
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol., 14 December 2022
Sec. Breast Cancer
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1026434
 François Poumeaud1
François Poumeaud1 Anna Fontanier2Jérémie Dion3Quentin Mathevet2Olivier Cointault4Emmanuelle Uro-Coste5Céline Marty2
Anna Fontanier2Jérémie Dion3Quentin Mathevet2Olivier Cointault4Emmanuelle Uro-Coste5Céline Marty2 Florence Dalenc1Pierre Girardie6
Florence Dalenc1Pierre Girardie6 Anaïs Rataboul1*
Anaïs Rataboul1*We report the fourth described case of severe toxic rhabdomyolysis occurring in an 81-year-old woman caused by the concomitant administration of palbociclib taken at the usual dosage (125 mg per day) and simvastatin. To the best of our knowledge, this is the first reported case successfully treated by plasma exchanges, with complete functional recovery within two months. The severity of this case justifies further consideration of pharmacokinetic interactions between palbociclib or other CDK-4-6 inhibitors and statins, which potentially increase the risk of an adverse event.
Cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors combined with endocrine therapy (aromatase inhibitor or fulvestrant) are the standard-of-care for estrogen receptor (ER)-positive/HER2-negative metastatic breast cancer (MBC) without visceral crisis/failure and result in longer progression-free and overall survival with a good toxicity profile (1, 2). Palbociclib is one of the commonly used oral CDK4/6inhibitors. Inter-individual variations in exposure to the drug are large as it is extensively metabolized by cytochrome P450 3A4 (CYP3A4) and its brain penetration is limited by efflux transporters (3). Specific precautions must therefore be taken to avoid any potential interactions with other substances metabolized by CYP3A4.
Statins are widely prescribed to the general population, especially simvastatin which is metabolized by CYP3A4. Consequently, CYP3A4 inhibitors, such as palbociclib, may increase the plasma concentration of simvastatin, thus increasing the risk of an adverse reaction. To date, four cases of severe toxic rhabdomyolysis related to inhibitors of cyclin-dependent kinase 4 and 6 drugs have been reported in the literature (Table 1). All of these occurred with the association of statin-drugs (3 with simvastatin, 1 with atorvastatin) with conventional doses of palbociclib (3 cases) (4–6) or ribociclib (1 case) (7). It seems unlikely thatCDK4/6 inhibitors would cause inflammatory myopathy or rhabdomyolysis since no such cases have been reported for either palbociclib (8–10), ribociclib (11, 12) or abemaciclib. Here, we describe a case of severe toxic rhabdomyolysis due to the concomitant exposure to palbociclib and simvastatin in a woman suffering from MBC, and the first report of its successful treatment via a plasma exchange-based therapy.
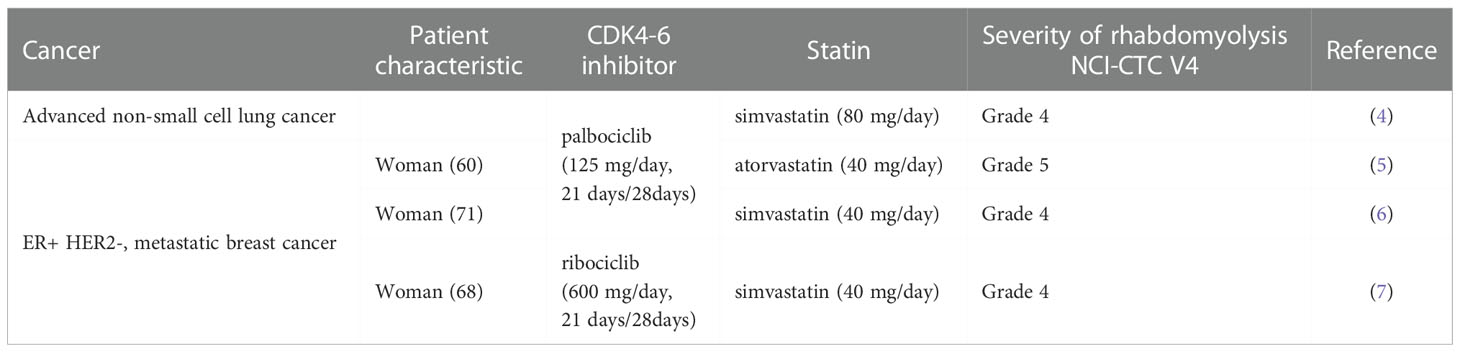
Table 1 Reported toxic myositis in patients treated with cyclin-dependent inhibitors.
