 Raquel Guiomar1*
Raquel Guiomar1* Inês A. Trindade1
Inês A. Trindade1 Sérgio A. Carvalho1,2
Sérgio A. Carvalho1,2 Paulo Menezes3,4
Paulo Menezes3,4 Bruno Patrão3
Bruno Patrão3 Maria Rita Nogueira3
Maria Rita Nogueira3 Teresa Lapa5,6
Teresa Lapa5,6 Joana Duarte7José Pinto-Gouveia1Paula Castilho1
Joana Duarte7José Pinto-Gouveia1Paula Castilho1- 1University of Coimbra, Center for Research in Neuropsychology and Cognitive Behavioral Intervention, Faculty of Psychology and Educational Sciences, Coimbra, Portugal
- 2Digital Human-Environment Interaction Lab, School of Psychology and Life Sciences, Lusófona University, Lisbon, Portugal
- 3University of Coimbra, Institute of Systems and Robotics, Coimbra, Portugal
- 4University of Coimbra, Department of Electrical and Computer Engineering, Coimbra, Portugal
- 5Pain Unit, Coimbra Hospital and University Centre, Coimbra, Portugal
- 6Faculty of Health Sciences, University of Beira Interior, Covilhã, Portugal
- 7Department of Psychology, Lund University, Lund, Sweden
Background: This pilot study aims to test the usability of the iACTwithPain platform, an online ACT-based intervention for people with chronic pain, to obtain information on which intervention and usability aspects need improvement and on expected retention rates.
Methods: Seventy-three Portuguese women with chronic pain were invited to complete the first three sessions of the iACTwithPain intervention assess their quality, usefulness and the platform’s usability. Twenty-one accepted the invitation. Additionally, eight healthcare professionals working with chronic medical conditions assessed the platform and the intervention from a practitioner’s point of view.
Results: This study presented a considerable attrition rate (71.43%) among chronic pain participants, with six completers. There were no significant differences in demographic or clinical variables between dropouts and completers except for completed education (participants who dropped out presented less education than completers). Reasons for dropout were related to difficult personal events occurring during the time of the intervention, lack of time, or having forgotten. There seemed to be an overall satisfaction with both the intervention, its contents and form of presentation of information, and the platform, concerning its design, appearance, and usability. Real image videos were preferred over animations or audio by chronic pain participants. Healthcare professionals emphasized the appealing and dynamic aspects of the animation format.
Conclusion: This study informs the ongoing improvement of the iACTwithPain platform and provides valuable information on aspects researchers should consider while developing online psychological interventions for chronic pain. Further implications are discussed.
Introduction
Chronic pain can be defined as persistent pain lasting more than 3 months, has a prevalence of approximately 20% in adults (Elliott et al., 1999), can have a detrimental impact in mobility and quality of life (Smith et al., 2001), and productivity (Dorner et al., 2016). Chronic pain is associated with high economic burden, and is considered as one of the most expensive long-term health conditions in industrialized countries (Bernfort et al., 2015; Groenewald and Palermo, 2015; Mayer et al., 2019).
Acceptance of pain is considered an important factor for a successful adaptation to chronic pain, linked to less depression, pain-related anxiety, and disability (McCracken and Eccleston, 2003). These findings have supported the application of acceptance-based therapies, such as Acceptance and Commitment Therapy [ACT; Hayes et al. (2012)], to this population. ACT is an empirically validated psychological approach for chronic pain (APA Presidential Task Force on Evidence-Based Practice, 2006) that promotes acceptance and engagement with values-guided behavior despite chronic pain symptoms (Vowles and McCracken, 2008). The efficacy of ACT for chronic pain has been demonstrated in a meta-analysis by Veehof et al. (2011), and in a broader review including both acceptance and mindfulness-based interventions (Veehof et al., 2016). At the same time, the pertinence of promoting self-compassion [i.e., the ability to be sensitive to personal suffering and being motivated to kindly alleviate it; (Neff, 2003; Gilbert, 2009)] in chronic pain has been highlighted due to its protective role against depressive symptomatology (Carvalho et al., 2018) and the positive effects compassion-focused interventions have presented in this population (Gooding et al., 2020). The combination of ACT and compassion for chronic pain was recently implemented in a pilot test with promising results (Carvalho et al., 2021a).
In recent years, online-delivered interventions have generated increased interest due to their accessibility, flexibility and cost-effectiveness (Bergmo, 2015). In particular, online-based ACT has been proved to be efficacious for chronic pain in a recent meta-analysis. Online-ACT was greater than control conditions in reducing pain interference, pain intensity, depression, and anxiety, and in increasing mindfulness, and psychological flexibility (Trindade et al., 2021a). For these reasons, and additionally considering the advantages of online interventions to improve health-related outcomes (Bergmo, 2015), and for chronic pain in particular (Trindade et al., 2021a), the iACTwithPain intervention platform was developed by the authors of this paper (iACTwithPain research team). iACTwithPain is an ACT- and Compassion-based intervention tailored explicitly to chronic pain. It comprises eight sessions to be completed on an online platform throughout 8 weeks (1 session per week). The efficacy of the iACTwithPain intervention in improving chronic pain impact and related health and quality of life markers will be tested in full in a randomized controlled trial (Carvalho et al., 2021b). It is the aim of the current study to pilot test the usability of the platform by examining the feedback of clinicians and chronic pain patients of first three sessions in order to obtain information on which intervention and usability aspects need improvement, and on expected retention rates. Given our team’s combined expertise in psychology, design and engineering, we hypothesize qualitative feedback from participants reflecting pertinent content for patients with chronic pain, and an online platform that is intuitive, engaging and esthetically pleasing. We additionally expect high usability scores, as measured by the System Usability Scale [SUS; Martins et al. (2015)], relating to participants’ use of the platform.
Methods
Ethical Approval and Data Safety
This study was approved by Ethical Committee of the Faculty of Psychology and Educational Sciences of the University of Coimbra (on 28/11/2019), and was conducted in accordance with the ethical standards in the 1964 Declaration of Helsinki and its later amendments. All collected data will be stored (for 5 years) using high standard security mechanisms, and thus ensuring confidentiality. Data will be in anonymized and can only be assessed by the research team.
