
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 25 April 2023
Sec. Health Psychology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1099419
 Catarina Tomé-Pires1,2*
Catarina Tomé-Pires1,2* Enric Aragonès2,3
Enric Aragonès2,3 Concepción Rambla2,3Germán López-Cortacans2,3
Concepción Rambla2,3Germán López-Cortacans2,3 Elisabet Sánchez-Rodríguez4,5,6Antonia Caballero2,3
Elisabet Sánchez-Rodríguez4,5,6Antonia Caballero2,3 Jordi Miró4,5,6
Jordi Miró4,5,6Background and aims: Self-management interventions have the potential to improve patient’ pain condition as they involve tasks aimed at managing symptoms and reducing interference with activities, mood and relationships due to pain. However, research on factors that facilitate or hinder pain self-management has overlooked patients with both chronic musculoskeletal pain and depression in primary care settings, also leaving unattended patient views on the usefulness of such programs. Thus, the main aim of this study was to gather meaningful information to help promoting adequate self-management. Specifically, it attempts to identify patients’ perceptions of barriers and facilitators of group-based psychoeducational intervention and to explore its perceived usefulness in promoting self-management.
Method: This qualitative study explored perceived barriers and facilitators of a psychoeducational intervention for the management of chronic musculoskeletal pain and depression previously tested in a Randomized Control Trial. We conducted focus groups and individual interviews with fifteen adult patients with both chronic musculoskeletal pain and depression recruited from primary care centres in Tarragona province (Catalonia, Spain). A content thematic analysis was carried out to examine the data. This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Results: Findings revealed that perceived barriers included lack of motivation, time constraints, pain, depression, ineffectiveness of pain-relief strategies and activity avoidance. Facilitators were having a supportive family/friends, the positive effects of self-management, high motivation, being a proactive patient. Peer support and identification, the positive effect of sessions, and free expression were highlighted as key elements of the psychoeducational intervention.
Conclusion: The psychoeducational intervention was perceived as useful in promoting self-management practices. Barriers and facilitators in using self-management strategies were related, mainly, to internal personal characteristics of the patients being similar among different cultural backgrounds and distinct chronic conditions.
Implications: These findings can help to guide clinicians in the development and implementation of more effective pain self-management interventions for patients with chronic pain and depression by attending to their needs and preferences.
Chronic pain is a major health problem that can have deleterious effects on individuals’ physical, social and psychological functioning (Breivik et al., 2013; Burke et al., 2015; Dueñas et al., 2016). It is estimated that between 30 and 50% of people with chronic pain have depression (Bair et al., 2003; Dueñas et al., 2015; Zartaloudi et al., 2020). Both chronic pain and depression are common and relevant conditions in primary care patients (Fernández et al., 2010; Serrano-Blanco et al., 2010; Barrett and Chang, 2016; Dueñas et al., 2016).
Effective pain self-management has been established as a key therapeutic goal for individuals with chronic pain (Lukewich et al., 2015; Gordon et al., 2017; Devan et al., 2018; Fu et al., 2018; López-López et al., 2020). Multidisciplinary pain programmes encourage patients to learn and use self-management skills to cope with pain and its effects on function (Loeser and Turk, 2001; Ehde et al., 2014; Takahashi et al., 2018, 2019; Vanhaudenhuyse et al., 2018; Vartiainen et al., 2019; Nees et al., 2020). Results from clinical-based studies (e.g., arthritis, back pain, neck pain, fibromyalgia) repeatedly show that self-management leads to better clinical outcomes (e.g., reduce pain intensity and psychological distress) (Newman et al., 2004; Barlow et al., 2009; Devan et al., 2018).
Previous studies have shown that common barriers to the use of pain self-management strategies are related to individuals’ internal personal characteristics, as for example, fear of movement due to pain (Austrian et al., 2005; Bair et al., 2009; Lukewich et al., 2015; Mann et al., 2017), low self-efficacy (Gordon et al., 2017), sustained motivation (Matthias et al., 2016; Gordon et al., 2017; Devan et al., 2018), over-reliance on medication (Bair et al., 2009; Gordon et al., 2017), pain and depression interference (Austrian et al., 2005; Jerant et al., 2005; Lukewich et al., 2015; Craner et al., 2016; Gordon et al., 2017; Mann et al., 2017; Devan et al., 2018) and also external, as poor patient-physician communication (Jerant et al., 2005; Lukewich et al., 2015; Gordon et al., 2017; Mann et al., 2017), time constraints (Austrian et al., 2005; Bair et al., 2009; Fu et al., 2018), lack of close support (Jerant et al., 2005; Bair et al., 2009; Gordon et al., 2017; Devan et al., 2018), and limited treatment options (Austrian et al., 2005; Jerant et al., 2005; Park et al., 2013). In contrast, facilitators to chronic pain self-management have been briefly addressed in the literature, reporting internal personal characteristics of patients as, for example, self-discovery (Devan et al., 2018), beliefs about treatment benefits (Park et al., 2013), high self-esteem (Craner et al., 2016), and external characteristics as supportive family or friends (Park et al., 2013; Lukewich et al., 2015; Craner et al., 2016; Matthias et al., 2016; Mann et al., 2017; Devan et al., 2018), having economic resources (Park et al., 2013), and access to healthcare services (Lukewich et al., 2015; Mann et al., 2017).
Although chronic pain is a common health problem encountered in primary care (Fernández et al., 2010; Serrano-Blanco et al., 2010; Gordon et al., 2017), programmes supporting self-management are often difficult to implement in such context (Warsi et al., 2003; Turk et al., 2008). Therefore, supporting self-management of chronic pain in primary care is challenging as optimal self-management may be difficult to achieve (Newman et al., 2004; Lukewich et al., 2015; Gordon et al., 2017). In fact, we recently noticed several challenges in the implementation and testing of a pain self-management multicomponent programme (RCT) conducted in primary care centres. Despite its clinical improvements (e.g., lower depression levels) we observed a low adherence to the intervention. Furthermore, a deep analysis is required to understand what facilitates and hampers self-management interventions in this specific setting calling into attention the need to consider a patient-centered approach (Jayadevappa and Chhatre, 2011; Lin et al., 2020).
A closer look to the literature on barriers and facilitators to pain self-management reveals several gaps and shortcomings. Therefore, this problem is still insufficiently explored. First, most studies have relied on samples of adults with various chronic pain conditions (e.g., Jerant et al., 2005; Park et al., 2013; Devan et al., 2018) making it difficult to distinguish whether recommendations are valid for specific chronic pain conditions. Second, only a few studies specifically investigated patients with chronic musculoskeletal pain attending primary care settings, including those with comorbid depression (Bair et al., 2009; Damush et al., 2016). Third, research in this field remains limited to Anglo-Saxon countries evidencing the need to explore more cultural backgrounds. Forth, studies reporting data on patients’ perceived usefulness of self-management programmes are scarce (Cuperus et al., 2013; Nees et al., 2020) and need further examination. Indeed, pain-related improvements have been found to be influenced by the patients’ perceived treatment helpfulness (Nees et al., 2020).
Based on these previous considerations and filling the research gap in barriers and facilitators to pain self-management, the present study has a 2-fold purpose: (1) to explore what worked (i.e., facilitators) and did not work (i.e., barriers) in the self-management intervention delivered to a sample of Spanish adults with chronic musculoskeletal pain and depression in primary care (Aragonès et al., 2016), and (2) to examine whether the intervention was found useful in promoting self-management practices. Contributions made from this study should be of wide interest and guide pain care practices of healthcare professionals dealing with chronic pain and depression in primary care settings.
This qualitative study is a further analyses after a previous RCT (Aragonès et al., 2016). In this study we used a qualitative descriptive approach and carried out qualitative interviews (i.e., focus groups and individual telephonic interviews), to gather and explore in more depth perceptions of barriers/facilitators and the usefulness of the psychoeducational intervention. As part of the RCT (Aragonès et al., 2019) this study had a clinical trial registration completed on ClinicalTrials.gov (NCT02605278).
Data was collected in eight urban primary care centres located in Salou, Reus, and Tarragona (Catalonia, Spain). The total population of Catalonia is 7,747,709 (Institut d’Estadística de Catalunya, 2023). Catalonia, like other autonomous communities in Spain, has a well-developed public primary care system with universal coverage. This healthcare system operates following the Beveridge model, similar to countries such as United Kingdom, Italy, and Portugal (Salvador-Carulla et al., 2010). It functions via catchment areas and primary care centres staffed by a variety of healthcare professionals (e.g., family physicians/general practitioner, pediatricians, nurses). To ensure continuity and a long-term relationship with patients, healthcare professionals are assigned a stable list of individuals under their care. This primary care system is also linked to hospital outpatient clinics and community mental health centres, which provide specialized outpatient care through referrals from primary care (Borkan et al., 2010; Salvador-Carulla et al., 2010). Further, the psychologist (the first author of the study—CTP—with interest and experience in the pain field) who developed and implemented the psychoeducational programme was based in primary care centres. During the study period, research team members were mainly based in primary care centres and were Assistant Lecturers in Psychology (CTP and ESR), Full Professor (JM), GP physicians (EA,AC and CR) and a Registered Nurse (GLC).
