 Alejandro Arévalo-Martínez
Alejandro Arévalo-Martínez Juan Manuel Moreno-Manso*
Juan Manuel Moreno-Manso* María Elena García-Baamonde
María Elena García-Baamonde Macarena Blázquez-Alonso
Macarena Blázquez-Alonso Pilar Cantillo-Cordero
Pilar Cantillo-Cordero- Department of Psychology, University of Extremadura, Badajoz, Spain
The World Health Organization (WHO), in its last review of its International Classification of Diseases, established a new classification for chronic pain. Among the principal categories, of particular interest is chronic primary pain as a new type of diagnosis in those cases in which the etiology of the disease is not clear, being termed as chronic primary visceral pain when it is situated in the thorax, abdomen, or pelvis. Due to the novelty of the term, the objective of the systematic review was to examine the psychopathological and neuropsychological disorders associated with chronic primary visceral pain. We carried out a search of the scientific literature following the PRISMA directives using the Pubmed, Medline, PsycInfo and Scopus databases. A total of 33 articles were selected after applying the inclusion and exclusion criteria. The analysis of the studies showed that most persons with chronic primary visceral pain suffer from at least one psychological disorder; the most prevalent being anxiety, depressive or somatoform disorders. The most frequent psychopathological symptoms are anxiety, depression and somatization. Similarly, the findings are insufficient to determine the existence of deficits in the domains of executive functioning, memory and intelligence. However, the existence of attention biases does seem to be clear. This review supposes a starting point for conceptualizing chronic primary visceral pain. It is necessary to continue further research so as to obtain a better understanding of this pathology and the disorders associated.
Introduction
Chronic pain is one of the most frequent health problems in the adult population, with a variable prevalence of between 11 and 50% worldwide (De Souza et al., 2017; Andrews et al., 2018; Murray et al., 2021). It is a prolonged and severe multifactorial illness involving biological, psychological, and social factors (Vargas et al., 2018; Korwisi et al., 2021). The World Health Organization (WHO) together with the International Association for the Study of Pain (IASP), in their last review of the International Classification of Diseases (ICD-11), defined chronic pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage. Chronic pain is pain that persists or recurs for longer than 3 months” (World Health Organization, 2018, MG30 Chronic Pain).
The research carried out over the last few decades has provided evidence of the multiple consequences of chronic pain on a psychopathological and neuropsychological level (Fine, 2011; Mills et al., 2019; Cáceres-Matos et al., 2020). From the psychopathological point of view, the presence of chronic pain is associated with a high probability of developing psychological disorders, depression, anxiety and sleep disorders being those that present the greatest co-morbidity (Arango-Dávila and Rincón-Hoyos, 2018; Cáceres-Matos et al., 2020); while from the neuropsychological point of view, the most common cognitive difficulties occur in the domains of attention, memory, intelligence and the executive functioning (Berryman et al., 2014; Corti et al., 2021). Similarly, such variables as age, the presence of anxiety or depression, sleep disorders, the use of medication and the type, intensity, and duration of the pain, among others, would seem to have a significant influence on the cognitive performance of persons suffering from chronic pain (Moriarty et al., 2017; Ojeda et al., 2018).
The integral classification of the ICD-11 allows us to approach chronic pain from a biopsychosocial point of view, establishing seven main diagnostic categories that, in turn, arte subdivided into specific diagnostic subcategories (World Health Organization, 2018; Korwisi et al., 2021). In the first category, called chronic primary pain, no underlying disease or known harmful process can explain the symptoms of the chronic pain; while, in the six remaining categories, called chronic secondary pain, the underlying disease or known harmful process does explain the symptoms of the chronic pain (see Figure 1) (Treede et al., 2019; Korwisi et al., 2021).
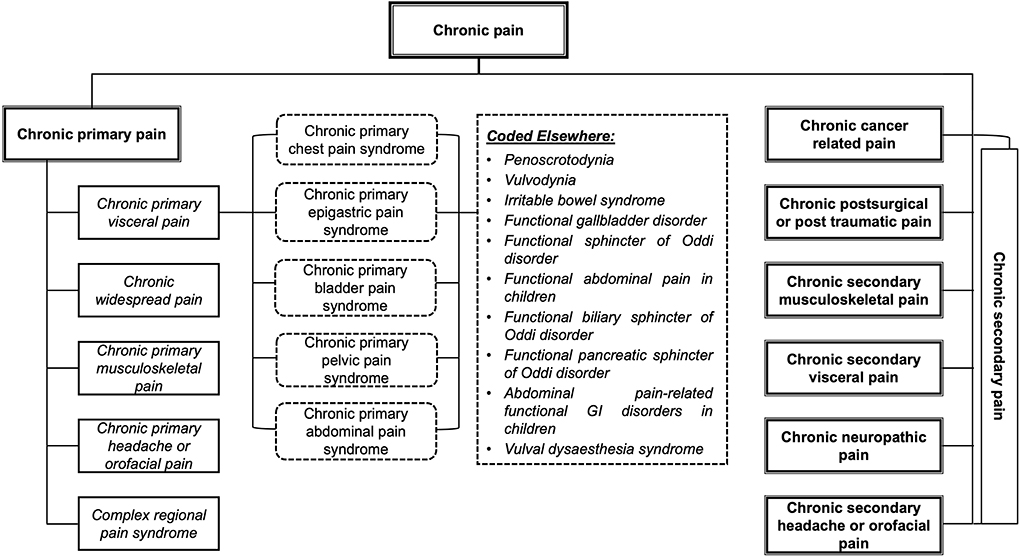
Figure 1. Classification of chronic pain: chronic primary pain and chronic secondary pain. Version adapted from Treede et al. (2019).
Chronic primary pain is a new kind of diagnosis that aims to redress the deficiencies identified in the previous versions of the ICD, allowing a diagnosis when the etiology is not clear, but there is evidence of significant emotional distress and/or functional impairment (Nicholas et al., 2019). It can be defined as chronic pain present in one or various anatomical regions associated with significant emotional distress and/or functional impairment that affect the basic, instrumental, and advanced activities of daily life (World Health Organization, 2018; Treede et al., 2019). It is the result of the interaction between biological, psychological, and social factors, yet it can be diagnosed independently of the influence of the first two, except when a different diagnosis can better explain the symptoms (Nicholas et al., 2019). This approach goes beyond considering chronic primary pain as a symptom and starts to consider it as a health condition or prolonged illness in itself (Nicholas et al., 2019; Treede et al., 2019).
Within the five subcategories of chronic primary pain, chronic primary visceral pain (CPVP) represents an important condition that, as do the other subcategories, negatively affects the life of a person and the different contexts in which that person's life is led, be it social life, family life or work life, and is associated with a low quality of life, as well as problems with both physical and psychological health (Dueñas et al., 2016; Vargas et al., 2018; Cáceres-Matos et al., 2020). In order to define CPVP1, the ICD-11 uses the following criteria (World Health Organization, 2018):
(A) Chronic primary pain.
(B) Situated in the thoracic, abdominal or pelvic regions.
(C) Associated with significant emotional distress and/or functional impairment.
(D) The specific anatomical situation of the pain is compatible with the typical pain coming from specific internal organs.
