 Marlise Lima Brandão1†
Marlise Lima Brandão1† Helen Hermana Miranda Hermsdorff2Arieta Carla Gualandi Leal2
Helen Hermana Miranda Hermsdorff2Arieta Carla Gualandi Leal2 Josefina Bressan2
Josefina Bressan2 Adriano Marçal Pimenta3*†
Adriano Marçal Pimenta3*†- 1Posgraduate Program in Nursing, Universidade Federal do Paraná, Curitiba, Paraná, Brazil
- 2Department of Nutrition and Health, Universidade Federal de Viçosa, Viçosa, Minas Gerais, Brazil
- 3Department of Nursing, Universidade Federal do Paraná, Curitiba, Paraná, Brazil
Background: Post-Acute COVID-19 Syndrome (PACS) is an important sequalae of COVID-19. Then, our objective was to analyze the risk and protective factors for PACS in Brazilian adults participating in the Cohort of Universities of Minas Gerais (CUME Study), with emphasis on COVID-19 vaccination and food consumption.
Methods: In this sub-study, we included 2,065 participants of CUME Study who answered the baseline questionnaire in 2016 or 2018 or 2020 or 2022, and the follow-up COVID-19/PACS-specific questionnaire in 2023. PACS diagnosis was based on self-reporting of continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation. To estimate the risk and protective factors for PACS, hierarchical multivariate statistical analysis was conducted using the Cox regression technique, producing two models: (1) focusing on consumption of macro and micronutrients; (2) focusing on consumption of food groups.
Results: After a median of 5.5 years of follow-up, 54.4% of the participants reported PACS. When we analyzed the consumption of macro and micronutrients, higher intake of proteins (HR: 1.36; 95% CI: 1.06–1.74-4th quartile) and lipids (HR: 1.23; 95% CI: 1.02–1.48-4th quartile) were risk factors for PACS. On the other hand, higher intake of vitamin C (HR: 0.78; 95% CI: 0.64–0.94-4th quartile), vitamin D (HR: 0.81; 95% CI: 0.67–0.99-4th quartile), and zinc (HR: 0.66; 95% CI: 0.52–0.83-4th quartile) were protective factors for the outcome (model 1). When we analyzed the consumption of food groups, higher intake of eggs (HR: 1.59; 95% CI: 1.34–1.89-4th quartile) increased the risk of PACS, whereas, respectively, higher and intermediate consumption of white meat (HR: 0.84; 95% CI: 0.71–1.00-4th quartile) and vegetables (HR: 0.81; 95% CI: 0.67–0.99-2nd quartile; HR: 0.81; 95% CI: 0.67–0.99-3rd quartile) decreased the risk of the outcome (model 2). In both models, pre-infection COVID-19 vaccination was a protective factor for PACS.
Conclusion: A healthy diet, with higher consumption of white meat, vegetables and specific micronutrients (vitamin C, vitamin D, zinc), in parallel with pre-infection COVID-19 vaccination, is essential to reduce the risk of PACS.
Introduction
COVID-19 was declared a public health emergency of international concern between January 30, 2020 and May 5, 2023. During this period, the disease was responsible for over 770 million cases and 7 million deaths worldwide (1, 2).
Currently, we are experiencing an endemic period of COVID-19. However, the disease continues to pose a significant global health challenge, as individuals still experience illness, death, and sequelae stemming from its acute phase (3).
Among these sequelae, Post-Acute COVID-19 Syndrome (PACS) is particularly notable. The World Health Organization (WHO) defines PACS as “the continuation or development of new symptoms of COVID-19 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation” (3).
A meta-analysis estimated the average prevalence of PACS to be 64% (4). This high prevalence has become a substantial challenge for healthcare professionals and systems worldwide. Understanding the risk and protective factors for PACS is therefore essential for the development of effective strategies, policies, and health programs aimed at its prevention.
Scientific findings consistently identified the following risk factors: (a) socioeconomic, such as female sex, advancing age, white skin color, and low income (5–12); (b) health conditions, such as pre-existing diagnoses of obesity (8, 9, 13), hypertension (14, 15), diabetes (16), dyslipidemia (8, 17), and chronic respiratory diseases (12, 18, 19); (c) clinical conditions related to the acute phase of COVID-19, such as the number of symptoms (5–7, 14, 20, 21), severity (5, 22–24), and hospitalization (12, 14, 16, 25). Conversely, protective factors have been identified, particularly infection with the Omicron variant (5, 6) and being infected during later waves of the acute COVID-19 phase (26).
Despite these findings, few studies have explored the relationship between the status of COVID-19 vaccination (pre- or post-infection) and the occurrence of PACS (27, 28), leaving this area of scientific evidence underdeveloped. Additionally, to our knowledge, no studies have investigated how macronutrient and micronutrient intake or the specific consumption of food groups might influence the risk of PACS incidence.
Therefore, the objective of this study was to analyze the risk and protective factors for PACS in Brazilian adults participating in the Cohort of Universities of Minas Gerais (CUME Study), with an emphasis on COVID-19 vaccination and food consumption.
Materials and methods
The CUME Study
The CUME Study is an open prospective cohort initiated in 2016. The cohort includes graduates of both sexes, aged 18 years or older, from seven public federal higher education institutions located in the state of Minas Gerais, Brazil. Its primary objective is to analyze the impact of the dietary patterns of the Brazilian population and nutritional transition on non-communicable chronic diseases.
Participant recruitment is ongoing, allowing for continuous sample growth with each follow-up wave, which occurs every 2 years. Previously recruited participants complete follow-up questionnaires (Q_2, Q_4, Q_6…, Q_n), while new participants respond to the baseline questionnaire (Q_0).
Further details regarding the study design, dissemination strategies, and the profile of the initial baseline participants are available in a prior publication (30).
As the CUME Study is a multicenter study, there may be similarities in the processes of variable definition, description, categorization, and data collection across publications derived from its database. For example, we have recently published the findings of the pilot study of the present research (31).
Ethical considerations
The CUME Study was conducted in accordance with the guidelines established in the Declaration of Helsinki. All procedures involving study participants were reviewed and approved by the Research Ethics Committee of the participating institutions (CAAE: 67808923.7.1001.5153). An informed consent form was obtained from all participants prior to their inclusion in the study.
Data collection
Data collection is conducted through a virtual platform where participants access the informed consent form, and the questionnaires. After agreeing to the informed consent form, participants are directed to complete the respective questionnaires.
The present research is a sub-study that included participants who answered the baseline questionnaire (Q_0) in March–August 2016 or March–August 2018 or March–August 2020 or March–September 2022, and the follow-up COVID-19/PACS-specific questionnaire (Q_CoV) in October–November 2023.
The baseline questionnaire of the CUME Study (Q_0) was structured into two sections: the first contemplated socioeconomic variables, lifestyle habits, self-reported morbidities, continuous medication use, clinical and laboratory exams conducted within the past 2 years, and anthropometric data. The second was titled Food Frequency Questionnaire (FFQ) which was comprised of 144 items, categorized into eight food groups (dairy products, meats and fish, cereals and legumes, oils and fats, fruits and vegetables, beverages, and other foods or prepared dishes).
The COVID-19/PACS-specific questionnaire (Q_CoV) is the main data collection instrument of this sub-study. It contained questions about COVID-19 occurrence, testing, symptoms, hospitalization, vaccination, PACS occurrence, and PACS symptoms.
Sample, inclusion, and exclusion criteria
All participants who completed the baseline (Q_0) and the COVID-19/PACS-specific (Q_CoV) questionnaires were included (n = 3,666). The following exclusion criteria were applied: (a) Participants without a prior diagnosis of COVID-19 (n = 1,298), as only individuals who had experienced the acute phase of the disease could develop PACS; (b) Foreign participants (n = 11), as cultural differences might influence both the exposure and the outcome variables; (c) Brazilian participants living abroad (n = 253), as different countries adopted varying measures to combat the COVID-19 pandemic and have diverse healthcare system structures, potentially affecting both the exposure and outcome variables; (d) Participants reporting extreme energy intakes [(≤500 kcal/day or ≥6,000 kcal/day), n = 39], which could indicate low accuracy in dietary intake data (29).
After applying these exclusion criteria, the final sample for this study consisted of 2,065 participants (Figure 1).
