 Jesús Funuyet-Salas1*†
Jesús Funuyet-Salas1*† Agustín Martín-Rodríguez1†
Agustín Martín-Rodríguez1† Mercedes Borda-Mas1
Mercedes Borda-Mas1 María Luisa Avargues-Navarro1
María Luisa Avargues-Navarro1 Miguel Ángel Gómez-Bravo2
Miguel Ángel Gómez-Bravo2 Manuel Romero-Gómez3Rupert Conrad4†
Manuel Romero-Gómez3Rupert Conrad4† María Ángeles Pérez-San-Gregorio1†
María Ángeles Pérez-San-Gregorio1†- 1Department of Personality, Assessment, and Psychological Treatment, Faculty of Psychology, University of Seville, Seville, Spain
- 2Hepatic-Biliary-Pancreatic Surgery and Liver Transplant Unit, University Hospital Virgen del Rocío, Seville, Spain
- 3Digestive Diseases Unit, University Hospital Virgen del Rocío, Seville, Spain
- 4Department of Psychosomatic Medicine and Psychotherapy, University of Bonn, Bonn, Germany
Our objective was to analyze the differences in posttraumatic growth in 240 liver transplant recipients based on two factors. First, self-perceived health: better (Group 1 = G1) and worse (Group 2 = G2). Second, vitality: more (Group 3 = G3) and less (Group 4 = G4). The Posttraumatic Growth Inventory, SF-36 Health Survey (Item 2) and SF-12 Health Survey (vitality dimension) were used. Firstly, analyzing main effects recipients with better (G1) compared to worse (G2) self-perceived health, showed greater posttraumatic growth. Interaction effects were found on essential posttraumatic growth domains such as new possibilities (p = 0.040), personal strength (p = 0.027), and appreciation of life (p = 0.014). Statistically significant differences showed that among transplant recipients with worse self-perceived health (G2), those with more vitality had higher levels on abovementioned posttraumatic growth dimensions. However, in transplant recipients with better self-perceived health (G1) respective dimensions were not significantly influenced by the level of vitality. Among the recipients with less vitality (G4), those with better self-perceived health showed higher scores on abovementioned posttraumatic growth dimensions. We conclude that positive self-perceived health might compensate for a lack of vitality as well as a high level of vitality may compensate for negative self-perceived health regarding the development of crucial aspects of posttraumatic growth after liver transplantation.
Introduction
At the time of insufficiency or failure of a vital organ, transplantation presents an effective therapeutic alternative offering longer and better quality of life (Kugler et al., 2013). Specifically, liver transplantation is the best option when acute liver disease is triggered with severe short-term prognosis (Karam et al., 2003; Sirivatanauksorn et al., 2012).
Liver transplantation is a critical and determinant moment in life. In general, it gives hope of reestablishing a severely harmed state of health and quality of life, frequently after having lived with the disease and dysfunctionality for a long time (Ziȩba et al., 2015). However, transplantation may be a traumatic and highly stressful experience, among other reasons, because of the risks involved. Among these are death, relapse of the disease and dependency on immunosuppressants which may negatively interfere with the recipient’s quality of life (Grinyó et al., 2012; Pérez-San-Gregorio et al., 2012). Fantasies about the donor, symptoms of anxiety, depression and posttraumatic stress, or rejection of body image are psychological problems that usually appear after transplantation (Pérez-San-Gregorio et al., 2005; Baranyi et al., 2013; Annema et al., 2015).
The birth of positive psychology in the 1990s motivated development of a salutogenic perspective promoting health by studying, for example, strengths of individuals after a traumatic experience (Wu et al., 2015; Martz and Livneh, 2016). From this perspective, the focus of attention ceases to be placed exclusively on problems derived from transplantation by concentrating on the possibility of developing a positive transformation of life attributed to this traumatic experience (Anand-Kumar et al., 2014). Thus emerged the concept of posttraumatic growth, which alludes to a subjective experience of positive psychological change as a consequence of living through a highly stressful situation (Tedeschi and Calhoun, 2004), which challenges a person’s most basic core beliefs, self-concept and setting. It also favors elaboration of new cognitive schemas and development of different coping strategies (Tedeschi and Calhoun, 1995; Martins-da-Silva et al., 2011).
Posttraumatic growth has been widely studied in cancer patients (Casellas-Grau et al., 2018; Sharp et al., 2018; Tobin et al., 2018) and in those who have undergone hematopoietic stem cell transplantation (Forinder and Norberg, 2014; Jeon et al., 2015; Rosenberg et al., 2015). However, there has been relatively few research in liver transplant recipients. On the one hand, respective studies indicate that posttraumatic growth increases identification of recipients with their family and with other recipients (Scrignaro et al., 2016). On the other hand, they point to a close association between development of strong posttraumatic growth and the use of an affective, predominantly positive tone in telling about past life events (Ziȩba et al., 2015). Pérez-San-Gregorio et al. (2017b) also showed that a high level of posttraumatic growth is related to more use of adaptive, healthy coping strategies.
Other studies on posttraumatic growth and quality of life did not find a significant positive relationship between these two factors, such as the one by Moore et al. (2011) with a sample of 202 patients diagnosed with hepatobiliary carcinoma. A similar conclusion was found in a study by Fox et al. (2014) with 64 lung transplant recipients, which found only a minimal association between posttraumatic growth and quality of life related to physical functioning.
However, to date it is still unclear which mechanisms underlie the development of posttraumatic growth (Tedeschi and Calhoun, 2004). Nevertheless, it is clear that it involves cognitive and affective-motivational processes to be able to restructure cognitive schemata and their emotional underpinnings. In the context of posttraumatic growth after liver transplantation the construct of self-perceived health is very relevant. There is growing evidence for its importance regarding quality of life across a wide spectrum of disease entities. Thus, its influence on quality of life has been demonstrated in patients with cancer (Cameron et al., 2012; Hirsch et al., 2012), cardiovascular pathology (Bachmann et al., 2016; Ko and Boo, 2016), hepatitis and HIV (Marcellin et al., 2011; Elliott et al., 2017; Zhu et al., 2017). A study by Martín-Rodríguez et al. (2012) demonstrated the influence of self-perceived health on mental health in cirrhosis patients on the transplant waiting list and liver transplant recipients. According to a study by Pérez-San-Gregorio et al. (2013) on 168 liver transplant recipients, those with worse self-perceived health showed worse quality of life than those with better self-perceived health, especially in the bodily pain and general health dimensions. Against this backdrop, self-perceived health can be seen as a construct which can assist in predicting a patient’s affective development and potential posttraumatic growth after liver transplantation.
A second construct closely linked to posttraumatic growth is vitality (Tedeschi and Calhoun, 1996, 2004). A “positive feeling of having energy available to the self” (Nix et al., 1999, p. 266) is a widely accepted definition, accentuating the aspect of subjectively assessing one’s own emotional state. Even though self-perceived health and vitality are regarded as closely associated as, for example, in the construction of the SF-36, there is some evidence (Guérin, 2012) that it makes sense to disentangle them, as self-perceived health embraces the cognitive component of health-related self-assessment, whereas (self-perceived) vitality its affective-motivational component.
Against this backdrop, our study analyzes the differences in posttraumatic growth after liver transplantation as a function of two factors, self-perceived health and vitality. We specifically hypothesized that better self-perceived health and higher vitality of transplant recipients may mutually facilitate higher posttraumatic growth.
Materials and Methods
Participants
This research was approved by the Ethics Committee of the Virgen del Rocío University Hospital of Seville. At the beginning of recruitment all 569 patients still alive from a total clinical sample of 1053 recipients who had undergone transplantation surgery at the Virgen del Rocío University Hospital in Seville from 1990 to 2014 were informed about the possibility of study participation by the Association of Liver Transplant Recipients and the Hepatic-Biliary-Pancreatic Surgery and Liver Transplant Unit. Inclusion criteria for participants were as follows: (a) over 18 years of age, (b) informed consent, (c) reception of only one liver transplant. Exclusion criteria were (a) difficulties in understanding the evaluation instruments, (b) severe or disabling psychiatric disorder. The recruited sample consisted of 240 patients, 185 men and 55 women, with a mean age of 60.21 (SD = 9.30) years. Of the recipients, 61.7, 22.5, and 15.8% had a low (did not complete high school), intermediate (high school education), and higher formal education (A level), respectively. For further details, see Pérez-San-Gregorio et al. (2017a).