Although the existing relations between the diagnosis of chronic pain and the development of psychopathological and neuropsychological disorders seem to display sufficient evidence, the conceptualization of chronic primary pain as a new diagnostic category presents numerous practical implications that should be explored. One such implication is the possibility of identifying the disorders on a biological, psychological and social level associated with each one of the diagnostic subcategories and, from there, developing specific multidisciplinary treatments for the existing deficits (Nicholas et al., 2019). In this sense, despite the fact that many works of research have evaluated the psychological disorders associated with chronic pain in an isolated manner (Fine, 2011; Riegel et al., 2014; De Souza et al., 2017; Moriarty et al., 2017; Arango-Dávila and Rincón-Hoyos, 2018; Ojeda et al., 2018; Racine, 2018; Vargas et al., 2018; Corti et al., 2021), neither the systematic reviews nor the meta-analyses currently published (Berryman et al., 2014; Riegel et al., 2014; Dueñas et al., 2016; Mills et al., 2019; Cáceres-Matos et al., 2020) have been able to identify the psychopathological and neuropsychological disorders in each one of the subcategories of chronic primary pain, in accordance with the new classification proposal by the ICD-11.
Thus, the objective of this present review is to critically describe and analyse the works published in the last 10 years concerning the psychopathological and neuropsychological evaluation of CPVP, using the inclusion criteria established by the WHO in the ICD-11 to do so.
Method
Search and inclusion criteria
The bibliographic material was selected from journals, but not PhDs or chapters from books, indexed over the last 10 years (January 2012 – May 2022), in English or Spanish, through the following databases: Pubmed, Medline, PsycInfo and Scopus. Given the existence of different diagnostic subtypes in the CPVP and their relation to the disorders under review, we carried out a combined search using the following terms: (Chronic primary visceral pain OR Chronic visceral pain OR Chronic primary chest pain syndrome OR Chronic primary epigastric pain syndrome OR Chronic primary bladder pain syndrome OR Chronic primary pelvic pain syndrome OR Chronic primary abdominal pain syndrome OR Penoscrotodynia OR Vulvodynia OR Irritable bowel syndrome OR Functional gallbladder disorder OR Functional sphincter of Oddi disorder OR Functional biliary sphincter of Oddi disorder OR Functional pancreatic sphincter of Oddi disorder OR Vulval dysaesthesia syndrome) AND (psychopathology OR mental disorder OR mental illness OR neuropsychology OR neuropsychological test OR neuropsychological assessment OR cognitive impairment OR cognitive dysfunction OR cognitively impaired OR executive function OR cognitive function OR cognitive performance OR memory OR attention).
In order to be included in this review, the publications had to comply with the following additional criteria: (a) they must be empirical works of research evaluating psychopathological and/or neuropsychological disorders in any of the subtypes of CPVP; (b) they must have a sample of adult persons between 18 and 85 years of age; (c) the CPVP must not be the consequence of an illness; (d) the sample must not have additional illnesses; (e) they must use psychological and/or neuropsychological evaluation tests; (f) they must include the results of the psychological and/or neuropsychological evaluation in the base line; (g) they must include the necessary data for determining the existence of psychopathological and/or neuropsychological disorders in the sample.
As exclusion criteria, we discarded: (a) publications in which the abstract made no reference to CPVP or any of the subtypes or the related psychopathological and/or neuropsychological variables; (b) publications that did not specify the subtype of CPVP or in which, when specified, these did not form part of the objectives of the publication.
Codification of the studies
We set out a series of variables concerning the reviewed publications related to the design and methodology of the study: (a) the country in which the research was carried out, (b) the design of the study, (c) the subtypes of CPVP, (d) the existence of a control group and/or other additional groups, (e) the number of participants, (f) the gender and age of the participants, (g) the instruments used to evaluate the CPVP and the psychopathological and neuropsychological disorders, (h) the variables of the CPVP, both psychopathological and neuropsychological, (i) and the results of the evaluation of the CPVP and the psychopathological and neuropsychological disorders.
Results
Selection of the studies and the characteristics
From the results of the bibliographic search, we identified a total of 14,091 articles. After eliminating 1,499 duplicated articles and 11,589 more that were unrelated to the subject matter, we reviewed 1,003 articles based on the title and content of the abstract. Of these, we excluded a further 906 articles as they did not adjust to the objective of the review. A total of 97 articles concerning psychopathological and neuropsychological disorders were taken into consideration for the review, of which 64 were excluded following a reading of the complete text as they did not comply with the inclusion criteria. A total of 33 articles were finally included in the present review. The details are shown in the PRISMA flow diagram of Figure 2.
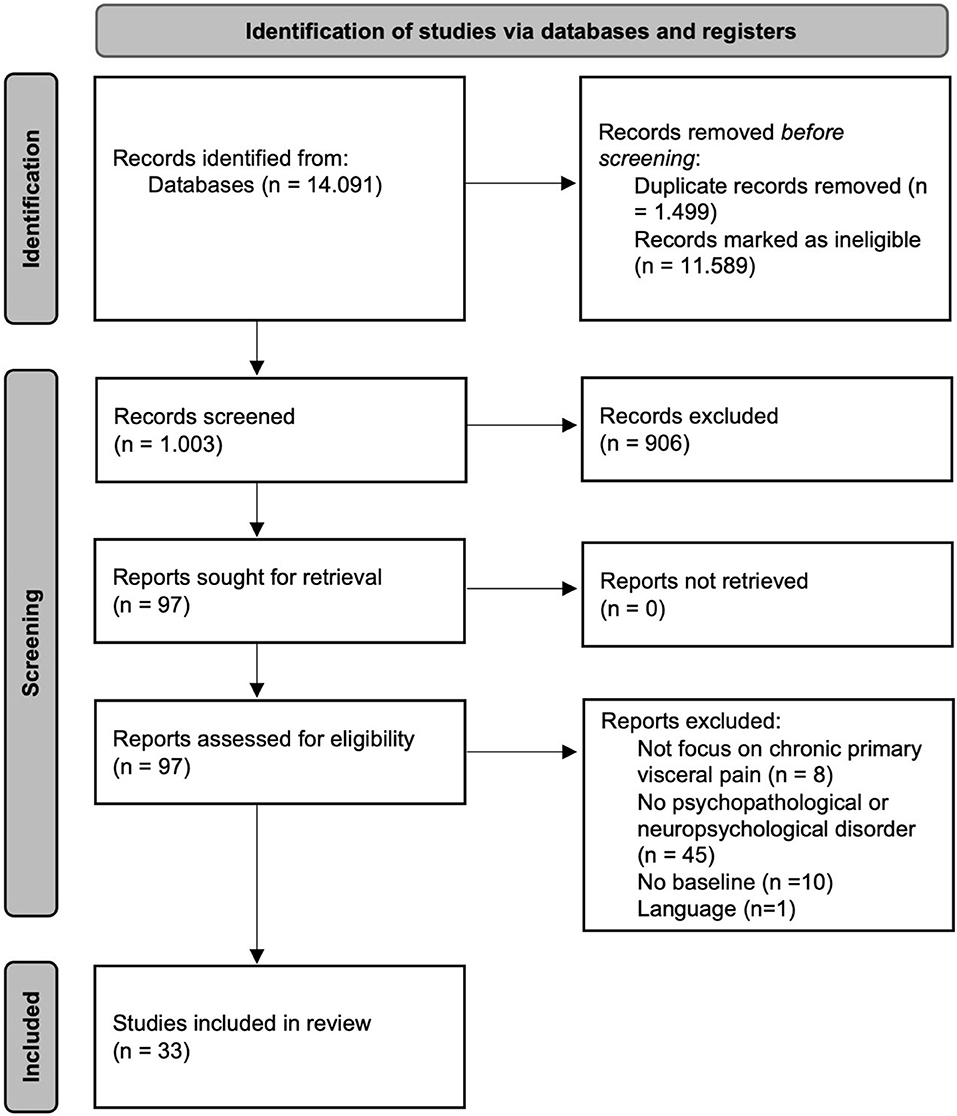
Figure 2. PRISMA flow diagram (Page et al., 2021).