Sample Size Calculation
According to Faulkner (2003), on average, a sample of five participants can detect 85% of the usability problems. Therefore, we aim to have a sample of at least 5 in each group (participants with chronic pain and health professionals). Assuming a conservative dropout rate of 83% (Bangor et al., 2009) for the clinical sample, at least 30 participants should be invited to enroll in the study.
Procedures
The study’s chronological order was as follows: (1) participants recruitment (presentation of the study and informed consent); (2) during the following 2 weeks participants tested the iACTwithPain platform; (3) in the third week the usability and quality assessment questionnaire was administered; (4) participants who dropped out from the study were contacted to fill in a questionnaire (reasons for dropping out).
Seventy-three Portuguese women with chronic pain, enrolled in a different study who had demonstrated interest in taking part in the current one, were invited to complete the first three sessions of the iACTwithPain intervention and assess their quality and usefulness, as well as to assess the platform’s usability. Inclusion criteria were: age between 18 and 65 years; diagnosis of chronic pain; internet access; and proficiency in Portuguese. Exclusion criteria were: not providing informed consent; or pain due to malignancy, trauma, or surgery. Twenty-one accepted the invitation to participate, signed an informed consent, and were enrolled in the study. Participants with chronic pain that did not complete the three sessions were asked to fill out a questionnaire on the reasons for attrition.
Additionally, nine healthcare professionals working with chronic medical conditions (four psychologists, four physicians, and one nurse) were also invited to assess the platform and the intervention from a practitioner’s point of view. Of these, eight signed an informed consent before the start of the study and were enrolled in the study.
The iACTwithPain Platform
The iACTwithPain intervention was designed based on the psychological flexibility model (Vowles and McCracken, 2008; Trindade et al., 2020) and compassion-focused interventions applied to chronic pain (Carvalho et al., 2018). The psychologists’ members of the iACTwithPain team have expertise in developing and efficacy testing ACT and compassion-based interventions for chronic conditions such as chronic pain (Carvalho et al., 2021b), cancer (Trindade et al., 2020), inflammatory bowel disease (Trindade et al., 2021b), and psychiatric disorders (Duarte et al., 2017). Moreover, the team’s knowledge of the psychological impact of chronic pain and the underlying psychological processes (Carvalho et al., 2018, 2019, 2021c) were taken into consideration. During iACTwithPain development, the principles of ACT and compassion-based interventions were strictly followed to ensure pertinent and rigorous therapeutic sessions. As described in the RCT protocol (Carvalho et al., 2021b) treatment integrity guidelines for ACT (Plumb and Vilardaga, 2010) were followed and included: (a) training in ACT and compassion focused therapy models, ensuring that the therapists fully grasp the concepts and principles of the interventions and have previous competence/experience in their application; (b) the content of the sessions are ACT-consistent (for example focus on the function rather than the content); and the known processes of change of ACT and compassion were followed during the development of the intervention.
Participants will be randomly assigned to two experimental arms: and ACT-only intervention or an ACT and compassion-focused intervention. All sessions will be the same except for sessions five and six. The ACT and compassion-focused group will be exposed to compassion themes and exercises (e.g., what is compassion, developing compassion toward the self and others, obstacles to compassion). The ACT-only group will reinforce previous topics (e.g., willingness, acceptance, defusion, and observing self) without introducing new information or practices. The ACT intervention will include the following core themes: (a) Awareness of internal experiences (mindfulness; self-as-context); (b) Openness to experience difficult experiences (acceptance of pain: willingness toward thoughts, emotions and physical sensations; and cognitive defusion); (c) Engagement with valued action (values clarification and commitment to meaningful actions); (d) Self-Compassion (promoting self-kindness in times of difficulty; for the ACT and compassion-focused group only). Sessions will comprise video-animations (with videoscribes and therapists’ avatars), real-image videos, texts, and audios guiding meditative practices. iACTwithPain is a self-paced intervention and therefore the participant can decide when to login and complete each session. Nevertheless, the intervention was designed so that sessions are completed weekly (one session per week, over 8 weeks). Each new session will become available in the platform every Monday. Emails notifying the participants that a new session is available will be sent weekly.
Session 1 is completed immediately after session 0, and the following sessions are then completed once per week. A brief introductory session (session 0) will welcome participants to the intervention and introduce the platform. Participants are asked to practice between-session mindfulness and/or compassion-based meditative exercises as often as possible. In this usability study, participants were asked to complete the introductory session (session zero), session one and two. Session one focuses on psychoeducation about chronic pain, promotion of creative hopelessness, introduction to mindfulness practice, and mindfulness of breathing practice. Session two focuses on the usefulness of mindfulness to manage suffering, promotion of mindfulness practice, and body scan practice (see Table 1 for more detailed information). Mindfulness exercises throughout the intervention focus on a non-judgmental, open, and accepting attitude toward the present moment. Visual examples from these sessions are presented in Figure 1.

Table 1. Structure and contents of session 0, 1, and 2.
