 Giulio Costantini
Giulio Costantini Marco Di Sarno
Marco Di Sarno Emanuele Preti
Emanuele Preti Juliette Richetin
Juliette Richetin Marco Perugini
Marco Perugini- 1Department of Psychology, University of Milan-Bicocca, Milan, Italy
- 2Personality Disorders Lab, Milan, Italy
This work investigates the relationship between goals and mitigation behaviors during the COVID-19 pandemic in Italy. Study 1 (pilot) identified goals ascribed to following and violating mitigation-related indications. Study 2 investigated the structure of and link between COVID-related goals and behaviors in a large community sample (N = 995, 301 men). Our results showed substantial relationships between goals and behaviors. Goals were best described by a bi-dimensional structure (being safe vs. being free), whereas behaviors clustered into a three-component structure (hygiene, distancing, going out). Hierarchical multiple regressions demonstrated the incremental validity of goals in the prediction of behaviors. Network analysis suggested that goals imbued with social content were more directly related to both risky and preventive behaviors. Motivational aspects emerged as important contributors to the organization of behaviors in the context of the COVID-19 pandemic.
Introduction
The world pandemic of the coronavirus disease 2019 (COVID-19) originated in China at the end of the year, caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). In early 2020, COVID-19 became an issue of public interest in Italy (Italian Ministry of Health [IMH], 2020). On February 21st, 20 days before the World Health Organization (WHO) confirmed the disease to be pandemic, Italy was the first European country to identify a local cluster of SARS-CoV-2. In the absence of effective pharmaceutical measures to contain the infection, the most effective mitigation strategies available were based on social distancing (Fong et al., 2020; Koo et al., 2020; Prem et al., 2020). Being confronted with a rapidly growing number of SARS-CoV-2 cases, Italy was the first European country to impose severe restrictions on the population in an attempt to reduce the increasing diffusion of the virus and the mounting pressure on the national health system (Remuzzi and Remuzzi, 2020). Such restrictions were first implemented in northern regions, the most severely hit by the virus, but were soon extended to the rest of the country. They included strict curfew measures, the lockdown of most commercial and public activities, quarantine for those infected, and limitations concerning public and private social contacts1. Such mitigation measures were enforced in Italy in their strictest version until the beginning of May, for approximately 2 months. These measures were called “Phase 1” lockdown, followed by a “Phase 2” in which restrictions were gradually reduced according to the virus diffusion.
From a psychological standpoint, individuals have shown a broad pattern of responses to the diffusion of the virus (e.g., Wang et al., 2020) and the restrictive measures imposed (e.g., Brooks et al., 2020). For example, the pandemic has had consequences for laypersons’ and healthcare professionals’ mental health (Duan and Gang, 2020; Preti et al., 2020a,b; Tan et al., 2020). Besides, given the importance of individual behaviors for the efficacy of mitigation measures, understanding psychological responses to this new and extreme situation has become of utmost importance.
Recent studies suggested relatively high levels of compliance with COVID-mitigation norms in the initial phases of the infection, including social distancing (e.g., social gathering avoidance, curfew) and hygienic practices (e.g., handshake avoidance) (Barari et al., 2020; Li et al., 2020; Van Bavel et al., 2020). However, compliance seemed to be generally higher among women, senior respondents, individuals reporting better physical health (Barari et al., 2020), those who identified more with their nation (Van Bavel et al., 2020), those perceiving the situation to be more controllable as well as more severe (Li et al., 2020), and those viewing realistic threats to their physical and financial safety (Kachanoff et al., 2020).
Individual behaviors, feelings, and cognitions are shaped by individual motives (Perugini and Conner, 2000; Kruglanski et al., 2002, 2015; Costantini et al., 2020). Goals are cognitive representations of outcomes we wish to approach or avoid (Elliot and Fryer, 2008) and represent a subset of motivational concepts with a relevant impact on our life. They thus serve a crucial regulatory function for our behaviors (Heller et al., 2009) both in the short- and long-term (Kruglanski and Szumowska, 2020).
In the health domain, research on goals provides insights into why people engage in health-compromising behaviors and fail or succeed in changing health-related behaviors (e.g., Sheeran et al., 2017). Previous research suggested that understanding health-related behaviors arguably requires a deep knowledge of individuals’ goals. People pursue multiple goals at the time, some of which are incompatible, and health-related behaviors result from the interplay of such goals and their relative importance (Gebhardt, 2006). For instance, it has been shown how healthy behaviors (e.g., physical activity, sexual behaviors) are influenced by several goals, not only related to being healthy and safe but also to social motivations (e.g., having active social lives) or self-presentation (e.g., being appreciated by others) (Gebhardt and Maes, 1998; Martin et al., 2001). Social distancing during COVID-19 pandemic has shown to correlate strongly with conventional health behaviors, suggesting that insights into general health behaviors can also be transferred to investigate mitigation behaviors (Bourassa et al., 2020).
During COVID-19 pandemic, the restrictions imposed arguably challenged the possibility for individuals to pursue personal goals. However, recent research shows that affirming a sense of autonomy, despite restrictions related to COVID-19, increases psychological well-being (Cantarero et al., 2020). Hence, knowledge of personal goals that people ascribe to behaviors related to COVID-19 might be crucial in shaping such behaviors (e.g., through media campaigns). However, little is known regarding the specific motivations that individuals ascribe to COVID-related behaviors and cognitions and how they shape their adherence to COVID-related norms.
The aim of this paper is twofold. First, we aim at identifying a comprehensive set of goals that individuals ascribe not only to adhering but also to violating norms related to COVID-19 mitigation. Second, we aim at investigating the relationship between the identified goals and specific mitigation-related behavioral outcomes. This would allow identifying a set of goals that could be leveraged, for instance, to develop interventions promoting adherence to norms related to COVID-19 and discouraging their violation (e.g., Freitas et al., 2004; Prestwich et al., 2010; Oettingen, 2012; Wieber and Gollwitzer, 2017). The work is articulated in two studies, both carried out in Italy between March and April 2020, during the “Phase-1” lockdown. Both studies received approval by the Ethical Committee in charge.
Study 1
Materials and Methods
Study 1 is a pilot study aiming at the identification of a comprehensive set of goals that individuals ascribed to enacting and violating COVID-mitigation norms, using qualitative responses collected during the “Phase-1” lockdown in Italy.
Participants
Seventy-seven participants (30 men, 38.9%) with a mean age of 40.1 years (SD = 18.1) took part in the study.
Materials and Procedure
Before the beginning of the study, participants provided online informed consent. Using Qualtrics2, participants read a set of 12 appropriate COVID-mitigation indications (e.g., “stay at home,” “wash hands frequently”), based on directions from the WHO and the Italian Ministry of Health (Italian Ministry of Health [IMH], 2020; e.g., World Health Organization [WHO], 2020a). Then, they were asked to generate 3 to 5 goals that they could pursue by respecting official recommendations and another set of 3 to 5 goals that they could pursue by violating such indications. Goals for respecting vs. violating norms were investigated separately, considering that goals for action and inaction are distinct and not necessarily opposite (Richetin et al., 2011). There were no pre-specified response options: participants wrote free-text goals in each of the two conditions. For the sake of clarity, participants were provided with a brief description of what a goal is (e.g., “something you try to obtain through behaviors”) and what it is not (e.g., “causes or explanations”), as well as with typical examples of goals and non-goals.
Since Study 1 was generative, we could not determine the sample size using power analysis. Our setup required to indicate between 6 and 10 responses (i.e., 3 to 5 for respecting and violating norms, respectively). Thus, seventy-seven participants ensured between 462 and 770 responses. Based on previous studies employing similar methods (Costantini and Perugini, 2018; Costantini et al., 2020), they were deemed enough to convey a sufficient amount of information regarding COVID-related goals.
Results
Participants generated 540 verbal responses (7.02 on average per participant). Of these, 283 were elicited by the respecting-norms question (i.e., goals related to following indications) and 257 by the violating-norm question (i.e., goals related to not following them). A series of steps were taken to summarize and aggregate the responses. A first analysis was performed to obtain an initial clustering of goals, which was further manually refined to get a final set of goals. Crucially, both steps were performed blind to whether each goal was ascribed to following vs. violating COVID-mitigation indications.
To perform an initial automatic classification, all responses were analyzed with software-based methods. Details of this procedure are presented in Supplementary Materials. An initial set of 80 clusters was identified after this step, including between 2 and 25 responses for each cluster.
We then needed to refine this initial set of clusters manually. Despite the instructions specifying what a goal was, some responses could not be clearly classified as goals (e.g., “I don’t know,” “I trust science”). Furthermore, some clusters included heterogeneous content and needed to be further split into different clusters (e.g., responses “avoid to become infected” and “avoid to infect my relatives” were both in the same cluster). Other clusters included content that overlapped and needed to be merged with one another (e.g., responses “avoid getting infected” and “avoid getting the virus” were in different clusters). Through consensual discussion among the authors, we identified and removed clusters that were regarded as non-goals, merged clusters that were similar in content, and separated clusters that included heterogeneous content. This led to the identification of 33 goal classes. We then reviewed all responses and classified each goal into one of those classes. Some classes referred mainly to consequences of behavior instead of goals (e.g., “getting sick,” “harm others,” “harm the economy”) and were excluded, thus leaving a final set of 22 classes. The final list of classes is presented in Table 1, with the total number of responses falling within each class, and the number of responses split by the original eliciting question (respecting vs. violating norms). Some classes mainly represented responses that had been elicited by the norm-respecting question (e.g., class “containment of the contagion” included 68 responses, all elicited by the norm-respecting question), whereas other classes mainly included responses elicited by the norm-violating question (e.g., class “pursue personal freedom” included 8 responses, 7 of which elicited by the norm-violating question). We tested whether these 22 classes were significantly associated with the eliciting condition, using a chi-square test for independence, with bootstrapped p-values. The chi-square tested the null hypothesis of independence between the type of eliciting question and the goal class (i.e., responses in each class were elicited with the same frequency by the two questions of respecting vs. violating norms). Results suggested rejecting the null hypothesis, indicating a significant association between goals and the eliciting condition, χ2(21) = 256.35, p < 0.001. In other words, goals ascribed to respecting COVID-mitigation indications generally fell into different classes compared to goals ascribed to violating such norms.
