 Ferozkhan Jadhakhan
Ferozkhan Jadhakhan Nichola Lambert1
Nichola Lambert1 Nicola Middlebrook
Nicola Middlebrook David W. Evans
David W. Evans Deborah Falla
Deborah Falla
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 12 August 2022
Sec. Health Psychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.943479
Background: Exercise has been used to manage symptoms of post-traumatic stress disorder (PTSD). The effect of exercise on PTSD outcomes has been previously explored in several studies. However, it still remains unclear what type of exercise/physical activity, intensity and duration is most effective for reducing symptoms of PTSD. A systematic review was conducted to determine which forms of exercise or physical activity have the greatest effect on PTSD outcome scores including an evaluation of exercise frequency and volume.
Methods: The following electronic databases were systematically searched from January 1980 to June 2021: MEDLINE, PsycINFO, PubMed and Web of Science. Inclusion criteria were studies investigating adults aged 18 or over, reporting the effect of exercise and physical activities on PTSD symptom outcome scores. Two reviewers independently extracted information on study characteristics, exposure and outcomes. In total of 3,217 articles were screened and 23 full text articles further assessed, with 13 RCT's included in the review, covering seven exercise/physical activity interventions. The study protocol was registered prospectively with PROSPERO (CRD42021255131).
Results: Thirteen studies from four countries involving a total of 531 patients were selected for inclusion. Individual forms of exercise/physical activity examined showed some effect on reducing PTSD symptoms but combined exercises (resistance training, aerobic, strength and yoga) administered over a 12 week period, three times a week for 30–60 min showed greater effects on PTSD symptoms.
Conclusion: The limited evidence suggests that a combined exercise intervention has the best evidence for a having a beneficial effect on PTSD symptoms.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=255131.
Post-traumatic stress disorder (PTSD) is a mental health disorder that can affect people of any age, either immediately or years after direct or indirect exposure to a traumatic event (American Psychiatric Association., 2013). Such events can range from car accidents, combat situations, physical assaults or sudden bereavement (Williamson et al., 2019). It is estimated that 1 in 3 adults will experience a traumatic event at some point in their lives (McManus et al., 2016). The symptoms of PTSD may include intrusion (e.g., flashbacks), hyper-arousal (e.g., heightened alert and an enhanced startle reflex), avoidance of situations or places that remind them of the traumatic event, emotional detachment from their feelings or others, and negative thoughts about themselves (Bisson et al., 2015). An acute reaction to a traumatic event can resolve within a month, but for those left untreated this may last several years (Kessler et al., 1995; Smid et al., 2012). In some cases PTSD can manifest later in life (late onset), sometime years after the experience of a traumatic event (Chopra, 2018). While the average duration if treated is 36 months, approximately one third may still not fully resolve (Smid et al., 2012).
In a large sample of the general population of England, the 2014 Adult Psychiatric Morbidity Survey (APMS) (Baker, 2020) found that 3.7% of men and 5.1% of women aged 16 and over met criteria for PTSD. The Trauma Screening Questionnaire (TSQ) was used to examine the experience of PTSD with a total of ≥6 points out of a possible 10 indicating a positive screen for PTSD (Brewin et al., 2002). Prevalence rates for PTSD in different countries range from 1 to 12% and this range is thought to be due to a number of factors including study methodologies, diagnostic criteria used, likelihood of experiencing an event, and social factors (Klein and Alexander, 2009). Certain groups such as military personnel and those working in emergency services have a greater incidence of PTSD (Perkonigg et al., 2000; McFarlane et al., 2009; Fear et al., 2010; Greenberg et al., 2011).
Current National Institute for Health and Care Excellence (NICE) guidelines (NICE, 2018) recommend a range of treatments depending on the severity and time from trauma, which varies from ‘watch and wait', Cognitive Behavioral Therapy (CBT), Eye Movement Desensitization and Reprocessing (EMDR) and medication. Previous systematic reviews and meta-analyses found moderate effects of exercise on depression, anxiety and PTSD (Bartley et al., 2013; Jayakody et al., 2014; Mura et al., 2014; Stonerock et al., 2015; Kvam et al., 2016; Ravindran et al., 2016; Schuch et al., 2016; Stubbs et al., 2016, 2017; Asher et al., 2017; Krogh et al., 2017). These results were not sufficiently reliable to ensure stable long term benefit. A recent review confirmed these findings showing a small to medium effect (ES: 0.29, 95% CI: 0.10–0.49, P <0.01) of exercise on PTSD symptom severity whereas a sub-group analysis showed no significant effect of exercise on anxiety and depression severity (Bjorkman and Ekblom, 2021). A previous Cochrane review (Lawrence et al., 2010) attempted to investigate the benefits of exercise in the context of sport and games for PTSD but found only five studies, none of which met the review inclusion criteria, suggesting more research is required to assess the effectiveness of exercise in alleviating symptoms of PTSD. Previous reviews have examined the effect of exercise on PTSD in the general population and found that exercise reduces PTSD symptoms as a standalone intervention or adjunct to usual care; the comparability of the studies included in these reviews were limited by heterogeneity in terms of population characteristics, outcome measures, definitions of comparator group and sampling methods. For example, Rosenbaum et al. (2015a,b) conducted a systematic review to evaluate the effect of physical activity interventions on PTSD. Results from their meta-analysis of four randomized controlled trials (RCTs) with a total of 200 participants revealed that physical activity significantly reduced symptoms of PTSD, compared to control groups (Hedges' g = −0.35, 95% CI [−0.63 to −0.07], p = 0.02). The authors, however, rated the quality of the studies as satisfactory, following assessment of allocation concealment, assessor blinding and publication bias.
Another systematic review by Whitworth and Ciccolo (2016) investigated the effects of exercise specifically in veterans with PTSD. This review was based on nine observational, two qualitative and two experimental studies. They concluded that there was some evidence to suggest that exercise could reduce PTSD symptoms. However, the studies included showed heterogeneity in their outcome measures and not all studies were specifically testing the effects of exercise on PTSD. A more recent systematic review by McGranahan and O'Connor (2021) which included four RCTs, focused on exercise training effects on sleep quality and symptoms of anxiety and depression in people with PTSD. They analyzed PTSD scores, but only as a secondary outcome measure. The results suggested a small to moderate effect size (Hedges'd = 0.33, 95% CI [−0.66–0.00], p <0.05) toward improvement in PTSD symptoms. Despite the knowledge gained from this body of work, it still remains unclear what type of exercise and or physical activity (structured or unstructured), and what duration and intensity of exercise is most effective for reducing symptoms of PTSD (Friedman, 2019). Physical activity and/or exercise can be in the form of cycling, walking, household or occupational activity or a moderate intensity exercise such as horse-riding. Structured physical activity is generally planned with an underlying goal. Therefore, the purpose of the current systematic review is to examine the available evidence concerning the effect of various types of physical activity and/or exercise interventions, the frequency of intervention and duration of sessions that has the greatest effect on PTSD symptoms.
A comprehensive search of MEDLINE, PubMed, PsycINFO and Web of Science was conducted for articles published from January 1980 to 25th June 2021. A search strategy was developed using keywords with some modifications to allow for alternative spellings and synonyms (Supplementary material 1). Databases were searched from January 1980 since this was the date PTSD was first classified as a disorder in the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association., 2013). Prior to the search commencing (8th June 2021), the protocol for this review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; identification number CRD42021255131). Following a preliminary search, a pragmatic decision was made to widen the eligibility criteria to include people with PTSD attributed to causes other than only musculoskeletal trauma. The review was conducted and reported in accordance with the Preferred reporting System and Meta-Analysis (PRISMA) 2020 statement (Page et al., 2021) (Supplementary material 2).
