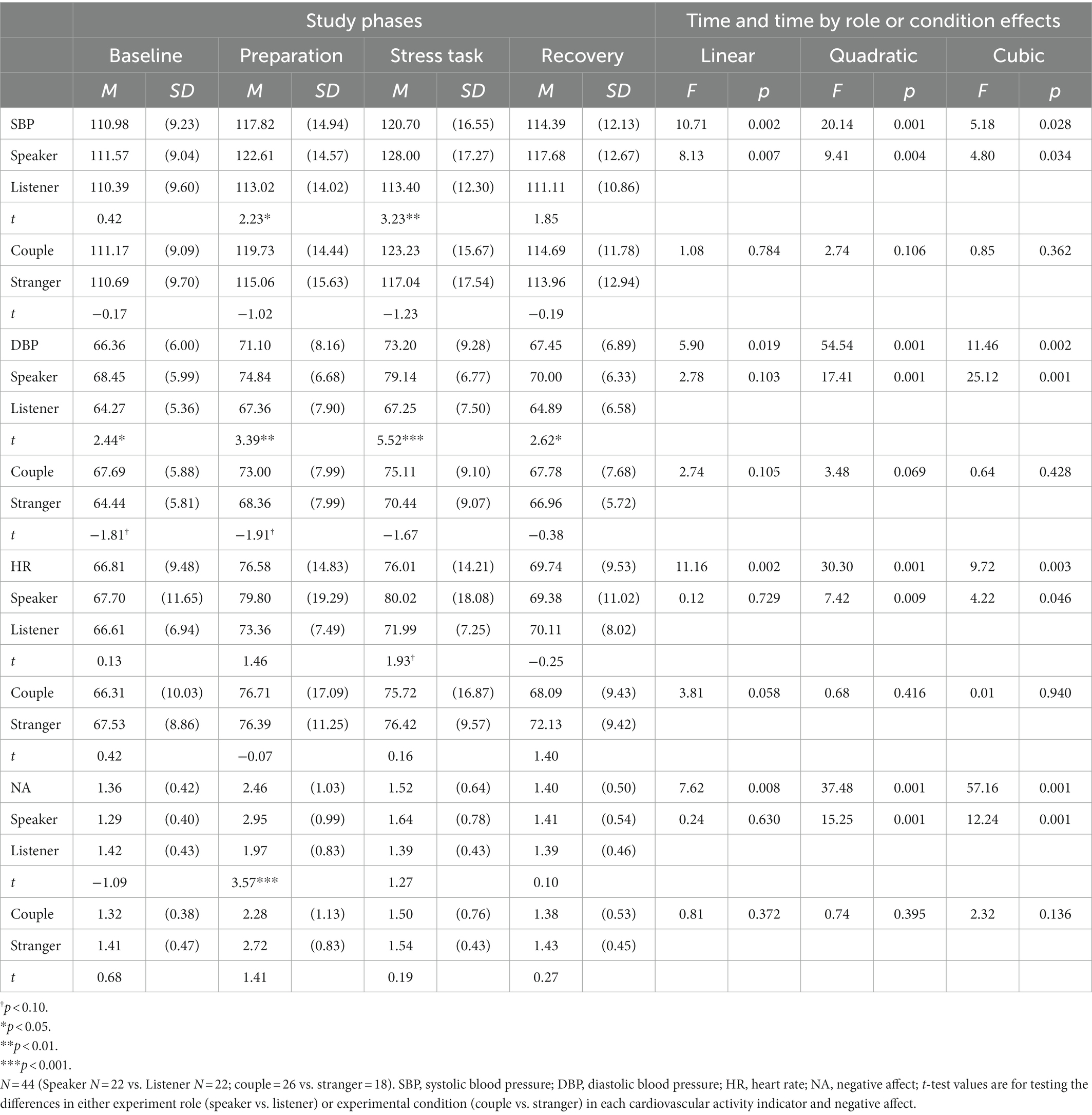
Table 2. Descriptives of cardiovascular activity indicators and negative affect by study phases, experimental role (speaker vs. listener), and experimental condition (paired with own partner: couple vs. with stranger); and t-test for each role or condition effects within a study phase.
