 Yu-Fang Guo
Yu-Fang Guo Xin-Xin Wang2
Xin-Xin Wang2- 1School of Nursing and Rehabilitation, Shandong University, Jinan, Shandong, China
- 2Clinical Psychology Department, Peking University Sixth Hospital, Beijing, China
- 3Department of Critical Care Medicine, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, China
- 4Committee of the Communist Youth League, Shandong University, Jinan, Shandong, China
Aims: To develop a feasible and effective nurse-manager dualistic intervention program to support nurses coping with burnout symptoms.
Background: Person-organization combined interventions were recommended as the most effective approach for reducing burnout symptoms. However, few interventions have been developed in the nursing field.
Methods: The Medical Research Council, United Kingdom (MRC UK), Framework for Development and Evaluation of Complex Interventions, was employed for nurse-manager dualistic intervention program development. The following three steps were followed for developing the dualistic intervention program: (1) identifying the evidence base by conducting extensive reviews of the relevant literature and a mixed study; (2) identifying/developing a theory by selecting the job demands-resources model and proposing the theoretical framework for intervention development; and (3) modifying the process and outcomes of the nurse-manager dualistic intervention program.
Results: The intervention program consists of six group sessions over 9 weeks. Researchers/managers are supposed to deliver the program. The main contents of the intervention are (1) inception (session 1); (2) discovery (session 2); (3) dream (session 3); (4) design (session 4); (5) destiny (session 5); and (6) keep (session 6). The emphasis of the intervention is on helping nurses dealing with burnout symptoms.
Conclusion: Following the guidance of the MRC framework, a feasible and potentially effective nurse-manager dualistic intervention program was developed for nurses coping with burnout. Future studies are needed to model the intervention and assess the effects and replicability of the intervention.
Introduction
Burnout is a psychological response to chronic work-related stress that is characterized by emotional exhaustion, cynicism, and reduced professional accomplishment. According to Leiter and Maslach (2004), a chronic mismatch between a person and an organization plays a key role in burnout development. The severe conflict between personal and organizational values negatively influences job involvement, decision-making participation, and organizational identification, which, in turn, leads to burnout (Leiter and Maslach, 2004). As one of the most important psychological occupational hazards, burnout develops progressively and negatively affects work attitude and behavior, which causes damages at a personal (e.g., poor work performance, turnover intention, and absence) and organizational level (e.g., low organizational commitment, poor peer supports, and substantial financial costs) (Fish et al., 2022; Li et al., 2022; Shapiro et al., 2022). A growing body of empirical evidence shows that burnout prevalence is high in healthcare professions, especially in the nursing group, with 20%−80% of nurses acknowledging severe burnout symptoms worldwide (Matsuishi et al., 2021; Membrive-Jimenez et al., 2022; Wei et al., 2022). Therefore, it is urgent to develop effective intervention strategies to alleviate nurse burnout, which ultimately contributes to high levels of work passion, work performance, psychological wellbeing, and organizational commitment.
Background
Since the 1980s, numerous studies have been conducted to figure out effective intervention approaches that prevent and alleviate burnout symptoms. According to types, purposes, and target populations of the interventions, researchers normally classify the burnout interventions into one of the following three broad categories: (1) person-directed interventions aim to reduce individuals' burnout experience, usually through promoting their coping skills, acquiring supports from family and organization, or changing negative cognition and behaviors (Dreison et al., 2018); (2) organization-directed interventions concentrate on modifying the organization and job characteristics related to burnout, such as negative work environment, inadequate organizational resources, injustice, and work overload (Edu-Valsania et al., 2022); (3) person-organization combined interventions focus on promoting coping strategies of individuals and employee-driven organizational change via interaction of individuals with organizations and aspects of their job (Awa et al., 2010).
Typical person-directed interventions mainly include classic cognitive-behavioral therapies (e.g., emotional self-regulation, cognitive restructuring, and relaxation), mindfulness training, and physical exercise. Most of the interventions, presented in a workshop or online software, were initiated and determined by the employees themselves, to strengthen their psychological and behavioral states, which were completely outside the organizational problems (Schaufeli and Enzmann, 1998). For example, Bagheri et al. (2019) employed a stress-coping strategy and group cognitive-behavioral therapy on clinical nurses and found that the intervention significantly reduced nurse burnout and the effectiveness lasted after a month. Duarte and Pinto-Gouveia (2016) provided a mindfulness-based intervention on oncology nurses and found a significant decrease in burnout, compassion fatigue, and stress and a significant increase in life satisfaction and self-compassion, with medium to large effect sizes. Semerci et al. (2021) used progressive muscle relaxation exercises on burnout and compassion of nurse managers and found that the intervention significantly alleviates burnout and compassion fatigue of managers.
A further narrative review identified several studies that showed no effect of person-directed interventions on nurse burnout. The nurse-led cognitive-behavioral therapy analyses by Partlak Gunusen et al. (2021) and mindfulness analyses by Wong et al. (2021) did not show any positive effects on nurse burnout. Taken together, since burnout develops idiosyncratically due to person and organization mismatch, the negative effects of organizational conditions on burnout have not been involved in person-directed interventions. Moreover, the effectiveness of person-directed interventions on nurse burnout reduction needs further evidence to be proven. In addition, concerns about the limited long-term effects of person-directed interventions have been raised by researchers and managers (Jensen et al., 2006; Westermann et al., 2014).