An 81-year-old woman presented with a six-day history of progressive muscle pain and progressive weakness of the lower limbs. She had taken simvastatin for over twenty years, and simvastatin 20 mg plus ezetimibe 10 mg for five years to treat dyslipidemia. She had also been prescribed apixaban, venlafaxine, L-thyroxine and allopurinol for several years. She presented with an ER+/HER2-negative de novo MBC with bone extension in the summer of 2021. She had a slightly increased tumor marker (CA 15.3 241 kU/L) at baseline.
A first-line metastatic combination treatment with an aromatase-inhibitor (letrozole 2,5 mg per day) and CDK4-6 inhibitor (palbociclib125 mg per day, 21 days/28) was initiated. After 20 days of concomitant treatment, she presented with a generalized mild-intensity myalgia associated with the onset of a proximal motor deficit of the lower limbs, which subsequently extended to the upper limbs and developed into discrete myalgia. At day 23 after treatment initiation, she presented with proximal muscle weakness affecting both the lower and upper limbs, she was unable to brush her hair or to straighten-up. She then had a fall and laid on the floor for one hour before being transferred to the nearby emergency unit.
In the emergency unit, she was diagnosed with proximal tetraparesis and intense rhabdomyolysis (CPK 18.000 UI/L, approximately 90 times over the upper limit of 170 UI/L) which was inconsistent with the absence of extensive hematoma. There was no alteration of glomerular filtration.
Timeline: The patient initiated palbociclib on December 4th for 21 days. At day 23, she exhibited first muscle weakness and was admitted to the emergency unit. Corticotherapy and saline hydration were initiated at day 28 and plasmatic exchanges at day 32 for three sessions.
When transferred to the medical oncology department, the patient presented with a severe proximal tetraparesis predominantly involving the proximal inferior-muscle girdle, which was associated with a dropped head syndrome secondary to severe weakness of the neck extensors but not affecting the diaphragm or deglutition. Cranial nerve examination and sensory evaluation were non-pathological. A careful clinical examination found no evidence of cutaneous lesions consistent with dermato-polymyositis.
Three hypotheses were explored to substantiate the etiology of the myogenic deficit with concomitant rhabdomyolysis:
-In light of the active MBC, we initially suspected an auto-immune disorder and paraneoplastic syndrome. However, her imaging data pointed to a controlled disease, no visceral lesions, no new bone lesions and a biologically stable disease (CA 15.3 level stable at 249 kU/L despite altered hepatic function). Notably, thorax tomodensitometry revealed no pulmonary lesions compatible with diffuse interstitial lung disease. An extensive screen for a panel of myositis autoantibodies was negative (see Supplementary Data). Free carnitine was dramatically increased and significant acylcarnitinemia was compatible with massive rhabdomyolysis. These findings were consistent with a diagnosis of myositis.
A bacterial screen with several pairs of negative hemocultures to test for a suspected infectious myositis was negative. Tests for viral primo-infections or reactivation were tested, and were negative (see Supplementary data). Viral PCR tests were all negative and/or below the significance threshold and were therefore deemed to be clinically irrelevant. Furthermore, there was no evidence that the patient had contracted a COVID-19 infection during her hospitalization.
We finally suspected a toxic rhabdomyolysis due to a palbociclib/simvastatin interaction, which appeared to be consistent with the timing of the symptoms reported by the patient. Further discussion with the patient revealed she was self-medicating with fenugreek (trigonellafoenum-graecum), an orexigenic phytotherapy with cytochrome inhibitory properties, which may have promoted the interaction between the CDK4-6 inhibitor and the statin.
