 Eleonora Topino
Eleonora Topino Alessio Gori
Alessio Gori Holger Cramer
Holger Cramer- 1Department of Human Science, LUMSA University, Rome, Italy
- 2Department of Health Sciences, University of Florence, Florence, Italy
- 3Department of Internal and Integrative Medicine, Evang. Kliniken Essen-Mitte, Faculty of Medicine, University of Duisburg-Essen, Essen, Germany
Postural awareness (PA) refers to a subjective conscious awareness of body posture and falls within the framework of mind–body integration. The aim of this research was to validate and evaluate psychometric properties of the Postural Awareness Scale (PAS) in an Italian population sample (n = 928; 45.04% men and 54.96% women; mean age = 29.96 years, standard deviation = 11.44). The results obtained with Velicer’s Minimum Average Partial Test, Horn’s Parallel Analysis, and exploratory factor analysis showed a two-factor solution, as supported by the confirmatory factor analysis: ease/familiarity with postural awareness and need for attention regulation with postural awareness. Furthermore, the findings highlighted both a good internal consistency (α = 0.76 for the total scale and α = 0.80, α = 0.79 for the two subscales) and a satisfactory construct validity. Furthermore, multivariate analysis of variance was carried out to assess differences in PA between specific subgroup. In particular, the positive effects of physical activity and healthy body weight were confirmed, whereas no significant differences related to gender or age were found. All these findings suggest that the Italian version of the PAS is a rapid instrument with good psychometric properties, which can be useful both for research and clinical practice.
Introduction
The postural awareness is “the subjective conscious awareness of body posture that is mainly based on proprioceptive feedback from the body periphery to the central nervous system” (Cramer et al., 2018b, paragraph 1). It is a fundamental element for controlling posture in a process of adaptation based on sensory, motor, and cognitive aspects (Balasubramaniam and Wing, 2002). The body posture, in fact, can be influenced by a certain number of conditioning factors: mechanical aspects, heredity, race, flexibility, muscular strength, vision, and habits, but it is also involved in relationships of mutual interdependence with emotional and psychological factors (Brito, 1995; Wright et al., 2000). The scientific literature confirms the close relationship between posture and psychological dimensions, as demonstrated in several studies concerning assertiveness levels and action trends (e.g., Maner et al., 2010; Huang et al., 2011; Arnette and Pettijohn, 2012; Van der Toorn et al., 2015), self-efficacy (Anderson and Galinsky, 2006), self-esteem (Stepper and Strack, 1993; Dijkstra et al., 2007; Kwon and Kim, 2015), and mood (Hackford et al., 2019). These findings fall within a framework of mind–body interaction supported by different lines of research. The field of trauma studies, for example, increasingly focuses on this reciprocal influence, describing somatically driven individuals, with strong emotions accompanied by dysregulated physical sensations: these activations derive from reminders to previous adverse experiences that were not elaborated and repeated in the body (Van Der Kolk, 2014; Fisher, 2017). Furthermore, trauma affects self-awareness, specifically the sensory one (Bluhm et al., 2009), and alters the “postural body scheme” (Gurfinkel, 1994), involved in the perception of self with respect to the external world and in the actions directed to it. All this seriously alters the psychological perception of being able to manage one’s life, which is closely linked to the possibility of experiencing control of the physical sphere (Van Der Kolk, 2008). Therefore, maintaining or increasing one’s postural awareness levels allows the management of one’s “postural body scheme,” developing more adaptive attitudes through reflection and intention (Massion, 1994). Thus, the vision of James Grotstein (1997) who spoke of the mind and the body as a “strangely coupled unity” appears pertinent. He depicts them in a single entity with two inseparable aspects, like two sides of the same coin: they are considered like two different categories dependent on the perspective of the observer (Solano, 2010). In this theoretical framework, body awareness and mindfulness are parallel to the construct of postural awareness and strongly associated with it.
Body awareness concerns attention to bodily sensations and implies access to consciousness of proprioceptive (including posture) and interoceptive aspects (Mehling et al., 2009). It allows the participation of bodily sensations in everyday life and the observation of changes and physical responses to emotions and environment. It finds a good application and positive feedback in many contexts of clinical care such as, for example, those for recovery from physical and/or psychological traumas (Herman, 1992; Bishop et al., 2004), for substance abuse (Marlatt and Ostafin, 2005), for eating disorders (Zerbe, 1995), and for personality disorders (Friis et al., 1989). On the contrary, the concept of bodily dissociation is characterized by the avoidance of inner experience (Price and Thompson, 2007); it could represent a protective strategy against painful memories, thoughts, or feelings and is a mechanism commonly used for defense against physical suffering (Bakal, 2001) and trauma (Van der Kolk, 2006).
Closely associated, mindfulness is an awareness of the present moment with total acceptance of it (Brown and Ryan, 2003). Mindfulness intertwines focused attention with meta-awareness, allowing deep insight and clarifying the nature of the elements that constitute the experience (Wallace, 2006). This presence disposition is closely connected to higher levels of physical and mental health, better postural control through the conscious management of attentional focus (Kee et al., 2012), and more likely to maintain healthy habits such as sufficient sleep (Roberts and Danoff-Burg, 2010), physical activity (Murphy et al., 2012), and healthy eating (Gilbert and Waltz, 2010).
In this frame of mind–body relationship, postural awareness has still been little investigated, even though it is related to other important constructs explored above. Some studies support its effectiveness in chronic pain situations: in this field, considering the impact of this condition on people’s lives and the psychological difficulties that ensue, new treatment models have been developed based on the association of physical experiences to states of greater awareness and mindfulness (Mattsson, 1998; Rosberg, 2000). Specifically, postural awareness training has proved particularly effective for chronic low back pain conditions (Moseley et al., 2004; Ahmed et al., 2016). These favor the control of one’s physical disposition and the maintenance of healthy postural patterns in everyday life, important elements to avoid chronicization and further deterioration (Cramer et al., 2018b); a faulty posture, in fact, increases stress on muscles, tendons, ligaments, and bones (Yamak et al., 2018).
The Postural Awareness Scale: A Measure of Body Posture Awareness
The Postural Awareness Scale (PAS) is a German self-report measure designed by Cramer et al. (2018b), which allowed them to grasp the increases of this variable on subjects with chronic pain following the implementation of a multimedia mind–body training program. In particular, they found that improvements in body posture awareness were longitudinally associated with reduced pain in patients with spinal/shoulder pain, in line with other research on this topic (e.g., Lauche et al., 2017). The scale consists of 12 items, grouped into two factors (explaining the 58.8% of the variance in the original study); the first one is “ease/familiarity with postural awareness,” which refers to an effortless awareness and connectedness; the second factor is “need for attention regulation with postural awareness” and indicates a forced awareness. The original scale and both its factors demonstrated satisfactory internal consistency and good validity converging with other measures related to body awareness and mindfulness. Specifically, the subscale ease/familiarity with postural awareness showed important associations with the measures related to the connection with one’s body (Cramer et al., 2018b), significantly correlating with the scores of the Body Awareness Questionnaire (BAQ; Shields et al., 1989), of the trust in bodily sensations subscale [Body Responsiveness Questionnaire (BRS); Daubenmier, 2005; Cramer et al., 2018a], and of the Conscious Presence and Self-Control scale (Büssing et al., 2013). The need for attention regulation with postural awareness subscale, on the other hand, did not significantly correlate with the BAQ, but showed a relevant association with the BRS Perceived Connection between Mental and Physical Process subscale, reflecting the need to strive for achieving or maintaining a link between cognitive process and bodily needs. To conclude, both factors were also significantly correlated to the subscales of the Dresden Body Image Inventory (Pöhlmann, 2014), indicating the association between high levels of posturalawareness and a more positive attitude toward one’s body and appearance.
Rationale for the Study
Further studies on postural awareness would add useful contributions to the mind–body integration perspective, with possible positive repercussions in the field of psychological and psychotherapeutic intervention. The scientific literature shows the efficacy of some interventions for the improvement of posture aspects such as balance (Wayne et al., 2004; Kee et al., 2012), coordination (Jay et al., 2013), control (Pluchino et al., 2012), and awareness (Roll et al., 2002). However, up to now, particularly complex (Barrus, 1996; Aminian and Najafi, 2004) and/or hardly usable outside the laboratory setting (Lanningham-Foster et al., 2005; Wong et al., 2007) tools have been used to measure these outcomes. With the exception of PAS, no self-report tools have been found to allow a more agile assessment of subjective postural awareness (Cramer et al., 2018b). The simplicity of this self-administered scale would enable a measurement of postural awareness in the absence of technical devices and within a psychological setting.
The aim of the present research is the validation (and evaluation of psychometric properties) of the Italian PAS, originally created in German by Cramer et al. (2018b), to allow its use in research and clinical practice. In light of the excellent psychometric characteristics of the original instrument, we hypothesize to obtain an Italian version with a good internal coherence and a similar and equally good factor structure.
Materials and Methods
Participants
The study involved 928 individuals (45.04% men and 54.96% women) with an age ranging from 18 to 77 years (mean = 29.96, standard deviation = 11.44). The sample included participants from Northern (37.50%), Central (32.54%), and Southern (29.96%) Italy. Most individuals were unmarried (71.55% single). Of the 928 participants, 456 (49.14%) were students, and 255 (27.48%) were employed; 44.61% of them held a secondary school diploma, 27.37% a bachelor’s, and 19.83% a master’s degree; 48.28% of the sample was Catholic Christian, and 45.37% was atheist. Three hundred seventy-four participants (40.30%) did not practice any type of sports, whereas 260 (28.02%) trained in the gym (Table 1).
