
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 01 July 2022
Sec. Neuropsychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.936639
 Virgile Clergue-Duval1,2,3,4*
Virgile Clergue-Duval1,2,3,4* Thomas Barré1,2Emmanuel Cognat3,4,5Anne-Laure Brichet2,6Claire Géraud1,2
Thomas Barré1,2Emmanuel Cognat3,4,5Anne-Laure Brichet2,6Claire Géraud1,2 Julien Azuar1,2,3Philippe Michaud2,7Dorothée Lecallier2,6Sonia Arfaoui-Geffroy2,8Eric Hispard1,2
Julien Azuar1,2,3Philippe Michaud2,7Dorothée Lecallier2,6Sonia Arfaoui-Geffroy2,8Eric Hispard1,2 Claire Paquet3,4,5
Claire Paquet3,4,5 Frank Bellivier1,3,4Frank Questel1,2,3
Frank Bellivier1,3,4Frank Questel1,2,3 Florence Vorspan1,3,4 and all members of the ResAlCog care network
Florence Vorspan1,3,4 and all members of the ResAlCog care network
The disease progression of severe alcohol-related cognitive impairment (ARCI) is debated. The aim of this study was to compare the cognitive change of patients with severe ARCI in inpatient setting to that of patients with Alzheimer’s disease (AD). Fifteen consecutive patients with severe ARCI were recruited between 2013 and 2015. They received inpatient detoxification, neurological assessment, and inpatient cognitive rehabilitation in specialized facilities. Twelve patients, with documented AD matched on sex and initial cognitive impairment severity, were selected. All have benefited from two neuropsychological assessments. The neurocognitive change was tested in both groups with pair-wised Wilcoxon tests. ARCI and AD patients’ time course was compared with Mann–Whitney–Wilcoxon test. In ARCI group, first assessment occurred at 2.9 (± 2.2) months of abstinence and follow-up 6.5 (± 2.9) months later, the mean age was 56.5 (± 7.4) years, and 12 were men. In AD group, follow-up occurred at 12.8 (± 2.9) months (p < 10–3), the mean age was 72.3 (± 8.4) years (p < 10–3), and 10 were men. ARCI patients significantly improved on one executive function test (TMT-B; p < 0.05), while AD patients have worsened memory subtests on Free-and-Cued-Selective-Reminding Test (p < 0.05). These tests showed a statistically different change between severe ARCI and AD group (p < 0.05). Severe ARCI patients have improved in executive functioning, discernible on the TMT-B test, in specific care setting, including abstinence maintenance and rehabilitation. The disease progression was different from that observed in AD patients.
In the general population, alcohol use disorder is the strongest modifiable risk factor for dementia onset and the primary risk factor for early dementia (Schwarzinger et al., 2018). The development of intensive cognitive rehabilitation therapy with prolonged abstinence has been demonstrated to significantly improve alcohol-related cognitive impairments (ARCI) in non-amnesic and non-demented patients (Rupp et al., 2012; Bates et al., 2013; Maillard et al., 2020). Severe ARCI (formerly labeled “alcoholic dementia”) and Wernicke–Korsakoff syndrome have been initially described as an acquired irreversible condition. However, the prognosis of the disorder, especially with the development of new intensive cognitive rehabilitation programs, is still debated. Some authors proposed a specific and tailored cognitive rehabilitation training associated with alcohol abstinence. Those rehabilitation programs were diverse but included, for example, motoric procedural learning by the repetition of simple motor tasks, cognitive procedural learning, and memory training (including the repetition of laws and algorithms; Oudman et al., 2015), repetitive memory training (Kashima et al., 1999), and intensive errorless training with the support of external reminders, calendars, and alarms (Kopelman et al., 2009; Svanberg and Evans, 2013). Furthermore, the adjunction of behavioral therapy reinforcement of the memory training, and the rule provision in executive tasks, improved the performances (Svanberg and Evans, 2013). Most of the evidence of improvement abilities in patients diagnosed with Wernicke–Korsakoff syndrome or severe ARCI come from comparative studies comparing the learning abilities of patients with Wernicke–Korsakoff syndrome with those of healthy controls on one test at a time (Svanberg and Evans, 2013; Oudman et al., 2015). Those studies have limited sample sizes (ranging from single case report to 5 to 10 patients compared to matched controls). Very few studies prospectively assessed the global functioning of patients before and after a comprehensive cognitive rehabilitation program. To date, despite the demonstrated abilities of each rehabilitation exercise to improve one or the other cognitive function assessed by a specific test, the transferability of those results in a global improvement of patient functioning is not clearly demonstrated.
Among the few prospective data on the change of cognitive impairment in Wernicke–Korsakoff syndrome or severe ARCI, two studies deserve a specific attention (Fujiwara et al., 2008; Maillard et al., 2021). Regarding the episodic memory impairment, both Fujiwara et al. (n = 20) and Maillard et al. (n = 8) showed the stability of impairment (Fujiwara et al., 2008; Maillard et al., 2021). Regarding the executive functions, the results were discordant and only Fujiwara et al. showed a possible improvement in some of the executive functions at follow-up after 2 years, but the patients were abstinent since several years at baseline (Fujiwara et al., 2008). This wide variability may be related to the heterogeneity in patients included as having Wernicke–Korsakoff syndrome, already a difficult classification (Schwarzinger et al., 2018; Azuar et al., 2021), as well as the heterogeneity of assessment in terms of choice in neurocognitive tests, of time since the diagnosis or time between the test and the retest.
