 Haofei Zhao
Haofei Zhao Jinyao Yi
Jinyao Yi Shuqiao Yao
Shuqiao Yao
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 21 June 2019
Sec. Quantitative Psychology and Measurement
Volume 10 - 2019 | https://doi.org/10.3389/fpsyg.2019.01360
This article is part of the Research Topic Scale Development and Score Validation View all 23 articles
The 15-item Geriatric Depression Scale (GDS-15) is widely used to screen depression among elders. But the factor structure of the Chinese version GDS-15 remains unclear. This study was conducted to determine the best-fit factor structure of GDS-15 and to assess measurement invariance across gender groups in a sample of Chinese elders recruited from Mainland China (final sample N = 2428). The best-fit factor structure was examined by confirmatory factor analysis (CFA). Multigroup CFA was utilized to test the measurement invariance across genders of the factor structure. The results of CFA revealed that a three-factor model, including life satisfaction (four items), general depressive affect (seven items), and withdrawal (three items), fits the structure of the GDS-15 best. Measurement invariance across genders was supported, fully assuming different degrees of invariance.
Depression is a common mental disorder among older adults, with some 15% of community-dwelling older adults experiencing clinically significant depressive symptoms (Blazer, 2003). Late-life depression is linked to serious consequences, such as impaired daily functioning, increased health care use, and reduced quality of life (Castelo et al., 2010). Hence, assessment of depressive symptoms is an important mental health evaluation in this population.
The Geriatric Depression Scale (GDS), which was the first screening instrument to be tailored to geriatric patients (Yesavage et al., 1982), has become widely used to measure depression levels in the elderly. To reduce the time required for GDS administration and thus avoid respondent fatigue, a 15-item short-form GDS was developed from the original 30-item scale (Sheik and Yesavage, 1986). Unlike other depression tools such as the Epidemiological Studies Depression Scale (CES-D) and the Beck Depression Inventory (BDI), both versions of the GDS do not contain somatic items that may be less valid because they are common in elders (Sheik and Yesavage, 1986; Stiles and Mcgarrahan, 1998). Moreover, items of GDS use an easy response format (yes/no) preferred among older respondents. The 15-item GDS (GDS-15) retains the advantages of the original 30-item GDS, including simplicity of administration, an easy response format, and economy of time, and its validity and reliability have been demonstrated repeatedly (Cwikel and Ritchie, 1989; Lesher and Berryhill, 1994; Almeida and Almeida, 1999; Fountoulakis et al., 1999; Tang et al., 2005; Chaaya et al., 2008). Both ICD-10 criteria and DSM-IV criteria have shown that the GDS-15 is valid for measuring depression (Almeida and Almeida, 1999). GDS-15 may have more practical appeal because of the time restraints faced in clinical practice (Yao et al., 2009). In addition, the scale has been translated into multiple languages and translated versions have been proved for assessing depressive symptoms in people from various ethnic backgrounds (Iwamasa et al., 1998; Liu et al., 1998; Ishine et al., 2005; Malakouti et al., 2006; Onishi et al., 2006; Chiesi et al., 2018), including ethnic Chinese people living in Western countries (Mui, 1996; Lai, 2000).
Although the psychometric properties of the long and short GDS scales have been documented (Jang et al., 2001; Broekman et al., 2008; Pocklington et al., 2016), the factor structure of the Chinese version GDS-15 is still unclear. Mitchell et al. (1993) first proposed a three-factor model: general depressive affect (seven items), life satisfaction (four items), and withdrawal (three items). Item 10 “memory” failed to fit any of these factors. However, a number of other studies have reported different GDS-15 structures with two (Mui, 1996; Friedman et al., 2005; Brown et al., 2007), three (Incalzi et al., 2003; Imai et al., 2014), and four (Onishi et al., 2004; Lai et al., 2010) factors. Results of previous studies investigating the factor structure of the Chinese version GDS-15 have been mixed. Mui (1996) reported a two-factor model consisting of “happy mood” and “sad mood.” Implementing the GDS-15 among aging Chinese in Canada, Lai and Colleagues reported a two-factor model (i.e., affective mood, cognitive mood; Lai, 2000) and a more detailed four-factor model (i.e., positive mood, negative mood, inferiority/disinterested, uncertainty, Lai et al., 2005). Most subjects of the studies above lived in Western societies. Only one study employing exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) reported a four-factor solution focused on depression among aging Chinese in Mainland China, with the following factors: positive and negative mood, energy level, inferiority, and disinterested (Lai et al., 2010). Researchers have deduced that the differences of these factor models may be related to cultural differences in the concept and expression of depression (Kim et al., 2013). For example, dominant social values of people in Western countries are individualism and personal level democratic values, whereas Chinese living in Mainland China takes more value on collectivism and at-large benefits, due to a different political and social system. These differences above in beliefs and social contexts play an important role in personal expression of affection (Mui, 2010; Kim et al., 2013).
