 Nadav Brumer
Nadav Brumer Elizabeth Elkins
Elizabeth Elkins Jennifer Parada
Jennifer Parada Jake Hillyer
Jake Hillyer Alexandra Parbery-Clark
Alexandra Parbery-Clark- 1Auditory Research Laboratory, Center for Hearing and Skull Base Surgery, Swedish Neuroscience Institute, Seattle, WA, United States
- 2Department of Psychology, Bellevue College, Bellevue, WA, United States
- 3College of Medicine, University of Arizona, Phoenix, AZ, United States
Purpose: Recent studies using the Montreal Cognitive Assessment (MoCA) suggest delayed recall is challenging for cochlear implant (CI) users. To better understand the underlying processes associated with delayed recall in CI users, we administered the MoCA and the California Verbal Learning Test, Third Edition (CVLT-3), which provides a more comprehensive assessment of delayed recall ability.
Methods: The MoCA and CVLT-3 were administered to 18 high-performing CI users. For the CVLT-3, both the traditional scoring and a newer scoring method, the Item-Specific Deficit Approach (ISDA), were employed.
Results: The original MoCA score and MoCA delayed recall subtest score did not relate to performance on any CVLT-3 measures regardless of scoring metric applied (i.e., traditional or ISDA). Encoding performance for both the CVLT-3 and ISDA were related. Consolidation, which is only distinctly defined by the ISDA, related to CVLT-3 cued delay recall performance but not free delay recall performance. Lastly, ISDA retrieval only related to CVLT-3 measures when modified.
Conclusion: Performance on the MoCA and CVLT-3 in a high performing CI patient population were not related. We demonstrate that the ISDA can be successfully applied to CI users for the quantification and characterization of delayed recall ability; however, future work addressing lower performing CI users, and comparing to normal hearing controls is needed to determine the extent of potential translational applications. Our work also indicates that a modified ISDA retrieval score may be beneficial for evaluating CI users although additional work addressing the clinical relevance of this is still needed.
Introduction
Hearing Loss (HL) and dementia are two of the most prevalent health concerns for the aging population (Kravitz et al., 2012; Olusanya et al., 2014; Rigters et al., 2018; Ogawa et al., 2019). Approximately two-thirds of adults in the United States over the age of 70 have HL and this number is expected to nearly double in the next four decades (Goman et al., 2017). Additionally, an estimated 5.8 million people in the United States and 10% of individuals 65 or older are impacted by Alzheimer’s disease, the most common type of dementia (Zhao, 2020). Mild cognitive impairment (MCI) is a distinct clinical term describing cognitive decline that can precede the formal diagnosis of dementia and is characterized by cognitive deficits not explained by typical aging (Eshkoor et al., 2015). These deficits include difficulties with memory, language, and problem-solving, without the disruption of daily living activities (Petersen, 2011). MCI, Alzheimer’s disease, and other types of dementia are commonly diagnosed by measuring performance on delayed recall tasks, among other cognitive markers (Klages et al., 2005; Dubois et al., 2014; García-Herranz et al., 2016).
Delayed recall is a complex skill involving multiple memory systems. Memory is believed to consist of three storage systems: sensory, short-term memory (STM), and long-term memory (LTM; Murdock, 1967; Atkinson and Shiffrin, 1968). Stimuli move through these systems via three sequential cognitive processes: encoding, consolidation, and retrieval (see Figure 1; Melton, 1963; Brown and Craik, 2000; Baddeley, 2002). Encoding refers to a mental representation or an external perceptual or sensory stimulus in the brain (Tromp et al., 2015). The stimulus is then consolidated when it is actively stored in STM, where, if it remains long enough, will be transferred into LTM, which is understood to have a capacity limited only by its ability to be accessed (i.e., retrieval; Tulving and Pearlstone, 1966). Due to the sequential nature of these processes, stimuli retrieved from LTM (e.g., delayed recall) must be encoded and consolidated first. Given the multiple cognitive processes involved, it is complicated to identify where breakdowns associated with poor delayed recall occur. For example, if stimuli are correctly recalled shortly after presentation, it can be posited that some level of encoding has occurred. Alternately, if the same stimuli are not recalled after a delay period, an impaired consolidation or retrieval mechanism is more likely to be at fault. As such, delayed recall measures are often thought to reflect retrieval abilities, whereas immediate recall tasks are meant to reflect encoding abilities (Delis et al., 2017).
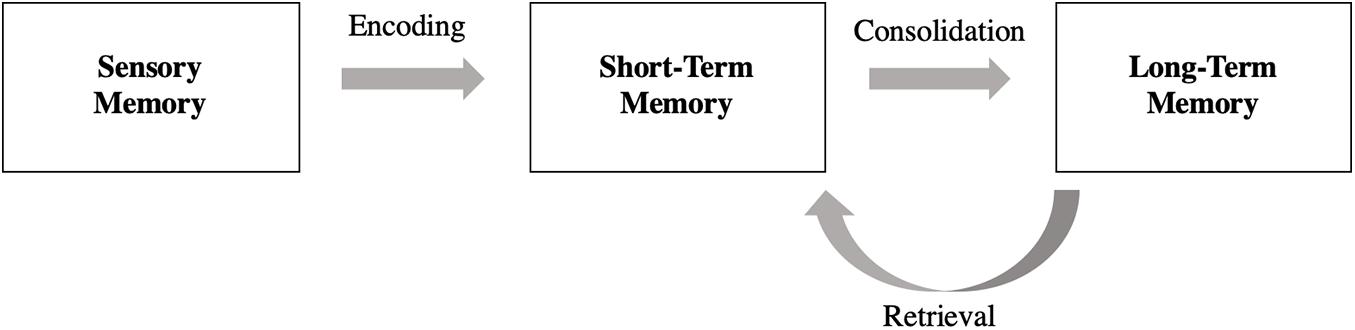
Figure 1. Multimodal memory model and associated cognitive processes: the sequential model begins with sensory memory and ends with long-term memory. Stimuli move through these three memory storage units through cognitive processes known as: encoding, consolidation, and retrieval.
Delayed recall tasks appear to present a greater challenge for individuals with HL compared to individuals without HL (Boxtel et al., 2000; Dupuis et al., 2015; Chandramouli et al., 2019). Specifically, performance on the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005), a test used to assess cognitive functioning and screen for MCI and dementia, demonstrated that individuals with HL struggled to recall delayed recall stimuli more frequently than individuals without HL (Dupuis et al., 2015). This effect is further supported by the association between poorer baseline hearing in both ears and greater declines in delayed verbal memory found over a 2-year period (Armstrong et al., 2020). In fact, Deal et al. (2015) demonstrated an association between HL and a greater longitudinal decline in delayed recall performance over a 20-year period. Recent work suggests that using MoCA alternate scores (i.e., a scoring method whereby specific auditory subtests are systematically removed; Dupuis et al., 2015) may have clinical significance for the hearing-impaired population (Al-Yawer et al., 2019). Our own research has demonstrated that individuals with HL, specifically those with cochlear implants (CIs; surgical implants effective for those with profound hearing loss in which other assistive hearing devices are not appropriate) performed better on the MoCA presented in both a visual and auditory format when delayed recall was removed (Hillyer et al., 2020; Parada et al., 2020). However, removing test items from the total score may also decrease sensitivity (Dupuis et al., 2015). Using the California Verbal Learning Test—Third Edition (CVLT-3; Delis et al., 2017), a neuropsychological assessment of verbal learning and delayed recall, Pisoni et al. (2018) demonstrated more retrieval-induced forgetting of stimuli in delayed recall tasks in experienced CI users compared to those without HL. Additionally, CI users benefited more from semantically cued words than individuals without HL suggesting that semantic cueing allowed individuals with HL to access words that were encoded but not accessible to non-cued retrieval (Chandramouli et al., 2019; Kronenberger and Pisoni, 2019). Taken together, the current literature suggest that an impaired retrieval mechanism may underlie delayed recall deficits in individuals with HL.
While the CVLT-3 offers a more comprehensive assessment of delayed recall than the MoCA (e.g., allows for the distinction of short and long delay free and cued recall), it does not provide distinct measures of individual memory processes (i.e., encoding, consolidation and retrieval). Where traditional metrics of the CVLT-3 (e.g., learning slope, recognition-hits) reflect an overlap between memory processes (Delis et al., 1991), the Item-Specific Deficit Approach (ISDA, Wright et al., 2009) was developed with the goal of providing more distinct indices of encoding, consolidation and retrieval. The ISDA is a scoring method that evaluates list-learning performance at the item level rather than by overall trial performance across immediate recall and subsequent delayed recall trials. For example, the CVLT-3 calculates scores as a summation of total words recalled within each trial whereas the ISDA takes into account the amount of times each word has been recalled across multiple trials. This item-level approach also aims to compensate for the effects of inattention, which may prevent a participant from initially encoding a target word for later recall. This scoring method may be similarly helpful for participants with HL who may not encode a target word due to mishearing or not hearing, thus affecting their overall performance.
