
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 09 August 2022
Sec. Quantitative Psychology and Measurement
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.966770
 Pingping Guo1,2
Pingping Guo1,2 Nianqi Cui2
Nianqi Cui2 Minna Mao1,2Xuehui Zhang3
Minna Mao1,2Xuehui Zhang3 Dandan Chen2Ping Xu1,2Xiaojuan Wang1,2Wei Zhang1,2Qiong Zheng1,2Le Zhang1Zhenzhen Xiang1Yin Jin1
Dandan Chen2Ping Xu1,2Xiaojuan Wang1,2Wei Zhang1,2Qiong Zheng1,2Le Zhang1Zhenzhen Xiang1Yin Jin1 Suwen Feng1*
Suwen Feng1*Background and aim: The postpartum depression literacy (PoDLi) of perinatal women is closely related to the occurrence, recognition, and treatment of postpartum depression, therefore valid instruments for evaluating the level of PoDLi are of great significance for both research and clinical practice. This study aimed to cross-culturally adapt the postpartum depression literacy scale (PoDLiS) into Chinese and to test its psychometric properties among Chinese perinatal women.
Materials and methods: A cross-sectional study was conducted from April to May 2022 in a tertiary hospital in Hangzhou, Zhejiang Province, China. 619 out of the 650 perinatal women that were approached via a convenience sampling method completed the Chinese version of the PoDLiS (C-PoDLiS). Content validity [the content validity index of items (I-CVI) and scale-level content validity index (S-CVI)] was evaluated by an expert panel. Psychometric properties, including item analysis, structure validity (exploratory factor analysis, confirmatory factor analysis), convergent and discriminant validity, reliability (internal consistency, test-retest reliability), criterion validity (concurrent validity, predictive validity), and floor/ceiling effect were examined.
Results: The final version of C-PoDLiS is a six-factor structure consisting of 27 items, which explained 61.00% of the total variance. Adequate content validity (I-CVI = 0.833–1.00, S-CVI = 0.920) was ensured by the expert panel. The modified confirmatory factor analysis model revealed that the 6-factor model fitted the data well (χ2/df = 1.532, root mean square error of approximation = 0.042, goodness of fit = 0.900, incremental fit index = 0.949, comparative fit index = 0.948, Tucker–Lewis index = 0.940). The total Cronbach’s α was 0.862, the total McDonald’s ω was 0.869, and the test-retest reliability coefficient was 0.856. Results of convergent validity (average variance extracted = 0.486–0.722) and discriminant validity provided good or acceptable psychometric support. Significant correlations between scores of the C-PoDLiS and Mental health literacy scale (r = 0.155–0.581, p < 0.01) and Attitudes toward seeking professional psychological help short form scale (r = 0.361–0.432, p < 0.01) supported good concurrent and predictive validity, respectively. No floor/ceiling effect was found.
Conclusion: The C-PoDLiS was demonstrated to be a sound instrument with good reliability and validity for evaluating Chinese perinatal women’s PoDLi levels. Its use in the future can facilitate data aggregation and outcome comparisons across different studies on this topic.
Depression has affected over 350 million people globally (World Health Organization [WHO], 2016). It is further predicted that by 2030, depression will be the leading cause of disease burden worldwide (World Health Organization [WHO], 2013; Bernstein et al., 2021). Women are nearly twice more likely to undergo depression across their lifespan than men (Albert, 2015), whereas the perinatal period appears to be a stage of higher risk for developing this disease due to biological changes as well as role transitions in family and society (Staneva et al., 2015; Bjelica et al., 2018). In particular, postpartum depression (PPD) is the most common psychiatric condition during the perinatal period (Evagorou et al., 2016), which is defined as a depressive episode with moderate to severe severity that occurs within the first 12 months after childbirth (O’Hara and McCabe, 2013) and is characterized by an inability to experience pleasure, spontaneous crying, appetite and sleep disturbance, fatigue, attention and concentration impairment, feelings of guilt and despair, and even thoughts of suicide (American Psychiatric Association, 2013). The reported worldwide prevalence statistics of PPD varied widely [ranging from 3.2 to 63.3% (Evagorou et al., 2016)] as a consequence of differences in sample population, instruments, diagnostic criteria, and the time point of screening, with an overall prevalence of 17.7% (Hahn-Holbrook and Cornwell-Hinrichs, 2018) and a major PPD prevalence of 6% (Ashley et al., 2016). Furthermore, research showed that these rates may be even higher in vulnerable groups of women (e.g., racial and ethnic minorities, adolescents, and low socioeconomic status) (Pooler et al., 2013) and in developing regions (Husain et al., 2006; Özcan et al., 2017). Actually, PPD has become one of the greatest unaddressed global challenges of the 21st century (Rahman et al., 2013). PPD can lead to a great number of short-term and long-term negative consequences for the mother, baby, and family without timely and effective management (O’Hara and McCabe, 2013; Field, 2018), which include but are not limited to increased risks of suicide and future episodes of depression in the mother, earlier discontinuation of breastfeeding, impaired mother-child bonding, increased economic costs, and tensions and broken relationships between family members. Noteworthily, these adverse effects can be minimized with effective treatments (Williams et al., 2016). Hence, early detection and efficient treatment of PPD are quite essential.
Unfortunately, the existing evidence revealed an unsatisfactory situation in the recognition and treatment of PPD (McCarthy and McMahon, 2008; Bilszta et al., 2010; Ko et al., 2012). On the one hand, since no procedure for standardizing PPD screening has been established in the majority of countries around the world, the identification of PPD is largely dependent on women×s knowledge of the associated symptomatology (Fonseca et al., 2015). However, the phenomenon is often that women report having limited knowledge about PPD. As such, they have difficulties distinguishing between the normative distress associated with the transition to parenthood and the PPD symptoms (Bilszta et al., 2010), as well as assessing the severity of the PPD symptoms (McCarthy and McMahon, 2008). Research showed that only about 40% of PPD cases are diagnosed (Ko et al., 2012). On the other hand, in spite of the availability of effective psychological and pharmacological treatment strategies, the vast majority of women are less likely to engage in professional help-seeking for PPD and proactively disclose their symptoms (Fonseca et al., 2015). According to studies, less than half of women with PPD sought professional assistance or engaged in standard treatments (Dennis and Chung-Lee, 2006; Sharma and Sharma, 2012; Geier et al., 2015). To date, two categories of barriers that may prevent women from seeking professional help for PPD have been identified (Dennis and Chung-Lee, 2006), including system-related barriers that are relatively difficult to change and pertain to circumstances beyond the individual’s control (e.g., childcare responsibilities, work constraints, inconvenient traffic, financial difficulties, inequal health resource distribution) and individual-level barriers (e.g., poor awareness concerning PPD, confusion related to the symptoms and treatments of PPD, feelings of guilt, shame, and stigma about PPD). The individual-level barriers, more explicitly, are the shortage of knowledge and the inaccurate views and perceptions regarding PPD (Dennis and Chung-Lee, 2006; Fonseca et al., 2015), which is called “low postpartum depression literacy (PoDLi)” (Fonseca et al., 2017) and has attracted much attention in recent years due to its modifiability and improveability.
Postpartum depression literacy is essentially a subset of mental health literacy (MHL), referring to knowledge, attitude, and beliefs about PPD as well as the ability to make informed treatment decisions (Mirsalimi et al., 2020). The most classic and comprehensive conceptual framework of MHL was introduced by Jorm (2000), which encompasses the following six components: (i) the ability to recognize different types of mental health disorders; (ii) knowledge and beliefs regarding the causes and risk factors; (iii) knowledge and beliefs of self-help strategies; (iv) knowledge and beliefs about professional help available; (v) attitudes that facilitate recognition and appropriate help-seeking behaviors; and (vi) knowledge of how to seek mental health information. Studies of the general population revealed that depression and limited depression literacy often co-exist (Francis et al., 2007), and individuals with limited depression literacy were almost three times as likely as those with sufficient depression literacy to undergo depressive symptoms (Gazmararian et al., 2000). Moreover, documented evidence suggests that low levels of PoDLi may contribute to new mothers’ minimization and normalization of their symptoms of PPD (Bilszta et al., 2010; Callister et al., 2019), and lead them to engage in maladaptive behaviors such as alcohol consumption (Guy et al., 2014). On the contrary, if a person’s depression literacy is promoted, he/she will respond better to depression treatments and be more willing to seek professional help for depression symptoms (Francis et al., 2007). Given the close relationship between depression literacy and the occurrence, recognition, treatment, and management of depression (Gazmararian et al., 2000; Francis et al., 2007), accurately assessing the PoDLi level among perinatal women is critical, which is a prerequisite to implement PPD awareness improving programs for early recognition and treatment on PPD.
Nevertheless, only two studies have been carried out to investigate the depression literacy level in perinatal women by using the 22-item depression literacy questionnaire (Fonseca et al., 2017) and vignettes for major depressive episodes (Buist et al., 2007) that are both designed for the general public and may lead to deviations in evaluation results. Given the above situation, Mirsalimi et al. (2020) initially developed the postpartum depression literacy scale (PoDLiS) in the guide of Jorm’s MHL framework for measuring perinatal women’s PoDLi levels. To date, PoDLiS has been adapted into the Malay version (Hairol et al., 2021), applied in Iran (Mirsalimi et al., 2020), India (Poreddi et al., 2021), and Malaysia (Hairol et al., 2021), and tested to be reliable and valid. But it is unclear whether PoDLiS is generalizable to other cultural contexts, as the existence and adaptation of one scale version does not guarantee measurement equivalence across other populations (Canino and Alegría, 2008; Onchonga et al., 2021).
As the most populous country in the world, China accounts for nearly one-fifth of the world’s population. According to the research results from different provinces, the PPD incidence in China ranged from 15 to 20% and still showed a significant increasing trend (Mu et al., 2019). Specifically, as per the most recent pregnancy and birth records (National Bureau of Statistics of China, 2018), it translates to potentially 5–7 million women with PPD—the largest numbers for any single country. Worse still, in China, there is a serious shortage of mental health professionals, insufficient promotion of related knowledge and maternal psychological monitoring, as well as an unoptimistic situation for PPD recognition and treatment (Xiang et al., 2018). Accordingly, it is imperative to extensively evaluate the PoDLi level in Chinese perinatal women, which is the first step in developing a PoDLi improvement program to ameliorate the prevention, recognition, and treatment of PPD. However, as far as we know, most of the studies in China focused on the prevalence of PPD (Mu et al., 2019; Nisar et al., 2020), while no study has investigated Chinese perinatal women’s PoDLi level. The lack of condition-specific measures for PoDLi may count a large part of the reason for this phenomenon. Thus, there is an increasing demand to develop a valid and reliable instrument for PoDLi assessment in China. Due to the high cost and long period required for developing a new scale, translating and testing a well-developed existing scale from another country seems to be an informed choice (Li et al., 2016). Thence, this study aimed to (World Health Organization [WHO], 2016) translate and cross-culturally adapt the PoDLiS to the Chinese context and (World Health Organization [WHO], 2013) psychometrically validate the Chinese version of PoDLiS (C-PoDLiS).
