 Akseli Laaksi1*
Akseli Laaksi1* Ilkka Laaksi1,2
Ilkka Laaksi1,2 Harri Pihlajamäki1,3
Harri Pihlajamäki1,3 Jani P. Vaara4Tiina Luukkaala5,6
Jani P. Vaara4Tiina Luukkaala5,6 Heikki Kyröläinen4,7
Heikki Kyröläinen4,7- 1Faculty of Medicine and Health Technology, University of Tampere, Tampere, Finland
- 2Centre for Military Medicine, Finnish Defence Forces, Riihimäki, Finland
- 3Department of Orthopedics and Traumatology, Seinäjoki Central Hospital, Seinäjoki, Finland
- 4Department of Leadership and Military Pedagogy, National Defence University, Helsinki, Finland
- 5Research, Development and Innovation Centre, Tampere University Hospital, Tampere, Finland
- 6Health Sciences, Faculty of Social Sciences, University of Tampere, Tampere, Finland
- 7Faculty of Sport and Health Sciences, University of Jyväskylä, Jyväskylä, Finland
Purpose: The present study examined the association of vitamin D measured by serum 25(OH)D with physical performance outcomes and serum levels of anabolic hormones in young men.
Methods: 412 young men (age 19 ± 1 year) entering their compulsory military service volunteered to participate in the study. The study consisted of two groups from two different military bases: Group A was studied in January and group B in July. The groups were first compared with each other and due to statistically significant (p < 0.001 analyzed with independent samples t-test) differences in physical condition (sit-up, push-up, and standing long jump-tests and testosterone levels) between the groups, groups were analyzed separately. The serum levels of 25(OH)D, testosterone (TES), sex hormone binding globulin (SHBG), and insulin-like growth factor-1 (IGF-1) were analyzed by electrochemiluminescence immunoassay. Physical performance tests consisted of muscular fitness (sit-ups, push-ups, standing long jump) and aerobic fitness (12-minute-running) tests. The association of serum 25(OH)D with physical performance tests and anabolic hormones was analyzed using linear regression.
Results: After controlling for the group, body mass index, and leisure-time physical activity, serum 25(OH)D level was positively associated with aerobic and muscular fitness (β = 0.15–0.20, all p < 0.05). Also, the participants with sufficient serum 25(OH)D levels (≥75 nmol/L) had better aerobic and muscular fitness and higher TES in group B, and better upper extremity muscular fitness in group A (all p < 0.05). In group A, there were 166 participants with serum levels of 25(OH) D < 75 nmol/L and 18 ≥ 75 nmol/L. In group B, the amounts were 92 (<75 nmol/L) and 136 (≥75 nmol/L), respectively.
Conclusion: Serum 25(OH)D was positively associated with both aerobic and muscular fitness and those with sufficient vitamin D levels, had higher levels of TES. Thus, maintaining a sufficient serum 25(OH)D level may be beneficial for physical performance and anabolic state in young men.
1 Introduction
Vitamin D is primarily produced endogenously in the skin from 7-dehydrocholesterol, which is induced by ultraviolet B radiation (UVB) from the sun. In addition to endogenous production, vitamin D can be obtained from the diet, such as fatty fish, fortified dairy products, and dietary supplements. Vitamin D is metabolized in the body by hydroxylation in the liver to 25(OH)D, which is then transported to the kidneys or target tissues to be hydroxylated again to its most active form of 1,25(OH)2D (Holick, 2007). After the second hydroxylation vitamin D mediates its effects through a specific receptor in cells called vitamin D receptor (VDR) (Haussler et al., 1998). Vitamin D status is assessed by serum 25(OH)D levels (Utiger, 1998). The Nordic Nutrition Recommendations set 50 nmol/L in serum 25(OH)D as a lower limit value for vitamin D sufficiency (Nordic Council of Ministers, 2014). However, the Global Endocrine Society’s Practice Guidelines Committee recommends that a serum 25(OH)D level of ≥75 nmol/L is considered sufficient for musculoskeletal health (Holick, 2017).
Vitamin D is known to have an important role in bone metabolism by promoting intestinal calcium and phosphate absorption, renal tubular calcium reabsorption, and calcium mobilization from the bone by its most active form of 1,25(OH)2D (Charoenngam et al., 2019). However, it is not so well-known that vitamin D may also be associated with physical performance. In cross-sectional studies among healthy adults and athletes, vitamin D has been found to be positively associated with muscular power and strength (Hamilton et al., 2014; Koundourakis et al., 2014; Hildebrand et al., 2016) and aerobic performance (Koundourakis et al., 2014; Carswell et al., 2018; Zeitler et al., 2018). Nevertheless, a narrative review showed that the association between vitamin D and physical performance in athletes has been inconclusive (Ksiażek et al., 2019), while there exists only a limited number of studies among healthy adults.
The beneficial effects of vitamin D on physical performance may exist through increasing blood levels of anabolic hormones such as testosterone (TES) and insulin-like growth factor-I (IGF-1). A large (n = 20 567) systematic review and meta-analysis showed an association between vitamin D deficiency and decreased testosterone levels (D’Andrea et al., 2021). A positive correlation between serum 25(OH)D level and IGF-1 has been found in several observational studies as well (Forouhi et al., 2008; Bogazzi et al., 2011; Ameri et al., 2013a). However, studies that have examined the association of these hormones with serum 25(OH)D together with physical performance are rare. In addition to TES level, it is important to measure sex hormone binding globulin (SHBG) as the circulating TES is mostly bound on albumin and SHBG, and thus high SHBG could indicate lower bioavailable TES (Goldman et al., 2017).
