 Xiaosong Li
Xiaosong Li Yuru Lan
Yuru Lan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 14 April 2025
Sec. Nutritional Epidemiology
Volume 12 - 2025 | https://doi.org/10.3389/fnut.2025.1538396
This article is part of the Research TopicNutrition and Mood DisordersView all 6 articles
Introduction: Although previous researches have suggested that certain dietary nutrients, such as carotenoids, have an effect on depression, epidemiological evidence on the relationship between lycopene and depression remains limited. This study aimed to investigate the association between dietary lycopene intake and depression risk in American adults.
Methods: Data from 18,664 participants in the National Health and Nutrition Examination Survey (NHANES, 2007–2016) were analyzed, with depression defined by a nine-item Patient Health Questionnaire (PHQ-9) score ≥ 10. Dietary lycopene intake was estimated from the mean of two 24-h dietary recalls. Binary logistic regression and restricted cubic spline (RCS) models were employed to assess the relationship.
Results: Depression prevalence was 8.98%, and adjusted analyses indicated that higher dietary lycopene intake was significantly associated with a reduced depression risk compared to the lowest quartile (ORs for the second, third, and fourth quartiles: 0.851 [95% CI, 0.737–0.982], 0.829 [95% CI, 0.716–0.960], and 0.807 [95% CI, 0.695–0.938], respectively). Additionally, a U-shaped relationship was observed, with a reduction in depression risk associated with dietary lycopene intake ranging from 0 to 10,072 μg/d (P-non-linear = 0.017).
Discussion: This study suggested that higher dietary lycopene intake may confer a protective effect against depression in American adults.
Depression is a multifactorial mood disorder characterized by persistent emotional disturbances and substantial health impacts (1). In 2008, the World Health Organization identified major depressive disorder as the third leading contributor to the global burden of disease, projecting it to become the leading cause by 2030, highlighting the urgent need for effective prevention and treatment strategies (2, 3). Although existing antidepressant medications have demonstrated some efficacy, their widespread application is constrained by side effects and significant individual variability in treatment response (4, 5). Therefore, exploring novel strategies for the prevention and treatment of depression, particularly through non-pharmacological approaches like dietary interventions, is of significant scientific and clinical importance.
Growing evidence suggest that dietary nutrients and natural products can alleviate depression through various biological mechanisms (6, 7). Lycopene, a potent natural antioxidant, is abundantly present in red fruits and vegetables, including tomatoes, watermelons, and red grapefruits. Its significant anti-inflammatory and antioxidant properties have been extensively documented in studies on various diseases (8–15). Given the roles of oxidative stress and inflammation in the pathophysiology of depression, lycopene’s unique biological properties make it a promising candidate for addressing depression (16–19). The potential role of lycopene in depression remains underexplored, with limited epidemiological evidence and mechanistic studies on its association with depression risk.
By utilizing data from the National Health and Nutrition Examination Survey (NHANES), this study aims to evaluate the association between dietary lycopene intake and depression risk among American adults. Through this research, we aim to offer a scientific basis for dietary interventions in depression and a theoretical foundation for the use of natural products in mental health.
This study analyzed data from five consecutive NHANES cycles (2007–2016). After excluding 24,196 participants without complete depression scale data, 4,003 participants with missing dietary data, 195 pregnant participants and 3,530 participants lacking information on any of the covariates, a final sample of 18,664 participants was included (Figure 1). NHANES protocols were approved by the National Center for Health Statistics Ethics Review Board, and all participants provided written informed consent. As this study utilized only publicly available data, no additional ethical approval was necessary.
