
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol., 06 April 2021
Sec. Psychology for Clinical Settings
Volume 12 - 2021 | https://doi.org/10.3389/fpsyg.2021.641770
This article is part of the Research TopicIndividualized Psychotherapy Treatment of Young People with Mental DisordersView all 14 articles
 Julian Edbrooke-Childs1,2*
Julian Edbrooke-Childs1,2* Luís Costa da Silva1,2
Luís Costa da Silva1,2 Anja Čuš3
Anja Čuš3 Shaun Liverpool1,4
Shaun Liverpool1,4 Catarina Pinheiro Mota5,6
Catarina Pinheiro Mota5,6 Giada Pietrabissa7,8Thomas Bardsley1
Giada Pietrabissa7,8Thomas Bardsley1 Celia M. D. Sales5,9
Celia M. D. Sales5,9 Randi Ulberg10,11Jenna Jacob1,2
Randi Ulberg10,11Jenna Jacob1,2 Nuno Ferreira12
Nuno Ferreira12Objective: Symptom improvement is often examined as an indicator of a good outcome of accessing mental health services. However, there is little evidence of whether symptom improvement is associated with other indicators of a good outcome, such as a mutual agreement to end treatment. The aim of this study was to examine whether young people accessing mental health services who meaningfully improved were more likely to mutually agree to end treatment.
Methods: Multilevel multinomial regression analysis controlling for age, gender, ethnicity, and referral source was conducted on N = 8,995 episodes of care [Female = 5,469, 61%; meanAge = 13.66 (SD = 2.87) years] using anonymised administrative data from young people's mental health services.
Results: Compared to young people with no change in mental health difficulties, those showing positive meaningful changes in mental health difficulties were less likely to have case closure due to non-mutual agreement (Odds Ratio or OR = 0.58, 95% Confidence Interval or CI = 0.50–0.61). Similarly, they were less likely to transfer (OR = 0.61, 95% CI = 0.49–0.74) or end treatment for other reasons (OR = 0.59, 95% CI = 0.50–0.70) than by case closure due to mutual agreement.
Conclusion: The findings suggest that young people accessing mental health services whose symptoms meaningfully improve are more likely to mutually agree to end treatment, adding to the evidence that symptom improvement may be appropriate to examine as an indicator of a good outcome of accessing mental health services.
Worldwide, poor mental well-being of young people (YP) has been recognized as being a key challenge to be addressed (Camilletti, 2018). Prevalence data estimates that rates of mental health disorders in YP can reach up to 13.5%, with anxiety and depression leading as the most common presentations (Polanczyk et al., 2015; Cohen et al., 2018). In England, recent survey data reported that one in eight 5 to 19 year olds had at least one mental health disorder and one in twenty met criteria for two or more mental health diagnoses (NHS Digital, 2019). Consequently, treatment options including psychotherapy and more recently digital interventions are being incorporated to support YP and families (Das et al., 2016; Liverpool et al., 2020). Although there is some evidence suggesting the effectiveness and efficacy of these interventions, many studies report limitations such as low engagement, non-adherence, and dropout from treatment, having implications for premature endings and case closure (Kazdin et al., 1994; Kazdin, 1997; Gopalan et al., 2010).
Premature termination, defined as when a “client has left therapy before obtaining a requisite level of improvement or completing therapy goals” (Hatchett and Park, 2003, p. 226) is a significant and widespread problem in the field of mental health (Barrett et al., 2008). Up to 50% of clients discontinue psychological services prematurely (Barrett et al., 2008) which undermines the potential benefits of treatment and reduces the cost-effectiveness of these interventions (Westmacott et al., 2010). Several studies examining potential variables associated with this phenomenon (i.e., client, therapist, and treatment) have been conducted (Wierzbicki and Pekarik, 1993; Garfield, 1994; Sales, 2003; Clarkin and Levy, 2004), but results are largely inconsistent due to the plethora of terms that are often interchangeably used (i.e., attrition, dropout, early termination, pre-mature termination, early withdrawal, among others) (Wierzbicki and Pekarik, 1993) and the methods adopted to operationalize these constructs (Swift et al., 2009). To illustrate, main categorizations of dropout usually include duration of the therapy (i.e., when the YP in a study terminates treatment before the pre-defined cut off) and therapist judgment of whether the treatment termination is a dropout. However, it is often difficult for therapists to detect how clients are responding to therapy (Hannan et al., 2005). Nonetheless, therapists' and the YPs' or carers' assumptions about treatment goals and expectations may differ (Barrett et al., 2008), leading to non-mutually agreed decisions (de Haan et al., 2013). In fact, whether or not criteria for “clinical improvement” or recovery have been met, clients may prematurely end treatment because the necessary gains in functioning have been obtained prior to the end of a set number of sessions, or because they may want to try other interventions on their own, outside of treatment.
On the other hand, clients may recognize a lack of improvement and believe that additional sessions will not be helpful, another perspective that can also be difficult to detect during therapy (Lambert et al., 2005). Further, the type of treatment a client receives also influences rates of non-mutually agreed endings in therapy (Barrett et al., 2008). Treatments involving both medications and therapy in the extant literature have consistently shown lower rates of attrition than either medication or therapy alone (Arnow et al., 2007). Another reason for dropout includes the YP's diagnosis (Westmacott et al., 2010). Researchers reported higher rates of attrition among clients with more severe diagnoses (i.e., externalizing problems) and more complex diagnostic pictures (i.e., comorbidity) (Thormählen et al., 2003). There is also some evidence showing that external factors may also influence YP's use of health care services or constitute barriers to continuing treatment. Such factors include difficulties in finding mental health services, cost for services, degree of family involvement, and social support networks. Beyond that, practical issues such as greater distance traveled, scheduling conflicts, and long waiting lists can negatively influence community perception of the mental health services resulting in earlier dropout from care (Westmacott et al., 2010). Therefore, a need-based definition is a valuable method for categorizing treatment dropouts and mitigates disadvantages of existing definitions of dropout (Dossett and Reid, 2019).