Participants were randomly assigned to one of the two experimental role conditions (speaker vs. listener) just before the preparation phase began. As shown in speaker-listener rows in Table 2, the main effect of experimental role was significant on SBP [F(1,42) = 5.24, p = 0.027] and DBP [F(1,42) = 15.16, p = 0.001], marginally significant on NA [F(1,42) = 3.80, p = 0.058], but not significant on HR [F(1,42) = 1.12, p = 0.296]. Participants in the speaker condition had higher blood pressure levels than those in the listener condition. The experimental role of curvilinear time interaction effects was significant in all three cardiovascular activity markers and self-reported negative affect (ps < 0.004). At the baseline (before participants were assigned to an experimental role), DBP was higher among participants in the speaker condition, which was not expected. At the preparation and/or stress task phases, the group differences were significant across all cardiovascular activity markers and negative affect. At the recovery phase, DBP remained higher among participants in the speaker condition. Results confirm that giving a speech about the stressful situation that pertains to close relationships and health issues of the partner creates greater physiological and psychological strains than does listening to the speech.
Participants were also randomly assigned to one of two experimental pairing conditions (paired with own partner vs. stranger). As shown in couple-stranger rows in Table 2, the main effect of experimental condition was nonsignificant on all three cardiovascular markers and negative affect [0.17 < Fs(1,42) < 2.48, 0.12 < ps < 0.68]. Overall, being paired with one’s own partner did not produce outcomes that differed from outcomes when being paired with a stranger. As shown in time-by-condition effects columns in Table 2, the experimental condition-by-time interaction effects were marginally significant for DBP (those paired with their own partners increased DBP more than those paired with a stranger while preparing for the stress task) and HR (linear pattern of increases in HR in the couple condition while non-significant linear pattern in the stranger condition). Results suggest that imagining being involved in a car accident is stressful regardless whether the other person involved is a romantic partner or a stranger.
As shown in Table 3, attachment security was negatively related to SBP at the baseline, which tended to remain at both the preparation and stress task phases. A similar effect was also noted in DBP, showing marginally significant linear effect of negative association of attachment security with DBP, which became stronger as the study phases proceeded. However, with regard to self-reported negative affect, attachment security was positively associated at the baseline only. Attachment avoidance was not related to any outcomes studied. Attachment anxiety expressed as worry was positively associated with HR at baseline, which association decreased as the study phases proceeded. Attachment anxiety expressed as a desire to merge was negatively related to DBP at the baseline only and negatively related to NA at the recovery phase only.
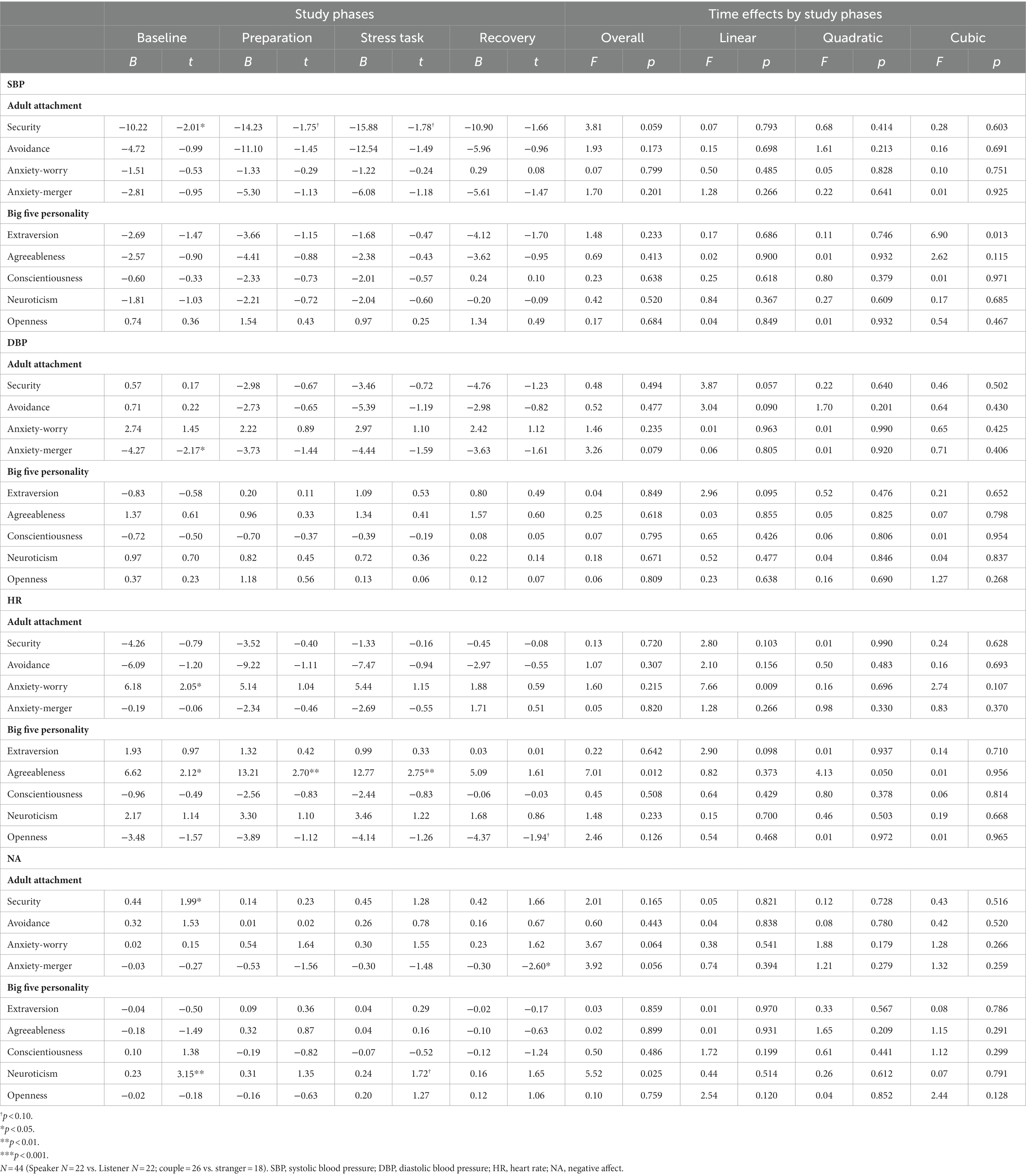
Table 3. Individual difference effects on cardiovascular activity indicators and negative affect.
Among the five major personality factors, extraversion was marginally increased its positive association with DBP and decreased its association with HR as the study phases proceeded. Agreeableness was positively related to HR, which magnitude of association increased from the baseline through stress task phases, then became non-significantly associated at the recovery phase. Conscientiousness was not related to any study outcomes. Neuroticism was positively related to negative affect at the baseline and marginally so at the stress task phase. Finally, openness was marginally negatively related to HR at the recovery phase only. Results suggest cardiovascular and self-reported reactivity to the STITCH task tended to vary by individual characteristics that reflect one’s sensitivity to close relationship-and health-related stress.