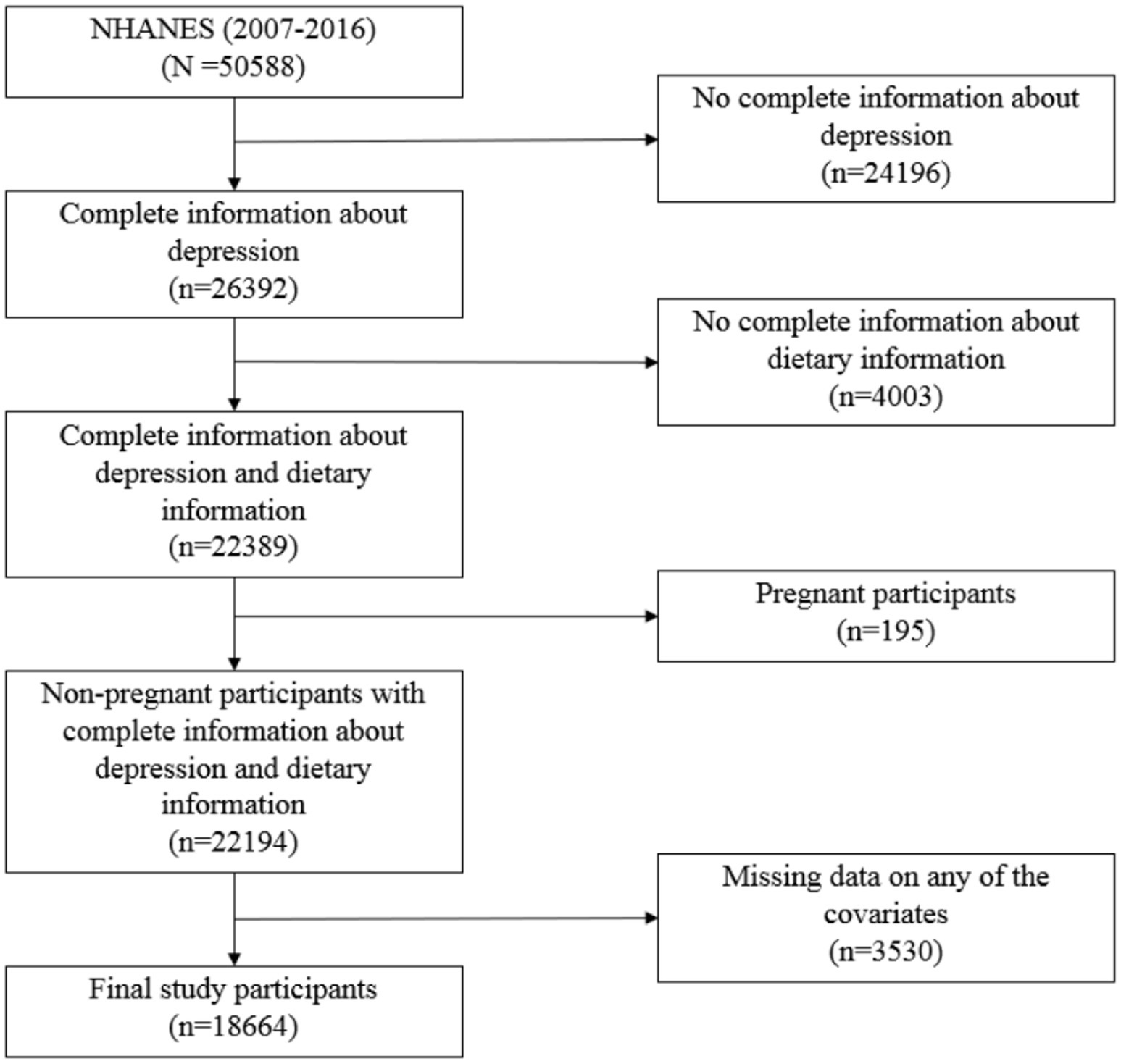
Figure 1. Flowchart of National Health and Nutrition Examination Survey (NHANES) data processing.
Dietary lycopene intake was determined based on participants’ 24-h dietary recall data, including lycopene content from food, beverages, and water (both tap and bottled). The average of two 24-h dietary recalls was used to calculate individual dietary lycopene intake. Participants were categorized into four groups using the quartile method, with the lowest quartile serving as the reference group.
Depression was assessed using the nine-item Patient Health Questionnaire (PHQ-9), a validated tool with moderate consistency compared to clinical psychiatric interviews. The PHQ-9 evaluates depressive status through self-reported symptoms (e.g., appetite, self-esteem, sleep quality, and attention) over the preceding 14 days (20). It includes nine questions scored based on participants’ responses, with a total score of ≥10 indicating depression (21).