Organization-directed interventions involve developing welcoming programs, using rewards and incentives, implementing work-family balance plans and humanizing work schedules, improving job characteristics and leadership of managers, training and coaching employees, and creating supportive environments (Shanafelt and Noseworthy, 2017; DeChant et al., 2019). Kersten et al. (2019) used a dialysis-specific training program (including healthy behavior management, promotion of work characteristics, and organizational resource identification and enhancement) to reduce nurse burnout and found that burnout had improved after the intervention, although the effects were not stable over time and the effect sizes were small. Wei et al. (2017) developed an active intervention, including communication skills, conflict coping strategies, efficacy elevation, working skills, and emotion management, and conducted a randomized control trial on burnout nurses. They found significant decreases in emotional exhaustion and depersonalization in nurses. Kelly et al. (2012) explored the effect of creating a positive organizational culture via Magnet hospital on burnout and found that nurses from Magnet hospital reported lower burnout symptoms than nurses from the non-Magnet hospital. Despite several organization-directed intervention studies reporting positive findings, these interventions do not target specific personal issues, which might lack feasibility for individuals and hardly motivate their subjectivity (Tsutsumi et al., 2009). Furthermore, difficulties in repetitive verification and challenges in the popularization and application of the interventions make it hard to conclude (Dreison et al., 2018).
Person-organization combined interventions are multifaceted, initiated, and determined by both employees and managers. The typical interventions often use stress management with organizational environment improvement (e.g., stress coping strategies with organizational support and psychotherapy with job crafting and time management). A previous systematic review showed that combined intervention approaches were completely different in terms of content, form, duration, and frequency (Pijpker et al., 2019). Adams et al. (2019) used a 2-month cultural change toolkit, including meaningful recognition, shared decision-making, and increased leadership involvement and support, to promote nurse burnout and found a significant burnout reduction after the implementation. Liu et al. (2022) provided a 1-year rational emotional intervention combined with hierarchical management to burnout nurses and found that nurses experienced lower levels of burnout after the intervention. Given the comprehensiveness of combined interventions, it is recommended as the most effective intervention type. However, most of the combined interventions focus on stress reduction and work condition promotion, which hardly tackles the burnout root of the person and organization mismatch issue. In addition, few interventions simultaneously motivate personal strengths and organizational resources to cope with burnout adversity, which impacts the positive attributes and organizational involvement of nurses.
Appreciative inquiry (AI), developed by Cooperrider (1986), is based on a relational constructionist view that places a strong emphasis on human perceptions, social collaboration, and appreciative systems. As a new organizational development intervention, AI seeks innovative ideas from employees and searches for success for employees and their organizations via affirmation, appreciation, and dialogue (Koster and Lemelin, 2009). AI advocates a positive slant of inquiry based on future possibilities instead of problem-based short-term solutions and focuses on positive changes arising from the interaction between employees' language, relationships, and functioning in an organization (Cooperrider and Whitney, 2000, 2005). There are four phases of inquiry cycles that form the process of AI: (1) discovery uses emotional touchpoints and photoelicitation to discover what is working well and appreciate what is the best of what has been; (2) dream envisions what would be the ideal dream for the future; (3) design co-constructs a vision for the ideal future; and (4) destiny plans the work strategies toward the desired vision. Through this 4D (discovery, dream, design, and destiny) cyclical process, AI provides a flexible framework for discovering and utilizing personal strengths and organizational resources to achieve organizational goals. AI has been widely employed in several fields, such as education (Stulz et al., 2021), organization management (Martyn et al., 2019), and healthcare promotion (Shrivastava et al., 2020), and is proven to be an effective method in generating personal growth (Sturm et al., 2020), leadership promotion (Bleich and Hessler, 2016), environment change (Ebert et al., 2020), capacity building (Magnussen et al., 2019), and organizational development (Hilde et al., 2010).
Therefore, taking the intrinsic causes of burnout and the benefits of person-organization combined interventions into account, this study aimed to employ the 4D cycle of AI to develop an AI-based nurse-manager dualistic intervention program to support burnout nurses, guided by the MRC framework for developing and evaluating complex interventions.
Methods
This was an interventional development study. The framework for the development and evaluation of complex interventions developed by MRC, UK, was employed as a stepwise guideline for developing the nurse-manager dualistic intervention program. There are four stages of the MRC framework, namely, development, feasibility/piloting, evaluation, and implementation. In this study, we just reported the development stage of the AI-based nurse-manager dualistic intervention (NMDI) program. The following three steps of the development stage were followed: identifying the evidence base, identifying/developing theory, and modifying processes and outcomes. Table 1 shows the activities we undertook for developing an AI-based NMDI program following the guidelines of the MRC. This study was approved by the Human Research Ethics Committee of the School of Nursing and Rehabilitation, Shandong University (NO. 2020-R-030). Approvals were gained from the two tertiary hospitals in Baoding where the study was carried out.
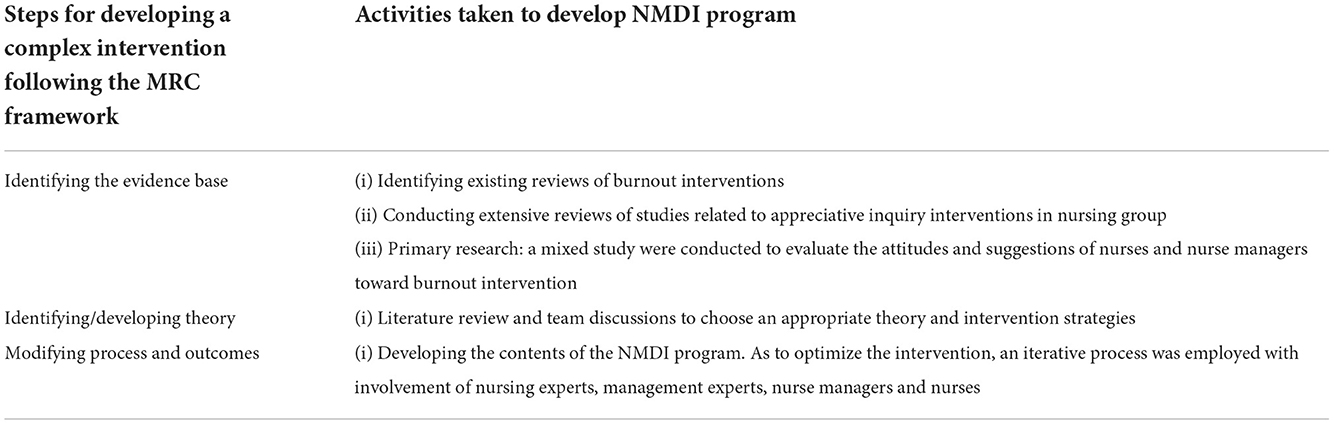
Table 1. Activities for developing NMDI program following the guidelines of the MRC.