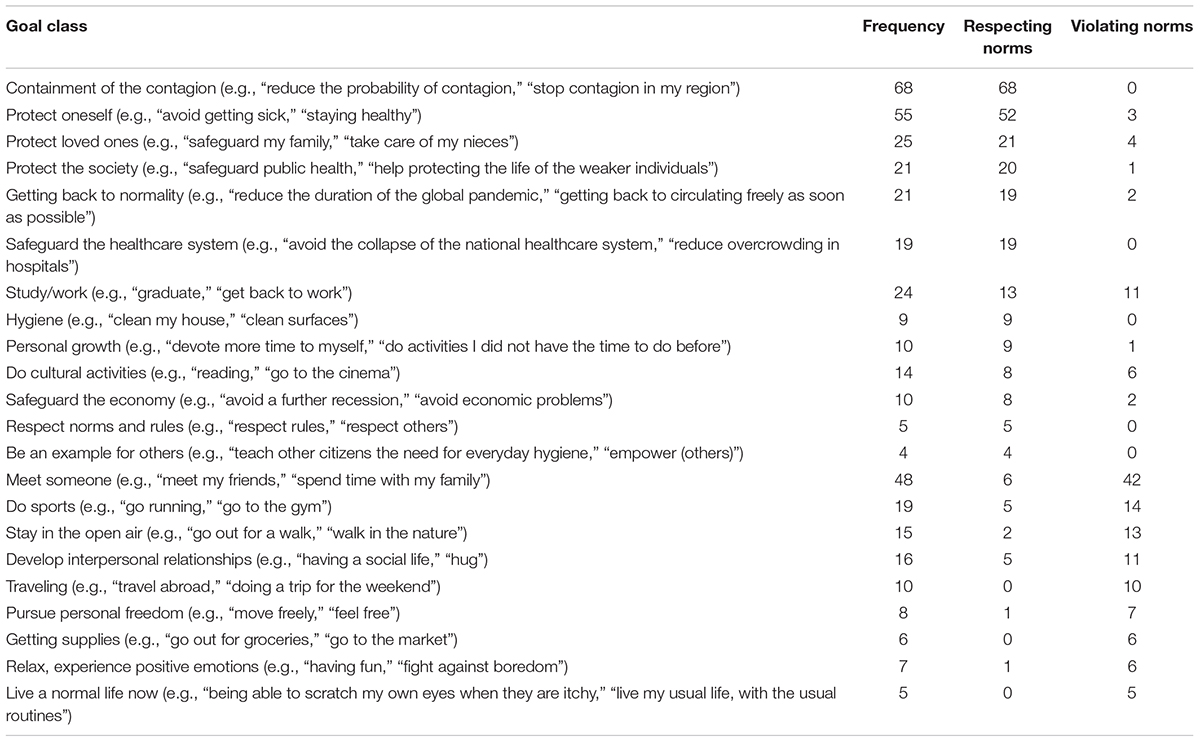
Table 1. Goal classes emerged in Study 1, their frequency, and the number of times they were ascribed to respecting and to violating COVID-mitigation indications.
Discussion
Study 1 allowed identifying a broad set of goals that individuals ascribe to respecting and to violating COVID-mitigation indications. We used the resulting categorization (i.e., the 22 classes of Table 1) to generate a questionnaire to assess goals related to COVID-19, the COVID-19 Goal Questionnaire. In particular, we generated 25 statements, each corresponding to an item of the Goal Questionnaire. The 25 statements were based on the original 22 goal classes, but were articulated and rearranged to emphasize competitions between motivations. In particular, items contrasted normality and restrictions (e.g., “Try not to change my life because of the epidemic”), immediate and long-term social gratifications (e.g., “Meet my friends immediately, even if this may involve risks”), health issues and renounces (e.g., “Contain the contagion, even if this may imply important sacrifices”), economic and health-related priorities (e.g., “Protect my economic situation, even at the cost of some risks for my health”), personal health and entertainment (e.g., “Stay safe, even if this means getting bored”), others’ and personal well-being (e.g., “Give more importance to my well-being than to the general well-being”), and respecting versus violating norms and rules (e.g., “Do something for the sake of breaking the rules”).
Study 2
The main aim of Study 2 was to investigate connections between goals and behaviors related to COVID-19. The preregistered hypothesis was a significant correlation between the leading principal components of COVID-related goals and behaviors relevant for COVID-19 mitigation, reflecting a general connection between goals and behaviors.
Several additional exploratory analyses were performed to further deepen the relationships among specific types of goals and behaviors. First, principal component analysis (PCA) was employed to summarize the main dimensions of variance of goals and of behaviors related to COVID-19 with a limited number of components (Comrey and Lee, 1992). Second, hierarchical regression was employed to assess the relative contribution of different goals in predicting behavior. Our main interest was in deepening the relationship between goals and behaviors. Still, we considered other variables relevant to COVID-19 to investigate goals’ incremental validity. Demographic variables are known to be related to mitigation behaviors and adhesion to norms (e.g., Barari et al., 2020). This also seems to depend on the fact that individuals have different vulnerabilities to COVID-19 according to their age and gender, with the elderly and males being more vulnerable (Aschwanden et al., 2020; Jin et al., 2020). Furthermore, since at the time of the study, the SARS-CoV-2 was unevenly spread throughout Italy, we considered the potential effect of respondents’ current location by splitting Italian regions into low-risk (southern regions, with a lower prevalence of cases), medium risk (Piedmont, Veneto, and Emilia-Romagna), and high-risk (Lombardy). A detailed distribution of our sample by location/region is in Supplementary Table 1. We also reasoned that individuals might have different levels of concern and knowledge about COVID-19: Correct information is a necessary (though not sufficient) element to promote healthy behaviors (Tan et al., 2015; Wu and Shen, 2021). Furthermore, whereas some individuals might have been directly affected by COVID-19, others might have only had an indirect experience of the virus. Health behavior is shaped by fear of negative consequences (e.g., Rogers, 1975, 1983). All these elements might result in different behaviors, irrespective of personal goals. We thus inspected whether goals would provide additional information about behaviors related to COVID-19, even after controlling for age, gender, location, education, knowledge, concerns, and personal impact of COVID-19.
The aforementioned analyses focused on the pattern of relationships among principal components of behaviors and goals. We thus employed psychometric network analysis (Epskamp et al., 2018c; Costantini et al., 2019) to further investigate the pattern of relationships involving specific goals and behaviors, beyond what could be captured by broader components.
Materials and Methods
Participants and Procedure
This study is part of a project on personality, motivation, and COVID-related behaviors in which we collected data from two samples of participants. Both samples completed a common set of measures: for the purpose of this paper, only those data were analyzed. The two data collections can be found in two independent preregistrations3. However, both studies were preregistered with the same hypothesis, a correlation between the first principal components of goals and of behaviors, which is the focus of this work. Data were collected between April 17th and 30th, 2020.
One thousand six hundred seventy-five participants began the online survey using Qualtrics, lasting around 40 min. Inclusion criteria were being in Italy at the time of the questionnaire completion and being above 18 years old. An item to detect careless responding was included in the questionnaire to filter out participants (Self-Reported Single-Item “Use-Me” indicator), as recommended by Meade and Craig (2012). Six hundred and eighty participants were excluded from the analyses, either because they indicated careless responding to the “Use-Me” indictor (N = 40), or because they quit the questionnaire before completing the indicator (N = 640). The final sample was N = 995, 301 men, 688 women, two who self-identified as transsexual, and four who self-identified as “other.” The age range was 18–79, Mage = 32.88, SD = 13.05. There were no missing values4.
In our preregistration, we planned for a sample size of at least N = 300, which would allow detecting a correlation as small as r = 0.14 with a power of 0.80 at the conventional alpha level of 0.05 in a one-tailed test. However, we did not define an a priori stopping rule, aiming for a sample size as large as possible before running analyses. The final sample of N = 995 allows detecting a correlation as small as r = 0.08 under the same conditions.
Measures
Before the beginning of the study, participants provided online informed consent. All participants completed the following measures, in the following order:
Demographic Information Questionnaire included gender, age, education, location, and occupation (student status). Participants also provided information regarding their personal experience with COVID-19 (see Table 2).
COVID-19 Knowledge Questionnaire. Participants completed ten questions investigating their knowledge of COVID-19 (e.g., “COVID-19 always causes symptoms”) with a three-option response format (true/false/I don’t know), and only one option being correct. Correct knowledge was determined based on what was considered to be correct by WHO and the Italian Ministry of Health at that point in time. Correct answers were coded as 1, and a sum score was computed, with higher scores indicating sounder knowledge.
COVID-19 Goal Questionnaire. Participants rated the personal importance of 25 goals related to COVID-19, using a five-point scale ranging from 1 (not at all important) to 5 (extremely important). This scale was derived from Study 1 (see paragraph 2.3).
COVID-19 Behaviors Questionnaire. Participants indicated the frequency with which they enacted each of 18 behaviors on a scale from 1 (Never or almost never) to 5 (Always or almost always). The scale was adapted from the directions of the WHO and the Italian Ministry of Health. Some behaviors corresponded to rules/laws emitted during the lockdown (e.g., “Avoid gatherings”). Some were recommendations with a more personal value (e.g., “wash hands frequently”), and some represented subtle transgressions of the rules (e.g., “Leave home very often to do sports outdoor”).
COVID-19 Concern Questionnaire (Conway et al., 2020). The scale is a six-item measure assessing concern for the coronavirus disease (e.g., “Thinking about the coronavirus (COVID-19) makes me feel threatened”) with a five-point scale ranging from 1 (completely false for me) to 5 (completely true for me). This and the following scale were translated into Italian through back-translation. Cronbach’s alpha for the scale was 0.86 in our sample.
