 Martti T. Tuomisto
Martti T. Tuomisto Jane E. Roche
Jane E. Roche
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 19 December 2018
Sec. Psychology for Clinical Settings
Volume 9 - 2018 | https://doi.org/10.3389/fpsyg.2018.02592
Introduction: Experiences of forced migration include traumas that are interpersonal in nature, as well as ongoing emotional responses, stress, and frustration in post-migration setti ngs. Open questions exist, regarding anger/anger-like responses following experiences of persecution and ongoing stress. The aim of this study was to explore the adaptive and maladaptive underlying mechanisms of anger/anger-like responses, cultural, linguistic, and social contingencies, and possible interventions for problematic anger behavior.
Method: We searched two databases (PsycINFO and PILOTS) with the following search terms: (refugee OR “asylum seek*” OR IDP OR “internal* displac*” OR “forced migra*” OR “involuntary migra*”) AND anger.
Findings: This search yielded 34 studies that were included in the final review. Although, anger is a moral, adaptive, and prosocial response, dysfunctional anger/anger-like responses arise from PTSD, “moral injury,” complicated grief, and independent forms of anger behavior. Cultural, linguistic, and social issues also emerged from the search. Finally, considerations for treatment and intervention are discussed.
Discussion: Anger responses following experiences of forced migration may require assessment beyond PTSD models currently framed by DSM and ICD. A very promising framework is the Adaptation and Development after Persecution and Trauma (ADAPT) model.
Implications: Further longitudinal and epidemiological research will be necessary to continue testing the ADAPT model and to begin the process of assessing its cross-cultural coherence in other refugee populations (e.g., see Hinton et al., 2003). As anger behavior is also a societal issue, avenues for reconciliation, expression of grievances, employment, civic participation, and integration are needed.
Approximately 68.8 million people have been forced to escape their homes due to recent conflicts around the world (UNHCR, 2015). Exposed to life threatening situations, multiple losses (Silove, 1999; Rees and Silove, 2011), and persecution (UN General Assembly, 1951), the quality of life and mental health of refugees1 may be compromised (Silove, 1999; Silove et al., 2000; Cohen, 2008; Meyer, 2013) and further compounded by post-migratory stressors, including marginalization, acculturation problems, poverty, or stressful asylum procedures (cf. Silove, 1999; Meffert et al., 2010; Rousseau and Foxen, 2010).
A prevalent area of study for refugees is post-traumatic stress disorder (PTSD), the framework of which, in recent years, has gone through a number of changes in both the Diagnostic Statistical Manual (American Psychiatric Association, 2013) and the International Classification of Diseases (ICD; Friedman, 2013, 2014). Under the traditional fear-based trauma model, adaptive anger responses (e.g., irritability, aggressive behavior) indicate physiological reactions to aversive stimuli (i.e., arousal; Chemtob et al., 1997), but become conditioned anxiety responses to reminders of the traumatic event(s). No longer designated as an anxiety disorder, however, the DSM-5 PTSD model now accounts for higher-order verbal processes mediated by complex social behavior and contexts, in accordance with modern learning theory (Zoellner et al., 2011; Salcioglu and Başoglu, 2013; Friedman, 2014).
The ICD-11 will also identify these changes in a new category called “Complex PTSD” (Cloitre et al., 2013; Friedman, 2014). Accordingly, human-instigated trauma potentially alters the survivor's long-term social behavior and fundamental thoughts about the world and oneself (Doerr-Zegers et al., 1992). Persistent, complex anger behavior often elicits such alterations (Bryant and Nickerson, 2013; cf. Silove, 1996) and problems with managing emotional responses (Nickerson et al., 2015a).
Despite controversy and arguments that PTSD should remain an anxiety disorder (Zoellner et al., 2011), these shifts in the field represent well-intentioned efforts to adapt to transnational, albeit morally and politically charged issues, reflecting Başoglu's (2001) call for more research on the changes in emotions and thoughts that follow experiences of mass injustice. However, (Bensimon et al., 2013) argue that the new models fail to reflect the complex, inhumane, and national character of forced migration-related traumas; distinct, not only in their threat to survival, but also in their other forms of uncontrollability (cf. Seligman, 1975; Silove, 1996; Başoglu, 2001; Bryant and Nickerson, 2013). Studies on Holocaust survivors (Danieli, 1998) and American war veterans (Koffel et al., 2012) indicate anger responses may be more fundamental to such experiences. Post-migration contexts may also worsen (Brooks et al., 2011; Rees et al., 2013) or lead to the development of anger responses independent from anxious and depressive behavior (Zarowsky, 2004; Silove, 2007; Nickerson et al., 2015a).
The overarching themes emerging from our search dealt with experiences of injustice, repeated, human-instigated incidents of trauma, and subsequent anger/anger-related responses. Moral issues (Summerfield, 2003; Zarowsky, 2004), as well as protective and survival functions of anger behavior, are regarded as essential (Kanninen et al., 2003; Kim et al., 2013). Most often, research highlights anger/anger-related responses in relationship to PTSD (e.g., see Abe et al., 1994; Hinton et al., 2009; Bryant and Nickerson, 2013), often exposing shortcomings in the conventional trauma model (e.g., see Bryant and Nickerson, 2013; Nickerson et al., 2015b). Anger responses also fall under other frameworks including “moral injury” (i.e., the lifelong effects of bearing witness to acts that compromise moral principles and expectations; Litz et al., 2009) and complicated grief (Tay et al., 2015a). Anger responses independent from anxiety, moral injury, and grief are also explored (Silove et al., 2009; Brooks et al., 2011; Tay et al., 2015a). Additionally, several studies highlight the importance of validating and properly translating measurements when studying anger/anger-related responses across refugee populations (e.g., see Ekblad et al., 2002; Summerfield, 2003; Silove et al., 2009; Meffert et al., 2010; Brooks et al., 2011; Rees and Silove, 2011; Liddell et al., 2013; Tay et al., 2015b). Notwithstanding adverse emotional and social behavior (e.g., see Mandic and Mihaljevic, 1993; Başoglu et al., 2005; Hinton et al., 2009; Meffert et al., 2014), anger/anger-related responses can be prosocial when individuals are connected to their social causes (e.g., campaigning for restitution or rights; Zarowsky, 2004; Kira et al., 2009; Rees and Silove, 2011).
Our purpose was to conduct a literature review and focus specifically on anger/anger-like responses that follow experiences of forced migration. To our knowledge, this is the first review on this particular topic. The aim of this study was to explore the complexity of responses to traumatic situations in the context of forced migration, particularly, the relationship between PTSD and anger responses. A central question for this study was this: are anger responses symptoms of PTSD or are they independent? Another important question is the following: in what cases is anger independent from PTSD and why? Exploring these questions has implications for diagnosis and treatment. Deepening scientific understanding on this front will broaden and enrich responses and treatment options for the increasingly large flows of people forced to flee situations characterized by injustice.
We conducted a systematic review and studied samples of people forced to migrate within or outside the borders of their home countries due to war, conflict, persecution, marginalization, poverty, or other humanitarian disaster. These samples originate from a wide range of involuntary migrant populations, including refugees, asylum seekers,2 failed asylum seekers, IDPs,3 or those with other forms of humanitarian protection (e.g., Subsidiary Protection; Temporary Humanitarian Protection).
We used two databases (PsycINFO and PILOTS) between 1979 and 2016 with the following search terms: (refugee OR “asylum seek*” OR IDP OR “internal* displac*” OR “forced migra*” OR “involuntary migra*”) AND anger.
This search yielded 61 different articles (see Figure 1). Between September 2015 and May 2016, two independent readers facilitated the selection of papers that were in English. Papers were eligible if the study's aims included assessing anger-related phenomena or had findings or implications about anger-related phenomena. In addition, papers were eligible if participants fit the above definition(s) of forced migrants. To screen them for scientific rigor, included articles had to have an empirical basis (i.e., quantitative, qualitative, or mixed methods). However, we also included some clinical case studies to explore treatment recommendations. To screen for quality, we included only peer-reviewed articles. In the final review, 34 studies were included. Omitted studies were purely theoretical in nature, unrelated to the topic, were not peer-reviewed, or were only summaries of empirical issues.
