
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychol. , 29 April 2022
Sec. Psychology for Clinical Settings
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.840881
This article is part of the Research Topic Developing Democracy: Positive and Negative Effects of Youth Civic and Political Participation View all 4 articles
 Parissa J. Ballard1*†
Parissa J. Ballard1*† Stephanie S. Daniel1†Grace Anderson2†Aubry N. Koehler1Elimarie Caballero Quinones3Ashley Strahley4
Stephanie S. Daniel1†Grace Anderson2†Aubry N. Koehler1Elimarie Caballero Quinones3Ashley Strahley4 Linda M. Nicolotti3
Linda M. Nicolotti3
Community volunteering is an under-utilized, at least under-researched, strategy to supplement existing treatment for affective disorders. We present findings from a feasibility study incorporating community volunteering into clinical treatment for depression and anxiety among adolescents and young adults. This exploratory pilot study had four aims: to investigate recruitment feasibility; to describe participants’ experiences with volunteering; to explore psychosocial assets by which volunteering might decrease depressive and anxiety symptoms; and to document preliminary changes in mental health outcomes before and after the volunteering intervention. Interviews and surveys were employed with participants (N = 9; ages 14–20, Mage = 16 years old; eight women and one man) newly diagnosed with: mild to moderate depression (single episode), mild to moderate anxiety, or adjustment disorder. Recruitment was feasible overall, successes and challenges are discussed. Experiences with volunteering were very positive. Qualitative findings revealed perceived positive effects of volunteering on mood and well-being such as helping with social anxiety and being a positive distraction. Qualitative findings revealed several psychosocial assets that improved related to volunteering (e.g., sense of purpose/meaning and sense of community). On average, participants reported a 19% decrease in depressive symptoms from the pre-survey (before volunteering) to the post-survey (after volunteering). Although more research is warranted, the implication of this study for practicing psychologists treating adolescents and young adults for mild to moderate depression and/or anxiety is that they may wish to consider incorporating community volunteer activities into treatment. Volunteering was a desirable activity for interested participants in treatment for affective disorders.
Community volunteering, or taking part in unpaid work for the benefit of others, can present young people with a transformative opportunity to develop positive relationships, social connections, and skills while contributing to their community. Research investigating associations between volunteering, mental health and well-being points to robust positive associations [e.g., Piliavin and Siegl (2015)] using observational methods [e.g., Jenkinson et al. (2013)] with community samples. Volunteering has not yet been systematically examined as a potential supplement or adjunct to treatment interventions with adolescents and young adults in clinical treatment for affective and/or anxiety disorders.
Affective disorders, such as depression and anxiety, are salient mental health concerns during adolescence and young adulthood [e.g., Beesdo et al. (2009)] and effective treatment interventions to address affective disorders are highly significant. Effective pharmacological and non-pharmacological treatment approaches (such as cognitive behavioral therapy) for depression (Butler et al., 2006; Weersing et al., 2017) and anxiety (Davis et al., 2011) are well-established, and innovations consistently improve and supplement treatment approaches. Non-pharmacological interventions, such as those based in positive psychology, are desirable to many people either instead of or in conjunction with medication. Based on theoretical and empirical findings detailing positive associations between volunteering and mental health and well-being (Konrath and Brown, 2013; Piliavin and Siegl, 2015; Creaven et al., 2017; Ballard et al., 2021), we believe that volunteering can help young people develop psychosocial assets and reduce symptoms of affective disorders. Importantly, volunteering fits within existing evidenced-based approaches to treating depressive and/or anxiety disorders [see Ballard et al. (2021) for full review] and is conceptually consistent with principles of positive psychology interventions, cognitive-behavioral therapy (CBT) and behavioral therapy approaches, including exposure therapy for certain anxiety disorders (Reinecke et al., 1998; Heimberg and Becker, 2002; Butler et al., 2006; David-Ferdon and Kaslow, 2008). Volunteering may also be a form of behavioral activation. In addition, it may reduce symptoms common to both depression and anxiety like rumination and overthinking by helping teens broaden their perspectives and potentially shift their thought patterns and orientation from self-focus to include a focus on others, consistent with CBT strategies. Volunteering can also provide a structured, predictable, and supportive social environment to make connections with others in a task-oriented way with an accountability structure, which provides a mechanism for socialization that may be a helpful example of “in vivo” social exposure in an exposure therapy approach for social anxiety (Rodebaugh et al., 2004). Therefore, community volunteerism may be a promising but under-utilized, or at least under-researched, strategy to supplement clinical treatment for adolescent affective disorders.