To assess the independent association between dietary lycopene intake and depression risk, we adjusted for potential confounders encompassing sociodemographic, behavioral, and health-related variables. Sociodemographic factors included sex (male, female), age (20–44 years, 45–64 years, ≥65 years), race (non-Hispanic White, non-Hispanic Black, Hispanic American, other racial groups), and education level (less than high school, high school or equivalent, above high school). Family income was categorized based on the poverty income ratio (PIR) into low-income (PIR <1), middle-income (1 ≤ PIR < 4), and high-income (PIR ≥ 4) levels (22). Marital status was classified as married/living with a partner, widowed, divorced/separated, or never married (23).
Behavioral factors included BMI, smoking status, drinking status, physical activity, and dietary quality. BMI was grouped as normal/underweight (BMI ≤ 25), overweight (25 < BMI < 30), and obese (BMI ≥ 30) (24). Smoking status was categorized as never smokers (<100 lifetime cigarettes), current smokers (≥100 lifetime cigarettes), and former smokers (had quit smoking) (25). Drinking status was classified as no (<12 drinks in the past 12 months) or yes (≥12 drinks in the past 12 months). Physical activity data, collected using the Global Physical Activity Questionnaire, was categorized as active (≥600 MET-min/week) or inactive (26, 27). Dietary quality was measured using the Healthy Eating Index-2015 (HEI-2015), calculated from two complete 24-h dietary recalls. Scores ranged from 0 to 100 and were categorized into quartiles (28, 29).
Health status included a history of diabetes, defined as a self-reported physician diagnosis (30). These adjustments ensured robust evaluation of the association between dietary lycopene intake and depression risk.
Continuous variables with non-normal distributions are expressed as medians and interquartile ranges, while categorical variables are presented as counts and percentages. Group comparisons of participant characteristics were performed using the Wilcoxon rank-sum test for continuous variables and the χ2 test for categorical variables. Binary logistic regression models were applied to assess the association between dietary lycopene intake and depression risk. Restricted cubic spline (RCS) model was used to examine potential non-linear relationships, with knots placed at the 5th, 50th, and 95th percentiles of dietary lycopene intake. Statistical analyses were conducted using SPSS software (Version 25.0, SPSS Inc., Chicago, IL, United States), and RCS analyses were performed with the “rms” package in R. All tests were two-tailed, and p-values <0.05 were considered statistically significant.
A total of 18,664 participants aged 20 years or older were recruited for this study, including 9,080 men and 9,584 women. Of the participants, 8.9% were diagnosed with depression. The basic characteristics of all participants are summarized in Table 1. Participants with depression had significantly lower dietary lycopene intake compared to those without depression. Notably, more than half (55.07%) of the participants with depression had dietary lycopene intake below the median intake of the entire participants, while in the group without depression, the proportion exhibited a more evenly distributed dietary lycopene intake. Several covariates showed significant differences between the two groups. Adults with depression were more likely to be female, aged 45–64 years, have a low educational level, have a PIR <1, and be widowed, divorced, or separated. They were also more likely to be obese, current smokers, physically inactive, have lower HEI-2015 scores, have diabetes, and report lower dietary lycopene intake. Further analysis revealed that the median dietary lycopene intake among participants without depression was 2,541 μg/d (interquartile range: 764–6,582 μg/d), whereas the median dietary intake for adults with depression was 2,099 μg/d (interquartile range: 418–5,545 μg/d). The Wilcoxon rank-sum test confirmed a significant difference in dietary lycopene intake between the two groups, suggesting a potential association between dietary lycopene intake and depression risk.

Table 1. Characteristics of adults aged 20 years or older according to depression status.
Model 1 was adjusted for sociodemographic variables, including sex, age, race, education level, family income, and marital status. Model 2 included additional adjustments for BMI, smoking status, drinking status, physical activity, and the HEI-2015 score. Model 3 further accounted for diabetes. Compared with participants in the lowest quartile of dietary lycopene intake, those in the second, third, and fourth quartiles had odds ratios (ORs) of 0.839 (95% CI, 0.728–0.966), 0.837 (95% CI, 0.724–0.966), and 0.805 (95% CI, 0.695–0.933), respectively, for the risk of depression after adjusting for demographic factors (Table 2). After adjusting for behavioral and health-related confounders, higher dietary lycopene intake remained significantly associated with a reduced risk of depression, with a further increase in dietary lycopene intake linked to an additional decrease in risk.
