 Simone Mayer1,2*
Simone Mayer1,2* Stefanie Fuchs2
Stefanie Fuchs2 Madeleine Fink3
Madeleine Fink3 Norbert Schäffeler2
Norbert Schäffeler2 Stephan Zipfel2Franziska Geiser4
Stephan Zipfel2Franziska Geiser4 Heinz Reichmann1
Heinz Reichmann1 Björn Falkenburger1Marco Skardelly5,6,7
Björn Falkenburger1Marco Skardelly5,6,7 Martin Teufel2,3,8
Martin Teufel2,3,8- 1Department of Neurology, University Hospital Carl Gustav Carus Dresden, Dresden, Germany
- 2Department of Psychosomatic Medicine and Psychotherapy, University Hospital Tübingen, Tübingen, Germany
- 3Department of Psychosomatic Medicine and Psychotherapy, LVR University Hospital Essen, Essen, Germany
- 4Department of Psychosomatic Medicine and Psychotherapy, University Hospital Bonn, Bonn, Germany
- 5Center for Neuro-Oncology, Comprehensive Cancer Center Tübingen-Stuttgart, University Hospital Tübingen, Tübingen, Germany
- 6Department of Neurosurgery, University Hospital Tübingen, Tübingen, Germany
- 7Department of Neurosurgery, District Hospital Reutlingen, Reutlingen, Germany
- 8Section of Psycho-Oncology, West German Cancer Center (WTZ), University Hospital Essen, Essen, Germany
Objective: Hopelessness and depression are strongly associated with suicidality. Given that physical and psychological outcomes can be altered with hope, hope is a therapeutic goal of increasing importance in the treatment of brain tumor patients. Moreover, it is not yet understood which factors affect the perception of hope in brain tumor patients. In addition, it remains uncertain whether lower-grade brain tumor patients suffer less from psycho-oncological distress than higher-grade brain tumor patients.
Methods: Neuro-oncological patients were examined perioperatively with the Distress Thermometer (DT) and the Herth Hope Index (HHI). In addition, psychological comorbidities (anxiety GAD-2, depression PHQ-2) and an assessment of general psycho-oncological distress were recorded.
Results: Sixty-six brain tumor patients were included (median age 53 years, 35% higher-grade brain tumors, i.e., WHO grade III/IV). No differences between higher- and lower-grade brain tumor patients were observed for general psycho-oncological distress and hope. However, higher-grade brain tumor patients showed a significantly higher level of depression (p ≤ 0.001) and more negative expectations regarding therapeutic success (H = 4.873, p ≤ 0.050). The extent of depression correlated negatively with hope.
Conclusion: Unexpectedly, higher-grade brain tumor patients remained as hopeful as lower-grade brain tumor patients despite the devastating diagnosis, higher levels of depression, and a worse expectation of therapeutic success. Conversely, lower-grade brain tumor patients experience as much psycho-oncological distress as patients with a higher-grade brain tumor, underpinning the imperative need for comprehensive psycho-oncological screening. For all brain tumor patients, considering hope is important to avoid suicides resulting from hopelessness and depression.
Introduction
Hope is inherent in human nature, i.e., it is mainly determined by innate personality traits; but the disease process of cancer can have an impact on an individual’s level of hope (Corn et al., 2020). Hope can be fostered by psychotherapeutic treatment (Rustøen et al., 2011) and should therefore be considered as a beneficial therapeutic target to improve quality of life in cancer patients (Corn et al., 2020).
Quality of life, self-esteem, coping, adjustment to an illness, well-being, satisfaction with information received, and relationships are important factors for the feeling of hope (Vellone et al., 2006). In consequence, aspects of hope, such as positive expectations and optimism, can influence psychological and physical outcomes (Leedham et al., 1995; Duggal et al., 2016).
It is expected that hope depends on the tumor stage since patients with an early stage diagnosed tumor feel more hope than patients with an advanced stage or recurring tumor (Acquaye et al., 2016). There is a tendency toward increased psychological distress in more aggressive tumors with worse prognosis (Trad et al., 2015). But even patients with a lower-grade brain tumor have a high psychological burden. More than 10 years after surgery they still experience an impairment of their quality of life (Nassiri et al., 2019). Conversely, patients receiving palliative treatment do not differ significantly in their experience of hope from patients receiving curative therapy (Sanatani et al., 2008). Therefore, it cannot be conclusively determined whether patients with a higher-grade brain tumor experience more hope than patients with a lower-grade brain tumor. However, there is no doubt that hope is clinically relevant because it may help patients to improve their health behavior, accept help from caregivers, and stay in treatment, which contributes to longer survival (Aspinwall and Tedeschi, 2010; Mahendran et al., 2016). In some studies, a direct effect of hope on survival has also been investigated, but this remains controversial (Nagano et al., 2006; Nakaya et al., 2008).
Depression, anxiety, and general psycho-oncological distress have a negative impact on quality of life in cancer patients (Mehnert et al., 2010, 2018). These factors are assumed to correlate with feelings of hope in brain tumor patients. The recognition of depression and mood disorders, which are frequent in brain tumor patients (Bunevicius et al., 2013b), is immensely important in long-term cancer care (Mitchell et al., 2011). The distress burden of depression remains high during the course of the brain tumor disease (Renovanz et al., 2019), which may lead to a poorer quality of life associated with increased mortality (Gathinji et al., 2009). Depression and hopelessness are associated with the construct of demoralization (Ignatius and De La Garza, 2019). Demoralization, in turn, evokes a desire for hastened death or suicide (Rzeszut and Assael, 2021). Because suicide rates are twice as high in cancer patients as in the general population, it is important to recognize the risk factors depression and demoralization associated with hopelessness (McFarland et al., 2019).
As of today, despite quite a few studies, findings on the experience of hope at different stages of cancer are inconsistent. Given the potential of hope to alter oncologic outcomes in cancer patients and the opportunity to improve quality of life, there is a growing demand for more research in this area (Corn et al., 2020).
The aim of this study was to investigate if patients with a higher-grade brain tumor have less hope and more general psycho-oncological distress than patients with a lower-grade brain tumor. In addition, we compared patients with a lower- vs. higher-grade brain tumor with respect to psycho-oncological issues and determined the factors that are associated with the experience of hope.
