
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 09 April 2020
Sec. Health Psychology
Volume 11 - 2020 | https://doi.org/10.3389/fpsyg.2020.00614
 Julie Lillebostad Svendsen1,2*
Julie Lillebostad Svendsen1,2* Elisabeth Schanche3
Elisabeth Schanche3 Berge Osnes2,4
Berge Osnes2,4 Jon Vøllestad3,5
Jon Vøllestad3,5 Endre Visted1,3
Endre Visted1,3 Ingrid Dundas3Helge Nordby2
Ingrid Dundas3Helge Nordby2 Per-Einar Binder3
Per-Einar Binder3 Lin Sørensen2
Lin Sørensen2Background: Dispositional mindfulness and self-compassion are shown to associate with less self-reported emotional distress. However, previous studies have indicated that dispositional self-compassion may be an even more important buffer against such distress than dispositional mindfulness. To our knowledge, no study has yet disentangled the relationship between dispositional self-compassion and mindfulness and level of psychophysiological flexibility as measured with vagally mediated heart rate variability (vmHRV). The aim was thus to provide a first exploratory effort to expand previous research relying on self-report measures by including a psychophysiological measure indicative of emotional stress reactivity.
Methods: Fifty-three university students filled out the “Five Facet Mindfulness Questionnaire” (FFMQ) and the “Self-Compassion Scale” (SCS), and their heart rate was measured during a 5 min resting electrocardiogram. Linear hierarchical regression analyses were conducted to examine the common and unique variance explained by the total scores of the FFMQ and the SCS on level of resting vmHRV.
Results: Higher SCS total scores associated significantly with higher levels of vmHRV also when controlling for the FFMQ total scores. The SCS uniquely explained 7% of the vmHRV. The FFMQ total scores did not associate with level of vmHRV.
Conclusion: These results offer preliminary support that dispositional self-compassion associates with better psychophysiological regulation of emotional arousal above and beyond mindfulness.
How we relate to our experiences and ourselves when dealing with difficult emotions is important for our psychological health (Gross and Munoz, 1995). Dispositional mindfulness and self-compassion are two related and inherent human capacities (Kabat-Zinn, 2003). Mindfulness is a multi-faceted construct that can be defined as “paying attention in a particular way; on purpose, in the present moment, and non-judgmentally” (Kabat-Zinn, 2003). Self-compassion emphasizes being mindful to one’s own suffering together with the active wish to alleviate it and relate to oneself with a kind and caring attitude (Neff, 2003b). It is described as a positive mental capacity especially important for the health promoting outcomes associated with mindfulness-based interventions (Van Dam et al., 2011) in mediating decreased levels of symptoms of depression (Kuyken et al., 2010) and stress responses (Shapiro et al., 2005). Mindfulness and self-compassion are partially overlapping in their emphasis on non-judgment, acceptance and tolerance. At the same time, self-compassion focuses more exclusively on suffering, and more explicitly emphasizes kindness for the self (Neff and Dahm, 2015). This could capture a distinct dimension of human experience that can be meaningfully separated from mindfulness, and that may also be particularly important for dealing with challenging emotions.
To disentangle dispositional self-compassion from mindfulness, self-report measures are typically used (Kuyken et al., 2010; Van Dam et al., 2011; Woodruff et al., 2014). A widely employed mindfulness scale is the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006), measuring five distinct mindful aspects: observing, describing, acting with awareness, non-judgment, and non-reactivity to inner experiences. This measure is reckoned to include both attentional and attitudinal components of being mindful, in contrast to another widely use scale called the Mindful Attention and Awareness Scale (MAAS; Brown and Ryan, 2003), which exclusively focuses on present moment attention. The most commonly used self-report measure of self-compassion is the Self-Compassion Scale (SCS; Neff, 2003a), distinguishing between self-kindness versus self-judgment, common humanity versus isolation, and mindfulness versus overidentification. Thus, as operationally defined by Neff (2003a), mindfulness is an embedded part of self-compassion, however, this form of mindfulness is more narrowly focused on suffering, whereas mindfulness as measured by the FFMQ taps a broader range of experiences – both positive, neutral and negative ones.
A handful of studies have compared the predictive values of dispositional mindfulness and self-compassion on self-reported outcome measures. Van Dam et al. (2011) focused on the common and unique variance of dispositional mindfulness as measured with the MAAS and dispositional self-compassion with the SCS on self-reported symptoms of anxiety, depression, worry, and life quality. They found that both constructs were significant predictors, however, self-compassion uniquely explained up to ten times more variance of positive outcomes on these measures than mindfulness. Woodruff et al. (2014) sought to replicate these findings using the multi-faceted mindfulness-measure FFMQ. Similar to Van Dam et al. (2011) they found that both mindfulness and self-compassion significantly explained lower levels of anxiety, depression, negative affect, and unhappiness, and that self-compassion uniquely explained a higher degree of variance in these outcome variables than mindfulness. The central role of dispositional self-compassion as a buffer against emotional problems has further been shown in relation to level of shame (Woods and Proeve, 2014) and post-traumatic symptoms (Dahm et al., 2015), in self-compassion being a stronger predictor of lower levels of these symptoms than mindfulness. Interestingly, a recent study also showed self-compassion to predict emotional flexibility (Beshai et al., 2017). It showed that only self-compassion predicted better abilities in mood drop and spontaneous mood-recovery when including both mindfulness (measured with the MAAS) and self-compassion (measured with the SCS) as predictors in the same regression model.