Despite the administration of intravenous corticotherapy (1.5 mg/kg/day) as well as a appropriate hydration with 2L/day of sodium chloride, her CPK levels continued to increase to 47.000 UI/L, presumably because palbociclib and simvastatin bind strongly to plasma proteins (85 and 95%, respectively). We therefore performed a series of plasma exchanges to wash out any residual bound palbociclib and simvastatin. The patient underwent three sessions of apheresis on alternative days (see Figure 1). We performed a selective plasma separation with a pore size that was small enough for the transfer of albumin but not of higher molecular weight molecules. Two plasma volumes were treated during each session. Tolerance was excellent with no adverse event occurring during or after hospitalization. One month after discharge, the patient was able to walk unassisted in her home, to groom herself and had no muscular impediments. At two months from discharge, she presented no sequelae and was perfectly autonomous in her daily life activities. Palbociclib was definitively discontinued, and the patient was treated with letrozole alone. CT-scan at three months showed progression of the bone metastasis which was treated with tamoxifen, followed by capecitabine for seven months due to disease progression. This patient is currently living independently at home and can perform her daily activities without material assistance.
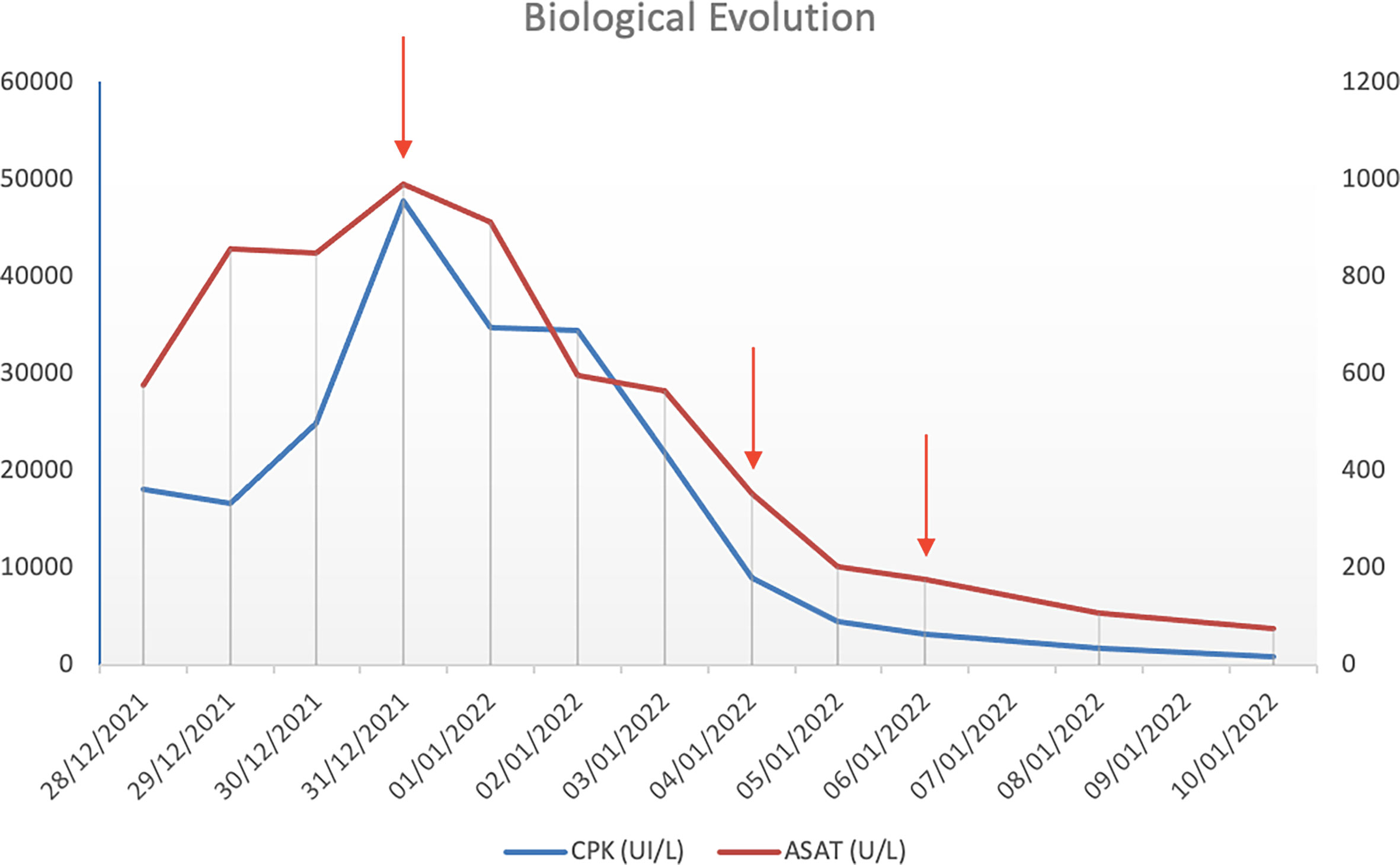