COVID-19 Impacts Questionnaire (Conway et al., 2020). The measure is a nine-item questionnaire assessing the financial and psychological impact of the coronavirus disease and the difficulty in obtaining necessary resources during the lockdown. Participants used a five-point Likert scale ranging from 1 (completely false for me) to 5 (completely true for me). Cronbach’s alphas in our sample were 0.77 (resource scale), 0.80 (psychological scale), and 0.92 (financial scale).
Data Analyses
All analyses were performed using R (R Core Team [RCT], 2020). We used the packages psych (Revelle, 2019) and GPArotation (Bernaards and Jennrich, 2005) to perform PCA on both goals and behaviors. The preregistered hypothesis of a general relationship between goals and behaviors was tested by extracting the first principal component from each questionnaire separately and by inspecting the correlation between these two component scores. The structure of the COVID-19 Goal Questionnaire was then further examined using PCA. Criteria for selecting the number of components included eigenvalues higher than 1, exploration of the scree-plot, and parallel analysis (Horn, 1965; Comrey and Lee, 1992; Hayton et al., 2004). The extracted components were then rotated using oblimin, and component scores were saved to use in subsequent analyses. A similar analysis was performed for exploring the structure of the COVID-19 Behaviors Questionnaire. We then examined the correlations among specific components of goals and behaviors.
Hierarchical multiple regression models were carried out to investigate the incremental effects of goals in predicting behaviors (component scores). In the first step, demographic variables were included as predictors (gender, age, education, location); in the second step, COVID-19 knowledge, impacts, and concern scales were added to the models; in the third and last step, goal classes were also included.
The relationship among specific behaviors and goals was explored using network analysis in the form of a Gaussian Graphical Model (Costantini et al., 2015, 2019; Epskamp et al., 2018c). We estimated the network using the graphical lasso algorithm, based on polychoric correlations, as implemented in the R package qgraph (Epskamp et al., 2012, 2018b). The lasso regularization parameter was selected through the Extended Bayesian Information Criterion (Chen and Chen, 2008; Foygel and Drton, 2010), with the hyperparameter gamma set to the default value of 0.50 (Epskamp and Fried, 2018). We examined the centrality of each node (Freeman, 1978). Since our interest was mainly into connections between goals and behaviors, as opposed to connections among goals and behaviors separately, we focused on bridge strength centrality, which quantifies the amount of connectivity of a node with nodes of another group of nodes (Jones et al., 2019), using the networktools package (Jones, 2020). To control the replicability of our results, we also computed the bootstrap-based correlation stability coefficient (CS-coefficient) of bridge centrality using package bootnet (Epskamp et al., 2018a). The CS-coefficient corresponds to the maximum proportion of cases that could be dropped, such that the correlation between the original bridge strength and the one computed in the reduced sample would still be larger than r = 0.70 with 95% probability. Values of the CS-coefficient larger than 0.25 indicate sufficient stability, whereas values of 0.50 or larger are preferable.
Results
Descriptive Statistics
Around one-third of our participants were students (N = 364, 36%), and only 36 of them attended high school. Around 53% of the sample (N = 525) had a university level of education or above, whereas 41% of our participants (N = 407) had achieved a high-school diploma, 6% a secondary school (N = 59), and four participants had a primary-school level of education (< 1%). Many participants (N = 549, 55%) declared to know at least one person (e.g., nurse, doctor) employed in the National Health System against COVID-19.
Table 2 presents means and standard deviations for scales of concern and impacts, COVID-19 knowledge, and COVID-related symptoms and tests. Participants had a good knowledge of the disease on average, and only a handful had been diagnosed with the disease (N = 5).
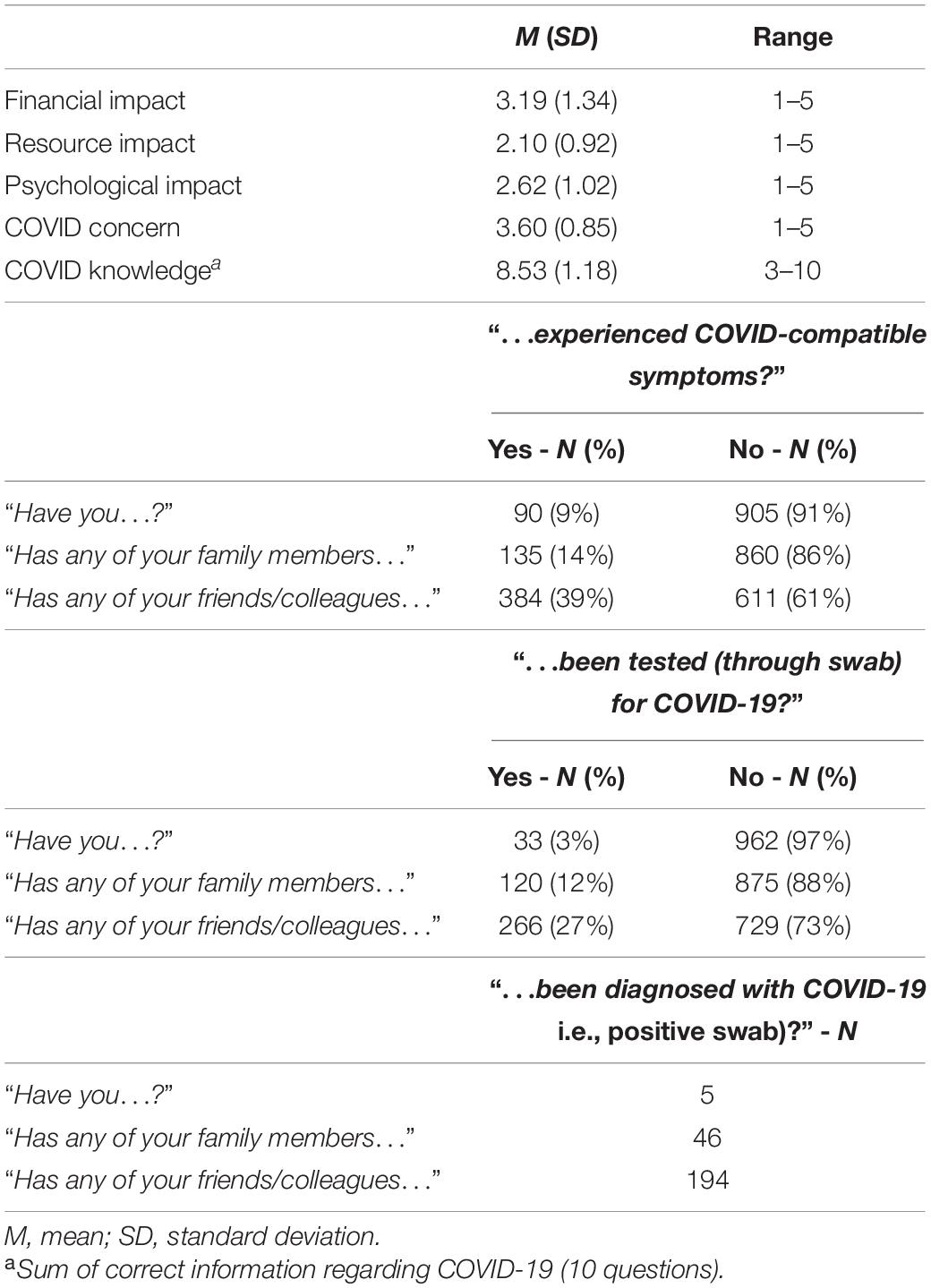
Table 2. COVID-related sample characteristics.
Behaviors and Goals
Following the preregistered hypothesis plan, we extracted the first principal component from goals and behaviors separately and retained all items with loadings < | 0.30| (only two behaviors were discarded). The goal component, explaining 33% of variance, had positive loadings by goals connected to pursuing personal freedom despite risks connected to COVID-19 and negative loadings by goals connected to pursuing security despite personal freedom (for details, see Supplementary Table 2). The behavioral component (21% of variance) had positive loadings by behaviors connected to social distancing and hygiene and negative loadings by behaviors connected to leaving the house (see Supplementary Table 3). The correlation between the two was r = −0.41, p < 0.001 (similar analyses considering the two preregistered subsamples separately yielded nearly identical results, rs = −0.38 and −0.43, ps < 0.001), indicating as hypothesized a substantial general connection between goals and behaviors.
To further explore the relationships among goals and behaviors, respectively, we examined in detail the structure of each questionnaire. Parallel analysis and scree-test suggested a two-component solution for the COVID-19 Goals Questionnaire. The two components explained 40% of the cumulative variance and were correlated −0.50, corroborating the use of an oblique rotation procedure. Table 3 presents loadings for the two-component solution: The two latent factors were named “safe” (G1) and “free” (G2), the first one reflecting goals to protect oneself and others from the virus, and the second representing goals to be free from restrictions. Two items, #9 and #19, showed somewhat smaller loadings and were both related to preserving the economy.

Table 3. PCA loadings for the COVID-19 goal questionnaire.
As to behaviors, parallel analysis and scree-test suggested a three-component solution for the measure, explaining 43% of the cumulative variance. Components were correlated between −0.04 to −0.22 (details in Table 4). Loadings are presented in Table 5. We named the three components “hygiene” (B1), “social distancing” (B2), and “going out” (B3), respectively. The first reflected hygiene-focused behaviors, such as washing hands. The second included items assessing the tendency to keep safety distance in social relationships. The third component comprised norm-incongruent behaviors, specifically related to going out and/or meeting people.
