 Ricardo Fueyo-Díaz1,2*
Ricardo Fueyo-Díaz1,2* Rosa Magallón-Botaya1,3
Rosa Magallón-Botaya1,3 Santiago Gascón-Santos1,2
Santiago Gascón-Santos1,2 Ángela Asensio-Martínez1,2
Ángela Asensio-Martínez1,2 Guillermo Palacios-Navarro4
Guillermo Palacios-Navarro4 Juan J. Sebastián-Domingo1,3,5
Juan J. Sebastián-Domingo1,3,5- 1Aragon Institute of Health Sciences IACS, Zaragoza, Spain
- 2Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain
- 3Department of Medicine, Psychiatry and Dermatology, University of Zaragoza, Zaragoza, Spain
- 4Department of Electronic Engineering and Communications, University of Zaragoza, Zaragoza, Spain
- 5Department of Digestive Diseases, Hospital Royo Villanova, Zaragoza, Spain
The aim of this study was to develop a scale to assess the levels of specific self-efficacy in order to enhance adherence to a gluten-free diet and the life quality of celiac patients. Celiac disease is a chronic small intestinal immune-mediated enteropathy precipitated by exposure to dietary gluten in genetically predisposed people. The only treatment is a strict lifelong gluten-free diet. Within the framework of Social Cognitive Theory, expectation of self-efficacy is understood as the degree in which a person believes himself to be capable of performing a certain task (e.g., adhering to a gluten-free diet), a construct which has been widely studied in its relation with adopting healthy behaviors, but scarcely in relation to celiac disease. A validation study was carried out in various stages: preparation of the protocol; construction of the questionnaire and a pilot run with 20 patients; validation of the scale with 563 patients and statistical analysis. A 25-item scale was developed. Feasibility was excellent (99.82% of participants completed all the questions). Factorial analysis pointed to the existence of five factors that explained 70.98% of the variance with a Cronbach alpha of 0.81 for the scale overall and between 0.64 and 0.90 for each factor. The scale showed a Spearman's Rho coefficient of 0.279 with the General self-efficacy Scale. This easily administered scale provides good psychometric properties for evaluating specific self-efficacy of celiac patients in adhering to treatment. It seeks to be the first scale that provides not only a measurement of specific self-efficacy in celiac disease, but also to determine its levels for each of the areas as a first step toward designing interventions of self-management and empowerment programs to cope with the disease.
Introduction
Celiac disease (CD) is a chronic small intestinal immune-mediated enteropathy precipitated by exposure to dietary gluten in genetically predisposed people (Ludvigsson et al., 2013). Numerous studies report a prevalence of between 1:67 and 1:250, for the USA and Europe (Leffler et al., 2008), while 1:100 is a widely accepted figure (Catassi et al., 2007). The only valid treatment known today is a lifelong strict gluten-free diet (GFD). Despite the benefits of a GFD, rates for strict adherence range from 42 to 91% depending on definition and method of assessment (Hall et al., 2009).
Within Social Cognitive Theory, Bandura defines self-efficacy as “beliefs in one's capabilities to organize and execute the course of action required to produce given attainments” (Bandura, 1997, p.3). Thus, the expectation of self-efficacy has been widely studied in many spheres such as physical activity (Schwarzer et al., 2008), tobacco addiction (Hendricks et al., 2010), multiple sclerosis (Chiu et al., 2011), or patients with arthritis (Lorig et al., 2014). However, it has received scant attention for celiac disease (Ford et al., 2012). High levels of self-efficacy are related to the perception of well-being and adherence to healthy eating (Luszczynska et al., 2005). Recently, self-efficacy has been linked to better adherence to GFD and better quality of life in celiac patients (Ford et al., 2012).
Qualitative studies show that celiac patients have to cope with problems mainly in five areas: eating in the workplace, shopping, traveling, eating out, and eating at home with others (Sverker et al., 2005). These difficulties can lead to negative emotions and affect relationships. Celiac patients with low self-efficacy can find eating and drinking situations potentially stressful and, hence, are not able to keep to their GFD in such circumstances, or if they are able to, it is at the cost of a lower life quality (Leffler et al., 2008).
There are a few questionnaires aimed to evaluate self-efficacy in a general way: Sherer's General Self Efficacy Scale (Sherer et al., 1982), recently translated into Spanish and validated (Herrero et al., 2014), Schwarzer's General Self Efficacy Scale (Schwarzer and Jerusalem, 1995), and the New General Self Efficacy Scale (Chen et al., 2001). All three scales provide solid psychometric information (Scherbaum et al., 2006) but none of them provide a specific measure of self-efficacy. Bandura (1997) emphasizes the convenience of specifically evaluating self-efficacy expectation and in a way that is closely linked to the demands of a particular situation, rather than making general evaluations of that situation. We have not found any scale to assess specific self-efficacy in celiac patients.
