 Carla Oliveira
Carla Oliveira Anabela Pereira
Anabela Pereira Paula Vagos
Paula Vagos Catarina Nóbrega1
Catarina Nóbrega1 José Gonçalves
José Gonçalves Beatriz Afonso
Beatriz Afonso- 1Department of Education and Psychology, University of Aveiro, Aveiro, Portugal
- 2Department of Psychology and Education, Portucalense Institute for Human Development (INPP), Universidade Portucalense, Porto, Portugal
Serious mental health disorders are increasing among college students and university counseling services are often overburdened. Mobile applications for mental health have been growing exponentially in the last decade and they are emerging in university settings as a promising tool to promote and intervene in college students' mental health. Additionally, considering the recent covid-19 pandemic, mHealth interventions, due to its nature and possibilities, may play an important role in these institutions. Our main objectives are to explore mhealth interventions in universities, regarding its conceptual framework, acceptability and efficacy outcomes and understand its impact and contributions to address treatment delivery and psychological difficulties resulting from covid-19 pandemic. The literature search was conducted in scientific databases, namely, Web of Science, Pubmed, and Scopus. A search in app stores was not conducted, thus regarding commercially available apps, only those found in our database search were included in our review. We selected studies with mobile applications addressing psychological interventions for college students. A total of 2,158 participants were included in the 8 selected studies and most interventions were delivered through mobile apps only and based in cognitive behavioral therapy. Results suggested that college students accept and adhere to these interventions and preliminary evidence of efficacy was demonstrated in different disorders, such as stress, anxiety, depression and risky behaviors such as alcohol and tobacco abuse and sexual knowledge. We conclude that universities, particularly college counseling services, may benefit from mhealth interventions, not only to address college students' mental health but to decrease some of its difficulties related to lack of human resources. Specifically in covid-19 pandemic context, these interventions may contribute significantly by promoting and delivering psychological interventions at a safe distance.
Introduction
Over the last decade numerous mental health mobile applications have been developed and made available for users (Bakker et al., 2016). Smartphones demonstrate numerous advantages such as great computing capacity, mobility, and more rapid and efficient access to information by using mobile applications (Donker et al., 2013). The enthusiasm of smartphones for healthcare initiatives led to the emergence of a novel field called mHealth (Ben-Zeev et al., 2014) defined as the use of mobile technologies to deliver or support psychological or mental health interventions and includes mobile devices such as smartphones, tablets, Personal Digital Assistants, and wearable devices (Clough and Casey, 2015b; Alyami et al., 2017). In clinical settings, mHealth may enhance face-to-face treatments, increase patient engagement in therapy sessions and adherence to therapy principles; provide better use of clinician time and resources and improve treatment outcome and risk of relapse (Clough and Casey, 2015b). Several studies have shown that mental health apps and cognitive behavioral therapy (CBT)-based apps are efficacious (Rathbone et al., 2017; Linardon et al., 2019). However, despite clinical potential, interest and early supporting evidence, one factor that seems to limit mental health apps is low engagement or poor adherence to the intervention (Torous et al., 2018).
One of the areas were mental health apps can have a significant impact is in universities. College years are a sensitive period to the onset of several mental health disorders (Kessler et al., 2007) and many studies have reported a significant rise in serious mental health illness among college students (Hunt and Eisenberg, 2010; Storrie et al., 2010; Auerbach et al., 2018). Major Depressive Disorder (MDD) and Generalized Anxiety Disorder (GAD) were identified as the most common disorders found in college students (Auerbach et al., 2018). University counseling services constitute a valuable resource to support college student mental health and wellness (Spooner, 2000) and a challenge that seems to be common across several counseling services is the growing student demand for these services and the limited resources to face these demands (Johnson and Kalkbrenner, 2017; Shaw et al., 2017; Auerbach et al., 2018; Lee and Jung, 2018). College students are also large consumers of technology and communicate frequently online (Shaw et al., 2017). A study by Wilansky et al. (2016) referred that mobile applications may increase youth adherence to Cognitive Behavioral Therapy (CBT) and improve treatment outcomes. Research suggests that mHealth is already being used to increase students' awareness and to deliver health-related interventions with increasing popularity; preliminary findings indicate that students are open and willing to use these interventions (Johnson and Kalkbrenner, 2017).
Mobile technologies for mental health assume an important role considering our current reality of pandemics resulting from covid-19 infectious disease. Covid-19 is an infectious disease cause by a coronavirus that rapidly expanded worldwide, and some of the protective measures include physical distancing, wearing a mask, avoiding crowds and close contact, and regularly cleaning your hands (World Health Organization, 2020). College students, alongside with children and health workers, are one of the most exposed groups to develop post-traumatic stress disorder, anxiety, depression and other symptoms of distress (Saladino et al., 2020). Studies conducted during covid-19 pandemic in China concluded that almost half of Chinese college students that participated in the study experienced anxiety symptoms (Fu et al., 2021) and are more likely to suffer from stress, anxiety and depression than the general population (Li et al., 2020). Several studies highlight the need to monitor students' mental health during the pandemic and the delivery of timely and appropriate interventions (Cao et al., 2020; Fu et al., 2021) such as the importance of technological devices or digital interventions (Saladino et al., 2020). Covid-19 brought several challenges to mental health services delivery, thus many therapists rapidly adhered to telehealth to replace in-person contact (Taylor et al., 2020). The same authors state that this disease presents an imperative for mental health services to make digital mental health interventions available in routine care and not only in response to covid-19 crisis.
Previous systematic reviews with college students and mobile interventions often explore a wide range of mHealth interventions and technology (e.g., Johnson and Kalkbrenner, 2017). Our review will focus on (1) mental health mobile applications that include a psychological intervention targeting a mental disorder, (2) college students, and (3) randomized controlled trials and acceptability and feasibility studies. We aim to explore how mobile apps are being developed to address college students' mental health in universities, if they accept and adhere to these interventions and if these interventions demonstrate efficacy. A search will be made for peer-reviewed articles of mental health mobile apps in scientific databases. The present review will not conduct a search in app stores mainly because acceptability and efficacy outcomes are not usually reported in app stores and because it would demand a different type of search strategy. Thus, in the current review we aim to review all published literature, in scientific databases, on psychological interventions using mobile applications, in the last 12 years, for college students. Our main objective is to review efficacy outcomes, through randomized controlled trials, of mobile app-based psychological interventions compared to traditional therapy or a waiting list control group in reducing psychological symptomatology among college students. Additionally, we intend to explore how mobile interventions are being accepted by college students and which conceptual frameworks are being used to develop these interventions. Considering the recent context of covid-19 pandemics, we aim to reflect on the impact and contributions of mHealth interventions for universities and college students.
Methods
We used the search method of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al., 2009).