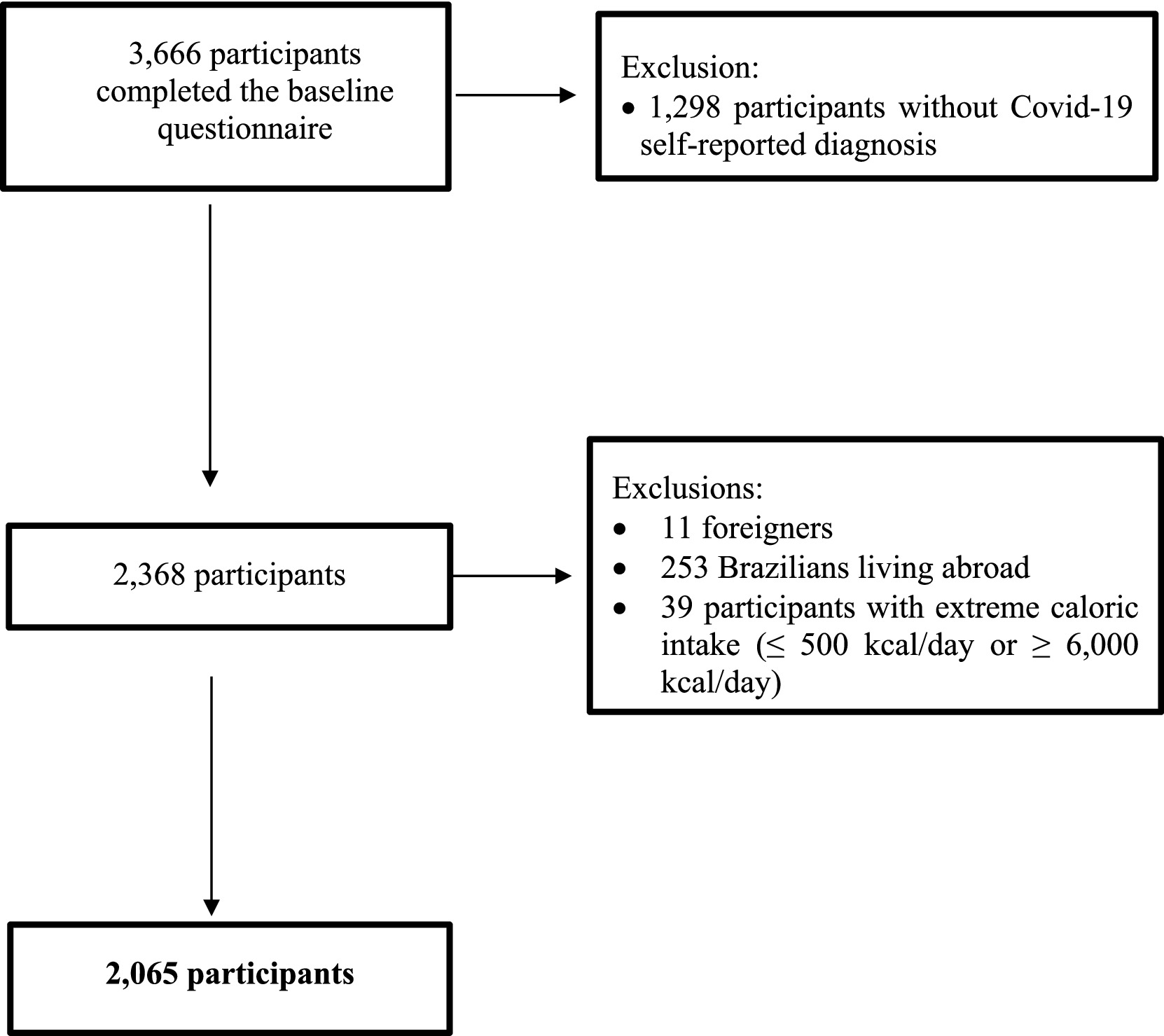
Figure 1. Flowchart of participant inclusion in the CUME Study, 2016–2023.
Outcome variable: Post-Acute COVID-19 Syndrome
The COVID-19/PACS-specific questionnaire (Q_CoV) included a question to assess PACS, based on the World Health Organization (WHO) definition: “PACS is defined as the continuation or development of new COVID-19 symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation” (3). Participants were asked to check the main symptoms they currently experienced or had experienced, considering this definition: intense fatigue; chronic pain; liver diseases; muscle weakness; difficulty breathing; cognitive deficits, such as changes in memory; neurological symptoms, such as loss of smell, dizziness, and headaches; anxiety disorders, and post-traumatic stress.
Participants were classified as not having PACS if they reported no symptoms, while those reporting one or more symptoms were classified as having PACS.
Exposure variables: risk and protective factors for Post-Acute COVID-19 Syndrome
Exposure variables were obtained from the baseline questionnaire (Q_0) and categorized according to CUME Study standards, as described in previous studies (30, 31), namely: (a) Socioeconomic: biological sex (female, male), age group (20–29 years old, 30–39 years old, 40–49 years old, 50–74 years old), skin color (white–yes and black/brown/yellow/indigenous–no), marital status (in a stable union–yes and single/widowed/separated/divorced–no), area of study (health sciences–yes and earth and exact sciences/biological sciences/engineering/applied social sciences/agricultural sciences/linguistics/study of languages and arts–no), educational level (graduation/specialization, master’s, doctorate/post-doctorate), professional situation (working–yes and retired, student, unemployed–no), family income (<4 minimum wages; 5–9 minimum wages, ≥10 minimum wages); (b) Lifestyle variables included current smoking (yes and no), heavy episodic drinking (yes and no), physical activity (sedentary, insufficiently active, active), dietary intake (food groups: dairy, red meat, white meat, eggs, cereals and legumes, fats and oils, fruits, vegetables, alcohol; macronutrients: carbohydrates, proteins and lipids; micronutrients: iron, vitamin C, vitamin D, magnesium, selenium, zinc); (c) Health conditions: self-reported medical diagnoses of obesity (yes and no), hypertension (yes and no), type 2 diabetes mellitus (yes and no), dyslipidemia (yes and no), hypercholesterolemia (yes and no), hypertriglyceridemia (yes and no), high levels of LDL-c (yes and no), low levels of HDL-c (yes and no), asthma (yes and no) and bronchitis (yes and no).
Additionally, some covariates were obtained from the COVID-19/PACS-specific questionnaire (Q_CoV), namely: number of times infected with SARS-CoV-2 (1, 2, 3, 4 and ≥5), waves of infection (first, second, third, endemic period, post-pandemic period), number of COVID-19 symptoms (0, 1–2, 3–5 and ≥6), seeking healthcare (yes and no), hospitalization (yes and no), vaccination status (received the vaccine before COVID-19 infection, received the vaccine after COVID-19 infection).
Family income was categorized in minimum wages, according to the value in force in the year of data collection.
Heavy episodic drinking was defined as the consumption of four or more drinks of any alcoholic beverage for women and five or more drinks of any alcoholic beverage for men on a single occasion within the past 30 days (32).
Physical activity was assessed using a list of 24 leisure activities, described in minutes per week. Initially, it was categorized as light, moderate and vigorous, and then the variable “level of physical activity” was created, categorized as “active” (≥150 min/week of moderate intensity or ≥75 min/week of vigorous activity or ≥150 min/week of vigorous and moderate intensity); insufficiently active” (<150 min/week of moderate intensity; <75 min/week of vigorous intensity; <150 min/week of vigorous and moderate intensity; light intensity activities); and inactive (absence of physical activity during leisure time) (33).
The FFQ filled out by each participant provided information on their dietary intake. Participants selected the items from the food groups they consumed during the year prior to study and, when selecting a food, had to describe the portion sizes consumed in household measures (teaspoon; tablespoon; ladle; knife tip; pasta server; saucer; cup or glass) or traditional portions (units; slices; or pieces). Subsequently, the frequencies of weekly, monthly and annual intake of each food were transformed into daily consumption. Then, the daily food intake, in grams or milliliters, was calculated (portion size versus consumption frequency). The values of energy intake (Kcal) and nutrients were calculated according to data provided in the Table of Reference Measures for Foods Consumed in Brazil (34), using as a complement the Brazilian Food Composition Table (35) and data from the United States Department of Agriculture (36).
Dietary intakes according to food groups, macronutrients and micronutrients were adjusted for caloric intake using the residual method (37) and were previously validated in a sub-sample of the CUME Study (38).
The percentage contribution of daily energetic intake (%/d) of macronutrients was obtained by dividing the total consumption of each macronutrient by total energy intake, and classified according to dietary reference intakes: Carbohydrates: adequate = 45–65%, low <45%, high ≥65%; Proteins: adequate = 10–35%, low <10%, high ≥35%; Lipids: adequate = 25–35%, low <25%, high ≥35% (39).
We also classified the consumption of micronutrients according to dietary reference intakes: Iron: adequate (men = 6–45 mg/d; women aged 19–50 = 8.1–45 mg/d; women aged ≥50 = 5–45 mg/d), low (men <6 mg/d; women aged 19–50 <8.1 mg/d; women aged ≥50 <5 mg/d), high ≥45 mg/d; Vitamin C: adequate (men = 75–2,000 mg/d; women = 60–2,000 mg/d), low (men <75 mg/d; women <60 mg/d), high ≥2,000 mg/d; Vitamin D: adequate (people aged 19–50 = 5–50 μg/d; people aged 51–70 = 10–50 μg/d; people aged ≥70 = 15–50 μg/d), low (people aged 19–50 <5 μg/d; people aged 51–70 <10 μg/d; people aged ≥70 <15 μg/d), high ≥50 μg/d; Magnesium: adequate (men aged 19–30 = 330–350 mg/d; men of other ages = 350 mg/d; women aged 19–30 = 255–350 mg/d; women of other ages = 265–350 mg/d); high ≥350 mg/d; Selenium: adequate = 45–400 μg/d, low <45 μg/d, high ≥400 μg/d; Zinc: adequate (men = 9.4–40 mg/d; women = 6.8–40 mg/d), low (men <9.4 mg/d; women <6.8 mg/d), high ≥40 mg/d (39).
Obesity was defined according to the cut-off point proposed by WHO (Body Mass Index–BMI ≥ 30 kg/m2) (40). Hypertension was considered when the participants self-reported a medical diagnosis of the disease or systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or use of antihypertensive medication (41). Type 2 diabetes mellitus was also considered when the participants self-reported a medical diagnosis of the disease or glycemia ≥126 mg/dL or using oral antidiabetic medication or using insulin (42). Hypercholesterolemia, hypertriglyceridemia, high blood levels of LDL-c and low blood levels of HDL-c were identified when participants self-reported, respectively, cholesterol ≥190 mg/dL, triglycerides ≥150 mg/dL, LDL-c ≥ 130 mg/dL and HDL-c < 40 mg/dL (43). Finally, if the participants had hypercholesterolemia and/or hypertriglyceridemia and/or high blood levels of LDL-c and/or low blood levels of HDL-c, they were classified with dyslipidemia (43).
