 Rebecca McPhillips
Rebecca McPhillips Peter Salmon3
Peter Salmon3 Adrian Wells
Adrian Wells Peter Fisher
Peter Fisher- 1Faculty of Biology, Medicine and Health, School of Psychological Sciences, Manchester Academic Health Science Center, University of Manchester, Manchester, United Kingdom
- 2Department of Research and Innovation, Greater Manchester Mental Health Trust, Manchester Academic Health Science Center, Manchester, United Kingdom
- 3Division of Clinical Psychology, Psychological Sciences, University of Liverpool, Liverpool, United Kingdom
Introduction: Cognitive behavioral therapy (CBT) alleviates emotional distress in mental health settings, but has only modest effects in cardiac patients. Metacognitive therapy (MCT) also alleviates depression and anxiety in mental health settings and is in its initial stages of evaluation for cardiac patients.
Aim: Our objective is to compare how CBT and MCT models conceptualize cardiac patients' distress, and to explore why CBT has had limited benefit for cardiac patients and whether MCT has the potential to be more efficacious.
Method: Forty-nine cardiac rehabilitation patients, who screened positively for anxiety and/or depression, provided semi-structured interviews. We analyzed transcripts qualitatively to explore the “fit” of patients' accounts of their distress with the main elements of cognitive behavioral and metacognitive theories. Four illustrative cases, representative of the diverse presentations in the broader sample, were analyzed in detail and are presented here.
Results: Conceptualizing patients' distress from the perspective of CBT involved applying many distinct categories to describe specific details of patients' talk, particularly the diversity of their concerns and the multiple types of cognitive distortion. It also required distinction between realistic and unrealistic thoughts, which was difficult when thoughts were associated with the risk or consequences of cardiac events. From the perspective of MCT a single category—perseverative negative thinking—was sufficient to understand all this talk, regardless of whether it indicated realistic or unrealistic thoughts, and could also be applied to some talk that did not seem relevant from a CBT perspective.
Discussion: Conceptualizing distress from the perspective of CBT presents multiple, diverse therapeutic targets, not all of which a time-limited therapy would be able to address. Given the difficulty of identifying them as unrealistic or not, thoughts about disease, death or disability may not be amenable to classic CBT techniques such as reality testing. MCT proved more parsimonious and, because it did not distinguish between realistic and unrealistic thoughts, might prove a better fit to emotional distress in cardiac patients.
Introduction
Depression and anxiety are problems commonly associated with cardiovascular disease. A meta-analysis found that generalized anxiety disorder and panic disorder are over twice as prevalent in coronary heart disease (CHD) patients than in the general population, and are comorbid with depressive disorders in approximately 50% of cases, a rate of comorbidity that is similar to community and psychiatric samples (Tully et al., 2016). Reviews of studies of depression in patients with myocardial infarction (MI) found that 20% of patients from eight studies that used structured clinical interviews reached criteria for major depression, and 14 studies that used validated self-report measures identified depression in 40% of MI patients (Carney and Freedland, 2003; Thombs et al., 2006). Emotional distress in this population is linked to poorer quality of life, increased risk of future cardiac events and mortality, increased use of healthcare, and poorer treatment adherence (Frasure-Smith et al., 2000; Bush et al., 2001; Lespérance et al., 2002; Gehi et al., 2005; Goyal et al., 2005; Carney et al., 2008; Yohannes et al., 2010; Dickens et al., 2012; Müller et al., 2012; Tully et al., 2016).
Cognitive Behavioral Therapy (CBT) is widely recommended to treat anxiety and depression (Ballenger et al., 2001; Allgulander et al., 2003; American Psychiatric Association, 2010; National Institute for Health and Care Excellence, 2011, 2016; Bandelow et al., 2014), including in cardiac patients (Lichtman et al., 2008; National Institute for Health and Care Excellence, 2009; Heart Foundation, 2012; Irish Association of Cardiac Rehabilitation, 2013). Its underpinning theory (Table 1) states that: (i) patients experience negative automatic thoughts (NATs) about themselves, the world and the future, which can be triggered by events such as an MI; (ii) NATs reflect patients' negative beliefs about themselves and the world around them (these can indicate deeply entrenched “core beliefs,” or “schemas,” and “intermediate beliefs,” which are more malleable assumptions, attitudes and rules); (iii) cognitive distortions maintain NATs and negative beliefs (Beck, 1964a,b, 1976). CBT therapists help patients to identify and modify NATs and negative beliefs, typically by challenging patients' beliefs in the accuracy of their thoughts, a process termed “cognitive challenging” or “reality testing” (Beck, 1964a,b, 1976; Beck et al., 1979; Beck and Emery, 1985). Since its inception, CBT theory has been extended to incorporate maladaptive behaviors, including avoidance and reassurance seeking, and heightened attention, for example to bodily symptoms (Table 1) (Clarke and Beck, 2010; Beck, 2011; Beck and Haigh, 2014).
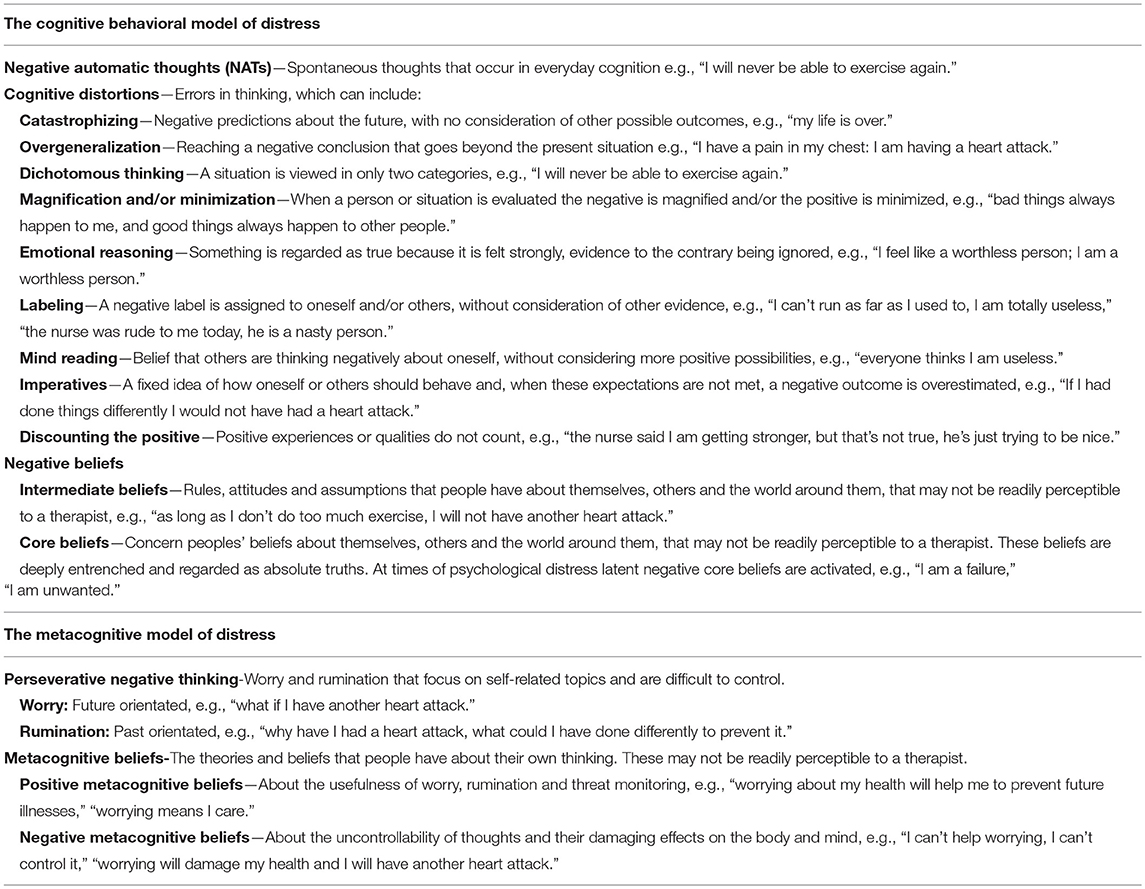
Table 1. Key elements of the cognitive behavioral and metacognitive models of distress.