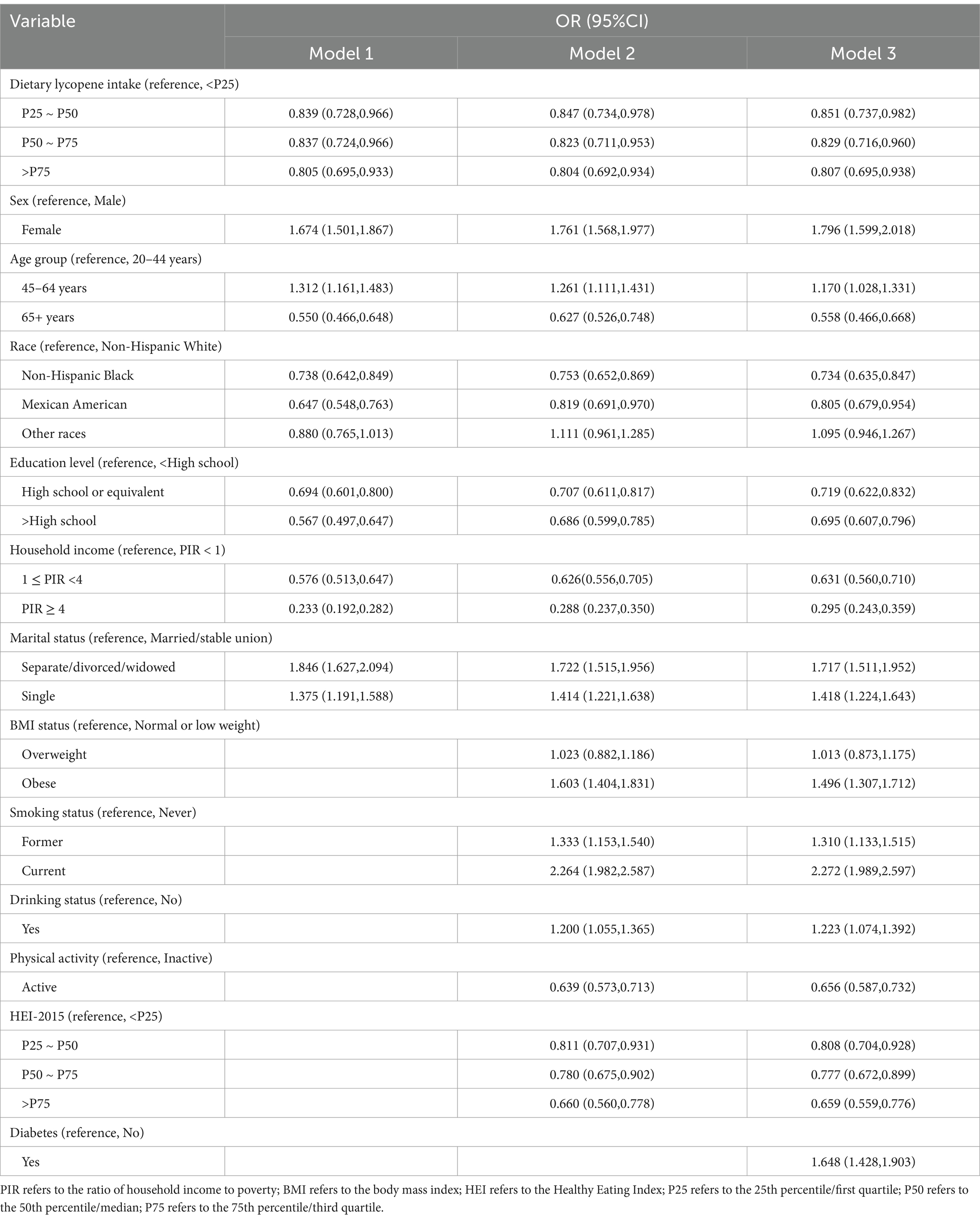
Table 2. Multifactorial analysis of dietary lycopene intake and depression risk.
