 Mauricio González-Arias
Mauricio González-Arias Agustín Martínez-Molina
Agustín Martínez-Molina Susan Galdames
Susan Galdames Alfonso Urzúa
Alfonso Urzúa
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 12 June 2018
Sec. Emotion Science
Volume 9 - 2018 | https://doi.org/10.3389/fpsyg.2018.00963
This article is part of the Research Topic Research on Emotion and Learning: Contributions from Latin America View all 35 articles
Alexithymia can be defined as inability to identify and describe emotions in the self. Has shown to be related to several psychological and pathological processes that can result in unsatisfactory interpersonal relationships and decreased social adjustment. Advances in research of alexithymia require the development and validation of assessment instruments, and its application to different population. With this aim, we studied the psychometric properties of the Twenty-Item Toronto Alexithymia Scale (TAS-20) in Chilean population using various modeling procedures (e.g., CFA, ESEM) in different structures (i.e., Correlated, Unidimensional, Hierarchical or Wording factors). Among the 10 models tested, the four-dimensional structure offered the best fit but with item-loading problems in the last factor (Pragmatic Thinking). We suggest that the studied version of the scale needs improvement (theoretical and empirical) to ensure optimal indices of validation for Chilean population.
The concept of Alexithymia (Sifneos, 1973) can be defined as cognitive and an affective deficit in the way that some individuals recognize and communicate emotional states (Taylor, 1984). This concept has proved to be related to several psychological and pathological processes such as: interoceptive awareness (Herbert et al., 2011), traumatic memories (Nandrino et al., 2006), suicide risk (De Berardis et al., 2017), depression (Arancibia and Behar, 2015; Melin et al., 2017), eating disorders (Behar et al., 2014), somatoform and conversion disorders (Arancibia et al., 2016), chronic pain (Saariaho et al., 2017) and also psychosomatic illness (Kano and Fukudo, 2013; Porcelli et al., 2017), among others. Resulting in unsatisfactory interpersonal relationships and decreased social adjustment (Taylor and Bagby, 2012). Alexithymia has also been associated with different kinds of addictive disorders, such as pathological gambling (Lumley and Roby, 1995; Maniaci et al., 2017), Internet addiction (Dalbudak et al., 2013; Scimeca et al., 2014), maladaptive sexual behavior (Scimeca et al., 2013), and abnormal illness behavior (Scimeca et al., 2016).
Taylor (1984), basing on a literature review of alexithymia, proposes a scale to measure this construct (Toronto Alexithymia Scale-TAS-26), based on five dimensions: (1) difficulty identifying feelings and distinguishing between feelings and bodily sensations of emotional arousal; (2) difficulty describing feelings to others; (3) externally oriented thinking (or lack of introspection); (4) social conformism and (5) lack of daydreaming and other imaginative activity (Taylor et al., 1985).
Later, Bagby et al. (1994) proposes a revised brief version of this self-report Likert scale: the TAS-20. This scale conserved only the first three traits as factors. In some way, the last two traits remained present in factors 2 and 3 as a more general operatory thinking component oriented to the preference for the external details of everyday life instead of thought content related to inner experience.
TAS-20 has been validated in clinical and non-clinical population, including mental and chronic physical illness. As point out by Taylor et al. (2003), the English version of TAS-20 has been translated to many different languages. In the last years, there have been validation reports in Arabic population (El Abiddine et al., 2017), Chinese population (Zhu et al., 2007), Croatian (Kocijan et al., 2015), Portuguese (Brazil) (Yoshida, 2007), Greek (Tsaousis et al., 2010), Dutch (Adolescents) (Meganck et al., 2012), and Turkish population (Gülec et al., 2009; Bolat et al., 2017). In Latin-American countries there has been reported a Peruvian (Loiselle and Cossette, 2001) and two Mexican versions (Pérez-Rincón et al., 1997; Moral, 2010).
In the psychometric field, the TAS-20 has demonstrated good internal consistency and test–retest reliability. The validation studies yielded to a three-factor structure congruent with the theoretical construct of alexithymia and this structure remains relatively stable in several cultures and languages (Taylor et al., 2003). In addition, it has been shown invariance of the three factors between men and women (Parker et al., 2003). Despite, is also possible to find research reports with results that show good fit indicators for four or more factors models (Tsaousis et al., 2010; Meganck et al., 2012).
Evidence has been found about the possible role of culture in the factorial structure. Culhane et al. (2009), presented evidence of invariance comparing US-Anglo and US-Hispanic student samples. On the opposite, Peruvian (Loiselle and Cossette, 2001) and Mexican (Pérez-Rincón et al., 1997; Moral, 2010) studies showed poorer fit indices. These different findings open the question about the possible role of culture in the factorial structure. The Peruvian sample contrasted a three-factor model using Confirmatory Factor Analysis. These authors reported lack of fit, particularly in the third factor, and they mention as possible reasons that this problematic factor includes 4 negative keyed items (4 of the 5 total, and 4 of 8 of the third factor), which they think it could mean a greater difficulty in answering these items and a low reliance on introspection when describing affective states. With this respect, Fernández-Jiménez et al. (2013) says that these Spanish adaptations of the scale have certain limitations: (a) the Mexican and Peruvian versions present some local particularities in language use, when compared with the Spanish spoken in Spain; (b) Latin-American versions, and the version developed in Spain, contain some items whose back-translation does not adequately reflect the meanings of the original English version of the items; (c) the indices to assess the fit of the proposed models do not meet the standards that are currently recommended (CFI ≥ 0.95, TLI ≥ 0.95, and RMSEA < 0.06; Hu and Bentler, 1999; Schreiber, 2017). Moreover, the size of the sample with which the psychometric properties of Spanish version were supported was tight for some of the tested models according to Wolf et al. (2013) indications.
In Chile, only one undergraduate thesis was found to evaluate the reliability and validity of the TAS-20 in 236 university students in the city of Chillán (Sáez and Tiznado, 2012). However, only a principal component analysis was applied in this study.
Advances in research of alexithymia require the development and validation of assessment instruments, and its application to different population. With this aim, we studied the psychometric properties of the Twenty-Item Toronto Alexithymia Scale (TAS-20), which now is, the most widely used instrument to measure Alexithymia. We have applied this scale to Chilean university students and we performed analysis using different model testing procedures.