In mental health populations, meta-analyses show that CBT is an efficacious treatment for anxiety and depression when compared to wait-list or a range of comparison conditions, with medium effect sizes of 0.73 and 0.71, respectively (Hofmann and Smits, 2008; Cuijpers et al., 2013). By contrast, meta-analyses of CBT-based interventions in cardiac patients have been disappointing (Linden, 2013). When compared to usual care or comparison conditions, including physical exercise or educational interventions, effect sizes have ranged from 0.12 to 0.44 (Welton et al., 2009; Dickens et al., 2013; Rutledge et al., 2013; Jeyanantham et al., 2017; Reavell et al., 2018). A recently updated Cochrane review assessed the efficacy of psychological interventions in CHD patients compared with usual care (Richards et al., 2017). Although this review did not report effects for CBT specifically, we calculated the effect size across those reviewed studies that evaluated interventions based on CBT and that reported outcomes for depression and/or anxiety (Burgess et al., 1987; Black et al., 1998; Berkman et al., 2003; Claesson et al., 2005; McLaughlin et al., 2005; Michalsen et al., 2005; Koertge et al., 2008; Freedland et al., 2009; Merswelken et al., 2011; Turner et al., 2012, 2014; O'Neil et al., 2015). Again, effect sizes were small: 0.29 and 0.24 for anxiety and depression, respectively. The dominant study in the Cochrane review, and the largest RCT of CBT for cardiac patients yet undertaken, is the ENRICHD study (Writing Committee for the ENRICHD Investigators, 2003). ENRICHD found that, although CBT improved depression when compared to a usual care control condition, albeit with a small effect size of 0.33, these effects were not maintained at follow up. Paradoxically, there was no effect on the primary outcomes of cardiovascular morbidity and mortality, even though further analysis showed that depression was an independent risk factor for mortality (Carney et al., 2003).
Why CBT has had only modest benefit in cardiac patients, particularly when compared to mental health populations, is not clear. Interventions for cardiac patients have sometimes been delivered by physical health practitioners, particularly nurses, not specialized in psychological interventions (e.g., Burgess et al., 1987; Frasure-Smith and Prince, 1989; Van Elderen-Van Kemenade et al., 1994; Cowan et al., 2001), perhaps reflecting the practical difficulties and resource constraints in offering psychological therapy in the context of continuing clinical care. However, it has also been suggested that the defining practice of CBT—reality testing—might be inappropriate in a clinical context where patients' NATs often reflect a reality shaped by morbidity and disability and real risks of sudden and untimely death (Greer et al., 2010; Taylor-Ford, 2014).
A different psychological intervention that has proven effective in mental and physical health settings is metacognitive therapy (MCT) (Wells, 2009). MCT is based on the metacognitive model of psychological distress (Wells and Matthews, 1996; Wells, 2009). In this model (Table 1) psychological disorder is linked to: (i) the cognitive attentional syndrome (CAS), which is characterized by patterns of perseverative negative thinking (worry and rumination) that is extended and difficult to control, threat monitoring, and attempts to control thoughts, for example by thought suppression and reassurance seeking; (ii) underlying metacognitive beliefs that can be conceptually divided into positive and negative beliefs about perseverative thinking. Positive beliefs concern the theme that repetitive negative thinking (e.g., worry) is a helpful way of anticipating problems, whilst negative beliefs concern the theme that such thinking is uncontrollable and dangerous. Whilst the CBT model emphasizes the content of thoughts, MCT emphasizes perseveration of negative thinking as the process maintaining distress. Unlike CBT, the MCT therapist does not challenge the content of perseverative negative thinking or the veracity of beliefs about the self and world. Instead the therapist helps the patient bring perseverative negative thinking under control, and challenges underlying metacognitive beliefs.
In a recent meta-analysis of anxiety and depression treatment trials in mental health populations, MCT was more effective than waitlist control, with a very high effect size of 1.81, and was more effective than CBT, with a large effect size of 0.97 (Normann et al., 2014). Although no randomized controlled trial (RCT) of MCT for psychological distress in physical health populations is yet complete, support for its potential relevance to distressed cardiac rehabilitation (CR) patients comes from evidence of the association between metacognitive beliefs and psychological distress in a range of physical diseases including cancer (Thewes et al., 2013; Cook et al., 2015), Parkinson's disease (Allot et al., 2005; Brown and Fernie, 2015; Fernie et al., 2015) epilepsy (Fisher and Noble, 2017), chronic fatigue syndrome (Maher-Edwards et al., 2011, 2012), fibromyalgia (Kollmann et al., 2016), and diabetes (Purewal and Fisher, 2018). Clinically significant reductions in anxiety and depression in an open trial of MCT for emotional distress in adolescent and young cancer survivors (Fisher et al., 2015) and in a case series in adult cancer survivors (Fisher et al., 2017) add support for the potential relevance of MCT to anxious and/or depressed cardiac patients.
While RCTs are the “gold standard” for establishing the efficacy of psychological interventions, it is now recognized that complementary kinds of research are needed to provide information that RCTs, alone, cannot. In particular, qualitative methods can illuminate the transferability of interventions into real-life (O'Cathain et al., 2013). Specifically, O'Cathain et al. (2013) point to the need for qualitative methods to assess the “fit” between interventions, as idealized in theory and protocols, and the reality of the conditions they are intended to treat. UK Medical Research Council guidance therefore advocates a combination of quantitative and qualitative methods in treatment evaluation, the value of qualitative methods being specifically to help understanding complex causal pathways and generate new theory (Campbell et al., 2000; Moore et al., 2015). Over recent years, qualitative methods have also been used more widely to examine aspects of the “fit” between formal psychological theory and the “lived experience” of patients with physical health problems, including CR patients (Ciechanowski and Katon, 2006; Tang et al., 2009; Angus et al., 2018). In the present study our primary objective was to compare how CBT and MCT models conceptualize cardiac patients' distress, and specifically to explore the “fit” between these models and patients' own accounts of their experience of distress. Our secondary objectives were to identify potential reasons why CBT has low efficacy in this group and to explore whether MCT has the potential to be more efficacious. Our data were interviews in which CR patients described their distress. We addressed these objectives by examining patients' accounts qualitatively from the perspectives of both CBT and MCT, thereby exploring the “fit” between formal theory and patients' experience.
Methods
Sample
This research was conducted as part of the UK NIHR funded PATHWAY programme (PATHWAY; RP-PG-1211-20011; Ethical approval from NRES Committee North West, REC reference: 15/NW/0163), a RCT that compares usual CR to CR plus six sessions of Group-MCT delivered by CR practitioners with additional training in MCT (Wells et al., 2018). Inclusion criteria were a score of ≥ 8 on the depression and/or anxiety subscale of the Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983) and meeting CR eligibility criteria (British Association for Cardiovascular Prevention and Rehabilitation, 2012). Upon entry to the PATHWAY programme, patients completed the HADS (to indicate probable clinical levels of distress) and the Impact of Event Scale Revised (IES-R) (to assess symptoms of post-traumatic stress disorder; Weiss, 2007), and a clinical record form which collected socio-demographic information, details of their cardiac condition, any comorbid health conditions, and any past and/or current medication and/or therapies for psychological distress (Table 2). To enable nested qualitative studies, patients who gave or withheld written informed consent to join the trial were asked for written informed consent for qualitative interviews.