The binary logistic regression analysis presented in Table 2 indicated an association between dietary lycopene intake and the risk of depression. To further investigate this relationship, RCS analysis was employed. The RCS results confirmed a significant non-linear trend (P-overall <0.001; P-non-linear = 0.017) (Figure 2). After adjusting for potential confounders, the analysis demonstrated that within the intake range of 0–10,072 μg/day, higher dietary lycopene intake was associated with a progressively lower risk of depression, consistent with the binary logistic regression findings. However, beyond this threshold, further increases in dietary lycopene intake reverse the beneficial effect of reducing depression risk.

Figure 2. Restricted cubic spline (RCS) model of the association between dietary lycopene intake and depression risk. CI, confidence interval; OR, odds ratio.
In this study, we investigated the relationship between dietary lycopene intake and depression risk using data from a nationally representative sample of the U.S. population. After comprehensive adjustment for covariates, dietary lycopene intake was consistently associated with a reduced risk of depression across three analytical models. It was also found a threshold point for the protective effect of lycopene against depression.
Existing evidence highlight the multifactorial nature of depression, with diet emerging as a critical modifiable factor (29, 31–34). Several studies have examined the protective role of various carotenoids in depression. A cross-sectional study in American adult population found that levels of five common serum carotenoids were negatively associated with depression risk (35). Similar results have been suggested in studies of older adults, where dietary carotenoid intake was inversely related to depression risk (36–38). A meta-analysis on carotenoid intake and depression risk indicated that higher overall dietary carotenoid intake was associated with a reduced risk of depression (39). However, most of these studies have focused on total carotenoid intake, with few investigations specifically examining the relationship between dietary lycopene intake and depression risk. Lycopene, one of the most potent antioxidants among carotenoids, has garnered significant attention for its potential benefits in neurodegenerative and psychiatric disorders (40–42). A cross-sectional study of individuals aged 70 years and older identified an independent association between a tomato-rich diet and a reduced prevalence of depression, suggesting that such a diet may play a protective role against depression (43). However, it is important to note that older adults are more likely to have multiple diseases, which may affect their mental health, meaning the findings may not be generalizable to the entire population. These findings provide indirect support for the reliability of our results.
The pathophysiology of depression is closely linked to inflammation, with neuroinflammation recognized as a key contributing factor (44–47). Meta-analyses have consistently demonstrated elevated levels of inflammatory markers, such as interleukins and C-reactive protein, in patients with depression, underscoring the role of inflammation in its development (14, 15, 47). Lycopene’s potential antidepressant effects may stem, in part, from its ability to suppress neuroinflammation. Animal studies have shown that lycopene effectively reduces proinflammatory cytokine levels and alleviates neuroinflammatory responses (48, 49). Additionally, lycopene has been reported to improve depressive and anxiety-like behaviors by mitigating neuroinflammation, upregulating neurotrophic factors, and enhancing postsynaptic density protein expression (50).
Depression is also intricately associated with oxidative stress, which arises from an imbalance between reactive oxygen species production and antioxidant defenses. The brain, due to its high oxygen consumption, lipid-rich composition, and relatively weak antioxidant defenses, is particularly vulnerable to oxidative stress, resulting in structural and functional neuronal damage (12). Lycopene has been shown to attenuate oxidative stress and endoplasmic reticulum stress by reducing oxidative markers and inhibiting activation of the protein kinase-like endoplasmic reticulum kinase signaling pathway (51).
In summary, lycopene exerts its beneficial effects on depression through its dual roles in modulating inflammation and oxidative stress, supporting its potential as a dietary strategy for the prevention and management of depression. Notably, the results also revealed an inversion phenomenon in the correlation observed, occurring upon surpassing a particular threshold. This inversion may be attributed to the oversaturation of antioxidant activity. Lycopene, a highly efficacious antioxidant, primarily functions to alleviate oxidative stress by neutralizing free radicals (52). Nevertheless, as the quantity of dietary lycopene intake escalates, the antioxidant system attains a state of saturation, rendering any additional lycopene ineffective in further augmenting antioxidant effects, and consequently, diminishing its overall benefits. This discovery underscores the importance of regulating dietary lycopene intake within a prudent range to maximize its health-promoting benefits.