The countries in which the research work of the 33 selected articles was carried out show a high degree of heterogeneity, but the major origins were Germany (15%), the United States (12%), China, India and Italia (9% each). These were followed by Iran, the United Kingdom and Turkey (6% each), as well as Australia, Canada, South Korea, Croatia, France, Ireland, Japan and Norway (3% each).
Design of the study, CPVP subtypes and the existence of a control group and/or additional groups
Table 1 presents the principal characteristics of the articles included in the review. The rest of the variables, referring to psychopathological and neuropsychological disorders respectively, can be seen in Tables 2, 3. The methodological design followed by the majority of the research works is the cross-sectional study (82%), while the rest use a longitudinal study (18%).
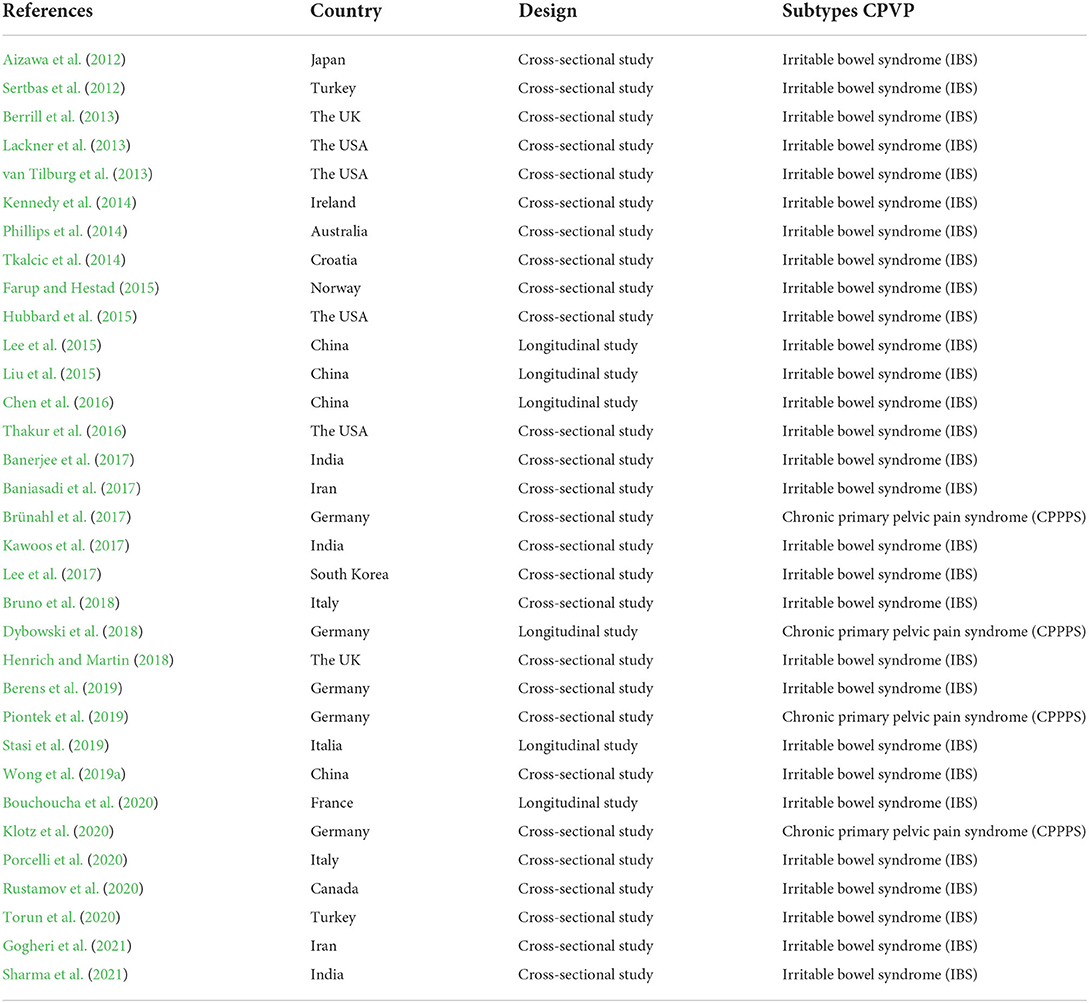
Table 1. Characteristics of the studies included in the review.
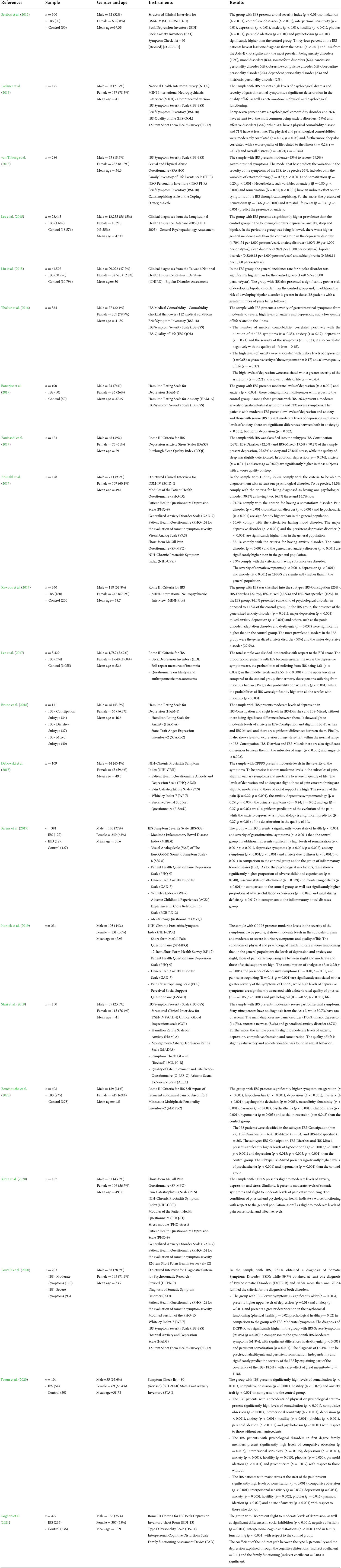
Table 2. Psychopathological disorders.
