
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 19 August 2021
Sec. Health Psychology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.723035
This article is part of the Research Topic Psychological Distress, Burnout, Quality of Life, and Wellness among Healthcare Workers View all 14 articles
 Anna Larysz1†
Anna Larysz1† Izabella Uchmanowicz2,3*†
Izabella Uchmanowicz2,3*†Background: The nursing profession is predisposed toward depressed mood and depressive symptoms. The multidirectionality and intensity of stressors in the nurses' occupational environment are of great significance in this respect. The study aimed to evaluate the impact of selected sociodemographic factors on depressive symptoms among cardiac nurses.
Methods: This cross-sectional study included 336 cardiac nurses (302 women and 34 men) and was conducted between December 2019 and September 2020 in four hospital cardiac units in Wroclaw, Poland. Sociodemographic data were collected using a self-developed survey. The following standardized instruments were used for the study outcomes: Patient Health Questionnaire-9 (PHQ-9) and Beck Depression Inventory (BDI).
Results: The study among cardiac nurses showed mild depression in 11.61%, moderate depression in 5.06%, and severe depression in 2.68%. Linear regression models showed that significant (p < 0.05) predictors of the PHQ-9 score included (1) higher occupational education (bachelor's degree), graduation “only” from medical high school or “other” education; (2) work experience of 16–20 years; (3) living in a relationship; (4) living in a rural area. Linear regression models showed that significant (p < 0.05) predictors of the BDI score included (1) higher occupational education (bachelor's degree); (2) graduation “only” from medical high school or “other” education; (3) living in a relationship.
Conclusions: Depressive symptoms are a significant problem among Polish cardiac nurses. The prevalence of depressive symptoms is affected by the education level, employment form, marital status, and place of residence.
Depression and mood disorders are serious health problems, especially in developed countries. It is estimated that 12.9% of the worldwide population is affected by depression, with the highest percentage in South America (20.6%) and the lowest in Australia (7.3%) (Lim et al., 2018). In Poland, approximately 3% of the population suffers from depression (Kiejna et al., 2015), and women are more frequently affected than men (Lim et al., 2018).
Due to the incidence of depression in developed countries, the countries have to bear high economic and social costs (Kessler and Bromet, 2013). Economic costs are associated with the treatment of depression, and therefore, approximately PLN 170 million (about EUR 37.8 million) is spent on this purpose in Poland. The social costs are PLN 1–2.6 billion (about EUR 0.22–0.58 billion) annually (Drapała et al., 2014). It was also reported that the annual cost of inpatient care of depression in 2016 was EUR 491 in Poland and EUR 2,848 in Germany (Zaprutko et al., 2018). In addition, there are also indirect costs linked to sickness absenteeism, which is four times more frequent in individuals with depression, and reduced productivity (Cocker et al., 2014).
It is well known that nursing is a profession that especially predisposes to depression (Duan-Porter et al., 2018). The primary reason is the multidirectional character and intensity of occupational stressors (Sarafis et al., 2016; Yoshizawa et al., 2016), coexisted anxiety (Maharaj et al., 2006), and deteriorated psychosomatic wellbeing (Gu et al., 2019), especially considering among frontline nurses in emergency departments during the COVID-19 outbreak (An et al., 2020). Additional predisposing factors include shift work, multi-tasking, constant readiness to deal with a suffering person, a sense of responsibility for the therapeutic process, problems with autonomy in decision-making, a decreasing number of nurses due to staff shortages, and insufficient psychological and financial compensation (Hersch et al., 2016; Kliszcz, 2017). Previous studies have shown that the incidence of depression in early education, already among nursing students, is ~ 24% (Cheung et al., 2016). In contrast, the prevalence of depression among active nurses ranges from 8.8% in Norway (Øyane et al., 2013) to 64.25% in Poland (Kubik et al., 2018).
Anxiety, depression, and aggression, as psychopathological representations of negative affective states, are emotions that are frequently suppressed by highly socialized individuals (Neumann et al., 2010; Compare et al., 2014). The way social roles are fulfilled and factors related to the occupational environment itself may imply the emergence of depressive states. The complexity of the aforementioned biopsychosocial conditions determining the essence of nursing as a profession that overexploits physical and mental potential should be noted. Without a doubt, studies on depression in this professional group are still considered important and necessary. The constantly changing work-related occupational factors and the specificity of nurses' work in a given specialty indicate the need to update scientific evidence and current knowledge. Moreover, there are still limited studies on the subject in relation to nurses who specialize in cardiology. Therefore, this study aimed to evaluate the influence of selected sociodemographic factors on the prevalence of depressive symptoms among cardiac nurses.
This cross-sectional study included 336 cardiac nurses (302 women and 34 men) aged between 20–60 years and was conducted between December 2019 and September 2020 in four hospital cardiac units in Wroclaw, Poland. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed in the design and reporting of this study (von Elm et al., 2007).
The study group consisted of cardiac nurses working in hospital wards in Wroclaw, Poland. The exclusion criteria included nurses who were not specialized in cardiology, those diagnosed with some prior mental disorder, and those who did not give their informed consent to participate in the study.