Methods
A cross-sectional, single-center study was conducted between September 2015 and November 2016 with brain tumor patients of the Neurosurgery Department of Tübingen University Hospital. Inclusion criteria were patients who understood the local language and presented with any kind of brain tumor that requires a biopsy or craniotomy. Exclusion criteria were severe problems with the German language, severe physical problems (e.g., sedation, concentration deficits), illiteracy, or severe difficulties in usage of a tablet PC. Seventy-one patients were consecutively screened, with five patients excluded (one brain metastasis in renal cell carcinoma, two Adenoma of the adenohypophysis, one unclear mass without biopsy, one schizophrenia). Sixty-six patients were assessed and included in the analysis. The patients gave electronic informed consent and predominantly completed the questionnaire on a tablet PC in the hospital. The patients were accustomed to using a tablet PC (Schäffeler et al., 2013). The assessment took place perioperatively (61 out of 66 patients were interviewed the day before surgery, 5 out of 66 patients were interviewed 4–6 days after surgery).
Ethics approval was obtained beforehand from the local ethics committee of the Medical Faculty at the University of Tübingen (reference number 602/2014BO2).
The assessment for socio-demographic data included marital status, current living situation, highest level of education, and working state. The assessment for mental history included questions about psychotropic medication and psychotherapeutic treatment at present or past. The patients were classified into lower-grade (WHO stage I/II) and higher-grade (WHO stage III/IV) brain tumor patients (Table 1). For 56 out of 66 patients it was the first brain surgery while 10 out of 66 patients received a recurrent resection (Table 2).
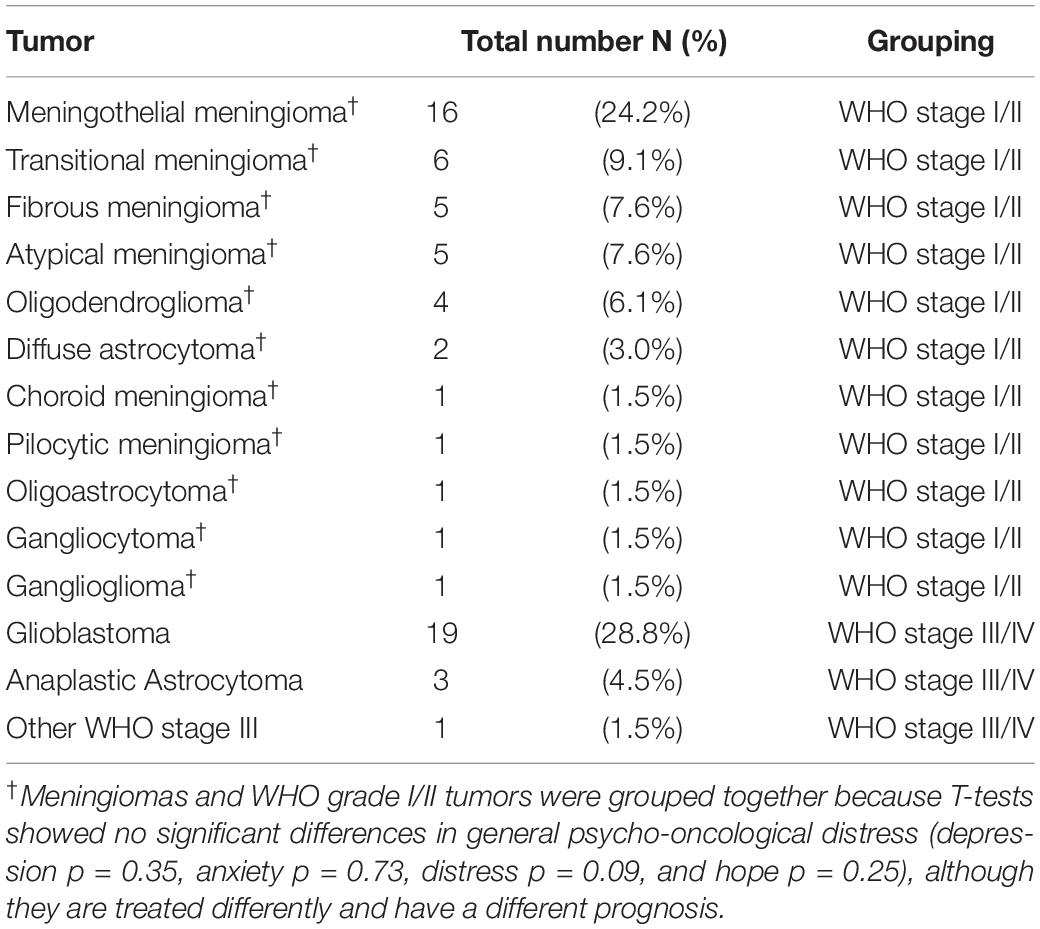
Table 1. Classification of patients in the respective WHO stage group (N = 66).
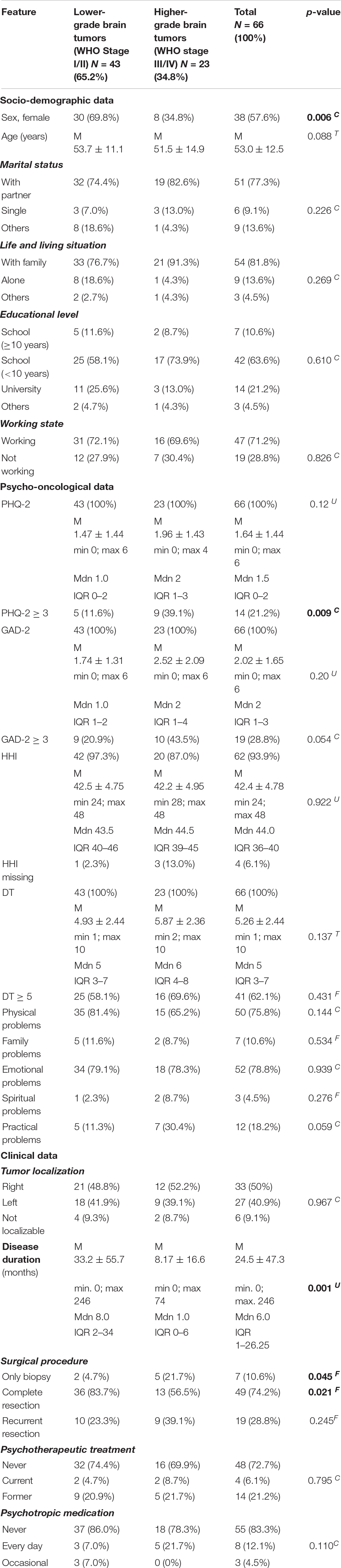
Table 2. Sample description.