This pilot study incorporated community volunteering into clinical treatment for adolescent depression and anxiety to examine feasibility and collect qualitative data to explore participant experiences. First, we investigate the feasibility of recruiting participants from community behavioral health practices into the study. Next, we describe participants’ experiences with volunteering and explore psychosocial assets by which volunteering might decrease depressive and anxiety symptoms. Finally, we document preliminary changes in mental health outcomes before and after the volunteering intervention.
Participants were adolescents and young adults (N = 9; between ages 14–20, Table 1). Eligible participants were newly diagnosed (treatment <8 months) with mild to moderate depression or anxiety (single episode), comorbid depression and anxiety, or an adjustment disorder. Inclusion criteria also included elements specific to participating in an fMRI scan such as: being right-handed (which can affect brain functioning on certain tasks), not experiencing claustrophobia, and no contraindications for an fMRI scan.1
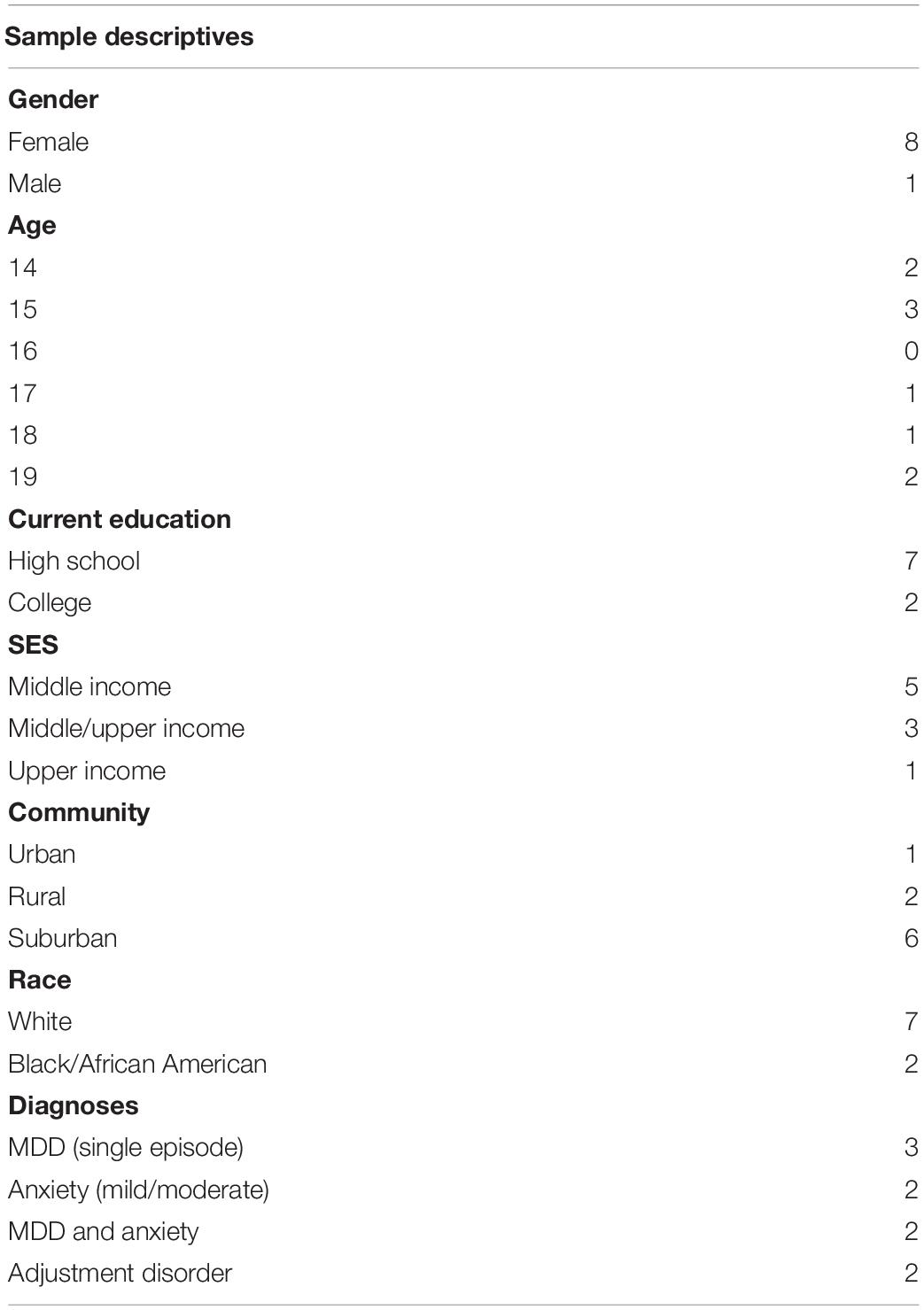
Table 1. Description of the sample (N = 9).