Dispositional mindfulness (e.g., Delgado-Pastor et al., 2013; Krygier et al., 2013; Nijjar et al., 2014; Watford and Stafford, 2015; May et al., 2016; Shearer et al., 2016) and dispositional self-compassion (Rockliff et al., 2008; Kok et al., 2013; Arch et al., 2014; Matos et al., 2017; Petrocchi et al., 2017) are further also linked to psychophysiological flexibility as measured with higher vagally mediated heart rate variability (vmHRV). However, as far as we know, no study has yet attempted to disentangle the effect of dispositional self-compassion from dispositional mindfulness on vmHRV. Higher vmHRV is used as a psychophysiological index of the ability to regulate emotional arousal in flexible and adaptive ways according to situational contexts (Thayer and Lane, 2000, 2009; Appelhans and Luecken, 2006; Holzman and Bridgett, 2017). Resting vmHRV is suggested to reflect about 50% of trait-like aspects of the typical interplay between the sympathetic and parasympathetic branches of the autonomic nervous system (Bertsch et al., 2012). The sympathetic nervous system (SNS) increases heart rate, whereas the parasympathetic nervous system (PNS) slows down heart rate via the vagus nerve. The PNS has a shorter latency of response, thus allowing for higher variability between heartbeats. Higher resting vmHRV variability reflects as such a predominant PNS stimulation on the beat-to-beat heart rate. Lack of flexibility in the up- and down regulation of mood and emotional responses, i.e., emotional arousal, can be reflected in a lower vmHRV (Appelhans and Luecken, 2006). Previous research has shown that higher levels of symptoms of anxiety (Chalmers et al., 2014), depression (Kemp et al., 2010), and worry (Chalmers et al., 2016) are associated with lower levels of vmHRV. Our research group found that dispositional self-compassion as measured with the SCS associated with higher vmHRV, measured both during rest and during 24-h, and that this positive effect of self-compassion on vmHRV remained when adjusting for the effects of symptoms of anxiety and negative rumination (Svendsen et al., 2016). Similarly, it has been shown that individuals high in dispositional self-compassion have higher vmHRV in response to an acute stressor than individuals low in self-compassion (Luo et al., 2018). It has also been shown that self-compassion training increases vmHRV (Rockliff et al., 2008; Kok et al., 2013; Arch et al., 2014; Matos et al., 2017; Petrocchi et al., 2017). To our knowledge, only a few studies have investigated the relationship between dispositional mindfulness and vmHRV. One of these (Prazak et al., 2012) found that university students reporting higher levels of dispositional mindfulness on the Kentucky Inventory of Mindfulness Skills had higher vmHRV than those reporting to be less mindful. Two studies have found mixed results of the relationship between mindfulness as measured with the MAAS and vmHRV. One (Mankus et al., 2013) only found a positive association between high dispositional mindfulness on the MAAS and high vmHRV among individuals reporting to be high on symptoms of general anxiety, and not among those reporting to be low on general anxiety symptoms. The other (Brzozowski et al., 2017) found no association between reports on the MAAS and vmHRV. Fogarty et al. (2015) found only an association between the FFMQ total scores and level of vmHRV after an emotional stress induction task in men but not women. Likewise, Kadziolka et al. (2016) found the FFMQ-subscales of “Observe” and “Acting with Awareness” to relate to a higher vmHRV after a stress induction task. Interestingly, in contrast to measuring dispositional mindfulness, a more consistent relationship is found between mindfulness training and increased levels of vmHRV (e.g., Takahashi et al., 2005; Ditto et al., 2006; Tang et al., 2009; Joo et al., 2010; Delgado-Pastor et al., 2013; Krygier et al., 2013; Nijjar et al., 2014; Azam et al., 2015; Watford and Stafford, 2015; May et al., 2016; Shearer et al., 2016), although one study did not find such an effect of mindfulness training on level of vmHRV (Nyklicek et al., 2013).
In the present study the aim was to explore if dispositional self-compassion related with vmHRV above and beyond mindfulness. Several authors have emphasized the importance of measuring peoples’ dispositional levels, since pre-existing dispositional mindfulness may influence what is considered an effect of mindfulness training (such as when using vmHRV as an effect measure; Tang et al., 2016; Wheeler et al., 2016; Zhuang et al., 2017). The use of self-report instrument of dispositional self-compassion with SCS and mindfulness with FFMQ allowed for comparison of the effects found on vmHRV with previous findings using self-reported symptoms as outcome variables (e.g., Van Dam et al., 2011; Woodruff et al., 2014). However, the experimental design of relying solely on self-reports in a small sample of healthy adults and including only resting vmHRV as a trait-measure of psychophysiological flexibility may limit the generalizability of the findings. The objective was therefore to conduct an explorative pilot study in which the results can be important for generating hypotheses for future studies. We primarily explored the common and unique explained variance of dispositional self-reported mindfulness and self-compassion on level of resting vmHRV. A secondary aim was to replicate previous findings that self-compassion explained variance beyond mindfulness on self-reported distress symptoms of anxiety and negative rumination.
Participants were recruited through ads and posters to the student population of the University of Bergen, Norway (see also Svendsen et al., 2016; Visted et al., 2017; Sorensen et al., 2018, 2019). Initially we included 56 participants, but three participants were excluded due to poor data quality on the vmHRV-measures. Thus, the sample consisted of 53 students (36 female, mean age = 23.6 years, SD = 2.52; mean body mass index (BMI) = 21.80, SD = 2.33).
Written informed consent was obtained from all participants, in accordance with the Helsinki declaration. The protocol was approved by the Regional Committees for Medical and Health Research Ethics – South East Norway, Gullhaugveien 1-3, 0318 Oslo (study number 2014/148). Exclusion criteria were usage of sedative or psychoactive medication, heart conditions, and previous experience with mindfulness, i.e., attendance at mindfulness courses, retreats, or other kinds of formalized mindfulness instruction.
When participants arrived on the testing day, they received a detailed explanation of the tests involved, but no information regarding hypotheses of the study. They were then seated in a room in which they were asked to fill out a package of questionnaires, including the SCS, the FFMQ, the Rumination Reflection Questionnaire (RRQ), the State-Trait Anxiety Questionnaire, as well as information about age, gender, and BMI. One at a time, they were invited to move to an experimental room, in order to record their heart rate with an electrocardiogram (ECG). Participants were asked not to exercise, smoke or drink caffeine six hours prior to the experiment.
Participants were offered a brief and intensive mindfulness course free of charge, and were not offered any additional compensation for participation in the study.
The ECG was recorded with a standard lead-II setup and digitized at 1000 Hz. Data from all participants were collected at approximately the same time in the afternoon in order to control for circadian effects. The signal was obtained through an A/D converter (Biopac, MP36, BIOPAC System, Inc., Santa Barbara, CA, United States) recorded with Biopac 4.0 BSL (BIOPAC Systems, Inc., Santa Barbara, CA, United States). VmHRV was assessed during a 5-min period in which the participants were asked to find a position that felt comfortable and relax as much as possible.
Heart-rate data were manually checked for artifacts (movement, electrode noise, and extraordinary peaks) offline, and then subjected to a vmHRV analysis with Kubios version 2.0 (Tarvainen et al., 2014). In the current study, we used the high frequency (HF) power measured in milliseconds as a measure of vmHRV. HF is considered to be a valid measure of vmHRV (Task force, 1996; Thayer and Sternberg, 2006; Li et al., 2009; Williams et al., 2015), and is the most commonly used in previous research investigating the relationship between self-compassion, mindfulness and vmHRV (Takahashi et al., 2005; Tang et al., 2009; Delgado-Pastor et al., 2013; Kok et al., 2013; Krygier et al., 2013; Nyklicek et al., 2013; Nijjar et al., 2014; Azam et al., 2015; Watford and Stafford, 2015; May et al., 2016). The HF measure correlated highly (r = 0.94, p > 0.001) with the time domain Root-mean square of successive R-R intervals (RMSSD), also a measure of vagus-mediated autonomic influence on the heart (Task force, 1996; Shaffer and Ginsberg, 2017). Additional correlations between the RMSSD and the total scores of the FFMQ and the SCS are included in Supplementary Material.