Eligibility Criteria and Information Sources
Inclusion criteria considered (1) target population: college students; (2) types of intervention: psychological interventions delivered through mobile applications (self-guided); mobile applications combined with web-based interventions or mobile applications combined with face-to-face treatments; (3) Primary outcome measures that target specific psychological disorders or symptomatology (i.e., anxiety, depression, social anxiety, stress, PTSD, alcohol abuse); (4) clear report of the psychological intervention, specifying theoretical basis or treatment model and therapeutic techniques; (5) Types of studies: randomized controlled trials (RTC) or quasi-experimental designs that clearly report efficacy outcomes and feasibility and acceptability studies since they contribute with valuable information about conceptual framework and some provide preliminary effectiveness results; (6) written in English; (7) published in the selected scientific databases. Exclusion criteria consisted in (1) studies with young adults (not students); (2) mobile interventions based on text messages; (3a) mobile interventions targeting physical or medical conditions (e.g., diabetes, physical activity, nutrition, weight control etc.); (3b) studies about mobile learning apps (e.g., anatomy); (3c) studies about smartphone addiction; (4) internet and computerized based interventions; (5) study protocols.
Our main objective is to review conceptual framework, acceptability, and efficacy outcomes of mobile app interventions addressing mental health for college students. A search of mobile apps commercially available in the app store was not conducted in this review since, although important, demands a different type of search and selection process, and often don't report acceptability and efficacy results (in the app store). Thus, we considered that it would be more suited to do a review, with this group of apps, separately. A narrative approach was used for extraction and synthesis of the data. Studies were identified through three major electronic databases, namely, Web of Science, Pubmed, and Scopus. An update literature search was performed in January 2021 using the same information sources.
Search and Study Selection Process
The following search keywords were considered “mobile interventions,” “smartphones,” “mobile application,” “mHealth,” “mobile technology,” “college students,” “students,” “university,” “campus.” Two authors independently conducted a thorough search in the three major scientific databases with the mentioned keywords, using primarily the combination “mobile interventions” AND “college students” with year filter between 2008 and 2019. A search update was performed in January 2021 with the same study selection process. In a first instance, studies including keywords in titles and/or abstracts were selected for further thorough review. After identifying eligible studies, duplicates were removed, and full papers were examined regarding eligibility criteria. A list of studies was produced by each author. Afterwards, both authors discussed their list of included studies, and by agreement, a final list of studies was produced.
Data Extraction
Data extraction was performed by two independent researchers and included year of publication, demographic characteristics of participants, study design (RCT, quasi-experimental studies, single-arm pre-test post-test), study participants and interventions (i.e., population, conditions, sample size, outcome measures, mobile app characteristics, theoretical basis, and intervention modality), main results and findings.
Assessment of Methodological Quality
The present review resorted to critical appraisal tools from the Joanna Briggs Institute for randomized controlled trials and quasi experimental studies (non-randomized experimental studies). The Checklist for Randomized Controlled Trials [The Joanna Briggs Institute (JBI), 2017a] was utilized to assess the methodological quality of the included RCTs and the Checklist for Quasi-Experimental Studies (non-randomized experimental studies) [The Joanna Briggs Institute (JBI), 2017b] to assess methodological quality of quasi-experimental studies and studies with a one group pre-test post-test design. Each study was assessed using JBI checklists for RCT or quasi-experimental studies.
Results
Study Selection
As we can see in Figure 1 our search identified 957 published articles. Afterwards, we removed 23 duplicates and a review of title and abstracts excluded 904 articles. A total of 30 full-text articles were assessed for eligibility, where 11 were excluded due to motives of being a study protocol, thus not presenting feasibility or efficacy outcomes; lack of a psychological intervention or a psychological disorder; being web-based intervention or having no access to article full text. A total of 19 studies were included and examined in accordance with inclusion criteria.
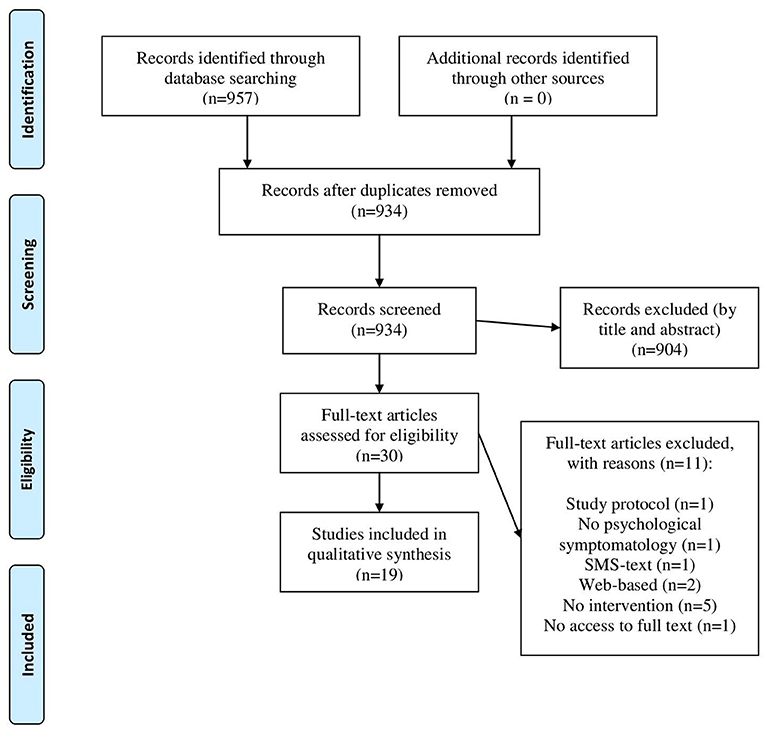
Figure 1. PRISMA flow diagram. From: Moher et al. (2009).
Demographic Characteristics
A total of 3,399 college students were included in the selected studies (n = 19) for this systematic review. Eleven studies included college students with self-reported psychological symptomatology (i.e., elevated stress, generalized anxiety disorder (GAD), PTSD), two studies included first-year college students and the remaining studies included non-treatment seeking college students (n = 6). Most studies occurred in the USA (n = 12), others occurred in Germany (n = 1), Sweden (n = 1), Canada (n = 1), United Kingdom (UK) (n = 2), Australia (n = 1), and Iran (n = 1).
Intervention Characteristics
Mobile intervention apps for college students target anxiety (n = 7), depression (n = 7), stress (n = 5), alcohol consumption and risky drinking (n = 4), smoking (n = 1), and sexual behaviors (n = 1), Post-traumatic stress disorder (PTSD) (n = 1). Table 1 resumes all further interventions characteristics.