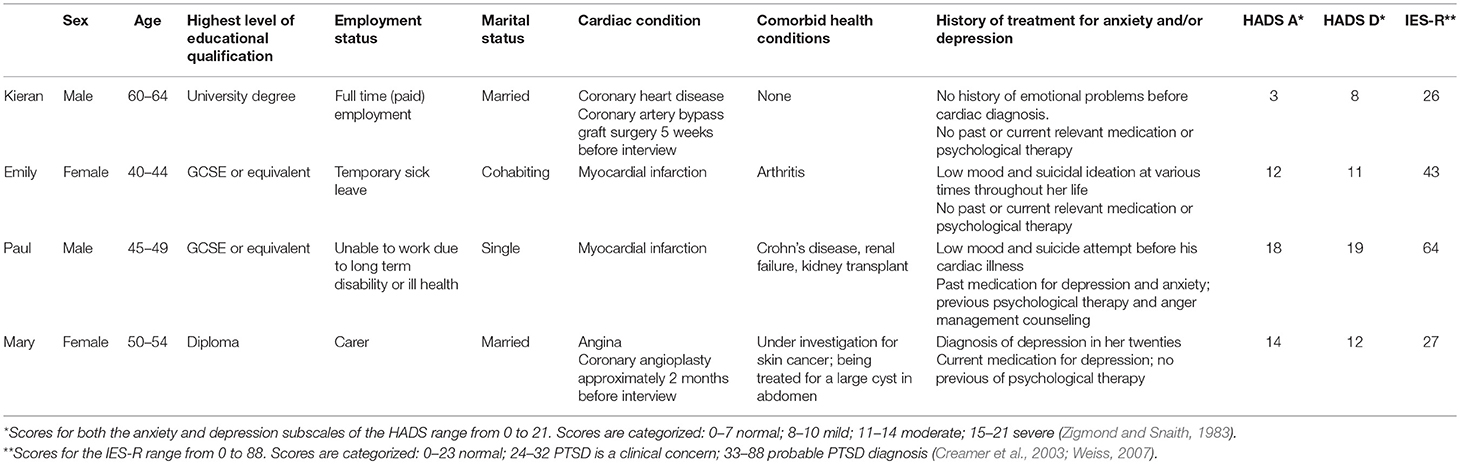
Table 2. Selected cases.
Of the first 79 patients who consented to take part in the RCT, 77 agreed to being contacted about qualitative research. Sixty patients, purposively sampled to include women and men with differing levels of distress and clinical profiles, were contacted by telephone, of whom 46 provided written informed consent to the qualitative study and took part in interviews. Of the first 43 patients who declined consent for the RCT, 15 consented to be contacted about qualitative interviews, all of whom we contacted by telephone, and 3 of whom provided written informed consent to be interviewed. The total number of patients interviewed was 49; 15 were female, and patients ages ranged from 38 to 79, median 57. Most patients described themselves as White British, 2 as Caribbean, 2 as Asian, and 2 as Australasian. Patients' cardiac conditions were MI, adult congenital heart disease, stable heart failure, stable angina, and atrial fibrillation (Supplementary Table 1). Patients were interviewed during CR, but before starting Group-MCT as part of the PATHWAY trial.
Procedure
RM conducted interviews in a conversational style in patients' homes (n = 39), a private office (n = 7), where patients received CR (n = 2), or in a public café (n = 1), as each patient requested. RM's first meeting with each patient was at this interview. No other author met any patient. To begin each interview, RM explained that she was not a therapist, and assured patients that their comments would be anonymized before disclosure to the research team. An interview guide using open questions and prompts facilitated patients' talk; closed questions were used to probe specific points. The pace, sequencing and length of interviews therefore depended on patients. Interviews lasted 29–105 min (mean 58 min). The interview guide was modified in parallel with analysis, to test and develop emerging ideas. Each patient was asked about their emotional experiences since their cardiac event (e.g., “can you tell me how you've been feeling since your heart attack?”), and to describe in detail distress they had experienced including the content of distressing thoughts, the nature of distressing emotions, when they experienced these thoughts and emotions, and how they responded to them (e.g., “what goes through your mind when you are feeling low?,” “what do you do when you feel sad or anxious?”). They were also asked about their understanding of the causes and consequences of their distress, and their thoughts and feelings about their future (e.g., “why do you think you feel like this?,” “what do you feel about the future?”).
Interviews were audio-recorded, transcribed verbatim and pseudo-anonymized. Microsoft Word was used to manage the data during analysis (La Pelle, 2004). In line with recent recommendations, we sought to tailor methods to specific research questions in order to ensure fidelity to the data and utility in achieving research goals (Levitt et al., 2017). Analysis therefore followed three stages. First, inductive analysis first followed a constant comparative approach whereby we identified commonalities and contrasts in how patients described and understood their distress. RM led this analysis, which was tested and refined in regular discussion amongst RM, PF, and PS, who all read the transcripts, and periodically including AW who read selected extracts. Findings from this stage of analysis will be reported separately.
We then returned to the transcripts and re-examined patients' accounts of their distress from the perspectives of the CBT and MCT models. Analysis combined deductive and inductive elements. The main categories of the CBT and MCT models provided an initial template. The inductive element was not to develop those categories, as in the usual approach to template analysis (Crabtree and Miller, 1999), but to understand their “fit” with patients' experience. Our primary criterion for “fit” was parsimony: how simply the models could be related to patients' accounts of their distress. In addition, we were interested in how readily and how extensively each model could be applied across the varied manifestations of patients' distress; that is, how therapeutically “workable” each model would be. We did not apply a checklist, but relied on our interpretation of the patients' subjective experience; that is, we took a stance resembling that of a therapist who seeks to identify aspects of patients' talk with which s/he can engage. Recognizing that the meaning of data in qualitative research is produced jointly by the participant and the interviewer or analyst—just as in therapy it is a product of the therapist and patient in interaction—we emphasized reflexivity; that is, we regarded our own experience of applying the template as data to be discussed and reflected on. When analyzing from the perspective of the CBT model, we focused on identifying distinct NATs, and then categorized the cognitive distortions apparent in these (Beck, 1976). Often, multiple distortions could be identified in the same text but, to simplify presentation, we coded only the most salient one. When analyzing from the perspective of the MCT model, we focused on identifying talk showing perseverative negative thinking—worry or rumination. When we saw possible underlying beliefs—negative beliefs from the perspective of CBT, or metacognitive beliefs from the perspective of MCT—these were also coded. This part of the analysis proceeded iteratively; any text coded as relevant to one model was re-examined from the alternate perspective. RM led this stage of the analysis also, in regular discussions with PS and PF, and periodically with AW. Taking a “disputational” approach, we identified and developed competing interpretations and tested their validity by evidence-based argumentation amongst the group.
Across the sample, we saw several respects in which the perspectives of the CBT and MCT models could be used to conceptualize CR patients' distress differently. We then purposively selected four transcripts reflecting diversity in the presentation and clinical context of distress for detailed analysis to illustrate that divergence (Table 2). We included patients whose distress was linked primarily to their cardiac event, and those whose distress was linked to other health and non-health problems. We also sought diversity in the profile and intensity of distress as indicated by HADS and IES-R scores. Analysis proceeded as for the overall sample, but focusing only on detailed scrutiny of these cases.
The research team brought different perspectives to analysis. RM has experience of research in medical sociology and the psychology of health language and communication, and specifically of qualitative research on patient experiences of physical health care. AW, PF, and PS are clinical psychologists with experience of physical health care: AW has contributed to the development of CBT and is the originator of MCT, and is experienced in treating various psychopathologies in different patient populations using both therapies; PF is experienced in CBT and MCT and in applying MCT to physical health populations; PS has expertise in qualitative analysis of patients' needs and experiences in physical health care, in the development and synthesis of qualitative methods, and in critical analysis of psychological theory in health care.
Table 3 shows data extracts from each transcript and relevant coding. We selected extracts that illustrated the main features of the analysis across the range of each patient's concerns. In Table 3 extracts are shown in the sequence in which they arose in the interview, italicized text provides context for each extract, ellipses are used to indicate omitted talk, and square brackets indicate RM's talk and explanatory comments. Figures in parenthesis in the main text indicate corresponding extracts in Table 3. Pseudonyms are used and identifying details removed to preserve anonymity.

Table 3. Cardiac patients' emotional distress conceptualized from the perspectives of cognitive behavioral and metacognitive models of distress.
Results
As will be reported elsewhere, inductive analysis of all interview transcripts identified CR patients' diverse concerns about their cardiac event, including the continuing risk to their lives and the constraints that reduction in energy or confidence, as well as continuing medical treatment or surveillance, imposed on their lives. Patients also reported dwelling on regrets from their early life and worrying about current or future challenges unrelated to their physical health.