All vmHRV data were subjected to a HRV analysis with Kubios version 2.0 (Tarvainen et al., 2014), and HF and RMSSD was calculated. Trend components were removed with the smoothness priors detrending method (λ = 500).
The SCS (Neff, 2003a) consists of 26 items reflecting three positive and three negative subscales. The positive subscales are: self-kindness (e.g., “I try to be loving toward myself when I’m feeling emotional pain.”), common humanity (e.g., “When things are going badly for me, I see the difficulties as part of life that everyone goes through”), and mindfulness (e.g., “When something upsets me I try to keep my emotions in balance”). The negative subscales are: self-judgment (e.g., “When times are really difficult, I tend to be tough on myself”), isolation (e.g., “When I think about my inadequacies, it tends to make me feel more separate and cut off from the rest of the world”), and over-identification (e.g., “When I’m feeling down I tend to obsess and fixate on everything that’s wrong”). Items are rated on a five-point Likert-type scale where 1 equals “almost never” and 5 equals “almost always.” Low scores on the negative subscales and high scores on the positive subscales reflect an overall high level of self-compassion.
The SCS has been shown to have good reliability and cross-cultural validity (Neff et al., 2008). We employed a Norwegian validated translation of the SCS (Dundas et al., 2016; see Supplementary Material to article for validation of the scale in Norwegian).
The FFMQ (Baer et al., 2006) is a 39 items self-report measure of mindfulness. Items are rated on a five-point Likert -type scale from 1 (“never or very rarely true”) to 5 (“very often or always true”), measuring five factors: observing (e.g., “I notice the smells and aromas of things”), describing (e.g., “I am good at finding words to describe my feelings”), acting with awareness (e.g., “I find myself doing things without paying attention”; reverse scored item), non-judging of inner experience (e.g., “I think some of my emotions are bad or inappropriate and I should not feel them”; reverse scored item), and non-reactivity to inner experience (e.g., “I perceive my feelings and emotions without having to react to them”).
The FFMQ has shown high construct validity (Baer et al., 2006, 2008). The five subscales are internally consistent, with alpha coefficients ranging from 0.76 to 0.91 (Baer et al., 2006). The test-retest reliability was demonstrated to be good to excellent in a Dutch sample (Veehof et al., 2011). In the present study we used a Norwegian validated translation of the FFMQ (Dundas et al., 2013).
In order to measure trait anxiety, we used the Trait subscale of the State-Trait Anxiety Inventory (STAI; Spielberger et al., 1983), consisting of 20 items. Examples of items are “I am a steady person” (reversed) and “I have disturbing thoughts.” Scores are rated on a four point Likert scale ranging from 1 (”almost never”) to 4 (”almost always”). The Trait scale of the STAI has shown excellent internal consistency (average α < 0.89) and test-retest reliability (average r = 0.88; Barnes et al., 2002). In the present study we used a Norwegian translation of the STAI (Spielberger et al., 1983).
Rumination was measured using the 12-item Rumination subscale of the RRQ (Trapnell and Campbell, 1999). Example items are “Long after an argument or disagreement is over with, my thoughts keep going back to what happened” and “I often find myself re-evaluating something I have done.” Answers are rated on a five-point Likert-type scale ranging from 1, indicating “strongly disagree”, to 5, equaling “strongly agree”. We employed a Norwegian validated translation of the RRQ-Rum scale (Verplanken et al., 2007).
All vmHRV measures were log transformed as to approximate a normal distribution. The data were statistically analyzed using SPSS version 24.0. Pearson bivariate correlational analyses were conducted to test the relationship between vmHRV, the SCS scores, and the FFMQ scores, respectively. In order to ensure that the bivariate relationships observed were not confounded by shared variance between the total scores from the FFMQ and the SCS, two linear hierarchical regression analyses were run to test the common and unique explained variance of the total scores of the FFMQ and the SCS, respectively, on the level of vmHRV. To determine the unique explained variance of the FFMQ and the SCS, respectively, the FFMQ was in the first regression model entered in the first step and the SCS in the second step, and thereafter, in the second regression model, the SCS was entered in the first step and the FFMQ in the second step (i.e., with F analysis of stepwise change in explained variance). In these hierarchical linear regression models, effects were adjusted for level of BMI (Koenig et al., 2014) and gender (Koenig and Thayer, 2016) on vmHRV. Further, the common and unique explained variance of the total scores of the FFMQ and the SCS, respectively, were also tested with linear hierarchical regression models with self-reported levels of anxiety and negative rumination, respectively, as outcome variables. These results are briefly presented in the section “Results,” and tables can be found in Supplementary Material.
No outliers were detected (±3 standard deviations from the sample mean). Missing item scores for six participants were replaced by sample mean for each item. The skewness and kurtosis levels for FFMQ, SCS, and vmHRV were within border limits (z > 1.96 or z < −1.96; Field, 2013).
In the current study, the level of self-compassion (SCS) ranged from 1.31 to 4.27, with a mean level of 2.78 (SD = 0.83). The level of mindfulness (FFMQ) ranged from 2.03 to 4.74, with a mean of 3.04 (SD = 0.64). The SCS total score and the FFMQ total score demonstrated excellent internal consistencies with Cronbach’s alpha coefficients of 0.96 and 0.95, respectively. The level of trait anxiety (trait subscale of the STAI) ranged from 20 to 69 with a mean of 43.75 (SD = 12.58), and the level of rumination (rumination subscale of the RRQ) ranged from 14.0 to 57.0, with a mean level of 43.71 (SD = 10.58). The trait subscale of the STAI and the rumination subscale of the RRQ evidenced excellent internal consistencies with Cronbach’s alphas of 0.95 and 0.93, respectively.
There was a significant correlation between the total scores of the SCS and the FFMQ (see Table 1). Only the SCS total score, and not the FFMQ total score, correlated significantly with level of vmHRV (see also Supplementary Table 1). Higher SCS total scores correlated with higher levels of vmHRV. There was no significant correlation between vmHRV and the demographic variables of BMI, gender, and age.
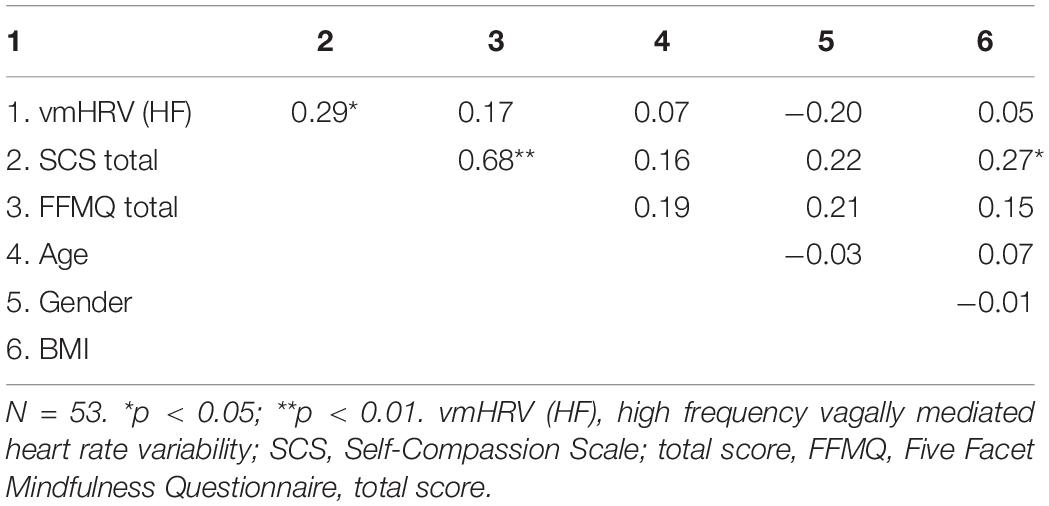
Table 1. Bivariate correlations between vmHRV, SCS, and FFMQ total scores, and covariates.