The stress a medical illness imposes on the family of the patient and the impact of an illness diagnosis on quality of life and health outcomes can be substantial (Kim and Given, 2008; Kent et al., 2016). There likely are important individual differences in vulnerability to such stresses. However, proper tools to assess reactions to such types of stresses do not exist. Accordingly, we attempted to develop a task to induce stress in the laboratory, using an analog procedure that raises concerns similar to those that naturally arise in the close relationship and health context. Using a laboratory analog in which the same context is presented to everyone, rather than trying to assess stress regulation in the medical setting itself has several benefits. The task, which we call the STITCH task, required participants to visualize either their own romantic partner or a stranger being hurt by a hit-and-run car accident (a proxy situation of a medical illness in the family), or to visualize being the victim of such an accident.
This task proved to induce stress successfully, as evidenced in both cardiovascular activities and self-reported negative affect. Stress induced by the STITCH task provoked empathic cardiovascular and self-reported affect reactivities equally in romantic couples and pairs of strangers. As expected, reactivity was greater among those who were required to speak about the event than among those who had a more passive role. The results from this initial validation study provide sound evidence that the STITCH task can be a useful tool to induce close relationship and health-related stress. The STITCH task could be used to assess the extent to which the patient and family caregiver(s) are able to mutually use each other as resources for stress management. This, in turn, could be used as a predictor of later health outcomes.
Future studies will be fruitful in providing further validation of this newly developed stress induction tool. A particularly interesting direction for further work will be to examine phenomena predicted by relationship theories. For example, some have posited coregulation, in which two members of a dyad mutually calm each other’s reactions to a mutual stress (Butler, 2017; Randall et al., 2021). Elucidating the dyadic regulatory processes involving reactivity to and recovery from such the mutual stressors will help guiding precise and effective management of cardiovascular responses and negative affect for both members in the dyad. Identifying further individual and dyadic differences that moderate physiological and self-reported affective reactions to the STITCH task is also needed.
Validating the STITCH task with populations of medical patients and their caregivers as well as testing discriminant validity will be another important step. Furthermore, only the participants who are assigned to the caregiver role speak in the current STITCH task. Because public speaking per se is a psychological and physiological stressor, adding a phase where those assigned to the patient role also speak would help elucidate the effects of patients vs. caregivers from those of listeners vs. speakers. Finally, we hope to use this task to examine long-term implications of physiological and affective reactivities to the STITCH task in the quality of life and health outcomes of those who had experienced a medically stressful circumstance personally or in the family. Such information will expand current knowledge in understanding the impact of medical illness in the family and shed light on ways in which preventing premature aging and improving public health.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the University of Miami. The patients/participants provided their written informed consent to participate in this study.