When considering the transcripts from the perspectives of CBT or MCT, CR patients' distress was conceptualized very differently. From the perspective of CBT, we identified relatively focused and distinct sections of patients' talk that contained NATs, and that displayed many cognitive distortions (Beck, 1976), although it was often difficult to agree which category of distortion to allocate specific NATs to. It was also sometimes difficult to decide whether specific negative thoughts, particularly relating to cardiac disease, were realistic or unrealistic. We were also able to identify patients' negative beliefs about themselves, (such as being inadequate), about the world around them (such as other people seeing them as inadequate), and about the future (for example that life is pointless). From the perspective of MCT, we identified longer sections of patients' talk, which could readily be understood as perseverative negative thinking (worry or rumination), and which encompassed many of the different NATs and cognitive distortions that were categorized in detail from the CBT perspective. These chains of perseverative negative thinking included some talk that had not been coded as relevant from a CBT perspective. We also identified patients' positive metacognitive beliefs, including that rumination would help them understand why they had experienced a cardiac event and that worry would prepare them for a future one. We identified negative metacognitive beliefs, also, specifically that thinking about illness was uncontrollable and harmful and threatened their mental health or risked worsening their cardiac disease.
Table 2 describes the four cases selected to develop and illustrate these findings. Kieran, with HADS scores suggesting mild depression, described no history of emotional problems before his diagnosis of CHD and subsequent coronary artery bypass graft (CABG). He attributed his unhappiness mainly to his cardiac illness and the threat it presented to enjoying his impending retirement. Emily, with HADS scores suggesting moderate anxiety and depression, had felt depressed and even suicidal before her MI, although she had never been diagnosed with anxiety or depression. Her concerns centered on fear of another MI and difficulty sleeping. Paul, whose HADS scores suggested moderate anxiety and depression, had been diagnosed with depression and anxiety, had attempted suicide previously, and had received psychotherapy and anti-depressant medication. In addition to concerns about the loss of his career, and therefore his home, because of his MI, Paul dwelled on the breakdown of previous romantic relationships and on difficulties in his relationship with his father during childhood. Mary had been diagnosed with angina and treated with a coronary angioplasty. Her HADS scores suggested moderate anxiety and depression. She had a history of depression, and still took anti-depressant medication. Her concerns centered on her son's alcoholism and her problematic relationship with her husband.
Conceptualizing Patients' Distress From a Cognitive Behavioral Perspective
Each patient's talk showed a diverse range of NATs concerning fear of their cardiac disease and the impact this already had on their lives, or may have in future. Paul (3b,d,e) and Mary (4b,c,e,f) also voiced NATs about social and family relationships, and Kieran (1d) and Paul (3b,c,d,e) about past events. Every patient's talk also indicated possible negative beliefs. Like their NATs, these were diverse. Some were specifically related to cardiac disease. For instance, Kieran (1d,e) described believing that his retirement would be less fulfilling than he had imagined, because of limitations he envisaged as a result of his CHD, Emily (2a,b) indicated the belief that she would have another MI that would be fatal, Mary (4a) was concerned that she would be unable to fulfill her role as a carer, and Paul (3c,d) believed that the effects of his MI on his health might have been mitigated had he called an ambulance sooner, and treated earlier. However, many negative beliefs concerned other areas of life, even pre-dating cardiac disease. Mary (4b,c,d) talked openly about being “stupid,” “ugly,” and “worthless,” indicating persistent negative beliefs about herself that she described having for “years,” before being diagnosed with angina. Paul (3b,d) blamed himself for neglecting previous romantic relationships, and for not seeking medical help for his MI earlier than he did. Additionally, Paul (3e) described consistently expecting “bad things” to happen to him that he was helpless to influence, such as breakdown in relationships, complaining that he might have been able to prevent them had he been “brought up or treated differently.”
Every patient displayed several cognitive distortions (Beck, 1976). Catastrophizing was common, particularly in NATs concerning cardiac disease: for example, Emily's NATs (2a,b,d,e) that she would have a second MI, and that this would kill her, and Kieran's (1e) NAT that his CHD would devastate his retirement plans. For Paul and Mary, catastrophic thinking extended beyond cardiac disease, for instance in Paul's (3d) NAT that “bad things” happen to him and Mary's (4e) NAT that that her son would die if he returned to drinking alcohol. Patients' NATs contained further distortions, including magnification and minimization, imperatives, dichotomous thinking, and emotional reasoning. For example, Kieran's (1c) NATs contrasting his own experiences with others' illustrated magnification and minimization: he minimized others work and efforts to be healthy when complaining that “they haven't worked hard all their lives and they haven't gone to the gym,” and magnified their experiences when he suggested “they're enjoying themselves.” Paul's (3b,c) NATs concerning previous relationships and his MI contained imperatives: he lamented that “if only” he had done things differently his relationship might not have broken down, and that he “should” have called an ambulance sooner, and his NATs (3d) concerning the impact of his MI contained dichotomous thinking: that he “can't drive a truck,” and that his “career” [had] “gone.” Emily and Mary displayed NATs that contained emotional reasoning, as Emily (2c) described “feel[ing] stupid” because her STENT had “affected” her, in contrast to a friend who had been unaffected by a double heart bypass, and Mary (4b) “[felt] like a worthless person,” because her husband made her feel that “anything [she said] don't mean anything.”
Some of the NATs, negative beliefs and cognitive distortions described above seemed clearly unrealistic, for example Kieran's (1a) minimization and magnification. However, others reflected elements of patients' clinical reality. Because of the physical impact of his MI, Paul (3d) could no longer drive a truck, and so had lost his job and could not afford to keep his flat. Mary's (4a) concerns about not being able to work as a carer predict a likely, albeit temporary, consequence of her clinical reality. In many instances, however, it was difficult to categorize the NATs, negative beliefs or cognitive distortions as either realistic or unrealistic. For instance, Kieran's (1e) prediction that his CHD would preclude activities he had planned for retirement might reflect the reality of disability associated with CHD for many patients, and Emily's (2a,b) fear of a fatal MI might reflect a real, albeit potentially small, risk.
We coded only the most salient cognitive distortion for any NAT. However, multiple distortions could readily be identified in many NATs, and it was often difficult to decide which to prioritize. For instance, Kieran's (1b) NAT about being “the most unfit person I know' shows over-generalization, but might also be regarded as magnification and minimization or as labeling. Similarly, we coded Mary's (4e) NAT that, if her son drank alcohol again, it would kill him as catastrophic thinking, but it also might be understood as overgeneralization or dichotomous thinking.
In summary, each patient's distress could be readily conceptualized using the CBT model. This involved identifying a diverse range of NATs, negative beliefs and cognitive distortions. However, distinguishing between unrealistic and realistic NATs and negative beliefs could be difficult, particularly when they were associated with patients' cardiac disease.
Conceptualizing Patients' Distress From a Metacognitive Perspective
Every patient described experiences that could readily be interpreted as indicating perseverative negative thinking. For example, Paul (3a) explained that the only time that he did not ruminate was while asleep, Emily (2e) complained that rumination about the night of her MI prevented her from sleeping, and Mary (4e) reported being “worried sick” about her son “all the time,” all clearly indicating the repetitive and extended thinking that characterize perseverative negative thinking. Every patient also displayed perseverative negative thinking in “real time” during their interviews. For instance, Mary repeatedly talked about her son's drinking, her relationship with her husband, and about how she felt about herself, even when asked about seemingly unrelated topics. Similarly, Paul introduced regrets over his previous relationships and childhood repeatedly throughout his interview. The single category of perseverative negative thinking encompassed most of the talk that, from the perspective of CBT, was understood as diverse NATs, negative beliefs, and cognitive distortions. It also included sections of talk that were not coded as significant from the CBT perspective, for example Kieran's (1d) regrets about losing contact with old friends, Emily's (2e) description of mentally “re-running” her MI, Paul's (3a) explanation that the only time he is “alright” is when asleep, and Mary's (4f) account of “worrying” about her adult children, particularly her alcoholic son.
Each patient's account contained evidence of negative metacognitive beliefs (Wells, 1995). Kieran (1e) alluded to believing that he lacked control over thinking, when he described needing to keep busy during retirement so that he would not “always be thinking.” The other patients were more explicit about believing they lacked control. Mary (4f) and Paul (3e) reported being unable to “switch off” worrying or ruminating, and Emily (2e) described rumination that was “always there.” Emily and Paul also indicated possible beliefs about the harmfulness of thinking. Emily (2e) referred to her “medical background” as a “problem” because knowing “too much” made her “worse” (2e), while Paul (3f) explained that “thinking to [him]self” about the differences between himself and others was “more harmful than good.” Three patients' accounts also demonstrated positive metacognitive beliefs that thinking would help them to find answers and be prepared. Emily (2a,c,e) reported “re-running” the night of her MI and continuing to ask herself why her MI had affected her so badly. Similarly, Paul (3b) described “analyzing” a past relationship, lest he could have “foreseen and maybe done something about” its breakdown, and Mary (4e) explained that she deals “with something in [her] head that hasn't happened yet, but maybe it will.” Much of the text coded as metacognitive beliefs from the perspective of MCT was not coded at all from the perspective of CBT; for example text coded as Emily's (2a,e) metacognitive beliefs that thinking about the events that led to her MI was uncontrollable and harmful but would help her find answers, and as Mary's (4f) metacognitive beliefs that worrying is both uncontrollable and useful.