In hierarchical linear regression models, only the SCS total scores, and not the FFMQ total scores, significantly explained variance of the level of vmHRV (see Table 2). The FFMQ total scores did not significantly explain vmHRV independently of whether the scores were included in the first or second step of the model. The SCS total scores explained 7.3% of the level of vmHRV when controlling for the level of the FFMQ total scores in the first step of the model, and explained 11.7% when not controlling for the level of the FFMQ total scores (the SCS total scores were included in the first step). The covariate of gender predicted significantly level of vmHRV in the second step of the regression models when both the total scores of the FFMQ and the SCS were included as predictors. Level of BMI did not affect level of vmHRV as a covariate in the regression models.
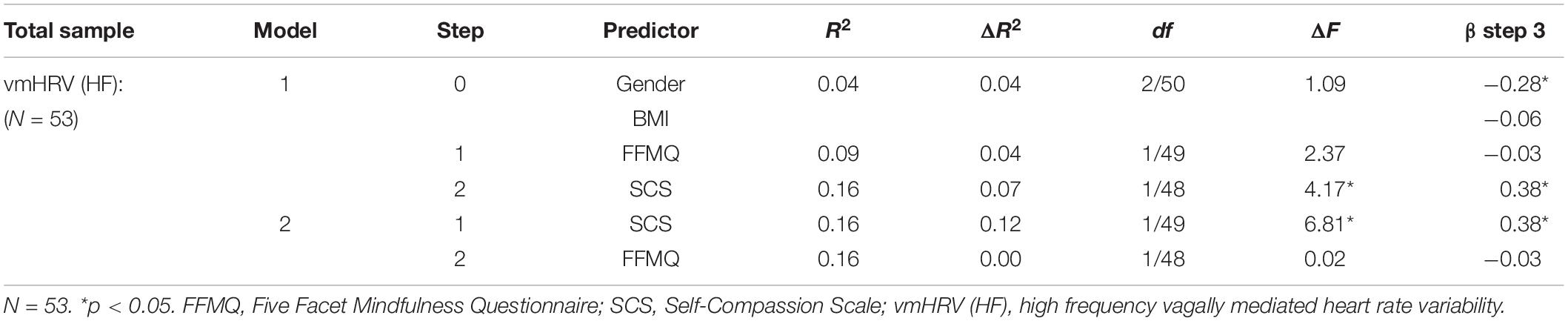
Table 2. Hierarchical regression analysis of the relation between FFMQ/SCS and vmHRV.
Linear hierarchical regression analyses showed that both the total scores from the FFMQ and the SCS significantly explained lower levels of self-reported trait anxiety and negative rumination when entered in the first step of the model, respectively (see Supplementary Table 2). The SCS total scores explained higher amounts of variance than the FFMQ total scores, whether entered in the first or second step. The FFMQ total scores only showed a trend for significantly explaining higher levels of trait anxiety when controlling for the effect of SCS total scores (by entering the FFMQ total scores in the second step).
The present pilot study provided preliminary results indicating that dispositional self-compassion is a stronger predictor of vmHRV than mindfulness. Self-compassion as measured with the total scores of the SCS associated uniquely with higher vmHRV when controlling for the effect of mindfulness as measured by the total scores of the FFMQ. This suggests that being more self-compassionate associates with a more flexible modulation of physiological responses compared to being low on self-compassion. We also found as previous research relying on self-report measures of emotional distress (e.g., Van Dam et al., 2011; Woodruff et al., 2014) that the total scores of the SCS explained more variance than the total scores of the FFMQ on self-report measures of anxiety and negative rumination. The main contribution of the present study was thus to expand previous research with self-reports by including a psychophysiological measure indicative of trait-like emotional stress reactivity.
Our preliminary findings suggest that dispositional self-compassion is an important psychological buffer against emotional stress. It seems to provide emotional safety when suffering and may also be related to increased self-efficacy that one will be able to provide oneself with the emotional support and warmth needed in times of difficulty (Finlay-Jones, 2017). Although mindfulness and self-compassion are deeply interconnected and reciprocally facilitate each other (Baer, 2010; Neff and Dahm, 2015), it has been hypothesized that self-compassion is distinguishable from mindfulness in several ways that may be particularly important for stress regulation. Self-compassion seems to be applicable predominantly in times of suffering, whereas mindfulness taps the ability to be present with a much broader specter of experiences (i.e., not only difficult experiences, but also positive and neutral ones; Germer, 2009; Neff and Dahm, 2015). Moreover, self-compassion seems to focus more on common humanity; the recognition that suffering is a normal part of life and that everyone fails sometimes (Neff and Dahm, 2015). Finally, self-compassion more explicitly emphasizes self-soothing (Neff and Dahm, 2015). This ability to soothe and comfort oneself is indeed theoretically proposed to be connected to vagal activity (Porges, 2007), leading to higher physiological flexibility across situations. Therefore, the current study has followed the recommendation of compassion research to include vmHRV as a primary outcome measure. Higher vmHRV may as such represent the physiological signature of a trait-like compassionate responding (Kirby et al., 2017).
Interestingly, we found that dispositional mindfulness as measured by the FFMQ was not significantly associated with level of vmHRV. It appears that there is stronger evidence for trained mindfulness to predict higher vmHRV (e.g., Ditto et al., 2006; Delgado-Pastor et al., 2013; Nijjar et al., 2014; Shearer et al., 2016) compared to dispositional mindfulness (e.g., Prazak et al., 2012; Mankus et al., 2013). Some of the studies that have found a significant association between dispositional mindfulness and level of vmHRV have measured heart rate under stress contingencies (Fogarty et al., 2015; Kadziolka et al., 2016) or included participants with high levels of anxiety symptoms (Mankus et al., 2013). In the present study we focused on resting vmHRV since this is the condition that have been highlighted to be a trait-marker of flexibility in psychophysiological regulation (Thayer and Lane, 2009; Thayer et al., 2009). However, it is shown that resting vmHRV explains about 50% of trait-like aspects of personality (Bertsch et al., 2012). This means that resting vmHRV will also reflect state aspects, which for instance can be influenced by the context of the test condition and each participant’s reaction to this context. Future studies are as such encouraged to study the common and unique associations between mindfulness and self-compassion and level of vmHRV also under stress conditions or after stress modulation.