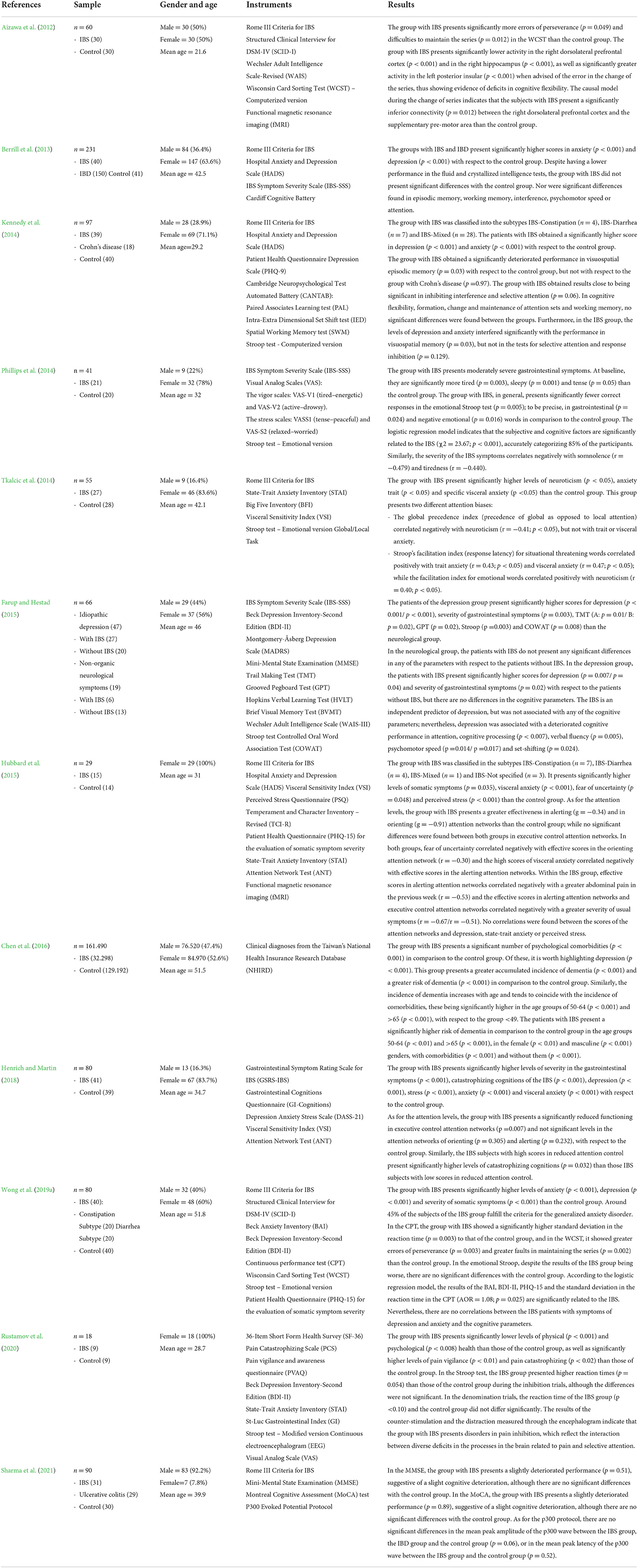
Table 3. Neuropsychological disorders.
The CPVP diagnosis was made by a health professional in a total of 31 articles (94%), and in the other 2 articles, although the research was carried out in the health context, it was not specified. As for the CPVP subtypes present in the review; the dominant one is the irritable bowel syndrome that appears in 29 of the articles (88%), followed by the chronic primary pelvic pain syndrome (12%). Of those studies whose main pathology is the irritable bowel syndrome, 7 of them (23%) classified the sample in accordance with the subtypes IBS-Constipation (32.1%), IBS-Diarrhea (31.8%), IBS-Mixed (29%) and IBS-Not specified (7.1%).
As for the presence of a control group, most of the studies use a healthy control group with no diagnosis (67%), while the rest use only the one group (33%) made up of subjects with the pathologies being investigated. Of the studies with a control group, four (18%) include an additional group with another gastrointestinal pathology to compare with the irritable bowel syndrome, to be precise: inflammatory bowel disease (9%), Crohn's disease (4.5%) and ulcerative colitis (4.5%).
Number, gender and age of the participants
The total number of participants evaluated in the reviewed studies is 255,068, these being 18 participants from the smallest sample (Rustamov et al., 2020) and 161,490 participants from the largest (Chen et al., 2016). The proportion of female (51%) and male (49%) participants is balanced, and the mean age is 40.5 years (SD = 7.9), with a range between 18 and 85 years of age.
It should be stated that those participants diagnosed as suffering from CPVP totalled 69,395 (27.21%) and, as with the total number of participants, the proportion of females (52%) and males (48%) is balanced and the mean age is 40.5 years (SD = 7.9).
Instruments for evaluation and variables of the CPVP, psychopathological and neuropsychological
As can be seen in Tables 2, 3, the instruments used in the reviewed studies present a great variability, with a total of 67 different instruments to evaluate the subtypes of CPVP and the psychopathological and neuropsychological disorders. In general, the Rome III Criteria for IBS (8%), the IBS Symptom Severity Scale (IBS-SSS) (6%), the Beck Depression Inventory (BDI) (4%), the Patient Health Questionnaire Depression Scale (PHQ-9) (4%) and the Stroop test (4%) were the most commonly used instruments. These instruments were used to evaluate a total of 66 different variables, of which the most commonly evaluated were: depression (10%), anxiety (9%), the symptoms of irritable bowel syndrome (6%), the severity of the symptoms of IBS (5%) and the inhibitive capacity (4%).
As for CPVP and its subtypes, a total of 13 of the instruments (19.4%) were aimed at its evaluation; the most commonly used being the Rome III Criteria for IBS (25%), the IBS Symptom Severity Scale (IBS-SSS) (21%), the Pain Catastrophizing Scale (PCS) (10%), the NIH-Chronic Prostatitis Symptom Index (NIH-CPSI) (8%) and the Visual Analog Scale (VAS) (8%). These instruments evaluated a total of 16 different variables (24.2%), the most commonly evaluated being: the symptoms of irritable bowel syndrome (22%), the severity of the symptoms of irritable bowel syndrome (20%), pain catastrophizing (9%), somatic symptoms (9%) and the specific distress of the gastrointestinal symptoms (5%).
As for the psychopathological disorders, 37 of the instruments (55.2%) were aimed at their evaluation, the most commonly used being: the Beck Depression Inventory (BDI) (7%), the Patient Health Questionnaire Depression Scale (PHQ-9) (7%), the Generalized Anxiety Disorder Scale (GAD-7) (6%), the Structured Clinical Interview for DSM-IV (SCID) (6%) and the Hospital Anxiety and Depression Scale (HADS) (5%). These instruments evaluated a total of 25 different variables (37.9%), the most commonly evaluated being: depression (24%), anxiety (22%), psychopathological symptomatology (9%), the quality of life related to health (6%) and the DSM-IV disorders (6%).
As for the neuropsychological disorders, 17 of the instruments (25.3%) were aimed at their evaluation, the most commonly used being: the Stroop test (23%), the Wisconsin Card Sorting Test (WCST) (8%), the Mini-Mental State Examination (MMSE (8%), the Attention Network Test (ANT) (8%) and the Wechsler Adult Intelligence (WAIS) (8%). These instruments evaluated a total of 25 different variables (37.9%), the most commonly evaluated being: attention (33%), inhibition (13%), the processing of information (9%), work memory (6%) and cognitive flexibility (6%).
Results of the evaluation of the CPVP, of the psychopathological and neuropsychological disorders
Chronic primary visceral pain
The severity of the CPVP and its subtypes were evaluated in a total of 18 articles (55%). The majority of the participants with this pathology presented moderate or severe thoracic, abdominal and/or pelvic symptoms. In particular, in the study of Lackner et al. (2013), the severity of the said symptoms was high. Concerning these symptoms, the pain catastrophizing and light to moderate levels of the somatic symptoms related to this disease should be highlighted (each one present in 28% of these articles), as well as the specific distress linked to the gastrointestinal symptoms (present in 17%) and the psychological anxiety also linked to the gastrointestinal symptoms (present in 6%). Other studies evaluated the general state of health (33% of these articles), showing evidence on the whole of a deteriorated physical and psychological functioning. Only Lackner et al. (2013) and Thakur et al. (2016) evaluates the quality of life related to the disease, obtaining a result indicating deterioration as a consequence of the gastrointestinal symptoms.
Psychopathological disorders
The psychopathological disorders of CPVP and its subtypes were evaluated in a total of 28 articles (85%). The psychological disorders with the greatest prevalence in the participants with this pathology, diagnosed in 9 of these articles (33%), were: those of anxiety, to be precise, generalized anxiety disorder (present in 25% of these articles); mood disorders, to be precise, major depressive disorder (present in 18%); and somatoform disorders (present in 14% of these articles); followed by bipolar disorder (present in 7%) and panic disorder, post-traumatic stress disorder, obsessive-compulsive disorder, sleep disorders, substance use disorders, anorexia nervosa, borderline personality disorder, dependent personality disorder, histrionic personality disorder and narcissistic personality disorder (each one present in 4%). It is worth highlighting the study of Liu et al. (2015), which focuses solely on evaluating the overall incidence rate and the risk of suffering bipolar disorder in a population with irritable bowel syndrome; the results were significantly higher than in the general, healthy population.