This study has several notable strengths. First, it utilizes a large, nationally representative sample from NHANES 2007–2016, making it the largest study to explore the relationship between dietary lycopene intake and depression risk. It fills a crucial gap in the epidemiological evidence regarding the association between the two. Second, by combining results from binary logistic regression and RCS models, we have provided evidence of a negative association between them. Third, our study reveals a potential non-linear relationship between dietary lycopene intake and depression risk, identifying a threshold point for the protective effects of lycopene (10,072 μg/day). In conclusion, the findings not only confirm the potential impact of lycopene on depression risk but also offer new perspectives on the role of dietary interventions in psychological health management.
It is important to acknowledge several limitations in this study. First, the cross-sectional design of the study limits the ability to establish causal relationship. Future research should consider designing a cohort study to examine how baseline levels of dietary lycopene intake affect depression risk, which could help clarify the causal relationship. Second, reliance on self-reported 24-h dietary recall data and the PHQ-9 questionnaire introduces the potential for recall bias and reporting bias, which may affect the accuracy of dietary and depression assessments. Furthermore, although this study has accounted for multiple factors in the analysis, there are still unmeasured variables, such as genetic susceptibility, medication use, and other dietary components, which may influence the interpretation of the results. Therefore, the inability to control for these potential confounding factors represents another limitation of this study.
In conclusion, the findings of this study highlight lycopene as a promising dietary intervention worthy of integration into public health strategies. The promotion of increased lycopene consumption may serve as an innovative approach to depression prevention and management, thereby contributing to the enhancement of population mental health outcomes. To optimize the preventive potential of lycopene against depression, achieving an optimal intake level is essential. Based on the analytical results of this study, a daily dietary lycopene intake of approximately 10 mg is recommended for adults. Consuming lycopene with foods rich in healthy fats is advised, as this enhances its absorption and bioavailability. A diversified diet, including an increased intake of tomato-based products, represents an effective strategy for meeting daily lycopene requirements. This study provides novel evidence supporting the role of lycopene in mental health applications. Further research and public health efforts should focus on raising awareness of lycopene’s benefits and encouraging dietary patterns that support mental health.
Despite its limitations, our study first reports an independent association between dietary lycopene intake and the risk of depression, providing a specific intake range (0–10,072 μg/day). This finding addresses the gap in epidemiological evidence linking them and may offer new dietary intervention strategies to reduce the risk of depression. These results provide theoretical support for promoting dietary patterns beneficial to mental health. However, further large-scale prospective studies are required to explore the role of lycopene in depression.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
This study involving humans was approved by the National Center for Health Statistics Ethics Review Board and all participants provided written informed consent. As this study utilized only publicly available data, no additional ethical approval was necessary. This study was conducted in accordance with the local legislation and institutional requirements.
XL: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. YL: Formal analysis, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
We would like to express our gratitude for the publicly accessible data from the NHANES study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Thapar, A, Eyre, O, Patel, V, and Brent, D. Depression in Young people. Lancet. (2022) 400:617–31. doi: 10.1016/S0140-6736(22)01012-1
2. Malhi, GS, and Mann, JJ. Depression. Lancet. (2018) 392:2299–312. doi: 10.1016/S0140-6736(18)31948-2