In summary, conceptualizing cardiac patients' distress from the perspective of MCT proved more parsimonious than from that of CBT; the diverse range of NATs, cognitive distortions and negative beliefs identified from the perspective of CBT were largely contained within the single category of perseverative negative thinking, which also included text not coded as relevant to CBT. There were possible metacognitive beliefs, also often in text not coded as relevant to CBT. Examining accounts from the perspective of MCT did not require decisions as to whether distressing thoughts were unrealistic.
Discussion
We addressed our primary objective by comparing how CR patients' accounts of distress can be understood from CBT and MCT perspectives. Focusing on the content of patients' concerns, taking a CBT perspective meant allocating specific elements of patients' accounts of their distress across many discrete categories: different NATs and negative beliefs and the multiple cognitive distortions that maintain them. In contrast, MCT was more parsimonious in that a single category—perseverative negative thinking—encompassed most of that text. Moreover, understanding distress from the perspective of CBT involved difficult judgments as to whether negative thoughts were realistic or unrealistic, whereas this distinction was not necessary from an MCT perspective. Our findings therefore address our secondary objectives in pointing to potential reasons why CBT has low efficacy for cardiac patients and why MCT might have a better fit with distress in this population.
Our findings suggest two respects in which the CBT model might be a poor fit with CR patients' distress. First, patients described diverse NATs and negative beliefs, encompassing not only cardiac disease but other areas of their lives including problems that long pre-dated their cardiac diagnosis. In the context of a time-limited therapy, it will rarely be possible for a CBT therapist to address all these for any patient. CBT therapists are advised to target specific NATs and negative beliefs according to how distressing or dysfunctional they are, or how persistent they are (Beck, 1976). However, CBT theory does not itself specify how a therapist can choose between multiple NATs and negative beliefs that might all be distressing, dysfunctional and persistent, and does not stipulate how addressing specific NATs and negative beliefs will alleviate distress caused by unaddressed NATs and negative beliefs. Furthermore, since a single NAT can contain more than one cognitive distortion, it can be difficult to decide which is the “main” one, leading to the risk that the CBT therapist will not target the most critical distortion.
The second reason why the CBT model had questionable fit with CR patients' distress was because of the importance it attaches to identifying and challenging unrealistic thoughts and beliefs. In the context of a recent life-threatening cardiac event, continuing vulnerability to cardiac problems, and attendant disability and uncertainty about the future, patients had many negative thoughts and beliefs that could not be readily categorized as realistic or unrealistic. Reality testing patients' realistic concerns about their health, and about the toll that ill-health has taken, or might take, on their lives is, at best, inappropriate and, at worst, absurd (Greer et al., 2010). CBT theory has therefore evolved to address the challenge of realistic negative thoughts in the context of life-threatening disease, particularly cancer (Greer et al., 2010; Moorey and Greer, 2012; van de Wal et al., 2015; Temple, 2017). However, adaptations of the theory center on differentiating between realistic and unrealistic concerns; realistic concerns can then be targeted using problem solving. Trying to decide whether NATs and negative beliefs are realistic or not, particularly in the context of real disability, and small but potentially fatal risks of further cardiac events, adds further complexity to the therapeutic process. Moreover, engaging patients in such decisions risks exacerbating their distress—for instance where they focus on a small, but real chance of a further MI in the future.
MCT requires fewer difficult or arbitrary decisions from a therapist. It is not necessary to identify the negative thoughts that are “most important,” or to distinguish realistic from unrealistic ones. Instead, an MCT therapist would understand the diverse concerns of CR patients as evidence of a single process of perseverative negative thinking. Moreover, elements of patients' accounts that cannot be understood in terms of any of the classic categories of the CBT model are significant from the perspective of MCT when they are further examples of perseverative negative thinking. Our findings also showed that patients make their metacognitive beliefs, which, according to the MCT model, maintain perseverative negative thinking, accessible to therapists. MCT might therefore have a better fit with distress in CR patients, because MCT therapists can target perseverative negative thinking, and the metacognitive beliefs that underlie this, and thereby address patients' diverse concerns, both unrealistic and realistic, in a time-limited therapy.
Limitations
As a qualitative study in a single setting, our findings cannot automatically be generalized. However, our qualitative approach allowed us to explore the “fit” between theory and reality in a way that is grounded in patients' own accounts of their distress. The selection of only four patients' transcripts for detailed analysis risks what Onwuegbuzie and Leech (2007) call “key informant bias” if those accounts do not represent the full sample. To minimize this risk, we selected cases across the range of severity of distress and diversity of concerns seen in the whole sample. Moreover, these patients' concerns resembled those seen in previous qualitative reports of cardiac patients' distress (Jensen and Petersson, 2003; Andersen et al., 2008; Dekker, 2014). Qualitative research is necessarily shaped by researchers' own perspectives in both data collection and analysis phases. Two members of the research team, while expert in both MCT and CBT, have been proponents of MCT. However, by including authors with experience in using qualitative methods to voice patients' own perspectives and challenge idealized theories, and by adopting an iterative, “disputational” approach to analysis, we sought to ensure an analysis that was thoroughly tested and informed from multiple perspectives while being grounded in patients' accounts.
Conclusions
A strength of this study is the combination of inductive and deductive analysis. By using CBT and MCT as templates through which to view CR patients' emotional distress, we have been able to explore the fit between patients' distress and these two therapeutic modalities. The findings help to understand the limited efficacy of CBT in cardiac patients, and suggest that MCT might offer a better fit with distress in this population. Both on scientific grounds, and to reduce the risk of wasting resources in evaluating interventions that are a poor fit to the needs of the target population, we suggest that studies such as this should be prioritized early in the development and evaluation of psychological interventions, or in the application of interventions to new populations, before progressing to the stage of RCTs. Such studies can ensure that RCTs are focused in areas of the greatest potential benefit to patients. More specifically, our findings can inform improvements in psychological intervention in the context of cardiac care. We propose that, rather than conducting further RCTs of CBT for cardiac patients, evaluations of potentially more compatible psychological interventions such as MCT are required.
Author Contributions
RM collected the data and led the data analysis of each transcript in its entirety. PF and PS contributed to the data analysis in its entirety. AW contributed to the data analysis of selected extracts from specific transcripts. RM led the development of the manuscript. PF, PS contributed to the first and subsequent drafts of the manuscript. AW contributed to later drafts of the manuscript.
Funding
This research is funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Scheme (RP-PG-1211 20011). The views and opinions expressed are those of the authors and do not necessarily reflect those of the NIHR, NHS or the Department of Health and Social Care.
Conflict of Interest Statement
AW is a co-director of the MCT Institute.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank all participants in this study, and also the PATHWAY team; Senior Research Assistants, Helen Morley, Rebecca Anderson, Lora Capobianco, and Cintia Faija and Administrators, Wendy Clarke and Avinash Atwal, who contributed to recruiting participants and organizing the study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2018.02288/full#supplementary-material
Abbreviations
CABG, Coronary artery bypass graft; CAS, Cognitive attentional syndrome; CBT, Cognitive behavioral therapy; CHD, Coronary heart disease; CR, Cardiac rehabilitation; HADS, Hospital anxiety and depression scale; IES-R, Impact of event scale—revised; MCT, Metacognitive therapy; MI, Myocardial infarction; NAT, Negative automatic thought; NICE, National Institute for Health and Care Excellence; RCT, Randomized controlled trial.