The psychopathological symptoms with the greatest prevalence in CPVP, evaluated in 22 of these articles (79%), were: moderate levels of anxiety (present in 46% of these articles), depression (present in 39%) and stress (present in 18%), followed by somatization, compulsive obsession, hostility, psychoticism (each one present in 7%) and interpersonal sensitivity, phobias, paranoid ideation, insomnia, anxiety due to illness, adverse childhood experiences, mentalizing deficits, hypochondria, neuroticism, hysteria, social inhibition, interpersonal cognitive distortions and fear of uncertainty (each one present in 4%). Only Lackner et al. (2013), Dybowski et al. (2018) and Piontek et al. (2019) evaluated the quality of life of the participants with this pathology, obtaining as a result a significant deterioration in the said quality of life.
Neuropsychological disorders
The neuropsychological disorders of CPVP and its subtypes were evaluated in a total of 12 articles (36%). The executive functions, evaluated in 11 of these articles (92%), show uneven results. Aizawa et al. (2012) and Wong et al. (2019a), through the Wisconsin Card Sorting Test (WCST), show evidence of deficiencies in cognitive flexibility and in problem solving in the participants with this pathology. They have significantly more errors of permanence and difficulties to maintain the series than the control group; meanwhile, Kennedy et al. (2014), through the Intra-Extra Dimensional Set Shift test (IED), found no significant differences in cognitive flexibility in a comparison of both groups. Kennedy et al. (2014), Phillips et al. (2014) and Wong et al. (2019a), through the Stroop test (computerized and emotional versions), show evidence of deficiencies in response inhibition and cognitive processing of emotional content in the participants with CPVP; meanwhile, Rustamov et al. (2020), through the Stroop test–Modified version, shows for this group insignificant reaction times in inhibition, but still higher than those of the control group. Similarly, Berrill et al. (2013) and Kennedy et al. (2014) found no significant differences in processing speed and work memory, respectively, in comparison to the control group.
Attention, evaluated in 8 of these articles (67%), shows congruent results. Aizawa et al. (2012) and Wong et al. (2019a), through the Wisconsin Card Sorting Test (WCST), show evidence in the participants con CPVP of deficits in this cognitive domain. On evaluating the different attention networks in an individualized manner, Hubbard et al. (2015) and Henrich and Martin (2018), using the Attention Network Test (ANT), showed evidence that the participants with this pathology had a slightly better efficiency in orientation attention networks and warning attention networks (sustained attention) in comparison to the control group; while in the executive control attention networks (selective attention) they showed a reduced functioning in comparison to the control group. These results are coherent with those of Kennedy et al. (2014), Phillips et al. (2014) and Wong et al. (2019a), which showed deficits, though mostly insignificant, in the selective attention of the participants with CPVP.
In intelligence, evaluated in 2 of these articles (17%) using the Wechsler Adult Intelligence Scale (WAIS), despite the fact that there were no significant differences with respect to the control group; there was evidence of a lower performance level in the fluid and crystallized intelligence tests of the participants with CPVP. In memory, evaluated in 2 of these articles (17%), the results were uneven. Kennedy et al. (2014), using the Paired Associates Learning test (PAL), showed evidence in the participants with this pathology of a significantly deteriorated performance in episodic visuospatial memory with respect to the control group; however, Berrill et al. (2013), using the Cardiff Cognitive Battery, showed very similar results in episodic visuospatial memory in both groups.
Chen et al. (2016) evaluate the risk of dementia in CPVP, showing evidence of a greater accumulated incidence of dementia and a greater risk of dementia with the irritable bowel syndrome in comparison to the control group. Similarly, Sharma et al. (2021), using the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA) test, showed evidence of a slight cognitive deterioration in participants with these pathologies in comparison to the control group.
Discussion
The present study has carried out the first systematic review of the psychopathological and neuropsychological disorders associated with CPVP, in accordance with the new conceptualization of chronic pain from the WHO and the International Association for the Study of Pain (IASP) in the last revision of the ICD-11 (World Health Organization, 2018). Following an extensive search in the different databases and verification of their suitability for the objectives of the present study, a total of 33 articles were included in this current review.
In general, the studies that evaluate the severity of this pathology conclude that the severity of the thoracic, abdominal and/or pelvic symptoms is frequently considered to be between moderate and severe. Among those who suffer it, they usually have symptoms of pain catastrophizing, somatic symptoms, anxiety in the face of gastrointestinal symptoms, psychological distress, a deteriorated physical and psychological health and a low quality of life as a consequence of the illness (Lackner et al., 2013; Thakur et al., 2016).
Those articles that evaluate the psychopathological disorders of CPVP present similar results. The majority of the participants evaluated present at least one psychological disorder and a considerable percentage even have two (Lackner et al., 2013; Brünahl et al., 2017; Kawoos et al., 2017), the most common being anxiety disorders, depressive disorders and somatoform disorders. Correspondingly, anxiety, depression, somatization, compulsive obsession, and hostility are to be found among the commonest psychopathological symptoms, with moderate intensities. Examining the existing correlations throughout the articles, Lackner et al. (2013), van Tilburg et al. (2013), Thakur et al. (2016), Lee et al. (2017), Dybowski et al. (2018) and Piontek et al. (2019) show that physical and psychological comorbidities, high levels of anxiety, high levels of depression, insomnia, severity of the pain, pain catastrophizing, somatization and age are all significant predictors of a greater severity of the symptoms CPVP, of the evolution of the pain and of a deteriorated quality of life. Similarly, Farup and Hestad (2015), Banerjee et al. (2017) and Porcelli et al. (2020) all show that the level of severity of the CPVP is a predictor of the severity of the associated psychopathological disorders. The greater the severity of the CPVP, the greater the severity of the levels of anxiety and depression, and the worse the psychosocial functioning, the quality of sleep and the conditions of physical and psychological health will be.
Conversely, several works of research have suggested that chronic pain is associated with a deterioration in attention, memory, intelligence and executive functioning (Berryman et al., 2014; Kennedy et al., 2014; Corti et al., 2021); in particular, within this latter domain, with the processes controlling response inhibition, working memory, cognitive flexibility, planning, problem solving and decision taking. Nevertheless, the findings concerning the neuropsychological disorders of the CPVP demonstrated in this current review point toward a great diversity that can even be contradictory.
The findings in executive functioning and memory are the ones that show the greatest ambiguity, particularly in the domains of cognitive flexibility, response inhibition and episodic visuospatial memory. Notwithstanding the above, deficits were found in the domains of problem solving and cognitive processing of emotional content, while the speed of processing and working memory did not seem to suffer any deterioration in the population in question. Although none of the studies reviewed showed correlations between the symptoms of depression and anxiety in CPVP and the results in the cognitive domains; Farup and Hestad (2015) and Wong et al. (2019a) did show evidence that the presence of depression and/or anxiety can act as predictors of a deteriorated cognitive performance in attention, cognitive processing, verbal fluency, psychomotor speed and cognitive flexibility.