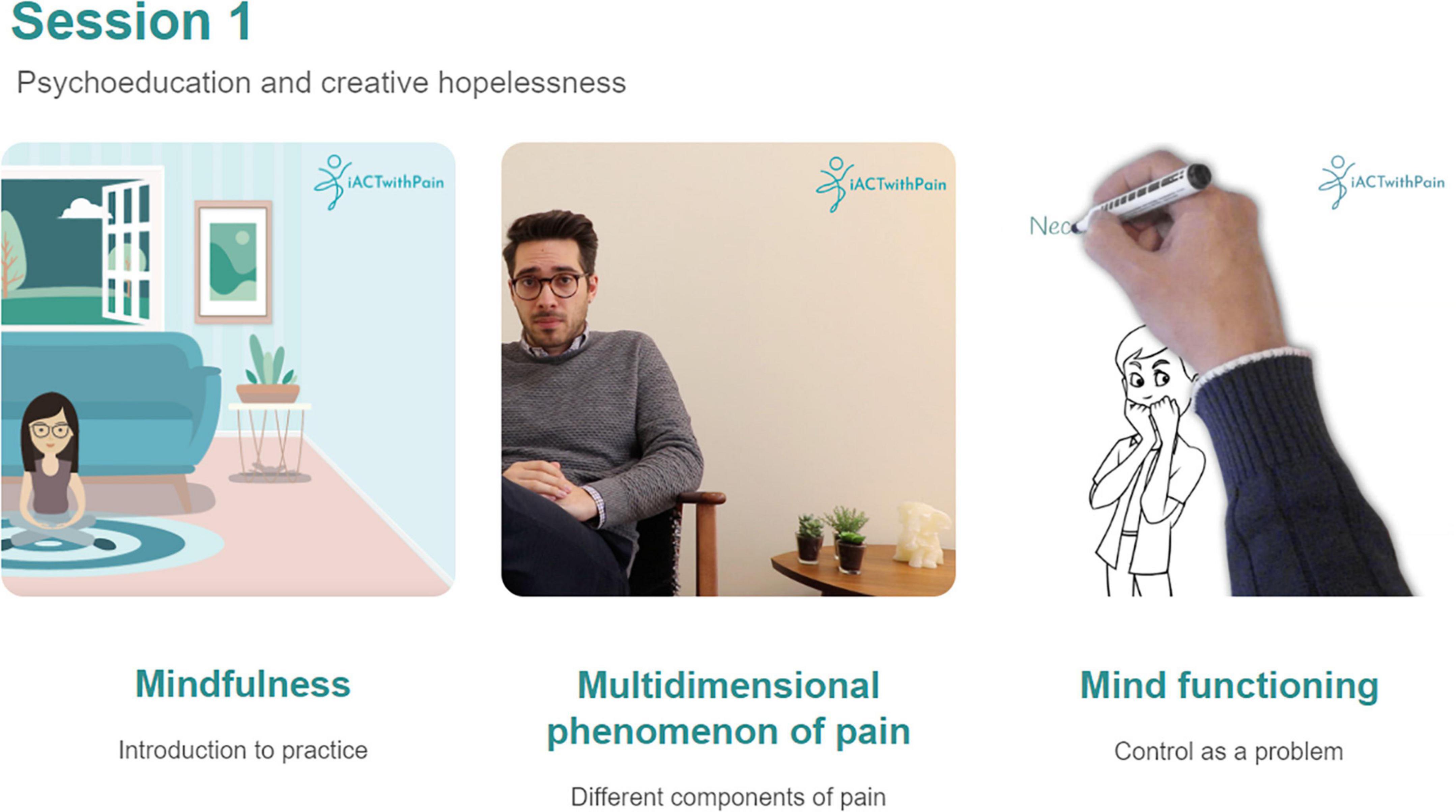
Figure 1. Example of session 1 contents depicting the three types of videos (left to right: video-animation with a therapist avatar, real-image video with a therapist, and videoscribe animated video).
Measures
Primary Outcome
Both groups of participants (patients and professionals) were asked to complete the SUS [(Brooke, 1996); original validation (Bangor et al., 2008); portuguese validation (Martins et al., 2015)]. This scale is robust and widely used to evaluate the usability of products and user interfaces (Bangor et al., 2009). The European Portuguese validation is equivalent to the original version in terms of semantics and content, and presented good psychometric properties e.g., high convergent validity and satisfactory inter-rater percentage of agreement (Martins et al., 2015). It provides a single reference score for participants’ view of the usability of a product or service. It comprises ten items rated on a 5-point Likert scale (1: Strongly Disagree; 5: Strongly Agree) and has been shown to present adequate psychometric properties (Bangor et al., 2008). The SUS items were coded by subtracting 1 from the odd items’ score, subtracting even items’ score from 5 (correction for the reverse scored items), and multiplying the re-coded values by 2,5 (Martins et al., 2015). This results in new scores ranging from 0 to 100, where higher scores indicate better usability. According to the adjective ratings proposed by Bangor et al. (2008), SUS scores from 0 to 25 are “Worst imaginable,” 25–39 “Poor,” 39–52 “Ok,” 52–73 “Good,” 73–85 “Excellent,” and 85–100 are “Best imaginable” (Bangor et al., 2008).
Secondary Outcomes
Participants with chronic pain and healthcare professionals were asked to complete a set of self-report questions regarding the quality of the intervention (e.g., content clarity, pertinence of the intervention themes, platform design and organization, individual session quality), session duration, and preferences on type of presentation format (e.g., video, audio). These questions were developed by the research team to tailor to the specific platform characteristics that this study aims to assess. The platform kept track of participant engagement concerning the number of logins in the platform and engagement with mindfulness practice audios or videos.
Statistical Analyses
All analysis were performed on SPSS (Statistical Package for the Social Sciences), version 25 (IBM Corp., Armonk, NY, United States). Descriptive and frequency analyses were conducted to analyze participants’ evaluations of the platform/intervention, as well as engagement with the platform. Mann–Whitney U and Fisher’s exact test were conducted to analyze differences between groups of participants (e.g., completers, dropouts). The retention rate was computed as the proportion of participants that completed the three sessions.
Results
In this study we aimed to pilot test the usability of the iACTwithPain platform, in what concerns our primary outcome – usability scores; and secondary outcomes – qualitative assessment, engagement, and retention rate.
Primary Outcome – Usability
Sample of Participants With Chronic Pain
Regarding usability scores (SUS), on average, iACTwithPain’s platform was rated as excellent (N = 5, M = 76.50, SD = 16.83). Two participants rated it as good (M = 58.75, SD = 1.77), one rated it as excellent (82.5), and two rated it as best imaginable (M = 91.25, SD = 5.30).
Sample of Healthcare Professionals
On average, the iACTwithPain’s platform usability (SUS) was rated by healthcare professionals as excellent (N = 5, M = 84.50, SD = 7.79). Two participants rated it as excellent (M = 80.00; SD = 2.50), and three as best imaginable (M = 91.25; SD = 8.84).