Demographic data such as belonging to an ethnic minority (de Haan et al., 2018) or lower socioeconomic status group (de Haan et al., 2014), having a younger mother, and living in a single-parent household (de Haan et al., 2013) are social and family variables that increase the likelihood of dropping out of treatment. Despite this, variables related to the treatment itself and those related to the therapist were also found to be overall stronger dropout predictors than the pre-treatment child and family or parent/carer variables. Specifically, dropout increases when adolescents experience lower quality of the therapeutic relationship, lower perceived relevance of treatment, more treatment participation barriers, and more stressors (Carter, 1995; Garcia and Weisz, 2002). Significant predictors of dropout are also the adolescent's experience of their therapist as being directive, controlling, and confronting; the therapist not showing care and concern; and dissatisfaction with the focus of therapy (Jethwa et al., 2019). More cancellations or no-shows over the course of the treatment have also been consistently found as a reliable predictor of dropout (Kazdin et al., 1994; Chasson et al., 2008; de Haan et al., 2013). Emerging evidence highlights the importance of including cultural understanding and adoption in the therapeutic relationship in order to retain YP in mental health settings (Yeh et al., 1994; Carter, 1995; Cunningham et al., 2002; Lau, 2006; Huey and Polo, 2008; Miller et al., 2008; Bibi et al., 2017).
Nonetheless, treatment dropout is often regarded as a negative outcome in therapy. A mixed-method study that explored YP's reasons for dropout from treatment highlighted that nearly one third of the sample indicated they had received satisfactory treatment or experienced symptom improvement (O'Keeffe et al., 2019a). Therefore, when clients end treatment non-mutually, their therapists are often not aware whether their clients were (dis)satisfied with the therapy (Westmacott et al., 2010). However, therapists of YP who dropped out due to symptom improvement reported they were not clinically concerned about this group of dropouts. This indicates that treatment terminations following clients who benefitted from therapy may not yet meaningfully be accounted for in existing explanatory models of dropout from treatment (O'Keeffe et al., 2019a).
There is a growing interest in improving outcomes for YP accessing mental health services, with the main focus thus far being on improving symptoms and aiming for “recovery”. However, other outcomes may also be important, and in particular, whether YP and therapist mutually agree with the end of treatment. This line of reasoning may have implications for the evaluation of outcomes at the case level and service level, including accuracy of data and effective use of costs to the National Health Services (Mental Health Taskforce to the NHS in England, 2016). Therefore, it is important to broaden our understanding of the influence of demographics, referral process, and symptom improvements on case closure. Evidence that non mutual case closure may not necessarily be a problem may reflect more self-efficacy, competence, self-rated improvement, and autonomy among YP and their carers (Simon et al., 2012; O'Keeffe et al., 2019b). Despite this wealth of knowledge, we are yet to fully understand if symptom improvement is an indicator of a “good” outcome.
In this vein, the present study aimed to examine whether levels of meaningful improvement in symptoms were associated with reasons for ending treatment, using multilevel multinomial regression analysis controlling for age, sex, ethnicity, and referral source. We hypothesized that youths whose problems meaningfully improved were more likely to mutually agree to end treatment.
Three datasets held by the Child Outcomes Research Consortium on children and young people (0-25 years old) who accessed mental health services in the United Kingdom (UK) between 2002 and 2019 were merged (Costa da Silva et al., submitted). The data corpus was collected by clinicians and service administrators from YP mental health services across England, including those participating in a programme offered by the National Health Services to implement evidence-based practice between 2011 and 2015 (Fonagy et al., 2017). From this merged dataset, cases were included in the present analysis if: (a) the child or young person was aged 6-25 years to reflect the age range that the included measures could be self-reported, (b) the case was closed, (c) there was at least one paired outcome measure completed at time 1 and time 2, and (d) there was a reason for case closure. This resulted in a final dataset of N = 8,995 episodes of care (i.e., independent observations) [Female = 5,469, 61%; meanAge = 13.66 (SD = 2.87) years]. Detailed demographic characteristics are shown in Table 1.
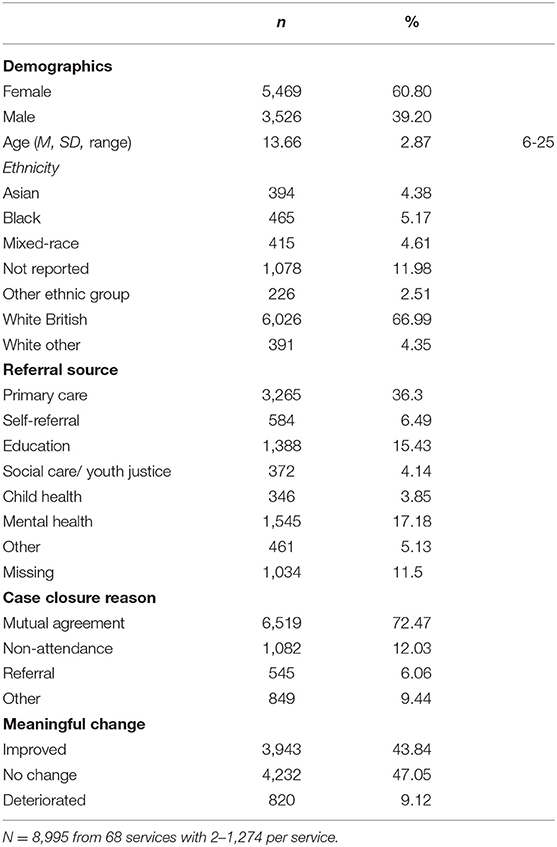
Table 1. Descriptive statistics for all study variables.
