 Amirhossein Hashemi1
Amirhossein Hashemi1 Ali Akbar Oroojan
Ali Akbar Oroojan Maryam Rassouli
Maryam Rassouli Hadis Ashrafizadeh
Hadis Ashrafizadeh
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol., 20 April 2023
Sec. Consciousness Research
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1048929
Background and objective: Some individuals report a near-death experience (NDE) after a life-threatening crisis, which refers to a range of subjective experiences related to impending death. This experience is a phenomenon with transcendental elements, which leads to deep permanent changes in both the individual and the social lives of the NDEr's. Therefore, this study aims to review the near-death experiences of individuals with different religious and cultural views.
Methodology: This is a systematic analysis study. All the case report, case series and qualitative research studies which presented patients' NDE experiences were included in the study, without language restrictions, and in the period of 1980–2022. The stages of screening, selection, data extraction, and quality assessment have been gone through by two of the researchers. Data analysis and synthesis has been done qualitatively. JBI Critical Appraisal Checklist tool was used to evaluate the quality of the included studies.
Findings: After the initial search, 2,407 studies were included, 54 of which underwent final examination. The total number of the NDEr's in the studies was 465 men, women, and children. Among these studies, 27 were case reports, 20 were case series, and 7 were qualitative studies. Near-death experiences have been categorized into 4 main categories and 19 subcategories. The main categories include emotional experiences (2 subcategories), cognitive experiences (4 subcategories), spiritual and religious experiences (4 subcategories), and supernatural experiences [9 subcategories in two categories (out of body experiences, and supernatural and metaphysical perceptions)].
Conclusion: The most frequent near-death experiences were supernatural experiences, especially the experience of leaving the body. The basis and the content of the patterns mentioned by the NDEr's are similar, and the differences are in the explanation and the interpretation of the experience. There is a common core among them such as out-of-body experiences, passing through a tunnel, heightened senses, etc. Therefore, correct knowledge of near-death experiences leads to providing helpful answers to patients.
Near-death experiences (NDEs) are deep psychic, conscious, semi-conscious, or recollected experiences of someone who is approaching or has temporarily begun the process of dying which usually occur in life-threatening conditions (Greyson, 2007). In these experiences, the individual seems to be awake, and observes his/her body and the world from a point outside the physical body (Blanke et al., 2009). There are common features such as a feeling of inner peace, out of body experiences, traveling in a dark environment or “void” (usually associated with passing through a tunnel), reviewing one's life from childhood onwards, seeing a bright light, entering an extraterrestrial “other realm,” and communicating with “sentient beings” (Ring, 1980; Greyson, 1983; Moody, 2001; Martial et al., 2017). In a general classification, two factors have been introduced as the origin of these experiences. Van Lommel et al. (2001) and Hess (2019) differentiate between theories that link NDE to physiological changes in the brain and theories which see NDEs as a psychological reaction to approaching death (Van Lommel et al., 2001; Hess, 2019). The previous studies have highlighted the uniqueness of NDE memories in the autobiographical memory (Williams et al., 2008), stating that NDE memories contain more sensory, emotional, and self-referential details in comparison with the memories of other real and imaginary events, or the memories of a coma or impaired consciousness following an acquired brain dysfunction without NDE (Thonnard et al., 2013). Near-death experiences occur in various situations, including cardiac arrest in MI(myocardial infarction) (clinical death), the shocks caused by the blood loss after delivery or in postoperative complications, septic or anaphylactic shocks, electrocution, the coma caused by traumatic brain injury, intracerebral hemorrhage or cerebral infarction, suicide attempts, near drowning or suffocation experiences, apnea, and other cases where death is unavoidable (Van Lommel et al., 2001, 2017). The occurrence of near-death experiences is increasing thanks to improved survival rates through modern medical techniques. The results of a study show that sharing and investigating this phenomenon may happen 5–10 years after the occurrence of the experience, which often prevents the accurate evaluation of physiological and pharmacological factors (Van Lommel et al., 2001). In addition, the results of studies show that the prevalence of this phenomenon in the patients who have gone into cardiac arrest varies between 3.6 and 23% (Parnia et al., 2001; Schwaninger et al., 2002; Klemenc-Ketis et al., 2010). Other retrospective studies have estimated that between 43 and 48% of adults, and 85% of children who have been affected by life-threatening illnesses may have experienced the NDE phenomenon (Ring, 1980; Sabom, 1982; Morse, 2013).
The occurrence of these experiences leads to positive consequences in some NDEr such as a more altruistic life, higher spiritual growth, having interest in the meaning of life, fewer materialistic values, or a reduction in the fear of death (Noyes, 1980; Groth-Marnat and Summers, 1998; Knoblauch et al., 2001; Parnia et al., 2001; Moody, 2005; Khanna and Greyson, 2014a). Their subjective nature and the lack of a clear framework for these experiences make the description and the interpretation of these experiences dependent on individual, cultural, or religious factors (Van Lommel et al., 2017). Near-death experiences vary depending on the survivors' own cultural and religious background (Parnia, 2017), and are almost always described based on the individual's religious beliefs. Most of the early studies on NDEs only depict positive emotions (Ring, 1980, 1984).
Some studies have also mentioned negative experiences in NDEs, including “hellish” ones, although it seems that some NDEr's may still be reluctant to share their experiences (Charland-Verville et al., 2014; Cassol et al., 2019). Numerous quantitative and qualitative studies have been published on patients' experiences of this phenomenon. In the oldest study in this field, Raymond A. Moody compared the continental differences of experiencers (Moody, 2001, 2005; Schlieter and Schlieter, 2018). Combining research results allows qualitative studies to be conducted to reveal new insights or to identify whether subject saturation has occurred (Campbell et al., 2012). In addition to qualitative evidence, the majority of studies have collected quantitative data on patients' experiences through structured questionnaires or interviews. The results of the researches that have been carried out since 1981 in the field of NDE indicate that the treatment staff, especially nurses and doctors, have little knowledge of these experiences, while this knowledge is necessary to identify the NDEr's and help them cope with their experiences (Foster et al., 2009). As it was mentioned, these experiences cause deep and lasting changes in patients' personalities, which highlights the necessity of helping these patients to properly understand and perceive the NDE phenomenon and integrate its consequences (Foster et al., 2009; Van Lommel, 2010).
As far as the knowledge of the researchers allows, no systematic analysis has been designed in this field so far. Due to the fact that different studies have reached different results and the results of these studies have not been certain, so it is necessary to search for a definite result for a correct understanding of this phenomenon. In the present study, prior registration (Priori), data combination, more inclusive search based on the use of thesaurus systems MeSH and Emtree, investigation in large databases such as SCOPUS, WOS, MEDLINE/PubMed, Embase, Google scholar and ProQuest, use From Gray Literature, including: Thesis and conference papers and Proceedings, as well as the use of experts' opinions and the review of key journals, this systematic review can have a more comprehensive review of the relevant subject. Examining these experiences may pose challenges to the researchers of sciences such as psychology, parapsychology, psychiatry, medicine, philosophy of religion, and psychology of religion, each of which requires competent and well-reasoned answers. This systematic review reports a combination of the evidence related to patients' experiences- case reports, case series, and qualitative research- in order to achieve a comprehensive perception of patients' experiences. Considering the potential causes and the unpredictable aspect of this phenomenon, an overview of patients' experiences seems necessary.
This study focused on two specific review questions: (1) “What common experiences regarding the NDEr's accounts of NDE phenomena can be drawn from the results of the existing studies?”, and (2) “What broad knowledge can be gained from the NDEr's accounts of these common experiences?”
This systematic review has been prepared based on the Joanna Briggs Institute Reviewers' Manual (Mcarthur et al., 2015). Furthermore, the process of selecting the primary studies was done based on the PRISMA-P 2015 checklist (Institute of Medicine (US) Committee on Standards for Systematic Reviews of Comparative Effectiveness Research, 2011), and consensus-based clinical case reporting guideline development guidelines (Gagnier et al., 2013).
In the current research, all case reports, case series, and qualitative research studies mentioning near-death experiences have been selected for entering. Other types of studies including cohort studies, case control, cross sectional, review, and clinical trial were not included in this research.
In this study, the eligible population included the individuals who had experienced unavoidable death and NDE without any age, gender, race, or ethnicity restrictions.
Without any language restrictions, studies were searched in PubMed/Medline, Scopus, Medline/Ovid, SPORTD (EBSCO), CENTRAL, and EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Google Scholar search engines from Dec 15, 1980 to June 15, 2022. These were searched in ISI, Scopus, and ProQuest database. The details regarding the process of searching in the PubMed database have been provided below.