A cross-sectional survey study was performed for the translation, cross-cultural adaptation, and psychometric property validation of the PoDLiS in Mainland China. The Strengthening the Reporting of Observational Studies in Epidemiology statement (von Elm et al., 2007) was used to report the findings. Perinatal women from the maternity wards of a tertiary hospital in Hangzhou, Zhejiang Province, were recruited via the convenience sample method from April to May 2022. Self-administered pen-and-paper questionnaires were distributed by two authors (both are well-trained nursing Ph.D. candidates) and were retrieved immediately after being completed to check the missing content and ensure the questionnaire’s integrity. Per the methodological recommendations, 10 cases per candidate item are required for exploratory factor analysis (EFA), and the sample size should be at least 200 to be able to build a confirmatory factor analysis (CFA) model (Wu, 2010). Thus, a minimum sample size of 510 was estimated “a priori.” A total of 650 questionnaires were finally distributed due to the sufficient sample sources. After eliminating invalid questionnaires, 619 questionnaires were suitable for statistical analysis (Figure 1). The sample was splitted into two parts according to the order of questionnaire collection to perform EFA (sample 1: N = 310) and CFA (sample 2: N = 309).
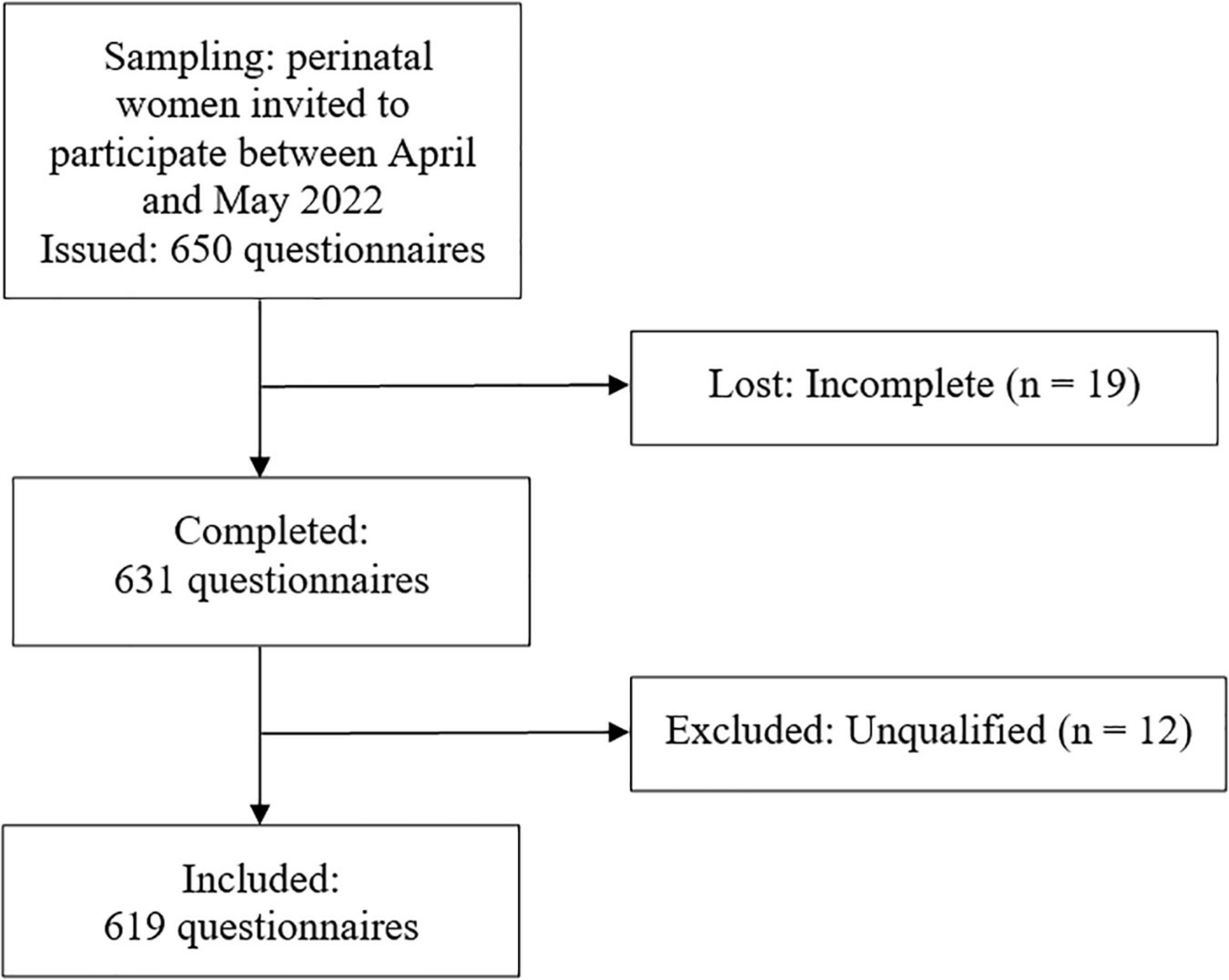
Figure 1. Flowchart of the data collection.
The following criteria were employed for inclusion, which were similar to those of Mirsalimi et al. (2020) that tested psychometric characteristics of the PoDLiS: (a) being at least 18 years old; (b) being pregnant or within 12 months of giving birth; (c) being able to read and articulate in Chinese (primary education must be completed); and (d) agreed to participate in this study. Perinatal women with serious medical illness requiring individualized assessment, tracking as “a high-risk pregnancy” (e.g., diabetes, hypertension), with positive screening for psychosis, suicidality, and substance abuse disorders, or with communication barriers (deafness or blindness) were excluded.
A self-compiled questionnaire comprising 11 questions was applied to collect socio-demographic information from participants, including age, education level, religion, monthly family income, residence, employment status, marital status, parity, perinatal period, whether they had suffered from depression or other mood disorders previously, and whether they had studied psychology before.
The PoDLiS is a self-reported instrument designed to assess the level of PoDLi in perinatal women. The original PoDLiS was constructed by Mirsalimi et al. (2020) and is composed of 31 items (8 reverse-scored items) and 7 dimensions: ability to recognize PPD; knowledge of risk factors and causes; knowledge and belief of self-care activities; knowledge about professional help available; beliefs about professional help available; attitudes that facilitate recognition of PPD and appropriate help-seeking; and knowledge of how to seek information related to PPD. Each item of PoDLiS is valued on a 5-point Likert scale from 1 (strongly disagree/not likely at all) to 5 (strongly agree/very likely). The total score for PoDLiS as well as scores for each dimension are calculated by adding up the coded values and then dividing them into the number of items, ranging from 1 to 5, with higher scores denoting better PoDLi level. The original version of PoDLiS has good construct validity and internal reliability. The Cronbach’s α for the whole scale was 0.78, and the α coefficients for seven domains were between 0.70 and 0.83.
The mental health literacy scale (MHLS) was developed by O’Connor and Casey (2015) to assess the level of MHL. The Chinese version of MHLS includes 35 items and 6 subscales (the capacity to recognize mental health disorders; knowledge of risk factors; familiarity with self-treatment; awareness of available professional help; knowledge of how to seek information; and attitudes that promote recognition or effective aid-seeking behavior), of which the 1–15 items have a 4-point Likert scale (1–4) and the 16–20 items have a 5-point Likert scale (1–5) (Ma, 2019). The total score of MHLS ranged from 35 to 160, with higher scores representing an adequate MHL. As reported, the Chinese version of MHLS has good reliability and validity and can be applicable to different populations in China (Han et al., 2019; Ma, 2019; Chen et al., 2021). The Cronbach’s α of MHLS was 0.840 for this study. The MHLS was completed by a sample of 290 people for testing concurrent validity.
The attitudes toward seeking professional psychological help short form scale (ATSPPH-SF) was developed by Fischer and Farina (1995). The Chinese version of ATSPPH-SF consists of 10 items and 2 domains: openness to seeking treatment for emotional problems and value and need in seeking treatment (Fang et al., 2019). Item responses are based on a 4-point Likert scale (0–3). The total score of ATTSPH-SF ranges from 0 to 30, with higher scores indicating a higher propensity to seeking help. The reliability and validity of the Chinese version of the ATSPPH-SF has been extensively verified (Fang et al., 2019; Chen et al., 2020). In the current study, a Cronbach’s α of 0.766 was obtained. The ATSPPH-SF was completed by a sample of 100 people to test predictive validity.
Permission to translate the English version of PoDLiS to the Chinese language was granted by the developers (Mirsalimi, PhD) (Mirsalimi et al., 2020). An internationally accepted multiphase translation guideline (Beaton et al., 2000) was followed in the translation and validation process.
Two fluent translators in both languages (one was an obstetrics nursing postgraduate who was familiar with the concepts explored, while the other didn’t have a medical background) independently translated the original PoDLiS into Chinese.
After any discrepancies about the words, phrases, and items in the translation process were fully discussed by two translators, a synthesis forward translation version was obtained.
Two bilingual native English speakers, who were blinded to the original PoDLiS with no medical background, translated the synthesis version back into English independently, creating two backward translation versions.
All reports were compared and reviewed by a specialist committee that was composed of eight experts (an obstetrics expert, a psychologist, a methodologist, a linguistics professional, and four translators) to reach a consensus on discrepancies and achieve semantic, idiomatic, cultural, and conceptual equivalence. Additionally, the expert panel referred back to the original English version to capture the accurate meaning of each item. Ultimately, we sent the synthesis forward translation version, two back-translation versions, and unaddressed translation issues to the developer for confirmation, then integrated their feedback to generate an integrated version. All problems, discrepancies, and discussion in each translation stage were documented.
Expert consulting was carried out to assess the content validity of the C-PoDLiS and to confirm whether the items were designed properly to create the constructs. The survey consisted of four parts of content, including biographical information (education level, working experience, etc.), the original English PoDLiS, the integrated version of C-PoDLiS, and an assessment file for content equivalence (using a 4-point ordinal rating scale: 1 = irrelevant; 2 = somewhat relevant and needs major modification; 3 = quite relevant but needs minor modification; 4 = extremely relevant). Experts were also asked regarding the clarity of each item and their revision suggestions. The survey was emailed to six experts in accordance with the recommendation of guideline (Beaton et al., 2000) (three nursing professors, two clinical experts in obstetric care, and a mental health expert) and got feedback from all of them. Then, the specialist committee discussed and integrated all revision suggestions to generate a pre-final version for pilot testing.
