 Sanne P. A. Rasing
Sanne P. A. Rasing Daan H. M. Creemers1,2
Daan H. M. Creemers1,2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 28 June 2017
Sec. Psychopathology
Volume 8 - 2017 | https://doi.org/10.3389/fpsyg.2017.01066
Depression and anxiety disorders are among the most common mental disorders during adolescence. During this life phase, the incidence of these clinical disorders rises dramatically, and even more adolescents suffer from symptoms of depression or anxiety that are just below the clinical threshold. Both clinical and subclinical levels of depression or anxiety symptoms are related to decreased functioning in various areas, such as social and academic functioning. Prevention of depression and anxiety in adolescents is therefore imperative. We conducted a meta-analytic review of the effects of school-based and community-based prevention programs that are based on cognitive behavioral therapy with the primary goal preventing depression, anxiety, or both in high risk adolescents. Articles were obtained by searching databases and hand searching reference lists of relevant articles and reviews. The selection process yielded 32 articles in the meta-analyses. One article reported on two studies and three articles reported on both depression and anxiety. This resulted in a total of 36 studies, 23 on depression and 13 on anxiety. For depression prevention aimed at high risk adolescents, meta-analysis showed a small effect of prevention programs directly after the intervention, but no effect at 3–6 months and at 12 months follow-up. For anxiety prevention aimed at high risk adolescents, no short-term effect was found, nor at 12 months follow-up. Three to six months after the preventive intervention, symptoms of anxiety were significantly decreased. Although effects on depression and anxiety symptoms were small and temporary, current findings cautiously suggest that depression and anxiety prevention programs based on CBT might have small effects on mental health of adolescents. However, it also indicates that there is still much to be gained for prevention programs. Current findings and possibilities for future research are discussed in order to further improve the effectiveness of targeted prevention on internalizing disorders.
Depression and anxiety are among the most common mental disorders during adolescence (Kessler et al., 2001; Roza et al., 2003), with a prevalence of 5.6% for depression (Costello et al., 2006; Stallard et al., 2012) and a prevalence of 3–20% for anxiety (Albano et al., 2003). Research has shown that among 13–17 year old adolescents the lifetime prevalence is estimated to be 12.6% for depression and 32.4% for anxiety disorders (Kessler et al., 2012). Even more adolescents suffer from subclinical levels of depression or anxiety, with 21.4% of the adolescents estimated to suffer from subclinical depression symptoms (Smit et al., 2003). Unfortunately, the number of adolescents suffering from subclinical anxiety is unknown.
Depression and anxiety during adolescence are associated with decreased psychosocial functioning (Birmaher et al., 1996), that is, malfunctioning in social relations (Strauss et al., 1987), poor academic performance or school drop-out (Strauss et al., 1987; Birmaher et al., 1996), and an increased risk for substance abuse, other mental health problems, and suicide (Birmaher et al., 1996). Further, adolescents with a depression or anxiety disorder are at considerable risk for developing recurrent depression and anxiety disorders later in life (Pine et al., 1999; Aalto-Setala et al., 2002; Copeland et al., 2014). These negative consequences are comparable between adolescents who meet the criteria for a depression or anxiety disorder and adolescents with subclinical depression and anxiety symptoms (Lewinsohn et al., 2000; Aalto-Setala et al., 2002; Beesdo et al., 2009). Therefore, it is imperative to reduce the incidence of depression and anxiety, but also to prevent further development of depression and anxiety symptoms. Because depression and anxiety symptoms rise dramatically during adolescence, this seems to be the appropriate age to implement prevention, because the risk for depression and anxiety rises during this phase. Further, adolescents are, better than younger children, able to understand the concepts that are being taught in the prevention programs due to their improved reasoning (Hankin et al., 1998; Stice et al., 2009).
Several prevention programs have been developed to prevent depression and anxiety during adolescence. These programs utilize different types of prevention strategies and focus on populations with different risks of developing depression or anxiety (Mrazek and Haggerty, 1994). First, universal prevention programs are intended for all individuals in a population, regardless of their level of risk. These programs have shown mixed results in reducing and preventing depression and anxiety symptoms (Horowitz and Garber, 2006; Sheffield et al., 2006; Fisak et al., 2011; Teubert and Pinquart, 2011; Merry et al., 2012; Hetrick et al., 2016). Second, selective prevention programs are developed to target populations with risk factors, which are known to be related to the onset of depression and anxiety. Selective prevention programs can be aimed at children of parents with psychopathology or children from lower socio-economical environments (Hyun et al., 2005; Garber et al., 2009; Fisak et al., 2011; Merry et al., 2012; Hetrick et al., 2015). Third, indicated prevention programs are developed to target adolescents who already have elevated symptoms of depression or anxiety, but the symptoms do not qualify for a clinical diagnosis. Results of selective and indicated prevention programs, together also called targeted prevention, have shown to be more promising than universal prevention (Horowitz and Garber, 2006; Stice et al., 2009; Fisak et al., 2011; Merry et al., 2012; Hetrick et al., 2016).
Selective and indicated prevention programs are both aimed at populations with risk factors for depression or anxiety. An important risk factor is parental psychopathology, as children are three times more likely to develop a major depressive disorder and two to seven times more likely to develop an anxiety disorder when their parents suffer from depression or anxiety, respectively (Kashani et al., 1990; Birmaher et al., 1996; Beidel and Turner, 1997; Merikangas et al., 1998; Bijl et al., 2002; Lieb et al., 2002; Van Dorsselaer et al., 2006; Micco et al., 2009).
Another risk factor for the development of adolescent depression and anxiety is the experience of stressful life events during adolescence (Grant et al., 2004; Fox et al., 2010; Auerbach et al., 2012). Studies have shown that increased depressive and anxiety symptoms are often preceded by stress (Ge et al., 1994; Garber et al., 2002), and particularly in girls, stress and depression are closely associated during adolescence (Larson and Ham, 1993; Ge et al., 1994; Rudolph and Hammen, 1999). Further, the existence of subclinical symptoms of depression or anxiety, or undiagnosed clinical levels of these disorders, is a risk factor for the development of a clinical disorder (Clarke et al., 1995; Lowry-Webster et al., 2001; Weissman et al., 2006).
Whereas prevention in high risk populations aims to decrease the likelihood of the onset of a depressive or anxiety disorder or decrease in symptoms, treatment aims to reduce existing symptoms (Garber and Weersing, 2010). In targeting symptoms, prevention seems to parallel treatment in these goals. As we know from reviews of meta-analyses (Butler et al., 2006; Hofmann et al., 2012), cognitive behavioral therapy demonstrated to be an effective treatment for a wide range of psychological problems, including depression and anxiety. Based on the overlap in goals (i.e., decreasing symptoms) between treatment and prevention, techniques of the cognitive behavioral approach seem to be suitable techniques to use in the prevention of depression and anxiety in high-risk adolescents. Although, several prevention programs for depression and anxiety are based on cognitive behavioral theories, to our knowledge, the effects of depression and anxiety prevention programs with this same theoretical background for high-risk adolescents were never reviewed or studied in a meta-analysis. In this meta-analysis, we examined whether prevention programs based on the cognitive behavioral approach are effective in preventing depression and anxiety in high-risk adolescents.
Several reviews and meta-analyses have been conducted to evaluate the effectiveness of depression prevention programs and anxiety prevention programs for adolescents (Neil and Christensen, 2009; Calear and Christensen, 2010; Christensen et al., 2010; Teubert and Pinquart, 2011; Merry et al., 2012). These meta-analyses were focused on either depression or anxiety, and on prevention in general and not on high risk populations. In contrast to those, the present study focused specifically on depression and anxiety prevention programs based on cognitive behavioral therapy approaches for adolescents with a high risk on developing depression or anxiety.
This review intended to identify and describe school-based and community-based prevention programs based on cognitive behavioral therapy with a primary goal of preventing depression, anxiety, or both in adolescents at risk for developing these disorders. Furthermore, we aimed to determine their effectiveness in reducing symptoms of depression and anxiety in the short-term and in the long-term.
The study design will be reported in accordance with the PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions (Liberati et al., 2009).
