 Yao Gao
Yao Gao Xiao-Na Song3†
Xiao-Na Song3† Sha Liu
Sha Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Nutr., 15 April 2025
Sec. Nutrition, Psychology and Brain Health
Volume 12 - 2025 | https://doi.org/10.3389/fnut.2025.1551375
This article is part of the Research TopicThe Role of Nutrition in Mitigating Depression: Mechanisms, Interventions, and OutcomesView all 4 articles
Late-life depression (LLD), a growing public health challenge in aging societies, profoundly impacts physical and mental health by exacerbating cognitive decline, functional disability, and comorbid chronic diseases. Emerging research highlights vitamin supplementation as a promising adjunctive therapy for LLD, targeting its multifactorial pathogenesis involving mitochondrial dysfunction, neuroinflammation, and oxidative stress. Specific vitamins, including B-complex vitamins (B1, B6, B9, B12), vitamin D, and antioxidants (C, E), demonstrate therapeutic potential through mechanisms ranging from neurotransmitter regulation to mitochondrial function enhancement. For instance, vitamin D modulates serotonin synthesis and calcium signaling, while B vitamins mitigate homocysteine-mediated neurotoxicity and support energy metabolism. Antioxidants counteract neural oxidative damage linked to depressive severity. Clinical studies reveal that vitamin D deficiency (<20 ng/mL) correlates with elevated depression risk, and combined B-vitamin supplementation shows symptom alleviation in nutritionally deficient subgroups. However, evidence remains heterogeneous due to variability in dosing protocols, bioavailability, and population-specific factors like comorbidities. Despite growing evidence, critical gaps persist regarding optimal dosages, bioavailability variations, and long-term outcomes in elderly populations. This review synthesizes current evidence on vitamin-mediated cellular pathways in LLD management, evaluates clinical efficacy across interventions, and proposes personalized nutritional strategies to optimize therapeutic outcomes. By integrating mechanistic insights with clinical data, this analysis aims to guide evidence-based vitamin supplementation protocols for LLD within geriatric care frameworks.
Late-life depression (LLD) is a multifaceted disorder influenced by a combination of biological and environmental factors, such as mitochondrial dysfunction, neurotransmitter dysregulation, hormonal imbalances, inflammation, and oxidative stress. As the global aging population continues to grow, the prevalence of depression in older adults is steadily increasing. According to recent studies, the incidence of depression among the elderly is notably higher compared to other age groups, and its symptoms are frequently misattributed to the normal aging process, leading to delayed or inadequate treatment for many patients (1). Depression not only impacts the mental health of the elderly but also elevates the risk of physical health issues, including cardiovascular disease, type 2 diabetes, and Alzheimer’s disease (2, 3). Consequently, identifying and managing depression in later life is of paramount importance.
Recent awareness has grown regarding the potential role of vitamins in enhancing mental health, particularly brain health. Extensive empirical evidence indicates that deficiencies in vitamin D, B vitamins, and other micronutrients are linked to an increased incidence of depression (4, 5), especially among women and overweight older adults (6). Furthermore, evidence suggests that high total intakes of vitamins B6 and B12 exert a protective effect against depressive symptoms in older adults over time (7). Additionally, vitamins B12, D, and E, along with other nutrients, have demonstrated support for mitochondrial function, which is frequently compromised in LLD patients. For instance, niacin supplementation has been shown to increase NAD+ levels and improve mitochondrial function, potentially alleviating depressive symptoms (8). Beyond their role in supporting mitochondrial function, vitamin supplements may also influence inflammation and oxidative stress, both of which are linked to LLD. Vitamin E supplementation, for example, has been found to bolster antioxidant defenses and lower markers of oxidative stress, which are typically elevated in LLD patients (9). By enhancing the body’s capacity to manage oxidative stress and inflammation, vitamin supplements may contribute to improved mental health and cognitive function in older adults. These potential benefits underscore the importance of investigating the integration of vitamin supplements into LLD treatment strategies, offering hope for better outcomes in this population.
In summary, given the growing concerns about aging and associated mental health issues, it is essential to further explore the potential of vitamins as an intervention in future scientific and clinical practices.
Search PubMed for vitamins A, B, C, D, E and K and “depression in older adults”; or “LLD”; Or “late-life depression.” Each vitamin is combined with a disease—for example, “vitamin C” or “geriatric depression.” The search is limited to articles published in English within the last 15 years and involving humans. A total of 7,980 articles were retrieved through these searches. Identify relevant papers by reviewing their titles and abstracts; The list of references was also checked to identify any other articles. A total of 28 articles were discussed as they were deemed suitable for inclusion in this review.
Recent studies have elucidated the multi-dimensional role of vitamin supplements in disease management, yet significant heterogeneity persists in their clinical applications. Research on vitamin D has demonstrated a dose-dependent effect on cancer prevention and metabolic disease regulation; however, consensus regarding its cardiovascular protection remains elusive (10, 11). In the neuropsychiatric domain, vitamin D deficiency (<20 ng/mL) has been robustly linked to an elevated risk of depression in older adults. However, the efficacy of supplemental interventions in alleviating depressive symptoms is moderated by factors such as gender, baseline nutritional status, and others (12–15). The B vitamin family study presents a more intricate scenario: while dietary intake of vitamins B6 and B12 was negatively associated with depression risk, this association was not significant when derived from food sources, underscoring the importance of bioavailability differences (7) (Table 1). Notably, multivitamin interventions have shown synergistic benefits in improving mood and cognitive function in patients with mild cognitive impairment (16, 17), and in combination with n-3 fatty acids, they enhance neuroprotective effects (18, 19). Current evidence underscores the importance of personalized nutrition strategies, including dynamic adjustment of vitamin D dosage based on serum markers (20), balancing the therapeutic window of vitamin B6 against the risk of neurotoxicity (21) and integrating dietary interventions with targeted supplementation to optimize biological outcomes (22–24). These approaches will help improve the effectiveness of vitamin supplementation, mitigate potential side effects, and refine public health strategies and clinical treatment options.
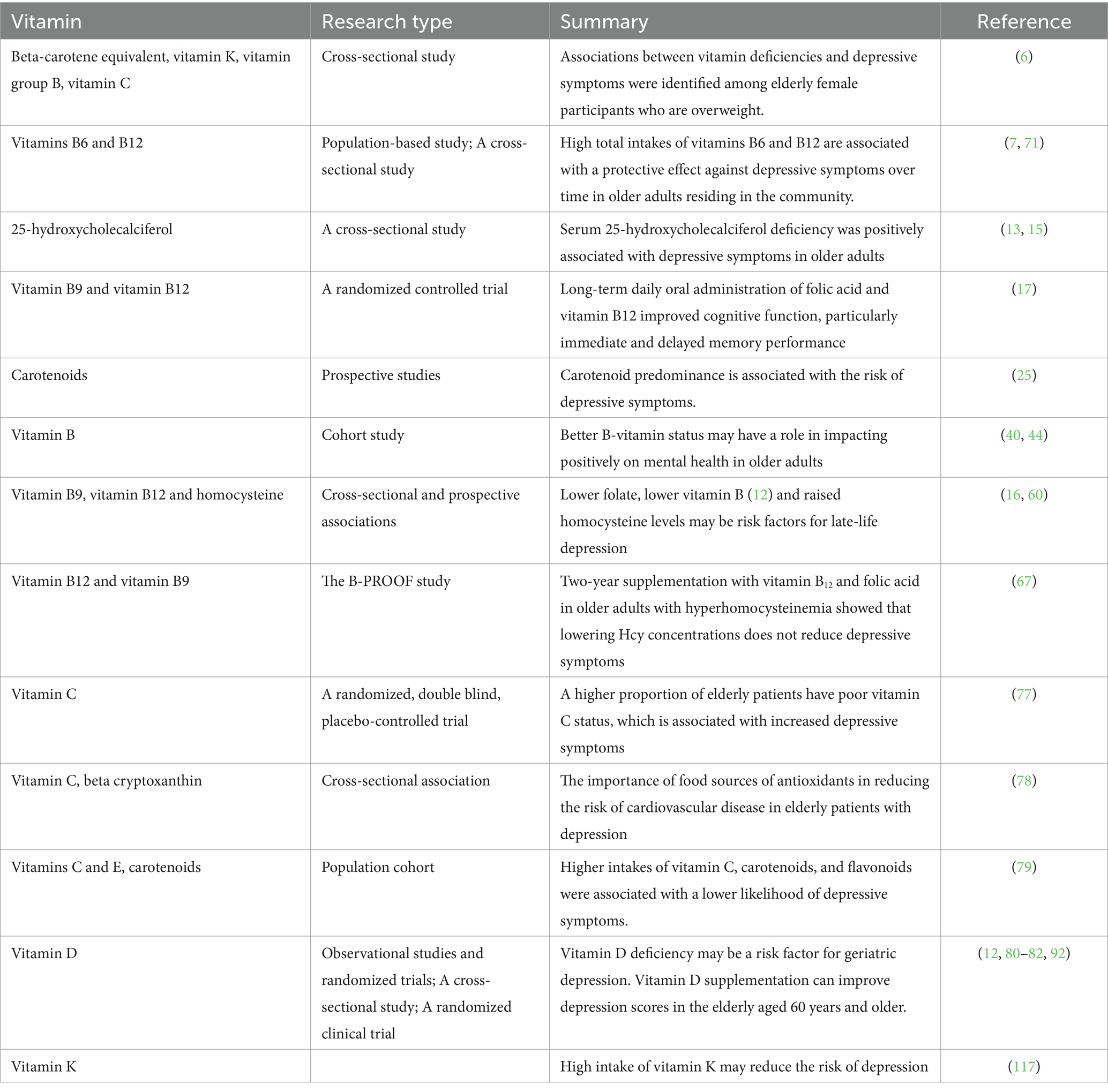
Table 1. Functions of vitamins.
