 André Rocha Mendonça
André Rocha Mendonça Lucas Machado Loureiro
Lucas Machado Loureiro Carlos Eduardo Nórte
Carlos Eduardo Nórte Jesus Landeira-Fernandez
Jesus Landeira-Fernandez- 1Department of Psychology, Pontifical Catholic University of Rio de Janeiro, Rio de Janeiro, Brazil
- 2Institute of Psychology, State University of Rio de Janeiro, Rio de Janeiro, Brazil
Introduction: Episodic memory is a cognitive process that allows the recall of experiences, learning, and the pursuit of future goals. During the aging process, episodic memory declines negatively, impacting social and psychological aspects in the elderly. Such intervention strategies as cognitive training are non-pharmacological ways of reducing these losses.
Objective: We systematically reviewed studies of the cognitive training of episodic memory in healthy elderly individuals and elderly individuals with clinical conditions.
Method: We systematically searched the PubMed, PsycNET, Web of Science, and SciELO databases using the descriptors “Episodic Memory” AND “Training” AND “Elderly” OR “Aging” OR “Dementia” in English and translated into Portuguese.
Results: Of the 572 articles that were identified by the search, 23 were included in the final analysis. The main variables that comprised the intervention protocols (i.e., characteristics of the sample, type of control group, mode of episodic memory training, and duration of training) were investigated, as well as the outcome variables, efficacy, and risk of bias. The main results indicated effectiveness with regard to different forms of the cognitive training of episodic memory.
Conclusion: Episodic memory training among the elderly can mitigate the negative effects of cognitive decline in dementia and healthy subjects promoting impacts at social, psychological, and economic levels. Although it is a widely studied topic, further empirical studies on the utility of episodic memory training in healthy elderly individuals and elderly individuals with clinical conditions are still needed.
Introduction
Episodic memory is a form of memory that allows the recall of events to enable learning and the pursuit of future goals based on an individual's experiences. According to Tulving (2002), episodic memory permits an individual to subjectively move through time (i.e., travel through his own self toward the past) while knowing that he is accessing remote experiences that were previously recorded. Thus, episodic memory has an explicit nature, and its content is consciously accessed. Additionally, the storage of information is long term and remains for an indefinite period of time, from days to decades. However, the total capacity of episodic memory to store information is still unknown.
Many studies of episodic memory have investigated interactions with cognitive resources, emotional regulation, environmental adaptation, attention, language, and executive function (Bahar-Fuchs et al., 2019). Episodic memory is related to autobiographical memory; both share a record of events based on place or time, thereby influencing the notion of self (Tulving, 2002). Affect also participates in the modulation of an event that is to be consolidated in episodic memory. Emotionally charged events are easier to record than others. The emotional state also influences the evocation of memories. The current affective state provides contextual mnemonic cues to evoke recorded information that is compatible with the experienced moment (da Costa Pinto, 2003; Pergher et al., 2006).
Higher life expectancies produce demands with regard to care that a given society provides for its elderly population (Assed et al., 2016). Studies of impacts on the physical and mental health of this population are increasing, especially with regard to deficits in episodic memory and their consequences on the lives of the elderly. These deficits result from impairments in the evocation of and access to mnemonic records, in addition to the lesser use of coding and storage strategies for new information, which may reflect natural senescence or cognitive decline (Aramaki and Yassuda, 2011). These mnemonic difficulties impact the lives of the elderly and can compromise daily function, such as remembering or associating information, managing finances, handling and controlling medications, orientating in time and space, and having autonomy in traveling outside the home to go shopping or enjoying leisure activities (Fandakova et al., 2012; Giovagnoli et al., 2017).
Among intervention strategies that have been developed to address episodic memory deficits, whether caused by senescence or psychopathological conditions, cognitive training has been the most used for the elderly (Bahar-Fuchs et al., 2013). Episodic memory training consists of exercises to reduce cognitive deficits and improve certain skills, thus providing healthier aging and maintaining an individual's daily function (Banducci et al., 2017). This type of non-pharmacological intervention employs systematic activities that focus on specific mental functions that seek to strengthen certain areas of cognition and meet specific objectives (Aramaki and Yassuda, 2011). Cognitive training can be structured individually or in groups. It usually occurs over a period of time. Its effects reflect behavioral and cognitive changes, measured by neuropsychological tests, the neurobiological base of which is anchored in cortical plasticity (Apóstolo et al., 2011; Nousia et al., 2018).
Controlled studies have reported favorable effects of cognitive training on a wide range of cognitive functions, such as attention, memory, processing speed, language, planning skills, and different problem-solving strategies, with positive effects in healthy elderly individuals (Chambon et al., 2014). Improvements were also found in such aspects as mood and well-being in patients with mild cognitive impairment (MCI) and Alzheimer's disease (AD; Kurz et al., 2008). However, Chambon et al. (2014) reported that memory performance can be stimulated not only by establishing mnemonic strategies to sustain the processes of learning, autonomy, and well-being but also by reducing negative beliefs about memory in aging.
The mapping of non-pharmacological methods of intervention is necessary to reduce the impact of dementia, ameliorate the negative impacts of senescence on memory, and manage practical issues about daily function and daily demands that burden caregivers. A meta-analysis by Floyd and Scogin (1997) was one of the first studies in this domain that sought to map the effectiveness of memory training in subjective memory function and mental health in the elderly. The authors stated that the uplift of subjective memory function was made even better by including pretraining that involved skills like the use of images and interventions to improve the attitudes of the participants. In the Brazilian context, a systematic review by Santos and Flores-Mendoza (2017) provided an overview of the Brazilian literature on cognitive training for the elderly, highlighting the trend in group interventions, instead of individual ones, that seek to stimulate episodic memory.