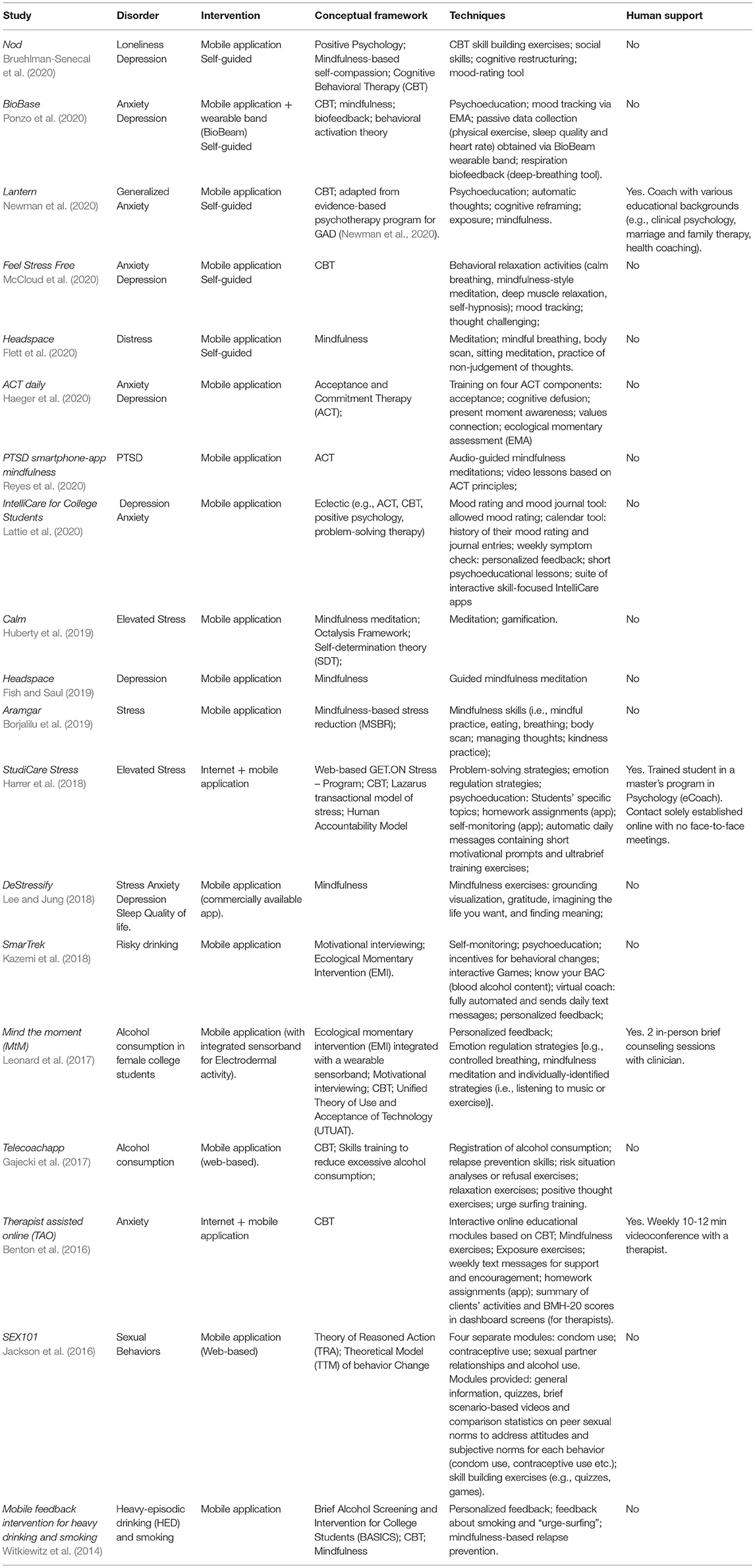
Table 1. Mobile interventions characteristics.
We considered that most studies, with self-guided apps, focus on prevention (n = 15) and the studies that included human support (therapists and coaches) and a TAU group were more focused on a treatment approach (n = 4). However, many studies with self-guided apps, included students with elevated psychological symptomatology (i.e., elevated stress, diagnosed PTSD, or GAD), and it isn't always clear the nature of their intervention.
Intervention modality varied between a combination of internet and mobile app intervention (n = 2) and mobile app intervention only (n = 17), from these 17 studies, two apps were combined with a wearable band to permit passive data collection. When combining mobile apps with internet interventions, the mobile app functioned mostly as a tool offering support for homework assignment or working as a diary app by enabling monitoring of mood fluctuations or stress levels [e.g., Harrer et al. (2018)]. Human support was considered in 4 mobile apps (Lantern; TAO; StudiCare Stress; Mind the Moment), two mobile interventions included therapists and two included a coach, StudiCare Stress app included a trained master's student in Psychology (named an eCoach) and Lantern app included a coach with various educational backgrounds. Human support varied from weekly 10–12 min brief videoconferences, to 2 face to face sessions and online sessions only.
Regarding conceptual framework most researchers used CBT intervention or CBT third wave techniques to conceptualize these apps (n = 17). Most CBT apps include mindfulness exercises (n = 11), some are solely based on mindfulness (n = 4) or acceptance and commitment therapy (ACT) (n = 2). One mobile app is focused on CBT and a biofeedback intervention (BioBase app). Some used CBT intervention as a part of a larger program such as GET.ON Stress, a stress management program, adapted to college students; or BASICS, an alcohol intervention program for college students. In some cases, CBT was combined with other psychological models such as Lazarus Transactional Model of Stress (GET.ON Stress program) or the Unified Theory of Use and Acceptance of Technology (UTAUT). The StudiCare Stress app also included an adherence-focused guidance concept according to the human accountability model. Only two studies did not resort to CBT, the SmarTrek app that used motivational interviewing and the SEX101 that used two psychological models, the Theory of Reasoned Action (TRA; Fishbein and Ajzen, 1975) and the Transtheoretical Model (TTM) of behavior Change (Prochaska and DiClemente, 1984). Additionally, SmartTreak and MtM added an Ecological Momentary Intervention (EMI) and Witkiewitz et al. (2014), BioBase app and ACT daily included an Ecological Momentary Assessment (EMA).
As for specific techniques more than half of the mobile apps include mindfulness exercises; other included psychoeducation or general information about the target disorder; include data collection self-monitoring; exposure; systematic desensitization and relaxation exercises. Other features refer to quizzes and interactive games; virtual coach; passive sensing through sensorband; all apps for risky drinking and excessive smoking included personalized feedback on drinking patterns and motives for drinking, feedback includes information about smoking and “urge-surfing” or strategies to increase student's emotional awareness. All apps were designed to provide education, collect data, monitor/track behavior, some provide personalized feedback or guidance in CBT exercises (in some cases homework assignments).
Few studies gave information regarding privacy and security. For example, Benton et al. (2016) referred that TAO security and privacy included authentication, password protection, and encryption of databases and Lee and Jung (2018) stated that data was collected and stored on secure systems and accessed through computers with password protection and encryption.
Methodological Quality
Tables 2, 3 resumes the methodological characteristics of the included studies. Eleven studies are randomized controlled trials (RCT) (Witkiewitz et al., 2014; Gajecki et al., 2017; Harrer et al., 2018; Lee and Jung, 2018; Fish and Saul, 2019; Huberty et al., 2019; Bruehlman-Senecal et al., 2020; Flett et al., 2020; McCloud et al., 2020; Newman et al., 2020; Ponzo et al., 2020) and two studies are considered quasi-experimental trials (Benton et al., 2016; Borjalilu et al., 2019). Four studies considered a single-arm pre-test-post-test study design (Jackson et al., 2016; Leonard et al., 2017; Haeger et al., 2020; Lattie et al., 2020; Reyes et al., 2020) and one study included two groups through an iterative process (Kazemi et al., 2018).