In order to participate in this debate, we choose to study the cognitive change of patients with established severe ARCI, where the initial evaluation was made after the elimination of all curable and easy to improve causes of cognitive deficit, and where all the differential diagnoses have been ruled out. All those patients were referred to a specialized addiction medicine ward for diagnosis. Furthermore, they all received intensive long lasting inpatient cognitive rehabilitation in specialized facilities using the most updated rehabilitation procedures. As alcohol abstinence was maintained in those care facilities, we can confidently rule out alcohol relapse as a cause of heterogeneity in the cognitive change.
The aims of this study were to observe the cognitive change of those patients with severe ARCI supported in specialized facilities in cognitive rehabilitation and to compare to the disease progression of patients with established Alzheimer’s disease matched on sex and initial cognitive impairment.
For this comparative chart review, study patients with severe ARCI were included. Patients were recruited in the addiction medicine ward of Parisian university hospital. All consecutive patients were included during 2 years between 2013 and 2015. Patients were screened after at least 1 month of inpatient detoxification using the Montreal Cognitive Assessment, with a threshold below 25 points (Nasreddine et al., 2005). They were then undergoing a full neuropsychological testing. Based on previous studies (Caine et al., 1997; Pitel et al., 2011; Sachdev et al., 2014), patients with severe ARCI were precisely defined as presenting with the three following criteria. First, the patient has to present at least two different impaired cognitive functions on the first neuropsychological assessment, including executive functions and episodic memory. Second, the patient had to present a retrospective documented clinical sign evocative of Wernicke’s encephalopathy such as malnourishment and/or a neurologic sign (ataxia or eye movement’s disorder). Malnourishment itself was defined as either weight loss ≥ 10%, with respect to any previously recorded weight from a previous medical record; or weight loss ≥ 5% in 1 month, with respect to a previously recorded weight; or Body Mass Index ≤ 17 kg/m2, or serum albumin < 30 g/l; or serum prealbumin < 110 mg/l. Third, any other documented etiology for dementia (degenerative or vascular) had to be ruled out with the adequate brain imaging and/or cerebrospinal fluid examination (Azuar et al., 2021).
All patients diagnosed with severe alcohol-related neurocognitive disorder were then referred to specific inpatient long lasting residential rehabilitation programs (all members of the ResAlCog care network). Cognitive rehabilitation program included patient stimulation in everyday life by all members of the healing staff and specific sessions of memory and executive functions rehabilitation provided by trained neuropsychologists.
Using these criteria, 31 patients with severe ARCI were selected between 2013 and 2015. Among them, 15 patients had a documented second standardized neuropsychological assessment allowing the description of a time change.
To constitute a control group, 12 patients were selected from Expert Center on Cognitive disorders located in the same hospital. All were diagnosed with mild cognitive impairment (MCI) due to Alzheimer’s disease (Albert et al., 2011). The two groups matched on sex and the initial level of cognitive impairment at the time of diagnosis according to screening tools. As patients from this outpatient program are evaluated with the MMSE (Folstein et al., 1975), the previously published correspondence between the Montreal Cognitive Assessment and MMSE (Trzepacz et al., 2015) was used to match the two groups.
Standardized test assessing executive functions, episodic memory, and visuo-spatial ability that are known to be impaired in patients with ARCI (Ihara et al., 2000; Pitel et al., 2008, 2009; Stavro et al., 2013; Le Berre et al., 2017) and also available in patients AD group was selected.
Executive functions were assessed with the Verbal fluency task (Cardebat et al., 1990), including a letter and a category fluency tasks. Flexibility was also assessed with the Trail Making Test (TMT-B) expressed as errors and speed (Reitan, 1955). To assess a processing speed as well as to adjust the patients on premorbid educational level, the Wechsler Adult Intelligence Scale III or IV (Saklofske and Schoenberg, 2011) was used, especially the coding subtest. Verbal conceptualization was assessed with the similarities subtest from the WAIS III or IV. Memory was assessed through with two different tests. The 16-item Free-and-Cued Recall, a French validated version of the free-and-cued-selective reminding test (FCSRT) (Van der Linden et al., 2004), was used for verbal and anterograde memory assessment. The Rey Complex Figure Test Copy (McKinlay, 2011), expressed in score and speed, was used for the Visuo-spatial processing.
The comparability of the two groups was tested with Chi-squared test for sex and Mann–Whitney–Wilcoxon test for age, initial cognitive impairment, and time elapsed between the two standardized neuropsychological testing.
In each group, pair-wised Wilcoxon tests were performed to test for a time effect between the two available standardized neuropsychological testing for all scores and speeds that were expressed as continuous variables. Chi-squared test was used for scores expressed as categories, such as Rey’s complex figure copy classification. Furthermore, the delta score between the two standardized neuropsychological testing was compared between severe ARCI and AD groups with Mann–Whitney–Wilcoxon test. The alpha risk was set at 0.05. All statistical analyses were performed with R software version 3.2 and SPSS software version 21.0.
For patients diagnosed with severe ARCI, 12 were men (80%), the mean age was 56.6 years (SD ± 7.4), the alcohol use disorder duration mean was 22 years (± 10), the first neuropsychological assessment occurred at 2.8 (± 2.1) months of abstinence, and the second assessment was performed at 6.5 (± 2.9) months after the first one. The clinical characteristics of patients with severe ARCI are provided in Table 1. The patients in ARCI group were younger than those in AD group (72.2 years (± 8.4); p < 0.001) and the average time elapsed between the two standardized neuropsychological testing was longer in AD group [12.8 months (±2.9); p < 0.001; Table 2]. There were no differences between the groups in sex (p = 0.83) or severity of the cognitive impairment (p = 0.93).