A total of 516 students voluntarily participated in this study. Most were female (n = 340, 65.8%, Mean Age = 22; SD = 5.1), and 176 were males (34.2%, Mean Age = 22; SD = 3.7). 54.7% (n = 282) of the students were from the cities of La Serena and Coquimbo, 8.9% (n = 46) from Iquique, 9.1% (n = 47) from Antofagasta, 8.1% (n = 42) from Santiago, 9.5% (n = 49) from Temuco and 9.7% (n = 50) from Punta Arenas, throughout Chile. They all spoke Spanish as their mother tongue.
The English version of the TAS 20 (see Table 1; Meganck et al., 2008) was translated and adapted to the Spanish language following the international guidelines (Hambleton, 1994; International Test Commission, 2010).
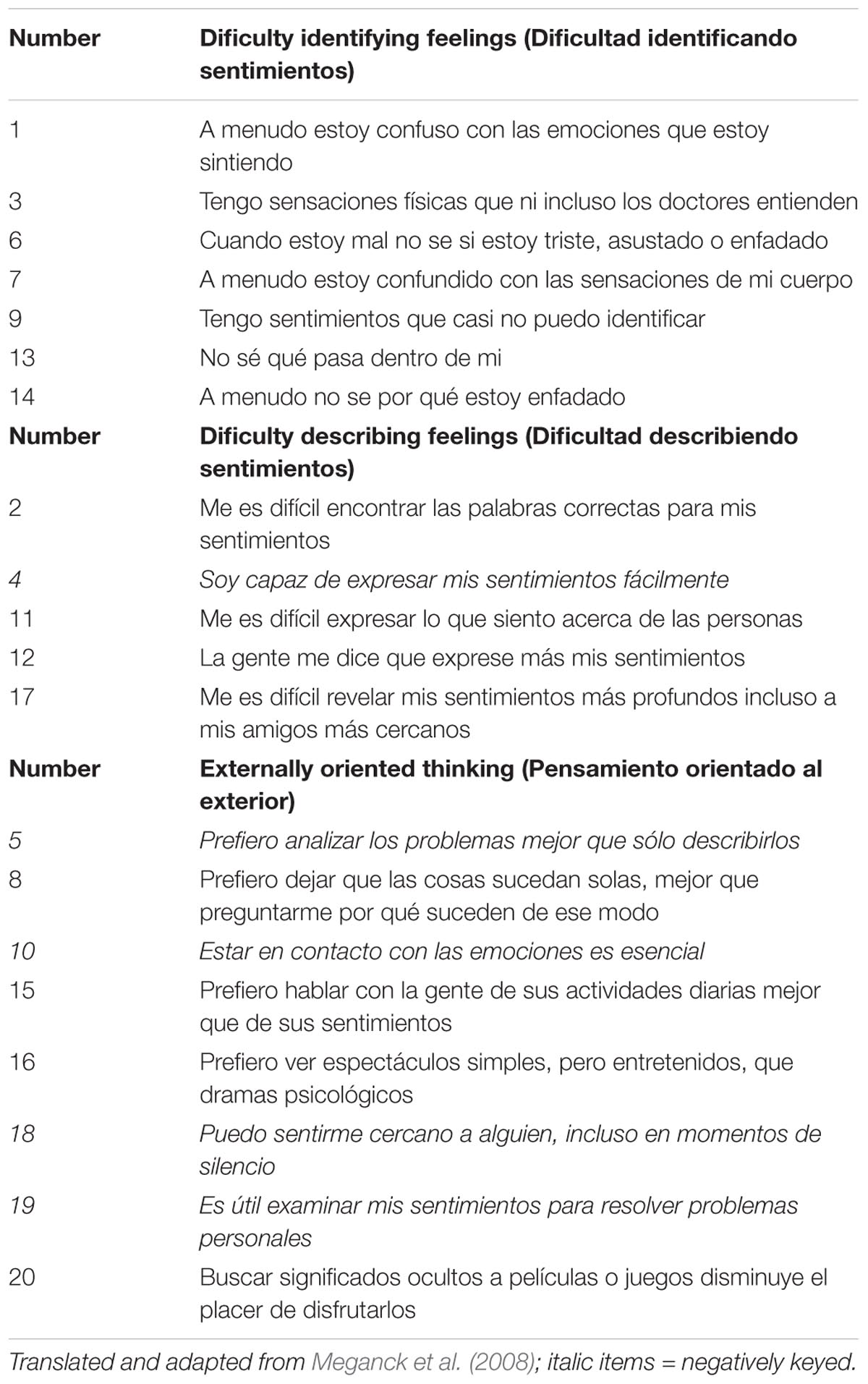
TABLE 1. Items of the TAS-20 Spanish version.
This Spanish version of TAS-20 includes 20 self-report questions distributed into three subscales: (1) difficulty identifying feelings and distinguishing between feelings and bodily sensations in emotional activation, (2) difficulty in the verbal expression of emotions, and (3) externally oriented thinking. The answers values fluctuate between 1 and 5 points (1 is the lack of it and 5 is most present), and items 4, 5, 10, 18, and 19 must be inverted before adding up scores. Total score interval is 20–100, while a person is considered alexithymic with a score ≥ 61.
The students voluntarily completed the scales after reading and written informed consents. All procedures in this study followed (a) the principles of Helsinki Declaration (World Medical Association, 2013), (b) the APA ethical standards (Including 2010 and 2016 Amendments), and (c) the guidelines of the National Commission for Scientific and Technological Research of Chile (CONICYT). There were no missing data in this study.
The six basic models tested by Meganck et al. (2008, 2012) were compared using Confirmatory Factor analysis (see Table 2). The first Model (a) is proposed as a unidimensional structure where all items reflect alexithymia. Model (b) is a two-factor structure with DIF and DDF items forming one factor and EOT items forming the second factor (Haviland and Reise, 1996; Loas et al., 1996; Erni et al., 1997). Model (c) (Kooiman et al., 2002) proposed the same structure of model (b) but with only 16 items (items 16, 17, 18, and 20 were erased). The fourth model (d) is composed by three factors: DIF, DDF, and EOT (Bagby et al., 1994) and the fifth model (e) is a three-factor solution (Ritz and Kannapin, 2000); DIF and DDF items as one factor and EOT split into two factors (PR and IM). Finally, the sixth model (f) is a four-factor solution that considers the dimensions DIF and DDF plus de sub-dimensions PR and IM that were split from EOT (Müller et al., 2003).