Databases Medline (from 1946), PsycInfo (from 1906), Embase (from 1974), and Eric (from 1965) were electronically searched in July 2013. This searched was updated in February 2017. The key search terms “adolescen* OR teen-age* OR youth*,” “prevent* OR early intervent*,” “depress* OR anx* OR mood OR internali#ing” AND “at risk OR high risk” were used.
Using these specified terms, we identified 2,331 articles. After removing 769 duplicates, 1,562 articles remained. First, titles and abstracts of the 1,562 remaining articles were screened by the first author to determine their relevance to the review. This resulted in the exclusion of 1,460 articles (1,174 articles included populations with other (mental) health problems than depression and/or anxiety; 45 articles were reviews, systematic reviews or meta-analyses; 10 articles reported on drug trials; 158 articles reported on other aspects than effectiveness; and 73 documents were not peer reviewed articles); thus 102 articles remained. Additionally, 29 articles were obtained by hand searching reference lists of relevant articles and reviews. Figure 1 demonstrates the flow chart of selected articles.
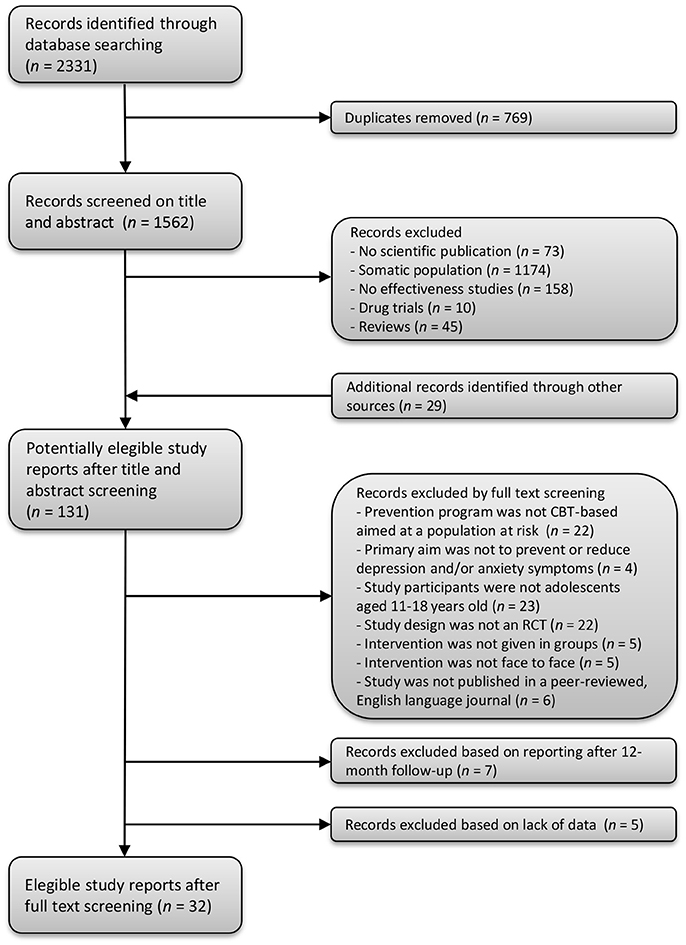
Figure 1. Flow chart of the search strategy and selection of study reports.
Second, of the 131 articles that were identified, the title, abstract and method section of each article were systematically reviewed and considered for inclusion. The inclusion criteria for the current review were that (1) the prevention program was CBT-based and targeted a population at risk (i.e., the program was selective or indicated prevention), (2) the reported intervention aimed to prevent or reduce depression and/or anxiety symptoms, (3) study participants included adolescents aged 11–18, (4) the study design was a randomized controlled trial, (5) the intervention was given in groups, (6) the intervention was delivered face to face, and (7) the study was published in a peer-reviewed, English language journal. Rating the articles was done by five independent reviewers (two postgraduates, one post-doc and two full professors) in which each article was handled by two reviewers. Agreement between raters was between 79 and 96 % (Cohen's Kappa = 0.58–0.92). Differences between reviewers were resolved by consensus. Main reasons for excluding articles can be found in Figure 1. Finally during data extraction, we learned that seven articles reported no measurements on depression or anxiety at baseline, 3 to 6- or 12-month follow-up but only longer duration of follow-up and five articles showed a lack of data, such as missing mean scores or standard deviations in order to calculate effect sizes, and these were also excluded. This resulted in 32 articles included in the meta-analyses.
All studies were coded for type of prevention, sample, number of participants, age of participants, percentage of females, group size, number and duration of sessions, characteristics of control condition, randomization, outcome measure, means and standard deviations at post-intervention, means and standard deviations at 6 months follow-up, and means and standard deviations at 12 months follow-up. Coding was done by two independent raters (both postgraduates). Overall agreement between raters was 95%. Differences between raters were resolved through discussion which led to total agreement.
We used the Cochrane Collaboration software Review Manager (RevMan version 5.3) to conduct meta-analyses. We analyzed the data with a random effects model, calculating the standardized mean differences (SMDs), also known as effect size Cohen's d (Cohen, 1977), and 95% confidence intervals (CIs). Cohen's effect sizes are generally categorized as small (0.2–0.5), moderate (0.5–0.8), or large (larger than 0.8). We based the effects sizes on the change in self-reported depression scores and anxiety scores. Heterogeneity between trials was assessed using Tau2 (estimated standard deviation of underlying effects across studies), Chi2 (whether observed differences in results are compatible with chance alone), and I2 statistic (in which higher values indicate higher heterogeneity), which is defined by the percentage of total variation across trials due to heterogeneity rather than chance (Higgins and Thompson, 2002).
The sample consisted of 32 articles. One article reported on two studies (Barrett et al., 2005), and three articles reported both on depression as well as anxiety (Gillham et al., 2006b; Manassis et al., 2010). This resulted in 36 studies, 23 on depression and 13 on anxiety.
In the depression study sample (see Table 1), 19 studies used indicated prevention, two used selective prevention, and two used a combination of selective and indicated prevention. Nineteen studies were conducted in schools, four were community-based. The size of the intervention groups varied from small groups of 3–15 adolescents in 16 studies, to large groups (school classes) in three studies. Four studies did not report group size. Intervention intensity ranged from four sessions of 60 min (total of 240 min) to 12 sessions of 120 min (total of 1,440 min). The control conditions were non-intervention groups (i.e., adolescents received no care or guidance at all) in seven studies, usual care groups (i.e., adolescents received personal care or guidance if requested) in 11 studies, waiting list groups (i.e., adolescents received the intervention after completion) in two studies, and active control conditions in three studies (Let's talk program, an educational brochure, and activity groups). In three studies study (Stallard et al., 2012, 2013; Kindt et al., 2014), the intervention was given in school classes as universal prevention, and afterwards the data for high-risk adolescents were analyzed separately. In the other 20 studies, the intervention was given to selected groups based on features of the participants (i.e., elevated levels of depression).
