
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 25 April 2023
Sec. Quantitative Psychology and Measurement
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1020596
 Ileana Schmalbach1*
Ileana Schmalbach1* Bjarne Schmalbach1
Bjarne Schmalbach1 Andreas Kalkbrenner2Markus Bassler3
Andreas Kalkbrenner2Markus Bassler3 Andreas Hinz4
Andreas Hinz4 Katja Petrowski1,2
Katja Petrowski1,2Background: Occupational stress and specifically job anxiety are crucial factors in determining health outcomes, job satisfaction as well as performance. In order to assess this phenomenon, the Job Anxiety Scale (JAS) is one of the instruments available. It consists of 70 items that are clustered in 14 subscales and five dimensions. This manuscript is a revised version of a retracted article that analyzed the properties of a short version of the JAS. Rather than shortening the scale, the authors of the JAS recommend to further assess the scale in its current state without modification of the factor structure. Hence, the aim of this paper is to assess the psychometric properties of the original JAS.
Methods: The sample consists of 991 – mostly psychosomatic – patients from two different clinics. We applied methods of factor analysis and bivariate correlations to explore and test factor structure and the nomological net of related constructs.
Results: The Job Anxiety Scale evinced satisfactory psychometric properties. We found very high internal consistency, and invariance across participant age. It displayed good discriminant validity and we found the expected pattern of convergent correlations. However, the model fit is not convincing.
Conclusion: With the Job Anxiety Scale, researchers can assess job related worries in a reliable manner. The questionnaire is particularly useful in large-scale surveys, in therapy or work-related contexts. However, the scale could be modified in order to aim for a better fit and assess job related anxiety in a more efficient way.
Occupational stressors are crucial predictors in explaining a wide range of positive and negative job-related outcomes. For instance, higher levels of job-related stress and anxiety are associated with lower levels of job satisfaction, commitment to the job, and burn out (Borg et al., 1991; Newbury-Birch and Kamali, 2001; Wu et al., 2021; Yang et al., 2021).
Further, job-related stress and anxiety is negatively linked to social support and well-being (Abdel-Halim, 1982; Warr, 1990; Dormann and Zapf, 2002; Greenglass, 2002; Huhtala et al., 2021) and positively related to adverse mental health outcomes (Hobson and Beach, 2000; Muschalla et al., 2013).
Recent and past researches (Motowidlo et al., 1986; Karatepe, 2012) have even suggested an impact on performance based on the frequency of stressful experiences. It is estimated that almost 5% of German employees are at risk of being absent from work due to job anxiety (Muschalla et al., 2013). This fact is associated with high costs for companies, health insurance and public pension funds. Thus, research into the phenomenon and a reliable and valid assessment of the construct are of great interest to researchers and practitioners alike. Even more in the face of the ongoing covid-19 pandemic, which can trigger and worsen job anxiety (Probst et al., 2020).
Individuals who experience job-related anxiety experience typical anxiety symptoms such as trembling, blushing or palpitations when they are at work or when they think about their work (Muschalla et al., 2010). Even though these symptoms have a major influence on work performance, there is no ICD code for workplace phobia. Haines and colleagues (Haines et al., 2002) used the criteria of phobia to characterize workplace related anxieties: Intense anxiety when approaching the workplace, incapacity to enter the workplace because of anxiety, respectively, panic symptoms and a reduction of anxiety when leaving the workplace. Bryson and colleagues (Bryson et al., 2013) implemented of parts of Warr’s anxiety-contentment axis model (Warr, 2007) for measuring job anxiety. Even though it is a clinically and economically important construct, there is only one questionnaire available for measuring job anxiety in a comprehensive manner – the Job Anxiety Scale (Linden et al., 2008).
Muschalla (2005) ran a pilot study, using an initial version of the JAS with 106 items. This version contained criteria of anxiety related to ICD-10 (World Health Organization, 1992), DSM-IV (American Psychiatric Association, 1994) and job-related anxieties often reported by patients. Based on this first trial, Linden and colleagues (Linden et al., 2008) modified the scale into its current version with 70 items. The items are clustered by theoretical assumptions in five dimensions. The five dimensions assess issues related to stimulus-related anxiety and avoidance behavior, social anxieties (e.g., bullying), insufficiency (e.g., Low self-esteem), health-and body-related anxieties, as well as job-related worrying. In addition, two items measure a global workplace-anxiety. For the assessment of job-related anxiety each subscale and dimension as well as a global mean value can be analyzed based on the 70 JAS items. Its psychometric properties, such as internal consistency (Linden et al., 2008; α = 0.98) and retest-reliability (Linden et al., 2008; Muschalla et al., 2013) (82–0.85) are good. The scale correlated (r = 0.67–0.69) with the Stait-Trait Anxiety Inventory (Spielberger, 1983) (STAI-T) illustrating its convergent validity (Linden et al., 2008; Muschalla et al., 2013). Nonetheless, the factorial structure of the scale has not been yet assessed until now.
