 Joanna Kuć
Joanna Kuć Małgorzata Żendzian-Piotrowska
Małgorzata Żendzian-Piotrowska- 1Department of Prosthodontics, Medical University of Bialystok, Bialystok, Poland
- 2Department of Hygiene, Epidemiology and Ergonomics, Medical University of Bialystok, Bialystok, Poland
Introduction: A lot of general dental practitioners suffer from job-related health problems. They are more prone to numerous different physical and psycho-emotional triggers that aggravate their working conditions.
The Aim: The aim of the study was to evaluate cervical physiotherapeutic treatment needs, daily ergonomic habits and the necessity for physical activity among students of dentistry at a medical university.
Materials and Methods: 112 generally healthy dentistry students (73 women, 39 men) were enrolled for the study. The age range was 20–32, with an average of 22.88 ± 2.7. The study included subjects in their second to fifth year of studies. The survey was conducted with respect to the questionnaires about possible physiotherapeutic treatments, physical activities, imaging tests and diagnoses as well as statements regarding the respondents’ knowledge and ergonomics habits. To estimate the association between the risk factor and neck disability as well as chronic pain, the Neck Disability Index, Perceived Stress Scale and the Graded Chronic Pain Scale were additionally applied.
Results: 35.71% of dentistry students had undergo physiotherapy in the preceding year. 26.79% of the respondents declared that they underwent rehabilitation on a regular basis. The most common reasons for treatment were complaints of the cervical (7.14%), lumbar (3.57%), and thoracic spine (1.79%) as well as a combination of these symptoms. 6.25% of the subjects had started rehabilitation due to muscle relaxation. 34.82% of the study participants did not do any physical activity. Females exercised more often than males (p = 0.02; 1–β = 0.65). Therapeutic exercises contributed to the improvement of well-being of 56% of students. 64.29% of the respondents chose a sitting position during pre-clinical and clinical classes and 26.79% of the subjects worked in sitting and standing postures.
Conclusion: 26.79% of dentistry students required periodic therapeutic rehabilitation. 34.82% of the respondents were advised to implement systematic physical activity. Due to professional conditions, dental students are exposed to an early cervical spine disorders. The main factor influencing an early onset of such dysfunctions is increased stress level. An average level of pro-health awareness may be the reason for elevated cost of rehabilitation among this group of patients.
Introduction
Occupational hazard is associated with the risk of job-related health problems. It can refer to the working environment, materials, substances, processes or situations that initiate or promote workplace incidents and/or disabilities. The role of occupation in the dynamics of health and sickness was first described by Bernardo Ramazzini in the 18th century (Fasunloro and Owotade, 2004).
A lot of general dental practitioners suffer from job-related health problems (Myers and Myers, 2004). They are more prone to numerous different physical and psycho-emotional triggers that aggravate their working conditions (Myers and Myers, 2004; Moodley et al., 2018). A static position, typically adapted during dental procedures, result in a 10% higher energy consumption, increased heart rate, overload on the cardiovascular and osteoarticular systems, overcharging of the body with a functionally-tailored reduced support surface, pain and discomfort in the calves (Anghel et al., 2007). The evaluation of momentary workloads does not reveal the amount of the experienced cumulative trauma (Newell and Kumar, 2005). In the long term, tissue load becomes a health-modulating factor (Newell and Kumar, 2005). Work-related static posture leads to the development of musculoskeletal disorders. Over 70% of dental students reported pain around the third year of their studies (Rising et al., 2005). 87.2% of the dentists manifested at least one symptom of musculoskeletal disorder in the last year of their clinical practice (Leggat and Smith, 2006). The factors promoting such problems include: constantly repeated movements, twisting of the trunk, multiple daily cervical flexion as well as strong arm movement (e.g., working with arms above the shoulder) and sedentary behavior (e.g., long time in a seated position without breaks; always working in the same position) (Valachi and Valachi, 2003a,b; Presoto and Garcia, 2016; Kuć and Żendzian-Piotrowska, 2020).
The pain within the musculoskeletal system appears at the time when dentists begin professional studies and remain at the university for the duration of their practice (Diaz-Caballero et al., 2010). A typical clinical pattern includes neck, shoulder, arm and wrist pain (Moodley et al., 2018). Complaints about the lumbar spine are also typical (Moodley et al., 2018). Functional changes are often manifested by a posture with the head inclined forward, loss of cervical lordosis and shoulder girdle protraction (Kuć and Żendzian-Piotrowska, 2020). Due to the common interface of the cervical spine and the trigeminocervical nucleus, many neurophysiological consequences within the orofacial area can be expected (Bogduk, 2001; Olivo et al., 2010).
It is known that muscle tension increases even despite maintaining the right posture and ensuring optimal ergonomics, which results in ischemia and hypomobility of the joints. This is related to long working hours (Valachi and Valachi, 2003a,b). The consequences of limited range of cervical spine motion (e.g., limited flexion, extension, rotation), muscle imbalance (size or strength discrepancy between right and left muscle groups), proprioception impairment (dysfunction of feedback between sensory receptors and the nervous system), seemingly idiopathic fatigue and pain (e.g., neck pain, headache, multi-site musculoskeletal pain), cause an urgent need for physical activity in relation to ergonomics (Letafatkar et al., 2019). The main goal is to prevent progression of the said changes to chronic phase of disability (Letafatkar et al., 2019).
Another important job-related health hazard of dentists concerns their psychological condition. In many cases, an occupational burnout syndrome occurs as a consequence of chronic emotional and interpersonal stressors (Maslach and Jackson, 1981). Burnout is defined as a negative work-related psychological condition associated with physical fatigue, emotional exhaustion and lack of motivation (Freudenberger, 1974). It appears as a significant risk factor of depression (Hakanen and Schaufeli, 2012). It can also adversely affect physical health, e.g., by causing cardiovascular and musculoskeletal diseases (Honkonen et al., 2006). There is a direct link between burnout of the dental health professionals, their low personal efficiency and a tendency to put patients at greater risk (Panagioti et al., 2018). Typical triggers of occupational stress among dentists include time pressure, work overload, absorbing, difficult and/or delayed patients, problems with staff, equipment or dental materials, as well as daily routine (Chohan et al., 2020). To prevent signs of burnout, attention should be paid to physical activity and work ergonomics should be provided (Gorter et al., 2000). It is also well known that the avoidance of emotional, mental and behavioral mental disabilities is an interdisciplinary subject that requires the implementation of numerous different strategies (O’Connell et al., 2009).
The Aim
The aim of the study was to evaluate cervical physiotherapeutic treatment needs, daily ergonomic habits and the necessity for physical activity among students of dentistry at a medical university.
Materials and Methods
The Subjects and Sample Size
One hundred and twelve generally healthy students (73 women and 39 men) of the faculty of medicine, division of dentistry of the Medical University of Bialystok, Poland were enrolled for the study. The age range was 20–32, with an average of 22.88 ± 2.7 (Meanfemale group = 22.99 ± 2.65; Meanmale group = 22.67 ± 2.80). The study included subjects in their second to fifth year of studies. The research was conducted in the period from January to April 2018.
General Description of the Method
The survey was conducted with the use of the following:
• A questionnaire about possible physiotherapeutic treatments and physical activities, including the following questions:
Which forms of physical therapy did you use within the last year? How often do you use rehabilitation procedures? What was the reason/cause for undertaking rehabilitation? How often do you use therapeutic exercises (e.g., yoga, stretching, isometric exercises, etc.)? How do the therapeutic exercises you use affect you?
• A questionnaire about possible imaging tests, diagnosis and confirmation of dysfunctions by a doctor or physiotherapist, including the following questions:
Which types of diagnostic imaging tests (Magnetic Resonance Imaging—MRI, Computed Tomography—CT, blood flow volume of carotid and vertebral arteries) were performed in your case and in which section of the spine? Which of the diagnoses were confirmed by a doctor or physiotherapist?
• Statements of the respondents regarding their knowledge and habits in the field of ergonomics, including the following questions:
What is the right definition of head protraction? Which body position do you assume most frequently when you use a laptop, Tablet or read a book? Which body position is the most common for you during your clinical practice at the university? What is your most common body position when you treat tooth decay located on the palatal side of the upper incisors?
• The Neck Disability Index (NDI), Perceived Stress Scale (PSS-10) and Graded Chronic Pain Scale (GCPS v. 2.0) were additionally applied to estimate the association between the risk factor and neck disability as well as chronic pain.
The response rate to the questionnaires amounted to 100%. The presented subjects and sample size remain in accordance with the study group described in the previous publication (Kuć and Żendzian-Piotrowska, 2020).
Statistical Analysis
A statistical analysis was performed using Statistica 13.1 (Statsoft Inc. United States) and G Power v. 3.1.9.4 software. The measure of central tendency (mean) and variation (standard deviation) were used to describe the distribution of quantitative variables (age of the respondents).
The multivariate frequency distribution of the variables was demonstrated in 2 × 2 contingency tables. The percentage within columns (percentage of the entire group, the female group and the male group, respectively) was also presented.
Due to the relatively small sized sample (expected number of frequencies ≤5), Fisher’s exact one-tailed test was applied to compare differences in frequency with respect to the gender. Differences with p < 0.05 were considered statistically significant.