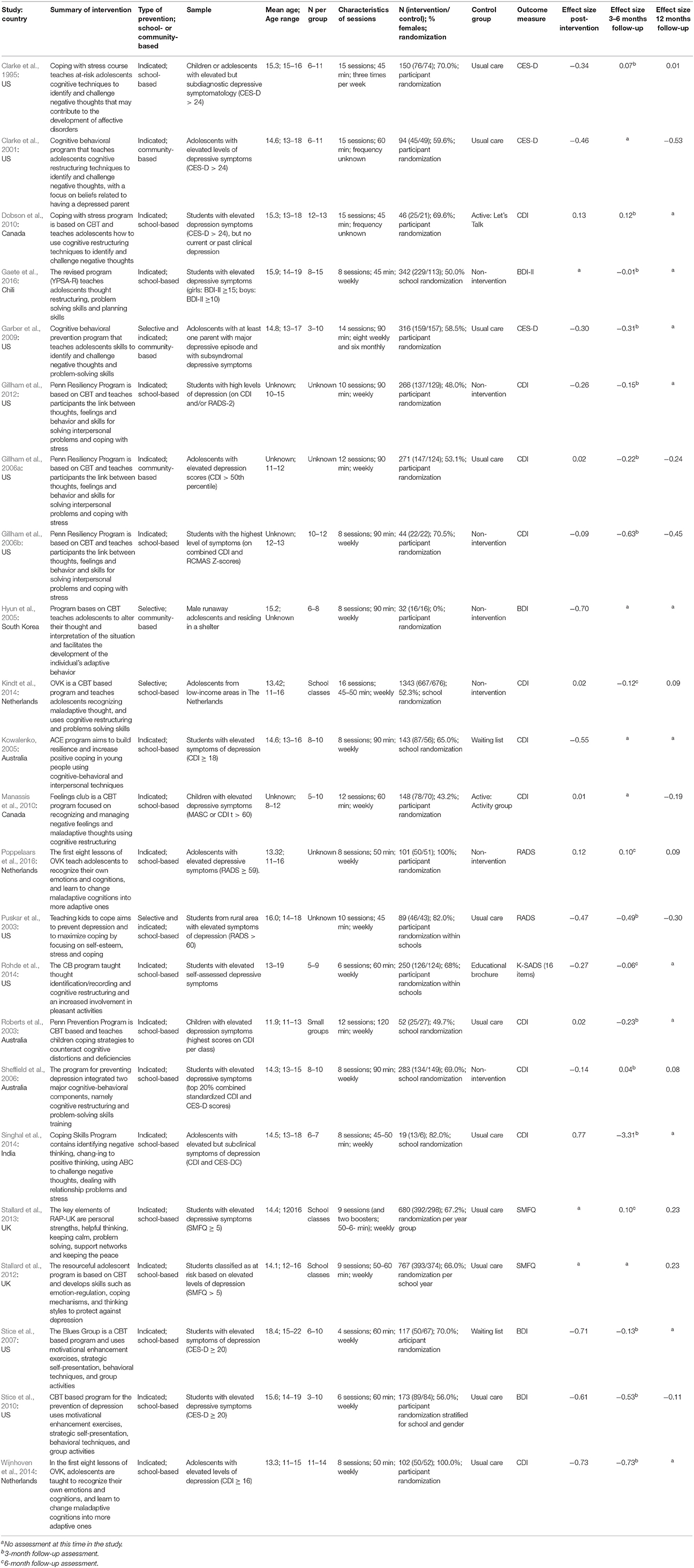
Table 1. Summary of descriptive characteristics of depression prevention programs.
In the anxiety study sample (see Table 2), 13 studies used indicated prevention. Twelve studies were conducted in schools, one was community-based. Intervention group sizes varied from small groups of 5–12 adolescents in eight studies to large groups (school classes of 30 students) in three studies. Two studies did not report group size. The length of the interventions varied from 6 sessions of 45 min (total of 270 min) to 10 sessions of 120 min (total of 1,200 min). The control conditions were non-intervention groups in nine studies, waiting list groups in two studies, and active control conditions in two studies (guidance class and activity class). In three studies (Lowry-Webster et al., 2001; Barrett et al., 2005), school classes were given a universal preventive intervention and the data for at-risk adolescents were analyzed separately. In the other 10 studies, the intervention was presented to selected groups (i.e., elevated levels of anxiety).
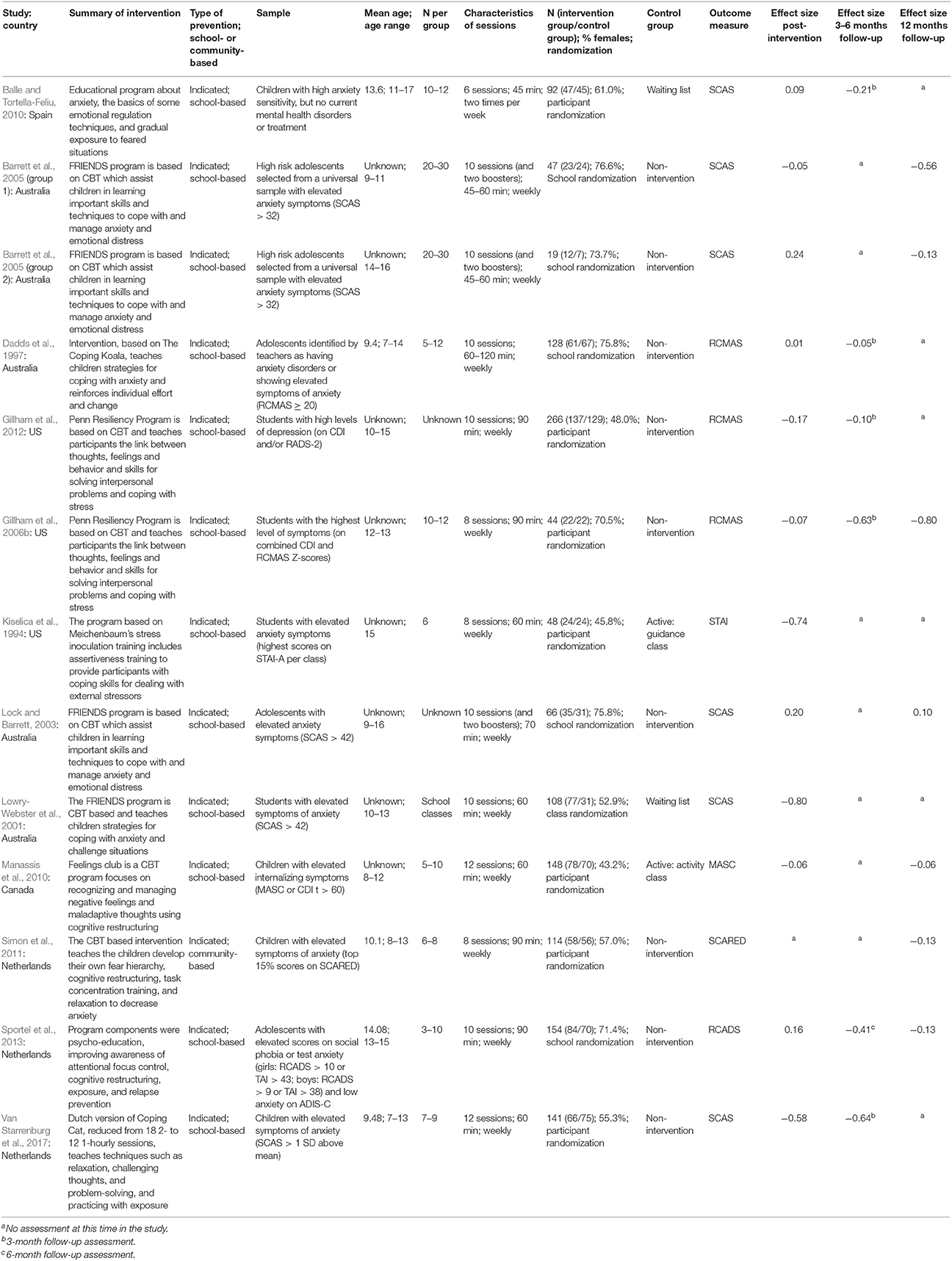
Table 2. Summary of descriptive characteristics of anxiety prevention programs.
Meta-analyses were conducted on the data presented in Tables 1, 2. Means, standard deviations, number of participants, weight of the study and effect sizes are presented in Figure 2 for depression studies and Figure 3 for anxiety studies. Both are accompanied by a forest plot reporting effect sizes and confidence intervals per study (respectively square points and horizontal lines) and the pooled result for all studies (diamond). Measures of heterogeneity Tau2, Chi2, and I2 were calculated and presented in Figures 2, 3.
