 Annika Krick
Annika Krick Miriam Arnold
Miriam Arnold Jörg Felfe
Jörg Felfe- 1Department of Work, Organizational and Business Psychology, Helmut Schmidt University Hamburg/University of the Federal Armed Forces, Hamburg, Germany
- 2Leibniz Institute for Resilience Research, Mainz, Germany
Introduction: Telework brings opportunities (e.g., flexibility) but also potential risks for health (e.g., fewer boundaries, constant availability). SelfCare could be a relevant work-related resource to reduce these health risks when working from home. SelfCare is part of the Health-oriented Leadership model and describes how individuals prioritize their own health, are aware of signs of stress, and actively promote their own health. In this paper, we postulate that telework enables more SelfCare at home, e.g., due to higher flexibility and autonomy. As SelfCare at home can be used more flexibly, it is also conceivable that the effectiveness of SelfCare increases the more employees work from home. Additionally, for hybrid working employees, the question arises whether SelfCare at both work contexts is distinct and makes an independent contribution to health and whether they even reinforce each other.
Methods: Our hypotheses were tested in a longitudinal study with N = 727 employees from different industries. This study examined (1) the level of SelfCare on-site and at home (within- and between-person-effects), (2) the moderating effect of telework intensity on the effectiveness of SelfCare at home on health and performance indicators, and (3) direct and interacting effects of SelfCare at home and on-site for health.
Results: Between- and within-person-differences show that SelfCare is more prevalent when working from home. Furthermore, SelfCare at home is related to less strain and health complaints as well as more relaxation and performance for individuals with higher telework intensity. SelfCare at home and on-site independently predict strain and health complaints and interact with regard to strain.
Discussion: SelfCare appears to be more relevant with higher telework intensity and is thus an even more important health resource in the telework context. Organizations should provide continuing interventions and online tools to promote SelfCare among employees and leaders. Since little is known about the level and the effects of SelfCare in the telework context, these findings expand previous research on Health-oriented Leadership in the telework context.
1 Introduction
Telework and particularly hybrid work arrangements (working both from home and on-site) have become the new normal and will characterize the future world of work (Bonin et al., 2020; Wang et al., 2021; Kunze and Hampel, 2023). The terms telework and working from home will be used as synonyms here. Telework has clear advantages when compared to work on-site in terms of higher autonomy and flexibility but also may have risks for health (Felfe et al., 2022). Potential risks are extended working hours, reduced recovery periods, and an increase in sedentary behavior (Göpner-Reinecke, 2019; Bonin et al., 2020; Bouziri et al., 2020). Niebuhr et al. (2022) even showed that a higher amount of weekly time working from home was associated with more stress-related symptoms. Therefore, it seems also important to counteract these health risks and to maintain and promote health when working at home. SelfCare could be a relevant work-related resource to reduce these health risks. SelfCare is part of the Health-oriented Leadership (HoL) concept (Franke et al., 2014) and describes how followers and leaders take care of their own health at work. SelfCare encompasses health-specific behavior and attitudes toward the own health. SelfCare is differentiated into three facets, Value, Awareness, and Behavior: (1) Individuals high in SelfCare prioritize their own health (Value), (2) are aware of their own health-related warning signs (e.g., signs of stress and overload such as depressed mood, social withdrawal, concentration difficulties; Awareness), (3) and take appropriate action to actively promote their own health (e.g., optimizing work routines, work conditions, or work-life-balance by setting priorities, caring for undisturbed working, avoiding unbalanced body-posture, caring for enough space, taking regular breaks, or avoiding overtime; Behavior; Franke et al., 2014).
So far, SelfCare has been mainly studied in the traditional work context. Ample research has already shown that SelfCare at the workplace (on-site) is beneficial to employees' health (Grimm et al., 2021; Kaluza and Junker, 2022; Arnold and Rigotti, 2023). But it is unknown, if SelfCare is also important when working at home. SelfCare at home and SelfCare on-site refer to the same behavior, just being displayed at different work locations. However, the extent to which employees exhibit SelfCare may depend on the workplace. For example, employees in one location may be more aware of their own warning signs, prioritize their health and adopt more positive health behaviors instead of compromising their health than in another location. As telework is associated with more flexibility and autonomy (Felfe et al., 2022) this could potentially offer better opportunities for SelfCare at home than in the office. The question if there are actually better opportunities for SelfCare at home has not yet been studied. The first aim of this study is therefore, to investigate the differences in the level of SelfCare depending on the work location and show that the SelfCare level will be higher at home. For this purpose, not only between-person differences between employees working fully from home and employees solely working on-site were examined, but also within-person differences were considered (employees working both from home and on-site).
Moreover, the effectiveness of SelfCare when working from home is yet unclear. As the effects of SelfCare on health indicators are well-examined in the traditional work context (Grimm et al., 2021; Arnold and Rigotti, 2023), it has to be shown that SelfCare at home is also effective for followers' health. As the effects of SelfCare on work-related attitudes and work performance are less examined in previous research, we also considered work performance as a relevant outcome to extend previous evidence for the effectiveness of SelfCare. If SelfCare levels are higher at home and SelfCare is also effective at home, it is conceivable that SelfCare at home is more effective the more days employees work from home (e.g., 4 days at home compared to 1 day at home). Golden and Veiga (2008) and Santiago Torner (2023) have already postulated the moderating effect of telework intensity on the relationship between leadership and employee outcomes. Therefore, the second aim of this study is not only to examine the effectiveness of SelfCare at home for health indicators and performance but also if this effect depends on telework intensity (defined as days per week working from home; from 1 day to 5 days; 1 or 2 days working from home represents a less intense form of telework compared to spending the major portion of one's work week away from the office which represents a high intense form of telework).
For hybrid work, there are two venues for taking care of one's health while at work: SelfCare at the office and SelfCare at home. The question arises whether SelfCare at both work contexts is distinct and contributes independently to health and whether they even reinforce each other. Concerning consistency, it could be most conducive to health if hybrid employees take care of their health at both places of work. Inconsistent patterns, however, may be detrimental to employees' health, e.g., when employees are successful in displaying SelfCare at home (i.e., taking regular breaks, reducing demands by optimizing their work routine by setting priorities, caring for undisturbed working, etc.), but endanger their health when working on-site (e.g., get often disturbed, miss taking breaks). Therefore, the third aim of this study is to examine the independent effects of SelfCare at home and SelfCare on-site and their interplay with regard to health.
This study offers significant theoretical and empirical contributions. First, from a theoretical perspective, findings contribute to the knowledge of hindering and facilitating context factors influencing the effectiveness of HoL. While there is research on boundary conditions for the effectiveness of StaffCare (Klebe et al., 2021a, 2023; Pischel et al., 2022), our study identifies work location (i.e., telework intensity) as a facilitating boundary condition for SelfCare and enhances our understanding of the situational contingencies of SelfCare that emerge from ongoing digitization (Krick and Felfe, 2022; Klebe et al., 2023). This study further aligns with research on the opportunities and risks associated with work digitization (Day et al., 2012; De Vincenzi et al., 2022; Niebuhr et al., 2022).
Second, theoretically, it is yet unclear if SelfCare displayed in different locations should be differentiated. Until now, SelfCare has been operationalized without reference to the work location. By focusing on hybrid working employees, this study provides first insights into the independent and amplifying effects of SelfCare at different work locations on health. This allows for a theoretical distinction between SelfCare in remote work environments and on-site and directly leads to practical implications in that our findings have important implications for workplace health promotion. From a practical point of view, examining the differing levels and the interaction of SelfCare at home and on-site provides important knowledge for organizations and practitioners about the importance and the effectiveness of SelfCare when working from home to develop and implement adequate occupational health promotion offers. This knowledge could be a starting point for valuable suggestions and practical implications regarding the use of SelfCare in everyday work life and provides guidelines for designing future work environments, on-site and at home.
Third, from an empirical point of view, this study is one of the first to examine SelfCare at home, considering the growing digital and hybrid working context. Against the background of hybrid work, it is important to know if opportunities for SelfCare differ between contexts and whether SelfCare at home is also relevant. The study contributes to the ongoing discourse on health promotion and Health-oriented Leadership in the digitalized world and provides initial empirical evidence for the relevance of SelfCare in remote work settings (Efimov et al., 2020; Felfe et al., 2022; Krick and Felfe, 2022). Our findings will complement and extend previous literature on SelfCare in the traditional context. By demonstrating the positive impact of SelfCare in remote and hybrid work environments, and initially on work performance as an outcome beyond health, this study extends the validity of the HoL concept and provides additional insights into its effectiveness in digital environments.
From a methodological perspective, this study allows for between-person and within-person differences in SelfCare. Comparing between-person and within-person effects offers a more differentiated picture and helps to clarify potential under- or overestimation due to working conditions. Furthermore, previous studies mainly measured whether employees work from home or not and examined telework as a dichotomous variable (e.g., Caniëls, 2023). Multiple studies criticize such a dichotomous approach and call for a more precise measurement of the intensity of digitalized work and telework (e.g., Bonin et al., 2020; Borle et al., 2021). We follow that call by considering telework intensity as a continuous moderator. Additionally, the study design with two measurement points expands upon previous cross-sectional findings and qualitative studies on SelfCare.
2 Risks and benefits of telework for health
The effects of telework on employee health and wellbeing are not clearly understood. On the one hand, telework is expected to enhance flexibility, potentially impacting both work and health positively. By eliminating commuting, telework reduces stress associated with travel (Murphy et al., 2023). The time saved from commuting can be used for recovery or physical activity, promoting overall health. In addition, telework allows employees to better manage their time and balance family and work commitments, especially for those with young children. This improvement in work-life-balance can positively impact health and wellbeing (Lunau et al., 2014).
Nevertheless, there are also potential risks of telework for employee health and wellbeing, highlighting the need for SelfCare at home. Niebuhr et al. (2022) showed that a higher amount of weekly time working from home was associated with more stress-related symptoms. First, telework can increase individual stress levels because employees try to manage both work and personal life simultaneously. Second, the overarching trend of extended working hours during telework beyond the typical office schedule leads to detrimental effects in the long term, e.g., impeded psychological detachment and recovery from work, decreased sleep quality as well as physical and mental wellbeing (Bonin et al., 2020; Wöhrmann et al., 2020; Cropley et al., 2023). Third, the blurring of work and personal boundaries may eliminate the expectation of being available only during designated working hours, leading to a feeling of being constantly available, even on weekends, potentially increasing work-related stress and negatively impacting overall wellbeing. Fourth, if employers are not legally obliged to address ergonomic concerns for telework, telework may result in poor posture and inadequate work setups at home, potentially leading to physical discomfort (e.g., Bouziri et al., 2020; Moretti et al., 2020). In addition, studies found an increase in sedentary behavior when working from home, which in turn can lead to adverse health effects (McDowell et al., 2020; Hunter et al., 2021). Lastly, while telework may have short-term benefits for minor illnesses, the lack of sufficient downtime can have negative health consequences in the long run if employees do not take adequate breaks. Given the aforementioned arguments, previous research shows both benefits for health but also potential risks when working from home. SelfCare seems to be a relevant resource to counteract these potential risks. Telework brings a shift in responsibility from employer to employee (Cropley et al., 2023). With this shift of control, employees have to regulate their working behavior, e.g., decide when they take rest breaks, design their working place at home, create personal boundaries between private life and work, or find a way to integrate both according to one's own needs (Müller and Niessen, 2019; Diewald, 2020; Niskanen, 2021). Sjöblom et al. (2022) particularly focused on self-related strategies. They found that these are negatively related to burnout among remotely working employees and call for additional research in this field.