Another systematic review by Mendes et al. (2019) considered studies of cognitive stimulation in groups of elderly individuals. The studies they found tended to corroborate the idea that cognitive stimulation among groups is a good strategy for health professionals who attempt to preserve cognitive skills and prevent their decline in the elderly. Their work not only reported an efficacy of this type of intervention in cognitive training, but also extended its benefits to the mood and socialization of individuals, contributing to a greater quality of life in general.
A further recent systematic review on the topic by Bahar-Fuchs et al. (2019) expanded the mapping of the effects of cognitive training by investigating various cognitive domains in elderly individuals with mild to moderate dementia. Their main results indicated that cognitive training has small to moderate positive effects on global cognition, and these gains can be maintained for 3–12 months after intervention when compared with a control group. Despite existing reviews, several empirical questions about training episodic memory in the elderly remain unanswered.
Objective
The present study systematically reviewed studies on the application of cognitive training for episodic memory in healthy elderly individuals and elderly individuals with clinical conditions, including MCI and AD. We investigated (1) sample characteristics (i.e., sex and age), (2) the existence of a control group and its profile (i.e., active or passive), (3) types of episodic memory training that were used (i.e., duration and stimuli), (4) the protocols that were used and their outcome variables, (5) methodological quality and risk of bias in the studies, (6) effectiveness of the intervention, and (7) effects of the intervention at follow-up.
Method
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) guidelines (Moher et al., 2009). The PRISMA method is based on a protocol that was developed in a meeting with 29 participants, including clinicians, researchers, and editors, that established criteria for conducting systematic reviews and meta-analyses.
According to Moher et al. (2009), the construction of the review should consist of the following steps: (1) group articles that are found in the databases, removing possible duplicates, (2) exclude articles after an initial evaluation of the titles, (3) review the abstracts of the remaining studies according to previously established criteria, (4) analyze the remaining studies in full to verify that they meet the eligibility criteria, and (5) extract and systematize the variables of interest in the included studies.
Study selection
The studies that were identified in the literature search were chosen according to the following inclusion criteria: (1) articles in English or Portuguese, (2) intervention based on episodic memory training, (3) subjects >60 years of age, (4) healthy elderly individuals or elderly individuals with some clinical condition, (5) cohort studies, and (6) outcome variables that were measured using instruments that objectively assess episodic memory. The exclusion criteria were the following: (1) case studies, (2) animal studies, (3) theoretical works, and (4) studies that did not objectively measure episodic memory.
Search strategy
Four databases were searched: PubMed; PsycNET, Web of Science, and SciELO. The searches were performed on December 11, 2019, using the following keywords: “Episodic Memory” AND “Training” AND “Elderly” OR “Aging” OR “Dementia.” We also searched the Portuguese words for these search terms, which were exclusively used in the SciELO database. The screening steps for resulting articles were performed and discussed by two authors of this study.
Results
Using the PRISMA method (Moher et al., 2009), the search yielded 572 articles in PubMed (135), Web of Science (254), PsycNET (173), and SciELO (10). Of these 572 articles, 340 were eligible after eliminating duplicate articles and performing the screening steps based on the title, abstract, and full text of the articles. According to the inclusion and exclusion criteria, 23 articles were subjected to data collection and analysis. Figure 1 summarizes the study selection process.
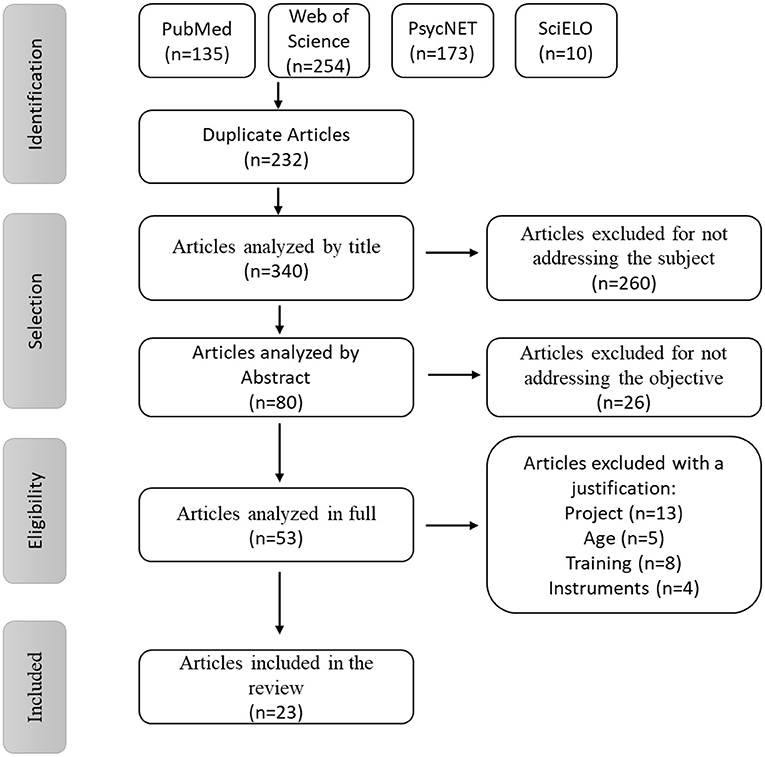
Figure 1. PRISMA flowchart adapted from Moher et al. (2009).