In this study, cardiac nurses from one academic city of Wroclaw were recruited by convenience sampling through personal contact with the research team. The printed questionnaires were prospectively distributed to the group of 469 nurses by their supervisors, who were informed of the eligibility criteria for participation in the study. Supervisors were also responsible for collecting the completed questionnaires. Nurses were informed that participation in the study is voluntary, and they were assured of complete anonymity. In total, 78% of completed questionnaires were returned with 22% missing data. It means that complete data from 366 cardiac nurses were included in the analysis. Researcher Anna Larysz was responsible for verification of the questionnaires' completeness, data collection, and its implementation into the database.
Sample size was calculated by using formula developed for observational and experimental nursing research studies: n = {(Z1–α/2)2 (p) (q)}/d2, where prevalence rate for assessment of depression among nurses was considered 40% (Sharma et al., 2020). Based on data from the Supreme Chamber of Nurses and Midwives, nearly 261,000 nurses were employed in Poland at the time of the study. It was determined that a minimum sample size of 334 completed questionnaires was needed to achieve a confidence level of 95% and that the real value is within ±5% of the confidence interval. The final statistical analysis was performed on data received from 366 study participants.
Sociodemographic and other related background data were collected using a self-developed survey for sociodemographic data.
The PHQ-9 is a standardized self-report questionnaire used for screening to diagnose depressive symptoms in the overall population. It ensures both the diagnosis of depression and the evaluation of the severity of its symptoms (Kroenke et al., 2001). The Polish version of the PHQ-9 was translated and validated by Tomaszewski et al. (2011). The PHQ-9 consists of nine main questions and one supplementary question. The answer to each question is scored from 0 to 3, depending on the incidence of a given symptom in the past 2 weeks (3—most frequent symptoms). The maximum score was 27, indicating the highest severity of depressive symptoms. The norm is the score of <5; the range of 5–9 indicates mild depression, 10–14 moderate depression, 15–19 moderately severe depression, and 20–27 severe depression (Tomaszewski et al., 2011).
The BDI is a standardized self-report questionnaire that measures characteristic behaviors and depressive symptoms. The questionnaire consists of 21 questions scored from 0 to 3 points; a higher score indicates more severe symptoms of depression (Beck et al., 1961). Internal consistency for the BDI ranges from 0.73 to 0.92 with a mean of 0.86 (Beck et al., 1988). Thus, the BDI shows high internal consistency, with alpha coefficients of 0.86 and 0.81 for psychiatric and non-psychiatric populations, respectively. This study uses the Polish adaptation by Parnowski and Jernajczyk (1977).
The study protocol was approved by the local Bioethics Committee of the Wroclaw Medical University, Poland (no. KB−164/2019). All nurses gave their written informed consent before participating in the study. The study was conducted following the Declaration of Helsinki and Good Clinical Practice guidelines.
The analysis of quantitative variables (i.e., expressed by number) was conducted by calculating the mean, standard deviation, median, quartiles, minimum and maximum values. The analysis of qualitative variables (i.e., not expressed by number) was conducted by calculating the number and percentage of occurrences of each value. Univariate and multivariate analyses of the effect of multiple variables on the quantitative variable were conducted using linear regression. The results are presented as values of the regression model's parameters with a 95% confidence interval. A significance level of 0.05 was adopted in the analysis. The analysis was conducted using the R program, version 4.0.3 (R Core Team, 2019).
A total of 336 cardiac nurses, including 302 (89.88%) women and 34 (10.12%) men, were included in the study. There were 16.67% nurses from the age group of 20–30, 42.43% nurses from the age group of 31–40, 33.33% nurses from the age group of 41–50, and 28.57% from the group of 51–60. The master's degree in nursing was held by 25% nurses, a bachelor's degree by 30.36% nurses, while as many as 30.95% nurses graduated from medical high school. As many as 54.68% of nurses had the greatest seniority that is more than 20 years. Moreover, the majority of the respondents (52.68%) had one job. Most surveyed nurses, 72.02%, were employed under an employment contract. The most typical monthly amount of working time was 101–180 h, and it concerned 57.74% of nurses. Typical working conditions included teamwork (75.60%) and shift work in the form of 12-h duty shifts (75.0%). The vast majority of respondents were in a relationship (69.94%) and lived in a city > 100,000 residents (63.69%) (Table 1).