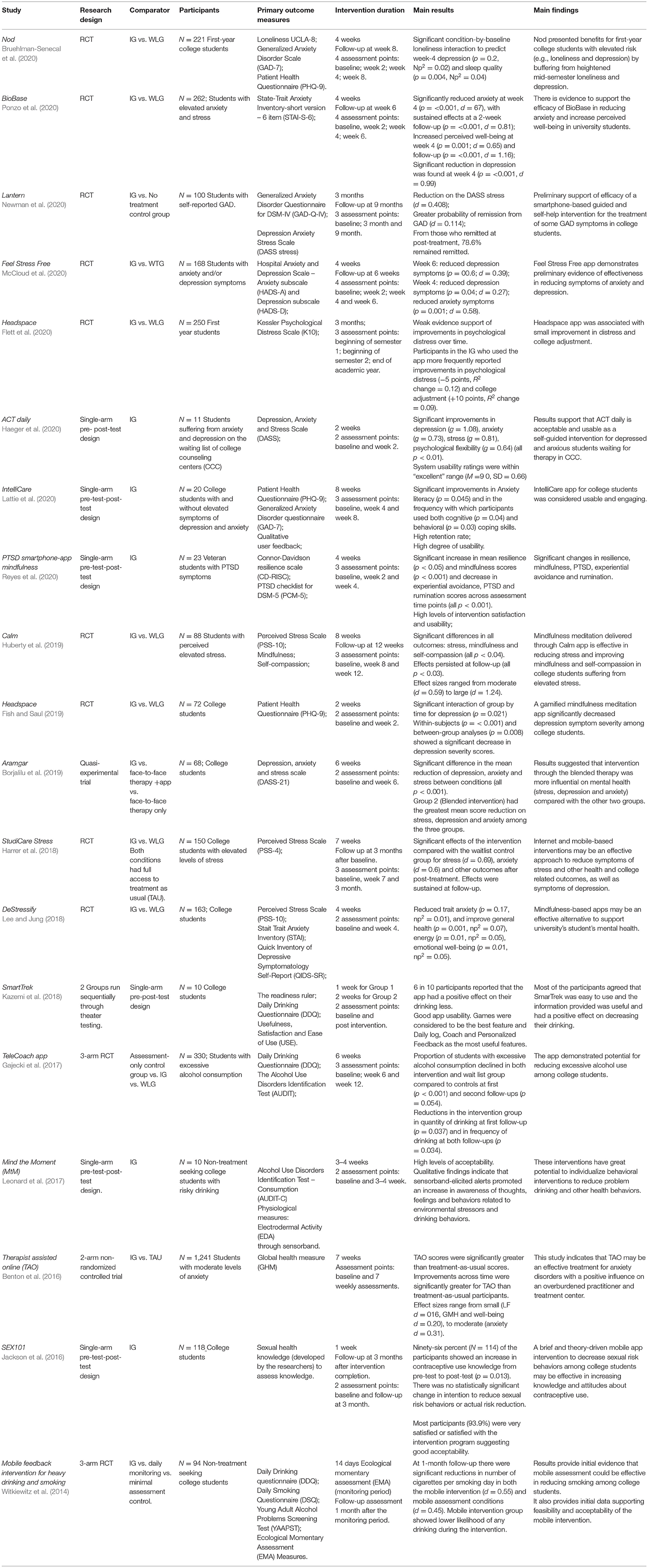
Table 2. Methodological characteristics.
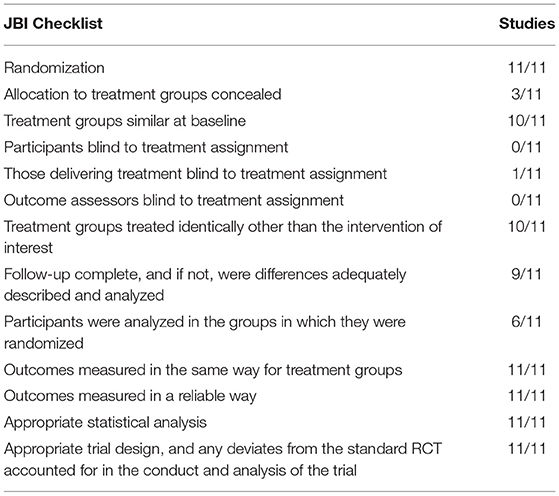
Table 3. JBI Checklist for randomized controlled trials.
Eleven of the included studies are RCTs and the total sample size ranges from 72 to 330 college student participants; the overall duration of the intervention range from 14 days to 3 months and when we consider follow-ups, the longest trial lasted for 9 months. Most RCTs included as a control group a waiting list control trial (n = 8). Following JBI critical appraisal tool, we consider that all RCTs reported that participants were randomly assigned to treatment groups, 9 out of 11 studies provided detailed description of the randomization procedure and two studies merely stated that the participants were randomly assigned. As for allocation concealment, three studies provided information about allocation concealment. For example, Harrer et al. (2018) stated that the randomization process was performed by a researcher not involved in the study, and although they weren't able to blind participants to study conditions, during the randomization process, they were able to conceal the allocation from participants, researchers, and e-coches. Ten studies provided information and reported similar groups at baseline. As for blinding participants, or those delivering treatment and even outcome assessors to treatment conditions may be difficult and even unachievable in this type of studies; several studies reported this issue, pointing to the inability to blind their participants to treatment conditions. There were incomplete follow-ups; however they were generally adequately described and analyzed. Six RCTs provided detailed information about intention-to-treat analyses (ITT); the remaining studies excluded participants, lost to follow-up, from analysis. All studies used primary outcome measures with good validity and reliability. The large majority of RCTs also included quantitative and/or qualitative self-report measures to evaluate usability, acceptability, user satisfaction, or app adherence.
The studies by Benton et al. (2016) and Borjalilu et al. (2019) were considered as quasi-experimental studies. The first study included a large sample size (n = 1,241) with overall duration of the intervention of 7 weeks. They included a wait-list treatment as usual control group and the intervention group received the intervention of study. The primary outcome measure was adequately validated and provided multiple measurements along the intervention as well as pre and post assessment. Differences between groups in terms of follow-up were adequately described and analyzed. This study presented many missing data and the linear mixed-effects models was utilized to estimate parameters for missing values. As for Borjalilu et al. (2019), they conducted a study with three conditions and 68 college students, who were randomly assigned into the three groups, but no further detailed information was given about the randomization process. There were pre- a post-assessments and follow up was complete. Outcomes were measured in a reliable way and participants, from both groups, were assessed in the same way.
In this review there is a significant number of a single group pre-test-post-test design studies that aimed to evaluate acceptability and feasibility; only one study (Jackson et al., 2016) aimed to evaluate efficacy with this design. Sample sizes were similar between studies, ranging from n = 10 to n = 23, with overall duration (intervention) of 3–4 weeks. Adequate and validated main outcome measures were used. The SEX101 (Jackson et al., 2016) had a larger sample size compared to the previous studies and a follow-up assessment of 3 months after intervention completion. However, the overall duration of the intervention was very small (pre-test and intervention had to be complete in 1 week and it takes 40 min to complete) and some outcome measures were developed by the researchers with few information regarding reliability.