Characteristics of the studies
Subjects and clinical conditions
Table 1 depicts the characteristics of the studies that were included in the present review. The number of participants who were recruited varied in the 23 studies that employed various models of cognitive intervention. The smallest group consisted of 16 participants (Aramaki and Yassuda, 2011), and the largest consisted of 2,802 participants (Willis et al., 2006), with an average of 392.57 participants per study (standard deviation = 787.628, standard error = 164.238, median = 57). The subjects were 60–89 years of age and their education ranged from 0–2 years (da Silva and Yassuda, 2009) to 16 years (Banducci et al., 2017; Savulich et al., 2017). In a large proportion of the studies, women represented the majority of the participants. With regard to the cognitive conditions of the different groups, 13 studies (56.52%) evaluated healthy elderly individuals (Ball et al., 2002; Willis et al., 2006; Carvalho et al., 2009; da Silva and Yassuda, 2009; Langbaum et al., 2009; Lima-Silva et al., 2010; Aramaki and Yassuda, 2011; Gross and Rebok, 2011; Legault et al., 2011; Fandakova et al., 2012; Chambon et al., 2014; Zimmermann et al., 2016; Banducci et al., 2017), six studies (26.09%) investigated elderly individuals with clinical conditions (either MCI or AD; Kurz et al., 2008; Jean et al., 2014; Neely et al., 2014; Giovagnoli et al., 2017; Savulich et al., 2017; Nousia et al., 2018), and four studies (17.39%) analyzed groups with both conditions (Belleville et al., 2006; González-Palau et al., 2014; Kinsella et al., 2016; McDougall et al., 2018).

Table 1. Characteristics of the studies that were included in the systematic review.
The participants were recruited from geriatric outpatient clinics or psychiatric institutions (Belleville et al., 2006; Kurz et al., 2008; Jean et al., 2014; Neely et al., 2014; Savulich et al., 2017; Nousia et al., 2018), community centers (Ball et al., 2002; Willis et al., 2006; Carvalho et al., 2009; Legault et al., 2011; Fandakova et al., 2012; González-Palau et al., 2014; Kinsella et al., 2016; Banducci et al., 2017; Giovagnoli et al., 2017; McDougall et al., 2018), schools and colleges for the elderly (da Silva and Yassuda, 2009; Lima-Silva et al., 2010; Aramaki and Yassuda, 2011; González-Palau et al., 2014), or home visits (Langbaum et al., 2009; Chambon et al., 2014). The elderly participants volunteered to undergo different forms of interventions. The majority of them underwent a screening stage that used brief screening batteries to assess the inclusion and exclusion criteria and control for confounding variables.
Comparison groups
Most of the studies (95.65%) included a control group. However, in a comparative study of two interventions, with an interval of 18 months between interventions (Aramaki and Yassuda, 2011), this was not possible because the control group that participated in the first intervention was stimulated during the interval between interventions, which prevented the reuse of the control group in the second intervention.
In 16 studies (69.57%), half (34.78%) used only an active control group, and the other half used only a passive control group. The remaining six studies (26.09%) included a control group with both conditions (active and passive).
Type of cognitive training
The structure of the stimulation programs and cognitive processes that were involved were similar, which focused mainly on attentional capacities, processing speed, and memory. The strategies for the stimulation of these skills, mostly episodic memory, involved physical exercises, the use of computers, and psychopedagogical sessions that sought to clarify doubts or negative beliefs about memory decline that is common in old age (Aramaki and Yassuda, 2011; Jean et al., 2014). The articles that were reviewed herein were categorized according to the type of training.
Neely et al. (2014) developed a collaborative stimulation program, in which the spouse or caregiver assisted the partner with dementia in tasks that require better episodic memory performance and daily occupational tasks to support activities of categorization and memorization. Legault et al. (2011) used a method that involved the integration of cognitive training with physical exercise. González-Palau et al. (2014) implemented the same method but included computers as a tool for cognitive training.
In addition to these three studies (13.04%), another four studies (17.39%) used computers as a tool for cognitive training, with applications that stimulated attentional processes, mainly episodic memory (Chambon et al., 2014; González-Palau et al., 2014; Savulich et al., 2017; Nousia et al., 2018). Three studies (13.04%) used cognitive training based on the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) program. In this model, the elderly participants underwent training that focused on strategies to achieve better memory, reasoning, and processing speed (Ball et al., 2002; Langbaum et al., 2009; Gross and Rebok, 2011).
The remaining 13 studies (56.52%) used conventional models to stimulate various cognitive processes, such as memory stimulation and name-face association (Jean et al., 2014) and associative recognition and the memorization and location of objects at specific points (Fandakova et al., 2012; Zimmermann et al., 2016). In addition to memory strategies, some studies focused on motor skills and relaxation exercises (Kurz et al., 2008; McDougall et al., 2018) and included psychoeducational sessions to reduce negative beliefs about memory in old age (Lima-Silva et al., 2010; Aramaki and Yassuda, 2011). Memory training also included other stimuli, such as theater scripts, and focused on attention, information processing, the memorization of words, phrases, and texts, and the categorization of previously learned information (Willis et al., 2006; Carvalho et al., 2009; da Silva and Yassuda, 2009; Kinsella et al., 2016; Banducci et al., 2017; Giovagnoli et al., 2017).
Intervention length
In addition to different training protocols, the durations of the interventions were also heterogeneous. The interventions included a maximum of 36 sessions and minimum of five sessions (mean = 11.05 sessions, standard deviation = 7.28 sessions, mode = 10 sessions.
Fandakova et al. (2012) was the only study that did not stipulate a specific number or duration of the sessions. The study by Legault et al. (2011) was not included in the overall session count because it involved three different groups, and each group underwent a different number of sessions.