Post hoc power analysis was performed using G Power v.3.1.9.4 software. Power (1-β) was assessed as the function of the population effect size, the number of cases (n) and α. The levels of power were presented with respect to the comparison of the differences between females and males in dichotomous approach of the examined aspect (e.g., using vs. not using physiotherapy; reasons vs not applicable; using vs not using therapeutic exercises; improvement of mood and physical condition vs all others).
Multiple linear regression models for NDI (Neck Disability Index) and GCPS v. 2.0 (Graded Chronic Pain Scale) estimation were developed by selecting the variables that contributed significantly to the evaluation of NDI and GCPS.
Ethical Approval
The study was performed after obtaining the consent of the Bioethics Committee of the Medical University of Bialystok, Poland no. R-I-002/513/2017. Participation in the study was voluntary and anonymous. Respondents received exhaustive information about the purpose of the research and had the right to terminate their participation at any time with no repercussions.
Results
One hundred and twelve people participated in the study, including 73 women and 39 men. The research group included 25% of all dentistry students. 33 (29.46%) of the respondents had been given massages in the preceding year. 13 (11.61%) students had undergone manual therapy. Four people (3.57%) had benefited from physical therapy and kinesiotaping. 72 (64.29%) subjects had not participated in any of the forms of physiotherapy (Table 1). There were no statistically significant differences in the frequency of having all kinds of physiotherapy in the preceding year with respect to gender (p > 0.05, 1-β < 0.4) (Table 1).
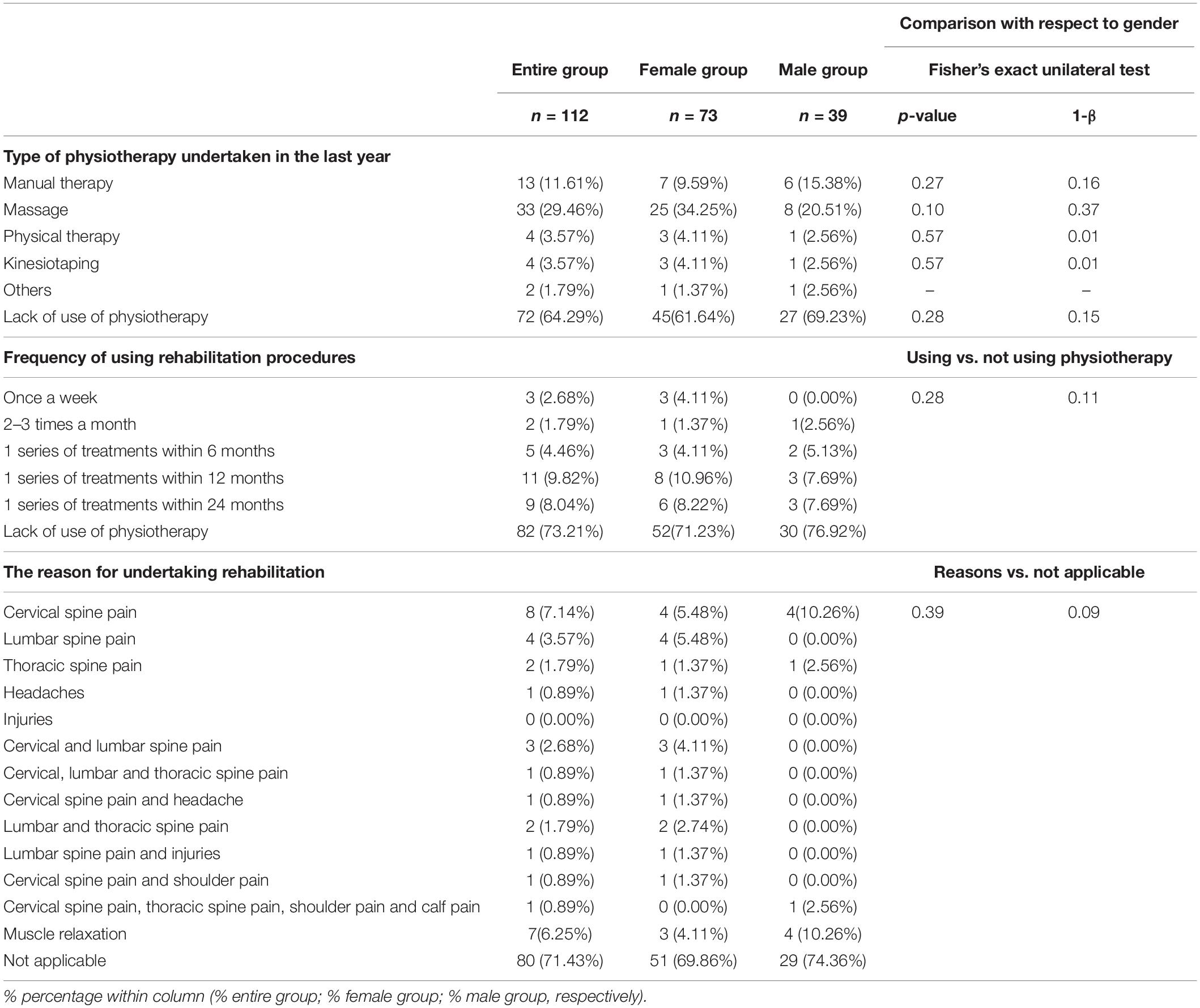
Table 1. Type of physiotherapy undertaken within the last year; frequency and reason for using rehabilitation procedures in the entire group (n = 112), the female group (n = 73), and the male group (n = 39).
82 (73.21%) respondents declared that they did not attend any rehabilitation at all (Table 1); 11 students (9.82%) undertook therapy once a year; 9 (8.04%) people had had 1 series of physiotherapeutic treatments within the preceding 24 months; 3 (2.68%) participants benefited from physiotherapy once a week; 2 (1.79%) people underwent rehabilitation 2–3 times a month (Table 1). There were no statistically significant differences in the frequency of physiotherapeutic procedures with respect to gender (p = 0.28, 1-β = 0.11) (Table 1).
The most common reason for attending rehabilitation among the entire study group (n = 112) were complaints about the cervical (7.14%), lumbar (3.57%), thoracic spine (1.79%) as well as a combination of these (8.92%) (Table 1). Seven people (6.25%) had started rehabilitation for the purpose of relaxation (Table 1). No statistically significant differences were noted between males and females (p = 0.39, 1-β = 0.09) (Table 1).
39 (34.82%) respondents did not do any physical activity (Table 2). Nobody exercised every morning and evening. 14 (12.5%) students trained regularly every few days. 29 (25.89%) subjects were physically active unsystematically, and other 24 (21.43%) worked out very rarely (Table 2). Physical activity was more often performed by women than men (p = 0.02; 1-β = 0.65) (Table 2). In the case of 62 (56%) students, therapeutic exercises contributed to the improvement of their well-being (Table 2). 1 (0.89%) person reported that physical activity adversely affected their health. For 2 (1.79%) subjects, therapeutic exercises caused cervical spine pain. There were no statistically significant differences in mood and fitness improvement with respect to gender (p = 0.20; 1-β = 0.36) (Table 2).
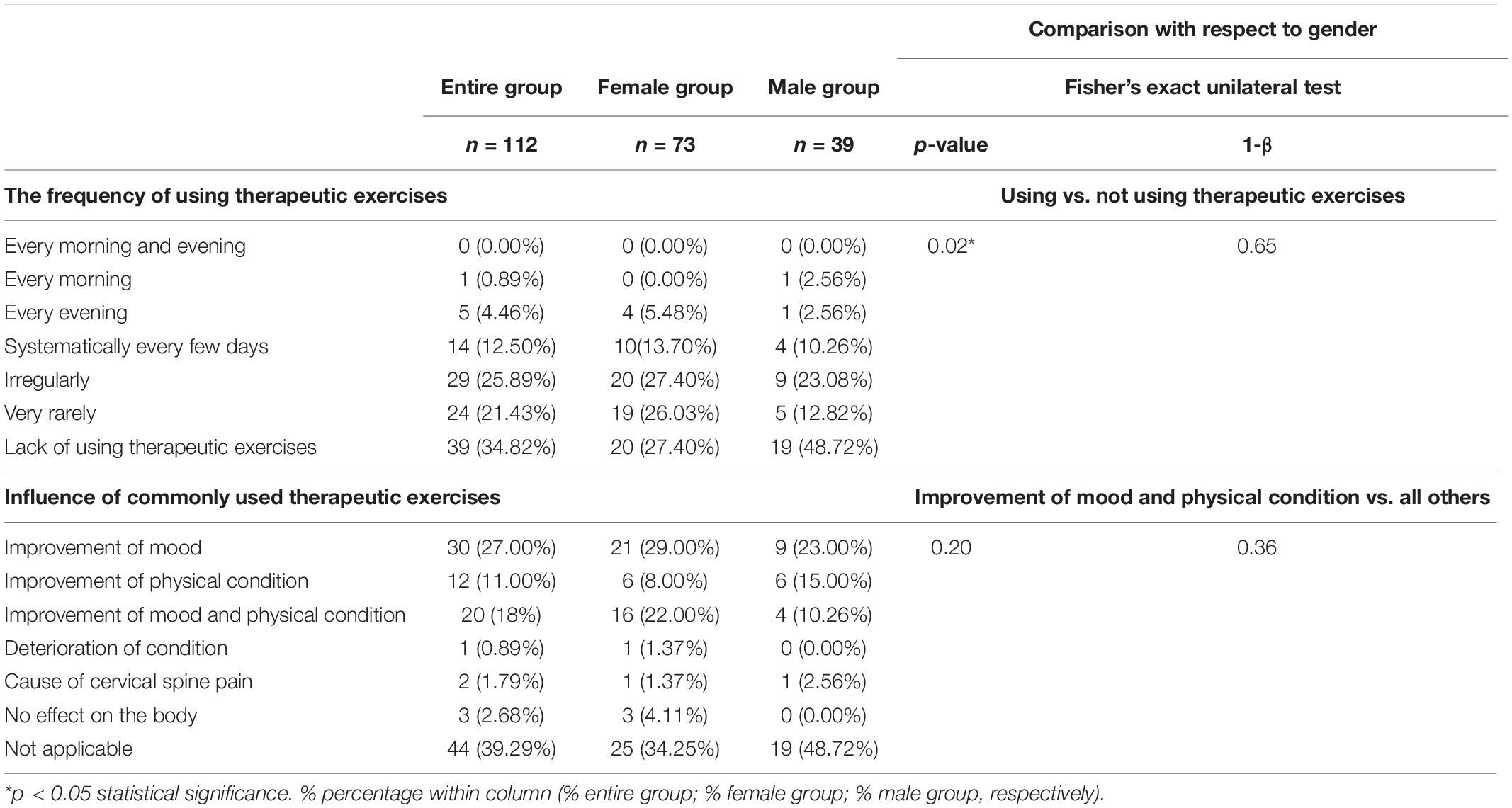
Table 2. The frequency of using therapeutic exercises (e.g., yoga, stretching, isometric exercises, etc.) and the influence of commonly used therapeutic exercises in the entire group (n = 112), the female group (n = 73), and the male group (n = 39).