(“End Of Life”[tiab] OR End-Of-Life OR[tiab] “Determination of Death”[tiab] OR “Near-Death Experience”[tiab] OR “Out of body Experiences”[tiab] OR “Cardiac Death”[tiab] OR (Death[tiab] AND Cardiac[tiab])) OR “Sudden Cardiac Death”[tiab] OR (“Cardiac Death”[tiab] AND Sudden[tiab]) OR (Death[tiab] AND “Sudden Cardiac”[tiab]) OR “Cardiac Sudden Death”[tiab] OR (Death[tiab] AND “Cardiac Sudden”[tiab]) OR (“Sudden Death”[tiab] AND Cardiac[tiab]) OR “Sudden Cardiac Arrest”[tiab] OR (Arrest[tiab] AND “Sudden Cardiac”[tiab]) OR (“Cardiac Arrests”[tiab] AND Sudden[tiab]) OR (“Cardiac Arrest”[tiab] AND Sudden[tiab]) OR “Brain Death”[tiab] OR (Death[tiab] AND Brain[tiab]) OR “Brain Dead*”[tiab] OR “Coma Depasse”[tiab] OR “Irreversible Coma”[tiab] OR (Coma[tiab] AND Irreversible[tiab]) OR Coma*[tiab] OR Comatose[tiab] OR Pseudocoma*[tiab]) AND 1980/12/15:2022/12/15[dp].
The selection of keywords of this systematic review was done through a combination of Mesh Term, Free Text words, and Emtree. In case of coming across the studies in other languages such as Portuguese, Chinese, Japanese, etc. while searching, Google translation service was used, and for more certainty in this regard, a translator familiar with that language was asked for help. The aim of this study was to obtain all the articles that have been published in the field in order to minimize the risk of publication and reference bias in this article. Besides, PubMed's “My NCBI” (National Center for Biotechnology Information) email alert service was used to identify newly published studies. Manual search including gray literature, the reference list of the primary included studies, and key journals were searched to find more studies. If the researchers came across a study which matched the objectives of the present study, in case of not having access to the full text of the articles, data's being unpublished, or the existence of wrong and ambiguous data, the responsible author of the article would be emailed, and every 1–10 days, three other emails would be sent. The authors of the article were assured that the article would be reported appropriately. If no message was received from the author of the article after 3 emails, the article would inevitably be excluded. The two authors would try to reach an agreement in case of any disagreement, and in case of not reaching an agreement, the opinion of a third knowledgeable individual would be used as the decision criterion.
At first, the studies obtained in the search phase were transferred to the End Note software (× 7), and duplicate articles were removed from the software. Then two researchers (H, A and AH, H) separately reviewed all the primary studies based on the titles and the abstracts of the articles, and presented a number of studies which were in line with the search strategy in order to determine eligible studies based on the inclusion criteria. The selected studies were classified into three categories: relevant, irrelevant, and uncertain. The articles which were reported to be irrelevant by both researchers were excluded from the study, then the same two researchers separately evaluated the obtained studies based on the full texts of the articles. Each researcher provided a list of selected articles and the two lists were compared. In case of any disagreement between the researchers, it would be resolved through discussion and exchange of opinions. In case they could not reach a consensus, a third individual would act as an arbitrator. Then the agreement between the two arbitrators would be evaluated and, after a general agreement, the result would be reported as a statistical Kappa coefficient. According to this, in the present study, there was no disagreement between the two researchers in the steps performed. The agreement coefficient is calculated to be 100%.
The assessment of the risk of bias and the quality of study methodology was performed by two researchers (H, A and AH, H), separately, using JBI Critical Appraisal Checklists for Case Series and Case Reports, and JBI Critical Appraisal Checklist for Qualitative Research (Moola et al., 2020). These tools consist of 10 questions, and each question is answered in 4 ways: yes, no, unclear, and not applicable. Then all the studies were placed in three categories: Low Risk, High Risk, and Moderate Risk of Bias. The researchers tried to reach consensus in case of any disagreement.
Case Series and Case Reports checklist questions included 10 questions, respectively (1−Were there clear criteria for inclusion in the case series? 2−Was the condition measured in a standard, reliable way for all participants included in the case series? 3−Were valid methods used for identification of the condition for all participants included in the case series? 4−Did the case series have consecutive inclusion of participants? 5−Did the case series have complete inclusion of participants? 6−Was there clear reporting of the demographics of the participants in the study? 7−Was there clear reporting of clinical information of the participants? 8−Were the outcomes or follow up results of cases clearly reported? 9−Was there clear reporting of the presenting site(s)/clinic(s) demographic information? 10−Was statistical analysis appropriate.), and the questions of the qualitative checklist included 10 questions (1-Is there congruity between the stated philosophical perspective and the research methodology? 2−Is there congruity between the research methodology and the research question or objectives? 3−Is there congruity between the research methodology and the methods used to collect data? 4−Is there congruity between the research methodology and the representation and analysis of data? 5−Is there congruity between the research methodology and the interpretation of results? 6−Is there a statement locating the researcher culturally or theoretically? 7−Is the influence of the researcher on the research, and vice- versa, addressed? 8−Are participants, and their voices, adequately represented? 9−Is the research ethical according to current criteria or, for recent studies, and is there evidence of ethical approval by an appropriate body? 10- Do the conclusions drawn in the research report flow from the analysis, or interpretation, of the data?) (Moola et al., 2020).
Data extraction was carried out by two researchers (H, A and AH, H), separately, using an information extraction form developed by the researcher. At first, an article was evaluated using this form as pilot evaluation, then it was used for evaluating other articles as well. Each researcher submitted the data extraction form of his articles and the two lists were compared. In case of any disagreement between the researchers, it would be resolved through discussion and exchange of opinions. If consensus was not reached, a third individual would act as an arbitrator, then the agreement between the two arbitrators would be evaluated. The following data be extracted from all studies: the first author's name, the article's year of publication, the country where the study had been done, the type of study design, the number of individuals who had experienced unavoidable death, and the characteristics including age (or age groups), gender, the NDEr's (near-death experiencers) underlying factors, and the type of NDE. The NDEr's quotes in the original studies were required for data analysis in order to preserve the meaning of the original text as a unit interpreted by the authors, or as raw data.
In order to analyze qualitative data, Graneheim and Lundman method was used (Graneheim and Lundman, 2004; Hsieh and Shannon, 2005). Semantic units were extracted from the participants' statements in the form of primary codes. The codes were also classified based on semantic and conceptual similarity and were as small and compressed as possible. There was a downward trend in data reduction in all analysis units and sub- and main classes. Finally, the data were placed in the main classes that were more general and conceptual, and the themes were abstracted. In addition, an example of data analysis has been shown in Table 1.
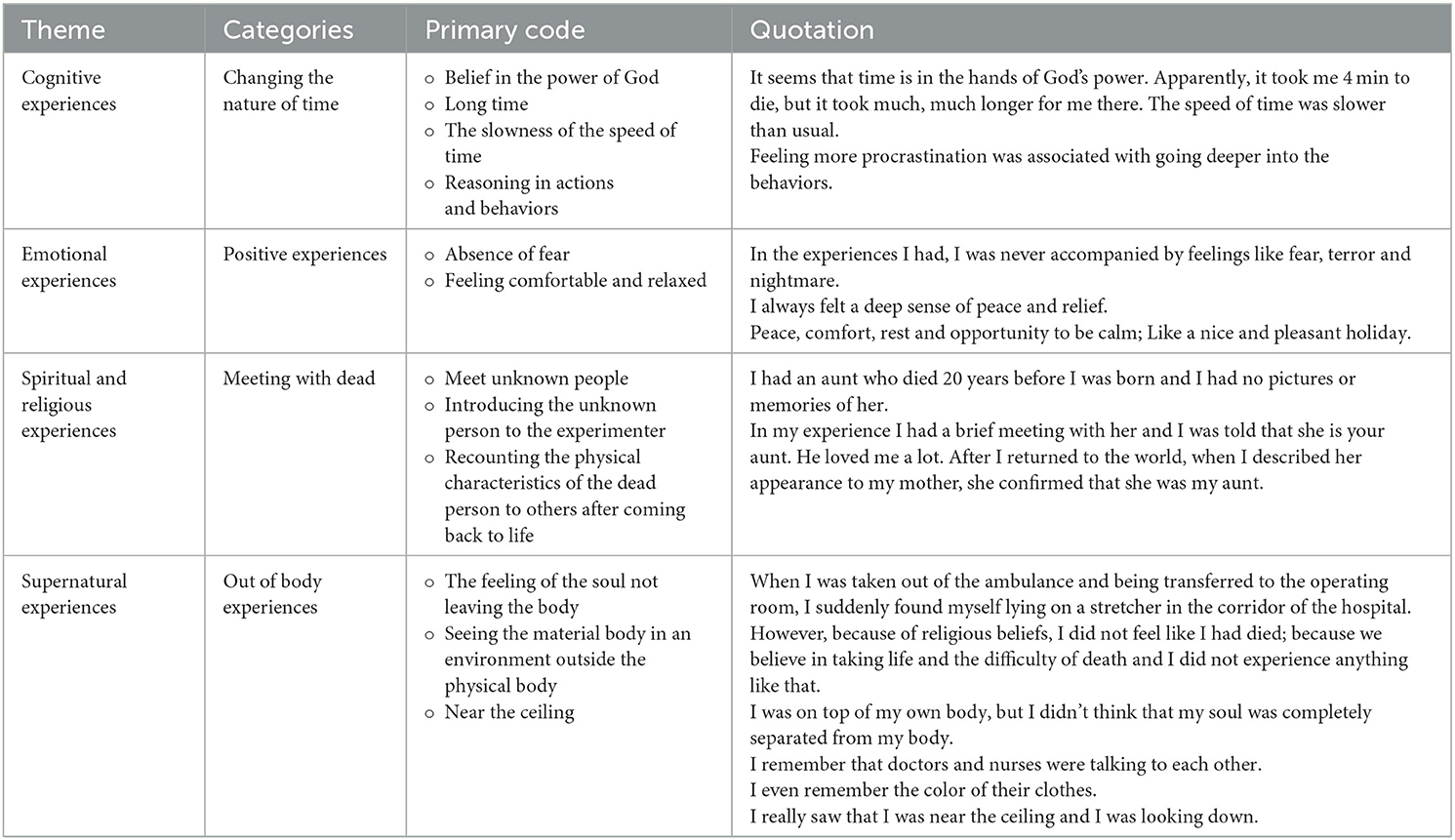
Table 1. An example of data analysis in the main themes.