According to the guideline that recommends a sample size of 30–40 participants for pre-testing (Beaton et al., 2000), the pre-final version was administered in the same tertiary hospital to a purposive sample of 33 eligible perinatal women with diverse characteristics (in terms of age, education, and occupational background) to examine face validity (comprehension of the meaning and appropriateness of the wording of test items), simplify the item wording, and assess the time consumption. The 33 samples were not included in the psychometric validation. Since no major suggestions emerged, the preliminary C-PoDLiS was only fine-tuned compared to the pre-final version.
According to the recommendation in the COSMIN (Consensus-based Standards for the Selection of Health Status Measurement Instruments) checklist (Mokkink et al., 2010a; Prinsen et al., 2018), the psychometric properties of the C-PoDLiS were assessed in terms of item analysis, structural validity, convergent and discriminant validity, reliability, a floor/ceiling effect, and criterion validity.
Data were analyzed using SPSS V.25.0, AMOS V.23.0, and jamovi V.2.2.5. Enumeration data was described by frequency and percentage (%), and the measurement data was described by mean and standard deviation (SD). P values < 0.05 were considered statistically significant.
The content validity index (CVI) was computed at both the item level (I-CVI) and the scale level (S-CVI). The I-CVI is the proportion of content experts giving either 3 or 4 on a 4-point scale, whereas the S-CVI is the average of the total I-CVI on the scale. As suggested by Polit and Beck (2009), I-CVI ≥ 0.78 and S-CVI ≥ 0.80 are considered to be appropriate if the number of experts is ≥6.
Item analysis was performed using the following analyses: (1) extreme groups’ analysis: items should be significantly discriminated between the upper 27% and the lower 27% of scoring groups (Odukoya et al., 2018); (2) critical ratio (CR): items with CR < 3.0 and a P value > 0.05 were deleted (Wu, 2010); (3) correlation coefficient method: an item was retained when its score was significantly correlated with the total scale score or the item-total correlation value was 0.30–0.80 (Wu, 2010); (4) Cronbach’s α or McDonald’s ω greatly improved (increasing the value of the α or ω coefficient for the overall scale by 0.5 or more) if an item was deleted (Wu, 2010).
To establish the structural validity of the C-PoDLiS, EFA was first conducted, and then the results were verified via CFA. Prior to EFA, the Kaiser–Meyer–Olkin (KMO) test (≥0.6 is considered acceptable) and Bartlett’s test of sphericity (significant tests demonstrate adequacy) were conducted to ensure the data’s suitability for factor analysis (Hu et al., 2019). For EFA analyses, the principal component analysis with the oblique rotation method (promax criterion) was applied as the correlation between the factors was >0.3 (Wu, 2010; Hu et al., 2019). The criterion for factor extraction and item retention was eigenvalues > 1.0, factor loadings > 0.45 (Wu, 2010), and items with consistent predefined sub-dimensions. The scree plot was also examined to determine the factor structure. For CFA analyses, the maximum likelihood estimation method was used to estimate the parameters. The t-value and factor loading of each item, as well as the goodness-of-fit, were considered when commenting on the fit of the CFA model. Items with either a t-value < 1.96 (Wu, 2010) or a factor loading < 0.32 (Qu et al., 2021) should be deleted. The goodness-of-fit of the CFA model was measured by the following indices: χ2/df, comparative fit index (CFI), goodness of fit (GFI), Tucker–Lewis index (TLI), incremental fit index (IFI), and root mean square error of approximation (RMSEA) (Brown, 2006). As recommended, a CFA model is adequately fitted when 1 < χ2/df < 3, RMSEA < 0.08, whereas CFI, GFI, TLI, and IFI > 0.90 (Brown, 2006).
Average variance extracted (AVE) was used to assess the internal convergent validity of a factor, with a score ≥ 0.5 indicating satisfactory convergent validity (Fornell and Larcker, 1981). To show discriminant validity, the √AVE score should exceed each of its correlations with other factors (Fornell and Larcker, 1981; Hair et al., 2010).
Scale reliability was evaluated in terms of internal consistency and stability. Internal consistency was tested by calculating the Cronbach’s α and McDonald’s ω (Peter, 2014). The intraclass correlation coefficient (ICC) was calculated via the test-retest reliability method to evaluate the stability of the C-PoDLiS (Perinetti, 2018). Thirty-one perinatal women who were randomly selected from the total samples completed the preliminary C-PoDLiS at a 2-week interval to establish test-retest reliability. Sufficient reliability is based on values of Cronbach’s α, McDonald’s ω, and ICC equal to or greater than 0.70 (Hair et al., 2010), whereas scores of these indicators between 0.60 and 0.70 signifie an acceptable level of reliability (Wu, 2010).
The floor/ceiling effect (the percentage of people scoring at the bottom and top of a scale) for the total scale were analyzed to assess the interpretability. Less than 15% of responses with the lowest or highest score were deemed acceptable, defining no substantial floor and ceiling effects (Mokkink et al., 2010b).
To evaluate the concurrent validity and predictive validity, the Spearman rank correlations were analyzed between the C-PoDLiS and other instruments (MHLS and ATSPPH-SF). The correlation of |r| = 0.10–0.30, |r| = 0.31–0.60, and |r| = 0.61–1.00 were considered low, moderate, and high, respectively (Andresen, 2000). According to previous studies, we hypothesized that the C-PoDLiS score would be positively associated with both the MHLS score and the ATSPPH-SF score.
This study was reviewed and approved by the hospital’s Research Ethics Review Committee (IRB-20220190-R). All the procedures that were carried out in this study were consistent with the 1964 Declaration of Helsinki and its later amendments (World Medical Association [WMA], 2008). The participants were informed of the purpose of the study as well as the anonymity and confidentiality of the survey before commencement. They were also informed that they can withdraw at any stage while being surveyed without any penalty. Written informed consent was obtained from all participants and they agreed that their data could be used in the project. The participants were not financially compensated. The survey did not disclose any personal information.
Based on the results of expert consultations, evidence from literature, and feedback from the pilot testing, some adjustments and modifications were made to obtain the preliminary version of the C-PoDLiS (see Supplementary Table 1). First, 2 new items were added (item 15 and item 21). Second, the items “Treatment for PPD, provided by a mental health professional, can be effective” and “Psychotherapy (for example, talking therapy or counseling) can be effective in treating PPD” of the original scale were merged into item 18; the items “I know where to seek information about PPD” and “I know how to use various sources to seek information about PPD” of the original scale were merged into item 28. Third, some words and phrases were changed. For instance, “mental health professional” in item 5 of the original scale was adjusted to “psychotherapist or psychiatrist.” Given that only one item was left in the dimension of “Knowledge about professional help available” after the item mergence, this dimension was integrated with the dimension of “Beliefs about professional help available,” generating a new dimension named “Knowledge and beliefs about professional help available.” In the pilot testing, 33 participants stated that the wording of the C-PoDLiS was clear and they had little difficulty understanding it. In the second round of expert consultations, the S-CVI was 0.920, and the I-CVI ranged from 0.833 to 1.00. Eventually, the preliminary C-PoDLiS with 31 items and 6 factors was generated for psychometric evaluation.
A total of 619 (out of a possible 650) perinatal women completed the survey (Figure 1), for an effective response rate of 95.23%. The mean age of participants was between 20 and 42 years (mean = 30.85, SD = 4.03). Perinatal women who were non-religious, married, lived in urban areas, had a specialty/bachelor’s degree, in the postpartum period, and were primiparous counted the most. The detailed demographics of participants are shown in Table 1.
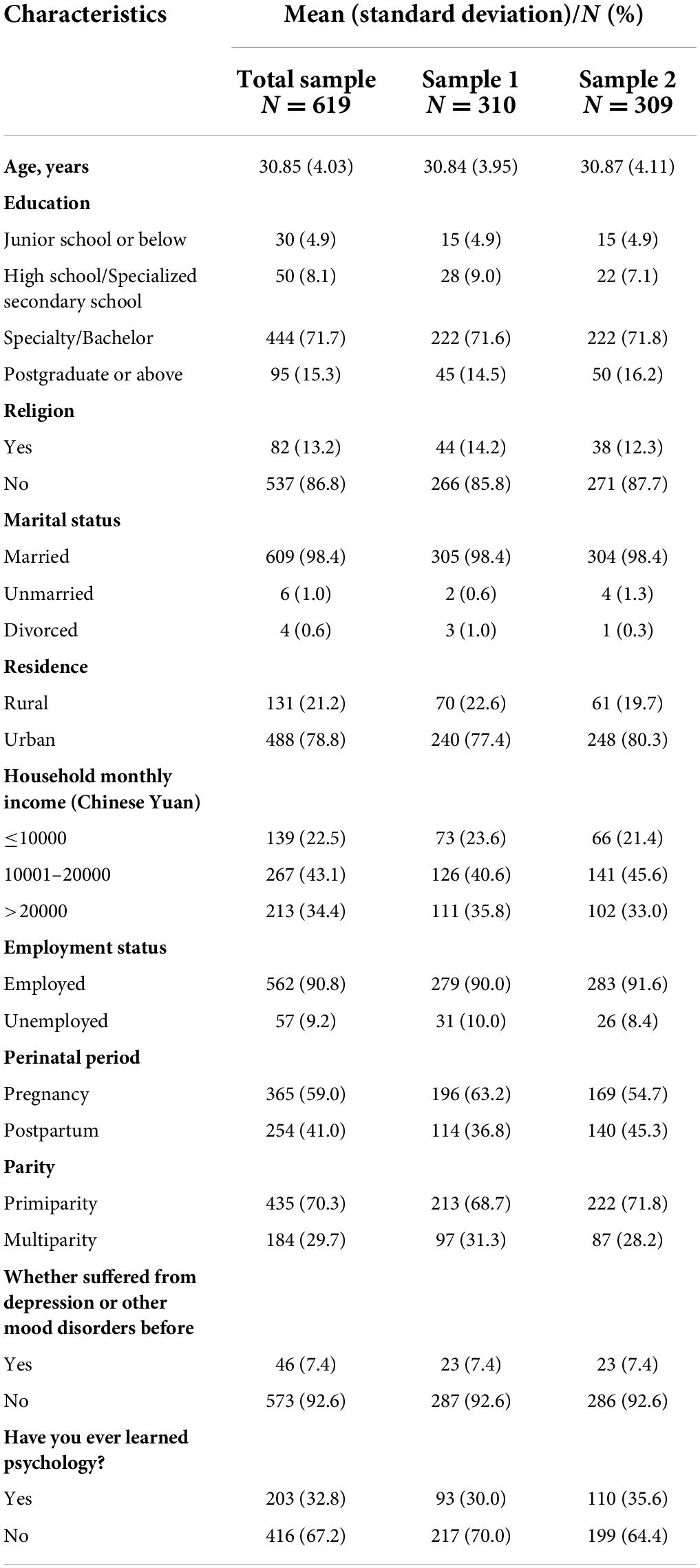
Table 1. Characteristics of the included participants.
