
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychol. , 20 January 2023
Sec. Neuropsychology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.1107001
 Edoardo Nicolò Aiello1,2†
Edoardo Nicolò Aiello1,2† Federica Solca1†
Federica Solca1† Lucia Catherine Greco3,4
Lucia Catherine Greco3,4 Antonino La Tona5
Antonino La Tona5 Silvia Torre1
Silvia Torre1 Laura Carelli1
Laura Carelli1 Claudia Morelli1Alberto Doretti1Eleonora Colombo1Stefano Messina1
Claudia Morelli1Alberto Doretti1Eleonora Colombo1Stefano Messina1 Debora Pain6Alice Radici6Andrea Lizio3Jacopo Casiraghi3
Debora Pain6Alice Radici6Andrea Lizio3Jacopo Casiraghi3 Federica Cerri3
Federica Cerri3 Agostino Brugnera5
Agostino Brugnera5 Angelo Compare5Susan Woolley7Jennifer Murphy8
Angelo Compare5Susan Woolley7Jennifer Murphy8 Lucio Tremolizzo9
Lucio Tremolizzo9 Ildebrando Appollonio9
Ildebrando Appollonio9 Federico Verde1,10
Federico Verde1,10 Valeria Ada Sansone3,11Christian Lunetta6
Valeria Ada Sansone3,11Christian Lunetta6 Vincenzo Silani1,10
Vincenzo Silani1,10 Nicola Ticozzi1,10†
Nicola Ticozzi1,10† Barbara Poletti1*†
Barbara Poletti1*†Background: The present investigation aimed at testing the psychometrics and diagnostics of the Italian version of the Caregiver Behavioral Questionnaire (CBQ) from the ALS Cognitive Behavioral Screen (ALS-CBS™), as well as its case–control discrimination, in a cohort of non-demented patients with ALS.
Methods: The caregivers of N = 265 non-demented patients with ALS and N = 99 healthy controls (HCs) were administered the CBQ and the Edinburgh Cognitive and Behavioural ALS Screen-Carer Interview (ECAS-CI). For N = 98 patients, an in-depth behavioural/psychopathological assessment via the Frontal Behavioural Inventory (FBI), the Dimensional Apathy Scale (DAS), the State and Trait Anxiety Inventory-Form Y (STAI-Y), and the Beck Depression Inventory (BDI) was also available. Factorial and construct validity, internal reliability, and diagnostics against an abnormal ECAS-CI score were tested in patients. Case–control discrimination was explored through logistic regression.
Results: The CBQ was internally reliable (McDonald’s ω = 0.90) and underpinned by a simple, unidimensional structure; it converged with ECAS-CI, FBI, and DAS scores and diverged from STAI-Y and BDI ones. A cutoff of ≤ 33 accurately detected abnormal ECAS-CI scores (AUC = 0.85), yielding optimal error- and information-based diagnostics. The CBQ was independent of demographic and disease-related variables and discriminated patients from HCs (p < 0.001).
Discussion: The Italian version of the CBQ from the ALS-CBS™ is a valid, reliable, diagnostically sound, and feasible screener for detecting frontotemporal-like behavioural changes in non-demented patients with ALS. Its adoption is thus recommended within clinical practice and research in the view of providing preliminary information on whether the administration of more extensive behavioural instruments is needed.
Up to 50% of amyotrophic lateral sclerosis (ALS) patients without dementia show frontotemporal-like changes in behavior over the course of the disease (Strong et al., 2017; Feldman et al., 2022). Since such behavioral dysfunctions negatively affect their prognosis and care management (Huynh et al., 2020), their early detection via clinimetrically sound, disease-specific screeners are clinically pivotal in this population (Gray and Abrahams, 2022). In addition, behavioral measures have been addressed within the context of both observational and interventional studies addressing patients with ALS (Beswick et al., 2021).
Among ALS-specific behavioral scales, the proxy-report checklist included within the ALS Cognitive Behavioral Screen (ALS-CBS™)—that is, the Caregiver Behavioral Questionnaire (CBQ) (Woolley et al., 2010)—has been shown to be cross-sectionally/longitudinally feasible and featured by optimal clinimetrics, at least as far as its original, English version is concerned (Simon and Goldstein, 2019; Gosselt et al., 2020).
In Italy, a back-translated version of the CBQ is available, with its convergent validity having been tested within the context of the Italian standardization of the ALS-CBS™ (Tremolizzo et al., 2020). In addition, evidence supportive of its cross-sectional feasibility for detecting behavioral changes in Italian, non-demented patients with ALS has been recently delivered (Greco et al., 2022).
