 Stefan Stewart1
Stefan Stewart1 Jose Manuel Dodero-Anillo2Javier Guijarro-Eguinoa1Pedro Arias3Arturo Gómez López De Las Huertas1Enrique Seco-Meseguer1
Jose Manuel Dodero-Anillo2Javier Guijarro-Eguinoa1Pedro Arias3Arturo Gómez López De Las Huertas1Enrique Seco-Meseguer1 Irene García-García1
Irene García-García1 Elena Ramírez García1,4Carlos Rodríguez-Antolín5
Elena Ramírez García1,4Carlos Rodríguez-Antolín5 Antonio J. Carcas1,4Sonia Rodriguez-Novoa6Rocio Rosas-Alonso3,5*
Antonio J. Carcas1,4Sonia Rodriguez-Novoa6Rocio Rosas-Alonso3,5* Alberto M. Borobia1,4*
Alberto M. Borobia1,4*- 1Clinical Pharmacology Department, IdiPAZ, La Paz University Hospital, Madrid, Spain
- 2Clinical Pharmacology, Hospital Universitario Puerto Real, Cadiz, Spain
- 3Pharmacogenetics Laboratory, Genetics Department, La Paz University Hospital, Madrid, Spain
- 4Pharmacology Department, School of Medicine, Universidad Autónoma de Madrid, Madrid, Spain
- 5Experimental Therapies and Novel Biomarkers in Cancer, Hospital La Paz Institute for Health Research—IdiPAZ, Madrid, Spain
- 6Genetics of Metabolic Diseases Laboratory, Genetics Department, La Paz University Hospital, Madrid, Spain
The field of pharmacogenetics (PGx) holds great promise in advancing personalized medicine by adapting treatments based on individual genetic profiles. Despite its benefits, there are still economic, ethical and institutional barriers that hinder its implementation in our healthcare environment. A retrospective analysis approach of anonymized data sourced from electronic health records was performed, encompassing a diverse patient population and evaluating key parameters such as prescribing patterns and test results, to assess the impact of pharmacogenetic testing. A head-to-head comparison with previously published activity results within the same pharmacogenetic laboratory was also conducted to contrast the progress made after 10 years. The analysis revealed significant utilization of pharmacogenetic testing in daily clinical practice, with 1,145 pharmacogenetic tests performed over a 1-year period and showing a 35% growth rate increase over time. Of the 17 different medical departments that sought PGx tests, the Oncology department accounted for the highest number, representing 58.47% of all genotyped patients. A total of 1,000 PGx tests were requested for individuals susceptible to receive a dose modification based on genotype, and 76 individuals received a genotype-guided dose adjustment. This study presents a comprehensive descriptive analysis of real-world data obtained from a public tertiary hospital laboratory specialized in pharmacogenetic testing, and presents data that strongly endorse the integration of pharmacogenetic testing into everyday clinical practice.
1 Introduction
Within the rapidly advancing field of personalized medicine, pharmacogenetics has come to prominence as a growing discipline that examines how genetic variations influence an individual’s response to drugs. Variants in genes that encode drug-metabolizing enzymes, drug transporters, and drug targets can significantly impact the disposition and action of drugs, which ultimately leads to variability in response (Bielinski et al., 2014). This is particularly relevant in medications where there is a marginal difference between a therapeutic and a toxic dose (i.e., a narrow therapeutic window) (Tong et al., 2021). As a result, pharmacogenetic (PGx) testing performed either preemptively or ad hoc has become increasingly important as a means of individualizing treatment plans, enhancing treatment efficacy, and mitigating the occurrence of adverse events (García-García and Borobia, 2021).
Our understanding of the impact of genetic variations on drug response is continuously expanding, as advances in genotyping and sequencing technologies allow for further insight into the complex interactions between genetics, drugs, and individual patients (Bielinski et al., 2014). Numerous studies, including randomized controlled trials, have demonstrated the efficacy of personalized drug therapy based on PGx testing for specific drug-gene combinations (Tong et al., 2016). The Preemptive Pharmacogenomic Testing for Preventing Adverse Drug Reactions (PREPARE) study, conducted by the Ubiquitous Pharmacogenomics Consortium, and the more recent 12-gene PGx panel implementation study stand as particularly notable (Swen et al., 2023).
Despite encountering slow initial uptake and wavering levels of acceptance among physicians, the integration of PGx information into clinical practice has gained momentum due to mounting evidence (Borobia et al., 2018). The development of precise, easily accessible, and cost-effective molecular analysis techniques has also contributed to its increasing adoption. Consequently, regulatory bodies such as the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have recognized the significance of PGx information and incorporated it into the drug label information making it readily available to both prescribers and patients (Borobia et al., 2018; Brunette et al., 2020; García et al., 2020; Díaz-Villamarín et al., 2022). In this context, clinical guidelines have been developed to aid prescribing clinicians, such as the ones by The Dutch Pharmacogenetics Working Group (DPWG) and the Clinical Pharmacogenetics Implementation Consortium (CPIC), which comprehensively evaluate the associations between over 100 gene-drug pairs (D’Andrea et al., 2015; Leusink et al., 2016; Díaz-Villamarín et al., 2022). More recently, the Spanish Society of Pharmacogenetics and Pharmacogenomics (SEFF) has developed its own clinical practice guidelines grounded in the national portfolio of services and the idiosyncrasies inherent to the Spanish National Health System (SNHS) (Sociedad Española de Farmacogenética y Farmacogenómica, 2023). These milestones coupled with the rise of precision medicine, have eventually led to the incorporation of pharmacogenetic biomarker testing into the services portfolio of many Health Services worldwide, including the SNHS (Borobia et al., 2018; García et al., 2020).
However, despite its potential benefits, there are still economic, ethical and institutional barriers that hinder its implementation beyond a limited number of tertiary hospitals in our healthcare environment (Borobia et al., 2018). One of the primary challenges faced is the lack of standardization within the field, which can lead to disparities in the interpretation of results, potentially precluding patients from receiving the benefits of personalized treatment plans or expose them to avoidable side effects (Weitzel et al., 2014).
In order to fully realize the potential of pharmacogenetics, clinical pharmacogenetic laboratories have a vital role to play in overcoming, not only the aforementioned challenges, but the current shortages of trained technical staff and insufficient expertise amongst healthcare personnel. This would not only improve patient outcomes by enhancing safety and effectiveness of medication use, but ultimately contribute to a more sustainable healthcare system (Borobia et al., 2018; Karamperis et al., 2021).
To assess the practical impact of pharmacogenetics in a real-world setting, we conducted a thorough descriptive analysis of annual data from the Clinical Pharmacogenetics Unit located within the La Paz University Hospital (LPUH), a tertiary public hospital equipped with over 1,300 beds that attends the population of northern Madrid. The LPUH Clinical Pharmacogenetics Unit was established in 2013 and its clinical protocols were developed by clinical pharmacologists and geneticists in collaboration with the clinical services that regularly request genetic tests (Borobia et al., 2018). Most of these protocols have well-defined guidelines for pharmacogenetic treatment recommendations. To further aid the petitioner in the optimization of dosing requirements or treatment selection (in the context of this study, we use the terms “petitioner” to refer to the individual ordering a pharmacogenetic test and “petitions” to denote the test orders), clinical and genetic information are assessed and integrated by a clinical pharmacologist who then emits individualised recommendations.