Depression was measured through the Beck Depression Inventory-II [BDI-II; Beck et al. (1996)]. Each of the 21 items is answered on a scale from 0–3 and items were summed. Scores of 0–13 are considered in the minimal range; 14–19 as mild; 20–28 as moderate, and 29–63 as severe depressive symptoms. Anxiety was examined using four relevant items from the BDI that are central to a generalized anxiety disorder diagnoses according to the DSM-V (agitation, irritation, changes in sleep patterns, and concentration difficulties). This study did not include an explicit measure of anxiety; when it emerged as an important construct for study inclusion and in the qualitative data, we used relevant items from the BDI to examine indicators of anxiety in the absence of a validated full measure.
With appropriate ethical and IRB approvals (IRB00053435), participants were screened by community mental health providers and referred to the study team, who explained study details and obtained written consent/assent from participants (and their parents for minors). The research team administered the pre-self-report survey and scheduled a pre- fMRI lab visit before the volunteering. We helped participants find a meaningful volunteer experience from a menu of local options, developed by the research team in a series of steps (contact first author for details) to support personal meaning and goodness-of-fit with volunteering experience. Participants were asked to report their volunteer hours weekly, and we checked in with participants every 2–4 weeks via text about the volunteering. When participants had completed 30 h, we conducted the post- survey, interview, and fMRI (when possible). Interviews were in-person or remote, via phone or WebEx, between August 2019-July 2020, lasted approximately 10 min, and were audio recorded. Participants were compensated $50 after the pre-study visit and another $75 after study completion.
We used an open trial design with no control group to explore the feasibility and acceptability of this intervention. We collected qualitative data (via interviews) after the volunteering intervention and surveys before and after the volunteering intervention. Findings come from analyzing the open-ended interview data (see Appendix A for the interview guide) to explore themes related to participants’ volunteer experiences and perceptions of volunteering as associated with their mood and well-being. Interviews were transcribed verbatim and we used a matrix analysis approach (Averill, 2002) in which a study team member deductively constructed a matrix of interest areas (domains) to organize the data based on the interview guide and qualitative study aims. Data were summarized into key points and organized in the matrix, along with illustrative quotes. Participant responses were then synthesized into themes within each domain.
Overall, providers were enthusiastic about the study; we met our recruitment target; and the intervention was acceptable for teens and providers. We describe two key challenges to feasibility, and the adaptations we made.
The first key challenge to feasibility was finding clinical providers with enough clientele who met study inclusion criteria. We discussed this study with 22 clinical providers; conversations were extremely fruitful, and providers were enthusiastic about the project. Many saw the value of volunteering for some of their clients, and some already suggested volunteering with clients in therapy. Some lacked knowledge of local volunteer opportunities, so welcomed this support from our study. However, many clinical providers did not think they had enough clientele to refer to the project due to our initial criteria (only MDD single episode diagnoses and having been in treatment for less than 3 months). To address this, we (1) expanded our inclusion criteria to include mild/moderate anxiety, single episode (unspecified; separation; other specified) and adjustment disorder (unspecified; with depressed mood; with anxiety; with anxiety and depressed mood) in addition to MDD (unspecified; mild; moderate; partial remission; unspecified depressive disorder) and (2) expanded to include teens who had been in treatment up to 8 months. Once these modifications in criteria were made, we were able to recruit teens fairly seamlessly. Four referring providers had 16 conversations about the study with eligible clients. Of those, 12 were interested in participating in the study. Of the 12, we successfully recruited nine into our study. Eight out of nine completed the study, and one was lost to follow-up. Four of the nine completed their 30 volunteering hours; several had to stop early due to COVID-19 (Table 2).