The Workplace Phobia Scale (Muschalla and Linden, 2008) (WPS) screens for job anxiety based on 13 items. These items were selected from the JAS rather than being empirically driven. The authors used all items from the subscale’s stimulus-related anxiety and avoidance behavior and two items of the global workplace-anxiety subscale. Since stimulus-related anxiety and avoidance behavior are the central aspects of phobia, the WPS captures phobia and criteria of clinic disorders. Even so, the WPS does not allow a wide non-phobia, clinic-specific, comprehensive assessment of job anxieties in the manner the JAS does. Specifically, cognitions of bullying and insufficiency as well as health-related thought patterns are not captured. Thus, the aim of the present study is to target this gap. Furthermore, as job anxiety is not an ICD diagnosis or clinical diagnosis, there is a need for a statistically sound scale that measures work-related worries in a comprehensive construct. Especially for surveys in non-clinical and work-related contexts a validated scale to measure job anxieties could be of great relevance. A primary relevant application relies in the field of occupational psychological and practice and for instance, the evaluation of risk assessment of unemployment in the context of medical rehabilitation. Concerning the latter, general performance restrictions due to illness, fears and low self-esteem are often directly related to the workplace.
This manuscript is a revised version of a retracted article that analyzed the properties of a short version of the JAS (Schmalbach et al., 2020). Rather than shortening the scale, Muschalla (2005) recommend to further assess the scale in its current state without modification of the factor structure. Hence, the aim of the study at hand is to analyze item and scale properties, conducted factor analysis and tests of measurement invariance. In addition, to determine convergent and discriminant validity, we examining its associations with a measure of psychosocial health, the HEALTH-49 (Rabung et al., 2007, 2009). To this end we expect significant moderate to high correlations between the subscales of the HEALTH-49 related to psychological and somatoform symptoms, difficulties in interactions and social distress and the JAS. On the other hand, we hypothesize sig. and negative associations between scales related to psychological well-being, self-efficacy, activity participation and social support. Based on the theoretical background of the scale we propose a 5-factor model that illustrates the theoretical assumptions of the scale and invariance for sex and age.
We recruited a German study sample in the Clinic of Psychotherapy and Psychosomatic Medicine, University Hospital Dresden (n = 284) and in the Rehabilitation Center Oberharz (n = 758). We focused on patients and individuals in rehabilitation because, first, the JAS was developed in a similar setting (Linden et al., 2008), and second, such a sample (vs. a general population sample) will yield a broader distribution of the characteristic in question.