Figure 1 Evolution of CPK and ASAT after three plasma exchange cycles (red arrows). The natural evolution of CPK and ASAT levels before initiation of plasmatic exchanges is symbolized by red arrows. As illustrated, three plasmatic exchanges led to a significant decrease in both CPK and ASAT levels.
Given the long waiting list to obtain an MRI test, the diagnosis was confirmed retrospectively by MRI of the lower-limb muscles at the end of plasmatic exchanges. It showed bilateral and symmetrical hyper-intense signals on short-tau-inversion-recovery (STIR) sequences, on most of the muscles explored. This was compatible with muscular oedema, specifically involving the medial gastrocnemii and solaris muscles (see Figure 2A). An MRI-guided muscle biopsy was therefore performed on the left quadricipital muscle. This revealed a muscle inflammation with macrophage infiltration, fibrillary involution and necrosis of myocytes, thereby confirming the diagnosis of necrosing myositis (see Figure 2B).
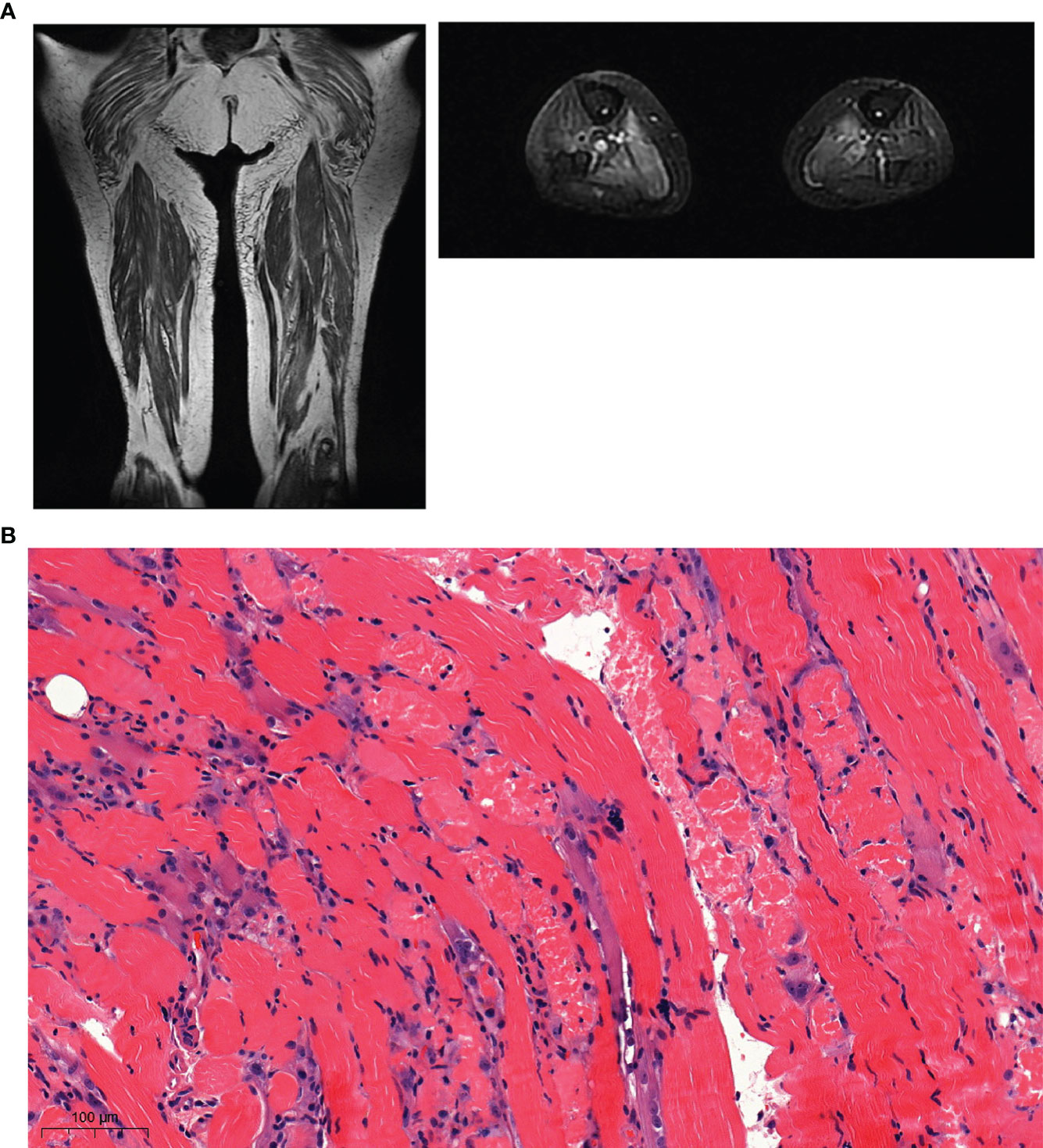
Figure 2 (A) Magnetic Resonance Imaging (MRI) of muscles of lower limbs, T1 Coronal and T2 axial reconstruction. MRI shows pathological bilateralhypersignal of proximal muscles: gluteal muscles, medial gastrocnemius muscles, solar muscles with relative respect of semitendinosus muscles. (B) Immuno-histo-chemical staining of the muscle biopsy. Standard muscle biopsy stain exhibiting muscle atrophy, degeneration, necrosis, macrophagic infiltration and muscle fiber irregularity.