The students reported having 22 high-imaging tests performed (Table 3), 6 (5.35%) computed tomography (CT) scans and 2 (1.79%) magnetic resonance imaging (MRI) tests of the head. 4 (3.57%) MRI tests and 1 CT scan (0.89%) of the cervical spine were performed. 5 (4.46%) students declared imaging of the lumbar spine, while other 3 (2.68%) reported imaging of the thoracic region (Table 3). A statistically significant higher prevalence of high-imaging tests was noted among females compared to males (p = 0.02; 1-β = 0.50) (Table 3).
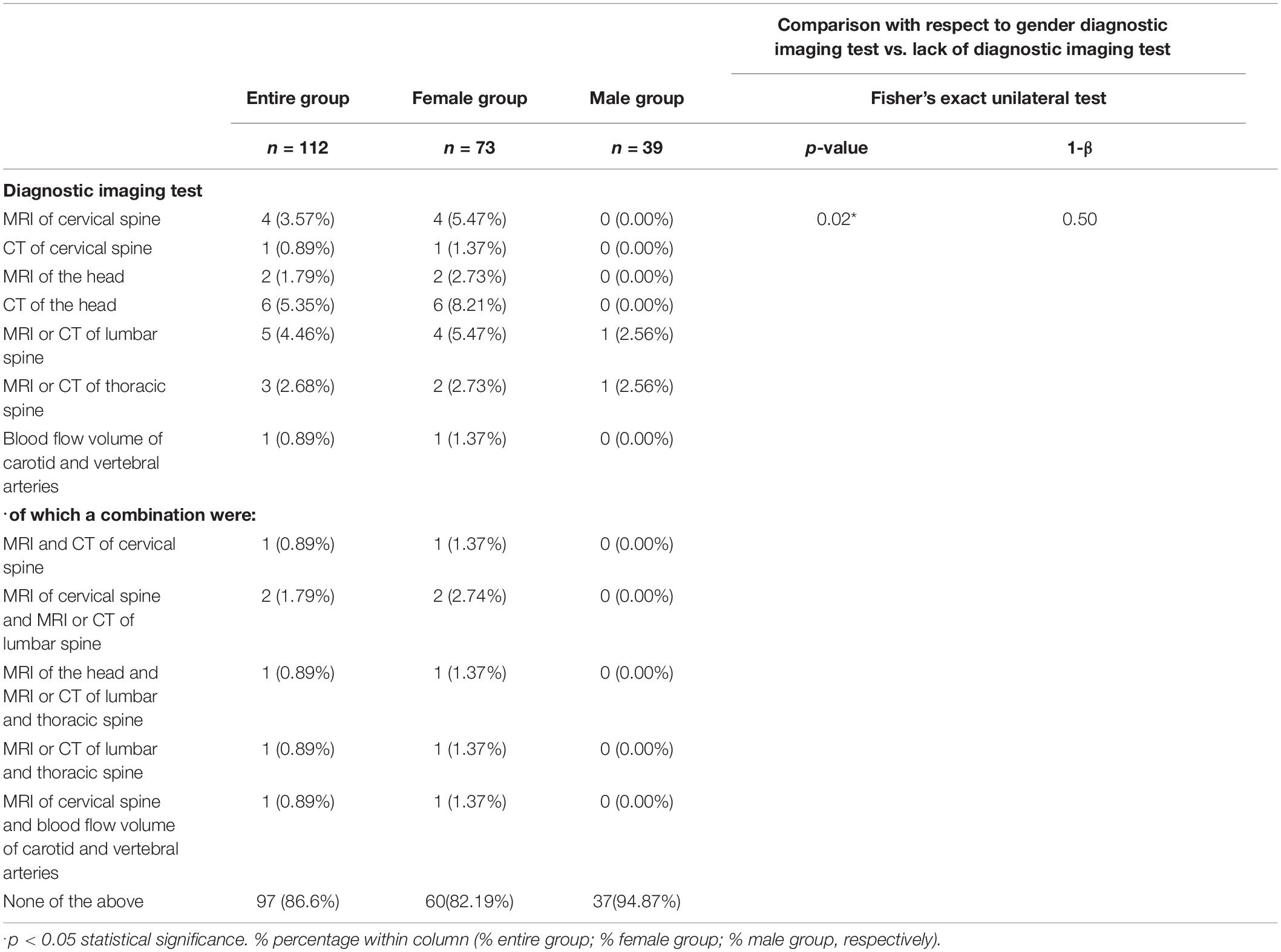
Table 3. The frequency of diagnostic imaging tests performed by the students in the entire group (n = 112), the female group (n = 73), and the male group (n = 39).
Nobody was operated on due to cervical spine injury, cervical discopathy or its sequelae, cancer within the cervical spine, cervical spine instability, birth defects, or cervical spine degeneration.
In 99 (88.39%) students no cervical spine dysfunction were confirmed by a doctor or physiotherapist (Table 4). Three people (2.68%) were diagnosed with cervical discopathy and loss of cervical lordosis. Individual participants (0.89%) declared instability, hypomobility, degenerative changes, whiplash injury, dehydration of intervertebral discs and reduction of vertebral bodies (Table 4).
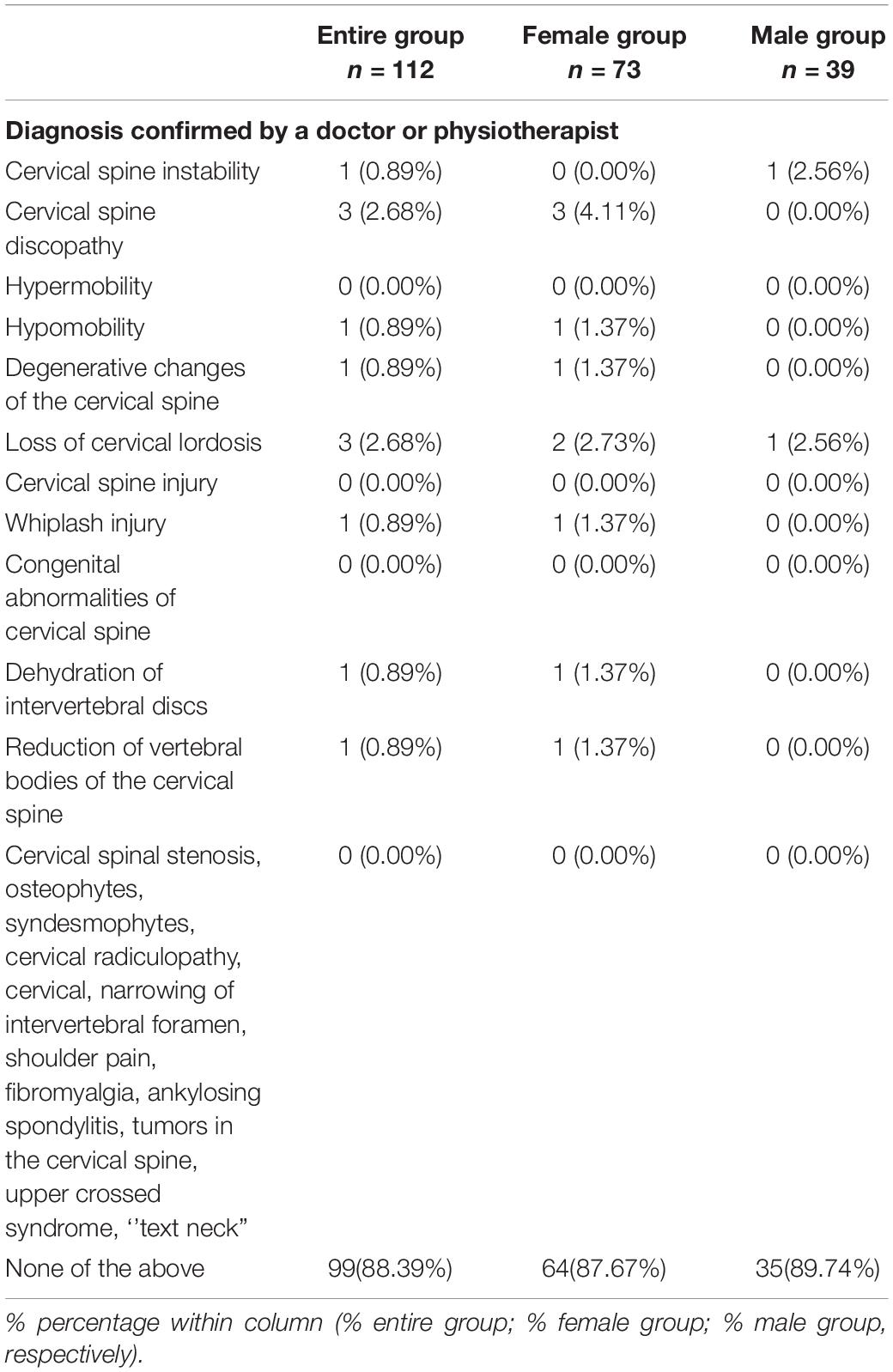
Table 4. Diagnosis confirmed by a doctor or physiotherapist in the entire group (n = 112), the female group (n = 73), and the male group (n = 39).