YK developed the study concept and contributed to the conceptualization of the research goals and aims, data collection and analysis, and writing and reviewing of the manuscript. CC contributed to the conceptualization of the research goals and aims and writing and reviewing of the manuscript. BH contributed to the conceptualization of the research goals and data collection. All authors contributed to the article and approved the submitted version.
The writing of this manuscript was supported by the National Institute of Nursing Research (R01NR016838) to YK.
The authors extend their appreciation to research assistants of this study: Olajide Bamishigbin, Carrie Brintz, Maria Caruso, Alex Gonzalez, Daniel Hall, Alexis Milton, and Amanda Ting. YK dedicates this research to the memory of Heekyoung Kim.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Beckes, L., and Coan, J. A. (2011). Social baseline theory: the role of social proximity in emotion and economy of action. Soc. Personal. Psychol. Compass 5, 976–988. doi: 10.1111/j.1751-9004.2011.00400.x
Butler, E. A. (2017). Emotions are temporal interpersonal systems. Curr. Opin. Psychol. 17, 129–134. doi: 10.1016/j.copsyc.2017.07.005
Carver, C. S. (1997). Adult attachment and personality: converging evidence and a new measure. Pers. Soc. Psychol. Bull. 23, 865–883. doi: 10.1177/0146167297238007
Chida, Y., and Hamer, M. (2008). Chronic psychosocial factors and acute physiological responses to laboratory-induced stress in healthy populations: a quantitative review of 30 years of investigations. Psychol. Bull. 134, 829–885. doi: 10.1037/a0013342
Chida, Y., and Steptoe, A. (2010). Greater cardiovascular responses to laboratory mental stress are associated with poor subsequent cardiovascular risk status a meta-analysis of prospective evidence. Hypertension 55, 1026–1032. doi: 10.1161/HYPERTENSIONAHA.109.146621
Costa, P. T., and McCrae, R. R. (1992). Revised NEO personality inventory (NEO PI-R) and NEO five-factor inventory: Professional manual. Odessa, FL: Psychological Assessment Resources.
Dias, R. D., and Neto, A. S. (2016). Stress levels during emergency care: a comparison between reality and simulated scenarios. J. Crit. Care 33, 8–13. doi: 10.1016/j.jcrc.2016.02.010
Dickerson, S. S., and Kemeny, M. E. (2004). Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Psychol. Bull. 130, 355–391. doi: 10.1037/0033-2909.130.3.355
Dimsdale, J. E. (2008). Psychological stress and cardiovascular disease. J. Am. Coll. Cardiol. 51, 1237–1246. doi: 10.1016/j.jacc.2007.12.024
Feeney, B. C., and Kirkpatrick, L. A. (1996). Effects of adult attachment and presence of romantic partners on physiological responses to stress. J. Pers. Soc. Psychol. 70, 255–270. doi: 10.1037/0022-3514.70.2.255
Ford, B. Q., Lam, P., John, O. P., and Mauss, I. B. (2018). The psychological health benefits of accepting negative emotions and thoughts: laboratory, diary, and longitudinal evidence. J. Pers. Soc. Psychol. 115, 1075–1092. doi: 10.1037/pspp0000157
Fraley, C. R., and Shaver, P. R. (2000). Adult romantic attachment: theoretical developments, emerging controversies, and unanswered questions. Rev. Gen. Psychol. 4, 132–154. doi: 10.1037/1089-2680.4.2.132
Giannakakis, G., Grigoriadis, D., Giannakaki, K., Simantiraki, O., Roniotis, A., and Tsiknakis, M. (2019). Review on psychological stress detection using biosignals. IEEE Trans. Affect. Comput. 13, 440–460. doi: 10.1109/TAFFC.2019.2927337
Hagger, M. S., and Orbell, S. (2003). A meta-analytic review of the common-sense model of illness representations. Psychol. Health 18, 141–184. doi: 10.1080/088704403100081321
Hazan, C., and Shaver, P. (1987). Romantic love conceptualized as an attachment process. J. Pers. Soc. Psychol. 52, 511–524. doi: 10.1037/0022-3514.52.3.511