Instruments
Each participant filled out the 21 items on the Posttraumatic Growth Inventory (Tedeschi and Calhoun, 1996) which evaluates perception of personal benefits after experiencing a traumatic event. This instrument is structured in a Likert-type scale from 0 (“I did not experience this change as a result of my crisis”) to 5 (“I experienced this change to a very great degree as a result of my crisis”) in the positive direction.
The scale includes five domains of posttraumatic growth named new possibilities, relating to others, personal strength, spiritual change, and appreciation of life. In the Spanish version of this instrument (Weiss and Berger, 2006), we found the following Cronbach’s alphas in our sample of patients: 0.94 for personal strength, 0.88 in relating to others, 0.80 in new possibilities, 0.77 in personal strength, 0.76 in appreciation of life and 0.73 in spiritual change.
To form the various levels of independent variables, the participants answered Item 2 on the Spanish version of the SF-36 Health Survey (Alonso et al., 1995) and the vitality subscale of the 12-Item Short-Form Health Survey (SF-12v.2) (Ware et al., 2002; Maruish, 2012).
Procedure
A 2 × 2 factorial design was carried out with the independent variables self-perceived health and vitality.
(a) Self-perceived health, with two levels (better or worse). This variable was selected based on the scores on Item 2 of the SF-36 (“Compared to 1 year ago, how would you rate your health in general now?”): (1) G1: liver transplant recipients with better self-perceived health: patients with scores over 54.2%, which referred to the following answers: “somewhat better now than 1 year ago” and “much better now than 1 year ago,” forming a subgroup of 110 patients, and (2) G2: liver transplant recipients with worse self-perceived health: patients with scores equal to or less than 54.2%, which referred to the following answers: “about the same than 1 year ago,” “somewhat worse now than 1 year ago” and “much worse now than 1 year ago,” forming a subgroup of 130 patients.
(b) Vitality, with two levels (more and less). This variable was selected based on the scores on the SF-12 vitality dimension (“How much of the time during the past 4 weeks, did you have a lot of energy?”): (1) G3: liver transplant recipients with more vitality: patients with scores over 45.4%, which referred the following answers: “most of the time” and “all of the time,” forming a subgroup of 131 patients, and (2) G4: liver transplant recipients with less vitality: patients with scores equal to or less than 45.4%, which referred to the following answers: “some of the time,” “a little of the time” and “none of the time,” forming a subgroup of 109 patients.
To establish the two subgroups corresponding to the factors self-perceived health and vitality, we proceeded as follows: First, the scores of each patient were taken into account for both variables, which varied from 0 to 100. Second, for both variables the scores were ordered from least to most. Afterward the accumulated percentages of the frequency distribution were taken into account two form two subgroups of patients for each variable, which embraced approximately half of the sample. From a clinical perspective, these divisions into two subgroups in each of the factors are very relevant, since they allow the categorization of patients with similar characteristics.
Statistical Analysis
Pearson’s chi-squared was used to compare the categorical variables (gender, marital status, education, and employment), and for the quantitative variables (age and months since transplantation), the t-test for independent samples was applied.
We also applied a covariance analysis to analyze the influence of two independent factors on the level of posttraumatic growth: level of self-perceived health (better or worse) and vitality (more or less). In this analysis, first age of the transplant patient was included as a covariate. In a second analysis age and time since transplantation were included as covariates. Results with p < 0.05 were regarded as significant, results with p < 0.10 ≥ 0.05 as statistical trend. Effect sizes were calculated using Cohen’s w (for categorical variables) and Cohen’s d (for quantitative variables). The data were analyzed with the SPSS 22 statistical program.
Results
The group of liver transplant recipients with better self-perceived health (G1) was made up of 89 men and 21 women with a mean age of 59.38 years (SD = 7.68), while the one with worse self-perceived health (G2) was made up of 96 men and 34 women, with a mean age of 60.91 (SD = 10.46). The group of liver transplant recipients with more vitality (G3) was made up of 105 men and 26 women with a mean age of 60.12 (SD = 8.79), and the one with less vitality (G4) had 80 men and 29 women with a mean age of 60.31 (SD = 9.92). The sociodemographic and clinical data for the four groups of liver transplant recipients are summarized in Tables 1, 2.
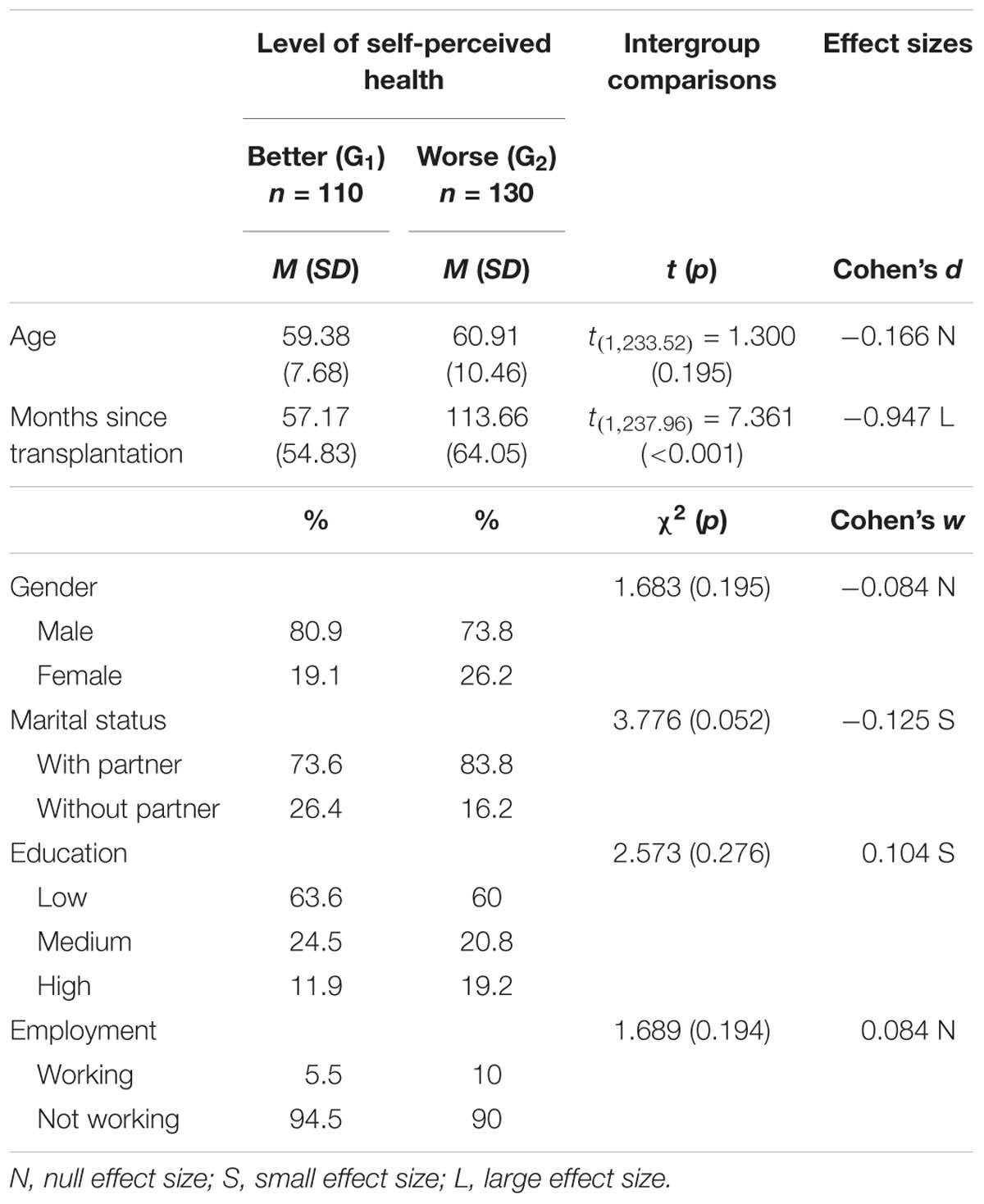
Table 1. Comparison of sociodemographic and clinical variables between two groups with better (G1) and worse (G2) self-perceived health.