72 (64.29%) subjects provided a proper definition of head protraction (Table 5). 46 (41.07%) students reported the correct amount of load (23.33 kg) of the cervical spine at its 45° flexion (Table 5). 46 (41.07%) respondents suggested a load of 23.33 kg. There were no statistically significant differences with respect to gender (p > 0.05) (Table 5).
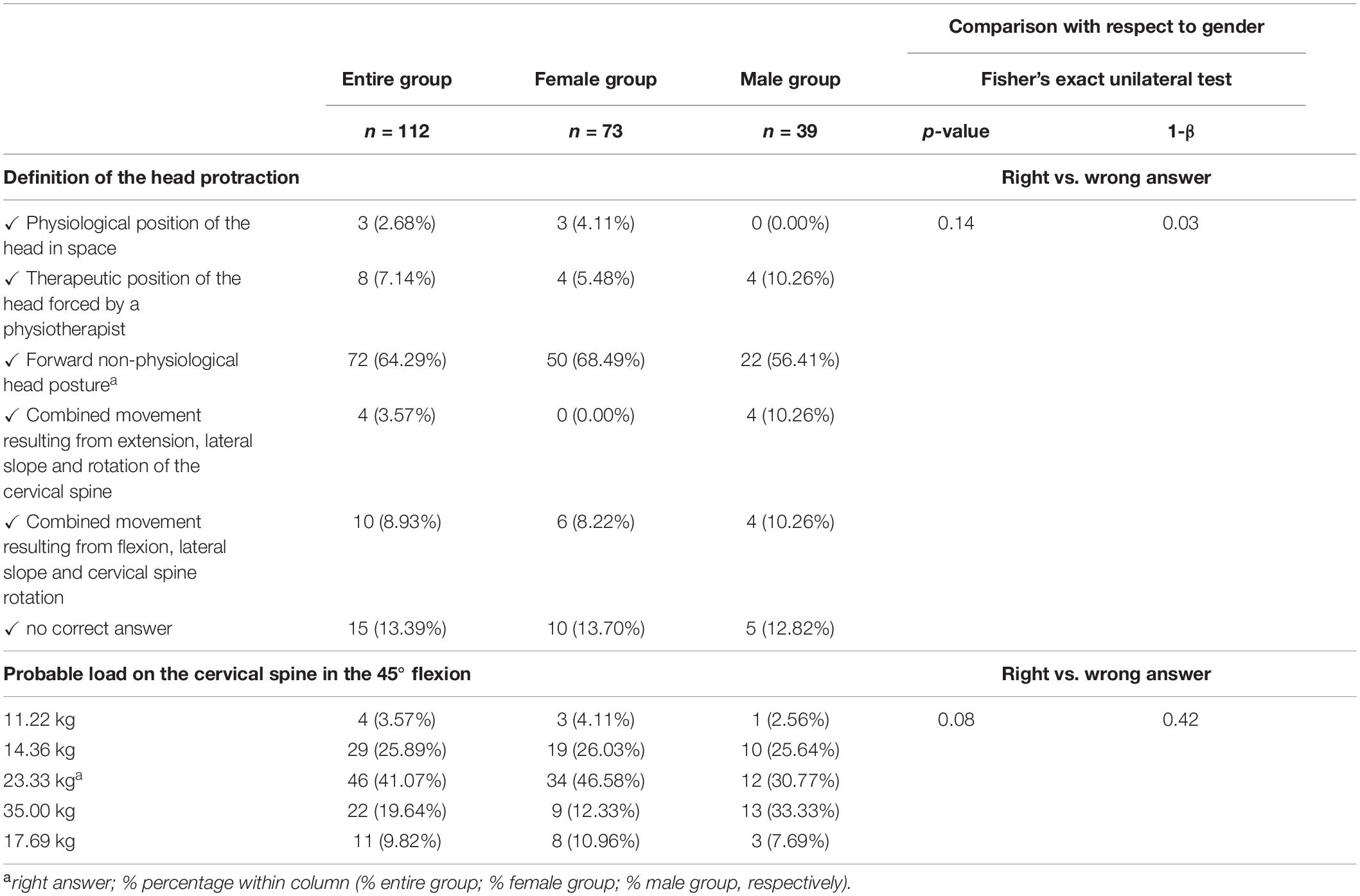
Table 5. Defining head protraction and probable load on the cervical spine in the 45° flexion in the entire group (n = 112), the female group (n = 73), and the male group (n = 39).
37 (33.03%) students indicated sitting at a desk in front of a computer/laptop or reading a book (Table 6). 30 (26.79%) people preferred lying on their back. 23 (20.54%) respondents used an armchair by raising and supporting their limbs with the footrest. 9 (8.04%) students remained in the lateral position, and 7 (6.25%) chose a position on the abdomen (Table 6). No statistically significant differences with respect to gender were found (p = 0.56; 1-β = 0.04) (Table 6).
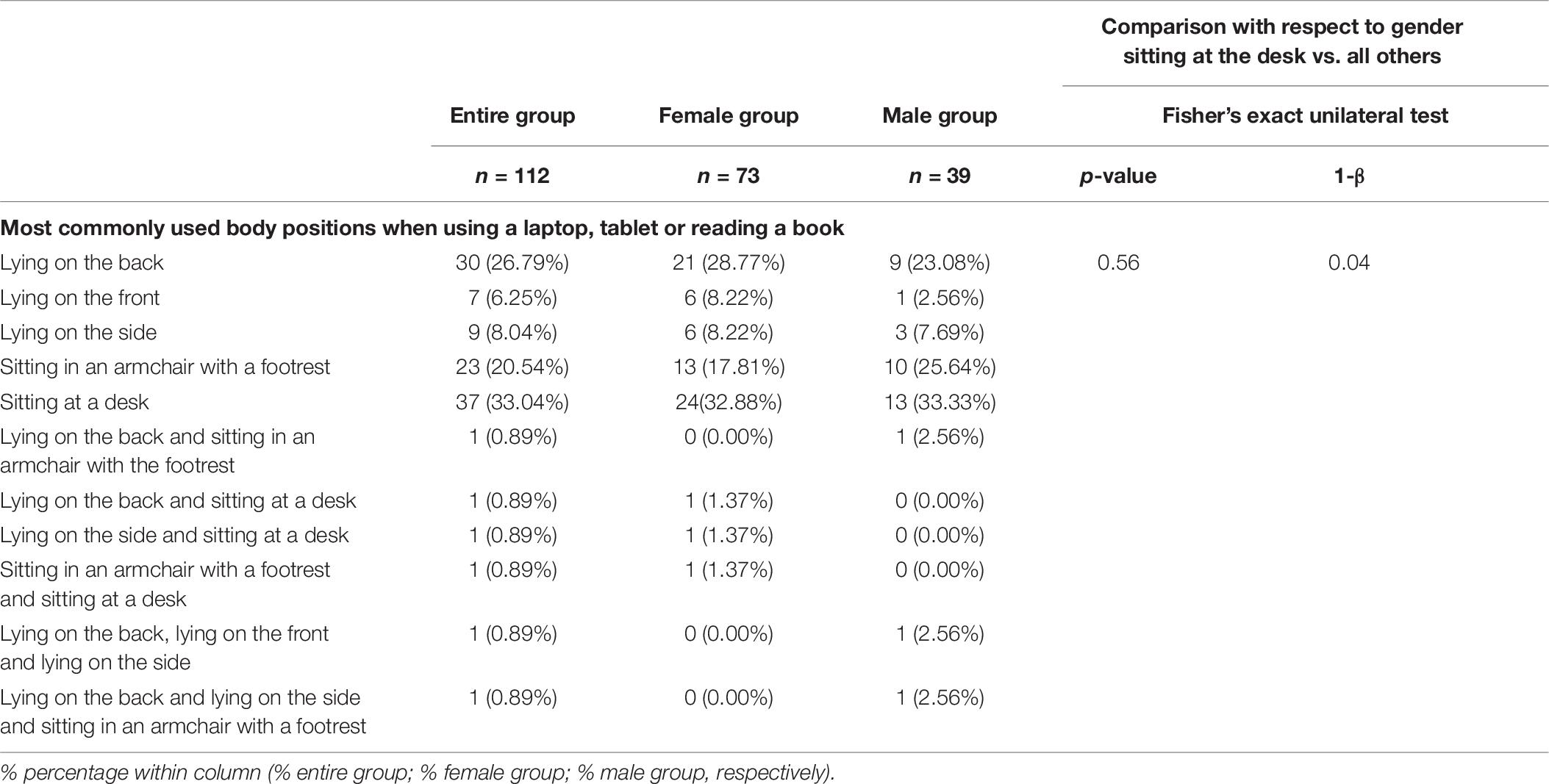
Table 6. The most commonly used body positions when using a laptop, tablet or reading a book in the entire group (n = 112), the female group (n = 73), and male group (n = 39).