The group-based psychoeducational intervention was based on a cognitive-behavioral orientation organized into nine-weekly sessions of 2 h led by a female psychologist (CTP). Details about the intervention are described in more detail elsewhere (Aragonès et al., 2016, 2019). This psychoeducational intervention was a key component of a multicomponent programme previously tested for the management of chronic musculoskeletal pain and depression (Aragonès et al., 2016). The programme also included: (1) optimized management of depression following a computerized clinical guide for depression and (2) care management activities (periodic clinical monitoring and support of patients). Psychoeducational group sessions took place in the participants’ reference primary care centres and included a presentation of the content to encourage interaction between participants, and the application of learned skills through practice outside the sessions. To engage participants in their own self-management process, we encouraged patients to take a proactive role. We asked them to put into practice some of the learnt exercises, (e.g., to practice breathing or distraction exercises) outside sessions (at home/work). “Homework” was assigned after each session, which was then reviewed at the beginning of each of the following sessions to check possible challenges they faced when performing it. The content of the psychoeducational sessions covered several areas considered relevant in the context of chronic pain management (see Table 1). To facilitate the sessions, a teaching manual was made available, along with other support materials (slide-based presentations, brochures, and forms) to all participants attending the sessions.
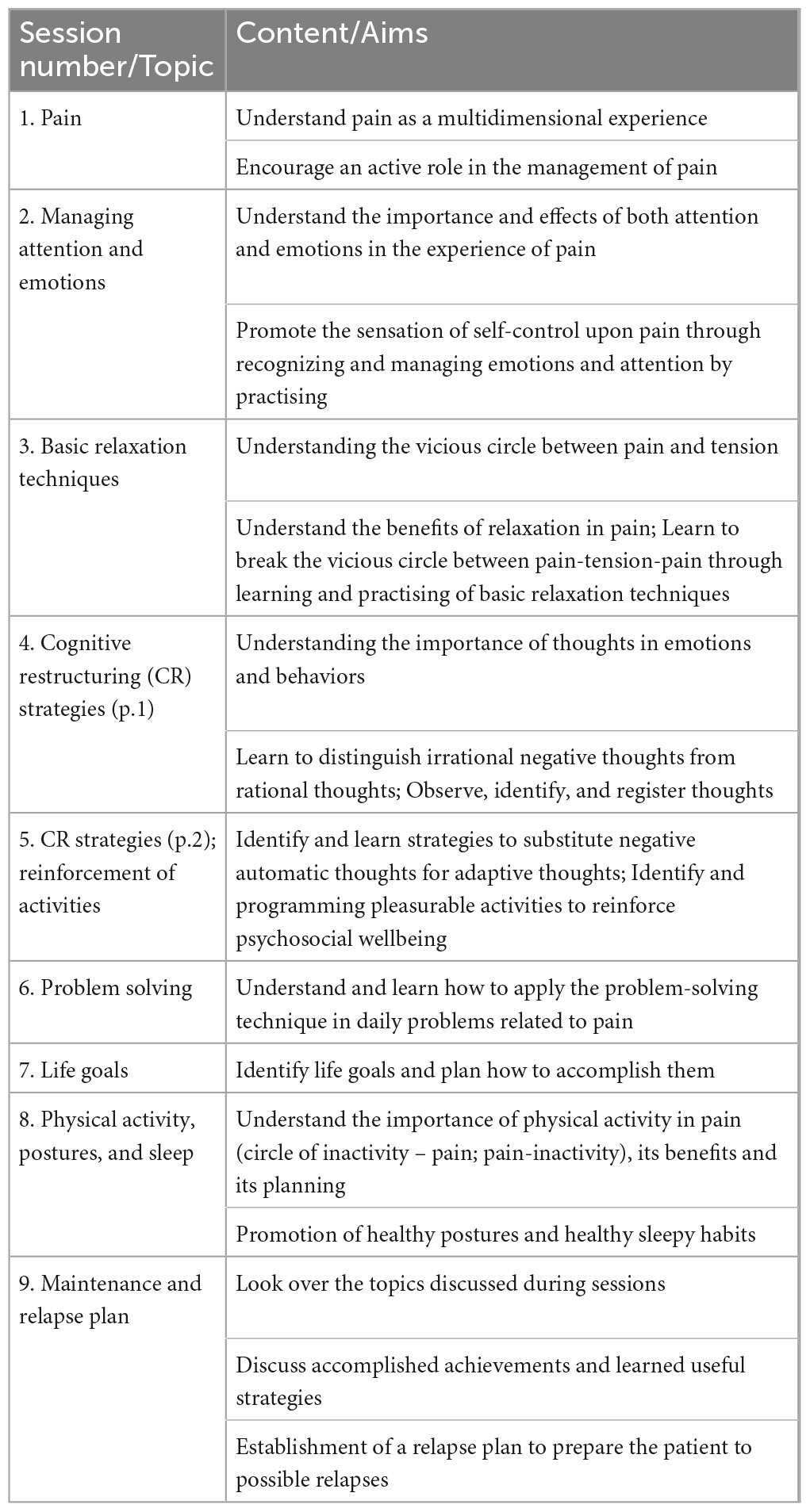
Table 1. Psychoeducational intervention program features.
In this study, we employed interviews as data the collection method (i.e., focus groups and individual interviews) to gain an in-depth understanding of the facilitators, barriers, and usefulness of the psychoeducational intervention as perceived by the participants. Interviews were carried out in a clinical setting, i.e., primary care centres.
Potential participants were recruited from the intervention arm of the RCT testing the clinical effectiveness of a multicomponent intervention in the management of chronic musculoskeletal pain and depression (Aragonès et al., 2016). The intervention arm of the RCT included 167 participants from whom 103 agreed to participate in the psychoeducational sessions. From those 103 participants, 51 attended at least half of the total number of sessions (i.e., 5 out of 9). Participants of this present study (N = 15) were adult patients, with chronic musculoskeletal pain of at least moderate severity [≥5 points in the severity subscale of the Brief Pain Inventory; BPI; (Cleeland and Ryan, 1994; de Andrés Ares et al., 2014) and diagnosed with major depression according to the DSM-5 (American Psychiatric Association, 2013), attending primary care centres in the province of Tarragona (Catalonia, Spain). The BPI is a questionnaire which measures pain intensity with four 0 to 10 numerical rating scales (0 = “no pain” to 10 = “pain as bad as you can imagine”). Respondents are asked to rate their current, worst, least, and average pain in the last week. An overall score of pain severity is obtained by averaging the four BPI pain intensity items].
Ten participants were recruited among those who fully participated in the original RCT and were split into two face-to-face focus groups (five in each group). The other five participants were recruited among patients who had been invited to the RCT but demonstrated little or no adherence to the psychoeducational programme (i.e., these were individuals who attended 0–2 session) and were interviewed individually by telephone. All participants were made aware of the researchers’ motivations for conducting the study.
Participants (N = 10) in the focus groups were selected from the intervention group of the original study (Aragonès et al., 2016). A purposive sampling was used to have access to a particular subset of people with specific characteristics. Their selection was intended to be representative in terms of sex, clinical site (i.e., primary care centre) and rates of attendance at psychoeducational intervention. That is to say, we included both men and women from different primary care centres (from the total of eight) and with different degrees of adherence to the psychoeducational intervention (from 0 to 9 sessions). A study researcher contacted potential participants via telephone. Then, they were informed and invited to participate in the focus group. Participants involved in the focus groups were from distinct psychoeducational groups and they did not know each other. The script for the focus groups was based on the one used by Bair et al. (2009) and then refined according to the aims of the current study (see Table 2). Focus groups were held in meeting rooms of two different primary care centres with sessions lasting approximately 60 min. Both groups had the same moderator (CTP), with whom they had established a relationship prior to the study commencement in the psychoeducational sessions, and two observers (a female psychologist—ESR—and a female nurse) who took notes during the session paying special attention to non-verbal language and verbal coherence. No one else were present besides the participants and researchers. Sessions were audio-recorded and then professionally transcribed. Transcripts were not returned to participants for comment or correction neither provided feedback on the findings. Interviews were not repeated. At the beginning of the session all participants were informed that the session would be recorded for research purposes and were then asked to give their consent to participate in the session.
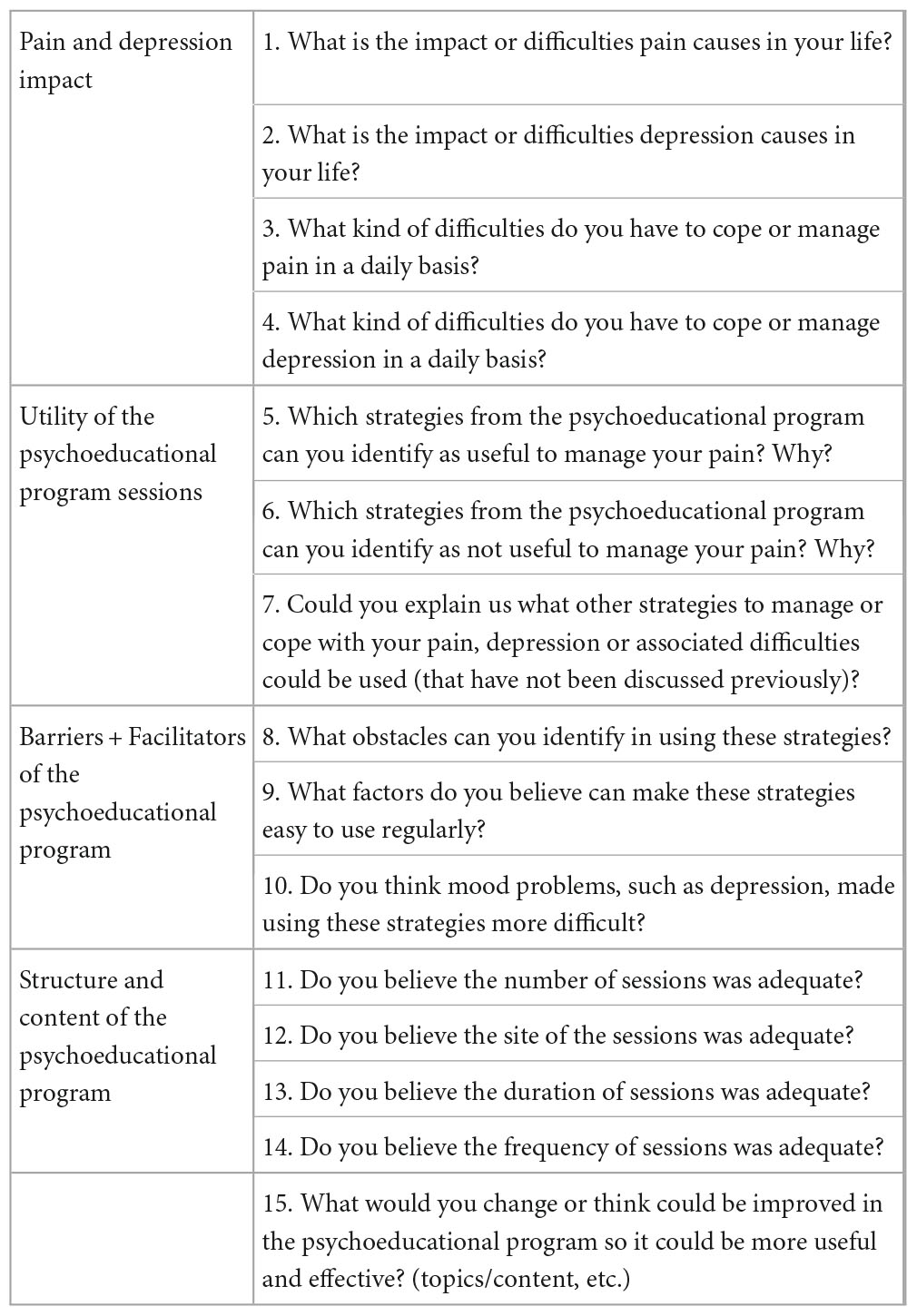
Table 2. Focus group script.