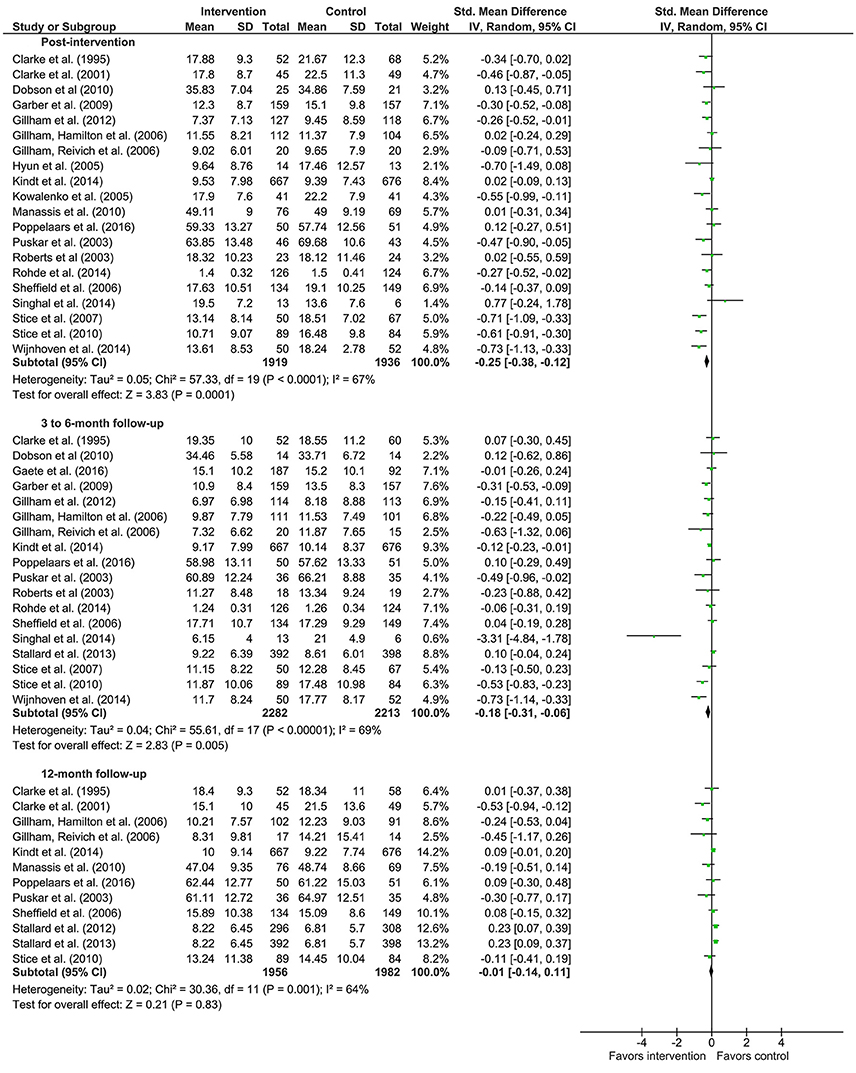
Figure 2. Forest plots of effects of depression prevention.
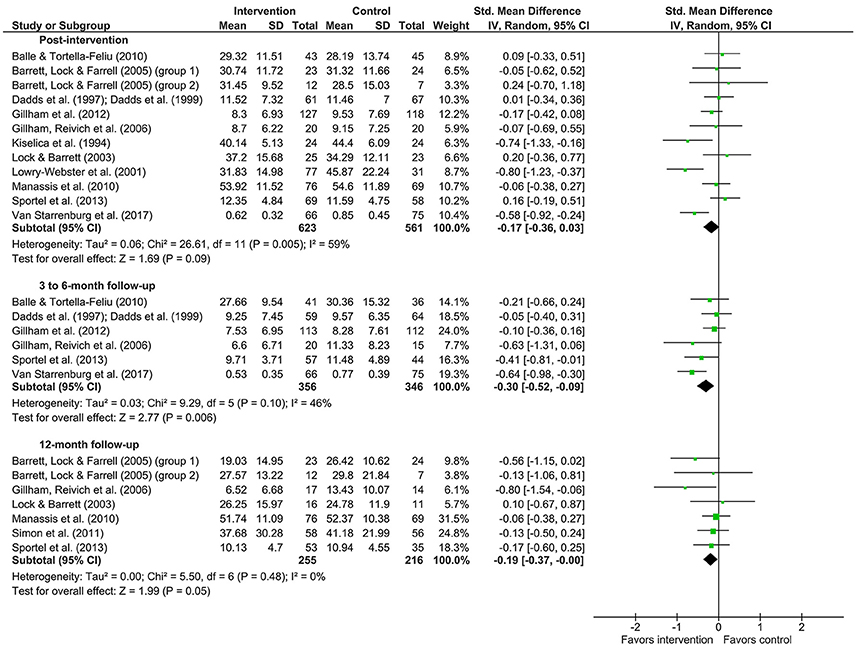
Figure 3. Forest plots of effects of anxiety prevention.
Concerning depression prevention, the meta-analysis showed that there was a small effect in improving depression symptoms post-intervention (20 studies; d = −0.25; 95% CI [−0.38, −0.12]). The meta-analytic Z-test showed a significant effect (Z = 3.83, p < 0.001). The heterogeneity test showed that the results of the various studies were moderately heterogeneous (Tau2 = 0.05, Chi2 = 57.33, p = <0.001; I2 = 67%).
There was no effect of depression prevention 3–6 months after the intervention (18 studies; d = −0.18; 95% CI [−0.31, −0.06]). The meta-analytic Z-test was significant (Z = 2.83, p = 0.005). The heterogeneity test revealed that the included studies were moderately heterogeneous (Tau2 = 0.04, Chi2 = 55.61, p < 0.001; I2 = 69%).
Depression prevention showed no effect (d = −0.01; 95% CI [−0.14, 0.11]) 12 months after the intervention (12 studies). The meta-analytic Z-test showed a non-significant effect (Z = 0.21, p = 0.83). The heterogeneity test showed that the various studies yielded moderate heterogeneous results (Tau2 = 0.02, Chi2 = 30.36, p = 0.001; I2 = 64%).
For anxiety prevention, the effect size (d = −0.17; 95% CI [−0.36,0.03]) for the post-intervention effects (12 studies) showed there was no effect. The meta-analytic Z-test showed a non-significant effect (Z = 1.69, p = 0.09). The heterogeneity test showed that the results of the included studies were moderately heterogeneous (Tau2 = 0.06, Chi2 = 26.61, p = 0.005; I2 = 59%).
Anxiety prevention showed a small effect (d = −0.30; 95% CI [−0.52, −0.09]) 3–6 months after the intervention (6 studies). The meta-analytic Z-test showed a significant effect (Z = 2.77, p = 0.006). The heterogeneity test revealed that the results of the included studies were low heterogeneous (Tau2 = 0.03, Chi2 = 9.29, p = 0.10; I2 = 46%).
Anxiety prevention 12 months after the intervention (7 studies) showed no effect (d = −0.19; 95% CI [−0.37, −0.00]). The meta-analytic Z-test showed a non-significant effect (Z = 1.99, p = 0.05). The heterogeneity test showed that the various studies yielded homogeneous results (Tau2 = 0.00, Chi2 = 5.50, p = 0.48; I2 = 0%).
This review described school-based and community-based prevention programs based on cognitive behavioral therapy with the primary goal of preventing depression and anxiety symptoms in adolescents at risk for developing these disorders. Furthermore, we determined the effectiveness in reducing symptoms of depression and anxiety directly after the intervention and at 3–6 and 12 months after the intervention.
The findings of our study revealed that selective and indicated depression prevention programs using techniques of cognitive behavioral therapy decrease symptoms of depression immediately after the intervention. However, the effects did not seem to last to 3–6 or 12 months after the intervention. In other words, the depression prevention generally decreases the symptoms of depression up to the end of the intervention. With this, the probability of the onset of a full-blown depressive disorder might slightly decrease. For anxiety prevention, we did not find evidence for effects directly after the intervention. However, there was an effect 3–6 to months after the intervention where anxiety prevention seems to reduce anxiety symptoms, although this effect disappeared 12 months after the intervention.