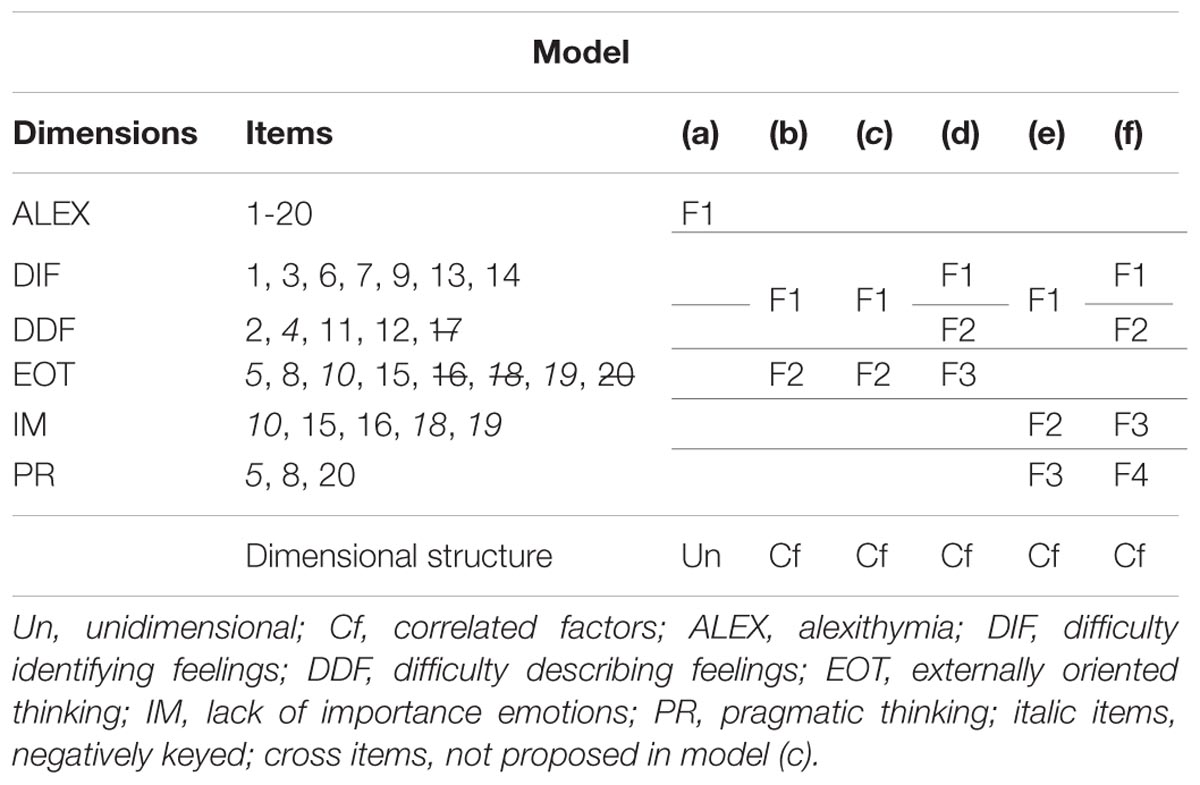
TABLE 2. Basic models of the TAS-20 (proposed in previous literature).
Further models were also tested in this study for those models described above that provided adequate fit to data: hierarchical (Hi), wording factor (Wf), and exploratory structural exploratory models (ESEMs). When the relationship between first-order factors is high, hierarchical models of indirect effects could be proposed. The Hi second-order structure was tested with the general alexithymia concept as a higher level.
The choice of one model or another is a theoretical, applied, and parsimony-based decision. The Wf was tested as an orthogonal method factor (bifactor) on which the negatively keyed items are located (4, 5, 10, 18, and 19). Finally, ESEM approach integrates the flexibility of EFA and the advantages of CFA (Asparouhov and Muthén, 2009; Garrido et al., in press). Even if these models are not contemplated in the classical frameworks (models 1–6), the exploratory approach could end up suggesting a more efficient latent structure than those that have been derived from previous studies (e.g., less or specific dimensions in a bifactor structure; Arias et al., 2016).
We firstly explored the reliability and adequacy of factor analysis indices for each TAS-20 scale. These statistics were: the explained proportion of variance (PEV), Barlett’s test and KMO index for the adequacy of the analysis, the number of advised dimensions in each scale with the parallel analysis technique (Garrido et al., 2013), Cronbach’s α and McDonald’s ω as an estimate of the reliability. For this purpose, we employed an unweighted least-squares (ULS) estimator based on polichoric correlations because of the ordinal nature of data. The use of robust estimators as ULS are recommended because they may produce more accurate parameter estimates than Maximum Likelihood (Forero et al., 2009; Schmitt, 2011; Li, 2014). If necessary an oblique rotation was used because of possible secondary and related dimensions (Promin; salient larger values > 0.30; Lorenzo-Seva, 1999).
In addition to the descriptive and complementary factorial indices of the scales, different latent structures were tested (CFA and ESEM). These models were executed using the same factorial considerations as the previous (polichoric correlations and ULSMV estimator available in Mplus version 7.4). Cut-off point recommendations of Schreiber (2017) were followed for goodness of fit indices criteria: CFI ≥ 0.95, TLI ≥ 0.95, and RMSEA < 0.06.
Table 3 shows descriptive statistics computed with SPSS 22. The average values of the scales showed a similar central tendency to those reported by previous studies for students (Taylor et al., 2003; Meganck et al., 2012). However, the variance of the items was slightly higher in the sample of Chilean students. The most closely related scales were DIF and DDF on the one hand, and IM and PR on the other.