Nevertheless, to this day, no full psychometric, diagnostic, and feasibility studies have been performed in Italy on the CBQ. Hence, the present investigation aimed at delivering, in a retrospective cohort of Italian, non-demented patients with ALS, (1) evidence on its factorial and construct validity, (2) internal reliability, (3) diagnostic properties, and (4) an assessment of its capability to discriminate them from healthy controls (HCs).
Data on N = 265 patients with ALS (Brooks et al., 2000) referred to three Northern Italian centers (i.e., IRCCS Istituto Auxologico Italiano; NEMO, Fondazione Serena Onlus; and Istituti Clinici Scientifici Maugeri IRCCS) between 2020 and 2022 was retrospectively retrieved. In addition, N = 99 HCs were prospectively recruited at the IRCCS Istituto Auxologico Italiano by means of authors’ personal acquaintances and advertising. Neither patients nor HCs had (other) neurological/psychiatric disorders or general-medical conditions possibly affecting neuropsychological functions (i.e., unstable internal medical/metabolic diseases or system/organ failures). No patient met either Gorno-Tempini et al. (2011) and Rascovsky et al. (2011) criteria for FTD. This study was approved by the local ethics committees; participants provided informed consent, and data were treated according to current regulations.
Patients’ and HCs’ first-degree relatives or spouses/partners were administered the Italian versions of the CBQ (Tremolizzo et al., 2020) and Edinburgh Cognitive and Behavioural ALS Screen-Carer Interview (ECAS-CI) (Poletti et al., 2016, 2022). The ECAS-CI was addressed as the main comparator against which the construct validity of the CBQ was tested (Sect. 2.3.1).
The CBQ is a 15-item, caregiver-report checklist covering the key, FTD-like behavioral signs/symptoms—that is, dysexecutive features of either an apathetic or a disinhibited nature—with items 6 and 15 instead targeting attention and language deficits, respectively. Each Likert-scaled item inquires about changes that occurred after the onset of the disease, ranging from 0 (“large change”) to 3 (“no change”); the total score on the CBQ, thus, ranges from 0 to 45, with lower scores indexing a higher level of behavioral dysfunction. The Italian CBQ is available upon the reasonable request of interested practitioners/researchers to the corresponding author. The ECAS-CI is likewise a caregiver-report checklist, comprising 13 dichotomous items (i.e., requiring “yes-or-no” answers) falling into the following clusters: disinhibition, apathy, loss of sympathy/empathy, perseveration, altered eating habits, and psychosis. The total score on the ECAS-CI ranges from 0 to 13, with higher scores on the ECAS-CI indexing a higher level of behavioral dysfunction. Both the CBQ and the ECAS-CI take no longer than 5 min to be completed.
All patients had been screened for cognitive impairment by the cognitive sections of the Italian ALS-CBS™ (Tremolizzo et al., 2020) and ECAS (Poletti et al., 2016) and assessed for motor-functional outcome via the ALS Functional Rating Scale-Revised (ALSFRS-R) (Cedarbaum et al., 1999).
In addition, out of the whole cohort, N = 98 patients had undergone an in-depth behavioral and psychopathological assessment via the Frontal Behavioural Inventory (FBI) (Alberici et al., 2007), Dimensional Apathy Scale (DAS) (Santangelo et al., 2017), State and Trait Anxiety Inventory-Form Y (STAI-Y1 and STAI-Y2—for the state and trait anxiety, respectively) (Spielberger et al., 1971), and Beck Depression Inventory (BDI) (Beck et al., 1961). The scores on such scales were addressed to further test the construct validity of the CBQ (Sect. 2.3.1).
Analyses were performed using R 4.11 and jamovi 2.3 software.2 The significance level was set at α = 0.05.
In patients, internal reliability and factorial validity of the CBQ were tested by McDonald’s ω and principal component analysis (PCA), respectively. Construct validity of the CBQ was assessed against ECAS-CI, FBI, DAS, STAI-Y1/-Y2, and BDI scores by means of Bonferroni-corrected Spearman’s correlations—because the vast majority of such measures were not distributed normally (i.e., skewness and kurtosis values >|1| and |3|, respectively) (Kim, 2013). The minimum sample sizes for internal reliability and construct validity analyses were set at N = 20 and N = 80, respectively, in agreement with Hobart et al.’s (2012) recommendations—which are specific to the standardization of psychometric scales within clinical neurological research. As far as the sample size for the PCA, Kyriazos’ (2018) empirical rule was referred to, according to which N = 100 observations are sufficient to run such an analysis.