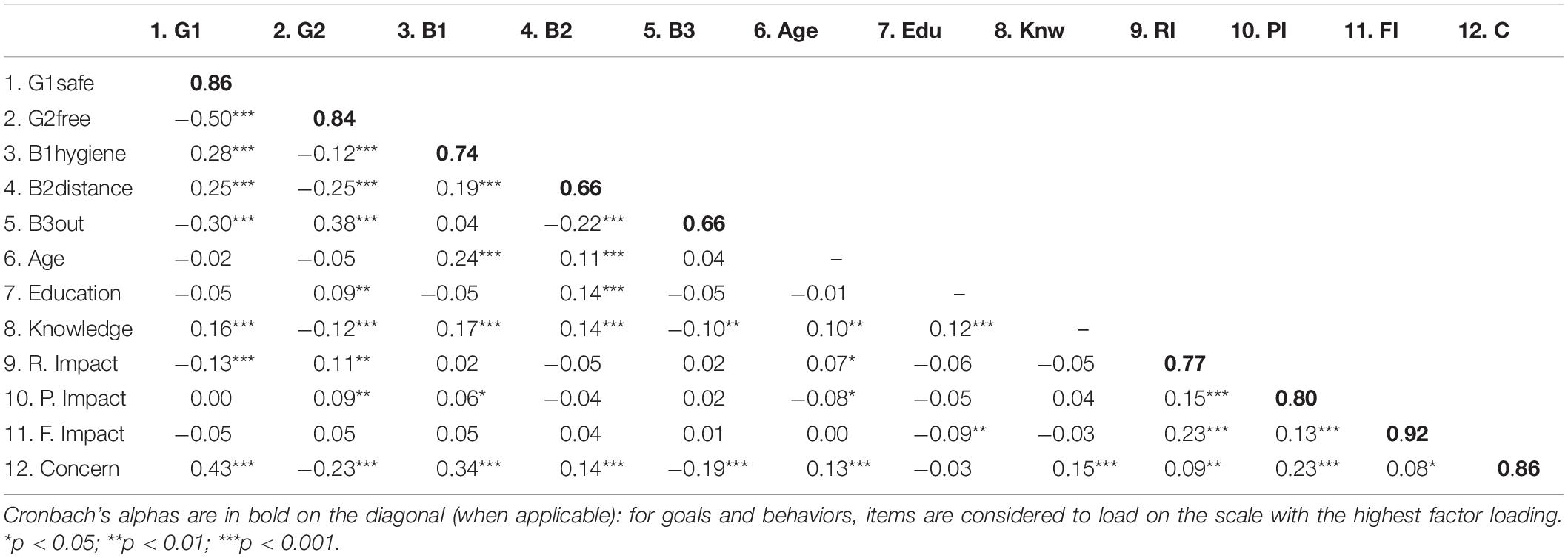
Table 4. Pearson correlations among latent scores, Conway scales, COVID knowledge, age, and education.
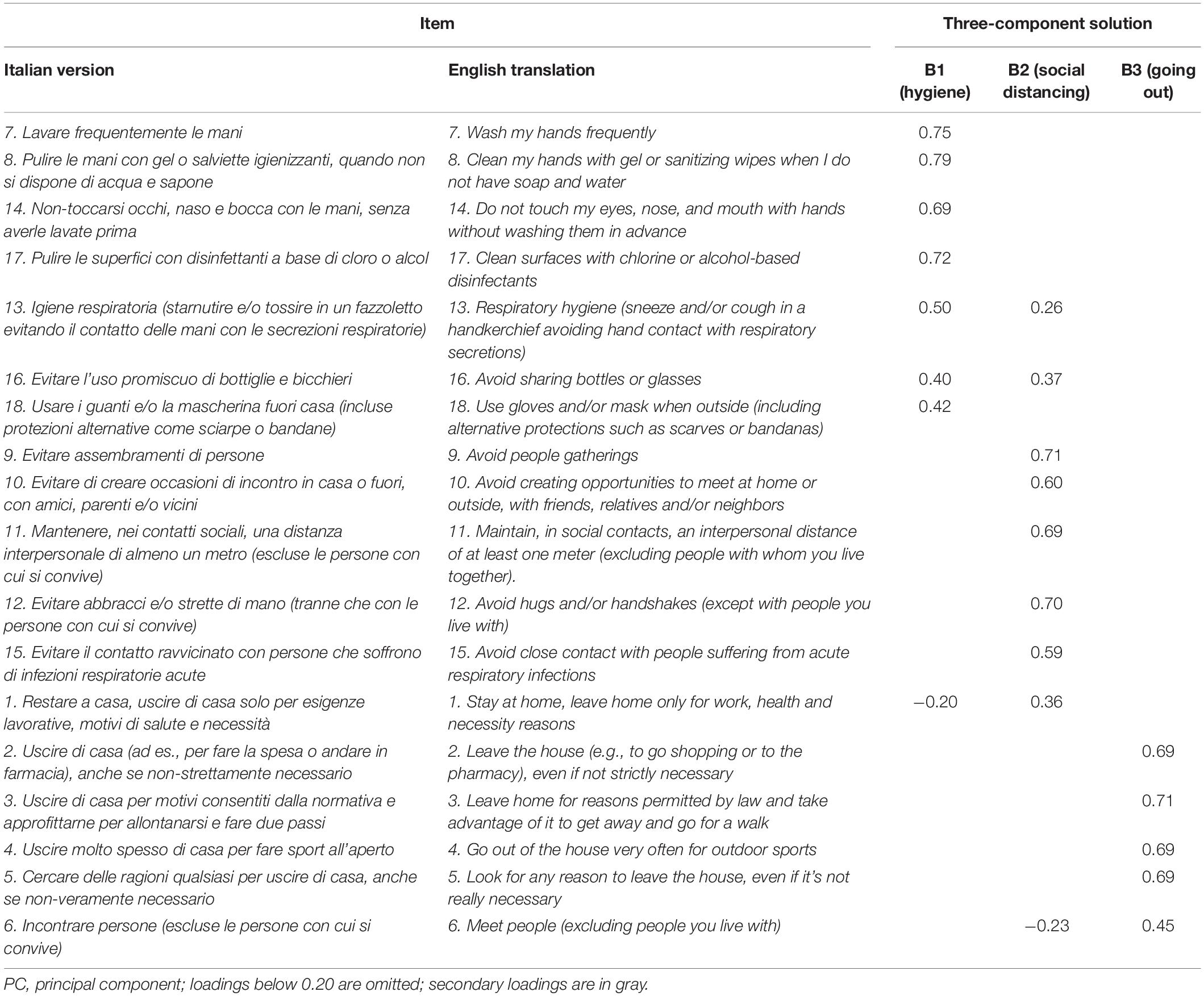
Table 5. PCA loadings for the COVID-19 behaviors questionnaire.
Table 6 presents descriptive statistics of goals and behaviors and differences by gender (men vs. women) and by location. Women scored higher on G1 “safe” and lower on G2 “free.” As for behaviors, women were higher on focused hygiene (B1) and lower on going-out behaviors (B3) on average. There was no gender difference in social distancing (B2). ANOVAs indicated there were significant differences in G1 “safe” based on the location of participants, with higher scores in low-risk regions, followed by Lombardy and medium/high-risk regions. At the same time, Lombardy had the lowest score on the “going out” scale.
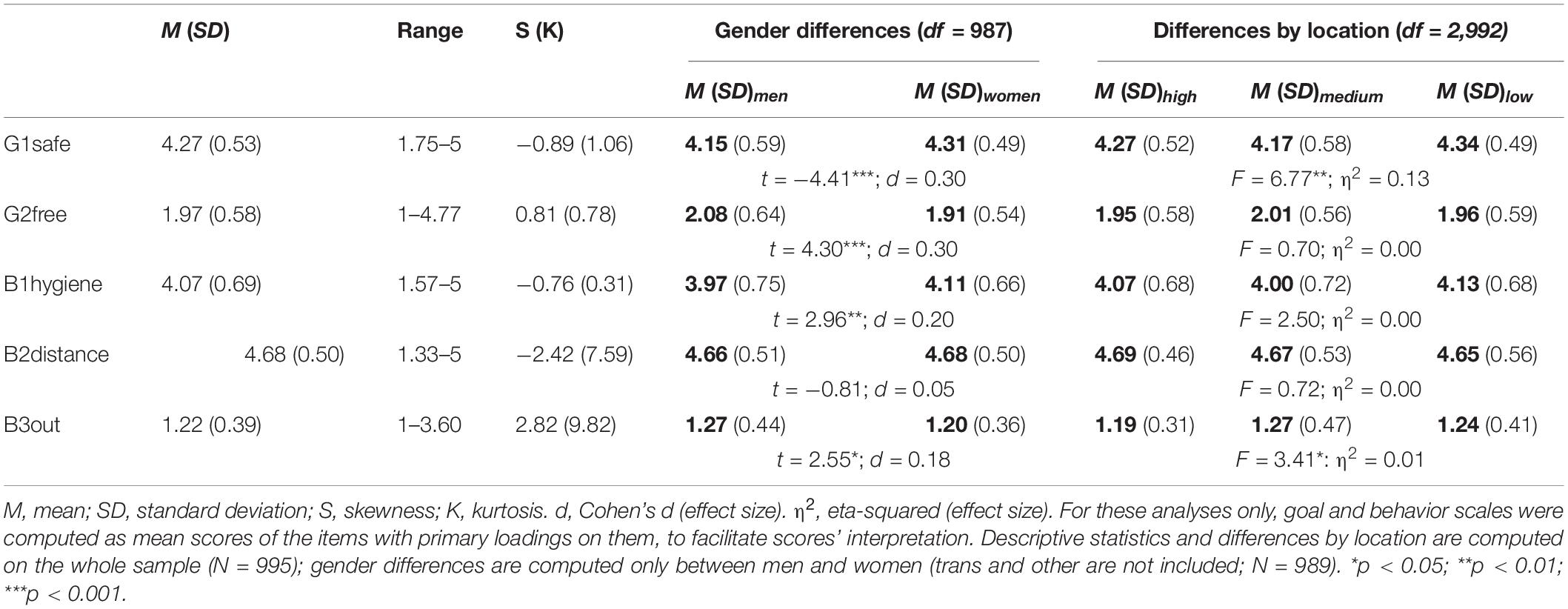
Table 6. Descriptive statistics of goals and behaviors.
Table 4 presents Pearson correlations among specific classes of goals and behaviors and knowledge, concern, and impact related to COVID-19. Given deviations from normality, Spearman rank-order correlations were also computed, with negligible differences (results are available upon request from the corresponding author). G1 “safe” correlated positively with B1 “hygiene” and B2 “distance,” but negatively with B3 “going out.” Goals to be free (G2), on the contrary, were positively correlated with B3 “going out,” and negatively with the other two composite behaviors (especially B2 “distance”). Behaviors were also significantly correlated with COVID-19 concern, and to a lower extent, with knowledge, age, and education. Correlations between behaviors and impact scales were trivial in magnitude.