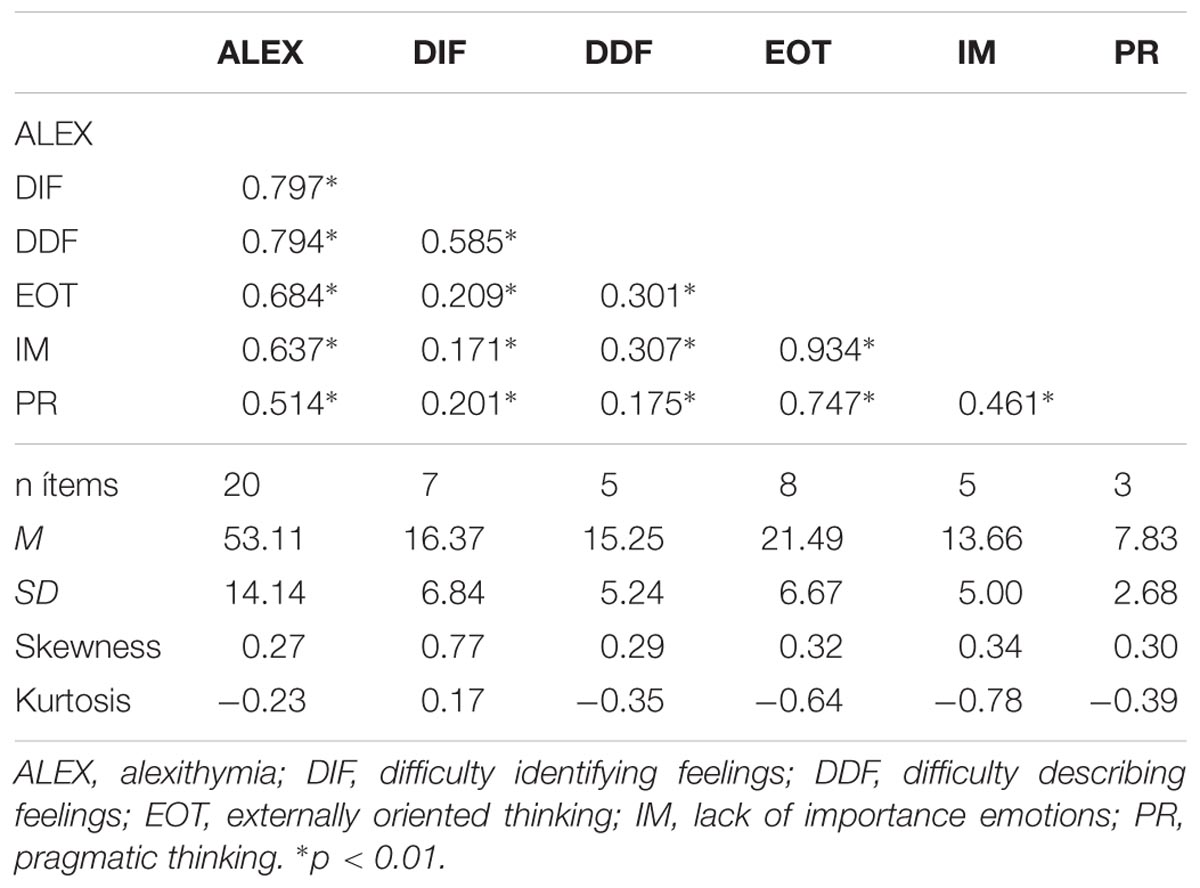
TABLE 3. Descriptive statistics and Pearson correlations for the TAS-20 scales.
DIF and DDF proposed scales (Table 4) had good exploratory values to be considered as possible single dimensions (one advised dimension per scale, adequate proportions of explained variance, Bartlett test p < 0.01 and KMO ≥ 0.8; Lorenzo-Seva and Ferrando, 2013). EOT, IM, and PR scales did not have adequate exploratory values to be considered as possible single dimensions. It should be noted its lack of reliability (α or ω < 0.70). Note that these factors reflect a small number of items (especially PR).
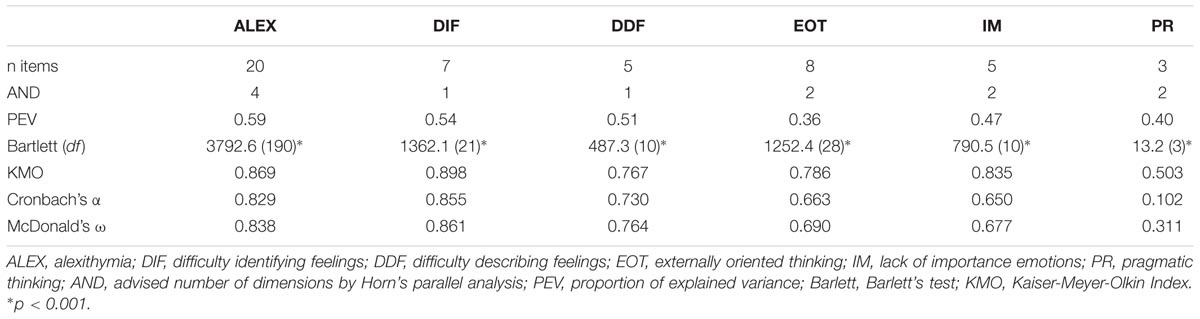
TABLE 4. Reliability and adequacy factor analysis indices for the TAS-20 proposed scales.
Reliability indices of the TAS-20 scales were similar to those reported by Bagby et al. (1994) and Meganck et al. (2012). Both DIF and DDF tend to show good magnitudes of reliability, whereas EOT (and its sub-factors IM and PR), as previous studies, showed inadequate reliability indices (<0.80).
All confirmatory modeling analyzes on the basic models reported poor or not adequate fit indices (Table 5). Only models (c) and (f) reached an acceptable CFI value (>0.90). Models (d) and (f) referred the lowest RMSEA. In relation to the other basic models and considering the set of indicators (χ2, RMSEA, CFI, and TLI), the best structure for these datasets was four correlated factors (f).
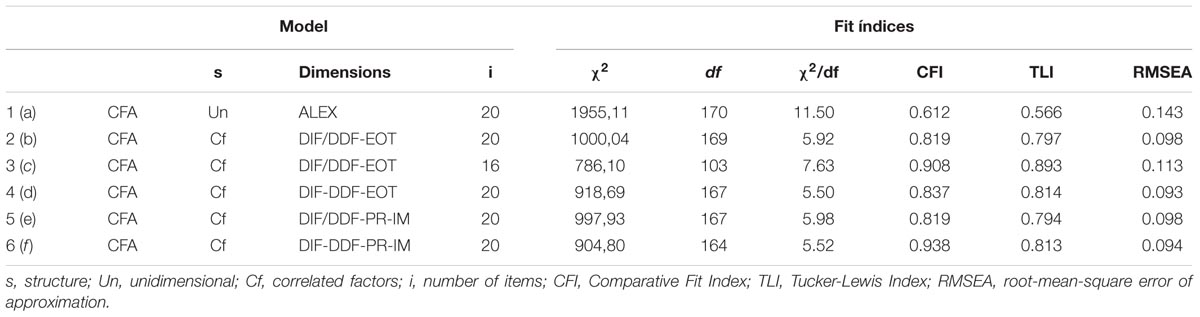
TABLE 5. Fit indices for the basic models of the TAS-20.