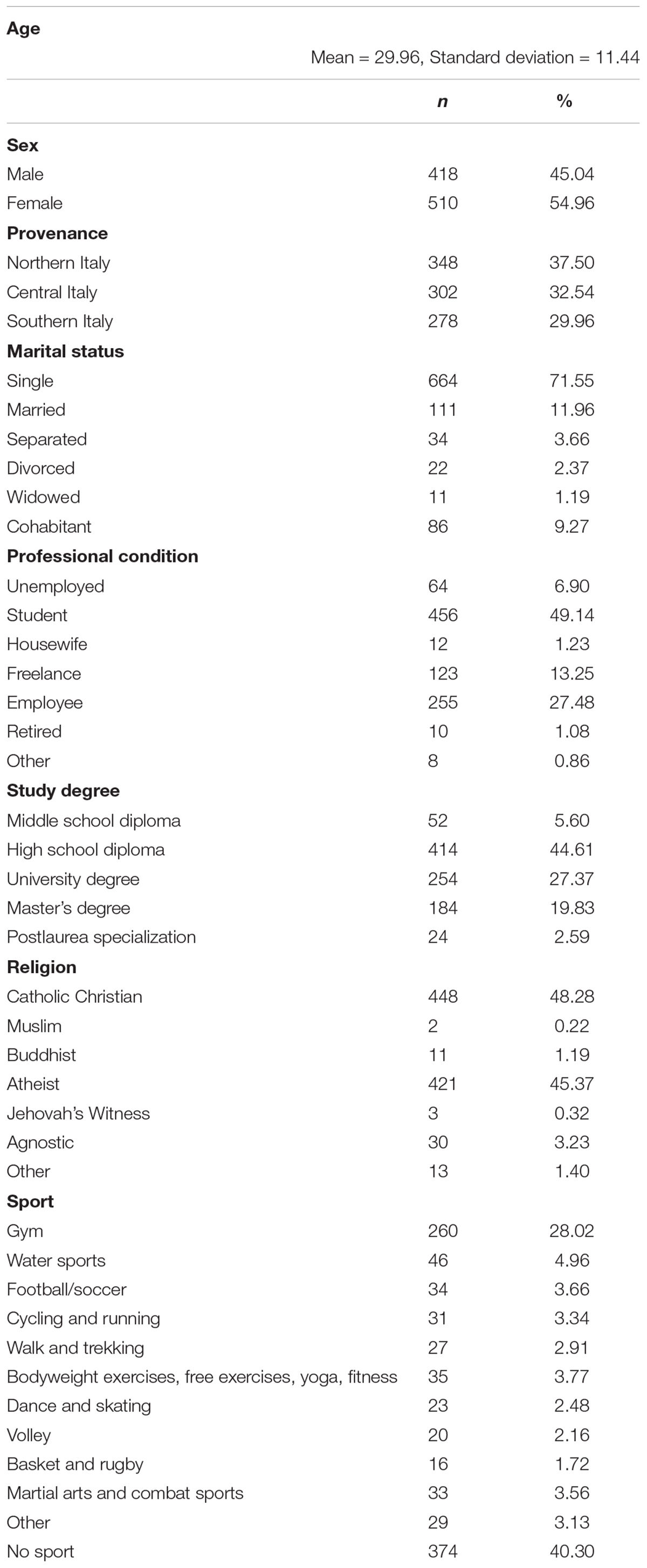
Table 1. Demographics variables of the sample (N = 928).
Procedures
Items of the original version of the PAS have been translated into Italian by a native German speaker living in Italy. Then, the Italian version was back-translated by a bilingual Italian German teacher, and the outcome was submitted to the author of the original measure, with the help of which the remaining inaccuracies were corrected. The researchers compared the translated version with the original text until a consensus on cross-language equivalence was reached. The participants were recruited on the internet with an anonymous link spread through a snowball-like procedure, and the presence of psychological or orthopedic issues was adopted as criteria for exclusion from the sample. All the subjects were informed about the aim of the research and gave written informed consent in accordance with the Declaration of Helsinki. The self-report measures together with a demographic questionnaire (i.e., age, sex, weight, height) were administered to participants, who did not take any compensation for their involvement in the study. The subjects were guaranteed privacy and anonymity.
Measures
Postural Awareness Scale
The PAS is a brief self-report measure designed to assess awareness of body posture (Cramer et al., 2018b), and it consists of 12 items scored on a 7-point scale anchored by 1 (not at all true for me) and 7 (very true for me). Results supported the internal consistency of the original German PAS, with a Cronbach α of 0.80 for the total scale and 0.81 and 0.77 for the two subscales (ease/familiarity with postural awareness e need for attention regulation with postural awareness, respectively). The scale scores range from 12 to 84, with higher scores being indicative of greater postural awareness. The scores were computed by adding up the answers to all the items, after reversing the values of items 1, 2, 3, 4, 5, and 12. In this study, an Italian version obtained by a back-translation process was used.
Body Image Concern Inventory
The Body Image Concern Inventory (BICI) is a self-report measure for assessing experiences related to dysmorphic concern (Littleton et al., 2005). In this study, the Italian version of the BICI (I-BICI; Luca et al., 2011) was used. It consists of 19 items divided into two subscales: dysmorphic symptoms and symptom interference. Response categories ranged from 1 (never) to 5 (always), and the scale scores range from 19 to 95. The aspects investigated were dissatisfaction and concern about appearance, checking and camouflaging behavior, reassurance seeking, social concerns, and avoidance related to appearance. In this sample, the I-BICI possesses good internal consistency, with a Cronbach α of 0.92 and 0.76 for the two subscales and α = 0.93 for the total scale.
Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (RSES) is a 10-item self-report questionnaire designed for assessing global self-esteem with items answered on a 4-point scale from strongly agree to strongly disagree (Rosenberg, 1965). The scale scores range from 0 to 30, in which scores between 15 and 25 are within normal range, whereas scores less than 15 suggest low self-esteem. In this study, the Italian version of the RSES (Prezza et al., 1997), showing good internal consistency (α = 0.90), was used.
General Self-Efficacy Scale
The General Self-Efficacy Scale (GSE) is a self-report measure of self-beliefs to cope with a variety of difficult demands in life (Schwarzer and Jerusalem, 1995). It consists of 10 items scored on a 4-point scale anchored by 1 (not at all true for me) and 4 (very true for me). The scale scores range from 10 to 40, with higher scores being indicative of a sense of personal competence in stressful situations. In this sample, the Italian versions of the GSE (Sibilia et al., 1995) showed a high internal consistency (α = 0.90).
Body Awareness Questionnaire
The BAQ is an 18-item self-report questionnaire designed to assess the sensitivity to normal and non-emotional body processes (Shields et al., 1989). Each item on the measure is rated on a 7-point scale ranging from 1 (not at all true for me) to 7 (very true for me). In this study, the Italian translation of BAQ (Shields et al., 1989; for the Italian version Cardinali, unpublished manuscript) possesses good internal consistency with a Cronbach α of 0.88.
West Haven–Yale Multidimensional Pain Inventory – Short Version
The West Haven–Yale Multidimensional Pain Inventory (WHYMPI-S) is a self-report measure designed to examine the impact of chronic pain on patients’ lives, quality of social support, and general activities (Kerns et al., 1985). In the present study, a short version of this measure was used: five items (2, 8, 9, 12, 19) of the 52 taken from the Italian version (Ferrari et al., 2000), showing a good internal consistency (α = 0.87), were readapted. The selected items evaluated interference in daily life, changes in the ability to participate in recreational and social activities, in the level of satisfaction deriving from involvement in family activities, in the level of suffering, and in friendship. Responses were on a 5-point Likert scale, and higher scores indicated higher levels of suffering and impact of chronic pain.
20-Item Toronto Alexithymia Scale
The 20-item Toronto Alexithymia Scale (TAS-20) is a well-known 20-item questionnaire, scored on a 1- to 5-point Likert scale, which assesses the level of alexithymia (Bagby et al., 1994). The scale measures three main dimensions: (1) difficulty in identifying feelings and distinguishing between feelings and bodily sensations in emotional activation, (2) difficulty in the verbal expression of emotions, and (3) externally oriented thinking. In this sample, the Italian version of the TAS-20 (Bressi et al., 1996), showing a good internal consistency with a Cronbach α of 0.86 for the total score (α = 0.84, 0.79, 0.65 for the subscales), was used.
Beck Depression Inventory II
The Beck Depression Inventory II (BDI-II) is a 21-item self-report multiple-choice inventory designed to assess the intensity of depression (Beck et al., 1996). Response categories range from 1 to 3, and the scale scores range from 0 to 63. It is composed of two subscales: a cognitive–affective and a somatic–performance subscale. In this study, the Italian translation of BDI-II (Ghisi et al., 2006) possesses high internal consistency with a Cronbach α of 0.91 for the total score (α = 0.84 and 0.88 for the subscales).
Mindfulness Attention Awareness Scale
The Mindfulness Attention Awareness Scale (MAAS) is a self-report measure designed to assess present attention and awareness (Brown and Ryan, 2003). In this study, the Italian version of the MAAS (Veneziani and Voci, 2015) was used. It includes 15 items to be rated on a 7-point Likert scale from 1 (almost always) to 7 (almost never), with higher scores being indicative of greater mindfulness. In this sample, the Italian version possesses a good internal consistency (α = 0.87).
Modified Somatic Perception Questionnaire
The Modified Somatic Perception Questionnaire (MSPQ) is a self-report measure of somatic and autonomic perceptions (Main, 1983). In this study, the Italian translation of MSPQ (Conti, 1999) was used. It consists of 22 items scored on a 0- to 4-point Likert scale, 13 of which are used for the final score (the others have a masking function). In the present sample, the Italian version possesses a good internal consistency (α = 0.85).
Data Analysis
All the statistical analyses were performed using the software SPSS 25.0 for Windows (IBM Corp, 2017, Armonk, NY, United States) and MPlus Version 8.1 (Muthén and Muthén, 1998–2017). Descriptive statistics were examined. To test the factor structure of the Italian PAS, the sample was randomly split. On the first subsample, Velicer’s Minimum Average Partial Test (MAP), Horn’s Parallel Analysis (HPA), and an exploratory factor analysis (EFA) with principal axis factoring extraction method (Promax rotation) were performed. Then, the factor structure was verified with a confirmatory factor analysis (CFA) on the second subsample, using the following fit indices: (1) the model χ2, which indicates a good model fit when p > 0.05 (Hooper et al., 2008); (2) the goodness-of-fit statistic (GFI), with recommended values ≥ 0.95 (Hooper et al., 2008); (3) the non-normed fit index (NNFI) with recommended values ≥ 0.95 (Hu and Bentler, 1999); (4) the comparative fit index (CFI), for which the recommended values are ≥ 0.95, although values between 0.90 and 0.95 indicate reasonable fit (Kline, 2005); (5) the root mean square error of approximation (RMSEA), with recommended values ≤0.05, although values up to 0.08 represent reasonable errors of approximation (Marsh et al., 2004); (6) the standardized root mean square residual, with recommended values ≤0.08 (Hooper et al., 2008; Hu and Bentler, 1999). After that, the reliability of the scale was calculated both with the Cronbach α coefficient and item-total correlation indices. In order to assess some aspects of construct validity, Pearson correlation was calculated between PAS, I-BICI, RSES, GSE, BAQ, WHYMPI-S, TAS-20, BDI-II, MAAS, and MSPQ. The choice of these measures was driven by the observation that there are no other self-report questionnaires for the assessment of postural awareness: measures evaluating aspects of awareness and somatic perceptions were therefore included. Moreover, as for large samples even low correlations could be significant, greater precision was searched in the evaluation of the discriminating validity of the two subscales of the PAS, by implementing a correlation coefficients comparison according to Meng et al. (1992). Finally, to assess the differences between specific subgroups, the multivariate analysis of variance (MANOVA) was carried out, by simultaneously entering all the background variables [gender, age, practice of sport, body mass index (BMI)] as fixed factors in a multivariate general linear model. Separate follow-up ANOVAs were conducted for the dependent variables when it was necessary, and post hoc analyses using Scheffé test were performed to support the interpretation of the differences between averages where needed.