The primary objective of this study is to highlight the activity, challenges, and advancements achieved by our Clinical Pharmacogenetic Unit over a 1-year period. In addition, our study aimed to conduct a head-to-head comparison of real-world data from previously published activity results within the same tertiary Pharmacogenetic Unit, spanning two different time periods: period 1 (January 2014 and December 2016) and period 2 (August 2021 and September 2022). Ultimately, this study aims to contribute to the expanding evidence base that supports the integration of PGx testing into routine clinical practice.
2 Materials and methods
2.1 Study design
We conducted a retrospective, single-center study to assess the impact of PGx testing during routine clinical practice at the LPUH Clinical Pharmacogenetics Unit. Established in 2013, it operates as a multidisciplinary entity, integrating the Clinical Pharmacology Department and the Genetics Department, both of which hold ISO 9001:2015 certification. Both departments play an essential role within the Unit; the geneticist is responsible of the technical, analytical and genetic data interpretation, whereas the clinical pharmacologist provides expertise on possible drug interactions, integrates patient’s clinical status with the obtained phenotype, and emits individualized treatment plans to be prescribed by the petitioner. It has implemented treatment adjustment protocols for the following preemptively genotyped drug-gene pairs: thiopurines/TPMT-NUDT15, tacrolimus/CYP3A5, voriconazole/CYP2C19, siponimod/CYP2C9, irinotecan/UGT1A1 abacavir/HLA-B57:01 and fluoropyrimidines/DPYD. MTHFR genotype is also analyzed following an institutional internal protocol, but no dose recommendation is done due to the lack of genotype-based clinical guidelines available. RYR1 and CACNA1S genes are only analyzed in patients who have presented an event clinically compatible with malignant hyperthermia.
The majority of requests received can be classified into two groups: when a request is made for drugs for which the PGx testing is required before treatment prescription (preemptive genotyping in high-risk populations), petitions and samples are directly forwarded to the genetics department for sample processing and analysis. The final report with genetic data provided by the geneticist includes dose-adjustment recommendations provided by the clinical pharmacologist who takes into account the patient’s clinical background, individual interactions, and other factors is sent to the requesting service. When a medical case is referred where a PGx test could be deemed appropriate or a request is made for a drug without established clinical protocols, the Clinical Pharmacogenetics Unit’s clinical pharmacologist assesses and decides, by integrating available clinical information with up-to-date pharmacogenetic evidence, whether a PGx test is indicated. If the PGx test is recommended, the analysis is performed and a PGx report is generated. All PGx reports are performed according to the recommendations of the European Molecular Genetics Quality Network (EMQN) (European Molecular Genetics Quality Network, 2023). An example of our reports is shown in Supplementary Figure S1.
This study included patients with various pathologies with a PGx test performed in a local pharmacogenetic laboratory between August 2021 and September 2022. Demographic characteristics including age and gender as well as relevant future or current prescription, PGx data and diseases, were obtained from medical records and the laboratory information system over a 1-year period.
A descriptive analysis of the study population was carried out which included the number of tests performed, what gene was requested, genotyping results and its proportion attending the total amount of requests of each type. Variables were described using the number of participants (n), mean and it is minimum and maximum range. We then compared the results obtained during from 2014 to 2016 with those obtained from 2021 to 2022.
2.2 Pharmacogenetic testing methodology
Blood samples were obtained in Vacutainer EDTA tube (Becton Dickinson, Franklin Lakes, NJ, USA). DNA was isolated using a Chemagen extraction robot (Perkin-Elmer, Boston, MA, USA). Within our Hospital’s service portfolio, the technology used for each type of test was as follows: OpenArray® technology (for the Pharmacogenetics of Fluoropyrimidines, Pharmacogenetics of Voriconazole, Pharmacogenetics of Thiopurines, Pharmacogenetics of Tacrolimus, Pharmacogenetics of Methotrexate, Pharmacogenetics of Siponimod); PCR combined with electrophoresis (for the Pharmacogenetics of Irinotecan); Real-time PCR (Hypersensitivity to Abacavir); Next-Generation Sequencing (Malignant Hyperthermia).
As previously described, most of the tests are carried out using the TaqMan™ OpenArray™ PGx Express Panel in the QuantStudio™ 12K Flex OpenArray® System (Thermo Fisher Scientific, Waltham, MA, USA) following manufacturer instructions. This panel simultaneously analyses 120 single nucleotide variants (SNVs) in 8 genes using TaqMan™ probes. Each TaqMan™ SNV assay contains two allele-specific probes and a primer pair to detect the specific SNV target. The validation study conducted for this technology was previously published (Rosas-Alonso et al., 2021). For each PGx test available in our lab, predefined SNVs were analyzed (Supplementary Table S1). It is important to note that the OpenArray™ PGx Express Panel used in our laboratory is a predefined non-customizable assay and, of the total 120 SNVs included, our pharmacogenetics unit only analyzes routinely 27 SNVs from this panel. The rationale behind this selection is rooted in our commitment to evidence based medicine and adherence to international pharmacogenetic guidelines from groups such as the Association for Molecular Pathology (AMP), CPIC, DPWG and the SEFF. These 27 SNVs were carefully chosen based on the extensive literature and guidance provided by these authoritative sources.
The PCR reaction was conducted under the following conditions: an initial step of 10 min at 93°C, followed by 45 s at 95°C, 13 s at 94°C, and 2 min at 53.5°C for 50 cycles. Data acquisition and analysis were carried out utilizing the Thermo Fisher Cloud. Genotypes were determined through the utilization of a customized script and alleles were inferred according to drug-specific guidelines (Chandran et al., 2010; Tuková et al., 2010; Birdwell et al., 2015; Moriyama et al., 2017; Jin et al., 2018; Gonsalves et al., 2019; García et al., 2020).
Genotyping test for irinotecan pharmacogenetics study analyses by specific fluorophore-labeled PCR the most common genetic variant affecting UGT1A1 gene, a TAn dinucleotide repeat variant (rs3064744) located in a TATAA consensus element in the UGT1A1 promoter, The forward primer sequence was GATTTGAGTATGAAATTCCAGCCAG, and the reverse primer sequence was CCAGTGGCTGCCATCCACT, which was fluorescently labeled with FAM. The PCR conditions consisted of an initial denaturation at 94°C for 3 min, followed by 31 cycles of denaturation at 94°C for 1 min, annealing at 60°C for 1 min, extension at 72°C for 7 min, and a final extension at 72°C for 7 min. Subsequently, fluorescent fragment sizing was performed using capillary gel electrophoresis. The analysis was carried out with GeneMapper® Software v4.0. The star allele was determined based on the length of the amplicon.
The abacavir hypersensitivity study was conducted using genotyping test of HLA-B to establish presence or absence of *57:01 allele, associated hypersensitivity reactions to abacavir. The study was performed using the commercial GENVINSET® HLA B57 kit (BDR, Zaragoza, Spain), which allows the detection of the HLA-B*57:01 allele using specific primers. The study was performed on the Cobas z 480 analyzer (Roche Diagnostics, Risch-Rotkreuz, Switzerland).