To improve the validity and richness of data collected from the focus groups, we decided to use semi-structured interviews. This data collection method is also an effective tool for gaining a deep understanding of participants’ experiences and perspectives regarding chronic health conditions (Pope et al., 2000). Semi-structured interviews are defined as an exploratory type-interview based on a flexible guide and focused on a main topic that it is to be explored (Magaldi and Berler, 2020). These interviews were found to be a suitable method to obtain data from individuals who were not interested in social interaction and had low adherence to the psychoeducational program. Moreover, conducting interviews via telephone provided greater flexibility. This contrasted with the focus groups, where participants were invited to gather face-to-face with other patients and engage in discussion and socialization. Initially, we had planned to conduct only focus groups to encourage discussion in a social context. However, in order to overcome the aforementioned issues, we had to consider adding another data collection method. Thus, this triangulation approach of informers (i.e., low vs. high adherent) and methodologies (i.e., focus groups and interviews) was used to validate the final themes and provide a higher level of assurance of unbiased interpretation. The interview was based on a framework of themes to be explored and prepared in advance (individuals interview’s questions were based on the focus group script; see Table 3). Inclusion criteria to participate in the telephonic interviews was low adherence participation to the psychoeducational intervention (i.e., only participants that attended 0–2 session). After five interviews we decided we reached relevant data (information was being repetitive) on the main barriers and facilitators to attend a psychoeducational programme and for that reason we decided it would be an appropriate number of participants. Interviews took between 20 and 30 min with an average of 23 min. As in the focus group, individual interviews were recorded with the participants’ permission after informed consent to participate.
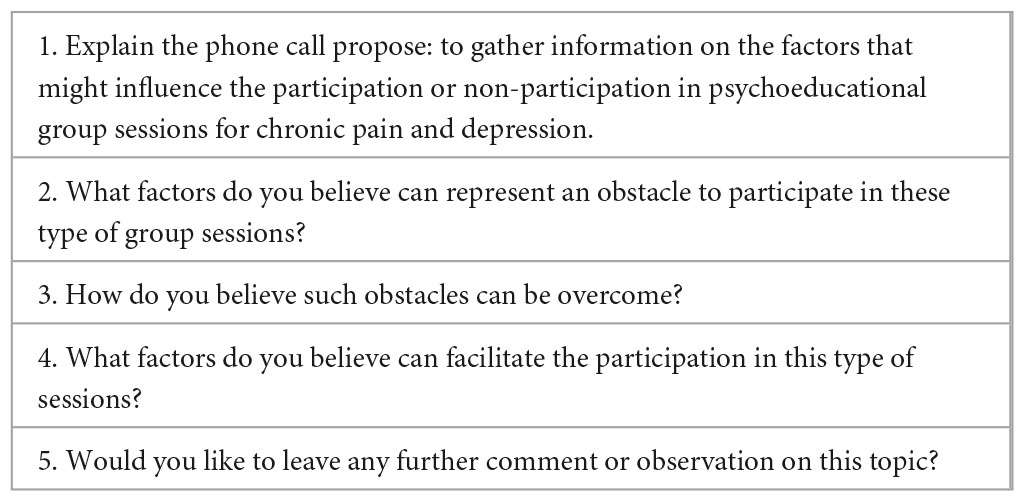
Table 3. Individual semi-structured interview script.
All study procedures were approved by the Research Ethics Committee of the Jordi Gol i Gurina Primary Care Research Institute (IDIAP), Barcelona (Ref: P14/142). All participants gave their informed consent to participate in the original RCT and in this study.
With the focus groups and individual interviews, we performed a content thematic analysis (Pope et al., 2000; Vaismoradi et al., 2016; Neuendorf, 2018). To analyse the data, several analytical steps were carried out: (1) four research team members (i.e., the four first authors—two females and two males) read each transcript independently and created a list of salient and significant participants’ quotes; (2) each researcher identified relevant themes by the creation of a preliminary list of themes reflected in the data; (3) identification of quotes and the preliminary themes were then reviewed and discussed among team members during weekly meetings to formalize an agreed upon code list. We used a mixed-strategy text codification based on previous research (Bair et al., 2009) and codes emerging from the data; (4) creation of preliminary categories grouping the codes by the criterion of analogy. Discrepancies in the choice of codes were resolved by consensus; (5) analysis of each final category, which was done independently by three members of the research team; and (6) drafting of a new text with the results. When analysing the transcripts, authors discussed data saturation and agreed that the data obtained in the two focus groups was enough to reach it. Data saturation was reached when researchers found out that all the needed data have been collected and there was not any new relevant information or data that could be collected from the participants (Guest et al., 2006; Fusch et al., 2018). To generate trustworthy and insightful findings, we solicited input from the research team members to capture similarities and differences in their perspective and generate unanticipated insights. By doing this, we aimed to guarantee the credibility, transferability, dependability and confirmability of the study’s findings (Nowell et al., 2017). Specific attention was given to themes marked by recurrence, repetition and emphasis (Owen, 1984). Data was summarized, grouped into conceptual themes (i.e., categories), and analysed based on standard qualitative research techniques (Crabtree and Miller, 1992). This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., 2007; see Supplementary material).
Socio-demographic and clinical characteristics of the focus group participants (N = 10) are reported in Table 4. Participants’ age ranged between 51 and 72 years old (mean age = 63.5 years old), eight were females. Five participants were married or had a partner, two were single, two were widows and one was divorced. Six participants had primary education, two had secondary education, and two had high school education. Attendance to the psychoeducational sessions (nine in the total) ranged between 6 and 9 sessions with a mean of 7.7 sessions for this group.
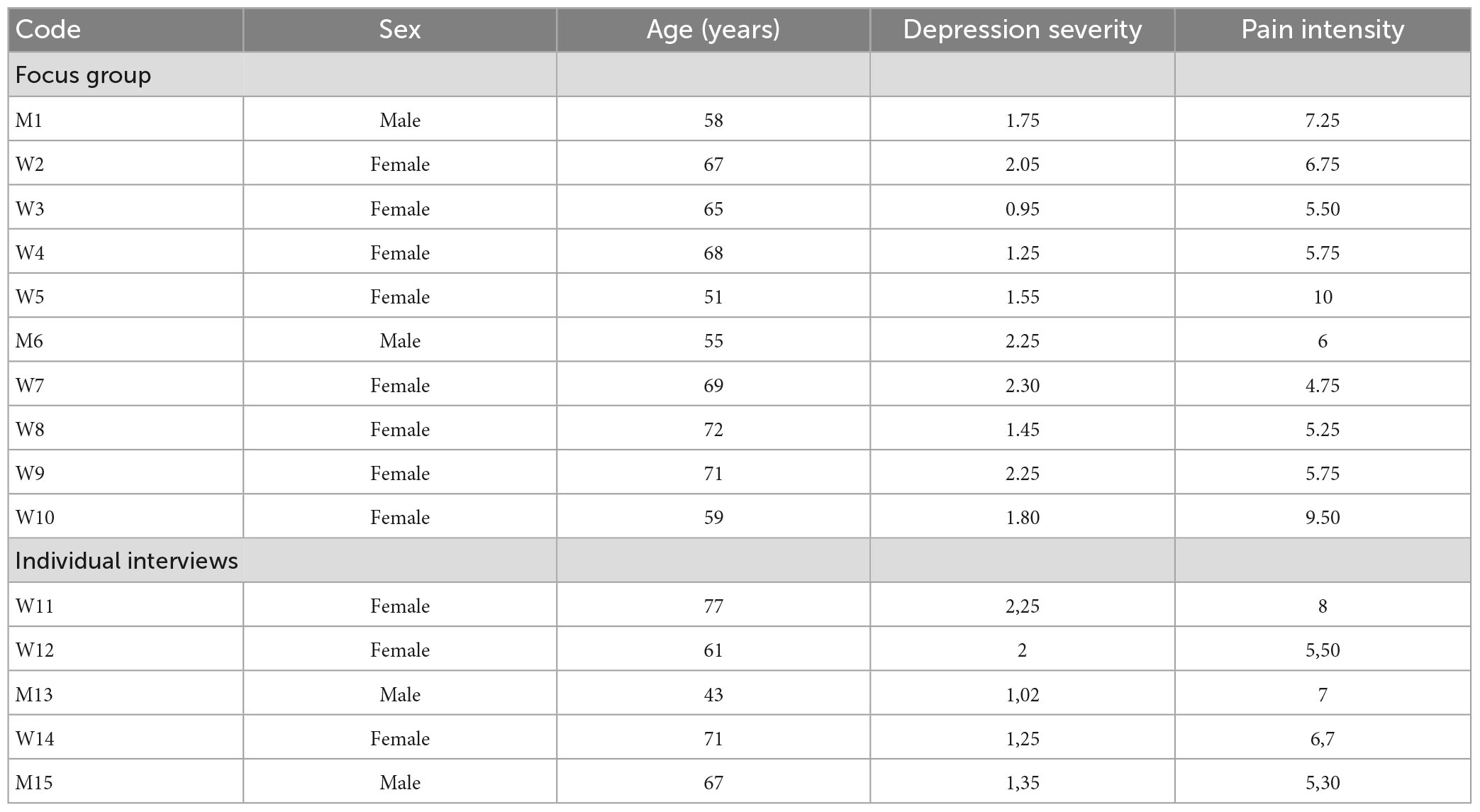
Table 4. Sociodemographics and clinical features of participants.