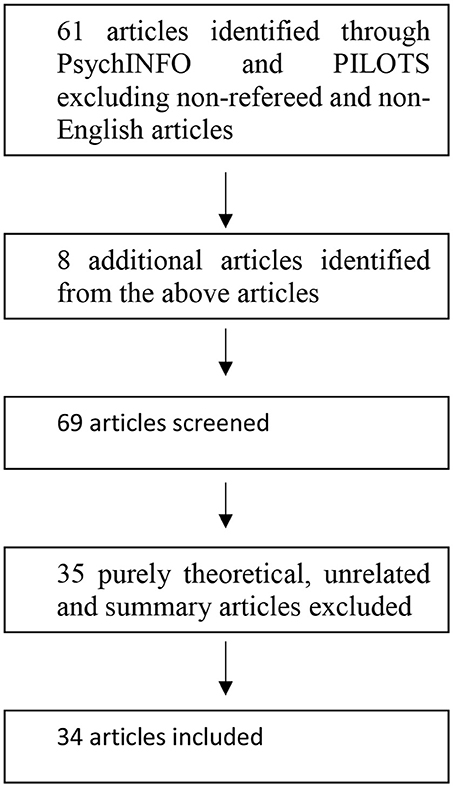
Figure 1. Flow chart of the selection of studies.
To facilitate the data extraction process, two independent researchers divided included papers into qualitative, quantitative, mixed methods, and clinical case studies. A template was used to record aims, methods, findings, and implications of each study. We compared and contrasted studies to one another and to theoretical and treatment literature. Our aim was to reduce the risk of bias of the conclusions in this way. To create a synthesis, we extracted common empirical themes as indicated in the titles of the article and questions that arose from the process. The topics covered in the review are presented in the Table 1.
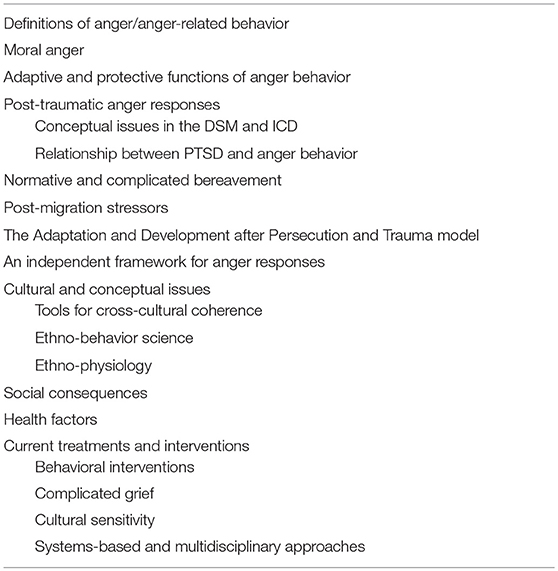
Table 1. Information covered in the systematic review: main topics and subtopics.
Although universally experienced, anger is the most contextually variable emotion, which makes it difficult to define and diagnose (Eckhardt and Deffenbacher, 1995; DiGiuseppe and Tafrate, 2007). In fact, only one anger diagnosis exists, called intermittent explosive disorder (IED; see later), and even it may not be regarded as pure anger diagnosis. Lang (1968) offers a model of three response systems (i.e., verbal, overt-motor, and physiological responses) that could be useful in understanding anger behavior. Other experts define anger as a primarily affective, but also cognitive (i.e., relating to thoughts or ideas about one's internal experience and external environment), biobehavioral, and sensory-motor (Novaco, 1986; Spielberger, 1999; DiGiuseppe and Tafrate, 2007) response to a self-reported injustice (Weiss et al., 2003), “frustration” (Berkowitz and Harmon-Jones, 2004), or threat (DiGiuseppe and Tafrate, 2007). Like other emotions, anger behavior may involve unlearned biobehavioral responses, respondent responses, or verbally mediated responses to other feelings, actions, social behavior, rules, and complex environmental factors (DiGiuseppe and Tafrate, 2007; see also Schacter and Singer, 1963; Tavris, 1989).
One recurring challenge in emotion theory arises in how to locate “anger-like” responses (e.g., hostile aggression, irritability, or paranoid behavior) along the wider spectrum of anger behavior (Berkowitz and Harmon-Jones, 2004). For example, irritability is defined as a primarily biobehavioral response that undermines an individual's ability to tolerate traumatic events and conditions threatening social networks and values (DiGiuseppe and Tafrate, 2007). Hostile behavior, which shows conceptual overlap with “trait” anger (Spielberger, 1999; Caroll, 2013), is defined as a learned, persistent tendency to respond with angry feelings, thoughts, or actions toward particular people, things, or ideas (DiGiuseppe and Tafrate, 2007; Smith et al., 2013). In addition, paranoid behavior may also lead to or include anger responses involving chronic thoughts and feelings that others are hostile to oneself (Tarrier and Taylor, 2014). However, some emotion theorists (e.g., Clore et al., 1993) contend that these anger-related behaviors do not constitute pure emotionality (i.e., unlearned or respondent behavior) because they involve operant responses. Aggressive behavior, also conceptually problematic, involves a wide range of both prosocial and antagonistic actions, from constructive verbal reproach to direct violence (Wolman, 1989). However, DiGiuseppe and Tafrate (2007) note that violence, mediated by a number of contingencies, does not necessarily result from an anger response [e.g., see “instrumental aggression” (Buss, 1971)]. A useful perspective that acknowledges the range and subtleties of adaptive and problematic anger-like behavior, but also discerns from unrelated responses (e.g., instrumental aggression), is that of social contingencies strengthening or weakening the behavior (Skinner, 1971), and the concurrent emotional or sensory responses seen as qualities of the behavior contingency. This view may also help us to address Euro-American biases (Summerfield, 2003; Zarowsky, 2004), especially amid complex, transnational contexts involving mass human rights violations (Silove, 2013).
Anger behavior has a social function (Tavris, 1989; DiGiuseppe and Tafrate, 2007); therefore, it is best explored among refugees from both psychiatric and value-based perspectives (e.g., see Summerfield, 2003; Zarowsky, 2004; Meffert et al., 2010; Rousseau and Foxen, 2010). For instance, studies highlight a justifiable tendency among participants to fixate on perpetrators of persecutory experiences that occurred before flight (for example, see Abe et al., 1994; Rees and Silove, 2011; Bryant and Nickerson, 2013). In the post-migration context, anger responses (i.e., high “trait anger”) among Sudanese refugees with PTSD (n = 22) were significantly correlated with reasonable and understandable feelings of injustice and betrayal due to illegal and abusive treatment by an institution in Egypt that is intended to help refugees (Meffert et al., 2010).
Ideally, anger responses also help individuals survive danger and cope with adverse conditions (Tavris, 1989; DiGiuseppe and Tafrate, 2007). For instance, Kim et al. (2013) determined in a sample of North Korean refugee women (n = 2,163) that those exhibiting paranoid and hostile behavior had been exposed to the severest and highest number of forced migration-related traumatic events. As causal inferences cannot be inferred from the study, it is unclear if these social behaviors were acquired as a result of these events or if they had been formed during their earlier life, possibly preparing the women for later incidents of trauma-related problems. Other evidence indicates that social anger behavior may function as avoidance behavior to protect against the development of PTSD-type responses (cf. Kanninen et al., 2003). For example, participants in a sample of Palestinian torture survivors and refugees (n = 176), who exhibited anger-related “character traits” acquired during abusive childhoods, were least likely to develop certain post-traumatic stress responses (Kanninen et al., 2003). This supports the view that anger-related contingencies are biologically more important than anxiety related contingencies in general.