3 SelfCare in the remote work context
SelfCare describes how leaders and followers take care of their health by prioritizing their health (Value), being aware of health-related warning signs (Awareness), and actively promoting their health (Behavior: e.g., reducing demands by optimizing personal work routine and working conditions such as setting priorities, caring for undisturbed working, daily planning, avoiding unbalanced body-posture, caring for enough, space, or avoiding draft; Franke et al., 2014). SelfCare is part of the Health-oriented Leadership concept (Franke et al., 2014) which differentiates between StaffCare (promoting followers' health) and SelfCare (promoting one's own health). SelfCare is well-studied for traditional work contexts (Grimm et al., 2021; Kaluza et al., 2021; Klug et al., 2022; Arnold and Rigotti, 2023), but it is an open question how important SelfCare is in digital and hybrid work arrangements, i.e., when SelfCare is displayed at home.
We are only aware of two qualitative studies that deal with HoL in a remote setting. Efimov et al. (2020) conducted an interview study with leaders of virtual teams and identified first insights regarding the feasibility of SelfCare when working from home. Their results showed that virtual leaders value health highly and are aware of health-oriented warning signs. Physical activity and boundary management were particularly mentioned as SelfCare behaviors. Tautz et al. (2022) focused more on StaffCare. Still, their interviews also showed that employees feel a high responsibility for their own health (“I think it is difficult for my supervisor to be responsible for my health while working from home. I see more of the responsibility on myself”)—indicating a high relevance of SelfCare when working from home. So far, however, it is not known whether SelfCare is facilitated or impeded when working from home than on-site.
We argue that telework offers more favorable circumstances for SelfCare compared to traditional office settings for several reasons: First, due to saved commuting time, employees working from home may have more opportunities (in terms of time) to take care of themselves. Second, due to high degrees of flexibility (Gajendran and Harrison, 2007; Ervasti et al., 2022), employees working from home can more easily adapt their work schedule to fit with their individual needs and have thus more possibilities to take care of their health, e.g., employees can ideally choose when to take a break, go for a walk, or do physical exercises (Nickson and Siddons, 2004; Kauffeld et al., 2016). SelfCare strategies could thus be more easily incorporated into the working day. This aligns with studies indicating that flexible work arrangements and the ability to work remotely contribute to enhanced employee wellbeing, fostering an improved balance between work and personal life, and boosting feelings of autonomy and self-leadership (Lundqvist et al., 2022). Third, as telework typically involves greater control and autonomy regarding daily routines, work design, work environment, and other aspects of the workday, such as scheduling, prioritization, and selection of work tasks (Eurofound, 2020; Moretti et al., 2020; Wöhrmann et al., 2020), implementing SelfCare strategies may be facilitated at home. It might be easier to reduce demands by optimizing personal work routines and working conditions (setting priorities, caring for undisturbed working, daily planning, avoiding unbalanced body posture, and caring for enough space). This is further underlined by a study that showed autonomy as a prerequisite for promoting self-leadership (Ho and Nesbit, 2014). Taken together these initial findings and based on this theoretical reasoning, we expect the following:
Hypothesis 1: SelfCare is more pronounced when working from home than when working on-site. These differences appear both on the between-person level (comparing employees fully working from home with employees not working from home) and the within-person level (comparing both working from home and on-site among hybrid working employees).
4 Effectiveness of SelfCare
Based on the assumptions of the HoL model, SelfCare is assumed to have positive effects on health (Franke et al., 2014). Many studies have already shown associations between SelfCare and various health indicators (positive with general health, e.g., Franke et al., 2014; Klug et al., 2019, 2022; Gosch et al., 2023; and wellbeing, e.g., Santa Maria et al., 2019; negative with strain and health complaints, e.g., Franke et al., 2014; Klug et al., 2019, 2022; Gosch et al., 2023; exhaustion, e.g., Grimm et al., 2021; Klebe et al., 2021b; Arnold and Rigotti, 2023; Gosch et al., 2023) and work engagement (Grimm et al., 2021; Kaluza et al., 2021; Arnold and Rigotti, 2023). While there is much evidence for positive effects of SelfCare for employees' health in the traditional office setting, it is unclear if these findings can be transferred to the remote setting (Tautz et al., 2022). Thus, the effectiveness of SelfCare when working from home remains unclear.
Previous studies have already examined other boundary conditions limiting or facilitating the effectiveness of HoL. Regarding StaffCare, studies showed that crises and ICT hassles (Information Communication Technology hassles, i.e., technology malfunctions such as program breakdowns, crashed, and freezing displays; Day et al., 2012) are such crucial factors for its effectiveness (Klebe et al., 2021a, 2023). For example, ICT hassles were shown to impair the effectiveness of StaffCare. Leaders' StaffCare is less related with employee work engagement, strain, and exhaustion with more ICT hassles. Regarding SelfCare, there is still a lack of research examining hindering and facilitating conditions for effectiveness.
We propose telework intensity as a possible moderator based on the calls for further research clarifying the role of high-intensity telework for employee health and well-being (Gajendran and Harrison, 2007; Beckel and Fisher, 2022; Lundqvist et al., 2022). Following the idea of Golden and Veiga (2008) or others (e.g., Santiago Torner, 2023) who showed that telework intensity moderates the relationship between leadership and well-being, we also consider telework intensity as a boundary condition for SelfCare. Golden and Veiga (2008) showed a more pronounced relationship between leadership and wellbeing for those working from home to a high extent compared to those who worked from home to a lesser extent. If telework is also a fruitful environment for SelfCare (regarding its level and efficiency), it is plausible that telework intensity may strengthen the relationship between SelfCare at home and employee health and performance.
At home, SelfCare may be more effective, as employees can choose the best time to take care of their health. Employees working from home are also more able to choose the most fitting strategies, while at the office, opportunities may be restricted for employees to care for their health (e.g., colleagues may interrupt, the feeling to be observed by others, missing materials such as a yoga mat). Due to the high autonomy and flexibility when working from home (Moretti et al., 2020), the telework setting might be a better environment for SelfCare to unfold its positive health effects (Sjöblom et al., 2022). The beneficial effects of SelfCare on health and performance might be higher for employees with the opportunity to work more days from home (high telework intensity) compared to those working fewer days from home (low telework intensity). For high levels of telework intensity, we expect stronger negative relationships of SelfCare with strain and health complaints and also stronger positive relationships with relaxation and performance. At low levels of telework intensity however, we expect a smaller but negative relationship of SelfCare with strain and health complaints and a smaller but positive relationship with relaxation and performance. In other words, if telework intensity is high, the lowest levels of strain/health complaints and the highest levels of performance can be expected with high SelfCare at home. However, high telework intensity may also come at a risk: for high telework intensity but low SelfCare we expect even higher strain levels due to specific health risks at home, such as extended working hours or permanent sedentary behavior. If telework intensity is low, less positive effects on outcomes can be expected with high SelfCare at home.
To replicate previous findings for the office context and provide first empirical evidence for the effectiveness in the telework context, we chose strain and health complaints as health outcomes. To extend previous evidence for the effectiveness of SelfCare, we also include relaxation as a relevant aspect of recovery and work performance (both at home) as further outcomes besides health. These outcomes have not yet been studied in the context of SelfCare. Based on these assumptions, we expect the following:
Hypothesis 2: Telework intensity moderates the relationship between SelfCare at home and health (H2a: strain, H2b: health complaints, H2c: relaxation at home) and work performance at home (H2d). The more a person works from home, the more effective their SelfCare is.
Research has already started on how the work location influences the effectiveness of leadership in general (e.g., Amano et al., 2021; Lamprinou et al., 2021), but has not yet considered Health-oriented Leadership. Until now, research on the independent within-person effects of on-site and remote leadership is missing (Lundqvist et al., 2022). The same applies to SelfCare as part of Health-oriented Leadership (Franke et al., 2014; Klug et al., 2022).
As hybrid working arrangements will be the new normal of the future working world (Kniffin et al., 2021; Mckinsey, 2021), a closer look is needed at SelfCare in hybrid work settings. Regarding these hybrid work settings, employees have two venues to take care of their health while working: on-site and at home. As the telework setting and the office setting are different workplaces, it is an open question whether SelfCare displayed at home and on-site are distinct and independently contribute to employees' health. SelfCare at home and on-site might have different qualities (e.g., social aspects, organizational restrictions, flexibility, and autonomy) and address different health risks. Although SelfCare on-site and at home may be related, some employees may better care for themselves at home, and others have better opportunities on-site. This reasoning leads to the expectation that SelfCare at home and on-site are distinct and might independently predict health.
Hypothesis 3: In hybrid working employees, SelfCare on-site and at home independently predict health indicators (H3a: strain, H3b: health complaints).
It is also an open question whether SelfCare at home and on-site even interact and reinforce each other. While the previous hypothesis (H3) focuses on the independent effects, the focus of the next hypothesis refers to the interplay between SelfCare at home and SelfCare on-site. Both types of effects can coexist independently. A possible interaction effect does not necessitate the presence of main effects, and having main effects does not yet constitute an interaction.
Considering different configurations of Care components, there is already research that looks at the consistency of SelfCare and StaffCare (e.g., Klug et al., 2019), which found distinct consistent und inconsistenten profiles, i.e., employees who experience high StaffCare but low SelfCare (self-sacrifice) and vice versa (follower sacrifice). Similarly, this differentiated perspective can be applied with a more fine grained perspective on SelfCare at different work locations.
In terms of consistency, it is conceivable that hybrid employees are the healthiest if they take care of their health in both work settings (at home and on-site) and are less healthy if they are not able to display SelfCare at all. Low opportunities for SelfCare at one workplace may jeopardize the positive effects of SelfCare at the other workplace, e.g., when employees are successful in displaying SelfCare at home (i.e., taking regular breaks, reducing demands by optimizing their work routine by setting priorities, caring for undisturbed working, etc.), but endanger their health when working on-site (e.g., often get disturbed, miss taking breaks). Poor SelfCare at home could also cause detrimental effects on health, e.g., employees take regular breaks when working on-site, they have an ergonomic work setting, but at home, employees do not care for an ergonomic work setting by their own. Based on this reasoning, we expect the following:
Hypothesis 4: In hybrid working employees, on-site SelfCare moderates the relationship between home SelfCare and health (H4a: strain, H4b: health complaints). Individuals who display SelfCare both at home and on-site are healthier.
5 Materials and methods
5.1 Data collection and samples
The study was conducted as an online survey, including two measurement points with a time lag of 3 months. There is an ongoing discussion in the literature regarding the appropriate time lag for assessing the relationship between dependent (DVs) and independent variables (IVs; Dormann and Griffin, 2015). Some scholars propose relatively short intervals (Dormann and Griffin, 2015), while others argue for longer intervals to capture the stronger relationship between work stressors, resources, and health outcomes over time (Ford et al., 2014). In our study, we opted for a time lag of 3 months as it appeared to strike a balance, allowing us to minimize confounding effects while still capturing the potential effects of SelfCare and health.