More recently, Schwarzer has proposed the Health Action Process Approach (HAPA model) as an explanatory framework for adherence to healthy habits (Schwarzer et al., 2011) in which self-efficacy plays a key role.
Traditional explanatory models of change fail to explain the gap between intention and action. The HAPA model distinguishes between pre-intentional motivational process and post-intentional volitive processes that lead to healthy habits. We think that this model is useful to explain adherence to GFD. The HAPA model is described in two-phases: a pre-intentional motivational and a post-intentional volitional phase. It is in the initial motivational phase, when the individual still needs to develop the intention to acquire a healthy habit (e.g., adherence to a GFD). In this phase, risks are seen as threatening but unlikely, especially by asymptomatic patients, and not important enough to build an intention. Conversely, they are important enough to motivate the patient toward a contemplation stage for the evaluation of the capabilities needed to take up a GFD (social skills, facing temptations, etc.) and negative consequences (giving up to certain foods, changing habits or extra work associated with the diet). In the same manner, positive consequences are important at this motivational phase (for example, a healthier diet or symptomatology improvement). According to this model, in this phase, high self-efficacy beliefs, together with positive outcome expectations, play a major role and both are necessary to develop an intention. But the development of an intention is not enough. Once developed, in a second phase, this intention needs to be turned into action and, finally, into a strict adherence for which self-regulation skills and strategies are required. In this volitional phase, planning, and self-efficacy beliefs to face transgression play a central role.
Using this model, we developed a scale to assess specific self-efficacy as a determinant in adherence to GFD and subsequently be able to investigate its impact on the quality of life in celiac patients.
Methods
A multi-phase prospective, observational study was designed in various stages (Grau, 1995): preparation of the protocol, construction of the questionnaire, and pilot run and validation of the questionnaire.
Phase 1: Preparation of a Protocol
Prior to the study, the research team drew up a protocol (Fueyo-Díaz et al., 2015). The study population was celiac patients who had been prescribed a lifelong GFD. A minimum age of 12 years was fixed as this is the age at which primary education ends and adolescents starting secondary education have to start managing their diet on their own. It is also assumed that by this age the patient has acquired sufficient language skills to be able to understand and reply to the questionnaire. A sample size of 10–15 patients per item was estimated as appropriated for the validation phase (Kline, 1998).
Phase 2: Construction of the Scale and Pilot Study
The research team created an initial questionnaire based on the Spanish version of the General Self-Efficacy Scale (GSES) (Baessler and Schwarzer, 1996) and follow the recommendations for constructing this type of scale (Bandura, 2006). This first questionnaire contained 80 questions, distributed in the areas identified by Sverker: (1) Shopping: the celiac patient can often experience problems with labels or when asking for gluten-free products over the counter, etc. (2) Travel: how they cope with the diet when using a foreign language or in a place where customs are different, etc. (3) Eating at home with others: this section aims to evaluate those situations in which the behavior of others has to be corrected when this may suppose a risk, identifying oneself as a celiac sufferer and not seeming brusque or rude when refusing food offered by others. (4) Eating out: this section examines aspects such as rejecting dishes that might not be safe. (5) Eating in the workplace or at school: here, social situations at work are explored, such as finding gluten-free options at business or school celebrations.
The initial questionnaire was then analyzed by a team of experts in celiac disease comprising researchers, physicians, psychologist, dietitians and patients. The number of items was whittled down to the 40 most significant. In order to analyze the face and construct validity, the new version of the questionnaire was then studied and assessed by a second team of experts. The opinions and comments of the experts helped to add, remove, or clarify the items and to decide on their inclusion in the definitive scale. After this second team of experts the number of items remained unaltered with 40 items. The scale was constructed to allow responses for all items from 0 (not at all able) to 10 (totally able) in order to evaluate the degree of self-efficacy respondents experienced in each of the situations proposed. To get both the scale and subscale scores we took the mean value of the answers. Although 99.82% of participants completed all the questions, missing data were completed with the mean value obtained by the rest of the subjects in the missed particular item. In clinical settings, although we recommend to use only completely filled questionnaires, missing values can be substituted by the mean in the subscale. A pilot study of the new version was carried out with 20 patients to check the relevance and comprehension of the questions selected.
Phase 3: Questionnaire Validation
The study was advertised through patients' associations and invitations to participate were sent out to their associates.