In 18 studies (78.26%), the intervention was applied in a group setting. In five studies (21.74%), the intervention was applied individually. Among the studies that reported the intervention duration, the minimum was 1 month (Kurz et al., 2008; Gross and Rebok, 2011). The training period in Giovagnoli et al. (2017) and Nousia et al. (2018) was 3 months, whereas Willis et al. (2006) and Jean et al. (2014) had the longest durations, ranging from 12 to 35 months. The length of each session also varied. Kurz et al. (2008) reported 6 h (360 min) per week. The minimum session length was 40 min (González-Palau et al., 2014). Seven studies (31.82%) had a session length of 60 min. Two studies (9.09%) had a session length of 120 min. Four studies (18.18%) had a session length of 40 min. Two studies (9.09%) had session lengths of 90 and 75 min, respectively, and four studies (18.18%) had a session length of 45 min. The study by Ball et al. (2002) was not included in this analysis because its session durations ranged from 60 to 75 mi.
Of the 23 studies, nine (39.13%) included a follow up after the post-evaluation stage. Jean et al. (2014) had a follow-up period of 1–4 weeks. Zimmermann et al. (2016) had a follow-up period of 4 months. Chambon et al. (2014) and Kinsella et al. (2016) had a follow-up period of 6 months. Willis et al. (2006) had a follow-up period of 1 year. Ball et al. (2002) and McDougall et al. (2018) had a follow-up period of 2 years. Langbaum et al. (2009) and Gross and Rebok (2011) had follow-up periods of 1, 2, 3, and 5 years after the intervervention.
Instruments to measure episodic memory
A total of 33 different instruments were used, including various tests, tasks, and questionnaires, to measure episodic memory and the participants' performance in pre- and post-intervention stages. Three instruments (9.09%; Rey Auditory-Verbal Learning Test [RAVLT], Rivermead Behavioral Memory Test–Paragraph Recall, and Hopkins Verbal Learning Test [HVLT], which is analogous to the RAVLT) were used in five studies (21.74%). Rey's Complex Figure, representing (3.03%) of the instruments that were used, was applied in three studies (13.04%). The Brief Cognitive Screening Battery (BCSB), Picture Memory, Mini Mental State Examination (MMSE), Verbal Hopkins Learning Task, name-face association task, recall memory, word list, and California Verbal Learning Test, 2nd edition (CVLT-II), represented 18.18% of the instruments that were used and were further described by two studies (8.70%). The remaining 23 instruments (69.70%) were applied at least once in the remaining 13 studies (56.52%). Notably, this analysis did not consider the use of a given instrument more than once in the same study but rather its frequency of use relative to the total number of studies.
Effectiveness
The analysis of effectiveness of the interventions was based on comparative performance in the experimental and control groups, which was grounded in training episodic memory and evaluations in the post-training phase. All 23 studies reported efficacy according to their own cognitive training program, but the studies compared the experimental and control groups in different ways. Thirteen studies (56.52%) performed a standard comparison [i.e., they compared post-training results between an experimental group and a control group; Belleville et al. (2006); Carvalho et al. (2009); da Silva and Yassuda (2009); Langbaum et al. (2009); Lima-Silva et al. (2010); González-Palau et al. (2014); Jean et al. (2014); Kinsella et al. (2016); Zimmermann et al. (2016); Banducci et al. (2017); Savulich et al. (2017); McDougall et al. (2018); Nousia et al. (2018)]. Five studies (21.74%) performed comparisons between experimental and control groups and further divided the control groups into passive and active conditions. The active subgroup was further divided into two additional groups according to the cognitive function that was trained (Ball et al., 2002; Gross and Rebok, 2011; Legault et al., 2011; Fandakova et al., 2012; Giovagnoli et al., 2017). Four studies (17.39%) compared the results using a control group, subdividing in active and passive control conditions (Willis et al., 2006; Kurz et al., 2008; Chambon et al., 2014; Neely et al., 2014). Only one study (4.35%) evaluated the experimental group without any control group (Aramaki and Yassuda, 2011).
Quality of the studies
The quality of the studies was analyzed using the Newcastle-Ottawa Scale (Wells et al., 2013). This scale uses three parameters (selection, comparability, and outcome), which are subdivided into specific questions that assign points to the quality of the study. The score ranges from zero (lowest quality) to 9 (highest quality). The analysis was performed independently by two researchers, and the final scores were established by consensus. Studies with a final score ≤ 5 were considered low quality. Studies with a final score >5 were considered high quality.
Only three papers (13.04%) had a final score ≤ 5. Of the 23 papers, four (17.39%) received a maximum score of 9, whereas six studies (26.09%) received a score of 8, obtaining high quality scores in the three parameters. Among the 23 studies, the outcome parameter was the one with the lowest overall score, with 11 papers (47.82%) receiving only 1 point out of a total possible three points. Table 2 presents this information in detail.