The findings in attention are the ones that show the greatest agreement. Although the studies show evidence of deficits in this domain, on making an individualized evaluation of the different attention networks, they do show a slightly better effectiveness than that of the general population in the attention networks of both orienting and alerting (sustained attention); while in the attention networks of executive control (selective attention), there is evidence of a reduced functioning. On examining the existing correlations, Tkalcic et al. (2014) showed a positive attention bias, with a greater latency in the response toward words related to threatening situations and negative emotional content. A positive correlation can be appreciated with the anxiety trait, specific visceral anxiety and neuroticism. Similarly, Hubbard et al. (2015) and Henrich and Martin (2018) found that the fear of uncertainty and the high severity of the usual symptoms of CPVP negatively correlate with effective scores in the orienting attention network; that the high scores of visceral anxiety, the presence of major abdominal pain in the previous week and the high severity of the usual symptoms of CPVP correlate negatively with effective scores in alerting attention networks; and that the high levels of catastrophizing cognitions correlate negatively with a reduced attention control. Lam et al. (2019) and Wong et al. (2019b) state that one of the principal explanations for the demonstrated biases in the attention network is the presence of chronic thoracic, abdominal and/or pelvic pain, anxiety related to the symptoms, hypervigilance of the pain and visceral hypersensitivity. Along the same lines, another possible explanation for the attention bias is the proposal made by Rustamov et al. (2020), which suggests that persons with chronic pain direct a great part of their attention resources to information related to the pain due to their inability to inhibit it.
As for the findings concerning intelligence, although there were no significant differences with respect to the general population, there was evidence of a lower performance in fluid intelligence and crystallized intelligence. It can be seen that the risk of dementia has only been evaluated in one study (Chen et al., 2016); the accumulated incidence and the risk of suffering dementia being greater in patients with chronic pain. The incidence of dementia increases with age in the population with this pathology and tends to coincide with the incidence of comorbidities, being significantly higher from fifty years of age upwards.
The current review has some limitations. The conceptualization of chronic primary pain and, in particular, of CPVP and its subtypes is very recent, which influences the fact that the majority of studies found in the databases have not been adapted to this classification and that, therefore, the number of studies is greatly reduced. Thus, the only subtypes included in this present review are the irritable bowel syndrome and the chronic primary pelvic pain syndrome.
The control of the comorbidity of the participants included in the review is a limitation. Although most of the exclusion criteria refer to the presence of other gastrointestinal diseases, organic diseases, serious medical conditions, serious psychological disorders before the diagnosis of CPVP, substance abuse and/or the consumption of certain medications, there is great heterogeneity between the different articles. This can cause some articles to consider variables that others do not, affecting the validity of the results.
The instruments used are another limitation. The reviewed studies use a great number of different instruments to evaluate the psychopathological and neuropsychological disorders of the participants, which complicates the comparison of the results of the different studies. Not all the studies evaluate the disorders present in the sample in the same way; since some focus on psychopathological disorders, others on neuropsychological disorders and yet others focus on both. Furthermore, while some studies evaluate the general disorders, others focus on particular domains. All this has an impact in the sense that some results, especially those related to the neuropsychological disorders, can be ambiguous and, to a certain extent, contradictory. Similarly, the relations between the variables shown in the different studies are also very diverse; in some cases, resulting in difficulties to relate the psychopathological and neuropsychological disorders with CPVP.
Likewise, the use of self-reports or clinical interviews can show disparate results (Stuart et al., 2014). Through the use of self-reports, the presence of psychopathological symptoms is evaluated; however, factors such as lack of understanding, social stigma, the influence of mood, poor memory, and social desirability can influence the results; while the clinical interview, despite being more complex and requiring more time to apply, is considered the gold standard for in-depth evaluation of the presence of psychological disorders (Hopwood et al., 2008; Stuart et al., 2014). Therefore, the importance of using the two procedures for adequate psychopathological evaluation (Hopwood et al., 2008).
There are also several limitations in connection to the sample. Eleven of the studies do not have a control group with which to compare the results of the evaluation and two have a CPVP sample size below twenty subjects, which has repercussions on the reliability of the results. Furthermore, although the mean age is similar in the majority of the reviewed studies, there are some cases in which the age range is wider, which may suppose a limitation.
In short, the current review describes and critically analyses the psychological disorders associated with CPVP. Despite the great scarcity of studies concerning this pathology in the scientific literature, the questions related with psychopathological and neuropsychological disorders have been debated and questioned, concluding that the subjective, emotional and cognitive factors are intimately related to CPVP. Nevertheless, some deficits, especially neuropsychological ones, have not been sufficiently evidenced throughout the reviewed studies, or they show ambiguous results.
For future research, we highlight several objectives. First, to widen the sample to other subtypes; second, to use homogeneous tests to identify associated psychopathological and neuropsychological disorders. Third, we consider it necessary to use homogeneous inclusion and exclusion criteria in the selection of the sample to avoid the presence of comorbidity that could affect the validity of the results. The recent classification of chronic pain and its diverse classifications suppose a starting point for the research to deal with this pathology therapeutically, giving us the possibility of developing specific treatments adapted to the existing disorders.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AA-M, JM-M, MG-B, MB-A, and PC-C: conceptualization, methodology, and writing—review and editing. AA-M, JM-M, MG-B, and MB-A: data curation and supervision. AA-M, JM-M, and PC-C: formal analysis. AA-M, JM-M, MG-B, and PC-C: writing—original draft preparation. All authors contributed to the article and approved the submitted version.
Funding
Financed jointly by FEDER & Junta de Extremadura funds (Exp. GR21024). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CPVP, Chronic primary visceral pain; IBS, Irritable bowel syndrome; IBD, Inflammatory bowel disease; CPPPS, Chronic primary pelvic pain syndrome; ICD, International Classification of Diseases; WHO, The World Health Organization.