The malignant hyperthymia testing was performed by analyzing the coding regions of the RYR1 and CACNA1S genes by a massive sequencing panel (NGS) of our own design using the KAPA HyperChoice technology (Roche Diagnostics, Risch-Rotkreuz, Switzerland). Sequencing was performed on the Novaseq6000 or HiSeq4000 platform (Illumina, San Diego, CA, USA). Bioinformatics analysis was carried out by the Bioinformatics Unit of the genetics department. Variant classification was performed based on the recommendations of the American College of Medical Genetics and Genomics (Richards et al., 2015) and variants were named according to the HGVS nomenclature (https://varnomen.hgvs.org/). The project accession PRJEB66347 in European Nucleotide Archive (ENA) has the high throughput sequencing data from cases of this study.
This study was conducted under the approval of the ethics committee of the La Paz University Hospital (PI-2915) and in conformance with the principles of the Declaration of Helsinki.
3 Results
3.1 Study population
Since its establishment within LPUH in 2013, the Clinical Pharmacogenetics Unit has conducted genotyping for an approximate total of 5,000 patients. The overall hierarchical functioning of the Unit varies based on the type of request received and is summarized in Figures 1A, B. Activity has been uninterrupted save for a 4-month hiatus caused by the COVID-19 pandemic, when LPUH had to reallocate most of its financial and human resources to help mitigate the overwhelming demand in healthcare. The PGx tests requested and performed at our hospital between August 2021 and September 2022 numbered 1,145, involving 655 patients’ participants. A total of 655 patients were genotyped, total average age was 55.58 years (ranging from 0 to 94 years) with 43.7% (286 out of 655) being aged 65 or older. More than half of the sample subjects were male (55.8%). The LPUH is a public healthcare facility that caters to the inhabitants of the northern region of Madrid, where the demographic makeup is primarily Caucasian. Our Pharmacogenetics Unit receives referrals for various medical conditions, including cancer patients eligible for fluoropyrimidines and irinotecan treatments, transplant candidates undergoing tacrolimus therapy, oncology patients suitable for voriconazole treatment or those diagnosed with aspergillosis, individuals with immune-mediated dermatological, rheumatological, or digestive diseases who are potential tacrolimus candidates, patients considered for methotrexate therapy, and those with a prior adverse response to anesthetic agents or a family history of malignant hyperthermia.
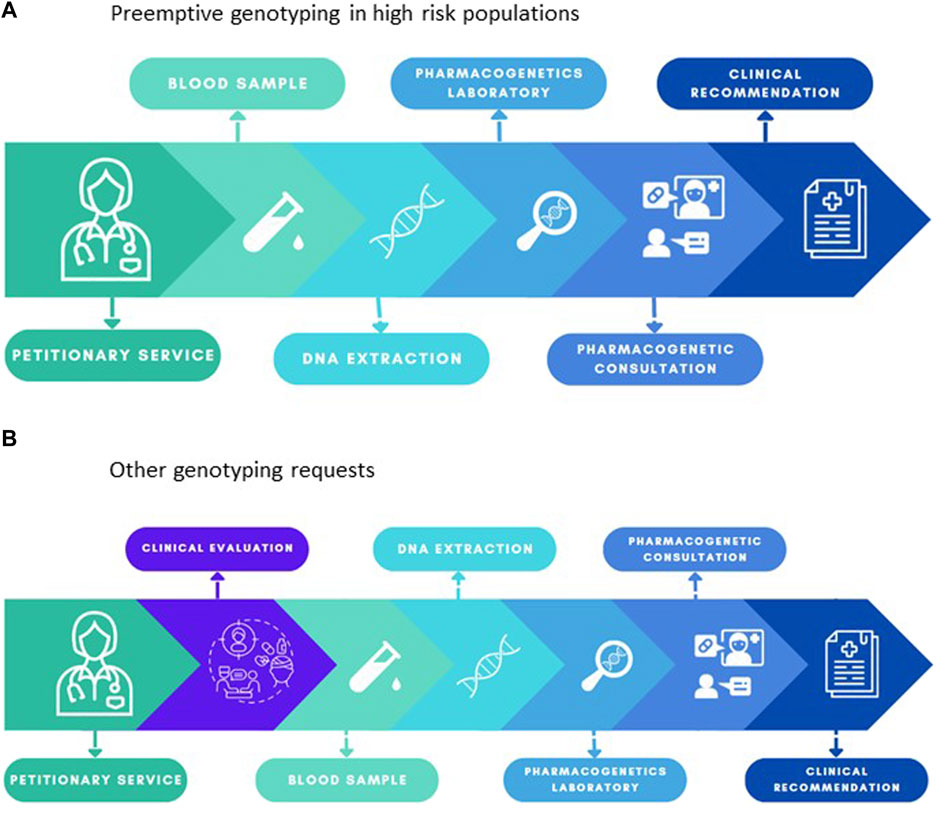
FIGURE 1. (A) Overall functioning of the Clinical Pharmacogenetics Unit for drugs for which the PGx testing is required before treatment prescription (preemptive genotyping in high-risk populations). (B) Overall functioning of the Clinical Pharmacogenetics Unit when a medical case is referred where a PGx test could be deemed appropriate or a request is made for a drug without established clinical protocols.
3.2 Pharmacogenetic genotyping results
By comparison, the total number of PGx tests carried out between January 2014 and December 2016 (Borobia et al., 2018) by this same pharmacogenetic laboratory stood at 2,539 (approximately 846 tests per year). This indicates an average increase rate of 35% in testing activity over the course of approximately 6 years.
Previously reported data revealed that the Internal Medicine/Infectious Disease department accounted for 76.3% (1939 out of 2,539) of the requested actionable genetic marker tests. However, in the current study, among the 17 different medical departments that sought PGx tests, the Oncology department accounted for the highest number, representing 58.47% (383 out of 655) of all genotyped patient (Figure 2A).
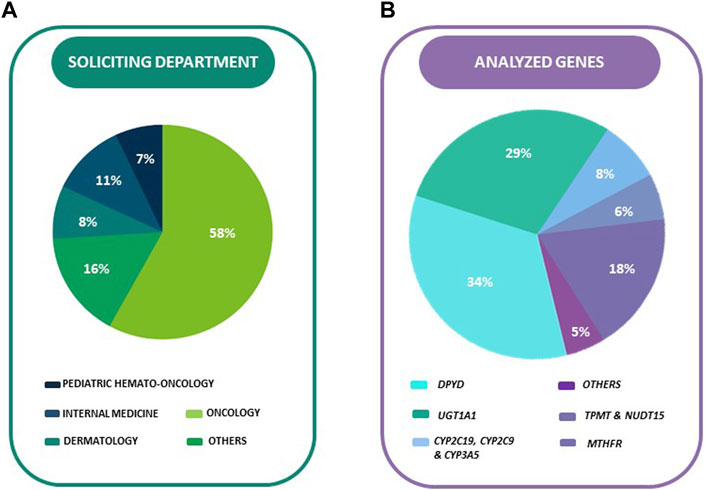
FIGURE 2. (A) Percentage (%) of analyzed genes in total sample. (B) Percentage (%) of analyzed genes in total sample.