References
Allgulander, C., Bandelow, B., Hollander, E., Montgomery, S. A., Nutt, D. J., Okasha, A., et al. (2003). World Council for Anxiety recommendations for the long-term treatment of generalized anxiety disorder. CNS Spectr. 8, 53–61. doi: 10.1017/S1092852900006945
Allot, R., Wells, A., Morrison, A. P., and Walker, R. (2005). Distress in Parkinson's disease: contributions of disease factors and metacognitive style. Br. J. Psychiatry 187, 182–183. doi: 10.1192/bjp.187.2.182
American Psychiatric Association (2010). Practice Guideline for the Treatment of Patients with Major Depressive Disorder. Available online at: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf
Andersen, J., Øyen, N., Bjorvatn, C., and Gjengedal, E. (2008). Living with Long QT Syndrome: a qualitative study of coping with increased risk of sudden cardiac death. Genet. Couns. 17, 489–498. doi: 10.1007/s10897-008-9167-y
Angus, J. E., Dale, C. M., Nielson, L. S., Kramer-Kile, M., Lapum, J., Pritlove, C., et al. (2018). Gender matters in cardiac rehabilitation and diabetes: using Bourdieu's concepts. Soc. Sci. Med. 200, 44–51. doi: 10.1016/j.socscimed.2018.01.003
Ballenger, J. C., Davidson, J. R., Lecrubier, Y., Nutt, D. J., Borkovec, T. D., Rickels, K., et al. (2001). Consensus statement on generalized anxiety disorder from the International Consensus Group on Depression and Anxiety. J. Clin. Psychiatry 62, 53–58. Available online at: https://www.psychiatrist.com/jcp/article/Pages/2001/v62s11/v62s1108.aspx
Bandelow, B., Lichte, T., Rudolf, S., Wiltink, J., and Beutel, E. M. (2014). The diagnosis of and treatment recommendations for anxiety disorders. Dtsch. Arztebl. Int. 111, 473–480. doi: 10.3238/arztebl.2014.0473
Beck, A. (1976). Cognitive Therapy and the Emotional Disorders. New York, NY: International Universities Press.
Beck, A. T. (1964a). Thinking and depression: I. Idiosyncratic content and cognitive distortions. Arch. Gen. Psychiatry 9, 324–333. doi: 10.1001/archpsyc.1963.01720160014002
Beck, A. T. (1964b). Thinking and depression: II. Theory and therapy. Arch. Gen. Psychiatry 10, 561–571. doi: 10.1001/archpsyc.1964.01720240015003
Beck, A. T., and Emery, G. (1985). Anxiety Disorders and Phobias: A Cognitive Perspective. New York, NY: Basic Books.
Beck, A. T., and Haigh, E. A. P. (2014). Advances in cognitive theory and therapy: the generic cognitive model. Annu. Rev. Clin. Psychol. 10, 1–24. doi: 10.1146/annurev-clinpsy-032813-153734
Beck, A. T., Rush, A. J., Shaw, B. F., and Emery, G. (1979). Cognitive Therapy of Depression. New York, NY: Guildford Press.
Beck, J. S. (2011). Cognitive Behavior Therapy: Basics and Beyond, 2nd Edn. New York, NY: Guilford Press.
Berkman, L. F., Blumenthal, J., Burg, M., Carney, R. M., Catellier, D., Cowan, M. J., et al. (2003). Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. J. Am. Med. Assoc. 289, 3106–3116. doi: 10.1001/jama.289.23.3106
Black, J. L., Allison, T. G., Williams, D. E., Rummans, T. A., and Gau, G. T. (1998). Effect of intervention for psychological distress on rehospitalization rates in cardiac rehabilitation patients. Psychosomatics 39, 134–143. doi: 10.1016/S0033-3182(98)71360-X
British Association for Cardiovascular Prevention Rehabilitation (2012). The BACPR Standards and Core Components for Cardiovascular Disease Prevention and Rehabilitation. Available online at: http://www.bacpr.com/resources/46C_BACPR_Standards_and_Core_Components_2012.pdf
Brown, R. G., and Fernie, B. A. (2015). Metacognitions, anxiety, and distress related to motor fluctuations in Parkinson's disease. J. Psychosom. Res. 78, 143–148. doi: 10.1016/j.jpsychores.2014.09.021
Burgess, A. W., Lerner, D. J. D., Agostino, R. B., and Vokonas, P. S. (1987). A randomized controlled trial of cardiac rehabilitation. Soc. Sci. Med. 24, 359–370. doi: 10.1016/0277-9536(87)90154-7
Bush, D. E., Ziegelstein, R. C., Tayback, M., Richter, D., Stevens, S., Zahalsky, H., et al. (2001). Even minimal symptoms of depression increase mortality risk after acute myocardial infarction. Am. J. Cardiol. 88, 337–341. doi: 10.1016/S0002-9149(01)01675-7
Campbell, M., Fitzpatrick, R., Haines, A., Sandercock, P., and Tyrer, P. (2000). Framework for design and evaluation of complex interventions to improve health. BMJ 231:694. doi: 10.1136/bmj.321.7262.694
Carney, R. M., Blumenthal, J. A., Catellier, D., Freedland, K. E., Berkman, L. F., Watkins, L. L., et al. (2003). Depression as a risk factor for mortality after acute myocardial infarction. Am. J. Cardiol. 93, 1277–1281. doi: 10.1016/j.amjcard.2003.08.007
Carney, R. M., and Freedland, K. E. (2003). Depression, mortality, and medical morbidity in patients with coronary heart disease. Biol. Psychiatry 54, 241–247. doi: 10.1016/S0006-3223(03)00111-2
Carney, R. M., Freedland, K. E., Steinmeyer, B., Blumenthal, J. A., Berkman, L. F., Watkins, L. L., et al. (2008). Depression and five year survival following acute myocardial infarction: a prospective study. J. Affect. Disord. 109, 133–138. doi: 10.1016/j.jad.2007.12.005
Ciechanowski, P., and Katon, W. J. (2006). The interpersonal experience of health care through the eyes of patients with diabetes. Soc. Sci. Med. 63, 3067–3079. doi: 10.1016/j.socscimed.2006.08.002
Claesson, M., Birgander, L. S., Lindahl, B., Nasic, S., Åström, M., Asplund, K., et al. (2005). Women's hearts: stress management for women with ischemic heart disease: explanatory analysis of a randomized controlled trial. J. Cardiopulm. Rehabil. 25, 93–102. doi: 10.1097/00008483-200503000-00009
Clarke, D. A., and Beck, A. T. (2010). Cognitive Therapy of Anxiety Disorders: Science and Practice. New York, NY: Guildford Press.
Cook, S. A., Salmon, P., Dunn, G., Holcombe, C., Comford, P., and Fisher, P. (2015). A prospective study of the association of metacognitive beliefs and processes with persistent emotional distress after diagnosis of cancer. Cognit. Ther. Res. 39, 51–60. doi: 10.1007/s10608-014-9640-x
Cowan, M. J., Pike, K. C., and Budzynski, H. K. (2001). Psychosocial nursing therapy following sudden cardiac arrest: impact on two-year survival. Nurs. Res. 50, 68–76. doi: 10.1097/00006199-200103000-00002
Crabtree, B., and Miller, W. (1999). “A template approach to text analysis: developing and using codebooks,” in Doing Qualitative Research, eds B. Crabtree and W. Miller (Newbury Park, CA: Sage), 163–177.