Assessment Instruments
Distress Thermometer (DT)
Distress Thermometer (DT) is a scale with values from 0 to 10. Zero means “no distress” and 10 means “extreme distress” (Roth et al., 1998; National Comprehensive Cancer Network, 1999, 2003). The patients indicate which value best describes their level of distress during the previous week. In addition, the DT comprises a problem list including 34 items on practical, emotional, family, spiritual, and physical problems (Mehnert et al., 2006; Rapp et al., 2018). A DT cut-off ≥ 5 is considered appropriate (Lambert et al., 2014). The DT is a valid and reliable screening instrument with 83% sensitivity and 68% specificity (Donovan et al., 2014).
Generalized Anxiety Disorder-2 (GAD-2)
Generalized Anxiety Disorder-2 (GAD-2) is a short form measurement with two questions for screening generalized anxiety disorder (Spitzer et al., 2006). From the summation of both questions, a scale value in the range of 0–6 points is calculated. Higher scores correspond to higher anxiety. A value ≥ 3 is regarded as a serious indicator of pathological anxiety (Spitzer et al., 2006; Kroenke et al., 2007). The GAD-2 performs well (area under the curve, 0.80–0.91) as a screening tool for anxiety disorders (Kroenke et al., 2007) and is well-suited for brain tumor patients, as demonstrated for neurological patients with acceptable internal consistency (Cronbach’s α = 0.77) (Hughes et al., 2018) and head and neck cancer patients with good internal consistency (Cronbach’s α = 0.87) (Hammermüller et al., 2021).
Patient Health Questionnaire-2 (PHQ-2)
Patient Health Questionnaire-2 (PHQ-2) is a short measurement consisting of two questions to detect depression (Löwe et al., 2005). The combined value of both questions (generated by addition) ranges from 0 to 6 with higher values indicating stronger depressive symptoms. A cut-off value of ≥ 3 is the optimum for screening a depression. The PHQ-2 shows a sensitivity of 87% and a specificity of 78% for major depressive disorder (Löwe et al., 2005). Preliminary results show that depression can be successfully identified in brain tumor patients by using the PHQ-2, which has moderate internal consistency (Cronbach’s α = 0.68) (Bunevicius et al., 2013a).
Herth-Hope-Index (HHI)
Herth-Hope-Index (HHI) is a proven and practical instrument in research and clinical setting for the assessment of hope and shows a good reliability and validity with12 items on a 4-point Likert scale ranging from 12 to 48 (higher sores indicate more hope) (Herth, 1992). The German version of the HHI used in this study shows high practicability, good internal consistency (Cronbach’s α = 0.82), and solid concurrent validity, especially for cancer patients (Geiser et al., 2015).
Questionnaire for Coping Parameters
Questionnaire for coping parameters was designed for this study. The questionnaire consists of the following six 10-point Likert-scale aspects: (i) expectations of therapeutic success, (ii) expectations of side effects, (iii) former resilience rating, (iv) current state of mental health, (v) ability to handle the disease, and (vi) social environment support.
Statistical Analyses
Statistical analysis was performed using statistical program for social sciences (SPSS) version 25 (IBM New York). Differences between the two dichotomous WHO stage groups (WHO stage I/II vs. WHO stage III/VI), were analyzed by means of Chi-square test for categorical variables, Mann-Whitney U test for metric scaled non-normally distributed variables, T-test for metric-scaled normally distributed variables, and Fisher’s exact test for small sample sizes (Table 2). In addition, the coping parameter differences between the two dichotomous WHO stage groups were investigated by means of the Kruskal-Wallis test (Figure 1). To identify parameters that are associated with hope in patients with a brain tumor, linear logistic regression was used. Aligned with the study sample’s N = 66 patients, the three variables depression, anxiety, and general psycho-oncological distress which had a statistical influence on univariate analysis were considered (Table 3). A p-value less than 0.05 was regarded as statistically significant.
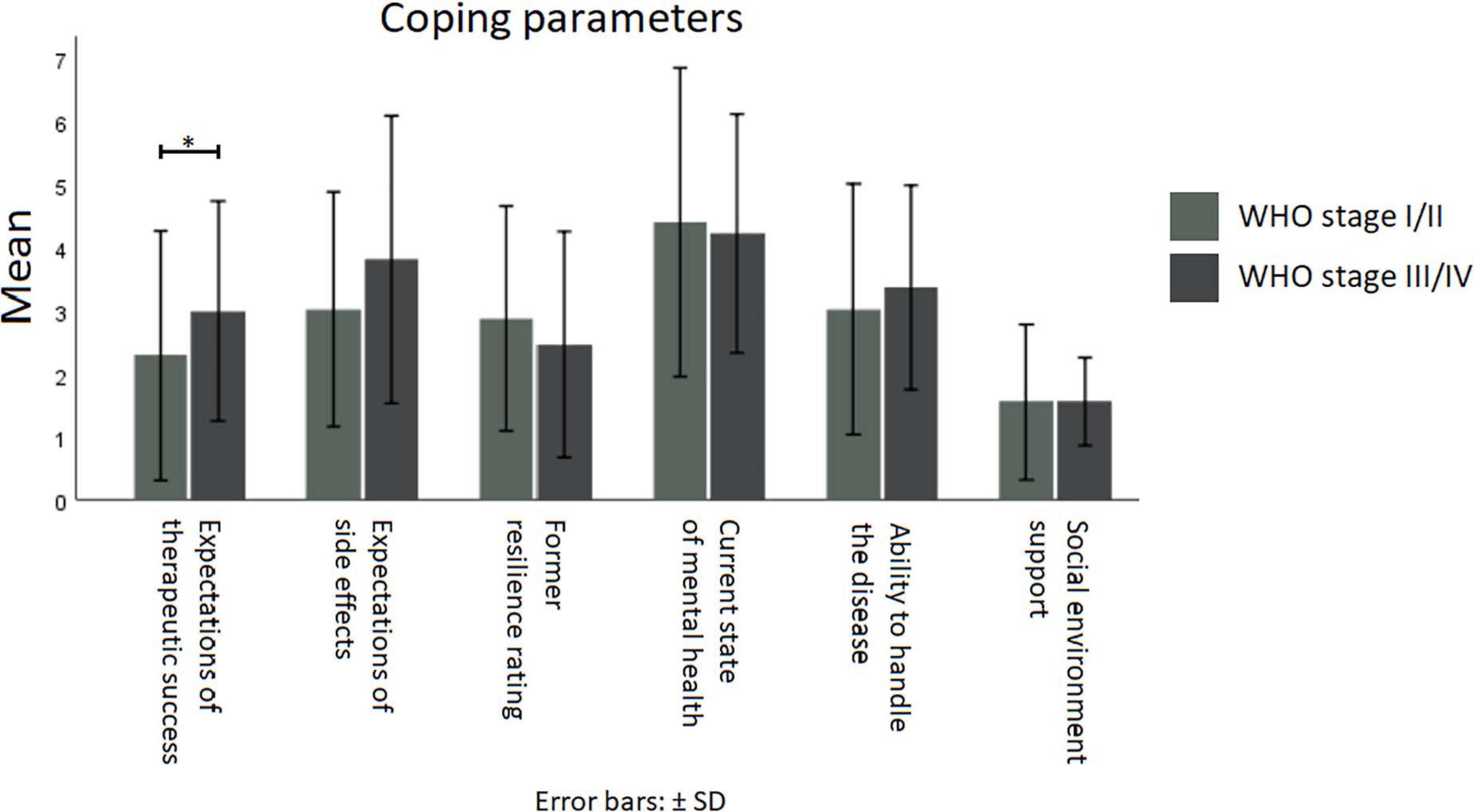
Figure 1. Means of coping parameters for WHO stages I/II (light gray) vs. stages III/IV (dark gray). Kruskal-Wallis test showed no differences between lower and higher WHO stages, except for the expectations of therapeutic success (H = 4.873, p ≤ 0.050, N = 66). *p ≤ 0.05.