In patients, the diagnostic properties of the CBQ—that is, sensitivity, specificity, positive and negative predictive values (PPV; NPV), and positive and negative likelihood ratios (LR +; LR–)—were computed, through a receiver-operating characteristics (ROC) analysis, at the optimal cutoff identified via Youden’s J statistic. An above-cutoff ECAS-CI score (Poletti et al., 2022) was addressed as the positive state (i.e., the presence of behavioral changes). In ROC analysis, the minimum sample size was set at N = 82, by forecasting a prevalence of up to 50% of patients with an above-cutoff ECAS-CI (i.e., allocation ratio of 1; 41 patients with an above- vs. below-cutoff ECAS-CI) (Strong et al., 2017), an AUC = 0.7, α = 0.05, and 1–β = 0.95 (Goksuluk et al., 2016).
Case–control discrimination of the CBQ was tested through a logistic regression (LR) that regarded the group as the dichotomous outcome (i.e., patients vs. HCs). Within such a model, age, education, and sex were entered as covariates—since the two groups were not matched for such variables [age: t(361) = 8.67; p < 0.001; education: t(361) = –3.70; p < 0.001; sex: χ2(1) = 7.68; p = 0.006].
In order to test whether demographic (i.e., age, education, and sex) or disease-related confounders (i.e., disease duration, ALSFRS-R scores, and presence of C9orf72 hexanucleotide repeat expansion) affected CBQ scores, a negative binomial regression (NBR) (Aiello et al., 2020) was run by covarying for cognition (i.e., ECAS scores) and psychopathological features (i.e., STAI-Y1, STAI-Y2, and BDI scores). A reversed CBQ (computed as 45-CBQ scores) was addressed as the outcome within the NBR in order for the data to fit the underlying probability distribution. Indeed, the CBQ proved to be heavily left-skewed and overdispersed; by reversing its scale, a right-skewed, overdispersed empirical distribution yielded, which could be thereupon modeled by the negative binomial; this allowed the transformed variable to keep the original metric and thus operationalization of the outcome measure (Aiello et al., 2020). Such an expedient already proved to be effective in circumventing ceiling/floor effects and high inter-individual variability in behavioral scores (Iazzolino et al., 2022; Poletti et al., 2022).