In a previous study conducted with a sub-sample of the CUME Study, the data of weight, height, BMI, cholesterol, triglycerides, HDL-c, glycemia and blood pressure, presented moderate to excellent agreement between self-reports and measurements taken directly by the researchers. Moreover, the medical diagnosis of hypertension and the medical diagnosis of type 2 diabetes mellitus were also validated (44).
In Brazil, three waves of the pandemic period of COVID-19 have been described: the first from February 23, 2020 to November 7, 2020; the second from November 8, 2020 to December 25, 2021; and the third from December 26, 2021 to May 21, 2022 (45). Additionally, we also included two other periods of COVID-19 occurrence in the present study: endemic (between May 22, 2022 and May 4, 2023) and post-pandemic (between May 5, 2023 and the date of the last day of data collection of the current study, November 30, 2023) (46).
The status of COVID-19 vaccination (pre-or post-infection) was based on the participants’ responses to the dates of the first SARS-CoV-2 infection and the first dose of immunization.
Data analysis
Initially, participants were characterized by presenting absolute and relative frequencies, means, standard deviation, median, and interquartile range (IQR) of their socioeconomic variables, lifestyle habits, food consumption, self-reported health conditions, COVID-19 clinical conditions, and COVID-19 vaccination status, stratified by the occurrence or non-occurrence of PACS.
Statistical differences were evaluated using Pearson’s chi-squared and the Mann–Whitney tests. A hierarchical multivariate analysis was conducted using the Cox regression technique, which is used to obtain estimates of the proportional Hazard Ratio (HR) (47), where the outcome variable becomes the time until the event occurs, and participants are counted as person-time (47).
Thus, the time to the occurrence of PACS was calculated in person-years for each participant as follows: (1) difference between the date of self-reported PACS and the date of completion of the baseline questionnaire (Q_0); (2) difference between the date of completion of the COVID-19/PACS-specific questionnaire (Q_CoV) and the date of completion of the baseline questionnaire (Q_0) when PACS was not self-reported.
To estimate the independent risk and protective factors for PACS, we fitted two models, dividing the variables into four blocks: (1) distal block = socioeconomic; (2) intermediate block 1 = lifestyle habits and food consumption; (3) intermediate block 2 = self-reported health conditions; (4) proximal block = COVID-19 clinical conditions and vaccination status against COVID-19. The differences between the two models were in intermediate block 1. The focus of model 1 was the consumption of macro and micronutrients, whereas in model 2, the focus was the consumption of food groups.
During the first stage, variables associated with PACS at a statistical significance level of 20% in the bivariate analysis were selected for the final model. Then, each variable in the distal block was inserted into the final model in descending order of statistical significance and removed one by one using the backward method until only those with statistical significance levels below 5% remained. Next, the same process was done for the variables in the other blocks. Therefore, in the end, the variables from the previous block adjusted the variables from the subsequent block.
Results
Frequencies of Post-Acute COVID-19 Syndrome and its symptoms
The current study included a total of 2,065 participants (571 males and 1,494 females). After a median of 5.5 years of follow-up (approximately 10,752 person-years), 1,124 participants reported symptoms of PACS (54.4%), in the following order of magnitude: cognitive deficits, such as changes in memory (74.2%); intense fatigue (43.0%); neurological symptoms, such as loss of smell, dizziness, and headaches (32.5%); muscle weakness (27.7%); anxiety disorders and post-traumatic stress (22.3%); difficulty breathing (15.2%); chronic pain (9.9%); and liver diseases (1.1%).
Descriptive analysis
Participants with PACS were more likely to be female and older, have a graduate/specialization level of education, and lower family income (Table 1). Moreover, the consumption of vegetables and zinc were, respectively, higher and lower among participants with the outcome (Table 2).
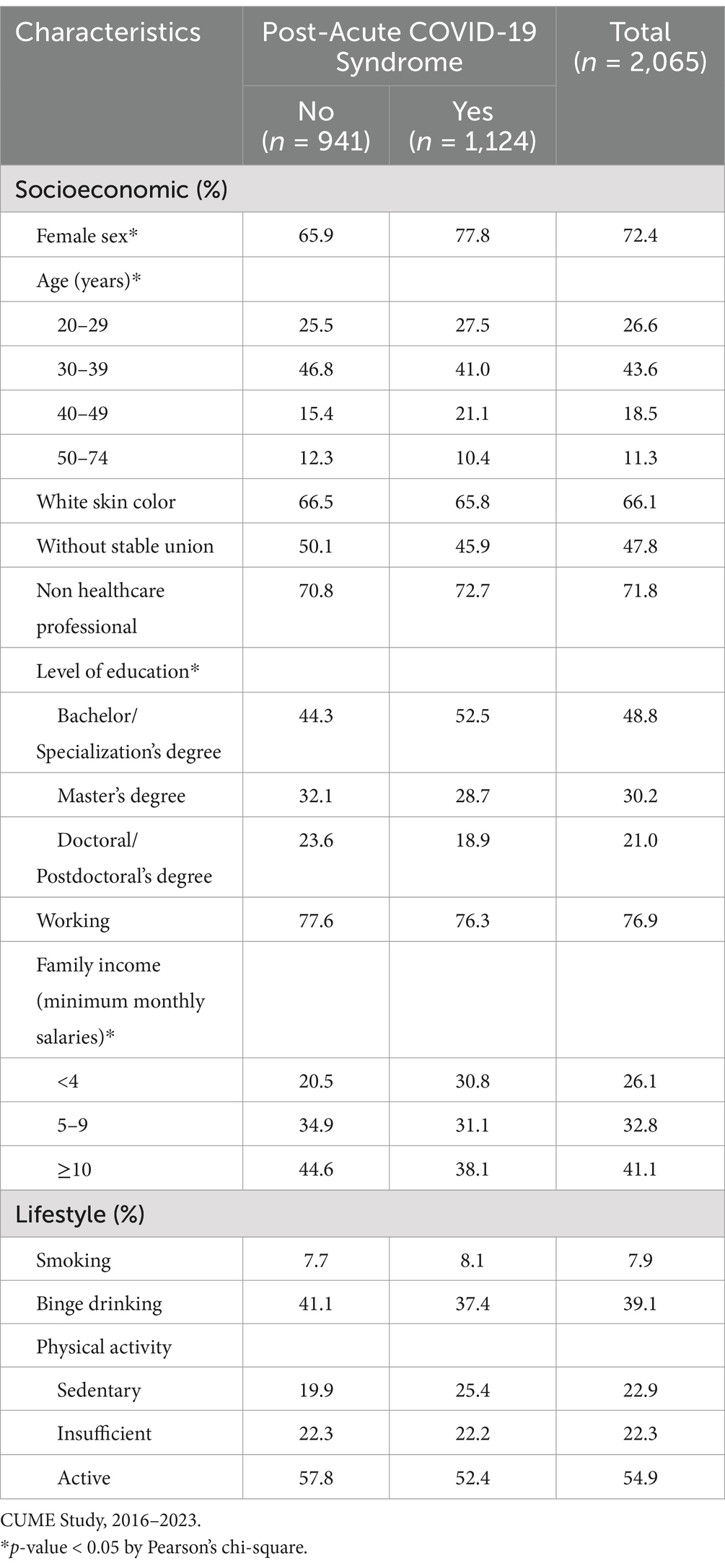
Table 1. Socioeconomic, lifestyle and food consumption characteristics of participants according to the diagnosis of Post-Acute COVID-19 Syndrome.