Therefore, the present cross-sectional study aimed to examine whether there is an association between 25(OH)D levels, physical performance (aerobic and muscular fitness), and anabolic hormones in young men. It was hypothesized that serum 25(OH)D levels would have positive associations with physical performance and levels of anabolic hormones.
2 Materials and methods
2.1 Participants
Young men (n = 412; age 19 ± 1 year, height 179 ± 7 cm, body mass 75 ± 13 kg, body mass index 24.0 ± 3.7), performing their compulsory military service, volunteered to participate in the present study. Written informed consent was given to the participants after passing the military entry medical examination as healthy. The present study has been approved by the Ethics Committee of the Pirkanmaa Hospital District, ETL code R17155, HUS/1557/2018, and the Finnish Defence Forces (AN21508, AP10027, AQ24718, AR13336).
2.2 Study protocol
The present cross-sectional study had two separate groups: group A (n = 184) and group B (n = 228) in two different military units in Finland. Groups were compared and then analyzed separately due to differences in physical performance; the participants in group A were conducting their military service in rapid deployment forces that requires better physical condition than a standard military service in Finland. The physical performance tests were arranged during the first 2 weeks of military service. In group A, the blood samples were drawn in the winter (January), while in another location (group B), the blood samples were drawn in the summer (July). In northern latitude countries, such as Finland, an adequate amount of sunlight exposure for vitamin D production in the skin is possible only between March and October (Engelsen et al., 2005). In addition, levels of serum TES, SHBG, and IGF-1 were analyzed for evaluating the anabolic status of the participants. The physical performance was studied by conducting sit-up, push-up, standing long jump, and 12-min running tests. The level of ≥75 nmol/L of serum 25(OH)D was used as sufficient in the present study. Group, body mass index (BMI), and leisure-time activity were used as covariates. Group was used as a covariate because the groups were measured during different seasons (summer/winter) and therefore, this difference can affect vitamin D levels through differences in sunlight exposure and further because there were fundamental differences in physical performance between the groups. BMI was selected due to its effects on serum 25(OH)D levels and physical performance. Leisure-time physical activity was selected for its effect on physical performance and the possible effect on serum 25(OH)D levels if the participants spend a lot of time outdoors while exercising and are thus more exposed to the sun.
2.3 Blood analyzes
After the venous blood samples were obtained from the antecubital vein, the samples were centrifuged at 2000 g for 20 min at room temperature for serum separation. Serum samples were then frozen and stored at −20°C for later analysis. The measurements of serum 25(OH)D were performed using electrochemiluminescence immunoassays (ECLIA). Levels of TES and SHBG were measured by electrochemiluminescence immunoassay (Immulite 100; Siemens Healthcare Diagnostics Products Ltd., Gwynedd, United Kingdom). IGF-1 was analyzed by electrochemiluminescence immunoassay (Siemens Immulite 2000 XPI, Siemens Healthcare Diagnostics Products Ltd., Gwynedd, United Kingdom). The inter-assay coefficients of variance (CV) for assays of TES, SHBG, and IGF-I were 7.0%–7.2%, 4.5%–6.2%, and 3.7%–7.4%, and that of sensitivity 0.5 nmol/L, 0.02 nmol/L, and 2.6 nmol/L, respectively.
2.4 Physical performance
Aerobic performance was measured by a 12-min running test, an explosive power output of the lower limbs by a standing long jump test, and dynamic muscular endurance by 1-min push-up and sit-up tests. In the 12-min running test, participants try to run as far as possible in the given time. The results can be used to estimate the maximum oxygen uptake (VO2 max) of the participants by using the formula:
The purpose of the standing long jump is to evaluate the maximum and explosive power output of the lower limbs. In the present study, the standing long jump was performed three times, starting on the ground level with the legs close to each other. Explosive bilateral takeoff was assisted by powerful swinging of the upper body and arms. The landing of each jump was performed bilaterally. The result of the best jump was expressed in meters as the shortest distance from the landing to the starting line, and the best result was taken for further analysis. Adequate recovery time (2–3 min) between performances was used. Standing long jump test reliability coefficients have been shown to vary between 0.93 and 0.96 (Markovic et al., 2004).
Dynamic muscular endurance of the abdominal and hip flexor muscles was measured by performing the sit-ups for as many repetitions as possible in 60 s. Sit-ups were done with each participant lying on the floor with hands behind his neck and directing his elbows forward. The knees were flexed at an angle of 90 deg with the legs slightly abducted. During the movement, each participant lifted his upper body and touched his elbows to his knees. The partner supports the performer’s ankles, following the correct performance technique and counting the number of repetitions (Viljanen et al., 1991).
The dynamic strength and endurance of the muscles of the shoulder area and upper extremities, as well as the static endurance of the muscles supporting the movement, are assessed by performing as many push-ups as possible in 60 s. Push-ups were started from the lowest face-down position. Each participant’s hands were kept at shoulder-width and level. The fingers were directed forward, and the legs were kept parallel and close to each other. During the movement, the arms were fully extended, and the torso was straightly tensed. In the second phase, the torso was lowered down to an elbow angle of 90°. The result of this test was expressed as the number of push-ups completed in 60 s [ACSM’s Guidelines for Exercise Testing and Prescription, 2000 (ACSM, 2000)]. The reliabilities for both the sit-up and the push-up tests have been reported to be high (intraclass correlation values ranged from 0.92 to 0.95) (Ryman Augustsson et al., 2009).