We included n = 169 females (59.5%) with a mean age of M = 36.64 (SD = 13.19) years and 115 males (40.5%) with a mean age of M = 37.39 (SD = 12.20) years. The overall mean age of the sample was M = 36.94 (SD = 12.88; range, 17–83) years. 26.7% of the sample lived alone in their household, 71.5% of the sample lived together with one or more people. The diagnoses for this group are displayed in Table 1.
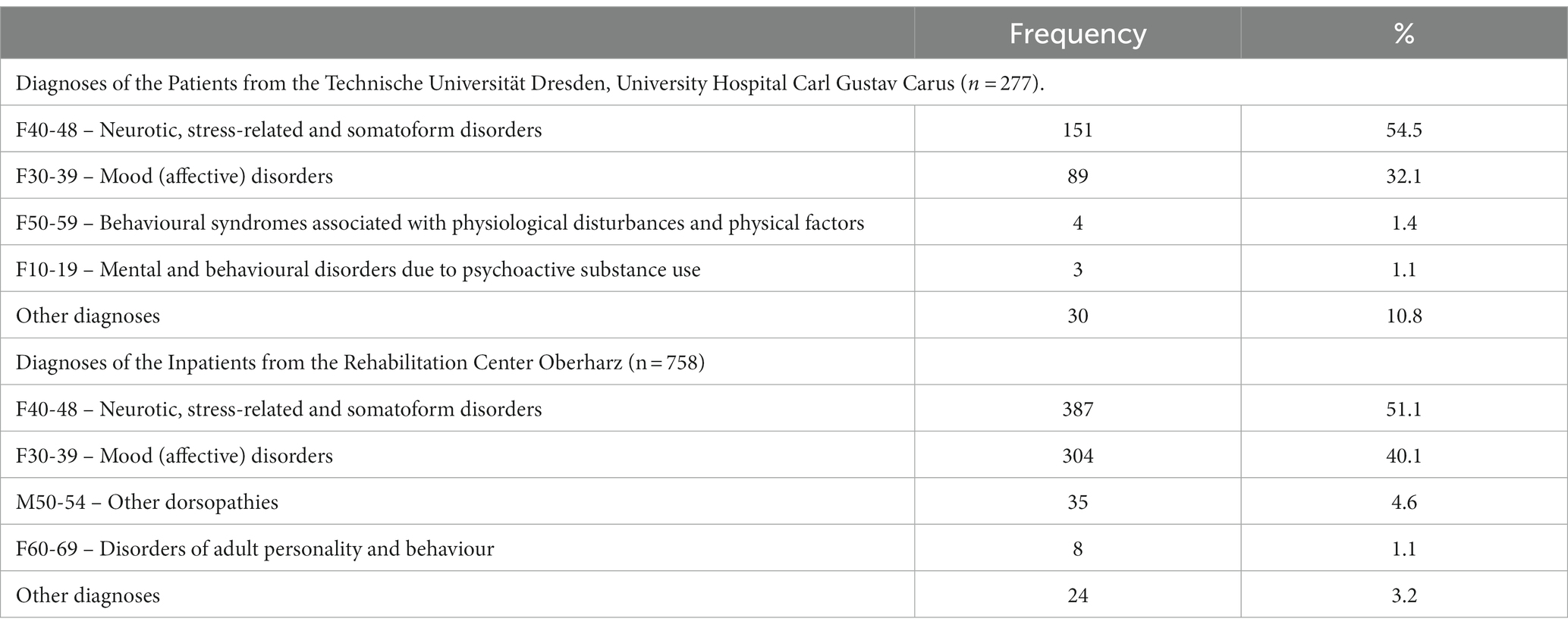
Table 1. Diagnoses of both subsamples.
The second group (N = 758) consists of patients from the “Rehabilitation Center Oberharz” (Rehazentrum Oberharz). Four hundred eleven females (54.2%) with a mean age of M = 46.90 (SD = 8.66) years and n = 347 males (45.8%) with a mean age of M = 47.14 (SD = 9.99) years were assessed in this sample. The overall mean age of the sample was M = 47.01 (SD = 9.29; range, 18–74) years. The diagnoses for this group are also displayed in Table 1.
All participants signed an informed consent form and received a data protection declaration in agreement with the Helsinki Declaration. The study was approved the ethics committee of the Medical Faculty of the Technische Universität, Dresden (EK 79032011). Verbal and written informed consent were obtained from all participants.
The JAS questionnaire (Linden et al., 2008) consists of five dimensions, 14 subscales and 70 items. Each item was scored on a 5-point Likert scale, ranging from of 0 (no agreement) to 4 (full agreement) – with no reverse-scored items. The scale shows an excellent reliability (Linden et al., 2008) (Cronbach’s α = 0.96).
We used the Hamburg Modules for the Assessment of Psychosocial Health (Rabung et al., 2007, 2009) (HEALTH-49) to measure general psychosocial well-being and health in the respondents. The scale comprises 49 items to assess nine subscales (and a psychological symptoms aggregate), which include mental health symptoms, self-efficacy, well-being, as well as social support and participation. As per Rabung et al. (2009) internal consistency is acceptable to very good for all subscales with values between α = 0.73 and 0.91.
All analyses were performed in R, using the packages lavaan (Rosseel, 2012). Missing values were replaced by linear interpolation up to a limit of 5% missing values. Data sets containing more than 5% missing values were deleted. To test the above-mentioned hypothesis concerning the factorial purpose, we conducted a confirmatory factor analysis using lavaan employing a robust maximum likelihood estimation (Satorra and Bentler, 2001) and robust formulas for the estimation of fit indices (Brosseau-Liard and Savalei, 2014). To evaluate model fit, we applied the commonly recommended indicators and cutoffs (Hu and Bentler, 1999; Schermelleh-Engel et al., 2003): χ2-test (non-significant), χ2/df (<2), Comparative Fit Index (CFI > 0.95), the Tucker-Lewis Index (TLI > 0.95), the Root Mean Square Error of Approximation (RMSEA < 0.08), and the Standardized Root Mean Square Residual (SRMR < 0.08). We report reliability as McDonald’s ω, which is the preferred measure of internal consistency (Dunn et al., 2014).