Participants (N = 5) from the telephonic semi-structured interviews had a low adherence rate that ranged between 0 and 2 sessions with a mean of 0.8 sessions. Participants’ age ranged between 43 and 77 years old (mean age = 63.8 years old) and three were females. Four participants were married or had a partner and one was divorced. Three participants had primary education and two had secondary education, and only one was currently working (Table 4).
Focus groups conducted with the high adherent patients as well as interviews conducted with low adherent patients identified several barriers and facilitators to pain self-management (see Table 5 and Figure 1).
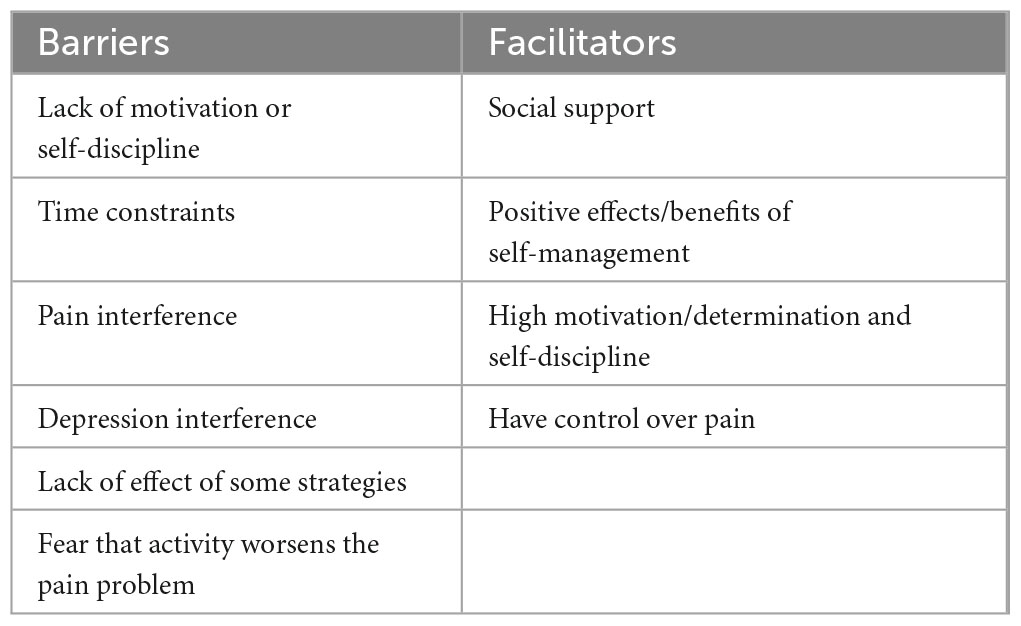
Table 5. Barriers and facilitators to use pain self-management strategies.
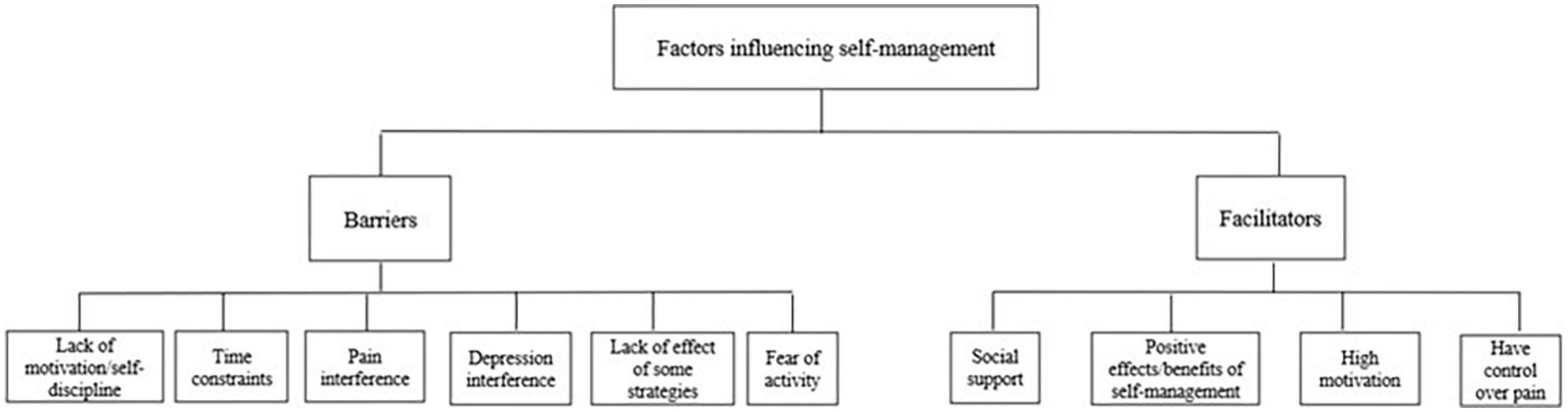
Figure 1. Coding tree for data analysis.
There were identified six categories regarding barriers for the use of pain self-management strategies (see Table 5) that are described below in order of frequency.
Most patients perceived lack of motivation/self-discipline as a key barrier to self-management adherence. Accordingly, poor intrinsic motivation to maintain self-management activities led to difficulties in adhering to them. They felt that their ability to do what needs to be done to improve their pain condition was largely compromised pulling them out from encouragement. Indeed, pain interference appears to compromise internal resources (e.g., motivation) to successful self-management: “Before, I used to do yoga but now I do not do anything. I am very lazy” (W2, high adherent). Nonetheless, they often felt they would improve their pain condition by engaging in such activities: “When the doctor tells you that you have to do rehabilitation then you go, but when I am at home on my own, I keep postponing and postponing doing things that can help to improve my pain, and then the day goes by and nothing is done” (M1, high adherent).
Patients believed that having no time was an important barrier to using self-management strategies. Indeed, self-management of chronic pain happens in a daily basis, and therefore the practical challenges such as the dedication of time to engage in certain activities can be perceived as a critical impediment: “I do not have time to do it. I work 24 h a day” (W10, high adherent); “I have no time for these things (to gather in a group to discuss pain and do things)” (W11, low adherent); “I cannot find time for myself…I always have many things to do” (M15, low adherent). Having to informally take care of someone (e.g., family member, close friend) was also felt as an obstacle to patients taking care of themselves. Accordingly, the sense of responsibility to take care of another person prevented them from being more active in self-managing their own pain condition: “I do not have the time for these things since I have to take care of my grandchildren” (W7, high adherent). Although patients commonly felt time constraints was a significant barrier, there was the perception that the problem was not time itself, but one’s motivation to engage in active self-management: “The problem is not the time, but us, because it is always possible to find 5 min to do something” (W4, high adherent).
The physical and psychological impact of pain was regarded as an important barrier to the use of self-management resources. Patients believed that pain negatively influenced their physical, social, and psychological functioning, and thus, feelings of powerlessness/frustration at the limitations caused by pain were commonly expressed by the patients. Indeed, chronic pain represented a barrier for increasing (physical or mental) or even to perform any activity level: “If I did not have any pain in my knee I could go for a walk or engage in social activities, but since I have it how can I go out? What can I do? Should I cut my leg?” (W5, high adherent); “Pain limits my mental activities a lot” (W7, high adherent); “I have pain all the time (…) no energy to do things” (W15, low adherent).
Patients felt that being in a negative mood and/or with significant depressive symptoms precluded them from engaging in active self-management. Self-management, which involves active participation of the patients themselves, was felt to be compromised by such depressive feelings. Those feelings were felt to impact their ability to proper problem-solving and adaptative coping with pain making it worse: “When I am sad, I do not want to do anything. Now that I see myself like this, unable to do things, I get very sad and then I sink into the sofa. I lose my appetite, I start thinking about who I was before my pain problem, and all this makes my pain worse” (W9, high adherent). Indeed, low motivation and initiative due to depression was perceived as a key barrier to participation in the psychoeducational programme as well as a barrier to adequate self-management: “My depression does not let me do things. I have no joy.” (W14, low adherent).
