
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Psychol. , 22 March 2019
Sec. Psychology for Clinical Settings
Volume 10 - 2019 | https://doi.org/10.3389/fpsyg.2019.00631
 Sara Palermo1,2*
Sara Palermo1,2* Agata Andò1
Agata Andò1 Adriana Salatino1
Adriana Salatino1 Stefano Sirgiovanni2Luana De Faveri2
Stefano Sirgiovanni2Luana De Faveri2 Antonella Carassa3
Antonella Carassa3 Maria C. Valentini2
Maria C. Valentini2 Rosalba Morese3*
Rosalba Morese3*Objective: Patients with lesions of the corpus callosum are rare and may present different symptoms of the disconnection syndrome. However, to-date studies on callosotomized patients have not been conclusive, likely because of the non-uniform nature of clinical features, the extent of resection, and methods used to investigate specific and related deficits. Agenesis of the corpus callosum (AgCC) may be asymptomatic and discovered incidentally or associated with very slight deficits diagnosed during neurological examinations. In this study, we reported a case of an apparently completely asymptomatic 23-year-old woman with appreciable agenesis of the splenium of the corpus callosum.
Methods: She underwent a neurological evaluation, a comprehensive battery of neuropsychological tests to identify any subclinical dysfunction that may affect the functionality of the subject in the daily life. Specifically, the possible presence of emotion dysregulation was examined by using a self-report questionnaire.
Results: She showed normal neuropsychological and emotional functioning, performing efficiently on tests measuring acquired brain impairment.
Discussion: The present case is discussed in terms of neuroplasticity – with a focus on putative compensatory mechanisms – emphasizing the variegated clinical feature patterns of brain defects present from birth.
The corpus callosum is the largest white matter commissure connecting the cerebral hemispheres (Aboitiz and Montiel, 2003; Schell-Apacik et al., 2008). It is regarded as having a role of transfer, integration and coordination of information between homologous brain areas and as being involved in learning, memory, thinking, three-dimensional visual ability, executive functions, as well as visual reaction time (Huang et al., 2015).
Agenesis of the corpus callosum (AgCC) is estimated to occur in approximately 0.2–0.7% of the general population (Schell-Apacik et al., 2008; Sefidbakht et al., 2016). Its prevalence in children with developmental disorders is as high as 230 in 10,000 (Jeret et al., 1986). AgCC encompasses complete absence as well as hypogenesis of the corpus callosum (Paul et al., 2007); the cause of AgCC in humans is not yet sufficiently known (only in 30–45% of cases). In the remaining 55–70% of individuals with AgCC, callosal agenesis is often an incidental neurological finding (Paul et al., 2014).
AgCC is associated with a wide range of cognitive, behavioral and neurological deficits (Schilmoeller and Schilmoeller, 2000). Three “cognitive patterns” observed in individuals with AgCC are the following: (1) neurodevelopmental disorders (i.e., autism spectrum); (2) normal intellectual ability (despite the presence of subtle neuropsychological deficits/abnormalities in the social cognition domain); and (3) overt neuropsychological impairment (Chiappedi and Bejor, 2010). AgCC is most often associated with mild limitations in tasks that involve interhemispheric transfer (Lassonde et al., 1991).
Slightly fewer than 33% of individuals with AgCC have “normal” or only slightly delayed development (Shevell, 2002) while the prognosis ranges from severely delayed to perfectly normal (Paul et al., 2007). For example, Lum et al. (2011) reported fMRI findings in three cases of asymptomatic AgCC. Nevertheless, when sensitive standardized neuropsychological measures are applied, a certain degree of impairment in higher-order cognition or social skills is observed (Paul et al., 2007). For example, AgCC individuals’ cognitive ratings of valence and arousal may show greater variance and may be less sensitive to negatively valenced stimuli (Paul et al., 2007). Moreover, AgCC subjects have been found to exhibit social-cognitive deficits and poor understanding of social-emotional aspects similar to those found in autism (Paul et al., 2004; Barnes et al., 2009; Turk et al., 2010; Lombardo et al., 2012). Interestingly, AgCC subjects can show impaired awareness of social and cognitive abilities (Brown and Paul, 2000; Paul et al., 2007), leading to delays in cognitive-behavioral profiling and difficulties in therapeutic engagement.
A few studies have been concerned the partial AgCC, in particular regarding the splenium. Knyazeva (2013) reported that ≪in the adult human brain, the function of the splenium in a given area is defined by the specialization of the area and implemented via excitation and/or suppression of the contralateral homotopic and heterotopic areas at the same or different level of visual hierarchy≫ (page 1). The anterior part contains thin late-myelinating fibers connecting the parietal and medial temporal regions, whereas the thick early-myelinating fibers connect primary/secondary visual areas (Barkovich and Kjos, 1988; Sano et al., 2008). The myelination pattern likely reflects the underlying complex splenium microarchitecture (Whitehead et al., 2014). The associative cortex actually develops after the primary cortical areas (Gogtay et al., 2004).
Knyazeva (2013) reported that ≪splenial fibers across brain areas are involved in a variety of functions, while their considerable variation between subjects implies a contribution of the splenium to plastic changes in the course of human development≫ (page 2).
The above considerations have led to specific questions about the long-term consequences of partial AgCC and whether lightweight behavioral-emotional symptoms might be able to escape detection due to coverage phenomena.
The present case report describes a young woman with agenesis of the splenium of the corpus callosum who appeared to be asymptomatic for her entire life.
At the time, we hypothesized that despite the apparent absence of symptoms, slight neuropsychological abnormalities could be hidden in the patient’s life history. In particular, we believed that behavioral abnormalities – of such entity as not to affect the patient’s daily life - could have emerged to a more careful evaluation of components generally not considered according to a purely neurological approach.
A 23-year-old woman was admitted to the Neuroradiology Division to participate in an experimental fMRI study as part of the “normal” control group. Inclusion criteria were the following: (1) no past or current mental illness assessed using the Mini-International Neuropsychiatric Interview (MINI) Plus: in particular, no major depression, dysthymia, mania or disinhibition based on DSM-V criteria; (2) no family history of mental illness or psychiatric hospitalization; (3) no history of head injury with loss of consciousness; (4) a Mini Mental State Examination (MMSE) (Folstein et al., 1975) score of ≥27; (5) no current pharmacological treatment, substance abuse or dependence that could substantially affect cognitive functioning.
At the pre-scan evaluation, the young woman was alert, conscious and oriented in time and space. Production and comprehension of language were preserved. The neurological examination was negative. The psychological interview for inclusion in the normal control group highlighted normal mental status and psychological adjustment, intellectual and problem-solving ability, processing speed and executive functioning.
