
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 06 December 2022
Sec. Genitourinary Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.990851
This article is part of the Research Topic Learning to Live With a Persistent Pandemic: Challenges of Balancing Resources between COVID-19 and Non-COVID-19 Patients In a New Era of Healthcare View all 9 articles
 Luigi Nocera1,2*
Luigi Nocera1,2* Lara F. Stolzenbach1,3
Lara F. Stolzenbach1,3 Claudia Collà Ruvolo1,4
Claudia Collà Ruvolo1,4 Mike Wenzel1,5
Mike Wenzel1,5 Christoph Wurnschimmel1,3Zhe Tian1Giorgio Gandaglia2Nicola Fossati2
Christoph Wurnschimmel1,3Zhe Tian1Giorgio Gandaglia2Nicola Fossati2 Vincenzo Mirone4
Vincenzo Mirone4 Felix K. H. Chun5Shahrokh F. Shariat6,7,8,9,10,11Markus Graefen3Fred Saad1Francesco Montorsi2Alberto Briganti2Pierre I. Karakiewicz1
Felix K. H. Chun5Shahrokh F. Shariat6,7,8,9,10,11Markus Graefen3Fred Saad1Francesco Montorsi2Alberto Briganti2Pierre I. Karakiewicz1Background: We tested whether a model identifying prostate cancer (PCa) patients at risk of pT3-4/pN1 can be developed for use during COVID19 pandemic, in order to guarantee appropriate treatment to patients harboring advanced disease patients without compromising sustainability of care delivery.
Methods: Within the Surveillance, Epidemiology and End Results database 2010-2016, we identified 27,529 patients with localized PCa and treated with radical prostatectomy. A multivariable logistic regression model predicting presence of pT3-4/pN1 disease was fitted within a development cohort (n=13,977, 50.8%). Subsequently, external validation (n=13,552, 49.2%) and head-to-head comparison with NCCN risk group stratification was performed.
Results: In model development, age, PSA, biopsy Gleason Grade Group (GGG) and percentage of positive biopsy cores were independent predictors of pT3-4/pN1 stage. In external validation, prediction of pT3-4/pN1 with novel nomogram was 74% accurate versus 68% for NCCN risk group stratification. Nomogram achieved better calibration and showed net-benefit over NCCN risk group stratification in decision curve analyses. The use of nomogram cut-off of 49% resulted in pT3-4/pN1 rate of 65%, instead of the average 35%.
Conclusion: The newly developed, externally validated nomogram predicts presence of pT3-4/pN1 better than NCCN risk group stratification and allows to focus radical prostatectomy treatment on individuals at highest risk of pT3-4/pN1.
Extraordinary demands are placed on healthcare system during the COVID19 pandemic. In consequence, non-COVID19 related activities are curbed (1–3). Radical prostatectomies (RPs), regardless of risk level may be postponed for several months, according to most recent guidelines (4–13). This recommendation may be inconsistent with patients at particularly elevated risk of pT3-4/pN1 stage. Presence of pT3-4/pN1 stage may eliminate or substantially reduce the curative potential of deferred definitive therapy. In consequence, pT3-4/pN1 stage may not be compatible with radical prostatectomy deferment, even during COVID19 pandemic.
NCCN guidelines stratify prostate cancer (PCa) patients into very low, low, favorable intermediate, unfavorable intermediate, high and very high risk groups according to their clinical parameters, such as PSA levels, clinical T stage, Gleason Grade Group at biopsy, number and percentage of positive biopsy cores. The optimal therapeutic strategy differs among groups, ranging from active surveillance for very low and low risk patients, to surgery or radiotherapy for the other groups (14). The rates of pT3-4/pN1 in PCa patients are not negligible and range from 16% (favorable intermediate risk) to 60% (very high risk), depending on risk level (15–18). Due to highly variable rate of pT3-4/pN1 stage, even within risk level subsets, accurate identification of patients at particularly high pT3-4/pN1 risk is challenging. To date, a specific tool designed for prediction of pT3-4/pN1 stage in favorable intermediate, unfavorable intermediate, high risk or very high risk RP candidates has not been devised. We address this void. Specifically, we postulated that pT3-4/pN1 stage can be more accurately predicted than using the existing NCCN risk group stratification.
In the Surveillance, Epidemiology and End Results (SEER) database (19), we focused on patients diagnosed with localized prostate cancer between 2010 and 2016, treated with radical prostatectomy (RP). Only individuals with known age, PSA level, clinical T stage, biopsy Gleason Grade Group (GGG), number of cores taken at biopsy (10 to 16), number of positive biopsy cores, pathological T stage and pathological N stage were included. Patients younger than 40 or older than 80 years were excluded, as well as patients with PSA level >40ng/ml (20). Patients harboring very low and low risk PCa were also excluded. Patients were then divided into two groups (development cohort and external validation cohort), based on region of residence. Specifically, the development cohort relied on patients from Midwestern, Southern and North-Eastern United States (n=13,977; 50.8%), according to SEER database. Conversely, the external validation cohort relied on patients from Western United States (n=13,552; 49.2%).
The endpoint of interest consisted of the ability to identify patients with extra-prostatic disease at RP, defined as pT3-4/pN1, using clinical characteristics: age at diagnosis, PSA, clinical T stage, biopsy GGG and percentage of positive biopsy cores.
Mean and standard deviations were reported for normally distributed, continuously coded variables. Median and interquartile ranges were reported for non-normally distributed, continuously coded variables. Frequencies and proportions were reported for categorical variables. The t-test, Mann-Whitney and chi-squared tests were used to compare means, medians and proportions, respectively. Statistical analyses consisted of several steps.