The results of the push-up, sit-up, and standing long jump tests were transformed into z-scores by standardizing them to be co-dimensional with each other. Then the mean of each z-score formed a common continuous variable, called muscular fitness index (MFI), as reported previously (Vaara et al., 2014).
Leisure-time physical activity was studied from self-fillable questionnaires. Participants responded to questions “How many times a week on average do you do endurance-type exercise?” and “How many times a week on average do you engage in exercise that develops muscular strength (e.g., gym training)?” (Think about the last 3 months) with eight response categories: 1 = none; 2 = once a week; 3 = 2 times a week; 4 = 3 times a week; 5 = 4 times a week; 6 = 5 times a week; 7 = 6 times a week; 8 = 7 times or more per week. In general, regarding physical activity questionnaires, acceptable to good reliability but poor to moderate validity has been reported (Helmerhorst et al., 2012).
2.5 Statistical analysis
Bivariate Pearson’s correlations (r) between serum 25(OH)D and physical performance, anabolic hormone levels, and controlling covariates were performed to show the logical progression of statistical choices and to confirm the relevance of candidate covariates. Then linear regression was used to assess the association of serum 25(OH)D levels with physical performance and anabolic hormone after controlling for the group, BMI, and leisure-time physical activity. The size of the analyzed data in multivariable-adjusted analyses varied from n = 329 to n = 349 due to some missing data in variables of BMI and leisure-time physical activity (n = 24), and physical performance and anabolic hormones variables themselves (see Table 2). Additionally, the groups were analyzed separately by dividing them into subgroups using a sufficient level of serum 25(OH)D ≥ 75 nmol/L (Holick, 2017) as a limit value. Differences in outcome variables between the subgroups were analyzed using independent samples t-tests. The results of the t-tests have been reported according to whether the equivalence of the variances has been assumed or not. Statistical analyses were performed with IBM SPSS Statistics for Macintosh, Version 27.0. Armonk, NY: IBM Corp (released 2020). A two-sided p-value under 0.05 was considered statistically significant. Post-hoc power analyses were performed using G*Power version 3.1.9.6.
3 Results
The mean serum 25(OH)D levels were significantly lower in group A (data gathered in January) than in group B (data gathered in July) (56.3 ± 14.5 nmol/L vs 78.3 ± 18.5 nmol/L, p < 0.001). The mean serum 25(OH)D of the whole study population was 68 ± 20 nmol/L. The results of physical performance and anabolic hormones are presented in Table 1.
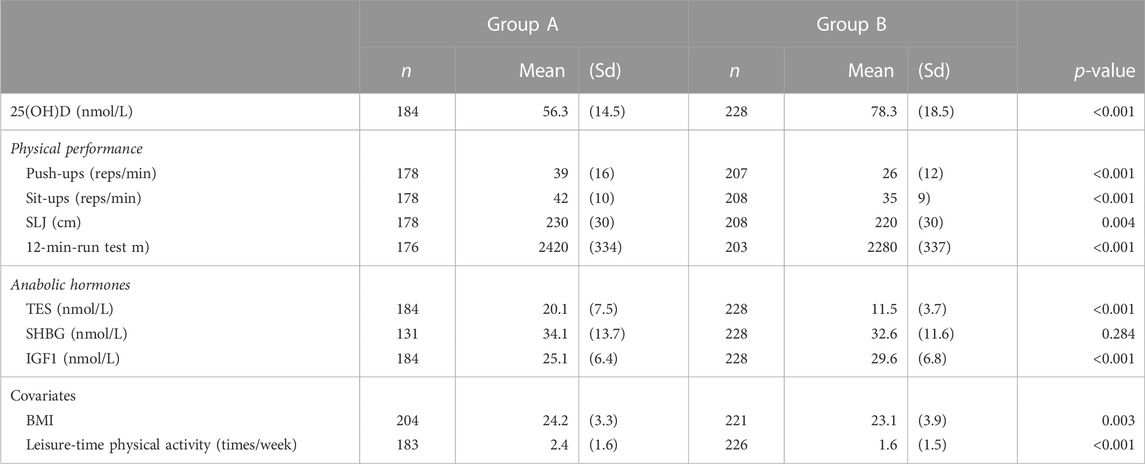
TABLE 1. Physical performance and anabolic hormone status and covariates between group A and B (N = 412). Standing long jump (SLJ), Muscular fitness index (MFI); Testosterone (TES); Sex hormone binding globulin (SHBG); Insulin-like growth factor-1 (IGF-1), Body mass index (BMI). Differences between groups were tested using Independent Samples t-test.
In the whole population, serum 25(OH)D levels correlated statistically significantly with testosterone (r = −0.294) and IGF-1 (r = 0.231); p < 0.001, n = 412 for both. When groups were analyzed separately, there were no statistically significant Pearson correlations (r) between serum 25(OH)D and physical performance or anabolic hormones in winter group A. Instead, in summer group B, positive weak correlations (all p < 0.05) were found between 25(OH)D and push-ups (r = 0.208), sit-ups (r = 0.235), standing long jumps (r = 0.257), 12-min running test (r = 0.288), MFI (r = 0.269), TES (r = 0.157) and SHBG (r = 0.138).