For the investigation of measurement invariance, we used the common step-wise model comparison approach (Meredith, 1993). In this procedure, one compares increasingly restrictive models to establish increasingly strict levels of invariance. Specifically, the first step is the comparison of the configural (unconstrained) model with the metric (equal factor loadings across compared groups) model. Second, one compares the metric to the scalar (equal item intercepts across compared groups) model. Finally, one compares the scalar to the strict (equal residual terms across compared groups) model. To evince measurement invariance, χ2 should not be significant and the difference in CFI and gamma hat (GH) should not exceed 0.01 (Milfont and Fischer, 2010). In order to determine convergent and discriminant validity we conducted Pearson’ product–moment correlations between the scales of the JAS and HEALTH-49.
The sample distribution showed a slightly pronounced left-skewedness, but the descriptive statistics were satisfactory for most of the JAS items (see Table 1); with some exceptions (item 31,53, 59, 69, 70) factor loadings exceeded 0.50 (0.513 ≤ λ ≤ 0.888), and reliability coefficients were between ω = 0.843 and 0.956 for the five subscales (see Table 2). The confirmatory analysis, revealed a 5-factor structure with unacceptable fit χ2(2335) = 12581.35, p < 0.001, CFI = 0.753, TLI = 0.744, RMSEA = 0.078, SRMR = 0.064. For exploratory purposes, we then tested a unidimensional model, showing a less acceptable fit, χ2(2345) = 14649.624, p < 0.001, CFI = 0.700, TLI = 0.691, RMSEA (90% CI) = 0.086, SRMR = 0.06, despite its very high internal consistency of ω = 0.976.
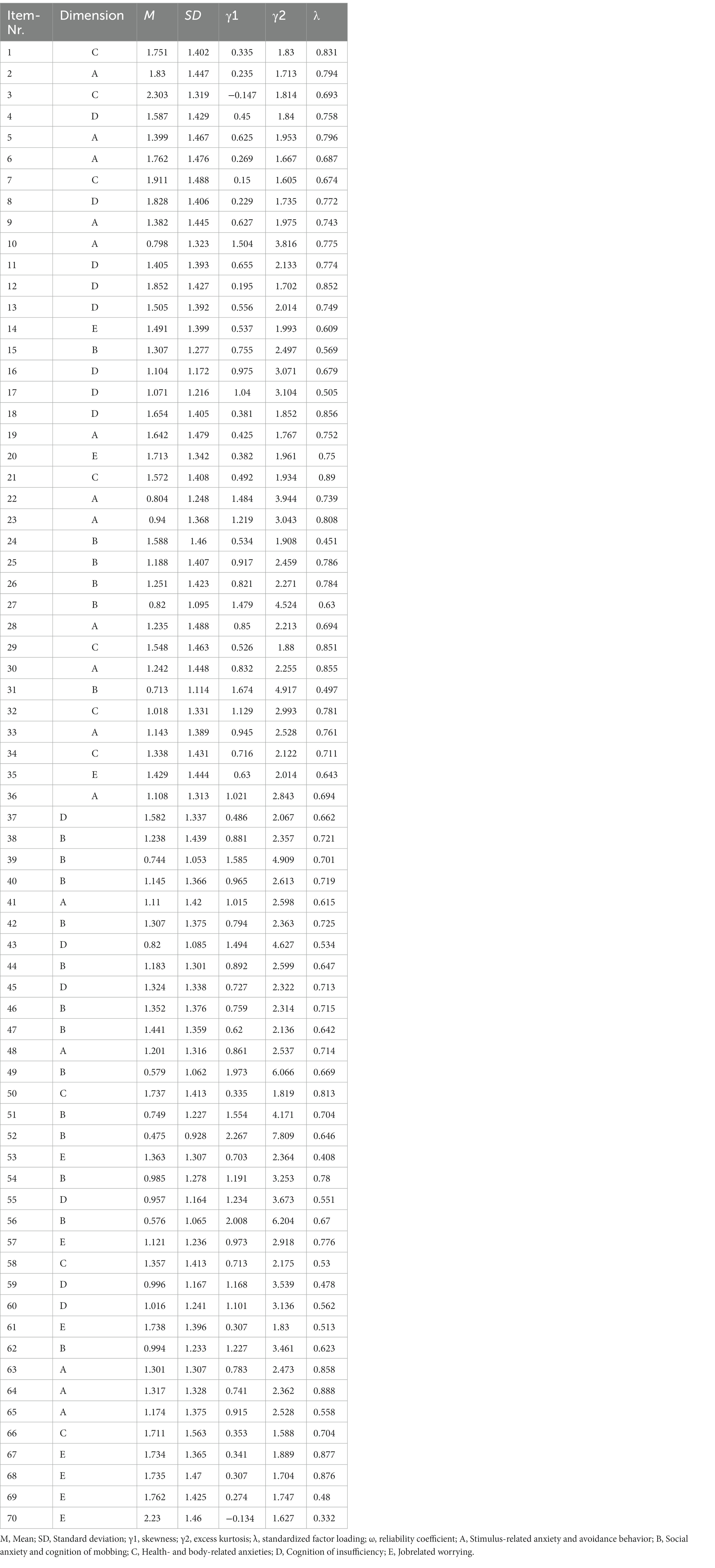
Table 2. Descriptive statistics of the JAS-70 items and scales.