Table 1 shows the participants’ backgrounds and neuropsychological measures.
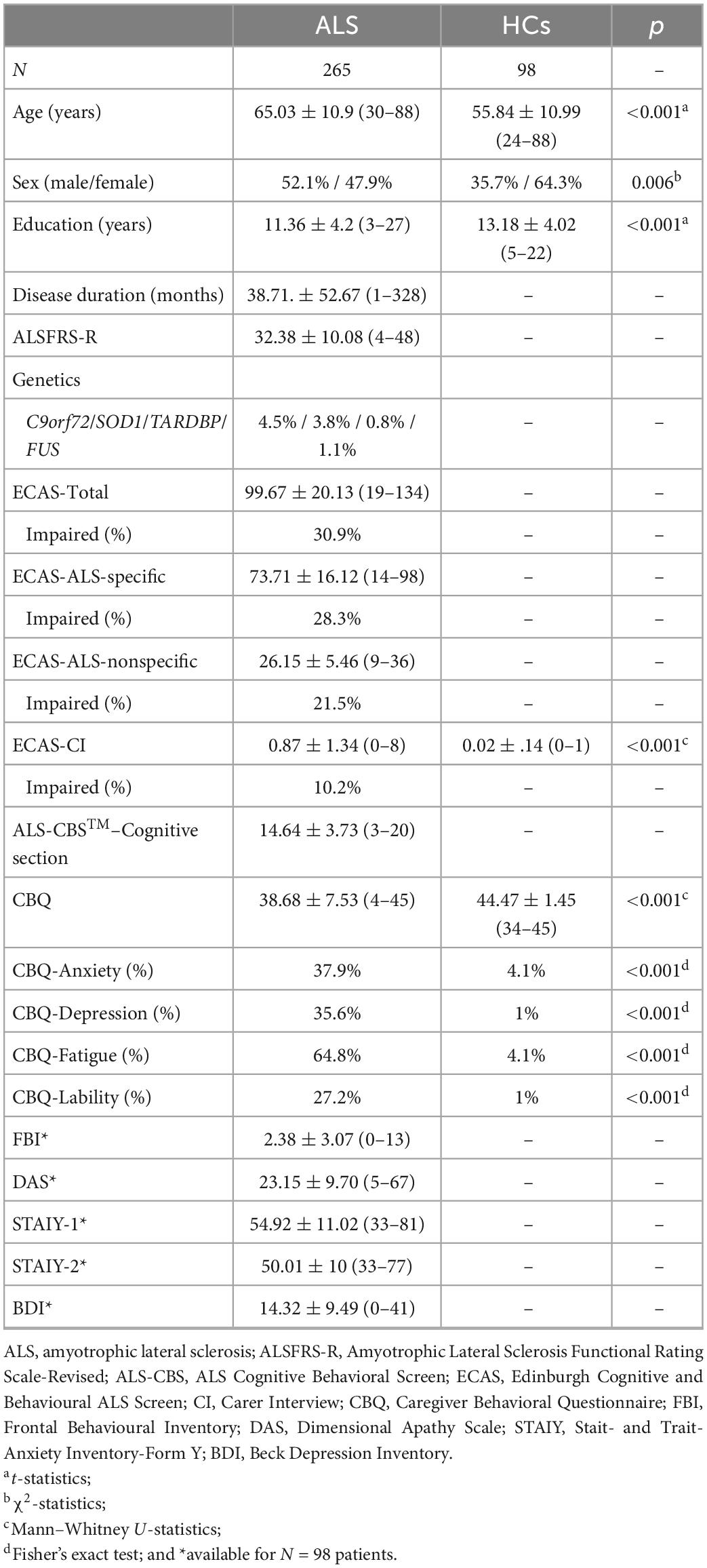
Table 1. Participants’ background and neuropsychological features.
In patients, the CBQ proved to be underpinned by a simple, mono-component structure (43.2% of variance explained) with no interstitial items (loading range = 0.46–0.79), as well as to be internally reliable (McDonald’s ω = 0.90). At αadjusted = 0.008, CBQ scores were strongly associated with the FBI [rs(98) = –0.80; p < 0.001] and ECAS-CI [rs(98) = –0.59; p < 0.001], moderately with the DAS [rs(98) = –0.34; p < 0.001], but not with STAI-Y1[rs(98) = –0.18; p = 0.0850], STAI-Y2 [rs(98) = –0.20; p = 0.052], and BDI scores [rs(98) = –0.21; p = 0.036].
Twenty-seven out of 265 patients presented with behavioral dysfunctions according to the ECAS-CI (10.2%). At the optimal cutoff of ≤ 33 (J = 0.6), the CBQ proved to be highly accurate [AUC = 0.85; SE = 0.04; 95% CI (0.78, 0.92)] (Figure 1), as well as to be featured by optimal error-based (sensitivity = 0.74; specificity = 0.86) and information-based diagnostics (PPV = 0.37; NPV = 0.97; LR + = 5.19; LR- = 0.30). A total of 20.4% of patients (54 out of 265) were classified as behaviorally dysfunctional by such a cutoff.
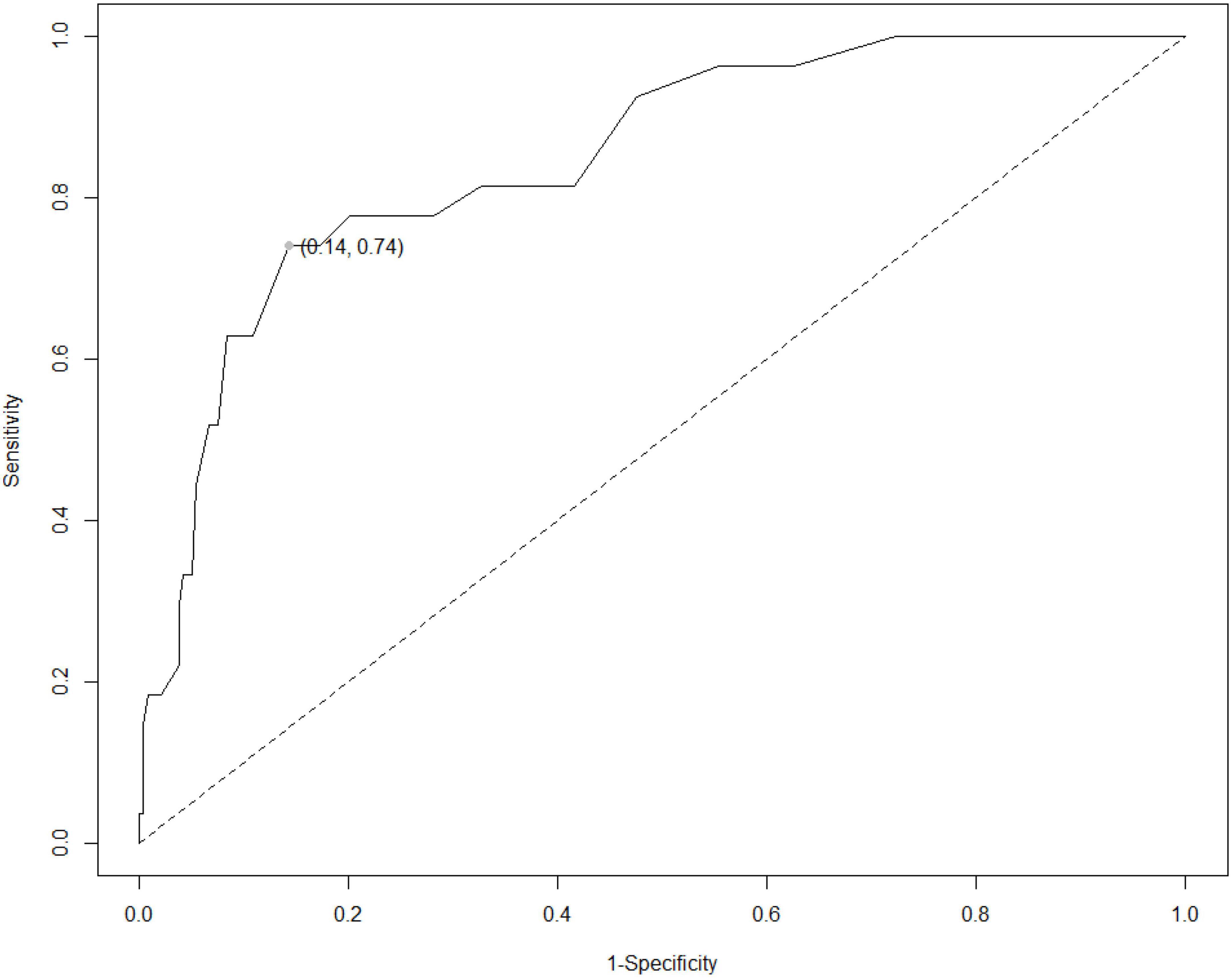
Figure 1. ROC curve for the CBQ against an above-cutoff value on the ECAS-CI. ROC, receiver-operating characteristics; ECAS-CI, Edinburgh Cognitive and Behavioural ALS Screen; CBQ, Caregiver Behavioral Questionnaire. The gray dot index the cutoff value identified via Youden’s index [≤ 33; J = 0.6; AUC = 0.85; SE = 0.04; 95% CI (0.78;0.92)]. The graphical representation was implemented by means of the R package reportROC (https://cran.r-project.org/web/packages/reportROC/reportROC.pdf).