72 (64.29%) students chose a sitting position during pre-clinical classes as well as when working with patients (Table 7). 30 (26.79%) of the respondents worked in a mixed manner: assuming both sitting and standing postures. 10 (8.93%) people preferred to work by standing. No participants of the study reported four-handed work with assistance (Table 7). 92 (82.14%) students used a dental mirror and binocular vision when treating a palatal decay in the upper incisors (Table 7). There were no statistically significant differences with respect to gender (p > 0.05) (Table 7).
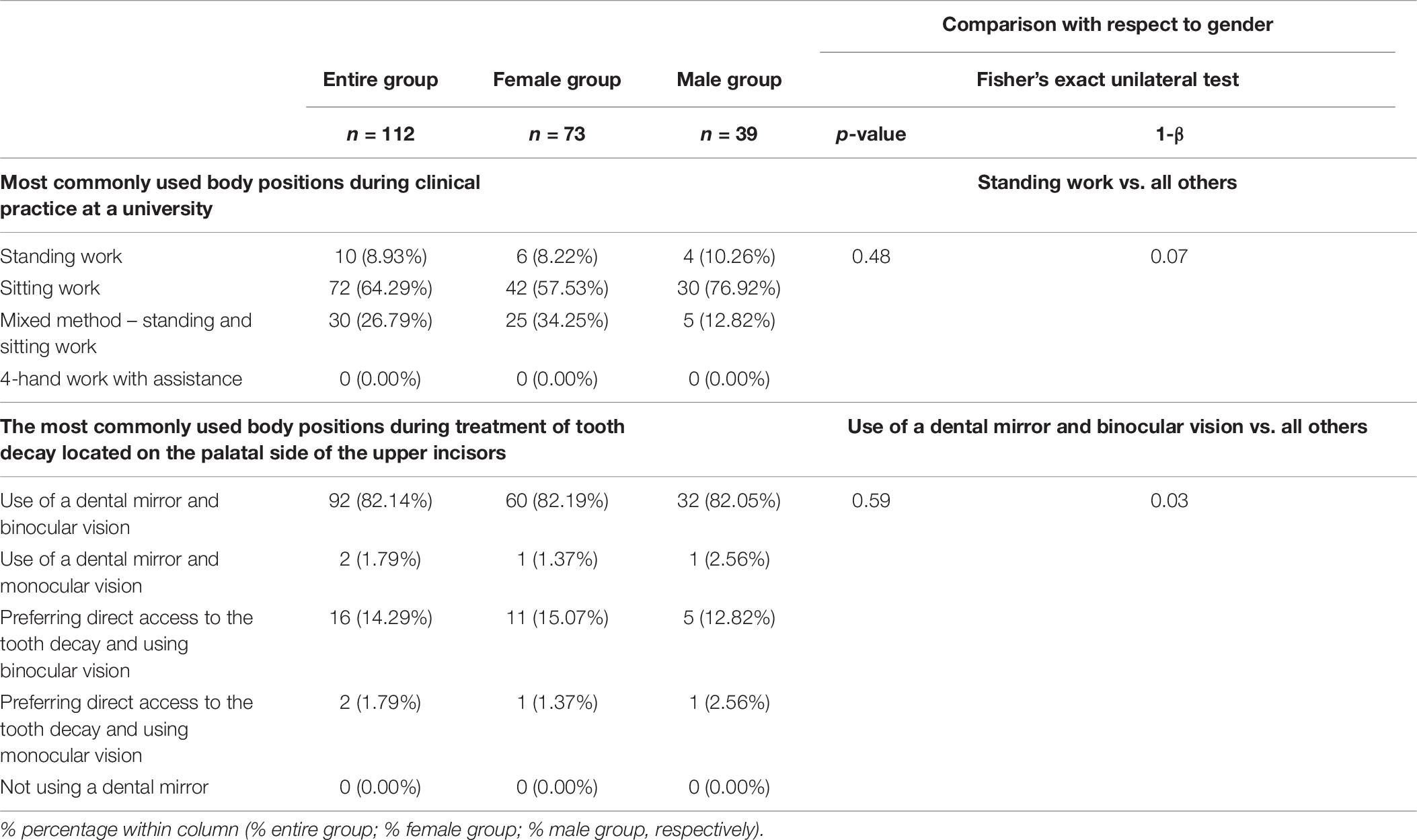
Table 7. The most commonly used body positions during clinical practice at a university in the entire group (n = 112), the female group (n = 73), and male group (n = 39).
The multiple linear regression model revealed that gender, GCPS and PSS-10 allow us to explain the approximately 30% differentiation of Neck Disability Index (NDI) (R2 = 0.31), and the prediction model is significantly better than the random one [F(3, 108) = 15.81; p < 0.00], where the average error in estimating the perceived stress level is S.E. = 3.11 (Table 8).

Table 8. Multiple linear regression model with NDI as the dependent variable and gender, GCPS v. 2.0, PSS-10 as independent variables.
The second model of multiple linear regression showed that a standing position during dental procedures and physiotherapy undertaken enable us to explain the approximately 10% differentiation of the Graded Chronic Pain Scale (GCPS v. 2.0.) (R2 = 0.11), and the prediction model is significantly better than the random one [F(2, 109) = 6.42; p < 0.00], where the average error in estimating the GCPS v. 2.0. is S.E. = 0.61 (Table 9).

Table 9. Multiple linear regression model with GCPS as the dependent variable and standing position during dental procedures and physiotherapy undertaken as independent variables.
Discussion
Occupational diseases affect dentists more often than general medicine practitioners or lawyers. Within this practical group, musculoskeletal complaints are reported 1.5 times more frequently than in other professions (Suciu et al., 2019). The incidence of cervical spondylosis is more pronounced among dentists even compared to agricultural workers (Suciu et al., 2019). This specialty is more burdensome than other medical staff which is determined by the limited intraoral operation area that promotes the adoption of the static posture (Suciu et al., 2019).
A specific dental working position leads to increased muscle tension and fatigue (Callaghan and McGill, 2001; Dantas and de Lima, 2015; Suciu et al., 2019). High static overload causes the compression of blood vessels and activity of the muscles, leading to inadequate oxygen supply, and consequently, pain. Depending on the type of cervical spine disorder, different kinds of physiotherapeutic intervention may be implemented. For example in chronic neck pain complicated by movement discoordination, education about ergonomics and lifestyle plays an important role (Blanpied et al., 2017). Physiotherapeutic procedures include mobilization of the cervical spine, strengthening exercises of the cervical and thoracic spine, mobilization of the scapular area, exercises improving strength, endurance and flexibility, functional training with elements of behavioral therapy, vestibular system rehabilitation and exercises improving eye, neck and head cooperation as well as neuromuscular coordination (Blanpied et al., 2017). The clinical goal of a manual therapy in this group of patients is maintenance of cervical lordosis in the range of 31–40° (McAviney et al., 2005). It should also be highlighted that work productivity of dentists who undergo a physical therapy is increased (Campo et al., 2008; Huang et al., 2014). This study results revealed that 64.29% of the respondents did not, in their own assessment, require any rehabilitation (Table 1). From a clinical point of view it seems to be just a matter of time. In the case of 26.79% of people, physiotherapy is undertaken on a regular basis, which may indicate a chronic, and at the same time recurrent nature of the emerging ailments (Table 1). Considering that the study focused on students, the frequency of physiotherapeutic treatments was relatively high. Due to professional predisposing factors, this situation requires monitoring.