Results
Descriptive Statistics
The descriptive statistics of the sample were reported in Table 1. The mean values of the PAS items ranged from 2.69 to 5.61 (Table 2).
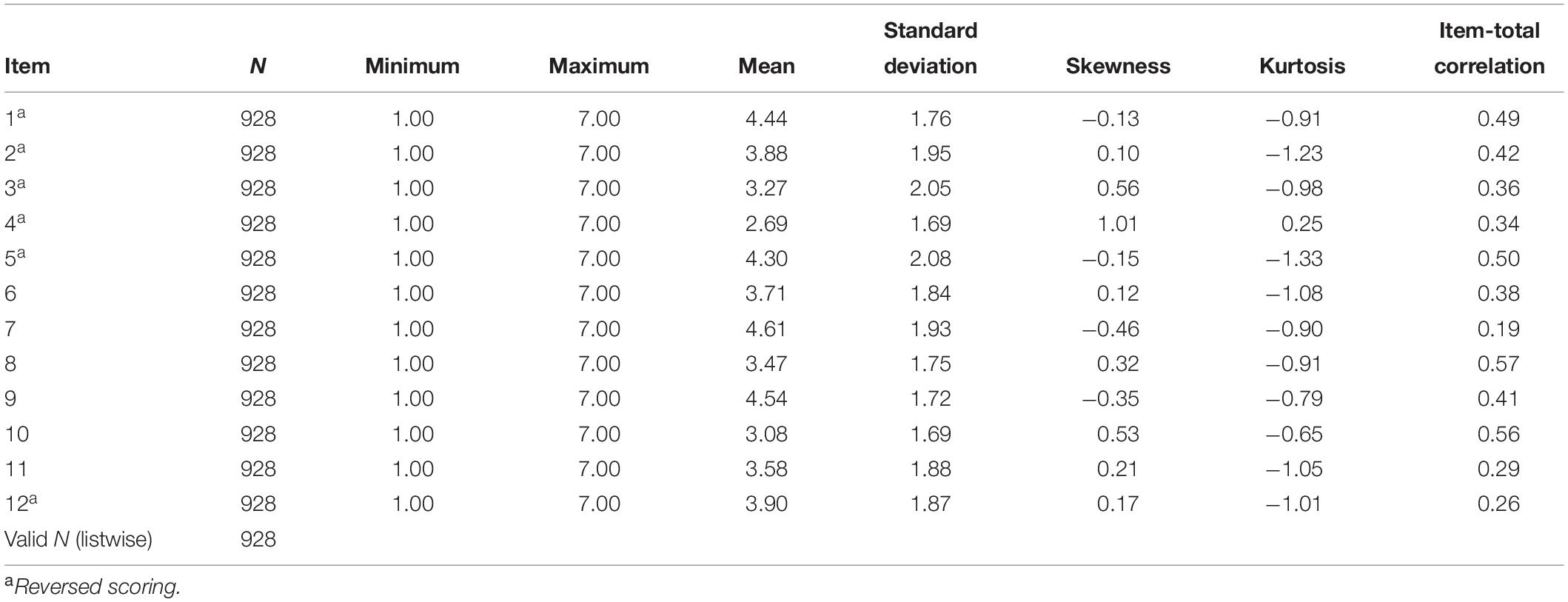
Table 2. Descriptive statistics and item-total correlations of each of the Italian PAS items.
Factor Structure of the Italian PAS
First, in accordance with O’connor (2000), the MAP and HPA were carried out (Table 3). Both the original MAP (Velicer, 1976) and the revised MAP (Velicer et al., 2000) suggested the retention of two factors, as well as the HPA (Horn, 1965).
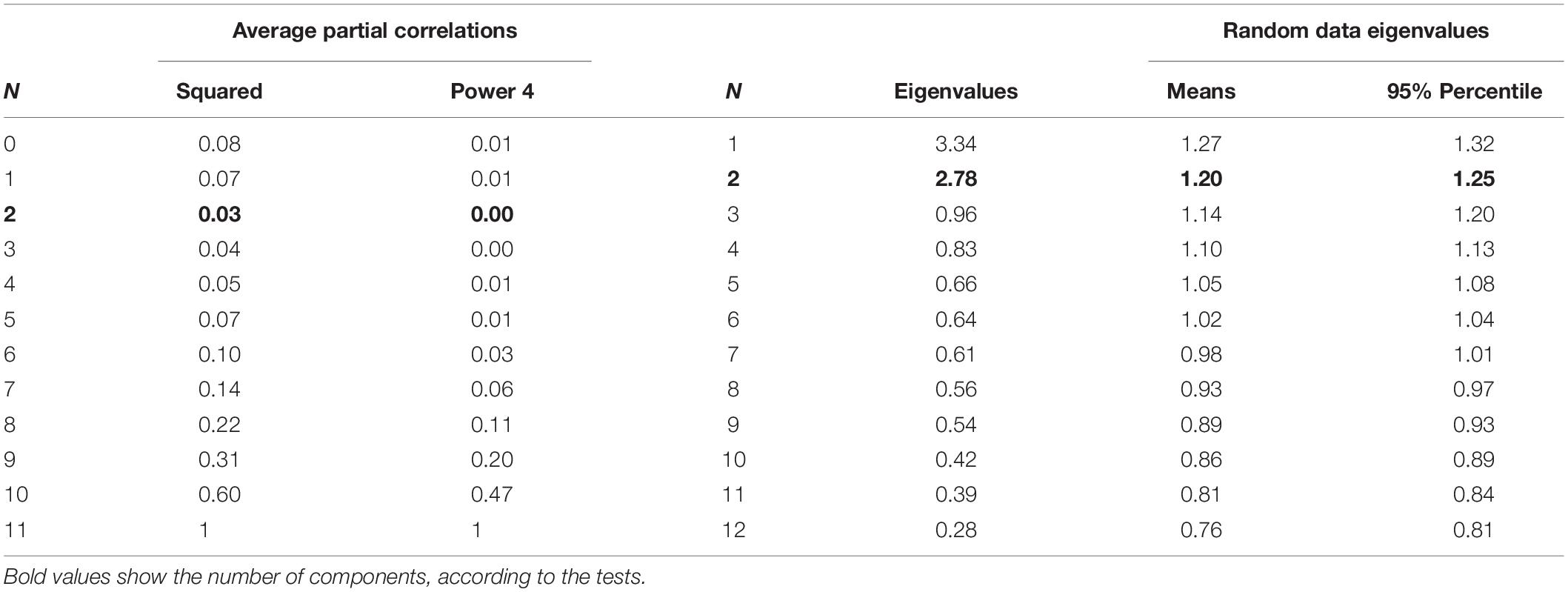
Table 3. MAP test and parallel analysis results for the number of components.
Furthermore, an EFA with principal axis factoring extraction method (Promax rotation) yielded two interpretable factors, which explained 51.00% of the total variance (Table 4 and Figure 1). The first factor (ease/familiarity with postural awareness) was made up of six items related to high postural awareness without effort and accounted for 27.82% of the total variance. The second factor (need for attention regulation with postural awareness) consisted of six items related to high efforts required to be aware of their own body posture; it accounted for 23.18% of the total variance.
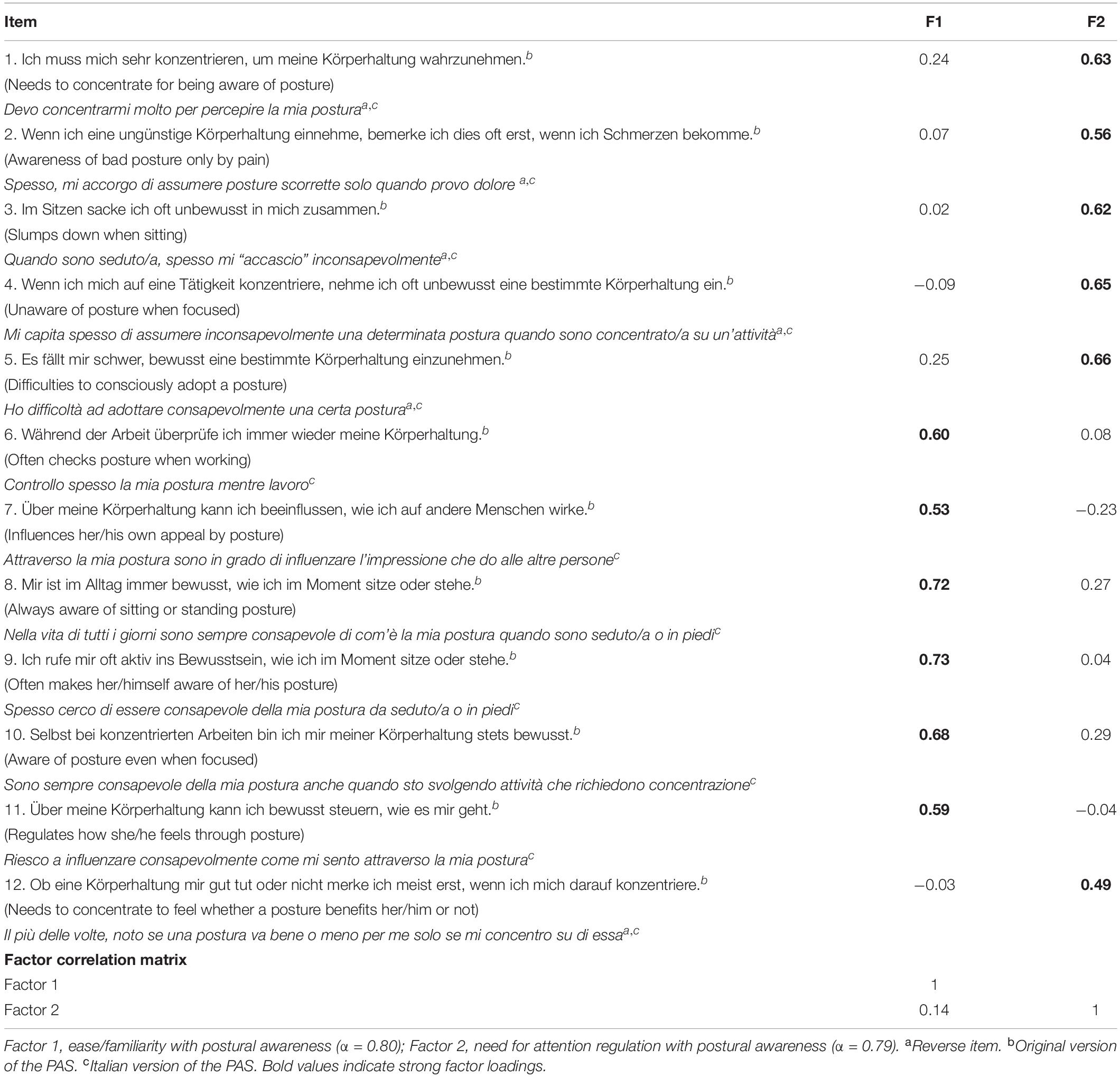
Table 4. Factor structure of the Italian PAS.