Findings obtained depending on samples from Western societies may not necessarily be applicable to the older adults in Mainland China. The study of Lai et al. (2010) focused only on lonely elder Chinese. It is necessary for us to examine which factor structure model is more suitable for Chinese elders, for which will be helpful for developing a standardized scoring method and enable us to explore any differences across studies. In the current study, CFA was conducted to compare factor structure models that were identified in previous studies. GDS-15 total score is usually used in practice and research. However, a total score should not be used unless the covariance between the first-order factors is adequately explained by the second-order factor (Marsh and Hocevar, 1985). There are no published studies of the second-order factor of GDS-15 reported; thus, we performed a second-order factor analysis to confirm the validity of GDS-15 total scores. The trend of women having more depression problems than men was recapitulated (Nolen-Hoeksema, 2001). Tang et al. (2005) have examined the differential item functioning (DIF) of GDS-15 items, but the study was based on a sample of Hong Kong Chinese patients with pneumoconiosis. No study has tested the measurement invariance of the GDS-15 across genders in the mainland Chinese population. As related to gender, if the measurement invariance does not hold across groups, differences in observed scores may not be directly comparable (Wang et al., 2013). The true differences across groups may be mixed with the measurement bias of assessment. Exploring measurement invariance is beneficial for increasing the accuracy of depression assessments and the comparability across groups.
Hence, to develop the Chinese version of GDS-15, the first purpose of this study was to examine the best factor structure of GDS-15 in a large representative sample. A second purpose was to test the gender invariance of the GDS-15. We employed the CFA to compare the existing factor models from previous studies. Second-order CFA was performed to confirm the validity of the GDS-15 total score. Subsequently, we assessed the measurement invariance across genders of the best-fitting model.
The inclusion criteria were as follows: age of 60–99 years old and ethnic Chinese resident of Beijing, Hunan, and Shandong province, China. The exclusion criteria were as follows: diagnosed with severe mental illness; insufficient cognitive ability to understand the questionnaire; unable to understand Mandarin and therefore unable to complete the questionnaire; cannot fill out the questionnaire due to other reasons. This study investigated the level of depression in the elderly, with 2,470 participants, and 42 failed to respond to all GDS-15 items. The final sample of 2,428 elderly Chinese volunteers included 1,141 men (47.0%) and 1,287 women (53.0%). The mean age of the men was 73.14 years [standard deviation (SD) = 8.07], and the mean age of the women was 71.78 years (SD = 7.70).
Postgraduate psychology researchers in China were recruited and trained to do this work. Participants completed the survey in a district activity center and elderly with visual impairment or lack of formal education would get support from researchers. The study was approved by the Ethics Committee of the Second Xiangya Hospital of Central South University. Each participant gave written informed consent prior to their inclusion in the study.
The Chinese version of the GDS-15, wherein each item was a yes or no question, was used to measure depressive symptoms. The positive depression symptom response was yes for 10 items and no for 5 items, such that a point was marked for each positive symptom response. Thus, higher values indicated more depressive symptoms. As recommended by a study conducted among Chinese elders (Boey, 2000), we adopted 8 as the cutoff score. Both validity and reliability of the GDS-15 were validated satisfactory among Chinese elders in previous studies (Mui, 1996; Liu and Guo, 2008). In the current study, the scale has been confirmed to show good internal consistency (Cronbach’s α = 0.873).
Preliminary analyses were done in SPSS Version 22 (IBM, 2013), and CFA was conducted in Mplus7.4 (Muthén and Muthén, 1998). Given that the response options of items were binary (yes and no), the maximum-likelihood (ML) estimator is not adequate as it could bias the results. The robust weighted least squares with mean and variance adjustment (WLSMV) estimator was used, which could account for the binary response scaling (Finney and DiStefano, 2013; Morin et al., 2017). The whole sample was randomly divided into sample 1 (n = 1,174) and sample 2 (n = 1,254). This method of randomly assigning a larger sample into two independent samples is a common approach (Lai et al., 2010; Wang et al., 2012; He et al., 2018).
We employed CFA in sample 1 to compare competing models and determine the best-fitting factor model. A total of seven competing models were compared (Table 1). Models from different versions of GDS-15 were not included in the current analysis. Regular chi-square difference tests were not conducted here for the comparison of non-nested competing models. Following generally accepted practice, we used the Tucker–Lewis index (TLI), the chi-square, comparative fit index (CFI), and root mean square error of approximation (RMSEA) to evaluate the fit of each model. CFI and TLI values ≥0.90 indicate adequate model fit (0.95, excellent fit), while RMSEA values ≤0.08 and 0.06 indicate acceptable and excellent, respectively (Kline, 2010; Vrieze, 2012).