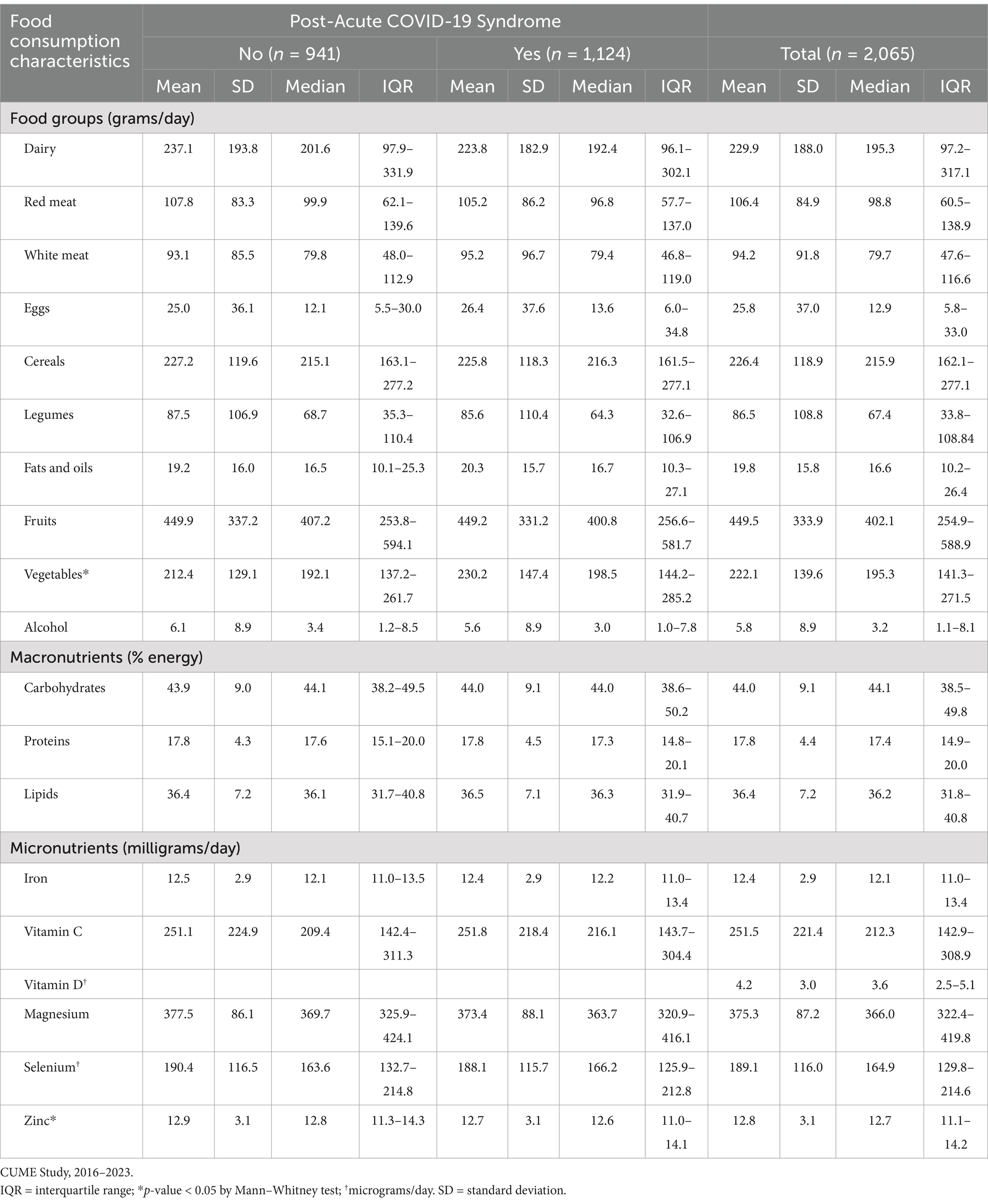
Table 2. Food consumption characteristics of participants according to the diagnosis of Post-Acute COVID-19 Syndrome.
Most participants had adequate consumption of proteins, iron, selenium and zinc. On the other hand, most participants had low consumption of carbohydrates and vitamin D, and high consumption of lipids and magnesium. Also, the intake of this last micronutrient was lower among participants with PACS (Supplementary Table 1).
Participants with PACS also were more likely to have prior diagnoses of obesity, hypertension, hypertriglyceridemia, and bronchitis. They also contracted COVID-19 twice or more times, were infected in the second wave of the pandemic period, had six or more COVID-19 symptoms, sought healthcare, were hospitalized, and received the vaccine after COVID-19 infection (Table 3).
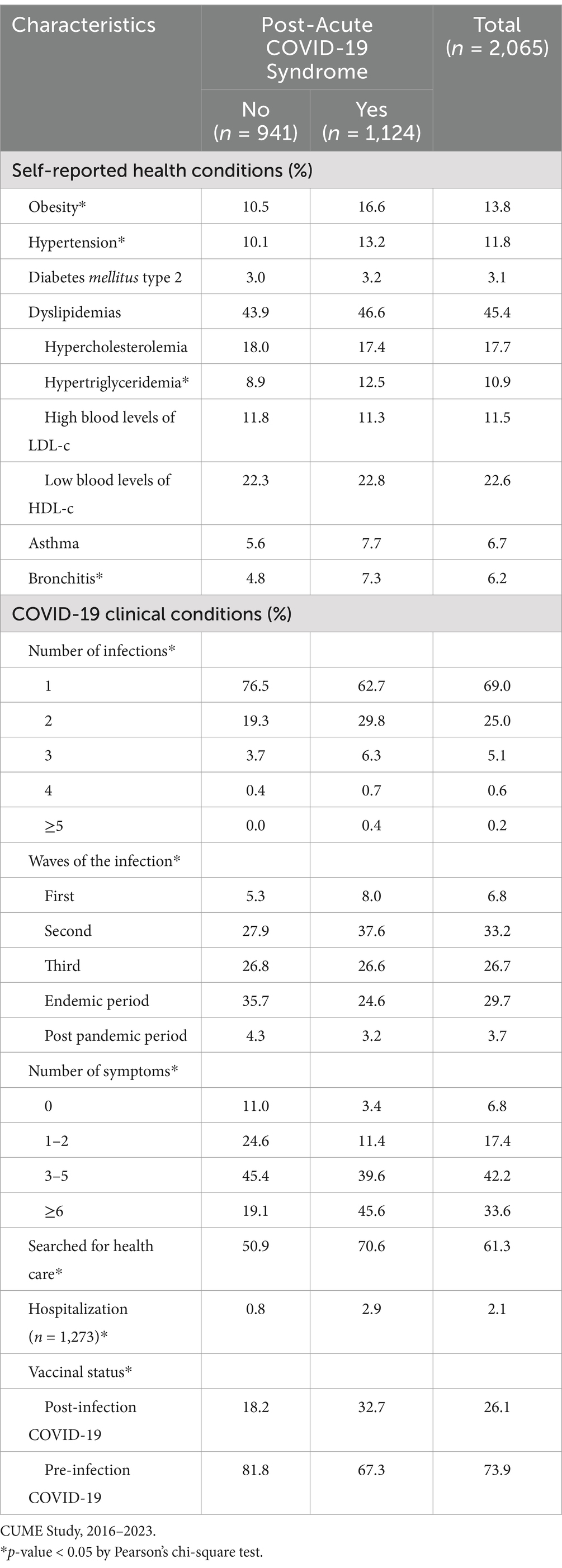
Table 3. Health and COVID-19 clinical conditions of participants according to the diagnosis of Post-Acute COVID-19 Syndrome.
Risk and protective factors for Post-Acute COVID-19 Syndrome
The hierarchical multivariate model of risk and protective factors for PACS, focusing on macro and micronutrients consumption (model 1) is presented in Table 4. Independent risk factors for PACS were: female (HR: 1.30; 95% CI: 1.13–1.49); age between 40 and 49 (HR: 1.40; 95% CI: 1.17–1.68); higher consumption of proteins (HR: 1.36; 95% CI: 1.06–1.74-4th quartile) and lipids (HR: 1.23; 95% CI: 1.03–1.47-3rd quartile; HR: 1.23; 95% CI: 1.02–1.48-4th quartile); prior diagnoses of obesity (HR: 1.45; 95% CI: 1.23–1.71), hypertriglyceridemia (HR: 1.24; 95% CI: 1.03–1.49), and bronchitis (HR: 1.26; 95% CI: 1.00–1.58); the number of COVID-19 infections (HR: 1.14; 95% CI: 1.04–1.25); having contracted COVID-19 in the second pandemic wave (HR = 1.56; 95% CI = 1.13–2.16); the number of COVID-19 symptoms (HR: 1.11; 95% CI: 1.08–1.13); and having sought healthcare during the acute phase of COVID-19 (HR: 1.33; 95% CI: 1.15–1.54). On the other hand, the independent protective factors for PACS were: higher family income (HR: 0.61; 95% CI: 0.52–0.71-5–9 minimum monthly salaries; HR: 0.51; 95% CI: 0.44–0.59-≥10 minimum monthly salaries); higher consumption of vitamin C (HR: 0.78; 95% CI: 0.64–0.94-4th quartile), vitamin D (HR: 0.81; 95% CI: 0.67–0.99-4th quartile), and zinc (HR: 0.78; 95% CI: 0.64–0.97-3rd quartile; HR: 0.66; 95% CI: 0.52–0.83-4th quartile); and pre-infection COVID-19 vaccination (HR: 0.69; 95% CI: 0.56–0.85).