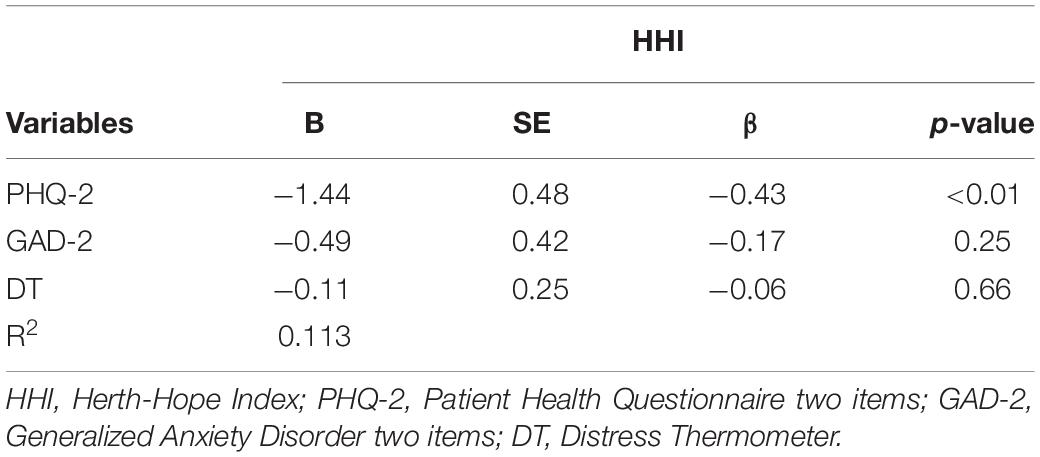
Table 3. Multivariate regression analysis (inclusion method) for determining factors associated with the perception of hope (N = 61).
Results
This study includes the complete data sets from 66 patients except the HHI which was completed by 62 patients. Apart from sex, socio-demographic data between the WHO stage groups were comparable. Patients with a lower-grade brain tumor were more frequently female (p = 0.006) compared with higher-grade brain tumor patients (Table 2).
Tumor-Specific Data
Compared with higher-grade brain tumor patients, patients with a lower-grade brain tumor suffered from a longer course of disease (p = 0.001) and more often received a complete resection (p = 0.021) rather than a biopsy (p = 0.045). Regarding the lateral location of the tumors, no notable difference between the groups was detected (Table 2).
Psycho-Oncological Data
The lion’s share of patients never received psychotherapeutic treatment (72.7%) or psychotropic medication (83.3%). Apart from depression, there were no differences in other psycho-oncological data, especially not in hope (p = 0.922), general psycho-oncological distress (p = 0.137), and anxiety (p = 0.054). Noteworthy, patients with a higher-grade brain tumor were more often depressed (p = 0.009). The observed overall prevalence of depression (21.2%) and anxiety (28.8%) are in line with previous studies (Arnold et al., 2008; Huang et al., 2017). Due to the DT cut-off ≥ 5, the patient’s distress levels in this study are higher compared with previously studies published which use ≥ 6 as DT cut-off (Liu et al., 2018).
According to the DT problem list, about three out of four patients reported emotional (78.8%) and physical problems (75.8%). The most represented within emotional problems were sadness (50%), fear (40.9%), and loss of interest (39.4%). Getting around (36.4%), nausea (31.8%), sleep (33.3%), and sexual problems (25.8%) were the most frequently reported physical problems. Of a lesser mention were practical (18.2%), family (10.6%), and spiritual problems (4.5%).
For disease duration, no differences in over threshold psycho-oncological data (anxiety p = 0.18 C, depression p = 0.55 C, general psycho-oncological distress p = 0.32 C, and hope 0.81 C) were observed using the median split of 6 months.
There are also no differences in gender in over threshold psycho-oncological data (anxiety p = 1.00 F, depression p = 0.56 F, general psycho-oncological distress p = 0.61 F, and hope 1.00 F).
Coping Factors and Hope
The HHI of this study showed an average of 42.4 out of 48 points (Table 2). Higher- and lower-grade brain tumor patients showed similar hope levels. This demonstrates that brain tumor patients’ hope levels are not significantly different compared with tumor patients in general (Geiser et al., 2015). Regarding the expectation of therapeutic success, a statistically significant difference between higher (n = 23) and lower WHO tumor stages (n = 43) was observed. Patients with a higher tumor stage showed lower expectations of therapeutic success (Kruskal-Wallis test, H = 4.873, p ≤ 0.050). Apart from that, no further differences in coping factors were identified (Figure 1).
Parameters Associated With Hope
Depression, without doubt, was identified as a negative factor influencing hope. The PHQ-2 score shows a unique statistically significant contribution (p < 0.01) in the multivariate linear regression analysis (R2 is 0.340 and the entire model is statistically significant with p < 0.001). Cases with missing data in the HHI were excluded from the model. The dependent variable was the total value in the HHI. In contrast, general psycho-oncological distress and anxiety has no statistically significant contribution.