The aim of this study was to further explore our previous findings from the MoCA where the largest change in passing rate was observed by removing the delayed recall subtest, suggesting that delayed recall is more challenging for this patient population (Parada et al., 2020). Given the potential clinical utility of the alternate MoCA scoring methods for people with HL, we considered original and alternate MoCA scores in relation to a more comprehensive delayed recall test: the CVLT-3. As such, we administered both the MoCA as well as the CVLT-3 to gain a clearer understanding of the underlying memory processes associated with delayed recall. Given that delayed recall is a complex cognitive process consisting of encoding, consolidation, and retrieval, we also used CVLT-3 scores to produce individual ISDA indices reflective of these processes. We predicted that higher delayed recall scores on the MoCA would relate to better performance on the CVLT-3. Given that the CVLT-3 and ISDA utilize the same raw scores, we also expected that respective measures of encoding and retrieval would relate to equivalent ISDA deficit indices.
Materials and Methods
Participants
Eighteen (11 female, 7 male) experienced, high-performing CI users (>6 months listening experience, M = 56.89 months, SD = 34.37 months, range of 10–145 months; see Table 1 for participant CI details), between the ages of 52 and 83 years (M = 68.56, SD = 10.37) were recruited from the patient pool at the Center for Hearing and Skull Base Surgery at The Swedish Neuroscience Institute in Seattle, Washington. Experienced CI users were recruited because maximum comfortable levels and threshold levels are optimally achieved after 6 months of use and programming (Gajadeera et al., 2017). CI assisted threshold levels were not related to age (all r ≤ 0.282, p ≤ 0.929). CI users in this study were considered high-performing based on their AzBio Sentence Test (Spahr et al., 2012) percentage scores, which reflect speech perception abilities in quiet and were all above 80% (M = 92.78, SD = 6.57, range = 20%; Hillyer et al., 2020). Inclusion criteria required participants to have no recorded symptoms or diagnosis of dementia, no report of cognitive decline and no history of congenital or pre-lingual hearing loss. All participants were native speakers of English, had at least a high school education and demonstrated normal IQ scores (M = 107.39, SD = 7.96), as measured by the Test of Non-verbal Intelligence—4th Edition (TONI-4; Brown et al., 2010). All participants had a passing score for at least one of the four scoring versions of the MoCA (see Table 2 for descriptions of scoring methods). All testing procedures were approved by the Swedish Medical Center Institutional Review Board (#SWD56152-14) and participants provided informed written consent. All testing was conducted in a clinic room at the Swedish Neuroscience Institute in Seattle, WA, United States. All testing (i.e., task order and test versions) was randomized across subjects.
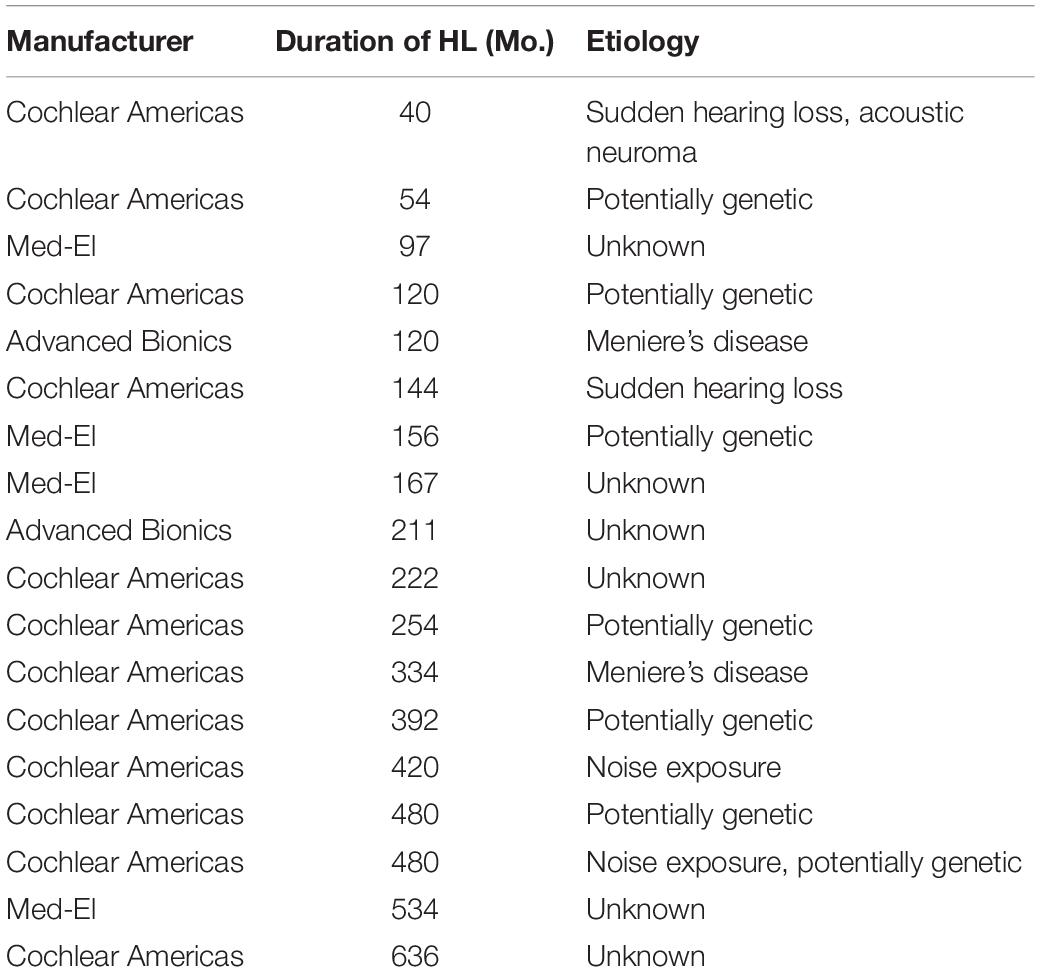
Table 1. Participant cochlear implant details.
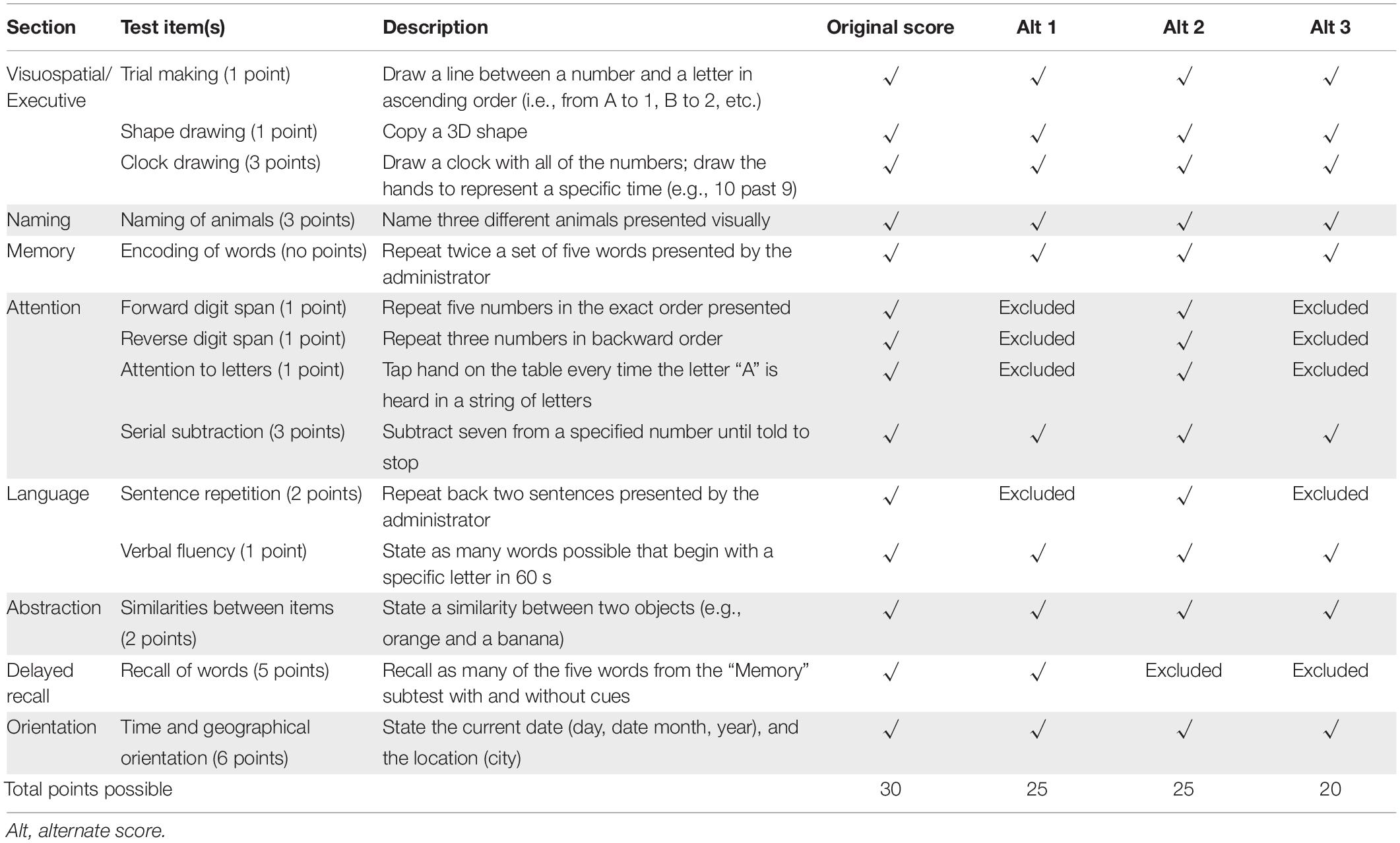
Table 2. Description of the standard MoCA and point allotment for original and alternate scoring methods.