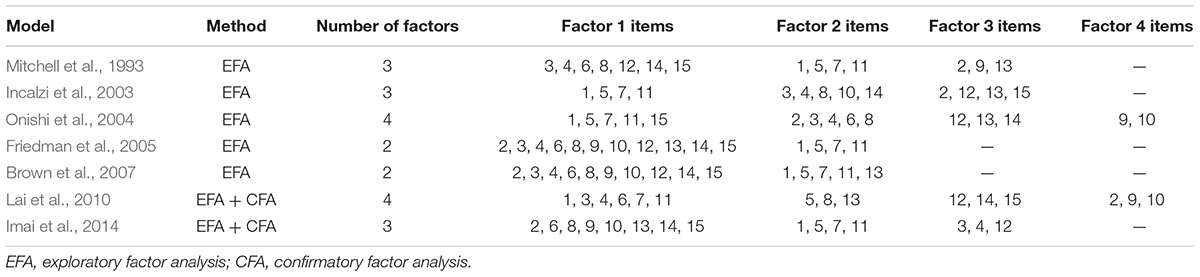
Table 1. Characteristics of each factor model tested.
We hypothesize that there is a higher-order factor Geriatric Depression that accounts for the commonality among first-order factors. First-order CFA was conducted in sample 2 to validate the best-fitting structure of the GDS-15 confirmed in sample 1. Subsequently, second-order CFA was performed to calculate the target coefficient that could be used to decide whether the first-order factors were adequately explained by the higher-order factor. As recommended by Comrey and Lee (2013), the magnitude of the factor loadings was interpreted as follows: ≥0.71, excellent; 0.63–0.70, very good; 0.55–0.62, good; 0.33–0.44, fair; ≤0.32, poor.
Multigroup CFA was implemented in the whole sample to test gender invariance of the best-fitting model. We considered four aspects of invariance including configural invariance (Model A), metric invariance (Model B), scalar invariance (Model C), and strict invariance (Model D). Model A was used to evaluate the structure of latent variables, and the results of which served as a baseline model. Model B was tested based on the results of configural invariance with factor loading equivalence constraints imposed to ensure similarity of the observed indicators and underlying traits across gender. Model C was based on the result of the last step and in which we constrained variable intercepts equal. Model D test was conducted with factor loadings, variable intercepts, and error variance constraints equally set. As suggested by Cheung and Rensvold (2002), CFI, TLI, and RMSEA changes were employed to evaluate invariance; ΔCFI ≤0.01, ΔTLL ≤0.01, and ΔRMSEA ≤0.015 were considered evidence of invariance (Cheung and Rensvold, 2002; Chen, 2007).
In the whole sample, the GDS-15 total scores had a mean (SD) of 4.03 ± 3.88 for males and 4.59 ± 4.10 for females. The GDS-15 total scores range was 0–15, with women having significantly higher scores than men (t = 3.46, df = 2,426, p < 0.05). Mean (SD) GDS-15 total scores did not differ significantly (t = 0.46, df = 2,426, p > 0.05) between sample 1 (4.29 ± 3.96) and sample 2 (4.36 ± 4.04). When score ≥8 was used as the cutoff score, 19.9% of the participant showed significant depressive symptoms.
As reported in Table 2, we obtained good fit indexes in all examined models. CFIs, TLIs, and RMSEAs were >0.95, >0.95, and <0.08, respectively. The best-fitting model was Mitchell’s three-factor model (WLSMV χ2 = 260.316, df = 74, TLI = 0.989, CFI = 0.991, RMSEA = 0.046). Next was Brown’s two-factor model (WLSMV χ2 = 438.968, df = 89, TLI = 0.980, CFI = 0.983, RMSEA = 0.058). For item 10 in Brown’s model, the factor loading loaded on its latent factor was 0.116 (<0.32), a poor loading. Therefore, the best-fitting model for older Chinese was Mitchell’s three-factor model. The results of first-order CFA in sample 2 showed that the three-factor model had an excellent fit to the data (Table 2). The correlations between the three factors in sample 1 ranged from 0.823 to 0.955 and those between the three factors in sample 2 ranged from 0.878 to 0.950 (see Table 3). All correlation coefficients were positive and statistically significant (p < 0.001).
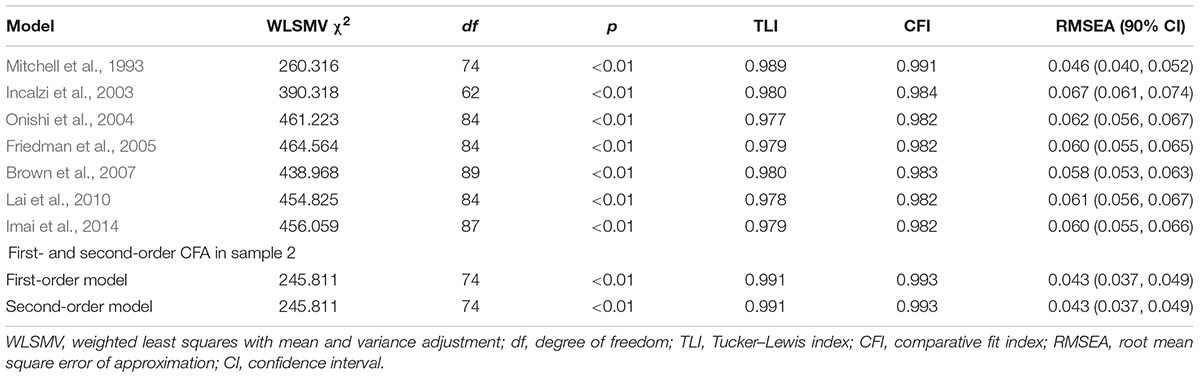
Table 2. Goodness-of-fit indices of the compared models.