The selection criteria for inclusion and exclusion of studies were formed following the PICOS (Population, Intervention, Comparator, Outcome and Study design) framework (McKenzie and Brennan, 2021) as follows.
Adults (aged ≥18 years) diagnosed with PTSD using a recognized measure of the presence of PTSD, for example, The Diagnostic and Statistical Manual of Mental Disorders (DSM−5 and or DSM-4) (American Psychiatric Association., 2000).
Randomized controlled trials.
Any form of exercise and/or physical activity interventions, structured or non-structured or a combination of both e.g., resistance training, cardiovascular exercise, walking, occupational activity, Tai-chi, and deep breathing exercise. The term “exercise” is commonly used to describe exercise or physical activity, which is planned, structured and repetitive and which serves to improve physical fitness (Caspersen et al., 1985).
Any study that compared exercise or physical activity with a control group (e.g., usual care or waiting list) for PTSD.
Any validated measure of PTSD symptoms, either self-report or clinician-rated, using measures such as the Clinician-Administered PTSD Scale (CAPS) (Weathers et al., 2018), the PTSD checklist (PCL-5) (Wortmann et al., 2016) and the Posttraumatic Stress Diagnostic Scale (PDS5) (Foa et al., 2015).
Studies not written in English were excluded, as were un-published work in non-peer reviewed journals. Systematic reviews, abstracts and non-experimental study designs were also not considered.
All records retrieved in the database search were imported into the Endnote (Clarivate Analytics, USA) publication management software. Initially, the titles and abstracts were screened, independently by two reviewers (NL and NM), according to the eligibility criteria. The full texts of selected articles were subsequently screened by the same reviewers independently. A screening checklist was used by both reviewers to aid selection. If an article was rated as unsure, it was discussed between the two reviewers. In the event of disagreement between the two reviewers, a third reviewer (DF) adjudicated the eligibility of the article.
Using a data extraction table, based on guidance from the Cochrane Handbook (Li et al., 2021), two reviewers (NL and NM) independently extracted the following data: study details (author, date, location), sample size, characteristics of the participants (age: mean/range, gender), population description, intervention characteristics (type, duration, frequency, time), comparison group, primary outcome measure (measuring PTSD), final assessment point, statistical methods, results and key findings. Any discrepancies were resolved by discussion and re-visiting the relevant study. A third reviewer (DF) was available to mediate any disagreement in data extraction.
The internal validity of the randomized controlled trials was assessed using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2) (Sterne et al., 2019). Two reviewers (NL and NM) independently assessed each of the included studies. A third assessor (DF) was available if needed. The RoB 2 tool consists of five domains of bias: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. For the assessment of bias due to deviations from intended interventions, the reviewers aimed to include all reported randomized participants (intention to treat analysis) in the final analysis and measure all participants outcome (effect of assignment) regardless of whether description of contamination between trial arms were reported in the studies. These effects will vary between studies if some patients do not receive the intervention or deviate from the assigned intervention (Schünemann et al., 2021). The reviewers used the RoB 2 Cribsheet to follow the algorithm to come to an assessment of bias for the individual domains and then to make an overall judgement of the study as either low risk, some concerns or a high risk of bias.
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework (Guyatt et al., 2011) was used to assess the overall level of evidence for the outcome of interest in the included studies. Consistent with GRADE, the quality of the summary evidence was assessed as high, moderate, low or very low. For each study, we evaluated, imprecision, inconsistency, indirectness, risk of bias including publication bias. Applicability of results were categorized by the study interventions and rated when making judgement about the quality of evidence presented in the included studies (Guyatt et al., 2011). Two members of the review team (NL and NM) independently conducted the GRADE rating using the guidance presented in the Cochrane Handbook (Schünemann et al., 2021). Any disagreements between reviewers were resolved in consultation with a third reviewer (DF).
Given the significant clinical and statistical heterogeneity between the studies included in this review, it was not possible to pool effect estimates of physical activity/exercise on PTSD symptoms using meta-analysis. Instead, we summarized effect estimates (mean difference or standardized mean difference) with 95% confidence intervals (CI) where appropriate in the included studies. Standardized Mean Difference (SMD) was extrapolated from reported (Cohen's d) values, exploring mean difference between groups; an effect size of 0.8 or greater was considered a relatively large effect size between two means in the sample population. A reporting guideline, synthesis without meta-analysis (SWiM) in systematic reviews (Campbell et al., 2020), was used in conjunction with the Preferred Reporting System and Meta-Analysis (PRISMA) 2020 statement (Page et al., 2021) to describe the study results. The SWiM was utilized as the data was not appropriate for meta-analysis because of high heterogeneity between studies in terms of design and definition of exposure and outcome measures, and therefore the results are described narratively.
Due to the diversity of the interventions, studies were grouped by the type of exercise intervention (aerobic, multi, resistance, sailing, yoga, mindfulness-based stretching and deep breathing exercise) for synthesis and grading the body of evidence rather than pooling across all exercise types. Vote counting was performed to assess if exercise interventions showed a direction of effect for PTSD outcome scores. Each intervention was classified according to whether it suggested a beneficial direction of effect, no change or detrimental effect. This was visually represented, along with the study sample size, in a direction of effect plot. This method of displaying results for a systematic review is deemed acceptable when meta-analysis is not appropriate (McKenzie and Brennan, 2021).
In total, the search strategy yielded 4,021 articles. After excluding 804 duplicates, the titles and abstracts of 3,217 articles were screened for relevance. Title and abstract screening resulted in the exclusion of 3,194 articles, primarily because these articles did not provide data on PTSD outcome, a clear diagnosis of PTSD, or were not a controlled trial. Of the 23 full-text articles that were assessed, 10 were excluded after further review. Three studies were excluded because no PTSD outcome measure was recorded, another two did not report a PTSD diagnosis, a further two studies reported duplicate data. One study was not an RCT and another one was a trial protocol. Thirteen articles were included in the final analysis. A flow diagram of the study selection process is presented in Figure 1.
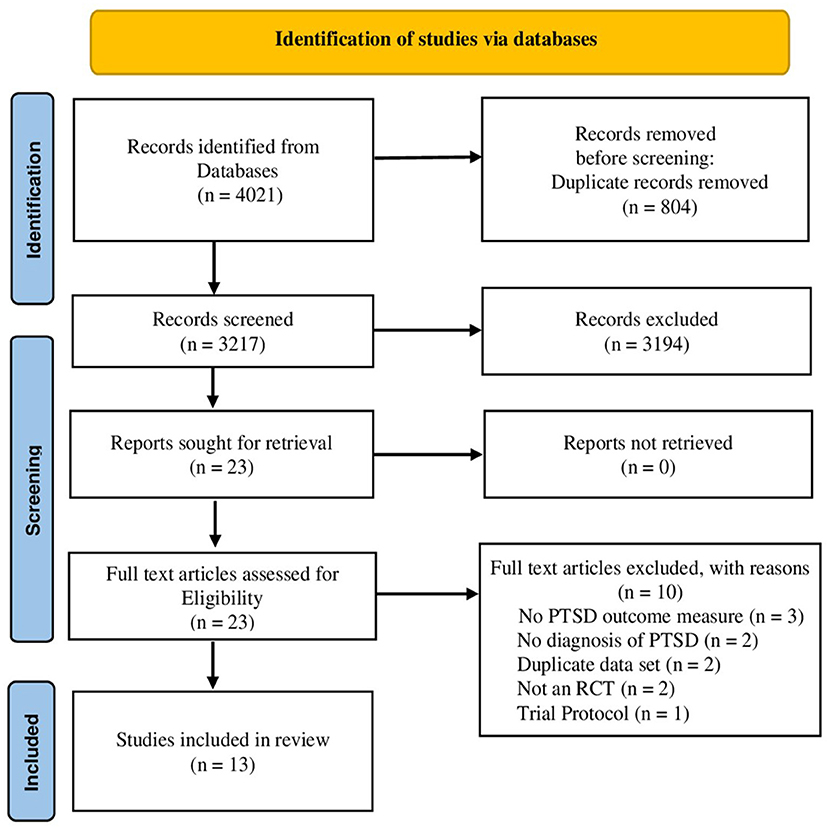
Figure 1. PRISMA Flowchart of the study selection process.