Carotenoids are a class of fat-soluble pigments with antioxidant, immunomodulatory, and neuroprotective properties. They can be categorized into carotenes (such as α-carotene, β-carotene, γ-carotene, and lycopene) and xanthophylls (such as lutein, zeaxanthin, and β-cryptoxanthin) based on their chemical structure. Notably, α-carotene, β-carotene, γ-carotene, and β-cryptoxanthin function as provitamin A compounds, which can be metabolized to form vitamin A. Research has demonstrated that elevated plasma levels of zeaxanthin and β-carotene are significantly associated with a reduced risk of depression in older adults (25). Additionally, total carotenoid and β-carotene concentrations have been found to be negatively correlated with temporal lobe atrophy, indicating a potential protective effect against age-related neurodegeneration (26). Importantly, while skin carotene content is positively correlated with information processing speed, it does not appear to be associated with attention or executive function, suggesting its potential as a specific biomarker for cognitive decline. Retinol, a precursor to vitamin A, and retinoic acid (RA), a metabolite in the nervous system, play crucial roles by regulating synaptic plasticity (27) and neurotransmitter homeostasis. Differences in retinol receptor distribution in the adult human brain (28, 29) suggest its involvement in the functional regulation of emotion-related brain areas such as the hippocampus and amygdala. Further research has demonstrated that RA signaling is enriched in depression-related brain regions (30). The synaptic scaling effect mediated by RA (31) and homomorphic regulation mediated by the RARα receptor (32–34) may rapidly exert antidepressant effects by restoring neurotransmitter balance. While vitamins exhibit potential in the biological mechanisms and treatment strategies for LLD (Figure 1), concerns regarding species differences, dose-dependent effects, and potential toxicity risks must be addressed. Future studies should aim to establish more precise associations between their neuroregulatory pathways and clinical translational feasibility.
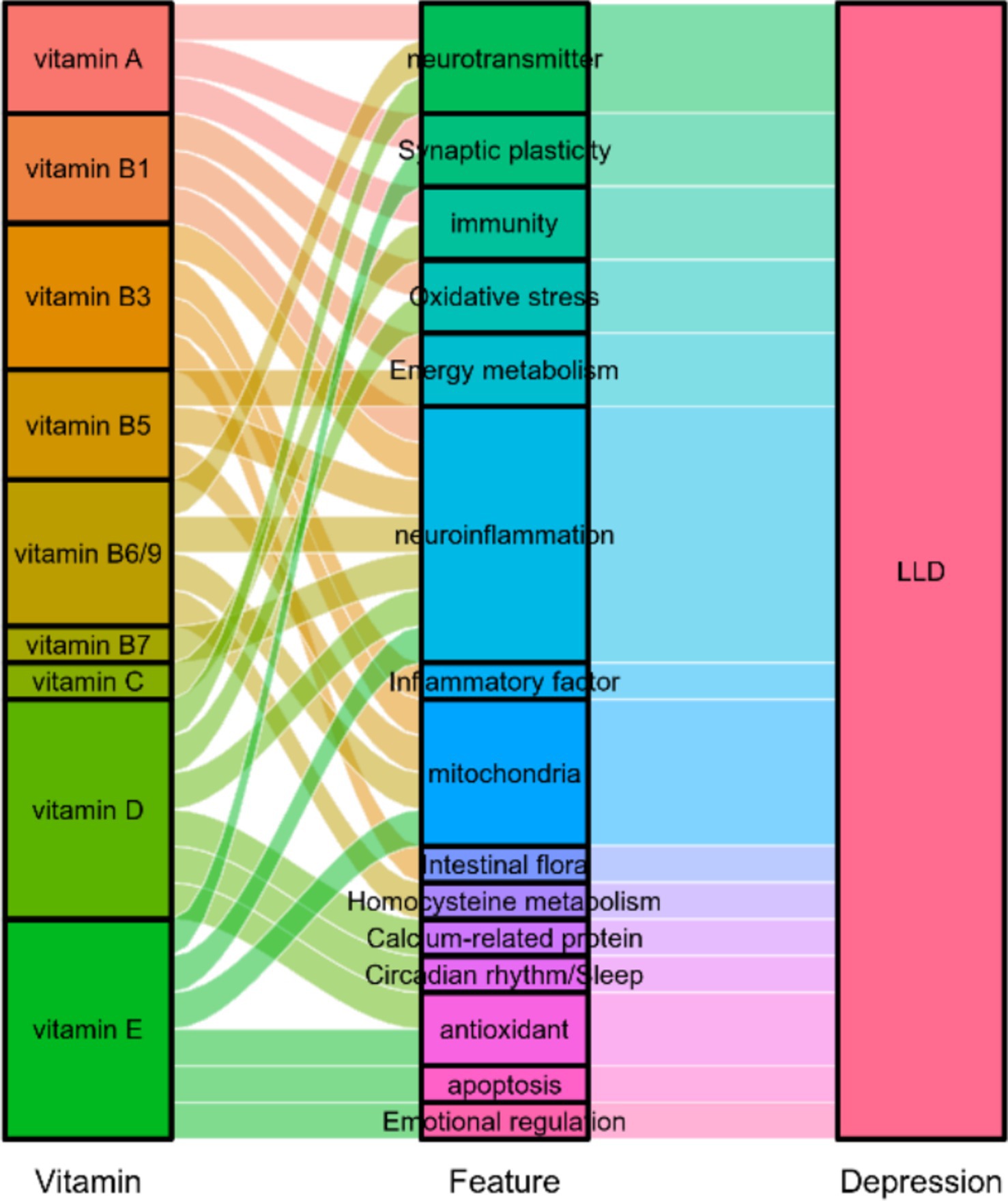
Figure 1. The potential role of vitamins in late-life depression.
As a family of water-soluble coenzymes, B vitamins play a central role in maintaining nervous system health by synergistically regulating key pathways of energy metabolism. Specifically, thiamine (Vitamin B1) catalyzes the oxidative decarboxylation reactions in the citric acid cycle, niacin (B3) facilitates oxidative phosphorylation via its role as NADH, pyridoxine (Vitamin B6) is crucial for amino acid metabolism, neurotransmitter synthesis, and lipid metabolism (35). Pantothenic acid (Vitamin B5) and biotin (Vitamin B7) function as coenzyme A and carboxylase cofactors, respectively, participating in the tricarboxylic acid cycle and fatty acid oxidation. Folic acid (Vitamin B9), in its reduced form as tetrahydrofolate, functions as an important cofactor in methylation reactions and as a carrier of carbon units in the synthesis of purines and pyrimidines (36, 37). This multi-target regulatory property makes B vitamins ideal candidates for addressing energy metabolism disturbances in LLD. Studies have demonstrated that LLD is closely associated with energy metabolism disorders, potentially stemming from impaired mitochondrial function and chronic inflammation, leading to neuronal apoptosis and oxidative stress (38). The brain, being an energy-intensive organ, relies heavily on ATP homeostasis maintained by B vitamins for processes such as synaptic transmission and neuroplasticity (39). Clinical evidence indicates that low levels of vitamin B1, B5, B6, and B9 are prevalent among LLD patients, with their deficiencies significantly correlated with the severity of depression and the rate of cognitive decline (6). Studies have shown that regular intake of fortified foods can optimize B vitamin status and thus help reduce depression (40) (Table 1). These findings underscore the multiple mechanisms of action and clinical application prospects of B vitamins in managing LLD. Restoring physiological levels of B vitamins through dietary supplementation or targeted interventions may offer new strategies to improve neuronal energy metabolism imbalance.