The present analysis involved secondary analysis of anonymised administrative data and therefore, an ethical review was not required (Tripathy, 2013).
Age, gender, and ethnicity were recorded by services as part of routine data recording. Ethnicity was captured using the categories from the 2001 Census (Office for National Statistics, 2019) and was generally based on self-report by the parent/carer or the young person. These were grouped for analysis as follows: White British (as the ethnic majority group), White Other (including Irish and Other White background), mixed-race (including Mixed White and Black Caribbean, Mixed White and Black African, Mixed White and Asian, and any other mixed background), Asian (including Indian, Pakistani, Bangladeshi, and Other), Black or Black British (including Caribbean, African, and Other), other ethnic groups (including Chinese and Other), and not stated. As used in previous research, referral source was recorded by services using 30 indicators, which were grouped into nine study variables for the present analysis (Edbrooke-Childs and Patalay, 2019). In the main analysis, referral from primary care was selected as the reference category as it was the largest group.
To measure symptom improvement, meaningful change according to self-reported measures was used. Meaningful change is the current analytic approach used by policy in England to examine national administrative data from child and adolescent mental health services. As we report elsewhere (Costa da Silva et al., submitted), meaningful change consisted of reliable change in standardized measures, or change more than would be expected solely from measurement error, and clinically important change in idiographic measures. For each completed measure at time 1 and time 2, it is therefore possible to improve, not change, or deteriorate according to reliable or clinically important change. YP were then classified as: (a) meaningfully improved if they met the criteria for improvement on at least one completed measure at time 1 and time 2 and did not deteriorate on any other measure, (b) not meaningfully changed if no completed measure at time 1 or time 2 met the criteria for reliable or clinically important change, or (c) meaningfully deteriorated if they met the criteria for deterioration on any completed measure at time 1 and time 2.
Case closure reason was recorded by services and grouped into four categories for the present analysis: mutual agreement, non-mutual agreement, transfer, and other.
To examine whether YP who meaningfully improved were more likely to mutually agree to end treatment, accounting for the nesting of episodes of care in services and controlling for age, gender, ethnicity, and referral source, multilevel multinomial logistic regressions were conducted in STATA 16 (StataCorp., 2019). Three preparatory models were estimated. In Model 0 (null model) the variance explained in case closure reason at the service-level was examined and no predictors were added. The intraclass correlation coefficient was 45%, indicating that there was significant service-level variation in case closure reason and confirming that multilevel modeling was the appropriate statistical approach. In Model 1, demographic characteristics were added: male; grand-mean-centered age; and ethnicity with the White British group as the reference category as it was the largest group. In Model 2, referral source was added with primary care as the reference category. In the final model, meaningful change was added with no change selected as the reference category as it was the largest group. The likelihood ratio test was used to compare successive models, which were significant, and all variables were therefore retained in the final model. In particular, the likelihood ratio test was significant for the final model compared to Model 2: χ2(6) = 111.3, p < 0.001.
The results of the final model are shown in Table 2. Compared to girls, boys were less likely to have case closure due to non-mutual agreement than case closure due to mutual agreement. Compared to younger YP, older YP were more likely to have case closure due to non-mutual agreement and transfer than case closure due to mutual agreement. Compared to White British YP, Black or Black British YP, mixed-race YP, and those from other White backgrounds were more likely to have case closure due to non-mutual agreement than case closure due to mutual agreement. Compared to White British YP, mixed-race YP were more likely to have case closure due to transfer than case closure due to mutual agreement. In contrast, compared to White British YP, YP with not reported ethnic backgrounds were less likely to have case closure reason due to transfer than case closure due to mutual agreement. Compared to White British YP, Asian YP, mixed-race YP, and YP with “other” ethnic backgrounds were less likely to have case closure due to other reasons than case closure due to mutual agreement. Compared to White British YP, YP with not reported ethnic backgrounds were more likely to have case closure due to other reasons than case closure due to mutual agreement.