It is possible that effects of mindfulness are best captured by measuring effects of training rather than using self-reports (e.g., Tang et al., 2015). However, mindfulness training is shown to increase self-compassion (Shapiro et al., 2005; Kuyken et al., 2010), therefore effects of mindfulness training can encompass also increased levels of self-compassion. In process-oriented research there is a wish to disentangle effects of self-compassion from mindfulness per se (Kuyken et al., 2010). Then the applied questionnaires of the FFMQ and the SCS are the most commonly used in the literature examining these concepts, despite them being under scrutiny on psychometrical grounds (Park et al., 2013; Williams et al., 2014; Strauss et al., 2016 see also Grossman and Van Dam, 2011). Thus, important to note, despite self-reports being a common method used in research investigating effects of self-compassion and mindfulness on mental health, it can be biased information (Grossman, 2011; Kazdin, 2014). For instance, it might be easier for participants to self-report on positive attitudes toward oneself than it is to self-report frequency of past mindful states (Van Dam et al., 2011). In fact, it has been raised concerns that mindfulness taps into higher-order cognitive processes that are challenging for individuals to be aware of and to report on in questionnaires (Van Dam et al., 2011; see also Nisbett and Wilson, 1977). Therefore, future studies can address this limitation by designing and/or using experimental conditions independently assessing self-compassion and mindfulness. For instance, a recent study of self-compassion and vmHRV (Kirschner et al., 2019) showed that an experimental condition of self-compassion was superior in predicting higher vmHRV compared to conditions not representing self-compassion.
The experimental design of the present study has several limitations that future studies are encouraged to address. As already mentioned, research has shown that the state component in resting vmHRV is greater than previously thought, encouraging the inclusion of experimentally conditioned states recordings such as a stress-induction (see Bertsch et al., 2012). The correlational design does not allow for causal interpretations, which could have been addressed by including repeated measures of vmHRV and/or self-compassion and ECG recordings during exercises of mindfulness and self-compassion. Also, we have followed the recommendation of about 5 min ECG recordings (Task force, 1996), which may be less reliable than applying longer recordings (Bourdillon et al., 2017). The use of self-reports could have been complemented by also including experimental conditions of self-compassion and mindfulness. Finally, the present pilot study included a small sample consisting of young, healthy and well-functioning students, which may not be representative of other populations. The statistical power may as such have been restricted to detect effects of for instance dispositional mindfulness on vmHRV. This can be observed in that the explained variance (R2) indicated a small effect size of the model when including the two related concepts of dispositional self-compassion and mindfulness as predictors of vmHRV.
In summary, the present pilot study suggests that dispositional self-compassion associates with better psychophysiological regulation of emotional arousal compared to mindfulness. Taking into account the explorative nature of this study, the results point to self-compassion having the potential to provide a buffer against psychophysiological stress reactivity and supports targeting self-compassion in clinical work. The findings correspond to recent developments in the clinical mindfulness field, toward increasing the explicit focus of self-compassion in mindfulness-based interventions (Feldman and Kuyken, 2011; Segal et al., 2013). Future studies are encouraged to continue shedding light on the unique and common benefits of being self-compassionate and mindful.
The datasets generated for this study are available on request to the corresponding author.
The participants gave informed consent in accordance with the Helsinki declaration, and the protocol was approved by the Regional Ethics Committee (South-East, Study number 2014/148).
LS and ES: project leaders. JS, ES, BO, JV, EV, HN, P-EB, and LS: conception and design. JS, ES, BO, JV, EV, and LS: collection of the data. JS and LS: analysis and interpretation, and writing of the manuscript. ES, BO, JV, EV, ID, HN, and P-EB: critical review of the manuscript. JS, ES, BO, JV, EV, ID, HN, P-EB, and LS: final approval for publication.
This study was funded through internal fundings by the University of Bergen and the Meltzer Fund (grant no. 810438/1.1).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.00614/full#supplementary-material
Appelhans, B. M., and Luecken, L. J. (2006). Heart rate variability as an index of regulated emotional responding. Rev. Gen. Psychol. 10, 229–240. doi: 10.1037/1089-2680.10.3.229
Arch, J. J., Brown, K. W., Dean, D. J., Landy, L. N., Brown, K. D., and Laudenslager, M. L. (2014). Self-compassion training modulates alpha-amylase, heart rate variability, and subjective responses to social evaluative threat in women. Psychoneuroendocrinology 42, 49–58. doi: 10.1016/j.psyneuen.2013.12.018
Azam, M. A., Katz, J., Fashler, S. R., Changoor, T., Azargive, S., and Ritvo, P. (2015). Heart rate variability is enhanced in controls but not maladaptive perfectionists during brief mindfulness meditation following stress-induction: a stratified-randomized trial. Int. J. Psychophysiol. 98, 27–34. doi: 10.1016/j.ijpsycho.2015.06.005