The department performing DPYD (95.36%, 370/388) and UGT1A1 (92.55%, 311/336) genetic testing was limited almost exclusively to Oncology. Dermatology was the main department that requested PGx combined tests for TPMT-NUDT15 (accounting for 29.41% of the requests, or 30 out of 102). Both Dermatology and Paediatric Haemato-Oncology had an equal number of requests for PGx tests for MTHFR (26.15% of the requests each, or 17 out of 65). Paediatric Haemato-Oncology had the highest percentage of requests for PGx tests for voriconazole (88.23% of their total requests, or 30 out of 34). Paediatric Nephrology was the main department ordering CYP3A5 genotyping (46.15%, 18/39), while CYP2C9 genotyping was exclusively ordered by the Neurology department (100%, 15/15). The HIV Clinic of Internal Medicine was the sole department ordering HLA B57:01 genotyping.
Over a third of the 1,145 PGx tests (33.89%, 388/1,145 were performed for the genotyping of DPYD (Figure 2B), with the second most requested test being the genotyping of UGT1A1 (29.34%, 336/1,145). The PGx tests performed for thiopurine S-methyltransferase (TPMT) and NUDT15 gene accounted for 17.82% of the total (204/1,145), followed by MTHFR at 5.68% (65/1,145), abacavir HLA B57:01 testing at 4.63% (53/1,145), CYP3A5 at 3.41% (39/1,145), and Voriconazole PGx (CYP2C19) at 3.32% (38/1,145). The least requested tests were the ones involving CYP2C9 at 1.22% (14/1,145) and malignant hyperthermia risk assessment, which accounted for only 0.70% of the total (4/1,145).
The mean response time (MRT) was determined as the number of elapsed days between the date of test request and the date of result report upload and exhibited a range of 1–176 days. The overall MRT for all tests was calculated to be 8.36 days, with a corresponding MRT for all PGx tests included in the OpenArray® platform of 7.01 days. The MRT for HLA B57:01 testing was found to be 15.75 days. The RYR1 and CACNA1S genotyping tests exhibited an MRT of 91.2 days, this extended MRT is due to the complexity of the technique combined with limited financial resources and low incidence of clinical events compatible with malignant hyperthermia. Among the genes included in the OpenArray®, the mean response time (MRT) was consistently under 10 days across all instances. The shortest MRT was observed for the DPYD test (6.36 days), while the greatest MRT was seen for the CYP3A5 test (8.66 days).
Of the 655 individuals who underwent genetic testing, 83.21% (545/655) were performed prior to the initiation of treatment (preemptively). A total of 1,000 PGx tests were requested for individuals susceptible to receive a dose modification based on genotype. Among these cases, it was found that 7.60% (76 out of 1,000) of the individuals received a dose adjustment according to the genotype results (Figure 3A).
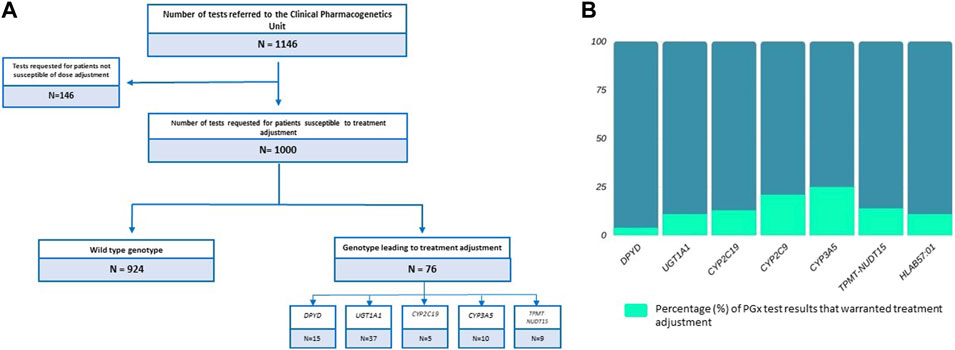
FIGURE 3. (A) Total number of pharmacogenetic tests performed in the study period. Number of tests requests requested for patients susceptible to treatment adjustment. Number of genotypes that led to treatment adjustment stratified by genes. (B) Percentage (%) of pharmacogenetic test results per gene that warranted a phenotype-based treatment adjustment.
The results of the PGx testing of DPYD, UGT1A1, CYP2C19, CYP3A5, and HLA-B57:01 indicated the following: 3.86% (15/388) of DPYD tests and 11.01% (37/336) of UGT1A1 tests required treatment adjustments of 5-Fluorouracil/Capecitabine and Irinotecan, respectively. A proportion of 13.15% (5/38) of CYP2C19 genetic tests prompted the administration of a different treatment from voriconazole. In the case of CYP3A5, 25.64% (10/39) of PGx tests led to adjustments in the starting dose of Tacrolimus in eligible kidney transplant patients. Finally, it was noted that 13.63% (9/66) of the TPMT/NUDT15 tests conducted resulted in a modification of the dose of either Azathioprine or 6-Mercaptopurine. Only 3 out of 14 CYP2C9 tests warranted dose modification of siponimod. In addition to pharmacogenomic tests performed using OpenArray technology, the results of HLA-B57:01 genotyping indicated that 11.32% (6/53) of patients were at elevated risk for developing abacavir hypersensitivity, thereby requiring an alternative Highly Active Antiretroviral Therapy (HAART) regimen (Figure 3B).
With respect to the RYR1 gene, a significant proportion (50%, 2/4) of individuals possessed at least one clinically relevant variant in the RYR1 gene. It is worth noting that all genetic assessments for malignant hyperthermia were performed on patients who had previously experienced a compatible adverse event in the operating room, hence none of these tests were conducted preemptively. One of the identified variants, NM_000540.2 (RYR1):c.15014C>T(p.Thr5005Met), was classified as a variant of uncertain significance, which indicates that further analysis, such as a more comprehensive assessment, would be required to draw definitive conclusions regarding the subject’s increased or decreased risk of developing malignant hyperthermia. On the other hand, the other detected variant, NM_000540.2 (RYR1):c.14545G>A p.(Val4849Ile), was classified as a pathogenic variant.
Finally, Table 1 showcases the absolute number of results obtained for each different genotype as well the proportion observed.