Although not widely mentioned by the high adherent patients, additional barriers to pain self-management were acknowledged, including the perceived lack of positive effects of self-management strategies. For example, some patients expressed fear that physical activity/exercise or any kind of activity would exacerbate their pain problem. Thus, due to fear of pain and/or reinjury, some patients were fear avoidant and perceived the use of certain strategies as not helpful. These beliefs prevented patients from engaging in active self-management.: “When I exercise my pain gets worse” (M1, high adherent); “If it hurts already, it may hurt even more after exercising” (W5, high adherent). Furthermore, low adherent participants pointed to the format of the psychoeducational programme, which was in group, and to no peer identification as obstacles to participate in self-management programs and strategies: “I don’t want to talk about me in front of others, about my pain and stuff (…). I don’t like group sessions for that reason. I feel others judge me” (W15, low adherent); “In the first session I felt very awkward. I was the youngest one and all the others were very depressed. I felt this was not good for me, for my pain (.) to suffer in group” (M13, low adherent).
Participants were able to identify factors that acted as facilitators in the use of self-management strategies (see Table 5). Four categories of facilitators were mentioned. The most common ones are presented below in decreasing order of frequency.
Support from family, friends or peers was the most common cited enabler that patients believed helped them to engage in pain relief strategies. Social support, i.e., support/social resources perceived by the patient to be available or provided within the context of informal (family, friends) or formal (peers, i.e., support group) relationships, was felt to play an important role in self-management. It appeared to increase patients’ self-efficacy, adaptative coping, and activation. Therefore, it encouraged them to become more proactive in implementing pain self-management practices. Family was viewed as a strong source of support: “I have my husband and my son that understand my situation and are the only ones who give me support” (W9, high adherent), as well as friends and peers: “I need someone to cheer me up” (W8, high adherent); “The opinions of others also helped a lot” (W9, high adherent).
Having benefits from using pain relief strategies was perceived as another important facilitating factor. According to the patients, such benefits emerged as a positive reinforcer to foster their pain self-management promoting high adherence to recommendations: “If I have pain, I benefit from doing things that help my pain, so it is for my own benefit” (W8); “If it is something that works for me I do it and that’s it” (W4).
While lack of motivation and discipline was perceived as a barrier to self-management, the presence of high motivation and sense of self-discipline was perceived as a significant factor in improving self-management. Patient motivation was felt to be particularly relevant to active participation and promotion of adaptive pain self-management: “Motivation and willpower to do it are important. If I cannot do it at 5 p.m., I will do it at 7 p.m., but I will do it. I have to find my time” (W4, high adherent); “You always have time to do it. You have to take your time” (W7, high adherent).
This facilitator was not widely discussed but emerged as relevant to some patients. The idea that chronic pain should not be avoided, but, instead, recognized and then controlled was central to some patients. Perceived control over pain refers to an individual’s belief about his/her own capacity of exerting influence on internal states, behaviors, and external environment. It represents a key protective factor for wellbeing as it fosters feelings of useful and worthwhile: “I have to do things. I have to walk” (W4, high adherent); “If I stay at home, I feel useless, worthless. I must go out, see people, and feel I can do things” (W2, high adherent).
Additional facilitators to pain self-management were acknowledged by low adherent participants, such as clinical homogeneity of participants attending the intervention, and individual format of sessions: “(…) In the group we should have similar mental health conditions, not just pain.” (M13, low adherent); “Individual sessions are better for me. I prefer to be alone” (M15, low adherent).
We also aimed to gather information on the different aspects of our psychoeducational programme to understand its usefulness. As mentioned previously patients’ perceptions about the usefulness of the self-management program are scarce. Furthermore, some questions related to the following aspects were also included: usefulness, structure, content, and use of self-management strategies.
Regarding the usefulness of the psychoeducational programme, most patients felt that the program was an important source of social support. Patients mentioned that being in a support group led to positive effects permitting peer identification (i.e., having the same clinical condition), and free expression of feelings and thoughts. Participants believed peer support and positive effects were important ingredients to guarantee the usefulness of the sessions: “What I found best in these sessions was the group, the people, and that you [the professional] dedicated time to explain things that were useful to us” (W7). Several patients stated that being able to compare themselves with others helped them to put their pain in perspective. Being with similar others in a group intervention was felt to be empowering, as it gave a strong sense of normality and connection and helped patients to feel less isolated: “The opinions of others also helped a lot” (W9); “These sessions were useful because we all have pain, and we did not feel alone” (W2). Catharsis was cited as relevant since support group sessions gave the opportunity to freely and openly express emotions and thoughts. They expressed that being listened to in an empathic environment, peer validation and being motivated by others was truly valuable: “The fact that we could talk helped us a lot” (W8).
When asked about the sessions’ structure most patients commented that they would like to have a greater number of sessions. Patients mentioned that they would benefit from a higher number of sessions since it helped them managing pain and feeling good: “We could have had more sessions as I felt really good and the things we learned helped me a lot” (W9). Some mentioned that the duration of sessions should be shorter than 2 h due to their pain and associated discomfort. A patient shared that chairs should be designed around their needs and be more comfortable. Thus, ergonomics was revealed to be critical to the delivery of psychoeducational sessions, which has special importance in the delivery of assistance to pain patients: “The chairs were very uncomfortable” (W9).
In relation to the sessions’ content participants mentioned it was appropriate. However, they suggested additional topics that were perceived as valuable for future self-management programmes. Patients felt the need to discuss the following topics as part of their worries regarding pain management: medication [“It is important to understand the side effects of medication” (M1)], the relationship between the health professional and the patient [“We could had talked about the relationship we have with our doctor” (W7)], sex and pain [“It seems a taboo topic, but I think it would be important to talk about sex since it is really affected by pain” (M6)], and suicide [”Why didn’t we talk about suicide and despair? A person may think about killing herself/himself because she/he cannot stand the pain anymore” (M6)].
During the psychoeducational sessions there were numerous pain control strategies that were discussed together with patients. Some of them were already part of the participants’ repertoire (as for example, physical activity or relaxation techniques), but others not. Most participants mentioned that the most useful learnt strategies for pain relief were those related to relaxation (e.g., breathing exercises), physical activity, attention management (i.e., distraction), and engagement in social activities. Positive benefits attained by practicing those strategies led to the reinforcement of adaptative self-management. The following statements illustrate those strategies’ use and benefits: “I carry on doing the breathing exercises we learned in the sessions and it still helps me. I do it when I go to bed” (M6); “After the psychoeducational sessions I looked for a physical activity and I started my swimming classes, which helped with my pain. to improve it and forget it” (W8).
Self-management is a complex and multifactorial process (de Ridder et al., 2008; Mann et al., 2017; Devan et al., 2018) influenced by several factors. This qualitative study aimed to gain a comprehensive understanding of how chronic pain patients with depression perceived, valued, and experienced pain self-management following a psychoeducational program that was previously tested (Aragonès et al., 2019).
This study found that factors that prevented patients from using self-management strategies were mainly related to the internal personal characteristics of the patients (e.g., lack of motivation) and pain-related issues (e.g., pain interference). Similar outcomes were found in previous research (Bayliss et al., 2003; Austrian et al., 2005; Jerant et al., 2005; Bair et al., 2009; Cuperus et al., 2013; Park et al., 2013; Lukewich et al., 2015; Matthias et al., 2016; Gordon et al., 2017; Mann et al., 2017; Devan et al., 2018) reporting both external and internal barriers. For example, in a study on veterans with musculoskeletal pain, it was found that the main barriers were related to motivation and engagement in the intervention (Matthias et al., 2016), while in other studies low-self-efficacy to manage pain (Mann et al., 2017) and pain interference (Bair et al., 2009) were revealed as the main barriers. In line with previous research, both the emotional and physiological effects of chronic disease were perceived as barriers to self-management (de Ridder et al., 2008). Moreover, low adherent participants, highlighted the format (group-based) of the psychoeducational sessions and no peer identification as the main obstacles preventing them to actively engage in self-management. Factors that facilitate self-management were related to the internal personal characteristics of the individuals (high motivation, having control over pain). Perceived facilitators reported by low adherent participants were related to personal characteristics, such as positive emotional state, less pain interference, but also related to features of the intervention itself, such as group patients having similar clinical characteristics, and time availability. Although less reported in the literature, facilitator factors found in this study support previous research on chronic pain self-management (Bair et al., 2009; Cuperus et al., 2013; Park et al., 2013; Matthias et al., 2016; Mann et al., 2017; Devan et al., 2018). For example, in adults with chronic pain positive attitude (Park et al., 2013), which includes, for example, high motivation, positive thinking and enjoyment of non-pharmacological pain management techniques (Wilcox et al., 2006), and self-confidence to manage pain (Mann et al., 2017) emerged as relevant facilitators.
Our study found that challenges and helpful factors for self-management in mixed chronic pain conditions, such as musculoskeletal pain, fibromyalgia or migraine, were more alike than different (Bair et al., 2009; Matthias et al., 2016; Devan et al., 2018; Takahashi et al., 2018). This finding suggests that self-management recommendations could potentially apply to different chronic pain conditions as they face similar challenges managing their pain. Furthermore, our study contributes to the existing literature by extending beyond previous reports that have largely focused on Anglo-Saxon countries.
The findings emphasize the complex and multifactorial nature of self-management. We believe that by including data from patients with varying levels of adherence, our study provides a more comprehensive understanding of the factors that influence self-management. Predictors of self-management were related to self-management delivery format (e.g., individual vs. group-based), for example, but also to psychological variables. Psychological variables, such as depression, motivation and kinesiophobia, were significant determinants of pain self-management and, thus, should be strongly addressed to ensure successful self-management. A recent study emphasized the role of such variables, including catastrophizing, in predicting multiple constructs of self-management (e.g., health-directed activities, skill and technique acquisition) (Banerjee et al., 2022).