Results
The identified evidence base
According to the framework of the MRC, we first identified the evidence base via a systematic review and a mixed study.
Review of interventions to alleviate burnout
A systematic review and meta-analysis of burnout interventions identified 29 studies (Dreison et al., 2018). Of these studies, 21 were organizational-directed interventions, with the subtypes of job training and education, coworker support groups, and clinical supervision; six were personal-directed interventions, and the most common subtype was a stress management workshop; and only two were personal-organizational combined interventions, with the subtypes of a stress management workshop, ongoing workgroups, and organizational consultation. Studies indicated that combined interventions, targeting both personal and organizational factors, were the most effective strategies for decreasing burnout symptoms (Awa et al., 2010; Morse et al., 2012).
Review of appreciative inquiry interventions in the nursing group
To increase our understanding of AI interventions, we conducted extensive reviews related to AI interventions aimed to improve the emotions, behavior, and performance of nurses. These reviews focused on the contents, implementation methods, participants, duration, and outcome measures of interventions. The findings of the review showed that most AI interventions followed the four core components (discover, dream, design, and destiny) to develop the interventions; a group-based method was commonly used to implement the interventions, and nurses were the main participants, with several studies involving managers, doctors, and other health-related professions. The duration of the interventions varied, ranging from 2 days to 2 years. Semi-structured interviews, self-rating questionnaires, work summaries, and work diaries were used as measures to evaluate the work attitude, emotion, behavior, and performance of nurses.
These literature reviews provided some important suggestions on the development of interventions targeting burnout reduction and AI application in nurses: person-organization combined interventions should be developed for alleviating nurse burnout; nurses and nurse managers should be involved in the intervention as a group; four core components of AI should be followed for developing the content of NMDI program; a comprehensive theoretical framework will be needed to guide the development of this multifaceted intervention and evaluate possible change processes.
A mixed study evaluating attitudes and suggestions from nurses and nurse managers toward burnout intervention
A semi-structured face-to-face interview was conducted among nurses and nurse managers to obtain a better understanding of nurses and managers coping with burnout and to evaluate their experiences and suggestions. After a conventional content analysis, three themes and six subthemes were identified. The three themes were as follows: needing help to cope with burnout, burnout intervention measures, and intervention environment.
A quantitative study was conducted to investigate the preference of nurses for burnout intervention. A total of 274 nurses were recruited from two tertiary hospitals. The results showed that over half of the nurses selected a group-based (53.6%) or online-to-offline model of intervention (67.9%), and the roles of managers were advisors and supervisors in the intervention (74.5%). Notably, 38.3% of nurses liked to take burnout interventions in hospitals, 46.0% preferred one time per week of the intervention, and 56.6% of nurses suggested that the length of each section for the intervention should be from 1 to 3 h.
Based on the findings, we drew up a primary conclusion on nurses' experiences of coping and living with burnout and made suggestions for developing effective intervention programs to support burnout nurses. This mixed study showed that nurses struggled with chronic burnout symptoms, that few resources can be used to deal with burnout, and that they had strong preferences in burnout intervention models and implementing forms. These findings not only emphasized the need for burnout interventions in a collaborative nurse-manager combined style but also provided us with valuable information that should be considered in the development of burnout interventions.
Identifying/developing theory
Numerous personal factors (e.g., self-efficacy and self-esteem) and organizational factors (e.g., peer support and job control) are involved in coping with stress and changing existing psychological burnout. Appropriate theories provide an overarching framework for personal and organizational factors that explain why burnout should be targeted by the intervention. Therefore, after a systematic review and a series of team discussions, we chose the job demand-resources model (JD-R) as the theoretical basis for developing our conceptual framework (Demerouti and Bakker, 2011). The model has been shown to predict work-related psychological and behavioral issues in employees (Garcia-Sierra et al., 2016; Hussein, 2018), and it has been used to develop interventions to alleviate stress and promote work engagement (Richard et al., 2012; Makowska-Tiomak et al., 2022).
Bakker and Demerouti (2007) classified two general categories of stress-related factors (job demands and job resources) in JD-R. Job demands are considered the physical, psychological, organizational, and social aspects of the job that require physical and psychological knowledge, skills, and efforts of employees and, therefore, lead to certain physical and psychological costs. Several kinds of job demands have been listed, such as work overload, irregular work arrangements, and an unfavorable working environment. Job resources refer to the physical, psychological, organizational, and social aspects of the job that could be contributing factors for work achievement, job demand reduction, and personal growth. The job resources may be from organizations (e.g., career opportunities, professional training, and salary), the interpersonal relationship (e.g., supervisor, support, and trust), the job position (e.g., role clarity, responsibility, and right), and the task (e.g., task identity, significance, and autonomy). Xanthopoulou et al. (2007) extended the JD-R model by including personal resources (e.g., self-efficacy, organizational-based self-esteem, and optimism) as predictors for exhaustion and work performance. The job demands and resources negatively interact with each other and then affect the development of job-related health impairments and motivation.