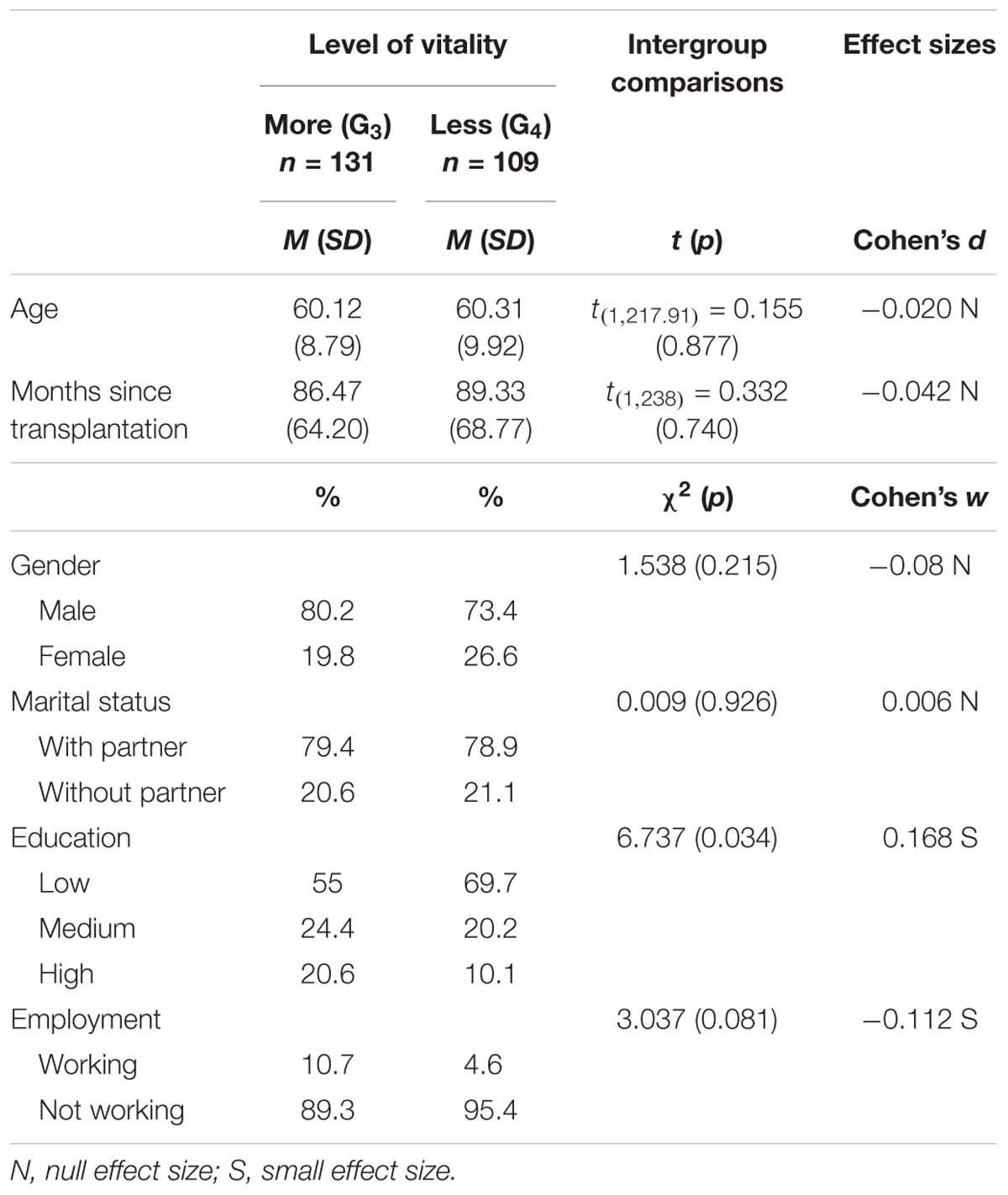
Table 2. Comparison of sociodemographic and clinical variables between two groups with more (G3) and less (G4) vitality.
With regard to the analysis of socio-demographic variables in better versus worse self-perceived health, there was a statistical trend in the direction of worse self-perceived health in recipients with a partnership (small effect size). Regarding the comparison of more versus less vitality there was a significant difference showing less vitality in recipients having a lower level of education with a small effect size. Furthermore, those recipients not working showed a statistical trend toward less vitality (small effect).
Regarding clinical variables those recipients with longer time since transplantation showed significantly poorer self-perceived health with a large effect size (p < 0.001, d = −0.947; Table 1).
In the next step of analysis we were interested in differences in posttraumatic growth in above mentioned subgroups controlling for age (Table 3). Regarding the level of posttraumatic growth, interaction effects were found between self-perceived health and vitality factors in the following variables: new possibilities [F(1,233) = 4.278, p = 0.040], personal strength [F(1,233) = 4.951, p = 0.027], and appreciation of life [F(1,233) = 6.109, p = 0.014] (Table 3). Regarding simple effects, as shown in Figure 1 and in Tables 4, 5, we found that among transplant recipients with worse self-perceived health, those with more vitality scored higher on the domains new possibilities (p = 0.017, d = 0.427), personal strength (p = 0.003, d = 0.541), and new appreciation of life (p = 0.053, d = 0.346) the latter by a statistical trend, while those with better self-perceived health showed no differences in those variables (Table 4 and Figure 1). We also found that among transplant recipients with less vitality, those with better self-perceived health showed higher scores (more posttraumatic growth) than those with worse self-perceived health on the scales new possibilities (p = 0.005, d = 0.598), personal strength (p = 0.003, d = 0.627), and new appreciation of life (p = 0.001, d = 0.718) variables, while those with more vitality did not show these differences as a function of self-perceived health (Table 5 and Figure 1).
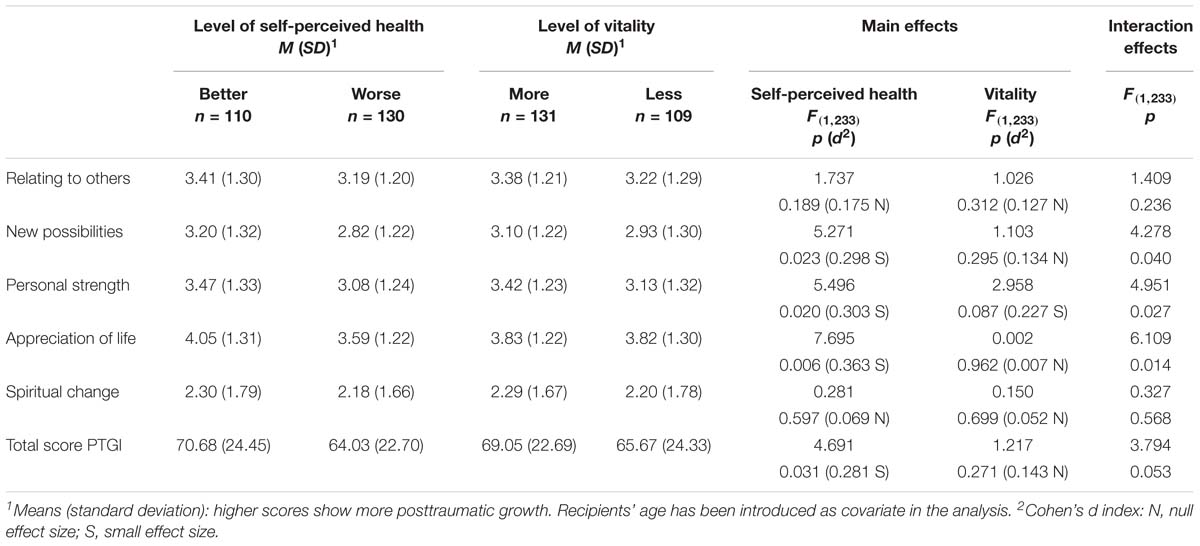
Table 3. Posttraumatic growth in liver transplant recipients based on level of self-perceived health and level of vitality with age as covariate.