The 13 selected studies (Gelkopf et al., 2013; Kim et al., 2013; Mitchell et al., 2014; van der Kolk et al., 2014; Fetzner and Asmundson, 2015; Powers et al., 2015; Rosenbaum et al., 2015a,b; Goldstein et al., 2018; Johnson et al., 2018; Reinhardt et al., 2018; Whitworth et al., 2019a,b; Hall et al., 2020) involved 531 participants. A significant level of heterogeneity was detected between studies regarding study design including study setting, data source and collection, classification and measures used to define PTSD symptoms, and reported effect estimates. Most studies were performed in the United States (n = 10), followed by Canada (n = 1), Australia (n = 1) and Israel (n = 1). Most studies were conducted in a community setting or utilized community care data (n = 10), followed by secondary care (n = 2) and an Army rehabilitation unit (n = 1). Studies included in this review were mostly randomized controlled trials (n = 7), followed by pilot RCTs (n = 5), and one feasibility/acceptability RCT (n = 1). Across all the studies, 54% of participants were male and 46% were female. Males constituted 64% of the intervention group and 34% of comparators. Participants were slightly older in the comparator group (mean age 45.9 years [SD +/−15.1]) compared to the intervention group (mean age 46.9 years [SD+/−15.4]). Race and ethnicity were poorly recorded (number of studies, % of sample): White in intervention group (8, 48.7%) compared to control (6, 22.4%), African-American in intervention group (2, 37.1%) compared to (2, 23.5%) in control group. An overview of the study characteristics is presented in Table 1.
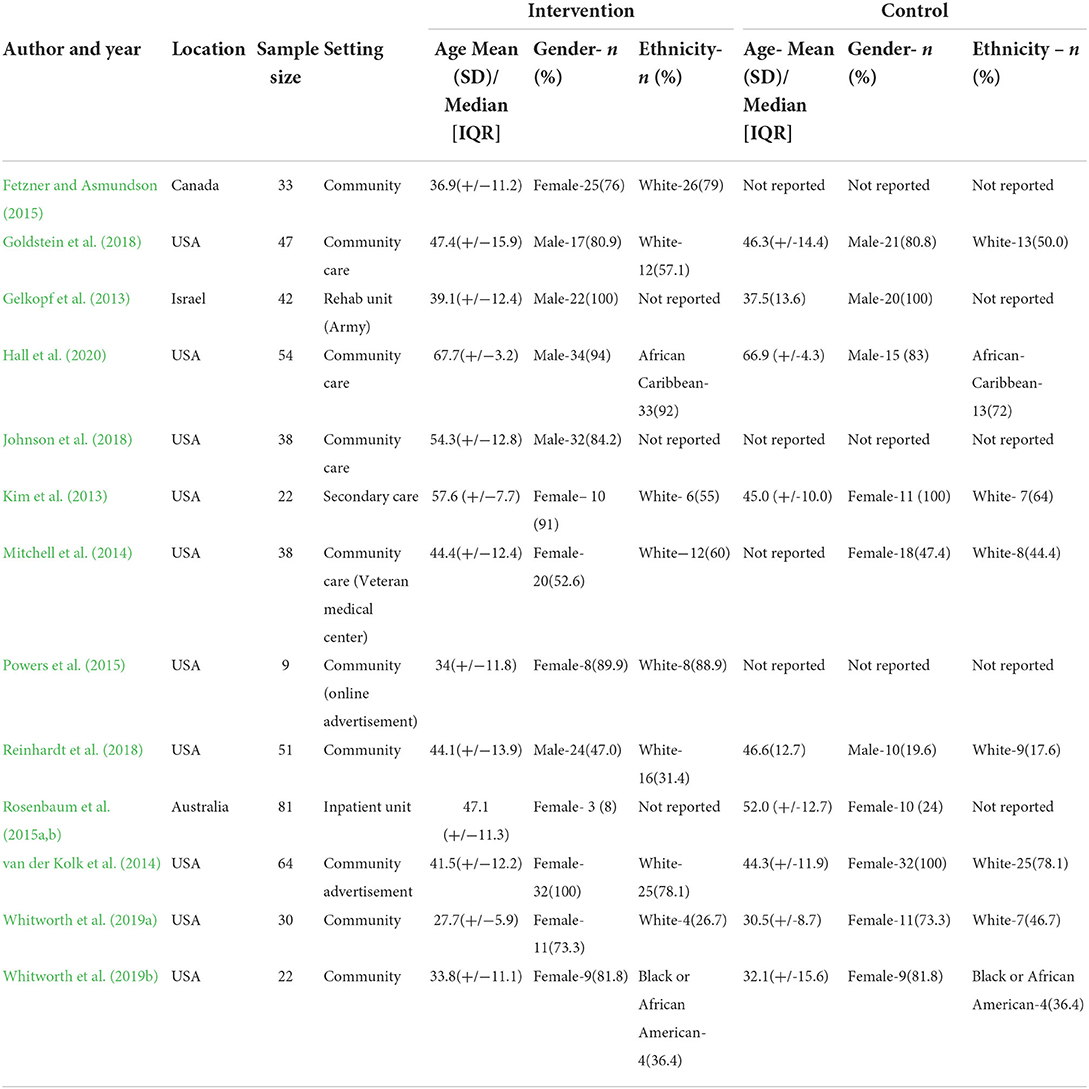
Table 1. Description of included studies.
Key features that impacted upon the methodological quality of each reviewed study are presented in Table 2. There is a significant risk of bias across the studies, with the overall risk of bias considered high or with some concerns. This was primarily the case with regard to allocation concealment, blinding of participants and key research team members, selective reporting, and blinding of outcome assessment. Seven studies (Gelkopf et al., 2013; Mitchell et al., 2014; van der Kolk et al., 2014; Powers et al., 2015; Johnson et al., 2018; Reinhardt et al., 2018; Whitworth et al., 2019a) were rated as having high risk of bias, five (Kim et al., 2013; Fetzner and Asmundson, 2015; Rosenbaum et al., 2015a,b; Goldstein et al., 2018; Whitworth et al., 2019b) with some concerns and only one (Hall et al., 2020) deemed low risk. Follow-up and attrition rates were poorly defined; most studies adequately described the follow-up period, and only one provided an adequate description of rates of and reasons for dropout (Hall et al., 2020). Only one study had a low risk of bias in all criteria of the checklist (Hall et al., 2020). For all studies, the analytical approach utilized was considered appropriate. Five studies (Kim et al., 2013; Fetzner and Asmundson, 2015; Powers et al., 2015; Whitworth et al., 2019a,b) reported a small sample size acknowledging this as a major limitation and demonstrating a paucity and poor quality of sample size calculations. Additionally, one study reported an imbalance in cases vs. control as a major limitation because of inadequate control counterpart (Powers et al., 2015).

Table 2. Risk of bias assessment.