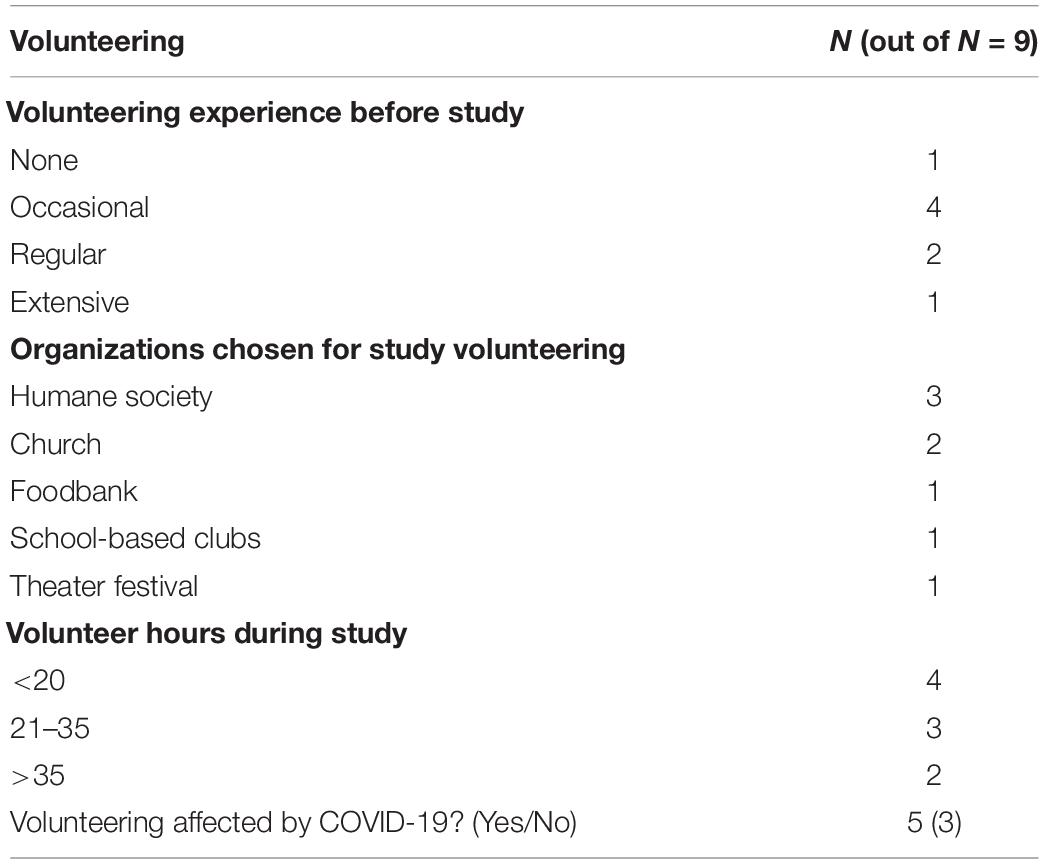
Table 2. Summary of study participants’ volunteer experience.
A second key challenge to this study was disruption due to COVID-19. Three study participants completed the study before COVID-19 (before March, 2020); five study participants had to pause their volunteering (although two had already completed 30 h). We paused data collection completely for 3 months and eventually transitioned to virtual data collection for the post survey and interviews. The months-long delay made it unlikely that we would see any Default Mode Network activity corresponding to the volunteering intervention; we stopped post fMRI data collection for six of our nine participants. Some post data were collected virtually in the summer of 2020; we asked about life during COVID-19 during interviews and had a sense that it was difficult for teens and that most had developed ways to cope.
Most teens had occasional volunteer experience prior to study participation. Teens tended to choose to volunteer at organizations such as the Humane Society and local churches or schools (Table 2). Qualitative interviews with participants indicated that teens were highly favorable about their volunteer experiences, and all expressed an interest in continuing to volunteer following the study (see Table 3 for themes and illustrative quotes). An important aspect of enjoyment was the alignment of the volunteer organization and/or specific duties with the individual’s interests. Several participants shared that they specifically enjoyed the opportunity to work with children or animals, or that their volunteer experience aligned with their career interests. Participants also discussed the importance of having choice about where they volunteered, which some noted was different from past volunteer experiences. Finally, participants noted when the volunteer experience was rewarding suggesting that volunteering can provide satisfaction and enjoyment derived from helping others.