First, within the development cohort (n=13,977) we fitted a logistic regression model predicting pT3-4/pN1 using age at diagnosis, PSA level, biopsy GGG and percentage of positive biopsy cores. Clinical T stage was not included in the final model, due to lack of statistical significance. Moreover, based on left-skewed distribution of PSA level, cubic spline-transformed values were used in nomogram development.
Second, within the external validation cohort (n=13,552), we tested the discriminant ability of the newly developed nomogram, as well as that of the NCCN risk group stratification. Testing relied on ROC-derived area under the curve (AUC) that assessed the discriminant ability of nomogram versus the NCCN risk group stratification. Statistical significance of differences in related AUC values was tested according to DeLong et al. methodology (21). Moreover, comparisons of predicted versus observed probabilities of pT3-4/pN1 according to the nomogram, as well as according to the NCCN risk group stratification were depicted graphically in the form of calibration plots. Furthermore, decision curve analyses (DCA) tested the net-benefit related to the use of the nomogram versus the NCCN risk group stratification (22). Finally, systematic analyses of several possible nomogram cut-offs were performed.
All statistical tests were performed using the R statistical package v.3.6.1 (R Project for Statistical Computing, www.r-project.org) (23). All tests were two-sided, with a significance level set at p<0.05.
Within the SEER database, we identified 27,529 patients that harbored favorable intermediate, unfavorable intermediate, high risk or very high risk localized PCa, according to NCCN risk group stratification (14). Of those, 13,977 patients (50.8%) from Midwestern, Southern and North-Eastern United States formed the development cohort. The remaining 13,552 patients (49.2%) from Western United States formed the external validation cohort. Rate of pT3-4/pN1 was 18.3, 36.6, 42.5 and 66.7% in respectively favorable intermediate, unfavorable intermediate, high and very high risk PCa patients. Moreover, rate of pT3-4/pN1 was 32.5 and 35.5% in respectively development and external validation cohorts (p<0.001). Descriptive characteristics of the population and differences between the development and the external validation cohorts are depicted in Table 1.
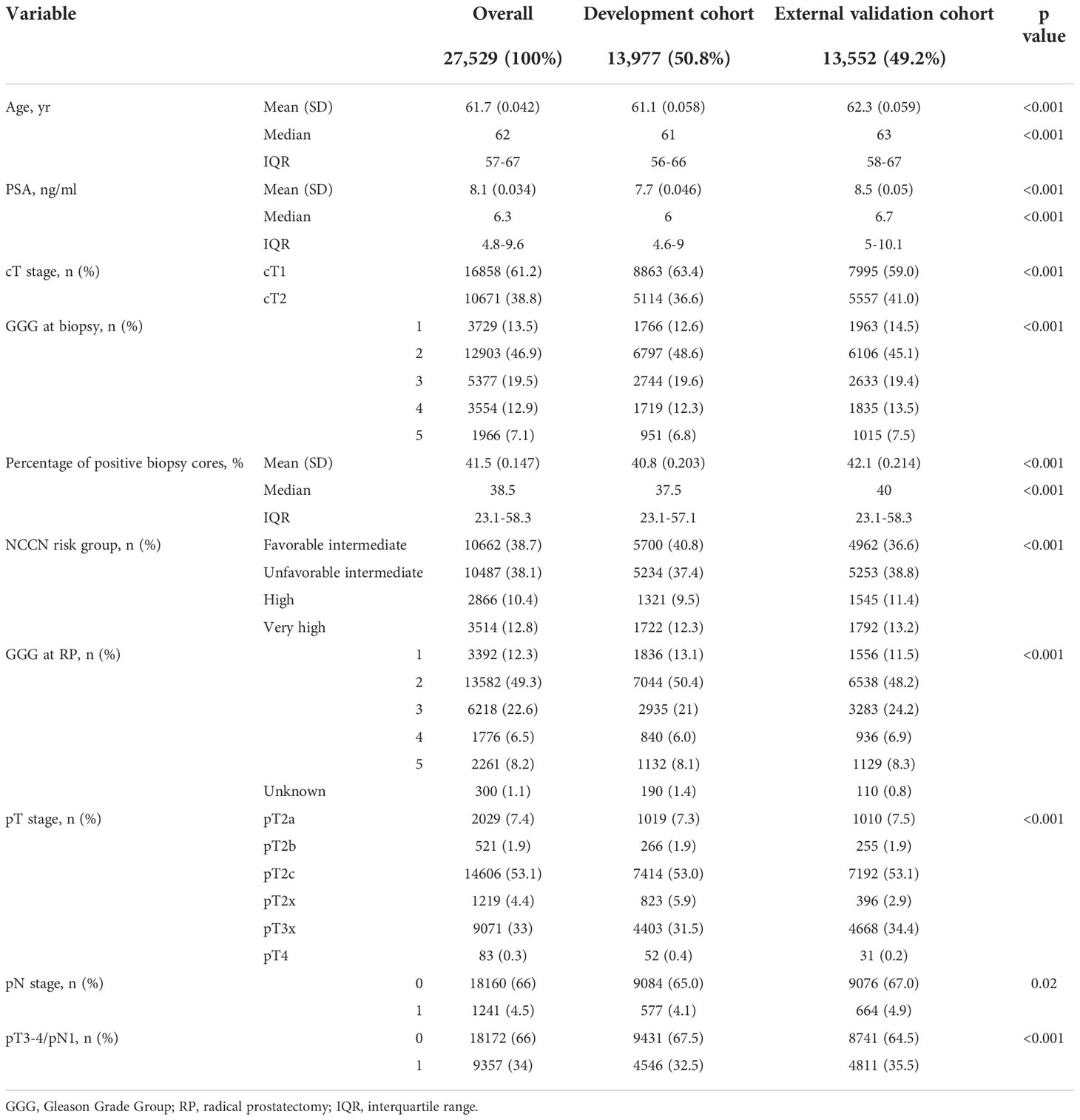
Table 1 Descriptive characteristics of 19,193 patients with clinically localized prostate cancer treated with radical prostatectomy between 2010 and 2016, identified within SEER database.