The young woman1 had a normal postnatal developmental history and complete functional independence of long-living. She has reached the main milestones of young adulthood. Moreover, she denied any functional or social dysfunction in everyday life.
Neuroimaging data was acquired using a 3T Philips Ingenia scanner. Structural images were collected using T1-weighted (TR = 8.1 ms, TI = 900 ms, TE = 3.7 ms, voxel size = 1 × 1 × 1 mm3) and axial T2-weighted FSE (TR = 3200 ms, TE = 100 ms, FOV = 432 × 432 mm, section thickness = 4 mm, acceleration factor = 2) sequences. The MRI showed no alterations of the brain parenchyma in the supra and infratentorial sites. Ventricles and sulci were of normal size and aligned. However, unexpected appreciable agenesis of the splenium of the corpus callosum was found (Figure 1) with no alterations in the brain parenchyma signal in the supra and infratentorial sites.
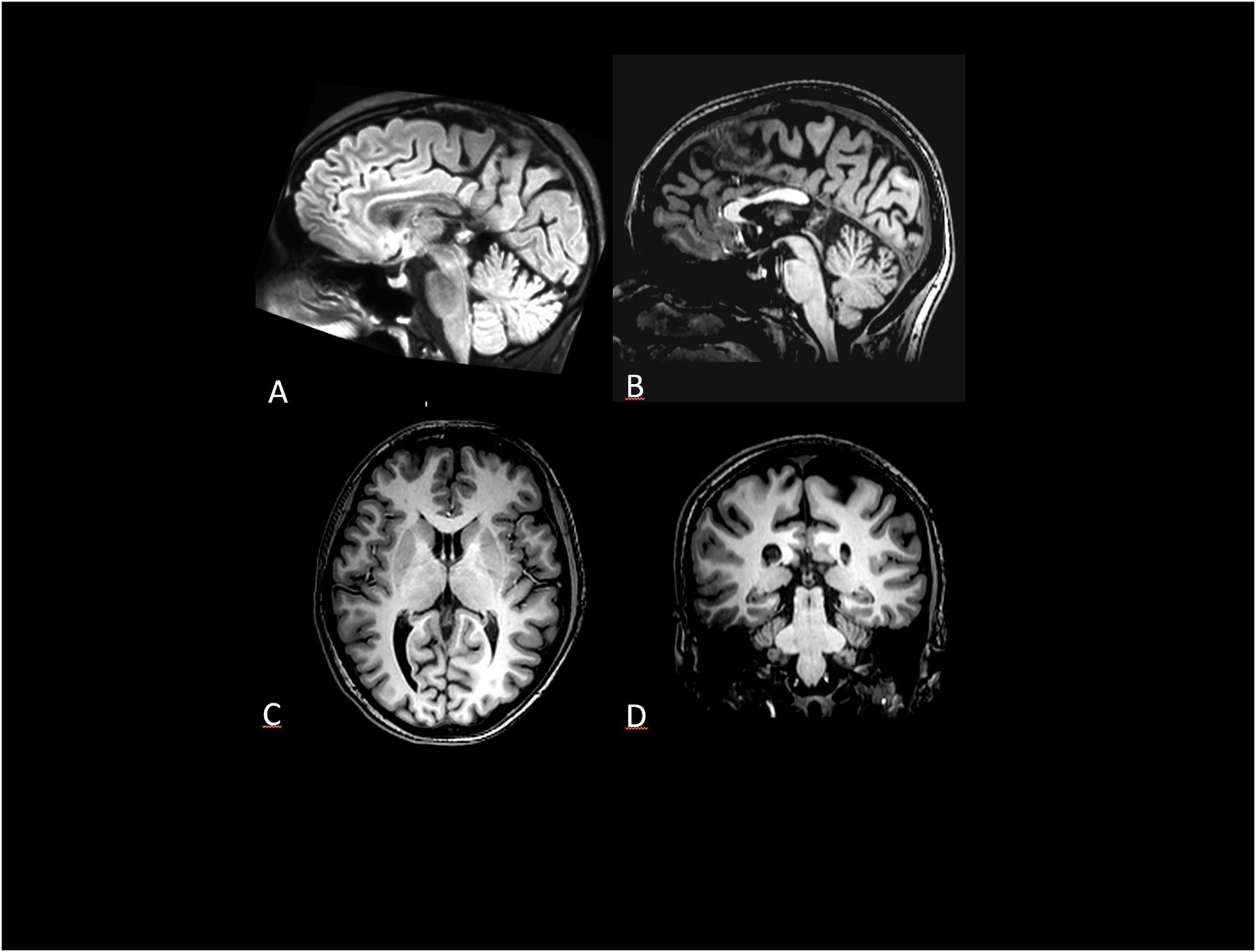
Figure 1. (A) Sagittal FLAIR 3D volume rendering and (B) Sagittal T1-WI shows normal rostrum, genu and body of corpus callosum and absent splenium (arrow) (C) Axial section through cavum septi pellucidi and internal cerebral vein within the cistern of the velum interpositum. (D) Coronal T1-WI: the retrothalamic cistern and medial wall of the lateral ventricles atri are delimited by cingulis and precuneus gyrus due to the splenium absence.
In view of such neuroimaging findings, YW was referred to the Neuroradiology Division in order to undergo a thorough neuropsychological evaluation (Palermo et al., 2015). The neurologist conducted a standardized interview with the patient on her health history before formalizing the diagnostic question to the neuropsychologist. The format of the health history is structured in order to organize patient information by following a written report for other health professionals. Subsequently, the neuropsychologist carried out a psychological anamnesis: it has the purpose of investigating aspects that serve to provide useful indications for the more possible precise psychological diagnosis. The complete interview is divided into the following topics: demographic data and marital status; physiological anamnesis; recent, near and remote anamnesis; functional anamnesis; psychological and psychopathological anamnesis; family history.
The Brief Psychiatric Rating Scale 4.0 (BPRS 4.0) was used to measure neuropsychiatric symptomatology (Roncone et al., 1999). Specific scales were employed to assess behavioral mood changes: the Apathy Evaluation Scale-Clinician version (AES-C) (Marin et al., 1991); the Hamilton Depression Rating Scale (HDR-S) (Hamilton, 1969); the Young Mania Rating Scale (YMRS) (Young et al., 1978). The Self-Regulation Skills Interview (SRSI) (Ownsworth et al., 2000, 2002), a clinical tool developed to measure higher levels of self-awareness and self-regulation skills that imply insight, motivation and compensation was also administered (Palermo et al., 2014).