After deleting two items (19 and 20) with no significant difference in the extreme group comparison, the CR values of the remaining 29 items were >3.0. Then, according to the results of the correlation coefficient method, all items met the standard and were retained. Specifically, the score of item 24 was significantly correlated with the total scale score (P < 0.01) despite the coefficient value being 0.236 (<0.3), whereas the item-total correlation values ranged from 0.303 to 0.593 for the remaining 28 items (Table 2). No individual item was found to greatly increase the Cronbach’s α or McDonald’s ω if deleted.
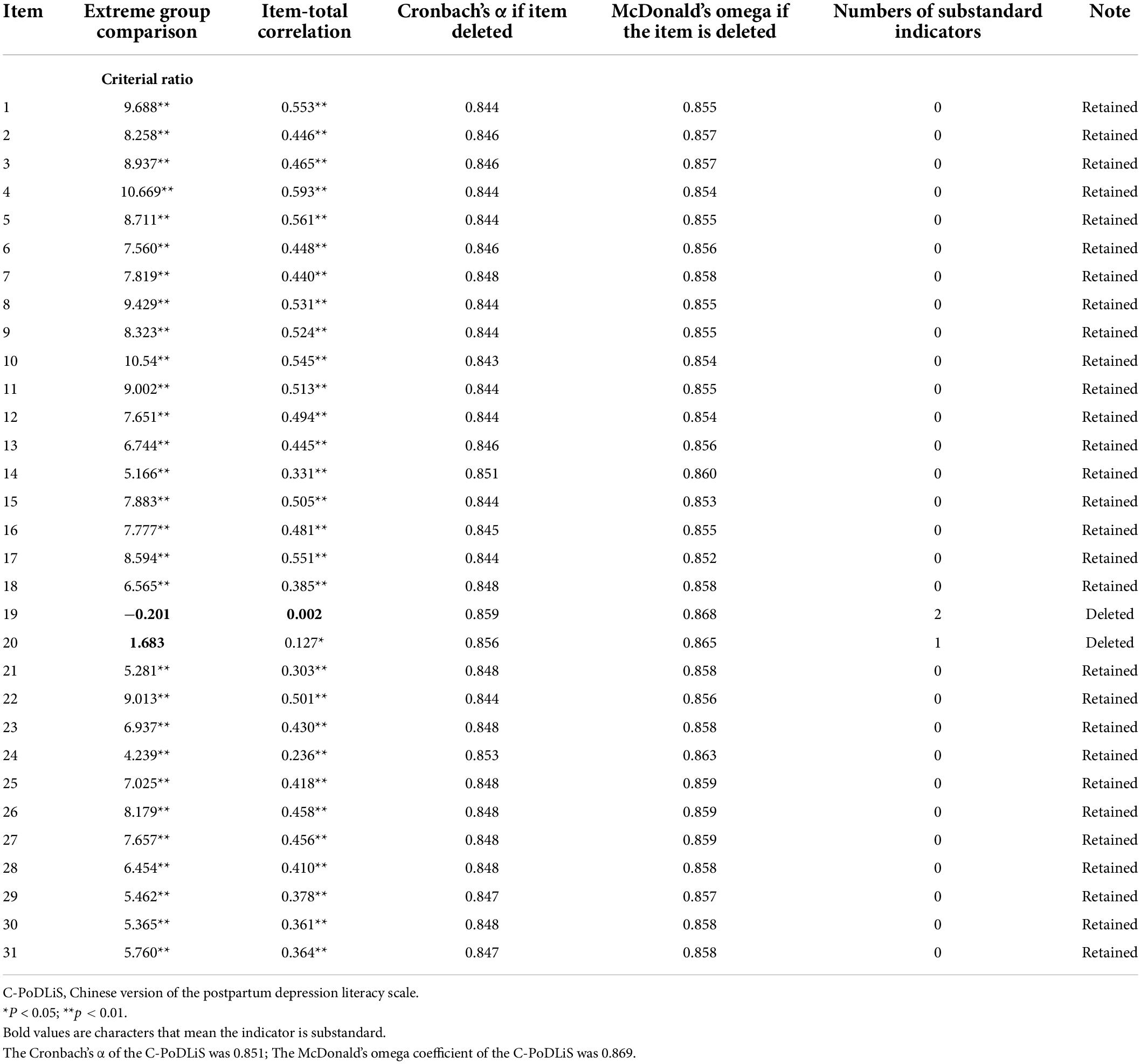
Table 2. Item analysis.
The results of 29 items showed a KMO value of 0.821 and the Bartlett spherical test value of 3490.603 (χ2 = 3490.603, df = 351, p < 0.001), which demonstrated that the data set was adequate for EFA. In the first EFA, the item 7 and item 14 were removed sequentially because they were inconsistent with the pre-defined subscales. Ultimately, on the basis of the scree plot (Figure 2) and a second EFA, six factors were extracted with eigenvalues > 1.0 (6.32, 2.88, 2.71, 1.76, 1.45, and 1.36) that explained 61.00% of the total variance, of which factors 1, 2, 3, 4, 5, and 6 explained 23.39, 10.65, 10.03, 6.51, 5.39, and 5.04% of the variance, respectively (Supplementary Table 2). Moreover, the factor loadings were >0.45, and the remaining 27 items loaded onto the predefined factor.
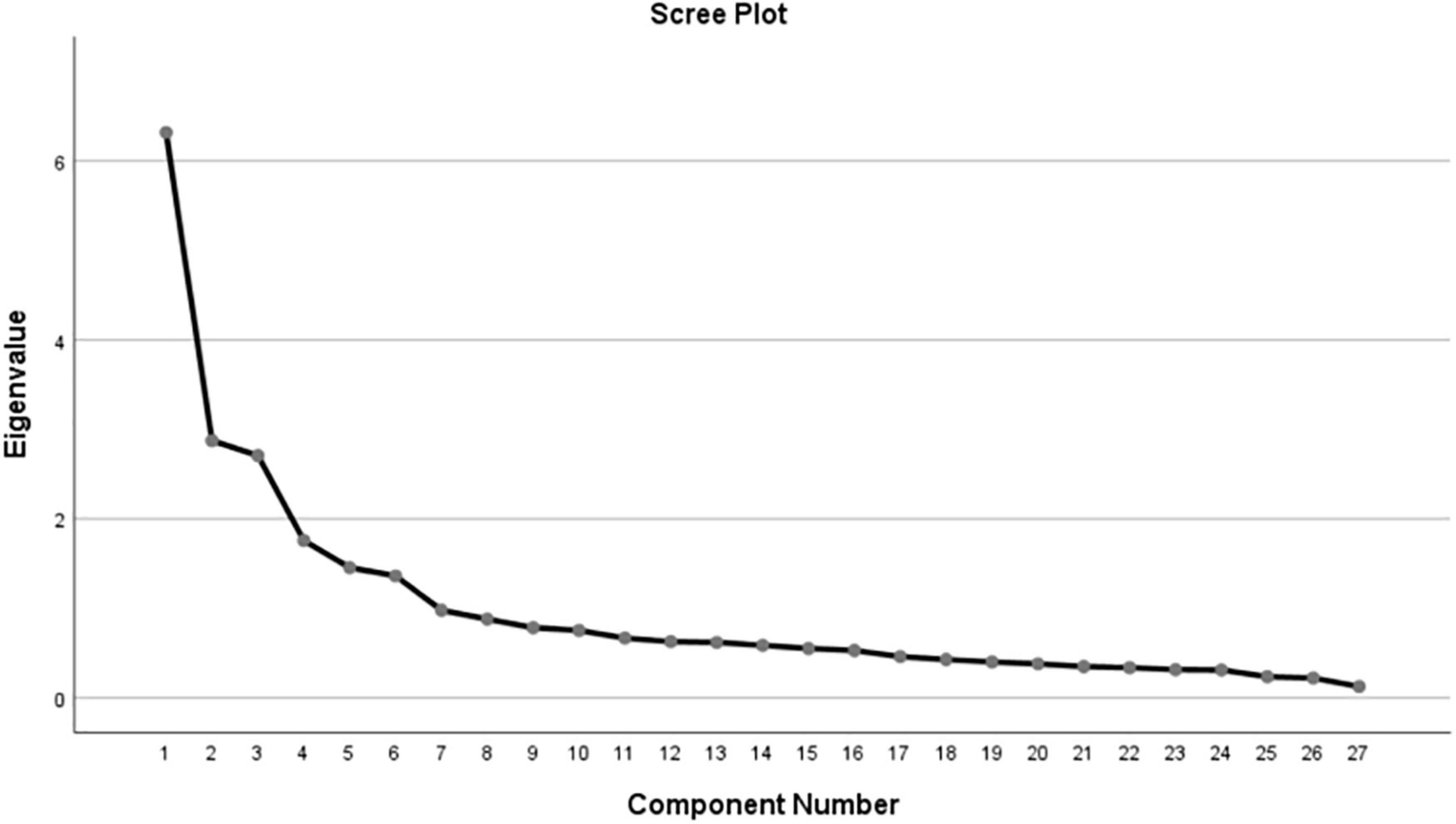
Figure 2. The scree plot.
Confirmatory factor analysis was conducted to confirm the EFA-derived 27-item six-factor structure. The t-values of all items were higher than 1.96 (the results were not shown specifically), and all items presented factor loadings > 0.32 (Figure 3). The initial model indices suggested an inadequate fit on the basis of GFI, IFI, CFI, and TLI (χ2/df = 2.062, RMSEA = 0.059, GFI = 0.863, IFI = 0.897, CFI = 0.895, and TLI = 0.881). Three paths of covariance between errors were added based on the modification indices. The adjusted model achieved a good fit to the data (χ2/df = 1.532, RMSEA = 0.042, GFI = 0.900, IFI = 0.949, CFI = 0.948, and TLI = 0.940) (Figure 3).