Baer, R. A. (2010). “Self-compassion as a mechanism of change in mindfulness and acceptance-based treatments,” in Assessing Mindfulness & Acceptance Processes in Clients : Illuminating the Theory and Practice of Change, ed. R. A. Baer (Oakland, CA: Context press), 135–153.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., and Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment 13, 27–45. doi: 10.1177/1073191105283504
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment 15, 329–342. doi: 10.1177/1073191107313003
Barnes, L. L. B., Harp, D., and Jung, W. S. (2002). Reliability generalization of scores on the Spielberger state-trait anxiety inventory. Educ. Psychol. Meas. 62, 603–618. doi: 10.1177/0013164402062004005
Bertsch, K., Hagemann, D., Naumann, E., Schachinger, H., and Schulz, A. (2012). Stability of heart rate variability indices reflecting parasympathetic activity. Psychophysiology 49, 672–682. doi: 10.1111/j.1469-8986.2011.01341.x
Beshai, S., Prentice, J. L., and Huang, V. (2017). Building blocks of emotional flexibility: trait mindfulness and self-compassion are associated with positive and negative mood shifts. Mindfulness 9, 939–948. doi: 10.1007/s12671-017-0833-8
Bourdillon, N., Schmitt, L., Yazdani, S., Vesin, J. M., and Millet, G. P. (2017). Minimal window duration for accurate HRV recording in athletes. Front. Neurosci. 11:456. doi: 10.3389/fnins.2017.00456
Brown, K. W., and Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 84, 822–848. doi: 10.1037/0022-3514.84.4.822
Brzozowski, A., Gillespie, S. M., Dixon, L., and Mitchell, I. J. (2017). Mindfulness dampens cardiac responses to motion scenes of violence. Mindfulness 9, 574–584. doi: 10.1007/s12671-017-0799-6
Chalmers, J. A., Heathers, J. A., Abbott, M. J., Kemp, A. H., and Quintana, D. S. (2016). Worry is associated with robust reductions in heart rate variability: a transdiagnostic study of anxiety psychopathology. BMC Psychol. 4:32. doi: 10.1186/s40359-016-0138-z
Chalmers, J. A., Quintana, D. S., Abbott, M. J., and Kemp, A. H. (2014). Anxiety disorders are associated with reduced heart rate variability: a meta-analysis. Front. 5:80. doi: 10.3389/fpsyt.2014.00080
Dahm, K. A., Meyer, E. C., Neff, K. D., Kimbrel, N. A., Gulliver, S. B., and Morissette, S. B. (2015). Mindfulness, self-compassion, posttraumatic stress disorder symptoms, and functional disability in U.S. Iraq and Afghanistan War Veterans. J. Trauma Stress 28, 460–464. doi: 10.1002/jts.22045
Delgado-Pastor, L. C., Perakakis, P., Subramanya, P., Telles, S., and Vila, J. (2013). Mindfulness (Vipassana) meditation: effects on P3b event-related potential and heart rate variability. Int. J. Psychophysiol. 90, 207–214. doi: 10.1016/j.ijpsycho.2013.07.006
Ditto, B., Eclache, M., and Goldman, N. (2006). Short-term autonomic and cardiovascular effects of mindfulness body scan meditation. Ann. Behav. Med. 32, 227–234. doi: 10.1207/s15324796abm3203_9
Dundas, I., Svendsen, J. L., Wiker, A. S., Granli, K. V., and Schanche, E. (2016). Self-compassion and depressive symptoms in a Norwegian student sample. Nordic Psychol. 68, 58–72. doi: 10.1080/19012276.2015.1071203
Dundas, I., Vollestad, J., Binder, P. E., and Sivertsen, B. (2013). The five factor mindfulness questionnaire in Norway. Scand. J. Psychol. 54, 250–260. doi: 10.1111/sjop.12044
Feldman, C., and Kuyken, W. (2011). Compassion in the landscape of suffering. Contemp. Buddhism 12, 143–155. doi: 10.1080/14639947.2011.564831
Field, A. P. (2013). Discovering Statistics using IBM SPSS Statistics. London: SAGE Publications Ltd.
Finlay-Jones, A. L. (2017). The relevance of self-compassion as an intervention target in mood and anxiety disorders: a narrative review based on an emotion regulation framework. Clin. Psychol. 21, 90–103. doi: 10.1111/cp.12131
Fogarty, F. A., Lu, L. M., Sollers, J. J., Krivoschekov, S. G., Booth, R. J., and Consedine, N. S. (2015). Why it pays to be mindful: trait mindfulness predicts physiological recovery from emotional stress and greater differentiation among negative emotions. Mindfulness 6, 175–185. doi: 10.1007/s12671-013-0242-6
Germer, C. K. (2009). The Mindful Path to Self-Compassion: Freeing Yourself from Destructive Thoughts and Emotions. New York, NY: Guilford Press.
Gross, J. J., and Munoz, R. F. (1995). Emotion regulation and mental health. Clin. Psychol. Sci. Pract. 2, 151–164. doi: 10.1111/j.1468-2850.1995.tb00036.x
Grossman, P. (2011). Defining mindfulness by how poorly I think I pay attention during everyday awareness and other intractable problems for psychology’s (re)invention of mindfulness: comment on Brown et al. (2011). Psychol. Assess. 23, 1034–1040. doi: 10.1037/a0022713
Grossman, P., and Van Dam, N. T. (2011). Mindfulness, by any other name: trials and tribulations of sati in western psychology and science. Contemp. Buddhism 12, 219–239. doi: 10.1080/14639947.2011.564841
Holzman, J. B., and Bridgett, D. J. (2017). Heart rate variability indices as bio-markers of top-down self-regulatory mechanisms: a meta-analytic review. Neurosci. Biobehav. Rev. 74(Pt A), 233–255. doi: 10.1016/j.neubiorev.2016.12.032
Joo, H. M., Lee, S. J., Chung, Y. G., and Shin, I. Y. (2010). Effects of mindfulness-based stress reduction program on depression, anxiety and stress in patients with aneurysmal subarachnoid hemorrhage. J. Korean Neurosurg. Soc. 47, 345–351. doi: 10.3340/jkns.2010.47.5.345
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. Sci. Pract. 10, 144–156. doi: 10.1093/clipsy/bpg016
Kadziolka, M. J., Di Pierdomenico, E.-A., and Miller, C. J. (2016). Trait-like mindfulness promotes healthy self-regulation of stress. Mindfulness 7, 236–245. doi: 10.1007/s12671-015-0437-0
Kazdin, A. E. (2014). Research Design in Clinical Psychology, 4th Edn. Fareham: Ashford Colour Press Ltd.