Original Montreal Cognitive Assessment
The MoCA is a 30-point, 12-item auditory-visual neurocognitive test with eight subtests: visuospatial executive functioning, naming, memory, attention, language, abstraction, delayed recall and orientation, in that order (see Table 2 for descriptions of subtests). To evaluate delayed recall, the same five words presented in the memory subtest are recalled again after a roughly 5-min delay. Each participant was randomly assigned one of three MoCA versions (i.e., 7.1, 7.2, and 7.3) which have been shown to demonstrate equivalent reliability and validity (Costa et al., 2012; Nasreddine and Patel, 2016). In addition to standard scoring, three alternative scoring methods developed by Dupuis et al. (2015) and previously applied to CI users (Parada et al., 2020) were employed. Alternative scoring methods removed items from the attention, language, and delayed recall sections providing a means to examine the influence of specific subtests on general performance (see Table 2 for scoring methods, point allocation and cutoff scores). All MoCA subtest stimuli were administered in adherence with the MoCA test administration protocol, in either the auditory (e.g., visuospatial/executive, naming) or auditory-visual (e.g., memory, attention, language, abstraction, delayed recall, and orientation) modality. Higher scores indicated better performance.
California Verbal Learning Test, Third Edition
The CVLT-3 (Delis et al., 2017) is a neuropsychological assessment of verbal learning and memory presented in the auditory modality. This tool aims to connect performance on subtests to specific memory deficits and strategies. Each participant was administered the CVLT-3, where 16 target words were presented and then recalled repeatedly for five immediate recall trials. Following the immediate recall trials, a distractor list of 16 non-target words was presented and recalled, after which participants were instructed to recall the original target words without, and then with semantic cues (i.e., short-delay free and short-delay cued subtests). Following a 20-min delay period, the 16 target words were recalled again without, and then with semantic cues (i.e., long-delay free and long-delay cued subtests). Lastly, the recognition-hits subtest required participants to indicate a yes or no recognition of the 16 target words amongst 32 other distractor words. The CVLT-3 also provided a calculation for learning slope, or the rate at which learning occurred during the five immediate recall trials (see Table 3 for description of all subtests and metrics). Higher scores indicated better performance.
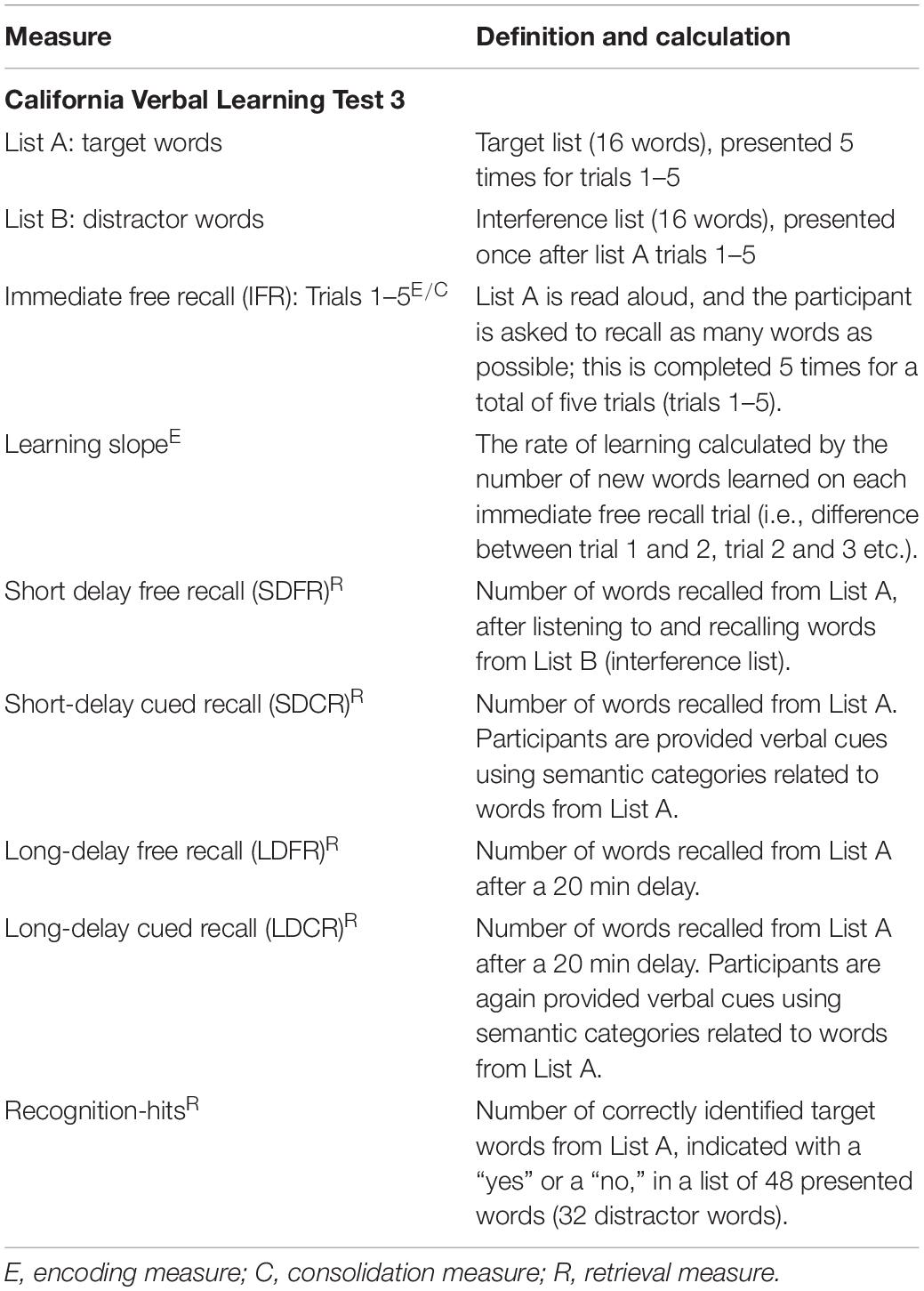
Table 3. CVLT-3 metrics.
Item-Specific Deficit Approach
The ISDA (Wright et al., 2009) is a scoring method that can be applied to any episodic memory test with multiple learning trials. The ISDA has been shown to have strong internal consistency for descriptive scales comprised of a small number of items (58–77%; Pedhazur and Schmelkin, 1991; Kehoe, 1994; Kline, 2005) and demonstrates an advantage over other traditional indices for predicting low memory performance (Wright et al., 2009). Compared to standard scoring methods, the ISDA weighs delayed recall performance more heavily in order to reflect one’s multimodal memory processing abilities. The ISDA scoring method was applied to CVLT-3 raw performance scores to calculate indices of encoding, consolidation, and retrieval (see Table 4). These indices reflect multimodal processes associated with delayed recall (see Figure 1) and therefore offer additional insight into delayed recall abilities not specifically isolated in the MoCA or CVLT-3. Because the ISDA requires participants to recall a target word during all four delayed recall subtests to avoid receiving a point toward a poorer overall retrieval deficit score, we also created an alternate ISDA retrieval index scoring method with a less stringent criteria. This alternate method requires the participant to recall a target word during at least three of the four delayed recall subtests, allowing the participant to miss the target word once before increasing their measured retrieval deficit, while also ensuring the target word is recalled on at least one short and long delay subtest. ISDA scores were calculated as a deficit, so higher scores reflected lower performance.
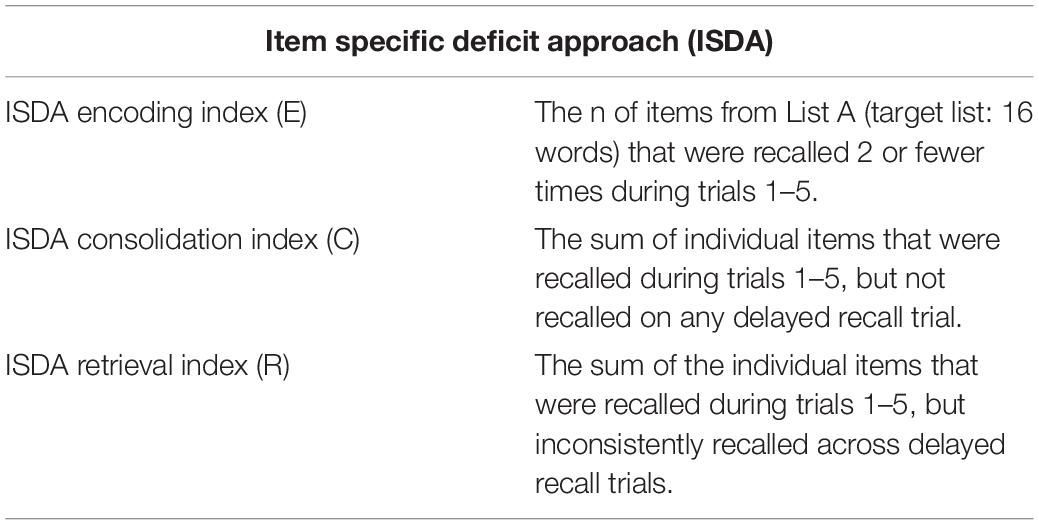
Table 4. ISDA metrics: for all measures, a higher score indicates a greater deficit and hence lower performance.