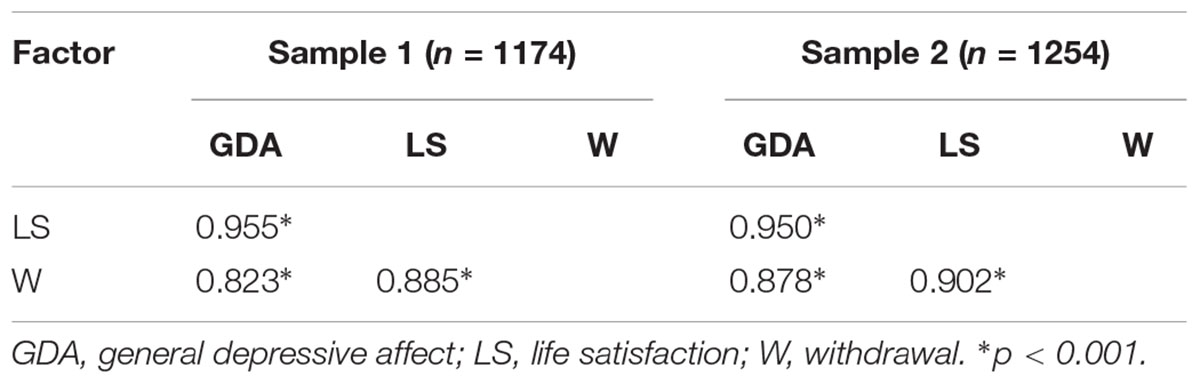
Table 3. Factor correlations.
As can be seen from Table 2, the second-order model had the same fit indices with the first-order model (WLSMV χ2 = 245.811, df = 74, TLI = 0.991, CFI = 0.993, RMSEA = 0.043). Standardized factor loadings for the second-order CFA were included in Table 4. The first-order factor loadings ranged from 0.552 to 0.997, showing that all items were loaded well on their latent factor. The second-order factor loadings were excellent, ranging from 0.913 to 0.987 (all >0.71).
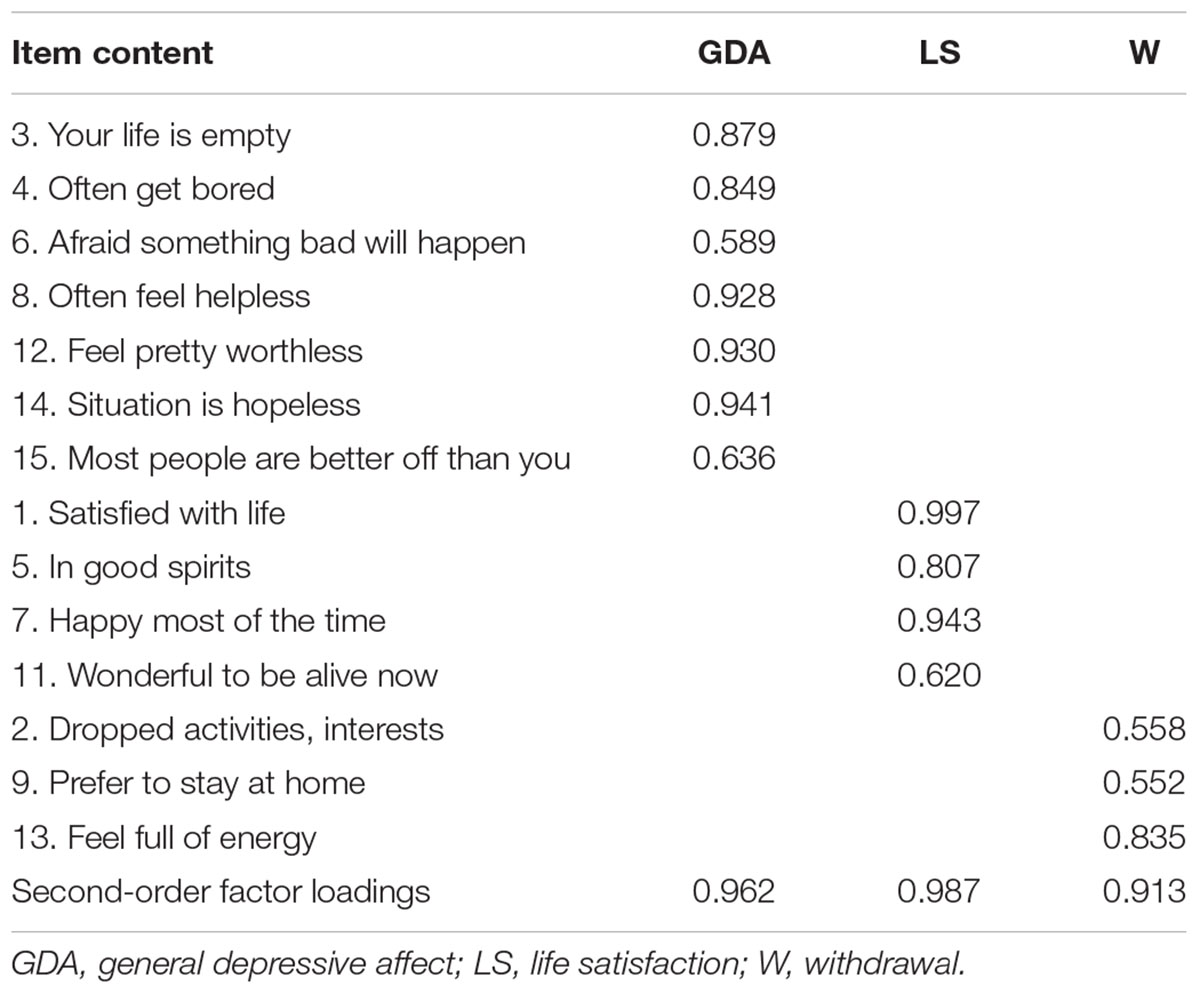
Table 4. Standardized factor loadings for the second-order CFA.