Within the development cohort, the multivariable logistic regression model underlying the nomogram predicting the probability of pT3-4/pN1 rested on age, PSA level, biopsy GGG and percentage of positive biopsy cores (Figure 1). All included variable represented independent predictors. Within the nomogram, biopsy GGG and percentage of positive biopsy cores represented the two strongest contributors to total risk points and were followed by PSA level and age, in that order.
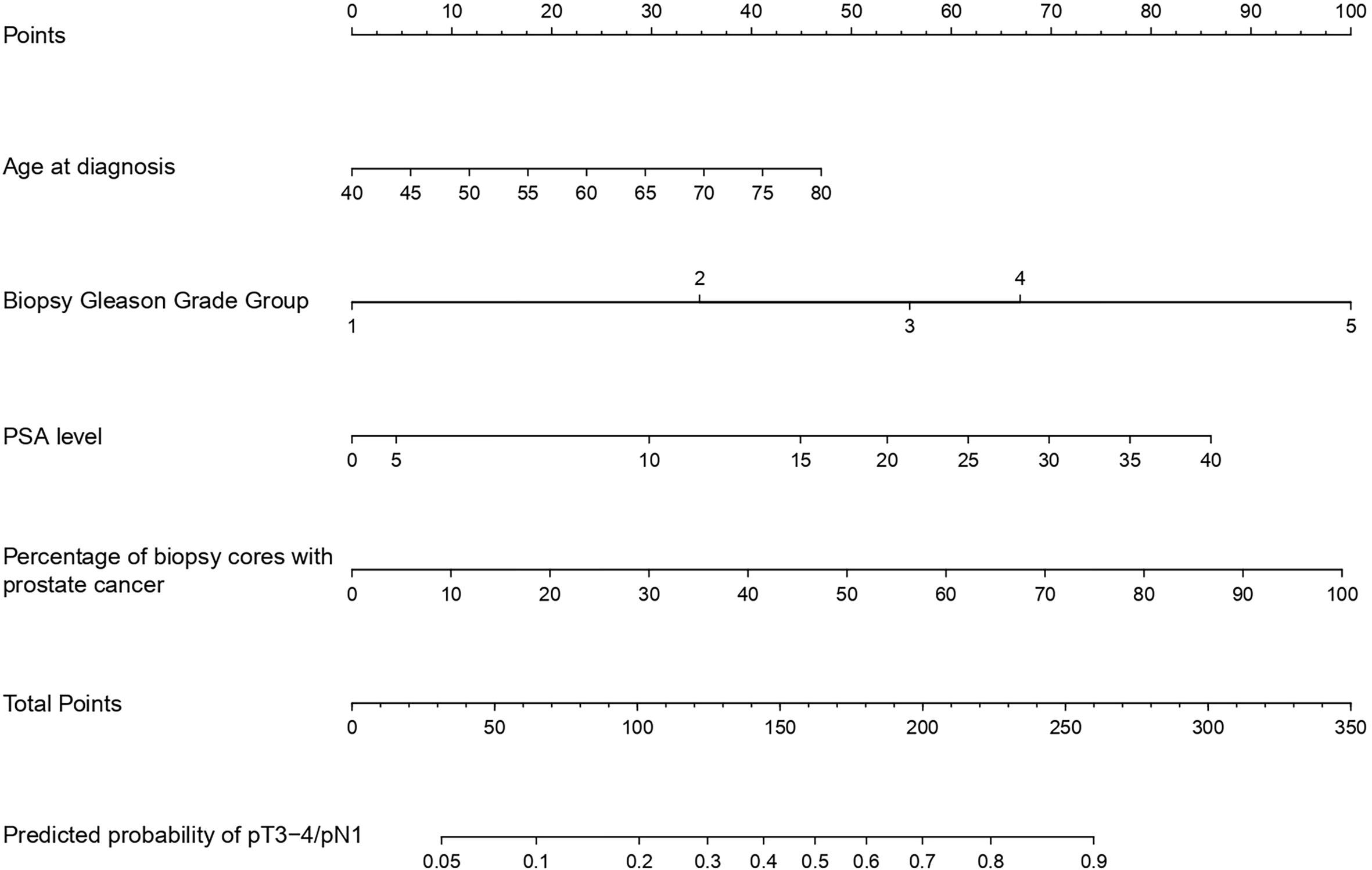
Figure 1 Model predicting the individual probability of pT3-4/pN1 at radical prostatectomy in prostate cancer patients.
Within the external validation cohort, the nomogram yielded an AUC of 74.4% (95% CI 73.5 – 75.3%) versus 68.0% (95%CI 67.1 – 68.9%) for the NCCN risk group stratification (p<0.001). In calibration plots, comparisons between predicted and observed values yielded smaller departures from ideal predictions for the nomogram, relative to the NCCN risk group stratification. Specifically, for the nomogram departures from ideal predictions ranged from -0.9 to +1.2%, for five equally-sized groups. Conversely, for the NCCN risk groups departures from ideal predictions ranged from +0.1 to +2.9% (Figure 2). Moreover in DCA, greater degree of net-benefit was recorded for the nomogram, across all threshold probabilities, relative to the NCCN risk group stratification (Figure 3).