The questionnaire was administered on line alongside the Spanish adaptation of the GSES (Baessler and Schwarzer, 1996). Along with these items, we incorporated sociodemographic variables on place of residence, the year of diagnosis, time on GFD, and age.
The questionnaires were completed anonymously and then returned to the research team. The questionnaire returned two types of measurements: an overall score for the questionnaire and scores for each of the five areas, so enabling the evaluation of specific self-efficacy in each of the areas analyzed.
The questionnaires were collected between June and September 2014.
Phase 4: Statistical Analysis
Construct validity was determined by factorial analysis (principal components with a VARIMAX rotation) based on eigenvalues >1 criterion (Kleinbaum et al., 1978). We included the necessary factors to obtain a capacity to explain approximately a 70% of the variance. The relevance of the factorial analysis was evaluated using a correlation matrix among the variables, the Barlett sphericity test to study the identity of the correlation matrix and the Kayes, Meyer, and Olkin statistic to measure sample suitability.
Concurrent validity was calculated with Spearman's Rho coefficient with the GSES scale for each of the areas and for the questionnaire as a whole while the Cronbach alpha was used to study overall reliability of the questionnaire and for each of the scales. Multiple comparisons were performed by one-way ANOVA and post-hoc evaluations by Scheffe' test. Kruskal–Wallis and U Mann–Whitney tests were performed when necessary. The SPSS v.21 program was used for the statistical analysis and 0.05 was taken as being statistically significant throughout.
This study was approved by the Aragon Scientific Research Ethics Committee (CEICA), registered under number PI 14/0011. The research team obtained written and informed consent from the participants, or their legal guardians.
Results
Participants
Five hundred and sixty-three valid 40-item questionnaires were collected. Patients were aged from 12 to 72 years (M: 37.37; SD: 13.80) and 77.8% were females. Age at diagnosis ranged from 1 to 69 (M: 28.15; SD: 15.26). Patients had been following a GFD from <1 year to 59 (M: 8.77; SD: 8.74) (Table 1). Feasibility was excellent, 99.82% of participants completed all the questions. There was no floor effect, and ceiling effect was low (3.9%).
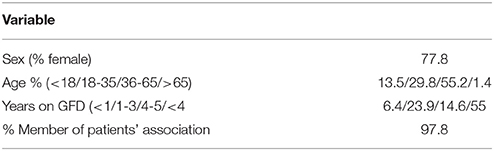
Table 1. Characteristics of participants.
Study of the Suitability of the Factorial Analysis
The relevance of the factorial analysis was evaluated using a correlation matrix among the variables. The associated p-value for the Barlett Sphericity Test was p < 0.001, indicating that there was, indeed, a relation between the items, which was a guarantee of the technical suitability of the factorial analysis. Finally, the KMO value was 0.934, which is well above the recommended 0.75. The obtained results showed that there was enough support to perform the pertinent factorial analysis.
Determination, Extraction, and Interpretation of Factors
Prior to the final factorial analysis, items that fulfilled the following criteria were eliminated: (1) any item that had >5% missing data; (2) any item that correlated poorly with the total scale (i.e., item-to-total correlation <0.40) and thus measured a different construct; (3) pairs of redundant items (i.e. an item-item correlation >0.75). The final questionnaire comprised 25 of the original 40 questions. These were grouped in five areas (Table 2).