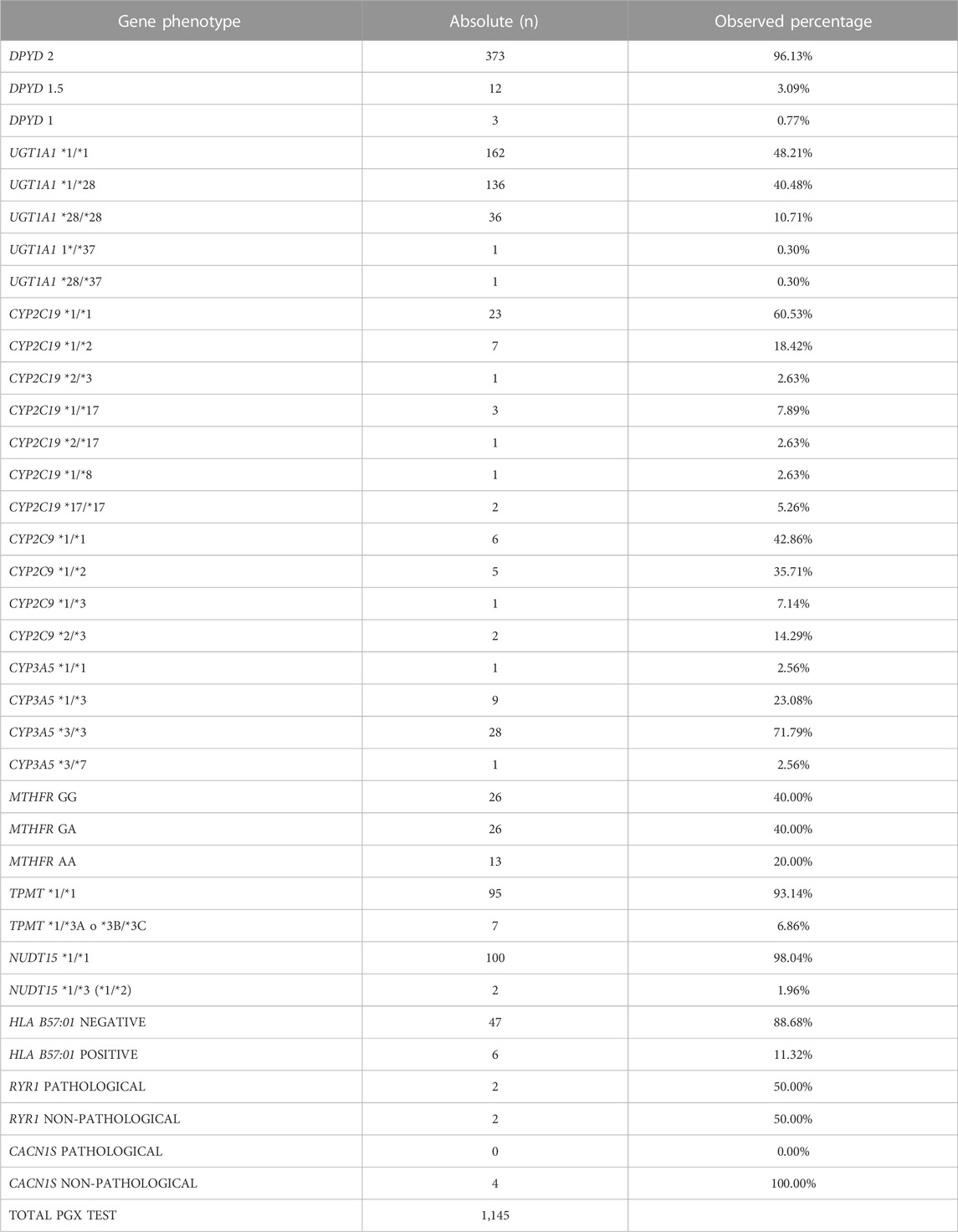
TABLE 1. Results obtained for each different genotype and observed proportion.
4 Discussion
The role of preemptive pharmacogenetics in enhancing treatment efficacy and significantly reducing adverse drug reactions is well established, as evidenced by recent publications (Turongkaravee et al., 2021; Swen et al., 2023). We have conducted a comprehensive analysis of the performance of our Clinical Pharmacogenetic Unit by examining the activities performed over a 1-year period. This study aims to evaluate the trends and outcomes observed in both test petitions and results, as well as the challenges faced by our Clinical Pharmacogenetics Unit. In order to showcase the advancements made, we performed a head-to-head comparison of real-world data with previously published activity results from the same Unit, over two different time periods. By comparing and contrasting our findings with previous research performed within the same setting, we seek to provide insights into significant achievements, identify areas for improvement, and outline future directions that have the potential to advance and enhance precision medicine practices.
Our analysis encompassed a total of 1,000 PGx tests specifically requested for individuals deemed susceptible to benefit from a dosage/treatment modification based on their genetic profile. The results revealed that a noticeable amount of these tests, 7.60% (76/1,000), led to modified treatments being implemented according to the genotype outcome. Few evidence has been published describing global prevalence of PGx variants in a similar population cohort to contrast this figure (Runcharoen et al., 2021).
Despite currently being the two most commonly requested PGx tests, fluoropyrimidines and immunosuppressants were found to constitute only 2.7% and 6.7%, respectively, of our previously reported overall laboratory activity (Borobia et al., 2018). This further reflects the increase of activity of both our laboratory and oncology services something concurrent with other reported results within Europe (Bignucolo et al., 2023). However, our proportion of DPYD of patients with decreased allele activity score (3.86%) differed from similar studies conducted in European cohorts that reported a higher prevalence, albeit in a larger sample size (Pallet et al., 2020) as well as the estimates provided by the European Medicines Agency (EMA) (European Medicines Agency, 2020). No definitive explanation for these differences was discerned; however, it is plausible that variations in demographics, ethnic diversity, and sample size may have contributed to the observed disparities.
In contrast, our CYP2C19 and CYP3A5 data reveals a higher variant prevalence compared to the figures described in Caucasian and European populations (Hicks et al., 2017; Buendía et al., 2020). Thus, the genetic characteristics observed in our region could potentially influence the prevalence rates observed in genetic studies. These results provide compelling support for the implementation of preemptive testing strategies of both these genes and highlight the heterogeneity in genotypes between different population subsets within Europe. In relative terms, our results show that the highest proportion of treatment adjustments was observed for tacrolimus among eligible kidney transplant patients, with 25.64% of PGx tests leading to modifications in the starting dose. This figure aligns more closely with the results published in Eastern populations, suggesting a potential shift in the demographic of the treated population (Maurya et al., 2022).
In absolute terms, DPYD and UGT1A1 testing led to the most significant treatment adjustments, identifying a total of 15 and 37 patients respectively that required a modified treatment approach. Both results emphasize the clinical value of incorporating PGx testing into routine practice and shed light on the potential benefits of personalized medicine in improving patient care.
The comparison of our data with a similar study conducted in a different setting and over a more extended timeframe is of particular significance. Zhang et al., despite exploring a lesser number of genotypes (CYP2C19, CYP2C9, MTHFR, VKORC1 and ALDH) highlighted P450 2C19 as their most frequently requested test, constituting 50.2% of their total inquiries (Zhang et al., 2021). In contrast, our study found that this specific test accounted for a mere 3.31% of the overall requested PGx tests. Notably, Zhang et al. reported that a majority of PGx requests in their setting originated from the Cardiology and Critical Care Units, representing a combined 55% of the total requests (Zhang et al., 2021). Surprisingly, the Oncology Department contributed only 0.6% of the total PGx requests in their study. However, the authors did not provide details on the availability of DPYD or UGT1A1 testing, which could potentially explain these substantial variations (Zhang et al., 2021). While it is crucial to recognize that these differences could be influenced by the indications specified by the Chinese Regulatory Authority, it is important to note that no information pertaining to this aspect was found in our research.
Previously published data by Borobia et al. analyzed the activity of LPUH PGx testing laboratory. The study spanned 3 years from January 2014 to December 2016. During this period, the laboratory conducted 2,539 PGx test (Borobia et al., 2018), 2,287 excluding IL28B genotyping which is no longer available due to the advent of new retroviral therapies (Ghany et al., 2020). When compared to our current data, testing activity has increased roughly 35% over the course of nearly 6 years. While our test menu has changed to accommodate emerging pharmacogenetic insights, the key driver behind the increased demand for testing might have been the regulatory guidance and heightened awareness among healthcare providers.
When examining specific test requests, significant disparities emerge upon comparing our data with that presented in the aforementioned paper. Particularly striking is the discernible decline observed in HLA-B57:01 screening requests (previously reported to be the most solicited test) which has diminished by nearly 91% annually (corresponding to a net disparity of 506 petitions) when compared to our present findings. This unmistakably signifies a change in the management of HIV patients by healthcare professionals, wherein the utilization of abacavir has been relegated to a later stage when compared to the contemporary approach of HAART combinations (Ruiz-Algueró et al., 2022).