Thereafter, we tested the measurement invariance of the 5-factor model across participant sex and age. Our results showed clear evidence for strict invariance across age groups, but not for sex. The results of these analyses are reported in Table 3.
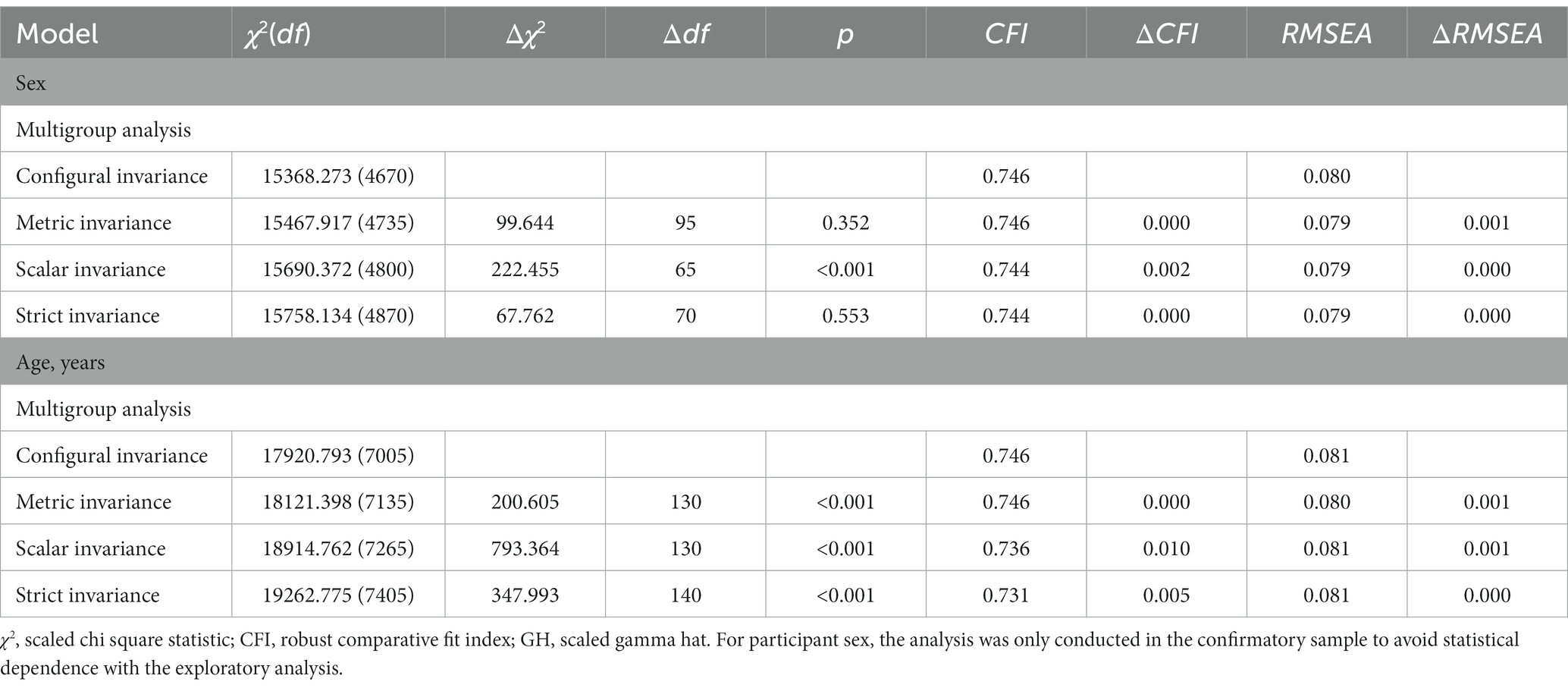
Table 3. Fit indices for the analysis of measurement invariance.
Next, we examined the convergent validity of the JAS (see Table 4). In this regard, we found the expected pattern of correlations with the HEALTH-49. Namely, symptoms of mental distress and social restrictions correlated positively high with job anxiety, and indicators of well-being and social integration evinced negative associations to the construct. To synthesize these results into a more comprehensive format we also ran a canonical correlation analysis. This yielded canonical correlation coefficients R of 0.620, 0.331, 0.231, 0.176, and 0.127 – with the first three being significant contributors (p < 0.001).