The Toronto Alexithymia Scale (TAS-20) (Bagby et al., 1994) is one of the most widely used tools for measuring alexithymia. Alexithymia refers to individuals who are unable to identify and describe their emotions or have a tendency to minimize their emotional experience and to focus their attention externally. Items are rated on a 5-point Likert scale. The TAS-20 uses cut-off scoring: ≤51 = non-alexithymia, ≥61 = alexithymia.
The Difficulties in Emotion Regulation Scale (DERS) (Gratz and Roemer, 2004) was administered to assess multiple aspects of emotion dysregulation. DERS is a 36-item, self-report questionnaire comprising six subscales developed to detect multiple aspects of emotion dysregulation: (1) Non-acceptance of emotional responses (Non-acceptance); (2) Difficulties engaging in goal directed behavior (Goals); (3) Impulse control difficulties (Impulse); (4) Lack of emotional awareness (Awareness); (5) Limited access to emotion regulation strategies (Strategies); (6) Lack of emotional clarity (Clarity) (Gratz and Roemer, 2004). Recently, Giromini et al. (2017) provided equations to calculate age- and gender-adjusted T-scores, so that clinicians would easily interpret the resultant T-transformed DERS scores, which have a mean of 50 and standard deviation of 10. DERS scores between 65 and 70 T should indicate the presence of difficulties in emotion regulation, whereas scores higher than 70 T indicate important problems in emotion regulation. DERS reported high alpha coefficients ranging from 0.80 to 0.89 for the different scales. Exploratory factor analysis was used to provide data on the factor structure of the DERS and identify the underlying dimensions of emotion regulation as assessed by this tool. We obtained T-transformed DERS scores. As mentioned before, DERS scores between 65 and 70 T indicate the presence of problems in emotion regulation and scores higher than 70 T indicate significant problems in emotion regulation.
Intelligence was assessed using the Wechsler Adult Intelligence Scale – IV edition (WAIS-IV) (Lang et al., 2015). The pre-morbid intelligence quotient was estimated using the Brief Intelligence Test (TIB) (Sartori et al., 1995; Colombo et al., 2002) that is the Italian version of Nelson’s National Adult Reading Test (Nelson, 1982). Cognitive abilities were analyzed through a comprehensive battery of tests to measure (Palermo et al., 2018a): attention through Attentional Matrices (Spinnler and Tognoni, 1987); executive functions by means of Trial Making Test parts A, B (Reitan and Wolfson, 1994); memory through Wechsler Memory Scale -Subtests 4 and 7 (Wechsler, 1945); language oral production by means of verbal fluency (Spinnler and Tognoni, 1987). The absence of unilateral visual-attentional neglect was assessed by menas of the Bells Test (Gauthier et al., 1989). Dysexecutive syndrome was assessed using ecological neuropsychological tasks created to simulate daily life situations: the Behavioral Assessment of the Dysexecutive Syndrome test battery (BADS) (Wilson et al., 1996). Theory of Mind visual stories (ToM1 and ToM2) were used to test perspective-taking skills (Amanzio et al., 2008), while the Reading the Mind in the Eyes task (RME) was used to measure social cognition and emotion recognition abilities (Baron-Cohen et al., 2001). Metacognition was assessed with the metacognitive version of the Wisconsin Card Sorting Test (m-WCST) (Koren et al., 2006).
Young women had a normal cognitive and intellectual level and obtained normative scores on all the neuropsychological tasks that were administered. The IQ total score – determined by means of the WAIS-IV – was 108 (average range). Not only visual scanning and visual integrative skills were within the normal range at the clinical observation, but visuospatial abilities were preserved when evaluated through WAIS-IV sub-tests. Visuo-constructional ability on the Block Design subtest was above average. Scores for the accessible fund of knowledge, concept information, knowledge of word meaning, verbal fluency, and word reading were all within the normal range. Abstract reasoning was within the normal range. Her ability to generate and test concepts when presented with a novel problem-solving task was normal. Immediate and delayed recall for verbal narrative were normal. Behavioral programs initiation was within the normal range. Moreover, YW did not show difficulties at cognitive level. In addition, attention and mental flexibility were also in line with normal limits. There was no dysexecutive syndrome as measured by the BADS.
From a neuropsychiatric point of view, test behavior was devoid of any impersistence, intrusions or perseveration. Scores of the neuropsychological evaluation are presented in Table 1.
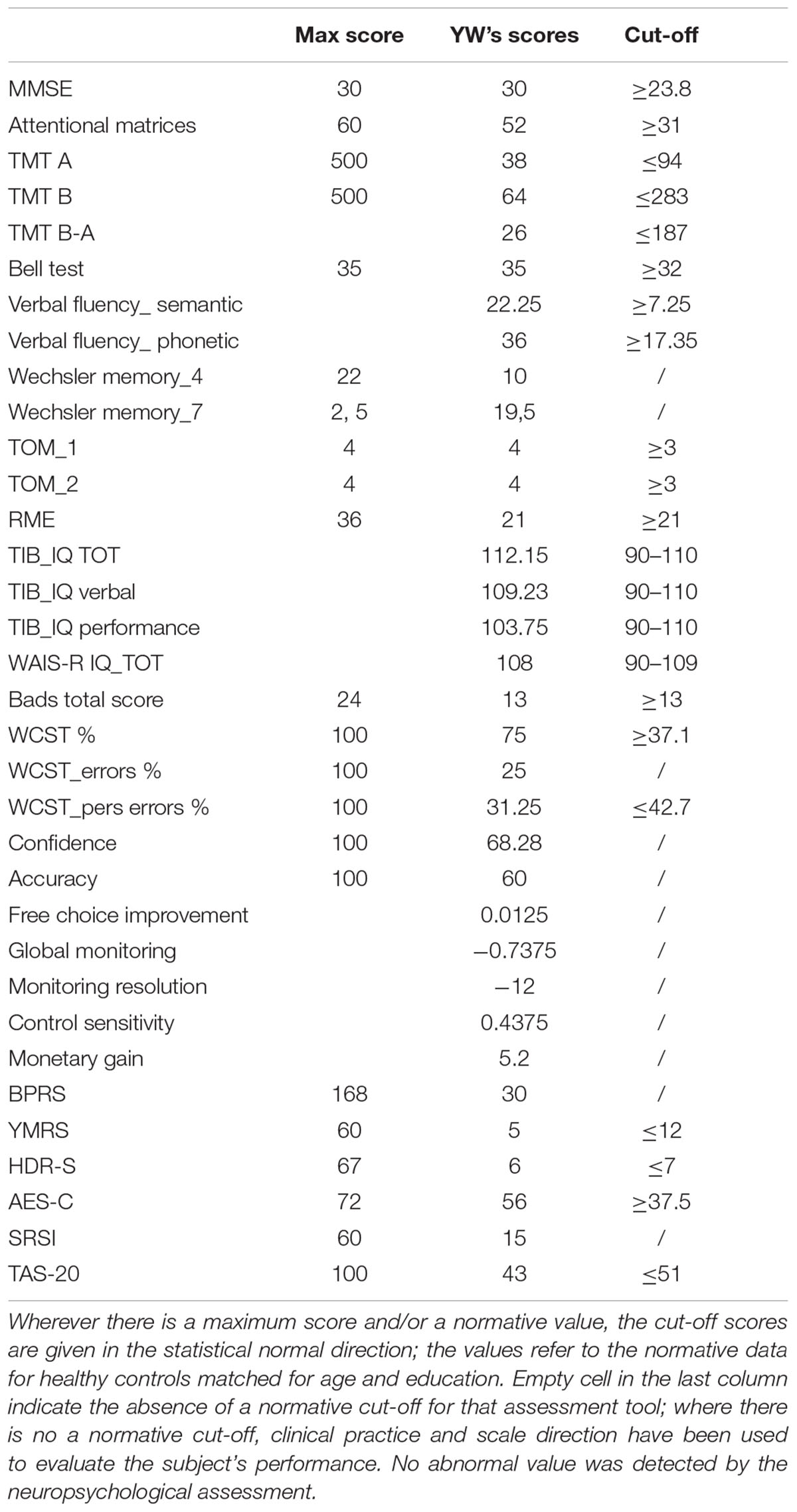
Table 1. Neuropsychiatric and neuropsychological evaluation synopsis.