Given that the first-order and second-order factor model had the same fit indices, we did not test the factorial invariance of the second-order model. The results showed that the three-factor model of GDS-15 is an excellent fit of the data in both males and females. Results of multigroup CFA revealed that measurement invariance across gender groups was entirely supported at the factorial structure and the strict level (see Table 5). The ΔCFIs, ΔTLIs, and ΔRMSEAs are lower than 0.01 in all models, suggesting that the gender invariance of GDS-15 has been confirmed. GDS-15 items have the same meanings across genders; that is, we can compare the latent mean differences across these groups.
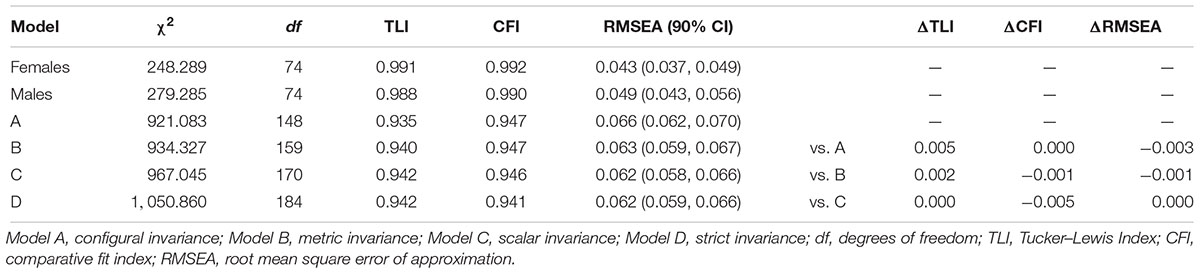
Table 5. Goodness-of-fit indices and model comparisons for measurement invariance models.
The 15-item Geriatric Depression Scale is a widely used questionnaire for evaluating late-life depression. This study determined the best factor structure of GDS-15 suitable for Chinese elders, and it is the first to employ second-order CFA to examine the validity of the GDS-15 total score. It is also the first study to examine the factorial invariance of the GDS-15 across gender groups among Chinese elders. The findings support that the GDS-15 is a valid instrument for screening depression and as a favorable choice in situation where economy of time is required.
Several previously reported alternative best-fit models were examined by CFA. Our CFA results revealed that the best factor structure of GDS-15 suitable for Chinese elders was the original three-factor model (i.e., general depressive affect, life satisfaction, and withdrawal). Item #10 “memory problems” was dropped from the three-factor model. The factor loadings of item 10 in other models were loaded poorly on their latent factor, suggesting that the most suitable factor structure of Chinese version GDS-15 was best explained by only 14 of the 15 items. Memory problems may be attributed to the aging process. Items (1, 5, 7, and 11) of life satisfaction were common items composing one factor (Friedman et al., 2005; Brown et al., 2007; Imai et al., 2014). Items (3, 4, 6, and 8) of the first factor were also common items composing one factor (Incalzi et al., 2003; Onishi et al., 2004). These findings indicate that the symptoms of depression are at least partly consistent across diverse geriatric populations. The best factor model of GDS-15 for Chinese elders implies the three sub-dimensions in late-life depression: general depressive affect, life satisfaction, and withdrawal. It is beneficial for us to detect and prevent late-life depression from these three aspects, which will improve the efficiency of primary care. The three factors were significantly correlated with each other both in sample 1 and in sample 2, indicating that the scale has high validity. The excellent second-order factor loadings indicated that first-order factors were adequately explained by the higher-order factor. The use of GDS-15 total score was meaningful. To the best of our knowledge, this study is the first study employing second-order factor analysis to examine the validity of the GDS-15 total score. It has significant meaning for both researchers and clinicians.