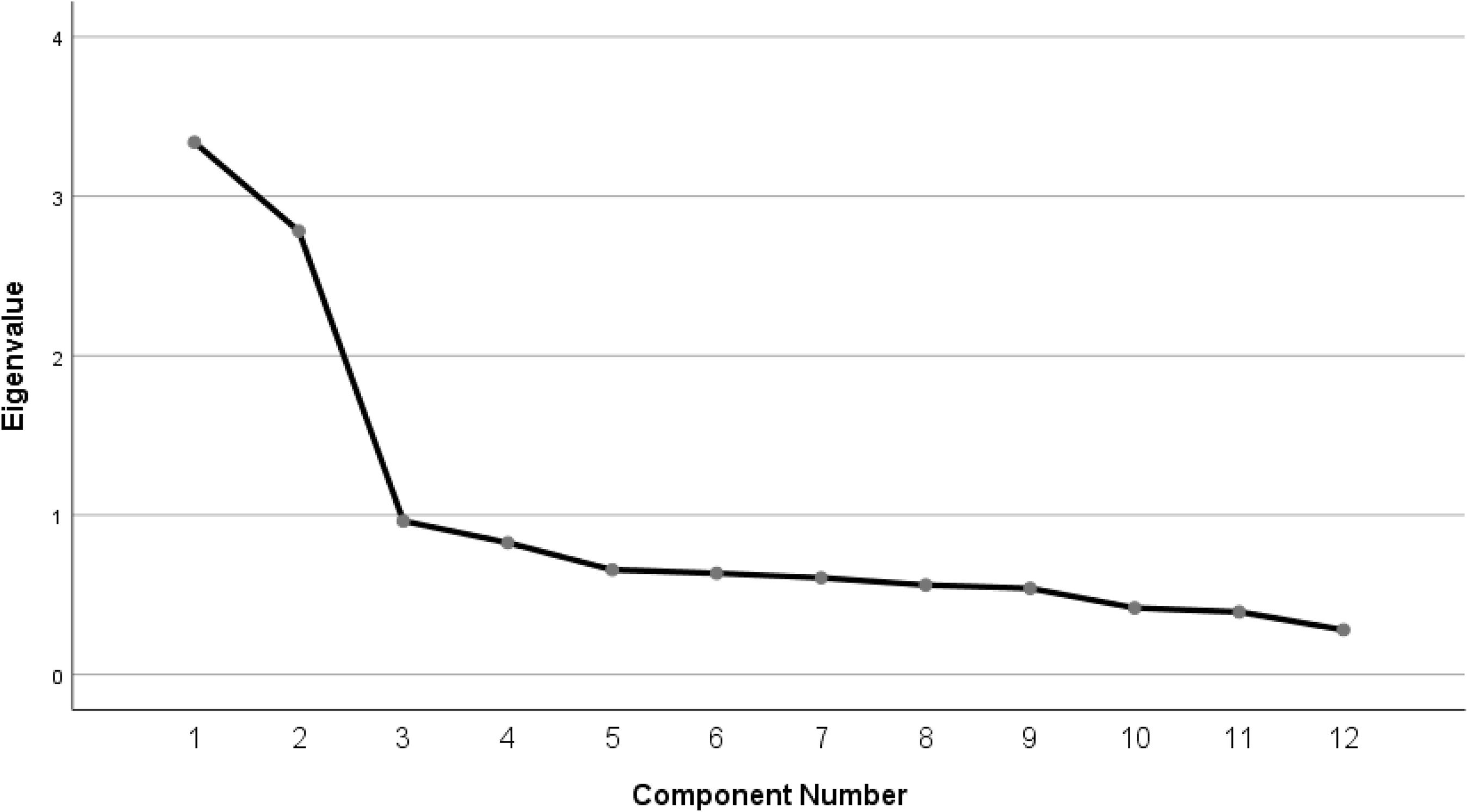
Figure 1. Scree plot.
Concerning the CFA, although the χ2 was significant with χ2(36, n = 463) = 134.877, p < 0.001, the other indices showed satisfactory values and supported the two-factor solution of the Italian PAS: GFI = 0.954, NNFI = 0.921, CFI = 0.940, RMSEA = 0.077, SRMR = 0.066.
Reliability of the Scale
A Cronbach α coefficient (α = 0.76 for the total scale and α = 0.80, 0.79 for the two subscales) suggested satisfactory reliability. Item-total correlations (Table 2) showed values ranging from 0.19 (Item 7) to 0.57 (Item 8).
Construct Validity
Intercorrelations between PAS subscale scores were r = 0.11, p < 0.01, and they significantly and positively correlated with the PAS total score (F1, r = 0.73, p < 0.01; F2, r = 0.76, p < 0.01).
The Italian PAS showed significant correlations with most measures used to assess construct validity (Table 5). More specifically, correlations of particular importance for the convergent validity were those shown with BAQ (r = 0.23, p < 0.01, for the total PAS scale; and r = 0.32, p < 0.01, for the first PAS subscale, but there was no significant correlation with the second PAS factor), RSES (r = 0.19, p < 0.01; r = 0.07, p < 0.05; r = 0.22, p < 0.01 for total PAS score, the first and the second PAS subscales, respectively), GSE (r = 0.25, p < 0.01; r = 0.24, p < 0.01; r = 0.14, p < 0.01 for total PAS score, the first and the second PAS subscales, respectively), and MAAS (r = 0.19, p < 0.01; r = 0.13, p < 0.01; r = 0.15, p < 0.01 for total PAS score, the first and the second PAS subscales, respectively). Regarding discriminant validity, specific relevance has been given to I-BICI and TAS-20 measurements. The PAS total score and its second subscale were significantly and negatively correlated with the I-BICI total scale (r = −0.28, p < 0.01; r = −0.37, p < 0.01, respectively), the first I-BICI subscale (r = −0.28, p < 0.01; r = − 0.37, p < 0.01, respectively), and the second I-BICI subscale (r = −0.20, p < 0.01; r = − 0.28, p < 0.01, respectively). Furthermore, the PAS total score and its subscales were significantly and negatively correlated with the TAS-20 total scale (r = −0.25, p < 0.01; r = − 0.09, p < 0.01; r = −0.28, p < 0.01, respectively), the first TAS-20 subscale (r = −0.22, p < 0.01; r = −0.31, p < 0.01, only total PAS and the second PAS factor, respectively), the second TAS-20 subscale (r = −0.18, p < 0.01; r = −0.21, p < 0.01, only total PAS and the second PAS factor, respectively), and the third TAS-20 subscale (r = −0.18, p < 0.01; r = − 0.14, p < 0.01; r = −0.13, p < 0.01, respectively).

Table 5. Correlations of the measures used to assess construct validity.
Then, a correlation coefficients comparison (Meng et al., 1992) was used to assess the discriminant validity of the PAS subscales (Table 6). The analysis showed that the subscales correlations with total PAS (z = −1.54, p = 0.124), the third factor of the TAS20 (z = −0.23, p = 0.817), and MAAS (z = −0.46, p = 0.644) were not significantly different.