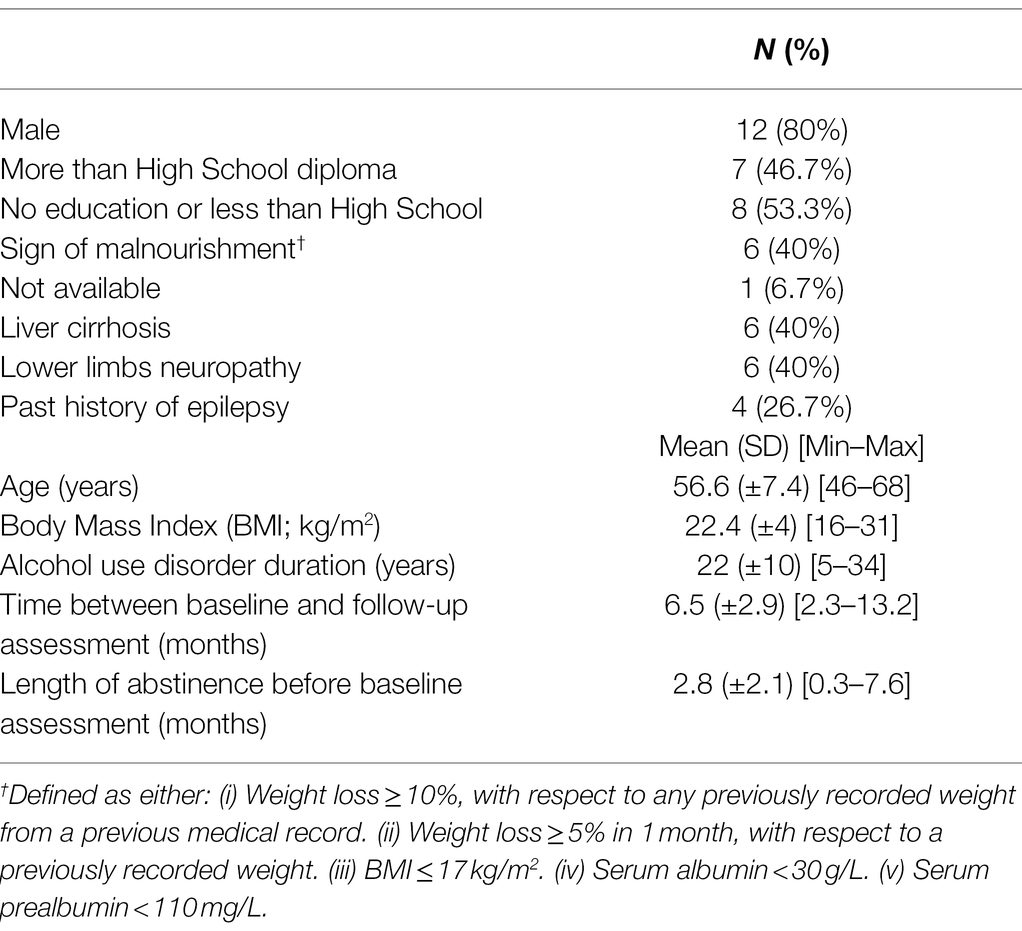
Table 1. Sociodemographic and clinical characteristics of the patients in the severe alcohol-related cognitive impairment group (N = 15) [Number (percentage) or mean (SD; minimum–maximum)].
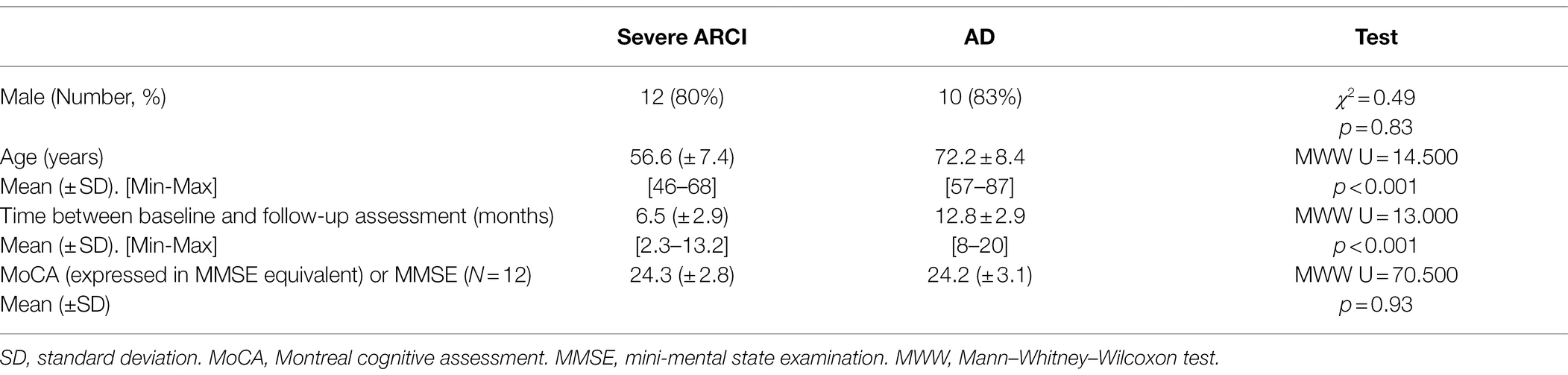
Table 2. Demographic and cognitive assessments characteristics in severe alcohol-related cognitive impairment (severe ARCI) group and Alzheimer’s disease (AD) group.
Patients with severe ARCI did significantly improve on two measures of executive functioning collected by the TMT-B test: errors (p = 0.016) and speed (p = 0.013; Table 3; Figure 1). Furthermore, it was observed a significant improvement in Rey complex figure copy classification (p = 0.049) in severe ARCI group. Indeed, 3 patients improved (construction type evolved from V to III, another one from V to IV, and one normalized from IV to I), 7 patients were stable, 1 patient worsened (from II to IV), among the 11 patients with data available on this test. No significant changes were observed in verbal fluency task, in WAIS, in FCSRT memory tests, and in Rey complex figure score and time (p > 0.05; Tables 3-5).