Data was collected by a market research institute. All participants gave their informed consent. The first wave of data (t1) was collected in spring 2022, and the second in autumn 2022 (t2). At t1, 1,058 employees participated, while 727 participated at t2, which corresponds to a dropout rate of 31.3%. The sample consisted of 100% full-time working employees. Employees included in the sample had different non-remote and remote working arrangements with 17.9% of participants working solely on-site (n = 130) and 82.1% working from home (n = 597) with varying telework intensity (15.4% working at least 1 day a week from home, 19.8% with 2 days a week, 17.1% with 3 days a week, 12.1% with 4 days a week to 17.7% of participants working 5 days a week or more from home). In total of 52.1% of the participants were female. In total of 57.9% of the participants had no leading position, while 42.1% were responsible for at least five employees (up to more than 20 employees). The mean age was M = 48.31 years (SD = 11.05). Participants worked in several sectors such as IT and telecommunication (11.1%), metal and electrical industry (8.9%), insurance and banking (10.2%), or transport and traffic (5.0%)—either in the private sector (73.7%) or in public services (26.3%). More than two-thirds of the participants reported that they worked in companies with more than 100 employees (100 to 500 employees: 25.6%; more than 500 employees: 45.5% (8.4% up to 10, 10.9% between 11 and 49, 9.6% between 50 and 99). Most of the participants (64.9%) lived in a household with two persons [single 26.7%, with child(ren) 33.3%, with others 3.6%]. When working at home, 69.8% indicated that they never need to care for children (9.5% rarely, 12.9% sometimes, 6.2% often, 1.5% almost always). A total of 80.2% reported that they never had to take care of relatives when working at home (5.7% rarely, 7.7% sometimes, 4.7% often, 1.7% almost always).
5.2 Measures
5.2.1 Telework intensity
Telework intensity was measured by using a single item. Participants were asked to rate the degree of working from home (“On average, how often did you work from home in the last 4 weeks?”). The scale included 1 = never, but my job could theoretically be done from home, 2 = maximum 1 day per week, 3 = 2 days per week, 4 = 3 days per week, 5 = 4 days per week, and 6 = at least 5 days per week.
5.2.2 SelfCare
We assessed SelfCare by the subscale “SelfCare” of the Health-oriented Leadership instrument by Pundt and Felfe (2017). SelfCare was measured at both t1 and t2. Participants were asked to rate their SelfCare within the last 4 weeks. Participants who never work at home were asked to rate their SelfCare when working at the office (SelfCare on-site assessed by employees fully working on-site), while participants who work both at the office and from home (SelfCare on-site and SelfCare at home) rated their SelfCare for both work locations separately. We focused on the subscales “awareness” and “behavior” but excluded “value” because we expect no difference in the attributed value of health between work locations. For reasons of economy, we selected 11 items (awareness: 4 items; behavior: 7 items; sample item: “I try to reduce my demands by optimizing my personal work routine, e.g., set priorities, care for undisturbed working, daily planning).” The scale ranged from 1 = not at all true to 5 = completely true. Cronbach's Alpha was α = 0.81 for t1 (α = 0.84 for t2) regarding SelfCare at home, α = 0.81 for t1 (α = 0.83 for t2) regarding SelfCare on-site (both assessed by employees working at both work locations), and α = 0.86 for t1 (α = 0.84 for t2) regarding SelfCare on-site for employees fully working on-site.
5.2.3 Strain (irritation)
Emotional irritation served as an indicator of participants' strain. Emotional irritation was measured at t2 with one subscale of the irritation scale by Mohr et al. (2005). For reasons of economy, we have dispensed with one item (“From time to time I feel like a bundle of nerves”), so that the scale consisted of four items. Items were for example “I get irritated easily, although I don't want this to happen.” The scale ranged from 1 = never to 5 = almost always. Cronbach's Alpha was α = 0.89.
5.2.4 Health complaints
We measured health complaints by using common physical and somatic symptoms adapted from a scale developed by Mohr (1986). Participants were asked to rate the frequency they experienced each physical (4 items, “headache, back, shoulder or neck pain,” “sleep disturbance,” “cardiopulmonary problems, hypertension,” “gastrointestinal problems”) and mental health complaints (2 items, “symptoms of depression and anxiety,” “exhaustion”) within the past 4 weeks. The scale ranged from 1 = never to 5 = almost always. Cronbach's Alpha was α = 0.85.
5.2.5 Relaxation
We measured relaxation as an important recovery aspect using the subscale of the Recovery Experience Questionnaire by Sonnentag and Fritz (2007). We omitted one item due to parsimony. Participants were asked to rate their relaxation when working from home (3 items, “I kick back and relax,” “I do relaxing things,” and “I use the time to relax”). The scale ranged from 1 = never to 5 = almost always. Cronbach's Alpha was α = 0.91.
5.2.6 Work performance
We measured work performance by using a self-developed single item. Participants were asked to rate their overall work performance when working at home (“Based on the last 4 weeks, how would you rate your overall work performances in terms of effectiveness and productivity when working from home?”). The scale ranged from 1 = sufficient to 5 = excellent.
5.2.7 Control variables
As some populations might have more strain and health complaints when working from home, we controlled for age and gender. For example, Matthews et al. (2022) showed that working from home was associated with increased odds of psychological distress in women. Oakman et al. (2023) revealed that telework was associated with increasing stress levels in older participants.
To analyze direct effects and indirect moderating effects on outcomes, and to reduce the risk for common method bias (Podsakoff et al., 2013), SelfCare both at home and on-site and telework intensity were used at t1 and outcomes 3 months later at t2.
5.3 Data analyses
We conducted a CFA to test our measurement model. We compared the fit of a differentiated 5-factor model with competing 4-, two 3-, and a single factor model. The hypothesized 5-factor model showed a better fit [χ2 = 1,528.97(349), p < 0.001; CFI = 0.900; RMSEA = 0.075] than the 4-factor model that did not differentiate between SelfCare at home and SelfCare on-site. The 5-factor model includes (1) SelfCare at home (higher order factor) separating awareness and behavior facets, (2) SelfCare on-site (higher order factor) separating awareness and behavior facets, (3) health complaints, (4) strain, and (5) relaxation. The improvement in the model fit was significant [Δχ2 = 20(4); p < 0.001], supporting the differentiation between five factors. The 3-factor model which also combined irritation and complaints revealed a lower fit. In contrast, the single factor model showed the lowest fit [χ2 = 4,782.99(363), p < 0.001; CFI = 0.625; RMSEA = 0.143].
To test whether SelfCare differs among employees who both work from home and on-site (H1a), we conducted a paired sample t-test (within-person-effects: SelfCare on-site vs. SelfCare at home, both assessed by employees working at both work locations). To analyze whether SelfCare differs between employees who fully work from home and employees who work completely on-site (H1b), we conducted a t-test for independent samples (between-person-effects: SelfCare on-site [employees working fully on-site] vs. SelfCare at home [employees working fully at home]). We analyzed these effects both at t1 and t2.
To test H2, H3, and H4, we conducted moderated linear regression analyses (model 1) using the SPSS macro PROCESS. Regarding H2, SelfCare at home and telework intensity were modeled as IVs predicting health (i.e., strain [H1a], health complaints [H1b], relaxation at home [H1c]) and work performance at home at t2 (H1d, DVs). Telework intensity at t1 was modeled as the moderating variable modifying the relationship between SelfCare at home at t1 (IV) and the health and performance outcomes at t2 (DVs). Before computing the product of telework intensity and SelfCare at home, both variables were mean-centered. Regarding H3 and H4, SelfCare at home and SelfCare on-site were modeled as IVs predicting health outcomes (i.e., strain [H3a] and health complaints [H3b]; DVs). Additionally, SelfCare on-site t1 was modeled as the moderating variable modifying the relationship between SelfCare at home at t1 (IV) and health outcomes at t2 (DVs) to test H4a and H4b. Before computing the product of SelfCare at home and SelfCare on-site, both variables were mean-centered. H3 and H4 were only tested with the two general health outcomes strain and health complaints. To account for individual differences in the outcomes, we controlled for age in years and gender. For the analyses, only complete datasets were considered. An overview of the study hypotheses can be found in Figure 1.
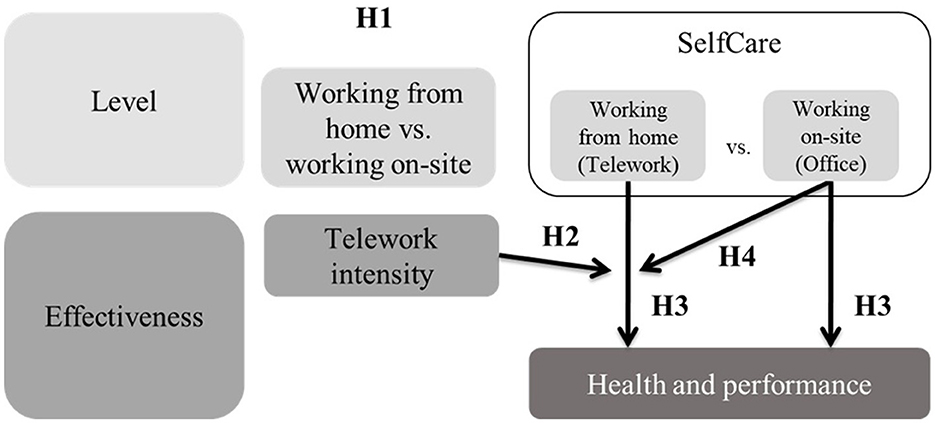
Figure 1. Overview of hypotheses.
6 Results
6.1 Differences in SelfCare regarding work location (between- and within-person-effects)
In H1 we expected that SelfCare is higher when working from home than when working on-site. Regarding within-person-effects (SelfCare on-site vs. SelfCare at home, both assessed by employees working at both work locations), the paired sample t-test revealed a significant difference: When assessing SelfCare at both work locations, SelfCare at home (M = 3.47, SD = 0.57) is higher than SelfCare on-site (M = 3.37, SD = 0.58; t(853) = 8.82, p < 0.001, Cohen's d = 0.34), confirming H1a. Regarding between-person-effects (SelfCare on-site vs. SelfCare at home), the t-test for independent samples also showed a significant difference, with higher values in SelfCare for employees when working fully at home (M = 3.59, SD = 0.62) compared to employees working fully on-site (M = 3.37, SD = 0.63; t(376) = 3.34, p < 0.001; Cohen's d = 0.62), supporting H1b. Similar results were found when analyzing SelfCare 3 months later (within-person-effects: t(660) = 6.15, p < 0.001; between-person-effects: t(304) = 2.30, p < 0.01). We additionally tested the difference between SelfCare on-site assessed by persons working fully or partly from home and persons solely working on-site. We found no differences (t(1, 056) = −0.032, p = 0.975).
We additionally tested the differences in the sub-facets of SelfCare Awareness and Behavior separately. There were both significant between- and within-person differences for Behavior: Regarding within-person-effects, employees report higher SelfCare Behavior when working from home (M = 3.40, SD = 0.62) compared to working on-site (M = 3.26, SD = 0.62; t(853) = 9.38, p < 0.001). Regarding between-person-effects, employees who fully work from home showed higher SelfCare Behavior (M = 3.53, SD = 0.66) compared to employees who fully work on-site (M = 3.24, SD = 0.68; t(376) = 4.20, p < 0.001). For Awareness, there was a within-person difference showing that employees reported higher levels of Awareness when working at home (M = 3.61, SD = 0.68) than when working on-site (M = 3.57, SD = 0.70; t(853) = 3.08, p < 0.01), but no significant difference between employees who working fully on-site (M = 3.61, SD = 0.71) and employees working fully at home (M = 3.69, SD = 0.75; t(376) = 1.08, p = 0.283). Similar results were found at t2.