Net of ECAS, STAI-Y1, STAI-Y2, and BDI scores, the NBR revealed that no demographic or disease-related features affected CBQ scores in patients [χ2(1) ≤ 2.2; p ≥ 0.138].
Net of age, education, and sex, the LR revealed that CBQ scores effectively discriminated patients from HCs [b = –0.5; p < 0.001; OR = 0.61, 95% CI (0.51;0.73)] with a classification accuracy of 82.4%.
The present study provides Italian practitioners and clinical researchers with the standardization of the CBQ from the ALS-CBS™ in non-demented patients with ALS. The CBQ proved to be (1) internally reliable, (2) underpinned by a unidimensional structure, (3) both convergently and divergently valid, (4) diagnostically sound, and (5) able to discriminate patients from HCs.
With regard to constructing validity, it is noteworthy that the CBQ selectively converged with dysexecutive behavioral features—as measured by the FBI, ECAS-CI, and DAS—by nonetheless diverging from psychopathological features—that is, STAI-Y1/STAI-Y2 and BDI scores. Moreover, the CBQ proved to be able to discriminate patients with ALS from HCs and to be independent of demographic and disease-related features. Interestingly, within the original, English study, similar findings have been detected: (1) convergent validity of the CBQ, (2) its independence of background confounders, and (3) its case–control discrimination (Woolley et al., 2010).
As far as the diagnostics is concerned, both error- and information-based properties proved to be optimal, with the exception of a poor PVV. However, it should be borne in mind that predictive values are prevalence-based metrics, with the PPV and NPV being directly and inversely related to the proportion of positive states within the study sample, respectively (Bossuyt, 2010). Therefore, given the low prevalence of the above-cutoff ECAS-CI scores, a low PPV was expected. By contrast, as not being based on disease prevalence, likelihood ratios are more generalizable and should be, thus, given more confidence by users when compared to predictive values themselves (Bossuyt, 2010).