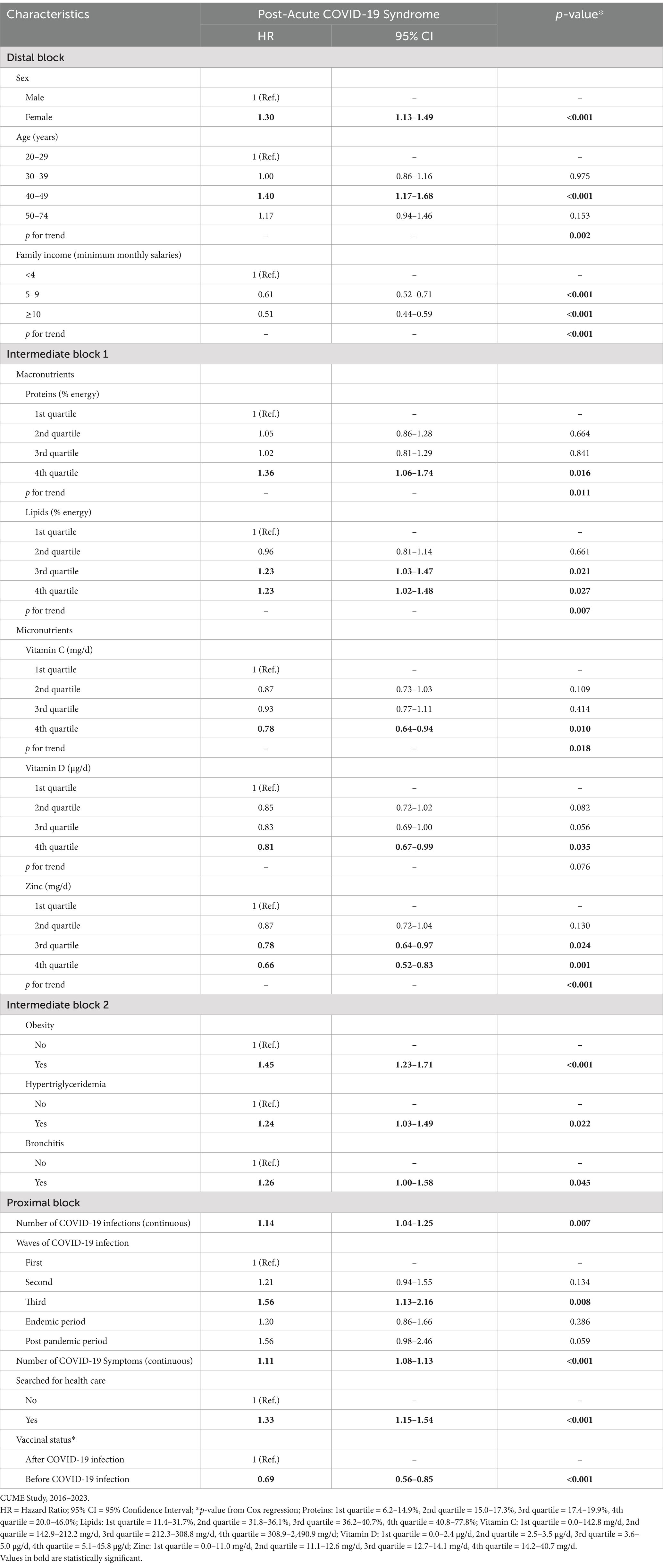
Table 4. Hierarchical multivariate model of risk and protective factors for Post-Acute COVID-19 Syndrome, highlighting macro and micronutrients.
The hierarchical multivariate model of risk and protective factors for PACS, focusing on food group consumption (model 2) is presented in Table 5. Respectively, the higher and the intermediate consumption of white meat (HR: 0.82; 95% CI: 0.69–0.97-2nd quartile; HR: 0.81; 95% CI: 0.68–0.96-3rd quartile) and vegetables (HR: 0.82; 95% CI: 0.69–0.97-2nd quartile; HR: 0.81; 95% CI: 0.68–0.96-3rd quartile) were protective factors for PACS, whereas the higher consumption of eggs constituted an independent risk factor for the outcome (HR: 1.59; 95% CI: 1.34–1.89-4th quartile).
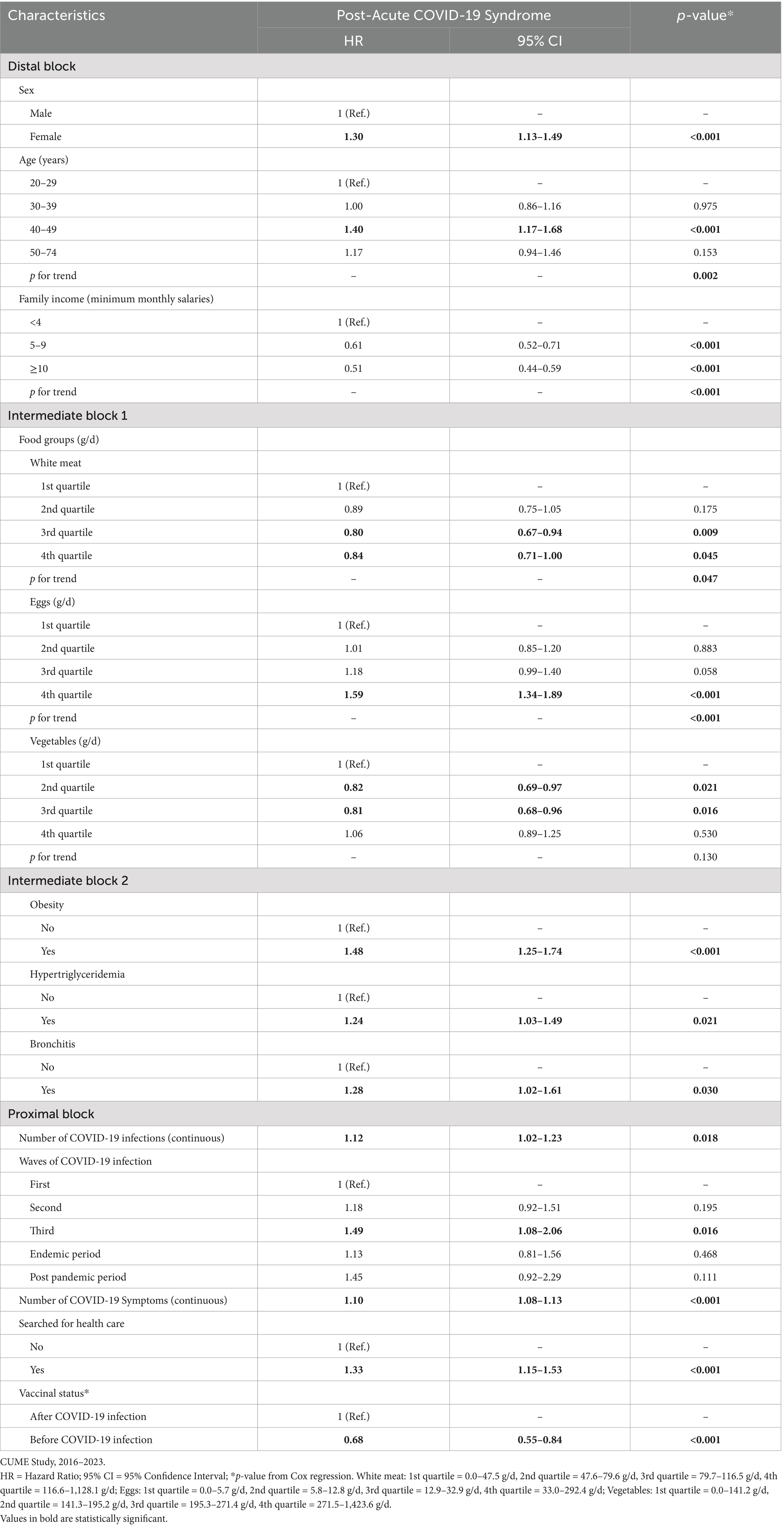
Table 5. Hierarchical multivariate model of risk and protective factors for Post-Acute COVID-19 Syndrome, highlighting food groups.
Discussion
This study employed multivariate hierarchical models to investigate independent risk and protective factors for PACS with an emphasis on COVID-19 vaccination and food consumption. Our results indicate several risk factors for PACS, including socioeconomic characteristics, pre-existing health conditions, dietary habits, COVID-19 acute period characteristics, and vaccination against COVID-19.
First, females exhibited a higher risk for PACS, consistent with previous studies, potentially due to hormonal and immunological differences (48). Estrogen exerts immunomodulatory effects, which may render women’s immune systems more susceptible to exacerbated reactions, such as the chronic inflammation observed in PACS (48, 49). Furthermore, estrogen can increase the expression of viral receptors in cells, facilitating viral entry, but it can also influence recovery and the inflammatory response post-infection (50). Additionally, the age group between 40 and 49 years was identified as a risk factor, aligning with epidemiological data indicating greater vulnerability in middle-aged adults (51).
Interestingly, higher protein and lipid intake was associated with an increased risk of PACS. While the exact relationship between dietary intake and PACS remains unclear, excessive consumption of these meats may alter the composition of the intestinal microbiota. White meats are rich in L-carnitine and choline, which serve as substrates for intestinal bacteria to produce trimethylamine (TMA), subsequently transformed into trimethylamine N-oxide (TMAO) (52, 53). TMAO can damage the vascular endothelium and activate inflammatory pathways, exacerbating systemic inflammation and predisposing individuals to the development of comorbidities that worsen COVID-19 (54, 55). Similarly, egg consumption was associated with an increased risk of PACS. While eggs are an excellent source of protein and nutrients (56, 57), excessive consumption within the context of a pro-inflammatory diet may contribute to an exacerbated inflammatory response. Further research is needed to elucidate this relationship.
Another significant factor was a prior diagnosis of obesity, strongly associated with an increased risk. This aligns with the literature highlighting obesity as a predisposing factor for severe COVID-19 and its long-term effects (58–60). Additionally, conditions like hypertriglyceridemia and bronchitis were identified as predictors of PACS, suggesting that cardiovascular and respiratory diseases may play a crucial role in the manifestation of the syndrome (61). COVID-19 directly and indirectly affects the respiratory system, and individuals with bronchitis may be more susceptible to viral infections and their sequelae due to pre-existing airway inflammation (62). This can exacerbate post-COVID recovery by worsening respiratory symptoms like shortness of breath and fatigue, as observed in our study and a multicenter cohort from Japan, South Korea, and the United Kingdom (63).
Conversely, our study identified protective factors for PACS. Higher family income emerged as a significant protective factor, aligning with longitudinal research, which showed that individuals with lower income exhibited more severe cardiovascular symptoms (64). This may reflect greater access to healthcare, better food quality, and improved living conditions, factors associated with less severe COVID-19 and its sequelae (65).
Furthermore, the intake of micronutrients like vitamin C, vitamin D, and zinc was associated with protection against PACS, suggesting that these immune response modulators may play crucial roles in reducing post-viral inflammation (66, 67).