The lack of physical activity among the respondents was not conducive to the prevention of musculoskeletal disorders (Table 2). A decreased level of physical activity is one of public health considerations of the twenty-first century (Blair, 2009; Verbunt et al., 2010). Mortality due to physical inactivity is estimated at 6%. Other leading factors include high blood pressure (13%), smoking tobacco (9%), increased levels of blood glucose (6%) as well as overweight and obesity (5%) (World Health Organization [WHO], 2017). The lack of physical activity increases the prevalence of cardiovascular diseases, diabetes and cancer (Blair, 2009). 21–25% of cases of diagnosed breast and colon cancer are physical inactivity-related. The same applies to 27% of diabetes and almost 30% of ischemic heart disease (World Health Organization [WHO], 2017). Insufficient physical activity is associated with 35 persistent conditions (Booth et al., 2011). “Exercise is Medicine” for 26 different chronic diseases (Pedersen and Saltin, 2015). Therapy exercises are prescribed with respect to psychiatric, metabolic, cardiovascular and pulmonary diseases as well as musculoskeletal disorders and cancer. In the group of dentists, a slightly increased tendency for lung cancer and overall cancer incidence exists (Simning and van Wijngaarden, 2007). Moreover, typically occurring symptoms are reflux, low back pain, headache, neck pain, osteoarthritis as well as rheumatoid and psoriatic arthritis (Nalliah et al., 2017).
In the presented study, 56% of the respondents admitted that their usual therapeutic exercises had a positive effect on their well-being (Table 2). Sharma and Golchha (2011) noted a statistically significant correlation between the number of physical activity sessions and reduction of ailments. These authors observed an improvement in health of 20–80%. Koneru and Tanikonda (2015) in turn, emphasized that yoga is the most effective form of therapy used in the prevention of neck, lumbar and shoulder girdle pain. Yoga helps strengthen the musculoskeletal system, improve flexibility, and release endorphins and hormones (Koneru and Tanikonda, 2015). In the case of dentists, in order to reduce the body’s static load resulting from straining the muscles of the back, neck and shoulders, as well as due to the proper mobilization of the muscles of the lower extremities and the torso, 30 min of daily activity is recommended (Koneru and Tanikonda, 2015). However, studies show that only 39% of dentists do sporting activities on a regular basis (Hashim and Al-Ali, 2013). It means that primary prevention among dentistry students is still required. The same applies to health promotion and a sufficient level of physical activity (Booth et al., 2011).
According to the WHO suggestions, “adults aged 18–64 should do at least 150 min of moderate-intensity aerobic physical activity throughout the week or do at least 75 min of vigorous-intensity aerobic physical activity throughout the week, or an equivalent combination of moderate- and vigorous-intensity activity. Aerobic activity should be performed in bouts of at least 10 min duration. For additional health benefits, adults should increase their moderate-intensity aerobic physical activity to 300 min per week, or engage in 150 min of vigorous-intensity aerobic physical activity per week, or an equivalent combination of moderate- and vigorous-intensity activity. Muscle-strengthening activities should be done involving major muscle groups on 2 or more days a week” (World Health Organization [WHO], 2017). Pursuant to the above-mentioned recommendations, the improvement of cardiorespiratory and muscular fitness as well as bone health are expected after introducing the appropriate amount of exercise. The risk of non-communicable diseases and depression would also be reduced (World Health Organization [WHO], 2017). It must be remembered that these suggestions are for the average population. Due to the specific conditions, physical activity in case of dentists should be tailored individually. For instance, to avoid muscle fatigue associated with the working position, exercises that strengthen the stabilizing muscle are recommended (Akuthota and Nadler, 2004). To provide proper core stability, only 10% of muscle contraction is needed (McGill, 2002). In the lumbar spine, low-intensity isometry and harmony of the deep muscles should be implemented, preferably by core strengthening, i.e., dynamic stability or torso neuromuscular training (McGill, 2002).
The study group declared 22 different types of imaging tests, including computed tomography and magnetic resonance imaging (Table 3). 86.6% of the respondents did not report these types of diagnostics (Table 3). Although most participants declared good health, the observed data is worrying. Perhaps the secondary type of prevention should be considered in dentistry students (Booth et al., 2011). It could mean the implementation of disease detection and management before any symptoms emerge, or the prevention of disability progression (Booth et al., 2011). Monitoring and screening tools play a crucial role in these methods (Booth et al., 2011).
Regarding structural disorders, no osteophytes, syndesmophytes or narrowing of the intervertebral holes were reported (Table 4). These results may suggest the functional nature of the disorder and an early phase of its development. Cases of diagnosed cervical spine instability, hypomobility, whiplash injury, dehydration of intervertebral discs or lowering of vertebral bodies were incidental. Some of them could be explained by trauma or conditioning of the body type. In people with discopathy and loss of cervical lordosis, the third type of prevention should be applied (Booth et al., 2011).
64.28% of the students correctly defined head protraction (Table 5). 13.39% were not familiar with the given terminology. Only 2.68% of the respondents consider protraction as a physiological position (Table 5). A random assessment of the cervical spine loads testified to insufficient job-related health knowledge (Table 5). 26.79% of people declared using a laptop or tablet and reading a book whilst lying on their back, 6.24% used a combination of lying on their back and other positions (Table 6). It should be assumed that lying on the back with a pillow could be a risk factor for pain. The position on the back induces head protraction and cervical spine flexion The range of the symptoms depends on the degree of cervical inclination and coincides with the previous observations of Ariëns et al. (2001). In most cases, this is accompanied by shoulder girdle protraction and increased kyphosis in the thoracic segment. On the other hand, lying on the front facing forward—depending on the situation—can lead to excessive extension in cervical segments. Combined twisting of the trunk in lying on the side, apart from pain symptoms, may contribute to disorders of the functioning of the motor apparatus of the eye and unilateral overload of the musculoskeletal system (Treleaven, 2008).
64.29% of the respondents performed practical tasks with patients or phantoms in the sitting position (Table 7). 26.78% of the students preferred a mixed manner of working (Table 7). No subjects worked with dental assistance, which was conditioned by the possibilities of practical training, including the technical capabilities of most universities. Students’ statements did not seem alarming, but it is difficult to assess whether, apart from the choice alone, the respondents actually properly adopted the declared postures. An incorrect sitting position can cause upper and/or lower crossed syndrome. The upper crossed syndrome is characterized by imbalance between the muscles of the head, neck and shoulder, with increased activity of pectoralis major and minor, trapezius, levator scapulae muscle, deltoid muscle, erector spinae muscles and suboccipital muscles (Kuć and Żendzian-Piotrowska, 2020). In the lower crossed syndrome, increased tension is applied to the iliopsoas, musculus rectus femoris, gastrocnemius, soleus, tibialis posterior, adductors of the thigh, musculus biceps femoris, semitendinosus and semimembranosus muscles, musculus tensor fasciae latae, musculus piriformis, erector spinae within the lumbar and thoracic region and musculus quadratus lumborum. Typical symptoms of this syndrome include weakness of the abdominal muscles (musculus rectus abdominis, musculus transversus abdominis, musculus obliquus abdominis), all gluteus muscles, musculus vastus lateralis et medialis, tibialis anterior and musculus peroneus longus et brevis (Page, 2006). The lower crossed syndrome decreases the corset muscle tone and is typically accompanied by the deepening of lumbar lordosis and the highlighting of the abdominal wall. In both syndromes, therapeutic treatment includes correction of peripheral disorders, restoration of muscle balance as well as improvement in stability and endurance in coordinated motion patterns (Page and Frank, 2007).
82.14% of the respondents used a dental mirror and binocular vision when treating cavities located on the palatal surface of the upper incisors. This may indicate excellent manual skills as well as optimal eye-hand coordination (Table 7). 14.29% of the students preferred direct binocular vision. Most likely these people worked in incorrect positions that forced combined movements of the cervical spine with lateral flexion and rotation as well as extension in the higher and flexion in the lower segments. Perhaps this is the result of insufficient coordination of the eye-hand complex or accompanying vision defects. However, it should be emphasized that extreme positions of the cervical spine may contribute to an increased tension of the suboccipital muscles, which may eventually lead to dysfunction, including the occurrence of myofascial pain. In turn, the use of a dental mirror or its absence in conjunction with monocular vision may cause abnormalities of vision and other problems.
Musculoskeletal symptoms increase stress level and affect physical and psychological condition, thus lowering the quality of life and work (Cherniack et al., 2010). Eighty three percent of dentists experience severe stress in their work (Baran, 2005). Around 60% see their profession as much more stressful than other jobs (Moore and Brødsgaard, 2001). Varela-Centelles et al. (2005) observed that 54.3% of dentists suffered from emotional exhaustion. In 56.6% of cases depersonalization was noted. 6.9% of the dentists demonstrated the lack of personal achievements. With respect to gender, a higher level of depersonalization was reported by males (Brake et al., 2003; Goehring et al., 2005). Myers and Myers (2004) noted that about 60% of dentists felt nervous and depressed. They lived under pressure and had difficulty sleeping. 58.3% of the study participants suffered from headache (Myers and Myers, 2004). 48.2% of the respondents were clearly tired for no apparent reason (Varela-Centelles et al., 2005). In 32% of the examined dentists a high level of minor psychiatric symptoms was noted (Myers and Myers, 2004). Humphris et al. (2002) reported that the level of emotional exhaustion was definitely higher in dentistry adepts than general medicine students. These authors emphasized that the level of stress and psychological disability were associated with the system of dentistry students’ education as well as immediate professional workload during their studies (Humphris et al., 2002).