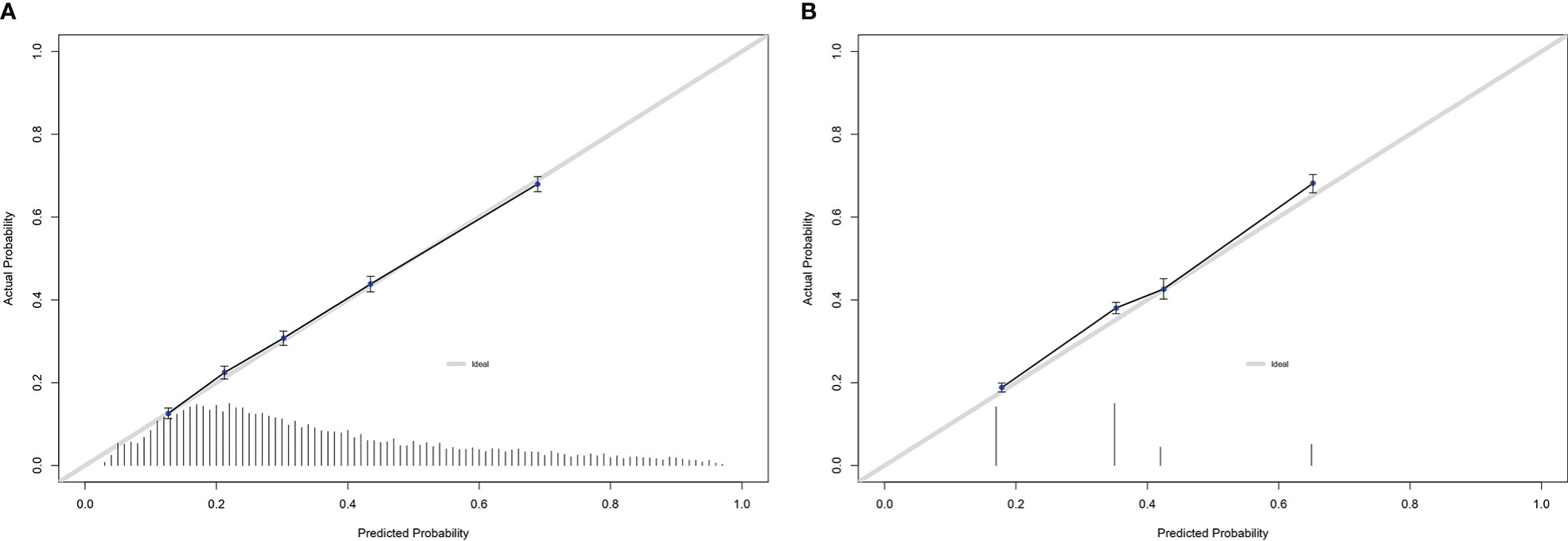
Figure 2 Calibration plots of observed versus predicted rates of pT3-4/pN1 within the external validation cohort of prostate cancer patients for: (A) the newly developed model; (B) NCCN risk group stratification.
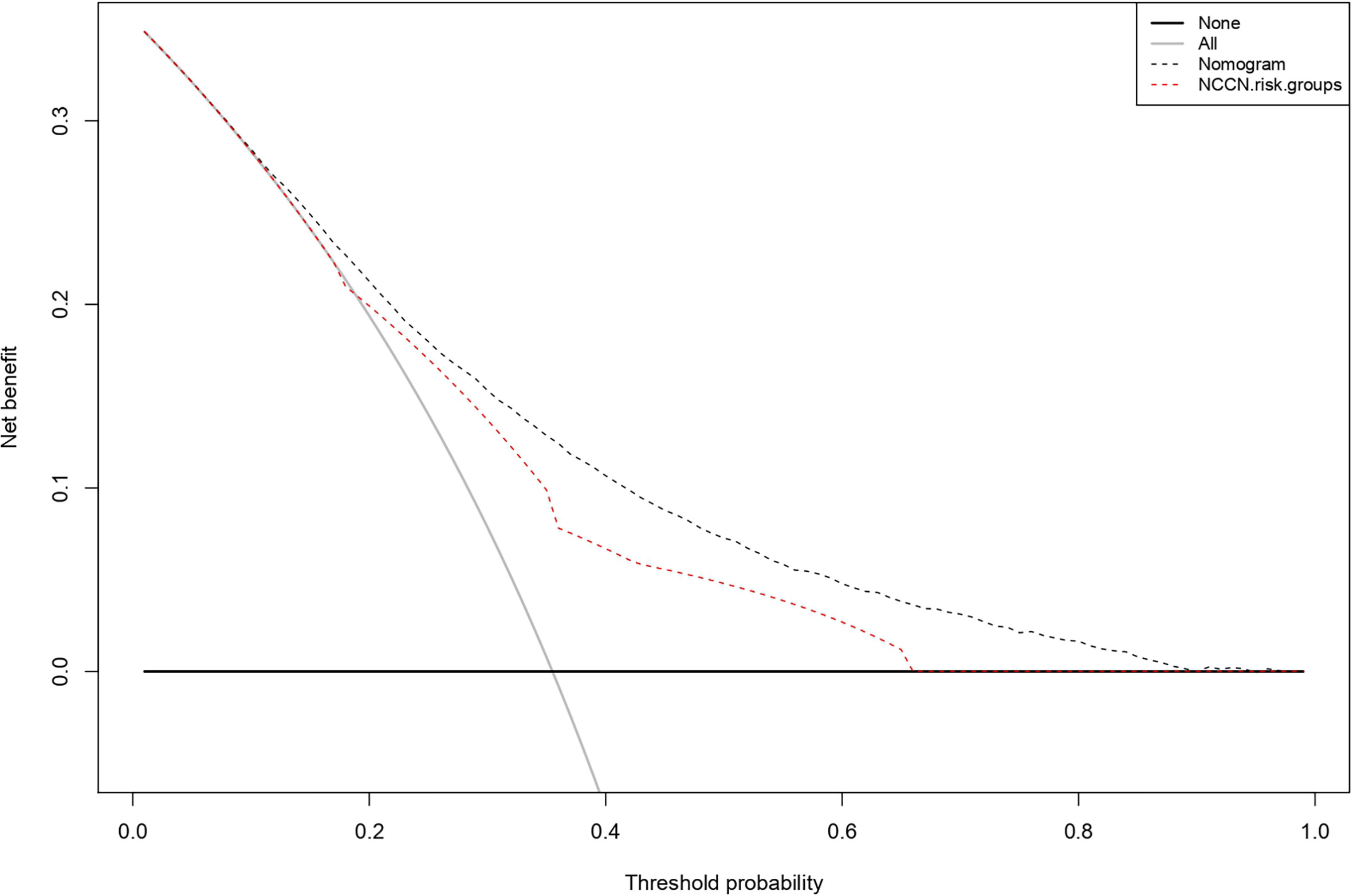
Figure 3 Decision curve analyses (DCA) demonstrating the net benefit associated with prediction of pT3-4/pN1 with the newly developed model versus a model based NCCN risk group stratification.