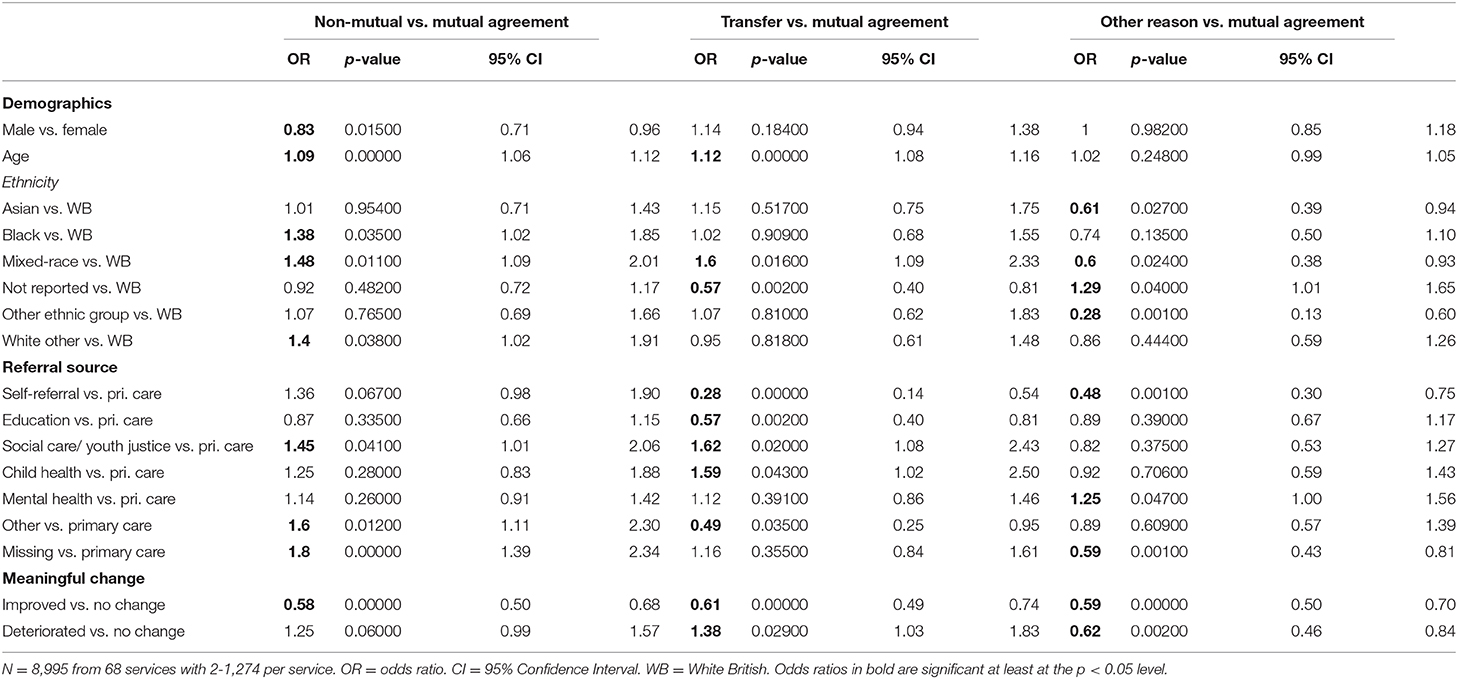
Table 2. Multilevel multinomial regression with demographics, referral source, and meaningful improvement predicting case closure reason.
Compared to YP referred by primary care, YP referred through social care/ youth justice, other sources, and with missing referral source were more likely to have case closure due to non-mutual agreement than case closure due to mutual agreement. Compared to YP referred by primary care, YP referred by self-referral, education, or other sources were less likely to have case closure due to transfer than case closure due to mutual agreement. In contrast, compared to YP referred by primary care, YP referred by social care/ youth justice or child health were more likely to have case closure due to transfer than case closure due to mutual agreement. Compared to YP referred by primary care, YP referred by mental health services were more likely to have case closure due to other reasons, and YP referred by self-referral or with missing referral source were less likely to have case closure due to other reasons, than case closure due to mutual agreement.
Compared to YP who did not meaningfully change in symptoms, YP who meaningfully improved in symptoms were less likely to have case closure due to non-mutual agreement, transfer, and other reasons than case closure due to mutual agreement. Compared to YP who did not meaningfully change in symptoms, YP who meaningfully deteriorated in symptoms were more likely to have case closure due to transfer, and were less likely to have case closure due to other reasons, than case closure due to mutual agreement.
To better understand symptom improvement as an indicator of a good outcome of accessing YP mental health services, this study examined whether levels of meaningful improvement were associated with reasons for ending treatment. Multilevel multinomial regression analyses were conducted controlling for age, gender, ethnicity, and referral source. As hypothesized, the results indicated that YP whose problems meaningfully improved were more likely to mutually agree to end treatment.
Our results are consistent with previous studies showing improved mental health to be associated with treatment completion when compared to YP who prematurely ended treatment (Kazdin et al., 1994; Chasson et al., 2008; de Haan et al., 2013). Nevertheless, the present study builds on the extant literature as it is the largest study on symptom improvement and reasons for case closure. Moreover, this study used an advanced statistical approach to account for service-level variation. This study also uses the latest approach to measuring symptom improvement using meaningful change.
A possible explanation could be that YP who do not experience improvement are more likely to go on to access adult care or other specialist services, which this study highlighted. This is consistent with studies in adult mental health services (Westmacott et al., 2010; Bartholomew et al., 2019). These findings may also be attributed to treatment engagement which can be affected by diagnostic agreement (Jensen-Doss and Weisz, 2008) and shared treatment decision-making experiences in YP mental health services (Edbrooke-Childs et al., 2015). Further, existing research suggests the most common reason for non-mutual treatment endings in YP therapeutic settings was a therapeutic relationship disconnect (Carter, 1995; Garcia and Weisz, 2002). Although the current findings show significant associations between meaningful change and mutual agreement to end treatment, a recent study found no significant evidence linking YP depressive symptoms to mutual agreement on treatment ending (O'Keeffe et al., 2019b). This inconsistency may warrant further investigations if we are to generalize findings across symptom type, treatment type, and the level of impact the psychosocial difficulties may have on the YP and their families.