Table 3. Results of cognitive tests of executive functions at baseline (B) and follow-up (F) in severe Alcohol-Related Cognitive Impairment (severe ARCI) group (n = 15) and in Alzheimer’s disease group (n = 12).
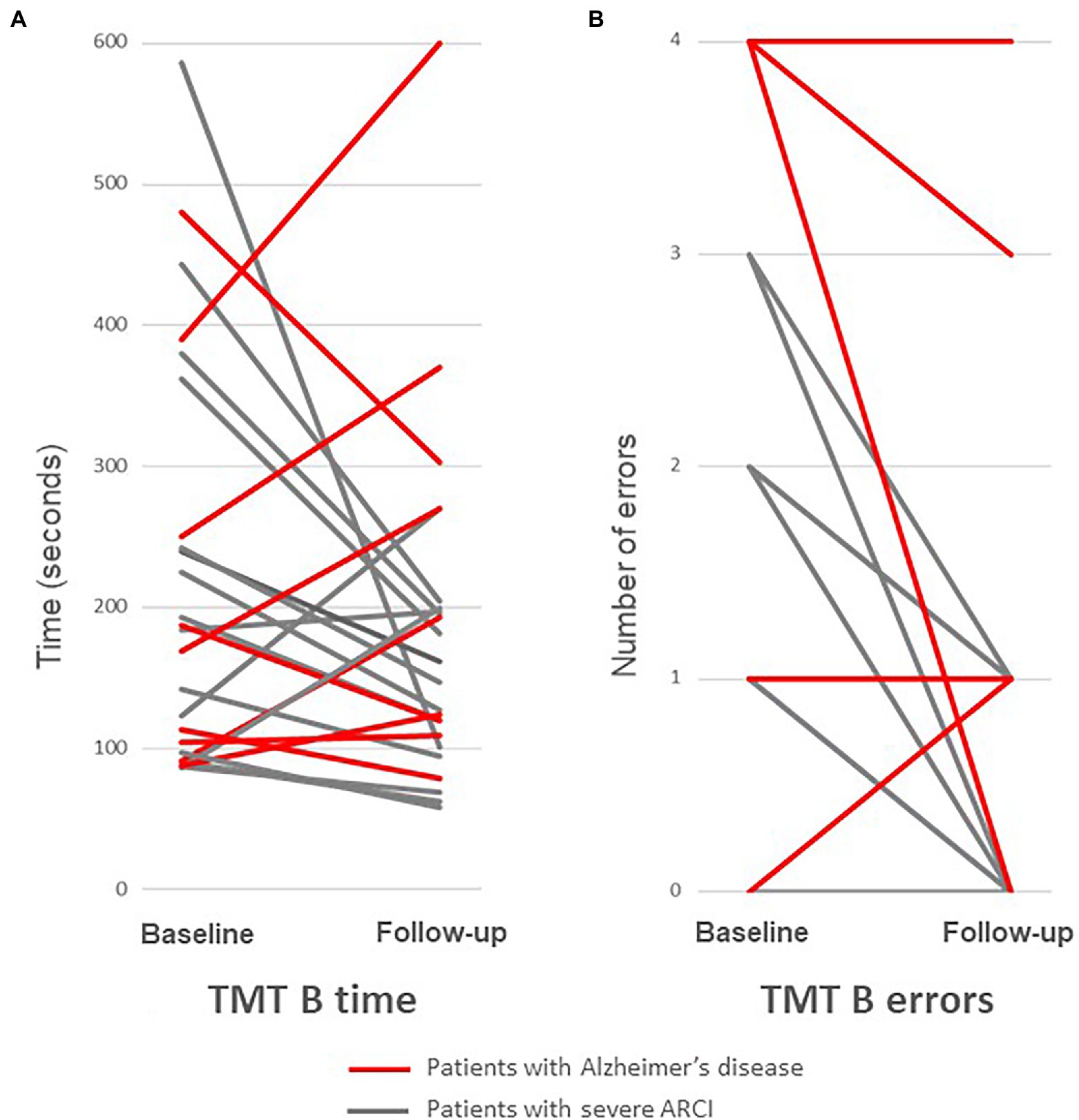
Figure 1. Change in TMT-B test between baseline and follow-up in severe Alcohol-Related Cognitive Impairment (severe ARCI) group (n = 13; in gray) and in Alzheimer’s disease group (n = 10; in red): TMT-B time (A) and TMT-B errors (B). Severe ARCI patients improve between baseline and follow-up (TMT-B time: p = 0.013 and TMT-B errors: p = 0.016, in Pair-wised Wilcoxon test), while AD patients were stable.