Intervention Outcomes and Effect Sizes
A study conducted by Newman et al. (2020) assessed the efficacy of Lantern, a self-help mobile app to treat generalized anxiety disorder. Study results demonstrated a significant reduction on the DASS stress scores (d = 0.408) and greater probability of remission from GAD (d = 0.114). Lantern revealed moderate effects in reducing anxiety, stress, and depression. BioBase is a biofeedback self-guided mobile app combined with wearable device (BioBeam), to treat anxiety in college students. Ponzo et al. (2020) conducted a RCT to assess BioBase efficacy and results indicated that a 4-week intervention significantly reduced anxiety (d = 0.67), depression (d = 0.99), and increased perceived well-being (d = 0.65) demonstrating moderate to large effects. Sustained large effects at 2-week follow-up was found for anxiety (d = 0.81) and perceived well-being (d = 1.16).
McCloud et al. (2020) conducted a RCT to assess efficacy of Feel Stress Free app for the treatment of depression and anxiety symptoms. Results showed that there was a significant reduction of depression symptoms at week 4 (d = 0.27) and week 6 (d = 0.39), and significant reduction of anxiety symptoms at week 4 (d = 0.58). Overall effect sizes ranged from small to moderate.
Bruehlman-Senecal et al. (2020) studied Nod, a mobile app designed to reduce loneliness during the transition to college. Their RCT results indicated significant condition-by-baseline loneliness interaction to predict week-4 depression (Np2 = 0.02) and sleep quality (Np2 = 0.04), suggesting that Nod buffered participants with higher baseline loneliness against heightened midquarter depression and poor sleep quality. Calm, is a mindfulness-based app, and its efficacy was tested among students with elevated stress. The study results of Huberty et al. (2019) found significant differences among conditions in all outcomes, namely, significant reduction in perceived stress (d = 1.24), significant improvements in mindfulness (d = 1.11), and self-compassion (d = 0.84).
Harrer et al. (2018) conducted a randomized controlled trial to evaluate the efficacy of Studicare Stress, a stress management intervention app for college students. Their results indicated significant effects of the intervention compared with the waitlist control group for stress at post-test (d = 0.69) and at 3-month follow-up, other secondary outcome measures also yielded significant effects such as anxiety (d = 0.76), depression (d = 0.63), college related productivity (d = 0.33), and academic work impairment (d = 0.34). Thus, Studicare Stress revealed moderate to large intergroup effects for the reduction of perceived stress and other health and college related outcomes.
Lee and Jung (2018) conducted a pilot study to evaluate efficacy of DeStressify, a mindfulness-based app on stress, anxiety, depressive symptomatology, sleep behavior, and other variables. Results indicated that when using the app during 4 weeks, students in the experimental group at post-test reported less trait anxiety ( = 0.040); an improve in several quality of life subscales, such as general health, that significantly differed between treatment condition in post-intervention scores ( = 0.07). A significant difference was also found in energy or fatigue subscale between treatment conditions ( = 0.05). An interaction effect was found in the emotional well-being subscale ( = 0.05). The author interpreted the partial eta squared values of 0.0099, 0.0588, and 0.1379 as small, medium, and large effect, respectively, following suggestions by Cohen (Field, 2009). This indicates that we can verify small (trait anxiety) to medium effects for general health, energy or fatigue and emotional well-being.
Telecoach app (Gajecki et al., 2017) was evaluated using a 3-arm randomized controlled trial and results demonstrated that the proportion of students with excessive alcohol consumption declined in both intervention and wait list control group compared to controls at first and second follow-ups. Secondary analysis showed reductions for the intervention group in quantity of drinking at first follow up and in frequency of drinking at both follow-ups. Across both follow-ups the odds ratios for not having excessive weekly alcohol consumption in the intervention group (1.95) was almost twice as high as for controls (1.00). Secondary analysis by gender showed that the odds ratio for not having excessive alcohol consumption among men in the intervention group compared to male controls was higher (2.68) than women in the intervention group (1.71) compared to women controls.
Witkiewitz et al. (2014) conducted a 3-arm randomized controlled trial to evaluate a mobile feedback intervention for heavy-episodic drinking (HED) and smoking among college students, and they concluded that at 1-month follow-up there were significant reduction in number of cigarettes per smoking day in both the mobile intervention (d = 0.55) and mobile assessment conditions (d = 0.45) with moderate effects. No significant results were observed on HED or concurrent smoking and drinking. As for Benton et al. (2016) quasi-experimental study, the intervention group showed improvements across time significantly greater than treatment as usual participants, for all primary outcomes except Life Functioning (LF) subscale. The size of these effects ranged from small (d = 0.16) for LF, Global Mental Health and Well-Being (d = 0.20) to medium for Anxiety (d = 0.31).
Usability, Acceptability, and Feasibility Outcomes
The large majority of the included studies evaluated acceptability and students' satisfaction with the intervention. From the 19 studies, eight studies explored adherence/satisfaction and six used adequately valid scales or methods to assess usability or satisfaction with app use. Some studies also used metrics obtained through the mobile app (n = 2). Most studies, created their own items to assess satisfaction with the intervention. Overall, we could observe good retention rates across studies, however as Gajecki et al. (2017) specifically noted in there study, there is a possibility that their fairly high retention levels could result from the desire of some participants to win an iPad (reward to participate in the study) with no actual intention to use the app. Out of the 19 studies, 10 gave rewards to their participants.
All studies that evaluated satisfaction reported moderate to high client satisfaction with the intervention. The MtM app (Leonard et al., 2017) demonstrated that 60% of the participants reported “mostly” or “very” satisfied with the sensorband and 50% with the mobile app. Also, 93.9% of the participants were very satisfied or satisfied with the intervention program of SEX101 app (Jackson et al., 2016). However, this particular study produced large attrition rates (50%) and as the authors of this study noted information regarding app components that need to be improved, added or removed should be collected. In the Witkiewitz et al. (2014) EMA app, over 65% of the participants reported an increase in awareness of their drinking and/or smoking and 60% stated that they would recommend this study to a friend because it provided greater awareness and they could help a friend reduce their drinking and/or smoking. Kazemi et al. (2018) demonstrated good usability of SmartTrek and the best feature reported by students was “Games” and the most useful features was “know your BAC” and “My strategies” that monitored alcohol intake, created behavioral change plans and reminded them of their goals. None of the studies, that provided human support (therapists), explored acceptability and satisfaction of the therapist with the intervention.
Implications and Contributions of mHealth Interventions for College Students in Covid-19 Context
Covid-19 infectious disease emerged in China and rapidly expanded around the globe, leading to an unexpected pandemic, which completely changed our daily lives and significantly limited physical and social contact with significant repercussions to our physical and mental health. Specifically in college students that live in a constant and thriving social interaction, covid-19 pandemic had a strong negative impact on mental health and may have contributed to the increase of several preexisting barriers and limitations to college counseling services. Considering these restraints, mHealth interventions may play an important role in a pandemic context due to its ubiquitous, remote and innovative functionalities that may facilitate access to evidence base treatments for mental health and also, its provider and facilitator (therapist).