Vitamin B1, as a central regulator of energy metabolism, directly facilitates mitochondrial ATP production by catalyzing the activities of α-ketoglutarate dehydrogenase and pyruvate dehydrogenase complexes in the tricarboxylic acid (TCA) cycle through its active form, thiamine pyrophosphate (TPP) (41). In LLD, vitamin B1 deficiency can impair TCA cycle function, leading to disrupted energy metabolism in emotion-regulating brain regions such as the hippocampus and prefrontal cortex (37). This disruption may be a critical mechanism underlying fatigue and cognitive impairment in LLD patients. Clinical studies have demonstrated that thiamine supplementation enhances the activity of enzymes related to mitochondrial function (42–44) and significantly alleviates depressive symptoms (45). Notably, the neuroprotective effects of vitamin B1 extend beyond supporting energy metabolism; it also effectively mitigates neuroinflammation and oxidative stress by inhibiting the release of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6 (46–48). Observational studies further indicate that maintaining adequate levels of vitamin B1 is positively correlated with cognitive function, including attention, working memory, and emotional regulation (49, 50) (Figure 1). These findings suggest that vitamin B1 supplementation may offer potential therapeutic strategies for improving brain function in LLD patients by synergistically regulating energy metabolism and inflammatory responses.
Vitamin B3, also known as niacin, plays a critical role in energy metabolism and mitochondrial function, which is essential in the context of LLD. Vitamin B3 serves as a precursor to nicotinamide adenine dinucleotide (NAD+), a coenzyme vital for cellular redox reactions and energy production. Research by Lapatto et al. indicates that vitamin B3, specifically niacinamide riboside, may enhance muscle mitochondrial function and modulate gut microbiome composition in humans (51). Furthermore, studies have shown that vitamin B3 can reduce oxidative stress and neuroinflammation, both of which are closely linked to the pathogenesis of LLD (52). By improving mitochondrial function and mitigating oxidative damage, vitamin B3 may offer a therapeutic avenue for alleviating LLD symptoms and enhancing overall brain health in older adults. This underscores its potential as a supportive treatment and addresses the interplay between metabolic and inflammatory aspects of the disease. Additionally, Liu et al. suggest that vitamin B3’s modulation of ATP, independent of SIRT1 activity, could be a promising approach for treating depressive disorders (53). Consequently, vitamin B3 may serve as a beneficial intervention for depression in elderly patients with LLD.
Vitamin B5, also known as pantothenic acid, plays a crucial role in energy metabolism as it serves as a precursor to the synthesis of Coenzyme A. Coenzyme A is an essential cofactor in numerous biochemical reactions, particularly those involved in energy production and mitochondrial function (54). The significant connection between vitamin B5 and energy metabolism implies its potential to influence the pathophysiological processes of LLD by enhancing mitochondrial health and boosting energy production. Research has demonstrated that vitamin B5 facilitates mitochondrial respiration and metabolic maturation, and exerts a critical regulatory effect on intracellular energy homeostasis (55). Given that mitochondrial dysfunction is linked to LLD, the role of vitamin B5 in supporting mitochondrial function may offer a therapeutic avenue to alleviate depressive symptoms in older adults. Furthermore, vitamin B5 is implicated in the regulation of inflammation, a critical factor in the onset and progression of LLD. Chronic inflammation can induce neuronal apoptosis and oxidative stress, thereby exacerbating depression in the elderly (38). Vitamin B5 exerts its anti-inflammatory effects by decreasing levels of inflammatory mediators and facilitating a shift towards an anti-inflammatory pathway (56). This anti-inflammatory potential enables vitamin B5 to mitigate immune disorders associated with LLD and improve depressive symptoms and overall prognosis. By modulating energy metabolism and inflammation, vitamin B5 may play multifaceted roles in addressing the underlying biological mechanisms of LLD, offering a promising adjunctive treatment strategy.
Vitamin B7, also known as biotin, has been identified as a potential modulator of neuroinflammation and neurotransmitters, both of which are implicated in LLD. Reininghaus et al. demonstrated that a 4-week regimen of probiotics combined with biotin supplementation in patients with major depression resulted in significant clinical benefits (57). Biotin has been shown to ameliorate neuroinflammatory dysfunctions, and in animal models, a novel biotin complex called bionicotinate magnesium (MgB) improved social behavior, learning, and memory deficits (58). These findings suggest that vitamin B7 may help mitigate the inflammatory processes associated with LLD. Furthermore, the combination of manganese chloride and biotin has been found to upregulate brain CYP1B1 expression and reduce neurotoxicity, indicating a protective effect on neurotransmitter regulation and cerebrovascular homeostasis (59). These results indicate that vitamin B7 may support neurotransmitter balance, reduce neuroinflammatory responses, and thereby alleviate some symptoms of LLD. Although further scientific evidence is required to confirm the therapeutic potential of vitamin B7 in LLD, the preliminary findings highlight its promising role in addressing the complex physiological mechanisms underlying this condition.
LLD is a complex condition influenced by the interplay between biological and environmental factors. Its pathophysiological mechanisms involve homocysteine metabolism disorders, mitochondrial dysfunction, and neuroinflammatory cascades. Research has demonstrated that hyperhomocysteinemia can exacerbate depressive symptoms in elderly individuals by inducing neurovascular damage and oxidative stress (60–62). The methylation metabolic network, which includes vitamins B6, B9, and B12, plays a central regulatory role in this process. Specifically, vitamin B6 acts as a cofactor for cystathionine β-synthase, facilitating the conversion of homocysteine to cysteine (63, 64). Vitamin B12, through methionine synthase, remethylates homocysteine to methionine, influencing the synthesis of neurotransmitters such as dopamine and norepinephrine (65). Clinical evidence indicates that combined supplementation of B9 and B12 can significantly reduce elevated homocysteine levels (66); however, its effect on depressive symptoms remains controversial. For instance, De Koning et al. found no antidepressant effect during a 2-year intervention (67), while Skarupski et al. observed that higher dietary intake of B6 and B12 was associated with reduced depressive symptoms (7). A very recent study showed that the current minimum recommendations were not designed for optimal cognitive function or longevity as participants with B12 levels deemed adequate by today‘s medical standards showed clear signs of neurological impairment, while healthy older adults (averaging 71 years of age) who did not have dementia or mild cognitive impairment averaged B12 levels at 414.8 pmol/L, much higher than the recommended minimum level (68). This inconsistency may be attributed to differences in study design, such as intervention duration or baseline nutritional status, or brain region-specific metabolic responses. Importantly, the role of B vitamins extends beyond homocysteine regulation. Vitamin B6 targets neurotransmitter imbalances and neuroinflammation by participating in 5-hydroxytryptamine synthesis (69, 70) and inhibiting the NF-κB pathway (9, 56). Cohort studies have further demonstrated that insufficient vitamin B6 intake is positively correlated with increased depression severity in middle-aged and older women (71). Additionally, deficiencies in both vitamins B6 and B9 are dose-dependently associated with cognitive decline and changes in brain structure (72, 73). While existing evidence underscores the multi-target potential of B vitamins in preventing and treating LLD, it remains essential to establish a therapeutic window and biomarker-guided personalized application strategies through standardized intervention trials.
Vitamin C (ascorbic acid), a crucial water-soluble antioxidant, exerts multidimensional protective effects on the health of the elderly by scavenging free radicals, promoting collagen synthesis, and modulating immune function. Research has demonstrated that short-term vitamin C supplementation can significantly enhance immune function in older adults (74). Moreover, dietary intake of vitamin C is inversely associated with the incidence of depression, particularly among elderly women (75, 76). Clinical observations further indicate that vitamin C deficiency is not only strongly linked to increased depressive symptoms following acute illness (77) but may also accelerate cognitive decline and increase susceptibility to infections. Notably, inadequate vitamin C intake is prevalent among the elderly globally, especially among those with limited access to fresh fruits and vegetables (78, 79). Therefore, implementing vitamin C fortification interventions for high-risk groups could serve as an important public health strategy to improve the quality of life of the elderly and reduce disease burden.