Statistical Analyses
Statistical analyses were completed using SPSS Version 22 (IBM Corp, 2017). Prior to analysis, normality of data was evaluated using Shapiro-Wilk tests. All measures were confirmed to be normally distributed with the exception of performance on the MoCA delayed recall subtests, and alternative 2 and 3 scoring methods. Furthermore, CVLT-3 data were analyzed relative to the mean normative scores provided by Delis et al., 2017 and confirmed to be within the normative range (i.e., T-scores between 30 and 70). While the ISDA does not have normative ranges, all data points were confirmed to be within 2 standard deviations of the mean. Age was significantly related to all CVLT-3 (all r ≤ −0.797, p ≤ 0.028) and ISDA (all r ≤ 0.688, p ≤ 0.018) scores. As such, age was included as a covariate for all Pearson R correlations evaluating these measures. Paired sample t-test comparisons were used to examine change across the MoCA original and alternate scores, the CVLT-3 performance on trials 1–5 as well as the differences between free and cued delayed recall abilities. All reported statistics reflect two-tailed significance values. Bonferroni corrections were applied when needed.
Results
Performance on the standard MoCA, including the MoCA delayed recall subtest, did not relate with performance on the immediate or delayed recall subtests of the CVLT-3, regardless of MoCA scoring method used. CVLT-3 subtest performance scores thought to reflect encoding abilities correlated with the ISDA encoding index, with the exception of learning slope. The ISDA retrieval index was not associated with any CVLT-3 measures; however, the alternate ISDA retrieval scoring method was related to the CVLT-3 long-delay free recall subtest. Consolidation abilities, which are only distinctly defined by the ISDA, were associated with CVLT-3 immediate recall trials 2 and 3 as well as both short and long delay cued recall subtests and recognition-hits, but not the delay free recall subtests.
Discrete Descriptive Statistics of Cognitive Tests
Montreal Cognitive Assessment
Similar to Parada et al. (2020), CI users showed the largest change in passing rate when the delayed recall subtest of the MoCA was removed (i.e., significant differences in passing rate between a.) the original with alternate 2 and 3 and, b.) alternate 1 with alternate 2 and 3 MoCA scoring methods; all p ≤ 0.039 and p ≤ 0.006, respectively). This was not observed between the original and alternate 1 (p = 0.250) or between alternate 2 and 3 scoring methods (p ≥ 0.999; see Table 5 for the means of each scoring method and passing rate).
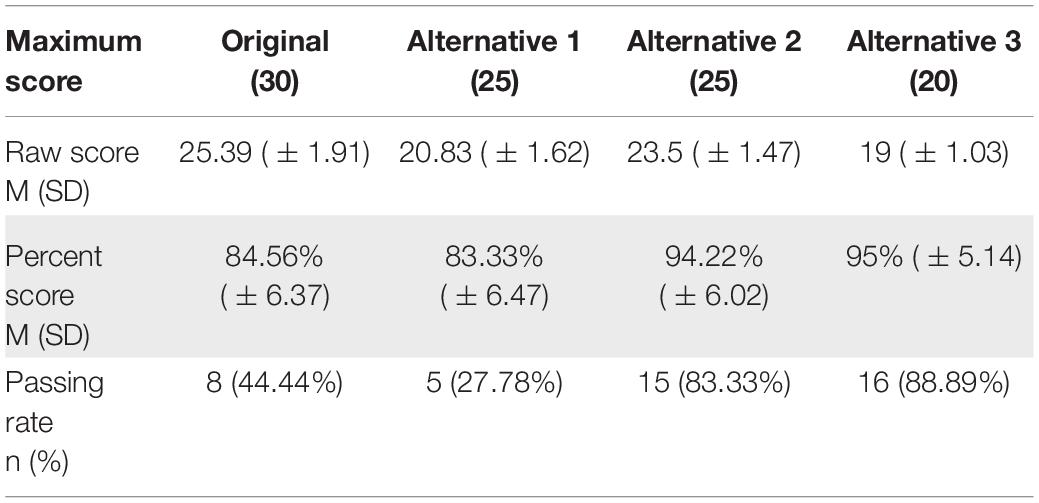
Table 5. MoCA participant scores across the different scoring methods.
California Verbal Learning Test, Third Edition
Paired sample t-tests between immediate recall trials 1–5 demonstrated significant differences between all trials [see Figure 2; all t(17) ≤ −4.44, p ≤ 0.001; Bonferroni adjusted α = 0.005] with the exception of trials 3 and 4 not being significantly different from each other [t(17) = −2.23, p = 0.039]. Additionally, paired samples t-tests between delayed recall subtests demonstrated a significant difference in performance for scores on the short-delay free recall subtest (M = 10.06, SD = 3.99) and short-delay cued recall subtest (M = 11.28, SD = 3.04) [t(17) = −3.05, p = 0.007] and a marginally significant difference in performance for the long-delay free recall subtest (M = 10.33, SD = 4.09) and long-delay cued recall subtest [M = 11.33, SD = 3.43; t(17) = −2.34, p = 0.032].
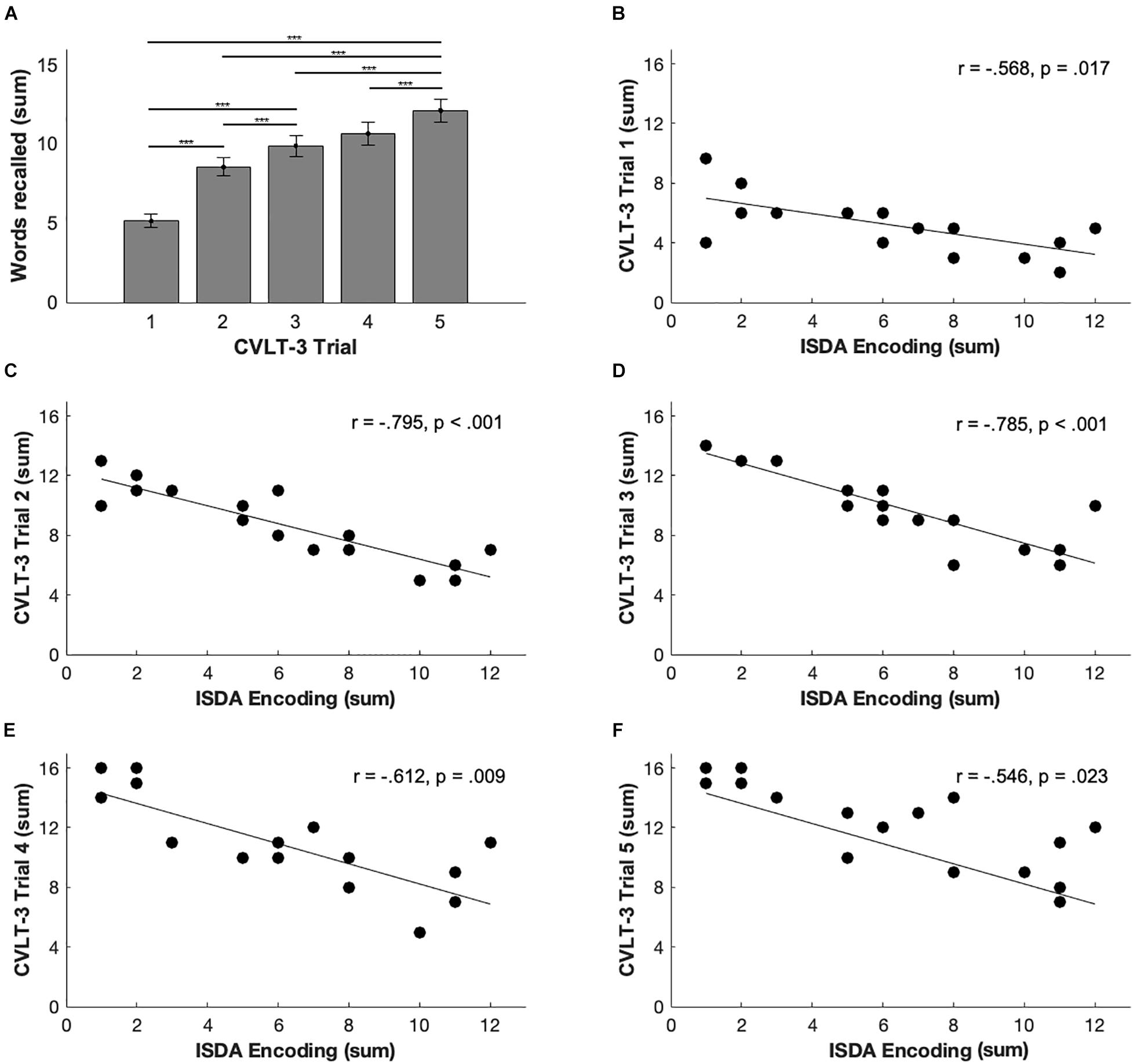
Figure 2. CVLT-3 and ISDA relationships. (A) Means and SDs for all participants across trials 1–5. Significant differences were noted between all trials except for trials 3 and 4 with Bonferroni correction *** ≤ 0.001. (B–F) Correlation plots indicating the relationship between each trial and the ISDA encoding measure. Significant correlation between each of the trials 1–4 with the ISDA measures except for trial 5 which did not meet significance with Bonferroni correction; α = 0.017.