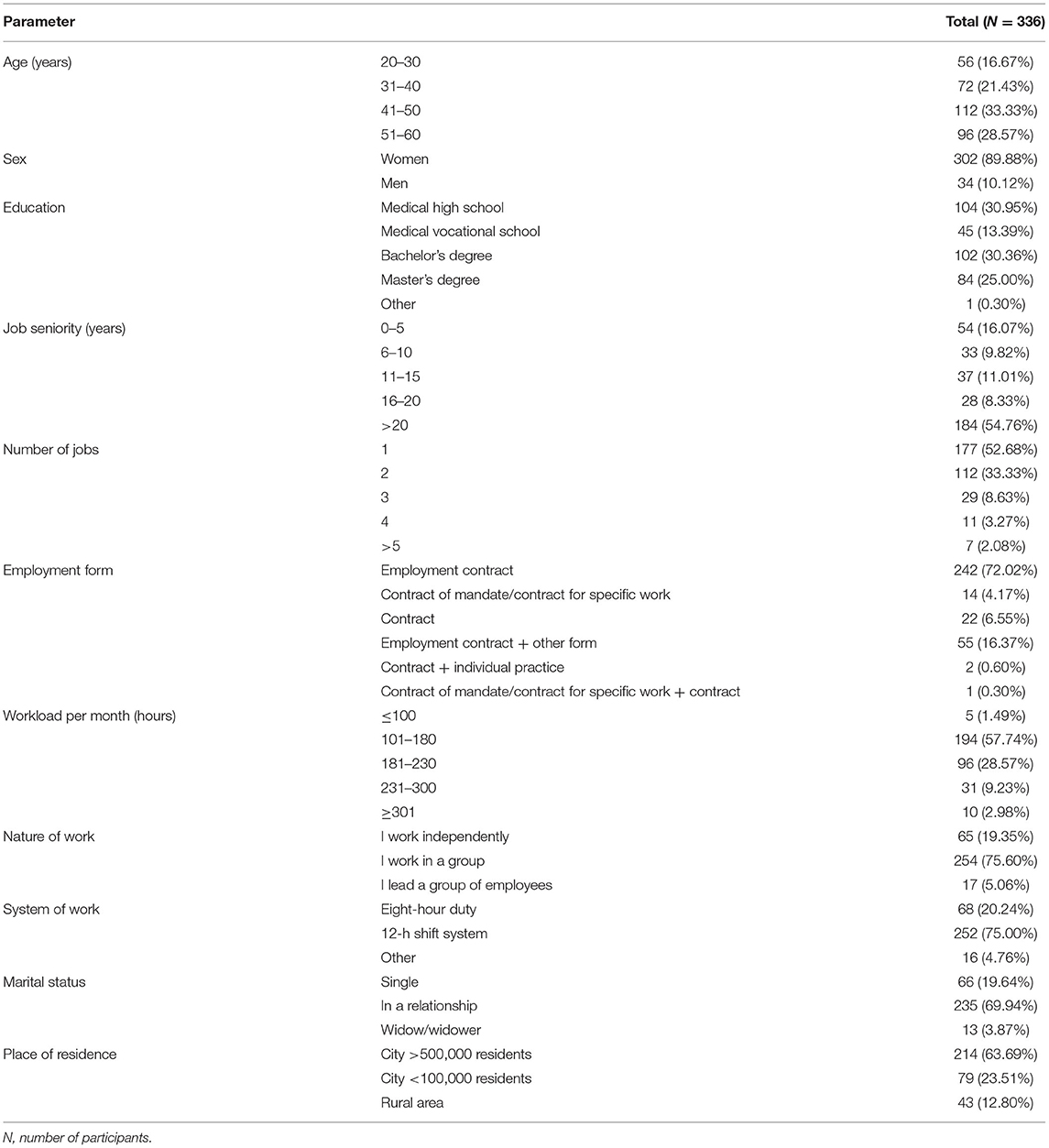
Table 1. Sociodemographic characteristics of surveyed cardiac nurses.
The PHQ-9 questionnaire assesses the severity of depression in a respondent. The tool has standards that ensure the interpretation of scores. A total of 141 out of 336 survey participants (41.96%) had no depressive symptoms, 117 respondents (34.82%) suffered from mild depression, 53 (15.77%) had moderate depression, 17 (5.06%) had moderately severe depression, and 8 (2.38%) suffered from severe depression (Table 2).
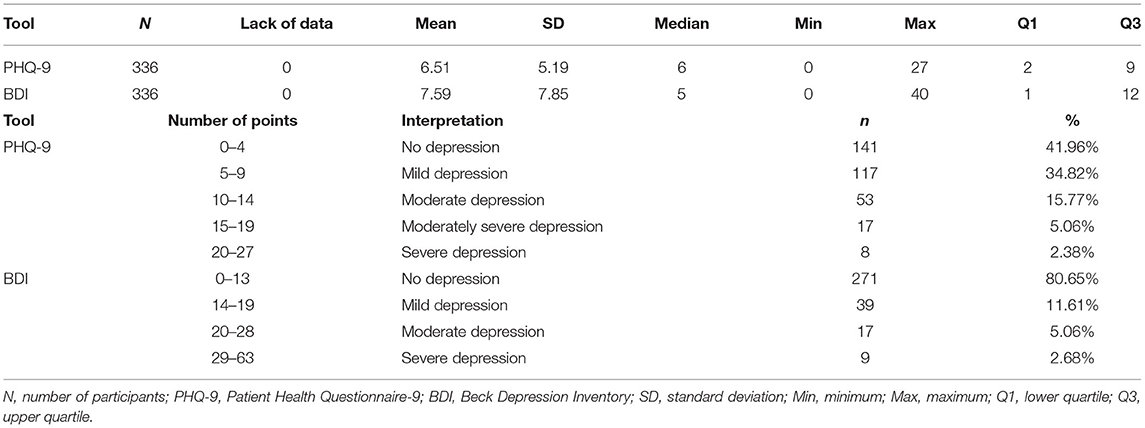
Table 2. Scores and standards for the PHQ-9 and BDI questionnaires.
The BDI provides an assessment of the severity of depressive symptoms in an individual completing the questionnaire. In addition, the BDI has standards that enable the interpretation of the obtained score (Table 2).
No depression was found in 271 out of 336 survey participants (80.65%), mild depression in 39 respondents (11.61%), moderate depression in 17 respondents (5.06%), and severe depression in 9 respondents (2.68%) (Table 2).