Vitamin D is a fat-soluble vitamin, with its metabolically active form, 1,25-dihydroxyvitamin D3 (1,25(OH)2D3), exerting neuroprotective effects via the vitamin D receptor (VDR), which is widely distributed in the cerebral cortex, cerebellum, and substantia nigra. Research has demonstrated a significant association between vitamin D deficiency and the occurrence of depressive symptoms in elderly individuals, particularly during seasons with low sunlight exposure (80, 81) (Table 1). Longitudinal studies have further confirmed that fluctuations in vitamin D levels can predict the development of depressive symptoms (12, 82). The antidepressant mechanisms of vitamin D involve multi-pathway regulation: maintaining neuronal function by regulating calcium ion homeostasis-associated proteins (83–85); enhancing the expression of tryptophan hydroxylase 2 (TPH2) through VDR activation, thereby promoting serotonin synthesis and inhibiting its metabolism to enhance monoaminergic neurotransmission (86–89); upregulating antioxidant genes such as NRF2 and inhibiting the inflammatory pathway of NF-κB, thus alleviating nerve oxidative damage (90, 91). Additionally, vitamin D influences circadian rhythms by modulating the serotonin-melatonin conversion axis and exerts potential protective effects through interactions with sex hormones (92). Clinical intervention studies have shown that supplementation with vitamin D3, combined with vitamins B6 and K1, effectively alleviates oxidative stress (93), and meta-analyses support its potential to improve depressive symptoms (94). However, other studies have shown that neither vitamin D3 nor omega-3 has shown any benefit for targeted and selective prevention of depression in the elderly (95). It is noteworthy that although vitamin D is one of the least toxic vitamins, excessive intake can lead to adverse clinical symptoms such as confusion, apathy, recurrent vomiting, and abdominal pain (96). Therefore, vitamin D intake should be maintained within a reasonable range. In summary, vitamin D deficiency is a risk factor for exacerbating depression in old age by interfering with neurotransmitter balance, calcium signaling, and antioxidant defense systems (Figure 1).
Vitamin E is a group of eight vitamers, four tocopherols and four tocotrienols, and both occur in alpha, beta, gamma, and delta forms. It exerts its neuroprotective effects through a multifaceted regulatory mechanism: by scavenging free radicals, it alleviates oxidative stress damage; additionally, it enhances mitochondrial energy metabolism efficiency (97, 98); modulates signaling pathways associated with synaptic plasticity, thereby influencing emotional and cognitive functions (99); and inhibits inflammatory pathways such as NF-κB, reducing neuroinflammatory responses mediated by microglia activation (100–102). Preclinical studies have confirmed that vitamin E supplementation significantly mitigates anxiety-like behaviors (103, 104) and reverses age-related immune disorders (105–107). Vitamin E plays a protective role in the pathological process of LLD via two mechanisms: first, it suppresses the expression of apoptosis-related molecules such as caspase-3, preserving neuronal structural integrity; second, it promotes hippocampal neurogenesis and repairs emotion-related neural circuits (108, 109). Observational studies further revealed a significant negative association between combined dietary intake of vitamins E and C and the incidence of depression (110). Collectively, these findings suggest that vitamin E may be a key nutrient in multi-target intervention strategies for LLD by synergistically regulating REDOX balance, inflammatory cascades, and apoptosis processes (Figure 1).
As a neuroprotective, fat-soluble vitamin, vitamin K in its active form methylnaphthoquinone-4 (MK-4) performs multiple biological functions in the central nervous system by participating in sphingoid metabolism. These functions include promoting nerve growth factor expression, regulating myelin formation, and maintaining neuronal homeostasis (111). Epidemiological studies have demonstrated that vitamin K intake is significantly negatively correlated with depressive symptoms (112). The underlying mechanisms involve multi-pathway synergistic regulation: down-regulating pro-inflammatory factors such as IL-1β and IL-6 while up-regulating IL-10 (113), thereby blocking the neuroinflammatory cascade (114); inhibiting lipid peroxidation and ferroptosis to maintain redox balance (115); activating the Sirt1-PGC-1α-TFAM signaling axis to enhance mitochondrial biogenesis and improve energy metabolism disorders (116). Notably, vitamin K2 alleviates LLD-related cognitive impairment and mood disorders by regulating mitochondrial autophagy and neurotransmitter homeostasis, particularly within the serotonin system (65). Although the direct causal relationship between vitamin K and LLD remains to be confirmed, existing evidence suggests that targeting the “inflammatory-oxidative-mitochondrial” pathological axis offers new insights for precision nutritional interventions for depression in older adults (6, 115, 117).
Vitamin supplements have shown multi-target intervention potential in managing LLD by modulating biological mechanisms such as neurotransmitter metabolism, inflammatory pathways, and oxidative stress. Existing studies have confirmed that specific nutrients, including vitamin D, B complex vitamins, and vitamin C, can alleviate mood disorders through enhancing neuroplasticity, regulating homocysteine metabolism, and scavenging free radicals, respectively. However, the heterogeneity of clinical trial results, particularly dose-dependent variations in vitamin D efficacy, underscores the need for cautious interpretation of available evidence. Standardization of study design, including baseline nutritional status assessment and controlled intervention cycles, along with population stratification based on chronic comorbidities, will be crucial to overcoming current limitations. Future research should focus on three key dimensions: (1) Establishing quantitative models linking nutrients, biomarkers, and clinical symptoms; (2) Investigating the synergistic effects of vitamin supplementation combined with psychological or pharmacological interventions; and (3) Developing personalized supplementation strategies based on metabolomics characteristics. These advancements will facilitate the transition from empirical supplementation to precise intervention in nutritional psychiatry, providing a theoretical foundation for a multi-modal treatment system for geriatric depression.