Secondary Outcomes – Qualitative Assessment, Engagement, and Retention Rate
Qualitative Assessment of the iACTwithPain Platform
Sample of Participants With Chronic Pain
Of the six completers, three preferred real image video format, two preferred animations, and one preferred sole audios. Table 2 presents participants’ feedback on each of these formats. Written feedback highlighted advantages to the real image video format, which was overall described as attractive and motivating to practice. One comment indicated that more investment in the background of the real-time videos should be made and that these videos could include animations. Described advantages for the audio format were accessibility and having less distractions. Animation videos were described as interesting and having an attractive and simple design.
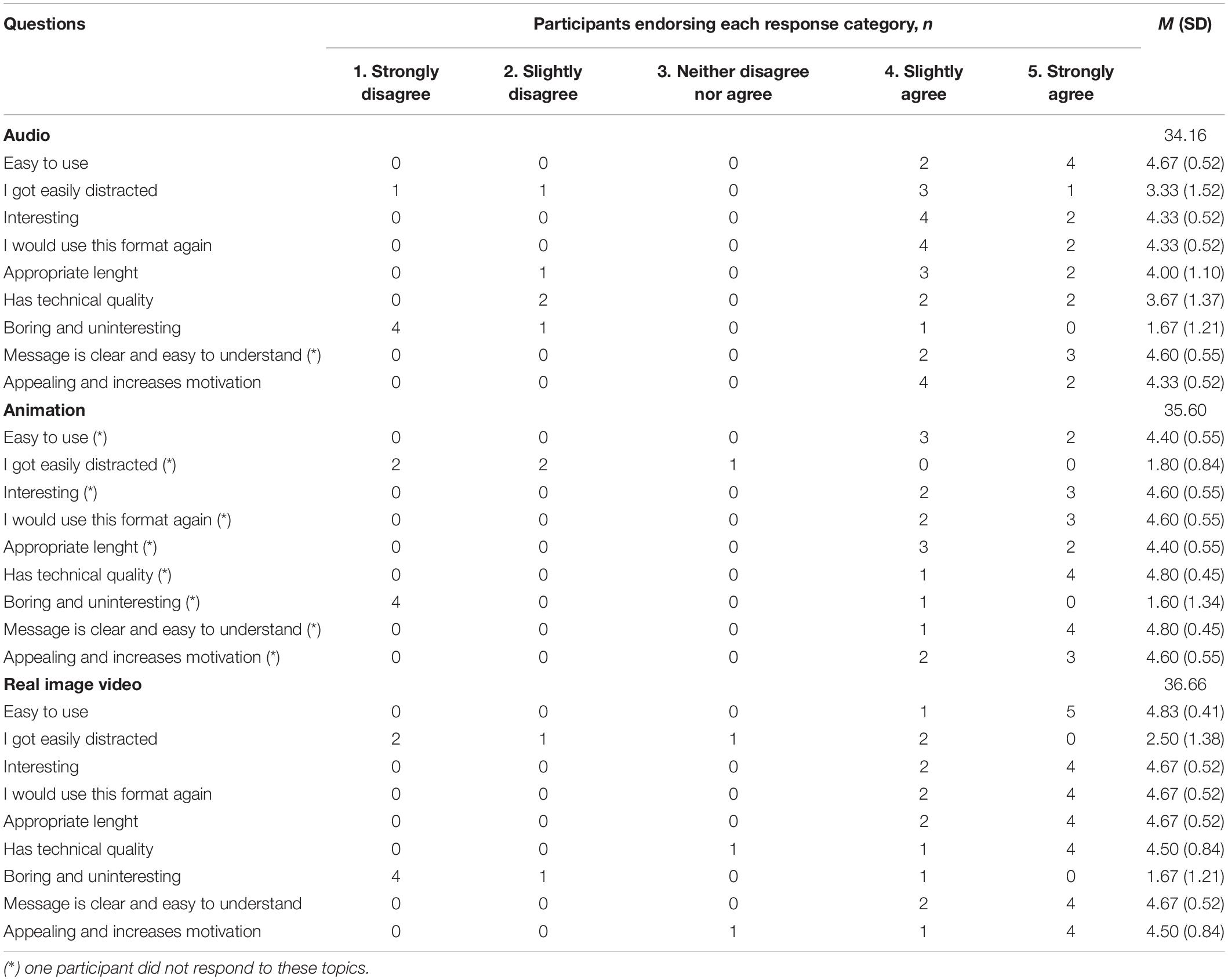
Table 2. Participants’ feedback on the different kinds of content format (n = 6).
Concerning other aspects of the intervention and platform, participants generally rated positively their satisfaction (on a scale from 0, no satisfaction, and 10, extremely satisfied) with the platform’s design (M = 7.50; SD = 2.01), color pattern (M = 8.33; SD = 1.37), and attractiveness (M = 7.67; SD = 1.75).
The topics covered by the two assessed sessions were very positively evaluated (M = 8.67; SD = 1.03). The topics found most useful to participants (n = 4) were psychoeducation about pain (n = 1), mindfulness of breathing (n = 1), and body scan practice (n = 2). Participants also provided positive answers (on a scale from 0, no satisfaction, and 10, extremely satisfied) regarding their interest in continuing the intervention (M = 7.33; SD = 3.20). Furthermore, four participants provided feedback on what they believe could be changed to improve these three sessions. One participant indicated that the sessions seemed to cover all important aspects. Another referred to longer intervals without instructions in the mindfulness practices, and two stated that they felt that strategies to reduce pain should be included in the intervention.
Sample of Healthcare Professionals
The healthcare professionals group seemed to prefer the animation (n = 3) and real image video (n = 2) formats. Real image videos (M = 34.20; SD = 2.68) and animations (M = 33.60; SD = 1.67) were overall more positively evaluated than audios (M = 27.80; SD = 3.49). Overall, written feedback about the audios indicated that this format is easy to use and accessible, although not particularly appealing or stimulating. Animations were described as attractive, and appealing, but impersonal. Real image videos were described as providing a connection with the therapeutic team and the opportunity to get to know the therapists better. Some technical issues were also identified regarding this format (e.g., indications to improve the flow of the video cuts; audio and video synchronization).