6.2 Effectiveness of SelfCare on health and performance
Regarding the main effects of SelfCare, all regression models showed that SelfCare at home negatively predicted strain and health complaints and positively predicted relaxation and work performance at home. All regression coefficients for the main and interaction effects, standard errors, 95% confidence intervals, and model summaries for all health and performance indicators are presented in Table 1.
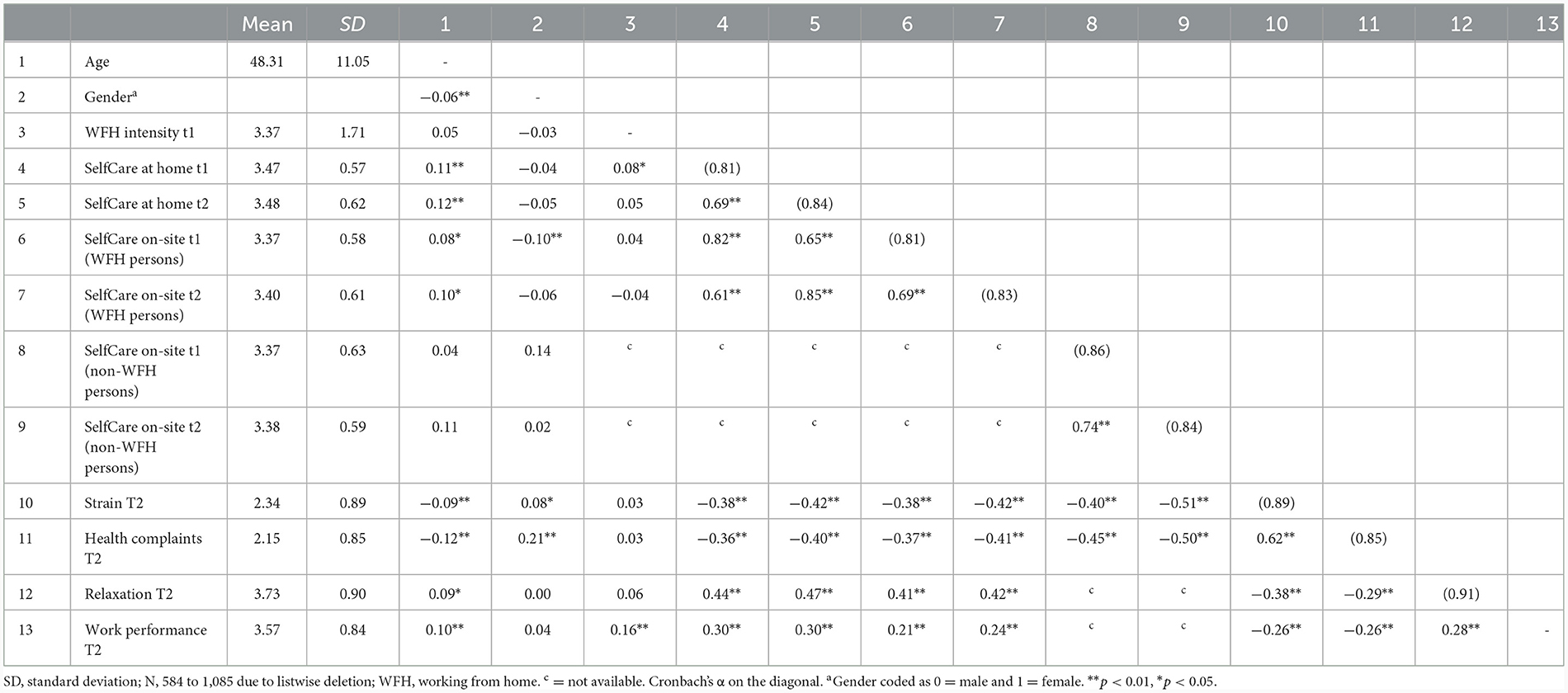
Table 1. Descriptives and correlations of variables for both studies.
6.2.1 Moderating effects of telework intensity
In H2, we postulated that the association between SelfCare at home and strain (H2a), health complaints (H2b), relaxation (H2c), and job performance (H2d) is higher for employees working more days from home. Regarding H2a, the overall moderation model accounted for significant variance in strain (R2 = 0.17). As predicted, the interaction term revealed that telework intensity interacted with SelfCare at home [B = −0.10, SE = 0.04, t = −2.51, p < 0.05, 95 % CI (−0.18, −0.02), ΔR2 = 0.01, F(1, 591) = 6.31, p < 0.05]. The conditional effect was coeff. = −0.43 (SE = 0.08, t = −5.11, p < 0.001, 95 % CI [−0.59, −0.26]) for low telework intensity and coeff. = −0.72 (SE = 0.08, t = −8.85, p < 0.001, 95 % CI [−0.88, −0.56]) for high telework intensity. The negative relationship between SelfCare at home and strain was stronger for higher telework intensity (Figure 2). H2a was supported.
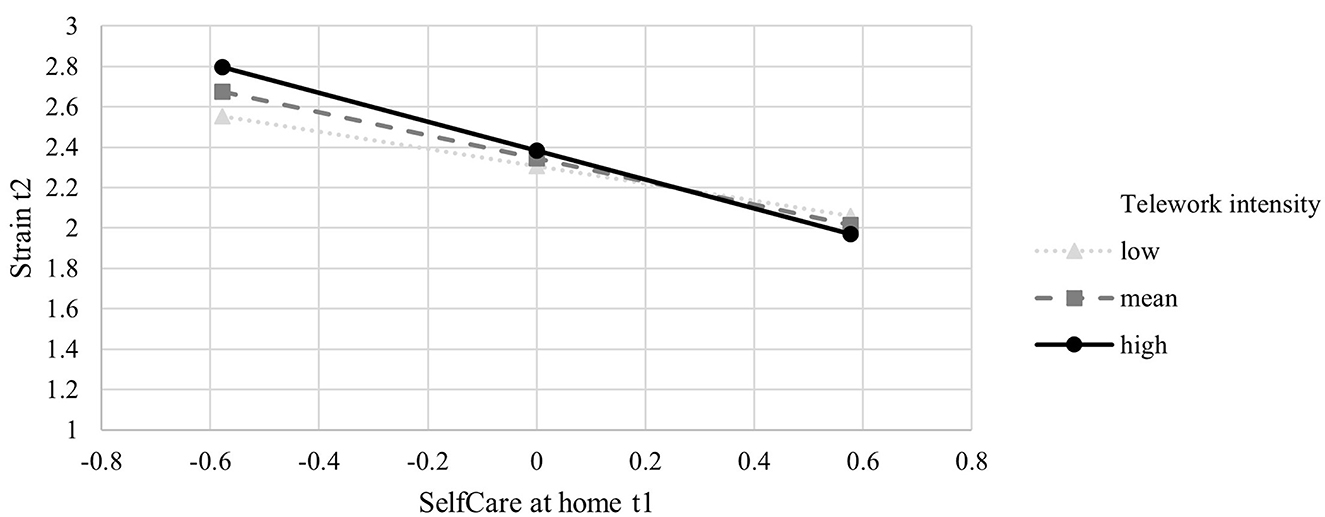
Figure 2. Moderation effect of telework intensity −1SD, M, and 1SD on the association between SelfCare at home and Strain (Simple Slopes).
Regarding H2b, the overall moderation model accounted for significant variance in health complaints (R2 = 0.20). As predicted, the interaction term revealed that telework intensity interacted with SelfCare at home [B = −0.09, SE = 0.04, t = −2.52, p < 0.05, 95 % CI (−0.17, −0.02), ΔR2 = 0.01, F(1, 591) = 6.34, p < 0.05]. The conditional effect was coeff. = −0.36 (SE = 0.08, t = −4.74, p < 0.001, 95 % CI [−0.51, −0.21]) for low telework intensity and coeff. = −0.63 (SE = 0.07, t = −8.48, p < 0.001, 95 % CI [−0.78, −0.48]) for high telework intensity. The negative relationship between SelfCare at home and health complaints was stronger for higher telework intensity (Figure 3). H2b was supported.
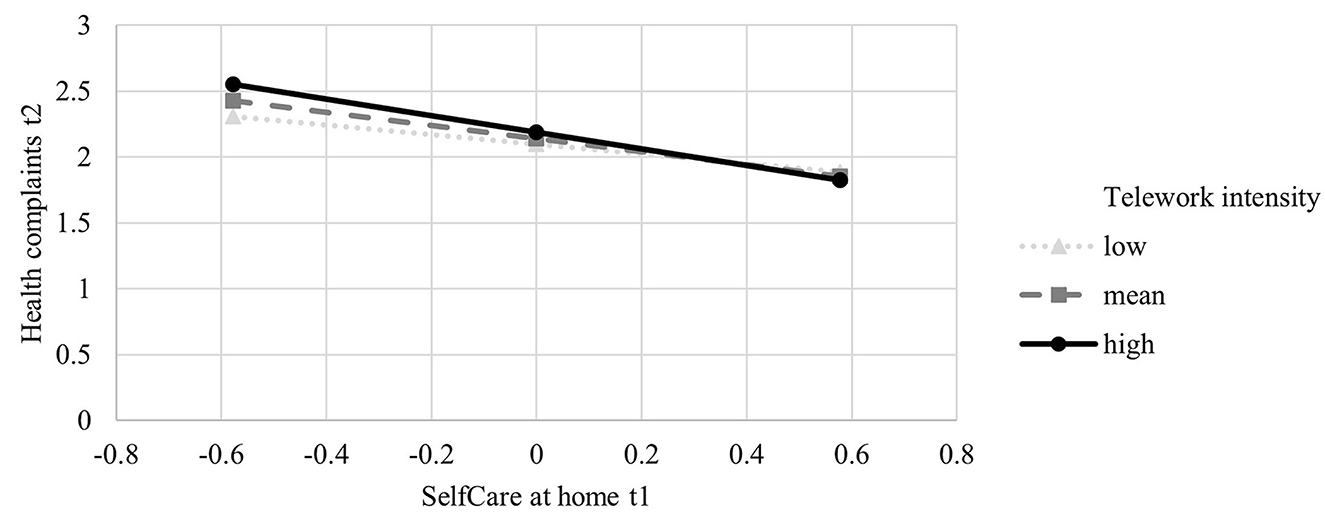
Figure 3. Moderation effect of telework intensity −1SD, M, and 1SD on the association between SelfCare at home and Health complaints (Simple Slopes).
Additionally, there was a main effect of SelfCare at home [B = −0.09, SE = 0.04, t = −2.52, p < 0.05, 95 % CI (−0.17, −0.02), ΔR2 = 0.01, F(1, 591) = 6.34, p < 0.05], but not for telework intensity [B = −0.09, SE = 0.04, t = −2.52, p < 0.05, 95 % CI (−0.17, −0.02), ΔR2 = 0.01, F(1, 591) = 6.34, p < 0.05].