YG: Conceptualization, Data curation, Formal analysis, Writing – original draft. X-NS: Conceptualization, Formal analysis, Writing – original draft. Z-PW: Visualization, Software, Writing – review & editing. J-ZH: Data curation, Writing – review & editing. X-ZD: Writing – review & editing. J-HZ: Supervision, Writing – review & editing. SL: Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Natural Science Foundation of China (82271546, 82301725); National Key Research and Development Program of China (2023YFC2506201); Key Project of Science and Technology Innovation 2030 of China (2021ZD0201805); China Postdoctoral Science Foundation (2023M732155); Fundamental Research Program of Shanxi Province (202203021212028); Research Project Supported by Shanxi Scholarship Council of China (20240041, 2022-190); Shanxi Provincial Administration of Traditional Chinese Medicine (2023ZYYC2034), Science and technology innovation project of higher education in Shanxi Province (2020L0204, 2022L132); Shanxi Medical University School-level Doctoral Initiation Fund Project (XD2102); Youth Project of First Hospital of Shanxi Medical University (YQ2203); Doctor Fund Project of Shanxi Medical University in Shanxi Province (SD2216); Shanxi Science and Technology Innovation Talent Team (202304051001049).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Uysal Cesur, N, and Poyraz, B. Three-year prognosis of late-life depression in an outpatient geriatric psychiatry clinic: medical comorbidities worsen outcomes. Psychiatry Q. (2023) 94:675–89. doi: 10.1007/s11126-023-10053-8
2. Evans-Lacko, S, Aguilar-Gaxiola, S, Al-Hamzawi, A, Alonso, J, Benjet, C, Bruffaerts, R, et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO world mental health (WMH) surveys. Psychol Med. (2018) 48:1560–71. doi: 10.1017/S0033291717003336
3. Marawi, T, Ainsworth, NJ, Zhukovsky, P, Rashidi-Ranjbar, N, Rajji, TK, Tartaglia, MC, et al. Brain-cognition relationships in late-life depression: a systematic review of structural magnetic resonance imaging studies. Transl Psychiatry. (2023) 13:284. doi: 10.1038/s41398-023-02584-2
4. Lin, CH, Wang, SH, and Lane, HY. Effects of sodium benzoate, a D-amino acid oxidase inhibitor, on perceived stress and cognitive function among patients with late-life depression: a randomized, double-blind, sertraline-and placebo-controlled trial. Int J Neuropsychopharmacol. (2022) 25:545–55. doi: 10.1093/ijnp/pyac006
5. Woo, YS, Kim, S, Jeong, JH, Jung, YE, Kim, MD, and Bahk, WM. Vitamin D deficiency/insufficiency among inpatients with depressive symptoms. Clin Psychopharmacol Neurosci. (2019) 17:121–4. doi: 10.9758/cpn.2019.17.1.121
6. Nguyen, TTT, Tsujiguchi, H, Kambayashi, Y, Hara, A, Miyagi, S, Yamada, Y, et al. Relationship between Vitamin intake and depressive symptoms in elderly Japanese individuals: differences with gender and body mass index. Nutrients. (2017) 9:1319. doi: 10.3390/nu9121319
7. Skarupski, KA, Tangney, C, Li, H, Ouyang, B, Evans, DA, and Morris, MC. Longitudinal association of vitamin B-6, folate, and vitamin B-12 with depressive symptoms among older adults over time. Am J Clin Nutr. (2010) 92:330–5. doi: 10.3945/ajcn.2010.29413
8. Xie, X, Yu, C, Zhou, J, Xiao, Q, Shen, Q, Xiong, Z, et al. Nicotinamide mononucleotide ameliorates the depression-like behaviors and is associated with attenuating the disruption of mitochondrial bioenergetics in depressed mice. J Affect Disord. (2020) 263:166–74. doi: 10.1016/j.jad.2019.11.147
9. Zheng, Z, Wang, H, Chen, Z, Gao, H, Gao, P, Gao, J, et al. Impact of chronic sleep deprivation on male reproductive health: insights from testicular and epididymal responses in mice. Andrology. (2024). doi: 10.1111/andr.13718
10. Chatterjee, R, Fuss, P, Vickery, EM, LeBlanc, ES, Sheehan, PR, Lewis, MR, et al. Vitamin D supplementation for prevention of Cancer: the D2d Cancer outcomes (D2dCA) ancillary study. J Clin Endocrinol Metab. (2021) 106:2767–78. doi: 10.1210/clinem/dgab153
11. Pei, YY, Zhang, Y, Peng, XC, Liu, ZR, Xu, P, and Fang, F. Association of Vitamin D Supplementation with cardiovascular events: a systematic review and Meta-analysis. Nutrients. (2022) 14:3158. doi: 10.3390/nu14153158
12. Alavi, NM, Khademalhoseini, S, Vakili, Z, and Assarian, F. Effect of vitamin D supplementation on depression in elderly patients: a randomized clinical trial. Clin Nutr. (2019) 38:2065–70. doi: 10.1016/j.clnu.2018.09.011
13. Ceolin, G, Matsuo, LH, Confortin, SC, D'Orsi, E, Rieger, DK, and Moreira, JD. Lower serum 25-hydroxycholecalciferol is associated with depressive symptoms in older adults in southern Brazil. Nutr J. (2020) 19:123. doi: 10.1186/s12937-020-00638-5
14. Almeida, OP, Hankey, GJ, Yeap, BB, Golledge, J, and Flicker, L. Vitamin D concentration and its association with past, current and future depression in older men: the health in men study. Maturitas. (2015) 81:36–41. doi: 10.1016/j.maturitas.2015.01.016
15. Williams, JA, Sink, KM, Tooze, JA, Atkinson, HH, Cauley, JA, Yaffe, K, et al. Low 25-hydroxyvitamin D concentrations predict incident depression in well-functioning older adults: the health, aging, and body composition study. J Gerontol A Biol Sci Med Sci. (2015) 70:757–63. doi: 10.1093/gerona/glu184
16. Lee, HK, Kim, SY, and Sok, SR. Effects of multivitamin supplements on cognitive function, serum homocysteine level, and depression of Korean older adults with mild cognitive impairment in care facilities. J Nurs Scholarsh. (2016) 48:223–31. doi: 10.1111/jnu.12201
17. Walker, JG, Batterham, PJ, Mackinnon, AJ, Jorm, AF, Hickie, I, Fenech, M, et al. Oral folic acid and vitamin B-12 supplementation to prevent cognitive decline in community-dwelling older adults with depressive symptoms—the beyond ageing project: a randomized controlled trial. Am J Clin Nutr. (2012) 95:194–203. doi: 10.3945/ajcn.110.007799
18. Fairbairn, P, Dyall, SC, and Tsofliou, F. The effects of multi-nutrient formulas containing a combination of n-3 PUFA and B vitamins on cognition in the older adult: a systematic review and meta-analysis. Br J Nutr. (2023) 129:428–41. doi: 10.1017/S0007114522001283
19. Li, M, Li, W, Gao, Y, Chen, Y, Bai, D, Weng, J, et al. Effect of folic acid combined with docosahexaenoic acid intervention on mild cognitive impairment in elderly: a randomized double-blind, placebo-controlled trial. Eur J Nutr. (2021) 60:1795–808. doi: 10.1007/s00394-020-02373-3
20. Zhong, X, Xiong, Y, Wei, D, Wang, S, Xiao, Z, Liu, M, et al. The influence of maternal vitamin D supplementation on infant vitamin D status: a systematic review and meta-analyses. Complement Ther Med. (2020) 52:102491. doi: 10.1016/j.ctim.2020.102491
21. Pecriaux, C. Interest of vitamin b6 for treatment of nausea and/or vomiting during pregnancy. Gynecol Obstet Fertil Senol. (2020) 48:840–3. doi: 10.1016/j.gofs.2020.09.005
22. Opie, RS, Itsiopoulos, C, Parletta, N, Sanchez-Villegas, A, Akbaraly, TN, Ruusunen, A, et al. Dietary recommendations for the prevention of depression. Nutr Neurosci. (2017) 20:161–71. doi: 10.1179/1476830515Y.0000000043
23. LaChance, LR, and Ramsey, D. Antidepressant foods: an evidence-based nutrient profiling system for depression. World J Psychiatry. (2018) 8:97–104. doi: 10.5498/wjp.v8.i3.97
24. Taylor, AM, and Holscher, HD. A review of dietary and microbial connections to depression, anxiety, and stress. Nutr Neurosci. (2020) 23:237–50. doi: 10.1080/1028415X.2018.1493808