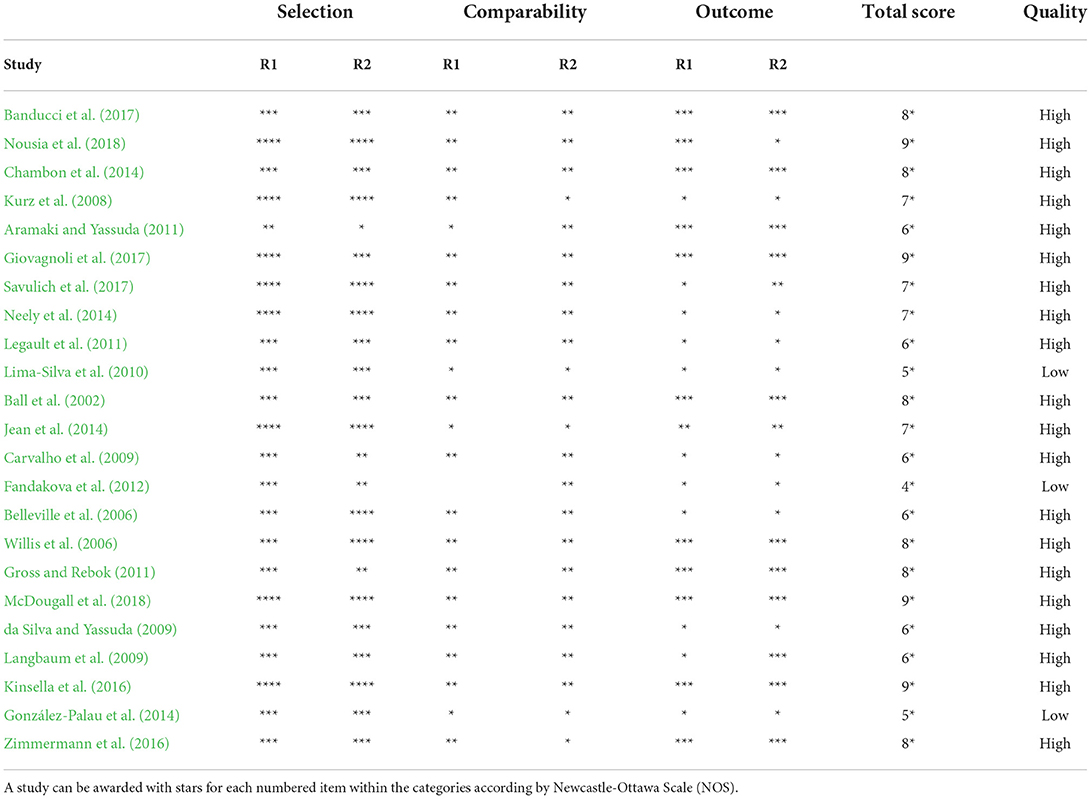
Table 2. Outline of quality assessment: appraisal of items of the Newcastle-Ottawa Scale by researcher 1 (R1) and researcher 2 (R2).
Figure 2 shows the quality of the studies, organized by criteria and the percentage of studies that were scored in each of the criteria. For the item “Representativeness of the sample and assessment of the outcome,” all 23 studies gained points. Only 10 studies (43.48%) received points for the item “Outcome not present at the start of the study,” in which 13 studies (56.52%) had only healthy elderly individuals as the experimental group (i.e., they did not have initial cognitive difficulties, which could have influenced the beneficial effects of cognitive training). Only 11 studies (47.82%) scored on the items about cohort follow-up. The 12 studies (52.47%) that did not score in this regard either did not present a longitudinal study or they collected data within a period of <3 months after training, which was considered by the researchers as too short. For the item “Comparability,” the score was based on the age of the subjects in the experimental and control groups, in addition to another factor, such as education and the presence or absence of a clinical diagnosis and its type.
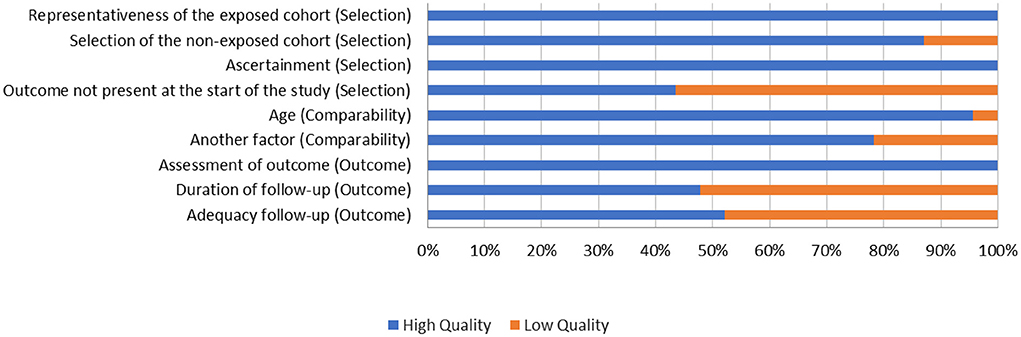
Figure 2. Methodological quality. Assessment of the included studies in each item of the Newcastle-Ottawa Scale, presented as a percentage.
Discussion
Despite being a widely studied topic, several empirical questions about interventions to improve memory during the aging process remain unanswered. The present systematic review sought to elucidate different designs of episodic memory training and their effectiveness in healthy elderly individuals with neurocognitive disorders. We identified 23 studies that met the inclusion criteria. The main variables that comprised the intervention protocols (i.e., characteristics of the sample, type of control group, mode of episodic memory training, and duration of training) were investigated, as well as the outcome variables, efficacy, and risk of bias.
The main results indicated effectiveness with regard to different forms of the cognitive training of episodic memory. These results are consistent with the literature on cognitive mechanisms that underlie this type of training. Episodic memory exercises can influence memory function at various levels, especially in the information coding and consolidation phases. Exercises that are performed before coding new information and during the period of memory consolidation (as opposed to exercises that are performed during memory coding) can improve the evocation of stored information (Loprinzi et al., 2017).
Another characteristic that was observed in the different studies is the effectiveness of training in healthy individuals and in subjects with dementia in the initial phase (Belleville et al., 2006; Chambon et al., 2014; Neely et al., 2014; Kinsella et al., 2016). According to Bahar-Fuchs et al. (2019), cognitive training can lead to overall improvements in cognitive functions in healthy individuals and, to a lesser extent, in subjects with some form of cognitive impairment. In the latter case, training specific functions, such as memory, more be more viable and beneficial.