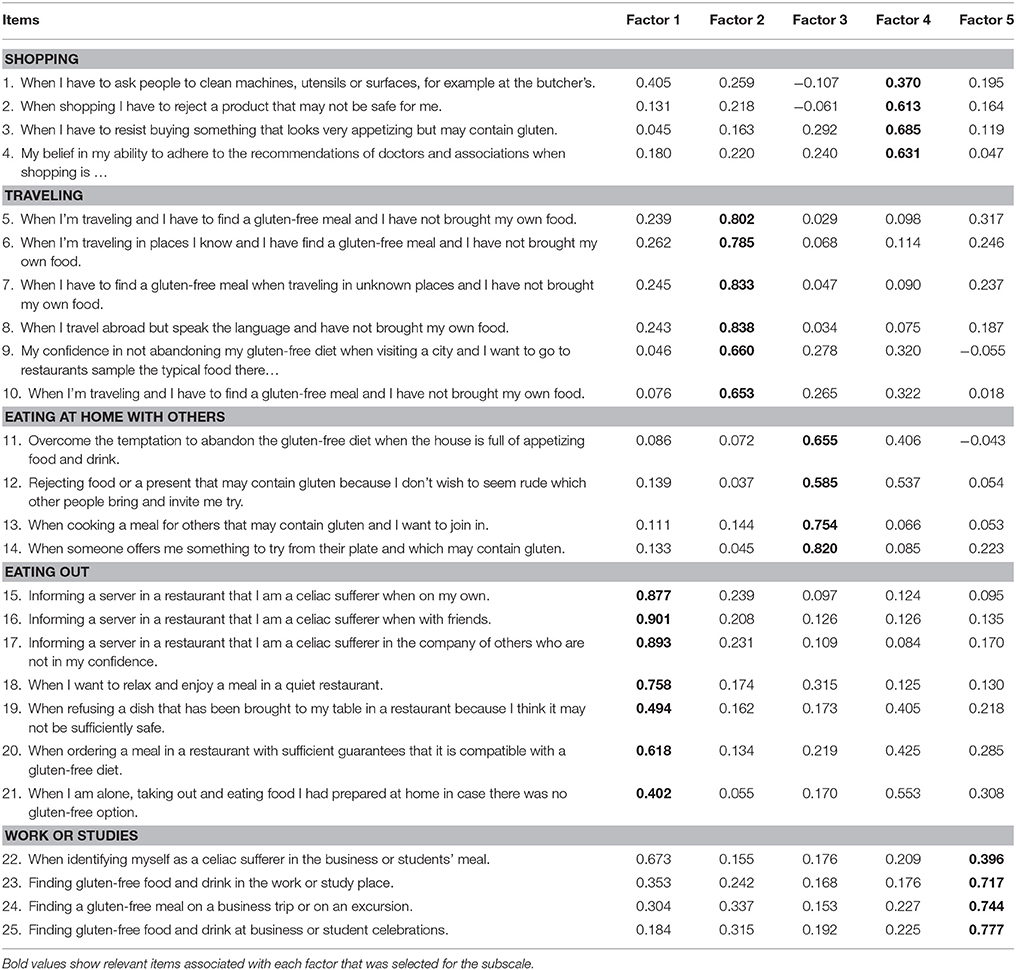
Table 2. Rotated components matrix.
Since the factorial analysis was confirmatory, we forced the model to extract five factors, explaining 70.98% of the total variance. The rotated components matrix (Table 2) shows the coefficients associated to each item, and its area or factor after a VARIMAX rotation.
The matrix shows the following structure: factor 1, “eating out,” explains 43.23% of the variance; factor 2, “traveling” explains 9.57% of the total variance; factor 3, “eating at home with others” 8.60% of the variance; factor 4, “shopping,” accounts for 4.97% of the variance. Lastly, factor 5, “work/studies,” explains 4.68% of the variance. The higher the factor loading, the higher the association of the item with the factor grouping. The highest values for each item are shown in boldface with two exceptions: Although item 1 “When I have to ask people to clean machines, utensils or surfaces, for example at the butcher's” and item 22 “When identifying myself as a celiac sufferer in the business or students' meal” load onto factor 1, we have considered their second highest load to keep them in their original areas, due to their meaning and importance in dealing with GFD and we will wait for future studies to either eliminate them or rewrite them and assign them to other area.
Determination of the Psychometric Properties
In order to analyze reliability, Cronbach's alpha was calculated for all the areas. The scores ranged from 0.64 for “shopping” to 0.90 for “traveling,” indicating a good reliability of the structure obtained from the factorial analysis, as can be seen in Table 3. The alpha coefficient for the whole scale was 0.81.
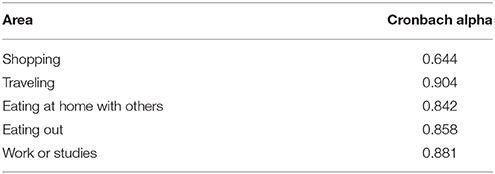
Table 3. Cronbach alpha.
The criterion validity was analyzed using the non-parametric Spearman's Rho correlation coefficient with the General Self-Efficacy Scale (GSES), which was administered alongside the questionnaire. The value was 0.279, indicating a low but significant correlation (Table 4).
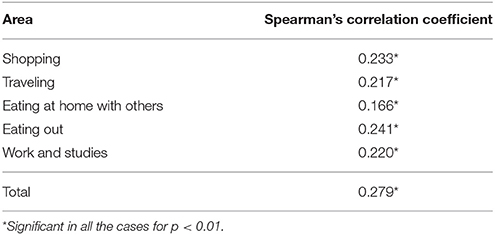
Table 4. Spearman's Rho correlation coefficients.