After searching, 2,407 articles were found. Using Endnote software, the titles and the abstracts of the articles were checked, and 905 duplicate articles were removed. Then the titles and the abstracts of 1,502 articles were examined by the researchers (H, A and AH, H). A total of 1,350 irrelevant articles were excluded based on the study objectives. At this stage, in case of doubting the relevance of an article with the study objectives, the full text of the article was reviewed by the researchers. In the next step, a search was done to access the full texts of the articles and, finally, the full text of 152 articles were reviewed. Considering the inclusion and the exclusion criteria based on the research objectives, some articles were excluded for the reasons given in the Prisma flowchart (Figure 1). To ensure that all the articles had been retrieved, the reference lists of the final articles were also manually searched; no studies were added in this stage. Finally, 54 studies were finalized.
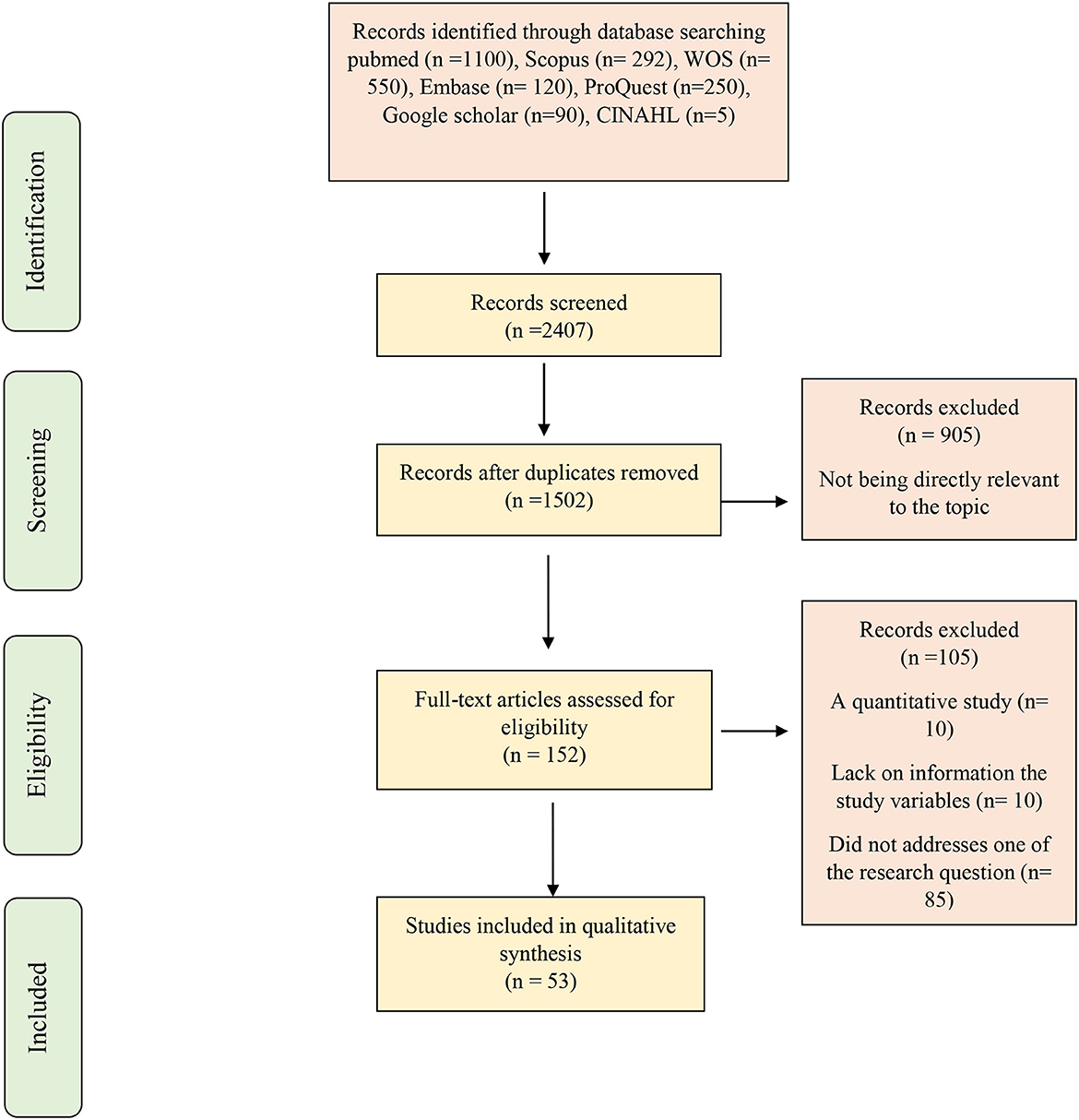
Figure 1. PRISMA schematic flowchart of enrolment and exclusions.
Tables 2, 3 summarizes the characteristics of the included studies. In this table, the name of the first author, the title of the article, the year of publication, the NDEr's characteristics, the NDE's underlying factors, and after-death experiences are stated separately for each study. The studies had been published from 1985 to 2021. The 460 NDEr's included men (n = 126), women (n = 150), children (n = 22) and N/C (n = 162). The studies included 27 case reports, 20 case series, and 7 qualitative studies.

Table 2. Characteristics of the case report studies and background detail of near-death experiencers (N = 27).

Table 3. Characteristics of the case series and qualitative studies and background detail of near-death experiencers (N = 27).
Near-death experiences have been classified into 4 main categories, and 19 sub-categories. The main categories include emotional experiences (2 subcategories), cognitive experiences (4 subcategories), spiritual and religious experiences (4 subcategories), and supernatural experiences (9 subcategories in two categories (out of body experiences, and supernatural and metaphysical perceptions). The Individuals reported heightened senses, in 39 studies and out-of-body experiences, in 35 studies. In 28 studies, the patients reported positive experiences including love, the feeling of peace, and tranquility, and in 6 studies, they reported negative experiences, mostly torture and hellish experiences. Most of the experiences presented by the NDEr's were supernatural and metaphysical experiences, which are shown in Figure 2 and Table 4.