Statins such as simvastatin and atorvastatin are cleared via a CYP3A4-mediated hepatic metabolic pathway. Since CDK 4-6 inhibitors such as palbociclib and ribociclib are time-dependent CP3A4-inhibitors, they may decrease hepatic clearance and increase the plasma concentrations of statins, thereby potentially exposing patients to toxicities (13). In silico pharmaco-kinetic modeling of atorvastatin and palbociclib found a CYP3A4-mediated increase in atorvastatin-lactones (associated with statin-induced-myopathy and rhabdomyolysis) when atorvastatin was co-administered with palbociclib (14). Since simvastatin and atorvastatin share the same CYP3A4 metabolic pathway, these results obtained in silico may also extrapolate to simvastatin.
In accordance with procedural recommendations, we reported the case to the pharmacovigilance department who further declared it to the French National Agency for Medicines and Health products Safety (ANSM). In France, no other cases of rhabdomyolysis have been reported with palbociclib or when palbociclib is combined with simvastatin or more generally when CK4/6 inhibitors and statins are given concomitantly. The pharmacovigilance department of our hospital has estimated that the area under curve (AUC) of simvastatin increased to 1.6 when palbociclib was added. The intrinsic causality of rhabdomyolysis by the combination of palbociclib and simvastatin was therefore considered very plausible (I5 score) (15). Using the Adverse Drug Reaction Probability Scale evaluates the interaction as plausible, with a score of 5 (16). As pitavastatin and fenofibrate are not CYP3A4 substrates their use should be recommended, instead of simvastatin or atorvastatin, when considering a combination treatment withCDK4-6 inhibitors (13).