Healthcare professionals presented favorable ratings on other aspects of the platform (on a scale from 0, no satisfaction, and 10, extremely satisfied): design (M = 8.40; SD = 1.52), color pattern (M = 8.80; SD = 1.30), and attractiveness (M = 8.40; SD = 1.34).
Concerning the contents of the intervention, positive ratings were also provided (0, no satisfaction – 10, extremely satisfied) for all assessed items: content quality (M = 9.60; SD = 0.55), pertinence of the topics (M = 9.40; SD = 0.89), topics sequencing (M = 8.60; SD = 0.55), and appropriateness of therapists’ posture (M = 9.20; SD = 0.84).
Participant Engagement and Retention
The completers’ sample logged into the platform on average 16.33 times (SD = 12.91), and evaluated the first session on average as 4 (SD = 0.63), and the second session as 3.83 (SD = 0.75), both on a scale of 1–5. In what concerns home practice, completers practiced on average 2.67 times (SD = 3.20) the practice from session one (mindfulness of breathing), and 2.20 times (SD = 2.68) the practice from session 2 (body scan).
The dropout sample logged into the platform on average 3.33 times (SD = 3.90). Four of these participants completed the first session, assessed it as 4.5 on average (from 1 to 5; SD = 0.58), and did the practice from session one on average 1.75 times (SD = 0.96). No participant from the dropout group assessed the second session nor engaged in the second practice.
Reasons for Dropout
Six of the 12 participants that dropped out from the study completed the attrition questionnaire. Three participants indicated a difficult personal situation after the beginning of the study as the reason for dropout, two referred to lack of time, and one referred to having forgotten to complete the intervention (although participants were reminded once a week to complete the sessions). No participant referred to any reason associated with the platform or the intervention. Two participants provided additional feedback, indicating that: (1) “it looked very well structured, simple, and potentially very useful”; and (2) “I really liked the intervention’s contents and how the platform was structured. I had a problem with the login once, but it was quickly fixed.”
Descriptive Statistics
Sample of Participants With Chronic Pain
The demographic and clinical characteristics of the participants that accepted to participate, the ones who dropped out, and the completers are presented in Table 3.
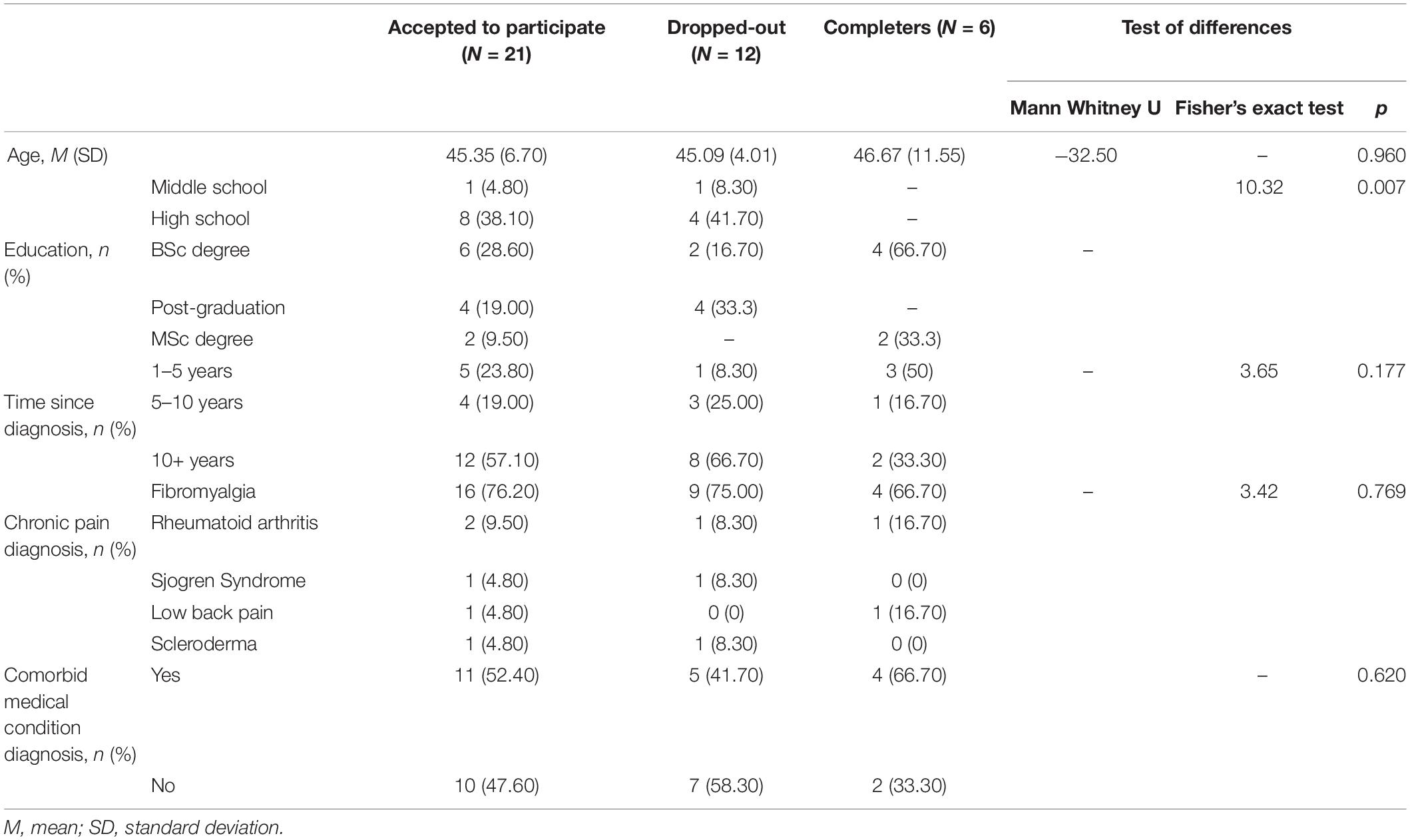
Table 3. Descriptives and frequencies of the demographic and clinical variables in study across groups, and tests of differences between participants who dropped out and completers.