Of the remaining available tests, the second most petitioned PGx test reported by Borobia et al., was TPMT, which contrasts greatly with our data. In our study, the medical oncology department emerged as the primary requester of PGx tests, primarily due to the high volume of patients attended with colorectal cancer. This data is consistent with both the mean age of all patients genotyped, as well as the two most petitioned tests. This could be explained, at least in part, by the inclusion of DPYD genotyping for these patients in the summary of product characteristics (SmPC) of capecitabine and 5-FU and security alerts issued by the Spanish Agency of Medicines and Medical Devices (Agencia Española del Medicamento y Productos Sanitarios, 2020), despite having proven to be a safe, effective, and cost-effective years prior (Henricks et al., 2018). This correlation has been reported by other laboratories across Europe (Bignucolo et al., 2023). Similarly, the genotyping of UGT1A1 is indicated prior to the administration of irinotecan (European Medicines Agency, 2021). Given the significant impact of colorectal cancer and the therapeutic implications of DPYD and UGT1A1 genotyping, it is understandable that medical oncology had the highest demand for PGx testing services in this study. This increase of activity showcases the impact Regulatory Agencies in enabling the widespread acceptance of PGx testing by encouraging the implementation of preemptive genotyping strategies.
These findings, as well as the increase in DPYD and UGT1A1 PGx petitions, underscore the clinical relevance and practical application of genotype-guided medication management in optimizing treatment efficacy and patient outcomes. They also showcase the impact of incorporating preemptive genotyping strategies into clinical guidelines and SmPC’s in enabling the implementation of PGx testing.
Despite the promising findings, we continue to encounter difficulties that exemplify why the widespread implementation of PGx testing remains a challenge. One such obstacle is the interpretation of a test result performed at a different laboratory (with a possibly different technique), something not uncommon given the increasing flux of patients across borders.
Another significant issue we encountered pertains to the lack of expertise and awareness by the petitioner, which occasionally led prescribing clinicians to order the same test repeatedly (duplicated tests were excluded from our analyses) or to do so in cases that were incongruous: a petition for a PGx test for TPMT in a patient that has been subjected to an orthotopic liver transplant, where the donor’s genotype can condition whether or not the patients suffer side effects in response to treatment (Breen et al., 2005).
Likewise, it was frequently observed that petitioners would request a PGx test, such as CYP3A5, for a kidney transplant recipient who was already undergoing treatment adjustment as per trough blood concentrations. In such a scenario, patient genotype would be of little clinical relevance, with blood concentrations guiding any treatment modifications (Borobia et al., 2009).
In our hospital, we have developed an internal record-keeping system that helps us identify instances of duplicate orders or cases where pharmacogenetic testing has been previously conducted for a particular patient. This internal system serves as a safeguard to prevent unnecessary repetition of tests. Additionally, for patients already undergoing therapeutic drug monitoring, such cases are identified through a manual review of the patient’s medical history by the clinician responsible for handling the test request. This review process also allows us to prioritize and manage cases that require urgent pharmacogenetic results.
It therefore becomes apparent that genetic information is complex, and effectively translating it into actionable recommendations for clinicians requires clear guidelines and standardized reporting formats. Our Clinical Pharmacogenetics Unit exemplifies a model useful to bridge some of these challenges by integrating the interpretation of complex genetic information with the patient’s clinical status, therapeutic goals, and concomitant therapy. Something only possible by establishing a multidisciplinary unit that comprises expert geneticists and clinical pharmacologists with pharmacogenetic expertise.
The findings of this study should be interpreted within the context of several limitations. Despite being active for 10 years, the data collected by the Clinical Pharmacogenetics Unit has been subject to various information system changes as the LPUH adapted its Information Technology infrastructure, and electronical medical health records platform among others. This precluded the study from spanning a longer time period, as collected data from the inception of the Unit was limited. The impact of the COVID-19 pandemic also hindered the activity of the Unit, not only because it suffered a complete cessation of activity during the lockdown period, but because in order to ease the economic burden caused by the pandemic financial reallocations were carried throughout the SNHS that rippled through units and departments that, despite being of great relevance for individual patient care, were not considered a priority at the time (Carrera-Hueso et al., 2021). The absence of robust cost-effective studies that warrant public health expenditure in PGx strategies such as the ones carried out by our Unit further worsened this issue. In this sense, promising new studies are currently underway, with some being developed within our own research group. These studies may offer compelling arguments regarding the impact of pharmacogenetics on SNHS sustainability (Monserrat Villatoro et al., 2020).
This study represents a significant contribution as it is, to the best of our knowledge, the first to offer comprehensive insights into the activity of a Clinical Pharmacogenetics Unit over two different time periods in the same setting. By doing so, we provide a deeper understanding of PGx practices in a real-world setting, with both their challenges and achievements. The findings presented highlight a notable rise in the utilization of PGx testing, indicating a growing awareness and acknowledgment among healthcare professionals regarding its significant role in customizing treatments according to individual genetic profiles. This increasing acceptance signals a shift towards a more personalized medicine, emphasizing the aim of delivering optimized and safe therapeutic interventions for every patient. By leveraging the insights provided by PGx testing, healthcare providers can make informed decisions and ensure the administration of treatments that are both efficacious and tailored to each patient’s unique genetic makeup.
The real-world data presented in this study contributes to the growing body of evidence supporting the integration of PGx testing into daily clinical practice, allowing for tailored treatments based on individual genetic profiles, ultimately enhancing patient care. The implementation of PGx strategies that include a multidisciplinary approach that includes a geneticist and a clinical pharmacologist has the potential to significantly enhance the efficient utilization of available resources within healthcare systems, bringing us one step closer to a truly individualized healthcare. By optimizing the efficacy of current treatments and reducing the incidence of adverse events, pharmacogenetics can also contribute to a more sustainable healthcare system. However, further studies are needed to comprehensively explore and validate the full extent of these benefits, ensuring that the integration of pharmacogenetic and economic approaches is evidence-based and widely applicable.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: European Nucleotide Archive (ENA), PRJEB66347.
Ethics statement
The studies involving humans were approved by the ethics committee of the La Paz University Hospital (PI-2915). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
Conceptualization: RR-A and AB. Methodology: SS, JMD-A, JG-E, PA, AGL, ES-M, IG-G, ERG, and CR-A. Funding Acquisition: IG-G, RR-A, and AB. Project Administration: AJC, SR-N, RR-A, and AB. Supervision: AJC, SR-N, RR-A, and AB. Writing draft: SS, RR-A, and AB. All authors reviewed the manuscript.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union (Grants numbers: JR21/00003, JR22/00036, CM22/00156, PMP22/00055).
Acknowledgments
We would like to express our sincere gratitude to the Next Generation Sequencing Unit and Bioinformatics Unit for their invaluable support and assistance in malignant hyperthermia genetic studies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1292416/full#supplementary-material
References
Agencia Española del Medicamento y Productos Sanitarios (AEMPS) (2020). Security Alert: fluorouracil, capecitabine, tegafur, and flucytosine in patients with dihydropyrimidine dehydrogenase deficiency. Available at: https://www.aemps.gob.es/informa-en/fluorouracilo-capecitabina-tegafur-y-flucitosina-en-pacientes-con-deficit-de-dihidropirimidina-deshidrogenasa/?lang=en (Accessed June 16, 2023).