25. Bardinet, J, Pouchieu, C, Chuy, V, Helmer, C, Etheve, S, Gaudout, D, et al. Plasma carotenoids and risk of depressive symptomatology in a population-based cohort of older adults. J Affect Disord. (2023) 339:615–23. doi: 10.1016/j.jad.2023.07.076
26. Thomas, A, Proust-Lima, C, Baillet, M, Helmer, C, Delcourt, C, Foubert-Samier, A, et al. Plasma carotenoids and medial temporal lobe atrophy in older adults. Clin Nutr. (2021) 40:2460–3. doi: 10.1016/j.clnu.2020.09.056
27. Fragoso, YD, Shearer, KD, Sementilli, A, de Carvalho, LV, and McCaffery, PJ. High expression of retinoic acid receptors and synthetic enzymes in the human hippocampus. Brain Struct Funct. (2012) 217:473–83. doi: 10.1007/s00429-011-0359-0
28. Lane, MA, and Bailey, SJ. Role of retinoid signalling in the adult brain. Prog Neurobiol. (2005) 75:275–93. doi: 10.1016/j.pneurobio.2005.03.002
29. Mey, J, and McCaffery, P. Retinoic acid signaling in the nervous system of adult vertebrates. Neuroscientist. (2004) 10:409–21. doi: 10.1177/1073858404263520
30. Bremner, JD, and McCaffery, P. The neurobiology of retinoic acid in affective disorders. Prog Neuro-Psychopharmacol Biol Psychiatry. (2008) 32:315–31. doi: 10.1016/j.pnpbp.2007.07.001
31. Suzuki, K, Kim, JW, Nosyreva, E, Kavalali, ET, and Monteggia, LM. Convergence of distinct signaling pathways on synaptic scaling to trigger rapid antidepressant action. Cell Rep. (2021) 37:109918. doi: 10.1016/j.celrep.2021.109918
32. Wang, HL, Zhang, Z, Hintze, M, and Chen, L. Decrease in calcium concentration triggers neuronal retinoic acid synthesis during homeostatic synaptic plasticity. J Neurosci Off J Soc Neurosci. (2011) 31:17764–71. doi: 10.1523/JNEUROSCI.3964-11.2011
33. Aoto, J, Nam, CI, Poon, MM, Ting, P, and Chen, L. Synaptic signaling by all-trans retinoic acid in homeostatic synaptic plasticity. Neuron. (2008) 60:308–20. doi: 10.1016/j.neuron.2008.08.012
34. Thapliyal, S, Arendt, KL, Lau, AG, and Chen, L. Retinoic acid-gated BDNF synthesis in neuronal dendrites drives presynaptic homeostatic plasticity. eLife. (2022) 11:11. doi: 10.7554/eLife.79863
35. Hellmann, H, and Mooney, S. Vitamin B6: a molecule for human health? Molecules. (2010) 15:442–59. doi: 10.3390/molecules15010442
37. Depeint, F, Bruce, WR, Shangari, N, Mehta, R, and O'Brien, PJ. Mitochondrial function and toxicity: role of the B vitamin family on mitochondrial energy metabolism. Chem Biol Interact. (2006) 163:94–112. doi: 10.1016/j.cbi.2006.04.014
38. Leonard, BE. Major depression as a Neuroprogressive prelude to dementia: what is the evidence? Mod Trends Pharmacopsychiatry. (2017) 31:56–66. doi: 10.1159/000470807
39. Harper, DG, Joe, EB, Jensen, JE, Ravichandran, C, and Forester, BP. Brain levels of high-energy phosphate metabolites and executive function in geriatric depression. Int J Geriatr Psychiatry. (2016) 31:1241–9. doi: 10.1002/gps.4439
40. Moore, K, Hughes, CF, Hoey, L, Ward, M, Cunningham, C, Molloy, AM, et al. B-vitamins in relation to depression in older adults over 60 years of age: the trinity Ulster Department of Agriculture (TUDA) cohort study. J Am Med Dir Assoc. (2019) 20:551–7.e1. doi: 10.1016/j.jamda.2018.11.031
41. Ho, TCS, Chan, AHY, and Leeper, FJ. Triazole-based thiamine analogues as inhibitors of thiamine pyrophosphate-dependent enzymes: 1, 3-Dicarboxylate for metal binding. ACS Omega. (2024) 9:42245–52. doi: 10.1021/acsomega.4c04594
42. Mrowicka, M, Mrowicki, J, Dragan, G, and Majsterek, I. The importance of thiamine (vitamin B1) in humans. Biosci Rep. (2023) 43:BSR20230374. doi: 10.1042/BSR20230374
43. Ghaleiha, A, Davari, H, Jahangard, L, Haghighi, M, Ahmadpanah, M, Seifrabie, MA, et al. Adjuvant thiamine improved standard treatment in patients with major depressive disorder: results from a randomized, double-blind, and placebo-controlled clinical trial. Eur Arch Psychiatry Clin Neurosci. (2016) 266:695–702. doi: 10.1007/s00406-016-0685-6
44. Zhang, G, Ding, H, Chen, H, Ye, X, Li, H, Lin, X, et al. Thiamine nutritional status and depressive symptoms are inversely associated among older Chinese adults. J Nutr. (2013) 143:53–8. doi: 10.3945/jn.112.167007
45. Palmieri, F, Monné, M, Fiermonte, G, and Palmieri, L. Mitochondrial transport and metabolism of the vitamin B‐derived cofactors thiamine pyrophosphate, coenzyme a,FADandNAD+, and related diseases: a review. IUBMB Life. (2022) 74:592–617. doi: 10.1002/iub.2612
46. Wang, J, Yu, Z, Peng, Y, and Xu, B. Insights into prevention mechanisms of bioactive components from healthy diets against Alzheimer's disease. J Nutr Biochem. (2023) 119:109397. doi: 10.1016/j.jnutbio.2023.109397
47. Vemuganti, R, Kalluri, H, Yi, JH, Bowen, KK, and Hazell, AS. Gene expression changes in thalamus and inferior colliculus associated with inflammation, cellular stress, metabolism and structural damage in thiamine deficiency. Eur J Neurosci. (2006) 23:1172–88. doi: 10.1111/j.1460-9568.2006.04651.x
48. Mikkelsen, K, Stojanovska, L, Prakash, M, and Apostolopoulos, V. The effects of vitamin B on the immune/cytokine network and their involvement in depression. Maturitas. (2017) 96:58–71. doi: 10.1016/j.maturitas.2016.11.012
49. Lu, J, Pan, X, Fei, G, Wang, C, Zhao, L, Sang, S, et al. Correlation of thiamine metabolite levels with cognitive function in the non-demented elderly. Neurosci Bull. (2015) 31:676–84. doi: 10.1007/s12264-015-1563-3
50. Nardone, R, Höller, Y, Storti, M, Christova, M, Tezzon, F, Golaszewski, S, et al. Thiamine deficiency induced neurochemical, neuroanatomical, and neuropsychological alterations: a reappraisal. ScientificWorldJournal. (2013) 2013:309143. doi: 10.1155/2013/309143
51. Lapatto, HAK, Kuusela, M, Heikkinen, A, Muniandy, M, van der Kolk, BW, Gopalakrishnan, S, et al. Nicotinamide riboside improves muscle mitochondrial biogenesis, satellite cell differentiation, and gut microbiota in a twin study. Sci Adv. (2023) 9:eadd5163. doi: 10.1126/sciadv.add5163
52. Marmolejo-Garza, A, Chatre, L, Croteau, DL, Herron-Bedoya, A, Luu, MDA, Bernay, B, et al. Nicotinamide riboside modulates the reactive species interactome, bioenergetic status and proteomic landscape in a brain-region-specific manner. Neurobiol Dis. (2024) 200:106645. doi: 10.1016/j.nbd.2024.106645
53. Liu, Z, Li, C, Fan, X, Kuang, Y, Zhang, X, Chen, L, et al. Nicotinamide, a vitamin B3 ameliorates depressive behaviors independent of SIRT1 activity in mice. Mol Brain. (2020) 13:162. doi: 10.1186/s13041-020-00703-4
54. Moiseenok, AG, and Kanunnikova, NP. Brain CoA and acetyl CoA metabolism in mechanisms of neurodegeneration. Biochemistry (Mosc). (2023) 88:466–80. doi: 10.1134/S000629792304003X
55. Takeda, Y, and Dai, P. Functional roles of pantothenic acid, riboflavin, thiamine, and choline in adipocyte browning in chemically induced human brown adipocytes. Sci Rep. (2024) 14:18252. doi: 10.1038/s41598-024-69364-w
56. Rakić, M, Lunić, T, Bekić, M, Tomić, S, Mitić, K, Graovac, S, et al. Vitamin B complex suppresses neuroinflammation in activated microglia: in vitro and in silico approach combined with dynamical modeling. Int Immunopharmacol. (2023) 121:110525. doi: 10.1016/j.intimp.2023.110525
57. Reininghaus, EZ, Platzer, M, Kohlhammer-Dohr, A, Hamm, C, Mörkl, S, Bengesser, SA, et al. PROVIT: supplementary probiotic treatment and Vitamin B7 in depression-a randomized controlled trial. Nutrients. (2020) 12:3422. doi: 10.3390/nu12113422