Moreover, it is noteworthy that the cutoff herewith derived is relatively close to the original threshold proposed by Woolley et al. (2010) for differentiating non-demented patients with ALS without from those with behavioral involvement, that is, ≤ 36—which was featured, similarly to the results of the present investigation, by optimal diagnostics (accuracy = 86%; sensitivity = 0.82; specificity = 0.86; PPV = 0.82; NPV = 0.92).
This study is of course not exhaustive of all clinimetric and feasibility features that should be tested for a given behavioral screener (Aiello et al., 2022). First, evidence on test–retest and inter-rater reliability, as well as on criterion validity, is still lacking and, thus, needs to be addressed by future investigations. Moreover, within the present study, patients were not classified according to Strong et al. (2017) criteria: Hence, further studies are needed to test whether the CBQ is sensitive to the severity of behavioral dysfunction across the ALS-FTD spectrum—as defined according to the abovementioned nosographic system. Finally, it is advisable that the longitudinal feasibility of the CBQ be also tested—especially in light of the facts that the English version of the CBQ proved effective to track involutionary trends in behavior over time in patients with ALS (Woolley et al., 2018) and that behavioral functioning is acknowledged to worsen with disease progression (Consonni et al., 2021).
In conclusion, the CBQ is a valid, reliable, diagnostically sound, and feasible screener for behavioral dysfunctions in non-demented patients with ALS. Its adoption is, thus, recommended within clinical practice and research in the view of providing preliminary information on whether the administration of more extensive behavioral instruments currently available in Italy (Aiello et al., 2022) is needed.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of IRCCS Istituto Auxologico Italiano (I.D.: 2013_06_25), by the Ethics Committee of Milano Niguarda Area 3 (I.D.: 393-09062021) and by the Ethics Committee of Istituti Clinici Scientifici Maugeri IRCCS (I.D.: CE 2495-12012021). The patients/participants provided their written informed consent to participate in this study.
EA: conceptualization, analyses, drafting, and revision. FS and LG: data collection, drafting, and revision. ALT: analyses and revision. ST, LC, CM, AD, EC, SM, DP, AR, AL, JC, and FC: data collection and revision. AB, AC, SW, JM, LT, IA, FV, VAS, CL, VS, and NT: resources and revision. BP: conceptualization, drafting, revision and resources. All authors contributed to the article and approved the submitted version.
This research was funded by the Italian Ministry of Health to IRCCS Istituto Auxologico Italiano (Ricerca Corrente, project 23C302). Publication fees have been covered by IRCCS Istituto Auxologico Italiano.
We are thankful to patients and their caregivers, as well as to healthy participants.
VS received compensation for consulting services and/or speaking activities from AveXis, Cytokinetics, Italfarmaco, Liquidweb S.r.l., and Novartis Pharma AG and receives or has received research supports from the Italian Ministry of Health, AriSLA, and E-Rare Joint Transnational Call. He is in the Editorial Board of Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, European Neurology and the American Journal of Neurodegenerative Diseases. BP and LC received compensation for consulting services and/or speaking activities from Liquidweb S.r.l. NT received compensation for consulting services from Amylyx Pharmaceuticals and Zambon Biotech SA. CL received compensation for consulting services and/or speaking activities from Cytokinetics, Italfarmaco, and Mitsubishi Tanabe Pharma Europe. VAS participates in Advisory Boards or teaching activities for Biogen, Roche, Avexis, PTC, Santhera, Sarepta, and Dyne. SW is employed by Syneos Health. Additionally, SW receives licensing fees when the ALS Cognitive Behavioural Screen (ALS-CBS™) is used in pharmaceutical trials. JM is employed full time at Biogen. JM does not receive compensation related to the ALS-CBS™.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aiello, E. N., Depaoli, E. G., and Gallucci, M. (2020). Usability of the negative binomial model for analyzing ceiling and highly-inter-individually-variable cognitive data. Neurol. Sci. 41, S273–S274.