In the development of motivation and reduced health/energy, two different underlying psychological processes were found. First, long-term, chronic job demands lead to massive consumption of mental and physical resources by employees and therefore result in health problems (e.g., physical pain and sleep disorders) and energy exhaustion (e.g., burnout). Second, job and personal resources are referred to as motivational factors, which could promote work engagement and work performance of employees, and eliminate cynicism. Studies demonstrated that job and personal resources played intrinsic and extrinsic motivational roles in satisfying the basic needs of employees, such as autonomy, relatedness, competence, and professional development, and ultimately led to positive work attitude and high work engagement (Fullemann et al., 2016; Trepanier et al., 2020; Kato et al., 2021). The JD-R model provides a conceptual basis for the NMDI program with regard to the process of improving job and personal resources and includes seven domains of performance, namely, feedback, job control, supervision and guidance, peer support, self-efficacy, self-esteem, and optimism. Hence, we proposed a theoretical framework for an AI-based NMDI program targeting burnout reduction (Figure 1).
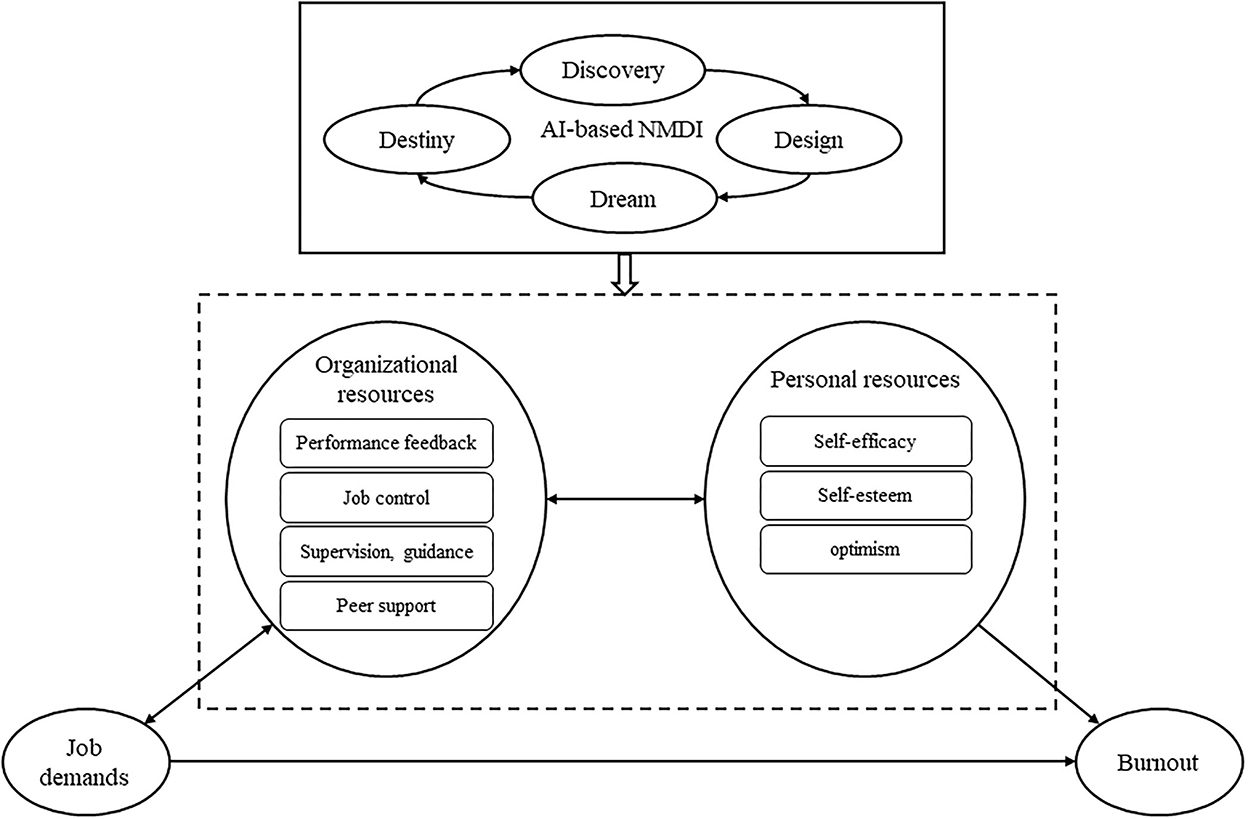
Figure 1. Theoritical framework for AI-based NMDI program targeting in burnout reduction.
According to the theoretical framework for an AI-based NMDI program, the literature review, and the mixed study, the AI-based NMDI program for nurses coping with burnout was developed. The essential components of the NMDI program were discovery (inquire the meaning of the nursing profession, discover an existing job and personal resources of nurses, and help nurses to excavate potential resources that goes unnoticed before), dream (create a nursing dream to change the current status and arouse energy and enthusiasm of nurses), design (construct compelling strategies for turning “dreams” into “reality” and essential elements for resources promotion must be in place), and destiny (practice strategies in normal clinical work with organizational support and share the best practical experience). The detailed contents for the AI-based NMDI programs are listed in Table 2.

Table 2. Titles, aims and contents of the AI-based NMDI program sessions.
The proposed AI-based NMDI program is an online and offline mixed burnout intervention program with five weekly sessions and one 4-week session (destiny). Each weekly session lasts for 120–180 min. While, for the 4-week destiny, each week hold a 60–90 min online meeting. Group intervention was employed in all of the sessions. Each group consists of six–eight participants. Managers (e.g., head nurse, vice director, and director of the nursing department) need to participate in each session of the program.