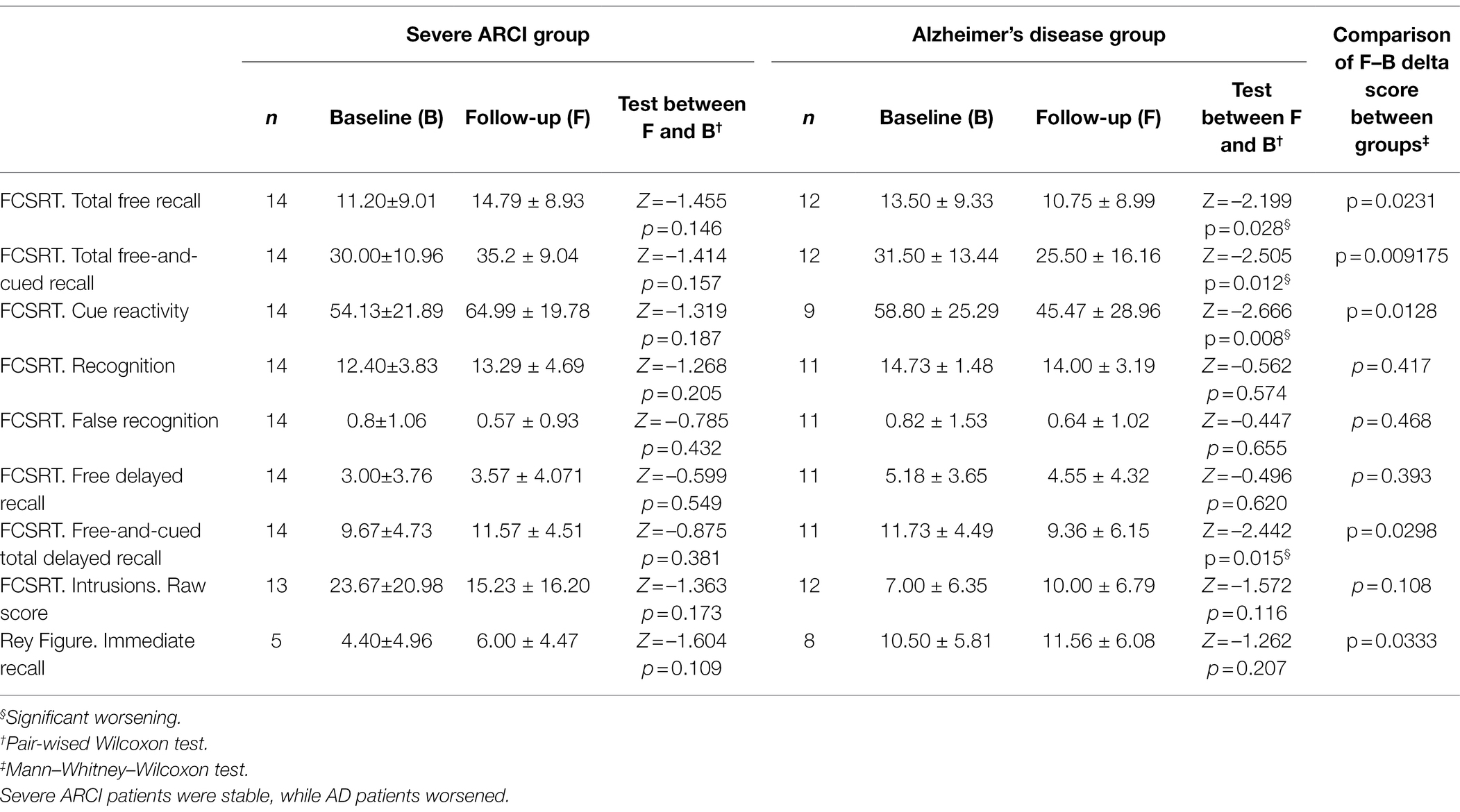
Table 4. Results of cognitive tests of memory at baseline (B) and follow-up (F) in severe Alcohol-Related Cognitive Impairment (severe ARCI) group (n = 15) and in Alzheimer’s disease group (n = 12).
In contrast, in AD patients, it was observed a significant worsening in several FCSRT memory subtests: FCSRT Total free recall (p = 0.028), Total free-and-cued recall (p = 0.012), Cue reactivity (p = 0.008), and Free-and-cued total delayed recall (p = 0.015). No significant changes were observed in the executive tests (TMT-B, verbal fluency test and WAIS) and in the Rey complex figure test (p > 0.05; Tables 3 and 4).
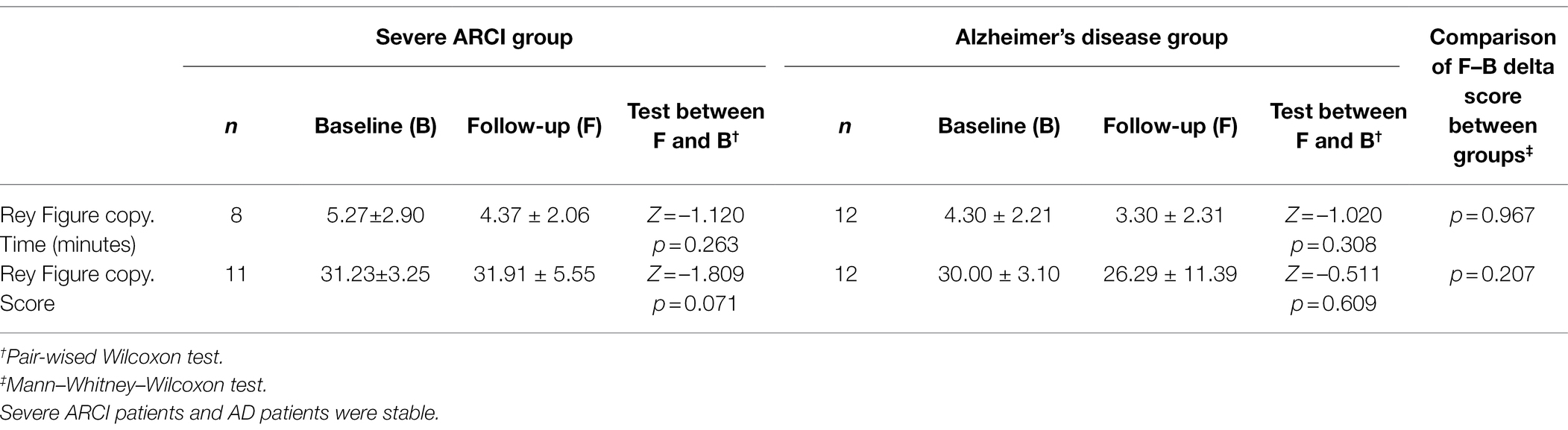
Table 5. Results of cognitive tests of visuo-spatial abilities at baseline (B) and follow-up (F) in severe Alcohol-Related Cognitive Impairment (severe ARCI) group (n = 15) and in Alzheimer’s disease group (n = 12).