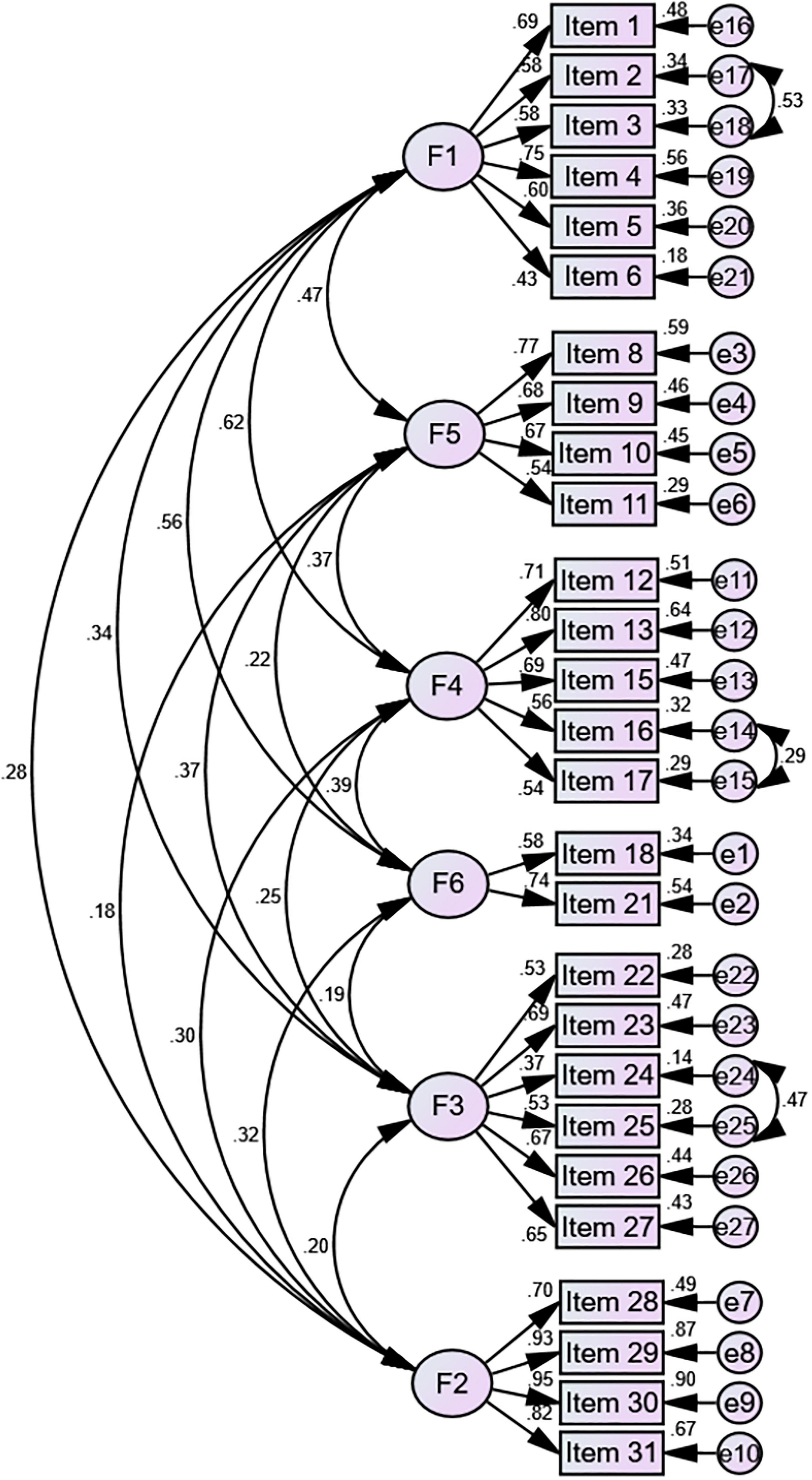
Figure 3. Modified confirmatory factor analysis of the six factor 27-item model.
The values of AVE for four subscales were above the desired threshold of 0.50 and for the other two subscales were very close to 0.5. Moreover, all subscales’ √AVE scores exceeded each of their correlations with other subscales (Table 3), indicating good discriminant validity.
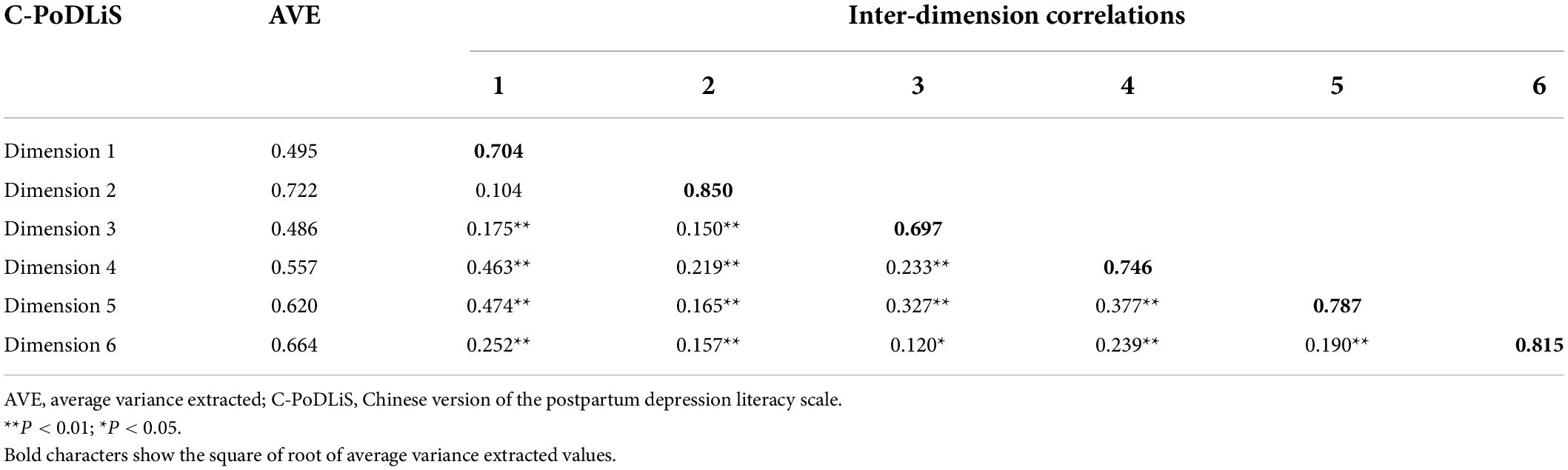
Table 3. Correlation coefficient and AVE.
The Cronbach’s α of the C-PoDLiS was 0.862, and the subscales ranged from 0.679 to 0.880. The McDonald’s ω was 0.869 for the total scale, whereas the subscales ranged from 0.689 to 0.889. And the ICC for the total scale was 0.856 and for the six factors ranged from 0.633 to 0.748 (Table 4).

Table 4. Reliability analysis of the C-PoDLiS.
The C-PoDLiS scores ranged from 1 to 5. These results revealed no floor and ceiling effects as no perinatal women recorded the highest or lowest possible score.
Regarding concurrent validity, the C-PoDLiS demonstrated significant positive correlations with MHLS and its six dimensions among 290 perinatal women (r = 0.155–0.581, p < 0.01) (Table 5). For predictive validity, the C-PoDLiS also had significant positive correlations with ATSPPH-SF and its two dimensions in a cross-sectional study of 100 perinatal women (r = 0.361–0.432, p < 0.01) (Table 6).

Table 5. Correlations of the C-PoDLiS and MHLS subscales.
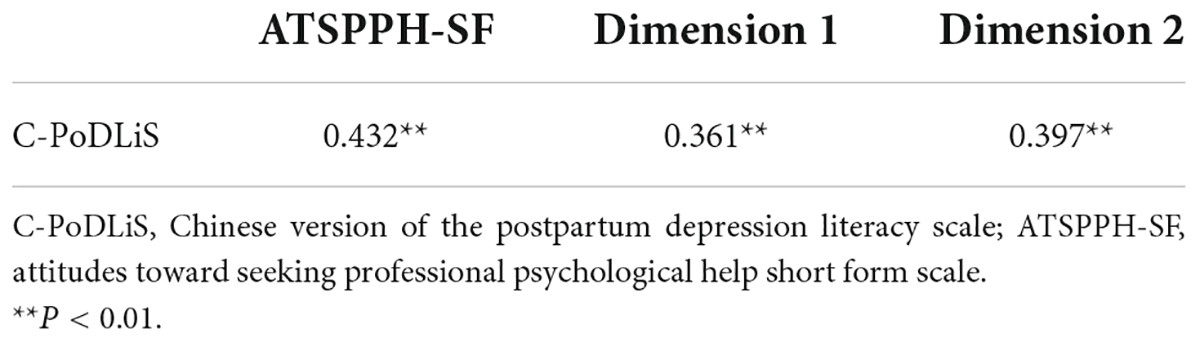
Table 6. Correlations of the C-PoDLiS and ATSPPH-SF subscales.
The final version of the C-PoDLiS has 27 items grouped into six domains. The detailed contents and the instructions for scoring are shown in the Supplementary Table 1. Regarding the PoDLi of participants in this study, the total mean score was 3.80 ± 0.38. The average scores of each factor ranking from the highest to the lowest were 4.25 ± 0.64 (factor 5: knowledge of risk factors and causes), 4.16 ± 0.51 (factor 4: knowledge and belief of self-care activities), 3.81 ± 0.60 (factor 3: attitudes toward promoting recognition of PPD or appropriate help-seeking behaviors), 3.65 ± 0.61 (factor 1: recognition abilities of PPD), 3.45 ± 0.71 (factor 6: knowledge and beliefs about professional help available), and 3.30 ± 0.70 (factor 2: ability to seek and judge information related to PPD).
The PoDLi is closely associated with the occurrence, recognition, and treatment of PPD (Gazmararian et al., 2000; Francis et al., 2007). Consequently, it is essential to find an evidence-based, convenient, and practical instrument specifically to quantity the level of PoDLi among perinatal women in China. To our knowledge, the present study is the first to cross-culturally adapt and validate the PoDLiS among the Chinese population. The psychometric validation was conducted under the guidelines of the COSMIN checklist (Mokkink et al., 2010a; Prinsen et al., 2018). The results suggested satisfactory internal consistency (Cronbach’s α = 0.862 and McDonald’s ω = 0.869), adequate stability (ICC = 0.856), sufficient or acceptable validity (content validity, structural validity, convergent and discriminant validity, concurrent validity, and predictive validity), and no floor or ceiling effect of the C-PoDLiS. The six-factor model explained 61.00% of the total variance. The participants completed the scale in a maximum of 10 min. Overall, the C-PoDLiS can serve as a valid, reliable, and practicable measurement tool for evaluating the level of PoDLi among perinatal women in mainland China.