The current findings also reflect further potential disparities and child mental health inequalities in the UK (Fairchild, 2019). In comparison to White British YP, Black or Black British YP, mixed-race YP, and YP from other White ethnic backgrounds were more likely to have case closure due to non-mutual agreement than have case closure due to mutual agreement. It is likely that such connections exist highlighting associations such as ethnic minority groups being more likely to access YP mental health services through non-voluntary routes, for example, social care/ youth justice (Edbrooke-Childs and Patalay, 2019). This is important because the current findings suggest that YP who access services through more compulsory sources, such as social care/ youth justice, were more likely to have case closure reason due to non-mutual agreement and transfer than case closure due to mutual agreement. These findings may possibly support previous research outlining socio-economic disadvantages as a predictor of dropout from treatment, which include factors such as a lack of transportation and childcare (Kazdin et al., 1994; Kazdin, 1997; de Haan et al., 2013). However, it is still unclear which mediating factors may influence these findings as previous research fails to associate these demographic factors with treatment outcome and ending (O'Keeffe et al., 2019a).
Yet, there is some suggestion that the interface between difficulties and the type of intervention may be the effective element in YP retention (Baruch et al., 1998; Johnson et al., 2009). This poses a question whether relevant and effective treatments are being offered to YP with the most severe and complex needs.
Whilst the finding that YP who achieve meaningful improvement are likely to end treatment on mutual terms, there are also methodological and outcome tracking considerations here. Previous research suggests that clients may disengage from treatment when they have reached a level of “recovery” that is important to them (Hynan, 1990; McKenna and Todd, 1997; Todd et al., 2003). Therefore, there may be a discord between the outcomes of importance to the clinician and young person. If YP feel as though they have reached a level of recovery or improvement that is important to them, they may discontinue treatment regardless of how much progress they have made on a symptom-based measure. Thus, highlighting the importance of collecting a range of outcome information, and further highlighting the importance of shared decision-making.
Although our findings suggest that YP who meaningfully improve are more likely to mutually agree to ending treatment, clinicians and researchers should consider that some YP may non-mutually end treatment if they self-assess as having sufficiently improved. This speaks in favor of ongoing evaluations of treatment goals and progress tracking. In light of the previous literature, it is also important to note that families with YP diagnosed with specific difficulties, having additional complexities, or experiencing external variables such as deprivation are more vulnerable to non-mutually end treatment. Therefore, researchers, clinicians, families, YP, and decision-makers should continue to work together to develop tailored service level programmes and individual interventions to ensure underrepresented and underserved families are reached. For example, the finding that YP from non-White British ethnic groups are more likely to drop out of treatment highlights the importance of reaching these groups. This includes considering the referral routes and types of interventions offered, including consideration of community-based interventions, which may widen reach and increase retention for the identified groups.
One area that was not possible to investigate in the present study is the parent/carer perspective, given the significant role parents and carers have in YP retention in mental health settings (Weisz et al., 1987; Garcia and Weisz, 2002). Future research should explore this, as parent/carer views may differ from those of the clinician and the young person. It is also important to continue research into the use of digital interventions. With growing interest in this area, through web-based appointment systems and texting to mobile phones, we may be able to better capture reasons for treatment dropouts and facilitate non-face-to-face support for YP. Further qualitative and quantitative studies are also welcomed to explore YP's own descriptions of good outcomes and treatment ending to triangulate or further develop our current descriptions.
A major strength of this study is the inclusion of a large sample size. Moreover, we investigated the factors associated with case closure and YP's mental health using multilevel modeling, a method that was able to account for of individual and service-level variation. However, these results should be interpreted in the context of several limitations. The large majority of the participants were female and identified as White-British ethnicity thus preventing us from making predictions on the impact that cultural variations may have on the study's findings. Moreover, the specific problems presented by YP may have influenced the study outcome, but we were unable to account for this in the present investigation.
Another limitation of the study relates to the numerous ways that dropout can be defined, bringing challenges to the ability to compare results between studies (Barrett et al., 2008; de Haan et al., 2013). Reliability of the study's results is also affected by the absence of detailed information on professionals' reasons for case closure and the lack of qualitative data from YP or parents/carers in order to provide a deeper understanding of the current sample. In addition, the unavailability of follow-up data prevents drawing conclusions about the efficacy and effectiveness of the intervention – therefore on the extent to which clients' decision to discontinue the therapy due to perceived improvements or dissatisfaction is supported by trends in symptoms or clinical outcomes. Without a randomized controlled design, inferences about causation, of symptom improvement and reason for case closure, cannot be made. Another constraint identified was the reliance on routine pre-collected data, resulting in less flexibility to include explanatory variables of interest, such as the parent/carer perspective. Although this may compromise the rigorous empirical research standards and cause-effect relationships, this method has the benefit of allowing us to investigate variables without additional research participation burden to YP (Mansfield et al., 2020).
Symptom improvement continues to be an important indicator assess a good outcome that in turn determines treatment ending. The findings of the current study provide support for this approach indicating that YP with improvements are more likely to mutually agree to ending treatment. However, it is noted that symptom improvement should be evaluated alongside other aspects of the YP's life situation. Although further research is needed to fully conceptualize and understand non-mutually agreed endings (e.g., dropout), the current findings contribute to informing evidence-based practice.
The data analyzed in this study is subject to the following licenses/restrictions: Request for administrative data can be made available upon request from the corresponding author. Requests to access these datasets should be directed to anVsaWFuLmNoaWxkc0Bhbm5hZnJldWQub3Jn.