Item-Specific Deficit Approach
On average, participants received the highest ISDA scores (and therefore experienced the largest deficit) on the encoding index (M = 6.38, SD = 3.65), followed by retrieval (M = 4.28, SD = 2.72), and consolidation (M = 2.78, SD = 2.56).
Analysis of Montreal Cognitive Assessment Delayed Recall Performance in Relation to California Verbal Learning Test, Third Edition Performance
Incongruent with our initial predictions, no relationships were observed between MoCA performance (for any scoring method) and CVLT-3 performance (all ρ ≤ 0.410, p ≤ 0.023; Bonferroni adjusted α = 0.013) or ISDA indices (all r ≤ 0.103, p ≤ 0.797). MoCA delayed recall subtest scores did not relate to CVLT-3 performance or calculated ISDA indices (all ρ ≤ 0.369, p ≤ 0.132).
Relationships Between California Verbal Learning Test, Third Edition Performance and Item-Specific Deficit Approach Indices
To understand the relationship between these two scoring methods in this patient population, correlational analyses were performed. A Bonferroni correction of α = 0.017 was applied to all correlations between CVLT-3 and ISDA scores. In accordance with our predictions concerning encoding and immediate free recall, performance on all CVLT-3 immediate recall measures related to the ISDA encoding index (all r ≤ −0.568, p ≤ 0.017) with the exception of trial 5 (r = 0.546, p = 0.023; see Figure 2). Performance on CVLT-3 immediate recall trials 2 and 3 were related to the ISDA consolidation index (all r ≤ −0.596, p ≤ 0.013). None of the immediate recall measures were related to the ISDA retrieval index (all r ≤ 0.116, p ≤ 0.987).
CVLT-3 short-delay free recall and short-delay cued recall measures were related to the ISDA encoding index (all r ≤ −0.546, p ≤ 0.009). Performance on both CVLT-3 cued delay recall subtests (short and long) and recognition-hits were related to the ISDA consolidation index (all r ≤ −0.580, p ≤ 0.015). While we expected delayed recall measures to correlate with ISDA retrieval scores, none of the CVLT-3 subtests were related to the ISDA retrieval index (r ≤ 0.116, p ≤ 0.987), but the CVLT-3 long-delay free recall subtest did relate to the alternate ISDA retrieval index (r = 0.641, p = 0.006). No other relationships between the alternate ISDA retrieval index and the CVLT-3 scores were observed (all r ≤ 0.149, p ≤ 0.696; see Table 6).
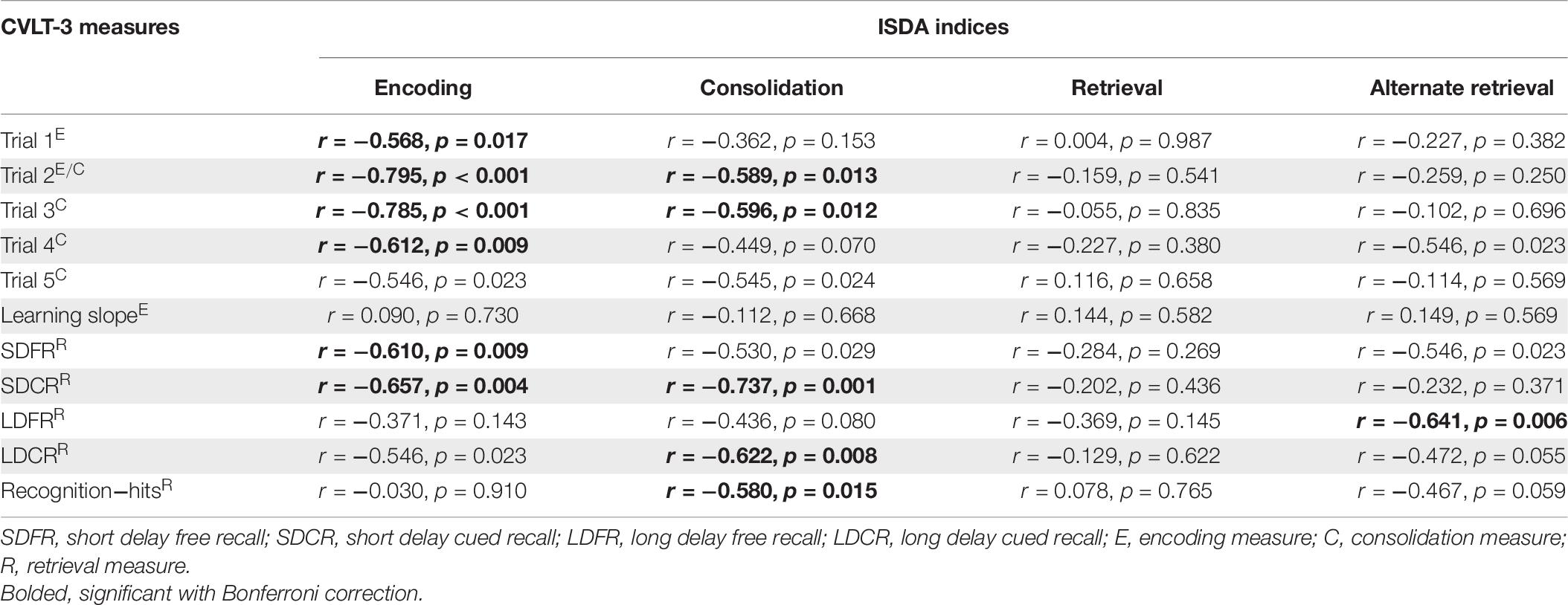
Table 6. Pearson correlations between the CVLT-3 and ISDA.
Discussion
The primary aim of this study was to further examine delayed recall performance in experienced, high-performing CI users to better understand the underlying memory processes characteristic of this group. The CVLT-3 was employed as a comprehensive test of delayed recall, in contrast with the MoCA, which includes only one delayed recall subtest. Incongruent with our predictions, performance on the MoCA delayed recall subtest did not relate to performance on any CVLT-3 subtests. While the CVLT-3 and MoCA are both widely used by clinicians, the lack of relationship between delayed recall performance as measured by the two tests highlights their differences when applied to CI users.
To better understand the lack of relationship between MoCA and CVLT-3 performance observed here, the differences between two tests need to be explored. Delayed recall consists of 45.5% of the overall score of the CVLT-3, whereas it only accounts for 16.6% of the overall score of the MoCA. Additionally, the delayed recall periods are different, with the CVLT-3 instructing for an approximately 20 min delay period between short-delay cued recall and long-delay free recall subtests, and the MoCA instructing for a 5 min delay period between initial immediate recall memory and delayed recall subtests (see Table 2). These differing delay periods have the potential to allow for different levels of consolidation and forgetting of stimuli based on the capacity of each memory system. This is because the assumed storage capability of STM is about 30 s with a capacity of about seven numeric digits (Miller, 1956; Craik and Lockhart, 1972). The longer delay period in the CVLT-3 may result in greater forgetting of target stimuli (i.e., the 16 words the participant is attempting to remember). Conversely, the word list in the CVLT-3 is read to the participant five times, allowing for further consolidation of the stimuli through repetition, while the MoCA word list is only read twice. Additionally, the CVLT-3 includes scoring for delay cued recall, whereas the 7.1-3 versions of the MoCA do not. The inclusion of delay cued recall, which utilizes semantic categories for recalling stimuli, allows for the exploration of other types of delayed recall that may use different cognitive processes from delay free recall. Taken together, differences in scoring methodology, delay periods, repetition and cueing complicate comparing delayed recall performance measured of the MoCA v. the CVLT-3.
Previous literature has examined cognitive performance in relation to hearing abilities for the MoCA (Dupuis et al., 2015; Ambert-Dahan et al., 2017; Lim and Loo, 2018; Hillyer et al., 2020; Parada et al., 2020; Shen et al., 2020; Utoomprurkporn et al., 2020) and CVLT-3 (Kramer et al., 2018; Moseley, 2018; Pisoni et al., 2018; Chandramouli et al., 2019), demonstrating that differences in cognitive abilities due to sensory impairments like HL should be taken into account during test administration. Our current findings present the first application of the ISDA to a population with HL. One potential strength of the ISDA is the ability to counteract the effects of inattention by measuring performance at the item level rather than by overall trial performance (Wiegner and Donders, 1999; Wright et al., 2009). This item-level approach may also offer the ability to account for the fact that not all 16 words are always properly encoded by tabulating scores based only on the words successfully recalled. The original CVLT-3 scoring method tabulates each score as a proportion of all 16 words, whether all 16 words were encoded at some point or not. In this study, our participants repeated 91% or approximately 15 of the 16 target words at least once across the five immediate recall trials, whereas they repeated 78% or approximately 13 out of the 16 target words at least once across all delayed recall subtests. These results support similar findings by Parada et al. (2020) suggesting that poorer delayed recall performance may be a result of an impaired consolidation and/or retrieval mechanism than an inability to properly hear and encode the words during the initial immediate recall trials. While the majority of words were properly encoded in our participant population, individuals with poorer speech discrimination could benefit from this item-level approach, as it may mitigate failures to encode test stimuli due not hearing or mishearing. More research is needed to address this.