Specifically, motivation was found to be the primary factor influencing self-management, which aligns with previous research (Choi et al., 2014; Jung and Jeong, 2016; Matthias et al., 2016). It plays a central role in determining how effectively patients learn to manage pain and use multiple pain coping strategies (Kerns et al., 2014; Jung and Jeong, 2016). Since self-management requires behavior change, motivation plays a vital role. Most theories and models of human behavior (e.g., social cognitive theories) consider behavior change to be primarily influenced by the perceived importance of behavior change and the belief that behavior change is possible (self-efficacy) (Bandura, 1986; Jensen et al., 2003). Such beliefs contribute to motivation, which in turn, affects behavior. That is well-posed by the motivational model for pain self-management, in which readiness to change behavior or motivation are essential to mediate the connection between a patient’s beliefs and her or his behavior (Jensen et al., 2003; Kratz et al., 2011). Despite motivation is a key predictor of effective self-management, there have been limited studies that explore the impact of motivational approaches intervention in self-management behavior (Molton et al., 2008; Kratz et al., 2011). The data underscore the importance of utilizing and incorporating into pain management treatments, a comprehensive model to understand motivation when pursuing effective self-management trials. Kinesiophobia, was another psychological variable revealed important in our study. In fact, it has also been pointed out as an important predictor of development and maintenance of chronic pain (Vlaeyen and Linton, 2000, 2012; Leeuw et al., 2007; Zale and Ditre, 2015; Gatchel et al., 2016), and self-management (Banerjee et al., 2022). It refers to fear-avoidance, which relates to the avoidance of movement or activities based on fear. Those dysfunctional interpretations can give rise to pain-related fear, and associated safety seeking behaviors such as avoidance/escape and hypervigilance, that can be a problem in long-lasting pain (Leeuw et al., 2007; Gatchel et al., 2016; Racine et al., 2017). In our sample, patients who fear that activity could worsen their pain condition avoided engagement in such activity. In addition, lower mood (i.e., depressive symptoms) was associated with poorer self-management. It appeared to hamper the patients’ ability to self-manage their pain or even to take initiative to adhere do self-management as found in previous literature (Bair et al., 2003; Dueñas et al., 2015; Zartaloudi et al., 2020).
Effective pain self-management involves patients taking an active role in managing their pain condition and being responsible for their own care (Stewart et al., 2014; Jonkman et al., 2016). Patients who participated in the psychoeducational intervention reported that self-management support was critical in learning coping skills to manage their chronic pain more effectively. This finding is not surprising considering previous research on self-management (Newman et al., 2004; Blyth et al., 2005; Devan et al., 2018), however, few pain self-management studies have conducted qualitative evaluations where patients explain, in their own words, what aspects of self-management they found valuable (Nees et al., 2020). Furthermore, the need to understand the patient’s preferences is essential to effective self-management as they are critical to promote a patient-centred care (PCC) perspective. PCC has been suggested as the number one recommendation for best musculoskeletal pain care (Lin et al., 2020) as it involves an emphatic and responsive approach to needs, values and expressed preferences of each individual patient (Rathert et al., 2012). Patients from this study reported that the psychoeducational intervention met their needs with clinical usefulness due to, for example, peer support and free expression of feelings/thoughts. We noticed that probably there was a dose-response in that attending a greater proportion of sessions led to better clinical outcomes. When looking at the different aspects of the intervention, such as the structure and content, patients reported that both were adequate, although they felt that some aspects could be improved for future interventions. Specifically, they pointed out the need to include additional topics pertinent in the context of chronic pain, such as medication side effects, sexual activity, health professional-patient relationship, and suicide. Studies reporting data on such needs are still scarce (Monga et al., 1998; Ambler et al., 2001; Cuperus et al., 2013; Racine et al., 2016) and thus warranted.
Data regarding the use and usefulness of pain self-management strategies from the patients’ views acknowledging such strategies is essential as they reflect an active process of decision-making that combines personal experiences with professional recommendations (Crowe et al., 2010). In this research, the most useful learnt strategies for pain relief were relaxation, physical activity, attention management (i.e., distraction), and engagement on social activities. Such pain self-management coping behaviors (Jensen et al., 2003) were associated with therapeutic benefits in our sample. Our findings are supported by a previous study, which found that preferred coping strategies were those that could be self-administered and included both physical and cognitive elements (Lansbury, 2000). Most common strategies used by participants to manage their chronic pain were medication, exercise, application of heat (Crowe et al., 2010) and resting (Blyth et al., 2005). However, they are contrary to the results reporting that the least-preferred strategies were the conventional treatments of medication, exercise and physiotherapy (Lansbury, 2000). Further studies are required to have a better understanding on the use and effect of specific self-management strategies on pain management.
The present study has some limitations that must be considered when interpreting the results. Participants of this study were mainly female patients. However, future research should attempt to focus on the perspective of male patients to increase the applicability of the study findings. Further, the results were based on the perspective of patients with musculoskeletal chronic pain and depression. Future studies focusing on healthcare professionals’ views in pain self-management are also required to complement the findings.
Despite the study’s limitations, an important strength of this qualitative study is that it is an in-depth analysis of a specific psychoeducational intervention tested previously (RCT) (Aragonès et al., 2019). It is a comprehensive reflection on the obstacles and facilitators that individuals with chronic pain and depression face when coping with pain. Enhancing patient self-management skills can improve pain-related outcomes (Von Korff and Moore, 2001; Damush et al., 2003; Dixon et al., 2007). Clinical implications relate to the need to address such information when dealing with chronic pain patients and when tailoring interventions, so that interventions become more effective by considering the factors that influence coping behavior. This may help healthcare professionals in their clinical encounters. Future research to determine whether patient centred interventions, motivation enhancement strategies or lower pain-related fear may increase active participation in pain self-management treatment programmes is warranted.
The psychoeducational intervention was perceived as useful in promoting self-management. The findings show that pain self-management barriers and facilitators were mainly related to internal personal characteristics of the patients being similar among different cultural backgrounds and distinct chronic conditions. Thus, if confirmed, these data suggest that effective primary care self-management programmes for patients with both chronic musculoskeletal pain and depression would improve from focusing on these results. However, additional longitudinal and experimental studies are needed to evaluate the benefits of this possibility.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Research Ethics Committee of the Jordi Gol i Gurina Primary Care Research Institute (IDIAP), Barcelona (Ref: P14/142). The patients/participants provided their written informed consent to participate in this study.
CT-P, EA, CR, GL-C, ES-R, AC, and JM contributed to conducting the underlying research (data collection and analyses) and drafting this manuscript. All authors contributed to the article and approved the submitted version.
This work was primarily funded by a research grant from the Carlos III Health Institute of Spain’s Ministry of the Economy and Competitiveness, under Health Strategy Action 2013–2016 (PI14/00573) and with co-funding from the European Regional Development Fund. A research award was also received from the Catalan Society of Family and Community Medicine (2015). EA received a grant for intensification of research activity from the Carlos III Health Institute (INT15/00232). EA and GL-C have benefited from grants for intensification of research activity from the IDIAP Jordi Gol. CR received a predoctoral grant from the IDIAP Jordi Gol (7Z16/008, 2015). JM’s work was funded by grants from the Catalan Agency for Management of University and Research Grants (AGAUR; Ref.: 2021SGR-730), Universitat Rovira i Virgili (PFR program), the Spanish Ministry of Economy, Industry and Competitiveness (RTI2018-09870-B-I00; RED2018-102546-T), the European Regional Development Fund (ERDF), Fundación Grünenthal, and ICREA Acadèmia.
We thank the help and support of Enriqueta Pujol Ribera, Mariona Pons i Vigués, and Anna Berenguera Ossó in the data analyses.
EA has received honoraria as a speaker or consultant from Lundbeck and Esteve.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1099419/full#supplementary-material
Ambler, N., De, C., Williams, A. C., Hill, P., Gunary, R., and Cratchley, G. (2001). Sexual difficulties of chronic pain patients. Clin. J. Pain 17, 138–145. doi: 10.1097/00002508-200106000-00006
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edit. Arlington, VA: APA. doi: 10.1176/appi.books.9780890425596
Aragonès, E., López-Cortacans, G., Caballero, A., Piñol, J., Sánchez-Rodríguez, E., Rambla, C., et al. (2016). Evaluation of a multicomponent programme for the management of musculoskeletal pain and depression in primary care: a cluster-randomised clinical trial (the DROP study). BMC Psychiatry 16:69. doi: 10.1186/s12888-016-0772-2
Aragonès, E., Rambla, C., López-Cortacans, G., Tomé-Pires, C., Sánchez-Rodríguez, E., Caballero, A., et al. (2019). Effectiveness of a collaborative care intervention for managing major depression and chronic musculoskeletal pain in primary care: a cluster-randomised controlled trial. J. Affect. Disord. 252, 221–229. doi: 10.1016/j.jad.2019.04.004
Austrian, J. S., Kerns, R. D., and Reid, M. C. (2005). Perceived barriers to trying self-management approaches for chronic pain in older persons. J. Am. Geriatr. Soc. 53, 856–861. doi: 10.1111/j.1532-5415.2005.53268.x
Bair, M. J., Matthias, M. S., Nyland, K. A., Huffman, M. A., Stubbs, D. W. L., Kroenke, K., et al. (2009). Barriers and facilitators to chronic pain self-management: a qualitative study of primary care patients with comorbid musculoskeletal pain and depression. Pain Med. 10, 1280–1290. doi: 10.1111/j.1526-4637.2009.00707.x
Bair, M. J., Robinson, R. L., Katon, W., and Kroenke, K. (2003). Depression and pain comorbidity. Arch Intern. Med. 163:2433. doi: 10.1001/archinte.163.20.2433
Bandura, A. (1986). Social Foundations of Thought and Action: a Social Cognitive Theory. New Jersey: Englewood Cliffs.