Başoglu (2001) theorizes that the “sense of injustice” that develops because of war- and conflict-related experiences potentially leads to adverse, long-term changes in thoughts and emotions about the world. The need to index this “sense of injustice” first became clear in a study on Southeast Asian refugees (n = 308) by Abe et al. (1994), who found that anger responses (i.e., anger toward the perpetrator) were what most significantly distinguished participants without PTSD from participants with it. It was deemed necessary to add an Anger Reaction Index to the research design of the study because the DSM-IV model of PTSD failed to account for appropriate anger-associated criteria, including those with a clear verbal basis. This shortcoming may have reflected conceptual bias in the earlier fear-based PTSD model (cf. Van de Vijver and Tanzer, 2004).
Other studies also reveal conceptual problems in DSM-IV (e.g., see Momartin et al., 2002; Hinton et al., 2003; Momartin and Coello, 2006; Charney and Keane, 2007; Bryant and Nickerson, 2013; Draijer and Van Zon, 2013). For instance, Momartin et al. (2002) explored trauma experiences among 126 Bosnian refugees resettled in Australia and discovered that anger responses (i.e., feelings of betrayal, distrust, and frustration) emerged from autobiographical accounts. They claimed that such conceptual issues are too abstract to be identified by DSM-IV criteria.
Shortcomings have also been observed with regard to the ICD-10 (Momartin and Coello, 2006; Bryant and Nickerson, 2013). For instance, a clinical case study of an Iraqi torture survivor revealed that the fear-based PTSD model was able to account for the client's anger-related arousal responses, but failed to encompass his persistent, negative thoughts and feelings and his tendency to fixate on past injustices (Bryant and Nickerson, 2013). Bryant and Nickerson (2013) determined that these thoughts and tendencies were not anxiety responses, but could be understood as anger-related changes in the client's long-term social behavior following ongoing exposure to mistreatment and betrayal in Iraq. Correspondingly, Momartin and Coello (2006) proposed in their clinical case study that their client's anger responses were not only dysfunctional, biobehavioral reactions. Rather, chronic anger behavior resulted from long-lasting changes in social behavior following experiences of torture. Accordingly, clients in both of these case studies were diagnosed with “Complex PTSD” (Momartin and Coello, 2006; Bryant and Nickerson, 2013).
The DSM 5 has also made changes that seemingly encompass trauma to a more complete extent (American Psychiatric Association, 2013; cf. Friedman, 2013; cf. 2014), adapting Criterion D to account for changes in social behavior and feelings and thoughts about the world (Friedman et al., 2011; Friedman, 2013, 2014; Levin et al., 2014). However, Nickerson et al. (2015b) suggest that these changes result from moral injury, a concept that is more extensive than what the DSM 5 model of PTSD offers. They found that it explained 10% of the variance in anger behavior in a clinical sample (n = 134) of resettled refugees and asylum seekers in Switzerland, thereby suggesting that it partially accounts for the presence of anger responses.
Studies also diverge with regard to the precise relationship between PTSD and anger behavior. For instance, Hinton's (2003) research on Cambodian refugees exhibited that anger responses acted as antecedents for triggering trauma memories among participants (in this case, slavery during the Khmer Rouge Regime). They hypothesized that participants remembered this particular trauma because of socially mediated, classically (respondently) conditioned, and biobehavioral anger behavior.
Other researchers posit that anger responses are avoidance behaviors (Charney and Keane, 2007; Draijer and Van Zon, 2013). For instance, Draijer and Van Zon (2013) proposed in their clinical case study that anger responses are forms of escape behavior that may lead to dissociation, when their client, a former Sierra Leonean child soldier resettled in the Netherlands, exhibited aggressive behavior as a means to avoid stimuli eliciting feelings of shame. Similarly, Charney and Keane's (2007) study revealed that anger responses among a sample of Bosnian refugees (n = 115) were associated with both arousal and avoidance behavior.
The process of bereavement commonly involves anger behavior (Kübler-Ross, 1969). However, prolonged grief may involve ruminative behavior (Morina, 2011). Some researchers suggest that the inhumane nature of forced migration-related losses disrupts the grieving process (Tay et al., 2015a). For instance, in evaluating the cross-cultural adequacy of DSM 5 and forthcoming ICD complicated grief models among West Papuan refugees (n = 230) in Papua New Guinea, a survey-based study revealed that complicated grief diverged from western models, being predicted by anger behavior arising from a chronic “sense of injustice” (Tay et al., 2015a). Similar findings emerged in Pirta's (2014) study on IDPs of Bhakra Dam in India, who were still grieving the loss of their homes from 50 years earlier. The authors proposed that anger responses elicited memories of home and prolonged bereavement.
In addition to experiences of persecution, refugees are frequently exposed to disempowering, unjust post-migration settings (Westermeyer and Uecker, 1997; Sedighdeilami, 2004; Silove et al., 2009; Meffert et al., 2010; Brooks et al., 2011). Accordingly, the relationship between post-migration conditions and maladaptive anger/anger-related responses has been explored (Lin et al., 1979; Silove, 1996; Westermeyer and Uecker, 1997; Ekblad et al., 2002; Sedighdeilami, 2004; Silove et al., 2009; Meffert et al., 2010; Brooks et al., 2011; Bryant and Nickerson, 2013). An earlier study on Vietnamese refugees (n = 293) in the USA, for example, signified that post-migration problems were associated with an increase in anger responses among participants (Lin et al., 1979). Additionally, the above investigation on Sudanese refugees revealed a significant correlation between high “trait anger” and experiences of institutional discrimination in the Egyptian asylum system (Meffert et al., 2010). Similarly, the above case study on the Iraqi torture survivor revealed that his problematic anger responses derived from his fixation on ongoing stressors, in addition to past trauma (Bryant and Nickerson, 2013).
Other studies implicate societal ostracism as a potential source of problematic anger responses (Ekblad et al., 2002; Sedighdeilami, 2004). For example, a 10 years longitudinal study on the psychological impact of pre- and post-migration variables on Hmong refugees (n = 102) in the USA revealed that hostile responses were predicted by stimuli eliciting feelings of alienation as a motivational variable, especially during the 1st year of resettlement (Westermeyer and Uecker, 1997). Likewise, Ekblad et al. (2002) proposed that hostile behavior in the above Kosovan sample (n = 131) arose not only from experiences of torture, but also from the decade of marginalization the community had endured after flight. Similarly, self-reported discrimination was associated with anger behavior among 205 Iranian refugees resettled in Canada (Sedighdeilami, 2004).
Several authors hypothesize that the combined effect of pre-migration trauma and post-migration socio-economic variables mediates the behavioral pathway to anger behavior among forced migrants (Silove et al., 2009; Brooks et al., 2011; Nickerson et al., 2015a). In exploring this particular relationship, Silove et al. (2009) tested the Adaptation and Development after Persecution and Trauma (ADAPT) model on an epidemiological sample of Timorese participants (n = 1,247), a community affected by mass displacement due to past Indonesian occupation, determining that over one quarter of those exhibiting problematic anger responses was a group of men unable to find employment. They later established that the relationship between human-instigated trauma and anger responses was mediated by ongoing hardship (e.g., unemployment, poor education, discrimination) in the post-conflict context (Brooks et al., 2011). The ADAPT model has also been refined by recent cross-sectional research demonstrating that problems with managing emotional behavior accounts for these composite effects (Nickerson et al., 2015a).
Both concurrent and independent anger responses have been explored (e.g., see Westermeyer and Uecker, 1997; Silove et al., 2009; Meffert et al., 2010; Brooks et al., 2011). For example, the above study on Hmong refugees revealed that chronic hostile behavior was significantly correlated with depression symptoms that developed during early stages of resettlement (Westermeyer and Uecker, 1997). However, according to other evidence, anger behaviors are independent responses (Silove et al., 2009; Brooks et al., 2011). For instance, the above studies on Timorese IDPs found that approximately 40% of the community met criteria for problematic anger behavior (Silove et al., 2009; Brooks et al., 2011). However, <10% of those exhibiting problematic anger behaviors had PTSD, while ~5% showed symptoms for anxiety and depression, thereby reinforcing the hypothesis that anger responses require independent frameworks for investigation.