Regarding the disease progression, in comparison of cognitive changes between severe ARCI and AD, it was observed a statistically difference in TMT-B time (p = 0.015), immediate recall score of Rey figure (p = 0.033), and several FCSRT memory subtests: FCSRT Total free recall (p = 0.023), Total free-and-cued recall (p = 9.2 × 10-3), Cue reactivity (p = 0.013), and Free-and-cued total delayed recall (p = 0.030; Table 3; Figure 1).
Two years later, the last clinical information available for the 15 patients with severe ARCI was that eight were still in specialized long-term rehabilitation facilities, where they will stay for several years. Three patients were in a nursing home where they will remain for their lifetime. Two patients were still hospitalized in an acute ward and were on waiting list for nursing home placement. Two patients had a clinically relevant improvement in terms of functional status that could qualify for “rehabilitation.” One of them could be discharged and go back home. Another one had been discharged and was homeless.
In this study, whose objectives were to observe the cognitive change in 15 patients with severe ARCI in comparison with 12 AD patients matched on sex and initial cognitive impairment, we observed a different disease progression between the two groups. In 15 severe ARCI patients, it was not observed a cognitive worsening of memory function at 6.5 months of follow-up, contrarily to AD patients. Moreover, in the very stringent severe ARCI group constituted to reduce clinical heterogeneity by having eliminated the others etiologies for dementia (Azuar et al., 2021) and where alcohol abstinence was documented and where continuous neuropsychological rehabilitation was delivered during a 9 month follow-up on average, it was observed a modest but statistically significant improvement on executive functions, discernible on the TMT-B test. The disease progression was different between severe ARCI and AD patients. Although most severe ARCI patients (all but two) remained severely impaired and could not be discharged, these results could demonstrate at least the absence of degenerative disease progression of the cognitive deficit, and even sensitivity to time and/or alcohol abstinence maintenance and/or cognitive rehabilitation programs.
Regarding the time needed to observe a cognitive improvement, in patients with alcohol use disorder and moderate cognitive impairment, screened immediately after alcohol cessation, Stravo et al. showed that moderate cognitive impairment remained stable during the first year of alcohol abstinence (Stavro et al., 2013). On the other hand, Pitel et al. recommended a 6 month abstinence period before retest to observe potential improvement (Pitel et al., 2009). In patients with Wernicke–Korsakoff syndrome, the improvement in executive function observed by Fujiwara et al. occurred after 2 years in specific remediation, in patients previously abstinent for several years (Fujiwara et al., 2008). Maillard et al. chose a 1-year period before the retest (Maillard et al., 2021). Compared to the latter two, the time of follow-up in this study, with a second assessment at 6.5 month after baseline, may have been too short to capture the comprehensive effect of both abstinence and rehabilitation. Nevertheless, these results show a discernible improvement in TMT-B test after this period, underlining the relevance of performing follow-up assessments as early as 6 months. TMT-B test could be a useful recovery marker, which had not been studied in the two previous studies (Fujiwara et al., 2008; Maillard et al., 2021). Of note, in populations of subjects without AUD and under the acute effect of alcohol with a blood alcohol concentration ≤ 1 mg/ml, Jongen et al. showed the absence of alteration of the TMT-B results (Jongen et al., 2016). This fact reinforces the specificity of TMT-B as a reversible marker of severe alcohol-induced executive function impairment rather than a marker of acute alcohol intoxication on cognitive abilities.
Strengths of this study were to study a hard to reach, relatively homogeneous population by carefully ruling out differential diagnoses, and the use of standardized neuropsychological testing allowed comparison, even with patients visiting a specialized AD center. Lastly, because patients with severe ARCI were maintained in specialized settings dedicated to cognitive rehabilitation belonging to the ResAlCog care network, it is possible to confidently state that the 15 patients described here maintained alcohol abstinence over time.
However, there were several limitations. First, there is not control group with healthy subjects to estimate effects of repeated testing or age-related decrease. Second, there is not control group with severe ARCI patients but without cognitive rehabilitation. Third, the number of patients is low although comparable to the only two previous published studies that we could identify. Fourth, some cognitive functions were not evaluated. For example, inhibition, evaluated with the Stroop test, was not available. Fourth, there is a possible reliability bias in data recorded, for example, regarding alcohol use in patients visiting the AD center. Fifth, the length between the two neuropsychological testing was not strictly comparable, between severe ARCI and AD patients. Lastly, we are not able to reliably associate the improvement in the result of this executive function test and the improvement observed for some patients regarding autonomy in everyday tasks.
This study opens three development perspectives. In terms of conceptualization this study clearly supports that even severely affected, ARCI patients have a different disease evolution pattern than patients affected by a neurodegenerative disorder. In terms of research on ARCI, future studies’ design should include multimodal prospective assessments of executive functions, including validated tests but also scales of autonomy in everyday tasks, above the classical various memory tests. In terms of care provided for those patients, as an improvement in the executive tests is observable as soon as 6 months, residential setting combining alcohol-free environment and specific cognitive rehabilitation programs should be proposed as soon as the diagnosis is confirmed for at least 6 months.
This study provides a new long-term course description of patients with severe ARCI who received optimal medical diagnosis, up-to-date cognitive rehabilitation, in a care setting where alcohol abstinence can be monitored. We observed an average partial improvement on executive functions, and two patients out of 15 had a clinically relevant functional improvement. Conversely to patients with AD selected to have a comparable initial cognitive impairment, no neuropsychological worsening was shown in severe ARCI patients, especially on memory tests. Among executive functions studied, flexibility and visuo-spatial planning improved. Studies based on larger samples followed for a longer period of time to confirm these data may be helpful.