After controlling the whole study population for the group, body composition, and leisure-time physical activity, 25(OH)D level was positively associated with push-up, sit-up, standing long jump, and 12-min running tests, and with MFI (Table 2).
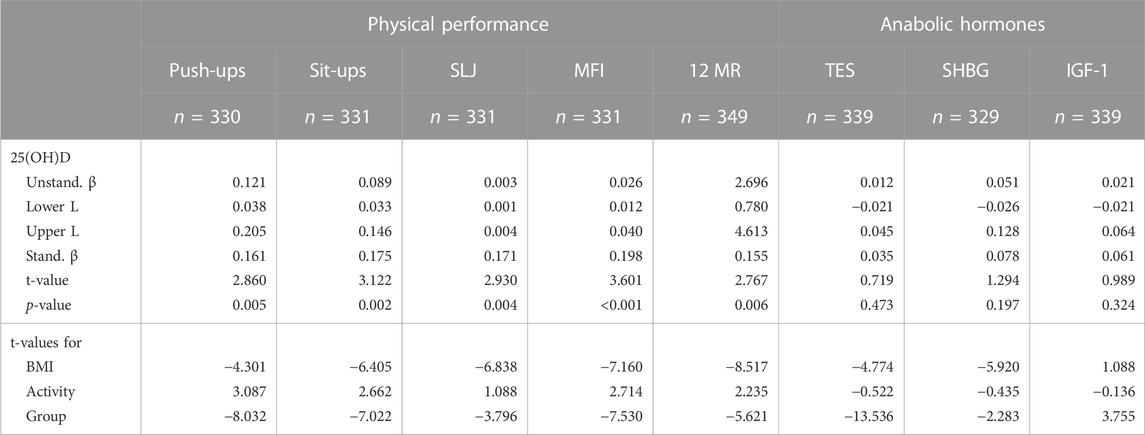
TABLE 2. Associations of serum 25(OH)D physical performance, and anabolic hormones using linear regression analysis adjusting analysis by group, body mass index, and exercise activity. Differences between groups were tested using Linear Regression analysis. Results are shown using unstandardized beta (Unstand. β) with lower (Lower L) and upper limit (Upper L) of 95% confidence interval, standardized beta (Stand. β), and p-values. Push-ups in 1 minute, Sit-ups in 1 min, SLJ = standing long jump, MFI = muscular fitness index (push-up, sit-up, and SLJ combined), 12 MR = 12-min running test, TES = testosterone, SHBG = sex hormone binding globulin, IGF-1 = insulin-like growth factor 1. The limit of a statistically significant (p < 0.05) t-value is t>|1.960| and highly significant (p < 0.001) the limit is t>|3.291|.
Of controlling variables, BMI had a weak negative correlation with serum 25(OH)D (r = −0.140) and physical performance tests (sit-ups: r = −0.234, standing long jumps: r = −0.314, 12-min running test: r = −0.249 and MFI −0.249). Leisure-time physical activity did not correlate with serum 25(OH)D but had weak positive correlations with all physical performance variables and TES (sit-ups: r = 0.259, push-ups: r = 0.282, standing long jumps: r = 0.172, 12-min running test: r = 0.165, MFI: r = 0.276 and TES: r = 0.120).
The differences between participants that had sufficient (≥75 nmol/L) and insufficient (<75 nmol/L) serum 25(OH)D levels were also tested with independent samples t-test (Table 3). As the physical condition differed between groups A and B (p < 0.001), due to differences in military units, the groups were analyzed separately. In group B, the participants with serum 25(OH)D level higher than the sufficient level, had significantly better results in the 12-min run test (p < 0.001), sit-ups (p = 0.048), standing long jumps (p = 0.010), and muscular fitness index (0.031) and higher levels of TES (0.004), while in group A, there were only significant differences in push-ups (p = 0.022), respectively.
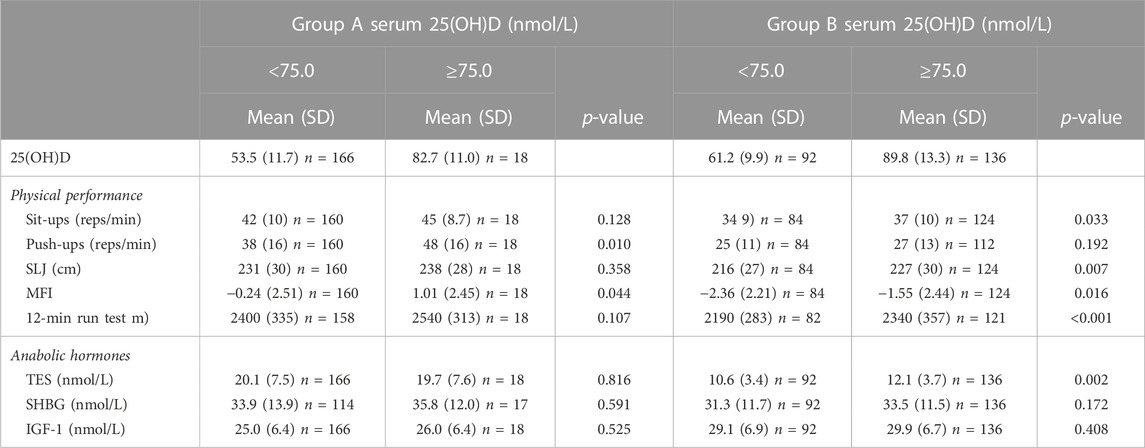
TABLE 3. Differences of the mean (±SD) anabolic hormone levels and physical performance test results between the subgroups divided by sufficient level (75 nmol/L) of serum 25 (OH) D in group A (data gathered in January) and B (data gathered in July). Standing long jump (SLJ); muscular fitness index (MFI); testosterone (TES); sex hormone binding globulin (SHBG); testosterone-sex hormone binding globulin ratio (TES/SHBG); insulin-like globulin factor-1 (IGF-1). Differences between groups were tested using Independent Samples t-test.