The neuropsychiatric examination was almost normal, with the young woman’s scores on the YMRS, HDR-S, and AES-C all being below the cut-off point. Her SRSI scores appeared to indicate preserved insight. Moreover, alexithymia was not present as measured by the TAS-20.
The DERS scale scores indicate the overall tendency to accept negative emotions, knowledge of emotions, abilities to control impulsive behaviors and to use of situationally appropriate strategies to modulate own emotional responses (see Table 2). In addition, it is noteworthy that YW obtained low DERS scores (i.e., lower than 50 T) on the Goals and Clarity scales, which is referred to the ability to perform a goal-directed behavior and clarity of emotions (see Table 2).
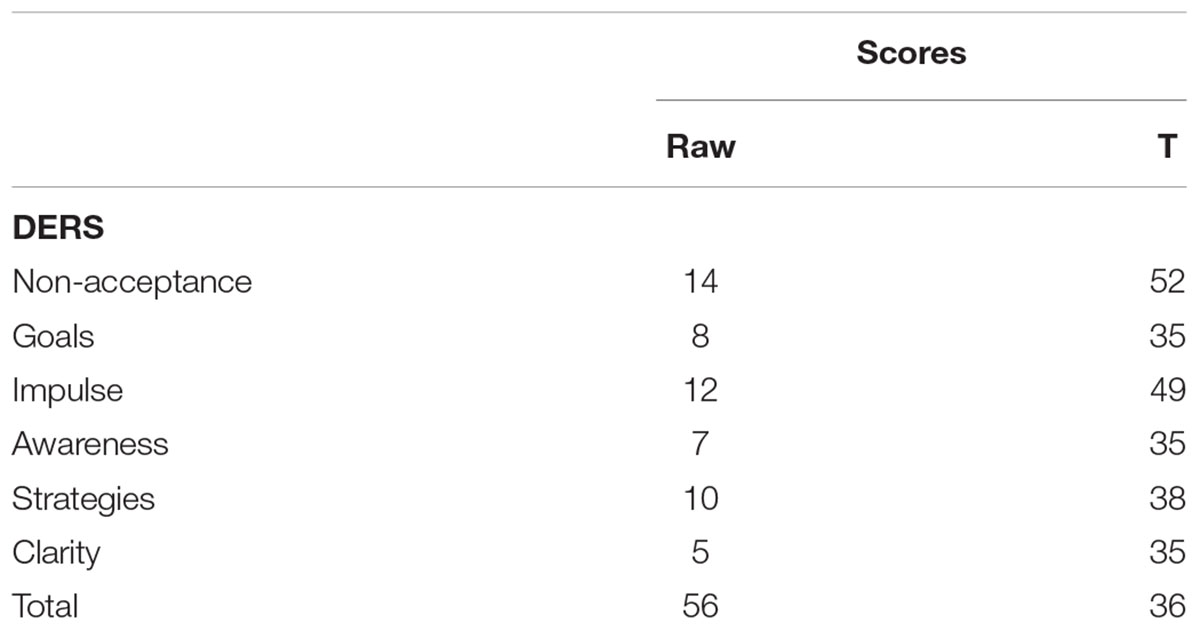
Table 2. DERS‘s results.
Patients with callosal alterations of different locations and extent or splenium agenesis should present distinct symptoms of disconnection syndrome (Campbell et al., 1981). However, studies in patients who have undergone callosotomy have not been conclusive, likely because of the heterogeneity of patients’ clinical features and age, the extent of resection, and the different methods used to investigate the related deficits (Bentin et al., 1984; Badan and Caramazza, 1997). While AgCC may be associated with neurological problems, it is thought that such conditions are due to anomalies in cerebral connections rather than in the corpus callosum itself (Sande and Garge, 2010). Considering the splenium of the corpus callosum, Park et al. (2014) reported that not only individuals who only had in situ lesions displayed relatively mild symptoms, but also they had no impaired cognition (unlike when multiple lesions in other callosal areas were ascertained).
In this case report, the fact that YW’s postnatal development history, long-term functional independence in her daily living, and current cognitive performance were normal supports the view that partial AgCC has not prevented normal cognitive development – unlike what happens in cases of complete agenesis (Paul et al., 2007).
The young woman’s neuropsychological functions were preserved, and she performed well on tests capable of detecting brain dysfunction such as the BADS, WCST, and RME. Although scores on self-report scales in adults with primary AgCC often imply diminished self-awareness (Brown and Paul, 2000), YW’s awareness appeared to be normal. The absence of two factors that might possibly contribute to low self-awareness, namely a generally impaired ability to understand or describe social situations (Paul et al., 2007) and metacognitive-executive dysfunctions (Palermo et al., 2014, 2015, 2017, 2018b; Morese et al., 2018), is an indication that the YW’s self-perception remained intact.
Although disconnection symptoms have been reported in AgCC, they were not exhibited by YM. Importantly, a disconnection syndrome is less likely to be exhibited by adults with AgCC and individuals who have undergone callosotomy during their childhood (Barr and Corballis, 2002).
The neuropsychological diagnostic investigations have therefore confirmed what we previously hypothesized and substantiated by YM’s close and remote anamnesis: no obvious functional or cognitive impairment affects YM’s daily living.