Footnotes
References
Aizawa, E., Sato, Y., Kochiyama, T., Saito, N., Izumiyama, M., Morishita, J., et al. (2012). Altered cognitive function of prefrontal cortex during error feedback in patients with irritable bowel syndrome, based on FMRI and dynamic causal modeling. Gastroenterology 143, 1188–1198. doi: 10.1053/j.gastro.2012.07.104
Andrews, P., Steultjens, M., and Riskowski, J. (2018). Chronic widespread pain prevalence in the general population: a systematic review. Eur. J. Pain 22, 5–18. doi: 10.1002/ejp.1090
Arango-Dávila, C. A., and Rincón-Hoyos, H. G. (2018). Depressive disorder, anxiety disorder and chronic pain: multiple manifestations of a common clinical and pathophysiological core. trastorno depresivo, trastorno de ansiedad y dolor crónico: múltiples manifestaciones de un núcleo fisiopatológico y clínico común. Rev. Colomb. Psiquiatr. 47, 46–55. doi: 10.1016/j.rcp.2016.10.007
Banerjee, A., Sarkhel, S., Sarkar, R., and Dhali, G. K. (2017). Anxiety and depression in irritable bowel syndrome. Indian J. Psychol. Med. 39, 741–745. doi: 10.4103/IJPSYM.IJPSYM_46_17
Baniasadi, N., Dehesh, M. M., Mohebbi, E., Hayatbakhsh-Abbasi, M., and Oghabian, Z. (2017). Assessing the sleep quality and depression-anxiety-stress in irritable bowel syndrome patients. Arq. Gastroenterol. 54, 163–166. doi: 10.1590/s0004-2803.201700000-08
Berens, S., Schaefert, R., Baumeister, D., Gauss, A., Eich, W., and Tesarz, J. (2019). Does symptom activity explain psychological differences in patients with irritable bowel syndrome and inflammatory bowel disease? Results from a multi-center cross-sectional study. J. Psychosom. Res. 126, 1–10. doi: 10.1016/j.jpsychores.2019.109836
Berrill, J. W., Gallacher, J., Hood, K., Green, J. T., Matthews, S. B., Campbell, A. K., et al. (2013). An observational study of cognitive function in patients with irritable bowel syndrome and inflammatory bowel disease. Neurogastroenterol. Motil. 25, 918–e704. doi: 10.1111/nmo.12219
Berryman, C., Stanton, T. R., Bowering, K. J., Tabor, A., McFarlane, A., and Moseley, G. L. (2014). Do people with chronic pain have impaired executive function? A meta-analytical review. Clin. Psychol. Rev. 34, 563–579. doi: 10.1016/j.cpr.2014.08.003
Bouchoucha, M., Devroede, G., Girault-Lidvan, N., Hejnar, M., Mary, F., and Benamouzig, R. (2020). Psychological profiles of irritable bowel syndrome patients with different phenotypes. Intest. Res. 18, 459–468. doi: 10.5217/ir.2019.09171
Brünahl, C., Dybowski, C., Albrecht, R., Riegel, B., Höink, J., Fisch, M., et al. (2017). Mental disorders in patients with chronic pelvic pain syndrome (CPPS). J. Psychosom. Res. 98, 19–26. doi: 10.1016/j.jpsychores.2017.04.011
Bruno, A., Zoccali, R. A., Pandolfo, G., Genovese, G., Merlino, M., Fries, W., et al. (2018). Negative emotions in irritable bowel syndrome: which differences among IBS subtypes?. Mediterr. J. Clin. Psychol. 6, 1–21. doi: 10.6092/2282-1619/2018.6.1730
Cáceres-Matos, R., Gil-García, E., Barrientos-Trigo, S., Porcel-Gálvez, A. M., and Cabrera-León, A. (2020). Consequences of chronic non-cancer pain in adulthood. Scoping review. Rev. Saúde Pública 54, 1–13. doi: 10.11606/s1518-8787.2020054001675
Chen, C. H., Lin, C. L., and Kao, C. H. (2016). Irritable bowel syndrome is associated with an increased risk of dementia: a nationwide population-based study. PLoS ONE 11, 1–12. doi: 10.1371/journal.pone.0144589
Corti, E. J., Gasson, N., and Loftus, A. M. (2021). Cognitive profile and mild cognitive impairment in people with chronic lower back pain. Brain Cogn. 151, 1–9. doi: 10.1016/j.bandc.2021.105737
De Souza, J. B., Grossmann, E., Perissinotti, D., de Oliveira Junior, J. O., da Fonseca, P., and Posso, I. P. (2017). Prevalence of chronic pain, treatments, perception, and interference on life activities: brazilian population-based survey. Pain Res. Manag. 2017, 1–9. doi: 10.1155/2017/4643830
Dueñas, M., Ojeda, B., Salazar, A., Mico, J. A., and Failde, I. (2016). A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 9, 457–467. doi: 10.2147/JPR.S105892
Dybowski, C., Löwe, B., and Brünahl, C. (2018). Predictors of pain, urinary symptoms and quality of life in patients with chronic pelvic pain syndrome (CPPS): a prospective 12-month follow-up study. J. Psychosom. Res. 112, 99–106. doi: 10.1016/j.jpsychores.2018.06.013
Farup, P. G., and Hestad, K. (2015). Cognitive functions and depression in patients with irritable bowel syndrome. Gastroenterol. Res. Pract. 2015, 1–9. doi: 10.1155/2015/438329
Fine, P. G. (2011). Long-term consequences of chronic pain: mounting evidence for pain as a neurological disease and parallels with other chronic disease states. Pain Med. 12, 996–1004. doi: 10.1111/j.1526-4637.2011.01187.x
Gogheri, T., Samavi, A., and Najarpourian, S. (2021). Structural relationship model of type D personality and depression with the mediating role of cognitive distortions and family functioning: a multi-group analysis. Curr. Psychol. 1–10. doi: 10.21203/rs.3.rs-157026/v1
Henrich, J. F., and Martin, M. (2018). Altered attentional control linked to catastrophizing in patients with irritable bowel syndrome. Br. J. Health Psychol. 23, 612–629. doi: 10.1111/bjhp.12307
Hopwood, C. J., Morey, L. C., Edelen, M. O., Shea, M. T., Grilo, C. M., Sanislow, C. A., et al. (2008). A comparison of interview and self-report methods for the assessment of borderline personality disorder criteria. Psychol. Assess. 20, 81–85. doi: 10.1037/1040-3590.20.1.81
Hubbard, C. S., Hong, J., Jiang, Z., Ebrat, B., Suyenobu, B., Smith, S., et al. (2015). Increased attentional network functioning related to symptom severity measures in females with irritable bowel syndrome. Neurogastroenterol. Motil. 27, 1282–1294. doi: 10.1111/nmo.12622
Kawoos, Y., Wani, Z. A., Kadla, S. A., Shah, I. A., Hussain, A., Dar, M. M., et al. (2017). Psychiatric co-morbidity in patients with irritable bowel syndrome at a tertiary care center in northern India. J. Neurogastroenterol. Motil. 23, 555–560. doi: 10.5056/jnm16166
Kennedy, P. J., Clarke, G., O'Neill, A., Groeger, J. A., Quigley, E. M., Shanahan, F., et al. (2014). Cognitive performance in irritable bowel syndrome: evidence of a stress-related impairment in visuospatial memory. Psychol. Med. 44, 1553–1566. doi: 10.1017/S0033291713002171
Klotz, S., Ketels, G., Löwe, B., and Brünahl, C. A. (2020). Myofascial findings and psychopathological factors in patients with chronic pelvic pain syndrome. Pain Med. 21, 34–44. doi: 10.1093/pm/pny097
Korwisi, B., Barke, A., Rief, W., Treede, R. D., and Kleinstäuber, M. (2021). Chronic pain in the 11th revision of the international classification of diseases: users' questions answered. Pain 1−13. doi: 10.1097/j.pain.0000000000002551
Lackner, J. M., Ma, C. X., Keefer, L., Brenner, D. M., Gudleski, G. D., Satchidanand, N., et al. (2013). Type, rather than number, of mental and physical comorbidities increases the severity of symptoms in patients with irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 11, 1147–1157. doi: 10.1016/j.cgh.2013.03.011
Lam, N. C., Yeung, H. Y., Li, W. K., Lo, H. Y., Yuen, C. F., Chang, R. C., et al. (2019). Cognitive impairment in Irritable Bowel Syndrome (IBS): a systematic review. Brain Res. 1719, 274–284. doi: 10.1016/j.brainres.2019.05.036
Lee, S. K., Yoon, D. W., Lee, S., Kim, J., Choi, K. M., and Shin, C. (2017). The association between irritable bowel syndrome and the coexistence of depression and insomnia. J. Psychosom. Res. 93, 1–5. doi: 10.1016/j.jpsychores.2016.12.007