Discussion
The data obtained in this study revealed that patients with a higher-grade brain tumor have just as much hope as lower-grade brain tumor patients despite a higher level of depression and a worse expectation of therapeutic success. This is all the more surprising because the evaluation also revealed that depression is negatively correlated with the feeling of hope. Contrary to the prevailing assumption, no differences in general psycho-oncological distress between higher- and lower grade brain tumor patients was observed. Despite over threshold values in the general psycho-oncological distress assessment, perioperatively, both groups experienced similar high levels of hope compared with the general population (Wahl et al., 2004).
In the group with the lower-grade brain tumors the female sex was more frequently represented. This finding is consistent with the literature as the increased occurrence of meningiomas has been hypothesized by female hormones (Wiemels et al., 2010). In general public, the distribution of the tumor entities of glioblastomas and meningiomas is similar (Wiemels et al., 2010; Crocetti et al., 2012). The other statistical differences in treatment and clinical characteristics, namely more complete resections and longer treatment durations of lower-grade brain tumor patients as well as more biopsies in patients with higher-grade brain tumors, result from the respective treatment guidelines and the pathophysiological tumor characteristics (Marosi et al., 2008).
Strengthening Hope—Reducing Depression
Hope is an important factor in the treatment of cancer patients (Ho et al., 2010). The feeling of hope is essential for a viable doctor-patient relationship and necessary in the mental processing of a life-threatening disease (Clayton et al., 2008; Werner and Steihaug, 2017).
We have demonstrated that in the present sample of patients with brain tumors, depression is negatively correlated with the feeling of hope, which is consistent with previous results (Thimm et al., 2013).
It is to be strongly expected that this finding will have a negative impact on the quality of life (Szramka-Pawlak et al., 2014). Hopelessness has been discussed as a factor for suicidal ideation (Liu et al., 2015; Robinson et al., 2015; Ribeiro et al., 2018) and traumatic brain injuries are just an additional risk factor (Fazel et al., 2014; Fralick et al., 2019). Hypothetically, also neurosurgical interventions should be added to the list. In particular, the occurrence of cognitive inhibition deficits as a consequence of altered brain activation, may facilitate suicidal acts (Richard-Devantoy et al., 2016). Suicidal ideations reported from brain tumor patients are not more frequent compared to the general population (Forkmann et al., 2012; Pranckeviciene et al., 2016). However, to this day, the consequences of hopelessness on this matter are not explicitly investigated. The effect of hope on suicidal ideation and its interaction with depression should be further investigated in particular in brain tumor patients. Fostering quality of life by supporting a sense of hope in all tumor stages and grades remains a central task for both, oncology and psycho-oncology.
It is expected that higher-grade brain tumors patients are more depressed and anxious than those with a lower-grade brain tumor. Much to our astonishment, no significant difference in distress levels between the groups was observed. The direct association of brain lesions with depression (Richard-Devantoy et al., 2016) is one possible explanation in particular because wide spreading of glioblastomas tumor cells is a typical characteristic of the course of the disease (Vollmann-Zwerenz et al., 2020).
In this study, both groups do not significantly differ in both, hope and distress. For the only minor differences in hope there are three likely causes, (i) higher-grade brain tumor patients deny their devastating prognosis (Williams et al., 2015), (ii) the measurement is not specific enough to detect even small differences in hope levels between higher- and lower-grade brain tumor patients (Redlich-Amirav et al., 2018; Rustøen et al., 2018), and (iii) hope with its dispositional aspects (Demirli et al., 2015) is a coping mechanism (Clayton et al., 2005). Hope as a coping mechanism may even increase when the prognosis is poor (Palacio and Arias, 2018). For the insignificant differences in distress, two causes seem likely, (i) the diagnosis “brain tumor” overshadows the patients’ assessments of the distress thermometer, and (ii) the denial and hope for cure protects against devastating distress levels even when the prognosis is disastrous. Consequently, in future psycho-oncological screenings, we urge to also pay the needed attention to patients with lower-grade brain tumors.
Hope Springs Eternal in Patients With a Brain Tumor
The patient group with a higher-grade brain tumor showed a more negative expectation regarding the therapeutic success, probably due to a comprehensive information about the worse course of the disease. Expectedly, high HHI values are found when the disease severity is low (e.g., no metastases, curative therapy) (Wakiuchi et al., 2015; Acquaye et al., 2016; Mahendran et al., 2016). Contrary to the expectation, however, also cancer patients with an unfavorable prognosis showed high HHI values which indicates that hope is not necessarily related to tumor entities or recurrence (Ballard et al., 1997; Felder, 2004). Also, in this instance, it seems plausible that hope grows also when the news is bad, provided it is sustained by trust in the treating team. For both, hope and quality of life, the paradox presumably applies that high burden can even increase hope or quality of life, because there is a shift in the disease appraisal (Albrecht and Devlieger, 1999).
The study is limited by the fact that the patient assessment was carried out perioperatively for logistical reasons. It goes without saying that it is preferable to survey patients at the time of diagnosis. Also, there is an imbalance between male (30.2%) and female (69.8%) patients in our cohort, caused by the more frequent occurrence of meningiomas in women. However, the imbalance is put into perspective in a subgroup analysis, which shows no gender dependent effect in the psycho-oncology data and the extent of hope. Because of the cross-sectional study design, no predictive statements can be made. The relatively small sample size could affect the validity and generalizability of the study. Longitudinal studies with a larger sample size allow predictive and valid statements.
Conclusion
As expected, also in our study, depression is substantially pronounced in higher-grade brain tumor patients. However, when it comes to hope, anxiety, and distress, no significant differences between higher- and lower-grade brain tumor patients were observed. Both, higher- and lower-grade brain tumor patients feel much hope, but at the same time also much anxiety and distress. The current investigation contributes with new findings that patients with lower-grade brain tumors also suffer from pathological anxiety and general psycho-oncological distress. There is a correlation between lower hope levels and depression. Therefore, beyond routine psycho-oncological screening, hope should be considered as an important factor in the treatment of brain tumor patients. We emphasize that psycho-oncological screenings, as they are performed in particular in the higher-grade brain tumor patient group, also should be implemented supposedly benign diseases like a meningioma.