How the absence of neuropsychological symptomatology could be explained – considering the presence of a cerebral structural anomaly that would suppose a functional repercussion?
A mechanism of functional compensation in AgCC has been identified in the hypertrophy of the anterior commissure (Fischer et al., 1992). The authors described a case of a patient with AgCC and enlarged anterior commissure verified by magnetic resonance imaging (MRI) exams that have obtained normal scores on both visual and tactile interhemispheric transfer tasks. Our clinical case could suggest considerations for the idea that adults with AgCC might benefit from some form of neural compensation during the early stages of growth and development (Paul, 2011).
The far-reaching plastic changes observed in AgCC and young patients who have undergone callosotomy might occur during a critical developmental phase that coincides with synaptic overproduction and redundancy (Lassonde and Jeeves, 1991). Neural functioning in isolated AgCC is evidence of the far-reaching plastic changes that take place in the developing human brain (Paul et al., 2014). Since resting-state functional brain connectivity can be surprisingly intact in isolated AgCC, it is possible that the brains of adults with AgCC might generate a typical, bilateral set of resting-state functional brain networks (Tyszka et al., 2011). Tyszka et al. (2011) reported that ≪almost all of the group-level independent components identified in controls were observed in AgCC and were predominantly bilaterally symmetric≫ (page 15154). According to the authors, when the corpus callosum is absent, ≪functional networks emerge flexibly with the development of normal cognition and behavior and can be realized in multiple structural architectures≫ (page 15154).
Despite this evidence, interhemispheric functional connectivity in AgCC appears to vary more when patients are engaged in cognitive tasks (Paul et al., 2014). Indeed, AgCC subjects do not have the features of the classic disconnection syndrome observed in patients who have undergone corpus callosotomy, but they might show mild disruption of interhemispheric transfer (Paul et al., 2014). The limits of such compensation might become more apparent when performing tasks that involve complex cognitive operations, require fast processing, and are less reliant on previous experience (Paul et al., 2007, 2014).
In line with these scientific findings, Hinkley et al. (2012) reported that disrupted callosal development can lead to reduced functional connectivity (FC) resulting in impairments in specific cognitive domains. Interestingly, the authors performed a planned comparison between patients with partial AgCC (pAgCC) and complete AgCC (cAgCC) in order to understand how callosal integrity can be associated with cognitive abilities. They concluded that concomitant anatomical tracts developed specifically in AgCC patients (Tovar-Moll et al., 2007; Wahl et al., 2009) might affect inter- and intra-hemispheric connectivity and the related underlying cognitive mechanisms (Hinkley et al., 2012). Indeed, a possible peculiarity in YW’s FC might therefore explain not only her normal cognitive profile but also her sufficient ability in accepting negative emotions, capacities to perform goal-directed behavior (this is the Goal scale), and clarity of her experienced emotions as reported by the Clarity scale. In fact, the scores YW obtained on all DERS scales are within the normal range (i.e., scores ≤50 T). She showed a good capacity of emotion regulation, although the Non-acceptance scale reported the highest score (T = 52) when compared to the scores obtained by the other DERS scales. This finding – as isolated and selective – substantiates what was our initial hypothesis: not at the cognitive level but at the level of subclinical behavioral-psychological slight impairment were to be looked for any deficit in the case of YW. In this regard, we may speculate that she usually tries to manage those negative emotions experienced as invasive by using rationalization as a defense mechanism in which negative feelings and emotions are explained in a seemingly rational manner to make them consciously tolerable (see the scores on the other DERS scales). Although previous studies have investigated the processing of verbal/psychophysiological indices of emotional arousal in relation to the left and right hemispheres (Wahl et al., 2009; Morese et al., 2016; Giromini et al., 2016), the way the two hemispheres normally interact in order to produce emotional responses to stimuli is yet to be explained (Paul et al., 2007). Some patients with AgCC reported high skin conductivity; in general, the level of skin-conductance responses can discriminate emotion between different categories (Paul et al., 2007). The authors suggested that largely intact right hemisphere mechanisms might support psychophysiological emotional responses. This mechanism might cause YW to behave consistently with the socio-relational stimuli coming from the environment. In addition, Paul et al. (2006) also suggested that the absence of interhemispheric communication in AgCC may affect normal verbal ratings of arousal, a mechanism that is consistent with some alexithymia models. Indeed, a hallmark of alexithymia is the difficulty of putting emotional states into words (Franz et al., 2008). Alexithymia is considered as a personality trait that is normally distributed in the population and is associated with increased risk of psychopathology (Franz et al., 2008). Alexithymia is associated with an inability to regulate affect using adaptive processes like expressing or suppressing emotions, using imagination, modulating arousal, getting and making use of social support, coping with distress, cognitive assimilation, and accommodation (Taylor et al., 1997). It is therefore thought to be among the factors contributing to conditions such as depression, anxiety, compulsive and addictive behavior, heightened or prolonged physiological arousal, physical symptoms, and even somatic symptom disorders (Taylor et al., 1997). The fact that YW obtained a normative score on the TAS-20 scale supports the idea that compensatory brain plasticity mechanisms are intensified during development, which is why she is able to behave normally in daily life.
It has been postulated that the posterior midline regions may have an important role for self-referential and social-cognitive development. Thus, the case of YW, who had pAgCC, is possibly less extreme than it would have been with cAgCC (Pfeifer and Peake, 2012). This aspect will be addressed in further clinical studies of our patient. Importantly, an approach that takes into account multiple levels of analysis, such as neuropsychological measures neuropsychological tests associated with functional neuroimaging, is needed in order to gain a clear understanding of YW’s behavioral and cognitive profile.
AgCC can be entirely asymptomatic or associated with very slight deficits diagnosed during neurological examinations. With an incidence of just 1 in 4000 in the general population, AgCC is rare and cases are very difficult to find. Nevertheless, we believe that this case report sheds light on how a structural defect could have a more complex effect than the one already known about brain function and highlights the need for clear guidelines to manage incidental MRI findings in the research setting. Indeed, the present case report wants to be a driving force for a more careful evaluation of occasional MRI findings so that subclinical psychological alterations that might negatively affect the quality of life of patients can be recognized and treated where necessary. Given that distinct methods engage and assess distinct mental processes (Bornstein, 2017), it is noteworthy that we used a multimethod assessment including different measures, in order to examine thoroughly the psychological functioning (resources and limits).
We suggested that theoretical models of brain alteration might be more effective if they integrate MRI, psychological and neuropsychological data, adopting a neurocognitive approach. In particular, a multidimensional approach involving instruments for the evaluation of complex, highly selective functions would be useful.