Outcome measures
All of the outcome measures were selected based on the theoretical framework of the AI-based NMDI program and were intended to be measured at baseline, after the NMDI program intervention, and 3 and 6 months after the intervention. The outcome measures assess the following variables: performance feedback, job control, supervision and guidance, peer support, self-efficacy, self-esteem, optimism, and burnout. All of the measures employed in the study are established scales with good reliability and validity.
The performance feedback, job control, supervision, and guidance of participants are assessed using the work resources subscales of the job demand and work resources scale (Li et al., 2014). The Colleague Support Scale for the nursing group, developed by Ma and Ye (2007), is employed to evaluate the peer support of participants. The 10-item General Self-Efficacy Scale, developed by Schwarzer et al. (1999), is used to evaluate the self-efficacy status of participants. The 3-item subscale of the Psychological Capital Questionnaire (Luthans et al., 2007) is used to measure the optimism of participants. The 10-item Rosenberg Self-Esteem Scale (Vispoel et al., 2001) is used to measure the self-esteem of participants. The Maslach Burnout Inventory-General Survey (Maslach and Jackson, 1981) is used to measure burnout symptoms experienced by participants.
General information on the sociodemographics and characteristics of both participants and hospitals are collected at baseline. The records written by participants and intervenors are collected after the intervention to support the analysis of intervention effects.
Discussion
This study was used to develop an AI-based nurse-manager dualistic intervention program to reduce burnout symptoms among nurses. Following the MRC framework for developing and evaluating complex interventions (Moore et al., 2015; Medical Research Council, 2022), a systematic and iterative procedure used for intervention development was described, which involved three steps identifying the evidence base, identifying/developing theory, and modifying process and outcomes. These were done by gathering extensive existing evidence from reviews of the literature, investigations, and interviews with nurses and nurse managers, and applying the job demand-resources model as a theoretical basis to strengthen the design for the intervention. This AI-based nurse-manager dualistic intervention program should be a feasible and effective intervention.
Our study is the first to address nurse burnout by organizing nurses and nurse managers as a whole to discover and utilize the personal strengths of nurses and hospital resources. Compared with current combined interventions (Rodrigues et al., 2018; Kersten et al., 2019), our study focused more on enhancing the value match between nurses and hospitals. There are six sessions for the AI-based nurse-manager dualistic intervention program, and all sessions are very closely interdependent. For instance, the discovery session, which aims to find out personal strengths and organizational resources, acts interdependently with the dream session to build a positive career dream toward work-related burnout symptoms. According to the 4D cycles of AI (Sandars and Murdoch-Eaton, 2017; AI Commons, 2018), the six sessions (inception, discovery, dream, design, destiny, and keep) have direct interrelationships that advance the process of appreciating, envisioning, and creating a “best” future for nurses and reduce their burnout symptoms.
A pilot study and randomized controlled trial (RCT) are recognized as necessary advancements for developing and assessing a complex intervention. A pilot study of the nurse-manager dualistic intervention program needs to be conducted to test the adequacy of the planned methods and procedures, the fidelity of implementation, and the retention of nurse participants, identify potential confounding factors, and evaluate the underlying mechanism for the intervention. The RCT study is highly recommended to measure the effects, safety, cost-effectiveness, and long-term impacts of the dualistic intervention. In addition, a mixed study incorporating both qualitative and quantitative methods could be adopted for evaluating objective outcomes and subjective attitudes of the participants.
The AI-based nurse-manager dualistic intervention program, developed in accordance with the JD-R model, is intended to eliminate the mismatch between nurses and hospitals via utilizing the personal strengths of nurses and hospital resources, which, in turn, prevent or alleviate nurse burnout. Thus, performance feedback, job control, supervision and guidance, peer support, self-efficacy, self-esteem, optimism, and burnout of nurses were chosen as the key outcomes. The strength of the relationships among the observed variables and a potential mechanism of the intervention are recommended to be analyzed in RCT studies.
Limitations
Using theory to design effective personal-organizational dualistic interventions posed a number of challenges, the biggest being the process of blending personal and organizational-oriented interventions. Moreover, another challenge was promoting the feasibility of the intervention to nurse participants and nurse managers. Future studies are suggested to explore the experiences, concerns, and needs of nurses and nurse managers coping with burnout, which could be used to develop these complex interventions. This study focused on the development of this AI-based NMDI program and the recruitment strategies of participants; the effects and generalizability of the program remain uncertain. Further pilot studies and single-center and multicenter studies are recommended to implement and evaluate this complex intervention.
Conclusion
Following the MRC framework for the development and evaluation of complex interventions, a potentially feasible and effective nurse-manager dualistic intervention program for burnout nurses was developed. Literature reviews, a qualitative and quantitative mixed study, and the job demand-resources model provided the evidence base for intervention development. Future pilot studies and randomized controlled trials need to be employed to evaluate the feasibility, effects, and mechanism of these nurse-manager dualistic intervention programs. Nurses and nurse managers are encouraged to use this dualistic intervention for alleviating burnout after advanced evidence on the effect of the intervention is reported by further studies.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Human Research Ethical Approval (No. 2020-R-030) was obtained from the Human Research Ethics Committee of School of Nursing and Rehabilitation, Shandong University. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Y-FG contributed to the study design, the literature review, data analysis, and writing and revising. X-XW contributed to the literature review, data collection, data analysis, and writing. F-YY and F-YS contributed to data analysis, writing, and revising. MD and Y-NJ contributed to the writing and revising. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the National Natural Science Foundation of China (72004120) and the Natural Science Foundation of Shandong Province (ZR2020QG058).