There were no statistically significant differences between completers and participants who dropped out regarding age, time since chronic pain diagnosis, chronic pain diagnosis, and diagnosis of comorbid medical conditions. However, there were significant differences regarding education - participants that dropped out presented less education. The final sample of completers was composed of women with chronic pain with ages between 35 and 65 years.
Sample of Healthcare Professionals
Regarding the group of healthcare professionals, out of the eight professionals that signed an informed consent, five (four psychologists and a physician) provided feedback. These five professionals, four women and a man, had worked in chronic pain contexts between 5 and 20 years (M = 10.40; SD = 6.19) in hospitals in the North and Center regions of Portugal.
Discussion
Overall, the pilot usability study of the iACTwithPain platform (and first three sessions: 0, 1, and 2) presented promising results in terms of usability scores (high for both clinical and healthcare professionals samples), quality assessment of the different content delivery methods, and engagement metrics. Qualitative feedback from participants and health professionals will be taken into consideration for the development of the full iACT intervention, and measures to avoid dropout will be adopted.
Of the six chronic pain participants that completed this pilot test, and the five healthcare professionals that provided feedback, there seemed to be an overall satisfaction with both the intervention, regarding its contents and form of presentation of information, and the platform, concerning its design, appearance, and usability. Real image videos, mainly used to introduce new topics, provide rationales, or exemplify the possible meditation positions, appeared to be more preferred than animations or audios by chronic pain participants. This was possibly due to a perception of “being closer” to the therapists, provided by the real image videos, which may help participants feel understood and find the motivation to practice. It may also be hypothesized that real image videos are more effective in tapping into tacit cognitive-emotional factors of efficacy in psychotherapy, such as an empathic and compassionate therapeutic relationship, which is more difficult to convey through non-human avatars. This was highlighted by healthcare professionals’ feedback, who nonetheless also emphasized the appealing and dynamic aspects of the animation format. However, for meditative practices, the audio format should have preferred use over real image videos or animations to avoid unnecessary distractions during practice. Finally, two participants with chronic pain indicated that they believed that strategies to reduce pain should be included in the intervention. Even though the first session of the iACTwithPain intervention states the rationale for accepting pain rather than attempting to reduce or control it (Vowles and McCracken, 2008), and the negative effects of doing the latter (McCracken et al., 2007), it seems that these participants still held on to the idea that pain must be avoided to lead a satisfactory life. Still, participants had only completed the two first sessions of the intervention, where ACT’s acceptance and values topics are not clearly focused on (these topics are presented more in-depth in later sessions). Therefore, it might be beneficial for the future RCTs to increase the focus on acceptance earlier in the intervention, by including, for example, experiential acceptance exercises or metaphors.
The study attrition rate was of 71.43%. Out of the 21 participants that signed the informed consent, 12 (57.14%) accessed the intervention, and 6 (28.57%) completed the study. No significant differences in demographic or clinical variables were found between dropouts and completers except for completed education, with participants who dropped out presenting less education than completers. This result is in line with findings from previous research, where lower educational level was associated with higher risk if dropping out (Karyotaki et al., 2015). Motives for dropout, offered by 6 of the 12 participants who did not finish the intervention, were unrelated to the intervention or platform. There were reasons related to difficult personal events occurring during the intervention, lack of time, or having forgotten. Similar results were found in a review about reasons for dropping out in ACT interventions (Karekla et al., 2019). The iACTwithPain platform will thus include mechanisms to identify when participants have not logged in to the platform for 3 days in a row, so the team can send engagement reminders to these participants. This strategy is aligned with previous studies showing that contingent reminders can improve motivation and boost behavior change (Webb et al., 2010). If emails are not enough to engage non-responsive participants, phone calls will be implemented, since previous online-based studies have suggested that closer contact with the therapist is associated with lower dropout rates (Cuijpers et al., 2008; Macea et al., 2010). Still, given that only half of the participants who dropped out provided reasons for having stopped participating, it is difficult to know whether the platform/intervention did not influence some participants’ dropout. Other factors that we did not account for might be influencing dropout, namely comorbid depression or anxiety, relationship status, or chronic pain severity, according to a review by Melville et al. (2010). The attrition rate presented by this study falls within the range of 2–83%, presented by a review on dropout rates from online treatments for psychological disorders (Melville et al., 2010). It should nonetheless be noted that the current intervention is directed at people with chronic pain, and most importantly, that this is a usability study, in which participants may present less motivation to participate in comparison with a trial of a full intervention.
This usability study will improve the iACTwithPain platform by informing which type of format is preferred and which one works best for each type of content. Considering feedback from the participants, the real image videos with therapists were overall preferred and viewed as engaging and motivating, so we will mostly select this format in the future intervention. Nevertheless, all types of exercises will be maintained (animations, videoscribes, real image videos, and audios), since some participants showed preference for these formats and since this will allow for a more varied and stimulating user experience. The audio format will be selected for guided exercises (e.g., 80th Birthday Party) or meditations (e.g., body scan), since participants reported that this format helped them maintain focus on the instructions of the exercises. Participants did not provide negative feedback regarding the attractiveness, navigation or esthetic elements (e.g., design and color pattern) of the platform. Therefore, no changes will be made to these elements. Finally, weekly automatic and contingent reminders (when a participant does not login in for three consecutive days) will be implemented to reduce the likelihood of participants dropping out from study.
This study has some limitations that are worth discussing. We did not assess previous experience with acceptance or compassion-based psychological interventions, so it was not possible to control the possible confounding effect of previous knowledge/experience on these approaches. The small sample size might have influenced the results obtained and might not generalize to broader samples. Only women enrolled in this study (although this was not a criterion for this study), which limits generalization of these results to male chronic pain samples. However, this usability study allowed the initial test of the iACTwithPain platform and provided valuable insights for developing the full intervention. A future feasibility study informed by the current one is being conducted by the iACTwithPain team and will assess several recruitment pathways/strategies, as well as the full intervention (both quantitatively and qualitatively).