Finally, we tested specific nomogram cut-offs that corresponded to the predefined NCCN risk group levels. For example, a nomogram cut-off of 49% would identify 3,321 patients (24.5%) of the original 13,552 patients as at high risk of pT3-4/pN1. Of those individuals, 2,147 (64.6%) indeed harbored pT3-4/pN1. This cut-off virtually perfectly corresponded to the definition of high risk or higher, according to NCCN risk group stratification. This definition (high risk or very high risk) identified virtually the same number of individuals: 3,337 (24.6%) for NCCN versus 3,321 (24.5%) for the nomogram. Of those 3,337 individuals, 1,879 (56.3%) indeed harbored pT3-4/pN1, versus 2,147 out of 3,321 (64.6%) for the nomogram (Table 2). Alternatively, a more sensitive nomogram cut-off of 24% would identify 8,580 patients (63.3%) of the original 13,552 patients as at high risk of pT3-4/pN1. Of those individuals, 3,970 (46.3%) indeed harbored pT3-4/pN1. This cut-off virtually perfectly corresponded to the definition of unfavorable intermediate risk or higher, according to NCCN risk group stratification. This definition (unfavorable intermediate risk, high risk or very high risk) identified virtually the same number of individuals: 8,590 (63.4%) for NCCN versus 8,580 (63.3%) for the nomogram. Of those 8,590 individuals, 3,877 (45.1%) indeed harbored pT3-4/pN1, versus 3,970 out of 8,580 (46.3%) for the nomogram (Table 2). Finally, a more specific nomogram cut-off of 64% would identify 1,761 patients (13.0%) of the original 13,552 patients as at high risk of pT3-4/pN1. Of those individuals, 1,324 (75.2%) indeed harbored pT3-4/pN1. This cut-off virtually perfectly corresponded to the definition of very high risk, according to NCCN risk group stratification. This definition (very high risk) identified virtually the same number of individuals: 1,792 (13.2%) for NCCN versus 1,761 (13.0%) for the nomogram. Of those 1,792 individuals, 1,221 (68.1%) indeed harbored pT3-4/pN1, versus 1,324 out of 1,761 (75.2%) for the nomogram (Table 2).
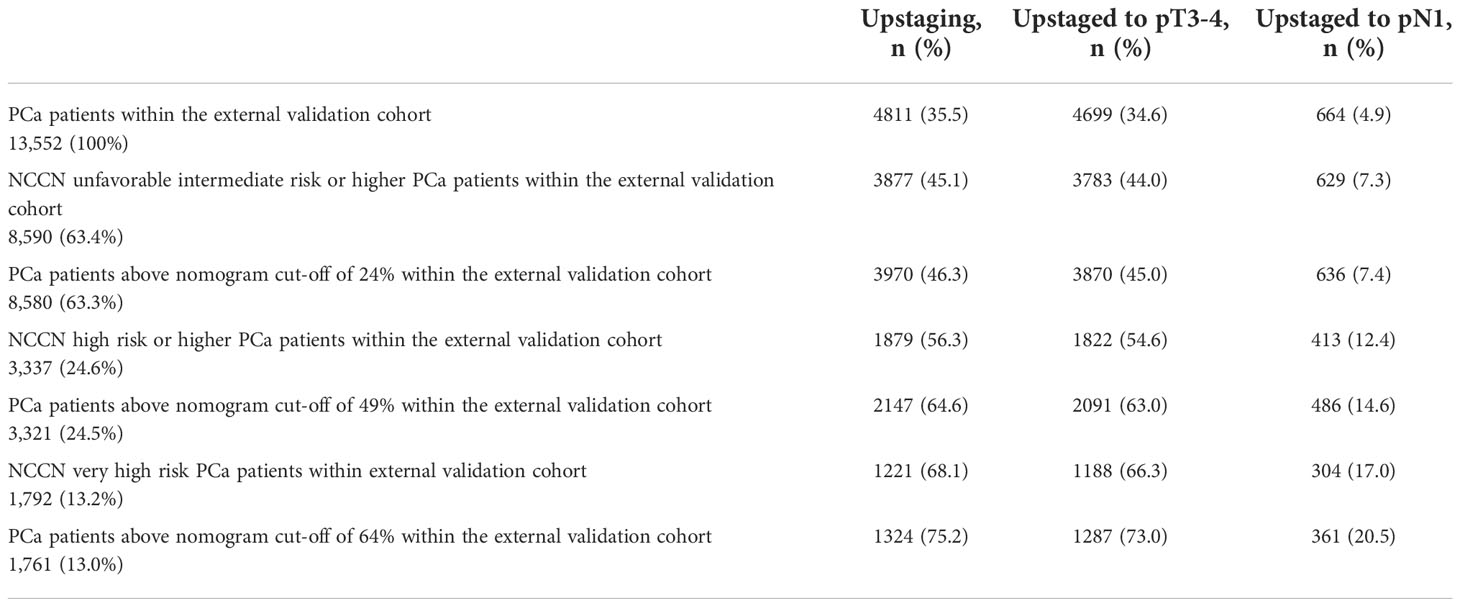
Table 2 Rates of upstaging according to NCCN risk groups and nomogram cut-offs of 24%, 49% and 64%.