For all 13 studies, the result of the GRADE was very low suggesting the true effect is likely to be substantially different from the estimated effect (Schünemann et al., 2013) (Table 3). Three studies (Kim et al., 2013; Rosenbaum et al., 2015a,b; Goldstein et al., 2018) used multiple types of exercise intervention and a GRADE ranking was undertaken. The GRADE ranking indicates low certainty that the exercise interventions are effective at reducing PTSD symptoms, with small RCTs indicating larger fully-powered trials are needed to adequately test these assumptions. Three studies (Mitchell et al., 2014; van der Kolk et al., 2014; Reinhardt et al., 2018) investigated the effect of yoga on PTSD symptoms; the GRADE ranking indicated moderate/low certainty that there is no effect on PTSD symptoms following a yoga intervention. Four studies (Powers et al., 2015; Goldstein et al., 2018; Whitworth et al., 2019a,b) investigated the effect of resistance training and aerobic exercise and PTSD symptoms; the GRADE ranking was low for both interventions, meaning that we have little certainty that the observed effects are the true effects of these interventions. Three further studies (Gelkopf et al., 2013; Kim et al., 2013; Johnson et al., 2018) tested the effectiveness of sailing, mindfulness-based stretching and deep breathing exercise, and therapeutic horseback riding; these were rated as either low or very low.
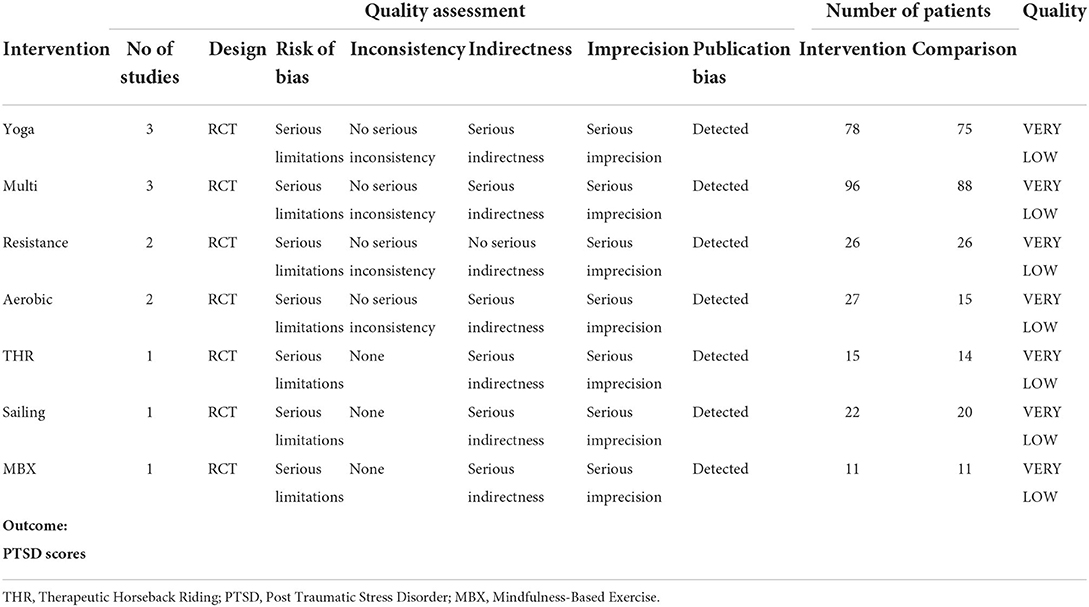
Table 3. GRADE rating on the level of evidence of the included studies.
The direction of effect plot (Table 4) indicates a beneficial direction of effect for all exercise intervention except resistance that suggested no change. A sign test was not performed following the direction of effect plot, due to the small number of studies limiting its power and the detection of publication bias in the studies (Nikolakopoulos, 2020).
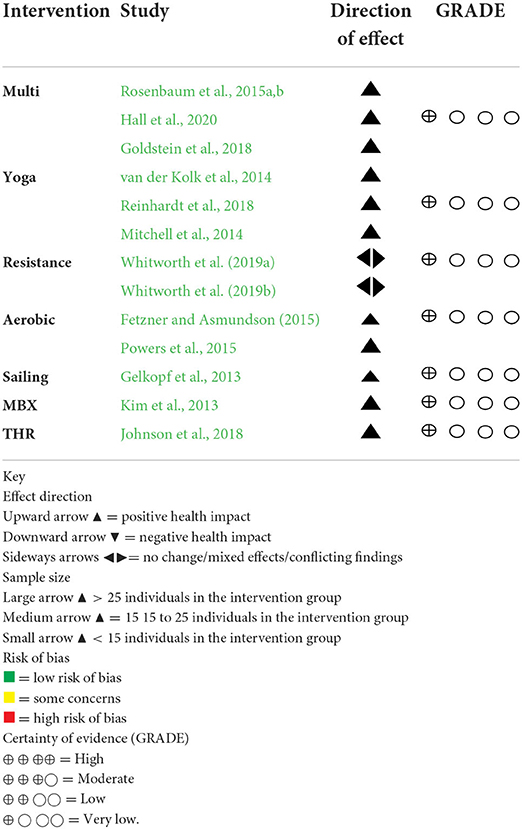
Table 4. Direction of effect Plot, RoB and certainty of evidence.
We noted significant diversity in the diagnostic criteria utilized to ascertain the presence of PTSD symptoms. The most important differences were: (1) where studies used a validated diagnostic tool or screening instrument; (2) Clinician rated assessment (3) Symptoms checklist. Five studies used the self-administered PTSD Checklist for Civilians (PCL-C) (Kim et al., 2013; Mitchell et al., 2014; Fetzner and Asmundson, 2015; Rosenbaum et al., 2015a,b; Reinhardt et al., 2018) and three studies used the Clinician-Administered PTSD Scale (CAPS) (van der Kolk et al., 2014; Goldstein et al., 2018; Reinhardt et al., 2018). Two studies used the PTSD Checklist for military personnel (PCL-M) (Johnson et al., 2018; Reinhardt et al., 2018) and two studies used the self-reported Post Traumatic Stress Diagnostic Scale (PDS5) (Whitworth et al., 2019a,b). One study used the Post-Traumatic stress Symptomology (PTS) (Gelkopf et al., 2013), two studies used the self-administered PTSD Checklist (PCL-5) (Whitworth et al., 2019a; Hall et al., 2020) and one study used the clinician-rated assessment of the PTSD Symptom Scale-Interview (PSSI) (Powers et al., 2015).
Five studies (Powers et al., 2015; Rosenbaum et al., 2015a,b; Goldstein et al., 2018; Johnson et al., 2018; Reinhardt et al., 2018) recruited participants with a DSM-IV diagnosis of PTSD, two (Johnson et al., 2018; Whitworth et al., 2019b) with DSM-V, and a further two studies (Kim et al., 2013; Fetzner and Asmundson, 2015) with PCL-C. One study recruited participants with probable PTSD based on the primary care screening from DSM-5 followed by a clinical interview (Mitchell et al., 2014). Another study used a modified 30-item Stanford Acute Stress Reaction Questionnaire (SASRQ) to establish a diagnosis of PTSD (Gelkopf et al., 2013). Table 5 provides detailed descriptions of the diagnostic criteria and PTSD measure used in the reviewed studies.