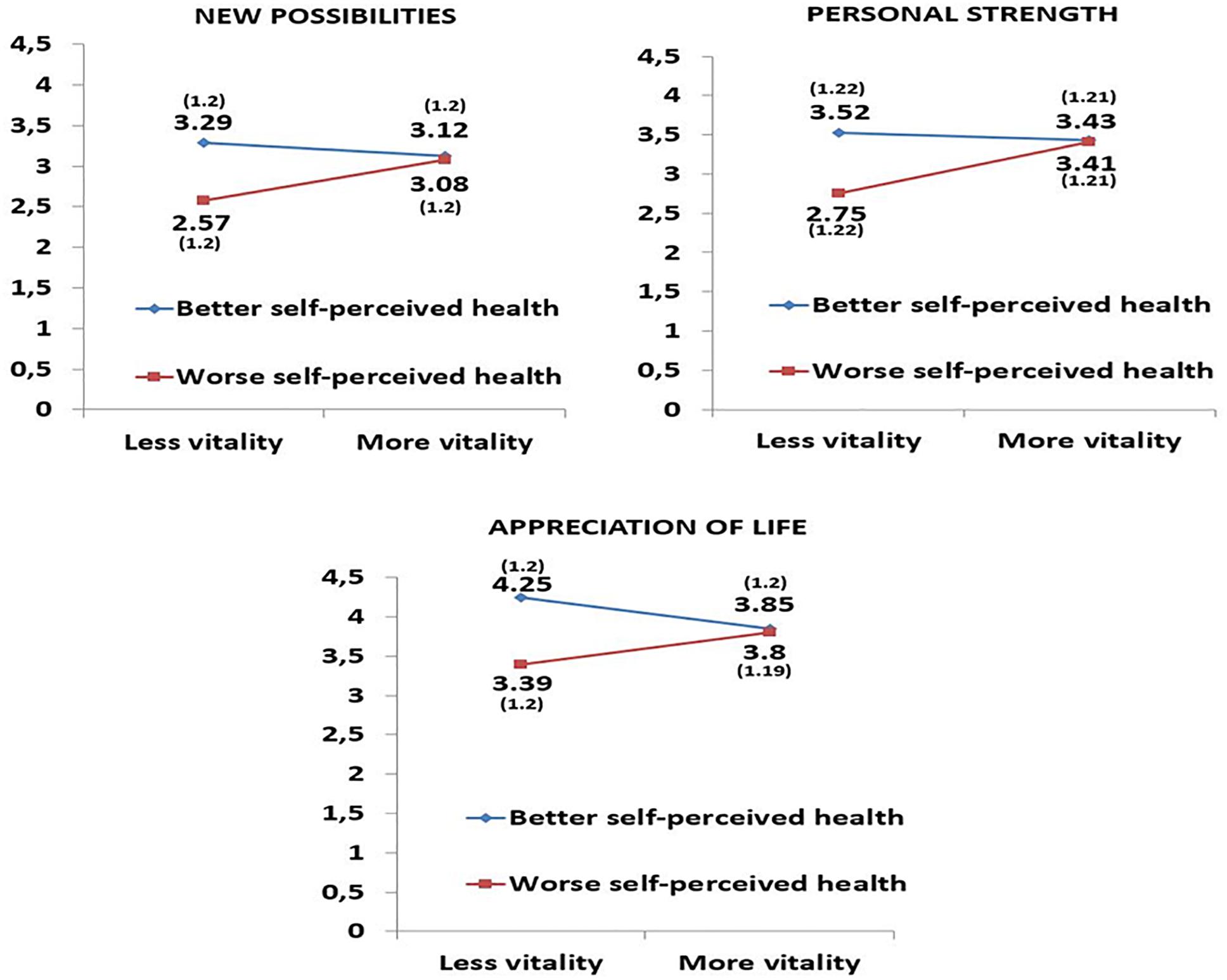
Figure 1. Interaction effects between the two factors self-perceived health (better and worse) and vitality (more and less). Means (standard deviations) adjusted for age of liver transplant recipients.
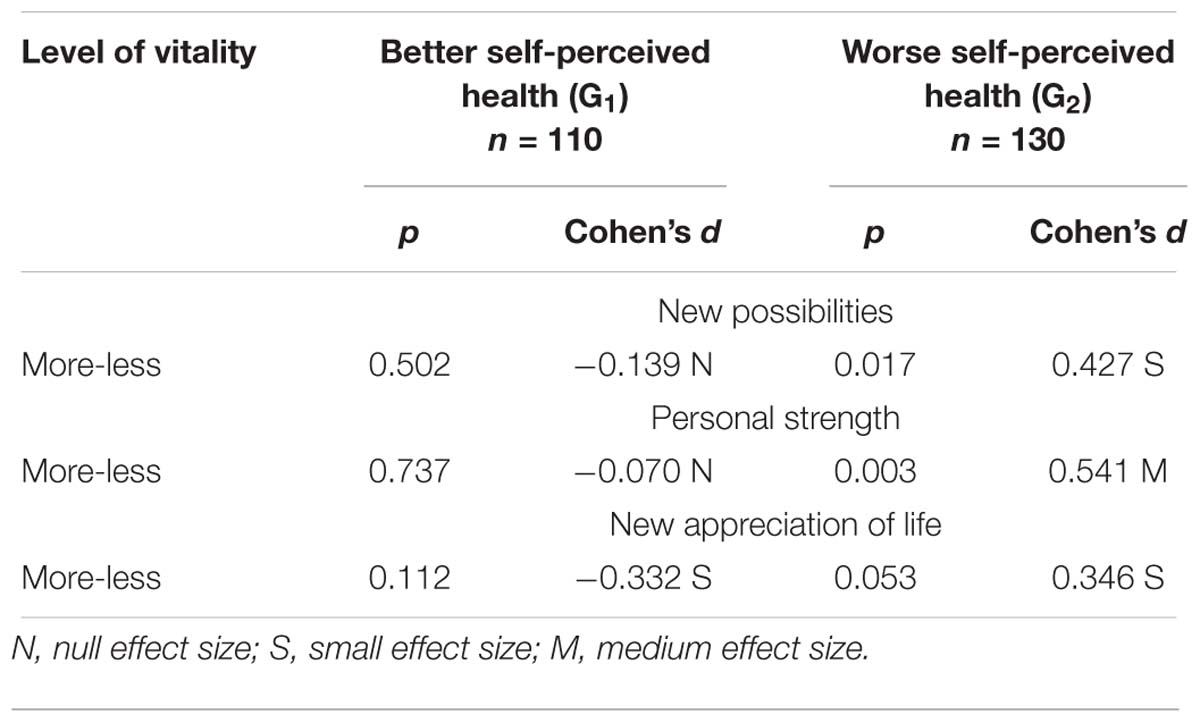
Table 4. Simple effects: comparisons between liver transplant recipients with better (G1) and worse (G2) self-perceived health at each of the levels of vitality.
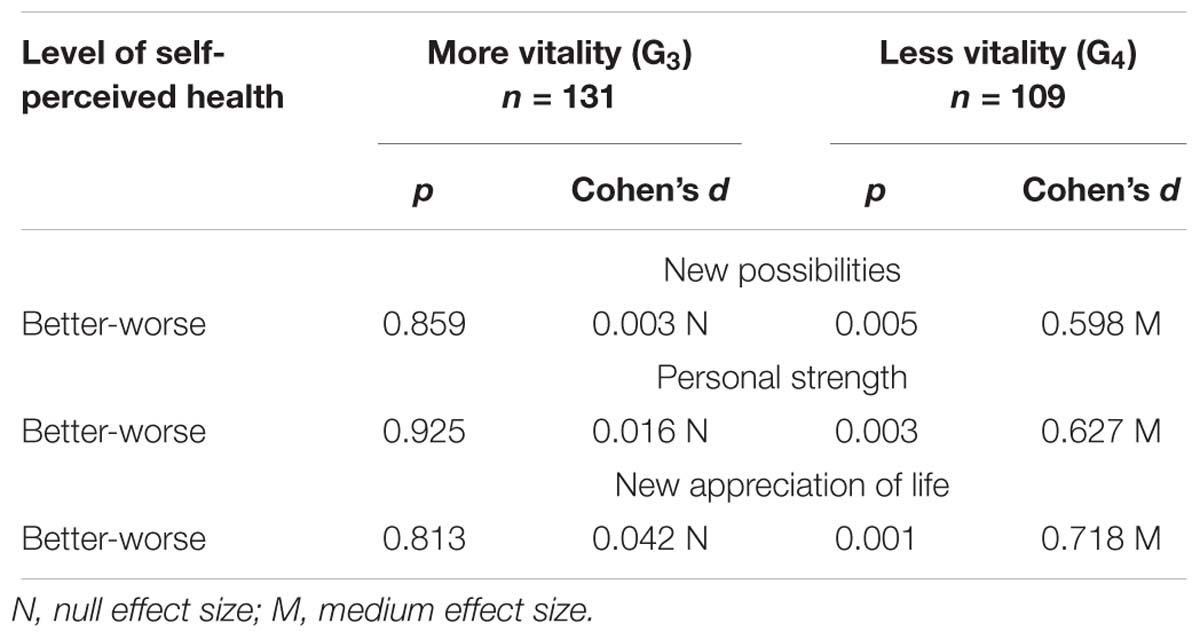
Table 5. Simple effects: comparisons between liver transplant recipients with more (G3) and less (G4) vitality at each level of self-perceived health.