Specific Self-Efficacy
Table 5 shows the results for specific self-efficacy for each of the areas. The areas in which most patients have difficulties adhering to a GFD is traveling, followed by shopping, and work. Scores below 7 are considered to represent low self-efficacy and scores below 5 indicate very low self-efficacy expectations. Scores below 70% of the highest score can be considered low self-efficacy. This is a valid method for determining a cut-off point for high and low self-scores in Likert type survey questionnaires (Child, 2006; Hicks and McFrazier, 2014).
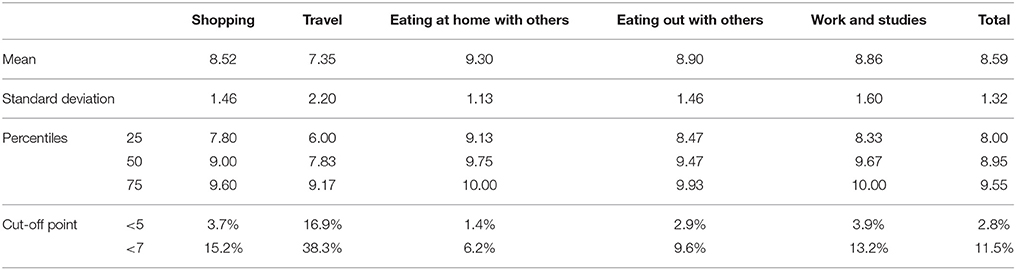
Table 5. Results Celiac-SE.
Differences were found for sex (p = 0.030) and for years on GFD between those with <1 year of experience and those with more than 5 years (p = 0.044). Differences for age were found between the adult group and young adults group (p = 0.000) and young adults participants and seniors (p = 0.000). No differences were found for age at diagnosis (Table 6).
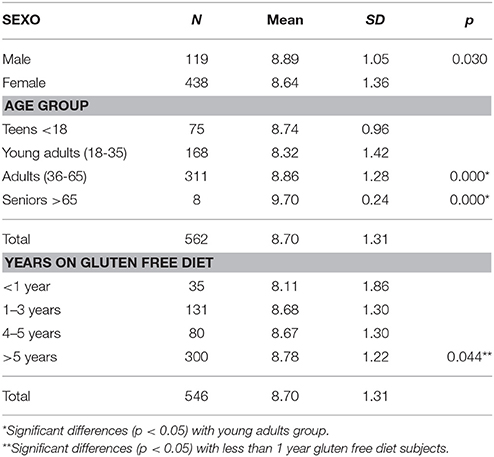
Table 6. Results Celiac-SE by sex, age, and experience.
Discussion
Self-efficacy expectation plays a central role in healthy habits and adherence to treatments (DiClemente et al., 1985, 1995; Brus et al., 1999; West et al., 1999; Lorig and Holman, 2003; Schwarzer et al., 2008), but this has not been studied in relation to celiac disease, in part because of the lack of specific tools to assess self-efficacy levels. Celiac-SE fills this gap.
The Celiac-SE has good psychometric properties, both valid and reliable in detecting specific levels of self-efficacy in celiac disease sufferers in the main spheres of life in which they can experience problems: eating in the workplace, shopping, traveling, eating out, and eating at home with others. The questionnaire is easily and quickly administered (15 min at the most) and determines the degree of specific self-efficacy in diagnosed celiac sufferers following a life-long GFD. Its construction followed scientific procedures in accordance with the recommendations for constructing scales of this type (Bandura, 2006), and was supported by the consensus of patients and experts. A factorial analysis revealed the existence of five factors that coincided with the areas intended to measure specific self-efficacy for following a GFD.
The test shows a high reliability indicating that the items are grouped around the five areas we wish to explore. The tool presents an acceptable concurrent validity, showing positive and significant correlations with the GSES of Baessler & Schwarzer. Although this coefficient is significant, its low value can be explained because the GSES scale measures general self-efficiency, as opposed to the specific self-efficacy measured by our scale.
Food intolerances are becoming increasingly frequent and better diagnosed in today's world. The tool will help patients and professionals alike to improve the formers' adherence to what is, to date, the only treatment available. New intervention models in health place emphasis on patients' responsibility and their empowerment to direct their treatment and improve their quality of life (Holman and Lorig, 2000, 2004; Bodenheimer et al., 2002; Carey and Doherty, 2012). The aim of this research was to provide tools to study these psychosocial factors in order to establish the bases for the design of self-management programs for sufferers of celiac disease (Fueyo-Díaz et al., 2017).