In the presented study, the multiple linear regression model emphasized the link between Neck Disability Index (NDI), gender, Graded Chronic Pain Scale (GCPS v. 2.0) and Perceived Stress Scale (PSS-10) (Table 8). Regression coefficients highlighted independent contributions of each factor to the global evaluation of NDI (Table 8). GCPS showed a stronger association with NDI than gender and PSS-10 (higher standardized coefficients—β and p-value) (Table 8). PSS-10 remained in the 2nd place.
This model indicated that the risk of neck disability was higher in subjects with increased levels of chronic pain expressed by changes of GCPS v. 2.0., a higher level of perceived stress demonstrated by PSS-10 and females. Jay et al. (2015) reported that increased high amount of stress and musculoskeletal pain led to decreased work ability. Similar observations were noted by Marklund et al. (2020). These authors stressed a strong link between multi-site pain, high stress levels and reduced work productivity (Marklund et al., 2020). Moreover, pain is considered as a strong predictor for persistent stress and the resulting inconveniences in the future (Marklund et al., 2020). Other authors emphasized the connection between high stress levels and chronic facial pain as well as neck and back pain (Linton, 2000; Fillingim et al., 2011; Nevalainen et al., 2017).
The second model of multiple linear regression showed the interplay between the Graded Chronic Pain Scale (GCPS v. 2.0), standing position and the applied physiotherapy. Physiotherapeutic treatment procedures showed a stronger association with GCPS than the standing position (higher standardized coefficients—β and p-value) (Table 9). It means that in the case of dentistry students who declared participation in physiotherapy, higher levels of chronic pain (GCPS v. 2.0) could be expected. Moreover, the standing position during dental procedures decreases the tendency for graded chronic pain. This seems to be in accordance with previously reported observations. Callaghan and McGill (2001) and Dantas and de Lima (2015) demonstrated that complaints within the lower back are more pronounced in the sitting than standing position in dentists. These phenomena may induce fatigue of the deep layer of the erector spinae muscles responsible for maintaining a static position. This is a probable cause of initial back pain and can also be connected with chronic pain (Movahed et al., 2011).
Strengths and Limitations
The results of this study reflect the need for holistic monitoring and screening among dentistry students with respect to job-related health problems. It is already possible to estimate the potential cost and benefits of treating dental occupational hazards in adepts. In each case, evaluation of individual patterns of work ergonomics, necessity for physical activity and cervical physiotherapeutic treatment needs is desirable and practicable. Our observations highlighted the need for primary, secondary and tertiary prevention (Booth et al., 2011). Studying dentistry should be preceded by verification of the risk factors and work load.
Self-reported questionnaires can be directed to a large group of people upon low financial cost. Due to the randomly sampled collection, these methods are often used as a primary screening tool in pilot studies. Bearing in mind that dentistry students are much closer to the aspects of ergonomics, physical activity and work-related musculoskeletal disorders, the information they provide tends to be more reliable. Despite the fact that the protocol used in the study did not contain sensitive questions, it is impossible to exclude the risk of social desirability bias.
Conclusion
A relatively low incidence of structural abnormalities within the cervical spine and a highly diversified distribution of functional disorders exist among dentistry students. 26.79% of them required periodic therapeutic rehabilitation and for 34.82% it was advisable to implement regular physical activity. Due to professional conditions, medical and dental students are exposed to early cervical spine disorders. The priority is to prevent and relieve symptoms of musculoskeletal disorders resulting from long-lasting static positions. The factor influencing an early onset of such dysfunctions is an increased stress. An average level of pro-health awareness may be the reason for elevated cost of rehabilitation among this group of patients. Preventive actions in the workplace, proper physical exercise program as well as education in dental ergonomics should be provided. Due to the small sample of the study size further research is needed on the subject.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. Datasets are available on request.
Ethics Statement
The studies involving human participants were reviewed and approved by the Bioethical Commission of the Medical University of Bialystok, Poland No. R-I-002/513/2017. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
JK developed and planned the study. MŻ-P contributed to the interpretation of the results and supervised the project. JK and MŻ-P participated in the writing of the manuscript. Both authors discussed the results and revised the manuscript, as well as read and approved the submitted version.
Funding
The work was funded by the Medical University of Bialystok, Poland, Grant Number SUB/1/DN/19/003/3330.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Anghel, M., Argeanu, V., Talpo, C., and Lungeanu, D. (2007). Músculoskeletal disorders (MSDS) consequences of prolonged static postures. J. Exp. Med. Surg. Res. 4, 167–172.
Ariëns, G., Bongers, P., Douwes, M., Miedema, M., Hoogendoorn, W., van der Wal, G., et al. (2001). Are neck flexion, neck rotation, and sitting at work risk factors for neck pain? Results of a prospective cohort study. Occup. Environ. Med. 58, 200–207. doi: 10.1136/oem.58.3.200
Baran, R. B. (2005). Myers Briggs Type Indicator, burnout, and satisfaction in Illinois dentists. Gen. Dent. 53, 228–235.
Blair, S. N. (2009). Physical inactivity: the biggest public health problem of the 21st century. Br. J. Sports Med. 43, 1–2.
Blanpied, P. R., Gross, A. R., Elliott, J. M., Devaney, L. L., Clewley, D., Walton, D. M., et al. (2017). Neck pain: revision 2017: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 47, A1–A83.
Bogduk, N. (2001). Cervicogenic headache: anatomic basis and pathophysiologic mechanisms. Curr. Pain Headache Rep. 5, 382–386. doi: 10.1007/s11916-001-0029-7
Booth, F. W., Roberts, C. K., and Laye, M. J. (2011). Lack of exercise is a major cause of chronic diseases. Comp. Physiol. 2, 1143–1211.
Brake, H. T., Bloemendal, E., and Hoogstraten, J. (2003). Gender differences in burnout among Dutch dentists. Commun. Dentistry Oral Epidemiol. 31, 321–327. doi: 10.1034/j.1600-0528.2003.t01-1-00010.x
Callaghan, J., and McGill, S. (2001). Low back joint loading and kinematics during standing and unsupported sitting. Ergonomics 44, 280–294. doi: 10.1080/00140130118276
Campo, M., Weiser, S., Koenig, K. L., and Nordin, M. (2008). Work-related musculoskeletal disorders in physical therapists: a prospective cohort study with 1-year follow-up. Phys. Ther. 88, 608–619. doi: 10.2522/ptj.20070127
Cherniack, M., Dussetschleger, J., and Bjor, B. (2010). Musculoskeletal disease and disability in dentists. Work 35, 411–418. doi: 10.3233/wor-2010-0978
Chohan, L., Dewa, C. S., El-Badrawy, W., and Nainar, S. H. (2020). Occupational burnout and depression among paediatric dentists in the United States. Int. J. Paediatr. Dentistry 30, 570–577. doi: 10.1111/ipd.12634
Dantas, F. F. O., and de Lima, K. C. (2015). The relationship between physical load and musculoskeletal complaints among Brazilian dentists. Appl. Ergon. 47, 93–98. doi: 10.1016/j.apergo.2014.09.003
Diaz-Caballero, A.-J., Gómez-Palencia, I.-P., and Díaz-Cárdenas, S. (2010). Ergonomic factors that cause the presence of pain muscle in students of dentistry. Med. Oral Patol. Oral Cir. Bucal. 15:e906. doi: 10.4317/medoral.15.e906
Fasunloro, A., and Owotade, F. J. (2004). Occupational hazards among clinical dental staff. J. Contemp. Dent. Pract. 5, 134–152. doi: 10.5005/jcdp-5-2-134
Fillingim, R. B., Ohrbach, R., Greenspan, J. D., Knott, C., Dubner, R., Bair, E., et al. (2011). Potential psychosocial risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J. Pain 12, T46–T60.
Freudenberger, H. J. (1974). Staff burn-out. J. Soc. Issues 30, 159–165. doi: 10.1111/j.1540-4560.1974.tb00706.x
Goehring, C., Gallacchi, M. B., Kunzi, B., and Bovier, P. (2005). Psychosocial and professional characteristics of bournout in Swiss primary care practitioners: a cross-sectional survey. Swiss Med. Wly. 135, 101–108.
Gorter, R. C., Eijkman, M. A., and Hoogstraten, J. (2000). Burnout and health among Dutch dentists. Eur. J. Oral Sci. 108, 261–267. doi: 10.1034/j.1600-0722.2000.108004261.x
Hakanen, J. J., and Schaufeli, W. B. (2012). Do burnout and work engagement predict depressive symptoms and life satisfaction? A three-wave seven-year prospective study. J. Affect. Disord. 141, 415–424. doi: 10.1016/j.jad.2012.02.043
Hashim, R., and Al-Ali, K. (2013). Health of dentists in U nited A rab E mirates. Int. Dent. J. 63, 26–29.