Aiello, E. N., D’Iorio, A., Montemurro, S., Maggi, G., Giacobbe, C., Bari, V., et al. (2022). Psychometrics, diagnostics and usability of Italian tools assessing behavioural and functional outcomes in neurological, geriatric and psychiatric disorders: a systematic review. Neurol. Sci. 43, 6189–6214. doi: 10.1007/s10072-022-06300-8
Alberici, A., Geroldi, C., Cotelli, M., Adorni, A., Calabria, M., Rossi, G., et al. (2007). The frontal behavioural inventory (Italian version) differentiates frontotemporal lobar degeneration variants from Alzheimer’s disease. Neurol. Sci. 28, 80–86. doi: 10.1007/s10072-007-0791-3
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., and Erbaugh, J. (1961). An inventory for measuring depression. Arch. General Psychiatry 4, 561–571. doi: 10.1001/archpsyc.1961.01710120031004
Beswick, E., Park, E., Wong, C., Mehta, A. R., Dakin, R., Chandran, S., et al. (2021). A systematic review of neuropsychiatric and cognitive assessments used in clinical trials for amyotrophic lateral sclerosis. J. Neurol. 268, 4510–4521. doi: 10.1007/s00415-020-10203-z
Bossuyt, P. M. (2010). Clinical validity: defining biomarker performance. Scand. J. Clin. Lab. Invest. 70, 46–52. doi: 10.3109/00365513.2010.493383
Brooks, B. R., Miller, R. G., Swash, M., and Munsat, T. L. (2000). El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis Motor Neuron Disord. 1, 293–299. doi: 10.1080/146608200300079536
Cedarbaum, J. M., Stambler, N., Malta, E., Fuller, C., Hilt, D., Thurmond, B., et al. (1999). The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. J. Neurol. Sci. 169, 13–21. doi: 10.1016/S0022-510X(99)00210-5
Consonni, M., Dalla Bella, E., Bersano, E., and Lauria, G. (2021). Cognitive and behavioural impairment in amyotrophic lateral sclerosis: a landmark of the disease? a mini review of longitudinal studies. Neurosci. Lett. 754:135898. doi: 10.1016/j.neulet.2021.135898
Feldman, E. L., Goutman, S. A., Petri, S., Mazzini, L., Savelieff, M. G., Shaw, P. J., et al. (2022). Amyotrophic lateral sclerosis. Lancet 400, 1363–1380. doi: 10.1016/S0140-6736(22)01272-7
Goksuluk, D., Korkmaz, S., Zararsiz, G., and Karaagaoglu, A. E. (2016). easyROC: an interactive web-tool for ROC curve analysis using R language environment. R. J. 8, 213–230. doi: 10.32614/RJ-2016-042
Gorno-Tempini, M. L., Hillis, A. E., Weintraub, S., Kertesz, A., Mendez, M., Cappa, S. F., et al. (2011). Classification of primary progressive aphasia and its variants. Neurology 76, 1006–1014. doi: 10.1212/WNL.0b013e31821103e6
Gosselt, I. K., Nijboer, T. C., and Van Es, M. A. (2020). An overview of screening instruments for cognition and behavior in patients with ALS: selecting the appropriate tool for clinical practice. Amyotrophic Lateral Sclerosis Frontotemporal Degenerat. 21, 324–336. doi: 10.1080/21678421.2020.1732424
Gray, D., and Abrahams, S. (2022). International evaluation of current practices in cognitive assessment for motor neurone disease. Br. J. Neurosci. Nursing 18, 38–44. doi: 10.12968/bjnn.2022.18.1.38
Greco, L. C., Lizio, A., Casiraghi, J., Sansone, V. A., Tremolizzo, L., Riva, N., et al. (2022). A preliminary comparison between ECAS and ALS-CBS in classifying cognitive–behavioural phenotypes in a cohort of non-demented amyotrophic lateral sclerosis patients. J. Neurol. 269, 1899–1904. doi: 10.1007/s00415-021-10753-w
Hobart, J. C., Cano, S. J., Warner, T. T., and Thompson, A. J. (2012). What sample sizes for reliability and validity studies in neurology? J. Neurol. 259, 2681–2694. doi: 10.1007/s00415-012-6570-y
Huynh, W., Ahmed, R., Mahoney, C. J., Nguyen, C., Tu, S., Caga, J., et al. (2020). The impact of cognitive and behavioral impairment in amyotrophic lateral sclerosis. Exp. Rev. Neurotherapeut. 20, 281–293. doi: 10.1080/14737175.2020.1727740
Iazzolino, B., Pain, D., Laura, P., Aiello, E. N., Gallucci, M., Radici, A., et al. (2022). Italian adaptation of the Beaumont Behavioral Inventory (BBI): psychometric properties and clinical usability. Amyotrophic Lateral Sclerosis Frontotemporal Degenerat. 23, 81–86. doi: 10.1080/21678421.2021.1946085