The present study has informed the improvement of the iACTwithPain platform before its final testing in a larger clinical trial. In addition, this study provides useful information on some aspects researchers should consider while developing online psychological interventions for chronic pain.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Faculty of Psychology and Educational Sciences, University of Coimbra, Portugal. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
IT: conceptualization, data curation, formal analysis, and writing—original draft, review and editing. RG: data curation, formal analysis, and writing—original draft. SC, PM, MN, TL, JD, and JP-G: writing—review and editing. BP: data curation and writing–review and editing. PC: funding acquisition, conceptualization, supervision, and writing—review and editing. All authors read and approved the final manuscript.
Funding
This project (REF: POCI-01-0145-FEDER-028829 | PTDC/PSI GER/28829/2017) was funded by the Fundo Europeu de Desenvolvimento Regional (FEDER) of the European Union, through the Programa Operacional Regional do Centro (CENTRO 2020) of Portugal-2020 and by the Fundação para a Ciência e Tecnologia I.P./MCTES through national funds (PIDDAC). RG was supported by a Ph.D. Grant (SFRH/BD/5099/2020), sponsored by FCT (Portuguese Foundation for Science and Technology).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ACT, Acceptance and Commitment Therapy; SUS, System Usability Scale; M, mean; SD, standard deviation.
References
APA Presidential Task Force on Evidence-Based Practice (2006). Evidence-based practice in psychology. Am. Psychol. 61, 271–285. doi: 10.1037/0003-066X.61.4.271
Bangor, A., Kortum, P. T., and Miller, J. T. (2008). An empirical evaluation of the system usability scale. Int. J. Hum. Comput. Interact. 24, 574–594. doi: 10.1080/10447310802205776
Bangor, A., Kortum, P., and Miller, J. (2009). Determining what individual SUS scores mean: adding an adjective rating scale. J. Usabil. Stud. 4, 114–123.
Bergmo, T. S. (2015). How to measure costs and benefits of eHealth interventions: an overview of methods and frameworks. J. Med. Internet Res. 17:e254. doi: 10.2196/jmir.4521
Bernfort, L., Gerdle, B., Rahmqvist, M., Husberg, M., and Levin, L. -Å (2015). Severity of chronic pain in an elderly population in Sweden—impact on costs and quality of life. Pain 156, 521–527. doi: 10.1097/01.j.pain.0000460336.31600.01
Brooke, J. (1996). SUS -A quick and dirty usability scale Usability and context. Usabil. Eval. Ind. 189, 1–7. doi: 10.1201/9781498710411-35
Carvalho, S. A., Gillanders, D., Palmeira, L., Pinto-Gouveia, J., and Castilho, P. (2018). Mindfulness, selfcompassion, and depressive symptoms in chronic pain: the role of pain acceptance. J. Clin. Psychol. 74, 2094–2106. doi: 10.1002/jclp.22689
Carvalho, S. A., Trindade, I. A., Duarte, J., Menezes, P., Patrão, B., Nogueira, M. R., et al. (2021b). Efficacy of an ACT and compassion-based eHealth program for self-management of chronic pain (iACTwithPain): study protocol for a randomized controlled trial. Front. Psychol. 12:630766. doi: 10.3389/fpsyg.2021.630766
Carvalho, S. A., Gillanders, D., Forte, T., Trindade, I. A., Pinto-Gouveia, J., Lapa, T., et al. (2021a). Self-compassion in acceptance and commitment therapy for chronic pain: a pilot study. Scand. J. Pain Online ahead of print, doi: 10.1515/sjpain-2021-0214
Carvalho, S. A., Trindade, I. A., Gillanders, D., Pinto-Gouveia, J., and Castilho, P. (2019). Cognitive fusion and depressive symptoms in women with chronic pain: a longitudinal growth curve modelling study over 12 months. Clin. Psychol. Psychother. 26, 616–625. doi: 10.1002/cpp.2386
Carvalho, S. A., Xavier, A., Gillanders, D., Pinto-Gouveia, J., and Castilho, P. (2021c). Rumination and valued living in women with chronic pain: how they relate to the link between mindfulness and depressive symptoms. Curr. Psychol. 40, 1411–1419. doi: 10.1007/s12144-018-0052-z
Cuijpers, P., van Straten, A., and Andersson, G. (2008). Internet-administered cognitive behavior therapy for health problems: a systematic review. J. Behav. Med. 31, 169–177. doi: 10.1007/s10865-007-9144-1
Dorner, T. E., Alexanderson, K., Svedberg, P., Tinghög, P., Ropponen, A., and Mittendorfer-Rutz, E. (2016). Synergistic effect between back pain and common mental disorders and the risk of future disability pension: a nationwide study from Sweden. Psychol. Med. 46, 425–436. doi: 10.1017/S003329171500197X
Duarte, C., Pinto-Gouveia, J., and Stubbs, R. J. (2017). Compassionate attention and regulation of eating behaviour: a pilot study of a brief low-intensity intervention for binge eating. Clin. Psychol. Psychother. 24, O1437–O1447. doi: 10.1002/cpp.2094
Elliott, A. M., Smith, B. H., Penny, K. I., Cairns Smith, W., and Alastair Chambers, W. (1999). The epidemiology of chronic pain in the community. Lancet 354, 1248–1252. doi: 10.1016/S0140-6736(99)03057-3
Faulkner, L. (2003). Beyond the five-user assumption: benefits of increased sample sizes in usability testing. Behav. Res. Methods Instrum. Comput. 35, 379–383. doi: 10.3758/bf03195514
Gilbert, P. (2009). Introducing compassion-focused therapy. Adv. Psychiatr. Treat. 15, 199–208. doi: 10.1192/apt.bp.107.005264
Gooding, H., Stedmon, J., and Crix, D. (2020). All these things don’t take the pain away but they do help you to accept it’: making the case for compassion-focused therapy in the management of persistent pain. Br. J. Pain 14, 31–41. doi: 10.1177/2049463719857099
Groenewald, C. B., and Palermo, T. M. (2015). The price of pain: the economics of chronic adolescent pain. Pain Manag. 5, 61–64. doi: 10.2217/pmt.14.52
Hayes, S. C., Strosahl, K. D., and Wilson, K. G. (2012). Acceptance and Commitment Therapy: The Process and Practice of Mindful Change, 2nd Edn. New York, NY: Guilford Press.