Bandura defines expectation of self-efficacy as “the judgement of one's ability to organize and execute given types of performances” (Bandura, 1997, p. 21), thus clearly distinguishing between expectation of self-efficacy and other psychological constructs such as feelings, outcome expectations, locus of control, etc. Thus, this scale seeks to explore not so much feelings and motivations for following a GFD, but the confidence a person has that he or she will be able to follow it. The contribution of this questionnaire is that it makes available a tool that can measure expectations of self-efficacy in specific situations which are real and frequent and which have their own specific demands, as opposed to measuring general expectation. Furthermore, the scale provides not only a measurement of self-efficacy, but also valuable information about its levels in the various situations in which a celiac disease sufferer moves. From the theoretical viewpoint, therefore, this study lies within the Social Cognitive Theory developed by Bandura (1985) and is a first step toward the future design of self-management programs for the disease of the type developed by Kate Lorig (Bodenheimer et al., 2002) at the University of Stanford. More recently, the research lines of Schwarzer on the HAPA model (Schwarzer et al., 2011) propose a more specific theoretical framework in which to interpret results and develop self-management programs for the disease.
The levels of specific self-efficacy found in this validation study are, in general, high. An explanation for these high scores may be the mastery in GFD management of the sample as participants had more than 8.77 years of experience. It seems self-efficacy beliefs are built during the first year of experience in GFD and reach their highest levels after 5 years on GFD. An explanation for differences for age could be that teens are, somehow, under parental advice at that age and it is between 18 and 35 years old when parents transfer responsibility for the diet and they must face the challenge for managing their diet by themselves when shopping, traveling or at work. These results are consistent with Social Cognitive Theory for which mastery experiences become the most important source of self-efficacy (Bandura, 1997). These relationships need of future research to find out if this scale would predict GFD adherence or quality of life soon after diagnosis.
Some limitations of the study are that it has been developed and validated in Spanish, although we do offer an English version should other researchers wish to validated it in other settings (Appendix). Due to its specific nature and its being closely linked to self-efficacy expectation, it was not considered necessary to study its test-retest reliability, although this could be studied in the future, as could its discriminant validity. Future studies are needed to confirm the factorial structure of the scale as well as to consider an item reduction, e.g., eliminating items 1 or 22 if it is confirmed they load in other factors.
In clinical settings, this scale may be useful to detect patients with low self-efficacy expectations in dealing with GFD and that, therefore, may show worse adherence to diet or worse quality of life. With a cut-off point of 7 for the lowest levels of self-efficacy, we see that around 11.5% present self-efficacy problems in managing their GFDs. These are the patients who could benefit from empowerment programs that can help them to address their illness with lower levels of stress and better life quality.
Conclusion
Control of the disease through a proper GFD has a direct impact on the celiac patients' perceived quality of life (Casellas et al., 2008, 2015). This tool will, in the future, enable us to explore the expectation of self-efficacy in a specific way, and, hence, its impact on adherence to a GFD and the subsequent quality of life. It should also help in the design of self-management programs for celiac disease and, with the appropriate adaptations, help other sufferers of diseases with dietary restrictions.
Author Contributions
RF-D, SG-S, ÁA-M, RM-B and JS-D were involved in conceptualizing the study, collecting, analyzing the data, and writing the manuscript. GP-N was involved in analyzing the data and the final revision of the work. All authors approved the final submitted version, and all agreed to be accountable for all aspects of the work.
Funding
This study was funded by project PI16/00570 (Instituto de Salud Carlos III) and by Fondo Europeo de Desarrollo Regional (FEDER) funds: Una manera de hacer Europa.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors wish to express their thanks for the help and support by the Aragon Celiac Association and other associations of the Spanish Federation of Associations of Celiac Patients, as well as to the Red de Investigación en Actividades de Prevención y Promoción de la Salud en Atención Primaria (RedIAPP- RD12/005/006).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2018.00342/full#supplementary-material
References
Baessler, J., and Schwarzer, R. (1996). Evaluación de la autoeficacia: adaptación española de la Escala de Autoeficacia general. Ansiedad Estrés 2, 1–8.
Bandura, A. (1985). Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (2006). “Guide for constructing self-efficacy scales,” in Self-Efficacy Beliefs of Adolescents, eds T. Urdan and F. Pajares (Greenwich, CT: Information Age Publishing).
Bodenheimer, T., Lorig, K., Holman, H., and Grumbach, K. (2002). Patient self-management of chronic disease in primary care. JAMA 288:2469. doi: 10.1001/jama.288.19.2469
Brus, H., van de Laar, M., Taal, E., Rasker, J., and Wiegman, O. (1999). Determinants of compliance with medication in patients with rheumatoid arthritis: the importance of self-efficacy expectations. Patient Educ. Couns. 36, 57–64. doi: 10.1016/S0738-3991(98)00087-1
Carey, M., and Doherty, Y. (2012). Supporting successful self-management in diabetes. Diabetes Prim. Care 14:297.