Using effect sizes, derived from independent samples t-test, actual post hoc power showed to be at least 80%.
4 Discussion
The main finding of the present study demonstrate that 25(OH)D was positively associated with aerobic and muscular fitness test results after controlling for the group, body composition, and physical activity. In addition, in group B (data gathered in summer), the participants with serum 25(OH)D level higher than the sufficient level (≥75 nmol/L) had significantly better results in aerobic performance, muscular fitness, and higher levels of TES. In group A (data gathered in winter), only push-up test results differed statistically significantly between the subgroups based on sufficient serum 25(OH)D levels, respectively. The groups were analyzed separately due to fundamental differences in their physical condition. The participants in group A were conducting their military service in rapid deployment forces requiring better physical performance than group B, in which the participants were in standard military service. As group A was measured in winter when the vitamin D intake from the sunlight is lower, the association of vitamin D would not have been visible if the groups had been analyzed together.
Due to the compulsory military service in Finland, the participants in the present study represent the normal population of young men. Although most of the studies in this field have been conducted on athletes, the results coincide with the present study, showing positive relationships between serum 25(OH)D levels and muscular power and endurance (Hamilton et al., 2014; Koundourakis et al., 2014; Hildebrand et al., 2016; Heileson et al., 2022). The mechanisms of how vitamin D affects muscular fitness remain hypothetical, although there are several potential pathways. Vitamin D is known to influence both calcium and phosphate metabolism (Charoenngam et al., 2019). Calcium has a fundamental role in muscle contraction (Berchtold et al., 2000) and thus, vitamin D may have indirect beneficial effects on muscle contraction and strength via its effects on systemic calcium levels (Girgis et al., 2013). In the present study, serum 25(OH)D levels were associated with better results in tests requiring efficient muscle actions (push-ups, sit-ups, standing long jump), indicating that it could be enhanced by vitamin D. Also, vitamin D has been suggested to have direct effects on skeletal muscle through vitamin D receptor (VDR), which has been found in human skeletal muscle cells (Pojednic and Ceglia, 2014). VDR-mediated effects have been suggested to have rapid non-genomic and genomic effects on intracellular calcium and phosphate homeostasis, muscle differentiation, contractile protein expression/activity, and phospholipid composition (Girgis et al., 2013). This is supported by abnormal skeletal muscle development and reduced strength in VDR-knockout mice (Endo et al., 2003; Girgis et al., 2015). This could be associated with better progress in training muscular fitness for those with sufficient vitamin D levels. The Global Endocrine Society’s Practice Guidelines Committee’s recommendation for 25(OH)D level for maximum musculoskeletal health is ≥ 75 nmol/L (Holick, 2017). Interestingly, in group B, participants above that level had better outcomes in almost all variables in physical performance and higher TES. In group A, parallel results were found but only push-ups were statistically significant.
The present study also showed a positive relationship between serum 25(OH)D and aerobic performance. Associations between serum 25(OH)D and aerobic performance have previously been shown in several studies (Forney et al., 2014; Carswell et al., 2018; Zeitler et al., 2018). Notably, in line with the present study (Carswell et al., 2018), found in military recruits that serum 25(OH)D levels were associated with aerobic performance, although they reported a non-significant association with muscular strength and power. The association between serum 25(OH)D levels and VO2max could relate to VDRs as well. VDRs have also been found in cardiac muscle cells (Reddy Vanga et al., 2010), indicating that vitamin D may also have beneficial effects on aerobic performance by influencing oxygen transportation and utilization (Dahlquist et al., 2015).
In addition to the direct effects of vitamin D through VDR and the indirect effect on calcium homeostasis, vitamin D may have a beneficial impact on physical performance by increasing the levels of TES in the blood (Wehr et al., 2010; Nimptsch et al., 2012; Anic et al., 2016). VDRs have also been found in areas of the male reproductive tract such as the Leydig cells (Jensen, 2014). Testosterone is known to induce increased muscle growth, i.e., hypertrophy, by multiple mechanisms which include increasing the size and number of muscle fibers, increasing the number of myonuclei, and increasing the number of muscle satellite cells. This leads to increased muscular strength and mass (Kautiainen et al., 2002; Herbst and Bhasin, 2004; Kadi, 2008) Therefore, it can be concluded that higher vitamin D levels may indirectly improve muscular strength and thus physical performance. In the present study, TES was found higher in participants with sufficient (≥75 nmol/L) serum 25(OH)D levels in group B. Most of the circulating TES is bound to albumin and SHBG and higher SHBG levels indicates lower bioavailable TES levels and thus alter the effects of TES in the human body (Goldman et al., 2017). Nevertheless, there were no significant results on the SHBG levels in the present study (only a weak positive correlation in group B, which disappeared after adjusting for covariates). IGF-1, on the other hand, is a hormone that, among numerous other effects, regulates anabolic and catabolic pathways in skeletal muscle (Yoshida and Delafontaine, 2020). Vitamin D has been shown to increase serum IGF-1 levels through the induction of transcription of several genes in the liver (Ameri et al., 2013b) IGF-1 is also associated with better physical performance outcomes in some studies (Cappola et al., 2001; Nindl et al., 2011). A systematic review and meta-analysis showed a significant increase in IGF-1 levels in participants supplemented daily with ≤25ug of vitamin D. In the present study, there was a weak positive correlation between IGF-1 and serum 25(OH)D levels, but the effect disappeared after adjusting for seasonally presentative group effect.