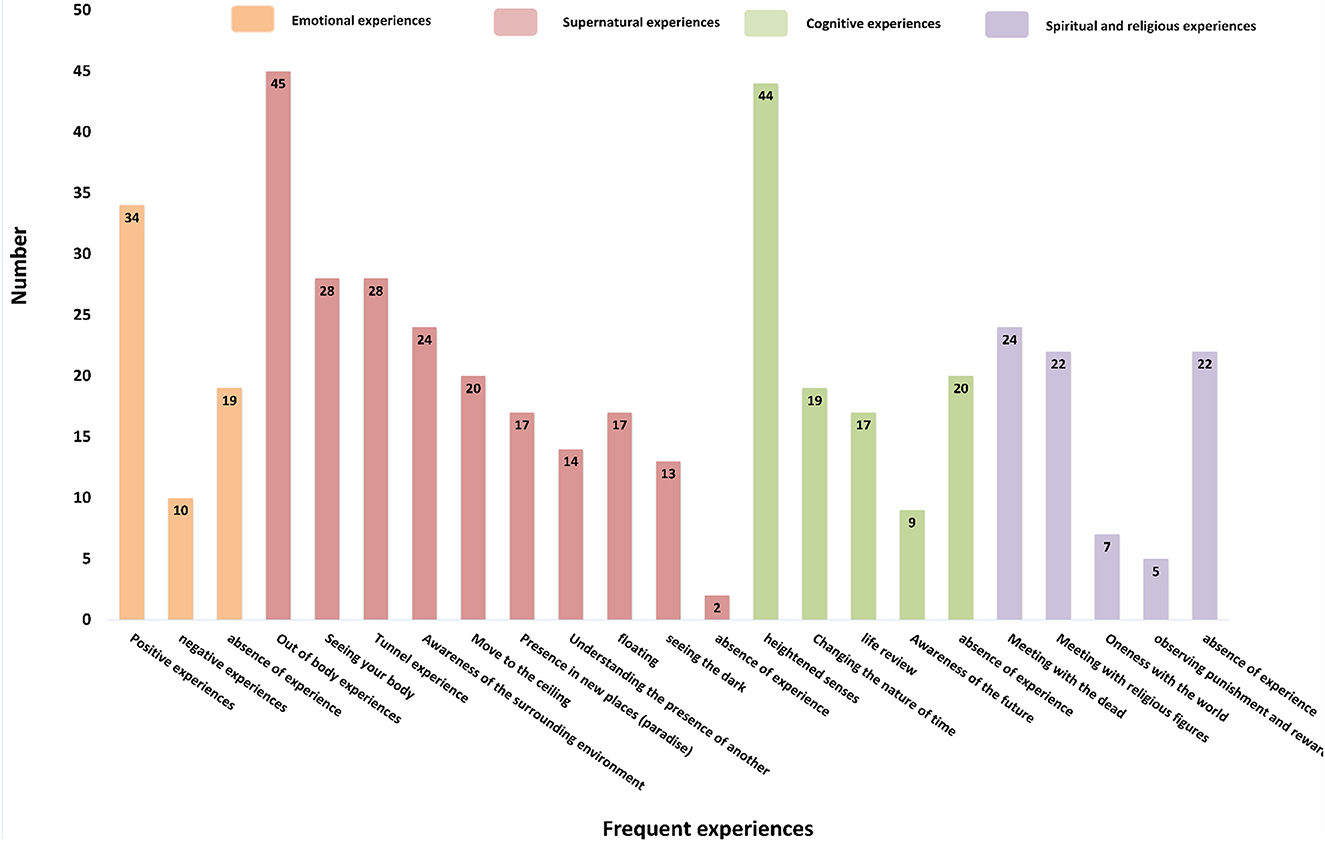
Figure 2. Categorization of individuals who had experienced unavoidable death.
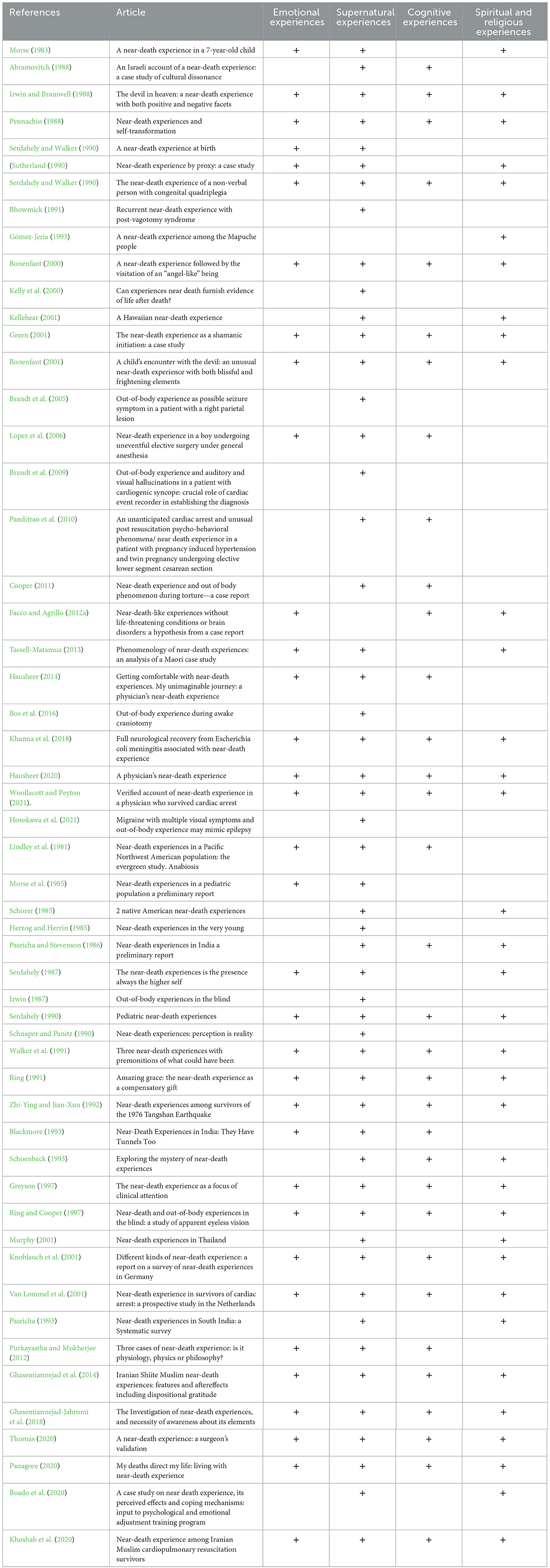
Table 4. The presence or absence of any category of experience in the included studies.
Despite all the differences in methodological design and quality, none of the 21 studies received more than 5 negative ratings; therefore, they were all included (Tables 5, 6). All the studies clearly described their research objectives, used an appropriate research methodology and design, and collected data in a way that answered the research question. In addition, Table 2 examines the quality of studies; 11 studies were of poor quality, 37 of medium quality, and 5 of good quality.
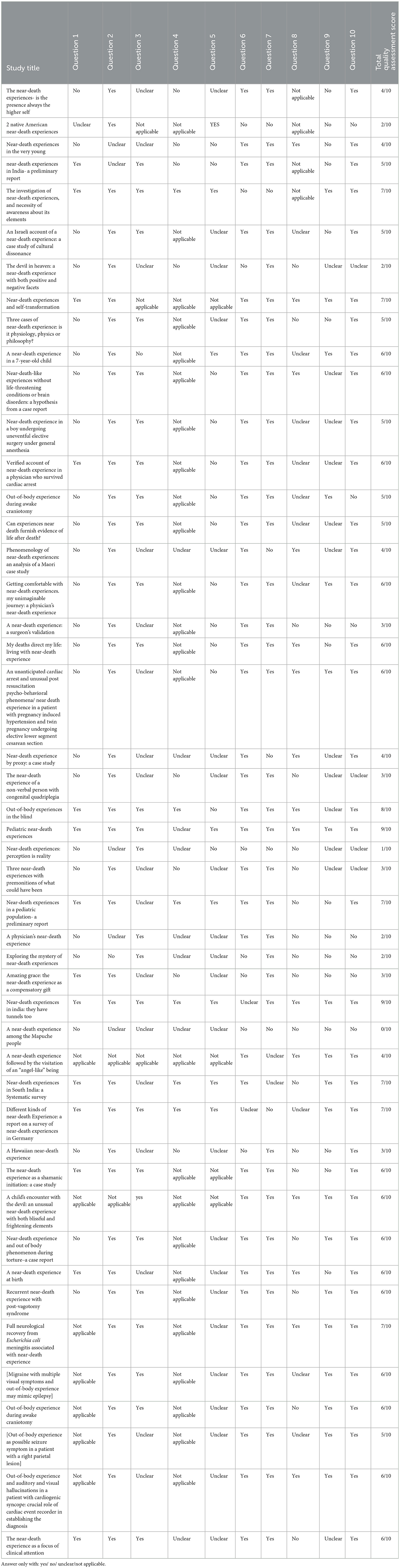
Table 5. Quality assessment for case study/case series that we include in this article.