As this was a secondary analysis of anonymised data, ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants' legal guardian/next of kin was not required to participate in the present analysis in accordance with the national legislation and the institutional requirements.
JE-C and JJ conceived of the study. JE-C lead the data analysis and methods and results writing, to which TB, CS, and JJ contributed. CPM, GP, CS, and NF reviewed the literature and wrote the introduction. RU, AČ, and SL wrote the discussion. All authors contributed to the analysis decisions, reviewed and edited the manuscript, and approved the final version.
This publication was supported by TREATme, a European Network on Individualized Psychotherapy Treatment of Young People with Mental Health Disorders under the European Cooperation in Science and Technology (COST) which was supported by the EU Framework Programme Horizon 2020 action CA16102.
TB reports other funding from NHS England & NHS Improvement, outside the submitted work. JE-C reports grants from NHS England & NHS Improvement, outside the submitted work, and he was involved in the programme of service transformation that some of the data in the present manuscript draws on.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank all members present and former of the CORC committee including: Ashley Wyatt, Mick Atkinson, Kate Martin, Ann York, Duncan Law, Julie Elliot, Isobel Fleming, Beth Ingram - and present and former members of the CORC team (including. JJ, LCS, and JEC): Kate Dalzell, Benjamin Richie, Alison Ford, Sally Marriott, Lee Atkins, Martha Reilly, Nicholas Tait, Anja Teichert, Rory Lawless, Anisatu Rashid, ophie D'Souza, and Rebecca Lane. The authors would also like to thank Florence Ruby for helpful comments on an earlier draft of the manuscript.
YP, Young people.
Arnow, B. A., Blasey, C., Manber, R., Constantino, M. J., Markowitz, J. C., Klein, D. N., et al. (2007). Dropouts versus completers among chronically depressed outpatients. J. Affect. Disord. 97, 197–202. doi: 10.1016/j.jad.2006.06.017
Barrett, M. S., Chua, W. J., Crits-Christoph, P., Gibbons, M. B., and Thompson, D. (2008). Early withdrawal from mental health treatment: implications for psychotherapy practice. Psychotherapy 45, 247–267. doi: 10.1037/0033-3204.45.2.247
Bartholomew, T. T., Lockard, A. J., Folger, S. F., Low, B. E., Poet, A. D., Scofield, B. E., et al. (2019). Symptom reduction and termination: client change and therapist identified reasons for saying goodbye. Couns. Psychol. Q. 32, 81–99. doi: 10.1080/09515070.2017.1367272
Baruch, G., Gerber, A., and Fearon, P. (1998). Adolescents who drop out of psychotherapy at a community-based psychotherapy centre: a preliminary investigation of the characteristics of early drop-outs, late drop-outs and those who continue treatment. Br. J. Med. Psychol. 71, 233–245. doi: 10.1111/j.2044-8341.1998.tb00988.x
Bibi, F., Millar, H., and Holland, A. (2017). The role of cultural factors in engagement and change in multisystemic therapy (MST). J. Fam. Ther. 39, 243–263. doi: 10.1111/1467-6427.12134
Camilletti, E. (2018). Realizing an Enabling Environment for Adolescent Well-Being: An Inventory of Laws and Policies for Adolescents in South Asia. UNICEF Office of Research - Innocenti.
Carter, R. (1995). The Influence of Race and Racial Identity in Psychotherapy: Toward a Racially Inclusive Model. New Jersey, NJ: John Wiley and Sons.
Chasson, G. S., Vincent, J. P., and Harris, G. E. (2008). The use of symptom severity measured just before termination to predict child treatment dropout. J. Clin. Psychol. 64, 891–904. doi: 10.1002/jclp.20494
Clarkin, J. F., and Levy, K. N. (2004). “The influence of client variables on psychotherapy,” in Bergin and Garfield's Handbook of Psychotherapy and Behavior Change, 5th ed, ed M. J. Lambert (New York, NY: Wiley and Sons), 194–226.