During COVID19 pandemic RPs for localized intermediate or high risk PCa qualify for potential postponement up to 3 months or even beyond, according to guideline recommendations (4–13). However, some patients with clinically localized PCa may harbor pT3-4/pN1 disease. The latter can drastically curtail RP curative potential, especially if RP postponement of several months is applied. Currently, patients at elevated risk of pT3-4/pN1 cannot be identified with a specific clinical aid, except for NCCN risk group stratification. We hypothesized that a more accurate tool that allows dynamic interactions between multiple risk factors, instead of fixed NCCN risk group format, can be devised and that its ability to identify pT3-4/pN1 patients may exceed that of NCCN risk group stratification. Our analyses revealed several noteworthy observations.
First, within the overall cohort of 27,529 patients with clinically localized intermediate or high risk PCa, 34% of patients harbored pT3-4/pN1 stage. The rate of pT3-4/pN1 ranged from 18.3 to 66.7% in respectively favorable intermediate (18.3%), unfavorable intermediate (36.6%), high (42.5%) and very high (66.7%) risk PCa patients. According to individual patient characteristics, the rate of pT3-4/pN1 demonstrated important variability, even within those four risk groups. In consequence, the individual risk of pT3-4/pN1 stage is highly variable and cannot be precisely ascertained with the use of NCCN risk group stratification alone. In consequence, accurate prediction of individual pT3-4/pN1 probability prior to RP represents an unmet need. Previous nomograms developed by this group of investigators (24) and by others (25, 26) focused on RP patients of all risk levels. However, the majority RP candidates included in those reports harbored low risk PCa, and would not qualify for RP in 2020. Therefore, those previous reports do not qualify for consideration to develop COVID19-specific guideline recommendations for RP postponement. In consequence, the development of a new tool is needed and justified.
Second, to address the study objective, we relied on the development cohort of 13,977 patients residing in Midwestern, Southern and North-Eastern United States to identify independent predictors of pT3-4/pN1 at RP, within a multivariable logistic regression model. Those consisted of age, PSA level, biopsy GGG and percentage of positive biopsy cores. The logistic regression model was then graphically converted into nomogram format. Within that nomogram, biopsy GGG and percentage of positive biopsy cores contributed the highest possible number of risk points. Nonetheless, they were closely followed by PSA level and age. These observations indicate that patient, biochemical, as well as biopsy tumor characteristics represent important predictors of pT3-4/pN1 probability at RP. Moreover, in its graphical representation, the nomogram exhibits the importance of dynamic interactions between different levels of risk factors, regardless of their absolute values and across their entire range, without pre-defined cut-offs.
Third, the application of the newly developed nomogram in the external validation cohort yielded several important results. First, its accuracy was higher than the one of NCCN risk group stratification (74 vs 68%). Second, its calibration revealed lesser departures from ideal predictions than those of NCCN risk group stratification. Finally in DCA, a higher net-benefit was recorded for the nomogram than for the NCCN risk group stratification. Taken together, the newly developed nomogram exhibited better performance than the NCCN risk group stratification, according to three classic testing benchmarks for a predictive tool.
Fourth, although the nomogram can provide an individual probability of pT3-4/pN1, we relied on the use of cut-offs to illustrate its relative benefit versus NCCN risk group stratification. For example, the use of a 49% nomogram cut-off allowed us to identify 3,321 patients. Within those, 2,147 (64.6%) harbored pT3-4/pN1. The cut-off of 49% virtually perfectly replicated the NCCN definition of high risk PCa. The use of that definition also identified 3,337 patients. Of those, 1,879 (56.3%) harbored pT3-4/pN1. In consequence, despite virtually the same numbers of high risk individuals identified by the nomogram (3,321) versus NCCN risk group stratification (3,337), the rate of observed pT3-4/pN1 was higher for the nomogram than for the NCCN risk group stratification (64.6 vs 56.3%). In consequence, it may be concluded that the newly developed nomogram outperformed the NCCN risk group stratification based on three established statistical benchmarks. The use of nomogram cut-offs also yielded a higher proportion of individuals with pathologically confirmed pT3-4/pN1 than the NCCN risk group stratification. The same scenario was recorded when a lower nomogram cut-off (more sensitive) was compared to the NCCN risk group stratification, as well as when a higher nomogram cut-off (more specific) was compared to the NCCN risk group stratification.
Several nomograms have already been proposed for PCa patients stratification (17, 18, 27–30). However, they focused either on one specific risk group or on the totality of PCa patients independent of the risk group. Differently, our nomogram considered patients for whom active treatment in suggested, as per guidelines (14).
Taken together, we developed a new nomogram to identify individuals with pathologically proven pT3-4/pN1 stage, in contemporary favorable intermediate, unfavorable intermediate, high and very high risk patients. In those PCa patients, the nomogram outperformed the existing NCCN risk group stratification, based on the three established testing benchmarks, namely accuracy, calibration and DCA. Finally, the application of nomogram cut-offs resulted in a higher proportion of individuals with pathologically proven pT3-4/pN1 stage than the use of corresponding NCCN risk group definitions. In consequence, the use the nomogram represents a better alternative to NCCN risk group stratification.