In line with our secondary aim to relate ISDA indices with equivalent CVLT-3 subtests, we found that performance on the CVLT-3 immediate recall measures thought to reflect encoding abilities were related to the ISDA encoding index, whereas consolidation measures demonstrated a different pattern. CVLT-3 cued delay recall performance related to the ISDA consolidation index, but CVLT-3 free delay recall performance did not. These results may be driven by the ISDA scoring criteria for consolidation, which requires participants to recall a target word on at least one of the four delayed recall subtests in order to not receive a point toward their consolidation index score. In other words, the inability to recall the target word on any delayed recall subtests (i.e., score of 0 out of 4) would result in an increased consolidation deficit. Consequently, it stands to reason that the ISDA consolidation index may relate to performance on delayed recall subtests where stimuli were remembered most frequently, which in our study were the delay cued subtests. Previous research in individuals with normal hearing has demonstrated that the cognitive processes associated with cued and free recall are different (Nobel and Shiffrin, 2001; Brainerd et al., 2002; Nyberg et al., 2002; Padilla-Walker and Poole, 2002; Ivanoiu et al., 2005; Cerciello et al., 2017). Similarly, in CI users, a potential difference in the cognitive processes associated with cued recall could be that cued recall, much like a recognition task (e.g., recognizing target words among other distractor words), is both a measure of familiarity and recall (Bastin and Van der Linden, 2003). Studies involving recognition tasks have indeed suggested that familiarity and recall are processes occurring independently of one another in the brain (Aggleton and Brown, 2006). In the context of the CVLT-3, the categorical cues given during the delay cued recall subtests may tap into a pre-existing system of familiar words already existing in the participant’s memory. With regards to our study, an increase in performance was observed when semantic cues were provided (1 extra word on average recalled; range of 0–7 words). Participants who may have used the provided CVLT-3 semantic cues to recall more words demonstrated proper encoding; however, they may have had more difficulty with retrieval since the benefit of semantic cues has been shown to demonstrate a retrieval deficit (Farrer and Drozdick, 2020). Participants who did not demonstrate an increase in performance (and therefore did not benefit from provided CVLT-3 cues) may have already been using their own semantic strategies to recall words, such as constructing unique semantic categories or using rehearsal devices. In future administrations of the CVLT-3, asking participants whether they constructed their own semantic cues or not prior to providing the CVLT-3 semantic cues would offer additional insight.
It would be expected that CVLT-3 retrieval performance be related to the ISDA retrieval index; however, in our study, we found that ISDA retrieval deficit calculated with the original scoring method did not relate to performance on any CVLT-3 retrieval measures. Alternately, our less stringent scoring method to calculate the ISDA retrieval deficit did reveal this expected relationship. This alternate ISDA retrieval index was calculated with relaxed criteria; specifically, a participant could recall a word across three or four subtests and avoid increasing their overall retrieval deficit score. In other words, a participant’s retrieval deficit score was not increased if they failed to recall a word on one subtest, but rather, they were given a point toward their retrieval deficit score if they failed to recall a word for two or more subtests. This alternate index still required the participant to recall a target word on at least one short delay and long delay condition. Our data indicated that 8.33 words on average satisfied the original ISDA retrieval index criteria and were recalled across all four delayed recall subtests, whereas with the less restrictive retrieval index, 10.44 words were recalled on at least three or more delayed recall subtests. While the mean difference between the original and alternate retrieval indices is only two words, the less restrictive retrieval index significantly related with a CVLT-3 retrieval measure (long-delay free recall). Our results highlight that the alternate ISDA retrieval index may be beneficial in capturing an element of retrieval that is not part of the ISDA original score. Indeed, long-delay free recall is often considered to be a more pure measure of retrieval abilities based on its lack of interference from distractor words (i.e., list B; Ebert and Anderson, 2009; Farrer and Drozdick, 2020). To understand the relationship between our alternate retrieval measure and the CVLT-3 short and long delay delayed recall conditions, we calculated which of the four conditions a participant was most likely to forget a target word. We found that when a word was recalled three out of the four possible times that the condition where a word was most likely forgotten was long-delay free recall. Specifically, we determined that target words were forgotten 21, 11, 27, and 14 times across all participants on the CVLT-3 short-delay free, short-delay cued, long-delay free, and long-delay cued subtests, respectively. With the original ISDA scoring method, these forgotten words would count toward an overall retrieval deficit without accounting for the fact that the majority of these instances of forgetting occurred during the long-delay free recall subtest. Perhaps our less stringent ISDA retrieval scoring method provided more sensitivity to the presence (or absence) of a retrieval deficit and therefore revealed this expected significant relationship with long-delay free recall ability. However, additional work is needed to determine the clinical utility of this alternate score in a CI patient population as well as expanding this scoring method to a normal hearing population.
Limitations and Future Work
This study had several limitations, mainly in its relatively small and specific sample size, and lack of age-matched normal hearing control subjects. Our study consisted of mostly older adults with high-performing speech perception abilities and thus, our findings may not generalize to all CI users. Future research should examine delayed recall abilities and apply the ISDA to other groups of CI users such as those with lower speech perception performance (Moberly et al., 2016), single sided deafness (SSD; Sharma et al., 2016), and younger participants (Cartocci et al., 2019) to further explore the validity of these constructs. Although our sample size is not atypical of research surrounding CIs (Moberly et al., 2018; Sladen et al., 2018; Mancini et al., 2020; Zhan et al., 2020), this may have limited our ability to detect smaller differences in performance and may have contributed to a lack of relationship between the MoCA and CVLT-3 measures. While the ISDA has been used in other clinical populations (Wright et al., 2009, 2010; Cattie et al., 2012; Oltra-Cucarella et al., 2014; Tayim et al., 2016; Basso et al., 2021), this was the first study to apply the ISDA scoring method to a CI population, and thus this study offers an additional set of constructs, rarely used in previous CI studies, to describe delayed recall abilities in this population. Another limitation of this study was that the modality of test presentation was either auditory (CVLT-3) or auditory-visual (MoCA), which introduces additional difficulties for individuals with HL. We previously explored differences in modality with the MoCA and a version of the MoCA for hearing-impaired populations (i.e., the HI-MoCA, a version of the MoCA that is presented entirely in the visual modality via PowerPoint presentation) that demonstrated little influence on overall performance for CI users (Lin et al., 2017; Parada et al., 2020). While previous literature has explored the utility of a non-auditory CVLT-II (Pisoni et al., 2018), future research could examine specific cognitive relationships alongside speech perception performance with a non-auditory administration of the CVLT-3. Additionally, employing tests such as the Free and Cued Selective Reminding Test (FCSRT; Buschke, 1984), which alternative to the CVLT-3 provides category cues to participants at the beginning of the assessment, could help further elucidate differences between free and cued delayed recall abilities in this population.
Conclusion
While CVLT-3 and ISDA measures did not relate with the MoCA, our work indicates that the ISDA can successfully be applied to CI users to quantify delayed recall ability. Specifically, the advantage of the ISDA is that it provides a discrete measure of consolidation, although our results also highlight that an alternate ISDA retrieval score may be needed. Our work, however, should be considered preliminary as additional work is needed to assess the clinical utility of the original and alternate ISDA scoring methods in both a normal hearing and more expansive CI patient population.
Data Availability Statement
The datasets presented in this article are not readily available because the Auditory Research Laboratory is part of a hospital system that does not allow for data sharing due to patient privacy requirements. Requests to access the datasets should be directed to corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Swedish Medical Center Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
NB, JP and AP-C completed the statistical analysis of data. NB created the figures and tables. NB, EE and AP-C wrote the manuscript. JP and JH contributed to editing the manuscript. All authors approved the submitted version, contributed to the study design, and participated in data collection.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We wish to thank the patients who donated their valuable time and the Swedish Neuroscience Institute for supporting this study.