Cohen, J. R., Andrews, A. R., Davis, M. M., and Rudolph, K. D. (2018). Anxiety and depression during childhood and adolescence: testing theoretical models of continuity and discontinuity. J. Abnorm. Child Psychol. 46, 1295–1308. doi: 10.1007/s10802-017-0370-x
Cunningham, P. B., Foster, S. L., and Henggeler, S. W. (2002). The elusive concept of cultural competence. Child. Serv. 5, 231–243. doi: 10.1207/S15326918CS0503_7
Das, J. K., Salam, R. A., Lassi, Z. S., Khan, M. N., Mahmood, W., Patel, V., et al. (2016). Interventions for adolescent mental health: an overview of systematic reviews. J. Adolesc. Health 59, 49–60. doi: 10.1016/j.jadohealth.2016.06.020
de Haan, A. M., Boon, A. E., de Jong, J. T. V. M., Hoeve, M., and Vermeiren, R. R. J. M. (2013). A meta-analytic review on treatment dropout in child and adolescent outpatient mental health care. Clin. Psychol. Rev. 33, 698–711. doi: 10.1016/j.cpr.2013.04.005
de Haan, A. M., Boon, A. E., de Jong, J. T. V. M., and Vermeiren, R. R. J. M. (2018). A review of mental health treatment dropout by ethnic minority youth. Transcult. Psychiatry 55, 3–30. doi: 10.1177/1363461517731702
de Haan, A. M., Boon, A. E., Vermeiren, R. R. J. M., Hoeve, M., and de Jong, J. T. V. M. (2014). Ethnic background, socioeconomic status, and problem severity as dropout risk factors in psychotherapy with youth. Child Youth Care Forum. 44, 1–16. doi: 10.1007/s10566-014-9266-x
Dossett, K. W., and Reid, G. J. (2019). Defining dropout from children's mental health services: a novel need-based definition. J. Child Fam. Stud. 29, 2028–2038. doi: 10.1007/s10826-019-01631-1
Edbrooke-Childs, J., Jacob, J., Argent, R., Patalay, P., Deighton, J., and Wolpert, M. (2015). The relationship between child- and parent-reported shared decision making and child-, parent-, and clinician-reported treatment outcome in routinely collected child mental health services data. Clin. Child Psychol. Psychiatry 21, 324–338. doi: 10.1177/1359104515591226
Edbrooke-Childs, J., and Patalay, P. (2019). Ethnic differences in referral routes to youth mental health services. J. Am. Acad. Child Adolesc. Psychiatry 58, 368–375.e1. doi: 10.1016/j.jaac.2018.07.906
Fairchild, G. (2019). Mind the gap: evidence that child mental health inequalities are increasing in the UK. Eur. Child Adolesc. Psychiatry 28, 1415–1416. doi: 10.1007/s00787-019-01418-1
Fonagy, P., Pugh, K., and O'Herlihy, A. (2017). The children and young people's improving access to psychological therapies (CYP IAPT) programme in England. Child Psychol. Psychiatry 429–35. doi: 10.1002/9781119170235.ch48
Garcia, J. A., and Weisz, J. R. (2002). When youth mental health care stops: therapeutic relationship problems and other reasons for ending youth outpatient treatment. J. Consult. Clin. Psychol. 70, 439–443. doi: 10.1037/0022-006X.70.2.439
Garfield, S. L. (1994). “Research on client variables in psychotherapy,” in Handbook of Psychotherapy and Behavior Change, eds A. E. Bergin and S. L. Garfield (New Jersey, NJ: John Wiley and Sons), 190–228.
Gopalan, G., Goldstein, L., Klingenstein, K., Carolyn Sicher Psy, D., Blake, C., and McKay, M. M. (2010). Engaging families into child mental health treatment: Updates and special considerations. J. Can. Acad. Child Adolesc. Psychiatry 19, 182–196.
Hannan, C., Lambert, M. J., Harmon, C., Nielsen, S. L., Smart, D. W., Shimokawa, K., et al. (2005). A lab test and algorithms for identifying clients at risk for treatment failure. J. Clin. Psychol. 61, 155–163. doi: 10.1002/jclp.20108
Hatchett, G. T., and Park, H. L. (2003). Comparison of four operational definitions of premature termination. Psychotherapy 40, 226–231. doi: 10.1037/0033-3204.40.3.226
Huey, S. J., and Polo, A. J. (2008). Evidence-based psychosocial treatments for ethnic minority youth. J. Clin. Child Adolesc. Psychol. 37, 262–301. doi: 10.1080/15374410701820174
Hynan, D. J. (1990). Client reasons and experiences in treatment that influence termination of psychotherapy. J. Clin. Psychol. 46, 891–895. doi: 10.1002/1097-4679(199011)46:6<891::AID-JCLP2270460631>3.0.CO;2-8
Jensen-Doss, A., and Weisz, J. R. (2008). Diagnostic agreement predicts treatment process and outcomes in youth mental health clinics. J. Consult. Clin. Psychol. 76, 711–722. doi: 10.1037/0022-006X.76.5.711
Jethwa, J., Glorney, E., Adhyaru, J., and Lawson, A. (2019). A grounded theory of multisystemic therapist roles in achieving positive outcomes for young people and families. J. Fam. Ther. 43, 1–19. doi: 10.1111/1467-6427.12287
Johnson, E., Mellor, D., and Brann, P. (2009). Factors associated with dropout and diagnosis in child and adolescent mental health services. Aust. N. Z. J. Psychiatry 43, 431–437. doi: 10.1080/00048670902817687
Kazdin, A. (1997). Practitioner review: psychosocial treatments for conduct disorder in children. J. Child Psychol. Psychiatry Allied Discip. 38, 161–178. doi: 10.1111/j.1469-7610.1997.tb01851.x
Kazdin, A., Mazurick, J., and Siegel, T. (1994). Treatment outcome among children with externalizing disorder who terminate prematurely versus those who complete psychotherapy. J. Am. Acad. Child Adolesc. Psychiatry 33, 549–557. doi: 10.1097/00004583-199405000-00013
Lambert, M., Harmon, C., Slade, K., Whipple, J., and Hawkins, E. (2005). Providing feedback to psychotherapists on their patients' progress: clinical results and practice suggestions. J. Clin. Psychol. 61, 165–174. doi: 10.1002/jclp.20113
Lau, A. S. (2006). Making the case for selective and directed cultural adaptations of evidence-based treatments: examples from parent training. Clin. Psychol. Sci. Pract. 13, 295–310. doi: 10.1111/j.1468-2850.2006.00042.x
Liverpool, S., Mota, C. P., Sales, C. M. D., Cuš, A., Carletto, S., Hancheva, C., et al. (2020). Engaging children and young people in digital mental health interventions: systematic review of modes of delivery, facilitators, and barriers. J. Med. Internet Res. 22:e16317. doi: 10.2196/16317
Mansfield, K. L., Gallacher, J. E., Mourby, M., and Fazel, M. (2020). Five models for child and adolescent data linkage in the UK: a review of existing and proposed methods. Evid. Based Ment. Health, 23, 39–44. doi: 10.1136/ebmental-2019-300140
McKenna, P. A., and Todd, D. M. (1997). Longitudinal utilization of mental health services: a timeline method, nine retrospective accounts, and a preliminary conceptualization. Psychother. Res. 7, 383–395. doi: 10.1080/10503309712331332093
Mental Health Taskforce to the NHS in England (2016). The Five Year Forward View for Mental Health. The Mental Health Taskforce. Available online at: https://www.england.nhs.uk/wp-content/uploads/2016/02/Mental-Health-Taskforce-FYFVfinal.pdf (accessed Febraury 1, 2021).