The datasets presented in this article are not readily available because it is the property of the ResAlCog network’s structures. Requests to access the datasets should be directed to FQ, ZnJhbmNrLnF1ZXN0ZWxAYXBocC5mcg==.
This study was conducted in adherence to the guidelines of Declaration of Helsinki and following French laws on biomedical research (Loi Jardé 2014, décrets d’application 2017). Our hospital has obtained a specific authorisation for the analysis of anonymized data collected during routine care, delivered by the French national board for information systems and freedom (Commission Nationale Informatique et Liberté; Number 2017–013). This chart review study design was approved by an internal ethics committee. Patients and their representatives were informed and could object to the use of their anonymized routine health care data for research purposes. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
FQ, FV, and EC designed the study. TB, EC, and FQ collected the data. VC-D, TB, and FV worked on data analyses. VC-D, TB, and FV drafted the manuscript, with support of EC and FQ. FQ and FV supervised the study. All authors contributed to the article and approved the submitted version.
FV had congress fees paid by CAMURUS AB, RECORDATI, and ACCORD Pharmaceutical. FV gave a single lecture for RECORDATI (2020) and for CAMURUS AB (2022) and served in advisory boards for CAMURUS AB (2019, 2022), and ACCORD HEALTH CARE (2021). All payments were made to a research entity and not directly to FV. CP is a member of the International Advisory Boards of Lilly, is a consultant with Fujiribio, Alzohis, Neuroimmune, and Gilead, and is involved as an investigator in several clinical trials for Roche, Esai, Lilly, Biogen, Astra-Zeneca, Lundbeck, and Neuroimmune, outside the submitted work. EC is involved as an investigator in several clinical trials for Roche, Esai, and Biogen, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors wish to thank all specialized structures of the care network ResAlCog: Hôpital Fernand Widal, Paris (Questel), Hôpital Gouin, Clichy (Levy, Dufour), Clinique du Parc, Saint-Ouen-l’Aumône (Guibe, Arfaoui-Geffroy), Clinique des Epinettes, Paris (Lecallier, Grosdidier), Hôpital René Muret, Sevran (Polomeni), Maison d’Accueil Spécialisée—Unité Serge Korsakoff, Villeneuve-la-Garenne (Michaud).
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Azuar, J., Bouaziz-Amar, E., Cognat, E., Dumurgier, J., Clergue-Duval, V., Barré, T., et al. (2021). Cerebrospinal fluid biomarkers in patients with alcohol use disorder and persistent cognitive impairment. Alcohol. Clin. Exp. Res. 45, 561–565. doi: 10.1111/acer.14554
Bates, M. E., Buckman, J. F., and Nguyen, T. T. (2013). A role for cognitive rehabilitation in increasing the effectiveness of treatment for alcohol use disorders. Neuropsychol. Rev. 23, 27–47. doi: 10.1007/s11065-013-9228-3
Caine, D., Halliday, G. M., Kril, J. J., and Harper, C. G. (1997). Operational criteria for the classification of chronic alcoholics: identification of Wernicke’s encephalopathy. J. Neurol. Neurosurg. Psychiatry 62, 51–60. doi: 10.1136/jnnp.62.1.51
Cardebat, D., Doyon, B., Puel, M., Goulet, P., and Joanette, Y. (1990). Evocation lexicale formelle et sémantique chez des sujets normaux. Performances et dynamiques de production en fonction du sexe, de l’âge et du niveau d’étude [Formal and semantic lexical evocation in normal subjects. Performance and dynamics of production as a function of sex, age and educational level]. Acta Neurol. Belg. 90, 207–217.
Folstein, M. F., Folstein, S. E., and McHugh, P. R. (1975). “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198. doi: 10.1016/0022-3956(75)90026-6
Fujiwara, E., Brand, M., Borsutzky, S., Steingass, H.-P., and Markowitsch, H. J. (2008). Cognitive performance of detoxified alcoholic Korsakoff syndrome patients remains stable over two years. J. Clin. Exp. Neuropsychol. 30, 576–587. doi: 10.1080/13803390701557271
Ihara, H., Berrios, G., and London, M. (2000). Group and case study of the dysexecutive syndrome in alcoholism without amnesia. J. Neurol. Neurosurg. Psychiatry 68, 731–737. doi: 10.1136/jnnp.68.6.731
Jongen, S., Vuurman, E. F. P. M., Ramaekers, J. G., and Vermeeren, A. (2016). The sensitivity of laboratory tests assessing driving related skills to dose-related impairment of alcohol: a literature review. Accid. Anal. Prev. 89, 31–48. doi: 10.1016/j.aap.2016.01.001
Kashima, H., Kato, M., Yoshimasu, H., and Muramatsu, T. (1999). Current trends in cognitive rehabilitation for memory disorders. Keio J. Med. 48, 79–86. doi: 10.2302/kjm.48.79
Kopelman, M. D., Thomson, A. D., Guerrini, I., and Marshall, E. J. (2009). The Korsakoff syndrome: clinical aspects, psychology and treatment. Alcohol Alcohol. 44, 148–154. doi: 10.1093/alcalc/agn118
Le Berre, A.-P., Fama, R., and Sullivan, E. V. (2017). Executive functions, memory, and social cognitive deficits and recovery in chronic alcoholism: a critical review to inform future research. Alcohol. Clin. Exp. Res. 41, 1432–1443. doi: 10.1111/acer.13431
Maillard, A., Laniepce, A., Cabé, N., Boudehent, C., Chételat, G., Urso, L., et al. (2021). Temporal cognitive and brain changes in Korsakoff syndrome. Neurology 96, e1987–e1998. doi: 10.1212/WNL.0000000000011749
Maillard, A., Poussier, H., Boudehent, C., Lannuzel, C., Vicente, A., Vabret, F., et al. (2020). Short-term neuropsychological recovery in alcohol use disorder: a retrospective clinical study. Addict. Behav. 105:106350. doi: 10.1016/j.addbeh.2020.106350
McKinlay, A. (2011). “Rey complex figure test,” in Encyclopedia of Child Behavior and Development. eds. S. Goldstein and J. Naglieri (Boston, MA: Springer).