Honkonen, T., Ahola, K., Pertovaara, M., Isometsä, E., Kalimo, R., Nykyri, E., et al. (2006). The association between burnout and physical illness in the general population—results from the Finnish Health 2000 Study. J. Psychos. Res. 61, 59–66. doi: 10.1016/j.jpsychores.2005.10.002
Huang, Q., Li, D., Zhang, J., Yang, D., Huo, M., and Maruyama, H. (2014). Comparison of the efficacy of different long-term interventions on chronic low back pain using the cross-sectional area of the multifidus muscle and the thickness of the transversus abdominis muscle as evaluation indicators. J. Phys. Ther. Sci. 26, 1851–1854. doi: 10.1589/jpts.26.1851
Humphris, G., Blinkhorn, A., Freeman, R., Gorter, R., Hoad-Reddick, G., Murtomaa, H., et al. (2002). Psychological stress in undergraduate dental students: baseline results from seven European dental schools. Eur. J. Dent. Educ. 6, 22–29. doi: 10.1034/j.1600-0579.2002.060105.x
Jay, K., Friborg, M. K., Sjøgaard, G., Jakobsen, M. D., Sundstrup, E., Brandt, M., et al. (2015). The consequence of combined pain and stress on work ability in female laboratory technicians: a cross-sectional study. Int. J. Environ. Res. Public Health 12, 15834–15842. doi: 10.3390/ijerph121215024
Koneru, S., and Tanikonda, R. (2015). Role of yoga and physical activity in work-related musculoskeletal disorders among dentists. J. Int. Soc. Prevent. Commun. Dent. 5, 199–204. doi: 10.4103/2231-0762.159957
Kuć, J., and Żendzian-Piotrowska, M. (2020). A pilot study evaluating the prevalence of cervical spine dysfunction among students of dentistry at the medical university. Front. Neurol. 11:200. doi: 10.3389/fneur.2020.00200
Leggat, P., and Smith, D. (2006). Musculoskeletal disorders self-reported by dentists in Queensland. Austral. Austral. Dent. J. 51, 324–327. doi: 10.1111/j.1834-7819.2006.tb00451.x
Letafatkar, A., Rabiei, P., Alamooti, G., Bertozzi, L., Farivar, N., and Afshari, M. (2019). Effect of therapeutic exercise routine on pain, disability, posture, and health status in dentists with chronic neck pain: a randomized controlled trial. Int. Arch. Occup. Environ. Health 93, 281–290. doi: 10.1007/s00420-019-01480-x
Linton, S. J. (2000). A review of psychological risk factors in back and neck pain. Spine 25, 1148–1156. doi: 10.1097/00007632-200005010-00017
Marklund, S., Mienna, C. S., Wahlström, J., Englund, E., and Wiesinger, B. (2020). Work ability and productivity among dentists: associations with musculoskeletal pain, stress, and sleep. Int. Arch. Occup. Environ. Health 93, 271–278. doi: 10.1007/s00420-019-01478-5
Maslach, C., and Jackson, S. (1981). The measurement of experienced burnout. J. Occup. Behav. 2, 99–113. doi: 10.1002/job.4030020205
McAviney, J., Schulz, D., Bock, R., Harrison, D. E., and Holland, B. (2005). Determining the relationship between cervical lordosis and neck complaints. J. Manipulat. Physiol. Ther. 28, 187–193. doi: 10.1016/j.jmpt.2005.02.015
McGill, S. (ed.) (2002). “Lumbar spine stability: myths and realities,” in Low Back Disorders: Evidence-Based Prevention and Rehabilitation, (Champaign, IL: Human Kinetics), 137–146.
Moodley, R., Naidoo, S., and van Wyk, J. (2018). The prevalence of occupational health-related problems in dentistry: a review of the literature. J. Occup. Health 60, 111–125. doi: 10.1539/joh.17-0188-ra
Moore, R., and Brødsgaard, I. (2001). Dentists’ perceived stress and its relation to perceptions about anxious patients. Commun. Dent. Oral Epidemiol. 29, 73–80. doi: 10.1034/j.1600-0528.2001.00011.x
Movahed, M., Ohashi, J.-Y., Kurustien, N., Izumi, H., and Kumashiro, M. (2011). Fatigue sensation, electromyographical and hemodynamic changes of low back muscles during repeated static contraction. Eur. J. Appl. Physiol. 111, 459–467. doi: 10.1007/s00421-010-1660-y
Myers, H., and Myers, L. (2004). ’It’s difficult being a dentist’: stress and health in the general dental practitioner. Br. Dent. J. 197, 89–93. doi: 10.1038/sj.bdj.4811476
Nalliah, R. P., Budd, A., and Allareddy, V. (2017). Pilot survey of the health of Massachusetts dentists. J. Investig. Clin. Dent. 8:e12263. doi: 10.1111/jicd.12263
Nevalainen, N., Lähdesmäki, R., Mäki, P., Ek, E., Taanila, A., Pesonen, P., et al. (2017). Association of stress and depression with chronic facial pain: a case-control study based on the Northern Finland 1966 Birth Cohort. CRANIO® 35, 187–191. doi: 10.1080/08869634.2016.1193960
Newell, T. M., and Kumar, S. (2005). Comparison of instantaneous and cumulative loads on the low back and neck in orthodontists. Clin. Biomech. 20, 130–137. doi: 10.1016/j.clinbiomech.2004.09.011
O’Connell, M. E., Boat, T., and Warner, K. E. (2009). Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. Washington, DC: National Academies Press.
Olivo, S. A., Fuentes, J., Major, P., Warren, S., Thie, N., and Magee, D. (2010). The association between neck disability and jaw disability. J. Oral Rehabil. 37, 670–679. doi: 10.1111/j.1365-2842.2010.02098.x
Page, P. (2006). Sensorimotor training: a “global” approach for balance training. J. Bodywork Mov. Ther. 10, 77–84. doi: 10.1016/j.jbmt.2005.04.006
Page, P., and Frank, C. (2007). The Janda Approach to Chronic Musculoskeletal Pain. Akron: Thera Band Academy.
Panagioti, M., Geraghty, K., Johnson, J., Zhou, A., Panagopoulou, E., Chew-Graham, C., et al. (2018). Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern. Med. 178, 1317–1331. doi: 10.1001/jamainternmed.2018.3713
Pedersen, B. K., and Saltin, B. (2015). Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 25, 1–72. doi: 10.1111/sms.12581
Presoto, C. D., and Garcia, P. P. N. S. (2016). Risk factors for the development of musculoskeletal disorders in dental work. J. Educ. Soc. Behav. Sci. 15, 1–6. doi: 10.9734/bjesbs/2016/25838
Rising, D. W., Bennett, B. C., Hursh, K., and Plesh, O. (2005). Reports of body pain in a dental student population. J. Am. Dent. Assoc. 136, 81–86. doi: 10.14219/jada.archive.2005.0032
Sharma, P., and Golchha, V. (2011). Awareness among Indian dentist regarding the role of physical activity in prevention of work related musculoskeletal disorders. Indian J. Dent. Res. 22:381. doi: 10.4103/0970-9290.87057
Simning, A., and van Wijngaarden, E. (2007). Literature review of cancer mortality and incidence among dentists. Occup. Environ. Med. 64, 432–438. doi: 10.1136/oem.2006.029223
Suciu, A., Repanovici, A., Cotoros, D., Druga, C., and Serban, I. (2019). Experimental device for monitoring dentists’ posture during work. Proc. Manuf. 32, 596–599. doi: 10.1016/j.promfg.2019.02.258
Treleaven, J. (2008). Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control—part 2: case studies. Manual Ther. 13, 266–275. doi: 10.1016/j.math.2007.11.002
Valachi, B., and Valachi, K. (2003a). Mechanisms leading to musculoskeletal disorders in dentistry. J. Am. Dent. Assoc. 134, 1344–1350. doi: 10.14219/jada.archive.2003.0048
Valachi, B., and Valachi, K. (2003b). Preventing musculoskeletal disorders in clinical dentistry: strategies to address the mechanisms leading to musculoskeletal disorders. J. Am. Dent. Assoc. 134, 1604–1612.
Varela-Centelles, P., Fontao, L. V., Martínez, A. G., Pita, A. B., and Valín, M. L. (2005). Professional burnout in dentists and stomatologists of the galician health service. Atencion Primaria 35, 301–305.
Verbunt, J. A., Smeets, R. J., and Wittink, H. M. (2010). Cause or effect? Deconditioning and chronic low back pain. Pain 149, 428–430. doi: 10.1016/j.pain.2010.01.020
Keywords: burnout, dentistry, ergonomics, health needs, physical activity, stress, well-being
Citation: Kuć J and Żendzian-Piotrowska M (2020) Evaluation of the Cervical Physiotherapeutic Treatment Needs, Work Ergonomics, and Necessity for Physical Activity Among Students of Dentistry at a Medical University. A Pilot Study. Front. Psychol. 11:559657. doi: 10.3389/fpsyg.2020.559657
Received: 06 May 2020; Accepted: 24 September 2020;
Published: 22 October 2020.
Edited by:
Bernadette Ann Murphy, Ontario Tech University, CanadaReviewed by:
Maria António Castro, Coimbra School of Health Technology, PortugalMahboobeh Zabihhosseinian, Ontario Tech University, Canada
Copyright © 2020 Kuć and Żendzian-Piotrowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joanna Kuć, a3Vjam9hbm5hQHBvY3p0YS5vbmV0LnBs