Miller, L. M., Southam-Gerow, M. A., and Allin, R. B. (2008). Who stays in treatment? Child and family predictors of youth client retention in a public mental health agency. Child Youth Care Forum 37, 153–170. doi: 10.1007/s10566-008-9058-2
NHS Digital (2019). Waiting Times for Children and Young People's Mental Health Services, 2018 - 2019 Additional Statistics. Available online at: https://digital.nhs.uk/data-and-information/find-data-and-publications/supplementary-information/2019-supplementary-information-files/waiting-times-for-children-and-young-peoples-mental-health-services-2018–2019-additional-statistics (accessed Febraury 1, 2021).
Office for National Statistics (2019). Office for National Statistics. UNEM01 SA: Unemployment by Age and Duration (Seasonally Adjusted).
O'Keeffe, S., Martin, P., Goodyer, I. M., Kelvin, R., Dubicka, B., Reynolds, S., et al. (2019a). Prognostic implications for adolescents with depression who drop out of psychological treatment during a randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 58, 983–992. doi: 10.1016/j.jaac.2018.11.019
O'Keeffe, S., Martin, P., Target, M., and Midgley, N. (2019b). “I just stopped going”: a mixed methods investigation into types of therapy dropout in adolescents with depression. Front. Psychol. 10:75. doi: 10.3389/fpsyg.2019.00075
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., and Rohde, L. A. (2015). Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry Allied Discip. 56, 345–365. doi: 10.1111/jcpp.12381
Sales, C. M. D. (2003). Understanding prior dropout in psychotherapy. Int. J. Psychol. Psychol. Ther. 3, 81–90.
Simon, G. E., Imel, Z. E., Ludman, E. J., and Steinfeld, B. J. (2012). Is dropout after a first psychotherapy visit always a bad outcome? Psychiatric Serv. 63, 705–707. doi: 10.1176/appi.ps.201100309
Swift, J. K., Callahan, J., and Levine, J. C. (2009). Using clinically significant change to identify premature termination. Psychotherapy 46, 328–335. doi: 10.1037/a0017003
Thormählen, B., Weinryb, R. M., Norén, K., Vinnars, B., Bågedahl-Strindlund, M., and Barber, J. P. (2003). Patient factors predicting dropout from supportive-expressive psychotherapy for patients with personality disorders. Psychother. Res. 13, 493–509. doi: 10.1093/ptr/kpg039
Todd, D. M., Deane, F. P., and Bragdon, R. A. (2003). Client and therapist reasons for termination: a conceptualization and preliminary validation. J. Clin. Psychol. 59, 133–147. doi: 10.1002/jclp.10123
Tripathy, J. P. (2013). Secondary data analysis: ethical issues and challenges. Iran. J. Public Health 42, 1478–1479.
Weisz, J. R., Weiss, B., and Langmeyer, D. B. (1987). Giving up on child psychotherapy: who drops out? J. Consult. Clin. Psychol. 55, 916–918. doi: 10.1037/0022-006X.55.6.916
Westmacott, R., Hunsley, J., Best, M., Rumstein-Mckean, O., and Schindler, D. (2010). Client and therapist views of contextual factors related to termination from psychotherapy: a comparison between unilateral and mutual terminators. Psychother. Res. 20, 423–435. doi: 10.1080/10503301003645796
Wierzbicki, M., and Pekarik, G. (1993). A meta-analysis of psychotherapy dropout. Prof. Psychol. Res. Pract. 24, 190–195. doi: 10.1037/0735-7028.24.2.190
Keywords: youth, mental health, outcome, case closure, dropout, meaningful change
Citation: Edbrooke-Childs J, Costa da Silva L, Čuš A, Liverpool S, Pinheiro Mota C, Pietrabissa G, Bardsley T, Sales CMD, Ulberg R, Jacob J and Ferreira N (2021) Young People Who Meaningfully Improve Are More Likely to Mutually Agree to End Treatment. Front. Psychol. 12:641770. doi: 10.3389/fpsyg.2021.641770
Received: 14 December 2020; Accepted: 08 March 2021;
Published: 06 April 2021.
Edited by:
Antonio Iudici, University of Padua, ItalyReviewed by:
Erping Long, National Institutes of Health (NIH), United StatesCopyright © 2021 Edbrooke-Childs, Costa da Silva, Čuš, Liverpool, Pinheiro Mota, Pietrabissa, Bardsley, Sales, Ulberg, Jacob and Ferreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julian Edbrooke-Childs, SnVsaWFuLkVkYnJvb2tlLUNoaWxkc0Bhbm5mcmV1ZC5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.