References
Aggleton, J. P., and Brown, M. W. (2006). Interleaving brain systems for episodic and recognition memory. Trends Cogn. Sci. 10, 455–463. doi: 10.1016/j.tics.2006.08.003
Al-Yawer, F., Pichora-Fuller, M. K., and Phillips, N. A. (2019). The Montreal Cognitive Assessment after omission of hearing-dependent subtests: psychometrics and clinical recommendations. J. Am. Geriatr. Soc. 67, 1689–1694. doi: 10.1111/jgs.15940
Ambert-Dahan, E., Routier, S., Marot, L., Bouccara, D., Sterkers, O., Ferrary, E., et al. (2017). Cognitive evaluation of cochlear implanted adults using CODEX and MoCA screening tests. Otol. Neurotol. 38, e282–e284. doi: 10.1097/MAO.0000000000001464
Armstrong, N. M., An, Y., Ferrucci, L., Deal, J. A., Lin, F. R., and Resnick, S. M. (2020). Temporal sequence of hearing impairment and cognition in the Baltimore longitudinal study of aging. J. Gerontol. A 75, 574–580. doi: 10.1093/gerona/gly268
Atkinson, R. C., and Shiffrin, R. M. (1968). Human memory: a proposed system and its control processes. Psychol. Learn. Motiv. 2, 89–195. doi: 10.1016/S0079-7421(08)60422-3
Basso, M. R., Whiteside, D., Combs, D., Woods, S. P., Hoffmeister, J., Mulligan, R., et al. (2021). Memory in multiple sclerosis: a reappraisal using the item specific deficit approach. Neuropsychology 35:207. doi: 10.1037/neu0000712
Bastin, C., and Van der Linden, M. (2003). The contribution of recollection and familiarity to recognition memory: a study of the effects of test format and aging. Neuropsychology 17:14. doi: 10.1037/0894-4105.17.1.14
Boxtel, M. V., Beijsterveldt, V. C., and Jolles, J. (2000). Mild hearing impairment can reduce verbal memory performance in a healthy adult population. J. Clin. Exp. Neuropsychol. 22, 147–154. doi: 10.1076/1380-3395(200002)22:1;1-8;FT147
Brainerd, C. J., Wright, R., Reyna, V. F., and Payne, D. G. (2002). Dual-retrieval processes in free and associative recall. J. Mem. Lang. 46, 120–152. doi: 10.1006/jmla.2001.2796
Brown, L., Sherbenou, R. J., and Johnsen, S. K. (2010). Test of Nonverbal Intelligence: TONI-4. Austin, TX: Pro-Ed.
Brown, S. C., and Craik, F. I. (2000). “Encoding and retrieval of information,” in The Oxford Handbook of Memory, eds E. Tulving and F. I. M. Craik (Oxford: Oxford University Press), 93–107.
Buschke, H. (1984). Cued recall in amnesia. J. Clin. Exp. Neuropsychol. 6, 433–440. doi: 10.1080/01688638408401233
Cartocci, G., Scorpecci, A., Borghini, G., Maglione, A. G., Inguscio, B. M. S., Giannantonio, S., et al. (2019). EEG rhythms lateralization patterns in children with unilateral hearing loss are different from the patterns of normal hearing controls during speech-in-noise listening. Hear. Res. 379, 31–42. doi: 10.1016/j.heares.2019.04.011
Cattie, J. E., Woods, S. P., Arce, M., Weber, E., Delis, D. C., Grant, I., et al. (2012). Construct validity of the item-specific deficit approach to the California verbal learning test in HIV infection. Clin. Neuropsychol. 26, 288–304. doi: 10.1080/13854046.2011.653404
Cerciello, M., Isella, V., Proserpi, A., and Papagno, C. (2017). Assessment of free and cued recall in Alzheimer’s disease and vascular and frontotemporal dementia with 24-item Grober and Buschke test. Neurol. Sci. 38, 115–122. doi: 10.1007/s10072-016-2722-7
Chandramouli, S. H., Kronenberger, W. G., and Pisoni, D. B. (2019). Verbal learning and memory in early-implanted, prelingually deaf adolescent and adult cochlear implant users. J. Speech Lang. Hear. Res. 62, 1033–1050. doi: 10.1044/2018_JSLHR-H-18-0125
Costa, A. S., Fimm, B., Friesen, P., Soundjock, H., Rottschy, C., Gross, T., et al. (2012). Alternate-form reliability of the Montreal cognitive assessment screening test in a clinical setting. Dement. Geriatr. Cogn. Dis. 33, 379–384. doi: 10.1159/000340006
Craik, F. I., and Lockhart, R. S. (1972). Levels of processing: a framework for memory research. J. Verbal Learning Verbal Behav. 11, 671–684. doi: 10.1016/S0022-5371(72)80001-X
Deal, J. A., Sharrett, A. R., Albert, M. S., Coresh, J., Mosley, T. H., Knopman, D., et al. (2015). Hearing impairment and cognitive decline: a pilot study conducted within the atherosclerosis risk in communities neurocognitive study. Am. J. Epidemiol. 181, 680–690. doi: 10.1093/aje/kwu333
Delis, D. C., Kramer, J. H., Kaplan, E., and Ober, B. A. (2017). California Verbal Learning Test (CVLT-3), 3rd Edn. London: Pearson.
Delis, D. C., Massman, P. J., Butters, N., Salmon, D. P., Cermak, L. S., and Kramer, J. H. (1991). Profiles of demented and amnesic patients on the California verbal learning test: implications for the assessment of memory disorders. Psychol. Assess. 3:19. doi: 10.1037/1040-3590.3.1.19
Dubois, B., Feldman, H. H., Jacova, C., Hampel, H., Molinuevo, J. L., Blennow, K., et al. (2014). Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol. 13, 614–629. doi: 10.1016/S1474-4422(14)70090-0
Dupuis, K., Pichora-Fuller, M. K., Chasteen, A. L., Marchuk, V., Singh, G., and Smith, S. L. (2015). Effects of hearing and vision impairments on the Montreal Cognitive Assessment. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 22, 413–437. doi: 10.1080/13825585.2014.968084
Ebert, P. L., and Anderson, N. D. (2009). Proactive and retroactive interference in young adults, healthy older adults, and older adults with amnestic mild cognitive impairment. J. Int. Neuropsychol. Soc. 15, 83–93. doi: 10.1017/S1355617708090115
Eshkoor, S. A., Hamid, T. A., Mun, C. Y., and Ng, C. K. (2015). Mild cognitive impairment and its management in older people. Clin. Interv. Aging 10:687. doi: 10.2147/CIA.S73922
Farrer, T. J., and Drozdick, L. W. (2020). Essentials of the California Verbal Learning Test: CVLT-C, CVLT-2, and CVLT3. Hoboken, NJ: John Wiley & Sons.
Gajadeera, E. A., Galvin, K. L., Dowell, R. C., and Busby, P. A. (2017). The change in electrical stimulation levels during 24 months postimplantation for a large cohort of adults using the Nucleus® cochlear implant. Ear Hear. 38, 357–367. doi: 10.1097/AUD.0000000000000405
García-Herranz, S., Díaz-Mardomingo, M. C., and Peraita, H. (2016). Neuropsychological predictors of conversion to probable Alzheimer disease in elderly with mild cognitive impairment. J. Neuropsychol. 10, 239–255. doi: 10.1111/jnp.12067
Goman, A. M., Reed, N. S., and Lin, F. R. (2017). Addressing estimated hearing loss in adults in 2060. JAMA Otolaryngol. Head Neck Surg. 143, 733–734. doi: 10.1001/jamaoto.2016.4642
Hillyer, J., Parada, J. C., and Parbery-Clark, A. (2020). Assessing performance on the Montreal Cognitive Assessment (MoCA) in experienced cochlear implant users: use of alternative scoring guidelines. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 27, 397–411. doi: 10.1080/13825585.2019.1624684
Ivanoiu, A., Adam, S., Van der, L. M., Salmon, E., Juillerat, A. C., Mulligan, R., et al. (2005). Memory evaluation with a new cued recall test in patients with mild cognitive impairment and Alzheimer’s disease. J. Neurol. 252, 47–55. doi: 10.1007/s00415-005-0597-2
Klages, J. D., Fisk, J. D., and Rockwood, K. (2005). APOE genotype, vascular risk factors, memory test performance and the five-year risk of vascular cognitive impairment or Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 20, 292–297. doi: 10.1159/000088317
Kline, T. (2005). Psychological Testing: A Practical Approach to Design and Evaluation. Thousand Oaks, CA: Sage. doi: 10.4135/9781483385693
Kramer, S., Vasil, K. J., Adunka, O. F., Pisoni, D. B., and Moberly, A. C. (2018). Cognitive functions in adult cochlear implant users, cochlear implant candidates, and normal-hearing listeners. Laryngoscope Investig. Otolaryngol. 3, 304–310. doi: 10.1002/lio2.172
Kravitz, E., Schmeidler, J., and Beeri, M. S. (2012). Cognitive decline and dementia in the oldest-old. Rambam Maimonides Med. J. 3:e0026. doi: 10.5041/RMMJ.10092
Kronenberger, W. G., and Pisoni, D. B. (2019). Assessing higher order language processing in long-term cochlear implant users. Am. J. Speech Lang. Pathol. 28, 1537–1553. doi: 10.1044/2019_AJSLP-18-0138
Lim, M. Y. L., and Loo, J. H. Y. (2018). Screening an elderly hearing impaired population for mild cognitive impairment using Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA). Int. J. Geriatr. Psychiatry 33, 972–979. doi: 10.1002/gps.4880
Lin, V. Y., Chung, J., Callahan, B. L., Smith, L., Gritters, N., Chen, J. M., et al. (2017). Development of cognitive screening test for the severely hearing impaired: hearing-impaired MoCA. Laryngoscope 127, S4–S11. doi: 10.1002/lary.26590
Mancini, P., Dincer, D., Alessandro, H., Portanova, G., Atturo, F., Russo, F. Y., et al. (2020). Bimodal cochlear implantation in elderly patients. Int. J. Audiol. 60, 469–478. doi: 10.1080/14992027.2020.1843080
Melton, A. W. (1963). Implications of short-term memory for a general theory of memory. J. Verbal Learning Verbal Behav. 2, 1–21. doi: 10.21236/AD0422425
Miller, G. A. (1956). The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol. Rev. 63:81. doi: 10.1037/h0043158
Moberly, A. C., Bates, C., Harris, M. S., and Pisoni, D. B. (2016). The enigma of poor performance by adults with cochlear implants. Otol. Neurotol. 37:1522. doi: 10.1097/MAO.0000000000001211
Moberly, A. C., Harris, M. S., Boyce, L., Vasil, K., Wucinich, T., Pisoni, D. B., et al. (2018). Relating quality of life to outcomes and predictors in adult cochlear implant users: are we measuring the right things? Laryngoscope 128, 959–966. doi: 10.1002/lary.26791
Moseley, S. A. (2018). Cognitive and Psychosocial Associations of Hearing Loss in Older Adults. New Orleans, LA: International Neuropsychological Society.