Banerjee, A., Hendrick, P., and Blake, H. (2022). Predictors of self-management in patients with chronic low back pain: a longitudinal study. BMC Musculoskelet Disord. 23:1071. doi: 10.1186/s12891-022-05933-2
Barlow, J., Turner, A., Swaby, L., Gilchrist, M., Wright, C., and Doherty, M. (2009). An 8-yr follow-up of arthritis self-management programmeparticipants. Rheumatology 48, 128–133. doi: 10.1093/rheumatology/ken429
Barrett, K., and Chang, Y. P. (2016). Behavioral interventions targeting chronic pain, depression, and substance use disorder in primary care. J. Nurs. Scholarsh. 48, 345–353. doi: 10.1111/jnu.12213
Bayliss, E. A., Steiner, J. F., Fernald, D., Crane, L. A., and Main, D. S. (2003). Descriptions of barriers to self-care by persons with comorbid chronic diseases. Ann. Fam. Med. 1, 15–17. doi: 10.1370/afm.4
Blyth, F. M., March, L. M., Nicholas, M. K., and Cousins, M. J. (2005). Self-management of chronic pain: a population-based study. Pain 113, 285–292. doi: 10.1016/j.pain.2004.12.004
Borkan, J., Eaton, C. B., Novillo-Ortiz, D., Rivero Corte, P., and Jadad, A. R. (2010). Renewing primary care: lessons learned from the Spanish health care system. Health Aff. 29, 1432–1441. doi: 10.1377/hlthaff.2010.0023
Breivik, H., Eisenberg, E., and O’brien, T. (2013). The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 13:1229. doi: 10.1186/1471-2458-13-1229
Burke, A. L. J., Mathias, J. L., and Denson, L. A. (2015). Psychological functioning of people living with chronic pain: a meta-analytic review. Br. J. Clin. Psychol. 54, 345–360. doi: 10.1111/bjc.12078
Choi, S., Song, M., Chang, S. J., and Kim, S. A. (2014). Strategies for enhancing information, motivation, and skills for self-management behavior changes: a qualitative study of diabetes care for older adults in Korea. Patient Prefer Adherence 8, 219–226. doi: 10.2147/PPA.S58631
Cleeland, C., and Ryan, K. (1994). Pain assessment: global use of the brief pain inventory. Ann. Acad. Med. Singapore 23, 129–138.
Crabtree, BF, and Miller, WL (eds). 1992. A Template Approach to Text Analysis: Developing and Using Codebooks. Doing Qualitative Research. Newbury Park, CA: Sage Publications
Craner, J. R., Skipper, R. R., Gilliam, W. P., Morrison, E. J., and Sperry, J. A. (2016). Patients’ perceptions of a chronic pain rehabilitation program: changing the conversation. Curr. Med. Res. Opin. 32, 879–883. doi: 10.1185/03007995.2016.1149053
Crowe, M., Whitehead, L., Jo Gagan, M., Baxter, D., and Panckhurst, A. (2010). Self-management and chronic low back pain: a qualitative study. J. Adv. Nurs. 66, 1478–1486. doi: 10.1111/j.1365-2648.2010.05316.x
Cuperus, N., Smink, A. J., Bierma-Zeinstra, S. M., Dekker, J., Schers, H. J., de Boer, F., et al. (2013). Patient reported barriers and facilitators to using a self-management booklet for hip and knee osteoarthritis in primary care: results of a qualitative interview study. BMC Fam. Pract. 14:181. doi: 10.1186/1471-2296-14-181
Damush, T., Kroenke, K., Bair, M., Wu, J., Tu, W., Krebs, E., et al. (2016). Pain self-management training increases self-efficacy, self-management behaviours and pain and depression outcomes. Eur. J. Pain 20, 1070–1078. doi: 10.1002/ejp.830
Damush, T. M., Weinberger, M., Perkins, S. M., Rao, J. K., Tieney, W. M., Qi, R., et al. (2003). The long-term effects of a selfmanagement program for inner-city, primary care patients with acute low back pain. Arch. Intern. Med. 163, 2632–2638. doi: 10.1001/archinte.163.21.2632
de Andrés Ares, J., Cruces Prado, L. M., Canos Verdecho, M. A., Penide Villanueva, L., del Valle Hoyos, M., et al. (2014). Validation of the short form of the brief pain inventory (BPI-SF) in Spanish patients with non-cancer-related pain. Pain Pract. 15, 643–653. doi: 10.1111/papr.12219
de Ridder, D., Geenen, R., Kuijer, R., and van Middendorp, H. (2008). Psychological adjustment to chronic disease. Lancet 19, 246–255. doi: 10.1016/S0140-6736(08)61078-8
Devan, H., Hale, L., Hempel, D., Saipe, B., and Perry Meredith, A. (2018). What works and does not work in a self-management intervention for people with chronic pain? qualitative systematic review and meta-synthesis. Phys. Ther. 98, 381–397. doi: 10.1093/ptj/pzy029
Dixon, K. E., Keefe, F. J., Scipio, C. D., and Perri, L. M. (2007). Psychological interventions for arthritis pain management in adults: a meta-analysis - database of abstracts of reviews of effects (DARE): quality-assessed reviews - NCBI bookshelf. Health Psychol. 26, 241–250. doi: 10.1037/0278-6133.26.3.241
Dueñas, M., Ojeda, B., Salazar, A., Mico, J. A., and Failde, I. (2016). A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 9, 457–467. doi: 10.2147/JPR.S105892
Dueñas, M., Salazar, A., Ojeda, B., Fernández-Palacín, F., Micó, J. A., Torres, L. M., et al. (2015). A nationwide study of chronic pain prevalence in the general spanish population: identifying clinical subgroups through cluster analysis. Pain Med. 16, 811–822. doi: 10.1111/pme.12640
Ehde, D. M., Dillworth, T. M., and Turner, J. A. (2014). Cognitive-behavioral therapy for individuals with chronic pain efficacy, innovations, and directions for research. Am. Psychol. 69, 153–166. doi: 10.1037/a0035747
Fernández, A., Saameño, J. ÁB., Pinto-Meza, A., Luciano, J. V., Autonell, J., Palao, D., et al. (2010). Burden of chronic physical conditions and mental disorders in primary care. Br. J. Psychiatry 196, 302–309. doi: 10.1192/bjp.bp.109.074211
Fu, Y., McNichol, E., Marczewski, K., and José Closs, S. (2018). The management of chronic back pain in primary care settings: exploring perceived facilitators and barriers to the development of patient–professional partnerships. Qual. Health Res. 28, 1462–1473. doi: 10.1177/1049732318768229
Fusch, P., Fusch, G., and Ness, L. (2018). Denzin’s paradigm shift: revisiting triangulation in qualitative research. J. Soc. Chang 10, 19–32. doi: 10.5590/JOSC.2018.10.1.02
Gatchel, R. J., Neblett, R., Kishino, N., and Ray, C. T. (2016). Fear-avoidance beliefs and chronic pain. J. Orthop. Sport Phys. Ther. 46, 38–43. doi: 10.2519/jospt.2016.0601
Gordon, K., Rice, H., Allcock, N., Bell, P., Dunbar, M., Gilbert, S., et al. (2017). Barriers to self-management of chronic pain in primary care: a qualitative focus group study. Br. J. Gen. Pract. 67, e209–e217. doi: 10.3399/bjgp17X688825
Guest, G., Bunce, A., and Johnson, L. (2006). How many interviews are enough? Field Methods 18, 59–82. doi: 10.1177/1525822X052799
Institut d’Estadística de Catalunya (2023). Estadística oficial de Catalunya. Barcelona: Generalitat de Catalunya.
Jayadevappa, R., and Chhatre, S. (2011). Patient centered care-a conceptual model and review of the state of the art. Open Health Serv. Policy J. 4, 15–25. doi: 10.2174/1874924001104010015
Jensen, M. P., Nielson, W. R., and Kerns, R. D. (2003). Toward the development of a motivational model of pain self-management. J. Pain 4, 477–492. doi: 10.1016/s1526-5900(03)00779-x
Jerant, A. F., Friederichs-Fitzwater, M. M., and von Moore, M. (2005). Patients’ perceived barriers to active self-management of chronic conditions. Patient Educ. Couns. 57, 300–307. doi: 10.1016/j.pec.2004.08.004
Jonkman, N. H., Schuurmans, M. J., Jaarsma, T., Shortridge-Baggett, L. M., Hoes, A. W., and Trappenburg, J. C. A. (2016). Self-management interventions: proposal and validation of a new operational definition. J. Clin. Epidemiol. 80, 34–42. doi: 10.1016/j.jclinepi.2016.08.001
Jung, M. J., and Jeong, Y. (2016). Motivation and self-management behavior of the individuals with chronic low back pain. Orthop. Nurs. 35, 330–337. doi: 10.1097/NOR.0000000000000233
Kerns, R. D., Burns, J. W., Shulman, M., Jensen, M. P., Nielson, W. R., Czlapinski, R., et al. (2014). Can we improve cognitive-behavioral therapy for chronic back pain treatment engagement and adherence? a controlled trial of tailored versus standard therapy. Health Psychol. 33, 938–947. doi: 10.1037/a0034406
Kratz, A. L., Molton, I. R., Jensen, M. P., Ehde, D. M., and Nielson, W. R. (2011). Further evaluation of the motivational model of pain self-management?: coping with chronic pain in multiple sclerosis. Ann. Behav. Med. 41, 391–400. doi: 10.1007/s12160-010-9249-6
Lansbury, G. (2000). Chronic pain management: a qualitative study of elderly people’s preferred coping strategies and barriers to management. Disabil. Rehabil. 22, 2–14. doi: 10.1080/096382800297079-1
Leeuw, M., Elle, M., Goossens, E. J. B., Linton, S. J., Crombez, G., Boersma, K., et al. (2007). The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J. Behav. Med. 30, 77–94. doi: 10.1007/s10865-006-9085-0
Lin, I., Wiles, L., Waller, R., Caneiro, J., Nagree, Y., Straker, L., et al. (2020). Patient-centred care: the cornerstone for high-value musculoskeletal pain management. Br. J. Sports Med. 54, 1240–1242. doi: 10.1136/bjsports-2019-101918
Loeser, J., and Turk, D. (2001). “Multidisciplinary pain management,” in Bonica’s Management of Pain, eds J. Loeser, S. Batler, and C. T. D. Chapman (Philadelphia, PA: Lippincott Williams & Wilkins).