We also tested two bifactor models with the purpose of exploring other dimensional structures (correlated and uncorrelated specific factors together with a general factor of alexithymia). These tested solutions were uninterpretable, that is, poor fit indices (i.e., RMSEA > 0.10) and mostly low or negative factor loadings.
CFA analysis considering Hi or Wf structures in model (f) did not meet acceptable fit indices. As expected, the alternative ESEM approach of the TAS-20 was supported by good fit indices (χ2/df < 0.3, RMSEA < 0.06, CFI and TLI > 0.90). Although not shown in Table 6, the rest of the basic models (a–e) were also tested with an ESEM approach. None of these models reported better ESEM fit indices than the (f).
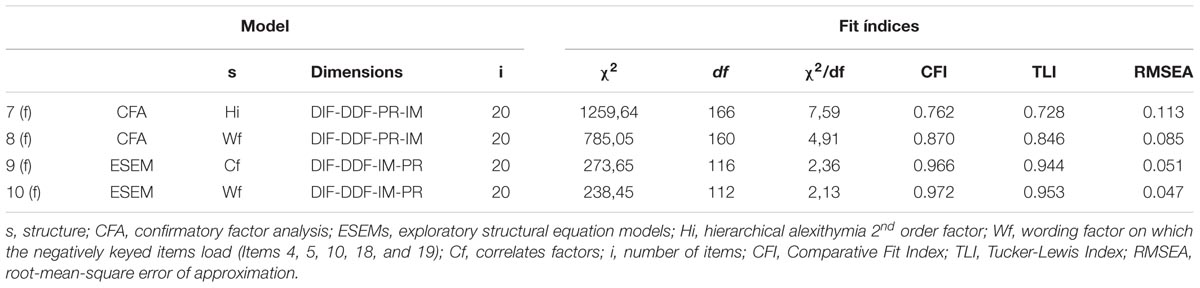
TABLE 6. Fit indices for the alternative structures of the TAS-20.
Table 7 shows the estimates of model 10 (f) (with the best fit-indices among the tested). In the table we can see clearly how the estimates loaded mainly in their corresponding factors (≥0.30) except for the fourth factor. PR was defined mainly by one loading (20) and two cross-loadings (15 and 16). Item 8 did not load substantially on any factor of the extracted ones.
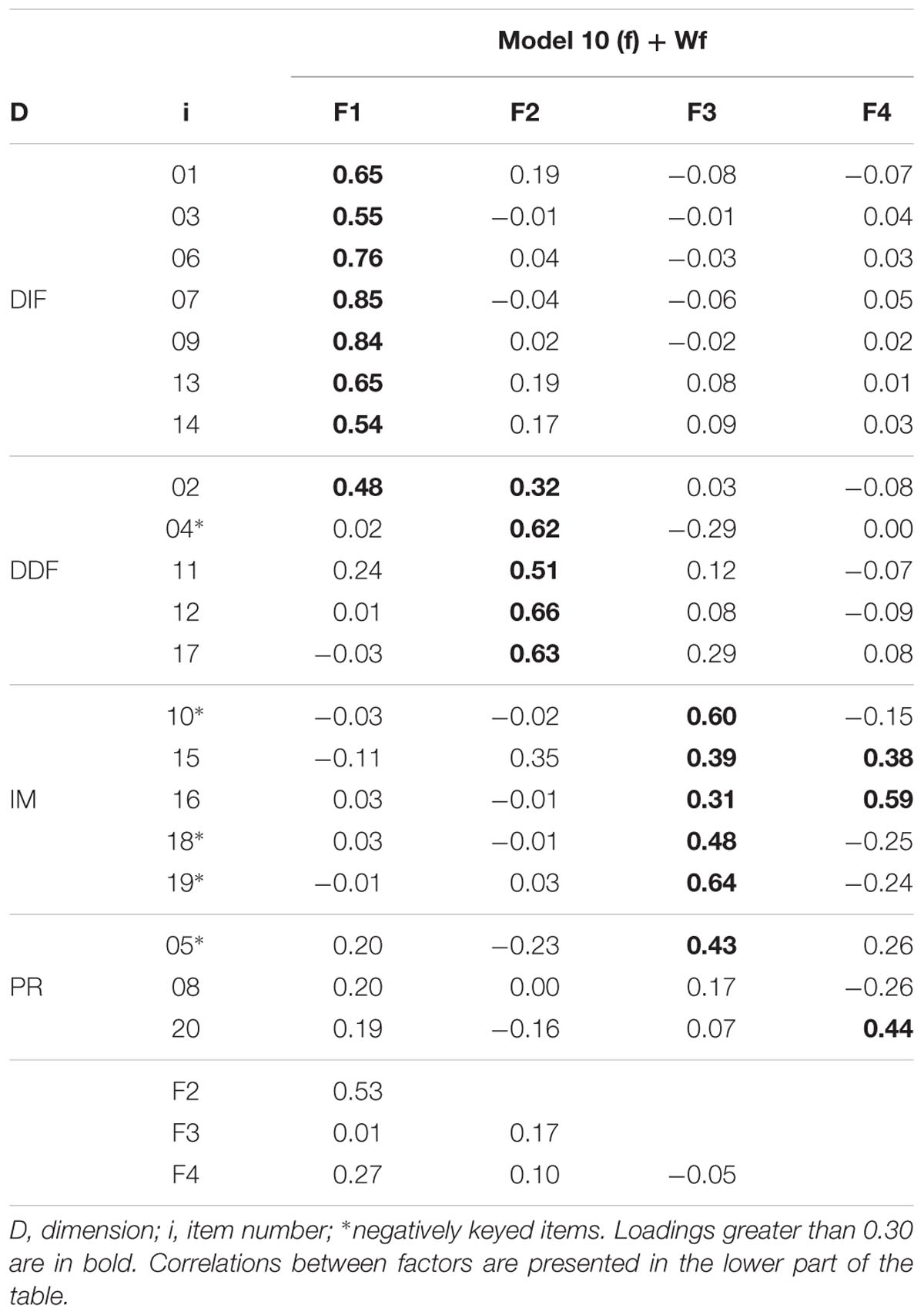
TABLE 7. ESEM estimates for (f) + Wording factor.