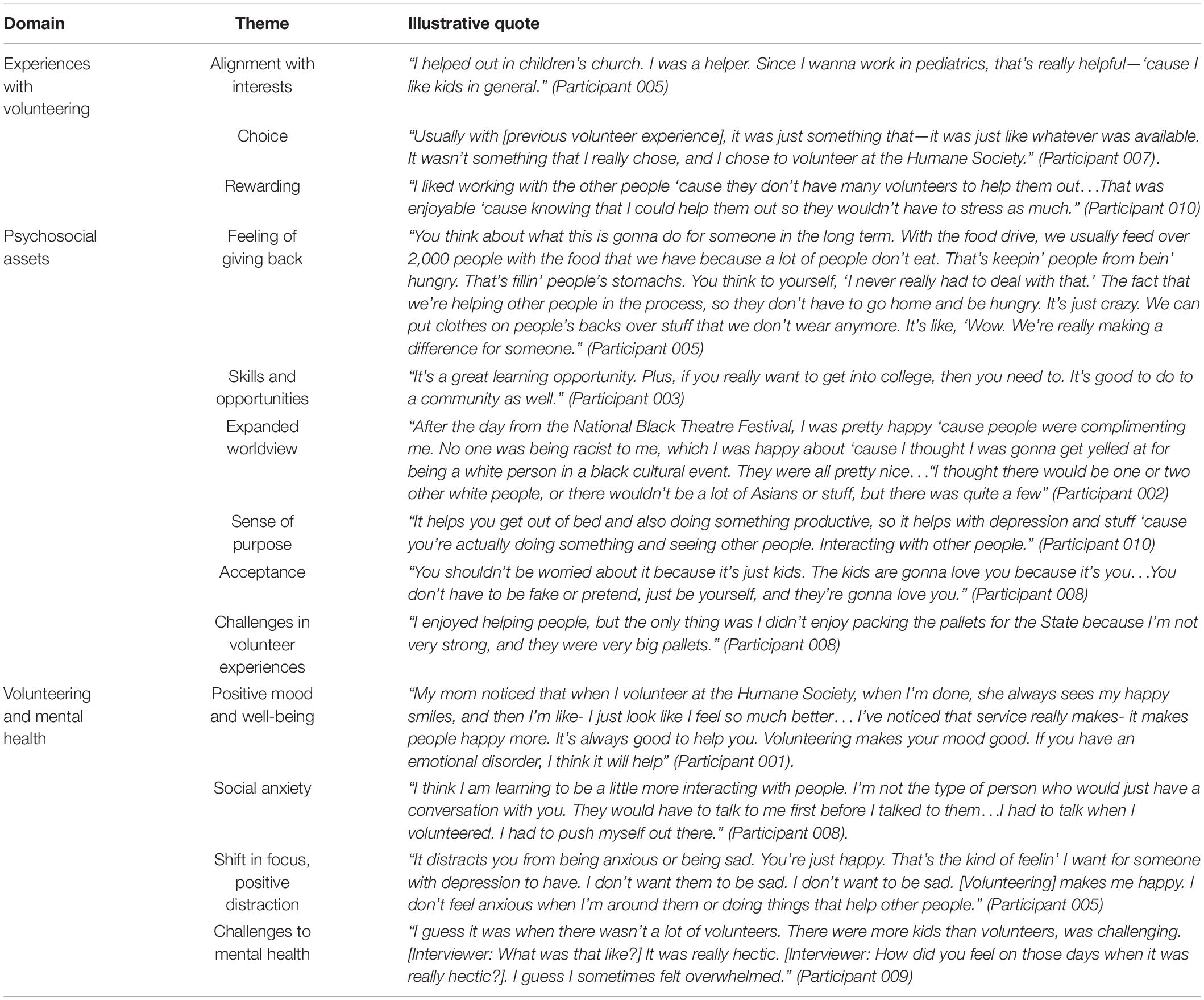
Table 3. Qualitative data domains, themes, and illustrative quotes.
Participant interviews revealed several psychosocial assets that were bolstered through volunteering and also noted challenges (Table 3). A positive aspect of the volunteer experience for adolescents and young adults was the feeling of giving back/making a difference. Several participants shared that they enjoyed “helping people,” or “making a difference for someone.” In addition to such psychological benefits, participants noted practical benefits such as gaining skills and opportunities and would recommend volunteering to other teens for opportunity to learn new things and for instrumental benefit such as building a resume or getting into college. One participant discussed how her volunteer experience challenged her and expanded her worldview, in particular, her expectations about racism and inclusivity. One participant explained how volunteering helped with her depression because it gave a sense of purpose and one participant recommended specifically that adolescents and young adults with anxiety should volunteer with children because children accept you as you are. When asked what was challenging, most participants shared challenges that they considered to be minor such as physical demands and getting children to behave.
Participants were asked about how their volunteering related to their mood and well-being, and if they would recommend volunteering for other adolescents and young adults with anxiety and/or depression (Table 4). All participants felt that volunteering positively affected their mood and well-being. Some felt happier when they volunteered, and one described her volunteer experience as “relaxing” and “calming.” Several participants shared that volunteering helped with their social anxiety, and that it was beneficial to push themselves to talk to people as part of their volunteer experience. All participants said that they would recommend volunteering to other adolescents and young adults with anxiety and/or depression. Several participants also described the benefit of volunteering in terms of shifting their focus and providing positive distraction. One participant felt that volunteering was different from other activities (e.g., music) because it is “like a job.” Two participants specified that it can get someone’s mind off of their anxiety and/or depression. Participants also described two types of challenges: volunteering provoking anxiety and motivational challenges. Two participants described feeling “overwhelmed” or experiencing anxiety-provoking moments during volunteering even though both participants were positive about their overall experience. Participants also shared that it was sometimes hard to be motivated to go to their volunteer assignment, but that they felt better while they were volunteering or afterward. It is noteworthy that participants discussed overcoming challenges during their volunteering.