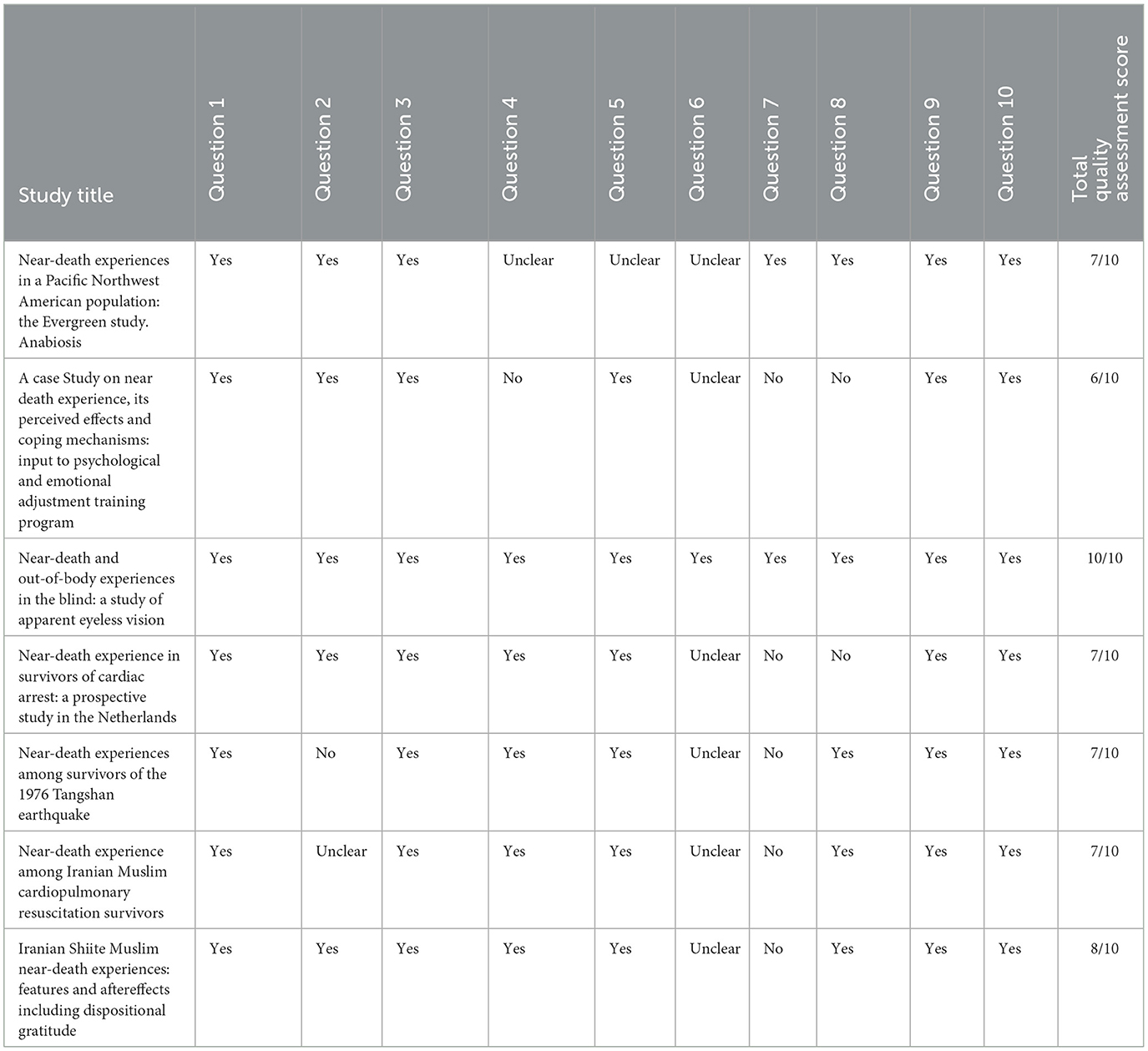
Table 6. Quality assessment for qualitative study that we include in this article.
This systematic revue study was conducted with the aim of explaining Individuals' near-death experiences and identifying common experiences. The results of this study are categorized into 4 main categories including emotional, cognitive, religious, spiritual and supernatural experiences.
Supernatural experiences were the most frequent category of experiences related to NDE, which consist of two subcategories: out of body experiences, and supernatural and metaphysical perceptions. In many studies, supernatural perceptions include passing through a tunnel involuntarily, moving toward the ceiling [out-of-body experience (OBE)], seeing one's own physical body from above whilst outside the body (the phenomenon of self-bilocation), having awareness of the places far from the body, self-permeability (passing through physical objects such as walls), being present in several locations at the same time (self-multilocation) (composed bodies), the feeling of being floating, entering a non-terrestrial location (heaven), and telepathy (non-verbal communication) with others. It can be said that the most important feature of NDEs is an out-of-body experience (OBE), which had been experienced by the majority of the NDErs. OBE is a type of autoscopy (literally, “watching oneself”) in which the soul is separated from the body, but the individual is in a fully conscious state or beyond normal consciousness (Long and Perry, 2010). Soul, in religion and philosophy, the immaterial aspect or essence of a human being that which confers individuality and humanity, often considered to be synonymous with the mind or the self. For most theologies, the Soul is further defined as that part of the individual, which partakes of divinity and transcends the body in different explanations (Ciocan, 2019). The individual seems to be awake, and watches his body and the world from a disembodied place and outside his physical body (Blanke et al., 2016), or perceives verified events that have occurred at a distance outside his/her scope (Greyson et al., 2009). A typical narrative is: “I was lying on the bed. Suddenly, I ascended in a suspended state, watching myself and the events that were taking place from somewhere above the floor, for example, near the ceiling.” (Green, 1968; Van Lommel, 2010). After an OBE, some individuals have had numerous supernatural perceptions. In some cases, there is a higher number of perceived experiences and, in others, there are fewer ones. However, there are many commonalities among the mentioned metaphysical experiences. The results of various studies show that after the soul leaves the body, NDErs enter a cylindrical tunnel, at the beginning of which there is absolute darkness and, at the end, a very dazzling light toward which the individual is guided. In most cases, this experience has been a very difficult one to forget. This experience is called a Tunnel Experience (TE) (Sabom, 1978). A tunnel experience may be defined as the perception of a realistic enclosed space which is much longer than its diameter. The peripheral features and the deep perspectives of this phenomenon indicate organizing the space around a central area in the visual field (Moody, 2001). Tunnel experiences have been reported in different forms including cylinder, pipe, tunnel, passage, corridor, spiral, well, funnel, shaft, hole, culvert, cave, long enclosure, sewer, cone, and so on (Drab, 1981). Greyson claims that crossing the tunnel occurs mostly for Indian and Buddhist NDEr's (Greyson, 2015). However, the results of another study conducted on the Muslim population have also confirmed similar experiences (Ghasemiannejad-Jahromi A and R., 2018). In his study, Todd Murphy states that tunnels are not seen or are very rare in Thai NDEs (Murphy, 2001). This systematic review study shows that the supernatural and metaphysical experiences of the participants have similar roots for every race and religion, with differences in the expression of details.
The second category of NDEs were spiritual and religious experiences, consisting of the 4 subcategories: meeting with the dead and acquaintances, meeting with religious figures, feeling oneness with the universe, and observing punishment and reward for actions. Some NDEr's have reported encounters with their deceased relatives and friends (Tassell-Matamua, 2013; Ghasemiannejad et al., 2014). Additionally, some children who have experienced NDEs have reported meeting the individuals whom they did not know at the time of the NDE, but later recognized as their deceased relatives from the family photos they had never seen before (Morse et al., 1985; Lopez et al., 2006). Other NDErs report encountering a recently deceased individual, whose death they hadn't been aware of (Greyson, 2010). One of the common aspects of the experiences was meeting with religious figures. The results of a study that compared NDE experiences in different cultures show that in western NDEs, when one is in the tunnel, he/she perceives that a group of deceased relatives and friends have come to welcome him/her, while in Thai NDEs, the experiences usually start with Yamatoots (Yamadutas are the messengers of death according to Hinduism, the agents of Yama, the god of the netherworld) (Murphy, 2001). In Thai NDEs, there is no experience of being light, and the Buddha appears only symbolically. One of the Thai experienced mentioned, “I asked [Yamatoot] to take me to visit the Lord Buddha. I told him I had to see the Buddha. Yamatoot looked up and pointed at the sky, saying, ‘That big star is the Buddha”' (Moody, 2001). In Western NDEs, the majority of the NDErs were Christians, and had seen the figures associated with Jesus Christ and the apostles (Greyson, 2010). In a study whose target population were Twelver Shīʿīsm (also known as Imāmīyyah, is the largest branch of Shīʿa Islam, comprising about 85 percent of all Shīʿa Muslims), the reported religious and spiritual figures were among Shiite imams (Ghasemiannejad-Jahromi et al., 2018). For a better understanding of this category, the individuals' religious and cultural backgrounds should be considered while interpreting the experiences, encounters, and observations. The results of some other studies reveal a feeling of oneness with the universe and the whole cosmos, where the NDErs had stated that they had unified with the whole universe or a part of creation such as plants, with no distance between them (Long and Perry, 2010; Ghasemiannejad et al., 2014). The idea that the individual is inextricably connected to the rest of the world, or that everything is part of a whole, can be found in many of the world's religious, spiritual, and philosophical traditions (Ivanhoe et al., 2018). Most of the individuals who have experienced the feeling of oneness say that they will choose this state of mind if they have eternal life. Oneness is perhaps the deepest and the most sublime state that a human being can achieve (Klussman, 2022). The last subcategory of spiritual-religious experiences was observing punishment and reward for actions. Research shows that some NDEr's are able to perceive the external consequences of their actions and deeds in the world, as well as their inner and hidden effects (Holden et al., 2009; Greyson, 2014; Khanna and Greyson, 2014b).