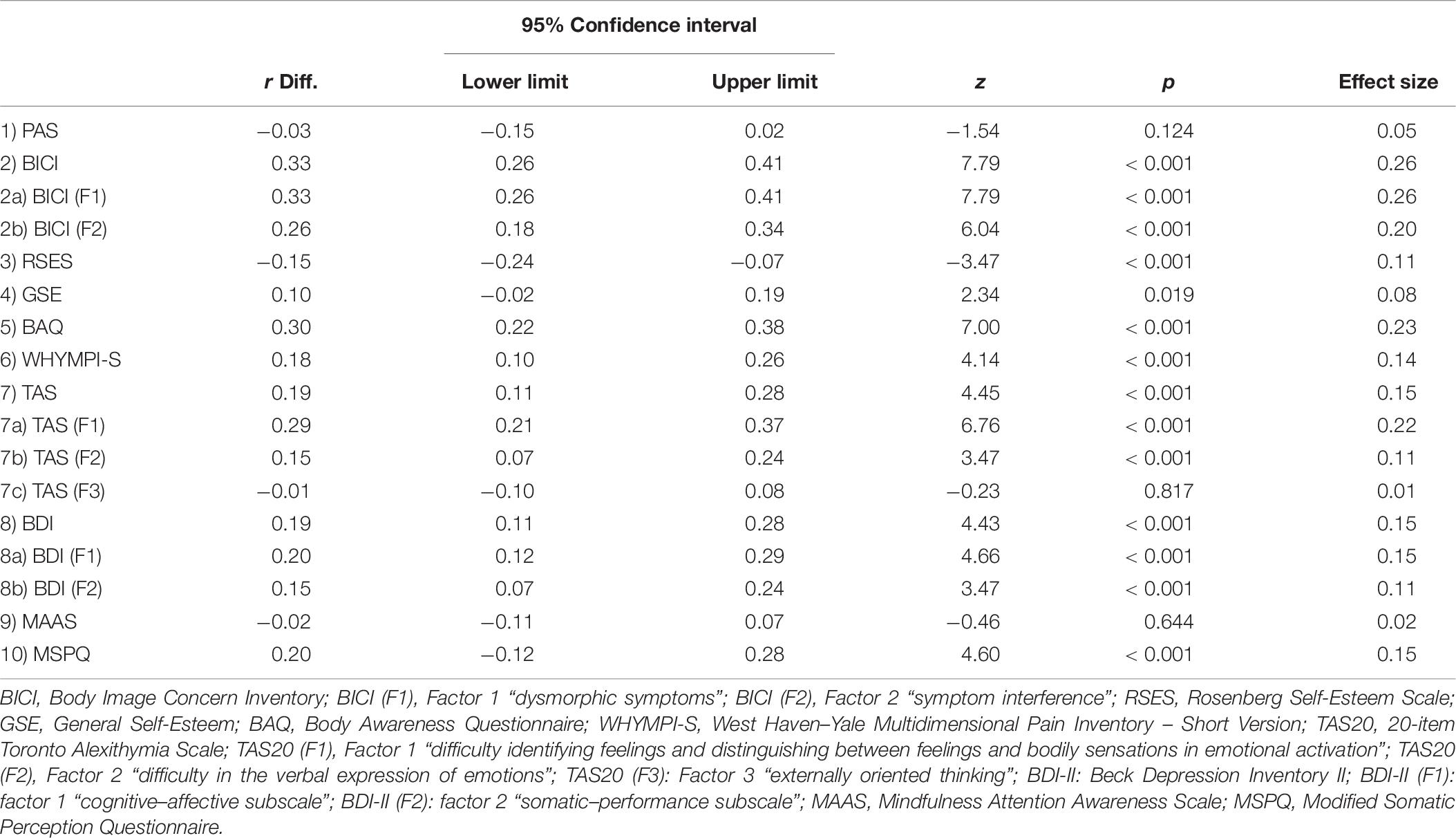
Table 6. Comparison of correlation coefficients between PAS subscales and the other variables.
General Linear Model
The results of the MANOVA revealed no significant differences regarding gender or age on level of postural awareness (Tables 7, 8).
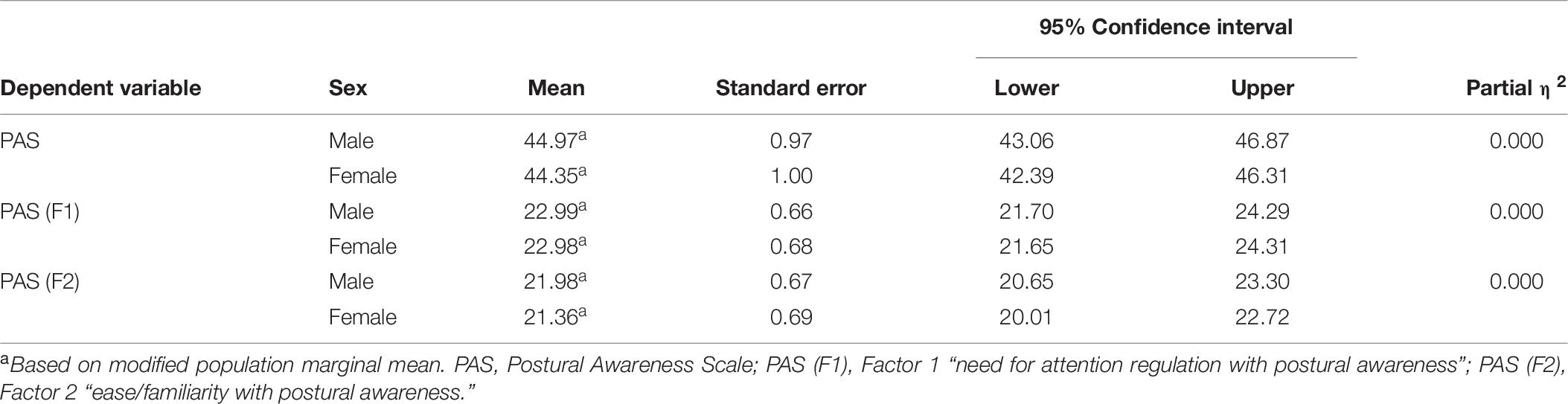
Table 7. Summary of PAS total scale and PAS subscales scores by men and women.
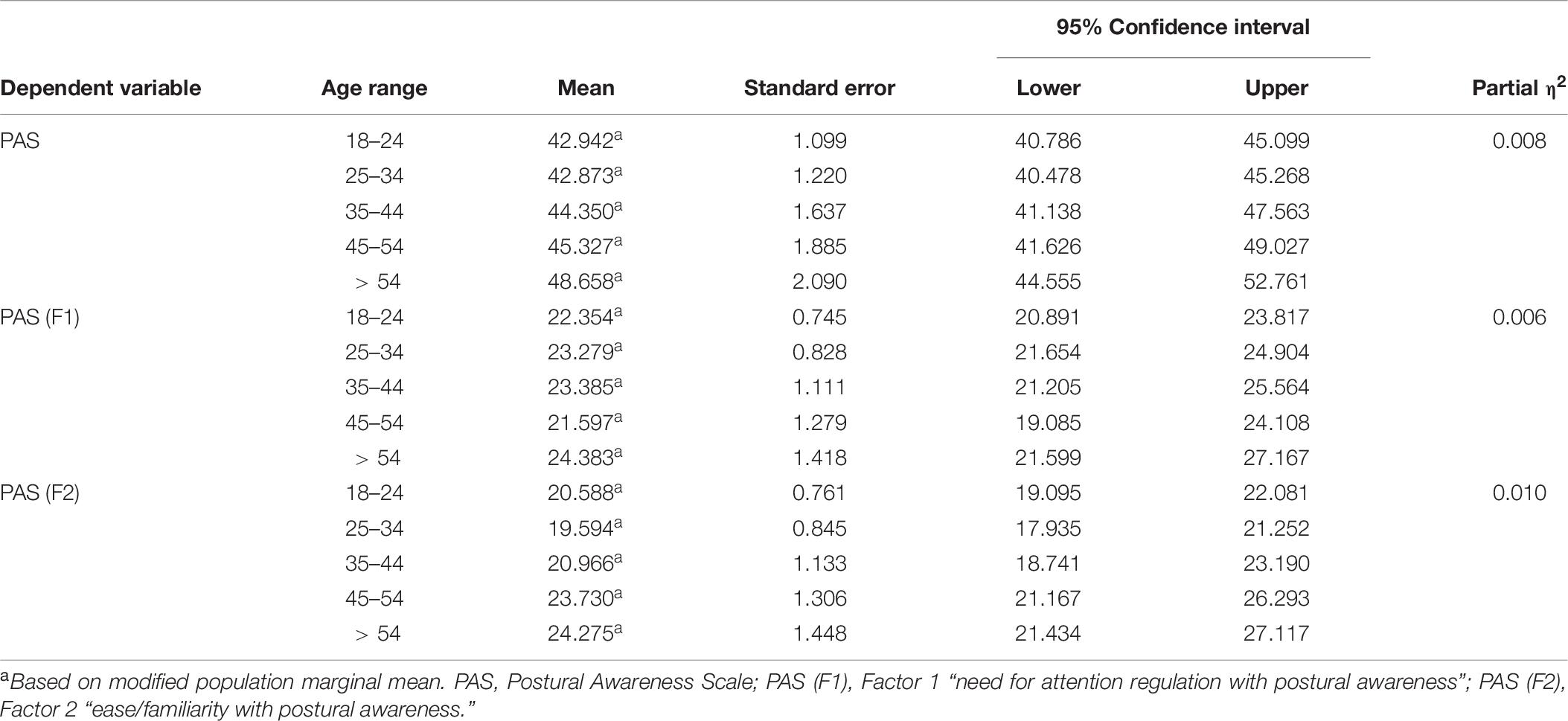
Table 8. Summary of PAS total scale and PAS subscales scores in different age range.
There was a significant difference between those who practice sport and those who do not (Table 9) when considered jointly on the variables total PAS, PAS (F1) and PAS (F2), Wilk’s Λ = 0.991, F(2,843) = 3.93, p = 0.020, partial η2 = 0.01. A separate ANOVA was conducted for each dependent variable, with each ANOVA evaluated at an α level of 0.025. There were significantly higher scores in those who practice sport than those who do not on both total PAS score and first PAS subscale, but not on the second one: F(1,844) = 7.80, p = 0.005, partial η2 = 0.01; F(1,844) = 5.87, p = 0.028, partial η2 = 0.01, respectively.
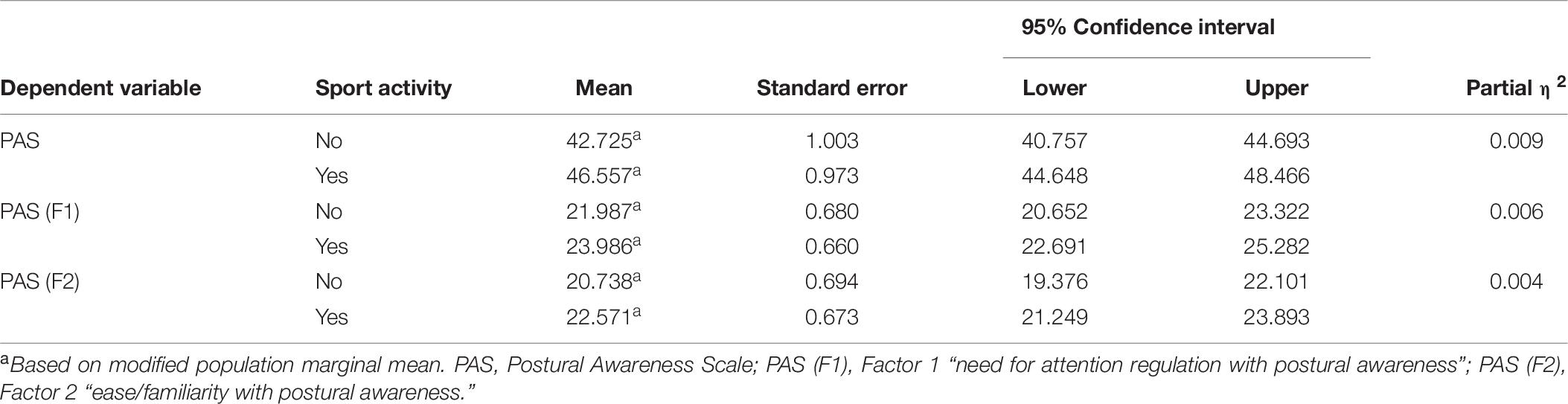
Table 9. Summary of PAS total scale and PAS subscales scores by people who practice or not sport.