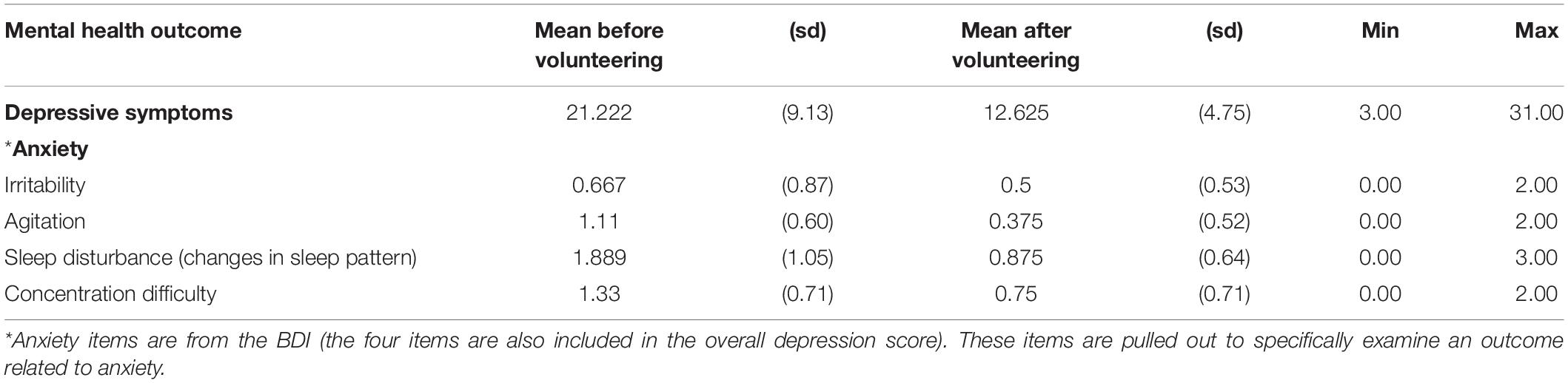
Table 4. Mental health before and after volunteering.
On average, participants reported a 19% decrease in depressive symptoms from before to after volunteering, calculated as average relative change scores on the BDI from Pre- to Post-. Participant BDI scores were 21.11 on average (Pre) to 12.63 (Post); this is a clinically significant change from the “moderate” to the “minimal” range for BDI scores. Decreases were observed on the four BDI items relevant to anxiety (Table 4).
Despite potential motivational and logistical challenges [see Ballard et al. (2021)] for a discussion, teens who were referred to our study were very interested in participating. Once enrolled, they were able to find meaningful volunteer opportunities and complete their hours (with the exception of disruptions due to COVID-19). Several factors made this feasible. Clinicians had a good sense of their clients’ readiness, which teens would benefit, and which families would be able to facilitate community volunteerism. In addition, the study set up an infrastructure to help participants find a local opportunity corresponded with volunteer organizations to aid teens in completing paperwork as needed and texted participants every few weeks to check in. This infrastructure would be hard for clinicians to provide so it is worth understanding the role this support played and additional ways to minimize clinician burden.
Participants’ experiences in volunteering were overwhelmingly positive. All participants planned to volunteer following the study. Specifically, results points to the importance of volunteer experiences fitting with teens’ interests and having the ability to choose their volunteer opportunity. Participants also emphasized that it was rewarding to help others.
Regarding psychosocial assets by which volunteering can decrease depressive symptoms, interviewees discussed the importance of feeling like they were making a difference via volunteering, developing tangible skills, and feeling accepted as well as a gaining a sense of purpose. This aligns with and extends previous research suggesting that volunteering can help develop independence and personal worth, social connectedness, sense of purpose, practice with problem-solving and leadership skills, increase the ability to work with others, and develop particular skill sets, which can contribute to positive mental health benefits [e.g., Malin et al. (2015), Piliavin and Siegl (2015), and Creaven et al. (2017)]. These are potentially important clinical targets for teens struggling with depression and anxiety.