Vitamin D exerts an essential immunomodulatory effect, balancing the immune response and reducing systemic inflammation, potentially preventing or minimizing PACS symptoms. It reduces the production of inflammatory cytokines, increases the production of antimicrobial peptides like cathelicidin, and promotes the function of regulatory T cells, which control the immune response (68). These effects help prevent chronic inflammation and exacerbated immune responses; factors frequently associated with PACS (67, 69). A population-based survey in Europe demonstrated that individuals with a blood concentration of vitamin D 25 (OH) ≥ 50 nmol/L had lower COVID-19 mortality compared to those with a blood concentration of vitamin D 25(OH) < 50 nmol/L (70).
Vitamin C and zinc modulate oxinflammation, combating reactive oxygen species and reducing the expression of TNF-α and IL-6, inflammatory cytokines associated with respiratory disease progression and PACS (71). These findings highlight the potential of nutritional adequacy as a strategy to reduce the risk of PACS and prevent complications during acute COVID-19.
When analyzing a multivariate model, higher consumption of white meat and vegetables was associated with a lower risk of PACS, likely reflecting the beneficial impact of a diet rich in lean proteins and antioxidant nutrients. White meats provide high-quality proteins and essential amino acids, crucial for immune function and tissue recovery, both important in viral infections and COVID-19 recovery (72). Vegetables are rich in vitamins and other nutrients essential for immune system function and combating oxidative stress (73–75). A nine-month prospective study in the United Kingdom, following over 3 million individuals, evaluated the association between diet quality and COVID-19 risk and severity. They observed that higher diet quality was associated with a lower risk of COVID-19 infection and milder symptoms compared to those in the lowest quartile of the diet score (76). These data reinforce the notion that a balanced diet, rich in micronutrients and high-quality proteins, can modulate the inflammatory response and improve recovery from viral diseases (72).
Another significant finding was the protective effect of vaccination against PACS. Individuals who received the vaccine before contracting the disease had a lower chance of developing PACS. This aligns with growing evidence that vaccination can reduce the risk of infection and minimize long-term disease effects (27). A meta-analysis of over 10 million patients with an average age of 50.6 years evaluated the potential protective effect of vaccines. They observed a lower prevalence of PACS symptoms in vaccinated individuals compared to unvaccinated individuals, with a decrease in symptoms (OR: 0.59; 95% CI 0.48–0.73). Furthermore, the OR of 0.77 indicated a 23% reduction in the risk of developing PACS (95% CI 0.75–0.79) associated with vaccination (28). Thus, COVID-19 vaccines play a crucial role in mitigating the severity of PACS.
Study limitations and strengths
It is suggested that our scientific findings should be interpreted with caution due to some limitations: (1) The symptoms of PACS were self-reported. However, studies conducted with a sample with high education, such as CUME Study, indicated excellent accuracy of self-reported data (77). Furthermore, in validation studies conducted with samples from our cohort, self-reported diagnoses of different outcomes showed excellent agreement with those measured directly by physicians and other health professionals (44, 78); (2) Our sample is not representative of the Brazilian population, and limited to participants with high education. However, our participants hold high and crucial positions for the Brazilian economy, and interruption of their work activities due to illness or death may result in significant social and economic burdens for the country; (3) All participants had mild cases of COVID-19, and most did not require hospitalization or invasive procedures during treatment; (4) Exposure variables, especially socioeconomic factors, lifestyle habits and food consumption, may be modifiable over time. Therefore, this should be considered when interpreting our findings. However, in a reproducibility sub-study of our FFQ, after one year between data collections, the overall agreement of the results was excellent (92.5%), with a mean intraclass correlation coefficient of 0.76 (38); (5) Some symptoms of PACS are similar to those of perimenopause and menopause, particularly memory changes, headaches, muscle weakness, and anxiety disorders (79). Therefore, because our sample was predominantly female, with almost one-third of women over 40 years of age, there may have been difficulties in differentiating self-reported symptoms of PACS from symptoms of perimenopause and menopause.
Strengths include a robust sample size, longitudinal study design with considerable follow-up time. Additionally, this study was developed with a general target audience, not restricted to hospital discharges, broadening the understanding of the studied theme to a wider spectrum of the population. Finally, it is important to highlight that we also validate the main self-reported data used in the present study (38, 44).
Conclusion
PACS is a high-magnitude event, constituting an important public health concern to be faced by health system managers and health professionals in the coming years after the end of the COVID-19 pandemic period.
Additionally, health policies and programs that promote a healthy diet with higher consumption of white meat, vegetables and specific micronutrients (vitamin C, vitamin D, zinc), in parallel with pre-infection COVID-19 vaccination, are essential to reduce the risk of PACS.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human beings were approved by the Research Ethics Committee of the Federal University of Viçosa (CAAE: 67808923.7.1001.5153) and endorsed by the Research Ethics Committees of the other institutions involved in this research. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MB: Conceptualization, Investigation, Writing – original draft. HH: Conceptualization, Data curation, Funding acquisition, Investigation, Project administration, Supervision, Writing – review & editing. AL: Writing – review & editing. JB: Conceptualization, Data curation, Funding acquisition, Investigation, Project administration, Writing – review & editing. AP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Project administration, Supervision, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by The Minas Gerais State Foundation for Research Support (FAPEMIG) [Minas Gerais-Brazil, Grant numbers: CDS-APQ-00571/13, CDS-APQ-02407/16, CDS-APQ-00424/17, CDS-APQ-00321/18] and National Council for Scientific and Technological Development (CNPq) [Brasília-Brazil, Grant number: 409098/2022-1]. AMP, HHMH, and JB are CNPq Fellows in Research Productivity.
Acknowledgments
We would like to thank all participants of the study, without whom this research would not have been possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1549747/full#supplementary-material
References
1. World Health Organization (WHO). WHO coronavirus (COVID-19) dashboard. Geneva: WHO. (2023). Available online at: https://data.who.int/dashboards/covid19/cases (Accessed December 19, 2024).
2. World Health Organization (WHO). WHO coronavirus (COVID-19) dashboard. Geneva: WHO. (2023). Available online at: https://data.who.int/dashboards/covid19/deaths (Accessed December 19, 2024).
3. World Health Organization (WHO). Clinical management of COVID-19: living guideline. Geneva: WHO. (2023). Available online at: https://iris.who.int/bitstream/handle/10665/372288/WHO-2019-nCoV-clinical-2023.2-eng.pdf?sequence=1 (Accessed December 19, 2024).
4. Ma, Y, Deng, J, Liu, Q, Du, M, Liu, M, and Liu, J. Long-term consequences of COVID-19 at 6 months and above: a systematic review and meta-analysis. Int J Environ Res Public Health. (2022) 19:6865. doi: 10.3390/ijerph19116865
5. Jassat, W, Mudara, C, Vika, C, Welch, R, Arendse, T, Dryden, M, et al. A cohort study of post-COVID-19 condition across the Beta, Delta, and omicron waves in South Africa: 6-month follow-up of hospitalized and nonhospitalized participants. Int J Infect Dis. (2023) 128:102–11. doi: 10.1016/j.ijid.2022.12.036
6. Durstenfeld, MS, Peluso, MJ, Peyser, ND, Lin, F, Knight, SJ, Djibo, A, et al. Factors associated with long COVID symptoms in an online cohort study. Open Forum Infect Dis. (2023) 10:ofad047. doi: 10.1093/ofid/ofad047
7. Emecen, AN, Keskin, S, Turunc, O, Suner, AF, Siyve, N, Basoglu Sensoy, E, et al. The presence of symptoms within 6 months after COVID-19: a single-center longitudinal study. Ir J Med Sci. (2023) 192:741–50. doi: 10.1007/s11845-022-03072-0
8. Lapa, J, Rosa, D, Mendes, JPL, Deusdará, R, and Romero, GAS. Prevalence and associated factors of post-COVID-19 syndrome in a Brazilian cohort after 3 and 6 months of hospital discharge. Int J Environ Res Public Health. (2023) 20:848. doi: 10.3390/ijerph20010848