Another category of NDEs were cognitive experiences, which consisted of 4 subcategories, including heightened senses, an altered nature of time, reviewing life events, and the sudden perception of a specific knowledge. In regard with the heightened senses, a review of the reports of the NDEr's shows that their visual descriptions are impressive (efficacious) and clear (obvious), all while these individuals are unconscious and often clinically dead at the time of experiencing and seeing such wonderful sights. In NDEs, all the senses of sight, hearing, touch, taste, and smell have been described. The heightened senses and the improved consciousness among these individuals even indicate that these experiences are to be very different from dreams and sleep, and at the moment it is difficult to find a recognized medical explanation for NDEs. This phenomenon is medically inexplicable. There is no other type of altered consciousness experience in which events are that clear, consciousness is that strong, and events follow one another in such a specific order. The research conducted in this field shows a stable pattern of enhanced consciousness and heightened senses, which leads to the clarity of NDEs and proves them (Bryant and Peck, 2009; Khanna and Greyson, 2014b). Moreover, according to some experienced, in NDEs, time loses its meaning and sense, and they see the events of their life in a fraction of a second (Holden et al., 2009). Reviewing the past events of one's life is another cognitive experience in which NDErs may see a part or all of their life. The individual's encounter with self is one of the most important and common features of these experiences. At this stage, one encounters his/her own words, actions, and thoughts, and sees his/her own life in the form of a book, show, or movie, and judges it. The results of other research show that while reviewing their lives, the individuals review their past actions, words, and thoughts, and realize that each of them has a special energy, which has affected both themselves and others in this world (Facco and Agrillo, 2012b; Tassell-Matamua, 2014). In addition, the results of various studies, including Long's research, state that the events observed in the NDEr's life reviews are based on reality. These results assume that if NDEs are real, it is expected that the events observed during the life review be confirmed by the individual, and vice versa, if NDEs are not real, significant errors must occur during the life review. However, the latter is not the case, and everything has been confirmed by the individuals (Bryant and Peck, 2009; Khanna and Greyson, 2014b).
The last category of near-death experiences is emotional experiences, which includes two subcategories: positive experiences and negative experiences. Many NDErs state that they have experienced immense peace, and that it has been their most memorable experience, in such a way that they hesitated whether or not to return to life. In addition, in the cases where an individual had died with severe pain, his/her pain had disappeared with the sudden experience of relaxation (Klemenc-Ketis et al., 2010; Long and Perry, 2010). Most of the early studies on NDEs depicted only positive emotions (Ring, 1980, 1984). However, an interdisciplinary study was published, in which they identified 55 NDErs, eleven of whom reported negative experiences (Lindley et al., 1981). Another study indicated that 1–10% of the samples had not described positive feelings (Charland-Verville et al., 2014), these different proportions can be attributed to very broad definitions of disturbing NDEs, as well as different methods (Greyson, 2003; Charland-Verville et al., 2014). Reviewing the conducted studies shows that hellish and purgatory scenes are rarely found in NDEs, but heavenly scenes are seen more often and are very similar to each other. It may be concluded that the disturbing dimensions of the experience, added to its mystical aspect, can prevent the individuals from sharing it (Cassol et al., 2019). Based on the results of a study, frightening NDEs are divided into three groups: 1. The negative events may be viewed as warnings about unwise actions, leading to self-analysis and, ultimately, a “spin” in the NDEr's life, 2. The NDEr may treat the event as if it is not important, and 3. The frightening event may lead to difficulty in integrating the experience, developing a sense of stigma (Greyson, 2014).
The present study has combined data focusing on the principle of comprehensiveness and quality. To perform a comprehensive search, the synonym recognition systems of Thesaurus Mesh and Emtree were used to determine the keywords. Then the search was done in the vastest electronic databases such as PubMed, Scopus, Web of Science, and ProQuest with a wide time range, using experts' opinions, without time or place limitations. Considering the variety of the experiences reported by the experienced, the results were reported qualitatively. Some of the studies date back to the years before 1990, some of whose PDFs were incomplete, and the data of a number of their cases had been presented incompletely.
It can be almost concluded that according to the researchers who have presented valuable research in this field, the basis and the content of the patterns mentioned by the NDEr's are similar, and the differences are in the explanation and the interpretation of the experience. There is a common core among them such as out-of-body experiences, passing through a tunnel, heightened senses, etc. This is what all ethnic groups and nations face, without exception and without being influenced by religion, race, culture, and the native customs of their countries. Besides this central core, a series of other events or actions take place, which are more detailed and rooted in the personal archive of the NDEr's, consisting of all kinds of symbols, images, and characters which have been important only to that person. It is clear that aspects of near-death experiences are influenced by culture, while there are also parts that are universal. The most critical versatile features include altered states of consciousness and delusions, which seem to occur in all cultures studied so far. However, the specific characteristics of this experience vary significantly according to cultural context. The first point is that apparently, the content of experiences shows variations. For example, in some cultures, certain religious figures may be seen, and unlike them, others may see their deceased relatives. Second, the pattern of this experience is diverse, so people from certain cultures may have the experience of leaving the body, going to the tunnel, and reviewing life, and unlike them, the experience of others does not include these, and finally, the concept and perception of the near-death experience are different among cultures. In the current study, four main NDE categories were extracted from case reports, case series, and qualitative research studies, in the majority of which the experiences were common. The heightened senses and the improved consciousness among these individuals even indicate that “these experiences are neither dreams, nor sleep, nor the disorders caused”; “This phenomenon is medically inexplicable.” The research conducted in this field show a stable pattern of enhanced consciousness and heightened senses, “which leads to the clarity of NDEs and proves their being real.” The familiarity of the treatment staff, especially nurses and doctors, with NDE components and elements, gaining knowledge in this regard, and an awareness of appropriate and pertinent interventions can lead to proper reactions and feedbacks in response to the NDEr.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
HA, AH, AO, and MR designed the study, supervised and directed the study, carried out the implementation, aided in designing the study, and worked on the manuscript. HA and AH processed the experimental data, performed the analysis, and drafted the manuscript. All authors discussed the results, commented on the manuscript, and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abramovitch, H. (1988). An Israeli account of a near-death experience: a case study of cultural dissonance. J. Near Death Stud. 6, 175–184. doi: 10.1007/BF01073366
Bhowmick, B. K. (1991). Recurrent near-death experience with post-vagotomy syndrome. J. R. Soc. Med. 84, 311. doi: 10.1177/014107689108400523
Blackmore, S. J. (1993). Near-death experiences in India: they have tunnels too. J. Near Death Stud. 11, 205–217. doi: 10.1007/BF01078238
Blanke, O., Faivre, N., and Dieguez, S. (2016). “Chapter 20 - leaving body and life behind: out-of-body and near-death experience,” in The Neurology of Conciousness, 2nd Edn., eds S. Laureys, O. Gosseries, and G. Tononi (San Diego, CA: Academic Press), 323–347. doi: 10.1016/B978-0-12-800948-2.00020-0
Blanke, O., Faivre, N., Dieguez, S., Laureys, S., Gosseries, O., and Tononi, G. (2009). The Neurology of Consciousness. London: Academic Publishers.
Boado, J. A. V., Kilala, A. M. C., Niduaza, J. C., and Padilla, D. D. M. (2020). A case study on near death experience, its perceived effects and coping mechanisms: input to psychological and emotional adjustment training program. Ann. Med. Psychol. 178, 535–539. doi: 10.1016/j.amp.2019.05.001
Bonenfant, R. J. (2000). A near-death experience followed by the visitation of an “angel-like” being. J. Near Death Stud. 19, 103–113. doi: 10.1023/A:1007861022420
Bonenfant, R. J. (2001). A child's encounter with the devil: an unusual near-death experience with both blissful and frightening elements. J. Near Death Stud. 20, 87–100. doi: 10.1023/A:1013058221999
Bos, E. M., Spoor, J. K. H., Smits, M., Schouten, J. W., and Vincent, A. (2016). Out-of-body experience during awake craniotomy. World Neurosurg. 92, 586.e589–586.e513. doi: 10.1016/j.wneu.2016.05.002
Brandt, C., Brechtelsbauer, D., Bien, C. G., and Reiners, K. (2005). [Out-of-body experience as possible seizure symptom in a patient with a right parietal lesion]. Nervenarzt 76, 1259, 1261–1252. doi: 10.1007/s00115-005-1904-y
Brandt, C., Kramme, C., Storm, H., and Pohlmann-Eden, B. (2009). Out-of-body experience and auditory and visual hallucinations in a patient with cardiogenic syncope: crucial role of cardiac event recorder in establishing the diagnosis. Epilepsy Behav. 15, 254–255. doi: 10.1016/j.yebeh.2009.02.047
Bryant, C. D., and Peck, D. L. (2009). Encyclopedia of Death and the Human Experience. Sage. doi: 10.4135/9781412972031
Campbell, R., Pound, P., Morgan, M., Daker-White, G., Britten, N., Pill, R., et al. (2012). Evaluating meta ethnography: systematic analysis and synthesis of qualitative research. Health Technol Assess. 15, 1–164 doi: 10.3310/hta15430
Cassol, H., Martial, C., Annen, J., Martens, G., Charland-Verville, V., Majerus, S., et al. (2019). A systematic analysis of distressing near-death experience accounts. Memory 27, 1122–1129. doi: 10.1080/09658211.2019.1626438
Charland-Verville, V., Jourdan, J.-P., Thonnard, M., Ledoux, D., Donneau, A.-F., Quertemont, E., et al. (2014). Near-death experiences in non-life-threatening events and coma of different etiologies. Front. Hum. Neurosci. 8, 203. doi: 10.3389/fnhum.2014.00203
Ciocan, C. T. (2019). The value of the soul in the religious views. An overview targeting the salvation of an individual. Dialogo 6, 233–244. doi: 10.18638/dialogo.2020.6.2.21
Cooper, M. J. (2011). Near-death experience and out of body phenomenon during torture–a case report. Torture. 21, 178–181.