Indeed, significant differences related to BMI (Table 10) were found when considered jointly on the variables total PAS, PAS (F1) and PAS (F2), Wilk’s Λ = 0.980, F(8,1686) = 1.12, p = 0.031, partial η2 = 0.01. A separate ANOVA was conducted for each dependent variable, with each ANOVA evaluated at an α level of 0.025. There was a significant difference among the different BMI range only on total PAS score: F(4,844) = 2.38, p = 0.050, partial η2 = 0.01. More specifically, post hoc analysis (Scheffé) showed that the group “normal weight” had a higher level of postural awareness.
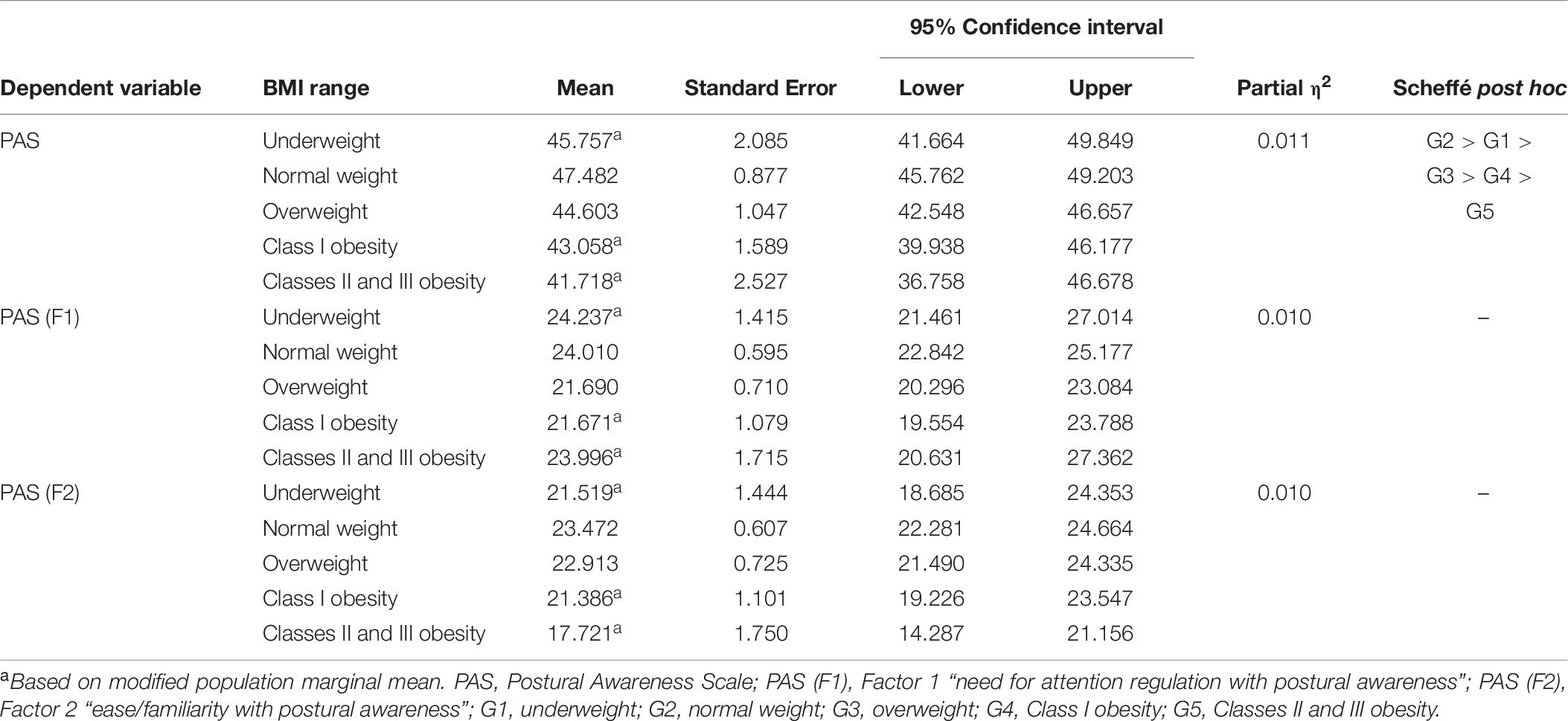
Table 10. Summary of PAS total scale and PAS subscales scores in different BMI range.
Discussion
The aim of this research was to analyze the psychometric characteristics of the Italian version of the PAS (Cramer et al., 2018b), a measure of body posture awareness. This tool fits into a perspective that connects posture to well-being (Lauche et al., 2017) and which, in turn, falls within a broader theoretical frame including a growing literature supporting the close link between physical and mental aspects (e.g., Ogden et al., 2012; Van Der Kolk, 2014; Fisher, 2017).
The Italian version of the PAS showed satisfactory psychometric properties with good indications of internal consistency and construct validity. The results obtained with MAP, HPA, and EFA supported a two-factor solution, as confirmed by the CFA and in line with the original version: the first regards the ability to have a high postural awareness in a natural and effortless way (Factor 1 “ease/familiarity with postural awareness”); the second refers the need of high efforts to be aware of their own posture (Factor 2 “need for attention regulation with postural awareness”). In line with what the authors of the original instrument indicated, the two subscales (both with good internal consistency) would seem to indicate the extremes of a continuum concerning the effort employed to be aware of one’s posture (Cramer et al., 2018b).
Positive and significant correlations were found with the mindfulness (MAAS) and the body awareness (BAQ) measurements, although in the relationship with the latter the second factor of the PAS (need for attention regulation with postural awareness) is an exception (in line with the results of the original version, in which there was a low association). The absence of association of this subscale could be interpreted looking at the need of efforts to be aware of his own posture as a difficulty and a lower spontaneity to have mental representation of body aspects. More specifically, the Multiple Code Theory (Bucci, 1999) considers the visceral and physical sensations as subsymbolic processes that, through a referential process, can be depicted within the symbolic register provided by language and images. A lack of integration of these elements does not allow having a full bodily processes awareness, which is a fundamental element for the distinction between emotive or physiological physical activations.
This condition causes tensions and dysregulated states of emotional arousal that could lead to psychosomatic problems (Ruesch, 1948; MacLean, 1949): all this could result in greater attention to somatic aspects, which, however, do not lead to awareness, but only to excessive worry and anxiety. The above is confirmed by the negative associations of postural awareness with alexithymia (especially externally oriented thinking) and the perception of physiological functions linked to states of anxiety and malaise (respectively, TAS-20 and MSPQ, which are instead positively correlated to each other). A lack of integration between symbolic and subsymbolic processes, therefore, does not allow to understand, express, and elaborate the somatic activations. In fact, the data show that both natural focus and active attention aimed at achieving and maintaining high levels of postural awareness are linked with a decrease of negative effect perception from the pain experiences (WHYMPI-S), which is in line with the scientific literature that shows that a higher non-judgmental bodily consciousness is associated with lower physical pain (Zeidan and Vago, 2016; Anheyer et al., 2017) and with a decrease in the anxiety that this condition determines (Flink et al., 2009). Furthermore, regarding the attention to aesthetic features, a negative and worried attitude toward one’s appearance would seem to be associated with a sense of detachment from the body and a complete unwillingness to make efforts to be aware of the posture assumed. Indeed, negative correlations were found between PAS and dysmorphic concern scores (BICI), except for the first factor (in line with the original study).
Positive correlations with self-esteem (RSES) and self-efficacy (GSE) and negative associations with depression (BDI-II) are also identified. Scientific literature supports evidence that certain bodily attitudes can influence self-confidence, the perception of being able to cope with difficulties, and emotional state (Keltner et al., 2003; Michalak et al., 2014; Nair et al., 2015; Cuddy, 2016); on the one hand, it could deduce that a greater posture awareness allows greater control over it and over the states it influences, favoring a more positive self-image; on the other hand, this could also be interpreted taking into account that higher levels of self-esteem and self-efficacy are associated to higher insight (Gori et al., 2015), also allowing a greater sense of mastery in one’s environment and a greater awareness of how body fits and interacts with it, facilitating a state of well-being.
Besides, to have more accurate interpretations about the differences between PAS subscales correlations, an inferential test was used to determine whether relevant pairs of correlations were statistically different in magnitude. The findings support the construct validity: significant associations were found between the positive correlations that the PAS subscales have with the PAS total score, between those with the MAAS and between the negative correlations that they have with the TAS20 “external oriented thinking” subscale.
Other important results obtained from the present research confirm the positive effects of physical activity and healthy body weight. Indeed, previous studies suggest that repeated exposure to bodily functions related to physical activity (e.g., increased breathing and heart rate) may lead to better body awareness in the various aspects that characterize it (Skrinar et al., 1986; Mehling et al., 2009), which in turn can be associated with greater body satisfaction and a decrease in disordered eating attitudes (Daubenmier, 2005). On the contrary, no significant differences were found regarding gender and age, in line with other research (Price and Thompson, 2007; Cramer et al., 2018b). This study has some limitations that need to be identified and discussed. First, several statistical comparisons have been carried out without any control procedure for false discovery rate, and this should be considered in the interpretation of the results: future research could overcome this limit, also correcting the p-values for multiple comparisons. Besides, as self-report tool, the PAS requires a self-assessment of aspects for which there could be a low level of consciousness; by definition, it is not possible to understand the actual association between self-report and the real postural awareness. Future research could use a multimodal approach (e.g., adding laboratory measurements and in-depth interviews) to have more complete assessments and overcome this limit, albeit with a greater expenditure of resources. Furthermore, the sample is composed only of Italian subjects, and this impacts the generalizability of the results in other cultures. Specifically, it could be interesting to study and analyze the differences in postural awareness levels in Eastern countries, considering, for example, the positive impact that different martial arts having their origin and diffusion have on this aspect (e.g., Lauche et al., 2017). Thus, future research could expand the sample by including employees from different geographical areas, to test the cross-cultural invariance of the results too.