Our study is not devoid of limitations, such as its retrospective and population-based nature that results in a limited number of assessable variables. For example, prostate magnetic resonance imaging findings, as well as molecular and genetic tests, repeat biopsy information or percentage of cancer per core were unavailable (31, 32). Moreover, SEER database does not allow adjustment or specific analyses that focus on later cancer control endpoints such as, for example BCR rates. Finally, lack of central review for biopsy, as well as RP pathology, also represents potential weakness (33, 34). However, it makes our findings generalizable to routine clinical practice, where central pathology is not available.
The newly developed, externally validated nomogram predicts presence of pT3-4/pN1 better than NCCN risk group stratification and allows to focus radical prostatectomy treatment on individuals at highest risk of pT3-4/pN1, during COVID19 pandemic and similar crises.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
LN: conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript, statistical analysis LS: acquisition of data, analysis and interpretation of data, critical revision of the manuscript CR: acquisition of data, analysis and interpretation of data, critical revision of the manuscript MW: acquisition of data, analysis and interpretation of data, critical revision of the manuscript CW: acquisition of data, analysis and interpretation of data, critical revision of the manuscript ZT: statistical analysis GG: critical revision of the manuscript NF: critical revision of the manuscript VM: critical revision of the manuscript FC: critical revision of the manuscript SS: critical revision of the manuscript MG: critical revision of the manuscript FS: critical revision of the manuscript FM: critical revision of the manuscript, supervision AB: critical revision of the manuscript, supervision PK: conception and design, drafting of the manuscript, critical revision of the manuscript, supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. COVID-19 . Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (Accessed April 29, 2020).
2. De Lorenzo R, Magnaghi C, Cinel E, Vitali G, Martinenghi S, Mazza MG, et al. A nomogram-based model to predict respiratory dysfunction at 6 months in non-critical COVID-19 survivors. Front Med (Lausanne) (2022) 9:781410. doi: 10.3389/fmed.2022.781410
3. Surgeons ACo. COVID-19: recommendations for management of elective surgical procedures 2020. Available at: www.facs.org/about-acs/covid-19/information-for-surgeons.
4. Katz EG, Stensland KS, Mandeville JA, MacLachlan LS, Moinzadeh A, Sorcini A, et al. Triaging office-based UrologY procedures during the COVID-19 pandemic. J Urol (2020) 204(1):9–10. doi: 10.1097/JU.0000000000001034:101097JU0000000000001034
5. Stensland KD, Morgan TM, Moinzadeh A, Lee CT, Briganti A, Catto JWF, et al. Considerations in the triage of urologic surgeries during the COVID-19 pandemic. Eur Urol (2020) 77(6):663–6. doi: 10.1016/j.eururo.2020.03.027
6. Ahmed K, Hayat S, Dasgupta P. Global challenges to urology practice during the COVID-19 pandemic. BJU Int (2020) 125(6):E5–6. doi: 10.1111/bju.15082
7. Carneiro A, Wroclawski ML, Nahar B, Soares A, Cardoso AP, Kim NJ, et al. Impact of the COVID-19 pandemic on the urologist’s clinical practice in Brazil: A management guideline proposal for low- and middle-income countries during the crisis period. Int Braz J Urol (2020) 46(4):501–10. doi: 10.1590/s1677-5538.ibju.2020.04.03
8. Ficarra V, Novara G, Abrate A, Bartoletti R, Crestani A, De Nunzio C, et al. Urology practice during the COVID-19 pandemic. Minerva Urol Nefrol (2020) 72(3):369–75. doi: 10.23736/S0393-2249.20.03846-1
9. Goldman HB, Haber GP. Recommendations for tiered stratification of urological surgery urgency in the COVID-19 era. J Urol (2020) 204(1):11–3. doi: 10.1097/JU.0000000000001067
10. Heldwein FL, Loeb S, Wroclawski ML, Sridhar AN, Carneiro A, Lima FS, et al. A systematic review on guidelines and recommendations for urology standard of care during the COVID-19 pandemic. Eur Urol Focus (2020) 6(5):1070–85. doi: 10.1016/j.euf.2020.05.020
11. Kutikov A, Weinberg DS, Edelman MJ, Horwitz EM, Uzzo RG, Fisher RI. A war on two fronts: Cancer care in the time of COVID-19. Ann Intern Med (2020) 172(11):756–8. doi: 10.7326/M20-1133
12. Mottrie A. EAU robotic urology section (ERUS) guidelines during COVID-19 emergency . Available at: https://uroweb.org/wp-content/uploads/ERUS-guidelines-for-COVID-def.pdf.
13. Ribal MJ, Cornford P, Briganti A, Knoll T, Gravas S, Babjuk M, et al. European Association of urology guidelines office rapid reaction group: An organisation-wide collaborative effort to adapt the European association of urology guidelines recommendations to the coronavirus disease 2019 era. Eur Urol (2020) 78(1):21–8. doi: 10.1016/j.eururo.2020.04.056
14. Mohler JL, Antonarakis ES, Armstrong AJ, D’Amico AV, Davis BJ, Dorff T, et al. Prostate cancer, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2019) 17(5):479–505.