Results of this study painted a preliminary picture of the level of PoDLi in perinatal women in China. The findings suggested that the PoDLi level (3.80 ± 0.38) among Chinese perinatal women was in the moderate range, which was very close to the findings in the Iran (3.79 ± 0.39) (Mirsalimi et al., 2020) and Malaysia (3.78 ± 0.37) (Hairol et al., 2021) samples, and a study in India (Poreddi et al., 2021) showed that only half of postpartum mothers had adequate levels of PoDLi. Consequently, there is an imperative need, both in China and many other developing countries, to sensitize perinatal women about PPD via various approaches such as presenting knowledge of PPD in community campaigns and pregnancy schools, thereby creating awareness of PPD and improving help-seeking behaviors. Moreover, the lowest mean score of factor was observed on factor 2: ability to seek and judge information related to PPD (3.30 ± 0.70) in this study, which was congruent with the study in India (Poreddi et al., 2021) but different from the study in Iran (Mirsalimi et al., 2020). Even more interesting is that the lowest-scoring dimension in the study from Iran (beliefs about professional help available) (Mirsalimi et al., 2020) was precisely the highest-scoring dimension in India (Poreddi et al., 2021). Accordingly, it could be concluded that the specific gaps and deficient elements in PoDLi vary widely among perinatal women in different countries, so PoDLi improvement programs in the future should be culturally tailored.
In the process of translation and cross-cultural adaptation, we strictly followed the international multiphase translation guidelines (Beaton et al., 2000) and sought advice from the developer of PoDLiS (Dr. Mirsalimi) to guarantee the content equivalence between the source and target versions. Compared with the PoDLiS, four items were merged, respectively, into two, two new items were added, and minor modifications to some words and statements were made in the preliminary C-PoDLiS, which has reduced the redundancy, improved the succinctness, and guaranteed the comprehensiveness of the scale’s content, as well as made the C-PoDLiS more in line with China’s actual condition and Chinese expression habits. What deserves to be mentioned is that most of the items had cultural equivalent terms in Chinese, so the translation could be completed without extensive cultural adaptation. In addition, based on the principle that a single item cannot be a dimension by itself (Wu, 2010), two dimensions of the original PoDLiS were merged. Therefore, the preliminary C-PoDLiS consisted of 6 domains, which was more in accordance with Jorm’s definition of MHL (Jorm, 2000) in spite of a slight difference from the 7-domain structure of the original PoDLiS (Mirsalimi et al., 2020). Eventually, the 33-participant pilot testing confirmed the good face validity of the C-PoDLiS and the second round of expert consultations revealed excellent content validity (I-CVI = 0.86–1.00 and S-CVI = 0.915).
With regard to item analysis, two items (item 13: “Antidepressants are addictive” and item 14: “Antidepressants cause brain damage”), both in the dimension of “Knowledge and beliefs about professional help available,” were omitted because of the non-significant differences in the extreme group comparison. One possible reason for the non-significant differences may be a general lack of knowledge of antidepressants by perinatal women (Muzik and Hamilton, 2016), which made it difficult to score these items correctly even for participants in the group with a higher score of PoDLiS. This phenomenon reinforces the notion that healthcare professionals are necessary to be proactive in improving perinatal women’s knowledge about professional treatment of PPD. Noteworthily, the new added item (item 33: “Antidepressants are effective in treating PPD”) that has similar content (all were about the efficacy of antidepressants) but a reverse scoring compared to the two deleted items, was finally retained in C-PoDLiS, which could remedy the defect of the damaged content comprehensiveness of the scale to some extent caused by the above-mentioned items’ deletion.
Factor analysis was carried out to determine the degree to which participants’ scores on C-PoDLiS were an adequate reflection of the dimensionality of the structure being measured and the conceptual framework on which it is based. In EFA, two items (item 14: “Religious practices, prayer and going to holy shrine are helpful for the prevention and management of PPD,” and item 7: “How likely is it that PPD might be caused by a genetic or inherited problem”) were eliminated because they loaded on a different factor compared to their pre-defined factor, which could not be explained theoretically. The reason for the mismatch of item 14 may be resulted from the difference in sample characteristics. To be specific, 86.75% (537/619) of the participants recruited in this study were non-religious, so religious activities could hardly be considered as self-care activities for most of them, while the data set in the original PoDLiS was from Iranian perinatal women who believe in Islam with great probability (Mirsalimi et al., 2020). What should be pointed out is that in some areas of mainland China, especially in the settlements and autonomous regions of ethnic minorities, religion is relatively common. Hence, considering that item 14 may be meaningful to some perinatal crowds in China, it is necessary for future studies to apply appropriate adjustments and retest this item. For item 7, whether or not genetic and inherited problems are the etiology of PPD is still controversial at present (Starnawska et al., 2021; Kiewa et al., 2022). Meanwhile, some experts pointed out in the first round of expert consultations that since genetic and inherited problems are incurable, item 7 could be a double-edged sword for perinatal women; on one hand, this item could enlighten the participants with genetic and inherited problems related to depression to pay more attention to their mental health during the perinatal period, while on the other hand, it might increase their concerns about developing PPD. After due consideration of experts’ suggestions and the results of EFA, item 7 was finally removed. Ultimately, the 27-item 6-factor model that was generated from EFA was in line with the pre-designed framework in the preliminary C-PoDLiS and explained a much higher proportion of the total variance than the original 31-item PoDLiS (61.00% vs. 49.00%), which reflected that the C-PoDLiS was more in accord with the Chinese cultural background and medical environment after adjustment. In CFA, the performance of the initial model fit indices was less satisfactory, so based on the modification recommendations, three error covariances were added (Figure 3). Before the modification, we had checked the specific contents of relevant items and believed that these covariances were plausible as there were indeed strong correlations between these items. Ultimately, all of the goodness-of-fit indexes in the adjusted model reached a good level. In addition, acceptable convergent validity (AVE = 0.486–0.722) and good discriminant validity were also given the reasonable fit of the 6-factor model. Generally speaking, C-PoDLiS is in line with the definition of PoDLi and is adequate to measure Chinese perinatal women’s level of PoDLi.
For reliability, the total Cronbach’s α was estimated to be 0.862 for excellent internal consistency, indicating that all items contribute to the global construct measured, which is far higher than the original version (Cronbach’s α 0.78) (Mirsalimi et al., 2020) and the Malay version (Cronbach’s α 0.73) (Hairol et al., 2021). When considering the factor structure, α values exceeding 0.7 were discovered for five factors, whereas factor 4 consisting of 2 items had a lower but acceptable Cronbach’s α (0.679). As Cronbach’s α is very sensitive to the number of items in scales, it is common to detect lower α values in factors with a few items (Streiner, 2003). The results of McDonald’s ω (0.689–0.0.889), a more accurate coefficient of internal consistency, further supported the satisfactory reliability of the C-PoDLiS. The ICC scores of the PoDLiS (0.633–0.856) were assessed for the first time in this study and revealed appropriate stability for the scale. This feature is quite important when the C-PoDLiS is applied to evaluate the effectiveness of interventions on ameliorating the PoDLi level. Additionally, the absence of floor/ceiling effects for the total score of C-PoDLiS suggested that C-PoDLiS could discriminate between participants at either extreme of the scale and confirmed its applicability in Chinese perinatal women.
The evaluation of criterion validity of C-PoDLiS represented a novelty because it had never been assessed before. In terms of concurrent validity, since there is no adequate instrument as a gold standard for assessing MHL or depression literacy, the concurrent validity of C-PoDLiS was measured with MHLS that has been extensively tested for good reliability and validity and has been widely applied among various Chinese populations (Han et al., 2019; Ma, 2019; Chen et al., 2021). As expected, statistically significant correlations between the scores of the C-PoDLiS and the MHLS were discovered (Table 6), suggesting that the C-PoDLiS was sensitive enough to assess similar features as the MHLS. However, all of the association coefficients were moderate or small, which might be caused by the differences in essential attributes of the items between the two scales, as the MHLS measures a broad, generic construct (MHL) and PoDLi is perhaps too specific for a relationship between the two instruments. Future studies may assess the correlation between the C-PoDLiS and other psychometrically sound instruments having similar constructs, such as the 22-item Depression Literacy scale (Fonseca et al., 2017), to further verify the concurrent validity of C-PoDLiS. Moreover, the testing of predictive validity based on correlations between the scores of the C-PoDLiS and ATSPPH-SF revealed moderately positive significant correlations, indicating that perinatal women with a greater level of PoDLi will have a more favorable attitude toward professional psychological help-seeking. The findings further verified C-PoDLiS’s good validity and were consistent with previous studies in urban adults (Ho et al., 2018) and adolescent males (Clark et al., 2020). Nevertheless, this correlation study was not able to establish a causal relationship between the C-PoDLiS and the ATSPPH-SF. It will be worthwhile for future studies to address this unknown by investigating whether PoDLi promotion strategies can also improve attitudes toward PPD and its treatment.
Some important limitations should be acknowledged. First, although we tried to control the biases of our results by expanding the sample size and distributing questionnaires by well-trained researchers, the generalizability of the results of this study might still be threatened, as the participants were recruited from the Han ethnic group at a single tertiary hospital in the southeast coastal area of China, and more than half of the participants had a monthly household income above the national average and were well educated with a specialty/bachelor’s degree or above. Future research should include more diverse samples from various regions of China covering perinatal women of different ethnics, incomes, and educational levels to guarantee adequate representation and generalizability of this instrument in the entire country. Second, this validation study was performed on the basis of classical test theory, so the conclusion on the quality of the instrument’s measurement properties were population-dependent. It will be beneficial to conduct rasch analysis based on the non-parametric item response theory in future research, which allows conclusion to be drawn independently from the tested population (Nguyen et al., 2022), to provide additional important information on C-PoDLiS psychometric properties. Third, it is difficult for us to adequately compare our findings with the other relevant studies (Mirsalimi et al., 2020; Hairol et al., 2021; Poreddi et al., 2021) for the reason that, except for the study of developing the original version of PoDLiS (Mirsalimi et al., 2020), none of the others (Hairol et al., 2021; Poreddi et al., 2021) had performed formal evaluation of the psychometric properties of PoDLiS with Cronbach’s α reported only. As such, future studies need to evaluate and report the psychometric properties of the PoDLiS formally, which can enable the comparison between different versions of the PoDLiS and promote the popularization of the scale internationally. Finally, the cross-sectional study design precluded the explanation of causal relationships among variables as well as the assessment of the responsiveness of the C-PoDLiS, so longitudinal research will be needed for further validation.