Incremental Effect of Goals and Behaviors
Results from hierarchical multiple regressions predicting the three behavior classes identified through PCA are presented in Table 7. Goals always explained a significant portion of variance above and beyond demographic variables, knowledge, impacts, and concern for COVID. Both goal classes were uniquely related to each of the three behavioral components in expected directions, with the only exception of goal class “free” that did not significantly predict hygiene (B1). COVID-19 knowledge remained positively associated with hygiene (B1) and social distancing (B2) after accounting for goals, but its association with “going out” (B3) became non-significant in the last step. After accounting for goals, concern for COVID-19 still reduced the tendency to go out (B3) and increased the enactment of focused hygiene (B1). On the contrary, its unique effect on social distancing (B2) became non-significant. Being in higher-risk regions only predicted reduced going out (B3) across regressions. Finally, age remained positively associated with all three behavior classes after accounting for goals. Older participants were more likely to enact hygienic practices (B1) and keep social distance (B2), but also to go out (B3).
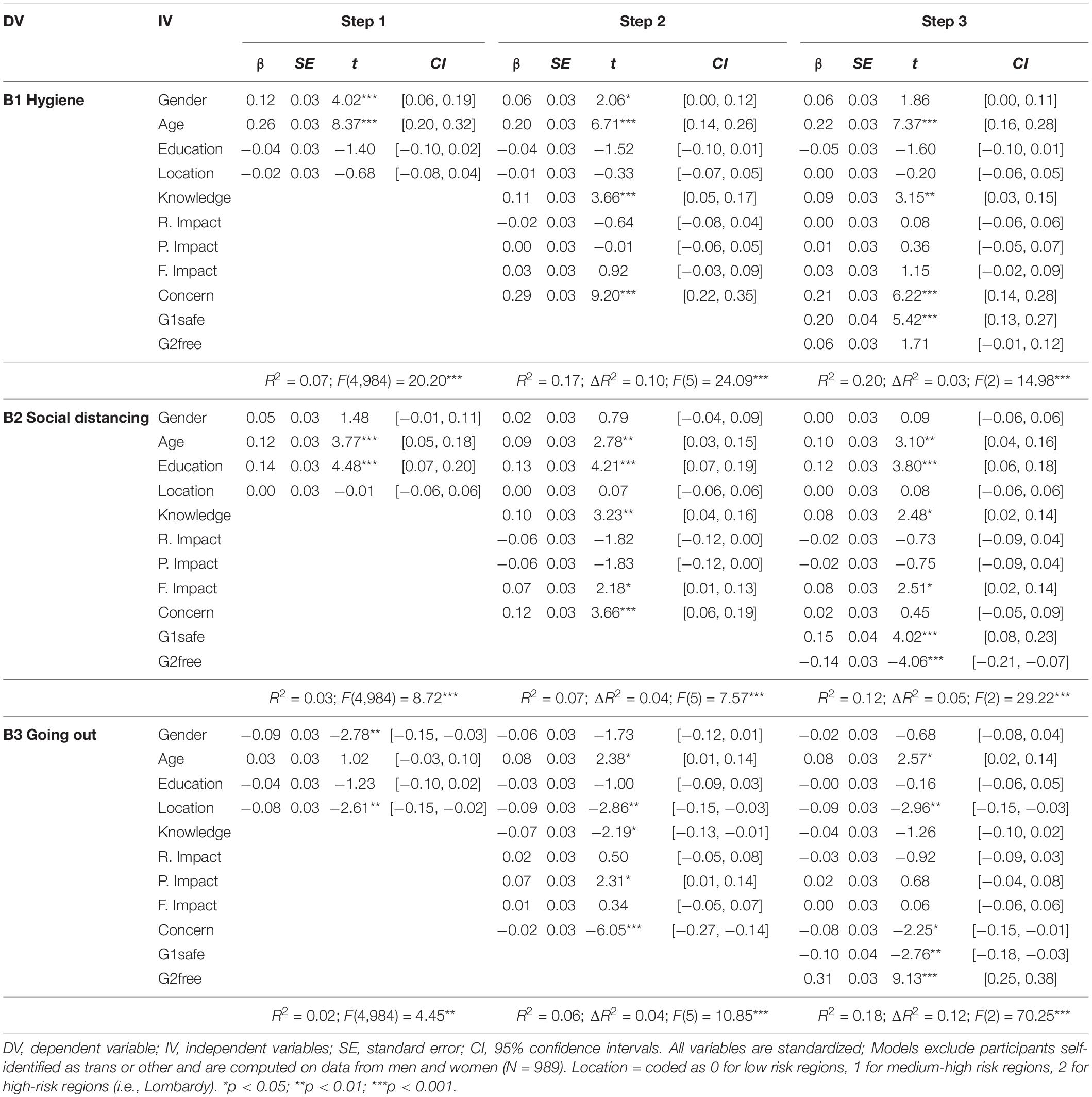
Table 7. Predicting behaviors: Incremental effects of goals.
Network Analyses of Goals and Behaviors
We further explored connections among goals and behaviors more specifically (i.e., at the item level) using network analysis. In the resulting network (Figure 1), nodes were divided into two main clusters, one including goals and the other one behaviors. Furthermore, nodes grouped according to the component structure previously identified. The CS-coefficient for bridge Strength was 0.45, thus indicating more than sufficient stability. There were several connections among nodes of the two clusters. However, not all goals entertained similarly strong connections with behaviors (Figure 2). Some goals (#4, #6, #9, #10, #23) were not directly connected to any behavior. Interestingly, two goals showed much larger connections with behaviors than all other nodes, namely goal #12 (“Do something for the sake of breaking the rules”) and goal #24 (“Set a good example to others”).
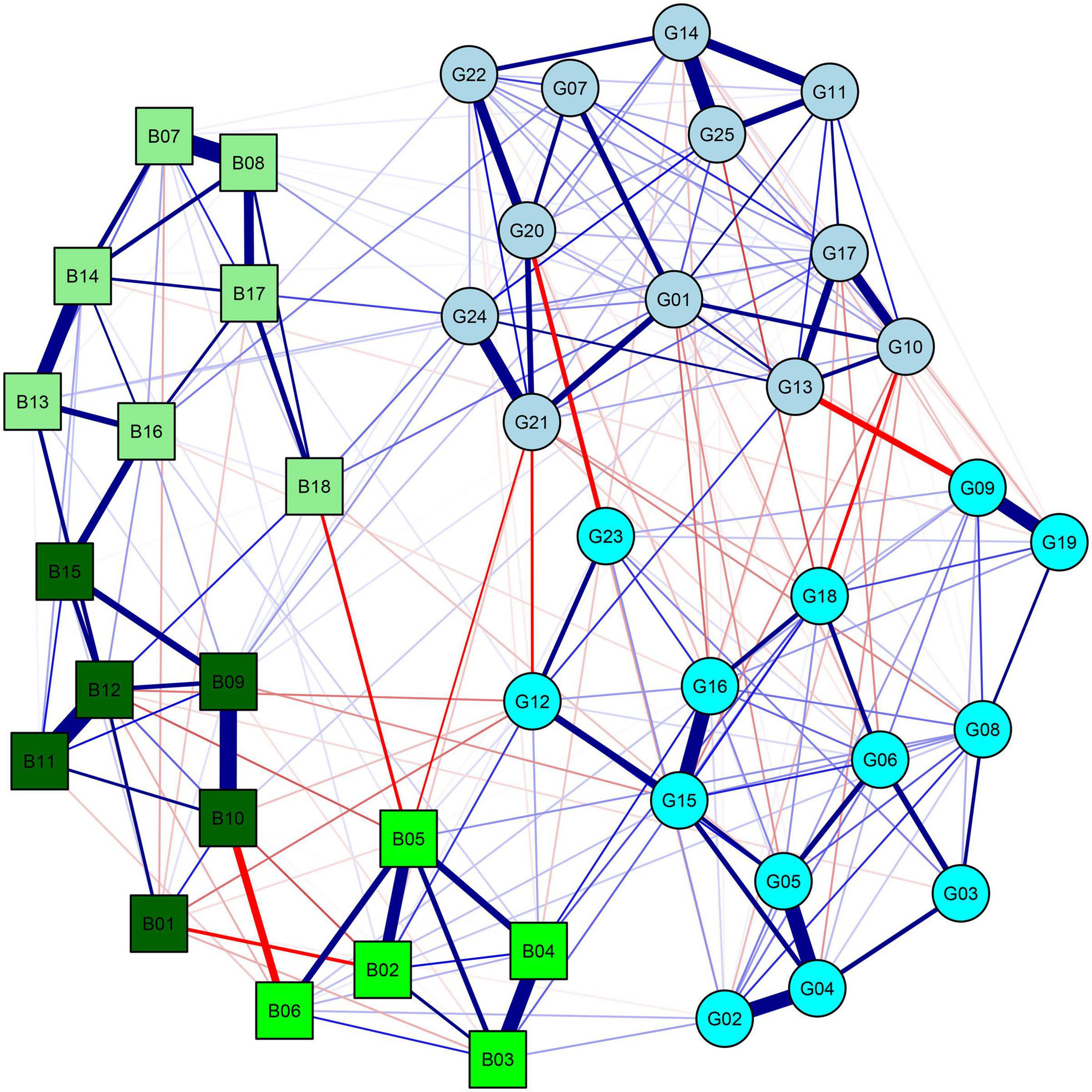
Figure 1. Network of goals and behaviors. Blue and red lines correspond to positive and negative relationships, respectively. Circles correspond to goals, and squared correspond to behaviors. A color was assigned to each behavior and goal according to its highest loadings in the PCA. See Tables 3, 5 for specific goals and behaviors and details about the PCA.