It would be important to replicate these observations on a group of patients, as the proposed conclusions could not be generalized. An important limitation of this work is undoubtedly the impossibility of assessing further cognitive domains in depth. This is because YW has been sent to our observation with an unspecific question by the attending neurologist. It would have been opportune to evaluate with greater attention the visuo-spatial abilities and the possible presence of spatial neglect. However, these elements seem to be not predictors of any anomalies in the DERS scores.
The study was approved by the Ethics Committee “A.O.U. Città della Salute e della Scienza di Torino – A.O. Ordine Mauriziano – A.S.L. Città di Torino” as part of the core research criteria followed by the Neuroradiological Division. All the implemented procedures ensured the safety, integrity, and privacy of patients. Any critical aspects, neither with regard to the fMRI acquisition, nor to the neuropsychological assessment could be noticed. Importantly, the study has been conducted according to the principles set forth by the Declaration of Helsinki (59th WMA General Assembly, Seoul, October 2008) and in accordance with the Medical Research Involving Human Subjects Act (WMO). Written informed consent was obtained from YW both for the purposes of research participation as well as for the publication of the case report, including indirectly identifiable data.
The case-report study is based on a concept developed by RM who wrote the manuscript and took part in the review and critique processes as PI. Moreover, RM conducted the MRI execution. SP organized the study, performed the neuropsychological assessment (organization and execution), wrote the manuscript and participated in the review and critique processes. AA participated in the administration, scoring evaluation and interpretation of all the psychological results. Moreover, she participated in writing the manuscript and in the review process. SS and LDF conducted the MRI acquisition. MV organized and conducted the MRI acquisition, participated in the interpretation of results and in writing the manuscript. AS participated in writing the manuscript. AC participated in writing the manuscript (review and critique). All the contributors gave their approval of this version of the manuscript to be submitted.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank our patient and her family for allowing us to complete all of the above study.
Aboitiz, F., and Montiel, J. (2003). One hundred million years of interhemispheric communication: the history of the corpus callosum. Braz. J. Med. Biol. Res. 36, 409–420. doi: 10.1590/S0100-879X2003000400002
Amanzio, M., Geminiani, G., Leotta, D., and Cappa, S. (2008). Metaphor comprehension in Alzheimer’s disease: novelty matters. Brain Lang. 107, 1–10. doi: 10.1016/j.bandl.2007.08.003
Badan, M., and Caramazza, A. (1997). Haptic processing by the left hemisphere in a split-brain patient. Neuropsychologia 35, 1275–1287. doi: 10.1016/S0028-3932(97)00051-1
Bagby, R. M., Taylor, G. J., and Parker, J. D. (1994). The twenty-item Toronto Alexithymia Scale-II: convergent, discriminant, and concurrent validity. J. Psychosom. Res. 38, 33–40. doi: 10.1016/0022-3999(94)90006-X
Barkovich, A. J., and Kjos, B. O. (1988). Normal postnatal development of the corpus callosum as demonstrated by MR imaging. AJNR Am. J. Neuroradiol. 9, 487–491.
Barnes, J. L., Lombardo, M. V., Wheelwright, S., and Baron-Cohen, S. (2009). Moral dilemmas film task: a study of spontaneous narratives by individuals with autism spectrum conditions. Autism Res. 2, 148–156. doi: 10.1002/aur.79
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., and Plumb, I. (2001). The “Reading the Mind in the Eyes” Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 42, 241–251. doi: 10.1111/1469-7610.00715
Barr, M. S., and Corballis, M. C. (2002). The role of the anterior commissure in callosal agenesis. Neuropsychology 16, 459–471. doi: 10.1037/0894-4105.16.4.459
Bentin, S., Sahar, A., and Moscovitch, M. (1984). Intermanual information transfer in patients with lesions in the trunk of the corpus callosum. Neuropsychologia 22, 601–611. doi: 10.1016/0028-3932(84)90024-1
Bornstein, R. F. (2017). Evidence-based psychological assessment. J. Pers. Assess. 99, 435–445. doi: 10.1080/00223891.2016.1236343
Brown, W. S., and Paul, L. K. (2000). Cognitive and psychosocial deficits in agenesis of the corpus callosum with normal intelligence. Cogn. Neuropsychiatr. 5, 135–157. doi: 10.1080/135468000395781
Campbell, A. L., Bogen, J. E., and Smith, A. (1981). Disorganization and reorganization of cognitive and sensorimotor functions in cerebral commissurotomy. Compensatory roles of the forebrain commissures and cerebral hemispheres in man. Brain 104, 493–511. doi: 10.1093/brain/104.3.493
Chiappedi, M., and Bejor, M. (2010). Corpus callosum agenesis and rehabilitative treatment. Ital. J. Pediatr. 36:64. doi: 10.1186/1824-7288-36-64
Colombo, L., Sartori, G., and Brivio, C. (2002). Stima del quoziente intellettivo tramite l’applicazione del TIB (test breve di intelligenza). G. Ital. Psicol. 3, 613–637.
Fischer, M., Ryan, S. B., and Dobyns, W. B. (1992). Mechanisms of interhemispheric transfer and patterns of cognitive function in acallosal patients of normal intelligence. Arch. Neurol. 49, 271–277. doi: 10.1001/archneur.1992.00530270085023
Folstein, M. F., Folstein, S. E., and McHugh, P. R. (1975). “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198. doi: 10.1016/0022-3956(75)90026-6
Franz, M., Popp, K., Schaefer, R., Sitte, W., Schneider, C., Hardt, J., et al. (2008). Alexithymia in the German general population. Soc. Psychiatry Psychiatr. Epidemiol. 43, 54–62. doi: 10.1007/s00127-007-0265-1
Gauthier, L., Dehaut, F., and Joannette, Y. (1989). The Bells Test: a quantitative and qualitative test for visual neglect. Int. J. Clin. Neuropsychol. 11, 49–54.