The characteristics of the instruments that were used to evaluate memory in these studies are particularly important for detecting cognitive decline and assessing effectiveness of the intervention. Most of the studies used instruments based on word list tasks (e.g., RAVLT, HVLT-R, and CVLT), which comprise verbal exposure, retention, and the subsequent evocation of words by the examinee. Despite the fact that the use of this paradigm to assess episodic memory is canonical, notable is the lack of more ecological and contextual assessments that explore functionality of the patient in everyday situations.
The ecological assessment of episodic memory in elderly individuals may be useful for identifying subtle amnesic deficits that generally escape formal assessment, thus allowing investigations of the impact of the context where they occur. Studies suggest only low correlations between these tests and subjective complaints of memory function in daily life (Chaytor and Schmitter-Edgecombe, 2003; Reid and MacLullich, 2006). More ecological interventions and outcome variables may produce longer-lasting effects because of the influence on behaviors that can compromise functionality of the elderly and are frequent subjective complaints. da Silva and Yassuda (2009), Jean et al. (2014), and Neely et al. (2014) were among the few studies that employed ecological measures.
The ecological training of episodic memory favors the stimulation of information storage, the creation of an effect of spatial temporal contiguity, and the consolidation of lived experiences because this kind of training fosters mental storage and evokes a complex scene or event. According to Raffard et al. (2010), episodic and autobiographical memory deficiencies could be attributable to a specific deficit in construction of the scene, in which the impairment is not restricted only to the retrieval and integration of relevant spatial and temporal components but also to the manipulation of mental images that are evoked from personal life situations.
Notable differences were observed between the various forms of cognitive training and the experimental methods that were used. Consistent with the observations of Bahar-Fuchs et al. (2019), although the inclusion and exclusion criteria were useful, the remaining studies varied with regard to the form of stimulus between the experimental and control groups, the total investigated population, and clinical condition of the subjects, which likely influenced the findings.
Methodological quality
Although we classified most of the studies as having a high risk of bias in at least two domains, our approach to classifying studies as high and low quality with regard to the risk of bias for the purpose of analyzing subgroups and classifying evidence has been relatively with low scores.
The low methodological quality of some of the studies for some of the criteria limits our ability to assess the base of evidence in the literature in this field. The quality of most of the studies of cognitive training interventions that were included in this review may have several risks of bias, particularly because of insufficient details with regard to heterogeneity of the instruments that were used to measure effectiveness, the variability of the interventions, and the lack of follow-up.
Although we classified all of the experimental interventions that were employed in the studies, they were clinically heterogeneous. Some of the interventions targeted only one cognitive domain, but some evaluated other domains simultaneously. We observed the diverse use of paper and pencil forms, training using computerized platforms, and ecological activities. Some interventions focused mainly on simple exercises, whereas others used a series of learning and performance strategies. The configurations (e.g., frequency and duration of the sessions) of the interventions were also diverse, and some were delivered at home, whereas others were delivered in the clinical settings.
In the reviewed studies, the results were evaluated according to different measures. In many cases, however, insufficient details were provided to determine which exact measure was used. When the studies reported individual subtest scores from test batteries or global indices, we considered each subtest as a measure of episodic memory. In some cases, the studies used unpublished tests that were developed specifically for the purposes of the particular study. This heterogeneity in the field reveals the plurality of approaches and measures, but it compromises the synthesis and integration of information.
Research limitations
According to the analysis of the studies (Table 1), the heterogeneity of the characteristics of the studies hampers generalization of the results, such as (1) gender differences between studies (although all of the studies included both sexes, the female gender prevailed), (2) studies without a control group in their design (Aramaki and Yassuda, 2011), (3) variability of the training duration, especially the number of sessions and stimulation time in each session, varying in 10 different categories based on duration, and the time varying in seven different categories, (4) modality of the forms of intervention, and (5) variety of the instruments used, which varied among four different categories according to the number of times the instrument was used among the different studies. The analysis of the effectiveness of cognitive training can be influenced by any of these factors.
Although the studies met the inclusion and exclusion criteria, two of these criteria limited the analysis of some of the research variables. Although cohort studies offer a broader picture of comparisons between groups, the inclusion of clinical cases would provide an in-depth view of a specific pathology and indicate how cognitive training can help patient in these cases. Additionally, although the focus of the analysis was on episodic memory, other cognitive processes, such as attention and executive function, are involved in the consolidation and evocation of information. Therefore, one suggestion would be to observe how episodic memory training can favor this type of memory.
Practical and theoretical implications
The present results rise the importance of cognitive training and socialization among the elderly, which can mitigate the manifestation of dementia and consequently the negative impact on daily life at the social, psychological, and economic levels (Kurz et al., 2008; Aramaki and Yassuda, 2011; Neely et al., 2014).
From a theoretical perspective, the present results are consistent with the literature. Cognitive training is based on the process of brain plasticity, stimulating changes in neural networks and favoring the cognitive functions that are stimulated. When considering the different intervention methods, one must consider the specific type of training with current cognitive status of the subject. For example, new learning skills and delayed recall should be trained in elderly individuals with early-stage AD or vascular dementia (Bahar-Fuchs et al., 2019).
Conclusion
Several systematic reviews with and without meta-analyses have evaluated the effectiveness of cognitive training for the elderly. However, few studies have mapped the literature with regard to the cognitive training of episodic memory. The present findings indicate that our general and specific objectives were achieved. The results demonstrate the benefits of cognitive training and importance of performing further studies of new forms of care for the elderly.