Concerning the main effects, we found statistically significant differences among transplant recipients with better and worse self-perceived health in the new possibilities (p = 0.023; d = 0.298), personal strength (p = 0.020; d = 0.303), and appreciation of life (p = 0.006; d = 0.363) variables, and total posttraumatic growth score (p = 0.031; d = 0.281). Specifically, those transplant recipients with better self-perceived health showed more posttraumatic growth (Table 3).
In a further analysis we looked at the difference in posttraumatic growth controlling for age and time since transplantation (Table 6). A statistically significant interaction effect was found for appreciation of life [F(1,233) = 4.799, p = 0.029]; the subscales new possibilities [F(1,233) = 2.842, p = 0.093]; and personal strength [F(1,233) = 3.227, p = 0.074] showed a statistical trend. Regarding simple effects (Tables 7, 8) we also found that among transplant recipients with less vitality, those with better self-perceived health showed higher scores (more posttraumatic growth) than those with worse self-perceived health on the scale new appreciation of life (p < 0.001, d = 0.813) as shown in Table 8 and Figure 2.
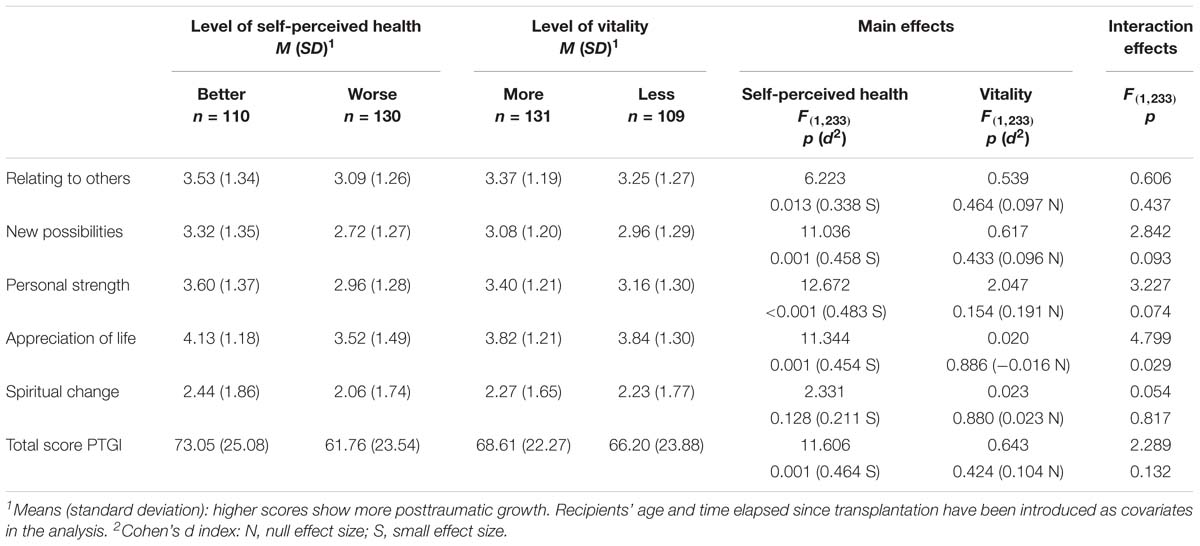
Table 6. Posttraumatic growth in liver transplant recipients based on level of self-perceived health and level of vitality with age and time since transplantation as covariates.
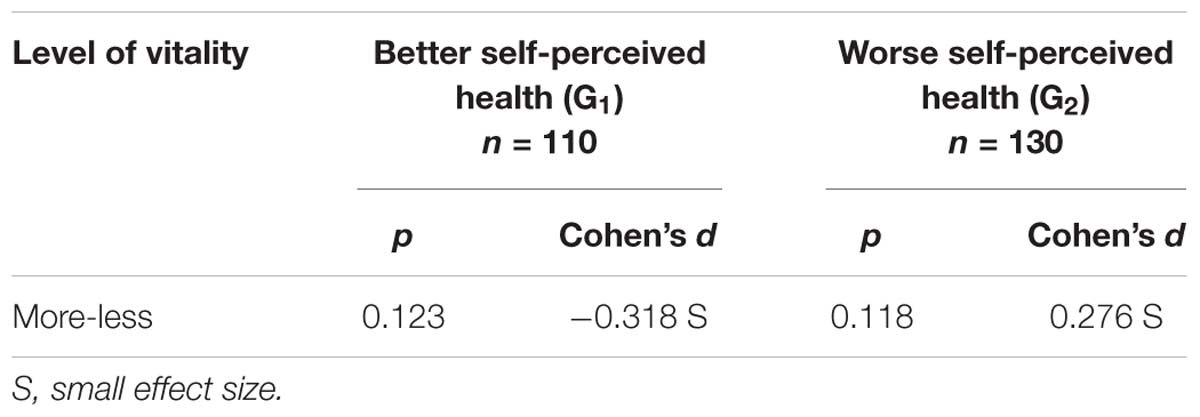
Table 7. Simple effects on appreciation of life: comparisons between liver transplant recipients with better (G1) and worse (G2) self-perceived health at each of the levels of vitality.
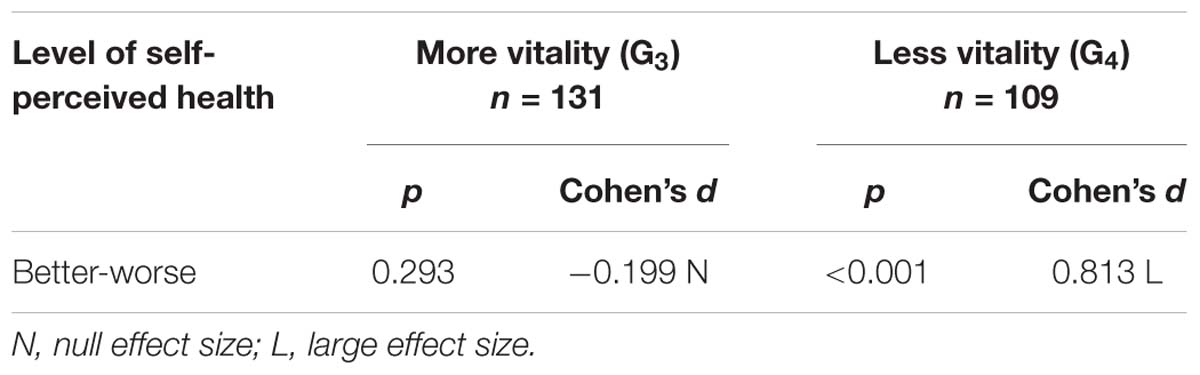
Table 8. Simple effects on appreciation of life: comparisons between liver transplant recipients with more (G3) and less (G4) vitality at each level of self-perceived health.