Although Silove et al. (2009) hypothesized that anger behavior in the Timorese community persisted after other post-traumatic stress responses had subsided; they determined that the combined effect of injustice and later socioeconomic stressors caused anger behavior to develop independently. A similar issue arose in the above study on Sudanese refugees (Meffert et al., 2010). Although Meffert et al. theorized that anger was a response to experiences of pre-flight trauma they inferred an insignificant correlation. Instead, they concluded that the unjust actions of the UNHCR were more strongly associated with high “trait” anger behavior. Momartin and Coello (2006) also proposed in the above case study that, because the client had suppressed anger responses for fear of punishment during imprisonment, covert anger behavior developed independently.
Research designs inappropriate for refugee populations may produce bias (e.g., response, item, and conceptual bias; cf. Van de Vijver and Tanzer, 2004). Assessments such as the State-Trait Anger Expression Inventory (STAXI) have been validated in few refugee populations. To develop appropriate and precise psychometric measures and to increase cultural competency and awareness of social variables that may influence how respondents evaluate others' actions and the world around them (cf. Betancourt et al., 2003, and Hinton et al., 2012), various studies have utilized “bottom up” methods such as community consultation (e.g., see Westermeyer and Uecker, 1997; Silove et al., 2009; Meffert et al., 2010; Brooks et al., 2011; Rees and Silove, 2011).
The “back translation” method is another common tool used for developing proper measures across populations (Heine, 2012). Meffert et al. (2010) used this method, as well as Westermeyer and Uecker (1997) in a study on hostile responses among Hmong refugees. While useful, back translation does not improve conceptual frameworks in measurement tools, as nuances in ethno-behavioral descriptions of anger and trauma (e.g., individualistic and collectivist perspectives) are sometimes overlooked (cf. Hinton et al., 2003, 2009; Horton, 2006). The need for sensitivity to these models has been highlighted in studies on Bosnian and Kosovoan refugees (Ekblad et al., 2002; Summerfield, 2003; cf. Van de Vijver and Tanzer, 2004). In Summerfield's client's local language, for example, the only phrase that equates to “trauma” is “spiritual bruise,” which is a “…much wider and more holistic concept of injury than a scientifically framed one” (Summerfield, 2003). Furthermore, anger behavior among Kosovoan refugees in Sweden (n = 131) was correlated with difficulty in managing and comprehending verbal, emotional, and existential responses to experiences of torture (Ekblad et al., 2002; c.f. Antonovsky, 2013, cited in p. 32). However, Ekblad, Prochazka and Roth conceded that self-report measurements were too individualized and were, therefore, inappropriate for this particular sample.
Other researchers have aimed to explore the cross-cultural applicability of diagnostic models, such as the IED, a DSM disorder revolving around impulse control (Rees and Silove, 2011; Liddell et al., 2013). On the one hand, a clinical concordance study on a sample of Timorese IDPs (n = 85) showed high convergence (AUC index = 0.90) between both community-based and DSM-IV definitions of IED (Liddell et al., 2013). On the other hand, a qualitative study on West Papuan refugees (n = 41) uncovered a local idiom, “Sakit Hati,” which involves a chronic tendency to fixate on experiences of persecution, specifically, by the Indonesian army, frequently resulting in “explosive” anger responses (Rees and Silove, 2011). Though very similar to IED, the authors concluded that “Sakit Hati” emerges as a primarily affective anger behavior.
Researchers should also be aware of ethno-behavioral perspectives on anger because they may influence how individuals report on, evaluate, or cope with it. For example, in Horton's (2006) qualitative study, a sample of Tibetan refugees (n = 109) disapproved of anger behavior, reporting on shorter and less intense anger episodes than a sample of Americans (n = 41). Likewise, Raney (2008), in a qualitative study on Tibetan refugee women (n = 12) in New York City, asked how participants felt about being forced to flee Tibet and having to resettle. Women narrated experiences of loss, terror, and isolation, but did not report feelings of anger.
Similar findings emerged from qualitative interviews with Buddhist monks (n = 6) from whom members of a USA-based Cambodian refugee community sought advice (Nickerson and Hinton, 2011). Reportedly, one third of this sample discouraged ruminating or feeling angry about injustices that had taken place under the Khmer Rouge Regime because doing so, according to Khmer belief, causes an upsurge of steam in the body resulting in cardiac arrest, also known as a “khyal attack” (Herbst, 1992; Hinton et al., 2003, 2009). Correspondingly, Hinton et al. (2009) found that 70% of a clinical sample (n = 68) of Khmer refugees resettled in the USA believed their anger would lead to such an attack.
Lack of social acceptance for anger behavior in both Tibetan and Khmer cultures may have led to response bias in the above studies. However, an “ethno-physiological” account of the above Khmer refugee community led Hinton et al. (2003, 2009) to hypothesize that that the Khmer fear of anger sets off a process of interoceptive conditioning. For this particular group, Hinton et al. (2003) proposed a cyclical mechanism for anger-triggered panic attacks, in which culturally-based verbal fears of biobehavioral anger responses will reinforce fear responses further. This hypothesis was supported by an earlier study on another clinical sample (n = 100), more than half of which condemned and avoided biobehavioral anger responses and, as a result, suffered panic attacks (Hinton et al., 2003). To further test this relationship, analysis of data from a somewhat larger sample (n = 143) revealed that anger-associated catastrophic cognitions explained high PTSD variance (54%). Clearly, cultural rules influence how individuals interpret biobehavioral anger responses, which then determines the course of subsequent responses. Again, such findings point to the importance of cultural sensitivity in research (cf. Betancourt et al., 2003, and Hinton et al., 2012).
While theories linking dysfunctional anger behavior among forced migrants and conflict on the meso and macro-level exist (e.g., see “etiology of terrorism;” Victoroff, 2005; Rice, 2009; Victoroff et al., 2012), our search uncovered correlations in the private sphere (c.f. Silove, 1999; Momartin and Coello, 2006; Hinton et al., 2009; Isakson and Layne, 2009; Silove et al., 2009; Brooks et al., 2011; Nickerson and Hinton, 2011; Bryant and Nickerson, 2013; Meffert et al., 2014). For example, maladaptive anger responses potentially contribute to self-injurious behavior among torture survivors (Momartin and Coello, 2006; Bryant and Nickerson, 2013), as well as family conflict, especially when acculturation gaps occur between generations (Hinton et al., 2009; Isakson and Layne, 2009; Nickerson and Hinton, 2011).
According to Silove et al. (2009), these negative social consequences may worsen especially when refugees have little means to improve their circumstances or advocate for social justice. Correspondingly, Meffert et al. (2014) theorize that PTSD-linked anger responses increase interpersonal conflict amongst populations living in broken, disempowered communities. Interestingly, problematic anger responses have decreased, in cases where individuals felt empowered through social support or were committed to and involved in their social causes (e.g., campaigns for restitution, migrant rights; Kira et al., 2009; Rees and Silove, 2011; cf. Zarowsky, 2004).
Despite prosocial benefits, the biobehavioral aspect of anger responses is a risk factor for health, especially cardiovascular health (Tuomisto et al., 2005; Smith et al., 2013). In the refugee context, a study on Iraqi refugees (n = 501) resettled in the USA revealed that anger (i.e., refusal to forgive Saddam Hussein's collaborators) predicted hypertension, as well as digestive and respiratory problems (Kira et al., 2009). In the same sample, however, anger (i.e., refusal to forgive Saddam Hussein himself) predicted a significant decrease in circulatory disorders. Kira et al. (2009) posited that shared, righteous anger gave the participants a sense of control, belonging, and validation, suggesting that health effects of anger behavior seem to be dependent on social contingencies (i.e., if the behavior is negatively vs. positively reinforced). These results point to the importance of psychosocial support for treatment and intervention.