Regarding changes in mental health outcomes before and after the volunteering intervention; participants discussed many ways that volunteering affected their mood and well-being. Specifically, volunteering made some feel happy and calm, served as a positive distraction for others, and decreased their social anxiety by giving them a structured opportunity to interact with others. A notable (although preliminary) finding was the decrease in depressive symptoms from the clinically “moderate range” to “minimal” range. Although we did not test statistical significance, this is a clinically significant decrease in depressive symptoms, and the 19% decrease is above what is considered a minimally clinically significant change [e.g., 17.5%, Button et al. (2015)]. Given the study design, we cannot attribute this decrease in depression severity to volunteering alone; participants continued with their treatment as usual over the time-frame of the study as volunteer experiences were intended to be a supplemental intervention to primary treatment.
This exploratory feasibility study did not include a control group which makes it impossible to determine the unique benefits and additive effects of community volunteering for developmental or treatment-as-usual effects. The small sample size, although by design, is a limitation regarding statistical significance testing and was not diverse with regards to gender or race/ethnicity, which limits generalizability. This exploratory study provides a basis for future research using rigorous design to compare treatment-as-usual to treatment-as-usual plus volunteering with a larger sample. Future studies should also include an explicit measure of anxiety to better assess the role of volunteering in reducing anxiety symptoms. Finally, future studies with larger samples can continue to test which aspects of volunteering are most beneficial for teens in the treatment of depression and anxiety, how to make such opportunities more broadly available to all teens, what supports make this intervention feasible for provides, and what is the necessary “dose” of volunteering to provide benefits to teens.
Our preliminary findings suggest that clinical providers treating adolescents and young adults for mild to moderate depression and/or anxiety may wish to consider incorporating community volunteer activities into treatment. Community volunteering was desirable and feasible participants. Incorporating volunteerism may be a useful modality in the treatment of internalizing disorders to increase behavioral activation, socialization, participation in meaningful activities, a focus on others rather than self, self-esteem and self-efficacy, and routine and structure. When considering who might benefit most, clinicians would need to consider diagnoses, disorder severity, and course of treatment. Clinicians might search for existing local resources that compile teen-friendly volunteering opportunities and consider how best to partner with local organizations to support alignment between youth volunteers and organizations. In sum, the use of volunteering as an addition to standard therapy approaches has promise for the treatment of depression and anxiety for adolescents and young adults, this strategy merits further empirical investigation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Wake Forest Institutional Review Board. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
PB conceptualized and led the writing for this manuscript and conducted the quantitative analysis. SD contributed to the conceptualization and writing. GA contributed to the literature review. AS conducted the qualitative analysis. SD, GA, AK, LN, EC, and AS contributed to discussing, framing, reviewing the literature, and editing the manuscript. All authors contributed to the article and approved the submitted version.
This research was supported by a grant from the Errett Fisher Foundation to PB and SD. We thank the Wake Forest Clinical and Translational Science Institute’s Program in Community-engaged Research (NCATS Grant UL1TR001420) for support. This research was also supported in part by the Qualitative and Patient-Reported Outcomes Developing Shared Resource of the Wake Forest Baptist Comprehensive Cancer Center’s NCI Cancer Center Support Grant P30CA012197 and the Wake Forest Clinical and Translational Science Institute’s NCATS Grant UL1TR001420.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We are grateful to study participants, the clinical providers who referred them to this study, and many clinicians for insightful discussions about the ideas presented in this manuscript.
Averill, J. B. (2002). Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qual. Health Res. 12, 855–866. doi: 10.1177/104973230201200611
Ballard, P. J., Daniel, S. S., Anderson, G., Nicolotti, L., Caballero Quinones, E., Lee, M., et al. (2021). Incorporating Volunteering Into Treatment for Depression Among Adolescents: developmental and Clinical Considerations. Front. Psychol. 12:1581. doi: 10.3389/fpsyg.2021.642910
Beck, A. T., Steer, R. A., and Brown, G. K. (1996). Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation.