Taking into consideration the included studies and their characteristics, acceptability, satisfaction and efficacy outcomes, we may determine that these interventions can significantly contribute in several important aspects related to college students' mental health. To our understanding, mobile app technologies may significantly contribute to promote mental health in college students targeting several specific disorders, such as anxiety, stress, depression, smoking, and alcohol abuse. It is also attainable to support students with coping strategies for elevated stress, anxiety, smoking, and alcohol abuse. Through mobile technologies, therapists may monitor and keep track of their patients' symptomatology and well-being, check homework assignments, and contact their patients' regularly through chat or messages, remotely. Overall, mobile technologies provide spontaneous and remote access to app content whenever we want, particularly in the comfort of our home. It helps us maintain physical distance from mental health professionals and counseling services without interrupting treatment.
Discussion
Summary of Evidence
Our search for studies addressing mobile health apps for college students in university settings gathered 19 studies with different conceptual frameworks and study designs. In this review we could verify an increase in studies using mobile interventions for college students over the years, particularly in the last year, which may indicate an increasing trend in mobile use for the delivery of health interventions for college students. The large majority of studies are being developed in North America and Europe.
Regarding target disorders we can verify that most apps target anxiety, depression and stress, others target risky or excessive drinking, PTSD and sexual behaviors. Overall, mobile interventions showed promising results to reduce psychological symptomatology associated with stress, depression, anxiety and general student's mental health. As for drinking, smoking, and sexual behaviors, the included apps seemed to reduce excessive drinking and smoking and increase contraceptive use and knowledge but not the intention to reduce sexual risk behaviors or actual risk reduction. Most of the mobile interventions showed medium to large effect sizes for the main variables the app was designed to intervene, which may indicate that these interventions are well conceptualized and grounded according to the best available empirical evidence. Some of the included studies aimed to evaluate acceptability and feasibility and overall, these apps demonstrate good acceptability and feasibility among college students, supporting the hypothesis that students may accept and adhere to these interventions.
When we explore conceptual frameworks of these mobile apps we verify that many studies adopted CBT as the main intervention, particularly Mindfulness exercises. Effectively, CBT is well-established and particularly known as an effective treatment for several mental health disorders, and have demonstrated its efficacy when delivered through apps (Rathbone et al., 2017). In some studies the intervention was complemented with psychological models, which have been shown to increase intervention efficacy (Webb et al., 2010). Aside from psychological models/theories for behavioral change, one study incorporated a technological model, namely the Unified Theory of Use and Acceptance of Technology (UTUAT). There seems to be a strong application of psychological models and intervention techniques, indicating that there is a concern in adequately conceptualizing these interventions following evidence base principles. However, considering that we are studying mobile health interventions with significant emphasis in technology, very few studies incorporated technological models. Also, security and privacy features are also rarely mentioned and increasingly relevant in this type of interventions, best practices should be known and shared, reflecting in a mobile app quality indicator.
Regarding therapist role in mobile interventions, only 4 studies incorporated human support, two studies included therapists and two studies included a trained psychology student. From the mentioned studies, one used the human accountability model to inform this support. We consider that even though most of these apps intend to reduce therapist time and subsequently reduce therapist caseload and overburdened, this process may be optimized and better conceptualized using human support models. Moreover, evidence shows that app based interventions with therapist support has shown to produce larger effects (Linardon et al., 2019).
As for methodological quality of the included studies, most studies aimed to evaluate efficacy and resorted to a randomized controlled trial, which is natural since RCTs are known as the golden standard to evaluate efficacy. All trials randomly assigned their participants to treatment conditions; however the number of studies that performed randomization concealment and blinding was almost non-existent. This reflects the difficulty of concealment and blinding in these type of studies and the limitation of the RCT study design when assessing efficacy in this type of interventions. Most studies also use a waiting list control group; given that many studies included students with elevated psychological symptomatology (that have to wait weeks/months to get access to the intervention) and the difficulty of blinding participants with this type of comparator we wonder if this is the best control group to use in this studies. Other research designs are also being explored in these studies and should be considered, so we can obtain efficacy results timelier and reliably (Clough and Casey, 2015a). Many studies adopted a pre-test post-test study design in order to evaluate acceptability and feasibility, even though this research design is considered a weak experimental study design, we consider that for the purpose and objectives of the studies this design was well-applied. Good overall retention rates may indicate treatment feasibility and acceptability. However, most studies were of short duration, with small samples and in controlled settings, with the addition of significant rewards. Additionally, many outcome measures were self-reported and not always congruent with app adherence rates. User metrics (e.g., how many times a participant accessed the app) provided by mobile apps may contribute to more accurate indicators of use and adherence to the intervention. Also, qualitative studies exploring perceived usefulness and user experience with the app intervention may also contribute to understand and overcome some barriers of adherence and engagement. Rewards are sometimes our best option to find participants, however when we are studying acceptability and adherence to these interventions, rewards may produce biased results. Recent studies opted to reward outcome measures completion, rather than app use.
A final question that emerged while exploring the studies is associated with the limited visual content of the apps included in the studies. Few studies included images/visual content of the mobile apps; some studies reported how they developed the app but provided little information about app design. A study by Torous et al. (2018) concluded that most mhealth apps suffer from low engagement and adherence and this may be, along with other issues, due to poor usability and because most apps are not user-friendly. It is important that researchers provide more frequently studies regarding user's needs and report multidisciplinary teams when building (native) apps, since this area often needs involvement of psychologists, software engineers, and designers/interaction designers. Also these tools, in clinical settings (e.g., counseling services), should be designed and optimized regarding all end users: students and therapists. Therapists' point of view and evaluation was often forgotten in the included studies that involved therapists.
Mobile apps may be customized and designed under practically unlimited possibilities. They can be developed to promote, prevent or intervene in a specific mental health disorder; to promote well-being and to deliver treatment under different levels of therapist support in different mental health services. Thus, they can be implemented and tailored according to specific needs. It is important to continue studying these interventions using user-centered designs and rigorous efficacy and effectiveness studies. We consider that universities, including college counseling services, may benefit from mhealth interventions, not only to address college student mental health but to decrease some of its difficulties related to few human resources. In a context of quarantine and confinement at home, where physical and social distance is imperative, these interventions assume special importance. They facilitate mental health promotion and support therapist and patient contact at a safe distance, avoiding treatment interruption.
Limitations
The current review presents a major limitation since we limited our search scope to the mentioned databases. Registered clinical trials and commercially available apps in app stores were not included, thus we may have missed already developed or apps that are being currently studied for college students. We may have failed to identify studies with relevant information regarding the application of mHealth intervention in college settings when we didn't consider “young adults,” since it may not include college students or occur in college settings.
Conclusion
The current systematic review shows that mobile apps for mental health intervention in college students exists and demonstrates good acceptability and feasibility. They also demonstrate efficacy among students. Overall we may conclude that mHealth interventions may turn out to be a great resource and tool to implement in counseling services, offering therapists and students many advantages. Particularly in the current pandemic context, these interventions demonstrate innumerous possibilities and promising solution to address college students' mental health and overcome many barriers associated with treatment access.