It appears that Cognitive-Behavior Therapy (CBT) is the most evidence-based intervention for problematic anger responses that arise from experiences of forced migration (Hinton et al., 2012; Nickerson et al., 2015b). However, hardly any evidence exists as to which form of CBT is the most appropriate for individuals with refugee backgrounds (R. Bryant, personal communication, October 3, 2013). On the one hand, exposure treatment, especially live exposure, is proven most effective for clients who suffer from PTSD (Paunovic and Öst, 2001; Mineka and Zinbarg, 2006). An additional benefit is that exposure therapy is simplest for paraprofessionals to learn and is most easily disseminated across mass groups of people. On the other hand, clients often resist the regimen required for success (Sharp et al., 2004; Hinton et al., 2012), which may account for the 50% failure rate (Salcioglu and Başoglu, 2013).
Although past research on war veterans suggests that high levels of anger behavior inhibit successful exposure-based treatment outcomes for PTSD (Forbes et al., 2008), Stenmark et al. (2014) found that it did not affect outcomes among a clinical sample of refugees (n = 54). Nevertheless, Hinton et al. (2012) recommend that stretching and mindfulness exercises follow sessions, so that the client learns to associate positive sensations with anger responses, instead of unpleasant ones. According to Momartin and Coello (2006), torture survivors especially benefit from supplementary exercises like these.
Although exposure therapy is proven successful in treating prolonged bereavement, its efficacy in treating complicated bereavement may actually rely upon verbal processes, unlike treatment for PTSD, which teaches clients to regulate and tolerate anger responses (R. Bryant, personal communication, October 3, 2013). Therefore, therapists should explore alternative instructional interventions, as clients tend to resist exposure. Although further research is needed, instructional interventions may teach clients to re-evaluate anger responses and learn new ones, thus preventing rumination.
No matter which form or combination of CBT is used, it is important for behavior therapists to increase cultural sensitivity and awareness of how cultural backgrounds influence anger responses (Hinton et al., 2012). For example, Nickerson and Hinton (2011) recommend that Acceptance and Commitment Therapy (ACT) be used in combination with techniques tailored to the individual's unique needs and cultural values.
Salcioglu and Başoglu (2013) advise against the use of multidisciplinary programs for treating PTSD. Although, Meffert et al. (2014) reported that Interpersonal Psychotherapy reduced post-traumatic anger responses in a randomized pilot study on Sudanese refugees (n = 22) in Cairo, the small sample size made it difficult to assess the significance of the study, thereby signifying the need for further research.
Nevertheless, the reviewed studies establish that problematic anger responses are also compounded by post-migration factors (see for example, Brooks et al., 2011; Nickerson et al., 2015b). Therefore, it may be necessary to address interpersonal dynamics of anger behavior, which are impacted by social and economic variables in post-migration contexts (cf. Rees et al., 2013). For instance, Hinton et al. (2009) recommend that education on post-traumatic stress responses and promotion of “cultural esteem” involve the whole family. Furthermore, policies and community-based programs promoting integration and civic participation are necessary to alleviate maladaptive anger responses and promote prosocial behavior (Rees et al., 2013).
Overall, experiences involving persecution, nationwide trauma, and multiple losses may lead to complex anger responses, further compounded by hostile post-migration environments (e.g., see Westermeyer and Uecker, 1997; Silove et al., 2009; Meffert et al., 2010; Brooks et al., 2011; Nickerson et al., 2015b). Therefore, diagnostic intervention should transcend conventionally framed PTSD models (cf. Silove, 1999, 2013) and, furthermore, focus on affect, rather than impulse control (cf. Rees and Silove, 2011).
Salcioglu and Başoglu (2013) recommend control-focused behavior therapy (C-FBT), instead of traditional exposure treatment, because it teaches clients to accept, rather than reduce, anger responses, and to acquire a “sense of control” over these responses. Accordingly, both C-FBT and traditional exposure treatment should involve training that increases the client's ability to adjust anger behavior in response to unpredictable circumstances (Bryant, personal communication, October 3, 2013; cf. Hinton et al., 2012).
Although Salcioglu and Başoglu (2013) claim that C-FBT has been validated across many samples of asylum seekers and refugees, a meta-analysis by Fuchs et al. (2013) maintains that ACT is the preferred method of intervention among clients originating from minority and marginalized backgrounds because of its humanistic, value-aware, and collaborative approach. Therefore, ACT not only draws upon the benefits of exposure therapy, but also provides a platform for clients to explore culturally-contingent thoughts and ideas without judgment (Eifert et al., 2006; Fuchs et al., 2013). Further research is needed to assess the validity of ACT across more refugee populations (Fuchs et al., 2013; see also Gardner and Moore (2013) on Contextual Anger Regulation Therapy).
Behavior analytic research involving multiple baseline designs (MBDs) will be especially useful for assessing the efficacy of interventions such as C-FBT and ACT (cf. Hawkins et al., 2007 and Hinton et al., 2003). As demonstrated in Hinton's (2003) study, MBDs are not only statistically reliable; they are also more practical and cost-effective than randomized controlled trials because they can be drawn from fewer sample sizes, making them ideal for epidemiological research (Hawkins et al., 2007).
Certainly, maladaptive and adaptive anger responses are not “mutually exclusive” (cf. Silove, 2013), because they are contextually determined. Problematically, DSM and ICD constructs may be too rigid to account for the range of anger responses that follow experiences of forced migration, which lie on a spectrum of normal and problematic behavior (cf. Silove, 1999, 2013). Alternatively, the ADAPT model allows researchers and practitioners to explore anger responses as contingent upon complex, constantly changing environmental variables.
This review's major strength lie in its novelty, scope, in-depth analysis, and detailed recommendations for future research. The review is also very timely as forced migration is ever increasing (e.g., because of population growth, climate change and following conflicts). This review, however, is limited in its reliance on relatively few studies to choose from overall. More research is needed to explore this topic, but a large quantitative review is not yet adequate because of limited research in the area.
Further epidemiological, cross-sectional, and longitudinal research, as well as “bottom-up” and single-case research designs, will be necessary to continue testing the ADAPT model and to begin the process of assessing its cross-cultural coherence in other refugee populations (e.g., see Hinton et al., 2003). Furthermore, Rees et al. (2013) recommend mixed methodology for exploring the social precipitants, contingencies, consequences of, and causal pathways between prosocial and problematic anger responses (cf. Brooks et al., 2011; cf. Kira et al., 2009; cf. Rees and Silove, 2011; cf. Zarowsky, 2004). As anger behavior is also a societal issue, avenues for reconciliation, expression of grievances, employment, civic participation, and integration are needed.
MT planned the study, analyzed the data, and wrote a part of the manuscript. JR planned the study, collected the data, analyzed the data, and wrote a part of the manuscript.
The study was funded by the University of Tampere.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Part of the article was previously published in a Master's thesis (Roche, 2016).
1. ^As defined by the United Nations (UN), a refugee is “[a] person who owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of his nationality and is unable or…unwilling to return to it” (UN General Assembly, 1951). For the purposes of this article, however, the authors herein use the term ‘refugee’ as an inclusive descriptor for all individuals with forced migration backgrounds (e.g., asylum seekers, Internally Displaced Persons (IDPS), those with Temporary Humanitarian Protection, Stateless Persons), unless stated otherwise.
2. ^As defined by UNHCR (2011), the UN Refugee Agency, “an asylum seeker is an individual who is seeking international protection [and] whose claim has not yet been finally decided on by the country in which he or she has submitted it.”
3. ^As defined by UNHCR, IDPs are persons within the borders of their own countries who have been forced to flee their homes to escape conflict, war, human rights violations, or humanitarian disasters.