Kemp, A. H., Quintana, D. S., Gray, M. A., Felmingham, K. L., Brown, K., and Gatt, J. M. (2010). Impact of depression and antidepressant treatment on heart rate variability: a review and meta-analysis. Biol. Psychiatry 67, 1067–1074. doi: 10.1016/j.biopsych.2009.12.012
Kirby, J. N., Doty, J. R., Petrocchi, N., and Gilbert, P. (2017). The current and future role of heart rate variability for assessing and training compassion. Front. Public Health 5:40. doi: 10.3389/fpubh.2017.00040
Kirschner, H., Kuyken, W., Wright, K., Roberts, H., Brejcha, C., and Karl, A. (2019). Soothing your heart and feeling connected: a new experimental paradigm to study the benefits of self-compassion. Clin. Psychol. Sci. 7, 545–565. doi: 10.1177/2167702618812438
Koenig, J., Jarczok, M. N., Warth, M., Ellis, R. J., Bach, C., Hillecke, T. K., et al. (2014). Body mass index is related to autonomic nervous system activity as measured by heart rate variability- A replication using short term measurements. J. Nutr. Health Aging 18, 300–302. doi: 10.1007/s12603-014-0022-6
Koenig, J., and Thayer, J. F. (2016). Sex differences in healthy human heart rate variability: a meta-analysis. Neurosci. Biobehav. Rev. 64, 288–310. doi: 10.1016/j.neubiorev.2016.03.007
Kok, B. E., Coffey, K. A., Cohn, M. A., Catalino, L. I., Vacharkulksemsuk, T., Algoe, S. B., et al. (2013). How positive emotions build physical health: perceived positive social connections account for the upward spiral between positive emotions and vagal tone. Psychol. Sci. 24, 1123–1132. doi: 10.1177/0956797612470827
Krygier, J. R., Heathers, J. A., Shahrestani, S., Abbott, M., Gross, J. J., and Kemp, A. H. (2013). Mindfulness meditation, well-being, and heart rate variability: a preliminary investigation into the impact of intensive Vipassana meditation. Int. J. Psychophysiol. 89, 305–313. doi: 10.1016/j.ijpsycho.2013.06.017
Kuyken, W., Watkins, E., Holden, E., White, K., Taylor, R. S., Byford, S., et al. (2010). How does mindfulness-based cognitive therapy work? Behav. Res. Ther. 48, 1105–1112. doi: 10.1016/j.brat.2010.08.003
Li, Z., Snieder, H., Su, S., Ding, X., Thayer, J. F., Treiber, F. A., et al. (2009). A longitudinal study in youth of heart rate variability at rest and in response to stress. Int. J. Psychophysiol. 73, 212–217. doi: 10.1016/j.ijpsycho.2009.03.002
Luo, X., Qiao, L., and Che, X. (2018). Self-compassion modulates heart rate variability and negative affect to experimentally induced stress. Mindfulness 9, 1522–1528. doi: 10.1007/s12671-018-0900-9
Mankus, A. M., Aldao, A., Kerns, C., Wright Mayville, E., and Mennin, D. S. (2013). Mindfulness and heart rate variability in individuals with high and low generalized anxiety symptoms. Behav. Res. Ther. 51, 386–391. doi: 10.1016/j.brat.2013.03.005
Matos, M., Duarte, C., Duarte, J., Pinto-Gouveia, J., Petrocchi, N., Basran, J., et al. (2017). Psychological and physiological effects of compassionate mind training: a pilot randomised controlled study. Mindfulness 8, 1699–1712. doi: 10.1007/s12671-017-0745-7
May, R. W., Bamber, M., Seibert, G. S., Sanchez-Gonzalez, M. A., Leonard, J. T., Salsbury, R. A., et al. (2016). Understanding the physiology of mindfulness: aortic hemodynamics and heart rate variability. Stress Int. J. Biol. Stress 19, 168–174. doi: 10.3109/10253890.2016.1146669
Neff, K. (2003a). Self-compassion: an alternative conceptualization of a healthy attitude toward oneself. Self Identity 2, 85–101. doi: 10.1080/15298860309032
Neff, K. (2003b). The development and validation of a scale to measure self-compassion. Self Identity 2, 223–250. doi: 10.1080/15298860309027
Neff, K., and Dahm, K. A. (2015). “Self-compassion: what it is, what it does, and how it relates to mindfulness,” in Handbook of Mindfulness and Self-Regulation, eds B. Ostafin, M. Robinson, and B. Meier (New York, NY: Springer), 121–137. doi: 10.1007/978-1-4939-2263-5_10
Neff, K., Pisitsungkagarn, K., and Hsieh, Y. P. (2008). Self-compassion and self-construal in the United States, Thailand, and Taiwan. J. Cross Cult. Psychol. 39, 267–285. doi: 10.1177/0022022108314544
Nijjar, P. S., Puppala, V. K., Dickinson, O., Duval, S., Duprez, D., Kreitzer, M. J., et al. (2014). Modulation of the autonomic nervous system assessed through heart rate variability by a mindfulness based stress reduction program. Int. J. Cardiol. 177, 557–559. doi: 10.1016/j.ijcard.2014.08.116
Nisbett, R. E., and Wilson, T. D. (1977). Telling more than we can know: verbal reports on mental processes. Psychol. Rev. 84, 231–259. doi: 10.1037/0033-295X.84.3.231
Nyklicek, I., Mommersteeg, P. M., Van Beugen, S., Ramakers, C., and Van Boxtel, G. J. (2013). Mindfulness-based stress reduction and physiological activity during acute stress: a randomized controlled trial. Health Psychol. 32, 1110–1113. doi: 10.1037/a0032200
Park, T., Reilly-Spong, M., and Gross, C. R. (2013). Mindfulness: a systematic review of instruments to measure an emergent patient-reported outcome (PRO). Qual. Life Res. 22, 2639–2659. doi: 10.1007/s11136-013-0395-8
Petrocchi, N., Ottaviani, C., and Couyoumdjian, A. (2017). Compassion at the mirror: exposure to a mirror increases the efficacy of a self-compassion manipulation in enhancing soothing positive affect and heart rate variability. J. Posit. Psychol. 12, 525–536. doi: 10.1080/17439760.2016.1209544
Porges, S. W. (2007). The polyvagal perspective. Biol. Psychol. 74, 116–143. doi: 10.1016/j.biopsycho.2006.06.009
Prazak, M., Critelli, J., Martin, L., Miranda, V., Purdum, M., and Powers, C. (2012). Mindfulness and its role in physical and psychological health. Appl. Psychol. Health Well Being 4, 91–105. doi: 10.1111/j.1758-0854.2011.01063.x
Rockliff, H., Gilbert, P., McEwan, K., Lightman, S., and Glover, D. (2008). A pilot exploration of heart rate variability and salivary cortisol responses to compassion-focused imagery. Clin. Neuropsychiatry J. Treat. Eval. 5, 132–139.
Segal, Z. V., Williams, J. M. G., and Teasdale, J. D. (2013). Mindfulness-Based Cognitive Therapy for Depression, 2nd Edn. New York, NY: Guilford Press.