The present study had several strengths. Muscular fitness was measured with three different muscle fitness tests: push-up, sit-up, and standing long jump which gives a comprehensive image of the muscular fitness state of the participants. Importantly, regression models were also controlled with BMI. High fat mass leads to decreased serum 25(OH)D levels (Wortsman et al., 2000) and impairs physical performance (Mattila et al., 2007) and hence is a major confounding factor. Another strength of the present study is the assessment of anabolic hormones TES and IGF-1. In addition, it is important to explore the seasonal variation of serum25(OH)D levels, especially, in high-latitude countries such as Finland, where adequate sunlight exposure exists only in a short period of summer months (Engelsen et al., 2005). Still, the study has some limitations. In group A, there were only 18 participants who reached over the sufficient serum 25(OH)D level of 75 nmol/L which may explain the lack of statistically significant differences between the sufficient and insufficient participants. The participants in group B had higher serum 25(OH)D levels and thus more statistical power in the sufficient group. The greatest limitation of the present study is that it is a cross-sectional study and therefore causal conclusion cannot be made. It is possible that the associations between serum 25(OH)D levels and physical performance could be partly explained by reverse causation: the more physically active participants may spend more time outdoors exposed to sunlight, hence have a better physical condition as well as higher serum 25(OH)D levels.
In conclusion, the hypotheses were supported, and the present study shows that serum 25(OH)D level could be positively associated with aerobic and muscular fitness. It is also possible that vitamin D is associated with physical performance only at a sufficient level of serum 25(OH)D, and the effects may be mediated or moderated through increasing the serum levels of testosterone. Further randomized control trial (RCT) research is needed in which the serum level of 25(OH)D must reach the sufficient limit for the supplementation group. This could be conducted in Finland during wintertime as we noticed that only a minor share of young Finnish men reaches the recommended 25(OH)D threshold in winter.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Pirkanmaa Hospital District, ETL code R17155, HUS/1557/2018 and the Finnish Defence Forces (AN21508, AP10027, AQ24718, AR13336). The patients/participants provided their written informed consent to participate in this study.
Author contributions
AL and TL contributed to the creation and analysis of the data. AL, IL, JV, HP, and HK contributed to the conception and design of the study. AL wrote the first draft of the manuscript. All contributed to the editing of the manuscript.
Funding
This study was funded by the Centre for Military Medicine Finnish Defence Forces, State Research Funding (PSHP), and National Defense Support Foundation (MPKS).
Acknowledgments
The authors would like to thank Ms. Liisa Rantahalvari for her assistance during the data collection. The authors would like to thank MD, PhD Juha-Petri Ruohola and MD Jussi Laaksonen for their contribution to launching this study and Professor Onni Niemelä, Ms. Susanna Luoma, and Ms. Tanja Toivanen for conducting laboratory analysis. The authors would also like to thank Macey Higdon for the revision of the language.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
ACSM (2000). ACSM’s Guidelines for exercise testing and prescription. Philadelphia, Pennsylvania, United States: Lippincott Williams & Wilkins.
Ameri P., Giusti A., Boschetti M., Bovio M., Teti C., Leoncini G., et al. (2013a). Vitamin D increases circulating IGF1 in adults: Potential implication for the treatment of GH deficiency. Eur. J. Endocrinol. 169, 767–772. doi:10.1530/EJE-13-0510
Ameri P., Giusti A., Boschetti M., Murialdo G., Minuto F., Ferone D. (2013b). Interactions between vitamin D and IGF-I: From physiology to clinical practice. Clin. Endocrinol. (Oxf) 79, 457–463. doi:10.1111/cen.12268
Anic G. M., Albanes D., Rohrmann S., Kanarek N., Nelson W. G., Bradwin G., et al. (2016). Association between serum 25-hydroxyvitamin D and serum sex steroid hormones among men in NHANES. Clin. Endocrinol. (Oxf) 85, 258–266. doi:10.1111/cen.13062
Berchtold M. W., Brinkmeier H., Müntener M. (2000). Calcium ion in skeletal muscle: Its crucial role for muscle function, plasticity, and disease. Physiol. Rev. 80, 1215–1265. doi:10.1152/physrev.2000.80.3.1215
Bogazzi F., Rossi G., Lombardi M., Tomisti L., Sardella C., Manetti L., et al. (2011). Vitamin D status may contribute to serum insulin-like growth factor I concentrations in healthy subjects. J. Endocrinol. Invest. 34, e200–e203. doi:10.3275/7228
Cappola A. R., Bandeen-Roche K., Wand G. S., Volpato S., Fried L. P. (2001). Association of IGF-I levels with muscle strength and mobility in older women. J. Clin. Endocrinol. Metab. 86, 4139–4146. doi:10.1210/jcem.86.9.7868
Carswell A. T., Oliver S. J., Wentz L. M., Kashi D. S., Roberts R., Tang J. C. Y., et al. (2018). Influence of Vitamin D supplementation by sunlight or oral D3 on exercise performance. Med. Sci. Sports Exerc 50, 2555–2564. doi:10.1249/MSS.0000000000001721