Acknowledgments
We thank all nurse participants for their involvement in the study and all research team members.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adams, A., Hollingsworth, A., and Osman, A. (2019). The implementation of a cultural change toolkit to reduce nursing burnout and mitigate nurse turnover in the emergency department. J. Emerg. Nurs. 45, 452–456. doi: 10.1016/j.jen.2019.03.004
AI Commons. (2018). Available online at: https://appreciativeinquiry.champlain.edu (accessed September 15, 2022).
Awa, W. L., Plaumann, M., and Walter, U. (2010). Burnout prevention: a review of intervention programs. Patient Educ. Couns. 78, 184–190. doi: 10.1016/j.pec.2009.04.008
Bagheri, T., Fatemi, M. J., Payandan, H., Skandari, A., and Momeni, M. (2019). The effects of stress-coping strategies and group cognitive-behavioral therapy on nurse burnout. Ann. Burns Fire Disasters 32, 184–189.
Bakker, A. B., and Demerouti., E. (2007). The job demands-resources model: state of the art. J. Manag. Psychol. 22, 309–328. doi: 10.1108/02683940710733115
Bleich, M. R., and Hessler, C. (2016). Appreciative inquiry and implementation science in leadership development. J. Contin. Educ. Nurs. 47, 207–209. doi: 10.3928/00220124-20160419-04
Cooperrider, D. (1986). Appreciative Inquiry: Toward a Methodology for Understanding and Enhancing Organizational Innovation [PhD]. Case Western Reserve University, Cleveland, OH.
Cooperrider, D., and Whitney, D. D. (2000). “A positive revolution in change: appreciative inquiry,” in Appreciative Inquiry: Rethinking Human Organization toward a Positive Theory of Change, eds D. Cooperrider, D. Whitney, and T. F. Yaeger (Champaign, FL: Stipes Publishing), 3–26.
Cooperrider, D., and Whitney, D. D. (2005). Appreciative Inquiry: A Positive Revolution in Change. San Francisco, CA: Berrett-Koehler Publishers.
DeChant, P. F., Acs, A., Rhee, K. B., Boulanger, T. S., Snowdon, J. L., Tutty, M. A., et al. (2019). Effect of organization-directed workplace interventions on physician burnout: a systematic review. Mayo Clin. Proc. Innov. Qual. Outcomes 3, 384–408. doi: 10.1016/j.mayocpiqo.2019.07.006
Demerouti, E., and Bakker, A. B. (2011). The job demands-resources model: challenges for future research. SA J. Indust. Psychol. 37, a974. doi: 10.4102/sajip.v37i2.974
Dreison, K. C., Luther, L., Bonfils, K. A., Sliter, M. T., McGrew, J. H., Salyers, M. P., et al. (2018). Job burnout in mental health providers: a meta-analysis of 35 years of intervention research. J. Occup. Health Psychol. 23, 18–30. doi: 10.1037/ocp0000047
Duarte, J., and Pinto-Gouveia, J. (2016). Effectiveness of a mindfulness-based intervention on oncology nurses' burnout and compassion fatigue symptoms: a non-randomized study. Int. J. Nurs. Stud. 64, 98–107. doi: 10.1016/j.ijnurstu.2016.10.002
Ebert, L., Mollart, L., Nolan, S. J., and Jefford, E. (2020). Nurses and midwives teaching in the academic environment: an appreciative inquiry. Nurse Educ. Today 84, 104263. doi: 10.1016/j.nedt.2019.104263
Edu-Valsania, S., Laguia, A., and Moriano, J. A. (2022). Burnout: a review of theory and measurement. Int. J. Environ. Res. Public Health 19, 1780. doi: 10.3390/ijerph19031780
Fish, J. A., Sharplin, G., Wang, L., An, Y., Fan, X. Z., Eckert, M., et al. (2022). Cross-cultural differences in nurse burnout and the relationship with patient safety: an east-west comparative study. J. Adv. Nurs. 78, 100–1011. doi: 10.1111/jan.15024
Fullemann, D., Brauchli, R., Jenny, G. J., and Bauer, G. F. (2016). Individual and group-level job resources and their relationships with individual work engagement. J. Occup. Health 58, 255–268. doi: 10.1539/joh.15-0044-OA
Garcia-Sierra, R., Fernandez-Castro, J., and Martinez-Zaragoza, F. (2016). Relationship between job demand and burnout in nurses: does it depend on work engagement? J. Nurs. Manag. 24, 780–788. doi: 10.1111/jonm.12382
Hilde, H., Gjerberg, E., and Johansen, M. (2010). Effect of the organizational development tool appreciative inquiry [Internet]. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH). Report from Norwegian Knowledge Centre for the Health Services (NOKC) No. 06–2010.