The findings of our study partially reflect the findings from previous research. They also reported the effects of depression prevention directly after the intervention (Horowitz and Garber, 2006; Calear and Christensen, 2010; Merry et al., 2012; Hetrick et al., 2016). In contrast to our study, they also reported effects during follow-ups. They reported, however, on a combination of several approaches of prevention in their studies, such as cognitive behavioral therapy, interpersonal therapy and mindfulness therapy, or focused on only school-based prevention programs, what might be an explanation for the different results. The studies that we included in the meta-analyses utilized a prevention program based on the principles of cognitive behavioral therapy, and therefore our findings can only be generalized to programs based on the cognitive behavioral approach. Cognitive behavioral therapy proved to be effective in treating depression in children and adolescents (Lewinsohn and Clarke, 1999; Michael and Crowley, 2002; Weisz et al., 2006). It is, therefore, likely that when these techniques are used in indicated and selective prevention of depression in adolescents, the results of these interventions are positive. Yet, effects of cognitive behavioral therapy based indicated and selective prevention programs seem to disappear after 3 months, and, therefore, improvements in effects on longer term are necessary before we can conclude that preventive interventions in high-risk populations, namely adolescents with substantial symptoms of depression, are meaningful for prevention of depression. In contrast to another review (Merry et al., 2012; Hetrick et al., 2016), we found no effects of depression prevention 3–6 and 12 months after the intervention. Our findings imply that depression prevention leads to short term symptoms reduction. The absence of an effect at 12 months after the intervention was also seen in the treatment of depression, where follow-ups of 1 year or more showed essentially no treatment effect (Weisz et al., 2006). There are several explanations for not finding an effect 12 months after the intervention. It is known that occasional long-term prevention sessions, so-called booster sessions, reduce the likelihood of relapse of depressive symptoms (Kroll et al., 1996). Without these booster sessions, the effectiveness of a prevention program might diminish during the following period. Most studies included in our meta-analyses did not use booster sessions following the preventive intervention, which might explain why depression prevention programs showed no effect 3–6 and 12 months after the intervention. Further, depression is known for its recurrent course and its fluctuations in level of depression symptoms (Judd et al., 1998; Kennedy and Paykel, 2004; Van Rijsbergen, 2014). This implies that in some adolescents depression symptoms might recur after some time, despite the preventive intervention they received, which is also advocated in different meta-analyses (Stockings et al., 2016). Especially when there is no change in the risk factors, the risk for depression remains high.
In contrast to other studies, we found that anxiety prevention programs did not show significant effects directly after the intervention or 12 months after the intervention (Neil and Christensen, 2009; Christensen et al., 2010), but there was an effect 3–6 months after the interventions. It is noteworthy that the effect sizes directly after the intervention and after 12 months in this study appear to be smaller compared to the effect sizes found in other reviews and meta-analyses. The main difference between our findings and those in other studies (Neil and Christensen, 2009; Christensen et al., 2010) concerns the inclusion criteria of the populations of the included studies. The previous reviews included studies on all types of anxiety prevention programs, namely studies with universal, selective, and indicated prevention programs. We, on the other hand, focused on adolescents at risk and included only studies with selective and indicated prevention programs using techniques of cognitive behavioral therapy. This implies that the severity of anxiety symptoms in our meta-analytic review was higher compared to other reviews, and to illustrate, adolescents in the studies we included reported elevated levels of anxiety up to clinical levels. The samples and the severity of their symptoms might play a role in the difference in outcome of this study and other review studies, more specifically, the level of symptoms might be too high in order for prevention programs to be effective direct after the intervention and for a longer period of time. Although the prevention programs that focused on anxiety used cognitive behavioral techniques, they were mainly based on social skills training (Dadds et al., 1997), relaxation exercises (Balle and Tortella-Feliu, 2010), and cognitive restructuring (Lock and Barrett, 2003). These techniques might be more effective in universal populations without symptoms of anxiety, as mentioned in earlier review studies (Neil and Christensen, 2009; Christensen et al., 2010), than in at-risk population, as in our study. The preventive interventions used in the studies that we reviewed may have lacked strong enough techniques for the prevention of anxiety in at-risk populations with symptoms up to clinical levels. The content of selective and indicated prevention programs for adolescents with elevated levels of anxiety that are almost reaching clinical levels of anxiety should presumably be more similar to the treatment of anxiety, as is done by Van Starrenburg et al. (2017). Therefore, we suggest that preventive interventions for anxiety in at-risk adolescents should not only use cognitive restructuring techniques, but should include exposure techniques and cognitive behavioral therapy as is done in treatment of anxiety disorders (Cartwright-Hatton et al., 2004; Compton et al., 2004; Rapee et al., 2009; Davis et al., 2011). This meta-analytic review focused on the selective and indicated prevention for depression and anxiety using cognitive behavioral therapy, whereas other studies included also universal prevention and other prevention techniques. This allowed us to draw conclusions about the cognitive behavioral therapy based prevention of depression and anxiety in adolescents with high risk for developing these disorders. We included only randomized controlled trials in our meta-analyses, which increased the internal validity of the studies in these meta-analyses. With this in mind, the results of the current studies can be interpreted with confidence. Limitations of the present study can be found in the studies included. The number of participants in some studies was low and differed largely in size across studies. We would like to indicate that the variations in sample size, in techniques used in the interventions, and in inclusion criteria resulted in lower heterogeneity between the anxiety prevention studies than between depression prevention studies. We think, however, that the similarities between the studies are larger than the methodological diversity. Another point of consideration about the lower effect sizes at longer follow-up, is the small number of studies with effects measured at longer follow-up periods. This causes a reduction of power with too few studies available to determine their true impact of selective and indicated prevention. Furthermore, the outcomes might have been influenced by the bias in selective reporting, as only studies with positive results were likely to be published and we selected only published studies. Also, some studies showed a lack of data, which we were not able to retrieve. Therefore, these studies were excluded from the meta-analysis, and this might have resulted in a bias outcome.
A small number of studies was included in the meta-analyses; therefore, potential moderating variables were not tested. Consequently, we cannot draw any conclusions about the influence of, for example, the size of the intervention groups, duration and intensity of the prevention programs, and the selection of the participants in the prevention programs, neither about sociodemographic characteristics, family history of depression, and level of elevated symptoms.
This review presents evidence that cognitive behavioral therapy based prevention of depression in groups for high-risk adolescents is effective in the short term. These at-risk groups mostly have elevated levels of depression, and with these prevention programs their symptoms, and also the risk on a full-blown depressive disorder, reduce. For anxiety, cognitive behavioral therapy based prevention programs appear to be effective after 3–6 months, but this effect disappears after 12 months. The findings of the current meta-analytic review cautiously suggest depression and anxiety prevention programs based on CBT might have small effects on mental health of adolescents, although there should be improvements in effects before supporting the implementation of selective and indicated depression and anxiety prevention programs. It indicates that there is still much to be gained for prevention programs aimed at anxiety prevention. We focused on prevention of depression and anxiety in adolescents at risk using cognitive behavioral techniques. We, therefore, did not include universal prevention studies and studies using other techniques in our meta-analyses. Consequently, we could not compare universal prevention to targeted prevention, and we cannot conclude on about prevention programs based on for example interpersonal therapy or mindfulness therapy. Evaluations of the cost-effectiveness of depression and anxiety prevention should also be done, as they are currently lacking in the prevention literature. We suggest that, based on the similarities between treatment of depressive and anxiety disorder and the targeted prevention, the content of selective and indicated prevention programs for adolescents with subclinical depression and anxiety could profit from including techniques that have shown to be effective in the treatment of depression and anxiety.
SR designed the manuscript, performed literature search, reviewed the literature, analyzed the data, and wrote the manuscript. DC, JJ, and RS contributed to the design of the manuscript, reviewed the literature, and revised the manuscript. All authors approved final version to be published.
This study was funded by a grant from the funding agency ZonMw (project number 159010001) and GGZ Oost Brabant.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank Lieke Wijnhoven and Mandy Gijzen for their contribution to reviewing the articles used in this study.
Aalto-Setala, T., Marttunen, M., Tuulio-Henriksson, A., Poikolainen, K., and Lonnqvist, J. (2002). Depressive symptoms in adolescence as predictors of early adulthood depressive disorders and maladjustment. Am. J. Psychiatry 159, 1235–1237. doi: 10.1176/appi.ajp.159.7.1235
Albano, A. M., Chorpita, B. F., and Barlow, D. H. (2003). “Childhood anxiety disorders,” in Child psychopathology, eds E. J. Mash and R. A. Barkley. 2nd Edn. (New York, NY: Guilford), 279–329.