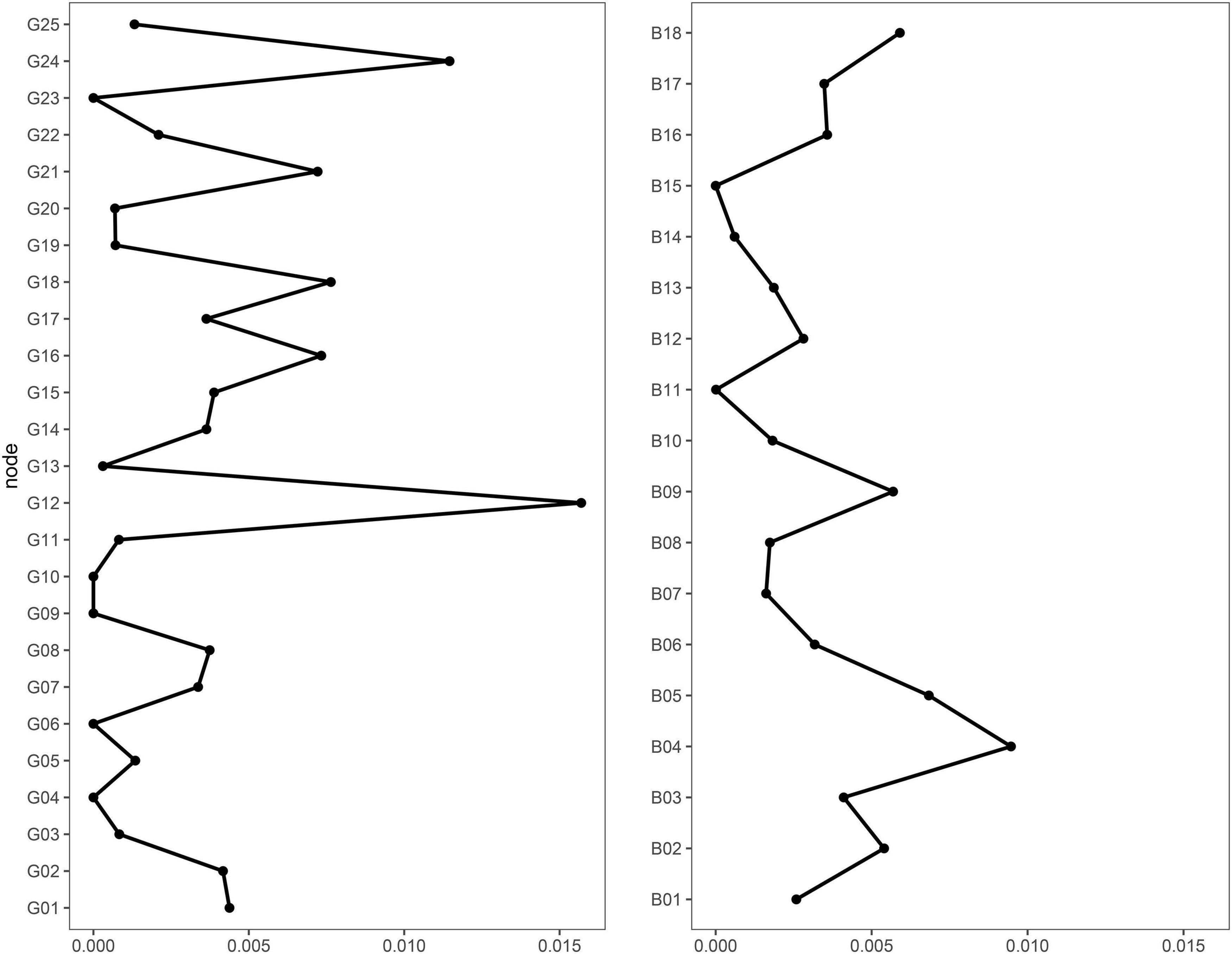
Figure 2. Bridge strength centrality (on the x axis) of goals and behaviors. See Tables 3, 5 for specific goals and behaviors and their corresponding number.
Goal #12 showed the strongest positive connections to behaviors #2 and #4, which were both related to leaving home in a period in which this was not allowed, and the strongest negative connections to behaviors #1 and #12, which were related to staying at home and avoiding personal contact. This result indicates that the motivation of simply breaking the rules might exert a unique influence on behaviors related to COVID-19. Goal #24 showed the strongest positive connections to behaviors #8, #17, and #18, which were related to COVID-mitigation actions (respectively, cleaning hands, cleaning surfaces, and using masks and gloves). In contrast, it did not show any negative connection with behaviors. This pattern suggests that the desire to be an example to others might directly motivate protective behaviors.
Discussion
The main aim of Study 2 was to investigate the connection between goals identified in Study 1 and COVID-mitigation behaviors. Results supported the hypothesis of a significant relationship between goals and behaviors in general. Still, further exploration of the structure of goals and behaviors and their connections provided the most interesting insights. Principal component analyses of goals revealed that they conformed to a bi-dimensional structure. The first component represented a general tendency to prioritize safety above other instances (e.g., fun, freedom, immediate well-being, financial issues, need to see beloved people). The second component included goals related to the prioritization of those instances over risk-safeguarding. This latter component also included somewhat antagonistic goals (e.g., breaking the rules, giving more importance to one’s well-being), as opposed to rather rule-abiding goals in the first component. COVID-mitigation behaviors, based on institutional prescriptions, were organized in a three-factor solution, including focused hygiene, social distancing, and risky behaviors (going out more than necessary). This structure is quite similar to other more intuitive classifications of COVID-related behaviors (Carvalho et al., 2020) and empirically driven measures of the same kind (Blagov, 2020).
Goals toward safety were positively connected to hygiene and social distancing practices and to a lower tendency to go out. On the contrary, goals to be free predicted an opposite pattern of behaviors. Multiple regression analyses showed that goals represented important predictors of behaviors, with significant unique effects above and beyond other demographic and psychological variables. This finding corroborates the idea that psychological aspects in general, and motivations in particular, are crucial elements in predicting behaviors related to COVID-19. Goals shape behaviors even more than other variables such as concern for and knowledge of the disease.
Network analysis further allowed to deepen connections between specific types of goals and behaviors. Our results showed that two goals had more direct connections with behaviors. Interestingly, these goals were somehow infused with social content. If goal #12 (breaking rules) may be seen as a reaction to the stringent and deeply unusual rules of the lockdown period, goal #24 (setting a good example) may be ascribed to a sense of social responsibility and collective interest. Behaviors directly related to goal #12 were openly rule-breaking. In contrast, all behaviors directly related to goal #24 described personal hygiene practices, with some particularly visible to others (e.g., wearing masks; goal #24 was not connected to COVID-mitigation behaviors of self-isolation and distancing, unlikely to be observable). In this sense, results suggest that social rewards might be important in shaping COVID-related behaviors, as much as other behaviors (Tamir and Hughes, 2018). This might be even more accentuated by the constant availability of reinforces in social networking websites (Rosenthal-von der Pütten et al., 2019). Crucially, our data suggest that individuals might actively seek social reinforcements by respecting the rules and thus being a good example to others or by intentionally violating them.
This study had some limitations that should be acknowledged. Albeit large, our sample was not fully representative of the Italian population. For instance, the sample included more females than males, and since the study was administered online, students and young adults were overrepresented (probably because they could access connected devices more easily). This might have introduced biases in the parameter estimates (Bethlehem, 2010). Another limitation is that behaviors were assessed through self-reports, which can be influenced by participants’ self-concept and social desirability. It could be interesting to investigate whether the emerged relationships generalize to observed behavior, as well as to critical outcomes connected to such behavior (e.g., being infected by COVID-19).
General Discussion
Throughout two studies, we identified a set of basic motivations that individuals ascribe to respecting and violating COVID-19 mitigation norms. Moreover, we established connections between specific types of goals and behaviors relevant to COVID-19 mitigation. Our results showed that the identified goals predicted relevant behaviors above and beyond demographic variables, knowledge, impact, and concerns related to COVID-19.
The bi-dimensional structure of goals that emerged flattened more specific differences in goals (e.g., protecting self versus others), emphasizing more macroscopic aspects of safety versus freedom, which emerge as the main organizers of motivational aspects related to COVID mitigation. This probably mirrors the salience of COVID-19 pandemic and the lockdown for most laypersons. The specific unique situation probably made certain contrasts between goals particularly salient, confronting people with the issue of attributing priority either to safety or to other instances. In a way, the dimensional goal structure that emerged in the present study also recalls previous theoretical accounts on motivations in health behaviors. It has been suggested that goals “compete” for relevance (Gebhardt, 2006), behaviors being the result of the relative salience and importance of individual goals (both related and unrelated to health). The importance of self-protection goals ultimately impacts people’s health choices (Floyd et al., 2000; Milne et al., 2000). We may consider the bi-dimensional structure of COVID-related goals as a reflection of this conflict, where goals to be safe represent the primary motivation toward protection. In this sense, our network analysis approach is informative and offers fine-grained insights into the role of these competing motivations and their relative importance for health behaviors. In fact, despite bi-dimensionally organized at the higher-order level, results reveal that individual goals with a more pronounced social content may have more direct connections with behaviors, promoting adhesion to norms (setting good examples) or facilitating transgressions (breaking the rules).
Researchers agree that for encouraging appropriate behaviors related to COVID-19, as for many other health-related behaviors, informing individuals regarding what they should and should not do is not enough (Bavel et al., 2020; National Academies of Sciences, Engineering, and Medicine [NASEM], 2020). This seems to be particularly true if the recommended behaviors are in conflict with one’s ideology (Calvillo et al., 2020) or the fulfillment of one’s needs (Cantarero et al., 2020). Furthermore, as acknowledged by the WHO (World Health Organization [WHO]., 2020b), the more the pandemic becomes part of a “new normality,” the more mitigation measures become a matter of personal responsibility, rather than just something that can be simply enforced by law. We argue that individual motives will gain even greater relevance in shaping behaviors during the post-lockdown phase when institutional curfew measures are not implemented.