In vitro, letrozole is an inhibitor of CYP450 2A6 and 2C19 but its clinical relevance is still unknown. Moreover, even if letrozole is a CYP3A4 substrate, and although an inhibitor such as palbociclib may decrease its metabolism and increase blood exposure, cases of myalgia have been described but no rhabdomyolysis. Finally, the treatment was not discontinued during hospitalization. Therefore, we cannot consider letrozole as the suspect cause of the adverse effect itself or of its onset.
In the present case, the co-treatment with fenugreek (taken for only two days) did not likely contribute to worsening the interaction, since several publications have reported that its in vivo metabolic inhibition mediated by CYP3A4 is not substantial (17–19). However, fenugreek contains quercetin, which is a strong CYP3A4 inhibitor and has been shown to increase the AUC of cyclosporin (20). In our patient, fenugreek may have decreased the metabolism of palbociclib and the simvastatin and therefore contributed to worsening the undesirable effect. Caution should thus be exercised when fenugreek is co-administered with CYP34A substrates.
Data concerning the increased risk of rhabdomyolysis with co-administration of statin and ezetimibe are conflicting. Whilst one case study reported on rhabdomyolysis occurring with the combination of statin and ezetimibe (21), a larger review of the literature found no increased risk of this drug combination (22, 23). The current recommendation to initiate ezetimibe for statin-induced myopathy (24), would perhaps also requires further investigation. Whether rhabdomyolysis may be attributed to ezetimibe in our patient cannot be chronologically evaluated, since it was introduced concomitantly with simvastatin. Moreover, pharmacologically ezetimibe is an inhibitor of intestinal cholesterol transport and has no physiological role in muscles. Finally, the literature does not support its involvement given the few cases reported when administered as a monotherapy. The statin would therefore seem to be incriminated in our case.
As in the other case reports, our patient received steroids (1.5 mg/kg/day intravenously) and abundant hydration with sodium chloride (2L per day) to prevent kidney failure. A Danish team administered experimental intravenous immunoglobulins (IgIV) for five days, while waiting for the auto-immune laboratory results (6). In the absence of clear supportive paraneoplastic and auto-immune evidence, and in light of the considerable risk of acute renal failure due to the active rhabdomyolysis (25) as well as the significant proteinuria that developed during hospitalization, we did not opt forIgIV. To our knowledge, however, we are the first team to report on the successful recovery of a patient by an experimental plasma exchange protocol, based on the pharmacokinetic properties of the drugs suspected of inducing the adverse effect.
This is the fourth reported case of severe toxic rhabdomyolysis occurring under palbociclib and statins (Table 1). All of them occurred with the co-administration of statin-drugs (3 with simvastatin, 1 with atorvastatin) and a conventional dosage of palbociclib (3 cases) (4–6) or ribociclib (1 case) (7). No such cases have to date been reported with abemaciclib. We also report on what we believe is the first successful use of plasma exchange for this indication. The current French RCP and FDA prescribing information for palbociclib mentions changes in plasma concentrations for CYP3A4 substrates with a narrow therapeutic index. Statins are not among these drugs and are therefore not mentioned. Substrates with strong adverse effects should be considered in the same way as those mentioned in the prescribing information and require close therapeutic monitoring and dose adjustment. Further clarification of this issue now required.