Table 4. Correlations between the JAS and the HEALTH-49.
The aim of the present study was to reevaluate the psychometric properties of the JAS and additionally confirm its factor structure. In contrast to other scales (e.g., WPS), the JAS is an empirically-derived extract which assess job related anxiety symptoms in a comprehensive manner.
In the present study, the JAS was found to be highly reliable. This result is in line with the research conducted by Linden et al. (2008) who found very good values for Cronbach’s alpha (α = 0.98) as well. Apart from the JAS being a reliable scale, we also found evidence for its strict measurement invariance across age groups, but not for sex. This means that group means across ages can be meaningfully compared and inferences can be drawn from these comparisons, which is a useful property in this scale. From the latter result it can be drawn, that men and women rate their job anxiety differently and their scores should be evaluated with this in mind. Despite these positive results, the confirmatory analysis, revealed a 5-factor structure with an unacceptable fit, as evidenced by low CFI and TLI values. This means that even if the measurement process is comparable between age and gender-groups, basic factorial validity is not given. This results from correlated measurement errors and could be rectified in a revised scale.
A strength of the present study is the very large sample of participants and the measurement invariance of the scale in terms of age, which enhances the quality of our results. Moreover, the JAS and its subscales displayed convergent validity with a measure of psychosocial health in the expected manner. The JAS correlated positively with depression, phobia/anxiety and psychological somatoform symptoms and negatively with social support and well-being, self-efficacy and activity/participation (see Table 4), which coincides with previous findings (Hobson and Beach, 2000; Greenglass, 2002; Muschalla et al., 2013; Huhtala et al., 2021).
It should be noted that the JAS correlated roughly equally (r ~ 0.30–0.40) with the phobia/anxiety subscale of the instrument and with other measures of psychological distress. This apparent “lack” of differential correlation patterns between the different forms of psychological distress can be explained by the fact that the phobia/anxiety subscale of the HEALTH-49 is focused on classic phobia symptoms such as agoraphobia and specific phobias (e.g., fear of elevators).
A useful application of the scale concerns the field of occupational psychological and practice. As an example, the JAS can be used for risk assessment in the context of incapacity for work, high termination rates, risk assessment of unemployment in the context of medical rehabilitation. Further the JAS can be used to assess conflicts in the work-place and improve working environment, reduce rates of terminations and improve performance at work. Future studies should differentiate these aspects concerning sex and gender and reveal differences between men and women and how they cope with job anxiety related concerns in order to shed light in this field. Moreover, it is recommended to adjust further scales concerning invariance in this matter.
Since the JAS is a self-report scale the validity of the assessment is tied to the individuals responding to it. Among other works, Razavi (Razavi, 2001) discusses the shortcomings of these measures – such as acquiescence and social desirability – as well as potential remedies.
The study is based on data collected in a clinical environment with a large proportion of psychosomatic and rehabilitation patients. Therefore, it appears questionable that the results can be transferred without reservation to other clinical and nonclinical populations. Additionally, the sample consisted of 991 patients from two different clinics. A larger sample size from more clinics – or even from the general population – would provide an even wider database. Only little research has been carried out concerning job-related anxiety. Usually, researchers adapt different instruments or constructs in order to measure job anxiety. Therefore, further research in clinical and nonclinical samples will be necessary in order to understand the underlying construct of job-related anxiety. Based on this knowledge, the JAS should be subject to further testing and be further developed. Also, so far it is still unclear how sensitive the JAS might react to changes in a person or an organization. Therefore, the sensitivity of the JAS regarding changes should be tested. Due to its length and its unacceptable fit, future researches could focus on shortening the scale for a more economic assessment and perhaps a better fit.
The aim of this study was to evaluate the psychometric properties of the empirically derived JAS and run a confirmatory analysis, which has been missing in past studies. Our analysis revealed satisfactory psychometric properties but did not confirm the 5-factorial structure. Thus, future studies could focus on shortening the scale and aim a better fit in order to screen job related anxiety in a more efficient and valid manner (REV4).
The raw data supporting the conclusions of this article will be made available by the authors, only by reasonable request.
The studies involving human participants were reviewed and approved by Technische Universität, Dresden (EK 79032011). The patients/participants provided their written informed consent to participate in this study.
KP and MB provided data and supervised the process of creating this paper. AK contributed substantially to conception and design. All authors have made substantial contributions to analysis and interpretation of data. IS and BS executed the statistical analyses. IS and BS wrote the manuscript. All authors revised it critically for important intellectual content, and read and approved the final manuscript.