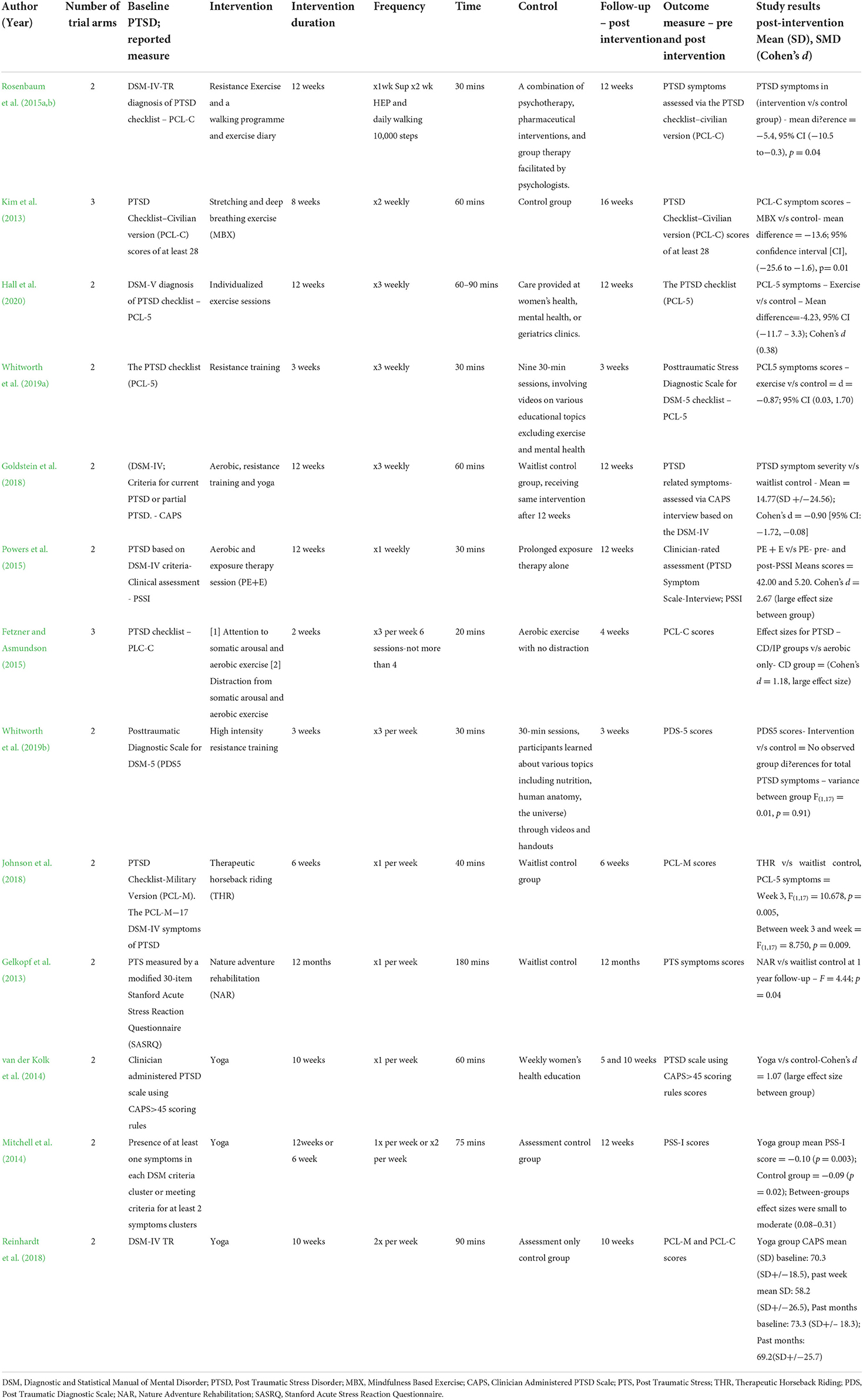
Table 5. Intervention and control component characteristics.
Five studies had follow-ups at 12 weeks following the end of the intervention period (Mitchell et al., 2014; Powers et al., 2015; Rosenbaum et al., 2015a,b; Goldstein et al., 2018; Hall et al., 2020). Of two studies with 10 weeks duration, one had a follow up at 10 weeks (Reinhardt et al., 2018) and the second at both 5 and 10 weeks (van der Kolk et al., 2014). One study had a follow-up point of 1 year following a 12-month intervention (Gelkopf et al., 2013). One study of 8 weeks duration had follow-ups at 4, 8 and 10 weeks (Kim et al., 2013). One study had a follow-up at the end of the 6-week intervention (Johnson et al., 2018). One study had a 4-week follow up assessment point after a 3-week intervention (Whitworth et al., 2019a). One study had a follow-up at the end of a 3-week intervention (Whitworth et al., 2019b). One study of 2 weeks duration had a follow-up directly after the intervention and additionally at 1 and 4 weeks (Fetzner and Asmundson, 2015).
Three studies (182 participants) combined multiple types of exercise in an intervention of 12 weeks duration (Rosenbaum et al., 2015a,b; Goldstein et al., 2018; Hall et al., 2020). One study combined aerobic, strength, balance and flexibility exercise, delivered over a span of 12 weeks with each session lasting for 60–90 min three times a week. This study reported a moderate between-group improvement in PTSD symptoms [standardized mean difference = −4.23, Cohen's d = de (95% CI −11.7 to 3.3)], participants in the intervention group showed a 16% improvement in PTSD symptoms whereas those in the waitlist group demonstrated a 7% improvement post-intervention (Hall et al., 2020). Another study that combined resistance exercise and walking for 30 min, three times a week over a 12 week period resulted in a significant between-group reduction in PTSD symptoms [mean difference = −5.4, 95% CI (−10.5 to −0.3), p = 0.04] (Rosenbaum et al., 2015a,b). One study which combined aerobic exercise, strength training with weights and resistance bands and yoga movements for 60 min per session three times a week over a 12 week period, reported a significant reduction in PTSD symptom severity compared to the waitlist control group [standardized mean difference = 14.77(SD +/−24.56); Cohen's d = −0.90 [95% CI: −1.72, to 0.08] (Goldstein et al., 2018). Two studies included military veterans (101 participants) (Goldstein et al., 2018; Hall et al., 2020) and one recruited adults inpatients within a psychiatric hospital (81 participants) (Rosenbaum et al., 2015a,b). Participants in all studies were predominantly male, with one study conducted on a much older age group (60–78 years) (Hall et al., 2020). All three studies used different PTSD symptom measures and all suggested a beneficial direction of effect for the PTSD scores; however, the certainty of evidence across the studies was very low.
Three studies (153 participants) investigated yoga (Mitchell et al., 2014; van der Kolk et al., 2014; Reinhardt et al., 2018). Two studies reported basing the intervention on Kripalu yoga, which combines physical postures, breathing, and meditation (Mitchell et al., 2014; Reinhardt et al., 2018). Both studies reported a small between group reduction in PTSD symptoms [mean difference = 0.02 (+/4.7); Cohen's d = 0.02; variance F test = 3.41; effect size (0.04, small), p = 0.09]. The third study reported the intervention based on Hatha yoga, which also utilized breathing, postures, and meditation and reported a significant between group reduction in PTSD symptoms [yoga vs. control-Cohen's d = 1.07 (large effect size between group)] (van der Kolk et al., 2014). Two studies (van der Kolk et al., 2014; Reinhardt et al., 2018) were of 10-weeks duration for 60–90 min twice a week and the third study was of either 12 weeks or 6 weeks depending on whether the yoga session was performed once or twice per week for 75 min per session (Mitchell et al., 2014). Two studies included only females (102 participants) with a mix of 93 civilians and 9 veterans (Mitchell et al., 2014; van der Kolk et al., 2014), and the third study consisted mainly of males (45 males, 6 females) who were either serving military personnel or veterans (Reinhardt et al., 2018). Two studies used the CAPS measure (van der Kolk et al., 2014; Reinhardt et al., 2018), with one of these studies also using the PCL-C and PCL-M (Reinhardt et al., 2018), with the PCL-C also being shared with the third study (Mitchell et al., 2014). All three studies suggested a beneficial direction of effect, but the overall certainty of the evidence was very low.
Two studies (52 participants) examined the effectiveness of a resistance exercise intervention over a 3-week period for 30 min, three times a week in an adult population with PTSD, living in the community (Whitworth et al., 2019a,b). The resistance exercise intervention was not effective at reducing PTSD symptoms compared to the control group [(Cohen's d = −0.87; 95% CI (0.03, 1.70); p = 0.05)] (Whitworth et al., 2019a). Additionally, the other study observed no group difference in PTSD symptoms (F = 0.01, p = 0.91) (Whitworth et al., 2019b). Of the 52 participants across the two studies, 77% were female. Both studies consisted of five resistance exercises: squat, bench press, pulldown, overhead press and biceps curl. Both studies used the same outcome measure of PDSD but both studies suggested no overall change to PTSD outcome scores. The certainty of evidence was very low for this intervention.