This study has several potential implications for academic and clinical practice. First, on the individual level, the assessment of PoDLi from a self-evaluated perspective may raise perinatal women’s awareness of their mental health status, which can in turn promote them to utilize professional help-seeking when necessary. Moreover, at the academic level, C-PoDLiS paves the way for healthcare professionals to further conduct studies with regard to PoDLi and its influencing factors. Their findings will be helpful in better understanding specific elements of PoDLi that are lacking among Chinese perinatal women as well as identifying individuals with poor PoDLi levels, which lays the foundation for developing more effective and targeted interventions to improve the PoDLi level. At the same time, medical staff can use C-PoDLiS to evaluate the effectiveness of intervention programs, thereby adjusting the intervention strategies timely according to the evaluated results to maximize the intervention effects. Furthermore, on the national level, C-PoDLiS can inform the decision-making process for public health officials and can serve as a reference tool for the government and stakeholders to establish affordable mental health policies, as it is highly understandable and easily administered and can penetrate all layers of the community. More importantly, on the global level, this study provided the world with the data of PoDLi in China, enriching the evidence in the relevant field. However, additional studies are still required to verify the validity of the PoDLiS in other countries and different regions with different cultures, because a universal instrument can help with data aggregation and outcome comparisons across different studies and populations, as well as facilitate cross-border discussion of the PoDLi.
Collectively, the 27-item, 6-dimension C-PoDLiS has satisfactory reliability and validity. It is an effective and concise instrument for evaluating the PoDLi level among perinatal women in China and consequently helping healthcare professionals to develop and implement effective and targeted interventions. Nevertheless, its application warrants further investigation in larger samples of Chinese perinatal women in different settings and areas.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Women’s Hospital, School of Medicine, Zhejiang University. The patients/participants provided their written informed consent to participate in this study.
All authors made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, involved in drafting the manuscript or revised it critically for important intellectual content, gave final approval of the revision to be published, participated sufficiently in the work to take public responsibility for appropriate portions of the content, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
We would like to express our sincere appreciation to the experts, the original author of the scale, and all of the study participants.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.966770/full#supplementary-material
ATSPPH-SF, attitudes toward seeking professional psychological help short form scale; AVE, average variance extracted; CFA, confirmatory factor analysis; CFI, comparative fit index; COSMIN, Consensus-based Standards for the Selection of Health Status Measurement Instruments; CR, critical ratio; C-PoDLiS, Chinese version of postpartum depression literacy scale; EFA, exploratory factor analysis; GFI, goodness of fit; ICC, intraclass correlation coefficient; I-CVI, content validity index of items; IFI, incremental fit index; KMO, Kaiser–Meyer–Olkin; MHL, mental health literacy; MHLS, mental health literacy scale; PPD, postpartum depression; PoDLi, postpartum depression literacy; PoDLiS, postpartum depression literacy scale; RMSEA, root mean square error of approximation; S-CVI, scale-level content validity index; TLI, Tucker–Lewis index.
Albert, P. (2015). Why is depression more prevalent in women? J. Psychiatry Neurosci. 40, 219–221. doi: 10.1503/jpn.150205
American PsychiatricAssociation (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5, (5th Edn). Washington, DC: American Psychiatric, Publishing. doi: 10.1176/appi.books.9780890425596
Andresen, E. M. (2000). Criteria for assessing the tools of disability outcomes research. Arch. Phys. Med. Rehabil. 81, S15–S20. doi: 10.1053/apmr.2000.20619
Ashley, J., Harper, B., Arms-Chavez, C., and LoBello, S. (2016). Estimated prevalence of antenatal depression in the US population. Arch. Womens Ment. Health 19, 395–400. doi: 10.1007/s00737-015-0593-1
Beaton, D. E., Bombardier, C., Guillemin, F., and Ferraz, M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25, 3186–3191. doi: 10.1097/00007632-200012150-00014
Bernstein, K., Lee, Y., Gona, P., Han, S., Kim, S., and Kim, S. (2021). Depression, Depression Literacy, and Sociodemographic Characteristics of Korean Americans: A Preliminary Investigation. J. Immigr. Minor. Health 23, 547–557. doi: 10.1007/s10903-020-01092-5
Bilszta, J., Ericksen, J., Buist, A., and Milgrom, J. (2010). Women’s experience of postnatal depression: Beliefs and attitudes as barriers to care. Aust. J. Adv. Nurs. 27, 44–54.
Bjelica, A., Cetkovic, N., Trninic-Pjevic, A., and Mladenovic-Segedi, L. (2018). The phenomenon of pregnancy - a psychological view. Ginekologia polska 89, 102–106. doi: 10.5603/GP.a2018.0017
Brown, T. A. (2006). Confirmatory Factor Analysis for Applied Research, (2nd Edn). New York, NY: Guildford Press.
Buist, A., Speelman, C., Hayes, B., Reay, R., Milgrom, J., Meyer, D., et al. (2007). Impact of education on women with perinatal depression. J. Psychosom. Obstet. Gynecol. 28, 49–54. doi: 10.1080/01674820601143187
Callister, L. C., Beckstrand, R. L., and Corbett, C. (2019). Postpartum depression and helpseeking behaviors in immigrant Hispanic women. J. Obstet. Gynecol. Neonatal Nurs. 40, 440–449. doi: 10.1111/j.1552-6909.2011.01254.x
Canino, G., and Alegría, M. (2008). Psychiatric diagnosis – is it universal or relative to culture? J. Child Psychol. Psychiat. 49, 237–250. doi: 10.1111/j.1469-7610.2007.01854.x
Chen, P., Liu, X., Wang, X., Yang, B., Ruan, J., and Liu, Z. (2020). Attitude Toward Seeking Professional Psychological Help Among Community-Dwelling Population in China. Front. Psychiatry 11:417. doi: 10.3389/fpsyt.2020.00417
Chen, S., Chen, K., Wang, S., Wang, W., and Li, Y. (2021). Initial Validation of a Chinese Version of the Mental Health Literacy Scale Among Chinese Teachers in Henan Province. Front. Psychiatry 12:661903. doi: 10.3389/fpsyt.2021.661903
Clark, L., Hudson, J., Rapee, R., and Grasby, K. (2020). Investigating the impact of masculinity on the relationship between anxiety specific mental health literacy and mental health help-seeking in adolescent males. J. Anxiety Disord. 76:102292. doi: 10.1016/j.janxdis.2020.102292
Dennis, C., and Chung-Lee, L. (2006). Postpartum depression help-seeking barriers and maternal treatment preferences: A qualitative systematic review. Birth 33, 323–331. doi: 10.1111/j.1523-536X.2006.00130.x
Evagorou, O., Arvaniti, A., and Samakouri, M. (2016). Cross-Cultural Approach of Postpartum Depression: Manifestation, Practices Applied, Risk Factors and Therapeutic Interventions. Psychiat. Q. 87, 129–154. doi: 10.1007/s11126-015-9367-1
Fang, S., Yang, B. X., Yang, F., and Zhou, Y. (2019). Study on reliability and validity of the Chinese version of the Attitudes toward Seeking Professional Psychological Help Scale-Short Form for community population in China. Chin. Nurs. Res. 33, 2410–2414.
Field, T. (2018). Postnatal anxiety prevalence, predictors and effects on development: A narrative review. Infant Behav. Dev. 51, 24–32. doi: 10.1016/j.infbeh.2018.02.005
Fischer, E. H., and Farina, A. (1995). Attitudes Toward Seeking Professional Psychological help: A shortened for and considerations for research. J. Coll. Stud. Dev. 36, 368–373. doi: 10.1037/t05375-000
Fonseca, A., Gorayeb, R., and Canavarro, M. C. (2015). Women’s help-seeking behaviours for depressive symptoms during the perinatal period: Socio-demographic and clinical correlates and perceived barriers to seeking professional help. Midwifery 31, 1177–1185. doi: 10.1016/j.midw.2015.09.002
Fonseca, A., Silva, S., and Canavarro, M. (2017). Depression Literacy and Awareness of Psychopathological Symptoms During the Perinatal Period. J. Obstet. Gynecol. Neonatal Nurs. 46, 197–208. doi: 10.1016/j.jogn.2016.10.006
Fornell, C., and Larcker, D. F. (1981). Structural equation models with unobservable variables and measurement error: Algebra and statistics. J. Mark. Res. 18, 382–388. doi: 10.1177/002224378101800313
Francis, L., Weiss, B. D., Senf, J. H., Heist, K., and Hargraves, R. (2007). Does literacy education improve symptoms of depression and self-efficacy in individuals with low literacy and depressive symptoms? A preliminary investigation. J. Am. Board Fam. Med. 20, 23–27. doi: 10.3122/jabfm.2007.01.060058
Gazmararian, J., Baker, D., Parker, R., and Blazer, D. G. (2000). A multivariate analysis of factors associated with depression: Evaluating the role of health literacy as a potential contributor. Arch. Intern. Med. 160, 3307–3314. doi: 10.1001/archinte.160.21.3307
Geier, M., Hills, N., Gonzales, M., Tum, K., and Finley, P. (2015). Detection and treatment rates for perinatal depression in a state Medicaid population. CNS Spectr. 20, 11–19. doi: 10.1017/s1092852914000510
Guy, S., Sterling, B. S., Walker, L. O., and Harrison, T. C. (2014). Mental health literacy and postpartum depression: A qualitative description of views of lower income women. Arch. Psychiatr. Nurs. 28, 256–262. doi: 10.1016/j.apnu.2014.04.001
Hahn-Holbrook, J., and Cornwell-Hinrichs, T. I. A. (2018). Economic and health predictors of national postpartum depression prevalence: A systematic review, meta-analysis, and meta-regression of 291 studies from 56 countries. Front. Psychiatry 8:248. doi: 10.3389/fpsyt.2017.00248
Hair, J. F., Black, B., Babin, B., Anderson, R. E., and Tatham, R. L. (2010). Multivariate Data Analysis, (7th Edn). Upper Saddle River: Prentice Hall.
Hairol, M. I., Ahmad, S., Sharanjeet-Kaur, S., Hum Wee, L., Abdullah, F., and Ahmad, M. (2021). Incidence and predictors of postpartum depression among postpartum mothers in Kuala Lumpur, Malaysia: A cross-sectional study. PLoS One 16:e0259782. doi: 10.1371/journal.pone.0259782
Han, Z., Wang, D., Ouyang, L., Niu, P., and Yun, Z. (2019). Adaptation and psychometric properties of mental health literacy scale in Chinese elite athletes. Hubei Sports Sci. 38, 226–229.