Data Availability Statement
Data are available upon request. Requests should be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Medical Faculty at the University of Tübingen. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SM: conception, data acquisition, data analysis, interpretation of the results, and writing of the manuscript. MS and SF: assistance in data acquisition, conception, and contributions to the writing of the manuscript. MF: assistance in data analysis and interpretation of the results. BF, NS, SZ, FG, and HR: contributions to the writing of the manuscript and interpretation of the results. MT: conception, data analysis, interpretation of the results, and contributions to the writing of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Open Access Funding by the Publication Fund of the TU Dresden.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Acquaye, A. A., Lin, L., Vera-Bolanos, E., Gilbert, M. R., and Armstrong, T. S. (2016). Hope and mood changes throughout the primary brain tumor illness trajectory. Neuro. Oncol. 18, 119–125. doi: 10.1093/neuonc/nov101
Albrecht, G. L., and Devlieger, P. J. (1999). The disability paradox: high quality of life against all odds. Soc. Sci. Med. 48, 977–988. doi: 10.1016/s0277-9536(98)00411-0
Arnold, S. D., Forman, L. M., Brigidi, B. D., Carter, K. E., Schweitzer, H. A., Quinn, H. E., et al. (2008). Evaluation and characterization of generalized anxiety and depression in patients with primary brain tumors. Neuro. Oncol. 10, 171–181. doi: 10.1215/15228517-2007-057
Aspinwall, L. G., and Tedeschi, R. G. (2010). The value of positive psychology for health psychology: progress and pitfalls in examining the relation of positive phenomena to health. Ann. Behav. Med. 39, 4–15. doi: 10.1007/s12160-009-9153-0
Ballard, A., Green, T., McCaa, A., and Logsdon, M. C. (1997). A comparison of the level of hope in patients with newly diagnosed and recurrent cancer. Oncol. Nurs. Forum 24, 899–904. doi: 10.1016/s0277-9536(98)00411-0
Bunevicius, A., Deltuva, V., Tamasauskas, S., Tamasauskas, A., and Bunevicius, R. (2013a). Screening for psychological distress in neurosurgical brain tumor patients using the patient health questionnaire-2. Psychooncology 22, 1895–1900. doi: 10.1002/pon.3237
Bunevicius, A., Tamasauskas, S., Deltuva, V., Tamasauskas, A., and Bunevicius, R. (2013b). Psychological distress symptoms’ clusters in brain tumor patients: factor analysis of depression and anxiety scales. Psychooncology 22, 2860–2863. doi: 10.1002/pon.3354
Clayton, J. M., Butow, P. N., Arnold, R. M., and Tattersall, M. H. N. (2005). Fostering coping and nurturing hope when discussing the future with terminally ill cancer patients and their caregivers. Cancer 103, 1965–1975. doi: 10.1002/cncr.21011
Clayton, J. M., Hancock, K., Parker, S., Butow, P. N., Walder, S., Carrick, S., et al. (2008). Sustaining hope when communicating with terminally ill patients and their families: a systematic review. Psychooncology 17, 641–659. doi: 10.1002/pon.1288
Corn, B. W., Feldman, D. B., and Wexler, I. (2020). The science of hope. Lancet Oncol. 21, e452–e459. doi: 10.1016/S1470-2045(20)30210-2
Crocetti, E., Trama, A., Stiller, C., Caldarella, A., Soffietti, R., Jaal, J., et al. (2012). Epidemiology of glial and non-glial brain tumours in Europe. Eur. J. Cancer 48, 1532–1542. doi: 10.1016/j.ejca.2011.12.013
Demirli, A., Türkmen, M., and Arık, R. S. (2015). Investigation of dispositional and state hope levels’ relations with student subjective well-being. Soc. Indic. Res. 120, 601–613. doi: 10.1007/s11205-014-0607-9
Donovan, K. A., Grassi, L., McGinty, H. L., and Jacobsen, P. B. (2014). Validation of the distress thermometer worldwide: state of the science. Psychooncology 23, 241–250. doi: 10.1002/pon.3430
Duggal, D., Sacks-Zimmerman, A., and Liberta, T. (2016). The impact of hope and resilience on multiple factors in neurosurgical patients. Cureus 8:e849. doi: 10.7759/cureus.849
Fazel, S., Wolf, A., Pillas, D., Lichtenstein, P., and Långström, N. (2014). Suicide, fatal injuries, and other causes of premature mortality in patients with traumatic brain injury. JAMA Psychiatry 71:326. doi: 10.1001/jamapsychiatry.2013.3935
Felder, B. E. (2004). Hope and coping in patients with cancer diagnoses. Cancer Nurs. 27, 320–324. doi: 10.1097/00002820-200407000-00009
Forkmann, T., Brähler, E., Gauggel, S., and Glaesmer, H. (2012). Prevalence of suicidal ideation and related risk factors in the german general population. J. Nerv. Ment. Dis. 200, 401–405. doi: 10.1097/NMD.0b013e31825322cf
Fralick, M., Sy, E., Hassan, A., Burke, M. J., Mostofsky, E., and Karsies, T. (2019). Association of concussion with the risk of suicide. JAMA Neurol. 76:144. doi: 10.1001/jamaneurol.2018.3487
Gathinji, M., McGirt, M. J., Attenello, F. J., Chaichana, K. L., Than, K., Olivi, A., et al. (2009). Association of preoperative depression and survival after resection of malignant brain astrocytoma. Surg. Neurol. 71, 299–303. doi: 10.1016/j.surneu.2008.07.016
Geiser, F., Zajackowski, K., Conrad, R., Imbierowicz, K., Wegener, I., Herth, K. A., et al. (2015). The german version of the herth hope index (HHI-D): development and psychometric properties. Oncol. Res. Treat. 38, 356–360. doi: 10.1159/000435900