Future studies addressing mobile apps in college students, should invest in user-centered design studies so we can better understand what students and therapists (also attending university counseling services workflow) value more in a mobile based psychological intervention, to better adapt and tailor the intervention to user's needs. Effectively, acceptability and feasibility results among therapists are lacking in studies that use mobile intervention with therapist support. Future investigations should also explore diversity when developing and studying future apps, examining the applicability and efficacy of other theories/models. Also, we consider that studies should describe the development process of the mobile application (e.g., by including visual content) so we can better understand what is actually being evaluated and how it may impact efficacy results, in terms of usability and design. Lastly, students are large consumers of technology and so it may be important to invest more in these interventions, doing larger studies with more students, with superior methodological quality and avoiding large monetary rewards.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
CO searched for studies to include in the systematic review and wrote sections of the manuscript. AP and PV revised the manuscript and contributed to the conception of the study. CN, JG, and BA contributed to organize data extraction and the search of studies in the scientific databases. All authors contributed to the manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Alyami, M., Giri, B., Alyami, H., and Sundram, F. (2017). Social anxiety apps: A systematic review and assessment of app descriptors across mobile store platforms. Evid. Based Ment. Health 20, 65–70. doi: 10.1136/eb-2017-102664
Auerbach, R. P., Mortier, P., Bruffaerts, R., Alonso, J., Benjet, C., Cuijpers, P., et al. (2018). WHO world mental health surveys international college student project: prevalence and distribution of mental disorders. J. Abnorm. Psychol. 127, 623–638. doi: 10.1037/abn0000362
Bakker, D., Kazantzis, N., Rickwood, D., and Rickard, N. (2016). Mental health smartphone apps: review and evidence-based recommendations for future developments. JMIR Mental Health 3:e7. doi: 10.2196/mental.4984
Benton, S. A., Heesacker, M., Snowden, S. J., and Lee, G. (2016). Therapist-assisted, online (TAO) intervention for anxiety in college students: TAO outperformed treatment as usual. Prof. Psychol. 47, 363–371. doi: 10.1037/pro0000097
Ben-Zeev, D., Schueller, S. M., Begale, M., Duffecy, J., Kane, J. M., and Mohr, D. C. (2014). Strategies for mHealth research: lessons from 3 mobile intervention studies. Administr. Policy Mental Health Mental Health Serv. Res. 42, 157–167. doi: 10.1007/s10488-014-0556-2
Borjalilu, S., Ali Mazaheri, M., and Talebpour, A. (2019). Effectiveness of mindfulness-based stress management in the mental health of Iranian university students: a comparison of blended therapy, face-to-face sessions, and mHealth app (Aramgar). Iran. J. Psychiatry Behav. Sci. 13:84726. doi: 10.5812/ijpbs.84726
Bruehlman-Senecal, E., Hook, C. J., Pfeifer, J. H., FitzGerald, C., Davis, B., Delucchi, K. L., et al. (2020). Smartphone app to address loneliness among college students: pilot randomized controlled trial. JMIR Mental Health 7:21496. doi: 10.2196/21496
Cao, W., Fang, Z., Hou, G., Han, M., Xu, X., Dong, J., et al. (2020). The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 287, 1–5. doi: 10.1016/j.psychres.2020.112934
Clough, B. A., and Casey, L. M. (2015a). Smart designs for smart technologies: research challenges and emerging solutions for scientist-practitioners within e-mental health. Prof. Psychol. Res. Pract. 46, 429–436. doi: 10.1037/pro0000053
Clough, B. A., and Casey, L. M. (2015b). The smart therapist: a look to the future of smartphones and mHealth technologies in psychotherapy. Prof. Psychol. Res. Pract. 46, 147–153. doi: 10.1037/pro0000011
Donker, T., Petrie, K., Proudfoot, J., Clarke, J., Birch, M. R., and Christensen, H. (2013). Smartphones for smarter delivery of mental health programs: a systematic review. J. Med. Internet Res. 15:2791. doi: 10.2196/jmir.2791
Fish, M. T., and Saul, A. D. (2019). The gamification of meditation: a randomized-controlled study of a prescribed mobile mindfulness meditation application in reducing college students' depression. Simulat. Gaming 50, 419–435. doi: 10.1177/1046878119851821
Fishbein, M., and Ajzen, I. (1975). Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley.
Flett, J. A. M., Conner, T. S., Riordan, B. C., Patterson, T., and Hayne, H. (2020). App-based mindfulness meditation for psychological distress and adjustment to college in incoming university students: a pragmatic, randomised, waitlist-controlled trial. Psychology Health 35, 1049–1074. doi: 10.1080/08870446.2019.1711089
Fu, W., Yan, S., Zong, Q., Anderson-Luxford, D., Song, X., Lv, Z., et al. (2021). Mental health of college students during the COVID-19 epidemic in China. J. Affect. Disord. 280, 7–10. doi: 10.1016/j.jad.2020.11.032
Gajecki, M., Andersson, C., Rosendahl, I., Sinadinovic, K., Fredriksson, M., and Berman, A. H. (2017). Skills training via smartphone app for university students with excessive alcohol consumption: a randomized controlled trial. Int. J. Behav. Med. 24, 778–788. doi: 10.1007/s12529-016-9629-9
Haeger, J. A., Davis, C. H., and Levin, M. E. (2020). Utilizing ACT daily as a self-guided app for clients waiting for services at a college counseling center: a pilot study. J. Am. Coll. Health. 12, 1–8. doi: 10.1080/07448481.2020.1763366
Harrer, M., Adam, S. H., Fleischmann, R. J., Baumeister, H., Auerbach, R., Bruffaerts, R., et al. (2018). Effectiveness of an internet- and app-based intervention for college students with elevated stress: randomized controlled trial. J. Med. Internet Res. 20:9293. doi: 10.2196/jmir.9293
Huberty, J., Green, J., Glissmann, C., Larkey, L., Puzia, M., and Lee, C. (2019). Efficacy of the mindfulness meditation mobile app “calm” to reduce stress among college students: randomized controlled trial. JMIR MHealth UHealth 7:14273. doi: 10.2196/14273
Hunt, J., and Eisenberg, D. (2010). Mental health problems and help-seeking behavior among college students. J. Adolesc. Health 46, 3–10. doi: 10.1016/j.jadohealth.2009.08.008
Jackson, D. D., Ingram, L. A., Boyer, C. B., Robillard, A., and Huhns, M. N. (2016). Can technology decrease sexual risk behaviors among young people? Results of a pilot study examining the effectiveness of a mobile application intervention. Am. J. Sexual. Educ. 11, 41–60. doi: 10.1080/15546128.2015.1123129