58. Sahin, K, Orhan, C, Karatoprak, S, Tuzcu, M, Deeh, PBD, Ozercan, IH, et al. Therapeutic effects of a novel form of biotin on propionic acid-induced autistic features in rats. Nutrients. (2022) 14:1280. doi: 10.3390/nu14061280
59. Wu, J, Li, Y, Tian, S, Na, S, Wei, H, Wu, Y, et al. CYP1B1 affects the integrity of the blood-brain barrier and oxidative stress in the striatum: an investigation of manganese-induced neurotoxicity. CNS Neurosci Ther. (2024) 30:e14633. doi: 10.1111/cns.14633
60. Wei, MD, Huang, YY, Zeng, Y, Lan, YX, Lu, K, Wang, Y, et al. Homocysteine modulates social isolation-induced depressive-like behaviors through BDNF in aged mice. Mol Neurobiol. (2023) 60:4924–34. doi: 10.1007/s12035-023-03377-w
61. Kim, JM, Stewart, R, Kim, SW, Yang, SJ, Shin, IS, and Yoon, JS. Predictive value of folate, vitamin B12 and homocysteine levels in late-life depression. Br J Psychiatry J Ment Sci. (2008) 192:268–74. doi: 10.1192/bjp.bp.107.039511
62. Kuo, HK, Sorond, FA, Chen, JH, Hashmi, A, Milberg, WP, and Lipsitz, LA. The role of homocysteine in multisystem age-related problems: a systematic review. J Gerontol A Biol Sci Med Sci. (2005) 60:1190–201. doi: 10.1093/gerona/60.9.1190
63. Prasad, K. Atherogenic effect of homocysteine, a biomarker of inflammation and its treatment. Int J Angiol. (2024) 33:262–70. doi: 10.1055/s-0044-1788280
64. Philipp, TM, Bottiglieri, T, Clapper, W, Liu, K, Rodems, S, Szabo, C, et al. Mechanism of action and impact of thiol homeostasis on efficacy of an enzyme replacement therapy for classical homocystinuria. Redox Biol. (2024) 77:103383. doi: 10.1016/j.redox.2024.103383
65. Tang, H, Zheng, Z, Wang, H, Wang, L, Zhao, G, and Wang, P. Vitamin K2 modulates mitochondrial dysfunction induced by 6-Hydroxydopamine in SH-SY5Y cells via mitochondrial quality-control loop. Nutrients. (2022) 14:1504. doi: 10.3390/nu14071504
66. Smith, AD, Smith, SM, de Jager, CA, Whitbread, P, Johnston, C, Agacinski, G, et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. (2010) 5:e12244. doi: 10.1371/journal.pone.0012244
67. de Koning, EJ, van der Zwaluw, NL, van Wijngaarden, JP, Sohl, E, Brouwer-Brolsma, EM, van Marwijk, HW, et al. Effects of two-year Vitamin B (12) and folic acid supplementation on depressive symptoms and quality of life in older adults with elevated homocysteine concentrations: additional results from the B-PROOF study, an RCT. Nutrients. (2016) 8:748. doi: 10.3390/nu8110748
68. Beaudry-Richard, A, Abdelhak, A, Saloner, R, Sacco, S, Montes, SC, Oertel, FC, et al. Vitamin B12 levels association with functional and structural biomarkers of central nervous system injury in older adults. Ann Neurol. (2025). doi: 10.1002/ana.27200
69. Vernì, F. Vitamin B6 and diabetes and its role in counteracting advanced glycation end products. Vitam Horm. (2024) 125:401–38. doi: 10.1016/bs.vh.2024.02.005
70. Śliwiński, W, and Gawlik-Kotelnicka, O. Circulating B vitamins metabolites in depressive disorders – connections with the microbiota-gut-brain axis. Behav Brain Res. (2024) 472:115145. doi: 10.1016/j.bbr.2024.115145
71. Odai, T, Terauchi, M, Suzuki, R, Kato, K, Hirose, A, and Miyasaka, N. Depressive symptoms in middle-aged and elderly women are associated with a Low intake of Vitamin B6: a cross-sectional study. Nutrients. (2020) 12:3437. doi: 10.3390/nu12113437
72. Selhub, J, Troen, A, and Rosenberg, IH. B vitamins and the aging brain. Nutr Rev. (2010) 68:S112–8. doi: 10.1111/j.1753-4887.2010.00346.x
73. Tucker, KL, Qiao, N, Scott, T, Rosenberg, I, and Spiro, A 3rd. High homocysteine and low B vitamins predict cognitive decline in aging men: the veterans affairs normative aging study. Am J Clin Nutr. (2005) 82:627–35. doi: 10.1093/ajcn.82.3.627
74. De la Fuente, M, Sánchez, C, Vallejo, C, Díaz-Del Cerro, E, Arnalich, F, and Hernanz, Á. Vitamin C and vitamin C plus E improve the immune function in the elderly. Exp Gerontol. (2020) 142:111118. doi: 10.1016/j.exger.2020.111118
75. Wang, A, Luo, J, Zhang, T, and Zhang, D. Dietary Vitamin C and Vitamin C derived from vegetables are inversely associated with the risk of depressive symptoms among the general population. Antioxidants (Basel). (2021) 10:1984. doi: 10.3390/antiox10121984
76. Zhao, D, Long, X, and Wang, J. Association of dietary vitamin C intake with depression in adults: a cross-sectional study of NHANES from 2005 to 2020. J Affect Disord. (2024) 358:113–20. doi: 10.1016/j.jad.2024.05.032
77. Gariballa, S. Poor vitamin C status is associated with increased depression symptoms following acute illness in older people. Int J Vitam Nutr Res. (2014) 84:12–7. doi: 10.1024/0300-9831/a000188
78. Payne, ME, Steck, SE, George, RR, and Steffens, DC. Fruit, vegetable, and antioxidant intakes are lower in older adults with depression. J Acad Nutr Diet. (2012) 112:2022–7. doi: 10.1016/j.jand.2012.08.026
79. Li, H, Sheng, LT, Tai, BC, Pan, A, and Koh, WP. Association between dietary antioxidant capacity in midlife and depressive symptoms in late life: The Singapore Chinese health study. Antioxidants (Basel). (2024) 13:576. doi: 10.3390/antiox13050576
80. Okereke, OI, and Singh, A. The role of vitamin D in the prevention of late-life depression. J Affect Disord. (2016) 198:1–14. doi: 10.1016/j.jad.2016.03.022
81. Albolushi, T, Bouhaimed, M, and Spencer, J. Lower blood Vitamin D levels are associated with depressive symptoms in a population of older adults in Kuwait: a cross-sectional study. Nutrients. (2022) 14:1548. doi: 10.3390/nu14081548
82. Di Gessa, G, Biddulph, JP, Zaninotto, P, and de Oliveira, C. Changes in vitamin D levels and depressive symptoms in later life in England. Sci Rep. (2021) 11:7724. doi: 10.1038/s41598-021-87432-3
83. Berridge, MJ. Vitamin D and depression: cellular and regulatory mechanisms. Pharmacol Rev. (2017) 69:80–92. doi: 10.1124/pr.116.013227
84. Bivona, G, Agnello, L, Bellia, C, Iacolino, G, Scazzone, C, Lo Sasso, B, et al. Non-skeletal activities of Vitamin D: From physiology to brain pathology. Medicina (Kaunas). (2019) 55:341. doi: 10.3390/medicina55070341
85. Croarkin, PE, Levinson, AJ, and Daskalakis, ZJ. Evidence for GABAergic inhibitory deficits in major depressive disorder. Neurosci Biobehav Rev. (2011) 35:818–25. doi: 10.1016/j.neubiorev.2010.10.002
86. Kaneko, I, Sabir, MS, Dussik, CM, Whitfield, GK, Karrys, A, Hsieh, JC, et al. 1, 25-Dihydroxyvitamin D regulates expression of the tryptophan hydroxylase 2 and leptin genes: implication for behavioral influences of vitamin D. FASEB J. (2015) 29:4023–35. doi: 10.1096/fj.14-269811
87. Sabir, MS, Haussler, MR, Mallick, S, Kaneko, I, Lucas, DA, Haussler, CA, et al. Optimal vitamin D spurs serotonin: 1, 25-dihydroxyvitamin D represses serotonin reuptake transport (SERT) and degradation (MAO-A) gene expression in cultured rat serotonergic neuronal cell lines. Genes Nutr. (2018) 13:19. doi: 10.1186/s12263-018-0605-7
88. Domínguez-López, S, Howell, R, and Gobbi, G. Characterization of serotonin neurotransmission in knockout mice: implications for major depression. Rev Neurosci. (2012) 23:429–43. doi: 10.1515/revneuro-2012-0044
89. Renteria, K, Nguyen, H, and Koh, GY. The role of vitamin D in depression and anxiety disorders: a review of the literature. Nutr Neurosci. (2024) 27:262–70. doi: 10.1080/1028415X.2023.2186318