Ho, G., Bressington, D., Leung, S., Lam, K., Leung, A., Molassiotis, A., et al. (2018). Depression literacy and health-seeking attitudes in the Western Pacific region: A mixed-methods study. Soc. Psychiatry Psychiatr. Epidemiol. 53, 1039–1049. doi: 10.1007/s00127-018-1538-6
Hu, Y., Tiew, L., and Li, F. (2019). Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practice. BMC Med. Res. Methodol. 19:21. doi: 10.1186/s12874-019-0662-7
Husain, N., Bevc, I., Husain, M., Chaudhry, I. B., and Atif, N. A. R. (2006). Prevalence and social correlates of postnatal depression in a low income country. Arch. Womens Ment. Health 9, 197–202. doi: 10.1007/s00737-006-0129-9
Jorm, A. F. (2000). Mental health literacy: Public knowledge and beliefs about mental disorders. Br. J. Psychiatry 177, 396–401. doi: 10.1192/bjp.177.5.396
Kiewa, J., Meltzer-Brody, S., Milgrom, J., Guintivano, J., Hickie, I., Whiteman, D., et al. (2022). Perinatal depression is associated with a higher polygenic risk for major depressive disorder than non-perinatal depression. Depress. Anxiety 39, 182–191. doi: 10.1002/da.23232
Ko, J. Y., Farr, S. L., Dietz, P. M., and Robbins, C. L. (2012). Depression and treatment among U.S. pregnant and nonpregnant women of reproductive age, 2005–2009. J. Womens Health 21, 830–836. doi: 10.1089/jwh.2011.3466
Li, K., Fu, M., Zhao, Q., and Chen, L. (2016). Translation and evaluation of Chinese version of the symptom experience index. Int. J. Nurs. Pract. 22, 556–564. doi: 10.1111/ijn.12464
Ma, X. X. (2019). Study on the Validity and Reliability of the Chinese Version of the Mental Health Literacy Scale. Ph.D thesis, Hangzhou: Hangzhou Normal University.
McCarthy, M., and McMahon, C. (2008). Acceptance and experience of treatment for postnatal depression in a community mental health setting. Health Care Women Int. 29, 618–637. doi: 10.1080/07399330802089172
Mirsalimi, F., Ghofranipour, F., Noroozi, A., and Montazeri, A. (2020). The postpartum depression literacy scale (PoDLiS): Development and psychometric properties. BMC Pregnancy Childbirth 20:13. doi: 10.1186/s12884-019-2705-9
Mokkink, L. B., Terwee, C. B., Patrick, D. L., Alonso, J., Stratford, P. W., Knol, D. L., et al. (2010a). The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 19, 539–549. doi: 10.1007/s11136-010-9606-8
Mokkink, L. B., Terwee, C. B., Patrick, D. L., Alonso, J., Stratford, P. W., Knol, D. L., et al. (2010b). The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 63, 737–745. doi: 10.1016/j.jclinepi.2010.02.006
Mu, T. Y., Li, Y. H., Pan, H. F., Zhang, L., Zha, D. H., Zhang, C. L., et al. (2019). Postpartum depressive mood (PDM) among Chinese women: A meta-analysis. Arch. Womens Ment. Health 22, 279–287. doi: 10.1007/s00737-018-0885-3
Muzik, M., and Hamilton, S. (2016). Use of Antidepressants During Pregnancy?: What to Consider when Weighing Treatment with Antidepressants Against Untreated Depression. Matern. Child Health J. 20, 2268–2279. doi: 10.1007/s10995-016-2038-5
National Bureau of Statistics of China (2018). Statistical Yearbook of China’s Health and Family Planning. Beijing: National Bureau of Statistics of China.
Nguyen, T., Lee, C., and Kim, M. (2022). Using item response theory to develop and refine patient-reported outcome measures. Eur. J. Cardiovasc. Nurs. 21, 509–515. doi: 10.1093/eurjcn/zvac020
Nisar, A., Yin, J., Waqas, A., Bai, X., Wang, D., Rahman, A., et al. (2020). Prevalence of perinatal depression and its determinants in Mainland China: A systematic review and meta-analysis. J. Affect. Disord. 277, 1022–1037. doi: 10.1016/j.jad.2020.07.046
O’Connor, M., and Casey, L. (2015). The Mental Health Literacy Scale (MHLS): A new scale-based measure of mental health literacy. Psychiatry Res. 229, 511–516. doi: 10.1016/j.psychres.2015.05.064
Odukoya, J., Adekeye, O., Igbinoba, A., and Afolabi, A. (2018). Item analysis of university-wide multiple choice objective examinations: The experience of a Nigerian private university. Qual. Quant. 52, 983–997. doi: 10.1007/s11135-017-0499-2
O’Hara, M., and McCabe, J. (2013). Postpartum depression: Current status and future directions. Annu. Rev. Clin. Psychol. 9, 379–407. doi: 10.1146/annurev-clinpsy-050212-185612
Onchonga, D., Hammoud, S., Kuriakose, S., and Muhammad, E. (2021). Exploring fear of childbirth in Kenya through evaluation of the readability of Wijma Delivery Expectancy/Experience Questionnaire Version A (W-DEQ-A). Sex. Reprod. Healthc. 28:100605. doi: 10.1016/j.srhc.2021.100605
Özcan, N., Boyacıoǧlu, N., and Dinç, H. (2017). Postpartum Depression Prevalence and Risk Factors in Turkey: A Systematic Review and Meta-Analysis. Arch. Psychiatr. Nurs. 31, 420–428. doi: 10.1016/j.apnu.2017.04.006
Perinetti, G. (2018). StaTips part IV: Selection, interpretation and reporting of the intraclass correlation coefficient. S. Eur. J. Orthod. Dentofac. Res. 5, 3–5. doi: 10.5937/sejodr5-17434
Peter, G. J. Y. (2014). The alpha and the omega of scale reliability and validity: Why and how to abandon Cronbach’s alpha and the route towards more comprehensive assessment of scale quality. Eur. Health Psychol. 16, 56–69.
Polit, D. F., and Beck, C. T. (2009). Essentials of Nursing Research: Appraising Evidence for Nursing Practice. Philadelphia: Lippincott Williams & Wilkins.
Pooler, J., Perry, D., and Ghandour, R. (2013). Prevalence and risk factors for postpartum depressive symptoms among women enrolled in WIC. Matern. Child Health J. 17, 1969–1980. doi: 10.1007/s10995-013-1224-y
Poreddi, V., Sundaram, V., Reddy, S., Bidadi, K., and Thimmaiah, R. (2021). Postpartum depression: Mental health literacy of Indian mothers. Arch. Psychiatr. Nurs. 35, 631–637. doi: 10.1016/j.apnu.2021.09.003
Prinsen, C. A. C., Mokkink, L. B., Bouter, L. M., Alonso, J., Patrick, D. L., de Vet, H. C. W., et al. (2018). COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 27, 1147–1157. doi: 10.1007/s11136-018-1798-3
Qu, D., Wang, Y., Zhang, Z., Meng, L., Zhu, F., Zheng, T., et al. (2021). Psychometric Properties of the Chinese Version of the Functional Assessment of Self-Mutilation (FASM) in Chinese Clinical Adolescents. Front. Psychiatry 12:755857. doi: 10.3389/fpsyt.2021.755857
Rahman, A., Surkan, P., Cayetano, C., Rwagatare, P., and Dickson, K. (2013). Grand challenges: Integrating maternal mental health into maternal and child health programmes. PLoS Med. 10:e1001442. doi: 10.1371/journal.pmed.1001442
Sharma, V., and Sharma, P. (2012). Postpartum depression: Diagnostic and treatment issues. J. Obstet. Gynaecol. Can. 34, 436–442. doi: 10.1016/s1701-2163(16)35240-9
Staneva, A., Bogossian, F., and Wittkowski, A. (2015). The experience of psychological distress, depression, and anxiety during pregnancy: A meta-synthesis of qualitative research. Midwifery 31, 563–573. doi: 10.1016/j.midw.2015.03.015
Starnawska, A., Bukowski, L., Chernomorchenko, A., Elfving, B., Müller, H., van den Oord, E., et al. (2021). DNA methylation of the KLK8 gene in depression symptomatology. Clin. Epigenet. 13:200. doi: 10.1186/s13148-021-01184-5
Streiner, D. (2003). Starting at the beginning: An introduction to coefficient alpha and internal consistency. J. Pers. Assess. 80, 99–103. doi: 10.1207/s15327752jpa8001_18
von Elm, E., Altman, D., Egger, M., Pocock, S., Gøtzsche, P., and Vandenbroucke, J. (2007). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 370, 1453–1457. doi: 10.1016/s0140-6736(07)61602-x
Williams, C., Turner, K., Burns, A., Evans, J., and Bennert, K. (2016). Midwives and women’s views on using UK recommended depression case finding questions in antenatal care. Midwifery 35, 39–46. doi: 10.1016/j.midw.2016.01.015
World Health Organization [WHO] (2013). Mental Health Action Plan 2013–2020: WHO Library Cataloguing-in-Publication Data. Geneva: WHO Press.
World Medical Association [WMA] (2008). WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects. Ferney-Voltaire: World Medical Association.
Wu, M. L. (2010). Questionnaire Statistical Analysis Practice: SPSS Operation and Application. Chongqing: Chongqing University Press.
Keywords: postpartum depression literacy, perinatal women, cultural adaptation, psychometric properties, scale, Chinese
Citation: Guo P, Cui N, Mao M, Zhang X, Chen D, Xu P, Wang X, Zhang W, Zheng Q, Zhang L, Xiang Z, Jin Y and Feng S (2022) Cross-cultural adaptation and psychometric properties of the Chinese version of the postpartum depression literacy scale. Front. Psychol. 13:966770. doi: 10.3389/fpsyg.2022.966770
Received: 13 June 2022; Accepted: 25 July 2022;
Published: 09 August 2022.
Edited by:
Noureddin Nakhostin Ansari, Tehran University of Medical Sciences, IranReviewed by:
Ipsa Mohapatra, Kalinga Institute of Medical Sciences (KIMS), IndiaCopyright © 2022 Guo, Cui, Mao, Zhang, Chen, Xu, Wang, Zhang, Zheng, Zhang, Xiang, Jin and Feng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suwen Feng, ZmVuZ3N3QHpqdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.