Linear regression models (separate for each of the analyzed characteristics) showed that significant (p < 0.05) predictors of the PHQ-9 score include (1) higher vocational education (bachelor's degree): the regression parameter is 1.873 thus it elevates the PHQ-9 score by 1.873 pts on average compared to a master's degree; (2) graduation “only” from medical high school or “other” education: the regression parameter is 1.557 thus it elevates the PHQ-9 score by 1.557 pts on average compared to a master's degree; (3) job seniority of 16–20 years: the regression parameter is −3.21 thus it lowers the PHQ-9 score by 3.21 pts on average compared to job seniority <5 years; (4) living in a relationship: the regression parameter is −2.338 thus it lowers the PHQ-9 score by 2.338 pts on average compared to being single or widowed; (5) living in a rural area: the regression parameter is −1.7, thus it lowers the PHQ-9 score by 1.7 pts on average compared to living in a city >100,000 residents (Table 3).
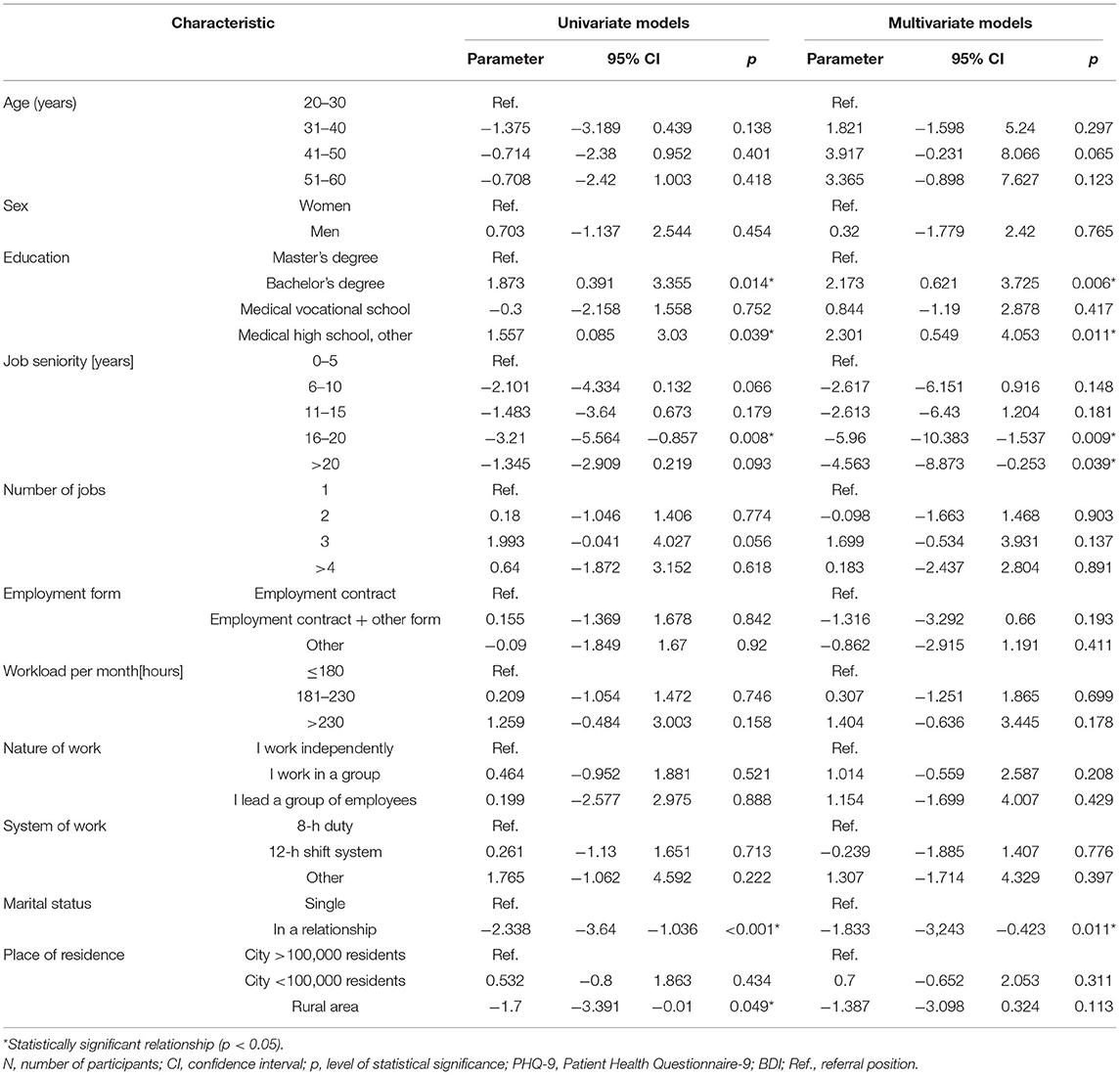
Table 3. Univariate and multivariate analyses for PHQ-9.