The original contributions presented in the study are included in the article/Supplementary material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
FP diagnosed and treated the patient, wrote, edited and corrected the main part of the article. AF wrote and corrected some parts of the manuscript. JD helped to diagnose the patient and corrected the manuscript. QM corrected some parts of the manuscript. OC performed the plasma exchanges and corrected some part of the manuscript. EU-C performed the analysis of the biopsy and corrected some parts of the manuscript. CM wrote and corrected some parts of the manuscript. FD wrote and corrected some parts of the manuscript. PG helped to diagnose the patient, wrote and corrected some parts of the manuscript. AR wrote and corrected some parts of the manuscript and handled the correspondence. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.1026434/full#supplementary-material
1. Gennari A, André F, Barrios CH, Cortés J, de Azambuja E, DeMichele A, et al. ESMO clinical practice guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol (2021) 32:1475–95. doi: 10.1016/j.annonc.2021.09.019
2. Cardoso F, Paluch-Shimon S, Senkus E, Curigliano G, Aapro MS, André F, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann oncology : Off J Eur Soc Med Oncol (2020) 31. doi: 10.1016/j.annonc.2020.09.010
3. Parrish KE, Pokorny J, Mittapalli RK, Bakken K, Sarkaria JN, Elmquist WF. Efflux transporters at the blood-brain barrier limit delivery and efficacy of cyclin-dependent kinase 4/6 inhibitor palbociclib (PD-0332991) in an orthotopic brain tumor model. J Pharmacol Exp Ther (2015) 355:264–71. doi: 10.1124/jpet.115.228213
4. Gopalan P, Pinder-Schenck M, Chiappori A, Ivey A, Villegas A, Kaye F. A phase II clinical trial of the CDK 4/6 inhibitor palbociclib (PD 0332991) in previously treated, advanced non-small cell lung cancer (NSCLC) patients with inactivated CDKN2A. J Clin Oncol (2014) 32:8077–7. doi: 10.1200/jco.2014.32.15_suppl.8077
5. Nelson KL, Stenehjem D, Driscoll M, Gilcrease GW. Fatal statin-induced rhabdomyolysis by possible interaction with palbociclib. Front Oncol (2017) 7:150. doi: 10.3389/fonc.2017.00150
6. Nersesjan V, Hansen K, Krag T, Duno M, Jeppesen TD. Palbociclib in combination with simvastatin induce severe rhabdomyolysis: a case report. BMC Neurol (2019) 19:247. doi: 10.1186/s12883-019-1490-4
7. Streicher C, Daulange A, Madranges N, Vayre L. Severe rhabdomyolysis induced by possible drug-drug interaction between ribociclib and simvastatin. J Oncol Pharm Pract (2021) 27:722–6. doi: 10.1177/1078155220945365
8. Cristofanilli M, Turner NC, Bondarenko I, Ro J, Im S-A, Masuda N, et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol (2016) 17:425–39. doi: 10.1016/S1470-2045(15)00613-0
9. Finn RS, Crown JP, Lang I, Boer K, Bondarenko IM, Kulyk SO, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol (2015) 16:25–35. doi: 10.1016/S1470-2045(14)71159-3
10. Iwata H, Im S-A, Masuda N, Im Y-H, Inoue K, Rai Y, et al. PALOMA-3: Phase III trial of fulvestrant with or without palbociclib in premenopausal and postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer that progressed on prior endocrine therapy-safety and efficacy in Asian patients. J Glob Oncol (2017) 3:289–303. doi: 10.1200/JGO.2016.008318
11. Tripathy D, Im S-A, Colleoni M, Franke F, Bardia A, Harbeck N, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial. Lancet Oncol (2018) 19:904–15. doi: 10.1016/S1470-2045(18)30292-4
12. Slamon DJ, Neven P, Chia S, Fasching PA, De Laurentiis M, Im S-A, et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. New Engl J Med (2020) 382:514–24. doi: 10.1056/NEJMoa1911149