Drab, K. J. (1981). The tunnel experience: reality or hallucination? Anabiosis J. Near Death Stud. 1, 126–128. doi: 10.17514/JNDS-1981:1(2)
Facco, E., and Agrillo, C. (2012a). Near-death-like experiences without life-threatening conditions or brain disorders: a hypothesis from a case report. Front. Psychol. 3, 490. doi: 10.3389/fpsyg.2012.00490
Facco, E., and Agrillo, C. (2012b). Near-death experiences between science and prejudice. Front. Hum. Neurosci. 6, 209. doi: 10.3389/fnhum.2012.00209
Foster, R. D., James, D., and Holden, J. M. (2009). “Practical applications of research on near-death experiences,” in The Handbook of Near-Death Experiences: Thirty Years of Investigation, eds J. M. Holden, B. Greyson, and D. James (Praeger/ABC-CLIO), 235–258.
Gagnier, J. J., Kienle, G., Altman, D. G., Moher, D., Sox, H., and Riley, D. (2013). The CARE guidelines: consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013, bcr2013201554. doi: 10.1136/bcr-2013-201554
Ghasemiannejad, A., Long, J., Nouri, F. F., and Krahnakian, K. (2014). Iranian shiite muslim near-death experiences: features and aftereffects including dispositional gratitude. J. Near Death Stud. 33, 30–42. doi: 10.17514/JNDS-2014-33-1-p30-42
Ghasemiannejad-Jahromi, A., Mehrabizadeh-Honarmand, M., Hashemi, S., Beshlideh, K., and Khojasteh-Mehr, R. (2018). The investigation of near-death experiences, and necessity of awareness about its elements. J Qualit. Res. Health Sci. 7, 337–348. Available online at: https://www.magiran.com/paper/1926929
Gómez-Jeria, J. S. (1993). A near-death experience among the Mapuche people. J. Near Death Stud. 11, 219–222. doi: 10.1007/BF01078239
Graneheim, U. H., and Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 24, 105–112. doi: 10.1016/j.nedt.2003.10.001
Green, J. T. (2001). The near-death experience as a shamanic initiation: a case study. J. Near Death Stud. 19, 209–225. doi: 10.1023/A:1007859024038
Greyson, B. (1983). The near-death experience scale. J. Nervous Mental Dis. 171, 369–375. doi: 10.1097/00005053-198306000-00007
Greyson, B. (1997). The near-death experience as a focus of clinical attention. J. Nerv. Ment. Dis. 185, 327–334. doi: 10.1097/00005053-199705000-00007
Greyson, B. (2003). Incidence and correlates of near-death experiences in a cardiac care unit. Gen. Hosp. Psychiatry 25, 269–276. doi: 10.1016/S0163-8343(03)00042-2
Greyson, B. (2007). Consistency of near-death experience accounts over two decades: are reports embellished over time? Resuscitation 73, 407–411. doi: 10.1016/j.resuscitation.2006.10.013
Greyson, B. (2010). Seeing dead people not known to have died: “Peak in Darien” experiences. Anthropol. Hum. 35, 159–171. doi: 10.1111/j.1548-1409.2010.01064.x
Greyson, B. (2014). “Near-death experiences,” in Varieties of Anomalous Experience: Examining the Scientific Evidence., eds E. Cardeña, S. J. Lynn, and S. Krippner (Washington, DC: American Psychological Association), 312–352. doi: 10.1037/14258-012
Greyson, B. (2015). Western scientific approaches to near-death experiences. Humanities 4, 775–796. doi: 10.3390/h4040775
Greyson, B., Holden, J. M., and James, D. (2009). The Handbook of Near-Death Experiences: Thirty Years of Investigation: Thirty Years of Investigation. United America: Praeger. 1, 316.
Groth-Marnat, G., and Summers, R. (1998). Altered beliefs, attitudes, and behaviors following near-death experiences. J. Hum. Psychol. 38, 110–125. doi: 10.1177/00221678980383005
Hausheer, J. R. (2014). Getting comfortable with near-death experiences. My unimaginable journey: a physician's near-death experience. Mo. Med. 111, 180–183
Hausheer, J. R. (2020). A physician's near-death experience. Narrat. Inquiry Bioeth. 10, 11–14. doi: 10.1353/nib.2020.0001
Herzog, D. B., and Herrin, J. T. (1985). Near-death experiences in the very young. Crit. Care Med. 13, 1074–1075. doi: 10.1097/00003246-198512000-00021
Hess, G. (2019). Physicalism, supernaturalism, and near-death experiences: A phenomenological perspective. J. Consciousness Stud. Imprint Academic. 26, 86–106.
Holden, J. M., Long, J., and Maclurg, B. J. (2009). “Characteristics of Western near-death experiencers,” in The Handbook of Near-Death Experiences: Thirty Years of Investigation, ed E. D. James (American Psychological Association), 109–133. Available online at: https://psycnet.apa.org/record/2009-13429-000
Hosokawa, K., Usami, K., Kajikawa, S., Shimotake, A., Tatsuoka, Y., Ikeda, A., et al. (2021). [Migraine with multiple visual symptoms and out-of-body experience may mimic epilepsy]. Rinsho Shinkeigaku 61, 530–536. doi: 10.5692/clinicalneurol.cn-001577
Hsieh, H.-F., and Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qual. Health Res. 15, 1277–1288. doi: 10.1177/1049732305276687
Institute of Medicine (US) Committee on Standards for Systematic Reviews of Comparative Effectiveness Research. (2011). Finding What Works in Health Care: Standards for Systematic Reviews. Eden J, Levit L, Berg A, Morton S, editors. Washington, DC: National Academies Press.
Irwin, H. J. (1987). Out-of-body experiences in the blind. J. Near-Death Stud. 6, 53–60. doi: 10.1007/BF01073268
Irwin, H. J., and Bramwell, B. A. (1988). The devil in heaven: a near-death experience with both positive and negative facets. J. Near-Death Stud. 7, 38–43. doi: 10.1007/BF01076748
Ivanhoe, P., Flanagan, O., Harrison, V., Schwitzgebel, E., and Sarkissian, H. (2018). The Oneness Hypothesis: Beyond the Boundary of Self . Columbia University Press.
Kellehear, A. (2001). An Hawaiian near-death experience. J. Near Death Stud. 20, 31–35. doi: 10.1023/A:1011164711148
Kelly, E. W., Greyson, B., and Stevenson, I. (2000). Can experiences near death furnish evidence of life after death? Omega 40, 513–519. doi: 10.2190/KNTM-6R07-LTVT-MC6K
Khanna, S., and Greyson, B. (2014a). Daily spiritual experiences before and after near-death experiences. Psychol. Relig. Spiritual. 6, 302. doi: 10.1037/a0037258
Khanna, S., and Greyson, B. (2014b). Near-death experiences and spiritual well-being. J. Relig. Health 53, 1605–1615. doi: 10.1007/s10943-013-9723-0
Khanna, S., Moore, L. E., and Greyson, B. (2018). Full neurological recovery from escherichia coli meningitis associated with near-death experience. J. Nerv. Ment. Dis. 206, 744–747. doi: 10.1097/NMD.0000000000000874
Khoshab, H., Seyedbagheri, S., Iranmanesh, S., Shahrbabaki, P. M., Dehghan, M., Tirgari, B., et al. (2020). Near-death experience among iranian muslim cardiopulmonary resuscitation survivors. Iran. J. Nurs. Midwifery Res. 25, 414–418. doi: 10.4103/ijnmr.IJNMR_190_19
Klemenc-Ketis, Z., Kersnik, J., and Grmec, S. (2010). The effect of carbon dioxide on near-death experiences in out-of-hospital cardiac arrest survivors: a prospective observational study. Critical Care 14, 1–7. doi: 10.1186/cc8952
Knoblauch, H., Schmied, I., and Schnettler, B. (2001). Different kinds of near-death experience: a report on a survey of near-death experiences in Germany. Journal of Near-Death Studies 20, 15–29. doi: 10.1023/A:1011112727078
Lindley, J. H., Bryan, S., and Conley, B. (1981). Near-death experiences in a Pacific Northwest American population: The Evergreen study. Anabiosis J Near Death Stud. 1:106–110. Available online at: https://digital.library.unt.edu/ark:/67531/metadc799156/m1/3/
Lopez, U., Forster, A., Annoni, J. M., Habre, W., and Iselin-Chaves, I. A. (2006). Near-death experience in a boy undergoing uneventful elective surgery under general anesthesia. Pediatr. Anesth. 16, 85–88. doi: 10.1111/j.1460-9592.2005.01607.x
Martial, C., Cassol, H., Antonopoulos, G., Charlier, T., Heros, J., Donneau, A. F., et al. (2017). Temporality of features in near-death experience narratives. Front. Hum. Neurosci. 11, 311. doi: 10.3389/fnhum.2017.00311
Mcarthur, A., Klugárová, J., Yan, H., and Florescu, S. (2015). Innovations in the systematic review of text and opinion. JBI Evid. Implement, 13, 188–195. doi: 10.1097/XEB.0000000000000060
Moola, S., Munn, Z., Tufanaru, C., Aromataris, E., Sears, K., Sfetcu, R., et al. (2020). “Systematic reviews of etiology and risk,” in JBI Manual for Evidence Synthesis, eds E. Aromataris and Z. Munn (JBI). doi: 10.46658/JBIMES-20-08
Morse, M. (1983). A near-death experience in a 7-year-old child. Am. J. Dis. Child. 137, 959–961. doi: 10.1001/archpedi.1983.02140360023008
Morse, M. (2013). “Parting visions: a new scientific paradigm,” in The Near-Death Experience (Routledge).