A Chilean version of TAS-20 has been studied and the results show evidence of its reliability and construct validity, detecting some problems that must be addressed in future studies (e.g., items 5, 8, and 15 could be complicated to translate into Spanish because it requires the interpretation of “mejor que” [best than] in the sense of “en vez de” [instead of]; or item 10 in our culture the meaning of “estar en contacto” could be interpreted as a more concrete physical touch and therefore its comprehension requires the capacity to understand a metaphor, which is not of a common sense use).
Among the 10 tested models, including a unidimensional factor or the combination of different factors, we only found relatively good fit estimates for a model of four factors. These results do not follow the direction of some previous studies in English speaking population (that support a three-factor structure). They rather show consistency with the results observed in Latino-American population reported by Loiselle and Cossette (2001) in a Peruvian sample and Moral (2010) in a Mexican sample. Compared to these studies there is also a difference to be considered, that is, the fourth factor shows weaker indices of fit in our study. As a possible explanation of differences, we adhere to Taylor et al. (2003) hypothesis that points out that differences between Latino-American and Anglo-American population could be due to translation problems or related to cultural aspects of alexithymia in Latino-American population. The third factor structure not only has been problematic in Latinamerica. Moreover, this can be enhanced by (a) respondent’s low reading comprehension skills, particularly affecting negatively keyed items and those that include more abstract ideas, (b) a culture that is not used to make verbal language distinctions between “internal and external” world, and (c) the presence of patriarchal cultural beliefs that contradict the idea of affectivity as a positive domain. These beliefs usually see emotions as dangerous and to be controlled (Arón, 2001; Blanco and De la Corte, 2003).
On the other hand, it could be as in previous studies, that the psychometric properties of some factors were not adequate (Zhu et al., 2007). For this reason, it is understandable that structures modeled with CFA forcing IM and PR dimensions regularly show inadequate adjustment. As an alternative analysis, (f) ESEM model showed the best-fit indices in comparison with previous studies. In this sense the work of Craparo et al. (2015) already showed an oblique solution that substantially improves the fit of a TAS-20 structure.
The improvements that we recommend include the revision of dimensions IM and PR items, particularly item number 8, for its lack of load on the extracted factors. It may be necessary to reduce the scale. Gori et al. (2012) measured alexithymia and reported good reliability and validity indices with only five items (the PTI-Alexithymia Scale; “PTI-AS”). The PTI-AS highly correlates with TAS-20.
A limitation of this study is that the sample includes only university students, so it is not generalizable to the entire population and it is not directly comparable with studies performed with samples of young adolescents or clinical population. Given the use of a non-probabilistic and homogeneous sample for this study, more empirical support of the proposed factorial solution of this study with Chilean samples is necessary (e.g., young adolescents or clinical population).
We found evidence that reliability and construct validity of TAS-20 are not optimal for Chilean student population. Factor analysis shows a structure of four-factor model being the best fit, but with problems in the fourth factor. Therefore, we suggest that the studied version of the scale needs improvement to ensure optimal indices of validation for Chilean population.
MG-A led the project and made part of the Introduction, Method, and Discussion. AM-M made part of the Introduction and the Discussion and led Method and Results. SG made part of the Introduction, part of the Method, and part of the Discussion. AU made part of the Introduction and the Discussion and led part of the Method.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Arancibia, M., and Behar, R. (2015). Alexitimia y depresión: evidencia, controversias e implicancias. Rev. Chil. Neuro Psiquiatría 53, 24–34. doi: 10.4067/S0717-92272015000100004
Arancibia, M., Sepúlveda, E., Martínez-Aguayo, J., and Behar, R. (2016). Current state of somatoform and conversion disorders in children and adolescents. Rev. Chil. Neuro Psiquiatría 54, 151–161.
Arias, V. B., Ponce, F. P., Martínez-Molina, A., Arias, B., and Núñez, D. (2016). General and specific attention-deficit/hyperactivity disorder factors of children 4 to 6 years of age: an exploratory structural equation modeling approach to assessing symptom multidimensionality. J. Abnorm. Psychol. 125, 125–137. doi: 10.1037/abn0000115
Arón, A. (2001). Violencia en la Familia. Programa de Intervención en Red: La Experiencia de San Bernardo. Santiago: Galdoc.
Asparouhov, T., and Muthén, B. (2009). Exploratory structural equation modeling. Struct. Equ. Modeling 16, 397–438. doi: 10.1080/10705510903008204
Bagby, R. M., Parker, J. D., and Taylor, G. J. (1994). The twenty-item Toronto Alexithymia Scale-I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 38, 23–32. doi: 10.1016/0022-3999(94)90005-1
Behar, R., Gramegna, G., and Arancibia, M. (2014). Perfeccionismo e insatisfacción corporal en los trastornos de la conducta alimentaria. Rev. Chil. Neuro Psiquiatría 52, 103–114. doi: 10.4067/S0717-92272014000200006
Blanco, A., and De la Corte, L. (2003). Poder, Ideología y Violencia: Ignacio Martín Baró. Madrid: Trotta.