The multivariate linear regression model showed that significant (p < 0.05) independent predictors of the PHQ-9 score include (1) higher vocational education (bachelor's degree): the regression parameter is 2.173 thus it elevates the PHQ-9 score by 2.173 pts on average compared to master's degree education; (2) graduation “only” from medical high school or “other” education: the regression parameter is 2.301 thus it elevates the PHQ-9 score by 2.301 pts on average compared to a master's degree; (3) job seniority of 16–20 years: the regression parameter is −5.96 thus it lowers the PHQ-9 score by 5.96 pts on average compared to job seniority <5 years; (4) job seniority >20 years: the regression parameter is −4.563 thus it lowers the PHQ-9 score by 4.563 pts on average compared to job seniority <5 years; (5) living in a relationship: the regression parameter is −1.833 thus it lowers the PHQ-9 score by 1.833 pts on average compared to being single or widowed (Table 3).
The linear regression models (separate for each of the analyzed characteristics) showed that significant (p < 0.05) predictors of the BDI score include (1) higher vocational education (bachelor's degree): the regression parameter is 3.151; thus, it elevates the BDI score by 3.151 pts on average compared to a master's degree; (2) graduation “only” from medical high school or “other” education: the regression parameter is 4.031 thus so it elevates the BDI score by 4.031 pts on average compared to a master's degree; (3) living in a relationship: the regression parameter is −3.551 thus it lowers the BDI score by 3.551 pts on average compared to being single or widowed (Table 4).
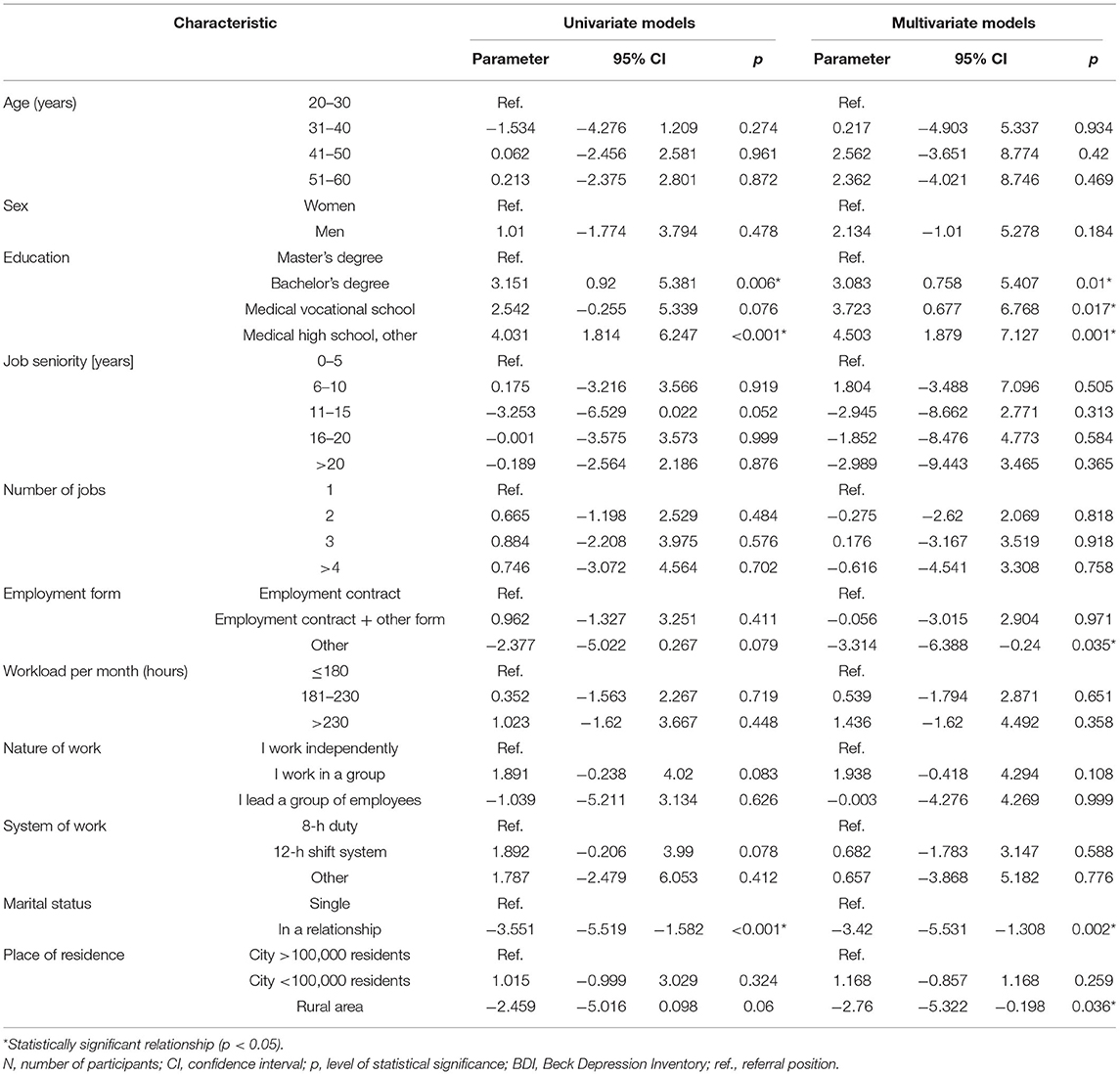
Table 4. Univariate and multivariate analyses for BDI.