Hussein, S. (2018). Work engagement, burnout and personal accomplishments among social workers: a comparison between those working in children and adults' services in England. Adm. Policy Ment. Health 45, 911–923. doi: 10.1007/s10488-018-0872-z
Jensen, L. D., Gonge, H., Jors, E., Ryom, P., Foldspang, A., Christensen, M., et al. (2006). Prevention of low back pain in female eldercare workers: randomized controlled work site trial. Spine 31, 1761–1769. doi: 10.1097/01.brs.0000227326.35149.38
Kato, Y., Chiba, R., and Shimazu, A. (2021). Work engagement and the validity of job-demands-resources model among nurses in Japan: a literature review. Workplace Health Saf. 69, 323–342. doi: 10.1177/21650799211002471
Kelly, L. A., McHugh, M. D., and Aiken, L. H. (2012). Nurse outcomes in magnet and non-magnet hospitals. J. Nurs. Admin. 42, S44–S49. doi: 10.1097/01.NNA.0000420394.18284.4f
Kersten, M., Vincent-Hoper, S., Krampitz, H., and Nienhaus, A. (2019). Development and evaluation of a training program for dialysis nurses-an intervention study. J. Occup. Med. Toxicol. 14, 3. doi: 10.1186/s12995-019-0223-3
Koster, R. L. P., and Lemelin, R. H. (2009). Appreciative inquiry and rural tourism: a case study from Canada. Tour. Geograp. 11, 256–269. doi: 10.1080/14616680902827209
Leiter, M. P., and Maslach, C. (2004). “Areas of worklife: a structured approach to organizational predictors of job burnout,” in Emotional and Physiological Processes and Positive Intervention Strategies Research in Occupational Stress and Well Being, eds P. Perrewe, and D. C. Ganster, Vol. 3. (Oxford: Elsevier), 91–134. doi: 10.1016/S1479-3555(03)03003-8
Li, J., Huang, R., Shen, Y., and Gao, L. (2014). Job demands-resources model of nurses' job burnout. Chinese J. Clin. Psychol. 5, 881–884. doi: 10.16128/j.cnki.1005-3611.2014.05.074
Li, N., Zhang, L., Li, X., and Lu, Q. (2022). Moderated role of social support in the relationship between job strain, burnout, and organizational commitment among operating room nurses: a cross-sectional study. Int. J. Environ. Res. Public Health 19, 10813. doi: 10.3390/ijerph191710813
Liu, S., Li, X., Yin, X., and Wang, L. (2022). Analysis of the effect of rational emotional intervention combined with hierarchical management mode on improving the psychological stress of emergency nurses and trainee nurses. Emerg. Med. Int. 2022, 2038018. doi: 10.1155/2022/2038018
Luthans, F., Avolio, B. J., Avey, J. B., and Norman, S. M. (2007). Positive psychological capital: measurement and relationship with performance and satisfaction. Pers. Psychol. 60, 541–572. doi: 10.1111/j.1744-6570.2007.00083.x
Ma, C., and Ye, Z. (2007). Study on the co-relationship between fellow support and nurses' job satisfaction. J. Nurs. Train. 22, 1447–1450. doi: 10.16821/j.cnki.hsjx.2007.16.004
Magnussen, I. L., Alteren, J., and Bondas, T. (2019). Appreciative inquiry in a Norwegian nursing home: a unifying and maturing process to forward new knowledge and new practice. Int. J. Qual. Stud. Health Well-being 14, 1559437. doi: 10.1080/17482631.2018.1559437
Makowska-Tiomak, E., Bedynska, S., Skorupska, K., and Paluch, J. (2022). Blended online intervention to reduce digital transformation stress by enhancing employees' resouces in COVID-19. Front. Psychol. 13, 732301. doi: 10.3389/fpsyg.2022.732301
Martyn, J. A., Scott, J., van der Westhuyzen, J. H., Spanhake, D., Zanella, S., Martin, A., et al. (2019). Combining participatory action research and appreciative inquiry to design, deliver and evaluate an interdisciplinary continuing education program for a regional health workforce. Aust. Health Rev. 43, 345–351. doi: 10.1071/AH17124
Maslach, C., and Jackson, S. E. (1981). The measurement of experienced burnout. J. Organ. Behav. 2, 99–103. doi: 10.1002/job.4030020205
Matsuishi, Y., Mathis, B. J., Masuzawa, Y., Okubo, N., Shimojo, N., Hoshino, H., et al. (2021). Severity and prevalence of burnout syndrome in paediatric intensive care nurses: a systematic review. Inters. Criti. Care Nurs. 67, 103082. doi: 10.1016/j.iccn.2021.103082
Medical Research Council. (2022). Developing and Evaluating Complex Interventions: New Guidance. Available online at: http://www.researchgate.net/publication/32899190_Developing_and_Evaluating_Complex_Interventions_New_Guidance_Online (accessed September 15, 2022).
Membrive-Jimenez, M., Velando-Soriano, A., Pradas-Hernandez, L., Gomez-Urquiza, J. L., Romero-Bejar, J. L., Ia Fuente, G. A. C. D., et al. (2022). Prevalence, levels and related factors of burnout in nurse managers: a multi-centre cross-sectional study. J. Nurs. Manag. 30, 954–961. doi: 10.1111/jonm.13575
Moore, G. F., Audrey, S., Barker, M., Bond, L., Bonell, C., Hardeman, W., et al. (2015). Process evaluation of complex interventions: Medical Research Council guidance. BMJ 350, h1258. doi: 10.1136/bmj.h1258
Morse, G., Salyers, M. P., Rollins, A. L., Mpnroe-De Vita, M., and Pfahler, C. (2012). Burnout in mental health services: a review of the problem and its remediation. Adm. Policy Ment. Health 39, 341–352. doi: 10.1007/s10488-011-0352-1
Partlak Gunusen, N., Sengun Inan, F., Ustun, B., Serttas, M., Sayin, S., Toksoy, S. Y., et al. (2021). The effect of a nurse-led intervention program on compassion fatigue, burnout, compassion satisfaction, and psychological distress in nurses: a randomized controlled trial. Perspect. Psychiatr. Care 57, 2014–2023. doi: 10.1111/ppc.12965
Pijpker, R., Vaandrager, L., Veen, E. J., and Koelen, M. A. (2019). Combined interventions to reduce burnout complaints and promote return to work: a systematic review of effectiveness and mediators of change. Int. J. Environ. Res. Public Health 17, 55. doi: 10.3390/ijerph17010055
Richard, G., Lenthall, S., Dollard, M., Opie, T., Knight, S., Dunn, S., et al. (2012). Organisational intervention to reduce occupational stress and turnover in hospital nurses in the Northern Territory, Australia. Collegian 19, 211–221. doi: 10.1016/j.colegn.2012.07.001
Rodrigues, N. P., Cohen, L. L., McQuarrie, S. C., and Reed-Knight, B. (2018). Burnout in nurses working with youth with chronic pain: a pilot intervention. J. Pediatr. Psychol. 43, 382–391. doi: 10.1093/jpepsy/jsx132
Sandars, J., and Murdoch-Eaton, D. (2017). Appreciative inquiry in medical education. Med. Teach. 39, 123–127. doi: 10.1080/0142159X.2017.1245852
Schaufeli, W. B., and Enzmann, D. (1998). The Burnout Companion to Study and Practice. London, UK: Taylor and Francis.