Lee, Y. T., Hu, L. Y., Shen, C. C., Huang, M. W., Tsai, S. J., Yang, A. C., et al. (2015). Risk of psychiatric disorders following irritable bowel syndrome: a nationwide population-based cohort study. PLoS ONE 10, 1–12. doi: 10.1371/journal.pone.0133283
Liu, C. J., Hu, L. Y., Yeh, C. M., Hu, Y. W., Chen, P. M., Chen, T. J., et al. (2015). Irritable brain caused by irritable bowel? A nationwide analysis for irritable bowel syndrome and risk of bipolar disorder. PLoS ONE 10, 1–10. doi: 10.1371/journal.pone.0118209
Mills, S., Nicolson, K. P., and Smith, B. H. (2019). Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 123, 273–283. doi: 10.1016/j.bja.2019.03.023
Moriarty, O., Ruane, N., O'Gorman, D., Maharaj, C. H., Mitchell, C., Sarma, K. M., et al. (2017). Cognitive impairment in patients with chronic neuropathic or radicular pain: an interaction of pain and age. Front. Behav. Neurosci. 11, 1–13. doi: 10.3389/fnbeh.2017.00100
Murray, C. B., de la Vega, R., Murphy, L. K., Kashikar-Zuck, S., and Palermo, T. M. (2021). The prevalence of chronic pain in young adults: a systematic review and meta-analysis. Pain 1–13. doi: 10.1097/j.pain.0000000000002541
Nicholas, M., Vlaeyen, J., Rief, W., Barke, A., Aziz, Q., Benoliel, R., et al. (2019). The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain 160, 28–37. doi: 10.1097/j.pain.0000000000001390
Ojeda, B., Dueñas, M., Salazar, A., Mico, J. A., Torres, L. M., and Failde, I. (2018). Factors influencing cognitive impairment in neuropathic and musculoskeletal pain and fibromyalgia. Pain Med. 19, 499–510. doi: 10.1093/pm/pnx024
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 372, 1–36. doi: 10.1136/bmj.n160
Phillips, K., Wright, B. J., and Kent, S. (2014). Irritable bowel syndrome and symptom severity: evidence of negative attention bias, diminished vigour, and autonomic dysregulation. J. Psychosom. Res. 77, 13–19. doi: 10.1016/j.jpsychores.2014.04.009
Piontek, K., Ketels, G., Albrecht, R., Schnurr, U., Dybowski, C., Brünahl, C. A., et al. (2019). Somatic and psychosocial determinants of symptom severity and quality of life in male and female patients with chronic pelvic pain syndrome. J. Psychosom. Res. 120, 1–7. doi: 10.1016/j.jpsychores.2019.02.010
Porcelli, P., De Carne, M., and Leandro, G. (2020). Distinct associations of DSM-5 Somatic Symptom Disorder, the Diagnostic Criteria for Psychosomatic Research-Revised (DCPR-R) and symptom severity in patients with irritable bowel syndrome. Gen. Hosp. Psychiatry 64, 56–62. doi: 10.1016/j.genhosppsych.2020.03.004
Racine, M. (2018). Chronic pain and suicide risk: a comprehensive review. Prog. Neuropsychopharmacol. Biol. Psychiatry 87, 269–280. doi: 10.1016/j.pnpbp.2017.08.020
Riegel, B., Bruenahl, C. A., Ahyai, S., Bingel, U., Fisch, M., and Löwe, B. (2014). Assessing psychological factors, social aspects and psychiatric co-morbidity associated with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) in men - A systematic review. J. Psychosom. Res. 77, 333–350. doi: 10.1016/j.jpsychores.2014.09.012
Rustamov, N., Wagenaar-Tison, A., Doyer, E., and Piché, M. (2020). Electrophysiological investigation of the contribution of attention to altered pain inhibition processes in patients with irritable bowel syndrome. J. Physiol. Sci. 70, 1–19. doi: 10.1186/s12576-020-00774-x
Sertbas, Y., Belli, H., Piskinpasa, N., Ural, C., Akbudak, M., Sertbas, M., et al. (2012). Assessment of psychiatric symptoms and co-morbidities in patients with irritable bowel syndrome. West Indian Med. J. 61, 544–548. doi: 10.7727/wimj.2012.166
Sharma, N., Dhiman, S., Bodh, V., Sharma, D., Sharma, R., Sharma, S., et al. (2021). Cognitive dysfunction in ulcerative colitis patients in remission and its comparison with patients with irritable bowel syndrome and healthy controls. Indian J. Gastroenterol. 40, 169–175. doi: 10.1007/s12664-020-01122-y
Stasi, C., Caserta, A., Nisita, C., Cortopassi, S., Fani, B., Salvadori, S., et al. (2019). The complex interplay between gastrointestinal and psychiatric symptoms in irritable bowel syndrome: a longitudinal assessment. J. Gastroenterol. Hepatol. 34, 713–719. doi: 10.1111/jgh.14375
Stuart, A. L., Pasco, J. A., Jacka, F. N., Brennan, S. L., Berk, M., and Williams, L. J. (2014). Comparison of self-report and structured clinical interview in the identification of depression. Compr. Psychiatry 55, 866–869. doi: 10.1016/j.comppsych.2013.12.019
Thakur, E. R., Quigley, B. M., El-Serag, H. B., Gudleski, G. D., and Lackner, J. M. (2016). Medical comorbidity and distress in patients with irritable bowel syndrome: The moderating role of age. J. Psychosom. Res. 88, 48–53. doi: 10.1016/j.jpsychores.2016.07.006
Tkalcic, M., Domijan, D., Pletikosic, S., Setic, M., and Hauser, G. (2014). Attentional biases in irritable bowel syndrome patients. Clin. Res. Hepatol. Gastroenterol. 38, 621–628. doi: 10.1016/j.clinre.2014.02.002
Torun, F., Koç, G., Ocak Serin, S., and Dilek Torun, S. (2020). Psychiatric symptoms and relationship of disease with stress and traumatic experiences in patients with irritable bowel syndrome. Riv. Psichiatr. 55, 292–296. doi: 10.1708/3457.34461
Treede, R. D., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., Benoliel, R., et al. (2019). Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 160, 19–27. doi: 10.1097/j.pain.0000000000001384
van Tilburg, M. A., Palsson, O. S., and Whitehead, W. E. (2013). Which psychological factors exacerbate irritable bowel syndrome? Development of a comprehensive model. J. Psychosom. Res. 74, 486–492. doi: 10.1016/j.jpsychores.2013.03.004
Vargas, C., Bilbeny, N., Balmaceda, C., Rodríguez, M. F., Zitko, P., Rojas, R., et al. (2018). Costs and consequences of chronic pain due to musculoskeletal disorders from a health system perspective in Chile. Pain Rep. 3, 1–10. doi: 10.1097/PR9.0000000000000656
Wong, K., Yuen, S., and Mak, A. (2019b). Neurocognitive characteristics of individuals with irritable bowel syndrome. East Asian Arch. Psychiatry 29, 48–56. doi: 10.12809/eaap1877
Wong, K. M., Mak, A., Yuen, S. Y., Leung, O., Ma, D. Y., Chan, Y., et al. (2019a). Nature and specificity of altered cognitive functioning in IBS. Neurogastroenterol. Motil. 31, 1–12. doi: 10.1111/nmo.13696
World Health Organization (2018). International Classification of Diseases (11th ed.). Available online at: https://icd.who.int/ (accessed June 29, 2022).
Keywords: chronic primary pain, chronic primary visceral pain, psychopathology, neuropsychology, systematic review
Citation: Arévalo-Martínez A, Moreno-Manso JM, García-Baamonde ME, Blázquez-Alonso M and Cantillo-Cordero P (2022) Psychopathological and neuropsychological disorders associated with chronic primary visceral pain: Systematic review. Front. Psychol. 13:1031923. doi: 10.3389/fpsyg.2022.1031923
Received: 30 August 2022; Accepted: 03 October 2022;
Published: 19 October 2022.
Edited by:
Manuel Fernández-Alcántara, University of Alicante, SpainReviewed by:
María Nieves Pérez-Marfil, University of Granada, SpainMichael Finn, Helen DeVos Children's Hospital, United States
Copyright © 2022 Arévalo-Martínez, Moreno-Manso, García-Baamonde, Blázquez-Alonso and Cantillo-Cordero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Manuel Moreno-Manso, am1tYW5zbyYjeDAwMDQwO3VuZXguZXM=