Two studies (42 participants) investigated the effectiveness of aerobic exercise on adults living in the community, diagnosed with PTSD (Fetzner and Asmundson, 2015; Powers et al., 2015). Both studies reported a significant between group difference in the reduction of PTSD following aerobic exercise mean = 42.0 (Cohen's d = 2.67) and Cohen's d = 1.18 respectively. Across the two studies, 79% of the participants were female. One study was of 12 weeks duration (one session per week), lasting 30 min (Powers et al., 2015), while the second study was of 2 weeks duration but with sessions three times a week (i.e., total of 6 sessions), each session was 20 min duration (Fetzner and Asmundson, 2015). The two studies used different PTSD outcome measures but both studies suggested a beneficial direction of effect, although the certainty of the evidence was very low.
One study (42 participants) trialed a weekly, 180 minutes per session sailing intervention over a one-year period with male military veterans (Gelkopf et al., 2013). This study reported a statistically significant reduction in PTSD following sailing compared to the control group (F: 4.44; p = 0.04). The PCL-M was used as the outcome measure as they were military. The results implied a beneficial direction of effect, but the study was at high risk of bias and the certainty of the evidence was very low.
One study (29 participants) investigated a twice a week, 60 min per session for 8 weeks mindfulness-based exercise intervention with adult nurses (97% female) (Kim et al., 2013). This study reported a superior group reduction in PTSD following the mindfulness- based exercise intervention compared to the control group (mean difference: −13.6; 95% (CI) [−25.6 to −1.6], p = 0.01). The PCL-C PTSD outcome measure was used with the results suggesting a beneficial direction of effect. The study was judged to be of moderate risk of bias and the certainty of evidence was very low.
One study (29 participants) evaluated an intervention of therapeutic horseback riding on military veterans, once a week for 6 weeks, each session lasting for 40 min (Johnson et al., 2018). This study reported significant between group differences in PTSD symptoms in the horse-riding group compared to a control group; symptoms significantly decreased between baseline and week 3, (F = 10.7, p = 0.005), and between week 3 and week 6 of riding, (F = 8.750, p = 0.009). The study utilized the PCL-M measure of PTSD and the results suggested a beneficial direction of effect, but the study was at high risk of bias and the certainty of evidence was very low.
This systematic review is the first to investigate and compare different forms of exercise/physical activity for their ability to reduce symptoms of PTSD. The review suggested that there was a beneficial direction of effect for all exercise/physical activity interventions except resistance exercise. An explanation as to why no direction of effect in the two studies investigating resistance exercise (Whitworth et al., 2019a,b) might be due to the short follow-up period (3 weeks), which was one of the shortest compared to the other reviewed studies. None of the exercise/physical activity interventions had any detrimental effects on PTSD outcome scores. Overall, the results indicate that there is better quality of evidence for multimodal exercise interventions (a mixture of cardiovascular and resistance training) having a beneficial direction of effect on PTSD symptoms. However, the GRADE assessment indicates only moderate certainty of evidence that exercise interventions are effective at reducing PTSD symptom, primarily due to concerns about wide variation between the included studies.
The findings of this review suggests that overall the risk of bias was high in approximately 50% of the included studies. The number of randomized controlled trials for each exercise type was limited, with three types only evaluated within a single study (mindfulness stretching and breathing, sailing and horse riding). Wide heterogeneity was seen in the use of PTSD outcome measures across the studies despite gold standards for PTSD measurement being reported (Hall et al., 2020). With small sample sizes and lack of reliability, the evidence is not strong enough to draw firm conclusions and determine which exercise intervention is the most effective in reducing PTSD symptoms. However, even though the overall effect size could not be reported within a meta-analysis, this review shows that exercise does have a beneficial effect on PTSD symptoms.
This review adds to previous systematic reviews from Rosenbaum et al. (2015a,b) and McGranahan and O'Connor (2021), who concluded that exercise has a beneficial effect on PTSD symptoms. However, the current review has highlighted that other physical activities, such as sailing (Gelkopf et al., 2013), therapeutic horseback riding (Johnson et al., 2018), and mindfulness-based stretching and deep breathing exercise (Kim et al., 2013), may also be beneficial. These interventions require further investigation as studies were singular and had small sample sizes. Additionally, the current review adds to a previous systematic review by Whitworth and Ciccolo (2016), exploring the effect of exercise on PTSD symptoms in military veterans. Their review included two non-randomized trials compared to the thirteen randomized controlled trials included in the current review, of which five were on military populations (Gelkopf et al., 2013; Goldstein et al., 2018; Johnson et al., 2018; Reinhardt et al., 2018; Hall et al., 2020).
The current review has several strengths. The protocol of this systematic review was registered prospectively online (PROSPERO) and the review adheres to the PRISMA guidelines. All stages of the review were conducted by two reviewers, including the risk of bias assessment and GRADE evaluation. However, there are some limitations which should be noted. Significant heterogeneity was found between the included studies, particularly pertaining to methods of ascertaining PTSD and physical/exercise type which precluded meta-analysis. A direction of effect plot was used, but this only focused on whether there is evidence of an effect, rather than the average size of effect (Campbell et al., 2020). The gender of participants in individual studies were often imbalanced or of a single gender, although overall the studies were more balanced with 54% males and 46% females. The study populations were heterogeneous in terms of participants being civilian, military or inpatients, so the results do not represent any one population. Furthermore, the effect of the different frequency, length of session and intensity of exercise/physical activity on PTSD has not been fully investigated in this review, further studies would be useful to address this aspect.
The research also did not differentiate between participants with PTSD and those with complex PTSD; where complex PTSD includes people who have experienced repeated traumatic events either as a child or as an adult (Bisson et al., 2015). Therefore, exercise/physical activity interventions and their results could be different for these individuals. Publication bias could have also influenced the results of this review due to small sample sizes and associated reduced methodological quality compared to larger studies (Friedman, 2019). Additionally, there were limitations in the study selection process such as restricting the search to English language publications.
Given that a number of different exercise and physical activities have been evaluated for reducing PTSD with quite different dynamics i.e., ranging from individual-based exercise to group activity and those such as sailing or horse-riding, it would be beneficial to understand which components of exercise are most important and how beneficial effects on PTSD are mediated (Light and Pillemer, 1984). Given that the best quality of evidence supported multimodal exercise intervention (i.e., combined cardiovascular and resistance training) these should be recommended for those with PTSD. Furthermore, future research should consider exploring whether there is an interaction between gender and the effects of exercises on PTSD symptoms.
This review quantifies the effect of different exercise and physical activity interventions on PTSD symptoms and demonstrated that physical/exercise interventions shows promise to improve PTSD symptoms. Adequately powered additional RCTs are required to provide more definitive evidence of a causal relationship between different types of exercise/physical activity and PTSD. Significant heterogeneity was found between the included studies, particularly pertaining to diagnosing PTSD, sample size, population and method employed, which precluded meta-analysis. Nonetheless, this review indicated that exercise and physical activity shows potential for improving PTSD symptoms.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
NL, NM, and DF contributed equally to the conception of this review. NL and NM performed screening for study selection, collected data from the included studies, and conducted quality assessment. FJ drafted the first version of this review and this was reviewed/revised by DF and DE. The final version was drafted by FJ. The search strategy was developed by NL and iteration discussed with NM and DF. The final version was approved by DF and DE. The search was performed by NL. FJ and NL performed data analysis/synthesis. NM ensured data extraction consistency. FJ drafted the manuscript and all authors critically reviewed the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.943479/full#supplementary-material
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders DSM-IV. 4th ed. Washington, DC: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association.doi: 10.1176/appi.books.9780890425596
Asher, G. N., Gartlehner, G., Gaynes, B. N., Amick, H. R., Forneris, C., Morgan, L. C., et al. (2017). Comparative benefits and harms of complementary and alternative medicine therapies for initial treatment of major depressive disorder: systematic review and meta-analysis. J. Altern. Complement. Med. 23, 907–919. doi: 10.1089/acm.2016.0261
Baker, C. (2020). Mental health statistics for England: prevalence, services and funding. House of Commons Library. Available online at: https://researchbriefings.files.parliament.uk/documents/SN06988/SN06988.pdf. (accessed May 11, 2022).