Hammermüller, C., Hinz, A., Dietz, A., Wichmann, G., Pirlich, M., Berger, T., et al. (2021). Depression, anxiety, fatigue, and quality of life in a large sample of patients suffering from head and neck cancer in comparison with the general population. BMC Cancer 21:94. doi: 10.1186/s12885-020-07773-6
Herth, K. (1992). Abbreviated instrument to measure hope: development and psychometric evaluation. J. Adv. Nurs. 17, 1251–1259. doi: 10.1111/j.1365-2648.1992.tb01843.x
Ho, S. M., Ho, J. W., Bonanno, G. A., Chu, A. T., and Chan, E. M. (2010). Hopefulness predicts resilience after hereditary colorectal cancer genetic testing: a prospective outcome trajectories study. BMC Cancer 10:279. doi: 10.1186/1471-2407-10-279
Huang, J., Zeng, C., Xiao, J., Zhao, D., Tang, H., Wu, H., et al. (2017). Association between depression and brain tumor: a systematic review and meta-analysis. Oncotarget 8, 94932–94943. doi: 10.18632/oncotarget.19843
Hughes, A. J., Dunn, K. M., Chaffee, T., Bhattarai, J. J., and Beier, M. (2018). Diagnostic and clinical utility of the GAD-2 for screening anxiety symptoms in individuals with multiple sclerosis. Arch. Phys. Med. Rehabil. 99, 2045–2049. doi: 10.1016/j.apmr.2018.05.029
Ignatius, J., and De La Garza, R. (2019). Frequency of demoralization and depression in cancer patients. Gen. Hosp. Psychiatry 60, 137–140. doi: 10.1016/j.genhosppsych.2019.04.013
Kroenke, K., Spitzer, R. L., Williams, J. B. W., Monahan, P. O., and Löwe, B. (2007). Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 146, 317–325. doi: 10.7326/0003-4819-146-5-200703060-00004
Lambert, S. D., Pallant, J. F., Clover, K., Britton, B., King, M. T., and Carter, G. (2014). Using rasch analysis to examine the distress thermometer’s cut-off scores among a mixed group of patients with cancer. Qual. Life Res. 23, 2257–2265. doi: 10.1007/s11136-014-0673-0
Leedham, B., Meyerowitz, B. E., Muirhead, J., and Frist, W. H. (1995). Positive expectations predict health after heart transplantation. Heal. Psychol. 14, 74–79. doi: 10.1037//0278-6133.14.1.74
Liu, F., Huang, J., Zhang, L., Fan, F., Chen, J., Xia, K., et al. (2018). Screening for distress in patients with primary brain tumor using distress thermometer: a systematic review and meta-analysis. BMC Cancer 18:124. doi: 10.1186/s12885-018-3990-9
Liu, R. T., Kleiman, E. M., Nestor, B. A., and Cheek, S. M. (2015). The hopelessness theory of depression: a quarter-century in review. Clin. Psychol. Sci. Pract. 22, 345–365. doi: 10.1111/cpsp.12125
Löwe, B., Kroenke, K., and Gräfe, K. (2005). Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 58, 163–171. doi: 10.1016/j.jpsychores.2004.09.006
Mahendran, R., Chua, S. M., Lim, H. A., Yee, I. J., Tan, J. Y. S., Kua, E. H., et al. (2016). Biopsychosocial correlates of hope in asian patients with cancer: a systematic review. BMJ Open 6:e012087. doi: 10.1136/bmjopen-2016-012087
Marosi, C., Hassler, M., Roessler, K., Reni, M., Sant, M., Mazza, E., et al. (2008). Meningioma. Crit. Rev. Oncol. Hematol. 67, 153–171. doi: 10.1016/j.critrevonc.2008.01.010
McFarland, D. C., Walsh, L., Napolitano, S., Morita, J., and Jaiswal, R. (2019). Suicide in patients with cancer: identifying the risk factors. Oncology (Willsiton Park) 33, 221–226.
Mehnert, A., Hartung, T. J., Friedrich, M., Vehling, S., Brähler, E., Härter, M., et al. (2018). One in two cancer patients is significantly distressed: prevalence and indicators of distress. Psychooncology 27, 75–82. doi: 10.1002/pon.4464
Mehnert, A., Lehmann, C., Graefen, M., Huland, H., and Koch, U. (2010). Depression, anxiety, post-traumatic stress disorder and health-related quality of life and its association with social support in ambulatory prostate cancer patients. Eur. J. Cancer Care 19, 736–745. doi: 10.1111/j.1365-2354.2009.01117.x
Mehnert, A., Müller, D., Lehmann, C., and Koch, U. (2006). Die deutsche version des NCCN distress-thermometers. Zeitschrift für Psychiatr. Psychol. und Psychother. 54, 213–223. doi: 10.1024/1661-4747.54.3.213
Mitchell, A. J., Chan, M., Bhatti, H., Halton, M., Grassi, L., Johansen, C., et al. (2011). Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 12, 160–174. doi: 10.1016/S1470-2045(11)70002-X
Nagano, J., Ichinose, Y., Asoh, H., Ikeda, J., Ohshima, A., Sudo, N., et al. (2006). A prospective japanese study of the association between personality and the progression of lung cancer. Intern. Med. 45, 57–63. doi: 10.2169/internalmedicine.45.1453
Nakaya, N., Saito-Nakaya, K., Akechi, T., Kuriyama, S., Inagaki, M., Kikuchi, N., et al. (2008). Negative psychological aspects and survival in lung cancer patients. Psychooncology 17, 466–473. doi: 10.1002/pon.1259
Nassiri, F., Price, B., Shehab, A., Au, K., Cusimano, M. D., Jenkinson, M. D., et al. (2019). Life after surgical resection of a meningioma: a prospective cross-sectional study evaluating health-related quality of life. Neuro. Oncol. 21, i32–i43. doi: 10.1093/neuonc/noy152
National Comprehensive Cancer Network. (1999). NCCN practice guidelines for the management of psychosocial distress. Oncology (Williston Park). 13, 113–147.