Morse, M., Conner, D., and Tyler, D. (1985). Near-death experiences in a pediatric population - a preliminary-report. Am. J. Dis. Child. 139, 595–600. doi: 10.1001/archpedi.1985.02140080065034
Murphy, T. (2001). Near-death experiences in Thailand. J. Near Death Stud. 19, 161–178. doi: 10.1023/A:1026413705216
Noyes, R. Jr. (1980). Attitude change following near-death experiences. Psychiatry 43, 234–242. doi: 10.1080/00332747.1980.11024070
Panagore, P. B. (2020). My deaths direct my life: living with near-death experience. Narrat. Inquiry Bioeth. 10, E3–E6. doi: 10.1353/nib.2020.0008
Panditrao, M. M., Singh, C., and Panditrao, M. M. (2010). An unanticipated cardiac arrest and unusual postresuscitation psycho-behavioural phenomena/ near death experience in a patient with pregnancy induced hypertension and twin pregnancy undergoing elective lower segment caesarean section. Indian J. Anaesth. 54, 467–469. doi: 10.4103/0019-5049.71035
Parnia, S. (2017). Understanding the cognitive experience of death and the near-death experience. QJM 110, 67–69. doi: 10.1093/qjmed/hcw185
Parnia, S., Waller, D. G., Yeates, R., and Fenwick, P. (2001). A qualitative and quantitative study of the incidence, features and aetiology of near death experiences in cardiac arrest survivors. Resuscitation 48, 149–156. doi: 10.1016/S0300-9572(00)00328-2
Pasricha, S. (1993). A systematic survey of near-death experiences in south India. J. Sci. Explor. 7, 161–171.
Pasricha, S., and Stevenson, I. (1986). Near-death experiences in India a preliminary report. J. Nervous Mental Dis. 174, 165–170. doi: 10.1097/00005053-198603000-00007
Pennachio, J. (1988). Near-death experiences and self-transformation. J. Near Death Stud. 6, 162–168. doi: 10.1007/BF01073364
Purkayastha, M., and Mukherjee, K. K. (2012). Three cases of near death experience: is it physiology, physics or philosophy? Ann. Neurosci. 19, 104–106. doi: 10.5214/ans.0972.7531.190303
Ring, K. (1980). Life at Death: A Scientific Investigation of the Near-Death Experience. Coward Mc Cann.
Ring, K. (1984). Heading toward Omega: In Search of the Meaning of the Near-Death Experience. William Morrow and Company.
Ring, K. (1991). Amazing grace: THE near-death experience as a compensatory gift. J. Near Death Stud. 10, 11–39. doi: 10.1007/BF01073294
Ring, K., and Cooper, S. (1997). Near-death and out-of-body experiences in the blind: a study of apparent eyeless vision. J. Near Death Stud. 16, 101–147. doi: 10.1023/A:1025010015662
Sabom, M. B. (1978). Physicians evaluate the near-death experience. Theta 6, 1–6. doi: 10.1080/07481187708252891
Schlieter, J., and Schlieter, J. (2018). “17 The formation of near-death experiences: moody, ritchie, and hampe,” in What Is It Like To Be Dead?: Near-Death Experiences, Christianity, and the Occult (Oxford: Oxford University Press). doi: 10.1093/oso/9780190888848.003.0003
Schnaper, N., and Panitz, H. L. (1990). Near-death experiences: perception is reality. J. Near Death Stud. 9, 97–104. doi: 10.1007/BF01074210
Schoenbeck, S. B. (1993). Exploring the mystery of near-death experiences. Am. J. Nurs. 93, 42–46. doi: 10.2307/3464363
Schorer, C. E. (1985). 2 Native American near-death experiences. Omega J. Death Dying 16, 111–113. doi: 10.2190/640W-8XPR-RCD5-5Y9L
Schwaninger, J., Eisenberg, P. R., Schechtman, K. B., and Weiss, A. N. (2002). A prospective analysis of near-death experiences in cardiac arrest patients. J. Near Death Stud. 20, 215–232. doi: 10.1023/A:1015258818660
Serdahely, W. J. (1987). The near-death experiences is the presence always the higher self. Omega J. Death Dying 18, 129–134. doi: 10.2190/4LAG-1UKK-C00U-BV02
Serdahely, W. J. (1990). Pediatric near-death experiences. J. Near Death Stud. 9, 33–39. doi: 10.1007/BF01074099
Serdahely, W. J., and Walker, B. A. (1990). A near-death experience at birth. Death Stud. 14, 177–183. doi: 10.1080/07481189008252359
Sutherland, C. (1990). Near-death experience by proxy: a case study. J. Near Death Stud. 8, 241–251. doi: 10.1007/BF01074277
Tassell-Matamua, N. (2013). Brief report: phenomenology of near-death experiences: an analysis of a Māori case study. J. Near Death Stud. 32, 107–117. doi: 10.17514/JNDS-2013-32-2-p107-117
Tassell-Matamua, N. A. (2014). Near-death experiences and the psychology of death. OMEGA J. Death Dying 68, 259–277. doi: 10.2190/OM.68.3.e
Thomas, K. (2020). A near-death experience: a surgeon's validation. Narrat. Inquiry Bioeth. 10, 26–29. doi: 10.1353/nib.2020.0013
Thonnard, M., Charland-Verville, V., Brédart, S., Dehon, H., Ledoux, D., Laureys, S., et al. (2013). Characteristics of near-death experiences memories as compared to real and imagined events memories. PLoS ONE 8, e57620. doi: 10.1371/journal.pone.0057620
van Lommel, P., van Wees, R., Meyers, V., and Elfferich, I. (2001). Near-death experience in survivors of cardiac arrest: a prospective study in the Netherlands. Lancet. 358, 2039–2045. doi: 10.1016/S0140-6736(01)07100-8
Van Lommel, P., Van Wees, R., Meyers, V., and Elfferich, I. (2017). “Near-death experience in survivors of cardiac arrest: a prospective study in the Netherlands,” in Parapsychology (Routledge), 91–97. doi: 10.4324/9781315247366-5
Walker, B. A., Serdahely, W. J., and Bechtel, L. J. (1991). Three near-death experiences with premonitions of what could have been. J. Near Death Stud. 9, 189–196. doi: 10.1007/BF01074181
Williams, H. L., Conway, M. A., and Cohen, G. (2008). “Autobiographical memory,” in Memory in the Real World, 3rd Edn, eds G. Cohen and M. A. Conway (Hove: Psychology Press), 21–90.
Woollacott, M., and Peyton, B. (2021). Verified account of near-death experience in a physician who survived cardiac arrest. Explore . 17, 213–219. doi: 10.1016/j.explore.2020.03.005
Keywords: near-death experience (NDE), out-of-body experience (OBE), death, systematic review, psychological experiences
Citation: Hashemi A, Oroojan AA, Rassouli M and Ashrafizadeh H (2023) Explanation of near-death experiences: a systematic analysis of case reports and qualitative research. Front. Psychol. 14:1048929. doi: 10.3389/fpsyg.2023.1048929
Received: 20 September 2022; Accepted: 31 March 2023;
Published: 20 April 2023.
Edited by:
Antonino Raffone, Sapienza University of Rome, ItalyReviewed by:
Patrizio E. Tressoldi, University of Padua, ItalyCopyright © 2023 Hashemi, Oroojan, Rassouli and Ashrafizadeh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hadis Ashrafizadeh, YXNocmFmaXphZGVoLmgxOTkzQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.