90. Garcion, E, Sindji, L, Leblondel, G, Brachet, P, and Darcy, F. 1, 25-dihydroxyvitamin D3 regulates the synthesis of gamma-glutamyl transpeptidase and glutathione levels in rat primary astrocytes. J Neurochem. (1999) 73:859–66. doi: 10.1046/j.1471-4159.1999.0730859.x
91. Rusu, ME, Bigman, G, Ryan, AS, and Popa, DS. Investigating the effects and mechanisms of combined Vitamin D and K supplementation in postmenopausal women: an up-to-date comprehensive review of clinical studies. Nutrients. (2024) 16:2356. doi: 10.3390/nu16142356
92. Amini, S, Jafarirad, S, Abiri, B, and Vitamin, D. Testosterone and depression in middle-aged and elderly men: a systematic review. Crit Rev Food Sci Nutr. (2023) 63:5194–205. doi: 10.1080/10408398.2021.2015284
93. Vignini, A, Nanetti, L, Raffaelli, F, Sabbatinelli, J, Salvolini, E, Quagliarini, V, et al. Effect of 1-y oral supplementation with vitaminized olive oil on platelets from healthy postmenopausal women. Nutrition. (2017) 42:92–8. doi: 10.1016/j.nut.2017.06.013
94. Musazadeh, V, Keramati, M, Ghalichi, F, Kavyani, Z, Ghoreishi, Z, Alras, KA, et al. Vitamin D protects against depression: evidence from an umbrella meta-analysis on interventional and observational meta-analyses. Pharmacol Res. (2023) 187:106605. doi: 10.1016/j.phrs.2022.106605
95. Vyas, CM, Mischoulon, D, Chang, G, Cook, NR, Weinberg, A, Copeland, T, et al. Effects of Vitamin D (3) and marine Omega-3 fatty acids supplementation on indicated and selective prevention of depression in older adults: results from the Clinical Center sub-cohort of the VITamin D and Omeg A-3 Tria L (VITAL). J Clin Psychiatry. (2023) 84:22m14629. doi: 10.4088/JCP.22m14629
96. Marcinowska-Suchowierska, E, Kupisz-Urbańska, M, Łukaszkiewicz, J, Płudowski, P, and Jones, G. Vitamin D toxicity-a clinical perspective. Front Endocrinol. (2018) 9:550. doi: 10.3389/fendo.2018.00550
97. Manosso, LM, Camargo, A, Dafre, AL, and Rodrigues, ALS. Vitamin E for the management of major depressive disorder: possible role of the anti-inflammatory and antioxidant systems. Nutr Neurosci. (2022) 25:1310–24. doi: 10.1080/1028415X.2020.1853417
98. Tucker, JM, and Townsend, DM. Alpha-tocopherol: roles in prevention and therapy of human disease. Biomed Pharmacother. (2005) 59:380–7. doi: 10.1016/j.biopha.2005.06.005
99. Ambrogini, P, Betti, M, Galati, C, Di Palma, M, Lattanzi, D, Savelli, D, et al. α-Tocopherol and hippocampal neural plasticity in physiological and pathological conditions. Int J Mol Sci. (2016) 17:2107. doi: 10.3390/ijms17122107
100. Muller, DP. Vitamin E and neurological function. Mol Nutr Food Res. (2010) 54:710–8. doi: 10.1002/mnfr.200900460
101. Tahir, M, Kang, MH, Park, TJ, Ali, J, Choe, K, Park, JS, et al. Multifaceted neuroprotective approach of Trolox in Alzheimer's disease mouse model: targeting Aβ pathology, neuroinflammation, oxidative stress, and synaptic dysfunction. Front Cell Neurosci. (2024) 18:1453038. doi: 10.3389/fncel.2024.1453038
102. Zeng, W, Takashima, K, Tang, Q, Zou, X, Ojiro, R, Ozawa, S, et al. Natural antioxidant formula ameliorates lipopolysaccharide-induced impairment of hippocampal neurogenesis and contextual fear memory through suppression of neuroinflammation in rats. J Chem Neuroanat. (2023) 131:102285. doi: 10.1016/j.jchemneu.2023.102285
103. Hughes, RN, and Collins, MA. Enhanced habituation and decreased anxiety by environmental enrichment and possible attenuation of these effects by chronic alpha-tocopherol (vitamin E) in aging male and female rats. Pharmacol Biochem Behav. (2010) 94:534–42. doi: 10.1016/j.pbb.2009.11.008
104. Desrumaux, CM, Mansuy, M, Lemaire, S, Przybilski, J, Le Guern, N, Givalois, L, et al. Brain Vitamin E deficiency during development is associated with increased glutamate levels and anxiety in adult mice. Front Behav Neurosci. (2018) 12:310. doi: 10.3389/fnbeh.2018.00310
105. Wu, D, and Meydani, SN. Age-associated changes in immune and inflammatory responses: impact of vitamin E intervention. J Leukoc Biol. (2008) 84:900–14. doi: 10.1189/jlb.0108023
106. Pae, M, and Wu, D. Nutritional modulation of age-related changes in the immune system and risk of infection. Nutr Res. (2017) 41:14–35. doi: 10.1016/j.nutres.2017.02.001
107. Meydani, SN, Lewis, ED, and Wu, D. Perspective: should Vitamin E recommendations for older adults be increased? Adv Nutr. (2018) 9:533–43. doi: 10.1093/advances/nmy035
108. Vicente, IST, Fleuri, LF, Xavier, WDS, Guimarães, MG, de Carvalho, P, Rodrigues, EJD, et al. The effects of dietary Orange Peel fragments enriched with zinc and vitamins C and E on the antioxidant and immune responses of Nile Tilapia under stress conditions. Animals. (2024) 14:2962. doi: 10.3390/ani14202962
109. Zhang, J, Ren, X, Nie, Z, You, Y, Zhu, Y, Chen, H, et al. Dual-responsive renal injury cells targeting nanoparticles for vitamin E delivery to treat ischemia reperfusion-induced acute kidney injury. J Nanobiotechnol. (2024) 22:626. doi: 10.1186/s12951-024-02894-7
110. Ding, J, and Zhang, Y. Associations of dietary Vitamin C and E intake with depression. A Meta-analysis of observational studies. Front Nutr. (2022) 9:857823. doi: 10.3389/fnut.2022.857823
111. Ferland, G. Vitamin K and brain function. Semin Thromb Hemost. (2013) 39:849–55. doi: 10.1055/s-0033-1357481
112. Zhang, Y, Tan, W, Xi, X, Yang, H, Zhang, K, Li, S, et al. Association between vitamin K intake and depressive symptoms in US adults: data from the National Health and nutrition examination survey (NHANES) 2013-2018. Front Nutr. (2023) 10:1102109. doi: 10.3389/fnut.2023.1102109
113. Wang, H, Liu, Z, Zhan, K, Ma, Q, Xu, L, Li, Y, et al. Vitamin K2 alleviates dextran sulfate sodium-induced colitis via inflammatory responses, gut barrier integrity, and the gut microbiota in mice. Int J Biol Macromol. (2024) 280:136091. doi: 10.1016/j.ijbiomac.2024.136091
114. Chen, Y, Le, D, Xu, J, Jin, P, Zhang, Y, and Liao, Z. Gut microbiota Dysbiosis and inflammation dysfunction in late-life depression: an observational cross-sectional analysis. Neuropsychiatr Dis Treat. (2024) 20:399–414. doi: 10.2147/NDT.S449224
115. Wang, L, Huang, S, Feng, Z, Xiao, J, Luo, G, and Zhang, Y. Assessing the role of antioxidant and pro-oxidant balance in mediating the relationship between vitamin K intake and depressive symptoms in adults. Front Nutr. (2024) 11:1384489. doi: 10.3389/fnut.2024.1384489
116. Feng, X, Zheng, Y, Mao, N, Shen, M, Chu, L, Fang, Y, et al. Menaquinone-4 alleviates hypoxic-ischemic brain damage in neonatal rats by reducing mitochondrial dysfunction via Sirt 1-PGC-1α-TFAM signaling pathway. Int Immunopharmacol. (2024) 134:112257. doi: 10.1016/j.intimp.2024.112257
Keywords: late-life depression, vitamins, clinical efficacy, cellular mechanisms, nutritional intervention
Citation: Gao Y, Song X-N, Wen Z-P, Hu J-Z, Du X-Z, Zhang J-H and Liu S (2025) The association of vitamin deficiency with depression risk in late-life depression: a review. Front. Nutr. 12:1551375. doi: 10.3389/fnut.2025.1551375
Edited by:
Roberta Zupo, University of Bari Aldo Moro, ItalyReviewed by:
Dina Keumala Sari, Universitas Sumatera Utara, IndonesiaCopyright © 2025 Gao, Song, Wen, Hu, Du, Zhang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence:Sha Liu, bGl1c2hhMTk4NDExNEAxNjMuY29t;Ji-Hui Zhang, YmZ5eXpoYW5namlodWlAMTI2LmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.