Auerbach, R. P., Richardt, S., Kertz, S., and Eberhart, N. K. (2012). Cognitive vulnerability, stress generation, and anxiety: symptom clusters and gender differences. Int. J. Cogn. Ther. 5, 50–66. doi: 10.1521/ijct.2012.5.1.50
Balle, M., and Tortella-Feliu, M. (2010). Efficacy of a brief school-based program for selective prevention of childhood anxiety. Anxiety Stress Coping 23, 71–85. doi: 10.1080/10615800802590652
Barrett, P. M., Lock, S., and Farrell, L. J. (2005). Developmental differences in universal preventive intervention for child anxiety. Clin. Child Psychol. Psychiatry 10, 539–555. doi: 10.1177/1359104505056317
Beesdo, K., Knappe, S., and Pine, D. S. (2009). Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr. Clin. North Am. 32, 483–524. doi: 10.1016/j.psc.2009.06.002
Beidel, D. C., and Turner, S. M. (1997). At risk for anxiety: I. Psychopathology in the offspring of anxious parents. J. Am. Acad. Child Adolesc. Psychiatry 36, 918–924. doi: 10.1097/00004583-199707000-00013
Bijl, R. V., Cuijpers, P., and Smit, F. (2002). Psychiatric disorders in adult children of parents with a history of psychopathology. Soc. Psychiatry Psychiatr. Epidemiol. 37, 7–12. doi: 10.1007/s127-002-8208-8
Birmaher, B., Ryan, N. D., Williamson, D. E., Brent, D. A., Kaufman, J., Dahl, R. E., et al. (1996). Childhood and adolescent depression: a review of the past 10 years, Part I. J. Am. Acad. Child Adolesc. Psychiatry 35, 1427–1439. doi: 10.1097/00004583-199611000-00011
Butler, A. C., Chapman, J. E., Forman, E. M., and Beck, A. T. (2006). The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin. Psychol. Rev. 26, 17–31. doi: 10.1016/j.cpr.2005.07.003
Calear, A. L., and Christensen, H. (2010). Systematic review of school-based prevention and early intervention programs for depression. J. Adolesc. 33, 429–438. doi: 10.1016/j.adolescence.2009.07.004
Cartwright-Hatton, S., Roberts, C., Chitsabesan, P., Fothergill, C., and Harrington, R. (2004). Systematic review of the efficacy of cognitive behaviour therapies for childhood and adolescent anxiety disorders. Br. J. Clin. Psychol. 43, 421–436. doi: 10.1348/0144665042388928
Christensen, H., Pallister, E., Smale, S., Hickie, I. B., and Calear, A. L. (2010). Community-based prevention programs for anxiety and depression in youth: a systematic review. J. Prim. Prev. 31, 139–170. doi: 10.1007/s10935-010-0214-8
Clarke, G. N., Hawkins, W., Murphy, M., Sheeber, L. B., Lewinsohn, P. M., and Seeley, J. R. (1995). Targeted prevention of unipolar depressive disorder in an at-risk sample of high school adolescents: a randomized trial of a group cognitive intervention. J. Am. Acad. Child Adolesc. Psychiatry 34, 312–321. doi: 10.1097/00004583-199503000-00016
Clarke, G. N., Hornbrook, M., Lynch, F. L., Polen, M., Gale, J., Beardslee, W. R., et al. (2001). A randomized trial of a group cognitive intervention for preventing depression in adolescent offspring of depressed parents. Arch. Gen. Psychiatry 58, 1127–1134. doi: 10.1001/archpsyc.58.12.1127
Cohen, J. (1977). Statistical Power Analysis for the Behavioral Sciences. New York, NY: Academic Press.
Compton, S. N., March, J. S., Brent, D. A., Albano, A. M., Weersing, V. R., and Curry, J. (2004). Cognitive-behavioral psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. J. Am. Acad. Child Adolesc. Psychiatry 43, 930–959. doi: 10.1097/01.chi.0000127589.57468.bf
Copeland, W. E., Angold, A., Shanahan, L., and Costello, E. J. (2014). Longitudinal patterns of anxiety from childhood to adulthood: the great smoky mountains study. J. Am. Acad. Child Adolesc. Psychiatry 53, 21–33. doi: 10.1016/j.jaac.2013.09.017
Costello, J. E., Erkanli, A., and Angold, A. (2006). Is there an epidemic of child or adolescent depression? J. Child Psychol. Psychiatry 47, 1263–1271. doi: 10.1111/j.1469-7610.2006.01682.x
Dadds, M. R., Spence, S. H., Holland, D. E., Barrett, P. M., and Laurens, K. R. (1997). Prevention and early intervention for anxiety disorders: a controlled trial. J. Consult. Clin. Psychol. 65, 627–635. doi: 10.1037/0022-006X.65.4.627
Davis, T. E. III., May, A., and Whiting, S. E. (2011). Evidence-based treatment of anxiety and phobia in children and adolescents: current status and effects on the emotional response. Clin. Psychol. Rev. 31, 592–602. doi: 10.1016/j.cpr.2011.01.001
Dobson, K. S., Hopkins, J. A., Fata, L., Scherrer, M., and Allan, L. C. (2010). The prevention of depression and anxiety in a sample of high-risk adolescents: a randomized controlled trial. Can. J. School Psychol. 25, 291–310. doi: 10.1177/0829573510386449
Fisak, B. J. Jr., Richard, D., and Mann, A. (2011). The prevention of child and adolescent anxiety: a meta-analytic review. Prevent. Sci. 12, 255–268. doi: 10.1007/s11121-011-0210-0
Fox, J. K., Halpern, L. F., Ryan, J. L., and Lowe, K. A. (2010). Stressful life events and the tripartite model: relations to anxiety and depression in adolescent females. J. Adolesc. 33, 43–54. doi: 10.1016/j.adolescence.2009.05.009
Gaete, J., Martinez, V., Fritsch, R., Rojas, G., Montgomery, A. A., and Araya, R. (2016). Indicated school-based intervention to improve depressive symptoms among at risk Chilean adolescents: a randomized controlled trial. BMC Psychiatry 16:267. doi: 10.1186/s12888-016-0985-4
Garber, J., Clarke, G. N., Weersing, V. R., Beardslee, W. R., Brent, D. A., Gladstone, T. R., et al. (2009). Prevention of depression in at-risk adolescents: a randomized controlled trial. JAMA 301, 2215–2224. doi: 10.1001/jama.2009.788
Garber, J., Keiley, M. K., and Martin, N. C. (2002). Developmental trajectories of adolescents' depressive symptoms: predictors of change. J. Consult. Clin. Psychol. 70, 79–95. doi: 10.1037/0022-006X.70.1.79
Garber, J., and Weersing, V. R. (2010). Comorbidity of anxiety and depression in youth: implications for treatment and prevention. Clin. Psychol. 17, 293–306. doi: 10.1111/j.1468-2850.2010.01221.x
Ge, X., Lorenz, F. O., Conger, R. D., Elder, G. H., and Simons, R. L. (1994). Trajectories of stressful life events and depressive symptoms during adolescence. Dev. Psychol. 30, 467–483. doi: 10.1037/0012-1649.30.4.467
Gillham, J. E., Hamilton, J., Freres, D. R., Patton, K., and Gallop, R. (2006a). Preventing depression among early adolescents in the primary care setting: a randomized controlled study of the Penn Resiliency Program. J. Abnorm. Child Psychol. 34, 203–219. doi: 10.1007/s10802-005-9014-7
Gillham, J. E., Reivich, K. J., Brunwasser, S. M., Freres, D. R., Chajon, N. D., Kash-Macdonald, V. M., et al. (2012). Evaluation of a group cognitive-behavioral depression prevention program for young adolescents: a randomized effectiveness trial. J. Clin. Child Adolesc. Psychol. 41, 621–639. doi: 10.1080/15374416.2012.706517
Gillham, J. E., Reivich, K. J., Freres, D. R., Lascher, M., Litzinger, S., Shatté, A., et al. (2006b). School-based prevention of depression and anxiety symptoms in early adolescence: a pilot of a parent intervention component. School Psychol. Q. 21, 323–348. doi: 10.1521/scpq.2006.21.3.323