Johnson, K. F., and Kalkbrenner, M. T. (2017). The utilization of technological innovations to support college student mental health: mobile health communication. J. Technol. Hum. Serv. 35, 314–339. doi: 10.1080/15228835.2017.1368428
Kazemi, D. M., Borsari, B., Levine, M. J., Shehab, M., Nelson, M., Dooley, B., et al. (2018). Real-time demonstration of a mHealth app designed to reduce college students hazardous drinking. Psychol. Serv. 16, 255–259. doi: 10.1037/ser0000310
Kessler, R. C., Amminger, G. P., Aguilar-Gaxiola, S., Alonso, J., Lee, S., and Ustun, T. B. (2007). Age of onset of mental disorders: a review of recent literature. Curr. Opin. Psychiatry 20, 359–364. doi: 10.1097/YCO.0b013e32816ebc8c
Lattie, E., Cohen, K. A., Winquist, N., and Mohr, D. C. (2020). Examining an app-based mental health self-care program, intellicare for college students: single-arm pilot study. JMIR Mental Health 7, 1–15. doi: 10.2196/21075
Lee, R. A., and Jung, M. E. (2018). Evaluation of an mhealth app (destressify) on university students' mental health: pilot trial. J. Med. Internet Res. 5:e2. doi: 10.2196/mental.8324
Leonard, N. R., Silverman, M., Sherpa, D. P., Naegle, M. A., Kim, H., Coffman, D. L., et al. (2017). Mobile health technology using a wearable sensorband for female college students with problem drinking: an acceptability and feasibility study. JMIR MHealth UHealth 5, 1–16. doi: 10.2196/mhealth.7399
Li, S., Wang, Y., Yang, Y., Lei, X., and Yang, Y. (2020). Analysis of influencing factors of anxiety and emotional disorders in children and adolescents during home isolation during the epidemic of novel coronavirus pneumonia. Chin. J. Child Health Care 28, 407–410. doi: 10.11852/zgetbjzz2020-0169
Linardon, J., Cuijpers, P., Carlbring, P., Messer, M., and Fuller-Tyszkiewicz, M. (2019). The efficacy of app-supported smartphone interventions for mental health problems: a meta-analysis of randomized controlled trials. World Psychiatry 18, 325–336. doi: 10.1002/wps.20673
McCloud, T., Jones, R., Lewis, G., Bell, V., and Tsakanikos, E. (2020). Effectiveness of a mobile app intervention for anxiety and depression symptoms in university students: randomized controlled trial. JMIR MHealth UHealth 8, 1–22. doi: 10.2196/15418
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and The PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Newman, M. G., Jacobson, N. C., Rackoff, G. N., Bell, M. J., and Taylor, C. B. (2020). A randomized controlled trial of a smartphone-based application for the treatment of anxiety. Psychotherapy Res. 31, 443–454. doi: 10.1080/10503307.2020.1790688
Ponzo, S., Morelli, D., Kawadler, J. M., Hemmings, N. R., Bird, G., and Plans, D. (2020). Efficacy of the digital therapeutic mobile app biobase to reduce stress and improve mental well-being among university students: randomized controlled trial. JMIR MHealth UHealth 8:17767. doi: 10.2196/17767
Prochaska, J. O., and DiClemente, C. C. (1984). The Transtheoretical Approach: Crossing the Traditional Boundaries of Change. Homewood, IL: J. Irwin.
Rathbone, A. L., Clarry, L., and Prescott, J. (2017). Assessing the efficacy of mobile health apps using the basic principles of cognitive behavioral therapy: systematic review. J. Med. Internet Res. 19:e399. doi: 10.2196/jmir.8598
Reyes, A. T., Bhatta, T. R., Muthukumar, V., and Gangozo, W. J. (2020). Testing the acceptability and initial efficacy of a smartphone-app mindfulness intervention for college student veterans with PTSD. Arch. Psychiatr. Nurs. 34, 58–66. doi: 10.1016/j.apnu.2020.02.004
Saladino, V., Algeri, D., and Auriemma, V. (2020). The psychological and social impact of covid-19: new perspectives of well-being. Front. Psychol. 11:577684. doi: 10.3389/fpsyg.2020.577684
Shaw, B. M., Lee, G., and Benton, S. (2017). “Work smarter, not harder: expanding the treatment capacity of a university counseling center using therapist-assisted online treatment for anxiety,” in Career Paths in Telemental Health, eds M. Maheu, K. Drude, and S. Wright (Cham: Springer), 197–204. doi: 10.1007/978-3-319-23736-7_19
Spooner, S. E. (2000). “The college counseling environment,” in College Counseling: Issues and Strategies for a New Millennium, eds D. C. Davis and K. M. Humphrey (Alexandria, VA: American Counseling Association), 3–14.
Storrie, K., Ahern, K., and Tuckett, A. (2010). A systematic review: students with mental health problems-A growing problem. Int. J. Nurs. Pract. 16, 1–6. doi: 10.1111/j.1440-172X.2009.01813.x
Taylor, C. B., Fitzsimmons-Craft, E. E., and Graham, A. K. (2020). Digital technology can revolutionize mental health services delivery: the COVID-19 crisis as a catalyst for change. Int. J. Eating Disord. 53, 1155–1157. doi: 10.1002/eat.23300
The Joanna Briggs Institute (JBI) (2017a). Checklist for Randomized Controlled Trials. Adelaide, SA: Joanna Briggs Institute.
The Joanna Briggs Institute (JBI) (2017b). Checklist for Quasi-Experimental Studies. Adelaide, SA: Joanna Briggs Institute.
Torous, J., Nicholas, J., Larsen, M. E., Firth, J., and Christensen, H. (2018). Clinical review of user engagement with mental health smartphone apps: evidence, theory and improvements. Evid. Based Ment. Health 21, 116–119. doi: 10.1136/eb-2018-102891
Webb, T. L., Joseph, J., Yardley, L., and Michie, S. (2010). Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 12, 1–18. doi: 10.2196/jmir.1376
Wilansky, P., Eklund, M., Milner, T., Kreindler, D., Kovacs, T., Shooshtari, S., et al. (2016). Cognitive behavior therapy for anxious and depressed youth: improving homework adherence through mobile technology. JMIR Res. Protoc. 5:e209. doi: 10.2196/resprot.5841
Witkiewitz, K., Desai, S. A., Bowen, S., Leigh, B. C., Kirouac, M., and Larimer, M. E. (2014). Development and evaluation of a mobile intervention for heavy drinking and smoking among college students. Psychol. Addict. Behav. 28, 639–650. doi: 10.1037/a0034747
World Health Organization (2020). Coronavirus Disease (COVID-19). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19 (accessed December, 21, 2020).
Keywords: college students, mental health, mHealth, cognitive-behavioral therapy, counseling services
Citation: Oliveira C, Pereira A, Vagos P, Nóbrega C, Gonçalves J and Afonso B (2021) Effectiveness of Mobile App-Based Psychological Interventions for College Students: A Systematic Review of the Literature. Front. Psychol. 12:647606. doi: 10.3389/fpsyg.2021.647606
Received: 30 December 2020; Accepted: 06 April 2021;
Published: 11 May 2021.
Edited by:
Nikolaos Kazantzis, Cognitive Behavior Therapy Research Unit, AustraliaReviewed by:
Emma Motrico, Loyola Andalusia University, SpainGuy Doron, Interdisciplinary Center Herzliya, Israel
Copyright © 2021 Oliveira, Pereira, Vagos, Nóbrega, Gonçalves and Afonso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carla Oliveira, Y2FybGFhbmRyZWlhQHVhLnB0