Bielinski, S. J., Olson, J. E., Pathak, J., Weinshilboum, R. M., Wang, L., Lyke, K. J., et al. (2014). Preemptive genotyping for personalized medicine: design of the right drug, right dose, right time-using genomic data to individualize treatment protocol. Mayo Clin. Proc. 89, 25–33. doi:10.1016/J.MAYOCP.2013.10.021
Bignucolo, A., De Mattia, E., Roncato, R., Peruzzi, E., Scarabel, L., D’Andrea, M., et al. (2023). Ten-year experience with pharmacogenetic testing for DPYD in a national cancer center in Italy: lessons learned on the path to implementation. Front. Pharmacol. 14, 1199462. doi:10.3389/fphar.2023.1199462
Birdwell, K. A., Decker, B., Barbarino, J. M., Peterson, J. F., Stein, C. M., Sadee, W., et al. (2015). Clinical pharmacogenetics implementation consortium (CPIC) guidelines for CYP3A5 genotype and tacrolimus dosing. Clin. Pharmacol. Ther. 98, 19–24. doi:10.1002/cpt.113
Borobia, A. M., Dapia, I., Tong, H. Y., Arias, P., Muñoz, M., Tenorio, J., et al. (2018). Clinical implementation of pharmacogenetic testing in a hospital of the Spanish national health system: strategy and experience over 3 years. Clin. Transl. Sci. 11, 189–199. doi:10.1111/cts.12526
Borobia, A. M., Romero, I., Jimenez, C., Gil, F., Ramirez, E., De Gracia, R., et al. (2009). Trough tacrolimus concentrations in the first week after kidney transplantation are related to acute rejection. Ther. Drug Monit. 31, 436–442. doi:10.1097/FTD.0b013e3181a8f02a
Breen, D. P., Marinaki, A. M., Arenas, M., and Hayes, P. C. (2005). Pharmacogenetic association with adverse drug reactions to azathioprine immunosuppressive therapy following liver transplantation. Liver Transpl. 11, 826–833. doi:10.1002/lt.20377
Brunette, C. A., Miller, S. J., Majahalme, N., Hau, C., MacMullen, L., Advani, S., et al. (2020). Pragmatic trials in genomic medicine: the integrating pharmacogenetics in clinical care (I-picc) study. Clin. Transl. Sci. 13, 381–390. doi:10.1111/cts.12723
Buendía, J. A., Halac, E., Bosaleh, A., Garcia de Davila, M. T., Imvertasa, O., and Bramuglia, G. (2020). Frequency of CYP3A5 genetic polymorphisms and tacrolimus pharmacokinetics in pediatric liver transplantation. Pharmaceutics 12, 898. doi:10.3390/pharmaceutics12090898
Carrera-Hueso, F. J., Álvarez-Arroyo, L., Poquet-Jornet, J. E., Vázquez-Ferreiro, P., Martínez-Gonzalbez, R., El-Qutob, D., et al. (2021). Hospitalization budget impact during the COVID-19 pandemic in Spain. Health Econ. Rev. 11, 43. doi:10.1186/s13561-021-00340-0
Chandran, V., Siannis, F., Rahman, P., Pellett, F. J., Farewell, V. T., and Gladman, D. D. (2010). Folate pathway enzyme gene polymorphisms and the efficacy and toxicity of methotrexate in psoriatic arthritis. J. Rheumatol. 37, 1508–1512. doi:10.3899/jrheum.091311
D’Andrea, E., Marzuillo, C., Pelone, F., De Vito, C., and Villari, P. (2015). Genetic testing and economic evaluations: a systematic review of the literature. Epidemiol. Prev. 39, 45–50.
Díaz-Villamarín, X., Piñar-Morales, R., Barrero-Hernández, F. J., Antúnez-Rodríguez, A., Cabeza-Barrera, J., and Morón-Romero, R. (2022). Pharmacogenetics of siponimod: a systematic review. Biomed. Pharmacother. 153, 113536. doi:10.1016/J.BIOPHA.2022.113536
European Medicines Agency (2020). EMA recommendations on DPD testing prior to treatment with fluorouracil, capecitabine, tegafur and flucytosine. Available at: https://www.ema.europa.eu/en/news/ema-recommendations-dpd-testing-prior-treatment-fluorouracil-capecitabine-tegafur-flucytosine (Accessed June 20, 2023).
European Medicines Agency (2021). Onivyde pegylated liposomal: annex I summary of product characteristics. Amsterdam: European Medicines Agency. Summary of product characteristics.
European Molecular Genetics Quality Network (2023). Recommendations of the European molecular genetics quality Network. Available at: https://www.emqn.org/participating-in-eqa/eqa-schemes-in-brief/ (Accessed June 14, 2023).
García, I. G., Carcas, A. J., and Borobia, A. M. (2020). Strategy to effectively and efficiently implement voriconazole pharmacogenetics in clinical practice. Pharmacogenomics 21, 647–649. doi:10.2217/pgs-2020-0029
García-García, I., and Borobia, A. M. (2021). Current approaches and future strategies for the implementation of pharmacogenomics in the clinical use of azole antifungal drugs. Expert Opin. Drug Metab. Toxicol. 17, 509–514. doi:10.1080/17425255.2021.1890715
Ghany, M. G., and Morgan, T. R.AASLD-IDSA Hepatitis C Guidance Panel (2020). Hepatitis C guidance 2019 update: american association for the study of liver diseases-infectious diseases society of America recommendations for testing, managing, and treating hepatitis C virus infection. Hepatology 71, 686–721. doi:10.1002/hep.31060
Gonsalves, S. G., Dirksen, R. T., Sangkuhl, K., Pulk, R., Alvarellos, M., Vo, T., et al. (2019). Clinical pharmacogenetics implementation consortium (CPIC) guideline for the use of potent volatile anesthetic agents and succinylcholine in the context of RYR1 or CACNA1S genotypes. Clin. Pharmacol. Ther. 105, 1338–1344. doi:10.1002/cpt.1319
Henricks, L. M., Lunenburg, C. A. T. C., de Man, F. M., Meulendijks, D., Frederix, G. W. J., Kienhuis, E., et al. (2018). DPYD genotype-guided dose individualisation of fluoropyrimidine therapy in patients with cancer: a prospective safety analysis. Lancet Oncol. 19, 1459–1467. doi:10.1016/S1470-2045(18)30686-7
Hicks, J. K., Sangkuhl, K., Swen, J. J., Ellingrod, V. L., Müller, D. J., Shimoda, K., et al. (2017). Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin. Pharmacol. Ther. 102, 37–44. doi:10.1002/cpt.597
Jin, Y., Borell, H., Gardin, A., Ufer, M., Huth, F., and Camenisch, G. (2018). In vitro studies and in silico predictions of fluconazole and CYP2C9 genetic polymorphism impact on siponimod metabolism and pharmacokinetics. Eur. J. Clin. Pharmacol. 74, 455–464. doi:10.1007/s00228-017-2404-2
Karamperis, K., Koromina, M., Papantoniou, P., Skokou, M., Kanellakis, F., Mitropoulos, K., et al. (2021). Economic evaluation in psychiatric pharmacogenomics: a systematic review. Pharmacogenomics J. 21, 533–541. doi:10.1038/s41397-021-00249-1