Grant, K. E., Compas, B. E., Thurm, A. E., Mcmahon, S. D., and Gipson, P. Y. (2004). Stressors and child and adolescent psychopathology: measurement issues and prospective effects. J. Clin. Child Adolesc. Psychol. 33, 412–425. doi: 10.1207/s15374424jccp3302_23
Hankin, B. L., Abramson, L. Y., Moffitt, T. E., Silva, P. A., Mcgee, R., and Angell, K. E. (1998). Development of depression from preadolescence to young adulthood: emerging gender differences in a 10-year longitudinal study. J. Abnorm. Psychol. 107, 128–140. doi: 10.1037/0021-843X.107.1.128
Hetrick, S. E., Cox, G. R., and Merry, S. N. (2015). Where to go from here? An exploratory meta-analysis of the most promising approaches to depression prevention programs for children and adolescents. Int. J. Environ. Res. Public Health 12, 4758–4795. doi: 10.3390/ijerph120504758
Hetrick, S. E., Cox, G. R., Witt, K. G., Bir, J. J., and Merry, S. N. (2016). Cognitive behavioural therapy (CBT), third-wave CBT and interpersonal therapy (IPT) based interventions for preventing depression in children and adolescents. Cochrane Database Syst. Rev. 9:CD003380. doi: 10.1002/14651858.CD003380.pub4
Higgins, J. P., and Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558. doi: 10.1002/sim.1186
Hofmann, S. G., Asnaani, A., Vonk, I. J., Sawyer, A. T., and Fang, A. (2012). The efficacy of cognitive behavioral therapy: a review of meta-analyses. Cognit. Ther. Res. 36, 427–440. doi: 10.1007/s10608-012-9476-1
Horowitz, J. L., and Garber, J. (2006). The prevention of depressive symptoms in children and adolescents. A meta analytic review. J. Consulting Clin. Psychol. 74, 401–415. doi: 10.1037/0022-006X.74.3.401
Hyun, M. S., Chung, H. I., and Lee, Y. J. (2005). The effect of cognitive-behavioral group therapy on the self-esteem, depression, and self-efficacy of runaway adolescents in a shelter in South Korea. Appl. Nurs. Res. 18, 160–166. doi: 10.1016/j.apnr.2004.07.006
Judd, L. L., Akiskal, H. S., Maser, J. D., Zeller, P. J., Endicott, J., Coryell, W., et al. (1998). A prospective 12-year study of subsyndromal and syndromal depressive symptoms in unipolar major depressive disorders. Arch. Gen. Psychiatry 55, 694–700. doi: 10.1001/archpsyc.55.8.694
Kashani, J. H., Vaidya, A. F., Soltys, S. M., Dandoy, A. C., Katz, L. M., and Reid, J. C. (1990). Correlates of anxiety in psychiatrically hospitalized children and their parents. Am. J. Psychiatry 147, 319–323. doi: 10.1176/ajp.147.3.319
Kennedy, N., and Paykel, E. S. (2004). Residual symptoms at remission from depression: impact on long-term outcome. J. Affect. Disord. 80, 135–144. doi: 10.1016/S0165-0327(03)00054-5
Kessler, R. C., Avenevoli, S., and Merikangas, K. R. (2001). Mood disorders in children and adolescents: an epidemiologic perspective. Biol. Psychiatry 49, 1002–1014. doi: 10.1016/S0006-3223(01)01129-5
Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., and Wittchen, H. U. (2012). Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 21, 169–184. doi: 10.1002/mpr.1359
Kindt, K., Kleinjan, M., Janssens, J. M. A. M., and Scholte, R. H. J. (2014). Evaluation of a school-based depression prevention program among adolescents from low-income areas: a randomized controlled effectiveness trial. Int. J. Environ. Res. Public Health 11, 5273–5293. doi: 10.3390/ijerph110505273
Kiselica, M. S., Baker, S. B., Thomas, R. N., and Reedy, S. (1994). Effects of stress inoculation training on anxiety, stress, and academic performance among adolescents. J. Couns. Psychol. 41, 335–342. doi: 10.1037/0022-0167.41.3.335
Kowalenko, N. (2005). Short-term Effectiveness of a school-based early intervention program for adolescent depression. Clin. Child Psychol. Psychiatry 10, 493–507. doi: 10.1177/1359104505056311
Kroll, L., Harrington, R., Jayson, D., Fraser, J., and Gowers, S. (1996). Pilot study of continuation cognitive-behavioral therapy for major depression in adolescent psychiatric patients. J. Am. Acad. Child Adolesc. Psychiatry 35, 1156–1161. doi: 10.1097/00004583-199609000-00013
Larson, R., and Ham, M. (1993). Stress and “storm and stress” in early adolescence: the relationship of negative events with dysphoric affect. Dev. Psychol. 29, 130–140. doi: 10.1037/0012-1649.29.1.130
Lewinsohn, P. M., and Clarke, G. N. (1999). Psychosocial treatments for adolescent depression. Clin. Psychol. Rev. 19, 329–342. doi: 10.1016/S0272-7358(98)00055-5
Lewinsohn, P. M., Solomon, A., Seeley, J. R., and Zeiss, A. (2000). Clinical implications of “subthreshold” depressive symptoms. J. Abnorm. Psychol. 109, 345–351. doi: 10.1037/0021-843X.109.2.345
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gotzsche, P. C., Ioannidis, J. P., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 6:e1000100. doi: 10.1371/journal.pmed.1000100
Lieb, R., Isensee, B., Höfler, M., Pfister, H., and Wittchen, H. U. (2002). Parental major depression and the risk of depression and other mental disorders in offspring: a prospective-longitudinal community study. Arch. Gen. Psychiatry 59, 365–374. doi: 10.1001/archpsyc.59.4.365
Lock, S., and Barrett, P. M. (2003). A longitudinal study of developmental differences in universal preventive intervention for child anxiety. Behav. Change 20, 183–199. doi: 10.1375/bech.20.4.183.29383
Lowry-Webster, H. M., Barrett, P. M., and Dadds, M. R. (2001). A universal prevention trial of anxiety and depressive symptomatology in childhood: preliminary data from an Australian study. Behav. Change 18, 36–50. doi: 10.1375/bech.18.1.36
Manassis, K., Wilansky-Traynor, P., Farzan, N., Kleiman, V., Parker, K., and Sanford, M. (2010). The feelings club: randomized controlled evaluation of school-based CBT for anxious or depressive symptoms. Depress. Anxiety 27, 945–952. doi: 10.1002/da.20724
Merikangas, K. R., Dierker, L. C., and Szatmari, P. (1998). Psychopathology among offspring of parents with substance abuse and/or anxiety disorders: a high-risk study. J. Child Psychol. Psychiatry Allied Discip. 39, 711–720. doi: 10.1017/S0021963098002522
Merry, S. N., Hetrick, S. E., Cox, G. R., Brudevold-Iversen, T., Bir, J. J., and Mcdowell, H. (2012). Cochrane review: psychological and educational interventions for preventing depression in children and adolescents. Evid. Based Child Health 7, 1409–1685. doi: 10.1002/ebch.1867
Micco, J. A., Henin, A., Mick, E., Kim, S., Hopkins, C. A., Biederman, J., et al. (2009). Anxiety and depressive disorders in offspring at high risk for anxiety: a meta-analysis. J. Anxiety Disord. 23, 1158–1164. doi: 10.1016/j.janxdis.2009.07.021
Michael, K. D., and Crowley, S. L. (2002). How effective are treatments for child and adolescent depression?: a meta-analytic review. Clin. Psychol. Rev. 22, 247–269. doi: 10.1016/S0272-7358(01)00089-7
Mrazek, P. J., and Haggerty, R. J. (1994). Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. Washington, DC: National Academy Press.