In order to compare the true differences across groups, assessment tools must be measurement invariant (Wu et al., 2012). The second purpose was to evaluate the measurement invariance of depressive symptoms across genders among Chinese elders. The three-factor structure of GDS-15 was well fitted to the data in both males and females. Multiple confirmatory factors showed that measurement invariance was supported, fully assuming different degrees of invariance. The establishment of configural invariance suggests that the number of factors and factor patterns of GDS-15 is equivalent among male and female. The determination of weak equivalence indicates that the observation items and potential factors of the scale have the same meaning across groups. Satisfying strong equivalence indicates that the cross-group difference of the observed variable mean can estimate the inter-group difference of the latent variable mean. The strict equivalence, which is the most stringent equivalent based on strong equivalence, reflects cross-group differences in latent variable variation. The results of this study confirm that GDS-15 is strictly equivalent, supporting that the GDS-15 factors have the same meaning across genders. Thus, comparisons of GDS-15 scores between men and women are meaningful. It is important that studies take measurement invariance into consideration when conducting cross-group research. Together with a recent work (He et al., 2018), our study supports the notion that the GDS (both the Long and the Short form) is a reliable, valid screening instrument for detecting depression in elderly Chinese individuals, with measurement invariance across genders. Owing to its ease of administration and short period of requirement, the GDS-15 is particularly useful in situations where the economy of time is required.
Several limitations of the present work should be acknowledged. Firstly, although all the study participants were from one of three provinces in China, they were otherwise heterogeneous in terms of gender, age, economic status, education, ethnicity, and region. These undetermined sample characteristics may exist in relation to gender differences in the GDS-15. Thus, the present results generalized to other dissimilar groups remain to be determined. Secondly, because the elderly with dementia or severe physical illness were excluded from this study, the current findings may not be applicable to these groups. Thirdly, our sample consisting of older Chinese cannot represent the worldwide population. Finally, validation of the gender invariance of this Chinese version of GDS-15 does not mean that the scale has invariance across time and culture, which should be determined in future research.
In conclusion, this study found that a three-factor model fitted the underlying structure of the Chinese version of GDS-15 best. The use of GDS-15 total score is valid. In addition, the three-factor structure of GDS-15 was shown to be invariant across gender groups. Therefore, the report of significant higher GDS-15 scores of females than males reflects a true gender difference, indicating that women have more depression problems than men in aging Chinese.
The datasets generated for this study are available on request to the corresponding author.
The study was approved by the Ethics Committee of the Second Xiangya Hospital of Central South University.
All authors revised and approved the submitted version. HZ performed the initial analyses and wrote the manuscript. JH helped with collecting the data and data analysis. SY and JY supervised the study.
This work was supported by the National Natural Science Foundation of China (Grant No. 81871074) and the National Science and Technology Project for Professional Basic Research (Grant No. 2015FY111600).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Almeida, O. P., and Almeida, S. A. (1999). Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 14, 858–865. doi: 10.1002/(SICI)1099-1166(199910)14:10<858::AID-GPS35>3.0.CO;2-8
Blazer, D. G. (2003). Depression in late life: review and commentary. J. Gerontol. A Biol. Sci. Med. Sci. 58, 249–265.
Boey, K. W. (2000). The use of GDS-15 among the older adults in Beijing. Clin. Gerontol. 21, 49–60. doi: 10.1300/J018v21n02_05
Broekman, B. F. P., Nyunt, S. Z., Niti, M., Jin, A. Z., Ko, S. M., Kumar, R., et al. (2008). Differential item functioning of the geriatric depression scale in an asian population. J. Affect. Disord. 108, 285–290. doi: 10.1016/j.jad.2007.10.005
Brown, P. J., Woods, C. M., and Storandt, M. (2007). Model stability of the 15-item geriatric depression scale across cognitive impairment and severe depression. Psychol. Aging 22, 372–379. doi: 10.1037/0882-7974.22.2.372
Castelo, M. S., Coelho, J. M., Carvalho, A. F., Lima, J. W. O., Noleto, J. C. S., Ribeiro, K. G., et al. (2010). Validity of the Brazilian version of the geriatric depression scale (GDS) among primary care patients. Int. Psychogeriatr. 22, 109–113. doi: 10.1017/s1041610209991219
Chaaya, M., Sibai, A. M., El Roueiheb, Z., Chemaitelly, H., Chahine, L. M., Al-Amin, H., et al. (2008). Validation of the Arabic version of the short geriatric depression scale (GDS-15). Int. Psychogeriatr. 20, 571–581. doi: 10.1017/s1041610208006741
Chen, F. F. (2007). Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. 14, 464–504. doi: 10.1080/10705510701301834
Cheung, G. W., and Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Res. Aging 9, 233–255. doi: 10.1207/S15328007SEM0902_5
Chiesi, F., Primi, C., Pigliautile, M., Baroni, M., Ercolani, S., Paolacci, L., et al. (2018). Does the 15-item geriatric depression scale function differently in old people with different levels of cognitive functioning? J. Affect. Disord. 227, 471–476. doi: 10.1016/j.jad.2017.11.045
Comrey, A. L., and Lee, H. B. (2013). A First Course in Factor Analysis. New York, NY: Psychology Press.