Despite these limitations, the results of this validation study suggest that the Italian version of the PAS is a rapid tool, simple in its administration and evaluation, and with good psychometric properties; these data imply the possibility of using this self-report easily both for research and clinical practice, elaborating interventions within the psychotherapeutic process that can act on the two dimensions of the postural awareness construct (“need for attention regulation with postural awareness” and “ease/familiarity with postural awareness”).
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors conceptualized and designed the study, collaborated for the realization of the back-translation, contributed to manuscript revision, read, and approved the submitted version. ET recruited the subjects, administered them the protocol, and wrote the first draft of the manuscript. AG and ET performed the data analysis. AG was the scientific supervisor of the study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Ahmed, H., Shaphe, M. A., Iqbal, A., Khan, A. R., and Anwer, S. (2016). Effect of trunk stabilization exercises using a gym ball with or without electromyography-biofeedback in patients with chronic low back pain: an experimental study. Physikalische Med. Rehabil. Kurortmed. 26, 79–83. doi: 10.1055/s-0042-102537
Aminian, K., and Najafi, B. (2004). Capturing human motion using body-fixed sensors: outdoor measurement and clinical applications. Comput. Anim. Virtual Worlds 15, 79–94. doi: 10.1002/cav.2
Anderson, C., and Galinsky, A. D. (2006). Power, optimism, and risk- taking. Eur. J. Soc. Psychol. 36, 511–536. doi: 10.1002/ejsp.324
Anheyer, D., Haller, H., Barth, J., Lauche, R., Dobos, G., and Cramer, H. (2017). Mindfulness-based stress reduction for treating low back pain: a systematic review and meta-analysis. Ann. Intern. Med. 166, 799–807. doi: 10.7326/m16-1997
Arnette, S. L., and Pettijohn, T. F. II (2012). The effects of posture on self- perceived leadership. Int. J. Bus. Soc. Sci. 3, 8–13.
Bagby, R. M., Parker, J. D., and Taylor, G. J. (1994). The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 38, 23–32. doi: 10.1016/0022-3999(94)90005-1
Bakal, D. A. (2001). Minding the Body: Clinical Uses of Somatic Awareness. New York, NY: Guilford Press.
Balasubramaniam, R., and Wing, A. M. (2002). The dynamics of standing balance. Trends Cogn. Sci. 6, 531–536. doi: 10.1016/s1364-6613(02)02021-1
Beck, A. T., Steer, R. A., and Brown, G. K. (1996). Beck depression inventory-II. San Antonio 78, 490–498.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: a proposed operational definition. Clin. Psychol. 11, 230–241. doi: 10.1093/clipsy.bph077
Bluhm, R. L., Williamson, P. C., Osuch, E. A., Frewen, P. A., Stevens, T. K., Boksman, K., et al. (2009). Alterations in default network connectivity in posttraumatic stress disorder related to early-life trauma. J. Psychiatry Neurosci. 34, 187.
Bressi, C., Taylor, G., Parker, J., Bressi, S., Brambilla, V., Aguglia, E., et al. (1996). Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: an Italian multicenter study. J. Psychosom. Res. 41, 551–559. doi: 10.1016/S0022-3999(96)00228-0
Brito, C. A. Jr. (1995). Alterações Posturais. Lianza S. Medicina de Reabilitação. Rio de Janeiro: Guanabara Koogan.
Brown, K. W., and Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 84:822. doi: 10.1037/0022-3514.84.4.822
Büssing, A., Walach, H., Kohls, N., Zimmermann, F., and Trousselard, M. (2013). Conscious Presence and Self Control as a measure of situational awareness in soldiers–A validation study. Int. J. Mental Health Syst. 7:1. doi: 10.1186/1752-4458-7-1
Cramer, H., Lauche, R., Daubenmier, J., Mehling, W., Büssing, A., Saha, F. J., et al. (2018a). Being aware of the painful body: validation of the German Body Awareness Questionnaire and Body Responsiveness Questionnaire in patients with chronic pain. PLoS One 13:e193000. doi: 10.1371/journal.pone.0193000
Cramer, H., Mehling, W. E., Saha, F. J., Dobos, G., and Lauche, R. (2018b). Postural awareness and its relation to pain: validation of an innovative instrument measuring awareness of body posture in patients with chronic pain. BMC Musculoskelet. Disord. 19:109. doi: 10.1186/s12891-018-2031-9
Daubenmier, J. J. (2005). The relationship of yoga, body awareness, and body responsiveness to self-objectification and disordered eating. Psychol. Women Q. 29, 207–219. doi: 10.1111/j.1471-6402.2005.00183.x
Dijkstra, K., Kaschak, M. P., and Zwaan, R. A. (2007). Body posture facilitates retrieval of autobiographical memories. Cognition 102, 139–149. doi: 10.1016/j.cognition.2005.12.009
Ferrari, R., Novara, C., Sanavio, E., and Zerbini, F. (2000). Internal structure and validity of the multidimensional pain inventory, Italian language version. Pain. Med. 1, 123–130. doi: 10.1046/j.1526-4637.2000.00020.x
Fisher, J. (2017). Healing the Fragmented Selves Of Trauma Survivors: Overcoming Internal Self-Alienation. Abingdon: Routledge.
Flink, I. K., Nicholas, M. K., Boersma, K., and Linton, S. J. (2009). Reducing the threat value of chronic pain: a preliminary replicated single-case study of interoceptive exposure versus distraction in six individuals with chronic back pain. Behav. Res. Ther. 47, 721–728. doi: 10.1016/j.brat.2009.05.003
Friis, S., Skatteboe, U. B., Hope, M. K., and Vaglum, P. (1989). Body awareness group therapy for patients with personality disorders. Psychother. Psychosom. 51, 18–24. doi: 10.1159/000288128
Ghisi, M., Flebus, G. B., Montano, A., Sanavio, E., and Sica, C. (2006). Beck Depression Inventory II Italian Version. Firenze: Editore Giunti OS.
Gilbert, D., and Waltz, J. (2010). Mindfulness and health behaviors. Mindfulness 1, 227–234. doi: 10.1007/s12671-010-0032-3
Gori, A., Craparo, G., Giannini, M., Loscalzo, Y., Caretti, V., La Barbera, D., et al. (2015). Development of a new measure for assessing insight: psychometric properties of the insight orientation scale (IOS). Schizophr. Res. 169, 298–302. doi: 10.1016/j.schres.2015.10.014
Grotstein, J. S. (1997). “Mens sane in Corpore Sano”: the mind and body as an “odd couple” and as an oddly coupled unity. Psychoanal. Inq. 17, 204–222. doi: 10.1080/07351699709534120
Gurfinkel, V. S. (1994). The mechanisms of postural regulation in man. Sov. Sci. Rev. F Phys. Gen. Biol. 7, 59–89.
Hackford, J., Mackey, A., and Broadbent, E. (2019). The effects of walking posture on affective and physiological states during stress. J. Behav. Ther. Exp. Psychiatry 62, 80–87. doi: 10.1016/j.jbtep.2018.09.004
Herman, J. L. (1992). Complex PTSD: a syndrome in survivors of prolonged and repeated trauma. J. Trauma Stress 5, 377–391. doi: 10.1016/j.janxdis.2005.04.003
Hooper, D., Coughlan, J., and Mullen, M. R. (2008). Structural equation modelling: guidelines for determining model fit. Electr. J. Bus. Res. Methods 6, 53–60.
Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika 30, 179–185. doi: 10.1007/BF02289447
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equa. Model. 6, 1–55. doi: 10.1080/10705519909540118
Huang, L., Galinsky, A. D., Gruenfeld, D. H., and Guillory, L. E. (2011). Powerful postures versus powerful roles: which is the proximate correlate of thought and behavior? Psychol. Sci. 22, 95–102. doi: 10.1177/0956797610391912
Jay, K., Jakobsen, M. D., Sundstrup, E., Skotte, J. H., Jørgensen, M. B., Andersen, C. H., et al. (2013). Effects of kettlebell training on postural coordination and jump performance: a randomized controlled trial. J. Strength Condition. Res. 27, 1202–1209. doi: 10.1519/JSC.0b013e318267a1aa
Kee, Y. H., Chatzisarantis, N. N., Kong, P. W., Chow, J. Y., and Chen, L. H. (2012). Mindfulness, movement control, and attentional focus strategies: effects of mindfulness on a postural balance task. J. Sport Exerc. Psychol. 34, 561–579. doi: 10.1123/jsep.34.5.561
Keltner, D., Gruenfeld, D. H., and Anderson, C. (2003). Power, approach, and inhibition. Psychol. Rev. 110:265. doi: 10.1037/0033-295x.110.2.265
Kerns, R. D., Turk, D. C., and Rudy, T. E. (1985). The west haven-yale multidimensional pain inventory (WHYMPI). Pain 23, 345–356. doi: 10.1016/0304-3959(85)90004-1
Kline, R. B. (2005). Principles and Practice of Structural Equation Modeling, 2nd Edn. New York, NY: Guilford.
Kwon, J., and Kim, S. Y. (2015). “The effect of posture on stress and self-esteem: comparing contractive and neutral postures,” in Proceedings of International Academic Conferences (No. 2705176), London: International Institute of Social and Economic Sciences, doi: 10.20472/IAC.2015.018.067
Lanningham-Foster, L. M., Jensen, T. B., McCrady, S. K., Nysse, L. J., Foster, R. C., and Levine, J. A. (2005). Laboratory measurement of posture allocation and physical activity in children. Med. Sci. Sports Exerc. 37, 1800–1805. doi: 10.1249/01.mss.0000175050.03506.bf
Lauche, R., Wayne, P. M., Fehr, J., Stumpe, C., Dobos, G., and Cramer, H. (2017). Does postural awareness contribute to exercise-induced improvements in neck pain intensity? A secondary analysis of a randomized controlled trial evaluating Tai Chi and neck exercises. Spine 42, 1195–1200. doi: 10.1097/BRS.0000000000002078
Littleton, H. L., Axsom, D., and Pury, C. L. (2005). Development of the body image concern inventory. Behav. Res. Ther. 43, 229–241. doi: 10.1016/j.brat.2003.12.006
Luca, M., Giannini, M., Gori, A., and Littleton, H. (2011). Measuring dysmorphic concern in Italy: psychometric properties of the Italian Body Image Concern Inventory (I-BICI). Body Image 8, 301–305. doi: 10.1016/j.bodyim.2011.04.007
MacLean, P. D. (1949). Psychosomatic disease and the” visceral brain”; recent developments bearing on the Papez theory of emotion. Psychosom. Med. 11, 338–353. doi: 10.1097/00006842-194911000-00003
Main, C. J. (1983). The modified somatic perception questionnaire (MSPQ). J. Psychosom. Res. 27, 503–514. doi: 10.1016/0022-3999(83)90040-5
Maner, J. K., Kaschak, M. P., and Jones, J. L. (2010). Social power and the advent of action. Soc. Cogn. 28, 122–132. doi: 10.1521/soco.2010.28.1.122
Marlatt, G. A., and Ostafin, B. D. (2005). “Being mindful of automaticity in addiction: a clinical perspective,” in Handbook of Implicit Cognition and Addiction, eds R. W. Wiers and A. W. Stacy (Thousand Oaks, CA: Sage), 489–493.