Neil, A. L., and Christensen, H. (2009). Efficacy and effectiveness of school-based prevention and early intervention programs for anxiety. Clin. Psychol. Rev. 29, 208–215. doi: 10.1016/j.cpr.2009.01.002
Pine, D. S., Cohen, E., Cohen, P., and Brook, J. (1999). Adolescent depressive symptoms as predictors of adult depression: moodiness or mood disorder? Am. J. Psychiatry 156, 133–135. doi: 10.1176/ajp.156.1.133
Poppelaars, M., Tak, Y. R., Lichtwarck-Aschoff, A., Engels, R. C. M. E., Lobel, A., Merry, S. N., et al. (2016). A randomized controlled trial comparing two cognitive-behavioral programs for adolescent girls with subclinical depression: a school-based program (Op Volle Kracht) and a computerized program (SPARX). Behav. Res. Ther. 80, 33–42. doi: 10.1016/j.brat.2016.03.005
Puskar, K. R., Sereika, S. M., and Tusaie-Mumford, K. (2003). Effect of the Teaching Kids to Cope (TKC) program on outcomes of depression and coping among rural adolescents. J. Child Adolesc. Psychiatr. Nurs. 16, 71–80. doi: 10.1111/j.1744-6171.2003.tb00350.x
Rapee, R. M., Schniering, C. A., and Hudson, J. L. (2009). Anxiety disorders during childhood and adolescence: origins and treatment. Annu. Rev. Clin. Psychol. 5, 311–341. doi: 10.1146/annurev.clinpsy.032408.153628
Roberts, C., Kane, R., Thomson, H., Bishop, B., and Hart, B. (2003). The prevention of depressive symptoms in rural school children: a randomized controlled trial. J. Consult. Clin. Psychol. 71, 622–628. doi: 10.1037/0022-006X.71.3.622
Rohde, P., Stice, E., Shaw, H., and Brière, F. N. (2014). Indicated cognitive behavioral group depression prevention compared to bibliotherapy and brochure control: acute effects of an effectiveness trial with adolescents. J. Consult. Clin. Psychol. 82:65. doi: 10.1037/a0034640
Roza, S. J., Hofstra, M. B., Van Der Ende, J., and Verhulst, F. C. (2003). Stable prediction of mood and anxiety disorders based on behavioral and emotional problems in childhood: a 14-year follow-up during childhood, adolescence, and young adulthood. Am. J. Psychiatry 160, 2116–2121. doi: 10.1176/appi.ajp.160.12.2116
Rudolph, K. D., and Hammen, C. (1999). Age and gender as determinants of stress exposure, generation, and reactions in youngsters: a transactional perspective. Child Dev. 70, 660–677. doi: 10.1111/1467-8624.00048
Sheffield, J. K., Spence, S. H., Rapee, R. M., Kowalenko, N., Wignall, A., Davis, A., et al. (2006). Evaluation of universal, indicated, and combined cognitive-behavioral approaches to the prevention of depression among adolescents. J. Consult. Clin. Psychol. 74, 66–79. doi: 10.1037/0022-006X.74.1.66
Simon, E., Bogels, S. M., and Voncken, J. M. (2011). Efficacy of child-focused and parent-focused interventions in a child anxiety prevention study. J. Clin. Child. Adolesc. Psychol. 40, 204–219. doi: 10.1080/15374416.2011.546039
Singhal, M., Manjula, M., and Vijay Sagar, K. J. (2014). Development of a school-based program for adolescents at-risk for depression in India: results from a pilot study. Asian J. Psychiatr. 10, 56–61. doi: 10.1016/j.ajp.2014.03.011
Smit, F., Bohlmeijer, E. T., and Cuijpers, W. J. M. J. (2003). Wetenschappelijke Onderbouwing Depressiepreventie: Epidemiologie, Aangrijpingspunten, Huidige Praktijk, Nieuwe Richtingen [Evidence Based Depression Prevention: Epidemiology, Pivotal Points, Current Practice and New Directions]. Utrecht: Trimbos Institute.
Sportel, B. E., De Hullu, E., De Jong, P. J., and Nauta, M. H. (2013). Cognitive bias modification versus cbt in reducing adolescent social anxiety: a randomized controlled trial. PLoS ONE 8:e64355. doi: 10.1371/journal.pone.0064355
Stallard, P., Phillips, R., Montgomery, A. A., Spears, M., Anderson, R., Taylor, J., et al. (2013). A cluster randomised controlled trial to determine the clinical effectiveness and cost-effectiveness of classroom-based cognitive–behavioural therapy (CBT) in reducing symptoms of depression in high-risk adolescents. Health Technol. Assess. 17, 1–109. doi: 10.3310/hta17470
Stallard, P., Sayal, K., Phillips, R., Taylor, J. A., Spears, M., Anderson, R., et al. (2012). Classroom based cognitive behavioural therapy in reducing symptoms of depression in high risk adolescents: pragmatic cluster randomised controlled trial. BMJ 345:e6058. doi: 10.1136/bmj.e6058
Stice, E., Burton, E., Bearman, S. K., and Rohde, P. (2007). Randomized trial of a brief depression prevention program: an elusive search for a psychosocial placebo control condition. Behav. Res. Ther. 45, 863–876. doi: 10.1016/j.brat.2006.08.008
Stice, E., Rohde, P., Gau, J. M., and Wade, E. (2010). Efficacy trial of a brief cognitive-behavioral depression prevention program for high-risk adolescents: effects at 1- and 2-year follow-up. J. Consult. Clin. Psychol. 78, 856–867. doi: 10.1037/a0020544
Stice, E., Shaw, H., Bohon, C., Marti, C. N., and Rohde, P. (2009). A meta-analytic review of depression prevention programs for children and adolescents: factors that predict magnitude of intervention effects. J. Consult. Clin. Psychol. 77, 486–503. doi: 10.1037/a0015168
Stockings, E. A., Degenhardt, L., Dobbins, T., Lee, Y. Y., Erskine, H. E., Whiteford, H. A., et al. (2016). Preventing depression and anxiety in young people: a review of the joint efficacy of universal, selective and indicated prevention. Psychol. Med. 46, 11–26. doi: 10.1017/S0033291715001725
Strauss, C. C., Frame, C. L., and Forehand, R. (1987). Psychosocial impairment associated with anxiety in children. J. Clin. Child Psychol. 16, 235–239. doi: 10.1207/s15374424jccp1603_8
Teubert, D., and Pinquart, M. (2011). A meta-analytic review on the prevention of symptoms of anxiety in children and adolescents. J. Anxiety Disord. 25, 1046–1059. doi: 10.1016/j.janxdis.2011.07.001
Van Dorsselaer, S., De Graaf, R., Verdurmen, J., Van 'T Land, H., Ten Have, M., and Vollebergh, W. (2006). Trimbos Kerncijfers Psychische Stoornissen: Resultaten Van Nemesis [Trimbos Key Figures Mental Disorders: Results of NEMESIS] (Netherlands Mental Health Survey and Incidence Study) Utrecht: Trimbos Institute.
Van Rijsbergen, G. D. V. (2014). Depression Vulnerability: is it Really What You Think?: Understanding the Impact of Emotion and Cognition on the Course of Depression. University of Groningen.
Van Starrenburg, M. L. A., Kuijpers, R. C. M. W., Kleinjan, M., Hutschemaekers, G. J. M., and Engels, R. C. M. E. (2017). Effectiveness of a cognitive behavioral therapy-based indicated prevention program for children with elevated anxiety levels: a randomized controlled trial. Prevent. Sci. 18, 31–39. doi: 10.1007/s11121-016-0725-5
Weissman, M. M., Wickramaratne, P., Nomura, Y., Warner, V., Pilowsky, D., and Verdeli, H. (2006). Offspring of depressed parents: 20 years later. Am. J. Psychiatry 163, 1001–1008. doi: 10.1176/ajp.2006.163.6.1001
Weisz, J. R., Mccarty, C. A., and Valeri, S. M. (2006). Effects of psychotherapy for depression in children and adolescents: a meta-analysis. Psychol. Bull. 132, 132–149. doi: 10.1037/0033-2909.132.1.132
Wijnhoven, L. A. M. W., Creemers, D. H. M., Vermulst, A. A., Scholte, R. H. J., and Engels, R. C. M. E. (2014). Randomized controlled trial testing the effectiveness of a depression prevention program (‘Op Volle Kracht’) among adolescent girls with elevated depressive symptoms. J. Abnorm. Child Psychol. 42, 217–228. doi: 10.1007/s10802-013-9773-5
Keywords: prevention, depression, anxiety, cognitive behavioral therapy, adolescents, meta-analysis, indicated, selective
Citation: Rasing SPA, Creemers DHM, Janssens JMAM and Scholte RHJ (2017) Depression and Anxiety Prevention Based on Cognitive Behavioral Therapy for At-Risk Adolescents: A Meta-Analytic Review. Front. Psychol. 8:1066. doi: 10.3389/fpsyg.2017.01066
Received: 18 November 2015; Accepted: 09 June 2017;
Published: 28 June 2017.
Edited by:
Xavier Noel, Free University of Brussels, BelgiumReviewed by:
Giuliano Emerenciano Ginani, Uniamérica, BrazilCopyright © 2017 Rasing, Creemers, Janssens and Scholte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sanne P. A. Rasing, cy5yYXNpbmdAYnNpLnJ1Lm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.