Bolat, N., Yavuz, M., Eliaçik, K., Zorlu, A., Evren, C., and Köse, S. (2017). Psychometric properties of the 20-Item Toronto Alexithymia Scale in a Turkish adolescent sample. Anatol. J. Psychiatry 18, 362–368. doi: 10.5455/apd.239284
Craparo, G., Faraci, P., and Gori, A. (2015). Psychometric properties of the 20-item Toronto Alexithymia Scale in a group of Italian younger adolescents. Psychiatry Investig. 12, 500–507. doi: 10.4306/pi.2015.12.4.500
Culhane, S. E., Morera, O. F., Watson, P. J., and Millsap, R. E. (2009). Assesing measurement and predictive invariance of the Toronto Alexithymia Scale-20 in U.S. Anglo and U.S. Hispanic student samples. J. Pers. Assess. 91, 387–395. doi: 10.1080/00223890902936264
Dalbudak, E., Evren, C., Aldemir, S., Coskun, K. S., Ugurlu, H., and Yildirim, F. G. (2013). Relationship of internet addiction severity with depression, anxiety, and alexithymia, temperament and character in university students. Cyberpsychol. Behav. Soc. Netw. 16, 272–278. doi: 10.1089/cyber.2012.0390
De Berardis, D., Fornaro, M., Orsolini, L., Valchera, A., Carano, A., Vellante, F., et al. (2017). Alexithymia and suicide risk in psychiatric disorders: a mini-review. Front. Psychiatry 8:148. doi: 10.3389/fpsyt.2017.00148
El Abiddine, F. Z., Dave, H., Aldhafri, S., El-Astal, S., Hemaid, F., and Parker, J. (2017). Cross-validation of the 20-item Toronto Alexithymia Scale: results from an Arabic multicenter study. Pers. Individ. Dif. 113, 219–222. doi: 10.1016/j.paid.2017.03.017
Erni, T., Lotscher, K., and Modestin, J. (1997). Two-factor solution of the 20-item Toronto Alexithymia Scale confirmed. Psychopathology 30, 335–340. doi: 10.1159/000285079
Fernández-Jiménez, E., Pérez-San-Gregorio, M., Taylor, G., Bagby, R., Ayearst, L., and Izquierdo, G. (2013). Psychometric properties of a revised Spanish 20-item Toronto Alexithymia Scale adaptation in multiple sclerosis patients. Int. J. Clin. Health Psychol. 13, 226–234. doi: 10.1016/S1697-2600(13)70027-9
Forero, C. G., Maydeu-Olivares, A., and Gallardo-Pujol, D. (2009). Factor analysis with ordinal indicators: a Monte Carlo study comparing DWLS and ULS estimation. Struct. Equ. Modeling 16, 625–641. doi: 10.1080/10705510903203573
Garrido, L. E., Abad, F. J., and Ponsoda, V. (2013). A new look at Horn’s parallel analysis with ordinal variables. Psychol. Methods 18, 454–474. doi: 10.1037/a0030005
Garrido, L. E., Barrada, J. R., Aguasvivas, J. A., Martínez-Molina, A., Arias, V. B., Golino, H., et al. (in press). Is small still beautiful for the strengths and difficulties questionnaire? Novel findings using exploratory structural equation modeling. Assessment.
Gori, A., Giannini, M., Palmieri, G., Salvini, R., and Schuldberg, D. (2012). Assessment of alexithymia: psychometric properties of the psychological treatment Inventory-Alexithymia Scale (PTI-AS). Psychology 3, 231–236. doi: 10.4236/psych.2012.33032
Gülec, H., Köse, S., Gülec, M. Y., Citak, S., Evren, C., Borckardt, J., et al. (2009). Reliability and factorial validity of the Turkish version of the 20-item Toronto Alexithymia Scale (TAS-20). Bull. Clin. Psychopharmacol. 19, 214–220.
Hambleton, R. (1994). Guidelines for adapting educational and psychological tests: a progress report. Eur. J. Psychol. Assess. 10, 229–244.
Haviland, M. G., and Reise, S. P. (1996). Structure of the twenty-item Toronto Alexithymia Scale. J. Pers. Assess. 66, 116–125. doi: 10.1207/s15327752jpa6601_9
Herbert, B., Herbert, C., and Pollatos, O. (2011). On the relationship between interoceptive awareness and alexithymia: is interoceptive awareness related to emotional awareness? J. Pers. 79, 1149–1175. doi: 10.1111/j.1467-6494.2011.00717.x
Hu, L., and Bentler, P. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Modeling 6, 1–55. doi: 10.1080/10705519909540118
International Test Commission (2010). International Test Commission Guidelines for Translating and Adapting Tests. Available at: http://www.intestcom.org
Kano, M., and Fukudo, S. (2013). The alexithymic brain: the neural pathways linking alexithymia to physical disorders. Biopsychosoc. Med. 7:1. doi: 10.1186/1751-0759-7-1
Kocijan, S., Gelo, J., and Karlovié, D. (2015). Validation study of the Toronto Alexithymia Scale (TAS-26) in croatian population. Acta Clin. Croat. 54, 272–278.
Kooiman, C. G., Spinhoven, P., and Trijsburg, R. W. (2002). The assessment of alexithymia. A critical review of the literature and a psychometric study of the Toronto Alexithymia Scale-20. J. Psychosom. Res. 53, 1083–1090. doi: 10.1016/S0022-3999(02)00348-3
Li, C. H. (2014). The Performance of MLR, USLMV, and WLSMV Estimation in Structural Regression Models with Ordinal Variables. Doctoral dissertation, Michigan State University, East Lansing, MI.
Loas, G., Otmani, O., Verrier, A., Fremaux, D., and Marchand, M. P. (1996). Factor analysis of the French version of the 20-item Toronto Alexithymia Scale. Psychopathology 29, 139–144. doi: 10.1159/000284983
Loiselle, C. G., and Cossette, S. (2001). Cross-cultural validation of the Toronto Alexithymia Scale (TAS-20) in U.S. and Peruvian populations. Transcult. Psychiatry 38, 348–362. doi: 10.1177/136346150103800305
Lorenzo-Seva, U. (1999). Promin: a method for oblique factor rotation. Multivariate Behav. Res. 34, 347–365. doi: 10.1207/S15327906MBR3403_3
Lorenzo-Seva, U., and Ferrando, P. J. (2013). FACTOR 9.2: a comprehensive program for fitting exploratory and semi-confirmatory factor analysis and IRT models. Appl. Psychol. Meas. 37, 497–498. doi: 10.1177/0146621613487794
Lumley, M. A., and Roby, K. J. (1995). Alexithymia and pathological gambling. Psychother. Psychosom. 63, 201–206. doi: 10.1159/000288960
Maniaci, G., Picone, F., van Holst, R. J., Bolloni, C., Scardina, S., and Cannizzaro, C. (2017). Alterations in the emotional regulation process in gambling addiction: the role of anger and alexithymia. J. Gambl. Stud. 33, 633–647. doi: 10.1007/s10899-016-9636-4
Meganck, R., Markey, S., and Vanheule, S. (2012). Reliability and factor structure in an adolescent sample of the Dutch 20-item Toronto Alexithymia Scale. Psychol. Rep. 111, 393–404. doi: 10.2466/02.08.15.PR0.111.5.393-404
Meganck, R., Vanheule, S., and Desmet, M. (2008). Factorial validity and measurement invariance of the 20-item Toronto Alexithymia Scale in clinical and nonclinical samples. Assessment 15, 36–47. doi: 10.1177/1073191107306140
Melin, E., Thunander, M., Landin-Olsson, M., Hillman, M., and Thulesius, H. (2017). Depression differed by midnight cortisol secretion, alexithymia and anxiety between diabetes types: a cross sectional comparison. BMC Psychiatry 17:335. doi: 10.1186/s12888-017-1495-8
Moral, J. (2010). Factor structure and reliability of TAS-20 in Mexican samples. Int. J. Hisp. Psychol. 2, 163–176.