Abe, J., Zane, N., and Chun, K. M. (1994). Differential responses to trauma: Migration-related discriminants of post-traumatic stress disorder among Southeast Asian refugees. J. Commun. Psychol. 22, 121–135.
American Psychiatric Association (2013). Diagnostic and Statistical Manual Of Mental Disorders: DSM 5. Washington, DC: American Psychiatric Association. doi: 10.1176/appi.books.9780890425596
Antonovsky, A. (2013). The structure and properties of the Sense of Coherence Scale. Soc. Sci. Med. 36, 725–733. doi: 10.1016/0277-9536(93)90033-Z
Başoglu, M. (2001). “Psychology of torture and its consequences”,” in International Encyclopedia of the Social and Behavioral Sciences, eds N. Smelser and P. Bates (Amsterdam: Elsevier), 15779–15783.
Başoglu, M., Livanou, M., Crnobarić, C., Frančišković, T., Suljić, E., Durić, D., et al. (2005). Psychiatric and cognitive effects of war in former Yugoslavia: association of lack of redress for trauma and posttraumatic stress reactions. JAMA 294, 580–590. doi: 10.1001/jama.294.5.580
Bensimon, M., Solomon, Z., and Horesh, D. (2013). The utility of Criterion A under chronic national terror. Isr. J. Psychiatry Relat. Sci. 50, 81–83.
Berkowitz, L., and Harmon-Jones, E. (2004). Toward an understanding of the determinants of anger. Emotion 4, 107–130. doi: 10.1037/1528-3542.4.2.107
Betancourt, J. R., Green, A. R., Carrillo, J. E., and Ananeh-Firempong, O. (2003). Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 118, 293–302. doi: 10.1016/S0033-3549(04)50253-4
Brooks, R., Silove, D., Steel, Z., Steel, C. B., and Rees, S. (2011). Explosive anger in postconflict Timor Leste: interaction of socio-economic disadvantage and past human rights-related trauma. J. Affect. Disord. 131, 268–276. doi: 10.1016/j.jad.2010.12.020
Bryant, R. A., and Nickerson, A. (2013). “Treatment of complex PTSD: the case of a torture survivor.” in Case Studies in Clinical Psychological Science: Bridging the Gap From Science to Practice, eds W. O'Donohue and S. O. Lilienfeld (Oxford: Oxford University Press), 167–197.
Buss, A. H. (1971). “Aggression pays,” in The Control of Aggression and Violence: Cognitive and Physiological Factors, ed J. L. Singer (New York, NY: Academic Press), 7–18.
Caroll, J. (2013). “Trait anger,” in Encyclopedia of Behavioral Medicine, eds M. D. Gellman and J. R. Turner (New York, NY: Springer), 1987–1989.
Charney, M. E., and Keane, T. M. (2007). Psychometric analyses of the Clinician-Administered PTSD Scale (CAPS) - Bosnian translation. Cult. Divers. Ethnic Minor. Psychol. 13:161–168. doi: 10.1037/1099-9809.13.2.161
Chemtob, C. M., Novaco, R. W., Hamada, R. S., Gross, D. M., and Smith, G. (1997). Anger regulation deficits in combat-related posttraumatic stress disorder. J. Trauma. Stress. 10, 17–35. doi: 10.1002/jts.2490100104
Cloitre, M., Garvert, D. W., Brewin, C. R., Bryant, R. A., and Maercker, A. (2013). Evidence for proposed ICD 11 PTSD and complex PTSD: a latent profile analysis. Eur. J. Psychotraumatol. 4, 1–12. doi: 10.3402/ejpt.v4i0.20706
Clore, G. L., Ortony, A., Dienes, B., and Fujita, F. (1993). “Where does anger dwell?,” in Perspectives on Anger and Emotion: Advances in Social Cognition, eds R. S. Wyer Jr and T. K. Srull (Hillsdale, NJ: Erlbaum), 57–87.
Cohen, J. (2008). Safe in our hands? A study of suicide and self-harm in asylum seekers. J. Forensic Leg. Med. 14, 235–244. doi: 10.1016/j.jflm.2007.11.001
Danieli, Y. (1998). International Handbook of Multigenerational Legacies of Trauma. New York, NY: Plenum Press. doi: 10.1007/978-1-4757-5567-1
DiGiuseppe, R., and Tafrate, R. C. (2007). Understanding Anger Disorders. Oxford: Oxford University Press.
Doerr-Zegers, O., Hartmann, L., Lira, E., and Weinstein, E. (1992). Torture: psychiatric sequelae and phenomenology. Psychiatry 55, 177–184. doi: 10.1080/00332747.1992.11024591
Draijer, N., and Van Zon, P. (2013). Transference-focused psychotherapy with former child soldiers: Meeting the murderous self. J. Trauma Dissoc. 14, 170–183. doi: 10.1080/15299732.2013.724339
Eckhardt, C. I., and Deffenbacher, J. L. (1995). “Diagnosis of anger disorders,” in Anger Disorders: Definition, Diagnosis, and Treatment, ed H. Kassinove (Oxford: Taylor and Francis), 35–44.
Eifert, G. H., Forsyth, J. P., and McKay, M. (2006). Act on Life Not on Anger: The New Acceptance and Commitment Therapy Guide to Problem Anger. Oakland, CA: New Harbinger Publications.
Ekblad, S., Prochazka, H., and Roth, G. (2002). Psychological impact of torture: a 3-month follow-up of mass-evacuated Kosovan adults in Sweden, lessons learnt for prevention. Acta Psychiatr. Scand. 106, 30–36. doi: 10.1034/j.1600-0447.106.s412.7.x
Forbes, D., Parslow, R., Creamer, M., Allen, N., McHugh, T., and Hopwood, M. (2008). Mechanisms of anger and treatment outcome in combat veterans with posttraumatic stress disorder. J. Trauma. Stress 21, 142–149. doi: 10.1002/jts.20315
Friedman, M. J. (2013). Finalizing PTSD in DSM-5: getting here from there and where to go next. J. Trauma. Stress 26, 548–556. doi: 10.1002/jts.21840
Friedman, M. J., Resick, P. A., Bryant, R. A., and Brewin, C. R. (2011). Considering PTSD for DSM-5. Depress. Anxiety 28, 750–769. doi: 10.1002/da.20767
Fuchs, C., Lee, J. K., Roemer, L., and Orsillo, S. M. (2013). Using mindfulness- and acceptance-based treatments with clients from nondominant cultural and/or marginalized backgrounds: clinical considerations, meta-analysis findings, and introduction to the special series. Cogn. Behav. Pract. 20, 1–12. doi: 10.1016/j.cbpra.2011.12.004
Gardner, F. L., and Moore, Z. E. (2013). Contextual Anger Regulation Therapy for the Treatment of Clinical Anger: A Mindfulness and Acceptance-Based Behavioral Approach. Abingdon: Routledge. doi: 10.4324/9780203864913
Hawkins, N. G., Sanson-Fisher, R. W., Shakeshaft, A., D'Este, C., and Green, L. W. (2007). The multiple baseline design for evaluating population-based research. Am. J. Prev. Med. 33, 162–168. doi: 10.1016/j.amepre.2007.03.020
Herbst, P. R. (1992). From helpless victim to empowered survivor: Oral history as a treatment for survivors of torture. Women Ther. 13, 141–154. doi: 10.1300/J015V13N01_13
Hinton, D. E., Hsia, C., Um, K., and Otto, M. W. (2003). Anger-associated panic attacks in Cambodian refugees with PTSD: A multiple baseline examination of clinical data. Behav. Res. Ther. 41, 647–654. doi: 10.1016/S0005-7967(02)00035-9
Hinton, D. E., Rasmussen, A., Nou, L., Pollack, M. H., and Good, M. (2009). Anger, PTSD, and the nuclear family: a study of Cambodian refugees. Soc. Sci. Med. 69, 1387–1394. doi: 10.1016/j.socscimed.2009.08.018
Hinton, D. E., Rivera, E. I., Hofmann, S. G., Barlow, D. H., and Otto, M. W. (2012). Adapting CBT for traumatized refugees and ethnic minority patients: examples from culturally adapted CBT (CA-CBT). Transcult. Psychiatry 49, 340–365. doi: 10.1177/1363461512441595
Horton, R. A. (2006). Refining Theory and Practice in the Cultural Psychology of Emotion: Tibetan “Anger” and the Roots of the Modern Tibetan Commitment to Non-Violence (India, United States). Dissertation Abstracts International, 67(5-B), 2876.