Regarding H2c, the overall moderation model accounted for significant variance in relaxation (R2 = 0.21). As predicted, the interaction term revealed that telework intensity interacted with SelfCare at home [B = 0.13, SE = 0.04, t = 3.49, p < 0.001, 95 % CI (0.06, 0.21), ΔR2 = 0.02, F(1, 576) = 12.20, p < 0.001]. The conditional effect was coeff. = 0.44 (SE = 0.08, t = 5.54, p < 0.001, 95 % CI [0.29, 0.60]) for low telework intensity and coeff. = 0.82 (SE = 0.08, t = 10.73, p < 0.001, 95 % CI [0.67, 0.98]) for high telework intensity. The positive relationship between SelfCare at home and relaxation at home was stronger for higher telework intensity (Figure 4). H2c was supported.
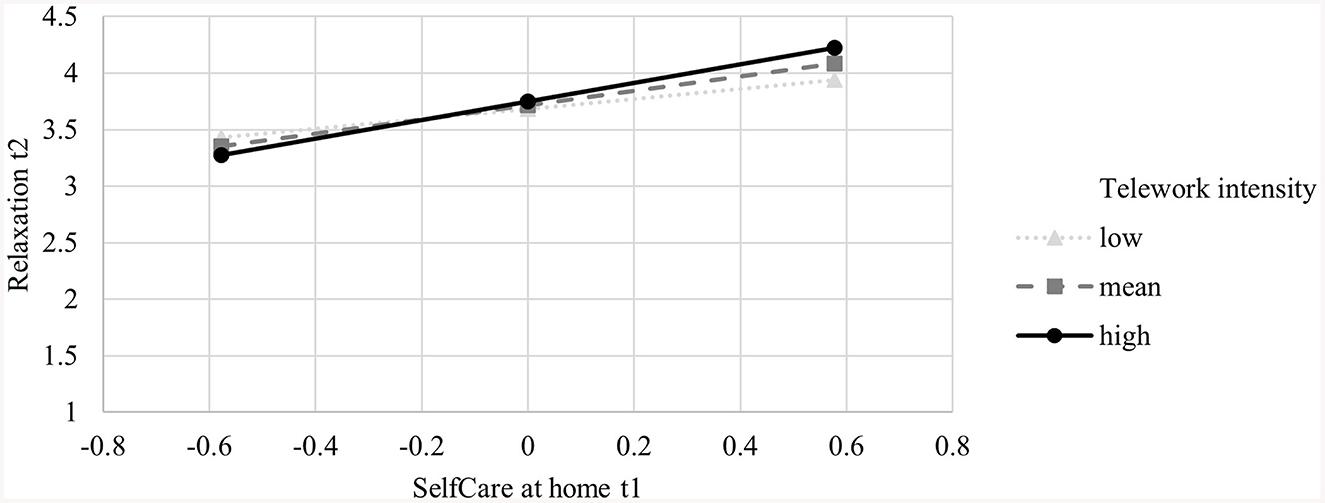
Figure 4. Moderation effect of telework intensity −1SD, M, and 1SD on the association between SelfCare at home and Relaxation (Simple Slopes).
Regarding H2d, the overall moderation model accounted for significant variance in job performance (R2 = 0.13). Contrary to our assumption, telework intensity did not interact with SelfCare at home [B = 0.07, SE = 0.04, t = 1.66, p = 0.09, 95 % CI (−0.01, 0.15), ΔR2 = 0.004, F(1, 549) = 2.76, p = 0.097]. H2d was thus not supported. The interaction term missed the significance level of 0.05, but interaction effect and conditional direct effects are in the expected direction. The conditional effect was coeff. = 0.32 (SE = 0.08, t = 3.76, p < 0.001, 95 % CI [0.15, 0.48]) for low telework intensity and coeff. = 0.51 (SE = 0.08, t = 6.29, p < 0.001, 95 % CI [0.35, 0.66]) for high telework intensity. Despite missing significance, the relationship between SelfCare at home and work performance at home was stronger for higher telework intensity (Figure 5). As can be seen in Table 2, telework intensity did not exert an influence on the relationship between SelfCare at home and work performance but showed a direct effect on work performance (B = 0.10, SE = 0.02, t = 4.11, p < 0.001, 95 % CI [0.05, 0.15]). Telework intensity did not show direct associations with the health indicators.
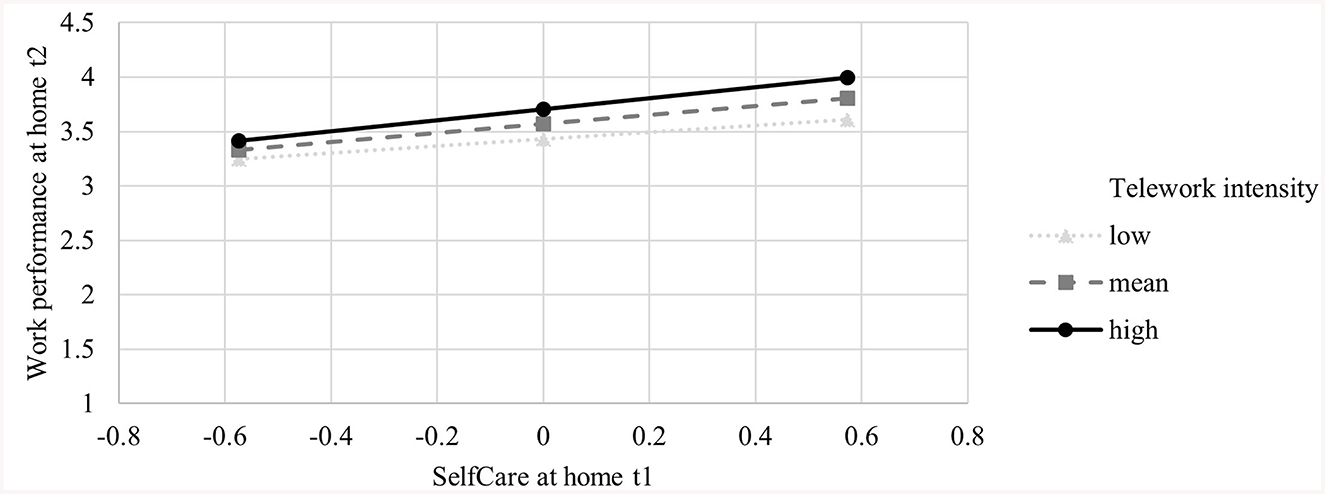
Figure 5. Moderation effect of SelfCare at the office −1SD, M, and 1SD on the association between SelfCare at home and Work performance (Simple Slopes).
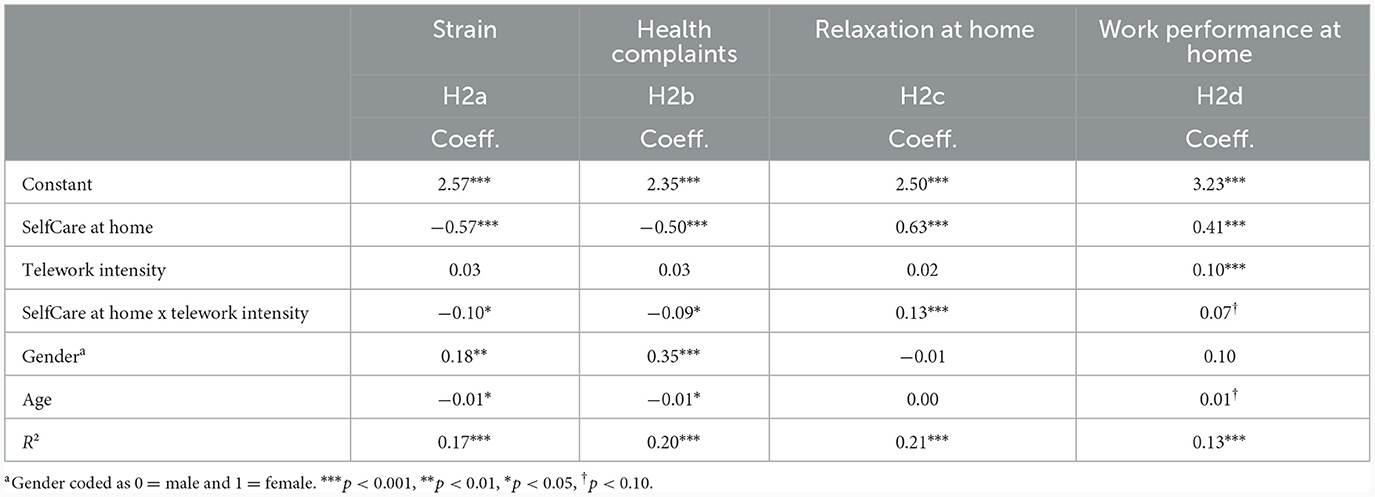
Table 2. Results of the moderated regression analyses (H2).
6.2.2 Direct and moderating effects of SelfCare on-site
In H3, we postulated that SelfCare at home and SelfCare on-site independently predict strain (H3a) and health complaints (H3b). Moreover, we expected that SelfCare at both work locations amplify each other. Employees displaying SelfCare both on-site and at home are supposed to experience less strain (H4a) and fewer health complaints (H4b).
Regarding H3a and H4a, the overall moderation model accounted for significant variance in strain (R2 = 0.18). As expected, SelfCare at home and SelfCare on-site both show significant main effects and independently predict strain (at home: B = −0.30, SE = 0.11, t = −2.66, p < 0.01, 95 % CI [−0.52, −0.08]); on-site: (B = −0.29, SE = 0.11, t = −2.59, p < 0.01, 95 % CI [−0.52, −0.07]). Employees with high levels of SelfCare at home report less strain and employees with high levels of SelfCare on-site report less strain. Additionally, the interaction term revealed that SelfCare at both work locations interacted [B = −0.15, SE = 0.08, t = −2.02, p < 0.05, 95 % CI (−0.30, −0.01), ΔR2 = 0.01, F(1, 591) = 4.08, p < 0.05]. The conditional effect was significant for high SelfCare on-site (coeff. = −0.39, SE = 0.12, t = −3.16, p < 0.01, 95 % CI [−0.863, −0.15]), but not for low SelfCare on-site (coeff. = −0.21, SE = 0.12, t = −1.77, p = 0.08, 95 % CI [−0.45, 0.23]). The negative relationship between SelfCare at home and strain was stronger for higher SelfCare on-site (Figure 6). H3a and H4a were supported.
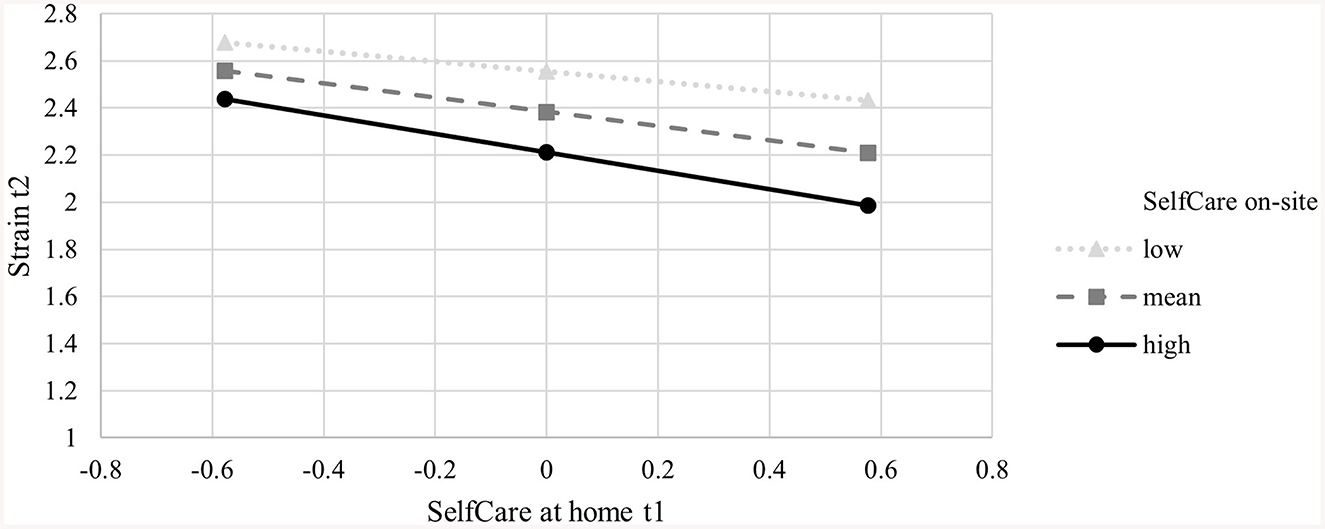
Figure 6. Moderation effect of SelfCare at the office −1SD, M, and 1SD on the association between SelfCare at home and Strain (Simple Slopes).