9. Munipalli, B, Paul, S, Mohabbat, A, Siddiqui, H, Li, Z, and Abu, DA. Clinical differences in symptomology, characteristics, and risk factors in patients with post-acute sequelae of COVID-19: an experience from a tertiary-care academic center. J Investig Med. (2023) 71:495–501. doi: 10.1177/10815589231153604
10. Muzyka, I, Yakhnytska, M, Savytska, M, and Zayachkivska, O. Long COVID prevalence and physiology-centered risks: population-based study in Ukraine. Inflammopharmacology. (2023) 31:597–602. doi: 10.1007/s10787-023-01177-1
11. Robertson, MM, Qasmieh, SA, Kulkarni, SG, Teasdale, CA, Jones, HE, McNairy, M, et al. The epidemiology of long coronavirus disease in US adults. Clin Infect Dis. (2023) 76:1636–45. doi: 10.1093/cid/ciac961
12. Wan, KS, Sundram, ER, Haddi, AAA, Dashuki, AR, Ahad, A, John, R, et al. Long COVID active case detection initiative among COVID-19 patients in Port Dickson, Malaysia: a retrospective study on the positive outcomes, the proportion of patients with long COVID and its associated factors. Peer J. (2023) 11:e14742. doi: 10.7717/peerj.14742
13. Wang, S, Li, Y, Yue, Y, Yuan, C, Kang, JH, Chavarro, JE, et al. Adherence to healthy lifestyle prior to infection and risk of post-COVID-19 condition. JAMA Intern Med. (2023) 183:232–41. doi: 10.1001/jamainternmed.2022.6555
14. Ko, ACS, Candellier, A, Mercier, M, Joseph, C, Schmit, J-L, Lanoix, J-P, et al. Number of initial symptoms is more related to long COVID-19 than acute severity of infection: a prospective cohort of hospitalized patients. Int J Infect Dis. (2022) 118:220–3. doi: 10.1016/j.ijid.2022.03.006
15. Tleyjeh, IM, Saddik, B, AlSwaidan, N, Al-Anazi, A, Ramakrishnan, RK, Alhazmi, D, et al. Prevalence and predictors of post-acute COVID-19 syndrome (PACS) after hospital discharge: a cohort study with 4 months median follow-up. PLoS One. (2021) 16:e0260568. doi: 10.1371/journal.pone.0260568
16. Yoo, SM, Liu, TC, Motwani, Y, Sim, MS, Viswanathan, N, Samras, N, et al. Factors associated with post-acute sequelae of SARS-CoV-2 (PASC) after diagnosis of symptomatic COVID-19 in the inpatient and outpatient setting in a diverse cohort. J Gen Intern Med. (2022) 37:1988–95. doi: 10.1007/s11606-022-07523-3
17. Adler, L, Gazit, S, Pinto, Y, Perez, G, Reuveni, MM, Yehoshua, I, et al. Long-COVID in patients with a history of mild or asymptomatic SARS-CoV-2 infection: a nationwide cohort study. Scand J Prim Health Care. (2022) 40:342–9. doi: 10.1080/02813432.2022.2139480
18. Pérez-González, A, Araújo-Ameijeiras, A, Fernández-Villar, A, Crespo, M, and Poveda, E. Long COVID in hospitalized and non-hospitalized patients in a large cohort in Northwest Spain, a prospective cohort study. Sci Rep. (2022) 12:3369. doi: 10.1038/s41598-022-07414-x
19. Subramanian, A, Nirantharakumar, K, Hughes, S, Myles, P, Williams, T, Gokhale, KM, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nature Med. (2022) 28:1706–14. doi: 10.1038/s41591-022-01909-w
20. Silverberg, JI, Zyskind, I, Naiditch, H, Zimmerman, J, Glatt, AE, Pinter, A, et al. Predictors of chronic COVID-19 symptoms in a community-based cohort of adults. PLoS One. (2022) 17:e0271310. doi: 10.1371/journal.pone.0271310
21. Chudzik, M, Babicki, M, Kapusta, J, Kałuzińska-Kołat, Ż, Kołat, D, Jankowski, P, et al. Long-COVID clinical features and risk factors: a retrospective analysis of patients from the STOP-COVID registry of the PoLoCOV study. Viruses. (2022) 14:1755. doi: 10.3390/v14081755
22. Wong, MC-S, Huang, J, Wong, Y-Y, Wong, GL-H, Yip, TC-F, Chan, RN-Y, et al. Epidemiology, symptomatology, and risk factors for long COVID symptoms: population-based, multicenter study. JMIR Public Health Surveill. (2023) 9:e42315. doi: 10.2196/42315
23. Larijani, MS, Ashrafian, F, Amiri, FB, Banifazl, M, Bavand, A, Karami, A, et al. Characterization of long COVID-19 manifestations and its associated factors: a prospective cohort study from Iran. Microb Pathog. (2022) 169:105618. doi: 10.1016/j.micpath.2022.105618
24. Peters, C, Dulon, M, Westermann, C, Kozak, A, and Nienhaus, A. Long-term effects of COVID-19 on workers in health and social services in Germany. Int J Environ Res Public Health. (2022) 19:6983. doi: 10.3390/ijerph19126983
25. Förster, C, Colombo, MG, Wetzel, A-J, Martus, P, and Joos, S. Persisting symptoms after COVID-19: prevalence and risk factors in a population-based cohort. Dtsch Arztebl Int. (2022) 119:167–74. doi: 10.3238/arztebl.m2022.0147
26. Bellan, M, Apóstolo, D, Albe, A, Crevola, M, Errica, N, Ratano, G, et al. Determinants of long COVID among adults hospitalized for SARS-CoV-2 infection: a prospective cohort study. Front Immunol. (2022) 13:1038227. doi: 10.3389/fimmu.2022.1038227
27. Scholkmann, F, and May, CA. COVID-19, post-acute COVID-19 syndrome (PACS, "long COVID") and post-COVID-19 vaccination syndrome (PCVS, "post-COVIDvac-syndrome"): similarities and differences. Pathol Res Pract. (2023) 246:154497. doi: 10.1016/j.prp.2023.154497
28. Man, MA, Rosca, D, Bratosin, F, Fira-Mladinescu, O, Ilie, AC, Burtic, SR, et al. Impact of pre-infection COVID-19 vaccination on the incidence and severity of post-COVID syndrome: a systematic review and meta-analysis. Vaccines (Basel). (2024) 12:189. doi: 10.3390/vaccines12020189
29. Schmidt, MI, Duncan, BB, Mill, JG, Lotufo, PA, Chor, D, Barreto, SM, et al. Cohort profile: longitudinal study of adult health (ELSA-Brasil). Int J Epidemiol. (2015) 44:68–75. doi: 10.1093/ije/dyu027
30. Gomes Domingos, AL, Miranda, AEDS, Pimenta, AM, Hermsdorff, HHM, Oliveira, FLP, Dos Santos, LC, et al. Cohort profile: the Cohort of Universities of Minas Gerais (CUME). Int J Epidemiol. (2018) 47:1743–4. doi: 10.1093/ije/dyy152
31. Eduvirgem, J, Bressan, J, Hermsdorff, HHM, Montenegro, LC, Brandão, ML, Neves, AAT, et al. Risk and protective factors for long COVID in Brazilian adults (CUME study). Front Med (Lausanne). (2024) 11:1344011. doi: 10.3389/fmed.2024.1344011
32. National Institute on Alcohol Abuse and Alcoholism (NIAAA). Drinking levels defined. Available online at: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking (Accessed October 25, 2023).
33. World Health Organization (WHO). Global recommendations on physical activity for health. Geneva: WHO (2010).
34. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2008–2009: tabela de medidas referidas para os alimentos consumidos no Brasil. Rio de Janeiro: IBGE (2011).
35. Núcleo de Estudos e Pesquisas em Alimentação, Universidade Estadual de Campinas. Tabela brasileira de composição de alimentos - TACO. 4th ed. Campinas: Universidade Estadual de Campinas (2011).
36. Agricultural Research Service, United States Department of Agriculture. FoodData central. Available online at: https://fdc.nal.usda.gov/ (Accessed October 25, 2023).
37. Willett, WC, Howe, GR, and Kushi, LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. (1997) 65:1220S–8S. doi: 10.1093/ajcn/65.4.1220S
38. Azarias, HGA, Marques-Rocha, JL, Miranda, AEDS, Dos Santos, LC, Gomes Domingos, AL, Hermsdorff, HHM, et al. Online food frequency questionnaire from the Cohort of Universities of Minas Gerais (CUME project, Brazil): construction, validity, and reproducibility. Front Nutr. (2021) 8:709915. doi: 10.3389/fnut.2021.709915
39. Padovani, RM, Amaya-Farfán, J, Colugnati, FAB, and Domene, SMA. Dietary reference intakes: application of tables in nutritional studies. Rev Nutr. (2023) 19:741–60. doi: 10.1590/S1415-52732006000600010
40. World Health Organization (WHO). Obesity: preventing and managing the global epidemic. Report of WHO consultation. Geneva: WHO (2000).
41. Chobanian, AV, Bakris, GL, Black, HR, Cushman, WC, Green, LA, Izzo, JL Jr, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. (2003) 42:1206–52. doi: 10.1161/01.HYP.0000107251.49515.c2
42. Sociedade Brasileira de Diabetes (SBD). Diretrizes da Sociedade Brasileira de Diabetes. 2019–2020. São Paulo: Editora Clannad (2019).
43. Xavier, HT, Izar, MC, Faria Neto, JR, Assad, MH, Rocha, VZ, Sposito, AC, et al. V Brazilian guidelines on dyslipidemias and prevention of atherosclerosis. Arq Bras Cardiol. (2013) 101:01–22. doi: 10.5935/abc.2013S010
44. Miranda, AES, Ferreira, AVM, Oliveira, FLP, Hermsdorff, HHM, Bressan, J, and Pimenta, AM. Validation of metabolic syndrome and its self-reported components in the CUME study. Rev Min Enferm. (2017) 21:e1069. doi: 10.5935/1415-2762.20170079
45. Moura, EC, Cortez-Escalante, J, Cavalcante, FV, Barreto, ICHC, Sanchez, MN, and Santos, LMP. Covid-19: temporal evolution and immunization in the three epidemiological waves, Brazil, 2020-2022. Rev Saude Publica. (2022) 56:105. doi: 10.11606/s1518-8787.2022056004907
46. World Health Organization (WHO). The transition from the acute phase of COVID-19: working towards a paradigm shift for pandemic preparedness and response in the WHO European region. Copenhagen: WHO Regional Office for Europe (2023).