Charoenngam N., Shirvani A., Holick M. F. (2019). Vitamin D for skeletal and non-skeletal health: What we should know. J. Clin. Orthop. Trauma 10, 1082–1093. doi:10.1016/j.jcot.2019.07.004
Cooper K. H. (1968). A means of assessing maximal oxygen intake: Correlation between field and treadmill testing. JAMA 203, 201–204. doi:10.1001/jama.1968.03140030033008
Dahlquist D. T., Dieter B. P., Koehle M. S. (2015). Plausible ergogenic effects of vitamin D on athletic performance and recovery. J. Int. Soc. Sports Nutr. 12, 33. doi:10.1186/s12970-015-0093-8
D’Andrea S., Martorella A., Coccia F., Castellini C., Minaldi E., Totaro M., et al. (2021). Relationship of vitamin D status with testosterone levels: A systematic review and meta-analysis. Endocrine 72, 49–61. doi:10.1007/s12020-020-02482-3
Endo I., Inoue D., Mitsui T., Umaki Y., Akaike M., Yoshizawa T., et al. (2003). Deletion of vitamin D receptor gene in mice results in abnormal skeletal muscle development with deregulated expression of myoregulatory transcription factors. Endocrinology 144, 5138–5144. doi:10.1210/en.2003-0502
Engelsen O., Brustad M., Aksnes L., Lund E. (2005). Daily duration of vitamin D synthesis in human skin with relation to latitude, total ozone, altitude, ground cover, aerosols and cloud thickness. Photochem Photobiol. 81, 1287–1290. doi:10.1562/2004-11-19-rn-375
Forney L. A., Earnest C. P., Henagan T. M., Johnson L. E., Castleberry T. J., Stewart L. K. (2014). Vitamin D status, body composition, and fitness measures in college-aged students. J. Strength Cond. Res. 28, 814–824. doi:10.1519/JSC.0b013e3182a35ed0
Forouhi N. G., Luan J., Cooper A., Boucher B. J., Wareham N. J. (2008). Baseline serum 25-hydroxy vitamin D is predictive of future glycemic status and insulin resistance: The medical research Council ely prospective study 1990–2000. Diabetes 57, 2619–2625. doi:10.2337/db08-0593
Girgis C. M., Cha K. M., Houweling P. J., Rao R., Mokbel N., Lin M., et al. (2015). Vitamin D receptor ablation and vitamin D deficiency result in reduced grip strength, altered muscle fibers, and increased myostatin in mice. Calcif. Tissue Int. 97, 602–610. doi:10.1007/s00223-015-0054-x
Girgis C. M., Clifton-Bligh R. J., Hamrick M. W., Holick M. F., Gunton J. E. (2013). The roles of vitamin D in skeletal muscle: Form, function, and metabolism. Endocr. Rev. 34, 33–83. doi:10.1210/er.2012-1012
Goldman A. L., Bhasin S., Wu F. C. W., Krishna M., Matsumoto A. M., Jasuja R. (2017). A reappraisal of testosterone’s binding in circulation: Physiological and clinical implications. Endocr. Rev. 38, 302–324. doi:10.1210/er.2017-00025
Hamilton B., Whiteley R., Farooq A., Chalabi H. (2014). Vitamin D concentration in 342 professional football players and association with lower limb isokinetic function. J. Sci. Med. Sport 17, 139–143. doi:10.1016/j.jsams.2013.03.006
Haussler M. R., Whitfield G. K., Haussler C. A., Hsieh J.-C., Thompson P. D., Selznick S. H., et al. (1998). The nuclear vitamin D receptor: Biological and molecular regulatory properties revealed. J. Bone Mineral Res. 13, 325–349. doi:10.1359/jbmr.1998.13.3.325
Heileson J. L., McGowen J. M., Moris J. M., Chapman-Lopez T. J., Torres R., Funderburk L. L. K., et al. (2022). Body composition, eicosapentaenoic acid, and vitamin D are associated with army combat fitness test performance. J. Int. Soc. Sports Nutr. 19, 349–365. doi:10.1080/15502783.2022.2094717
Helmerhorst H. J., Brage S., Warren J., Besson H., Ekelund U. (2012). A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Activity 9, 103. doi:10.1186/1479-5868-9-103
Herbst K. L., Bhasin S. (2004). Testosterone action on skeletal muscle. Curr. Opin. Clin. Nutr. Metab. Care 7, 271–277. doi:10.1097/00075197-200405000-00006
Hildebrand R. A., Miller B., Warren A., Hildebrand D., Smith B. J. (2016). Compromised vitamin D status negatively affects muscular strength and power of collegiate athletes. Int. J. Sport Nutr. Exerc Metab. 26, 558–564. doi:10.1123/ijsnem.2016-0052
Holick M. F. (2017). The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 18, 153–165. doi:10.1007/s11154-017-9424-1
Jensen M. B. (2014). Vitamin D and male reproduction. Nat. Rev. Endocrinol. 10, 175–186. doi:10.1038/nrendo.2013.262
Kadi F. (2008). Cellular and molecular mechanisms responsible for the action of testosterone on human skeletal muscle. A basis for illegal performance enhancement. Br. J. Pharmacol. 154, 522–528. doi:10.1038/bjp.2008.118
Kautiainen S., Rimpelä A., Vikat A., Virtanen S. M., Rimpela A. (2002). Secular trends in overweight and obesity among Finnish adolescents in 1977–1999. Int. J. Obes. 26, 544–552. doi:10.1038/sj.ijo.0801928
Koundourakis N. E., Androulakis N. E., Malliaraki N., Margioris A. N. (2014). Vitamin D and exercise performance in professional soccer players. PLoS One 9, e101659. doi:10.1371/journal.pone.0101659
Ksiażek A., Zagrodna A., Słowińska-Lisowska M. (2019). Vitamin D, skeletal muscle function and athletic performance in athletes—a narrative review. Nutrients 11, 1800. doi:10.3390/nu11081800
Markovic G., Dizdar D., Jukic I., Cardinale M. (2004). Reliability and factorial validity of squat and countermovement jump tests. Available at: https://journals.lww.com/nsca-jscr.