Regarding H3b and H4b, the overall moderation model accounted for significant variance in health complaints (R2 = 0.20). As expected, SelfCare at home and SelfCare on-site both show significant main effects and independently predict health complaints (at home: B = −0.24, SE = 0.10, t = −2.33, p < 0.05, 95 % CI [−0.45, −0.04]); on-site: B = −0.29, SE = 0.11, t = −2.76, p < 0.01, 95 % CI [−0.49, −0.08]). SelfCare at home and SelfCare on-site are each negatively associated with fewer complaints. The interaction term revealed no interaction effect [B = −0.04, SE = 0.07, t = −0.60, p = 0.55, 95% CI (−0.18, 0.09), ΔR2 =0.00, F(1, 591) = 0.36, p = 0.55]. SelfCare on-site did not amplify the association between SelfCare at home and health complaints. H3b was thus supported, but not H4b. All regression coefficients for the main and interaction effects, standard errors, 95% confidence intervals, and model summaries are presented in Table 3.
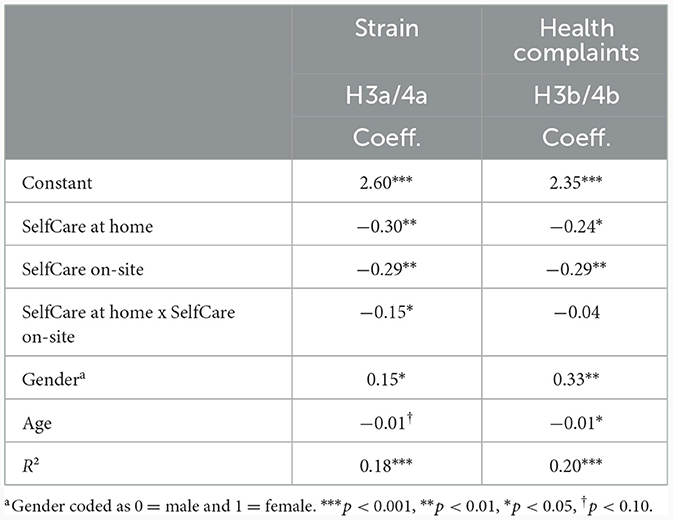
Table 3. Results of the moderated regression analyses (H3 and H4).
7 Discussion
This study aimed to understand the differential relationships between SelfCare and health and performance outcomes when considering the hybrid work environment as a contextual factor. The results of the study show that SelfCare at home is more pronounced than on-site both, for within-person and between-person comparisons of the SelfCare level. Looking at the sub-facets of SelfCare separately, we found clear within- and between-person differences for SelfCare Behavior. For Awareness there were also clear within-person differences, but no differences between employees with and without telework. Employees without teleworking may have overestimated their SelfCare because they had no direct comparison. A direct comparison of the two experiences could make the assessment more realistic. One detail we would like to highlight here is that the level of SelfCare on-site for employees working entirely on-site did not differ from the SelfCare on-site for employees in hybrid work arrangements. Thus, we can conclude that the differences in levels of SelfCare are not an artifact of people who are more competent choosing to work more from home but that it is much more likely that the home as a work environment allows for more SelfCare than the office environment.
Furthermore, the results support the assumption that the relationship between SelfCare and employee outcomes is stronger when working from home. This could be supported for strain, health complaints, and relaxation. Answering the call by Beckel and Fisher (2022) to clarify the role of high-intensity telework for employee health and wellbeing, we found telework intensity as one relevant moderator in the relationship between SelfCare and employee outcomes. These results allow the conclusion that SelfCare is especially important in reducing mental and physical health problems when working from home. Although the data did not support this assumption for performance as an outcome, the main effect showed that the higher the telework intensity, the higher employees' self-rated performance is. This shows that the widespread assumption among practitioners that employees slack off or are lazy when working from home does not apply. On the contrary: they report higher performance with higher telework intensity.
Testing both, SelfCare when working from home and on-site as parallel predictors of strain and health complaints as outcomes revealed that they independently predict the outcomes. Moreover, concerning strain as the outcome, the data supported the interaction between SelfCare when working from home and on-site (but not for health complaints). On the one hand, this indicates that high SelfCare when working on-site can boost the positive effects of SelfCare when working from home. On the other hand, these results show that low SelfCare when on-site impairs the effects of SelfCare when working from home as this relationship is not significant anymore under the condition of low on-site SelfCare. Thus, we enlarge the earlier findings by Klug et al. (2019) and show that consistency in SelfCare across work locations is important for the beneficial effects on employee strain.
7.1 Theoretical implications
First, against the background of hybrid work as the “new normal” (Franken et al., 2021) this study is the first to show that it is important to assess SelfCare specific to the working location. The present study underlines the notion that SelfCare also represents an important workplace resource for employees in digital and hybrid working contexts. As we found significant within-person differences in the level of SelfCare when working from home compared to on-site, we can conclude that there is not one general competency of SelfCare but that employees adapt their SelfCare according to the context they are working in.
Second, as previous research had focused on boundary conditions of the effectiveness of StaffCare on health outcomes, our results confirmed the intensity of telework as the first boundary condition for the relationship between SelfCare and outcomes and, therefore, extended previous research. It is a new insight that SelfCare still unfolds its positive effects when working from home, even more for employees who work more days from home. By showing the positive effects of SelfCare in the digital and hybrid work context for the first time, this study extends the existing validity of the HoL concept and adds to our knowledge on hindering and facilitating working conditions for the effects of SelfCare. To better understand how and why the effectiveness of SelfCare is amplified in digital and hybrid working environments, further theory development should take a differentiated view on potential underlying mechanisms and individual factors that facilitate or hinder SelfCare. For example, Neidlinger et al. (2022) showed that leaders with lower core self-evaluation benefit more in terms of health and work-life-balance when working from home. Other individual factors might be self-regulation or segmentation preferences.
Third, we provide a first answer to the question of whether SelfCare across working locations should be consistent or if inconsistency between different working locations is not problematic. Until now, most research has ignored different working locations. The results of the moderation analysis in this study reveal that consistency is important with regard to employee strain, as the negative relationship of SelfCare when working from home was stronger when SelfCare on-site was also high. More importantly, when SelfCare on-site was low, the negative relationship between SelfCare and strain was not significant anymore. This result supports the notion that few opportunities for SelfCare in the office can undermine the otherwise positive effects of SelfCare at home. Thus, consistency in SelfCare across working locations is an important aspect to consider.
Although we have only measured SelfCare as a specific form of self-leadership in this study, it can be assumed that also other strategies of self-leadership vary when comparing on-site work with work from home.
7.2 Practical implications
Our results show that SelfCare is slightly higher when working from home compared to working on-site. Means show that SelfCare levels are only medium. This highlights the importance of recognizing that both employees and organizations need to develop SelfCare skills to effectively maintain and promote their health in a remote work environment. However, while our study does not explicitly discuss whether remote work might threaten traditional leadership behaviors, it underscores the need for a more effective integration and implementation of SelfCare into daily work routines. Thus, organizations should implement interventions to promote SelfCare in both work contexts. Organizations and practitioners should develop interventions to effectively foster SelfCare, e.g., GoFüKo—a training to develop SelfCare and StaffCare competences (Krick and Felfe, 2024). This intervention familiarizes employees with the HoL concept and provides concrete exercises on how to develop SelfCare. Other studies showed that a mindfulness-based resource intervention especially developed for the work context was effective in increasing SelfCare (Krick and Felfe, 2020, 2023). Another study showed that employees high in SelfCare benefitted more from such interventions (Krick et al., 2021). In addition, intervention concepts and tools are needed that specifically address SelfCare in digital and hybrid contexts and focus on specific barriers and challenges that make SelfCare difficult when working from home. Recently, an online learning platform for leaders (DigiLAP; Digital Leadership Assistance Platform) was developed, specifically addressing SelfCare in the context of remote work and hybrid work (Krick et al., 2023). Future research is needed to further identify effective interventions to promote SelfCare, increasing both, SelfCare at home and on-site.
7.3 Limitations and directions for future research
Although this study makes valuable contributions to both theory and practice, it is important to acknowledge its limitations, which can provide valuable insights for future research. First, our data is primarily reliant on self-report measures, which potentially increases the possibility of response biases, same-source biases, and common method biases. These biases may have resulted in overestimating the correlations between study variables and underestimating interactions (Podsakoff et al., 2003). There are also multiple Monte Carlo studies (Evans, 1985; Lai et al., 2013) and statistical proof by Siemsen et al. (2010) indicating that an interaction effect cannot be produced by common method variance. However, we minimized these biases to some extent by utilizing diverse response options across the scales and ensuring confidentiality, thereby reducing the likelihood of habitual responding and response biases. To further minimize the potential common method bias, we employed longitudinal data and collected data on predictors and DVs at different time points. Despite this limitation, we believe that self-report measures were appropriate for our study objectives. Many of our variables focus on individual experiences that are challenging to assess without directly asking participants to describe and report their own experiences. However, future research should complement and validate self-reported data by incorporating more objective measures, particularly for health. Replicating our findings using alternative data sources and perspectives, such as leader-rated performance or objective physiological health measures like heart rate variability, cortisol, and blood pressure for assessing health indicators, would be beneficial.
Second, in this study, we chose a 3-month time interval to separate predictors and outcomes. Future studies could aim to establish knowledge on temporal dynamics in SelfCare. Therefore, it is recommended that future studies examine our model and other potentially relevant variables in shortitudinal field studies, such as a diary study. For example, a dairy study could investigate the interaction effect of SelfCare at home and on-site throughout the week to better understand interaction effects on a daily or weekly level. This would also allow for identifying optimal conditions for effective and sustainable SelfCare in hybrid work settings. The present study can serve as a starting point for further investigations in this area.
Third, it is an open question if SelfCare might also have a dark side. On the one hand, interdependence theory (Rusbult and van Lange, 2003) would suggest that, especially in jobs with high task interdependence, some aspects of SelfCare behavior can include the risk of being costly to coworkers. SelfCare behaviors such as taking part in stress management courses, prioritizing tasks, or asking for support from coworkers could enhance the workload of colleagues while relieving the burden of the person showing high SelfCare behaviors. On the other hand, based on social learning theory (Bandura, 1969) and the assumptions in the HoL model itself (Franke et al., 2014), one can expect that high SelfCare of individuals will be picked up by coworkers and thus might even contribute to an overall more positive health climate within a team. The findings by Gosch et al. (2023) support this notion, as the authors found a positive correlation between SelfCare and PeerCare. Further empirical evidence is necessary to test these competing assumptions in future studies to make sure that SelfCare does not comprise a dark side.