We acknowledge support by the Open Access Publication Fund of the TUD.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
JAS, Job Anxiety Scale; WPS, Workplace Phobia Scale; CFI, Comparative Fit Index; TLI, Tucker-Lewis Index; RMSEA, Root Mean Square Error of Approximation; SRMR, Standardized Root Mean Square Residual; ICD, International Statistical Classification of Diseases and Related Health Problems; DSM, Diagnostic and Statistical Manual of Mental Disorders; STAI-T, State-Trait-Anxiety Inventory; HEALTH, Hamburg Modules for the Assessment of Psychosocial Health.
Abdel-Halim, A. A. (1982). Social support and managerial affective responses to job stress. J. Organ. Behav. 3, 281–295. doi: 10.1002/job.4030030403
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). Washington, DC: American Psychiatric Association
Borg, M. G., Riding, R. J., and Falzon, J. M. (1991). Stress in teaching: a study of occupational stress and its determinants, job satisfaction and career commitment among primary schoolteachers. Educ. Psychol. 11, 59–75. doi: 10.1080/0144341910110104
Brosseau-Liard, P. E., and Savalei, V. (2014). Adjusting incremental fit indices for nonnormality. Multivar. Behav. Res. 49, 460–470. https://doi:10.1080/00273171.2014.933697. doi: 10.1080/00273171.2014.933697
Bryson, A., Barth, E., and Dale-Olsen, H. (2013). The effects of organizational change on worker well-being and the moderating role of trade unions. ILR Rev. 66, 989–1011. doi: 10.1177/001979391306600410
Dormann, C., and Zapf, D. (2002). Social stressors at work, irritation, and depressive symptoms: accounting for unmeasured third variables in a multi-wave study. J. Occup. Organ. Psychol. 75, 33–58. doi: 10.1348/096317902167630
Dunn, T. J., Baguley, T., and Brunsden, V. (2014). From alpha to omega: a practical solution to the pervasive problem of internal consistency estimation. Br. J. Psychol. 105, 399–412. doi: 10.1111/bjop.12046
Greenglass, E. R. (2002). “Work stress, coping, and social support: implications for women’s occupational well-being” in Gender, Work Stress and Health. eds. D. L. Nelson and R. J. Burke (Washington, DC: American Psychological Association), 85–96.
Haines, J., Williams, C. L., and Carson, J. M. (2002). Workplace phobia: psychological and psychophysiological mechanisms. Int. J. Stress. Manag. 9, 129–145. https://doi:10.1023/A:1015518030340. doi: 10.1023/A:1015518030340
Hobson, J., and Beach, J. R. (2000). An investigation of the relationship between psychological health and workload among managers. Occup. Med. 50, 518–522. doi: 10.1093/occmed/50.7.518
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 6, 1–55. doi: 10.1080/10705519909540118
Huhtala, M., Geurts, S., Mauno, S., and Feldt, T. (2021). Intensified job demands in healthcare and their consequences for employee well-being and patient satisfaction: a multilevel approach. J. Adv. Nurs. 77, 3718–3732. doi: 10.1111/jan.14861
Karatepe, O. M. (2012). Job resources, work engagement, and hotel employee outcomes: a time-lagged analysis. Econ. Res. 25, 644–665. doi: 10.1080/1331677X.2012.11517527
Linden, M., Muschalla, B., and Olbrich, D. (2008). Die Job-Angst-Skala (JAS). Ein Fragebogen zur Erfassung arbeitsplatzbezogener Ängste [the job anxiety scale (JAS). A questionnaire for capturing workplace-related fears]. Zeitschrift für Arbeits-und Organisationspsychologie 52, 126–134. doi: 10.1026/0932-4089.52.3.126
Meredith, W. (1993). Measurement invariance, factor analysis and factorial invariance. Psychometrika 58, 525–543. doi: 10.1007/BF02294825
Milfont, T. L., and Fischer, R. (2010). Testing measurement invariance across groups: applications in cross-cultural research. Int. J. Psychol. Res. 3, 111–130. doi: 10.21500/20112084.857
Motowidlo, S. J., Packard, J. S., and Manning, M. R. (1986). Occupational stress: its causes and consequences for job performance. J. Appl. Psychol. 71, 618–629. doi: 10.1037/0021-9010.71.4.618
Muschalla, B. (2005). Arbeitsplatzängste und Arbeitsplatzphobie. Entwicklung des Fragebogens “Job-Angst-Skala” zur Erfassung arbeitsplatzbezogener Ängste und seine Erprobung bei Patienten in der psychosomatischen Rehabilitation. Unveröffentlichte Diplomarbeit, Freie Universität Berlin