Knowledge of individuals’ motivations is now more crucial than ever for designing effective interventions (Wieber and Gollwitzer, 2017; Oettingen and Gollwitzer, 2018), media campaigns (National Academies of Sciences, Engineering, and Medicine [NASEM], 2020), and for the prediction of people’s behaviors related to COVID-19. Our findings suggest that motivations toward safety and freedom are potential targets for health-promotion interventions related to COVID-19. More generally, interventions promoting adherence to norms in situations of collective danger may find allies in socially oriented motivations. To encourage compliance, interventions should avoid exceedingly authoritarian messages (possibly boosting counter-reactive goals) and instead focus on providing opportunities for setting good examples in the social arena. Indeed, previous contributions suggest that rather than (or beside) enforcing, presenting mitigation behaviors as socially accepted and widely enacted behaviors is an effective way to increase adherence to rules (Webster et al., 2020; Young and Goldstein, 2021). In particular, social norms are less likely to undermine individuals’ sense of freedom (Young and Goldstein, 2021), thus reducing the risk of backfiring effects.
We believe our results may be interpreted in this light: communities could promote safety goals by showing that positive behaviors exist and are normative (which appears to be the case). Also, public messages may present mitigation behaviors as wise ways to exert one’s freedom, rather than only as obligations. These may help to build alternative ways to pursue one’s goals, tempering both safety and freedom motives. On the contrary, a sharp contrast between motivations to be free and to be safe – in this pandemic and other health-related situations – may result in polarized, potentially dangerous, behavioral responses.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://osf.io/hjmyx/?view_only=75d4c3b152a7429fb22fd35fcf9119db.
Ethics Statement
The studies involving human participants were reviewed and approved by Commissione per la Valutazione della Ricerca (CRIP), University of Milan-Bicocca. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors contributed to the conception and design of the study. GC and MDS performed statistical analyses. MDS wrote the first draft of the manuscript. GC wrote sections of the manuscript. MP supervised the project. All authors contributed to manuscript revision and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to thank Angela Mazza, Alessandra Ambrogi, Giovanni Maria Mauri, and Angelica Greco, for their assistance with the data collection process.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2021.635406/full#supplementary-material
Footnotes
- ^ For details, see http://www.governo.it/it/iorestoacasa-misure-governo
- ^ https://www.qualtrics.com/it/
- ^ Preregistrations are available at https://aspredicted.org/43rr6.pdf and https://aspredicted.org/j2q8i.pdf
- ^ We compared demographic data of 635 excluded participants who completed at least the demographic questionnaire and of the 955 who were included in the analyses. Despite the large samples involved, the excluded participants did not present significant differences in terms of age, t(1628) = 1.62, p = 0.105, gender χ2(1) = 3.02, p = 0.092, location χ2(100) = 107.77, p = 0.281, or occupation. Participants who were excluded from the study were slightly less educated (M = 3.34, SD = 0.63) than those who completed it (M = 3.46, SD = 0.70), t(1628) = 3.70, p < 0.001. This might reflect a lower willingness to participate in an online questionnaire or a greater difficultly to complete it for less educated people.
References
Aschwanden, D., Strickhouser, J. E., Sesker, A. A., Lee, J. H., Luchetti, M., Stephan, Y., et al. (2020). Psychological and Behavioural Responses to Coronavirus Disease 2019: the Role of Personality. Eur. J. Personal. doi: 10.1002/per.2281 [Epub online ahead of print].
Barari, S., Caria, S., Davola, A., Fetzer, T., Fiorin, S., Hensel, L., et al. (2020). Evaluating COVID-19 public health messaging in Italy?: self-reported compliance and growing mental health concerns. medRxiv[preprint]. doi: 10.1101/2020.03.27.20042820
Bavel, J. J. V., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., et al. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 4, 460–471. doi: 10.1038/s41562-020-0884-z
Bernaards, C. A., and Jennrich, R. I. (2005). Gradient projection algorithms and software for arbitrary rotation criteria in factor analysis. Educ. Psychol. Meas. 65, 676–696.
Bethlehem, J. (2010). Selection bias in web surveys. Int. Stat. Rev. 78, 161–188. doi: 10.1111/j.1751-5823.2010.00112.x
Blagov, P. S. (2020). Adaptive and dark personality traits in the Covid-19 pandemic: predicting health-behavior endorsement and the appeal of public-health messages. PsyArXiv [Preprint]. doi: 10.31234/osf.io/chgkn
Bourassa, K. J., Sbarra, D. A., Caspi, A., and Moffitt, T. E. (2020). Social distancing as a health behavior: county-level movement in the united states during the COVID-19 pandemic is associated with conventional health behaviors. Ann. Behav. Med. 54, 548–556. doi: 10.1093/abm/kaaa049
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/S0140-6736(20)30460-8
Calvillo, D. P., Ross, B. J., Garcia, R. J. B., Smelter, T. J., and Rutchick, A. M. (2020). Political Ideology Predicts Perceptions of the Threat of COVID-19 (and Susceptibility to Fake News About It). Soc. Psychol. Personal. Sci. 11:194855062094053. doi: 10.1177/1948550620940539
Cantarero, K., van Tilburg, W. A. P., and Smoktunowicz, E. (2020). Affirming Basic Psychological Needs Promotes Mental Well-Being During the COVID-19 Outbreak. Soc. Psychol. Personal. Sci. doi: 10.1177/1948550620942708 [Epub ahead of print].
Carvalho, L., de, F., Pianowski, G., and Gonçalves, A. P. (2020). Personality differences and COVID-19: are extroversion and conscientiousness personality traits associated with engagement with containment measures? Trends Psychiatry Psychother. 42, 179–184. doi: 10.1590/2237-6089-2020-0029
Chen, J., and Chen, Z. (2008). Extended Bayesian information criteria for model selection with large model spaces. Biometrika 95, 759–771. doi: 10.1093/biomet/asn034
Conway, L. G., Woodard, S. R., and Zubrod, A. (2020). Social psychological measurements of COVID-19: coronavirus perceived threat, government response, impacts, and experiences questionnaires. PsyArXiv [Preprint]. doi: 10.31234/osf.io/z2x9a
R Core Team [RCT] (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing. URL: https://www.R-project.org/.
Costantini, G., Epskamp, S., Borsboom, D., Perugini, M., Mõttus, R., Waldorp, L. J., et al. (2015). State of the aRt personality research: a tutorial on network analysis of personality data in R. J. Res. Personal. 54, 13–29. doi: 10.1016/j.jrp.2014.07.003
Costantini, G., and Perugini, M. (2018). A framework for testing causality in personality research. Eur. J. Personal. 32, 254–268. doi: 10.1002/per.2150
Costantini, G., Richetin, J., Preti, E., Casini, E., Epskamp, S., and Perugini, M. (2019). Stability and variability of personality networks. A tutorial on recent developments in network psychometrics. Personal. Individ. Differ. 136, 68–78. doi: 10.1016/j.paid.2017.06.011
Costantini, G., Saraulli, D., and Perugini, M. (2020). Uncovering the motivational core of traits: the case of conscientiousness. Eur. J. Personal. 34, 1073–1094. doi: 10.1002/per.2237
Duan, L., and Gang, Z. (2020). Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 7, 300–302. doi: 10.1016/S2215-0366(20)30073-0
Elliot, A. J., and Fryer, J. W. (2008). “The goal construct in psychology,” in Handbook of Motivation Science, eds J. Y. Shah and W. L. Gardner (U.S.: Guilford Press), 235–250.
Epskamp, S., Borsboom, D., and Fried, E. I. (2018a). Estimating psychological networks and their accuracy: a tutorial paper. Behav. Res. Methods 50, 195–212. doi: 10.3758/s13428-017-0862-1
Epskamp, S., Costantini, G., Haslbeck, J. M. B., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D., et al. (2018b). qgraph: Graph plotting methods, psychometric data visualization and graphical model estimation. R package version 1.5.
Epskamp, S., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D., and Borsboom, D. (2012). qgraph: network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 48, 1–18.
Epskamp, S., and Fried, E. I. (2018). A tutorial on regularized partial correlation networks. Psychol. Methods 23, 617–634. doi: 10.1037/met0000167
Epskamp, S., Waldorp, L. J., Mõttus, R., and Borsboom, D. (2018c). The Gaussian Graphical Model in Cross-Sectional and Time-Series Data. Multivariate Behav. Res. 53, 453–480. doi: 10.1080/00273171.2018.1454823
Floyd, D. L., Prentice-Dunn, S., and Rogers, R. W. (2000). A meta-analysis of research on protection motivation theory. J. Appl. Soc. Psychol. 30, 407–429. doi: 10.1111/j.1559-1816.2000.tb02323.x
Fong, M. W., Gao, H., Wong, J. Y., Xiao, J., Shiu, E. Y. C., Ryu, S., et al. (2020). Nonpharmaceutical measures for pandemic influenza in nonhealthcare settings—Social distancing measures. Emerg. Infect. Dis. 26, 976–984. doi: 10.3201/eid2605.190995
Foygel, R., and Drton, M. (2010). Extended Bayesian information criteria for Gaussian graphical models. Adv. Neural Inf. Process. Syst. 22, 2020–2028.
Freeman, L. C. (1978). Centrality in social networks conceptual clarification. Soc. Netw. 1, 215–239. doi: 10.1016/0378-8733(78)90021-7
Freitas, A. L., Gollwitzer, P. M., and Trope, Y. (2004). The influence of abstract and concrete mindsets on anticipating and guiding others’ self-regulatory efforts. J. Exp. Soc. Psychol. 40, 739–752. doi: 10.1016/j.jesp.2004.04.003
Gebhardt, W. A. (2006). “Contextualizing health behaviors: the role of personal goals,” in Self−Regulation in Health Behavior, eds D. de Ridder and J. de Wit (U.S.: John Wiley & Sons Ltd), 25–43. doi: 10.1002/9780470713150.ch2
Gebhardt, W. A., and Maes, S. (1998). Competing personal goals and exercise behaviour. Percept. Mot. Skills 86, 755–759. doi: 10.2466/pms.1998.86.3.755
Hayton, J. C., Allen, D. G., and Scarpello, V. (2004). Factor Retention Decisions in Exploratory Factor Analysis: a Tutorial on Parallel Analysis. Organ. Res. Methods 7, 191–205. doi: 10.1177/1094428104263675
Heller, D., Perunovic, W. Q. E., and Reichman, D. (2009). The future of person-situation integration in the interface between traits and goals: a bottom-up framework. J. Res. Personal. 43, 171–178. doi: 10.1016/j.jrp.2008.12.011
Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika 30, 179–185.