Murdock, B. B. Jr. (1967). Recent developments in short-term memory. Br. J. Psychol. 58, 421–433. doi: 10.1111/j.2044-8295.1967.tb01099.x
Nasreddine, Z. S., and Patel, B. B. (2016). Validation of Montreal cognitive assessment, MoCA, alternate French versions. Can. J. Neurol. Sci. 43, 665–671. doi: 10.1017/cjn.2016.273
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The Montreal Cognitive Assessment, MoCA: a brief screening toolfor mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Nobel, P. A., and Shiffrin, R. M. (2001). Retrieval processes in recognition and cued recall. J. Exp. Psychol. Learn. Mem. Cogn. 27, 384–413. doi: 10.1037/0278-7393.27.2.384
Nyberg, L., Forkstam, C., Petersson, K. M., Cabeza, R., and Ingvar, M. (2002). Brain imaging of human memory systems: between-systems similarities and within-system differences. Cogn. Brain Res. 13, 281–292. doi: 10.1016/S0926-6410(02)00052-6
Ogawa, T., Uchida, Y., Nishita, Y., Tange, C., Sugiura, S., Ueda, H., et al. (2019). Hearing-impaired elderly people have smaller social networks: a population-based aging study. Arch. Gerontol. Geriatr. 83, 75–80. doi: 10.1016/j.archger.2019.03.004
Oltra-Cucarella, J., Pérez-Elvira, R., and Duque, P. (2014). Benefits of deep encoding in Alzheimer’s disease. Analysis of performance in a memory task using the Item Specific Deficit Approach. Neurologia 29, 286–293. doi: 10.1016/j.nrleng.2013.06.002
Olusanya, B. O., Neumann, K. J., and Saunders, J. E. (2014). The global burden of disabling hearing impairment: a call to action. Bull. World Health Organ. 92, 367–373. doi: 10.2471/BLT.13.128728
Padilla-Walker, L. M., and Poole, D. A. (2002). Memory for previous recall: a comparison of free and cued recall. Appl. Cogn. Psychol. 16, 515–524. doi: 10.1002/acp.809
Parada, J. C., Hillyer, J., and Parbery-Clark, A. (2020). Performance on the standard and hearing-impaired Montreal Cognitive Assessment in cochlear implant users. Int. J. Geriatr. Psychiatry 35, 338–347. doi: 10.1002/gps.5267
Pedhazur, E. J., and Schmelkin, L. P. (1991). Measurement, Design, and Analysis: An Integrated Approach. Hillsdale, NJ: Lawrence Erlbaum Associates.
Petersen, R. C. (2011). Mild cognitive impairment. N. Engl. J. Med. 364, 2227–2234. doi: 10.1056/NEJMcp0910237
Pisoni, D. B., Broadstock, A., Wucinich, T., Safdar, N., Miller, K., Hernandez, L. R., et al. (2018). Verbal learning and memory after cochlear implantation in postlingually deaf adults: some new findings with the CVLT-II. Ear Hear. 39:720. doi: 10.1097/AUD.0000000000000530
Rigters, S. C., van der Schroeff, M. P., Papageorgiou, G., de Jong, R. J. B., and Goedegebure, A. (2018). Progression of hearing loss in the aging population: repeated auditory measurements in the rotterdam study. Audiol. Neurotol. 23, 290–297. doi: 10.1159/000492203
Sharma, A., Glick, H., Campbell, J., Torres, J., Dorman, M., and Zeitler, D. M. (2016). Cortical plasticity and re-organization in pediatric single-sided deafness pre-and post-cochlear implantation: a case study. Otol. Neurotol. 37:e26. doi: 10.1097/MAO.0000000000000904
Shen, J., Sherman, M., and Souza, P. E. (2020). Test administration methods and cognitive test scores in older adults with hearing loss. Gerontology 66, 24–32. doi: 10.1159/000500777
Sladen, D. P., Nie, Y., and Berg, K. (2018). Investigating speech recognition and listening effort with different device configurations in adult cochlear implant users. Cochlear Implants Int. 19, 119–130. doi: 10.1080/14670100.2018.1424513
Spahr, A. J., Dorman, M. F., Litvak, L. M., Van Wie, S., Gifford, R. H., Loizou, P. C., et al. (2012). Development and validation of the AzBio sentence lists. Ear Hear. 33:112. doi: 10.1097/AUD.0b013e31822c2549
Tayim, F. M., Flashman, L. A., Wright, M. J., Roth, R. M., and McAllister, T. W. (2016). Recovery of episodic memory subprocesses in mild and complicated mild traumatic brain injury at 1 and 12 months post injury. J. Clin. Exp. Neuropsychol. 38, 1005–1014. doi: 10.1080/13803395.2016.1182968
Tromp, D., Dufour, A., Lithfous, S., Pebayle, T., and Després, O. (2015). Episodic memory in normal aging and Alzheimer disease: insights from imaging and behavioral studies. Ageing Res. Rev. 24, 232–262. doi: 10.1016/j.arr.2015.08.006
Tulving, E., and Pearlstone, Z. (1966). Availability versus accessibility of information in memory for words. J. Verbal Learning Verbal Behav. 5, 381–391. doi: 10.1016/S0022-5371(66)80048-8
Utoomprurkporn, N., Woodall, K., Stott, J., Costafreda, S. G., and Bamiou, D. E. (2020). Hearing-impaired population performance and the effect of hearing interventions on Montreal Cognitive Assessment (MoCA): systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 35, 962–971. doi: 10.1002/gps.5354
Wiegner, S., and Donders, J. (1999). Performance on the California Verbal Learning Test after traumatic brain injury. J. Clin. Exp. Neuropsychol. 21, 159–170. doi: 10.1076/jcen.21.2.159.925
Wright, M. J., Schmitter-Edgecombe, M., and Woo, E. (2010). Verbal memory impairment in severe closed head injury: the role of encoding and consolidation. J. Clin. Exp. Neuropsychol. 32, 728–736. doi: 10.1080/13803390903512652
Wright, M. J., Woo, E., Schmitter-Edgecombe, M., Hinkin, C. H., Miller, E. N., and Gooding, A. L. (2009). The Item-Specific Deficit Approach to evaluating verbal memory dysfunction: rationale, psychometrics, and application. J. Clin. Exp. Neuropsychol. 31, 790–802. doi: 10.1080/13803390802508918
Zhan, K. Y., Lewis, J. H., Vasil, K. J., Tamati, T. N., Harris, M. S., Pisoni, D. B., et al. (2020). Cognitive functions in adults receiving cochlear implants: predictors of speech recognition and changes after implantation. Otol. Neurotol. 41, e322–e329. doi: 10.1097/MAO.0000000000002544
Keywords: cochlear implant, delayed recall, hearing loss, encoding, consolidation, retrieval, Montreal Cognitive Assessment, California Verbal Learning Test
Citation: Brumer N, Elkins E, Parada J, Hillyer J and Parbery-Clark A (2021) Examining Delayed Recall in Cochlear Implant Users Using the Montreal Cognitive Assessment, California Verbal Learning Test, Third Edition, and Item Specific Deficit Approach: Preliminary Results. Front. Psychol. 12:749045. doi: 10.3389/fpsyg.2021.749045
Received: 28 July 2021; Accepted: 04 October 2021;
Published: 04 November 2021.
Edited by:
Antonino Vallesi, University of Padua, ItalyReviewed by:
Giulia Cartocci, Sapienza University of Rome, ItalyBarbara Arfé, University of Padua, Italy
Alessandro Castiglione, University of Padua, Italy
Copyright © 2021 Brumer, Elkins, Parada, Hillyer and Parbery-Clark. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandra Parbery-Clark, QWxleGFuZHJhLlBhcmJlcnktQ2xhcmtAc3dlZGlzaC5vcmc=