Casellas, F., Rodrigo, L., Lucendo, A. J., Fernández-Bañares, F., Molina-Infante, J., Vivas, S., et al. (2015). Benefit on health-related quality of life of adherence to gluten-free diet in adult patients with celiac disease. Rev. Esp. Enfermedades Dig. 107, 196–201.
Casellas, F., Rodrigo, L., Vivancos, J. L., Riestra, S., Pantiga, C., Baudet, J. S., et al. (2008). Factors that impact health-related quality of life in adults with celiac disease: a multicenter study. World J. Gastroenterol. 14:46. doi: 10.3748/wjg.14.46
Catassi, C., Fabiani, E., Iacono, G., D'Agate, C., Francavilla, R., Biagi, F., et al. (2007). A prospective, double-blind, placebo-controlled trial to establish a safe gluten threshold for patients with celiac disease. Am. J. Clin. Nutr. 85, 160–166. doi: 10.1093/ajcn/85.1.160
Chen, G., Gully, S. M., and Eden, D. (2001). Validation of a new general self-efficacy scale. Organ. Res. Methods 4, 62–83. doi: 10.1177/109442810141004
Chiu, C.-Y., Lynch, R. T., Chan, F., and Berven, N. L. (2011). The Health Action Process Approach as a motivational model for physical activity self-management for people with multiple sclerosis: a path analysis. Rehabil. Psychol. 56, 171–181. doi: 10.1037/a0024583
DiClemente, C. C., Fairhurst, S. K., and Piotrowski, N. A. (1995). “Self-efficacy and addictive behaviors,” in Self-Efficacy, Adaptation, and Adjustment The Plenum Series in Social/Clinical Psychology, ed J. E. Maddux (Springer US), 109–141. Available online at: http://link.springer.com/chapter/10.1007/978-1-4419-6868-5_4 (Accessed September 22, 2015).
DiClemente, C. C., Prochaska, J. O., and Gibertini, M. (1985). Self-efficacy and the stages of self-change of smoking. Cogn. Ther. Res. 9, 181–200. doi: 10.1007/BF01204849
Ford, S., Howard, R., and Oyebode, J. (2012). Psychosocial aspects of coeliac disease: a cross-sectional survey of a UK population. Br. J. Health Psychol. 17, 743–757. doi: 10.1111/j.2044-8287.2012.02069.x
Fueyo-Díaz, R., Gascón-Santos, S., and Magallón-Botaya, R. (2017). “I can't eat that! Sticking to a gluten free diet,” in Celiac Disease and Non-Celiac Gluten Sensitivity, ed L. Rodrigo (InTech). Available online at: https://www.intechopen.com/books/celiac-disease-and-non-celiac-gluten-sensitivity/i-can-t-eat-that-sticking-to-a-gluten-free-diet
Fueyo-Díaz, R., Magallón-Botaya, R., Sánchez-Calavera, M. A., Asensio-Martínez, A., and Gascón-Santos, S. (2015). Protocolo para el diseño de una escala específica de auto-eficacia en la adherencia a una dieta sin gluten: escala de celiaquía y auto-eficacia. Rev. Esp. Nutr. Humana Dietética 19, 160–166. doi: 10.14306/renhyd.19.3.152
Hall, N. J., Rubin, G., and Charnock, A. (2009). Systematic review: adherence to a gluten-free diet in adult patients with coeliac disease. Aliment. Pharmacol. Ther. 30, 315–330. doi: 10.1111/j.1365-2036.2009.04053.x
Hendricks, P. S., Delucchi, K. L., and Hall, S. M. (2010). Mechanisms of change in extended cognitive behavioral treatment for tobacco dependence. Drug Alcohol Depend. 109, 114–119. doi: 10.1016/j.drugalcdep.2009.12.021
Herrero, R., Espinoza, M., Molinari, G., Etchemendy, E., Garcia-Palacios, A., et al. (2014). Psychometric properties of the general self efficacy-12 Scale in Spanish: general and clinical population samples. Compr. Psychiatry 55, 1738–1743. doi: 10.1016/j.comppsych.2014.05.015
Hicks, T., and McFrazier, M. (2014). College Student Self-Efficacy Research Studies. Lanham, MD: University Press of America.