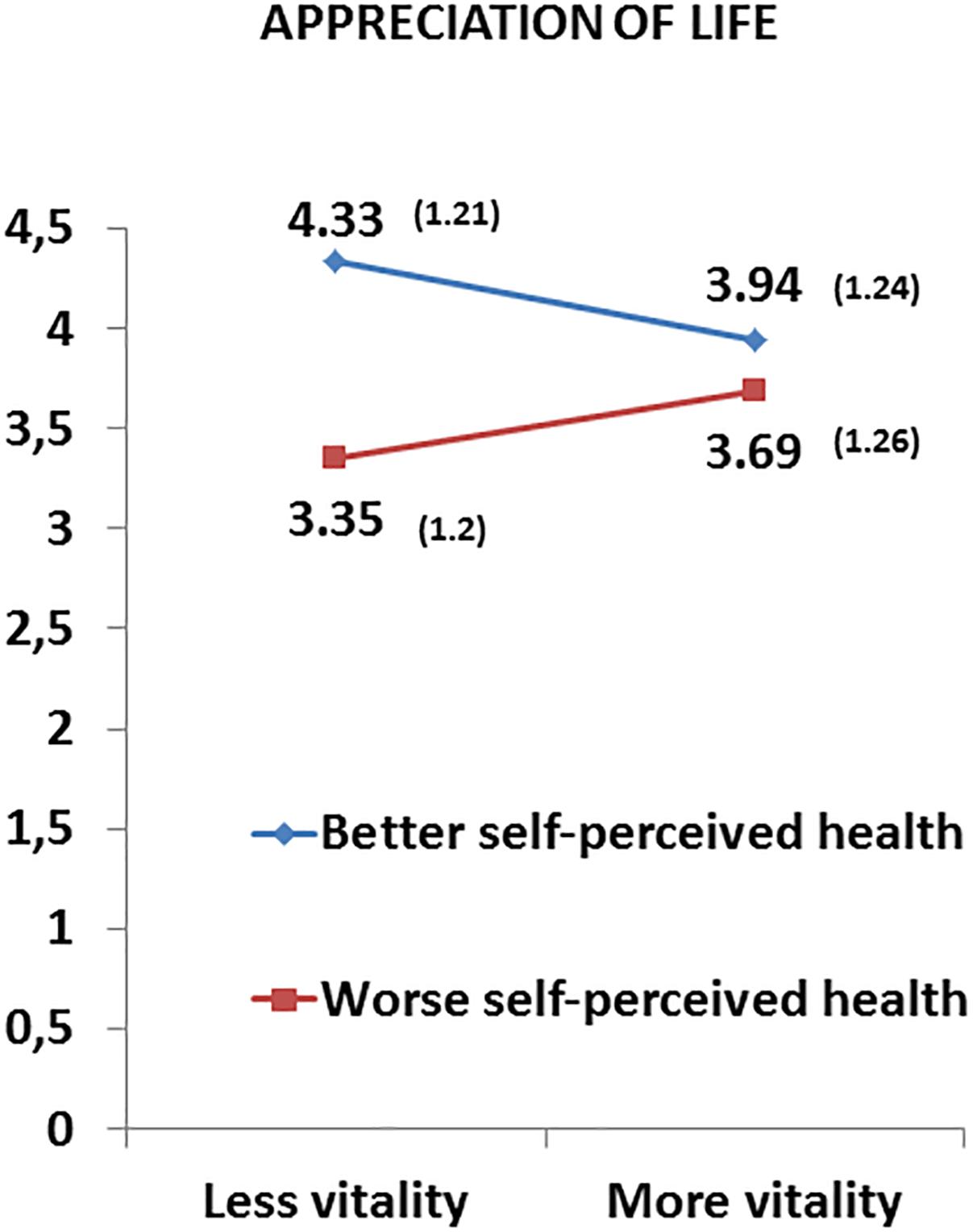
Figure 2. Interaction effects between the two factors self-perceived health (better and worse) and vitality (more and less) in appreciation of life. Means (standard deviations) adjusted for age and time since transplantation of liver transplant recipients.
Discussion
The current study analyses the mutual associations of self-perceived health and vitality on posttraumatic growth in liver transplant recipients. We divided the sample according to better or worse self-perceived health and more or less vitality into four groups. With regard to socio-demographic characteristics in recipients with more versus less vitality there was a statistically significant difference with regard to education. Lower education was associated with a lower level of vitality by a small effect size. Furthermore there was a statistical trend with a small effect size indicating that recipients not working reported less vitality. Comparing recipients with better versus worse self-perceived health those patients having a partnership showed a statistical trend with a small effect size in the direction of worse self-perceived health. As one might have expected in those recipients with worse self-perceived health a significantly longer time-span had passed since transplantation. Particularly long term treatment by immunosuppressants and the associated side effects might have been one important cause for an increase in health problems which corresponds to a decline in self-perceived health (Kugler et al., 2009).
Regarding the influence of self-perceived health and vitality on posttraumatic growth controlling for age significant interaction effects were found on the posttraumatic growth dimensions new possibilities, personal strength and new appreciation of life as opposed to the dimensions relating to others and spiritual change. Further analysis revealed that participants with worse self-perceived health scored significantly higher on abovementioned posttraumatic growth domains when they felt more vitality. On the other hand, in recipients with less vitality, the scores on these dimensions were higher when they had better self-perceived health. When we introduced time since transplantation as covariate in our analysis we found a significant interaction effect on the dimension appreciation of life and the dimensions personal strength and new possibilities showed a statistical trend. Analysis of the simple effects on the dimension appreciation of life revealed similar to the previous analysis that recipients with less vitality scored higher with better self-perceived health.
Previous studies confirm the positive association between self-perceived health and posttraumatic growth. In the article by Fox et al. (2014), lung transplant recipients who experienced more posttraumatic growth showed a better self-perceived general health. Similarly, a meta-analysis of 38 studies of persons diagnosed with cancer or HIV showed evidence that posttraumatic growth was related to better self-perceived physical and mental health (Sawyer et al., 2010). The construct of self-perceived health can be seen as the cognitive component of health-related self-assessment, whereas self-perceived vitality embraces its affective-motivational component. Vitality is characterized by three dimensions (Van Steenbergen et al., 2016): energy, or feeling energized; motivation, that means putting effort in achieving goals; and resilience, which consists of the ability to deal with everyday problems and challenges in life. Thus as our first analysis controlling for age showed having more vitality strengthened posttraumatic growth in those participants who did not realize a satisfactory state of health. Similarly, among the recipients who felt insufficient energy and motivation the awareness of better self-perceived health facilitated the awareness of personal strength, new possibilities and appreciation of life. In this context the close link between cognitive and affective-motivational aspects of mental well-being becomes apparent. Despite a lack of positive thinking the recipient, who feels energized, may realize new opportunities. On the other hand, a lack of energy might be compensated for by positive thoughts of one’s state of health. Respective associations were weaker when controlling for time since transplantation, nevertheless this analysis also revealed a large effect of better self-perceived health on the posttraumatic growth dimension appreciation of life in recipients with less vitality.
This is in line with the theory of posttraumatic growth by Tedeschi and Calhoun (1996, 2004) in which post-traumatic stress is understood to be the engine of post-traumatic growth and cognitive and affective processes are closely intertwined. The degree of posttraumatic growth reported tends to be related to the extent of cognitive engagement or rumination about elements related to the stressful event. The cognitive engagement corresponds to the level of threat associated with the traumatic event. Greater growth has been reported for individuals who reported higher levels of stress or threat (Linley and Joseph, 2004; Weiss, 2004). However, to date it is still not clear why some individuals can grow after a critical event and others are simply overwhelmed by the situation (Tedeschi and Calhoun, 2004). Specific cognitive and affective resources are underlying the ability to grow and according to our findings self-perceived health as well as vitality may be seen as relevant factors in this highly complex process.
In summary, our study could confirm differences in posttraumatic growth of liver transplant recipients according to their self-perceived health and vitality. These results demonstrate potential possibilities for strengthening posttraumatic growth (Jeon et al., 2015). Just as group psychotherapy and cognitive behavioral therapy are performed in cirrhosis patients on the transplantation waiting list (Su et al., 2014; Ramírez et al., 2015), it would be beneficial to implement interventions of this type in the post-transplant stage for the purpose of improving self-perceived health and vitality with potentially beneficial consequences for posttraumatic growth and quality of life. Integrating psychological diagnostics, therapy and outcome evaluation (Geiser et al., 2001) in the protocols for long-term follow-up of liver transplant recipients would facilitate the identification and reduction of psychological risk factors, thereby increasing the likelihood of optimizing recipients’ outcome (Morana, 2009; Dąbrowska-Bender et al., 2018).
Finally, it would be advisable, with a view to future lines of research, to consider some limitations observed in the design of this study. For example, the etiology of the liver disease leading to transplantation was not taken into consideration. There might have been differences in posttraumatic growth between transplantation recipients with alcoholic, viral or metabolic liver cirrhosis. Furthermore, due to its cross-sectional design, it was not possible to analyze the long-term development of specific alterations. A longitudinal study would solve this problem, and could reveal causal relationships between self-perceived health, vitality and posttraumatic growth. Furthermore, there are other variables which could affect the relationship between the above mentioned variables such as personality traits, which were not taken into account.