Bartley, C. A., Hay, M., and Bloch, M. H. (2013). Meta-analysis: aerobic exercise for the treatment of anxiety disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry. 45, 34–39. doi: 10.1016/j.pnpbp.2013.04.016
Bisson, J. I., Cosgrove, S., Lewis, C., Lewis, N. P., and Robert, N. P. (2015). Post-traumatic stress disorder. BMJ. 351, h6161. doi: 10.1136/bmj.h6161
Bjorkman, F., and Ekblom, O. (2021). Physical exercise as treatment for PTSD: A systematic review and meta-analysis. Mil. Med. 26, 497. doi: 10.1093/milmed/usab497
Brewin, C. R., Rose, S., Andrews, B., Green, J., Tata, P., McEvedy, C., et al. (2002). A brief screening instrument for post-traumatic stress disorder. Br. J. Psychiatry. 181, 158–162. doi: 10.1192/bjp.181.2.158
Campbell, M., McKenzie, J. E., Sowden, A., Katikireddi, A., Brennan, S. V., Ellis, S. E., et al. (2020). Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 368, 16890. doi: 10.1136/bmj.l6890
Caspersen, C. J., Powell, K. E., and Christenson, G. M. (1985). Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 100, 126–31.
Chopra, M. P. (2018). PTSD in late life: special issues. Psychiatric Times. 32, 1–9. Available online at: https://www.psychiatrictimes.com/view/ptsd-late-life-special-issues (accessed July 11, 2002).
Fear, N. T., Jones, M., Murphy, D., Hull, L., Iversen, A. C., Coker, B., et al. (2010). What are the consequences of deployment to Iraq and Afghanistan on the mental health of the UK armed forces? A cohort study. Lancet. 375, 1783–1797. doi: 10.1016/S0140-6736(10)60672-1
Fetzner, M. G., and Asmundson, G. J. (2015). Aerobic exercise reduces symptoms of posttraumatic stress disorder: a randomized controlled trial. Cogn. Behav. Ther. 244, 301–313. doi: 10.1080/16506073.2014.916745
Foa, E., McLean, C., Zang, Y., Zhong, J., Powers, M., Kauffman, B., et al. (2015). Psychometric properties of the posttraumatic diagnostic Scale for DSM-5 (PDS-5). Psychol. Assess. 28, 1166–1171. doi: 10.1037/pas0000258
Friedman, M. J. (2019). “Physical exercise as a potentially useful component of post-traumatic stress disorder treatment,” in D. L. Noordsy, eds. Lifestyle Psychiatry (Washington, DC: American Psychiatric Publishing).79–91.
Gelkopf, M., Hasson-Ohayon, I., Bikman, M., and Kravetz, S. (2013). Nature adventure rehabilitation for combat-related posttraumatic chronic stress disorder: a randomized control trial. Psychiatry Res. 209, 485–493. doi: 10.1016/j.psychres.2013.01.026
Goldstein, L. A., Mehling, W. E., Metzler, T. J., Cohen, B. E., Barnes, D. E., Choucroun, G. J., et al. (2018). Veterans Group Exercise: A randomized pilot trial of an Integrative Exercise program for veterans with posttraumatic stress. J. Affect. Disord. 227, 345–352. doi: 10.1016/j.jad.2017.11.002
Greenberg, N., Jones, E., Jones, N., Fear, N. T., and Wessely, S. (2011). The injured mind in the UK Armed Forces. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 366, 261–267. doi: 10.1098/rstb.2010.0210
Guyatt, G., Oxman, A. D., Akl, E. A., Kunz, R., Vist, G., Brozek, J., et al. (2011). GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 64, 383–394. doi: 10.1016/j.jclinepi.2010.04.026
Hall, K. S., Morey, M. C., Bosworth, H. B., et al. (2020). Pilot randomized controlled trial of exercise training for older veterans with PTSD. J. Behav. Med. 43, 648–659. doi: 10.1007/s10865-019-00073-w
Jayakody, K., Gunadasa, S., and Hosker, C. (2014). Exercise for anxiety disorders: systematic review. Br. J. Sports Med. 48, 187–196. doi: 10.1136/bjsports-2012-091287
Johnson, R. A., Albright, D. L., Marzolf, J. R., et al. (2018). Effects of therapeutic horseback riding on post-traumatic stress disorder in military veterans. Military Med. Res. 5, 1-13. doi: 10.1186/s40779-018-0149-6
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., and Nelson, C. B. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry. 52,1048–1060. doi: 10.1001/archpsyc.1995.03950240066012
Kim, S. H., Schneider, S. M., Bevans, M., Kravitz, L., Mermier, C., Qualls, C., et al. (2013). PTSD symptom reduction with mindfulness-based stretching and deep breathing exercise: randomized controlled clinical trial of efficacy. Clin. Endocrinol. Metab. 8, 2984–2992. doi: 10.1210/jc.2012-3742
Klein, S., and Alexander, D. A. (2009). Epidemiology and presentation of post-traumatic disorders. Psychiatry. 8, 282-287. doi: 10.1016/j.mppsy.2009.05.001
Krogh, J., Hjorthøj, C., Speyer, H., Gluud, C., and Nordentoft, M. (2017). Exercise for patients with major depression: a systematic review with meta-analysis and trial sequential analysis. BMJ Open. 7, e014820. doi: 10.1136/bmjopen-2016-014820
Kvam, S., Kleppe, C. L., Nordhus, I. H., and Hovland, A. (2016). Exercise as a treatment for depression: a meta-analysis. J. Affect. Disord. 202, 67–86. doi: 10.1016/j.jad.2016.03.063
Lawrence, S., De Silva, M., and Henley, R. (2010). Sports and games for post-traumatic stress disorder (PTSD). Cochrane Datab. Syst. Rev. 20, CD007171. doi: 10.1002/14651858.CD007171.pub2
Li, T., Higgins, J. P. T., and Deeks, J. J. (2021). “Chapter 5: Collecting data,” in Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J and Welch, V.A, eds. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration. Available online at: https://training.cochrane.org/handbook/current (accessed 11 May, 2022).
Light, R. J., and Pillemer, D. B. (1984). Summing Up: The Science of Reviewing Research. Cambridge, MA: Harvard University Press. doi: 10.4159/9780674040243
McFarlane, A. C., Williamson, P., and Barton, C. A. (2009). The impact of traumatic stressors in civilian occupational settings. J. Public. Health. Policy. 30, 311–327. doi: 10.1057/jphp.2009.21
McGranahan, M. J., and O'Connor, P. J. (2021). Exercise training effects on sleep quality and symptoms of anxiety and depression in post-traumatic stress disorder: A systematic review and meta-analysis of randomized control trials. Ment. Health Phys. Act. 20, 10035. doi: 10.1016/j.mhpa.2021.100385
McKenzie, J. E., and Brennan, S. E., (2021). “Chapter 12: Synthesizing presenting findings using other methods,” in Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J and Welch, V.A, eds. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration. Available online at: https://training.cochrane.org/handbook/current. (accessed 11, May 2022).