Isakson, B. L., and Layne, C. M. (2009). “The legacy of war: irritability and anger in an adolescent refugee,” inDSM-IV-TR Casebook and Treatment Guide for Child Mental Health, eds C. A. Galanter and P.A. Jensen (Arlington, VA: American Psychiatric Publishing), 483–500.
Kanninen, K., Punamäki, R., and Qouta, S. (2003). Personality and trauma: adult attachment and posttraumatic distress among former political prisoners. Peace Conflict J. Peace Psychol. 9, 97–126. doi: 10.1207/S15327949PAC0902_01
Kim, S. H., Kim, H. K., and Lee, N. (2013). Psychological features of North Korean female refugees on the MMPI−2: Latent profile analysis. Psychol. Assess. 25, 1091–1102. doi: 10.1037/a0033097
Kira, I. A., Lewandowski, L. A., Templin, T. N., Ramaswamy, V., Ozkan, B., and Mohanesh, J. (2009). The effects of post-retribution inter-group forgiveness: the case of Iraqi refugees. Peace Conflict J. Peace Psychol. 15, 385–413. doi: 10.1080/10781910903158669
Koffel, E., Polusny, M. A., Arbisi, P. A., and Erbes, C. R. (2012). A preliminary investigation of the new and revised symptoms of posttraumatic stress disorder in DSM 5. Depress. Anxiety 29, 731–738. doi: 10.1002/da.21965
Lang, P. J. (1968). “Fear reduction and fear behavior: problems in treating a construct,” in Research in Psychotherapy, ed J. M. Shlien (Washington, DC: American Psychological Association), 90–103.
Levin, A. P., Kleinman, S. B., and Adler, J. S. (2014). DSM 5 and posttraumatic stress disorder. J. Am. Acad. Psychiatry Law Online 42, 146–158.
Liddell, B. J., Silove, D., Tay, K., Tam, N., Nickerson, A., Brooks, R., et al. (2013). Achieving convergence between a community-based measure of explosive anger and a clinical interview for Intermittent explosive disorder in Timor-Leste. J. Affect. Disord. 150, 1242–1246. doi: 10.1016/j.jad.2013.06.006
Lin, K. M., Tazuma, L., and Masuda, M. (1979). Adaptational problems of Vietnamese refugees: I. Health and mental health status. Arch. Gen. Psychiatry 36, 955–961. doi: 10.1001/archpsyc.1979.01780090041005
Litz, B. T., Stein, N., Delaney, E., Lebowitz, L., Nash, W. P., Silva, C., et al. (2009). Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin. Psychol. Rev. 29, 695–706. doi: 10.1016/j.cpr.2009.07.003
Mandic, N., and Mihaljevic, Z. V. (1993). Psychological state of displaced persons from East Slavonia. Soc. Psihijatr. 21, 121–135.
Meffert, S. M., Abdo, A. O., Abd Alla, O. A., Elmakki, Y. O. M., Omer, A. A., Yousif, S., et al. (2014). A pilot randomized controlled trial of interpersonal psychotherapy for Sudanese refugees in Cairo, Egypt. Psychol. Trauma Theory Res. Pract. Policy 6, 240–249. doi: 10.1037/a0023540
Meffert, S. M., Musalo, K., Abdo, A. O., Abd Alla, O. A., Elmakki, Y. O. M., Omer, A. A., et al. (2010). Feelings of betrayal by the United Nations High Commissioner for Refugees and emotionally distressed Sudanese refugees in Cairo. Med. Conflict Surv. 26, 160–172. doi: 10.1080/13623699.2010.491395
Meyer, S. M. (2013). UNHCR's Mental Health and Psychosocial Support for Persons of Concern: Global Review. Geneva: United Nations High Commissioner for Refugees Policy Development and Evaluation Service. Available online at: http://www.unhcr.org/51bec3359.pdf
Mineka, S., and Zinbarg, R. (2006). A contemporary learning theory perspective on the etiology of anxiety disorders: it's not what you thought it was. Am. Psychol. 61, 10–26. doi: 10.1037/0003-066X.61.1.10
Momartin, S., and Coello, M. J. (2006). Self-harming behaviour and dissociation in complex PTSD: Case study of a male tortured refugee. Torture 16, 20–29.
Momartin, S., Silove, D., Manicavasagar, V., and Steel, Z. (2002). Range and dimensions of trauma experienced by Bosnian refugees resettled in Australia. Aust. Psychol. 37, 149–155. doi: 10.1080/00050060210001706806
Morina, N. (2011). Rumination and avoidance as predictors of prolonged grief, depression, and posttraumatic stress in female widowed survivors of war. J. Nerv. Ment. Dis. 199, 921–927. doi: 10.1097/NMD.0b013e3182392aae
Nickerson, A., Bryant, R. A., Schnyder, U., Schick, M., Mueller, J., and Morina, N. (2015a). Emotion dysregulation mediates the relationship between trauma exposure, post-migration living difficulties and psychological outcomes in traumatized refugees. J. Affect. Disord. 173, 185–192. doi: 10.1016/j.jad.2014.10.043
Nickerson, A., and Hinton, D. E. (2011). Anger regulation in traumatized Cambodian refugees: the perspectives of Buddhist monks. Cult. Med. Psychiatry 35, 396–416. doi: 10.1007/s11013-011-9218-y
Nickerson, A., Schnyder, U., Bryant, R. A., Schick, M., Mueller, J., and Morina, N. (2015b). Moral injury in traumatized refugees. Psychother. Psychosom. 84, 122–123. doi: 10.1159/000369353
Novaco, R. (1986). “Anger as a clinical and social problem,” in Advances in the Study of Aggression, Vol. II, ed R. J. Blanchard and D. C. Blanchard (New York, NY: Academic Press).
Paunovic, N., and Öst, L. G. (2001). Cognitive-behavior therapy vs. exposure therapy in the treatment of PTSD in refugees. Behav. Res. Ther. 39, 1183–1197. doi: 10.1016/S0005-7967(00)00093-0
Pirta, R. S., Chandel, N., and Pirta, C. (2014). Attachment and displacement: the resettlers of Bhakra Dam are hurt. Psychol. Stud. 59, 1–10. doi: 10.1007/s12646-013-0211-0
Raney, S. (2008). The Endangered Lives of Women: Peace and Mental Health Among Tibetan Refugees. Dissertation Abstracts International: Section B: The Sciences and Engineering, 69(3-B), 1969. Available online at: http://helios.uta.fi/docview/621746109?accountid=14242
Rees, S., and Silove, D. (2011). Sakit Hati: a state of chronic mental distress related to resentment and anger amongst West Papuan refugees exposed to persecution. Soc. Sci. Med. 73, 103–110. doi: 10.1016/j.socscimed.2011.05.004
Rees, S., Silove, D., Verdial, T., Tam, N., Savio, E., Fonseca, Z., et al. (2013). Intermittent explosive disorder amongst women in conflict affected Timor-Leste: associations with human rights trauma, ongoing violence, poverty, and injustice. PLoS ONE 8:e69207. doi: 10.1371/journal.pone.0069207
Rice, S. K. (2009). Emotions and terrorism research: a case for a social-psychological agenda. J. Crim. Justice 37, 248–255. doi: 10.1016/j.jcrimjus.2009.04.012
Roche, J. (2016). ‘Rights to Rights’ Realized: Agentive Anger Among Iraqi Asylum Seekers in Finland. Master's thesis, University of Tampere, Faculty of Social Sciences, Tampere. Available online at: http://urn.fi/URN:NBN:fi:uta-201610252470
Rousseau, C., and Foxen, P. (2010). “Look Me in the Eye”: empathy and the transmission of trauma in the refugee determination process. Transcult. Psychiatry 47, 70–92. doi: 10.1177/1363461510362338
Salcioglu, E., and Başoglu, M. (2013). “Current state of the art in treatment of posttraumatic stress disorder,” in New Insights Into Anxiety Disorders, ed F. Durbano (London: InTech), 379–406.