Kim, H. Y. (2013). Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restorat. Dentistry Endodont. 38, 52–54. doi: 10.5395/rde.2013.38.1.52
Kyriazos, T. A. (2018). Applied psychometrics: sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology 9:2207. doi: 10.4236/psych.2018.98126
Poletti, B., Aiello, E. N., Solca, F., Torre, S., Carelli, L., Ferrucci, R., et al. (2022). Diagnostic properties of the Italian ECAS Carer Interview (ECAS-CI). Neurol. Sci. Online ahead of print. doi: 10.1007/s10072-022-06505-x
Poletti, B., Solca, F., Carelli, L., Madotto, F., Lafronza, A., Faini, A., et al. (2016). The validation of the Italian Edinburgh cognitive and behavioural ALS screen (ECAS). Amyotrophic Lateral Sclerosis Frontotemporal Degenerat. 17, 489–498. doi: 10.1080/21678421.2016.1183679
Rascovsky, K., Hodges, J. R., Knopman, D., Mendez, M. F., Kramer, J. H., Neuhaus, J., et al. (2011). Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 134, 2456–2477. doi: 10.1093/brain/awr179
Santangelo, G., Raimo, S., Siciliano, M., D’Iorio, A., Piscopo, F., Cuoco, S., et al. (2017). Assessment of apathy independent of physical disability: validation of the dimensional apathy scale in Italian healthy sample. Neurol. Sci. 38, 303–309. doi: 10.1007/s10072-016-2766-8
Simon, N., and Goldstein, L. H. (2019). Screening for cognitive and behavioral change in amyotrophic lateral sclerosis/motor neuron disease: a systematic review of validated screening methods. Amyotrophic Lateral Sclerosis Frontotemporal Degenerat. 20, 1–11. doi: 10.1080/21678421.2018.1530264
Spielberger, C. D., Gonzalez-Reigosa, F., Martinez-Urrutia, A., Natalicio, L. F., and Natalicio, D. S. (1971). The state-trait anxiety inventory. Int. J. Psychol. 5, 145–158.
Strong, M. J., Abrahams, S., Goldstein, L. H., Woolley, S., Mclaughlin, P., Snowden, J., et al. (2017). Amyotrophic lateral sclerosis-frontotemporal spectrum disorder (ALS-FTSD): revised diagnostic criteria. Amyotrophic Lateral Sclerosis Frontotemporal Degenerat. 18, 153–174. doi: 10.1080/21678421.2016.1267768
Tremolizzo, L., Lizio, A., Santangelo, G., Diamanti, S., Lunetta, C., Gerardi, F., et al. (2020). ALS Cognitive Behavioral Screen (ALS-CBS): normative values for the Italian population and clinical usability. Neurol. Sci. 41, 835–841. doi: 10.1007/s10072-019-04154-1
Woolley, S., Goetz, R., Factor-Litvak, P., Murphy, J., Hupf, J., Lomen-Hoerth, C., et al. (2018). Longitudinal screening detects cognitive stability and behavioral deterioration in ALS patients. Behav. Neurol. 2018:5969137. doi: 10.1155/2018/5969137
Keywords: ALS Cognitive Behavioral Screen, amyotrophic lateral sclerosis, behavior, frontotemporal degeneration, dysexecutive
Citation: Aiello EN, Solca F, Greco LC, La Tona A, Torre S, Carelli L, Morelli C, Doretti A, Colombo E, Messina S, Pain D, Radici A, Lizio A, Casiraghi J, Cerri F, Brugnera A, Compare A, Woolley S, Murphy J, Tremolizzo L, Appollonio I, Verde F, Sansone VA, Lunetta C, Silani V, Ticozzi N and Poletti B (2023) Standardization of the Italian ALS-CBS™ Caregiver Behavioral Questionnaire. Front. Psychol. 13:1107001. doi: 10.3389/fpsyg.2022.1107001
Received: 24 November 2022; Accepted: 22 December 2022;
Published: 20 January 2023.
Edited by:
Silvia Paola Caminiti, San Raffaele Scientific Institute (IRCCS), ItalyReviewed by:
Fabiola De Marchi, Azienda Ospedaliero Universitaria Maggiore della Carità, ItalyCopyright © 2023 Aiello, Solca, Greco, La Tona, Torre, Carelli, Morelli, Doretti, Colombo, Messina, Pain, Radici, Lizio, Casiraghi, Cerri, Brugnera, Compare, Woolley, Murphy, Tremolizzo, Appollonio, Verde, Sansone, Lunetta, Silani, Ticozzi and Poletti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Poletti,  Yi5wb2xldHRpQGF1eG9sb2dpY28uaXQ=; orcid.org/0000-0003-4398-2051
Yi5wb2xldHRpQGF1eG9sb2dpY28uaXQ=; orcid.org/0000-0003-4398-2051
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.