For future studies a methodological approach based on the narrative theory as suggested by Gangeri et al. (2018) might be interesting to shed light on the complex mechanisms of posttraumatic growth. Thus, instead of quantifying different parameters by questionnaires, it would be important to analyze the personal narrative of recipients about life changes after liver transplantation.
Ethics Statement
Ethics Committee of the Virgen del Rocío University Hospital of Seville. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
All authors conceived and designed the work, revised the manuscript critically for important intellectual content, and approved the final version of the manuscript to be submitted. JF-S, AM-R, RC, and MÁP-S-G performed the bibliography research about the topic, collected, analyzed, and interpreted the data, and drafted the manuscript. MB-M, MLA-N, MÁG-B, and MR-G conceived and designed the work, and analyzed and interpreted the data.
Funding
This study was funded by the Spanish Ministry of Economy and Competitiveness (Project PSI2014-51950-P).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors want to thank all the participants.
References
Alonso, J., Prieto, L., and Antó, J. M. (1995). The Spanish version of the SF-36 health survey (SF-36 Health Questionnaire): an instrument for measuring clinical results. Med. Clin. 104, 771–776.
Anand-Kumar, V., Kung, M., Painter, L., and Broadbent, E. (2014). Impact of organ transplantation in heart, lung and liver recipients: assessment of positive life changes. Psychol. Health 29, 687–697. doi: 10.1080/08870446.2014.882922
Annema, C., Roodbol, P. F., Stewart, R. E., Porte, R. J., and Ranchor, A. V. (2015). Prevalence of psychological problems and associated transplant-related variables at different time periods after liver transplantation. Liver Transpl. 21, 524–538. doi: 10.1002/lt.24075
Bachmann, J. M., Goggins, K. M., Nwosu, S. K., Schildcrout, J. S., Kripalani, S., and Wallston, K. A. (2016). Perceived health competence predicts health behavior and health-related quality of life in patients with cardiovascular disease. Patient Educ. Couns. 99, 2071–2079. doi: 10.1016/j.pec.2016.07.020
Baranyi, A., Krauseneck, T., and Rothenhäusler, H. B. (2013). Posttraumatic stress symptoms after solid-organ transplantation: preoperative risk factors and the impact on health-related quality of life and life satisfaction. Health Qual. Life Outcomes 11:111. doi: 10.1186/1477-7525-11-111
Cameron, S., Springer, C., Fox-Wasylyshyn, S., and El-Masri, M. M. (2012). A descriptive study of functions, symptoms, and perceived health state after radiotherapy for prostate cancer. Eur. J. Oncol. Nurs. 16, 310–314. doi: 10.1016/j.ejon.2011.07.007
Casellas-Grau, A., Sumalla, E. C., Lleras, M., Vives, J., Sirgo, A., León, C., et al. (2018). The role of posttraumatic stress and posttraumatic growth on online information use in breast cancer survivors. Psychooncology 27, 1971–1978. doi: 10.1002/pon.4753
Dąbrowska-Bender, M., Kozaczuk, A., Pączek, L., Milkiewicz, P., Słoniewski, R., and Staniszewska, A. (2018). Patient quality of life after liver transplantation in terms of emotional problems and the impact of sociodemographic factors. Transplant. Proc. 50, 2031–2038. doi: 10.1016/j.transproceed.2018.03.113
Elliott, J. C., Hasin, D. S., and Des-Jarlais, D. C. (2017). Perceived health and alcohol use in individuals with HIV and Hepatitis C who use drugs. Addict. Behav. 72, 21–26. doi: 10.1016/j.addbeh.2017.03.004
Forinder, U., and Norberg, A. L. (2014). Posttraumatic growth and support among parents whose children have survived stem cell transplantation. J. Child Health Care 18, 326–335. doi: 10.1177/1367493513496666
Fox, K. R., Posluszny, D. M., DiMartini, A. F., DeVito-Dabbs, A. J., Rosenberger, E. M., Zomak, R. A., et al. (2014). Predictors of post-traumatic psychological growth in the late years after lung transplantation. Clin. Transplant. 28, 384–393. doi: 10.1111/ctr.12301
Gangeri, L., Scrignaro, M., Bianchi, E., Borreani, C., Bhoorie, S., and Mazzaferro, V. (2018). A longitudinal investigation of posttraumatic growth and quality of life in liver transplant recipients. Prog. Transplant. 28, 236–243. doi: 10.1177/1526924818781569
Geiser, F., Imbierowicz, K., Conrad, R., Schilling, G., and Liedtke, R. (2001). Differences between patients classified as “recovered” or “improved” and “unchanged” or “deteriorated” in a psychotherapy outcome study. Z. Psychosom. Med. Psychother. 47, 250–261. doi: 10.13109/zptm.2001.47.3.250
Grinyó, J. M., Cruzado, J. M., Bestard, O., Vidal-Castiñeira, J. R., and Torras, J. (2012). “Immunosuppression in the ERA of biological agents,” in Stem Cell Transplantation, eds C. López-Larrea, A. López-Vázquez, and B. Suárez-Álvarez (New York, NY: Springer Science Business Media), 60–72. doi: 10.1007/978-1-4614-2098-9_5
Guérin, E. (2012). Disentangling vitality, well-being, and quality of life: a conceptual examination emphasizing their similarities and differences with special application in the physical activity domain. J. Phys. Act. Health 9, 896–908. doi: 10.1123/jpah.9.6.896
Hirsch, J. K., Floyd, A. R., and Duberstein, P. R. (2012). Perceived health in lung cancer patients: the role of positive and negative affect. Qual. Life Res. 21, 187–194. doi: 10.1007/s11136-011-9933-4
Jeon, M., Yoo, I. Y., Kim, S., and Lee, J. (2015). Post-traumatic growth in survivors of allogeneic hematopoietic stem cell transplantation. Psychooncology 24, 871–877. doi: 10.1002/pon.3724
Karam, V., Castaing, D., Danet, C., Delvart, V., Gasquet, I., Adam, R., et al. (2003). Longitudinal prospective evaluation of quality of life in adult patients before and one year after liver transplantation. Liver Transpl. 9, 703–711. doi: 10.1053/jlts.2003.50148
Ko, Y., and Boo, S. (2016). Self-perceived health versus actual cardiovascular disease risks. Jpn. J. Nurs. Sci. 13, 65–74. doi: 10.1111/jjns.12087
Kugler, C., Geyer, S., Gottlieb, J., Simon, A., Haverich, A., and Dracup, K. (2009). Symptom experience after solid organ transplantation. J. Psychosom. Res. 66, 101–110. doi: 10.1016/j.jpsychores.2008.07.017
Kugler, C., Gottlieb, J., Warnecke, G., Schwarz, A., Weissenborn, K., Barg-Hock, H., et al. (2013). Health-related quality of life after solid organ transplantation: a prospective, multiorgan cohort study. Transplantation 96, 316–323. doi: 10.1097/TP.0b013e31829853eb
Linley, P. A., and Joseph, S. (2004). Positive change following trauma and adversity: a review. J. Trauma Stress 17, 11–21. doi: 10.1023/B:JOTS.0000014671.27856.7e
Marcellin, F., Lacombe, K., Fugon, L., Molina, J. M., Bonnard, P., Miailhes, P., et al. (2011). Correlates of poor perceived health among individuals living with HIV and HBV chronic infections: a longitudinal assessment. AIDS Care 23, 501–507. doi: 10.1080/09540121.2010.507953
Martín-Rodríguez, A., Pérez-San-Gregorio, M. A., Domínguez-Cabello, E., Fernández-Jiménez, E., and Pérez-Bernal, J. (2012). Affective status in liver transplant recipients as a function of self-perception of general health. Transplant. Proc. 44, 2619–2621. doi: 10.1016/j.transproceed.2012.09.052
Martins-da-Silva, S. I., Moreira, H., and Canavarro, M. C. (2011). Growing after breast cancer: a controlled comparison study with healthy women. J. Loss Trauma 16, 323–340. doi: 10.1080/15325024.2011.572039
Martz, E., and Livneh, H. (2016). Psychosocial adaptation to disability within the context of positive psychology: findings from the literature. J. Occup. Rehabil. 26, 4–12. doi: 10.1007/s10926-015-9598-x
Maruish, M. E. (2012). User’s Manual for the SF-12v2 Health Survey, 3rd Edn. Lincoln, RI: QualityMetric Incorporated.