Leusink, M., Onland-Moret, N. C., De Bakker, P. I. W., De Boer, A., and Maitland-Van Der Zee, A. H. (2016). Seventeen years of statin pharmacogenetics: a systematic review. Pharmacogenomics 17, 163–180. doi:10.2217/pgs.15.158
Maurya, M. R., Gautam, S., Raj, J. P., Saha, S., Ambre, S., Thakurdesai, A., et al. (2022). Evaluation of genetic polymorphism of CYP3A5 in normal healthy participants from western India - a cross-sectional study. Indian J. Pharmacol. 54, 97–101. doi:10.4103/ijp.ijp_279_21
Monserrat Villatoro, J., García García, I., Bueno, D., de la Cámara, R., Estébanez, M., López de la Guía, A., et al. (2020). Randomised multicentre clinical trial to evaluate voriconazole pre-emptive genotyping strategy in patients with risk of aspergillosis: vorigenipharm study protocol. BMJ Open 10, e037443. doi:10.1136/bmjopen-2020-037443
Moriyama, B., Obeng, A. O., Barbarino, J., Penzak, S. R., Henning, S. A., Scott, S. A., et al. (2017). Clinical pharmacogenetics implementation consortium (CPIC) guidelines for CYP2C19 and voriconazole therapy. Clin. Pharmacol. Ther. 102, 45–51. doi:10.1002/cpt.583
Pallet, N., Hamdane, S., Garinet, S., Blons, H., Zaanan, A., Paillaud, E., et al. (2020). A comprehensive population-based study comparing the phenotype and genotype in a pretherapeutic screen of dihydropyrimidine dehydrogenase deficiency. Br. J. Cancer 123, 811–818. doi:10.1038/s41416-020-0962-z
Richards, S., Aziz, N., Bale, S., Bick, D., Das, S., Gastier-Foster, J., et al. (2015). Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of medical genetics and Genomics and the association for molecular Pathology. Genet. Med. 17, 405–424. doi:10.1038/gim.2015.30
Rosas-Alonso, R., Queiruga, J., Arias, P., Del Monte, Á., Yuste, F., Rodríguez-Antolín, C., et al. (2021). Analytical validation of a laboratory-development multigene pharmacogenetic assay. Pharmacogenet Genomics 31, 177–184. doi:10.1097/FPC.0000000000000438
Ruiz-Algueró, M., Hernando, V., Riero, M., Blanco Ramos, J. R., de Zarraga Fernández, M. A., Galindo, P., et al. (2022). Temporal trends and geographic variability in the prescription of antiretroviral treatments in people living with HIV in Spain, 2004-2020. J. Clin. Med. 11, 1896. doi:10.3390/jcm11071896
Runcharoen, C., Fukunaga, K., Sensorn, I., Iemwimangsa, N., Klumsathian, S., Tong, H., et al. (2021). Prevalence of pharmacogenomic variants in 100 pharmacogenes among southeast asian populations under the collaboration of the southeast asian pharmacogenomics research Network (SEAPharm). Hum. Genome Var. 8, 7. doi:10.1038/s41439-021-00135-z
Sociedad Española de Farmacogenética y Farmacogenómica (2023). Recomendaciones farmacogenéticas de los grupos de trabajo de la SEFF para la implementación de la farmacogenética en la práctica clínica. Available at: https://seff.es/recomendaciones-grupos-de-trabajo-de-la-seff/ (Accessed August 9, 2023).
Swen, J. J., van der Wouden, C. H., Manson, L. E., Abdullah-Koolmees, H., Blagec, K., Blagus, T., et al. (2023). A 12-gene pharmacogenetic panel to prevent adverse drug reactions: an open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet 401, 347–356. doi:10.1016/S0140-6736(22)01841-4
Tong, H. Y., Borobia, A. M., Quintana-Díaz, M., Fabra, S., González-Viñolis, M., Fernández-Capitán, C., et al. (2021). Acenocoumarol pharmacogenetic dosing algorithm versus usual care in patients with venous thromboembolism: a randomised clinical trial. J. Clin. Med. 10, 2949. doi:10.3390/jcm10132949
Tong, H. Y., Dávila-Fajardo, C. L., Borobia, A. M., Martínez-González, L. J., Lubomirov, R., Perea León, L. M., et al. (2016). A new pharmacogenetic algorithm to predict the most appropriate dosage of acenocoumarol for stable anticoagulation in a mixed Spanish population. PLoS One 11, e0150456. doi:10.1371/journal.pone.0150456
Tuková, J., Chládek, J., Hroch, M., Nemcová, D., Hoza, J., and Dolezalová, P. (2010). 677TT genotype is associated with elevated risk of methotrexate (MTX) toxicity in juvenile idiopathic arthritis: treatment outcome, erythrocyte concentrations of MTX and folates, and MTHFR polymorphisms. J. Rheumatol. 37, 2180–2186. doi:10.3899/jrheum.091427
Turongkaravee, S., Jittikoon, J., Rochanathimoke, O., Boyd, K., Wu, O., and Chaikledkaew, U. (2021). Pharmacogenetic testing for adverse drug reaction prevention: systematic review of economic evaluations and the appraisal of quality matters for clinical practice and implementation. BMC Health Serv. Res. 21, 1042. doi:10.1186/s12913-021-07025-8
Weitzel, K. W., Elsey, A. R., Langaee, T. Y., Burkley, B., Nessl, D. R., Obeng, A. O., et al. (2014). Clinical pharmacogenetics implementation: approaches, successes, and challenges. Am. J. Med. Genet. C Semin. Med. Genet. 166C, 56–67. doi:10.1002/ajmg.c.31390
Keywords: pharmacogenetic dosing, preemptive genotyping, real-world data, personalized medicine, retrospective analysis
Citation: Stewart S, Dodero-Anillo JM, Guijarro-Eguinoa J, Arias P, Gómez López De Las Huertas A, Seco-Meseguer E, García-García I, Ramírez García E, Rodríguez-Antolín C, Carcas AJ, Rodriguez-Novoa S, Rosas-Alonso R and Borobia AM (2023) Advancing pharmacogenetic testing in a tertiary hospital: a retrospective analysis after 10 years of activity. Front. Pharmacol. 14:1292416. doi: 10.3389/fphar.2023.1292416
Received: 11 September 2023; Accepted: 02 October 2023;
Published: 19 October 2023.
Edited by:
Sean Patrick David, NorthShore University HealthSystem, United StatesReviewed by:
Rocio Gomez, Center for Research and Advanced Studies (CINVESTAV), MexicoAnn M. Moyer, Mayo Clinic, United States
Copyright © 2023 Stewart, Dodero-Anillo, Guijarro-Eguinoa, Arias, Gómez López De Las Huertas, Seco-Meseguer, García-García, Ramírez García, Rodríguez-Antolín, Carcas, Rodriguez-Novoa, Rosas-Alonso and Borobia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rocio Rosas-Alonso, cm9zYXMuYWxvbnNvLnJvY2lvQGdtYWlsLmNvbQ==; Alberto M. Borobia, YWxiZXJ0by5ib3JvYmlhQHNhbHVkLm1hZHJpZC5vcmc=