Kent, E. E., Rowland, J. H., Northouse, L., Litzelman, K., Chou, W. Y., Shelburne, N., et al. (2016). Caring for caregivers and patients: research and clinical priorities for informal cancer caregiving. Cancer 122, 1987–1995. doi: 10.1002/cncr.29939
Kim, Y. (2006). Gender, attachment, and relationship duration on cardiovascular reactivity to stress in a laboratory study of dating couples. Pers. Relat. 13, 103–114. doi: 10.1111/j.1475-6811.2006.00107.x
Kim, Y., and Given, B. A. (2008). Quality of life of family caregivers of cancer survivors: across the trajectory of the illness. Cancer 112, 2556–2568. doi: 10.1002/cncr.23449
Kim, Y., Shaffer, K. M., Rocha-Lima, C., Milton, A., and Carver, C. S. (2016). Exploring the role of ethnicity on perceptions of cancer and physical health recovery during the first year of survivorship. J. Health Psychol. 21, 1331–1338. doi: 10.1177/1359105314552304
Kirschbaum, C., Pirke, K. M., and Hellhammer, D. H. (2004). The Trier social stress test—a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 28, 76–81. doi: 10.1159/000119004
McCrae, R. R., Costa, P. T., and Martin, T. A. (2005). The NEO-PI-3: a more readable revised NEO personality inventory. J. Pers. Assess. 84, 261–270. doi: 10.1207/s15327752jpa8403_05
Nealey-Moore, J. B., Smith, T. W., Uchino, B. N., Hawkins, M. W., and Olson-Cerny, C. (2007). Cardiovascular reactivity during positive and negative marital interactions. J. Behav. Med. 30, 505–519. doi: 10.1007/s10865-007-9124-5
Northouse, L. L., Katapodi, M. C., Song, L. X., Zhang, L. L., and Mood, D. W. (2010). Interventions with family caregivers of cancer patients meta-analysis of randomized trials. CA Cancer J. Clin. 60, 317–339. doi: 10.3322/caac.20081
Pattyn, N., Migeotte, P. F., Neyt, X., van den Nest, A., and Cluydts, R. (2010). Comparing real-life and laboratory-induced stress reactivity on cardio-respiratory parameters: differentiation of a tonic and a phasic component. Physiol. Behav. 101, 218–223. doi: 10.1016/j.physbeh.2010.04.037
Pietromonaco, P. R., and Beck, L. A. (2019). Adult attachment and physical health. Curr. Opin. Psychol. 25, 115–120. doi: 10.1016/j.copsyc.2018.04.004
Randall, A. K., Tao, C., Leon, G., and Duran, N. D. (2021). Couples’ co-regualtion dynamics as a function of perceived partner dyadic coping. Anxiety Stress Coping 34, 597–611. doi: 10.1080/10615806.2021.1912740
Robles, T. F., Slatcher, R. B., Trombello, J. M., and McGinn, M. M. (2014). Marital quality and health: a meta-analytic review. Psychol. Bull. 140, 140–187. doi: 10.1037/a0031859
Schneider, T. R., Rench, T. A., Lyons, J. B., and Riffle, R. R. (2012). The influence of neuroticism, extraversion and openness on stress responses. Stress Health 28, 102–110. doi: 10.1002/smi.1409
Slavich, G. M. (2016). Life stress and health: a review of conceptual issues and recent findings. Teach. Psychol. 43, 346–355. doi: 10.1177/0098628316662768
Steptoe, A., Hamer, M., and Chida, Y. (2007). The effects of acute psychological stress on circulating inflammatory factors in humans: a review and meta-analysis. Brain Behav. Immun. 21, 901–912. doi: 10.1016/j.bbi.2007.03.011
STITCH Scenario (Individualized with “Chris” = Survivor; “Robin” = Caregiver).
Keywords: stress induction tool, close relationships, health, experimental design, cardiovascular reactivity, negative affect, individual differences
Citation: Kim Y, Carver CS and Hurwitz BE (2023) Developing a stress induction tool relevant to relationships in a health context. Front. Psychol. 14:1103081. doi: 10.3389/fpsyg.2023.1103081
Edited by:
Wendy Birmingham, Brigham Young University, United StatesReviewed by:
Marina Mondo, University of Cagliari, ItalyCopyright © 2023 Kim, Carver and Hurwitz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Youngmee Kim, ✉ eWtpbUBtaWFtaS5lZHU=
†Deceased
‡ORCID: Youngmee Kim, https://orcid.org/0000-0002-3109-6362
Charles S. Carver, https://orcid.org/0000-0002-3688-8545
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.