Moore, A. M., Gamblin, T. C., Geller, D. A., Youssef, M. N., Hoffman, K. E., Gemmell, L., et al. (2011). A prospective study of posttraumatic growth as assessed by self-report and family caregiver in the context of advanced cancer. Psychooncology 20, 479–487. doi: 10.1002/pon.1746
Morana, J. G. (2009). Psychological evaluation and follow-up in liver transplantation. World J. Gastroenterol. 15, 694–696. doi: 10.3748/wjg.15.694
Nix, G. A., Ryan, R. M., Manly, J. B., and Deci, E. L. (1999). Revitalization through self-regulation: the effects of autonomous and controlled motivation on happiness and vitality. J. Exp. Soc. Psychol. 35, 266–284. doi: 10.1006/jesp.1999.1382
Pérez-San-Gregorio, M. A., Martín-Rodríguez, A., Borda-Mas, M., Avargues-Navarro, M. L., Pérez-Bernal, J., Conrad, R., et al. (2017a). Post-traumatic growth and its relationship to quality of life up to 9 years after liver transplantation: a cross-sectional study in Spain. BMJ Open 7:e017455. doi: 10.1136/bmjopen-2017-017455
Pérez-San-Gregorio, M. A., Martín-Rodríguez, A., Borda-Mas, M., Avargues-Navarro, M. L., Pérez-Bernal, J., and Gómez-Bravo, M. A. (2017b). Coping strategies in liver transplant recipients and caregivers according to patient posttraumatic growth. Front. Psychol. 8:18. doi: 10.3389/fpsyg.2017.00018
Pérez-San-Gregorio, M. A., Martín-Rodríguez, A., Domínguez-Cabello, E., Fernández-Jiménez, E., and Bernardos-Rodríguez, Á (2013). Quality of life and mental health comparisons among liver transplant recipients and cirrhotic patients with different self-perceptions of health. J. Clin. Psychol. Med. Settings 20, 97–106. doi: 10.1007/s10880-012-9309-0
Pérez-San-Gregorio, M. A., Martín-Rodríguez, A., Domínguez-Cabello, E., Fernández-Jiménez, E., Borda-Mas, M., and Bernardos-Rodríguez, A. (2012). Mental health and quality of life in liver transplant and cirrhotic patients with various etiologies. Int. J. Clin. Health Psychol. 12, 203–218.
Pérez-San-Gregorio, M. A., Martín-Rodríguez, A., and Galán-Rodríguez, A. (2005). Psychological problems in transplantation. Int. J. Clin. Health Psychol. 5, 99–114.
Ramírez, P., Febrero, B., Martínez-Alarcón, L., Abete, C., Galera, M., and Cascales, P. (2015). Benefits of group psychotherapy in cirrhotic patients on the liver transplant waiting list. Transplant. Proc. 47, 2382–2384. doi: 10.1016/j.transproceed.2015.08.033
Rosenberg, A. R., Syrjala, K. L., Martin, P. J., Flowers, M. E., Carpenter, P. A., Salit, R. B., et al. (2015). Resilience, health, and quality of life among long-term survivors of hematopoietic cell transplantation. Cancer 121, 4250–4257. doi: 10.1002/cncr.29651
Sawyer, A., Ayers, S., and Field, A. P. (2010). Posttraumatic growth and adjustment among individuals with cancer or HIV/AIDS: a meta-analysis. Clin. Psychol. Rev. 30, 436–447. doi: 10.1016/j.cpr.2010.02.004
Scrignaro, M., Sani, F., Wakefield, J. R., Bianchi, E., Magrin, M. E., and Gangeri, L. (2016). Post-traumatic growth enhances social identification in liver transplant patients: a longitudinal study. J. Psychosom. Res. 88, 28–32. doi: 10.1016/j.jpsychores.2016.07.004
Sharp, L., Redfearn, D., Timmons, A., Balfe, M., and Patterson, J. (2018). Posttraumatic growth in head and neck cancer survivors: is it possible and what are the correlates? Psychooncology 27, 1517–1523. doi: 10.1002/pon.4682
Sirivatanauksorn, Y., Dumronggittigule, W., Limsrichamrern, S., Iramaneerat, C., Kolladarungkri, T., Kositamongkol, P., et al. (2012). Quality of life among liver transplantation patients. Transplant. Proc. 44, 532–538. doi: 10.1016/j.transproceed.2011.12.056
Su, J. H., Wang, S. Y., Liang, X., Zhu, M. L., Qiao, S., and Yin, H. Y. (2014). Mode and effect of cognitive-behavioral therapy for liver transplant recipients waiting for a liver transplant. Chin. J. Tissue Eng. Res. 18, 687–692. doi: 10.3969/j.issn.2095-4344.2014.05.006
Tedeschi, R. G., and Calhoun, L. G. (1995). Trauma and Transformation: Growing in the Aftermath of Suffering. Thousand Oaks, CA: Sage.
Tedeschi, R. G., and Calhoun, L. G. (1996). The Posttraumatic Growth Inventory: measuring the positive legacy of trauma. J. Trauma Stress 9, 455–471. doi: 10.1002/jts.2490090305
Tedeschi, R. G., and Calhoun, L. G. (2004). Posttraumatic growth: conceptual foundations and empirical evidence. Psychol. Inq. 15, 1–18. doi: 10.1207/s15327965pli1501_01
Tobin, J., Allem, J. P., Slaughter, R., Unger, J. B., Hamilton, A. S., and Milam, J. E. (2018). Posttraumatic growth among childhood cancer survivors: associations with ethnicity, acculturation, and religious service attendance. J. Psychosoc. Oncol. 36, 175–188. doi: 10.1080/07347332.2017.1365799
Van Steenbergen, E., Van Dongen, J. M., Wendel-Vos, G. C. W., Hildebrandt, V. H., and Strijk, J. E. (2016). Insights into the concept of vitality: associations with participation and societal costs. Eur. J. Public Health 26, 354–359. doi: 10.1093/eurpub/ckv194
Ware, J. E., Kosinski, M., Turner-Bowker, D. M., and Gandek, B. (2002). How to Score Version 2 of the SF-12 Health Survey (with a Supplement Documenting Version 1). Lincoln, RI: QualityMetric Incorporated.
Weiss, T. (2004). Correlates of posttraumatic growth in husbands of breast cancer survivors. Psychooncology 13, 260–268. doi: 10.1002/pon.735
Weiss, T., and Berger, R. (2006). Reliability and validity of a Spanish version of the posttraumatic growth inventory. Res. Soc. Work Pract. 16, 191–199. doi: 10.1177/1049731505281374
Wu, K., Zhang, Y., Liu, Z., Zhou, P., and Wei, C. (2015). Coexistence and different determinants of posttraumatic stress disorder and posttraumatic growth among Chinese survivors after earthquake: role of resilience and rumination. Front. Psychol. 6:1043. doi: 10.3389/fpsyg.2015.01043
Zhu, Y., Wu, J., Feng, X., Chen, H., Lu, H., Chen, L., et al. (2017). Patient characteristics and perceived health status of individuals with HIV and tuberculosis coinfection in Guangxi, China. Medicine 96:e6475. doi: 10.1097/MD.0000000000006475
Keywords: liver transplantation, posttraumatic growth, self-perceived health, vitality, patients
Citation: Funuyet-Salas J, Martín-Rodríguez A, Borda-Mas M, Avargues-Navarro ML, Gómez-Bravo MÁ, Romero-Gómez M, Conrad R and Pérez-San-Gregorio MÁ (2019) Relationship Between Self-Perceived Health, Vitality, and Posttraumatic Growth in Liver Transplant Recipients. Front. Psychol. 10:1367. doi: 10.3389/fpsyg.2019.01367
Received: 08 November 2018; Accepted: 27 May 2019;
Published: 11 June 2019.
Edited by:
Roumen Kirov, Institute of Neurobiology (BAS), BulgariaReviewed by:
Gabriella Martino, Universita’ degli Studi di Messina, ItalyTamar Silberg, Bar-Ilan University, Israel
Copyright © 2019 Funuyet-Salas, Martín-Rodríguez, Borda-Mas, Avargues-Navarro, Gómez-Bravo, Romero-Gómez, Conrad and Pérez-San-Gregorio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jesús Funuyet-Salas, amZ1bnV5ZXQxQHVzLmVz
†These authors have contributed equally to this work