47. Miot, HM. Análise de sobrevivência em estudos clínicos e experimentais. J Vasc Bras. (2017) 16:267–9. doi: 10.1590/1677-5449.001604
48. Qaderi, K, Hosseinirad, H, Kalhor, M, Zangeneh, S, Pournaghi, M, Khodavirdilou, R, et al. The relationship between sex steroids (E2, progesterone, and AMH) levels and severity and fatality of COVID-19: a systematic review. Heliyon. (2023) 9:e14218. doi: 10.1016/j.heliyon.2023.e14218
49. Mauvais-Jarvis, F, Klein, SL, and Levin, ER. Estradiol, progesterone, immunomodulation, and COVID-19 outcomes. Endocrinology. (2020) 161:bqaa127. doi: 10.1210/endocr/bqaa127
50. Chakraborty, B, Byemerwa, J, Krebs, T, Lim, F, Chang, CY, and McDonnell, DP. Estrogen receptor signaling in the immune system. Endocr Rev. (2023) 44:117–41. doi: 10.1210/endrev/bnac017
51. Lippi, G, Sanchis-Gomar, F, and Henry, BM. COVID-19 and its long-term sequelae: what do we know in 2023? Pol Arch Intern Med. (2023) 133:16402. doi: 10.20452/pamw.16402
52. Cocate, PG, Natali, AJ, de Oliveira, A, Alfenas Rde, C, Peluzio Mdo, C, Longo, GZ, et al. Red but not white meat consumption is associated with metabolic syndrome, insulin resistance and lipid peroxidation in Brazilian middle-aged men. Eur J Prev Cardiol. (2015) 22:223–30. doi: 10.1177/2047487313507684
53. Wang, C, Chu, Q, Dong, W, Wang, X, Zhao, W, Dai, X, et al. Microbial metabolite deoxycholic acid-mediated ferroptosis exacerbates high-fat diet-induced colonic inflammation. Mol Metab. (2024) 84:101944. doi: 10.1016/j.molmet.2024.101944
54. Araújo, SP, da Silva, A, Bressan, J, Juvanhol, LL, Castro, LCV, and Hermsdorff, HHM. Fat intake and high triglyceride-glucose index in individuals at cardiometabolic risk: an isocaloric substitution analyses. J Am Nutr Assoc. (2023) 42:452–8. doi: 10.1080/07315724.2022.2064001
55. Rocha, DM, Bressan, J, and Hermsdorff, HH. The role of dietary fatty acid intake in inflammatory gene expression: a critical review. Sao Paulo Med J. (2017) 135:157–68. doi: 10.1590/1516-3180.2016.008607072016
56. Puglisi, MJ, and Fernandez, ML. The health benefits of egg protein. Nutrients. (2022) 14:2904. doi: 10.3390/nu14142904
57. Réhault-Godbert, S, Guyot, N, and Nys, Y. The Golden egg: nutritional value, bioactivities, and emerging benefits for human health. Nutrients. (2019) 11:684. doi: 10.3390/nu11030684
58. Currey, J, Ellsworth, C, Khatun, MS, Wang, C, Chen, Z, Liu, S, et al. Upregulation of inflammatory genes and pathways links obesity to severe COVID-19. Biochim Biophys Acta Mol basis Dis. (2024) 1870:167322. doi: 10.1016/j.bbadis.2024.167322
59. Emamjomeh, A, Mohammadifard, N, Abbasi, M, Askari, M, Taheri, M, Javanbakht, S, et al. Association of obesity and the clinical course of hospitalised COVID-19 survivors. Clin Obes. (2024) 14:e12663. doi: 10.1111/cob.12663
60. Scherer, PE, Kirwan, JP, and Rosen, CJ. Post-acute sequelae of COVID-19: a metabolic perspective. eLife. (2022) 11:e78200. doi: 10.7554/eLife.78200
61. Fedorowski, A, Fanciulli, A, Raj, SR, Sheldon, R, Shibao, CA, and Sutton, R. Cardiovascular autonomic dysfunction in post-COVID-19 syndrome: a major health-care burden. Nat Rev Cardiol. (2024) 21:379–95. doi: 10.1038/s41569-023-00962-3
62. Ren, J, Pang, W, Luo, Y, Cheng, D, Qiu, K, Rao, Y, et al. Impact of allergic rhinitis and asthma on COVID-19 infection, hospitalization, and mortality. J Allergy Clin Immunol Pract. (2022) 10:124–33. doi: 10.1016/j.jaip.2021.10.049
63. Oh, J, Lee, M, Kim, M, Kim, HJ, Lee, SW, Rhee, SY, et al. Incident allergic diseases in post-COVID-19 condition: multinational cohort studies from South Korea, Japan and the UK. Nat Commun. (2024) 15:2830. doi: 10.1038/s41467-024-47176-w
64. Rabiee Rad, M, Abbasi, M, Salimian, E, Norouzi, M, Emamjomeh, A, Haghighatdoost, F, et al. Baseline socioeconomic status predicting post-COVID-19 symptoms: results from Isfahan COVID cohort (ICC) study. Prev Med Rep. (2024) 45:102814. doi: 10.1016/j.pmedr.2024.102814
65. Uddin, S, Khan, A, Lu, H, Zhou, F, Karim, S, Hajati, F, et al. Road networks and socio-demographic factors to explore COVID-19 infection during its different waves. Sci Rep. (2024) 14:1551. doi: 10.1038/s41598-024-51610-w
66. Barrea, L, Grant, WB, Frias-Toral, E, Vetrani, C, Verde, L, de Alteriis, G, et al. Dietary recommendations for post-COVID-19 syndrome. Nutrients. (2022) 14:1305. doi: 10.3390/nu14061305
67. Barrea, L, Verde, L, Grant, WB, Frias-Toral, E, Sarno, G, Vetrani, C, et al. Vitamin D: a role also in long COVID-19? Nutrients. (2022) 14:1625. doi: 10.3390/nu14081625
68. Engin, MMN, and Özdemir, Ö. Role of vitamin D in COVID-19 and other viral infections. World J Virol. (2024) 13:95349. doi: 10.5501/wjv.v13.i3.95349
69. Contreras-Bolívar, V, García-Fontana, B, García-Fontana, C, and Muñoz-Torres, M. Vitamin D and COVID-19: where are we now? Postgrad Med. (2023) 135:195–207. doi: 10.1080/00325481.2021.2017647
70. Ahmad, AS, Juber, NF, Al-Naseri, H, Heumann, C, Ali, R, and Oliver, T. Association between average vitamin D levels and COVID-19 mortality in 19 European countries-a population-based study. Nutrients. (2023) 15:4818. doi: 10.3390/nu15224818
71. de Man, A, Long, MT, and Stoppe, C. Vitamin C for all? Curr Opin Crit Care. (2024) 30:298–304. doi: 10.1097/MCC.0000000000001161
72. Detopoulou, P, Tsouma, C, and Papamikos, V. COVID-19 and nutrition: summary of official recommendations. Top Clin Nutr. (2022) 37:187–202. doi: 10.1097/TIN.0000000000000286
73. Carraro, JC, Hermsdorff, HH, Mansego, ML, Zulet, MÁ, Milagro, FI, Bressan, J, et al. Higher fruit intake is related to TNF-α hypomethylation and better glucose tolerance in healthy subjects. J Nutrigenet Nutrigenomics. (2016) 9:95–105. doi: 10.1159/000448101
74. Hermsdorff, HH, Zulet, MA, Puchau, B, and Martínez, JA. Fruit and vegetable consumption and proinflammatory gene expression from peripheral blood mononuclear cells in young adults: a translational study. Nutr Metab (Lond). (2010) 7:42. doi: 10.1186/1743-7075-7-42
75. Oliveira, TMS, Bressan, J, Pimenta, AM, Martínez-González, MÁ, Shivappa, N, Hébert, JR, et al. Dietary inflammatory index and prevalence of overweight and obesity in Brazilian graduates from the Cohort of Universities of Minas Gerais (CUME project). Nutrition. (2020) 71:110635. doi: 10.1016/j.nut.2019.110635
76. Merino, J, Joshi, AD, Nguyen, LH, Leeming, ER, Mazidi, M, Drew, DA, et al. Diet quality and risk and severity of COVID-19: a prospective cohort study. Gut. (2021) 70:2096–104. doi: 10.1136/gutjnl-2021-325353
77. Seguí-Gómez, M, de la Fuente, C, Vázquez, Z, de Irala, J, and Martínez-González, MA. Cohort profile: the 'Seguimiento Universidad de Navarra' (SUN) study. Int J Epidemiol. (2006) 35:1417–22. doi: 10.1093/ije/dyl223
78. Santos, BF, Oliveira, HN, Miranda, AES, Hermsdorff, HHM, Bressan, J, Vieira, JCM, et al. Research quality assessment: reliability and validation of the self-reported diagnosis of depression for participants of the Cohort of Universities of Minas Gerais (CUME project). J Affect Disord Rep. (2021) 6:100238. doi: 10.1016/j.jadr.2021.100238
Keywords: Post-Acute COVID-19 Syndrome, COVID-19, eating, vaccination, cohort studies
Citation: Brandão ML, Hermsdorff HHM, Leal ACG, Bressan J and Pimenta AM (2025) Vaccination and food consumption: association with Post-Acute COVID-19 Syndrome in Brazilian adults (CUME Study). Front. Nutr. 12:1549747. doi: 10.3389/fnut.2025.1549747
Edited by:
Elma Izze da Silva Magalhães, Federal University of Rio Grande do Sul, BrazilReviewed by:
Corinna Chidley, University of Derby, United KingdomLuz-Ma.-Adriana Balderas-Peña, Instituto Mexicano del Seguro Social, Mexico
Copyright © 2025 Brandão, Hermsdorff, Leal, Bressan and Pimenta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriano Marçal Pimenta, YWRyaWFuby5waW1lbnRhQHVmcHIuYnI=
†These authors have contributed equally to this work and share first authorship