Future studies should investigate the impact of clinical aspects at different levels: such as psychological, functional and physiological on episodic memory training. It is important to emphasize that memory is not an isolated process, as it is mutually influenced by other cognitive processes such as attention and executive functions, which also need to be investigated together in a global analysis. In addition, new review studies may expand the findings of the present study comparing the kind of syndromes and populations of different ages, cause deficits in episodic memory are not restricted to the elderly.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
CN and JL-F: conceived, supervised the review, and wrote the manuscript. AM, LL, and CN: carried out the review and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil (Finance Code 001), Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ), and a scholarship from Concelho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Apóstolo, J. L. A., Cardoso, D. F. B., Marta, L. M. G., and de Oliveira Amaral, T. I. (2011). Efeito da estimulação cognitiva em idosos. Revista de Enfermagem Referência III, 193–201. doi: 10.12707/RIII11104
Aramaki, F. O., and Yassuda, M. S. (2011). Cognitive training based on metamemory and mental images: follow-up evaluation and booster training effects. Dement. Neuropsychol. 5, 48–53. doi: 10.1590/s1980-57642011dn05010009
Assed, M. M., de Carvalho, M. K. H. V., de Almeida Rocca, C. C., and de Padua Serafim, A. (2016). Memory training and benefits for quality of life in the elderly. Dement. Neuropsychol. 10, 152–155. doi: 10.1590/S1980-5764-2016DN1002012
Bahar-Fuchs, A., Clare, L., and Woods, B. (2013). Cognitive training and cognitive rehabilitation for persons with mild to moderate dementia of the Alzheimer's of vascular type: a review. Alzheimer's Res. Ther. 5, 35. doi: 10.1186/alzrt189
Bahar-Fuchs, A., Martyr, A., Goh, A. M., Sabates, J., and Clare, L. (2019). Cognitive rehabilitation for people with mild to moderate dementia. Cochrane Database Syst. Rev. 8, CD013388. doi: 10.1002/14651858.CD013388
Ball, K., Berch, D. B., Helmers, K. F., Jobe, J. B., Leveck, M. D., Marsiske, M., et al. (2002). Effects of cognitive training interventions with older adults: a randomized controlled trial. J. Am. Med. Assoc. 288, 2271–2281. doi: 10.1001/jama.288.18.2271
Banducci, S. E., Daugherty, A. M., Biggan, J. R., Cooke, G. E., Voss, M., Noice, T., et al. (2017). Active experiencing training improves episodic memory recall in older adults. Front. Aging Neurosci. 9, 133. doi: 10.3389/fnagi.2017.00133
Belleville, S., Gilbert, B., Fontaine, F., Gagnon, L., Ménard, É., and Gauthier, S. (2006). Improvement of episodic memory in persons with mild cognitive impairment and healthy older adults: evidence from a cognitive intervention program. Dement. Geriatr. Cogn. Disord. 22, 486–499. doi: 10.1159/000096316
Carvalho, F. C. R., Neri, A. L., and Yassuda, M. S. (2009). Episodic memory training with emphasis on categorization for older adults without dementia and depression [Treino de memória episódica com ênfase em categorização para idosos sem demência e depressão]. Psicologia: Reflexao e Critica 23, 317–323. doi: 10.1590/S0102-79722010000200014
Chambon, C., Herrera, C., Romaiguere, P., Paban, V., and Alescio-Lautier, B. (2014). Benefits of computer-based memory and attention training in healthy older adults. Psychol. Aging 29, 731–743. doi: 10.1037/a0037477
Chaytor, N., and Schmitter-Edgecombe, M. (2003). The ecological validity of neuropsychological tests: a review of the literature on everyday cognitive skills. Neuropsychol. Rev. 13, 181–197. doi: 10.1023/b:nerv.0000009483.91468.fb
da Costa Pinto, A.. (2003). O impacto das emoções na memória: alguns temas em análise. Psicologia, Educação e Cultura 2, 215–240. Available online at: https://doi.org/hdl.handle.net/10216/18462">https://hdl.handle.net/10216/18462
da Silva, H. S., and Yassuda, M. S. (2009). Memory training for older adults with low education: mental images versus categorization. Educ. Gerontol. 35, 890–905. doi: 10.1080/03601270902782487
Fandakova, Y., Shing, Y. L., and Lindenberger, U. (2012). Heterogeneity in memory training improvement among older adults: a latent class analysis. Memory 20, 554–567. doi: 10.1080/09658211.2012.687051
Floyd, M., and Scogin, F. (1997). Effects of memory training on the subjective memory functioning and mental health of older adults: a meta-analysis. Psychol. Aging 12, 150–161. doi: 10.1037//0882-7974.12.1.150
Giovagnoli, A. R., Manfredi, V., Parente, A., Schifano, L., Oliveri, S., and Avanzini, G. (2017). Cognitive training in Alzheimer's disease: a controlled randomized study. Neurol. Sci. 38, 1485–1493. doi: 10.1007/s10072-017-3003-9
González-Palau, F., Franco, M., Bamidis, P., Losada, R., Parra, E., Papageorgiou, S. G., et al. (2014). The effects of a computer-based cognitive and physical training program in a healthy and mildly cognitive impaired aging sample. Aging Mental Health 18, 838–846. doi: 10.1080/13607863.2014.899972
Gross, A. L., and Rebok, G. W. (2011). Memory training and strategy use in older adults: results from the ACTIVE study. Psychol. Aging 26, 503–517. doi: 10.1037/a0022687