13. Bellet M, Ahmad F, Villanueva R, Valdivia C, Palomino-Doza J, Ruiz A, et al. Palbociclib and ribociclib in breast cancer: consensus workshop on the management of concomitant medication. Ther Adv Med Oncol (2019) 11:1758835919833867. doi: 10.1177/1758835919833867
14. Li S, Yu Y, Jin Z, Dai Y, Lin H, Jiao Z, et al. Prediction of pharmacokinetic drug-drug interactions causing atorvastatin-induced rhabdomyolysis using physiologically based pharmacokinetic modelling. Biomed Pharmacot (2019) 119:109416. doi: 10.1016/j.biopha.2019.109416
15. Théophile H, Dutertre J-P, Gérardin M, Valnet-Rabier M-B, Bidault I, Guy C, et al. Validation and reproducibility of the updated French causality assessment method: an evaluation by pharmacovigilance centres & pharmaceutical companies. Therapies (2015) 70:465–76. doi: 10.2515/therapie/2015028
16. Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther (1981) 30:239–45. doi: 10.1038/clpt.1981.154
17. Al-Jenoobi FI, Al-Thukair AA, Alam MA, Abbas FA, Al-Mohizea AM, Alkharfy KM, et al. Effect of trigonella foenum-graecum l. @ on metabolic activity of CYP2D6 and CYP3A4. Forsch Komplementmed (2015) 22:180–4. doi: 10.1159/000432412
18. Al-Jenoobi FI, Alam MA, Alkharfy KM, Al-Suwayeh SA, Korashy HM, Al-Mohizea AM, et al. Pharmacokinetic interaction studies of fenugreek with CYP3A substrates cyclosporine and carbamazepine. Eur J Drug Metab Pharmacokinet (2014) 39:147–53. doi: 10.1007/s13318-013-0149-6
19. Ahmmed SM, Mukherjee PK, Bahadur S, Kar A, Mukherjee K, Karmakar S, et al. Interaction potential of trigonella foenum graceum through cytochrome P450 mediated inhibition. Indian J Pharmacol (2015) 47:530–4. doi: 10.4103/0253-7613.165179
20. Clarke SJ, McLachlan AJ. Interaction between complementary and alternate medicine with conventional anti-cancer medicine. Cancer Forum (2011) 35:18–23. doi: 10.3316/informit.854155016595505
21. Piedra León M, García Unzueta MT, Otero Martínez M, Amado Señaris JA. [Rhabdomyolysis associated to combined ezetimibe-statin treatment]. Rev Clin Esp (2007) 207:425–6. doi: 10.1157/13108771
22. Kashani A, Sallam T, Bheemreddy S, Mann DL, Wang Y, Foody JM. Review of side-effect profile of combination ezetimibe and statin therapy in randomized clinical trials. Am J Cardiol (2008) 101:1606–13. doi: 10.1016/j.amjcard.2008.01.041
23. Florentin M, Liberopoulos EN, Elisaf MS. Ezetimibe-associated adverse effects: what the clinician needs to know. Int J Clin Pract (2008) 62:88–96. doi: 10.1111/j.1742-1241.2007.01592.x
24. Suzuki H, Watanabe Y, Kumagai H, Shuto H. Comparative efficacy and adverse effects of the addition of ezetimibe to statin versus statin titration in chronic kidney disease patients. Ther Adv Cardiovasc Dis (2013) 7:306–15. doi: 10.1177/1753944713513222
Keywords: rhabdomyolysis, palbociclib, simvastatin, interaction, myositis, plasmatic exchange
Citation: Poumeaud F, Fontanier A, Dion J, Mathevet Q, Cointault O, Uro-Coste E, Marty C, Dalenc F, Girardie P and Rataboul A (2022) Severe toxic rhabdomyolysis under combined palbociclib and simvastatin treatment: A case report. Front. Oncol. 12:1026434. doi: 10.3389/fonc.2022.1026434
Received: 23 August 2022; Accepted: 30 November 2022;
Published: 14 December 2022.
Edited by:
Thomas O. Krag, Rigshospitalet, DenmarkReviewed by:
Teodora Alexa-Stratulat, Grigore T. Popa University of Medicine and Pharmacy, RomaniaCopyright © 2022 Poumeaud, Fontanier, Dion, Mathevet, Cointault, Uro-Coste, Marty, Dalenc, Girardie and Rataboul. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anaïs Rataboul, cmF0YWJvdWwuYW5haXNAaXVjdC1vbmNvcG9sZS5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.