Fourth, with regard to the between-person comparisons, employees working fully from home at the time of the survey did not have a direct comparison when currently working on-site, but rather a comparison with their previous work on-site. The analyses were also conducted without employees who worked fully from home. The results were similar.
Fifth, although we could show a clear difference between SelfCare at home and SelfCare on-site, we can only speculate about the reasons. The literature emphasizes autonomy and flexibility (Moretti et al., 2020; Ervasti et al., 2022; Felfe et al., 2022), but other factors also may play a role. For example, flexibility might be a double-edged sword, as the perceived flexibility might depend on the hierarchy level/job position (e.g., perhaps only employees at lower job/hierarchy levels enjoy more flexibility at home, i.e., in the absence of close supervision from one's superior) or the job design (e.g., employees with tasks that highly depend on others might experience limited flexibility). To better understand the reasons why SelfCare is higher at home than on-site, these factors should be investigated in future studies (e.g., job level, experienced control by leaders, etc.). Furthermore, it would be interesting for future research to examine motivational aspects for SelfCare on-site and SelfCare at home to better understand the reasons why individuals engage in SelfCare behavior at the office and at home.
8 Conclusion
This study aimed to deepen our understanding of SelfCare in remote and on-site working contexts. The core finding underscores the significance of SelfCare practices, revealing that individuals exhibit higher levels of SelfCare when working from home compared to working on-site. Moreover, an intriguing result emerged as SelfCare at home demonstrated stronger associations with various outcomes the more employees work from home. Thereby, this study sheds light on the pivotal role of SelfCare in the context of teleworking, emphasizing its positive impact on individual wellbeing and performance. However, the study also highlights the importance of maintaining a consistent commitment to SelfCare across different working environments. As we navigate an era marked by increased flexibility in work arrangements, it becomes imperative for future studies to delve deeper into the frequency with which work is conducted outside traditional on-site settings. Understanding the dynamics of SelfCare in these varied contexts will provide invaluable insights for both researchers and practitioners aiming to promote employee health and productivity. In practical terms, the implications of our findings suggest that trainings on SelfCare should not only emphasize its importance but also integrate actionable strategies into the daily work routines of individuals.
Data availability statement
The datasets presented in this article are not readily available because of privacy restrictions. Requests to access the datasets should be directed to JF, ZmVsZmVAaHN1LWhoLmRl.
Ethics statement
Ethical approval was not required for the study involving humans because participation was completely voluntary and anonymous. Answering our questions did not cause any harm and was neither mentally nor psychologically stressful. The questionnaire did not contain any distressing material. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AK: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Project administration. MA: Writing – original draft, Writing – review & editing. JF: Conceptualization, Methodology, Supervision, Writing – review & editing, Project administration.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research [project Digital Leadership and Health] was funded by dtec.bw—Digitalization and Technology Research Center of the Bundeswehr. dtec.bw was funded by the European Union—NextGenerationEU. This publication has been funded by the Open-Access-Publication-Fund of the Helmut-Schmidt-University/University of the Federal Armed Forces Hamburg.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Amano, H., Fukuda, Y., Shibuya, K., Ozaki, A., and Tabuchi, T. (2021). Factors associated with the work engagement of employees working from home during the COVID-19 pandemic in Japan. Int. J. Environ. Res. Public Health. 18:10495. doi: 10.3390/ijerph181910495
Arnold, M., and Rigotti, T. (2023). How's the boss? Integration of the health-oriented leadership concept into the job demands-resources theory. J. Manager. Psychol. 38, 419–433. doi: 10.1108/JMP-01-2023-0030
Bandura, A. (1969). “Social-learning theory of identificatory processes,” in Handbook of Socialization Theory and Research, ed. D. A. Goslin (Chicago, IL: Rand McNally and Company), 213–262.
Beckel, J. L. O., and Fisher, G. G. (2022). Telework and worker health and well-being: a review and recommendations for research and practice. Int. J. Environ. Res. Public Health 19:3879. doi: 10.3390/ijerph19073879
Bonin, H., Eichhorst, W., Kaczynska, J., Kümmerling, A., Rinne, U., Scholten, A., et al. (2020). Kurzexpertise: Verbreitung und Auswirkungen von Mobiler Arbeit und Homeoffice. Berlin: Federal Ministry of Labor and Social Affairs.
Borle, P., Boerner-Zobel, F., Voelter-Mahlknecht, S., Hasselhorn, H. M., and Ebener, M. (2021). The social and health implications of digital work intensification. Associations between exposure to information and communication technologies, health and work ability in different socio-economic strata. Int. Arch. Occupat. Environ. Health 94, 377–390. doi: 10.1007/s00420-020-01588-5
Bouziri, H., Smith, D. R. M., Descatha, A., Dab, W., and Jean, K. (2020). Working from home in the time of COVID-19: how to best preserve occupational health? Occupat. Environ. Med. 77, 509–510. doi: 10.1136/oemed-2020-106599
Caniëls, M. C. J. (2023). How remote working increases the importance of positive leadership for employee vigor. Front. Psychol. 14:1089557. doi: 10.3389/fpsyg.2023.1089557
Cropley, M., Weidenstedt, L., Leick, B., and Sütterlin, S. (2023). Working from home during lockdown: the association between rest breaks and well-being. Ergonomics 66, 443–453. doi: 10.1080/00140139.2022.2095038
Day, A., Paquet, S., Scott, N., and Hambley, L. A. (2012). Perceived information and communication technology (ICT) demands on employee outcomes: the moderating effect of organizational ICT support. J. Occup. Health Psychol. 17, 473–491. doi: 10.1037/a0029837
De Vincenzi, C., Pansini, M., Ferrara, B., Buonomo, I., and Benevene, P. (2022). Consequences of COVID-19 on employees in remote working: challenges, risks and opportunities an evidence-based literature review. Int. J Environ. Res. Public Health. 19:11672. doi: 10.3390/ijerph191811672
Diewald, M. (2020). “Zukunftsperspektiven von Homeoffice nach Corona,” in Sonderband Zukunft der Arbeit, HR Consulting Review, eds. J. Nachtwei, and A. Sureth (VQP), 30–33.
Dormann, C., and Griffin, M. A. (2015). Optimal time lags in panel studies. Psychol. Method. 20, 489–505. doi: 10.1037/met0000041
Efimov, I., Harth, V., and Mache, S. (2020). Health-oriented self- and employee leadership in virtual teams: a qualitative study with virtual leaders. Int. J. Environ. Res. Public Health 17:6519. doi: 10.3390/ijerph17186519
Ervasti, J., Aalto, V., Pentti, J., Oksanen, T., Kivimäki, M., and Vahtera, J. (2022). Association of changes in work due to COVID-19 pandemic with psychosocial work environment and employee health: a cohort study of 24 299 Finnish public sector employees. Occupat. Environ. Med. 79, 233–241. doi: 10.1136/oemed-2021-107745
Eurofound (2020). Living, working and COVID-19, COVID-19 series. Luxembourg: Publications Office of the European Union.
Evans, M. G. (1985). A Monte Carlo study of the effects of correlated method variance in moderated multiple regression analysis. Organiz. Behav. Hum. Decis. Proc. 36, 305–323. doi: 10.1016/0749-5978(85)90002-0
Felfe, J., Krick, A., Hauff, S., Renner, K.-H., Klebe, L., Schübbe, K., et al. (2022). “Working from home: Opportunities and risks for working conditions, leadership and health,” in dtec.bw-Beiträge der Helmut-Schmidt-Universität, Universität der Bundeswehr Hamburg – Forschungsaktivitäten im Zentrum für Digitalisierungs- und Technologieforschung der Bundeswehr dtec.bw., eds. D. Schulz, A. Fay, M. Schulz et al. (Hamburg: Helmut-Schmidt-Universität, Universität der Bundeswehr), 335–341.
Ford, M. T., Matthews, R. A., Wooldridge, J. D., Mishra, V., Kakar, U. M., and Strahan, S. R. (2014). How do occupational stressor-strain effects vary with time? A review and meta-analysis of the relevance of time lags in longitudinal studies. Work Stress 28, 9–30. doi: 10.1080/02678373.2013.877096
Franke, F., Felfe, J., and Pundt, A. (2014). The impact of health-oriented leadership on follower health: Development and test of a new instrument measuring health-promoting leadership. Zeitschrift Personalforschung 28, 139–161. doi: 10.1177/239700221402800108
Franken, E., Bentley, T., Shafaei, A., Farr-Wharton, B., Onnis, L. A., and Omari, M. (2021). Forced flexibility and remote working: opportunities and challenges in the new normal. J. Manage. Organ. 27, 1131–1149. doi: 10.1017/jmo.2021.40
Gajendran, R. S., and Harrison, D. A. (2007). The good, the bad, and the unknown about telecommuting: meta-analysis of psychological mediators and individual consequences. J. Appl. Psychol. 92, 1524–1541. doi: 10.1037/0021-9010.92.6.1524
Golden, T. D., and Veiga, J. F. (2008). The impact of superior–subordinate relationships on the commitment, job satisfaction, and performance of virtual workers. Leadership Quart. 19, 77–88. doi: 10.1016/j.leaqua.2007.12.009
Göpner-Reinecke, C. (2019). Arbeiten im Homeoffice-Höhere Arbeitszufriedenheit, aber Stärkere Psychische Belastung. Berlin, Germany, London, England: Wissenschaftliches Institut der AOK (WIdO) und AOK-Bundesverband Pressemitteilung zum Fehlzeiten-Report 2019. Wissenschaftliches Institut der AOK (WIdO), AOK-Bundesverband.