Müller, J., Bühner, M., and Ellgring, H. (2003). Is there a reliable factorial structure in the 20-item Toronto Alexithymia Scale? A comparison of factor models in clinical and normal adult samples. J. Psychosom. Res. 55, 561–568. doi: 10.1016/S0022-3999(03)00033-3
Nandrino, J. L., Doba, K., Lesnef, A., Christophe, V., and Pezard, L. (2006). Autobiographical memory deficit in anorexia nervosa: emotion regulation and effect of duration of illness. J. Psychosom. Res. 61, 537–543. doi: 10.1016/j.jpsychores.2006.02.008
Parker, J. D., Taylor, G. J., and Bagby, R. M. (2003). The 20-Item Toronto Alexitimia Scale III. Reliability and factorial validity in a community population. J. Psychosom. Res. 55, 269–275. doi: 10.1016/S0022-3999(02)00578-0
Pérez-Rincón, H., Cortés, J., Ortiz, S., Peña, J., Ruiz, J., and Díaz-Martínez, A. (1997). Validación y estandarización de la versión española de la escala modificada de Alexitimia de Toronto. Salud Ment. 20, 30–34.
Porcelli, P., de Carne, M., and Leandro, G. (2017). The role of alexithymia and gastrointestinal-specific anxiety as predictors of treatment outcome in irritable bowel syndrome. Compr. Psychiatry 73, 127–135. doi: 10.1016/j.comppsych.2016.11.010
Ritz, T., and Kannapin, O. (2000). Zur konstruktvalidität einer Deutschen fassung der Toronto Alexithymia Scale [Construct validity of a German version of the Toronto Alexithymia Scale]. Z. Differ. Diagn. Psychol. 21, 49–64. doi: 10.1024//0170-1789.21.1.49
Saariaho, A., Saariaho, T., Mattila, A., Ohtonen, P., Joukamaa, M., and Karukivi, M. (2017). Alexithymia and depression in the recovery of chronic pain patients: a follow-up study. Nord. J. Psychiatry 71, 262–269. doi: 10.1080/08039488.2016.1275782
Sáez, C. A., and Tiznado, G. D. (2012). Validación de la Escala de Alexitimia de Toronto Versión Española (TAS – 20) (Tesis Para Optar al Grado de PSICÓLOGO). Chillán: Universidad del Bío-Bío.
Schmitt, T. A. (2011). Current methodological considerations in exploratory and confirmatory factor analysis. J. Psychoeduc. Assess. 29, 304–321. doi: 10.1177/0734282911406653
Schreiber, J. B. (2017). Update to core reporting practices in structural equation modeling. Res. Soc. Adm. Pharm. 13, 634–643. doi: 10.1016/j.sapharm.2016.06.006
Scimeca, G., Bruno, A., Cava, L., Pandolfo, G., Muscatello, M. R. A., and Zoccali, R. (2014). The relationship between alexithymia, anxiety, depression, and internet addiction severity in a sample of Italian high school students. Sci. World J. 2014:504376. doi: 10.1155/2014/504376
Scimeca, G., Bruno, A., Crucitti, M., Conti, C., Quattrone, D., Pandolfo, G., et al. (2016). Abnormal illness behavior and Internet addiction severity: the role of disease conviction, irritability, and alexithymia. J. Behav. Addict. 6, 92–97. doi: 10.1556/2006.6.2017.008
Scimeca, G., Bruno, A., Pandolfo, G., Micò, U., Romeo, V. M., Abenavoli, E., et al. (2013). Alexithymia, negative emotions, and sexual behavior in heterosexual university students from Italy. Arch. Sex. Behav. 42, 117–127. doi: 10.1007/s10508-012-0006-8
Sifneos, P. (1973). The prevalence of alexithymic characteristics in psychosomatic patients. Psychother. Psychosom. 22, 255–262. doi: 10.1159/000286529
Taylor, G. J. (1984). Alexithymia: concept, measurement, and implications for treatment. Am. J. Psychiatry 141, 725–732. doi: 10.1176/ajp.141.6.725
Taylor, G. J., and Bagby, R. M. (2012). “The alexithymia personality dimension,” in The Oxford Handbook of Personality Disorders, ed. T. A. Widiger (New York, NY: Oxford University Press), 648–673. doi: 10.1093/oxfordhb/9780199735013.013.0030
Taylor, G. J., Bagby, R. M., and Parker, J. D. (2003). The 20-item Toronto Alexithymia Scale IV. Reliability and factorial validity in different languages and cultures. J. Psychosom. Res. 55, 277–283. doi: 10.1016/S0022-3999(02)00601-3
Taylor, G. J., Ryan, D., and Bagby, R. M. (1985). Toward the development of a new self- report alexithymia scale. Psychother. Psychosom. 44, 191–199. doi: 10.1159/000287912
Tsaousis, I., Taylor, G., Quilty, L., Georgiades, S., Stavrogiannopouos, M., and Bagby, R. M. (2010). Validation of a Greek adaptation of the 20-items Toronto Alexithymia Scale. Compr. Psychiatry 51, 443–448. doi: 10.1016/j.comppsych.2009.09.005
Wolf, E. J., Harrington, K. M., Clark, S. L., and Miller, M. W. (2013). Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ. Psychol. Meas. 73, 913–934. doi: 10.1177/0013164413495237
World Medical Association. (2013). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. doi: 10.1001/jama.2013.281053
Yoshida, E. M. (2007). Validade da versao em portuues da Toronto Alexitimia Scale-TAS em amostra clínica. Psicol. Reflexao Crít. 20, 389–396. doi: 10.1590/S0102-79722007000300006
Keywords: alexithymia, emotion, TAS-20, psychometric properties, ESEM, wording factor
Citation: González-Arias M, Martínez-Molina A, Galdames S and Urzúa A (2018) Psychometric Properties of the 20-Item Toronto Alexithymia Scale in the Chilean Population. Front. Psychol. 9:963. doi: 10.3389/fpsyg.2018.00963
Received: 29 January 2018; Accepted: 24 May 2018;
Published: 12 June 2018.
Edited by:
Carlos Gantiva, University of San Buenaventura, ColombiaReviewed by:
Ioannis Tsaousis, University of Crete, GreeceCopyright © 2018 González-Arias, Martínez-Molina, Galdames and Urzúa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agustín Martínez-Molina, YWd1c3RpbkB1bml6YXIuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.