The multivariate linear regression model showed that significant (p < 0.05) independent predictors of the BDI score include (1) higher vocational education (bachelor's degree): the regression parameter is 3.083 thus it elevates the BDI score by 3.083 pts on average compared to a master's degree; (2) graduation “only” from medical vocational school: the regression parameter is 3.723 thus it elevates the BDI score by 3.723 pts on average compared to a master's degree; (3) graduation “only” medical high school or “other” education: the regression parameter is 4.503 thus it elevates the BDI score by 4.503 pts on average compared to a master's degree; (4) a form of employment other than an employment contract (solo trader or employment contract combined with another contract): the regression parameter is −3.314 thus it lowers the BDI score by 3.314 pts on average compared to an employment contract; (5) living in a relationship: the regression parameter is −3.42 thus it lowers the BDI score by 3.42 pts on average compared to being single or widowed; (6) living in a rural area: the regression parameter is −2.76 thus it lowers the BDI score by 2.76 pts on average compared to living in a city >100,000 residents (Table 4).
Previous research on the prevalence of depression among active nurses showed wide geographic variation. In highly developed countries, i.e., Norway or Canada, the prevalence is 8.8% and 9.1%, respectively. In the studies conducted in the Philippines, it was shown that depression affects one in five nurses (Batalla et al., 2019), while one in four nurses in Brazil (Schmidt et al., 2011), and one in three active nurses and India (Shajan and Nisha, 2019). The studies conducted in Yoon and Kim (2013), in Japan by Furihata et al. (2020), and in China by Xie et al. (2020) showed that 38.0, 41.7, and 43.83% of nurses, respectively, have depression-related symptoms.
In contrast, a study conducted in Poland by Kubik et al. (2018) showed that depression affects approximately two-thirds of nurses. In this study, the percentage of nurses who were diagnosed with symptoms indicative of depression varied due to a type of screening tool. In the assessment using BDI, <20% of the respondents had symptoms indicating depression, while according to the PHQ-9 scale, almost 60% of the respondents had depression. Due to differences in the tools used for assessing the presence of symptoms indicative of depression, it is complicated to compare the outcomes of the studies. However, some trends can be observed—in highly developed countries where health care funding is significantly higher, the percentage of nurses reporting a depression-related problem is significantly lower. This may be affected by better working conditions and access to professional psychological support, which nurses can use when needed. In the study by Kubik et al. (2018), more than 80% of nurses declared their willingness to use the help of a psychologist or psychotherapist in difficult situations.
The analysis showed that cardiac nurses with education lower than a master's degree were more likely to experience depressive symptoms. This association is consistent with the findings obtained by Ning et al. (2020), who found that depression was more prevalent among younger employees (≤40 years) and medical staff with junior titles. Nurses holding a master's degree may have better job salaries and benefits, so they have less opportunity to worry about Ariapooran (2019).
Ariapooran (2019) and Chiang and Chang (2012) showed that nurses with less seniority reported more depressive symptoms than those with more seniority, which was confirmed in this study in which nurses with more than 20 years of seniority were less likely to experience depressive symptoms than those with less seniority. Nurses with less seniority suffer more severe stress when caring independently for patients with difficult clinical conditions due to less work experience (Ning et al., 2020). It was confirmed that this might translate into an increased risk of depression development (Cheung et al., 2016).
Also, individuals in a relationship had a lower risk of developing depression than those who were single or widowed. This is consistent with the findings of Yoon and Kim (2013) and Ariapooran (2019), according to which single nurses had particularly high levels of depressive symptoms. Our results support the hypothesis that marriage provides greater emotional support to counteract stress reactions among nurses. Beam et al. (2017) showed that marriage reduces the genetic influence of perceived stress on depressive symptoms but does not reduce the influence of environmental factors. Furthermore, marriage may reduce the heritability of depressive symptoms associated with perceived stress. In contrast, Chiang and Chang (2012) and Cheung and Yip (2015) found that married nurses were more likely to have depressive symptoms than those who were single.
This study has also shown that the place of residence of cardiac nurses determined the occurrence of depressive symptoms—individuals living in rural areas had a lower intensity of symptoms indicative of depression. It is possible that communing with nature after work hours and pursuing more active outdoor leisure activities enable nurses to better cope with stressful situations that arise in the workplace.
The strengths of this study were the large sample size and the use of standardized instruments to measure symptoms of depression. However, there were several potential limitations in terms of methodological aspects. The main limitation of the study was linked to the data collection methods used, which were considered a one-time point rather than longitudinal. The study enrolled mainly women, which may be its bias. The method for the selection of the nurses was purposive sampling; the study was conducted among cardiac nurses of four hospitals but within one academic center; therefore, the conclusions cannot be generalized to the broader population of cardiac nurses. Also, some variables associated with depression, such as social support, health status, and pre-existing psychiatric disorders, were not examined. Due to the cross-sectional design of the study, causality between depression and other variables was unable to be investigated.
Furthermore, future research should focus on better recognition of depression among cardiac nurses and the entire nursing professional group, which is essential to consider interventions to improve working conditions and reduce important risk factors for depressive symptoms. Moreover, it is crucial to observe the direct impact of depressive symptoms and professional burnout syndrome on the quality of care provided and, above all, on patient safety. Such findings could be useful for preventing mental health problems among nurses.
Depression is a common problem among cardiac nurses. Therefore, considering the negative impact of depression on quality of care, health authorities should organize regular screening targeting depression and develop preventive measures to alleviate the risk of depression by providing a timely provision of financial support, online psychological counseling service, or on-site psychological guidance.