Jean, L., Simard, M., Wiederkehr, S., Bergeron, M. È., Turgeon, Y., Hudon, C., et al. (2014). Efficacy of a cognitive training programme for mild cognitive impairment: results of a randomised controlled study. Neuropsychol. Rehabil. 20, 377–405. doi: 10.1080/09602010903343012
Kinsella, G. J., Ames, D., Storey, E., Ong, B., Pike, K. E., Saling, M. M., et al. (2016). Strategies for improving memory: a randomized trial of memory groups for older people, including those with mild cognitive impairment. J. Alzheimer's Dis. 49, 31–43. doi: 10.3233/JAD-150378
Kurz, A., Pohl, C., Ramsenthaler, M., and Sorg, C. (2008). Cognitive rehabilitation in patients with mild cognitive impairment. Clin. Interv. Aging 3, 163–168. doi: 10.1002/gps.2086
Langbaum, J. B. S., Rebok, G. W., Bandeen-Roche, K., and Carlson, M. C. (2009). Predicting memory training response patterns: results from ACTIVE. J. Gerontol.: Ser. B. Psychol. Sci. Soc. Sci. 64, 14–23. doi: 10.1093/geronb/gbn026
Legault, C., Jennings, J. M., Katula, J. A., Dagenbach, D., Gaussoin, S. A., Sink, K. M., et al. (2011). Designing clinical trials for assessing the effects of cognitive training and physical activity interventions on cognitive outcomes: the Seniors Health and Activity Research Program Pilot (SHARP-P) study, a randomized controlled trial. BMC Geriatr. 11, 27. doi: 10.1186/1471-2318-11-27
Lima-Silva, T. B., Ordonez, T. N., dos Santos, G. D., Fabrício, A. T., Aramaki, F. O., de Almeida, E. B., et al. (2010). Effects of cognitive training based on metamemory and mental images. Dement. Neuropsychol. 4, 114–119. doi: 10.1590/s1980-57642010dn40200007
Loprinzi, P. D., Edwards, M. K., and Frith, E. (2017). Potential avenues for exercise to activate episodic memory-related pathways: a narrative review. Int. J. Lab. Hematol. 38, 42–49. doi: 10.1111/ejn.13644
McDougall, G. J., McDonough, I. M., and LaRocca, M. (2018). Memory training for adults with probable mild cognitive impairment: a pilot study. Aging Mental Health 23, 1433–1441. doi: 10.1080/13607863.2018.1484884
Mendes, A., Bennemann, R., and Milani, R. (2019). Treino cognitivo para grupos de idosos: uma revisão sistemàtica. Sociedade Portuguesa de Psicologia Da Saúde 20, 503–511. doi: 10.15309/19psd200218
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097. doi: 10.1371/journal.pmed.1000097
Neely, A. S., Vikstrom, S., and Josephsson, S. (2014). Collaborative memory intervention in dementia: caregiver participation matters. Neuropsychol. Rehabil. 19, 696–715. doi: 10.1080/09602010902719105
Nousia, A., Siokas, V., Aretouli, E., Messinis, L., Aloizou, A. M., Martzoukou, M., et al. (2018). Beneficial effect of multidomain cognitive training on the neuropsychological performance of patients with early-stage Alzheimer's disease. Neural Plast. 2018, 2845176. doi: 10.1155/2018/2845176
Pergher, G. K., Grassi-Oliveira, R., Ávila, L. M., and De Stein, L. M. (2006). Memria, humor e emoção. Revista de Psiquiatria, 28, 61–68. doi: 10.1590/S0101-81082006000100008
Raffard, S., D'Argembeau, A., Bayard, S., Boulenger, J. P., and Van der Linden, M. (2010). Scene construction in schizophrenia. Neuropsychology 24, 608–615. doi: 10.1037/a0019113
Reid, L. M., and MacLullich, A. M. J. (2006). Subjective memory complaints and cognitive impairment in older people. Dement. Geriatr. Cogn. Disord. 22, 471–485. doi: 10.1159/000096295
Santos, M. T., and Flores-Mendoza, C. (2017). Treino cognitivo para idosos: uma revisão sistemática dos estudos nacionais. Psico-USF 22, 337–349. doi: 10.1590/1413-82712017220212
Savulich, G., Piercy, T., Fox, C., Suckling, J., Rowe, J. B., O'Brien, J. T., et al. (2017). Cognitive training using a novel memory game on an iPad in patients with amnestic mild cognitive impairment (aMCI). Int. J. Neuropsychopharmacol. 20, 624–633. doi: 10.1093/ijnp/pyx040
Tulving, E.. (2002). Episodic memory: from mind to brain. Annu. Rev. Psychol. 53, 1–25. doi: 10.1146/annurev.psych.53.100901.135114
Wells, G., Shea, B., O'Connell, D., Peterson, J., Welch, V., Losos, M., et al (2013). The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa, ON: Ottawa Hospital Research Institute. Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed January 10, 2020).
Willis, S. L., Tennstedt, S. L., Marsiske, M., Ball, K., Elias, J., Koepke, K. M., et al. (2006). Long-term effects of cognitive training on everyday functional outcomes in older adults. J. Am. Med. Assoc. 296, 2805–2814. doi: 10.1001/jama.296.23.2805
Keywords: episodic memory, elderly, cognitive training, neuropsychology, systematic review
Citation: Mendonça AR, Loureiro LM, Nórte CE and Landeira-Fernandez J (2022) Episodic memory training in elderly: A systematic review. Front. Psychol. 13:947519. doi: 10.3389/fpsyg.2022.947519
Received: 18 May 2022; Accepted: 06 July 2022;
Published: 28 July 2022.
Edited by:
Naomi Sweller, Macquarie University, AustraliaReviewed by:
Fahad Naveed Ahmad, Wilfrid Laurier University, CanadaYulia Solovieva, Meritorious Autonomous University of Puebla, Mexico
Copyright © 2022 Mendonça, Loureiro, Nórte and Landeira-Fernandez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Eduardo Nórte, Y2FkdWxzbkBnbWFpbC5jb20=