Creamer, M., Bell, R., and Failla, S. (2003). Psychometric properties of the impact of event scale-revised. Behav. Res. Ther. 41, 1489–1496. doi: 10.1016/j.brat.2003.07.010
Cuijpers, P., Berking, M., Andersson, G., Quigley, L., Kleiboer, A., and Dobson, K. S. (2013). A meta-analysis of cognitive behavioural therapy for adult depression, alone and in comparison with other treatments. Can. J. Psychiatry 58, 376–385. doi: 10.1177/070674371305800702
Dekker, R. L. (2014). Patient perspectives about depressive symptoms in heart failure: a review of the qualitative literature. J. Cardiovasc. Nurs. 29, e9–e15. doi: 10.1097/JCN.0b013e318273a5d6
Dickens, C., Cherrington, A., Adeyemi, I., Roughley, K., Bower, P., Garrett, C., et al. (2013). Characteristics of psychological interventions that improve depression in people with coronary heart disease: a systematic review and meta-regression. Psychosom. Med. 75, 211–221. doi: 10.1097/PSY.0b013e31827ac009
Dickens, C., Cherrington, A., and McGowan, L. (2012). Depression and health-related quality of life in people with coronary heart disease: a systematic review. Eur. J. Cardiovasc. Nurs. 11, 265–275. doi: 10.1177/1474515111430928
Fernie, B. A., Spada, M. M., Chaudhuri, K. R., Kingelhoefer, L., and Brown, R. G. (2015). Thinking about motor fluctuations: an examination of metacognitions in Parkinson's disease. J. Psychosom. Res. 79, 669–673. doi: 10.1016/j.jpsychores.2015.05.001
Fisher, P. L., Byrne, A., and Salmon, P. (2017). Metacognitive therapy for emotional distress in adult cancer survivors: a case series. Cognit. Ther. Res. 41, 891–901. doi: 10.1007/s10608-017-9862-9
Fisher, P. L., McNicol, K., Bridget, Y., Smith, E., and Salmon, P. (2015). Alleviating emotional distress in adolescent and young adult cancer survivors: an open trial of metacognitive therapy. J. Adolesc. Young. Adult. Oncol. 4, 64–69. doi: 10.1089/jayao.2014.0046
Fisher, P. L., and Noble, A. J. (2017). Anxiety and depression in people with epilepsy: the contribution of metacognitive beliefs. Seizure 50, 153–159. doi: 10.1016/j.seizure.2017.06.012
Frasure-Smith, N., Lespérance, F., Gravel, G., Masson, A., Juneau, M., Talajic, M., et al. (2000). Depression and health-care costs during the first year following myocardial infarction. J. Psychosom. Res. 48, 471–478. doi: 10.1016/S0022-3999(99)00088-4
Frasure-Smith, N., and Prince, R. (1989). Long-term follow-up of the ischemic heart disease life stress monitoring program. Psychosom. Med. 51, 485–513.
Freedland, K. E., Skala, J. A., Carney, R. M., Rubin, E. H., Lustman, P. J., Davila-Roman, V. G., et al. (2009). Treatment of depression after coronary artery bypass surgery: a randomized controlled trial. Arch. Gen. Psychol. 66, 387–396. doi: 10.1001/archgenpsychiatry.2009.7
Gehi, A., Haas, D., and Pipkin, S. (2005). Depression and medication adherence in outpatients with coronary heart disease: findings from the heart and soul study. Arch. Intern. Med. 165, 2508–2513. doi: 10.1001/archinte.165.21.2508
Goyal, T. M., Idler, E. L., Krause, T. J., and Contrada, R. J. (2005). Quality of life following cardiac surgery: impact of the severity and course of depressive symptoms. Psychosom. Med. 67, 759–765. doi: 10.1097/01.psy.0000174046.40566.80
Greer, J. A., Park, E. R., Prigerson, H. G., and Safren, S. A. (2010). Tailoring cognitive-behavioural therapy to treat anxiety comorbid with advanced cancer. J. Cogn. Psychother. 24, 294–313. doi: 10.1891/0889-8391.24.4.294
Heart Foundation (2012). Reducing Risk in Heart Disease: An Expert Guide to Clinical Practice for Secondary Prevention of Coronary Heart Disease. Available online at: https://www.heartfoundation.org.au/images/uploads/publications/Reducing-risk-in-heart-disease.pdf
Hofmann, S. G., and Smits, J. A. J. (2008). Cognitive-behavioural therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J. Clin. Psychiatry 69, 621–632. doi: 10.4088/JCP.v69n0415
Irish Association of Cardiac Rehabilitation (2013). Cardiac Rehabilitation Guidelines. Available online at: http://www.iacr.info/wp-content/uploads/2015/03/IACR-Guidelines2013.pdf
Jensen, B. O., and Petersson, K. (2003). The illness experiances of patients after a first time myocardial infarction. Patient. Educ. Couns. 51, 123–131. doi: 10.1016/S0738-3991(02)00196-9
Jeyanantham, K., Kotecha, D., Thanki, D., Dekker, R., and Lane, D. A. (2017). Effects of cognitive behavioural therapy for depression in heart failure patients: a systematic review and meta-analysis. Heart. Fail. Rev. 22, 731–741. doi: 10.1007/s10741-017-9640-5
Koertge, J., Janszky, I., Sundin, O., Blom, M., Georgiades, A., Laszlo, K. D., et al. (2008). Effects of a stress management program on vital exhaustion and depression in women with coronary heart disease: a randomized controlled intervention study. J. Intern. Med. 263, 281–293. doi: 10.1111/j.1365-2796.2007.01887.x
Kollmann, J., Gollwitzer, M., Spada, M. M., and Fernie, B. A. (2016). The association between metacognitions and the impact of fibromyalgia in a German sample. J. Psychosom. Res. 83, 1–9. doi: 10.1016/j.jpsychores.2016.02.002
La Pelle, N. (2004). Simplifying qualitative data analysis using general purpose software tools. Field. Method. 16, 85–108. doi: 10.1177/1525822X03259227
Lespérance, F., Frasure-Smith, N., Talajic, M., and Bourassa, M. G. (2002). Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 105, 1049–1053. doi: 10.1161/hc0902.104707
Levitt, H. M., Motulsky, S. L., Wertz, F. J., Morrow, S. L., and Ponterotto, J. G. (2017). Recommendations for designing and reviewing qualitative research in psychology. Qual. Psychol. 4, 2–22. doi: 10.1037/qup0000082
Lichtman, J. H., Bigger, J. T., Blumenthal, J. A., Frasure-Smith, N., Kaufmann, P. G., Lesperance, F., et al. (2008). Depression and coronary heart disease recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research. Circulation 118, 1768–1775. doi: 10.1161/circulationaha.108.190769
Linden, W. (2013). How many meta-analyses does it take to settle a question? Psychosom. Med. 75, 332–334. doi: 10.1097/PSY.0b013e318295e046
Maher-Edwards, L., Fernie, B. A., Murphy, G., Nikcevic, A. V., and Spada, M. M. (2012). Metacognitive factors in chronic fatigue syndrome. Clin. Psychol. Psychother. 19, 552–557. doi: 10.1002/cpp.757
Maher-Edwards, L., Fernie, B. A., Murphy, G., Wells, A., and Spada, M. M. (2011). Metacognitions and negative emotions as predictors of symptom severity in chronic fatigue syndrome. J. Psychosom. Res. 70, 311–317. doi: 10.1016/j.jpsychores.2010.09.016
McLaughlin, T., Aupont, O., Bambauer, K., Stone, P., Mullan, M., Colagiovanni, J., et al. (2005). Improving psychological adjustment to chronic illness in cardiac patients: the role of depression and anxiety. J. Gen. Intern. Med. 20, 1084–1090. doi: 10.1111/j.1525-1497.2005.00256.x
Merswelken, M., Siebenhuener, S., Orth-Gomer, K., Zimmerman-Viehoff, F., and Deter, H. C. (2011). Treating anxiety in patients with coronary heart disease: a randomized controlled trial. Psychother. Psychosom. 80, 365–370. doi: 10.1159/000329177
Michalsen, A., Grossman, P., Lehmann, N., Knoblauch, N., Paul, A., Moebus, S., et al. (2005). Psychological and quality-of-life outcomes from a comprehensive stress reduction and lifestyle program in patients with coronary artery disease: results of a randomized trial. Psychother. Psychosom. 74, 344–352. doi: 10.1159/000087781
Moore, G., Audrey, S., Barker, M., Bond, L., Bonell, C., Hardeman, W., et al. (2015). Process evaluation of complex interventions: medical Research Council guidance. BMJ 350:h1258. doi: 10.1136/bmj.h1258
Moorey, S., and Greer, S. (2012). Oxford Guide to CBT for People with Cancer. 2nd Edn. New York, NY: Oxford Press.