Marsh, H. W., Hau, K. T., and Wen, Z. (2004). In search of golden rules: comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct. Equa. Model. 11, 320–341. doi: 10.1207/s15328007sem1103_2
Massion, J. (1994). Postural control system. Curr. Opin. Neurobiol. 4, 877–887. doi: 10.1016/0959-4388(94)90137-6
Mehling, W. E., Gopisetty, V., Daubenmier, J., Price, C. J., Hecht, F. M., and Stewart, A. (2009). Body awareness: construct and self-report measures. PLoS One 4:e5614. doi: 10.1371/journal.pone.0005614
Meng, X. L., Rosenthal, R., and Rubin, D. B. (1992). Comparing correlated correlation coefficients. Psychol. Bull. 111:172. doi: 10.1037/0033-2909.111.1.172
Michalak, J., Mischnat, J., and Teismann, T. (2014). Sitting posture makes a difference—embodiment effects on depressive memory bias. Clin. Psychol. Psychother. 21, 519–524. doi: 10.1002/cpp.1890
Moseley, G. L., Nicholas, M. K., and Hodges, P. W. (2004). A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin. J. Pain 20, 324–330. doi: 10.1097/00002508-200409000-00007
Murphy, M. J., Mermelstein, L. C., Edwards, K. M., and Gidycz, C. A. (2012). The benefits of dispositional mindfulness in physical health: a longitudinal study of female college students. J. Am. Coll. Health 60, 341–348. doi: 10.1080/07448481.2011.629260
Nair, S., Sagar, M., Sollers, J. III, Consedine, N., and Broadbent, E. (2015). Do slumped and upright postures affect stress responses? A randomized trial. Health Psychol. 34:632. doi: 10.1037/hea0000146
O’connor, B. P. (2000). SPSS and SAS programs for determining the number of components using parallel analysis and Velicer’s MAP test. Behav. Res. Methods Instr. Comput. 32, 396–402. doi: 10.3758/bf03200807
Ogden, P., Minton, K., and Pain, C. (2012). Il Trauma E Il Corpo: Manuale Di Psicoterapia Sensomotoria. Italy: Istituto di scienze cognitive.
Pluchino, A., Lee, S. Y., Asfour, S., Roos, B. A., and Signorile, J. F. (2012). Pilot study comparing changes in postural control after training using a video game balance board program and 2 standard activity-based balance intervention programs. Arch. Phys. Med. Rehabil. 93, 1138–1146. doi: 10.1016/j.apmr.2012.01.023
Pöhlmann, K., et al. (2014). The Dresden Body Image Inventory (DKB-35): validity in a clinical sample. Psychother. Psychosom. Med. Psychol. 64, 93–100. doi: 10.1055/s-0033-1351276
Prezza, M., Trombaccia, F. R., and Armento, L. (1997). La scala dell’autostima di Rosenberg: traduzione e validazione italiana. Boll. Psicol. Appl. 223, 35–44.
Price, C. J., and Thompson, E. A. (2007). Measuring dimensions of body connection: body awareness and bodily dissociation. J. Alternat. Complement. Med. 13, 945–953. doi: 10.1089/acm.2007.0537
Roberts, K. C., and Danoff-Burg, S. (2010). Mindfulness and health behaviors: is paying attention good for you? J. Am. Coll. Health 59, 165–173. doi: 10.1080/07448481.2010.484452
Roll, R., Kavounoudias, A., and Roll, J. P. (2002). Cutaneous afferents from human plantar sole contribute to body posture awareness. Neuroreport 13, 1957–1961. doi: 10.1097/00001756-200210280-00025
Rosberg, S. (2000). Kropp, Varande Och Mening i Ett Sjukgymnastiskt Perspektiv. Göteborg: Department of Social Work Institutionen för socialt arbete.
Rosenberg, M. (1965). Rosenberg self-esteem scale (RSE). Acceptance and commitment therapy. Measures Package 61:52.
Ruesch, J. (1948). The infantile personality; the core problem of psychosomatic medicine. Psychosom. Med. 10, 134–144. doi: 10.1097/00006842-194805000-00002
Schwarzer, R., and Jerusalem, M. (1995). Generalized self-efficacy scale. Measures in health psychology: a user’s portfolio. Causal Control Beliefs 1, 35–37.
Shields, S. A., Mallory, M. E., and Simon, A. (1989). The body awareness questionnaire: reliability and validity. J. Pers. Assess. 53, 802–815. doi: 10.1207/s15327752jpa5304_16
Sibilia, L., Schwarzer, R., and Jerusalem, M. (1995). Italian Adaptation of the General Self-Efficacy Scale. Resource Document. Available online at: http://userpage.fu-berlin.de/~health/italian.htm (accessed October 17, 2019).
Skrinar, G. S., Bullen, B. A., Cheek, J. M., McArthur, J. W., and Vaughan, L. K. (1986). Effects of endurance training on body-consciousness in women. Percept. Mot. Skills 62, 483–490. doi: 10.2466/pms.1986.62.2.483
Solano, L. (2010). Some thoughts between body and mind in the light of Wilma Bucci’s multiple code theory. Int. J. Psychoanal. 91, 1445–1464. doi: 10.1111/j.1745-8315.2010.00359.x
Stepper, S., and Strack, F. (1993). Proprioceptive determinants of emotional and nonemotional feelings. J. Pers. Soc. Psychol. 64:211. doi: 10.1037/0022-3514.64.2.211
Van Der Kolk, B. (2008). “Il disturbo traumatico dello sviluppo: verso una diagnosi razionale per bambini cronicamente traumatizzati,” in Trauma e Psicopatologia: un Approcio Evolutivo-Relazionale, eds V. Caretti and G. Craparo (Rome: Astrolabio Ubaldini), 81–93.
Van Der Kolk, B. (2014). Il Corpo Accusa il colpo. Mente, Corpo e Cervello Nell’elaborazione Delle Memorie Traumatiche. Milano: Raffaello Cortina, 2015.
Van der Kolk, B. A. (2006). “Clinical implications of neuroscience research in PTSD,” in Neuroscience and Psychoanalysis, eds G. Leo, D. Mann, G. Northoff, A. N. Schore, R. Skgold, B. A. Van Der Kolk, et al. (Italy: Frenis Zero Press), 159–196. doi: 10.1196/annals.1364.022
Van der Toorn, J., Feinberg, M., Jost, J. T., Kay, A. C., Tyler, T. R., Willer, R., et al. (2015). A sense of powerlessness fosters system justification: implications for the legitimation of authority, hierarchy, and government. Politic. Psychol. 36, 93–110. doi: 10.1111/pops.12183
Velicer, W. F. (1976). Determining the number of components from the matrix of partial correlations. Psychometrika 41, 321–327. doi: 10.1007/BF02293557
Velicer, W. F., Eaton, C. A., and Fava, J. L. (2000). “Construct explication through factor or component analysis: a review and evaluation of alternative procedures for determining the number of factors or components,” in Problems and Solutions In Human Assessment: Honoring Douglas N. Jackson at Seventy, eds R. D. Goffin and E. Helmes (Norwell, MA: Kluwer Academic), 41–77. doi: 10.1007/978-1-4615-4397-8_3
Veneziani, C. A., and Voci, A. (2015). The Italian adaptation of the Mindful Awareness Attention Scale and its relation with individual differences and quality of life indexes. Mindfulness 6, 373–381. doi: 10.1007/s12671-013-0270-2
Wallace, A. B. (2006). The Nature of Mindfulness and Its Role in Buddhist Meditation: A Correspondence Between B. Alan Wallace and the Venerable Bhikkhu Bodhi. Santa Barbara, CA: Santa Barbara Institute for Consciousness Studies.
Wayne, P. M., Krebs, D. E., Wolf, S. L., Gill-Body, K. M., Scarborough, D. M., McGibbon, C. A., et al. (2004). Can Tai Chi improve vestibulopathic postural control? Arch. Phys. Med. Rehabil. 85, 142–152. doi: 10.1016/S0003-9993(03)00652-X
Wong, W. Y., Wong, M. S., and Lo, K. H. (2007). Clinical applications of sensors for human posture and movement analysis: a review. Prosthetic. Orthotics Int. 31, 62–75. doi: 10.1080/03093640600983949
Wright, E. F., Domenech, M. A., and Fischer, J. R. (2000). Usefulness of posture training for patients with temporomandibular disorders. J. Am. Dent. Assoc. 131, 202–210. doi: 10.14219/jada.archive.2000.0148
Yamak, B., ımamoǧlu, O., ımamoǧlu, ı, and Çebi, M. (2018). The effects of exercise on body posture. Electr. Turkish Stud. 13, 1377–1388. doi: 10.7827/TurkishStudies.13911
Zeidan, F., and Vago, D. R. (2016). Mindfulness meditation–based pain relief: a mechanistic account. Ann. N. Y. Acad. Sci. 1373, 114–127. doi: 10.1111/nyas.13153
Keywords: posture, awareness, mind–body integration, Italian validation, self-report questionnaire
Citation: Topino E, Gori A and Cramer H (2020) Mind and Body: Italian Validation of the Postural Awareness Scale. Front. Psychol. 11:827. doi: 10.3389/fpsyg.2020.00827
Received: 26 November 2019; Accepted: 03 April 2020;
Published: 18 May 2020.
Edited by:
Pietro Cipresso, Italian Auxological Institute (IRCCS), ItalyReviewed by:
Carlo Chiorri, University of Genoa, ItalyAlen Hajnal, University of Southern Mississippi, United States
Copyright © 2020 Topino, Gori and Cramer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessio Gori, YWxlc3Npby5nb3JpQHVuaWZpLml0