Giromini, L., Ales, F., de Campora, G., Zennaro, A., and Pignolo, C. (2017). Developing age and gender adjusted normative reference values for the difficulties in emotion regulation scale (DERS). J. Psychopathol. Behav. Assess. 39, 705–714. doi: 10.1007/s10862-017-9611-0
Giromini, L., Ando’, A., Morese, R., Salatino, A., Di Girolamo, M., Viglione, D. J., et al. (2016). Rorschach Performance Assessment System (R-PAS) and vulnerability to stress: a preliminary study on electrodermal activity during stress. Psychiatry Res. 246, 166–172. doi: 10.1016/j.psychres.2016.09.036
Gogtay, N., Giedd, J. N., Lusk, L., Hayashi, K. M., Greenstein, D., Vaituzis, A. C., et al. (2004). Dynamic mapping of human cortical development during childhood through early adulthood. Proc. Natl. Acad. Sci. U.S.A. 101, 8174–8179. doi: 10.1073/pnas.0402680101
Gratz, K. L., and Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 26, 41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
Hamilton, M. (1969). A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 23, 56–62. doi: 10.1136/jnnp.23.1.56
Hinkley, L. B., Marco, E. J., Findlay, A. M., Honma, S., Jeremy, R. J., Strominger, Z., et al. (2012). The role of corpus callosum development in functional connectivity and cognitive processing. PLoS One 7:e39804. doi: 10.1371/journal.pone.0039804
Huang, X., Du, X., Song, H., Zhang, Q., Jia, J., Xiao, T., et al. (2015). Cognitive impairments associated with corpus callosum infarction: a ten cases study. Int. J. Clin. Exp. Med. 8, 21991–21998.
Jeret, J. S., Serur, D., Wisniewski, K. E., and Fisch, C. (1986). Frequency of agenesis of the corpus callosum in the developmentally disabled population as determined by computerized tomography. Pediatr. Neurosci. 12, 101–103. doi: 10.1159/000120229
Knyazeva, M. G. (2013). Splenium of corpus callosum: patterns of interhemispheric interaction in children and adults. Neural Plast. 2013:639430. doi: 10.1155/2013/639430
Koren, D., Seidman, L. J., Goldsmith, M., and Harvey, P. D. (2006). Real-world cognitive–and metacognitive–dysfunction in schizophrenia: a new approach for measuring (and remediating) more “right stuff”. Schizophr. Bull. 32, 310–326. doi: 10.1093/schbul/sbj035
Lang, M., Michelotti, C., and Bardelli, E. (2015). WAIS-IV. Wechsler Adult Intelligence-Scale-IV: Lettura dei Risultati e Interpretazione Clinica. Milano: Raffaello Cortina.
Lassonde, M., and Jeeves, M. A. (1991). Callosal Agenesis: A Natural Split-Brain? In Advances in Behavioral Biology. New York, NY:Plenum Press.
Lassonde, M., Sauerwein, H., Chicoine, A. J., and Geoffroy, G. (1991). Absence of disconnexion syndrome in callosal agenesis and early callosotomy: brain reorganization or lack of structural specificity during ontogeny? Neuropsychologia 29, 481–495.
Lombardo, M. V., Chakrabarti, B., Lai, M., Mrc Aims Consortium, and Baron-Cohen, S. (2012). Self-referential and social cognition in a case of autism and agenesis of the corpus callosum. Mol. Autism 3:14. doi: 10.1186/2040-2392-3-14
Lum, C., McAndrews, M. P., Holodny, A. I., McManus, K. A., Crawley, A., Chakraborty, S., et al. (2011). Investigating agenesis of the corpus callosum using functional MRI: a study examining interhemispheric coordination of motor control. Neuroimaging. 21, 65–68. doi: 10.1111/j.1552-6569.2009.00430.x
Marin, R. S., Biedrzycki, R. C., and Firinciogullari, S. (1991). Reliability and validity of the apathy evaluation scale. Psychiatry Res. 38, 143–162. doi: 10.1016/0165-1781(91)90040-V
Morese, R., Rabellino, D., Sambataro, F., Perussia, F., Valentini, M. C., Bara, B. G., et al. (2016). Group membership modulates the neural circuitry underlying third party punishment. PLoS One 11:e0166357. doi: 10.1371/journal.pone.0166357
Morese, R., Stanziano, M., and Palermo, S. (2018). Commentary: metacognition and perspective-taking in Alzheimer’s disease: a mini-review. Front. Psychol. 9:2010. doi: 10.3389/fpsyg.2018.02010
Nelson, H. E. (1982). National Adult Reading Test (NART): For the Assessment of Premorbid Intelligence in Patients with Dementia: Test Manual. Windsor: NFER-Nelson.
Ownsworth, T. L., McFarland, K., and Young, R. M. (2002). The investigation of factors underlying deficits in self-awareness and self-regulation. Brain Inj. 16, 291–309. doi: 10.1080/02699050110103986
Ownsworth, T. L., McFarland, K. M., and Young, R. M. (2000). Development and standardization of the Self-regulation Skills Interview (SRSI): a new clinical assessment tool for acquired brain injury. Clin. Neuropsychol. 14, 76–92. doi: 10.1076/1385-4046(200002)14:1;1-8;FT076
Palermo, S., Cauda, F., Costa, T., Duca, S., Gallino, G., Geminiani, G., et al. (2015). Unawareness of bipolar disorder: the role of the cingulate cortex. Neurocase 21, 438–447. doi: 10.1080/13554794.2014.917682
Palermo, S., Leotta, D., Bongioanni, M. R., and Amanzio, M. (2014). Unawareness of deficits in ischemic injury: role of the cingulate cortex. Neurocase 20, 540–555. doi: 10.1080/13554794.2013.826686
Palermo, S., Lopiano, L., Morese, R., Zibetti, M., Romagnolo, A., Stanziano, M., et al. (2018a). Role of the cingulate cortex in dyskinesias-reduced-self-awareness: an fMRI Study on Parkinson’s disease patients. Front. Psychol. 9:1765. doi: 10.3389/fpsyg.2018.01765
Palermo, S., Stanziano, M., and Morese, R. (2018b). Commentary: anterior cingulate cortex and response conflict: effects of frequency, inhibition and errors. Front. Behav. Neurosci. 12:171. doi: 10.3389/fnbeh.2018.00171
Palermo, S., Lopiano, L., Zibetti, M., Rosato, R., Leotta, D., and Amanzio, M. (2017). A novel framework for understanding reduced awareness of dyskinesias in Parkinson’s Disease. Parkinsonism Relat. Disord. 39, 58–63. doi: 10.1016/j.parkreldis.2017.03.009
Park, M. K., Hwang, S. H., Jung, S., Hong, S. S., and Kwon, S. B. (2014). Lesions in the splenium of the corpus callosum: clinical and radiological implications. Neurol. Asia 19, 79–88.