Müller, J., Hess, J., and Hager, A. (2012). Minor symptoms of depression in patients with congenital heart disease have a larger impact on quality of life than limited exercise capacity. Int. J. Cardiol. 154, 265–269. doi: 10.1016/j.ijcard.2010.09.029
National Institute for Health Care Excellence (2009). Depression in Adults with a Chronic Physical Health Problem: Recognition and Management. Available online at: https://www.nice.org.uk/guidance/cg91/resources/depression-in-adults-with-chronic-physical-health-problem-recognition-and-management-975744316357
National Institute for Health Care Excellence (2011). Generalised Anxiety Disorder and Panic Disorder in Adults: Management. Available online at: https://www.nice.org.uk/guidance/cg113/chapter/1-Guidance
National Institute for Health Care Excellence (2016). Depression in Adults: Recognition and Management. Available online at: https://www.nice.org.uk/guidance/cg90/chapter/Key-priorities-for-implementation
Normann, N., Emmerik, A. A. P., and Morina, N. (2014). The efficacy of metacognitive therapy for anxiety and depression: a meta-analytic review. Depress. Anxiety 31, 402–411. doi: 10.1002/da.22273
O'Cathain, A., Thomas, K. J., Drabble, S. J., and Rudolph, A. (2013). What can qualitative research do for randomised controlled trials? A systematic mapping review. BMJ Open 3:e002889. doi: 10.1136/bmjopen-2013-002889
O'Neil, A., Taylor, B., Hare, D. L., Sanderson, K., Cyril, S., Venugopal, K., et al. (2015). Long-term efficacy of a tele-health intervention for acute coronary syndrome pateints with depression: 12-month results of the Mood Care randomized controlled trial. Eur. J. Prev. Cardiol. 22, 1111–1120. doi: 10.1177/2047487374547655
Onwuegbuzie, A. J., and Leech, N. L. (2007). A call for qualitative power analyses. Qual. Quant. 41, 105–121. doi: 10.1007/s11135-005-1098-1
Purewal, R., and Fisher, P. L. (2018). The contribution of illness perceptions and metacognitive beliefs to anxiety and depression in adults with diabetes. Diabetes. Res. Clin. Pract. 136, 16–22. doi: 10.1016/j.diabres.2017.11.029
Reavell, J., Hopkinson, M. D., Clarkesmith, D., and Lane, D. A. (2018). Effectiveness of cognitive behavioural therapy for depression and anxiety in patients with cardiovascular disease: a systematic review and meta-analysis. Psychosom. Med. 80, 742–753. doi: 10.1097/PSY.0000000000000626
Richards, S. H., Anderson, L., Jenkinson, C. E., Whalley, B., Rees, K., Davies, P., et al. (2017). Psychological interventions for coronary heart disease. Cochrane Database Syst. Rev. 4:CD002902. doi: 10.1002/14651858.CD002902.pub4
Rutledge, T., Redwine, L. S., Linke, S. E., and Mills, P. J. (2013). A meta-analysis of mental health treatments and cardiac rehabilitation for improving clinical outcomes and depression among patients with coronary heart disease. Psychosom. Med. 75, 335–349. doi: 10.1097/PSY.0b013e318291d798
Tang, N. K., Salkovskis, P. M., Hodges, A., Soong, E., Hanna, M. H., and Hester, J. (2009). Chronic pain syndrome associated with health anxiety: a qualitative thematic comparison between pain patients with high and low health anxiety. Br. J. Clin. Psychol. 48, 1–20. doi: 10.1348/014466508X336167
Taylor-Ford, M. (2014). Clinical considerations for working with patients with advanced cancer. J. Clin. Psychol. Med. Settings. 21, 201–213. doi: 10.1007/s10880-014-9398-z
Temple, S. (2017). Brief Cognitive Behaviour Therapy for Cancer Patients: Re-visioning the CBT Paradigm. New York, NY: Routledge.
Thewes, B., Bell, M. L., and Butlow, P. (2013). Fear of cancer reoccurrence in young early-stage breast cancer survivors: the role of metacognitive style and disease-related factors. Psychooncology 22, 2059–2063. doi: 10.1002/pon.3252
Thombs, B. D., Bass, E. B., Ford, D. E., Stewart, K. J., Tsilidis, K. K., Patel, U., et al. (2006). Prevalence of depression in survivors of acute myocardial infarction. J. Gen. Intern. Med. 21, 30–38. doi: 10.1111/j.1525-1497.2005.00269.x
Tully, P. J., Harrison, N. J., Cheung, P., and Cosh, S. (2016). Anxiety and cardiovascular disease risk: a review. Curr. Cardiol. Rep. 18:120. doi: 10.1007/s11886-016-0800-3
Turner, A., Hambridge, J., Baker, A., Bowman, J., and McElduff, P. (2012). Randomized controlled trial of group cognitive behavioural therapy versus brief intervention for depression in cardiac patients. Aust. N. Z. J. Psychiatry. 47, 235–243. doi: 10.1177/0004867412460592
Turner, A., Murphy, B. M., Higgins, R. O., Elliott, P. C., Le Grande, M. R., Gobel, A. J., et al. (2014). An integrated secondary prevention group program reduces depression in cardiac patients. Eur. J. Prev. Cardiol. 21, 153–162. doi: 10.1177/2047487312467747
van de Wal, M. A., Gielissen, M. F. M., Servaes, P., Knoop, H., Speckens, A. E. M., and Prins, J. B. (2015). Study protocol of the SWORD-study: a randomised controlled trial comparing combined online and face-to-face cognitive behaviour therapy versus treatment as usual in managing fear of cancer recurrence. BMC Psychol. 3:12. doi: 10.1186/s403959-015-0068-1
Van Elderen-Van Kemenade, T., Maes, S., and Van den Broek, Y. (1994). Effects of a health education programme with telephone follow-up during cardiac rehabilitation. Br. J. Clin. Psychol. 33, 367–378. doi: 10.1111/j.2044-8260.1994.tb01133.x
Weiss, D. S. (2007). “The impact of event scale: revised,” in Cross-Cultural Assessment of Psychological Trauma, International and Cultural Psychology Series, eds J. P. Wilson and C. S. Tang (Boston, MA: Springer), 219–238.
Wells, A. (1995). Meta-cognition and worry: a cognitive model of generalized anxiety disorder. Behav. Cogn. Psychother. 23, 301–320. doi: 10.1017/S1352465800015897
Wells, A., and Matthews, G. (1996). Modelling cognition in emotional disorder: the S-REF model. Behav Res Ther. 11–12, 881–888. doi: 10.1016/S0005-7967(96)00050-2
Wells, A., McNicol, K., Reeves, D., Salmon, P., Davies, L., Heagerty, A., et al. (2018). Improving the effectiveness of psychological interventions for depression and anxiety in the cardiac rehabilitation pathway using group-based metacognitive therapy (PATHWAY Group MCT): study protocol for a randomised controlled trail. Trials. 19:215. doi: 10.1186/s13063-018-2593-8
Welton, N. J., Caldwell, D. M., Adamopoulos, E., and Vedhara, K. (2009). Mixed treatment comparison meta-analysis of complex interventions: psychological interventions in coronary heart disease. Am. J. Epidemiol. 169, 1158–1165. doi: 10.1093/aje/kwp014
Writing Committee for the ENRICHD Investigators (2003). The effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 289, 3106–3116. doi: 10.1001/jama.289.23.3016
Yohannes, A. M., Wilgoss, T. G., Baldwin, R. C., and Connolly, M. J. (2010). Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. Int. J. Geriatr. Psychiatry 25, 1209–1221. doi: 10.1002/gps.2463
Keywords: Cognitive behavioral therapy, metacognitive therapy, coronary heart disease, depression, anxiety, qualitative
Citation: McPhillips R, Salmon P, Wells A and Fisher P (2019) Qualitative Analysis of Emotional Distress in Cardiac Patients From the Perspectives of Cognitive Behavioral and Metacognitive Theories: Why Might Cognitive Behavioral Therapy Have Limited Benefit, and Might Metacognitive Therapy Be More Effective? Front. Psychol. 9:2288. doi: 10.3389/fpsyg.2018.02288
Received: 03 August 2018; Accepted: 02 November 2018;
Published: 04 January 2019.
Edited by:
Nuno Barbosa Rocha, Escola Superior de Saúde do Porto, Politécnico do Porto, PortugalReviewed by:
Timothy Charles Skinner, University of Copenhagen, DenmarkUlrich Schweiger, Universität zu Lübeck, Germany
Gerald Matthews, University of Central Florida, United States
Copyright © 2019 McPhillips, Salmon, Wells and Fisher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebecca McPhillips, cmViZWNjYS5tY3BoaWxsaXBzQG1hbmNoZXN0ZXIuYWMudWs=