Schacter, S., and Singer, J. E. (1963). Cognitive, social, and psychological determinants of emotional state. Psychol. Rev. 69, 379–399. doi: 10.1037/h0046234
Sedighdeilami, F. (2004). Psychological Adjustment of Iranian Immigrants and Refugees in Toronto (Ontario). Dissertation Abstracts International: Section B: Sciences and Engineering, 64(8-B), 4062. Available online at: http://helios.uta.fi/docview/620634158?accountid=14242
Seligman, M. E. (1975). Helplessness: On depression, Death, and Development. San Francisco, CA: Freeman.
Sharp, W., Schulenberg, S. E., Wilson, K. G., and Murrell, A. R. (2004). Logotherapy and acceptance and commitment therapy (ACT): an initial comparison of values-centered approaches. Int. Forum Logother. 27, 98–105.
Silove, D. (1996). Torture and refugee trauma: implications for nosology and treatment of posttraumatic syndromes. Int. Rev. Psychiatry 2, 211–232.
Silove, D. (1999). The psychosocial effects of torture, mass human rights violations and refugee trauma: towards an integrated conceptual framework. J. Nerv. Ment. Dis. 187, 200–207. doi: 10.1097/00005053-199904000-00002
Silove, D. (2007). “Adaptation, ecosocial safety signals, and the trajectory of PTSD,” in Understanding Trauma. Integrating Biological, Clinical, and Cultural Perspectives, ed R. Lemelson, M. Barad and L. Kirmayer (Cambridge: Cambridge University Press), 242–258.
Silove, D. (2013). The ADAPT model: a conceptual framework for mental health and psychosocial programming in post conflict settings. Intervention 11, 237–248. doi: 10.1097/WTF.0000000000000005
Silove, D., Brooks, R., Steel, C.atherine, R. B., Steel, Z., Hewage, K., Rodger, J., et al. (2009). Explosive anger as a response to human rights violations in post-conflict Timor-Leste. Soc. Sci. Med. 69, 670–677. doi: 10.1016/j.socscimed.2009.06.030
Silove, D., Steel, Z., and Watters, C. (2000). Policies of deterrence and the mental health of asylum seekers. JAMA 284, 604–611. doi: 10.1001/jama.284.5.604
Smith, P., Tuomisto, M. T., Blumenthal, J., Sherwood, A., Parkkinen, L., Kähönen, M., et al. (2013). Psychosocial correlates of atrial natriuretic peptide: a marker of vascular health. Ann. Behav. Med. 45, 99–109. doi: 10.1007/s12160-012-9414-1
Spielberger, C. D. (1999). STAXI-2: State-Trait Anger Expression Inventory-2: Professional Manual. Lutz, FL: Psychological Assessment Resources.
Stenmark, H., Guzey, I. C., Elbert, T., and Holen, A. (2014). Gender and offender status predicting treatment success in refugees and asylum seekers with PTSD. Eur. J. Psychotraumatol. 5:20803. doi: 10.3402/ejpt.v5.20803
Summerfield, D. (2003). War, exile, moral knowledge and the limits of psychiatric understanding: a clinical case study of a Bosnian refugee in London. Int. J. Soc. Psychiatry 49, 264–268. doi: 10.1177/0020764003494004
Tarrier, N., and Taylor, R. (2014). “Schizophrenia and other psychotic disorders,” in Clinical Handbook of Psychological Disorders: A Step-By-Step Treatment Manual, ed D. H. Barlow (New York, NY: Guilford Press), 502–532.
Tay, A. K., Rees, S., Chen, J., Kareth, M., and Silove, D. (2015b). The coherence and correlates of intermittent explosive disorder amongst West Papuan refugees displaced to Papua New Guinea. J. Affect. Disord. 177, 86–94. doi: 10.1016/j.jad.2015.02.009
Tay, A. K., Rees, S., Chen, J., Kareth, M., and Silove, D. (2015a). Factorial structure of complicated grief: associations with loss-related traumatic events and psychosocial impacts of mass conflict amongst West Papuan Refugees. Soc. Psychiatry Psychiatr. Epidemiol. 51, 395–406. doi: 10.1007/s00127-015-1099-x
Tuomisto, M. T., Majahalme, S., Kähönen, M., Fredrikson, M., and Turjanmaa, V. (2005). Psychological stress tasks in the prediction of blood pressure level and need of antihypertensive medication: 9-12 years of follow-up. Health Psychol. 24, 77–87. doi: 10.1037/0278-6133.24.1.77
UN General Assembly (1951). Convention Relating to the Status of Refugees, United Nations, Treaty Series, 189, 137. Available online at: http://www.refworld.org/docid/3be01b964.html
UNHCR (2011). Global Report. Geneva: United Nations High Commissioner for Refugees. Available online at: https://www.unhcr.org/gr11/index.xml
UNHCR (2015). Global Trends: Forced Displacement in 2015. Geneva: United Nations High Commissioner for Refugees. Available online at:http://www.unhcr.org/576408cd7
Van de Vijver, F., and Tanzer, N. K. (2004). Bias and equivalence in cross-cultural assessment: an overview. Eur. Rev. Appl. Psychol. 54, 119–135. doi: 10.1016/j.erap.2003.12.004
Victoroff, J. (2005). The mind of a terrorist: a review and critique of psychological approaches. J. Confl. Resolut. 49, 3–42. doi: 10.1177/0022002704272040
Victoroff, J., Adelman, J. R., and Matthews, M. (2012). Psychological factors associated with support for suicide bombing in the Muslim diaspora. Polit. Psychol. 33, 791–809. doi: 10.1111/j.1467-9221.2012.00913.x
Weiss, M. G., Saraceno, B., Saxena, S., and Van Ommeren, M. (2003). Mental health in the aftermath of disasters: Consensus and controversy. J. Nerv. Ment. Dis. 191, 611–615. doi: 10.1097/01.nmd.0000087188.96516.a3
Westermeyer, J., and Uecker, J. (1997). Predictors of hostility in a group of relocated refugees. Cult. Divers. Ment. Health 3, 53–60. doi: 10.1037/1099-9809.3.1.53
Zarowsky, C. (2004). Writing trauma: emotion, ethnography, and the politics of suffering among Somali returnees in Ethiopia. Cult. Med. Psychiatry 28, 189–209. doi: 10.1023/B:MEDI.0000034410.08428.29
Keywords: anger, grief, interpersonal relations, refugees, stress disorders, post-traumatic
Citation: Tuomisto MT and Roche JE (2018) Beyond PTSD and Fear-Based Conditioning: Anger-Related Responses Following Experiences of Forced Migration—A Systematic Review. Front. Psychol. 9:2592. doi: 10.3389/fpsyg.2018.02592
Received: 10 June 2018; Accepted: 03 December 2018;
Published: 19 December 2018.
Edited by:
Osmano Oasi, Catholic University of Sacred Heart, ItalyReviewed by:
Eleonora Volpato, Fondazione Don Carlo Gnocchi Onlus (IRCCS), ItalyCopyright © 2018 Tuomisto and Roche. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martti T. Tuomisto, bWFydHRpLnR1b21pc3RvQHV0YS5maQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.