Depression is a widely prevalent condition among Polish cardiac nurses. The prevalence of depressive symptoms is negatively affected by a lower level of education (lower than a master's degree) and living alone, while it is positively affected by more seniority (over 16 years) and living in a rural area.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Bioethics Committee of the Wroclaw Medical University, Poland (approval no. KB−164/2019). The patients/participants provided their written informed consent to participate in this study.
AL contributed to study conception and design, data acquisition, analysis and interpretation of data, and drafting of the manuscript. IU contributed to study conception and design, analysis and interpretation of data, and critical revision of the manuscript. All authors approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the patients for their contribution in this research.
An, Y., Yang, Y., Wang, A., Li, Y., Zhang, Q., Cheung, T., et al. (2020). Prevalence of depression and its impact on quality of life among frontline nurses in emergency departments during the COVID-19 outbreak. J. Affect. Disord.. 276, 312–315. doi: 10.1016/j.jad.2020.06.047
Ariapooran, S. (2019). Sleep problems and depression in Iranian nurses: the predictive role of workaholism. Iran. J. Nurs. Midwifery Res. 24, 30–37. doi: 10.4103/ijnmr.IJNMR_188_17
Batalla, V. R. D., Barrameda, A. L. N., Basal, J. M. S., Bathan, A. S. J., Bautista, J. E. G., Rebueno, M.a., et al. (2019). Moderating effect of occupational stress on spirituality and depression of registered nurses in tertiary hospital: a structural equation model. J. Adv. Nurs. 75, 772–782. doi: 10.1111/jan.13856
Beam, C. R., Dinescu, D., Emery, R. E., and Turkheimer, E. (2017). A twin study on perceived stress, depressive symptoms, and marriage. J. Health Soc. Behav. 58, 37–53. doi: 10.1177/0022146516688242
Beck, A. T., Steer, R. A., and Carbin, M. G. (1988). Psychometric properties of the beck depression inventory: twenty-five years of evaluation. Clin. Psychol. Rev. 8, 77–100. doi: 10.1016/0272-7358(88)90050-5
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., and Erbaugh, J. (1961). An inventory for measuring depression. Arch. Gen. Psychiatry 4, 561–571. doi: 10.1001/archpsyc.1961.01710120031004
Cheung, T., Wong, S., Wong, K., Law, L., Ng, K., Tong, M., et al. (2016). Depression, anxiety and symptoms of stress among baccalaureate nursing students in Hong Kong: a cross-sectional study. Int. J. Environ. Res. Public. Health 13, 779–804. doi: 10.3390/ijerph13080779
Cheung, T., and Yip, P. (2015). Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int. J. Environ. Res. Public. Health 12, 11072–11100. doi: 10.3390/ijerph120911072
Chiang, Y.-M., and Chang, Y. (2012). Stress, depression, and intention to leave among nurses in different medical units: implications for healthcare management/nursing practice. Health Policy 108, 149–157. doi: 10.1016/j.healthpol.2012.08.027
Cocker, F., Nicholson, J. M., Graves, N., Oldenburg, B., Palmer, A. J., Martin, A., et al. (2014). Depression in working adults: comparing the costs and health outcomes of working when ill. PLoS ONE 9:e105430. doi: 10.1371/journal.pone.0105430
Compare, A., Zarbo, C., Shonin, E., Van Gordon, W., and Marconi, C. (2014). Emotional regulation and depression: a potential mediator between heart and mind. Cardiovasc. Psychiatry Neurol. 2014:324374. doi: 10.1155/2014/324374
Drapała, A., Karczewicz, E., Zalewska, H., Gierczyński, J., Gryglewicz, J., Sielicki, P., et al. (2014). Depresja—analiza kosztów ekonomicznych i społecznych. Warsaw: Lazarski University.
Duan-Porter, W., Hatch, D., Pendergast, J. F., Freude, G., Rose, U., Burr, H., et al. (2018). 12-month trajectories of depressive symptoms among nurses—contribution of personality, job characteristics, coping, and burnout. J. Affect. Disord. 234, 67–73. doi: 10.1016/j.jad.2018.02.090
Furihata, R., Saitoh, K., Suzuki, M., Jike, M., Kaneita, Y., Ohida, T., et al. (2020). A composite measure of sleep health is associated with symptoms of depression among Japanese female hospital nurses. Compr. Psychiatry 97:152151. doi: 10.1016/j.comppsych.2019.152151
Gu, B., Tan, Q., and Zhao, S. (2019). The association between occupational stress and psychosomatic wellbeing among Chinese nurses. Medicine 98:e15836. doi: 10.1097/MD.0000000000015836
Hersch, R. K., Cook, R. F., Deitz, D. K., Kaplan, S., Hughes, D., Friesen, M. A., et al. (2016). Reducing nurses' stress: a randomized controlled trial of a web-based stress management program for nurses. Appl. Nurs. Res. 32, 18–25. doi: 10.1016/j.apnr.2016.04.003
Kessler, R. C., and Bromet, E. J. (2013). The epidemiology of depression across cultures. Annu. Rev. Public Health 34, 119–138. doi: 10.1146/annurev-publhealth-031912-114409