McManus, S., Bebbington, P. E., Jenkins, R., and Brugha, T. (2016). Mental Health and Wellbeing in England: The Adult Psychiatric Morbidity Survey 2014. Leed, UK: NHS Digital. Available online at: https://openaccess.city.ac.uk/id/eprint/23646/1/ (accessed May 11, 2022)
Mitchell, K. S., Dick, A. M., DiMartino, D. M., Smith, B. N., Niles, B., Koenen, K. C., et al. (2014). A pilot study of a randomized controlled trial of yoga as an intervention for PTSD symptoms in women. J. Trauma. Stress. 27, 121–128. doi: 10.1002/jts.21903
Mura, G., Moro, M. F., Patten, S. B., and Carta, M. G. (2014). Exercise as an add-on strategy for the treatment of major depressive disorder: a systematic review. CNS Spectr. 19, 496–508. doi: 10.1017/S1092852913000953
NICE (2018). National Institute for Health and Care Excellence Guidelines. Post-traumatic stress disorder [NG116]. NICE. 2018. Available online at: https://www.nice.org.uk/guidance/ng116/resources/posttraumatic-stress-disorder-pdf-66141601777861 (accessed May 11, 2022).
Nikolakopoulos, S. (2020). Misuse of the sign test in narrative synthesis of evidence. Res. Synth. Methods. 11, 714–719. doi: 10.1002/jrsm.1427
Page, M., McKenzie, J., Bossuyt, P., Boutron, I., Hoffmann, T., Mulrow, C., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 372, n71. doi: 10.1136/bmj.n71
Perkonigg, A., Kessler, R. C., Storz, S., and Wittchen, H. U. (2000). Traumatic events and post-traumatic stress disorder in the community: prevalence, risk factors and comorbidity. Acta Psychiatr. Scand. 101, 46–59. doi: 10.1034/j.1600-0447.2000.101001046.x
Powers, M. B., Medina, J. L., Burns, S., Kauffman, B. Y., Monfils, M., Asmundson, G. J., et al. (2015). Exercise augmentation of exposure therapy for PTSD: rationale and pilot efficacy data. Cogn. Behav. Ther. 44, 314–327. doi: 10.1080/16506073.2015.1012740
Ravindran, A. V., Balneaves, L. G., Faulkner, G., et al. (2016). Canadian Network for Mood and Anxiety Treatments (CANMAT) Depression Work Group. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 5. Complementary and alternative medicine treatments. Can. J. Psychiatry. 61, 576–587. doi: 10.1177/0706743716660290
Reinhardt, K. M., Noggle Taylor, J. J., Johnston, J., Zameer, A., Cheema, S., et al. (2018). Kripalu yoga for military veterans with PTSD: a randomized trial. J. Clin. Psychol. 74, 93–108. doi: 10.1002/jclp.22483
Rosenbaum, S., Sherrington, C., and Tiedmann, A. (2015a). Exercise augmentation compared with usual care for post-traumatic stress disorder: A randomized controlled trial. Acta Psychiatr. Scand. 131, 350–359. doi: 10.1111/acps.12371
Rosenbaum, S., Vancampfort, D., Steel, Z. J., Ward, P. B., and Stubbs, B. (2015b). Physical activity in the treatment of post-traumatic stress disorder: A systematic review and meta-analysis. Psychiatry Res. 230, 130–136. doi: 10.1016/j.psychres.2015.10.017
Schuch, F. B., Vancampfort, D., Richards, J., Rosenbaum, S., Ward, P. B., and Stubbs, B. (2016). Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J. Psychiatr. Res. 77, 42–51. doi: 10.1016/j.jpsychires.2016.02.023
Schünemann, H., Brozek, J., Guyatt, G., and Oxman, A. (2013). GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group. Available online at: http://www.gradeworkinggroup.org. (accessed May 12, 2022).
Schünemann, H. J., Higgins, J. P. T., Vist, G. E., Glasziou, P., Akl, E. A., Skoetz, N., et al. (2021). “Chapter 14: Completing ‘Summary of findings' tables and grading the certainty of the evidence,” in Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A, eds. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration. Available online at: https://training.cochrane.org/handbook/current. (accessed May 11, 2022).
Smid, G. E., van der Velden, P. G., Gersons, B. P. R., and Kleber, R. J. (2012). Late-onset posttraumatic stress disorder following a disaster: A longitudinal study. Psychol. Trauma. 4, 312–322. doi: 10.1037/a0023868
Sterne, A. C., Savovi,ć, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 366, l4898. doi: 10.1136/bmj.l4898
Stonerock, G. L., Hoffman, B. M., Smith, P. J., and Blumenthal, J. A. (2015). Exercise as treatment for anxiety: systematic review and analysis. Ann. Behav. Med. 49, 542–556. doi: 10.1007/s12160-014-9685-9
Stubbs, B., Vancampfort, D., Rosenbaum, S., et al. (2016). Challenges establishing the efficacy of exercise as an antidepressant treatment: a systematic review and meta-analysis of control group responses in exercise randomised controlled trials. Sports Med. 46, 699–713. doi: 10.1007/s40279-015-0441-5
Stubbs, B., Vancampfort, D., Rosenbaum, S., et al. (2017). An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: a meta-analysis. Psychiatry Res. 249, 102–108. doi: 10.1016/j.psychres.2016.12.020
van der Kolk, B. A., Stone, L., West, J., Rhodes, A., Emerson, D., Suvak, M., et al. (2014). Yoga as an adjunctive treatment for posttraumatic stress disorder: a randomized controlled trial. J. Clin. Psychiatry. 75, e559–e565. doi: 10.4088/JCP.13m08561
Weathers, F. W., Bovin, M. J., Lee, D. J., Schnurr, P. P., Kaloupek, D. G., Keane, T. M., et al. (2018). The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 30, 383–395. doi: 10.1037/pas0000486
Whitworth, J. W., and Ciccolo, J. T. (2016). Exercise and post-traumatic stress disorder in military veterans: a systematic review. Mil. Med. 181, 953–960. doi: 10.7205/MILMED-D-15-00488
Whitworth, J. W., Nosrat, S., SantaBarbara, N. J., and Ciccolo, J. T. (2019a). Feasibility of resistance exercise for posttraumatic stress and anxiety symptoms: a randomized controlled pilot study. J. Trauma Stress. 32, 977–984. doi: 10.1002/jts.22464
Whitworth, J. W., Nosrat, S., SantaBarbara, N. J., and Ciccolo, J. T. (2019b). High intensity resistance training improves sleep quality and anxiety in individuals who screen positive for posttraumatic stress disorder: A randomized controlled feasibility trial. Ment. Health Phys. Act. 16, 43–49. doi: 10.1016/j.mhpa.2019.04.001
Williamson, V., Murphy, D., and Greenberg, N. (2019). Post-traumatic stress disorder: diagnosis and management. Integr. J. Orthop. Traumatol. 2, 1–3. doi: 10.1002/tre.701
Keywords: post-traumatic stress disorder (PTSD), exercise, effectiveness, trauma, management
Citation: Jadhakhan F, Lambert N, Middlebrook N, Evans DW and Falla D (2022) Is exercise/physical activity effective at reducing symptoms of post-traumatic stress disorder in adults — A systematic review. Front. Psychol. 13:943479. doi: 10.3389/fpsyg.2022.943479
Received: 13 May 2022; Accepted: 25 July 2022;
Published: 12 August 2022.
Edited by:
Sara Carletto, University of Turin, ItalyReviewed by:
Omer Horovitz, Tel-Hai College, IsraelCopyright © 2022 Jadhakhan, Lambert, Middlebrook, Evans and Falla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Deborah Falla, ZC5mYWxsYUBiaGFtLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.