Muschalla, B., Heldmann, M., and Fay, D. (2013). The significance of job-anxiety in a working population. Occup. Med. 63, 415–421. doi: 10.1093/occmed/kqt072
Muschalla, B., and Linden, M. (2008). The job-phobia-scale – a screening instrument in medical rehabilitation. Ärztliche Psychotherapie 3, 258–262. doi: 10.1026/0932-4089.52.3.126
Muschalla, B., Linden, M., and Olbrich, D. (2010). The relationship between job-anxiety and trait-anxiety—a differential diagnostic investigation with the job-anxiety-scale and the state-trait-anxiety-inventory. J. Anxiety Disord. 24, 366–371. https://doi:10.1016/j.janxdis.2010.02.001. doi: 10.1016/j.janxdis.2010.02.001
Newbury-Birch, D., and Kamali, F. (2001). Psychological stress, anxiety, depression, job satisfaction, and personality characteristics in preregistration house officers. Postgrad. Med. J. 77, 109–111. doi: 10.1136/pmj.77.904.109
Probst, T., Humer, E., Stippl, P., and Pieh, C. (2020). Being a psychotherapist in times of the novel coronavirus disease: stress-level, job anxiety, and fear of coronavirus disease infection in more than 1,500 psychotherapists in Austria. Front. Psychol. 11. doi: 10.3389/fpsyg.2020.559100
Rabung, S., Harfst, T., Kawski, S., Koch, U., Wittchen, H. U., and Schulz, H. (2009). Psychometrische Überprüfung einer verkürzten Version der Hamburger Module zur Erfassung allgemeiner Aspekte psychosozialer Gesundheit für die therapeutische Praxis (HEALTH-49) [Psychometric inspection of a shortened version of the hamburg modules for the assessment of psychosocial health (HEALTH)]. Z. Psychosom. Med. Psychother. 55, 162–179. doi: 10.13109/zptm.2009.55.2.162
Rabung, S., Harfst, T., Koch, U., Wittchen, H. U., and Schulz, H. (2007). “Hamburger Module zur Erfassung allgemeiner Aspekte psychosozialer Gesundheit für die therapeutische Praxis (HEALTH)” – psychometrische Überprüfung eines neuen Selbstbeurteilungsinstruments zur multidimensionalen Erfassung psychosozialer Gesundheit. Phys. Med. Rehab. Kuror. 17, 133–140. doi: 10.1055/s-2007-940198
Razavi, T. (2001) Self-Report Measures: An Overview of Concerns and Limitations of Questionnaire Use in Occupational Stress Research. [Discussion Papers in Accounting and Management Sciences, 01-175]. Southampton: University of Southampton School of Management.
Rosseel, Y. (2012). lavaan: an R package for structural equation modeling. J. Stat. Softw. 48, 1–36. doi: 10.18637/jss.v048.i02
Satorra, A., and Bentler, P. M. (2001). A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 66, 507–514. doi: 10.1007/BF02296192
Schermelleh-Engel, K., Moosbrugger, H., and Müller, H. (2003). Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. Online 8, 23–74.
Schmalbach, B., Kalkbrenner, A., Bassler, M., Hinz, A., and Petrowski, K. (2020). RETRACTED ARTICLE: psychometric properties of a short version of the job anxiety scale. BMC Med. Res. Methodol. 20:87. doi: 10.1186/s12874-020-00974-4
Spielberger, C. D. (1983). Manual for the State–Trait Anxiety Inventory: STAI (Form Y). Palo Alto, CA: Consulting Psychologists Press
Warr, P. (1990). The measurement of well-being and other aspects of mental health. J. Occup. Psychol. 63, 193–210. doi: 10.1111/j.2044-8325.1990.tb00521.x
World Health Organization . (1992). The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. Geneva, Switzerland: World Health Organization
Wu, F., Ren, Z., Wang, Q., He, M., Xiong, W., Ma, G., et al. (2021). The relationship between job stress and job burnout: the mediating effects of perceived social support and job satisfaction. Psychol. Health Med. 26, 204–211. doi: 10.1080/13548506.2020.1778750
Keywords: job anxeity, health outcome, psychometric properties, psychology, job worries
Citation: Schmalbach I, Schmalbach B, Kalkbrenner A, Bassler M, Hinz A and Petrowski K (2023) Psychometric properties of the job anxiety scale. Front. Psychol. 14:1020596. doi: 10.3389/fpsyg.2023.1020596
Edited by:
Sergio Machado, Federal University of Santa Maria, BrazilReviewed by:
Maria Rita Sergi, University of G.'d'Annunzio, ItalyCopyright © 2023 Schmalbach, Schmalbach, Kalkbrenner, Bassler, Hinz and Petrowski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ileana Schmalbach, aXN0ZWZmZW5AdW5pLW1haW56LmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.