Kiejna, A., Piotrowski, P., Adamowski, T., Moskalewicz, J., Wciórka, J., Stokwiszewski, J., et al. (2015). The prevalence of common mental disorders in the population of adult Poles by sex and age structure—an EZOP Poland study. Psychiatr. Pol. 49, 15–27. doi: 10.12740/PP/30811
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Kubik, B., Jurkiewicz, B., Kołpa, M., and Stepie,ń, K. (2018). Nurses' health in the context of depressive symptoms. Med. Stud. 34, 147–152. doi: 10.5114/ms.2018.76876
Lim, G. Y., Tam, W. W., Lu, Y., Ho, C. S., Zhang, M. W., and Ho, R. C. (2018). Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 8:2861. doi: 10.1038/s41598-018-21243-x
Maharaj, H., Maharaj, D. S., and Daya, S. (2006). Acetylsalicylic acid and acetaminophen protect against oxidative neurotoxicity. Metab. Brain Dis. 21, 189–199. doi: 10.1007/s11011-006-9012-7
Neumann, I. D., Veenema, A. H., and Beiderbeck, D. I. (2010). Aggression and anxiety: social context and neurobiological links. Front. Behav. Neurosci. 4:12. doi: 10.3389/fnbeh.2010.00012
Ning, X., Yu, F., Huang, Q., Li, X., Luo, Y., Huang, Q., et al. (2020). The mental health of neurological doctors and nurses in Hunan Province, China during the initial stages of the COVID-19 outbreak. BMC Psychiatry 20:436. doi: 10.1186/s12888-020-02838-z
Øyane, N. M. F., Pallesen, S., Moen, B. E., Åkerstedt, T., and Bjorvatn, B. (2013). Associations between night work and anxiety, depression, insomnia, sleepiness and fatigue in a sample of Norwegian nurses. PLoS ONE 8:e70228. doi: 10.1371/journal.pone.0070228
Parnowski, T., and Jernajczyk, W. (1977). Inwentarz Depresji Becka w ocenie nastroju osób zdrowych i chorych na choroby afektywne (ocena pilotazowa). Psychiatr. Pol. 11, 417–425.
R Core Team (2019). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. Available online at: https://www.R-project.org/ (accessed June 1, 2021).
Sarafis, P., Rousaki, E., Tsounis, A., Malliarou, M., Lahana, L., Bamidis, P., et al. (2016). The impact of occupational stress on nurses' caring behaviors and their health related quality of life. BMC Nurs. 15:56. doi: 10.1186/s12912-016-0178-y
Schmidt, D. R. C., Dantas, R. A. S., and Marziale, M. H. P. (2011). Anxiety and depression among nursing professionals who work in surgical units. Rev. Esc. Enferm. USP 45, 487–493. doi: 10.1590/S0080-62342011000200026
Shajan, A., and Nisha, C. (2019). Anxiety and depression among nurses working in a tertiary care hospital in South India. Int. J. Adv. Med. 6, 1611–1615. doi: 10.18203/2349-3933.ijam20194228
Sharma, S. K., Mudgal, S. K., Thakur, K., and Gaur, R. (2020). How to calculate sample size for observational and experimental nursing research studies? Natl. J. Physiol. Pharm. Pharmacol. 10, 1–8. doi: 10.5455/njppp.2020.10.0930717102019
Tomaszewski, K., Zarychta, M., Bieńkowska, A., Chmurowicz, E., Nowak, W., and Skalska, A. (2011). Validation of the Patient Health Questionnaire-9 Polish version in the hospitalised elderly population. Psychiatr. Pol. 45, 223–233.
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., Vandenbroucke, J. P., et al. (2007). Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335, 806–808. doi: 10.1136/bmj.39335.541782.AD
Xie, N., Qin, Y., Wang, T., Zeng, Y., Deng, X., and Guan, L. (2020). Prevalence of depressive symptoms among nurses in China: a systematic review and meta-analysis. PLOS ONE 15:e0235448. doi: 10.1371/journal.pone.0235448
Yoon, S. L., and Kim, J.-H. (2013). Job-related stress, emotional labor, and depressive symptoms among korean nurses: job stress and emotional labor with depressive symptoms. J. Nurs. Scholarsh. 45, 169–176. doi: 10.1111/jnu.12018
Yoshizawa, K., Sugawara, N., Yasui-Furukori, N., Danjo, K., Furukori, H., Sato, Y., et al. (2016). Relationship between occupational stress and depression among psychiatric nurses in Japan. Arch. Environ. Occup. Health 71, 10–15. doi: 10.1080/19338244.2014.927345
Keywords: cardiac nurses, depression, occupational burnout, mood, anxiety, nurses
Citation: Larysz A and Uchmanowicz I (2021) Sociodemographic Factors and Depressive Symptoms Among Cardiac Nurses: A Cross-Sectional Study. Front. Psychol. 12:723035. doi: 10.3389/fpsyg.2021.723035
Received: 09 June 2021; Accepted: 26 July 2021;
Published: 19 August 2021.
Edited by:
Krystyna Kowalczuk, Medical University of Bialystok, PolandReviewed by:
Gianluca Pucciarelli, University of Rome Tor Vergata, ItalyCopyright © 2021 Larysz and Uchmanowicz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Izabella Uchmanowicz, aXphYmVsbGEudWNobWFub3dpY3pAdW1lZC53cm9jLnBs
†ORCID: Anna Larysz orcid.org/0000-0003-3266-6109
Izabella Uchmanowicz orcid.org/0000-0001-5452-0210
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.