National Comprehensive Cancer Network. (2003). Distress management. Clinical practice guidelines. J. Natl. Compr. Canc. Netw. 1, 344–374. doi: 10.6004/jnccn.2003.0031
Palacio, C., and Arias, M. (2018). The role of resilience and coping strategies of fighting spirit in the adaptation of patients with advanced cancer disease attending an oncological institution of medellín-colombia. J. Pain Symptom Manage. 56:e134. doi: 10.1016/j.jpainsymman.2018.10.427
Pranckeviciene, A., Tamasauskas, S., Deltuva, V. P., Bunevicius, R., Tamasauskas, A., and Bunevicius, A. (2016). Suicidal ideation in patients undergoing brain tumor surgery: prevalence and risk factors. Support. Care Cancer 24, 2963–2970. doi: 10.1007/s00520-016-3117-2
Rapp, M., Schipmann, S., Hoffmann, K., Wiewrodt, R., Steiger, H.-J., Kamp, M., et al. (2018). Impact of distress screening algorithm for psycho-oncological needs in neurosurgical patients. Oncotarget 9, 31650–31663. doi: 10.18632/oncotarget.25833
Redlich-Amirav, D., Ansell, L. J., Harrison, M., Norrena, K. L., and Armijo-Olivo, S. (2018). Psychometric properties of hope scales: a systematic review. Int. J. Clin. Pract. 72:e13213. doi: 10.1111/ijcp.13213
Renovanz, M., Soebianto, S., Tsakmaklis, H., Keric, N., Nadji-Ohl, M., Beutel, M., et al. (2019). Evaluation of the psychological burden during the early disease trajectory in patients with intracranial tumors by the ultra-brief patient health questionnaire for depression and anxiety (PHQ-4). Support. Care Cancer 27, 4469–4477. doi: 10.1007/s00520-019-04718-z
Ribeiro, J. D., Huang, X., Fox, K. R., and Franklin, J. C. (2018). Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br. J. Psychiatry 212, 279–286. doi: 10.1192/bjp.2018.27
Richard-Devantoy, S., Ding, Y., Lepage, M., Turecki, G., and Jollant, F. (2016). Cognitive inhibition in depression and suicidal behavior: a neuroimaging study. Psychol. Med. 46, 933–944. doi: 10.1017/S0033291715002421
Robinson, S., Kissane, D. W., Brooker, J., and Burney, S. (2015). A systematic review of the demoralization syndrome in individuals with progressive disease and cancer: a decade of research. J. Pain Sympt. Manage. 49, 595–610. doi: 10.1016/j.jpainsymman.2014.07.008
Roth, A. J., Kornblith, A. B., Batel-Copel, L., Peabody, E., Scher, H. I., and Holland, J. C. (1998). Rapid screening for psychologic distress in men with prostate carcinoma: a pilot study. Cancer 82, 1904–1908.
Rustøen, T., Cooper, B. A., and Miaskowski, C. (2011). A longitudinal study of the effects of a hope intervention on levels of hope and psychological distress in a community-based sample of oncology patients. Eur. J. Oncol. Nurs. 15, 351–357. doi: 10.1016/j.ejon.2010.09.001
Rustøen, T., Lerdal, A., Gay, C., and Kottorp, A. (2018). Rasch analysis of the herth hope index in cancer patients. Health Qual. Life Outcomes 16:196. doi: 10.1186/s12955-018-1025-5
Rzeszut, M., and Assael, R. (2021). Differentiating depression from demoralization in organ transplantation recipients. Prog. Transplant. 31, 88–90. doi: 10.1177/1526924820978602
Sanatani, M., Schreier, G., and Stitt, L. (2008). Level and direction of hope in cancer patients: an exploratory longitudinal study. Support. Care Cancer 16, 493–499. doi: 10.1007/s00520-007-0336-6
Schäffeler, N., Pfeiffer, K., Grischke, E., Wallwiener, D., Garbe, C., Zipfel, S., et al. (2013). Akzeptanz und reliabilität eines elektronischen psychoonkologischen screenings bei patientinnen mit brustkrebs: eine randomisiert-kontrollierte studie. Psychother. Psychosom. Med. Psychol. 63, 374–380. doi: 10.1055/s-0032-1333301
Spitzer, R. L., Kroenke, K., Williams, J. B. W., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder. Arch. Intern. Med. 166:1092. doi: 10.1001/archinte.166.10.1092
Szramka-Pawlak, B., Hornowska, E., Walkowiak, H., and Zaba, R. (2014). Hope as a psychological factor affecting quality of life in patients with psoriasis. Appl. Res. Qual. Life 9, 273–283. doi: 10.1007/s11482-013-9222-1
Thimm, J. C., Holte, A., Brennen, T., and Wang, C. E. A. (2013). Hope and expectancies for future events in depression. Front. Psychol. 4:470.
Trad, W., Koh, E. S., Daher, M., Bailey, A., Kastelan, M., Legge, D., et al. (2015). Screening for psychological distress in adult primary brain tumor patients and caregivers: considerations for cancer care coordination. Front. Oncol. 5:203. doi: 10.3389/fonc.2015.00203
Vellone, E., Rega, M. L., Galletti, C., and Cohen, M. Z. (2006). Hope and related variables in italian cancer patients. Cancer Nurs. 29, 356–366. doi: 10.1097/00002820-200609000-00002
Vollmann-Zwerenz, A., Leidgens, V., Feliciello, G., Klein, C. A., and Hau, P. (2020). Tumor cell invasion in glioblastoma. Int. J. Mol. Sci. 21:1932. doi: 10.3390/ijms21061932
Wahl, A. K., Rustøen, T., Lerdal, A., Hanestad, B. R., Knudsen, O. Jr., and Moum, T. (2004). The norwegian version of the herth hope index (HHI-N): a psychometric study. Palliat. Support. Care 2, 255–263. doi: 10.1017/s1478951504040349
Wakiuchi, J., Marchi, J. A., Norvila, L. S., Marcon, S. S., Sales, C. A., Wakiuchi, J., et al. (2015). Hope of cancer patients undergoing chemotherapy. Acta Paul. Enferm. 28, 202–208. doi: 10.1590/1982-0194201500035
Werner, A., and Steihaug, S. (2017). Conveying hope in consultations with patients with life-threatening diseases: the balance between supporting and challenging the patient. Scand. J. Prim. Health Care 35, 143–152. doi: 10.1080/02813432.2017.1333322
Wiemels, J., Wrensch, M., and Claus, E. B. (2010). Epidemiology and etiology of meningioma. J. Neurooncol. 99, 307–314. doi: 10.1007/s11060-010-0386-3
Keywords: depression, glioblastoma, brain tumor, meningioma, cancer, hope, distress, oncology
Citation: Mayer S, Fuchs S, Fink M, Schäffeler N, Zipfel S, Geiser F, Reichmann H, Falkenburger B, Skardelly M and Teufel M (2021) Hope and Distress Are Not Associated With the Brain Tumor Stage. Front. Psychol. 12:642345. doi: 10.3389/fpsyg.2021.642345
Received: 15 December 2020; Accepted: 26 April 2021;
Published: 28 May 2021.
Edited by:
Eun-Jung Shim, Pusan National University, South KoreaReviewed by:
Gregor Weissflog, Leipzig University, GermanyGiancarlo Pecorari, University of Turin, Italy
Copyright © 2021 Mayer, Fuchs, Fink, Schäffeler, Zipfel, Geiser, Reichmann, Falkenburger, Skardelly and Teufel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simone Mayer, c2ltb25lLm1heWVyQHVuaWtsaW5pa3VtLWRyZXNkZW4uZGU=