15. Zumsteg ZS, Chen Z, Howard LE, Amling CL, Aronson WJ, Cooperberg MR, et al. Modified risk stratification grouping using standard clinical and biopsy information for patients undergoing radical prostatectomy: Results from SEARCH. Prostate (2017) 77(16):1592–600. doi: 10.1002/pros.23436
16. Yang DD, Mahal BA, Muralidhar V, Nezolosky MD, Vastola ME, Labe SA, et al. Risk of upgrading and upstaging among 10 000 patients with Gleason 3 + 4 favorable intermediate-risk prostate cancer. Eur Urol Focus (2019) 5(1):69–76. doi: 10.1016/j.euf.2017.05.011
17. Nocera L, Colla Ruvolo C, Stolzenbach LF, Deuker M, Tian Z, Gandaglia G, et al. Improving the stratification of intermediate risk prostate cancer. Minerva Urol Nephrol (2021) 74(5):590–8. doi: 10.23736/S2724-6051.21.04314-7
18. Stolzenbach LF, Nocera L, Colla-Ruvolo C, Tian Z, Knipper S, Maurer T, et al. Improving the stratification of patients with intermediate-risk prostate cancer. Clin Genitourin Cancer (2021) 19(2):e120–8. doi: 10.1016/j.clgc.2020.11.003
19. About the SEER program. Available at: https://seer.cancer.gov/about/overview.html.
20. Preisser F, Bandini M, Nazzani S, Mazzone E, Marchioni M, Tian Z, et al. Development and validation of a lookup table for the prediction of metastatic prostate cancer according to prostatic-specific antigen value, clinical tumor stage, and Gleason grade groups. Eur Urol Oncol (2020) 3(5):631–9. doi: 10.1016/j.euo.2019.03.003
21. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics (1988) 44(3):837–45. doi: 10.2307/2531595
22. Vickers AJ, Elkin EB. Decision curve analysis: A novel method for evaluating prediction models. Med Decis Making (2006) 26(6):565–74. doi: 10.1177/0272989X06295361
23. RCT. R: A language and environment for statistical computing. (Vienna, Austria: R Foundation for Statistical Computing) (2017).
24. Gandaglia G, Ploussard G, Valerio M, Mattei A, Fiori C, Roumiguie M, et al. The key combined value of multiparametric magnetic resonance imaging, and magnetic resonance imaging-targeted and concomitant systematic biopsies for the prediction of adverse pathological features in prostate cancer patients undergoing radical prostatectomy. Eur Urol (2020) 77(6):733–41. doi: 10.1016/j.eururo.2019.09.005
25. Ohori M, Kattan MW, Koh H, Maru N, Slawin KM, Shariat S, et al. Predicting the presence and side of extracapsular extension: A nomogram for staging prostate cancer. J Urol (2004) 171(5):1844–9. doi: 10.1097/01.ju.0000121693.05077.3d
26. Martini A, Gupta A, Lewis SC, Cumarasamy S, Haines KG 3rd, Briganti A, et al. Development and internal validation of a side-specific, multiparametric magnetic resonance imaging-based nomogram for the prediction of extracapsular extension of prostate cancer. BJU Int (2018) 122(6):1025–33. doi: 10.1111/bju.14353
27. Gandaglia G, Fossati N, Zaffuto E, Bandini M, Dell’Oglio P, Bravi CA, et al. Development and internal validation of a novel model to identify the candidates for extended pelvic lymph node dissection in prostate cancer. Eur Urol (2017) 72(4):632–40. doi: 10.1016/j.eururo.2017.03.049
28. Stephenson AJ, Scardino PT, Eastham JA, Bianco FJ, Dotan ZA, Fearn PA, et al. Preoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Natl Cancer Inst (2006) 98(10):715–7. doi: 10.1093/jnci/djj190
29. Nasri J, Barthe F, Parekh S, Ratnani P, Pedraza AM, Wagaskar VG, et al. Nomogram predicting adverse pathology outcome on radical prostatectomy in low-risk prostate cancer men. Urology (2022) 166:189–95. doi: 10.1016/j.urology.2022.02.019
30. Zelic R, Garmo H, Zugna D, Stattin P, Richiardi L, Akre O, et al. Predicting prostate cancer death with different pretreatment risk stratification tools: A head-to-head comparison in a nationwide cohort study. Eur Urol (2020) 77(2):180–8. doi: 10.1016/j.eururo.2019.09.027
31. Kasivisvanathan V, Rannikko AS, Borghi M, Panebianco V, Mynderse LA, Vaarala MH, et al. MRI-Targeted or standard biopsy for prostate-cancer diagnosis. N Engl J Med (2018) 378(19):1767–77. doi: 10.1056/NEJMoa1801993
32. Panebianco V, Valerio MC, Giuliani A, Pecoraro M, Ceravolo I, Barchetti G, et al. Clinical utility of multiparametric magnetic resonance imaging as the first-line tool for men with high clinical suspicion of prostate cancer. Eur Urol Oncol (2018) 1(3):208–14. doi: 10.1016/j.euo.2018.03.008
33. Brimo F, Schultz L, Epstein JI. The value of mandatory second opinion pathology review of prostate needle biopsy interpretation before radical prostatectomy. J Urol (2010) 184(1):126–30. doi: 10.1016/j.juro.2010.03.021
Keywords: radical prostatectomy, Pt3+, PT3, pT4, PCA, prostate cancer, C19
Citation: Nocera L, Stolzenbach LF, Collà Ruvolo C, Wenzel M, Wurnschimmel C, Tian Z, Gandaglia G, Fossati N, Mirone V, Chun FKH, Shariat SF, Graefen M, Saad F, Montorsi F, Briganti A and Karakiewicz PI (2022) Predicting the probability of pT3 or higher pathological stage at radical prostatectomy: COVID19-specific considerations. Front. Oncol. 12:990851. doi: 10.3389/fonc.2022.990851
Received: 16 July 2022; Accepted: 16 November 2022;
Published: 06 December 2022.
Edited by:
Fumitaka Koga, Tokyo Metropolitan Komagome Hospital, JapanCopyright © 2022 Nocera, Stolzenbach, Collà Ruvolo, Wenzel, Wurnschimmel, Tian, Gandaglia, Fossati, Mirone, Chun, Shariat, Graefen, Saad, Montorsi, Briganti and Karakiewicz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luigi Nocera, bm9jZXJhLmx1aWdpQGhzci5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.