Schwarzer, R., Mueeler, J., and Greenglass, E. (1999). Assessment general perceived self-efficacy of on the internet: data collection in cyber space. Anxiety Stress Coping 3, 145–161. doi: 10.1080/10615809908248327
Semerci, R., Ozturk, G., Kostak, M. A., Elmas, S., Danaci, A. I., Musbeg, S., et al. (2021). The effect of progressive muscle relaxation exercises on compassion satisfaction, burnout, and compassion fatigue of nurse managers. Perspect. Psychiatr. Care 57, 1250–1256. doi: 10.1111/ppc.12681
Shanafelt, T. D., and Noseworthy, J. H. (2017). Executive leadership and physician well-being: nine organizational strategies to promote engagement and reduce burnout. Mayo Clin. Proc. 92, 129–146. doi: 10.1016/j.mayocp.2016.10.004
Shapiro, D., Duquette, C. E., Zangerle, C., Pearl, A., and Campbell, T. (2022). The seniority swoop: young nurse burnout, violence, and turnover intention in an 11-hospital sample. Nurs. Adm. Q. 46, 60–71. doi: 10.1097/NAQ.0000000000000502
Shrivastava, R., Couturier, Y., Girard, F., Bedos, C., Macdonald, M. E., Torrie, J., et al. (2020). Appreciative inquiry in evaluating integrated primary oral health services in Quebec Cree communities: a qualitative multiple case study. BMJ Open 10, e038164. doi: 10.1136/bmjopen-2020-038164
Stulz, V., Francis, L., Pathrose, S., Sheehan, A., and Drayton, N. (2021). Appreciative inquiry as an intervention to improve nursing and midwifery students transitioning into becoming new graduates: an integrative review. Nurse Educ. Today 98, 104727. doi: 10.1016/j.nedt.2020.104727
Sturm, E. C., Mellinger, J. D., Koehler, J. L., and Wall, J. C. H. (2020). An appreciative inquiry approach to the core competencies: taking it from theory to practice. J. Surg. Educ. 77, 380–389. doi: 10.1016/j.jsurg.2019.11.002
Trepanier, S. G., Vallerand, R. J., Menard, J., and Peterson, C. (2020). Job resources and burnout: work motivation as a moderator. Stress Health 36, 433–441. doi: 10.1002/smi.2939
Tsutsumi, A., Nagami, M., Yoshikawa, T., Kogi, K., and Kawakami, N. (2009). Participatory intervention for workplace improvements on mental health and job performance among blue-collar workers: a cluster ramdomized controlled trial. J. Occup. Environ. Med. 51, 554–563. doi: 10.1097/JOM.0b013e3181a24d28
Vispoel, W. P., Boo, J., and Bleiler, T. (2001). Computerized and paper-and-pencil versions of the Rosenberg Self-Esteem Scale: a comparison of psychometric features and respondent preferences. Educ. Psychol. Meas. 61, 461–474. doi: 10.1177/00131640121971329
Wei, H., Aucoin, J., Kuntapay, G. R., Justice, A., Jones, A., Zhang, C., et al. (2022). The prevalence of nurse burnout and its association with telomere length pre and during the COVID-19 pandemic. PLoS ONE 17, e0263603. doi: 10.1371/journal.pone.0263603
Wei, R., Ji, H., Li, J., and Zhang, L. (2017). Active intervention can decrease burnout in Ed nurses. J. Emerg. Nurs. 43, 145–149. doi: 10.1016/j.jen.2016.07.011
Westermann, C., Kozak, A., Harling, M., and Nienhaus, A. (2014). Burnout intervention studies for inpatient elderly care nursing staff: systematic literature review. Int. J. Nurs. Stud. 51, 63–71. doi: 10.1016/j.ijnurstu.2012.12.001
Wong, K. U., Palladino, L., and Langhan, M. L. (2021). Exploring the effect of mindfulness on burnout in a pediatric emergency department. Workplace Health Saf. 69, 467–473. doi: 10.1177/21650799211004423
Keywords: appreciative inquiry, burnout, formative intervention development, nurse, qualitative research, quantitative research
Citation: Guo Y-F, Wang X-X, Yue F-Y, Sun F-Y, Ding M and Jia Y-N (2022) Development of a nurse-manager dualistic intervention program to alleviate burnout among nurses based on the appreciative inquiry. Front. Psychol. 13:1056738. doi: 10.3389/fpsyg.2022.1056738
Received: 29 September 2022; Accepted: 16 November 2022;
Published: 06 December 2022.
Edited by:
Hans Henrik Knoop, Aarhus University, DenmarkReviewed by:
Elsa Vitale, Bari Local Health Authority, ItalyAnnamaria Pakai, University of Pécs, Hungary
Copyright © 2022 Guo, Wang, Yue, Sun, Ding and Jia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu-Fang Guo, Y2RndW95dWZhbmdAMTYzLmNvbQ==
†ORCID: Yu-Fang Guo orcid.org/0000-0002-9763-4119