Karekla, M., Constantinou, P., Ioannou, M., Gloster, A. T., and Kareklas, I. (2019). The phenomenon of treatment dropout, reasons and moderators in acceptance and commitment therapy and other active treatments: a meta-analytic review. Clin. Psychol. Eur. 1:e33058. doi: 10.32872/cpe.v1i3.33058
Karyotaki, E., Kleiboer, A., Smit, F., Turner, D. T., Pastor, A. M., Andersson, G., et al. (2015). Predictors of treatment dropout in self-guided web-based interventions for depression: an ‘individual patient data’ meta-analysis. Psychol. Med. 45, 2717–2726. doi: 10.1017/S0033291715000665
Macea, D. D., Gajos, K., Daglia Calil, Y. A., and Fregni, F. (2010). The efficacy of web-based cognitive behavioral interventions for chronic pain: a systematic review and meta-analysis. J. Pain 11, 917–929. doi: 10.1016/j.jpain.2010.06.005
Martins, A. I., Rosa, A. F., Queirós, A., Silva, A., and Rocha, N. P. (2015). European Portuguese validation of the System Usability Scale (SUS). Procedia Comput. Sci. 67, 293–300. doi: 10.1016/j.procs.2015.09.273
Mayer, S., Spickschen, J., Stein, K. V., Crevenna, R., Dorner, T. E., and Simon, J. (2019). The societal costs of chronic pain and its determinants: the case of Austria. PLoS One 14:e0213889. doi: 10.1371/journal.pone.0213889
McCracken, L. M., and Eccleston, C. (2003). Coping or acceptance: what to do about chronic pain? Pain 105, 197–204. doi: 10.1016/S0304-3959(03)00202-1
McCracken, L. M., Vowles, K. E., and Gauntlett-Gilbert, J. (2007). A prospective investigation of acceptance and control-oriented coping with chronic pain. J. Behav. Med. 30, 339–349. doi: 10.1007/s10865-007-9104-9
Melville, K. M., Casey, L. M., and Kavanagh, D. J. (2010). Dropout from internet-based treatment for psychological disorders. Br. J. Clin. Psychol. 49, 455–471. doi: 10.1348/014466509X472138
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self Identity 2, 223–250. doi: 10.1080/15298860309027
Plumb, J. C., and Vilardaga, R. (2010). Assessing treatment integrity in acceptance and commitment therapy: strategies and suggestions. Int. J. Behav. Consultation Ther. 6, 263–295. doi: 10.1037/h0100912
Smith, B. H., Elliott, A. M., Chambers, W. A., Smith, W. C., Hannaford, P. C., and Penny, K. (2001). The impact of chronic pain in the community. Fam. Pract. 18, 292–299. doi: 10.1093/fampra/18.3.292
Trindade, I. A., Ferreira, C., and Pinto-Gouveia, J. (2020). Acceptability and preliminary test of efficacy of the mind programme in women with breast cancer: an acceptance, mindfulness, and compassion-based intervention. J. Context. Behav. Sci. 15, 162–171. doi: 10.1016/j.jcbs.2019.12.005
Trindade, I. A., Guiomar, R., Carvalho, S. A., Duarte, J., Lapa, T., Menezes, P., et al. (2021a). Efficacy of online-based acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. J. Pain 22, 1328–1342. doi: 10.1016/j.jpain.2021.04.003
Trindade, I. A., Pereira, J., Galhardo, A., Ferreira, N. B., Lucena-Santos, P., Carvalho, S. A., et al. (2021b). The LIFEwithIBD intervention: study protocol for a randomized controlled trial of a face-to-face acceptance and commitment therapy and compassion-based intervention tailored to people with inflammatory bowel disease. Front. Psychiatry 12:699367. doi: 10.3389/fpsyt.2021.699367
Veehof, M. M., Oskam, M.-J., Schreurs, K. M. G., and Bohlmeijer, E. T. (2011). Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis. Pain 152, 533–542. doi: 10.1016/j.pain.2010.11.002
Veehof, M. M., Trompetter, H. R., Bohlmeijer, E. T., and Schreurs, K. M. G. (2016). Acceptance- and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cogn. Behav. Ther. 45, 5–31. doi: 10.1080/16506073.2015.1098724
Vowles, K. E., and McCracken, L. M. (2008). Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process. J. Consult. Clin. Psychol. 76, 397–407. doi: 10.1037/0022-006X.76.3.397
Webb, T. L., Joseph, J., Yardley, L., and Michie, S. (2010). Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Medic. Internet Res. 12:e4. doi: 10.2196/jmir.1376
Keywords: acceptance and commitment therapy, chronic pain, online intervention, usability study, IT
Citation: Guiomar R, Trindade IA, Carvalho SA, Menezes P, Patrão B, Nogueira MR, Lapa T, Duarte J, Pinto-Gouveia J and Castilho P (2022) Usability Study of the iACTwithPain Platform: An Online Acceptance and Commitment Therapy and Compassion-Based Intervention for Chronic Pain. Front. Psychol. 13:848590. doi: 10.3389/fpsyg.2022.848590
Received: 04 January 2022; Accepted: 24 June 2022;
Published: 22 July 2022.
Edited by:
Fanbo Meng, Jiangnan University, ChinaReviewed by:
Michael Bordieri, Murray State University, United StatesFrancisco Javier Cano-García, Seville University, Spain
Copyright © 2022 Guiomar, Trindade, Carvalho, Menezes, Patrão, Nogueira, Lapa, Duarte, Pinto-Gouveia and Castilho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Guiomar, cmFxdWVsZ3Vpb21hcjE4QGdtYWlsLmNvbQ==