López-López, L., Ariza-Mateos, M. J., Rodríguez-Torres, J., Cabrera-Martos, I., Granados-Santiago, M., Torres-Sánchez, I., et al. (2020). Results of a self-management program added to standard physical therapy in chronic neck pain. Patient Educ Couns. 104, 1438–1444. doi: 10.1016/j.pec.2020.11.014
Lukewich, J., Mann, E., VanDenKerkhof, E., and Tranmer, J. (2015). Self-management support for chronic pain in primary care: a cross-sectional study of patient experiences and nursing roles. J. Adv. Nurs. 71, 2551–2562. doi: 10.1111/jan.12717
Magaldi, D., and Berler, M. (2020). “Semi-structured interviews,” in Encyclopedia of Personality and Individual Differences, eds V. Ziegler-Hill and T. K. Shackelford (Berlin: Springer).
Mann, E. G., Harrison, M. B., LeFort, S., and VanDenKerkhof, E. G. (2017). What are the barriers and facilitators for the self-management of chronic pain with and without neuropathic characteristics? Pain Manag. Nurs. 18, 295–308. doi: 10.1016/j.pmn.2017.04.006
Matthias, M. S., Kukla, M., McGuire, A. B., Damush, T. M., Gill, N., and Bair, M. J. (2016). Facilitators and barriers to participation in a peer support intervention for veterans with chronic pain. Clin. J. Pain 32, 534–540. doi: 10.1097/AJP.0000000000000297
Molton, I. R., Jensen, M. P., Nielson, W., Cardenas, D., and Ehde, D. M. (2008). A preliminary evaluation of the motivational model of pain self-management in persons with spinal cord injury related pain. J. Pain 9:606. doi: 10.1016/j.jpain.2008.01.338
Monga, T. N., Tan, G., Ostermann, H. J., Monga, U., and Grabois, M. (1998). Sexuality and sexual adjustment of patients with chronic pain. Disabil. Rehabil. 20, 317–329. doi: 10.3109/09638289809166089
Nees, T. A., Riewe, E., Waschke, D., Schiltenwolf, M., Neubauer, E., and Wang, H. (2020). Multidisciplinary pain management of chronic back pain: helpful treatments from the patients’ perspective. J. Clin. Med. 9:145. doi: 10.3390/jcm9010145
Neuendorf, K. A. (2018). “Advanced research methods for applied psychology: design, analysis and reporting,” in Advanced Research Methods for Applied Psychology, ed. P. Brough (London: Taylor and Francis Group). doi: 10.4324/9781315517971
Newman, S., Steed, L., and Mulligan, K. (2004). Self-management interventions for chronic illness. Lancet 364, 1523–1537. doi: 10.1016/S0140-6736(04)17277-2
Nowell, L. S., Norris, J. M., White, D. E., and Moules, N. J. (2017). Thematic analysis: striving to meet the trustworthiness criteria. Int. J. Qual. Methods 16, 1–13. doi: 10.1177/1609406917733847
Owen, W. F. (1984). Interpretive themes in relational communication. Quart. J. Speech 70, 274–287. doi: 10.1080/00335638409383697
Park, J., Hirz, C. E., Manotas, K., and Hooyman, N. (2013). Nonpharmacological pain management by ethnically diverse older adults with chronic pain: barriers and facilitators. J. Gerontol. Soc. Work 56, 487–508. doi: 10.1080/01634372.2013.808725
Pope, C., Ziebland, S., and Mays, N. (2000). Qualitative research in health care. Anaysing qualitative data. BMJ 320, 114–116. doi: 10.1136/bmj.320.7227.114
Racine, M., Galán, S., de la Vega, R., Tomé Pires, C., Solé, E., Nielson, W. R., et al. (2017). Pain-related activity management patterns and function in patients with fibromyalgia syndrome. Clin. J. Pain 34, 122–129. doi: 10.1097/AJP.0000000000000526
Racine, M., Sánchez-Rodríguez, E., and Gá Lan, S. (2016). Factors associated with suicidal ideation in patients with chronic noncancer pain. Pain Med. 18, 283–293. doi: 10.1093/pm/pnw115
Rathert, C., Wyrwich, M. D., and Boren, S. A. (2012). Patient-centered care and outcomes: a systematic review of the literature. Med. Care Res. Rev. 70, 351–379. doi: 10.1177/1077558712465774
Salvador-Carulla, L., Costa-Font, J., Cabases, J., McDaid, D., and Alonso, J. (2010). Evaluating mental health care and policy in Spain. J. Ment. Health Policy Econ. 13, 73–86.
Serrano-Blanco, A., Palao, D. J., Luciano, J. V., Pinto-Meza, A., Luján, L., Fernández, A., et al. (2010). Prevalence of mental disorders in primary care: results from the diagnosis and treatment of mental disorders in primary care study (DASMAP). Soc. Psychiatry Psychiatr. Epidemiol. 45, 201–210. doi: 10.1007/s00127-009-0056-y
Stewart, C., Schofield, P., Elliott, A. M., Torrance, N., and Leveille, S. (2014). What do we mean by “older adults” persistent pain self-management”? a concept analysis.” Pain Med. 15, 214–224. doi: 10.1111/pme.12251
Takahashi, N., Kasahara, S., and Yabuki, S. (2018). Development and implementation of an inpatient multidisciplinary pain management program for patients with intractable chronic musculoskeletal pain in Japan: preliminary report. J. Pain Res. 11, 201–211. doi: 10.2147/JPR.S154171
Takahashi, N., Takatsuki, K., Kasahara, S., and Yabuki, S. (2019). Multidisciplinary pain management program forpatients with chronic musculoskeletal pain inJapan: a cohort study. J. Pain Res. 12, 2563–2576. doi: 10.2147/JPR.S212205
Tong, A., Sainsbury, P., and Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 19, 349–357. doi: 10.1093/intqhc/mzm042
Turk, D. C., Swanson, K. S., and Tunks, E. R. (2008). Psychological approaches in the treatment of chronic pain patients—when pills, scalpels, and needles are not enough. Can. J. Psychiatry 53, 213–223. doi: 10.1177/070674370805300402
Vaismoradi, M., Jones, J., Turunen, H., and Snelgrove, S. (2016). Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. Pract. 6, 100–101. doi: 10.5430/jnep.v6n5p100
Vanhaudenhuyse, A., Gillet, A., Malaise, N., Salamun, I., Grosdent, S., Maquet, D., et al. (2018). Psychological interventions influence patients’ attitudes and beliefs about their chronic pain. J. Tradit. Complement. Med. 8, 296–302. doi: 10.1016/j.jtcme.2016.09.001
Vartiainen, P., Heiskanen, T., Sintonen, H., Roine, R. P., and Kalso, E. (2019). Health-related quality of life change in patients treated at a multidisciplinary pain clinic. Eur. J. Pain 23, 1318–1328. doi: 10.1002/ejp.1398
Vlaeyen, J. W. S., and Linton, S. J. (2000). Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain 85, 317–332. doi: 10.1016/S0304-3959(99)00242-0
Vlaeyen, J. W. S., and Linton, S. J. (2012). Topical review fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 153, 1144–1147. doi: 10.1016/j.pain.2011.12.009
Von Korff, M., and Moore, J. C. (2001). Stepped care for back pain: activating approaches for primary care. Ann. Intern. Med. 134(9 Pt 2), 911–917. doi: 10.7326/0003-4819-134-9_part_2-200105011-00016
Warsi, A., LaValley, M. P., Wang, P. S., Avorn, J., and Solomon, D. H. (2003). Arthritis self-management education programs: a meta-analysis of the effect on pain and disability. Arthritis Rheum. 48, 2207–2213. doi: 10.1002/art.11210
Wilcox, S., Der Ananian, C., Abbott, J., Vrazel, J. E., Ramsey, C., Sharpe, P. A., et al. (2006). Perceived exercise barriers, enablers, and benefits among exercising and nonexercising adults with arthritis: results from a qualitative study. Arthritis Care Res. 55, 616–627. doi: 10.1002/art.22098
Zale, E. L., and Ditre, J. W. (2015). Pain-related fear, disability, and the fear-avoidance model of chronic pain. Curr. Opin. Psychol. 5, 24–30. doi: 10.1016/j.copsyc.2015.03.014
Keywords: chronic musculoskeletal pain, pain psychoeducation, depression, primary care, self-management, qualitative study
Citation: Tomé-Pires C, Aragonès E, Rambla C, López-Cortacans G, Sánchez-Rodríguez E, Caballero A and Miró J (2023) Perceived barriers, facilitators and usefulness of a psychoeducational intervention for individuals with chronic musculoskeletal pain and depression in primary care. Front. Psychol. 14:1099419. doi: 10.3389/fpsyg.2023.1099419
Received: 15 November 2022; Accepted: 03 April 2023;
Published: 25 April 2023.
Edited by:
Mohsen Saffari, Baqiyatallah University of Medical Sciences, IranReviewed by:
Tom Kingstone, Keele University, United KingdomCopyright © 2023 Tomé-Pires, Aragonès, Rambla, López-Cortacans, Sánchez-Rodríguez, Caballero and Miró. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catarina Tomé-Pires, Y3BpcmVzQGF1dG9ub21hLnB0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.