Cwikel, J., and Ritchie, K. (1989). Screening for depression among the elderly in Israel: an assessment of the short geriatric depression scale (S-GDS). Isr. J. Med. Sci. 25, 131–137.
Finney, S. J., and DiStefano, C. (2013). “Non-normal and categorical data in structural equation modeling,” in Structural Equation Modeling: A Second Course. 2nd Edn, eds G. R. Hancock and R. O. Mueller (Greenwich, CO: IAP), 439–492.
Fountoulakis, K. N., Tsolaki, M., Iacovides, A., Yesavage, J., O’Hara, R., Kazis, A., et al. (1999). The validation of the short form of the geriatric depression scale (GDS) in Greece. Aging Clin. Exp. Res. 11, 367–372. doi: 10.1007/bf03339814
Friedman, B., Heisel, M. J., and Delavan, R. L. (2005). Psychometric properties of the 15-item geriatric depression scale in functionally impaired, cognitively intact, community-dwelling elderly primary care patients. J. Am. Geriatr. Soc. 53, 1570–1576. doi: 10.1111/j.1532-5415.2005.53461.x
He, J. Y., Zhong, X., and Yao, S. Q. (2018). Factor structure of the geriatric depression scale and measurement invariance across gender among chinese elders. J. Affect. Disord. 238, 136–141. doi: 10.1016/j.jad.2018.04.100
Imai, H., Yamanaka, G., Ishimoto, Y., Kimura, Y., Fukutomi, E., Chen, W.-L., et al. (2014). Factor structures of a Japanese version of the Geriatric Depression Scale and its correlation with the quality of life and functional ability. Psychiatry Res. 215, 460–465. doi: 10.1016/j.psychres.2013.12.015
Incalzi, R. A., Cesari, M., Pedone, C., and Carbonin, P. U. (2003). Construct validity of the 15-item geriatric depression scale in older medical inpatients. J. Geriatr. Psychiatry Neurol. 16, 23–28. doi: 10.1177/0891988702250532
Ishine, M., Wada, T., Sakagami, T., Dung, P. T., Vienh, T. D., Kawakita, T., et al. (2005). Comprehensive geriatric assessment for community-dwelling elderly in Asia compared with those in Japan: III. Phuto in Vietnam. Geriatr. Gerontol. Int. 5, 115–121. doi: 10.1111/j.1447-0594.2005.00277.x
Iwamasa, G. Y., Hilliard, K. M., and Kost, C. R. (1998). The geriatric depression scale and japanese american older adults. Clin. Gerontol. 19, 13–24. doi: 10.1300/J018v19n03_03
Jang, Y., Small, B. J., and Haley, W. E. (2001). Cross-cultural comparability of the geriatric depression scale: comparison between older koreans and older americans. Aging Ment. Health 5, 31–37. doi: 10.1080/13607860020020618
Kim, G., DeCoster, J., Huang, C. H., and Bryant, A. N. (2013). A meta-analysis of the factor structure of the geriatric depression scale (GDS): the effects of language. Int. Psychogeriatr. 25, 71–81. doi: 10.1017/s1041610212001421
Kline, R. B. (2010). Principles and Practice of Structural Equation Modeling. 3rd Edn. New York, NY: The Guilford Press.
Lai, D., Tong, H., Zeng, Q., and Xu, W. (2010). The factor structure of a chinese geriatric depression scale-sf: use with alone elderly chinese in shanghai, china. Int. J. Geriatr. Psychiatry 25, 503–510. doi: 10.1002/gps.2369
Lai, D. W., Fung, T. S., and Yuen, C. T. (2005). The factor structure of a chinese version of the geriatric depression scale. Int. J. Psychiatry Med. 35, 137–148. doi: 10.2190/crk0-cbn7-qeve-xwpg
Lai, D. W. L. (2000). Measuring depression in Canada’s elderly Chinese population: use of a community screening instrument. Can. J. Psychiatry 45, 279–284. doi: 10.1177/070674370004500308
Lesher, E. L., and Berryhill, J. S. (1994). Validation of the geriatric depression scale—short form among inpatients. J. Clin. Psychol. 50, 256–260. doi: 10.1002/1097-4679(199403)50:2<256::AID-JCLP2270500218>3.0.CO;2-E
Liu, C. Y., Lu, C. H., Yu, S., and Yang, Y. Y. (1998). Correlations between scores on chinese versions of long and short forms of the geriatric depression scale among elderly chinese. Psychol. Rep. 82, 211–214. doi: 10.2466/pr0.82.1.211-214
Liu, L. J., and Guo, Q. (2008). Life satisfaction in a sample of empty-nest elderly: a survey in the rural area of a mountainous county in China. Qual. Life Res. 17, 823–830. doi: 10.1007/s11136-008-9370-1
Malakouti, S. K., Fatollahi, P., Mirabzadeh, A., Salavati, M., and Zandi, T. (2006). Reliability, validity and factor structure of the GDS-15 in Iranian elderly. Int. J. Geriatr. Psychiatry 21, 588–593. doi: 10.1002/gps.1533
Marsh, H. W., and Hocevar, D. (1985). Application of con?rmatory factor analysis to the study of self-concept: first- and higher order factor models and their invariance across groups. Psychol. Bull. 97, 562–582. doi: 10.1037//0033-2909.97.3.562
Mitchell, J., Mathews, H. F., and Yesavage, J. A. (1993). A multidimensional examination of depression among the elderly. Res. Aging 15, 198–219. doi: 10.1177/0164027593152004
Morin, A. J., Arens, A. K., Tracey, D., Parker, P. D., Ciarrochi, J., Craven, R. G., et al. (2017). Self-esteem trajectories and their social determinants in adolescents with different levels of cognitive ability. Am. J. Intellect. Dev. Disabil. 122, 539–560. doi: 10.1352/1944-7558-122.6.539
Mui, A. C. (1996). Geriatric depression scale as a community screening instrument for elderly Chinese immigrants. Int. Psychogeriatrics 8, 445–458. doi: 10.1017/s1041610296002803
Mui, A. C. (2010). Productive ageing in China: a human capital perspective. China J. Soc. Work 3, 112–124.