Paul, L. K. (2011). Developmental malformation of the corpus callosum: a review of typical callosal development and examples of developmental disorders with callosal involvement. J. Dev. Disord. 3, 3–27. doi: 10.1007/s11689-010-9059-y
Paul, L. K., Brown, W. S., Adolphs, R., Tyszka, J. M., Richards, L. J., Mukherjee, P., et al. (2007). Agenesis of the corpus callosum: genetic, developmental and functional aspects of connectivity. Nat. Rev. Neurosci. 8, 287–299. doi: 10.1038/nrn2107
Paul, L. K., Corsello, C., Kennedy, D. P., and Adolphs, R. (2014). Agenesis of the corpus callosum and autism: a comprehensive comparison. Brain 137(Pt 6), 1813–1829. doi: 10.1093/brain/awu070
Paul, L. K., Lautzenhiser, A., Brown, W. S., Hart, A., Neumann, D., Spezio, M., et al. (2006). Emotional arousal in agenesis of the corpus callosum. Int. J. Psychophysiol. 61, 47–56. doi: 10.1016/j.ijpsycho.2005.10.017
Paul, L. K., Schieffer, B., and Brown, W. S. (2004). Social processing deficits in agenesis of the corpus callosum: narratives from the Thematic Appreciation Test. Arch. Clin. Neuropsychol. 19, 215–225. doi: 10.1016/S0887-6177(03)00024-6
Pfeifer, J. H., and Peake, S. J. (2012). Self-development: integrating cognitive, socioemotional, and neuroimaging perspectives. Dev. Cogn. Neurosci. 2, 55–69. doi: 10.1016/j.dcn.2011.07.012
Reitan, R. M., and Wolfson, D. (1994). A selective and critical review of neuropsychological deficits and the frontal lobes. Neuropsychol. Rev. 3, 161–198. doi: 10.1007/BF01874891
Roncone, R., Ventura, J., Impallomeni, M., Falloon, I. R., Morosini, P. L., Chiaravalle, E., et al. (1999). Reliability of an Italian standardized and expanded Brief Psychiatric Rating Scale (BPRS 4.0) in raters with high vs. low clinical experience. Acta Psychiatr. Scand. 100, 229–236. doi: 10.1111/j.1600-0447.1999.tb10850.x
Sande, S., and Garge, S. (2010). Agenesis of the corpus callosum. J. Pediatr. Neurosci. 5, 83–88. doi: 10.4103/1817-1745.66662
Sano, M., Kuan, C. C., Kaga, K., Itoh, K., Ino, K., and Mima, K. (2008). Early myelination patterns in the central auditory pathway of the higher brain: MRI evaluation study. Int. J. Pediatr. Otorhinolaryngol. 72, 1479–1486. doi: 10.1016/j.ijporl.2008.06.011
Sartori, G., Colombo, L., Vallar, G., Rusconi, M. L., and Pinarello, A. (1995). T.I.B. Test di Intelligenza Breve per la valutazione del quoziente intellettivo attuale e premorboso. Professione Psicologo. G. Dellordine Psicol. 4, 1–24.
Schell-Apacik, C. C., Wagner, K., Bihler, M., Ertl-Wagner, B., Heinrich, U., Klopocki, E., et al. (2008). Agenesis and dysgenesis of the corpus callosum: clinical, genetic and neuroimaging findings in a series of 41 patients. Am. J. Med. Genet. 146A, 2501–2511. doi: 10.1002/ajmg.a.32476
Schilmoeller, G., and Schilmoeller, K. (2000). Filling a void: facilitating family support through networking for children with a rare disorder. Fam. Sci. Rev. 13, 224–233.
Sefidbakht, S., Dehghani, S., Safari, M., Vafaei, H., and Kasraeian, M. (2016). Fetal central nervous system anomalies detected by magnetic resonance imaging: a two-year experience. Iran. J. Pediatr. 26:e4589.
Shevell, M. I. (2002). Clinical and diagnostic profile of agenesis of the corpus callosum. J. Child Neurol. 17, 896–900. doi: 10.1177/08830738020170122601
Spinnler, H., and Tognoni, G. (1987). Standardizzazione e taratura Italiana di test neuropsicologici. Ital. J. Neurol. Sci. S8, 44–46.
Taylor, G. J., Bagby, R. M., and Parker, J. D. A. (1997). Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness. Cambridge: Cambridge University Press. doi: 10.1017/CBO9780511526831
Tovar-Moll, F., Moll, J., de Oliveira-Souza, R., Bramati, I., Andreiuolo, P. A., and Lent, R. (2007). Neuroplasticity in human callosal dysgenesis: a diffusion tensor imaging study. Cereb. Cortex 17, 531–541. doi: 10.1093/cercor/bhj178
Turk, A. A., Brown, W. S., Symington, M., and Paul, L. K. (2010). Social narratives in agenesis of the corpus callosum: linguistic analysis of the Thematic Apperception Test. Neuropsychologia 48, 43–50. doi: 10.1016/j.neuropsychologia.2009.08.009
Tyszka, J. M., Kennedy, D. P., Adolphs, R., and Paul, L. K. (2011). Intact bilateral resting-state networks in the absence of the corpus callosum. J. Neurosci. 31, 15154–15162. doi: 10.1523/JNEUROSCI.1453-11.2011
Wahl, M., Strominger, Z., Jeremy, R. J., Barkovich, A. J., Wakahiro, M., Sherr, E. H., et al. (2009). Variability of homotopic and heterotopic callosal connectivity in partial agenesis of the corpus callosum: a 3T diffusion tensor imaging and Q-ball tractography study. Am. J. Neuroradiol. 30, 282–289. doi: 10.3174/ajnr.A1361
Whitehead, M. T., Raju, A., and Choudhri, A. F. (2014). Normal centrolineal myelination of the callosal splenium reflects the development of the cortical origin and size of its commissural fibers. Neuroradiology 56, 333–338. doi: 10.1007/s00234-014-1323-5
Wilson, B. A., Alderman, N., Burguess, P. W., Emslie, H., and Evans, J. J. (1996). Behavioural Assessment of the Dysexecutive Syndrome. Bury St Edmunds: Thames Valley Test Company.
Keywords: MRI, splenium of the corpus callosum, emotional dysregulation, neuropsychological tests, social development
Citation: Palermo S, Andò A, Salatino A, Sirgiovanni S, De Faveri L, Carassa A, Valentini MC and Morese R (2019) Selective Emotional Dysregulation in Splenium Agenesis. A Case Report of a Patient With Normal Cognitive Profile. Front. Psychol. 10:631. doi: 10.3389/fpsyg.2019.00631
Received: 22 August 2018; Accepted: 06 March 2019;
Published: 22 March 2019.
Edited by:
Guenter Karl Schiepek, Paracelsus Medizinische Privatuniversität, Salzburg, AustriaReviewed by:
Damir del Monte, Paracelsus Medizinische Privatuniversität, Salzburg, AustriaCopyright © 2019 Palermo, Andò, Salatino, Sirgiovanni, De Faveri, Carassa, Valentini and Morese. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sara Palermo, c2FyYS5wYWxlcm1vQHVuaXRvLml0 Rosalba Morese, cm9zYWxiYS5tb3Jlc2VAdXNpLmNo
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.