Beesdo, K., Höfler, M., Leibenluft, E., Lieb, R., Bauer, M., and Pfennig, A. (2009). Mood episodes and mood disorders: patterns of incidence and conversion in the first three decades of life. Bipol. Disord. 11, 637–649. doi: 10.1111/j.1399-5618.2009.00738.x
Butler Andrew, C., Jason, E., Chapman, Evan, M., Forman, et al. (2006). The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin. Psychol. Rev. 26, 17–31. doi: 10.1016/j.cpr.2005.07.003
Button, K. S., Kounali, D., Thomas, L., Wiles, N. J., Peters, T. J., Welton, N. J., et al. (2015). Minimal clinically important difference on the Beck Depression Inventory-II according to the patient’s perspective. Psychol. Med. 45, 3269–3279. doi: 10.1017/S0033291715001270
Creaven, A., Healy, A., and Howard, S. (2017). Social connectedness and depression. J. Soc. Personal Relation. 36, 1400–1417. doi: 10.1177/0265407517716786
David-Ferdon, C., and Kaslow, N. J. (2008). Evidence-based psychosocial treatments for child and adolescent depression. J. Clin. Child Adolesc. Psychol. 37, 62–104. doi: 10.1080/15374410701817865
Davis, T. E. III, May, A., and Whiting, S. E. (2011). Evidence-based treatment of anxiety and phobia in children and adolescents: current status and effects on the emotional response. Clin. Psychol. Rev. 31, 592–602. doi: 10.1016/j.cpr.2011.01.001
Heimberg, R. G., and Becker, R. E. (2002). Cognitive-Behavioral Group Therapy for Social Phobia: Basic Mechanisms and Clinical Strategies. New York: Guilford Press.
Jenkinson, C. E., Dickens, A. P., Jones, K., Thompson-Coon, J., Taylor, R. S., Rogers, M., et al. (2013). Is volunteering a public health intervention? A systematic review and meta-analysis of the health and survival of volunteers. BMC Public Health 13:1–10. doi: 10.1186/1471-2458-13-773
Konrath, S., and Brown, S. (2013). The Effects of Giving on Givers. In M. L. Newman & N. A. Roberts (Eds.) Health and Social Relationships: The Good, the Bad, and the Complicated. Washington: American Psychological Association, 39–64. doi: 10.1037/14036-003
Malin, H., Ballard, P. J., and Damon, W. (2015). Civic Purpose: an Integrated Construct for Understanding Civic Development in Adolescence. Hum. Dev. 58, 103–130. doi: 10.1159/000381655
Piliavin, J. A., and Siegl, E. (2015). Health and Well-Being Consequences of Formal Volunteering.” In D. A. Schroeder & W. G. Graziano (Eds.) The Oxford handbook of prosocial behavior, 494–523. Oxford, UK: The Oxford University Press. doi: 10.1177/2378023117700903
Reinecke, M. A., Ryan, N. E., and DuBois, D. L. (1998). Cognitive-behavioral therapy of depression and depressive symptoms during adolescence: A review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatr. 37, 26–34. doi: 10.1097/00004583-199801000-00013
Rodebaugh, T. L., Holaway, R. M., and Heimberg, R. G. (2004). The treatment of social anxiety disorder. Clin. Psychol. Rev. 24, 883–908.
Weersing, V. R., Jeffreys, M., Do, M. T., Schwartz, K. T., and Bolano, C. (2017). Evidence base update of psychosocial treatments for child and adolescent depression. J. Clin. Child Adolesc. Psychol. 46, 11–43. doi: 10.1080/15374416.2016.1220310
Appendix A| Interview Guide.
Thank you for taking part in this study!
Can you tell me about your experience with volunteering?
Probe: What did you enjoy? What was challenging? How many hours did you complete?
How did Covid-19 (coronavirus) affect your volunteering for this study?
Do you think the volunteering affected your mood or well-being? How so?
Do you think you will continue volunteering or stop? Can you tell me why?
What was it like completing surveys? How about doing fMRI scans?
Would you recommend volunteering to other teens? Why or why not?
How has Covid-19 (coronavirus) affected your mood or well-being?
How has Covid-19 (coronavirus) affected your feelings of connection to other people and your community?
Do you have any questions for me?
Again, thank you for taking your time to speak with me and to participate in this research.
Keywords: affective disorders, adolescents, volunteering, mental health, treatment
Citation: Ballard PJ, Daniel SS, Anderson G, Koehler AN, Caballero Quinones E, Strahley A and Nicolotti LM (2022) An Exploratory Feasibility Study of Incorporating Volunteering Into Treatment for Adolescent Depression and Anxiety. Front. Psychol. 13:840881. doi: 10.3389/fpsyg.2022.840881
Received: 21 December 2021; Accepted: 04 April 2022;
Published: 29 April 2022.
Edited by:
Augustine Osman, University of Texas at San Antonio, United StatesReviewed by:
Carla Fonte, University Fernando Pessoa, PortugalCopyright © 2022 Ballard, Daniel, Anderson, Koehler, Caballero Quinones, Strahley and Nicolotti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Parissa J. Ballard, cGJhbGxhcmRAd2FrZWhlYWx0aC5lZHU=
†ORCID: Parissa J. Ballard, orcid.org/0000-0001-9125-4089; Stephanie S. Daniel, orcid.org/0000-0001-5606-6146; Grace Anderson, orcid.org/0000-0003-0035-483X
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.