Muthén, L. K., and Muthén, B. O. (1998). Mplus User’s Guide, 7th Edn. Los Angeles, CA: Muthén and Muthén.
Nolen-Hoeksema, S. (2001). Gender differences in depression. Curr. Dir. Psychol. Sci. 10, 173–176. doi: 10.1111/1467-8721.00142
Onishi, J., Suzuki, Y., Umegaki, H., Endo, H., Kawamura, T., and Iguchi, A. (2006). A comparison of depressive mood of older adults in a community, nursing homes, and a geriatric hospital: factor analysis of geriatric depression scale. J. Geriatr. Psychiatry Neurol. 19, 26–31. doi: 10.1177/0891988705284725
Onishi, J., Umegaki, H., Suzuki, Y., Uemura, K., Kuzuya, M., and Iguchi, A. (2004). The relationship between functional disability and depressive mood in Japanese older adult inpatients. J. Geriatr. Psychiatry Neurol. 17, 93–98. doi: 10.1177/0891988704264738
Pocklington, C., Gilbody, S., Manea, L., and McMillan, D. (2016). The diagnostic accuracy of brief versions of the geriatric depression scale: a systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 31, 837–857. doi: 10.1002/gps.4407
Sheik, J. L., and Yesavage, J. A. (1986). Geriatric depression scale (GDS): recent evidence and develpment of shorter version. Clin. Gerontol. 5, 165–173. doi: 10.1300/J018v05n01_09
Stiles, P. G., and Mcgarrahan, J. F. (1998). The geriatric depression scale: a comprehensive review. J. Clin. Geropsychol. 4, 89–110.
Tang, W. K., Wong, E., Chiu, H. F., Lum, C. M., and Ungvari, G. S. (2005). The geriatric depression scale should be shortened: results of rasch analysis. Int. J. Geriatr. Psychiatry 20, 783–789. doi: 10.1002/gps.1360
Vrieze, S. I. (2012). Model selection and psychological theory: a discussion of the differences between the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC). Psychol. Methods 17, 228–243. doi: 10.1037/a0027127
Wang, M. C., Armour, C., Wu, Y., Ren, F., Zhu, X. Z., and Yao, S. Q. (2013). Factor structure of the CES-D and measurement invariance across gender in Mainland Chinese adolescents. J. Clin. Psychol. 69, 966–979. doi: 10.1002/jclp.21978
Wang, M. C., Elhai, J. D., Dai, X. Y., and Yao, S. Q. (2012). Longitudinal invariance of posttraumatic stress disorder symptoms in adolescent earthquake survivors. J. Anxiety Disord. 26, 263–270. doi: 10.1016/j.janxdis.2011.12.009
Wu, W. F., Lu, Y. B., Tan, F. R., Yao, S. Q., Steca, P., Abela, J. R. Z., et al. (2012). Assessing measurement invariance of the Children’s Depression Inventory in Chinese and Italian primary school student samples. Assessment 19, 506–516. doi: 10.1177/1073191111421286
Yao, S. Q., Zeng, H., and Sun, S. Y. (2009). Investigation on status and influential factors of cognitive function of the community-dwelling elderly in Changsha City. Arch. Gerontol. Geriatr. 49, 329–334. doi: 10.1016/j.archger.2008.11.00
Keywords: depression, factor structure, measurement invariance, Chinese elders, gender differences
Citation: Zhao H, He J, Yi J and Yao S (2019) Factor Structure and Measurement Invariance Across Gender Groups of the 15-Item Geriatric Depression Scale Among Chinese Elders. Front. Psychol. 10:1360. doi: 10.3389/fpsyg.2019.01360
Received: 07 March 2019; Accepted: 24 May 2019;
Published: 21 June 2019.
Edited by:
Laura Badenes-Ribera, University of Valencia, SpainReviewed by:
Francesca Chiesi, University of Florence, ItalyCopyright © 2019 Zhao, He, Yi and Yao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shuqiao Yao, c2h1cWlhb3lhb0Bjc3UuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.