Holman, H., and Lorig, K. (2000). Patients as partners in managing chronic disease. BMJ Br. Med. J. Int. Ed. 320:526. doi: 10.1136/bmj.320.7234.526
Holman, H., and Lorig, K. (2004). Patient self-management: a key to effectiveness and efficiency in care of chronic disease. Public Health Rep. 119:239. doi: 10.1016/j.phr.2004.04.002
Kleinbaum, D. G., Kupper, L. L., and Muller, K. E. (1978). Applied Regression Analysis and Other Multivariable Methods. Boston, MA: PWS-KENT.
Kline, R. B. (1998). Principles and Practice of Structural Equation Modeling. New York, NY: Guilford Press.
Leffler, D. A., Edwards-George, J., Dennis, M., Schuppan, D., Cook, F., Franko, D. L., et al. (2008). Factors that influence adherence to a gluten-free diet in adults with celiac disease. Dig. Dis. Sci. 53, 1573–1581. doi: 10.1007/s10620-007-0055-3
Lorig, K., Laurent, D. D., Plant, K., Krishnan, E., and Ritter, P. L. (2014). The components of action planning and their associations with behavior and health outcomes. Chronic Illn. 10:50. doi: 10.1177/1742395313495572
Lorig, K. R., and Holman, H. (2003). Self-management education: history, definition, outcomes, and mechanisms. Ann. Behav. Med. 26, 1–7. doi: 10.1207/S15324796ABM2601_01
Ludvigsson, J. F., Leffler, D. A., Bai, J. C., Biagi, F., Fasano, A., Green, P. H., et al. (2013). The Oslo definitions for coeliac disease and related terms. Gut 62, 43–52. doi: 10.1136/gutjnl-2011-301346
Luszczynska, A., Scholz, U., and Schwarzer, R. (2005). The general self-efficacy scale: multicultural validation studies. J. Psychol. 139, 439–457. doi: 10.3200/JRLP.139.5.439-457
Scherbaum, C. A., Cohen-Charash, Y., and Kern, M. J. (2006). Measuring general self-efficacy: a comparison of three measures using item response theory. Educ. Psychol. Meas. 66, 1047–1063. doi: 10.1177/0013164406288171
Schwarzer, R., and Jerusalem, M. (1995). “Generalized self-efficacy scale,” in Measures in Health Psychology: A User's Portfolio. Causal and Control Beliefs, eds J. Weinman, S. Wright, and M. Johnston (Windsor: NFER-NELSON), 35–37.
Schwarzer, R., Lippke, S., and Luszczynska, A. (2011). Mechanisms of health behavior change in persons with chronic illness or disability: the health action process approach (HAPA). Rehabil. Psychol. 56, 161–170. doi: 10.1037/a0024509
Schwarzer, R., Luszczynska, A., Ziegelmann, J. P., Scholz, U., and Lippke, S. (2008). Social-cognitive predictors of physical exercise adherence: three longitudinal studies in rehabilitation. Health Psychol. 27, S54–S63. doi: 10.1037/0278-6133.27.1(Suppl.).S54
Sherer, M., Maddux, J. E., Mercadante, B., Prendtice-Dunn, S., Jacobs, B., and Rogers, R. W. (1982). The Self-efficacy scale: construction and validation. Psychol. Rep. 51, 663–671. doi: 10.2466/pr0.1982.51.2.663
Sverker, A., Hensing, G., and Hallert, C. (2005). ‘Controlled by food’– lived experiences of coeliac disease. J. Hum. Nutr. Diet. 18, 171–180. doi: 10.1111/j.1365-277X.2005.00591.x
Keywords: celiac disease, self-efficacy, adherence to a gluten-free diet, perceived quality of life, empowerment
Citation: Fueyo-Díaz R, Magallón-Botaya R, Gascón-Santos S, Asensio-Martínez Á, Palacios-Navarro G and Sebastián-Domingo JJ (2018) Development and Validation of a Specific Self-Efficacy Scale in Adherence to a Gluten-Free Diet. Front. Psychol. 9:342. doi: 10.3389/fpsyg.2018.00342
Received: 10 October 2017; Accepted: 28 February 2018;
Published: 16 March 2018.
Edited by:
Boris C. Rodríguez-Martín, Fundación Recal, SpainReviewed by:
Evelyn Fernández-Castillo, University “Marta Abreu” of Las Villas, CubaNaomi Kakoschke, Monash University, Australia
Copyright © 2018 Fueyo-Díaz, Magallón-Botaya, Gascón-Santos, Asensio-Martínez, Palacios-Navarro and Sebastián-Domingo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ricardo Fueyo-Díaz, cmZ1ZXlvQHVuaXphci5lcw==