Shaffer, F., and Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Front. Public Health 5:17. doi: 10.3389/fpubh.2017.00258
Shapiro, S. L., Astin, J. A., Bishop, S. R., and Cordova, M. (2005). Mindfulness-based stress reduction for health care professionals: results from a randomized trial. Int. J. Stress Manag. 12, 164–176. doi: 10.1037/1072-5245.12.2.164
Shearer, A., Hunt, M., Chowdhury, M., and Nicol, L. (2016). Effects of a brief mindfulness meditation intervention on student stress and heart rate variability. Int. J. Stress Manag. 23, 232–254. doi: 10.1037/a0039814
Sorensen, L., Osnes, B., Visted, E., Svendsen, J. L., Adolfsdottir, S., Binder, P. E., et al. (2018). Dispositional mindfulness and attentional control: the specific association between the mindfulness facets of non-judgment and describing with flexibility of early operating orienting in conflict detection. Front. Psychol. 9:2359. doi: 10.3389/fpsyg.2018.02359
Sorensen, L., Wass, S., Osnes, B., Schanche, E., Adolfsdottir, S., Svendsen, J. L., et al. (2019). A psychophysiological investigation of the interplay between orienting andexecutive control during stimulus conflict: a heart rate variability study. Physiol. Behav. 211, 1–8. doi: 10.1016/j.physbeh.2019.112657
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., and Jacobs, G. A. (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
Strauss, C., Lever Taylor, B., Gu, J., Kuyken, W., Baer, R., Jones, F., et al. (2016). What is compassion and how can we measure it? A review of definitions and measures. Clin. Psychol. Rev. 47, 15–27. doi: 10.1016/j.cpr.2016.05.004
Svendsen, J. L., Osnes, B., Binder, P.-E., Dundas, I., Visted, E., Nordby, H., et al. (2016). Trait self-compassion reflects emotional flexibility through an association with high vagally mediated heart rate variability. Mindfulness 7, 1103–1113. doi: 10.1007/s12671-016-0549-1
Takahashi, T., Murata, T., Hamada, T., Omori, M., Kosaka, H., Kikuchi, M., et al. (2005). Changes in EEG and autonomic nervous activity during meditation and their association with personality traits. Int. J. Psychophysiol. 55, 199–207. doi: 10.1016/j.ijpsycho.2004.07.004
Tang, Y.-Y., Holzel, B. K., and Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 16, 213–225. doi: 10.1038/nrn3916
Tang, Y.-Y., Holzel, B. K., and Posner, M. I. (2016). Traits and states in mindfulness meditation. Nat. Rev. Neurosci. 17:59. doi: 10.1038/nrn.2015.7
Tang, Y.-Y., Ma, Y., Fan, Y., Feng, H., Wang, J., Feng, S., et al. (2009). Central and autonomic nervous system interaction is altered by short-term meditation. Proc. Natl. Acad. Sci. U.S.A. 106, 8865–8870. doi: 10.1073/pnas.0904031106
Tarvainen, M. P., Niskanen, J. P., Lipponen, J. A., Ranta-aho, P. O., and Karjalainen, P. A. (2014). Kubios HRV - Heart rate variability analysis software. Comput. Methods Prog. Biomed. 113, 210–220. doi: 10.1016/j.cmpb.2013.07.024
Task force (1996). Task force. of the European Society of Cardiology and The North American Society of Pacing and electrophysiology. Heart rate variability - Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 17, 354–381. doi: 10.1161/01.CIR.93.5.1043
Thayer, J. F., Hansen, A. L., Saus-Rose, E., and Johnsen, B. H. (2009). Heart rate variability, prefrontal neural function, and cognitive performance: the neurovisceral integration perspective on self-regulation, adaptation, and health. Ann. Behav. Med. 37, 141–153. doi: 10.1007/s12160-009-9101-z
Thayer, J. F., and Lane, R. D. (2000). A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 61, 201–216. doi: 10.1016/S0165-0327(00)00338-4
Thayer, J. F., and Lane, R. D. (2009). Claude Bernard and the heart-brain connection: further elaboration of a model of neurovisceral integration. Neurosci. Biobehav. Rev. 33, 81–88. doi: 10.1016/j.neubiorev.2008.08.004
Thayer, J. F., and Sternberg, E. (2006). “Beyond heart rate variability - Vagal regulation of allostatic systems,” in Neuroendocrine and Immune Crosstalk, eds G. P. Chrousos, G. A. Kaltsas, and G. Mastorakos (Oxford: Blackwell Publishing), 361–372. doi: 10.1196/annals.1366.014
Trapnell, P. D., and Campbell, J. D. (1999). Private self-consciousness and the five-factor model of personality: distinguishing rumination from reflection. J. Pers. Soc. Psychol. 76, 284–304. doi: 10.1037/0022-3514.76.2.284
Van Dam, N. T., Sheppard, S. C., Forsyth, J. P., and Earleywine, M. (2011). Self-compassion is a better predictor than mindfulness of symptom severity and quality of life in mixed anxiety and depression. J. Anxiety Disord. 25, 123–130. doi: 10.1016/j.janxdis.2010.08.011
Veehof, M. M., ten Klooster, P. M., Taal, E., Westerhof, G. J., and Bohlmeijer, E. T. (2011). Psychometric properties of the dutch five facet mindfulness questionnaire (FFMQ) in patients with fibromyalgia. Clin. Rheumatol. 30, 1045–1054. doi: 10.1007/s10067-011-1690-9
Verplanken, B., Friborg, O., Trafimow, D., Woolf, K., and Wang, C. (2007). Mental habits: metacognitive reflection on negative self-thinking. J. Pers. Soc. Psychol. 92, 526–541. doi: 10.1037/0022-3514.92.3.526
Visted, E., Sorensen, L., Osnes, B., Svendsen, J. L., Binder, P.-E., and Schanche, E. (2017). The association between self-reported difficulties in emotion regulation and heart rate variability: the salient role of not accepting negative emotions. Front. Psychol. 8:328. doi: 10.3389/fpsyg.2017.00328
Watford, T. S., and Stafford, J. (2015). The impact of mindfulness on emotion dysregulation and psychophysiological reactivity under emotional provocation. Psychol. Conscious. Theory Res. Pract. 2, 90–109. doi: 10.1037/cns0000039
Wheeler, M. S., Arnkoff, D. B., and Glass, C. R. (2016). What is being studied as mindfulness meditation? Nat. Rev. Neurosci. 17:59. doi: 10.1038/nrn.2015.6
Williams, D. P., Cash, C., Rankin, C., Bernardi, A., Koenig, J., and Thayer, J. F. (2015). Resting heart rate variability predicts self-reported difficulties in emotion regulation: a focus on different facets of emotion regulation. Front. Psychol. 6:261. doi: 10.3389/fpsyg.2015.00261
Williams, M. J., Dalgleish, T., Karl, A., and Kuyken, W. (2014). Examining the factor structures of the five facet mindfulness questionnaire and the self-compassion scale. Psychol. Assess. 26, 407–418. doi: 10.1037/a0035566
Woodruff, S. C., Glass, C. R., Arnkoff, D. B., Crowley, K. J., Hindman, R. K., and Hirschhorn, E. W. (2014). Comparing self-compassion, mindfulness, and psychological inflexibility as predictors of psychological health. Mindfulness 5, 410–421. doi: 10.1007/s12671-013-0195-9
Woods, H., and Proeve, M. (2014). Relationships of mindfulness, self-compassion, and meditation experience with shame-proneness. J. Cogn. Psychother. 28, 20–33. doi: 10.1891/0889-8391.28.1.20
Keywords: self-compassion, mindfulness, heart rate variability, young adults, anxiety, rumination
Citation: Svendsen JL, Schanche E, Osnes B, Vøllestad J, Visted E, Dundas I, Nordby H, Binder P-E and Sørensen L (2020) Is Dispositional Self-Compassion Associated With Psychophysiological Flexibility Beyond Mindfulness? An Exploratory Pilot Study. Front. Psychol. 11:614. doi: 10.3389/fpsyg.2020.00614
Received: 08 May 2019; Accepted: 16 March 2020;
Published: 09 April 2020.
Edited by:
Hyemin Han, The University of Alabama, United StatesReviewed by:
Jonathan Greenberg, Harvard Medical School, United StatesCopyright © 2020 Svendsen, Schanche, Osnes, Vøllestad, Visted, Dundas, Nordby, Binder and Sørensen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julie Lillebostad Svendsen, anVsaWUuc3ZlbmRzZW5AdWliLm5v
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.