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Oudman, E., Nijboer, T. C. W., Postma, A., Wijnia, J. W., and Van der Stigchel, S. (2015). Procedural learning and memory rehabilitation in Korsakoff’s syndrome - a review of the literature. Neuropsychol. Rev. 25, 134–148. doi: 10.1007/s11065-015-9288-7
Pitel, A. L., Beaunieux, H., Witkowski, T., Vabret, F., de la Sayette, V., Viader, F., et al. (2008). Episodic and working memory deficits in alcoholic Korsakoff patients: the continuity theory revisited. Alcohol. Clin. Exp. Res. 32, 1229–1241. doi: 10.1111/j.1530-0277.2008.00677.x
Pitel, A. L., Rivier, J., Beaunieux, H., Vabret, F., Desgranges, B., and Eustache, F. (2009). Changes in the episodic memory and executive functions of abstinent and relapsed alcoholics over a 6-month period. Alcohol. Clin. Exp. Res. 33, 490–498. doi: 10.1111/j.1530-0277.2008.00859.x
Pitel, A.-L., Zahr, N. M., Jackson, K., Sassoon, S. A., Rosenbloom, M. J., Pfefferbaum, A., et al. (2011). Signs of preclinical Wernicke’s encephalopathy and thiamine levels as predictors of neuropsychological deficits in alcoholism without Korsakoff’s syndrome. Neuropsychopharmacology 36, 580–588. doi: 10.1038/npp.2010.189
Reitan, R. M. (1955). The relation of the trail making test to organic brain damage. J. Consult. Psychol. 19, 393–394. doi: 10.1037/h0044509
Rupp, C. I., Kemmler, G., Kurz, M., Hinterhuber, H., and Fleischhacker, W. W. (2012). Cognitive remediation therapy during treatment for alcohol dependence. J. Stud. Alcohol Drugs 73, 625–634. doi: 10.15288/jsad.2012.73.625
Sachdev, P. S., Blacker, D., Blazer, D. G., Ganguli, M., Jeste, D. V., Paulsen, J. S., et al. (2014). Classifying neurocognitive disorders: the DSM-5 approach. Nat. Rev. Neurol. 10, 634–642. doi: 10.1038/nrneurol.2014.181
Saklofske, D., and Schoenberg, M. (2011). “Wechsler adult intelligence scale (all versions),” in Encyclopedia of Clinical Neuropsychology. eds. J. Kreutzer, J. DeLuca, and B. Caplan (New York, NY: Springer).
Schwarzinger, M., Pollock, B. G., Hasan, O. S. M., Dufouil, C., and Rehm, J. (2018). Contribution of alcohol use disorders to the burden of dementia in France 2008–13: a nationwide retrospective cohort study. Lancet Public Health 3, e124–e132. doi: 10.1016/S2468-2667(18)30022-7
Stavro, K., Pelletier, J., and Potvin, S. (2013). Widespread and sustained cognitive deficits in alcoholism: a meta-analysis. Addict. Biol. 18, 203–213. doi: 10.1111/j.1369-1600.2011.00418.x
Svanberg, J., and Evans, J. J. (2013). Neuropsychological rehabilitation in alcohol-related brain damage: a systematic review. Alcohol Alcohol. 48, 704–711. doi: 10.1093/alcalc/agt131
Trzepacz, P. T., Hochstetler, H., Wang, S., Walker, B., and Saykin, A. J., Alzheimer’s Disease Neuroimaging Initiative (2015). Relationship between the Montreal cognitive assessment and Mini-mental state examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 15:107. doi: 10.1186/s12877-015-0103-3
Van der Linden, M., Coyette, F., Kalafat, M., Calicis, F., Wyns, C., and Adam, S. (2004). “L’épreuve de rappel libre/rappel indicé à 16 items (RL/RI-16) [The 16-item free recall/indexed recall test (RL/RI-16)],” in L’évaluation des troubles de la mémoire: présentation de quatre tests de mémoire épisodique avec leur étalonnage Neuropsychologie, ed. M. Van der Linden. (Marseille: Solal), 25–47.
Keywords: alcohol-related cognitive impairment, alcohol brain damage, alcohol use disorder, Alzheimer’s disease, cognitive impairment, disease progression
Citation: Clergue-Duval V, Barré T, Cognat E, Brichet A-L, Géraud C, Azuar J, Michaud P, Lecallier D, Arfaoui-Geffroy S, Hispard E, Paquet C, Bellivier F, Questel F, Vorspan F and all members of the ResAlCog care network (2022) Patients With Severe Alcohol-Related Cognitive Impairment Improve in Flexibility When Abstinence Is Maintained: A Comparative Study With Alzheimer’s Disease. Front. Psychol. 13:936639. doi: 10.3389/fpsyg.2022.936639
Edited by:
Fabrizio Stasolla, Giustino Fortunato University, ItalyReviewed by:
Luigi Tinella, University of Bari Aldo Moro, ItalyCopyright © 2022 Clergue-Duval, Barré, Cognat, Brichet, Géraud, Azuar, Michaud, Lecallier, Arfaoui-Geffroy, Hispard, Paquet, Bellivier, Questel, Vorspan and ResAlCog care network. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Virgile Clergue-Duval, dmlyZ2lsZS5jbGVyZ3VlLWR1dmFsQGFwaHAuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.