Italian Ministry of Health [IMH]. (2020). Coronavirus, le misure adottate dal Governo (16 June). URL: http://www.governo.it/it/approfondimento/coronavirus/13968
Jin, J. M., Bai, P., He, W., Wu, F., Liu, X. F., Han, D. M., et al. (2020). Gender Differences in Patients With COVID-19: focus on Severity and Mortality. Front. Public Health 8:152. doi: 10.3389/fpubh.2020.00152
Jones, P. J. (2020). Networktools: Tools for Identifying Important Nodes in Networks. URL: https://CRAN.R-project.org/package=networktools
Jones, P. J., Ma, R., and McNally, R. J. (2019). Bridge Centrality: a Network Approach to Understanding Comorbidity. Multivariate Behav. Res. 1–15. doi: 10.1080/00273171.2019.1614898 [Epub Online ahead of print].
Kachanoff, F., Bigman, Y. E., Kapsaskis, K., and Gray, K. (2020). Measuring Realistic and Symbolic Threats of COVID-19 and their Unique Impacts on Well-being and Adherence to Public Health Behaviors. Soc. Psychol. Personal. Sci. 2020, 1–14. doi: 10.1177/1948550620931634
Koo, J. R., Cook, A. R., Park, M., Sun, Y., Sun, H., Lim, J. T., et al. (2020). Interventions to mitigate early spread of SARS-CoV-2 in Singapore: a modelling study. Lancet Infect. Dis. 20, 678–688. doi: 10.1016/S1473-3099(20)30162-6
Kruglanski, A. W., Chernikova, M., Babush, M., Dugas, M., and Schumpe, B. M. (2015). “Chapter Three - The architecture of goal systems: multifinality, equifinality, and counterfinality in means—End Relations,” in Advances in Motivation Science, ed. A. J. Elliot (Amsterdam: Elsevier), 69–98. doi: 10.1016/bs.adms.2015.04.001
Kruglanski, A. W., Shah, J. Y., Fishbach, A., Friedman, R., Chun, W. Y., and Sleeth-Keppler, D. B. T. (2002). “A theory of goal systems,” in Advances in Experimental Social Psychology, Vol. 34, ed. M. P. Zanna (Cambridge: Academic Press), 331–378. doi: 10.1016/S0065-2601(02)80008-9
Kruglanski, A. W., and Szumowska, E. (2020). Habitual behavior is goal-driven. Perspect. Psychol. Sci. 15, 1256–1271. doi: 10.1177/1745691620917676
Li, J.-B., Yang, A., Dou, K., Wang, L.-X., Zhang, M.-C., and Lin, X.-Q. (2020). Chinese public’s knowledge, perceived severity, and perceived controllability of the COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: a national survey. PsyArXiv [Preprint]. doi: 10.31234/osf.io/5tmsh
Martin, K. A., Leary, M. R., and O’Brien, J. (2001). Role of self-presentation in the health practices of a sample of Irish adolescents. J Adolesc. Health 28, 259–262. doi: 10.1016/S1054-139X(00)00209-3
Meade, A. W., and Craig, S. B. (2012). Identifying careless responses in survey data. Psychol. Methods 17, 437–455. doi: 10.1037/a0028085
Milne, S., Sheeran, P., and Orbell, S. (2000). Prediction and intervention in health-related behavior: a meta-analytic review of protection motivation theory. J. Appl. Soc. Psychol. 30, 106–143. doi: 10.1111/j.1559-1816.2000.tb02308.x
National Academies of Sciences, Engineering, and Medicine [NASEM]. (2020). Encouraging Adoption of Protective Behaviors to Mitigate the Spread of COVID-19: Strategies for Behavior Change. Washington: The National Academies Press.
Oettingen, G. (2012). Future thought and behaviour change. Eur. Rev. Soc. Psychol. 23, 1–63. doi: 10.1080/10463283.2011.643698
Oettingen, G., and Gollwitzer, P. M. (2018). “Health behavior change by self-regulation of goal pursuit: mental contrasting with implementation intentions,” in The Routledge International Handbook of Self-Control in Health and Well-Being, eds D. T. D. de Ridder, M. A. Adriaanse, and K. Fujita (London: Routledge), 418–430.
Perugini, M., and Conner, M. (2000). Predicting and understanding behavioral volitions: the interplay between goals and behaviors. Eur. J. Soc. Psychol. 30, 705–731.
Prem, K., Liu, Y., Russell, T. W., Kucharski, A. J., Eggo, R. M., Davies, N., et al. (2020). The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. 5, e261–e270. doi: 10.1016/S2468-2667(20)30073-6
Prestwich, A., Perugini, M., and Hurling, R. (2010). Can implementation intentions and text messages promote brisk walking? A randomized trial. Health Psychol. 29, 40–49. doi: 10.1037/a0016993
Preti, E., Di Mattei, V., Perego, G., Ferrari, F., Mazzetti, M., Taranto, P., et al. (2020a). The psychological impact of epidemic and pandemic outbreaks on healthcare workers: rapid review of the evidence. Curr. Psychiatry Rep. 22:43.
Preti, E., Di Pierro, R., Fanti, E., Madeddu, F., and Calati, R. (2020b). Personality disorders in time of pandemic. Curr. Psychiatry Rep. 22:80. doi: 10.1007/s11920-020-01204-w
Remuzzi, A., and Remuzzi, G. (2020). COVID-19 and Italy: what next? Lancet 395, 1225–1228. doi: 10.1016/S0140-6736(20)30627-9
Revelle, W. (2019). psych: Procedures for Personality and Psychological Research. U.S.: Northwestern University.
Richetin, J., Conner, M., and Perugini, M. (2011). Not doing is not the opposite of doing: implications for attitudinal models of behavioral prediction. Personal. Soc. Psychol. Bull. 37, 40–54. doi: 10.1177/0146167210390522
Rogers, R. W. (1975). A protection motivation theory of fear appeals and attitude change. J. Psychol. 91, 93–114. doi: 10.1080/00223980.1975.9915803
Rogers, R. W. (1983). “Cognitive and physiological processes in fear appeals and attitude change: a revised theory of protection motivation,” in Social Psychophysiology: A sourcebook, eds J. T. Cacioppo and R. E. Petty (U.S.: Guilford Press), 153–176.
Rosenthal-von der Pütten, A. M., Hastall, M. R., Köcher, S., Meske, C., Heinrich, T., Labrenz, F., et al. (2019). “Likes” as social rewards: their role in online social comparison and decisions to like other People’s selfies. Comput. Hum. Behav. 92, 76–86. doi: 10.1016/j.chb.2018.10.017
Sheeran, P., Klein, W. M. P. P., and Rothman, A. J. (2017). Health behavior change: moving from observation to intervention. Ann. Rev. Psychol. 68, 573–600. doi: 10.1146/annurev-psych-010416-044007
Tamir, D. I., and Hughes, B. L. (2018). Social Rewards: from Basic Social Building Blocks to Complex Social Behavior. Perspect. Psychol. Sci. 13, 700–717. doi: 10.1177/1745691618776263
Tan, A. S. L., Lee, C., and Chae, J. (2015). Exposure to health (mis)information: lagged effects on young adults’ health behaviors and potential pathways. J. Commun. 65, 674–698. doi: 10.1111/jcom.12163
Tan, B. Y. Q., Chew, N. W. S., Lee, G. K. H., Jing, M., Goh, Y., Yeo, L. L. L., et al. (2020). Psychological impact of the COVID-19 pandemic on health care workers in singapore. Ann. Intern. Med. 173, 317–320. doi: 10.7326/M20-1083
Van Bavel, J. J., Cichocka, A., Capraro, V., Sjastad, H., Nezlek, J. B., Pavlovic, T., et al. (2020). National identity predicts public health support during a global pandemic. PsyArxiv [Preprint]. doi: 10.31234/osf.io/ydt95
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., et al. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 17:1729. doi: 10.3390/ijerph17051729
Webster, R. K., Brooks, S. K., Smith, L. E., Woodland, L., Wessely, S., and Rubin, G. J. (2020). How to improve adherence with quarantine: rapid review of the evidence. Public Health 182, 163–169. doi: 10.1016/j.puhe.2020.03.007
Wieber, F., and Gollwitzer, P. M. (2017). “Planning and the Control of Action,” in Knowledge and Action, eds P. Meusburger, B. Werlen, and L. Suarsana Cham: Springer.
World Health Organization [WHO]. (2020a). Coronavirus disease (COVID-19) Pandemic. URL: https://www.who.int/emergencies/diseases/novel-coronavirus-2019
World Health Organization [WHO]. (2020b). WHO Director-General’s opening remarks at the media briefing on COVID-19 - 23 July 2020. URL: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—23-july-2020
Wu, Y., and Shen, F. (2021). Exploring the impacts of media use and media trust on health behaviors during the COVID-19 pandemic in China. J. Health Psychol. 1359105321995964. doi: 10.1177/1359105321995964 [Epub online ahead of print].
Keywords: COVID-19, goals, behaviors, principal component analysis, network analysis
Citation: Costantini G, Di Sarno M, Preti E, Richetin J and Perugini M (2021) Would You Rather Be Safe or Free? Motivational and Behavioral Aspects in COVID-19 Mitigation. Front. Psychol. 12:635406. doi: 10.3389/fpsyg.2021.635406
Received: 30 November 2020; Accepted: 05 May 2021;
Published: 28 May 2021.
Edited by:
Elisa Pedroli, Istituto Auxologico Italiano (IRCCS), ItalyReviewed by:
Cosimo Tuena, Istituto Auxologico Italiano (IRCCS), ItalyPietro De Carli, University of Padua, Italy
Copyright © 2021 Costantini, Di Sarno, Preti, Richetin and Perugini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Di Sarno, bWFyY28uZGlzYXJub0B1bmltaWIuaXQ=
†These authors have contributed equally to this work and share first authorship