Gosch, N., Schulte, E.-M., and Kauffeld, S. (2023). Capturing the impact employees have on their coworkers and leaders: a holistic approach on health-specific support behavior from employees. Front. Psychol. 14:1183862. doi: 10.3389/fpsyg.2023.1183862
Grimm, L. A., Bauer, G. F., and Jenny, G. J. (2021). Is the health-awareness of leaders related to the working conditions, engagement, and exhaustion in their teams? A multi-level mediation study. BMC Public Health 21:1935. doi: 10.1186/s12889-021-11985-1
Ho, J., and Nesbit, P. L. (2014). Self-leadership in a Chinese context: work outcomes and the moderating role of job autonomy. J. Manager. Psychol. 17, 672–691. doi: 10.1177/1059601114539389
Hunter, J. R., Meiring, R. M., Cripps, A., Suppiah, H. T., Vicendese, D., Kingsley, M. I., et al. (2021). Relationships between physical activity, work ability, absenteeism and presenteeism in Australian and New Zealand adults during COVID-19. Int. J. Environ. Res. Public Health 18:12563. doi: 10.3390/ijerph182312563
Kaluza, A. J., and Junker, N. M. (2022). Caring for yourself and for others: team health climate and self-care explain the relationship between health-oriented leadership and exhaustion. J. Manager. Psychol. 37, 655–668. doi: 10.1108/JMP-10-2021-0567
Kaluza, A. J., Weber, F., van Dick, R., and Junker, N. M. (2021). When and how health-oriented leadership relates to employee well-being: the role of expectations, self-care, and LMX. J. Appl. Soc. Psychol. 51, 404–424. doi: 10.1111/jasp.12744
Kauffeld, S., Handke, L., and Straube, J. (2016). Verteilt und doch verbunden: Virtuelle Teamarbeit. Gruppe. Interaktion. Organisation. Zeitschrift Angewandte Organisationspsychol. 47, 43–51. doi: 10.1007/s11612-016-0308-8
Klebe, L., Felfe, J., and Klug, K. (2021a). Healthy leadership in turbulent times: the effectiveness of health-oriented leadership in crisis. Br. J. Manage. 32, 1203–1218. doi: 10.1111/1467-8551.12498
Klebe, L., Felfe, J., Krick, A., and Pischel, S. (2023). The shadows of digitisation: on the losses of health-oriented leadership in the face of ICT hassles. Behav. Inf. Technol. 32, 1–18. doi: 10.1080/0144929X.2023.2183053
Klebe, L., Klug, K., and Felfe, J. (2021b). The show must go on: The effects of crisis on health-oriented leadership and follower exhaustion during Covid-19 pandemic. Zeitschrift Arbeits Organisationspsychol. 65, 231–243. doi: 10.1026/0932-4089/a000369
Klug, K., Felfe, J., and Krick, A. (2019). Caring for oneself or for others? How consistent and inconsistent profiles of health-oriented leadership are related to follower strain and health. Front. Psychol. 10:2456. doi: 10.3389/fpsyg.2019.02456
Klug, K., Felfe, J., and Krick, A. (2022). Does self-care make you a better leader? A multisource study linking leader self-care to health-oriented leadership, employee self-care, and health. Int. J. Environ. Res. Public Health 19:6733. doi: 10.3390/ijerph19116733
Kniffin, K. M., Narayanan, J., Anseel, F., Antonakis, J., Ashford, S. P., Bakker, A. B., et al. (2021). COVID-19 and the workplace: Implications, issues, and insights for future research and action. Am. Psychol. 76, 63–77. doi: 10.1037/amp0000716
Krick, A., and Felfe, J. (2020). Who benefits from mindfulness? The moderating role of personality and social norms for the effectiveness on psychological and physiological outcomes among police officers. J. Occupat. Health Psychol. 25, 99–112. doi: 10.1037/ocp0000159
Krick, A., and Felfe, J. (2022). “Health-oriented leadership in a digital world: a literature review,” in dtec.bw-Beiträge der Helmut-Schmidt-Universität, Universität der Bundeswehr Hamburg – Forschungsaktivitäten im Zentrum für Digitalisierungs- und Technologieforschung der Bundeswehr dtec.bw., eds. D. Schulz, A. Fay, M. Schulz et al. (Hamburg: Helmut-Schmidt-Universität, Universität der Bundeswehr), 347–357.
Krick, A., and Felfe, J. (2023). Comparing the effectiveness of Mindfulness-based Intervention and Progressive Muscle Relaxation in a military context. Mindfulness. doi: 10.1007/s12671-023-02281-7
Krick, A., and Felfe, J. (2024). Gesundheitsorientierte Führungskompetenz: Trainingsmanual. Berlin Heidelberg, Springer.
Krick, A., Felfe, J., Klebe, L., and Tautz, D. (2023). “Hybrides Führen: Führen in Zeiten von Homeoffice,” in Fehlzeiten-Report 2023, eds. B. Badura, A. Ducki, H. Schröder et al. (Berlin, Heidelberg: Springer), 271–286. doi: 10.1007/978-3-662-67514-4_17
Krick, A., Felfe, J., and Klug, K. (2021). Building resilience: Trajectories of heart rate variability during a mindfulness-based intervention and the role of individual and social characteristics. Int. J. Stress Manag. 28, 220–231. doi: 10.1037/str0000227
Kunze, F., and Hampel, K. (2023). Konstanzer Home-Office Studie. Available online at: https://www.hrblue.com/de/konstanzer-home-office-studie/ (accessed September 29, 2023).
Lai, X., Li, F., and Leung, K. (2013). A monte carlo study of the effects of common method variance on significance testing and parameter bias in hierarchical linear modeling. Organiz. Res. Method 16, 243–269. doi: 10.1177/1094428112469667
Lamprinou, V. D. I., Tasoulis, K., and Kravariti, F. (2021). The impact of servant leadership and perceived organisational and supervisor support on job burnout and work–life balance in the era of teleworking and COVID-19. Leader. Organiz. Dev. J. 42, 1071–1088. doi: 10.1108/LODJ-12-2020-0526
Lunau, T., Bambra, C., Eikemo, T. A., van der Wel, K. A., and Dragano, N. (2014). A balancing act? Work-life balance, health and well-being in European welfare states. Eur. J. Public Health 24, 422–427. doi: 10.1093/eurpub/cku010
Lundqvist, D., Reineholm, C., Ståhl, C., and Wallo, A. (2022). The impact of leadership on employee well-being: on-site compared to working from home. BMC Public Health 22:2154. doi: 10.1186/s12889-022-14612-9
Matthews, T. A., Chen, L., Omidakhsh, N., Zhang, D., Han, X., Chen, Z., et al. (2022). Gender difference in working from home and psychological distress - A national survey of U.S. employees during the COVID-19 pandemic. Ind. Health 60, 334–344. doi: 10.2486/indhealth.2022-0077
McDowell, C. P., Herring, M. P., Lansing, J., Brower, C., and Meyer, J. D. (2020). Working from home and job loss due to the COVID-19 pandemic are associated with greater time in sedentary behaviors. Front. Public Health 8:597619. doi: 10.3389/fpubh.2020.597619
Mckinsey, A. (2021). The future of work after COVID-19. Available online at: https://www.mckinsey.com/featured-insights/future-of-work/the-future-of-work-after-covid-19 (accessed December 14, 2023).
Mohr, G. (1986). The Assessment of Mental Health Impairments of Industrial Workers. Frankfurt, Lang.
Mohr, G., Rigotti, T., and Müller, A. (2005). Irritation - Ein Instrument zur Erfassung psychischer Beanspruchung im Arbeitskontext. Skalen- und Itemparameter aus 15 Studien. German J. Work Organiz. Psychol. 49, 44–48. doi: 10.1026/0932-4089.49.1.44
Moretti, A., Menna, F., Aulicino, M., Paoletta, M., Liguori, S., and Iolascon, G. (2020). Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 17:6284. doi: 10.3390/ijerph17176284
Müller, T., and Niessen, C. (2019). Self-leadership in the context of part-time teleworking. J. Organiz. Behav. 40, 883–898. doi: 10.1002/job.2371
Murphy, L. D., Cobb, H. R., Rudolph, C. W., and Zacher, H. (2023). Commuting demands and appraisals: a systematic review and meta-analysis of strain and wellbeing outcomes. Organiz. Psychol. Rev. 13, 11–43. doi: 10.1177/20413866221131404
Neidlinger, S. M., Felfe, J., and Schübbe, K. (2022). Should I Stay or Should I Go (to the Office)?-Effects of working from home, autonomy, and core self-evaluations on leader health and work-life balance. Int. J. Environ. Res. Public Health 20:6. doi: 10.3390/ijerph20010006
Nickson, D., and Siddons, S. (2004). Remote Working. Linking People and Organizations. Amsterdam, Boston: Elsevier.
Niebuhr, F., Borle, P., Börner-Zobel, F., and Voelter-Mahlknecht, S. (2022). Healthy and happy working from home? Effects of working from home on employee health and job satisfaction. Int. J. Environ. Res. Public Health 19:1122. doi: 10.3390/ijerph19031122
Niskanen, E. (2021). Self-leadership in remote work (Bachelor's Thesis). Haaga-Helia University of Applied Sciences.
Oakman, J., Lambert, K. A., Weale, V. P., Stuckey, R., and Graham, M. (2023). The effect of preference and actual days spent working from home on stress and musculoskeletal pain in older workers. Int. Arch. Occup. Environ. Health. 96, 1113–1121. doi: 10.1007/s00420-023-01992-7
Pischel, S., Felfe, J., and Krick, A. (2022). Health-oriented leadership: antecedents of leaders' awareness regarding warning signals of emerging depression and burnout. German J. Hum. Resour. Manage. 37, 169–198. doi: 10.1177/23970022221130754
Podsakoff, N. P., Podsakoff, P. M., Mackenzie, S. B., and Klinger, R. L. (2013). Are we really measuring what we say we're measuring? Using video techniques to supplement traditional construct validation procedures. J. Appl. Psychol. 98, 99–113. doi: 10.1037/a0029570
Podsakoff, P. M., Mackenzie, S. B., Lee, J.-Y., and Podsakoff, N. P. (2003). Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 88, 879–903. doi: 10.1037/0021-9010.88.5.879
Pundt, F., and Felfe, J. (2017). Health-oriented Leadership. Instrument zur Erfassung gesundheitsförderlicher Führung. Göttingen, Hogrefe.
Rusbult, C. E., and van Lange, P. A. M. (2003). Interdependence, interaction, and relationships. Ann. Rev. Psychol. 54, 351–375. doi: 10.1146/annurev.psych.54.101601.145059
Santa Maria, A., Wolter, C., Gusy, B., Kleiber, D., and Renneberg, B. (2019). The impact of health-oriented leadership on police officers' physical health, burnout, depression and well-being. Policing 13, 186–200. doi: 10.1093/police/pay067
Santiago Torner, C. (2023). Ethical leadership and creativity in employees with University education: The moderating effect of high intensity telework. Intangible Capital 19:393. doi: 10.3926/ic.2238
Siemsen, E., Roth, A., and Oliveira, P. (2010). Common method bias in regression models with linear, quadratic, and interaction effects. Organiz. Res. Methods 13, 456–476. doi: 10.1177/1094428109351241
Sjöblom, K., Juutinen, S., and Mäkikangas, A. (2022). The importance of self-leadership strategies and psychological safety for well-being in the context of enforced remote work. Challenges 13:14. doi: 10.3390/challe13010014
Sonnentag, S., and Fritz, C. (2007). The Recovery Experience Questionnaire: development and validation of a measure for assessing recuperation and unwinding from work. J. Occupat. Health Psychol. 12, 204–221. doi: 10.1037/1076-8998.12.3.204
Tautz, D. C., Schübbe, K., and Felfe, J. (2022). Working from home and its challenges for transformational and health-oriented leadership. Front. Psychol. 13:1017316. doi: 10.3389/fpsyg.2022.1017316
Wang, B., Liu, Y., Qian, J., and Parker, S. K. (2021). Achieving effective remote working during the COVID-19 pandemic: a work design perspective. Appl. Psychol. 70, 16–59. doi: 10.1111/apps.12290
Keywords: telework, working from home, SelfCare, Health-oriented Leadership, health, wellbeing
Citation: Krick A, Arnold M and Felfe J (2024) SelfCare when working from home: easier but also more important. Front. Organ. Psychol. 2:1333689. doi: 10.3389/forgp.2024.1333689
Received: 05 November 2023; Accepted: 17 January 2024;
Published: 06 February 2024.
Edited by:
Nina M. Junker, University of Oslo, NorwayReviewed by:
Diana Hanke-Boer, University of Koblenz and Landau, GermanyChristian Stamov Roßnagel, Jacobs University Bremen, Germany
Copyright © 2024 Krick, Arnold and Felfe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Annika Krick, a3JpY2tAaHN1LWhoLmRl