Mattila V. M., Tallroth K., Marttinen M., Pihlajamäki H. (2007). Physical fitness and performance. Body composition by DEXA and its association with physical fitness in 140 conscripts. Med. Sci. Sports Exerc 39, 2242–2247. doi:10.1249/mss.0b013e318155a813
Mayorga-Vega D., Bocanegra-Parrilla R., Ornelas M., Viciana J. (2016). Criterion-related validity of the distance- and time-based walk/run field tests for estimating cardiorespiratory fitness: A systematic review and meta-analysis. PLoS One 11, e0151671. doi:10.1371/journal.pone.0151671
Nimptsch K., Platz E. A., Willett W. C., Giovannucci E. (2012). Association between plasma 25-OH vitamin D and testosterone levels in men. Clin. Endocrinol. (Oxf) 77, 106–112. doi:10.1111/j.1365-2265.2012.04332.x
Nindl B. C., Santtila M., Vaara J., Hakkinen K., Kyrolainen H. (2011). Circulating IGF-I is associated with fitness and health outcomes in a population of 846 young healthy men. Growth Hormone IGF Res. 21, 124–128. doi:10.1016/j.ghir.2011.03.001
Nordic Council of Ministers (2014). Nordic nutrition recommendations 2012: Integrating nutrition and physical activity responsible organisation. Berlin, Germany: Springer. doi:10.6027/Nord2014-002
Penry J. T., Wilcox A. R., Yun J. (2011). Validity and reliability analysis of cooper’s 12-minute run and the multistage shuttle run in healthy adults. J. Strength & Cond. Res. 25, 597–605. doi:10.1519/JSC.0b013e3181cc2423
Pojednic R. M., Ceglia L. (2014). The emerging biomolecular role of vitamin D in skeletal muscle. Exerc Sport Sci. Rev. 42, 76–81. doi:10.1249/JES.0000000000000013
Reddy Vanga S., Good M., Howard P. A., Vacek J. L. (2010). Role of vitamin D in cardiovascular health. Am. J. Cardiol. 106, 798–805. doi:10.1016/j.amjcard.2010.04.042
Ryman Augustsson S., Bersås E., Magnusson Thomas E., Sahlberg M., Augustsson J., Svantesson U. (2009). Gender differences and reliability of selected physical performance tests in young women and men. Adv. Physiother. 11, 64–70. doi:10.1080/14038190801999679
Utiger R. D. (1998). The need for more vitamin D. N. Engl. J. Med. 338, 828–829. doi:10.1056/NEJM199803193381209
Vaara J. P., Vasankari T., Fogelholm M., Häkkinen K., Santtila M., Kyröläinen H. (2014). Maximal strength, muscular endurance and inflammatory biomarkers in young adult men. Int. J. Sports Med. 35, 1229–1234. doi:10.1055/s-0034-1375615
Viljanen T., Viitasalo J. T., Kujala U. M. (1991). Strength characteristics of a healthy urban adult population. Eur. J. Appl. Physiol. Occup. Physiol. 63, 43–47. doi:10.1007/BF00760799
Wehr E., Pilz S., Boehm B. O., März W., Obermayer-Pietsch B. (2010). Association of vitamin D status with serum androgen levels in men. Clin. Endocrinol. (Oxf) 73, 243–248. doi:10.1111/j.1365-2265.2009.03777.x
Wortsman J., Matsuoka L. Y., Chen T. C., Lu Z., Holick M. F. (2000). Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 72, 690–693. doi:10.1093/ajcn/72.3.690
Yoshida T., Delafontaine P. (2020). Mechanisms of IGF-1-mediated regulation of skeletal muscle hypertrophy and atrophy. Cells 9, 1970. doi:10.3390/cells9091970
Keywords: vitamin D, young men, anabolic hormones, physical performance, military
Citation: Laaksi A, Laaksi I, Pihlajamäki H, Vaara JP, Luukkaala T and Kyröläinen H (2023) Associations of serum 25(OH)D levels with physical performance and anabolic hormones in young men. Front. Physiol. 14:1049503. doi: 10.3389/fphys.2023.1049503
Received: 20 September 2022; Accepted: 27 January 2023;
Published: 07 February 2023.
Edited by:
Jan Jacek Kaczor, University of Gdansk, PolandReviewed by:
Michal Zmijewski, Medical University of Gdansk, PolandLisa M. Hernández, Leidos, United States
Copyright © 2023 Laaksi, Laaksi, Pihlajamäki, Vaara, Luukkaala and Kyröläinen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Akseli Laaksi, aktlaa@utu.fi