3. Herrman, H, Patel, V, Kieling, C, Berk, M, Buchweitz, C, Cuijpers, P, et al. Time for united action on depression: a lancet-world psychiatric association commission. Lancet. (2022) 399:957–1022. doi: 10.1016/S0140-6736(21)02141-3
4. Turkmen, C, Machunze, N, Lee, AM, Bougelet, E, Ludin, NM, de Cates, AN, et al. Systematic review and Meta-analysis: the association between newer-generation antidepressants and insomnia in children and adolescents with major depressive disorder. J Am Acad Child Adolesc Psychiatry. (2025) 17:S0890-8567(25)00013-9. doi: 10.1016/j.jaac.2025.01.006
5. Pillinger, T, Howes, OD, Correll, CU, Leucht, S, Huhn, M, Schneider-Thoma, J, et al. Antidepressant and antipsychotic side-effects and personalised prescribing: a systematic review and digital tool development. Lancet Psychiatry. (2023) 10:860–76. doi: 10.1016/S2215-0366(23)00262-6
6. Upton, N. Developing our understanding of nutrition in depression. Br J Nutr. (2022) 127:1010–7. doi: 10.1017/S0007114521001744
7. Businaro, R, Vauzour, D, Sarris, J, Munch, G, Gyengesi, E, Brogelli, L, et al. Therapeutic opportunities for food supplements in neurodegenerative disease and depression. Front Nutr. (2021) 8:669846. doi: 10.3389/fnut.2021.669846
8. Joshi, B, Kar, SK, Yadav, PK, Yadav, S, Shrestha, L, and Bera, TK. Therapeutic and medicinal uses of lycopene: a systematic review. Int J Res Med Sci. (2020) 8:1195. doi: 10.18203/2320-6012.ijrms20200804
9. Zhu, R, Chen, B, Bai, Y, Miao, T, Rui, L, Zhang, H, et al. Lycopene in protection against obesity and diabetes: a mechanistic review. Pharmacol Res. (2020) 159:104966. doi: 10.1016/j.phrs.2020.104966
10. Ratto, F, Franchini, F, Musicco, M, Caruso, G, and Di Santo, SG. A narrative review on the potential of tomato and lycopene for the prevention of Alzheimer's disease and other dementias. Crit Rev Food Sci Nutr. (2022) 62:4970–81. doi: 10.1080/10408398.2021.1880363
11. Hsieh, MJ, Huang, CY, Kiefer, R, Lee, SD, Maurya, N, and Velmurugan, BK. Cardiovascular disease and possible ways in which lycopene acts as an efficient cardio-protectant against different cardiovascular risk factors. Molecules. (2022) 27:27 (10). doi: 10.3390/molecules27103235
12. Bhatt, S, Nagappa, AN, and Patil, CR. Role of oxidative stress in depression. Drug Discov Today. (2020) 25:1270–6. doi: 10.1016/j.drudis.2020.05.001
13. Przybylska, S. Lycopene – a bioactive carotenoid offering multiple health benefits: a review. Int J Food Sci Technol. (2019) 55:11–32. doi: 10.1111/ijfs.14260
14. Dowlati, Y, Herrmann, N, Swardfager, W, Liu, H, Sham, L, Reim, EK, et al. A Meta-analysis of cytokines in major depression. Biol Psychiatry. (2010) 67:446–57. doi: 10.1016/j.biopsych.2009.09.033
15. Howren, MB, Lamkin, DM, and Suls, J. Associations of depression with C-reactive protein, Il-1, and Il-6: a Meta-analysis. Psychosom Med. (2009) 71:171–86. doi: 10.1097/PSY.0b013e3181907c1b
16. Wei, Y, Gao, H, Luo, Y, Feng, J, Li, G, Wang, T, et al. Systemic inflammation and oxidative stress markers in patients with unipolar and bipolar depression: a large-scale study. J Affect Disord. (2024) 346:154–66. doi: 10.1016/j.jad.2023.10.156
17. Miller, AH, Maletic, V, and Raison, CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. (2009) 65:732–41. doi: 10.1016/j.biopsych.2008.11.029
18. Hassamal, S. Chronic stress, Neuroinflammation, and depression: an overview of pathophysiological mechanisms and emerging anti-Inflammatories. Front Psych. (2023) 14:1130989. doi: 10.3389/fpsyt.2023.1130989
19. Correia, AS, Cardoso, A, and Vale, N. Oxidative stress in depression: the link with the stress response, Neuroinflammation, serotonin, neurogenesis and synaptic plasticity. Antioxidants. (2023) 12:470. doi: 10.3390/antiox12020470
20. Kroenke, K, Spitzer, RL, and Williams, JB. The Phq-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
21. Wei, J, Lu, Y, Li, K, Goodman, M, and Xu, H. The associations of late-life depression with all-cause and cardiovascular mortality: the Nhanes 2005-2014. J Affect Disord. (2022) 300:189–94. doi: 10.1016/j.jad.2021.12.104
22. Yi, H, Li, M, Dong, Y, Gan, Z, He, L, Li, X, et al. Non-linear associations between the ratio of family income to poverty and all-cause mortality among adults in Nhanes study. Sci Rep. (2024) 14:12018. doi: 10.1038/s41598-024-63058-z
23. Araujo, ML, Mendonca, RD, Lopes Filho, JD, and Lopes, ACS. Association between food insecurity and food intake. Nutrition. (2018) 54:54–9. doi: 10.1016/j.nut.2018.02.023
24. Dreimuller, N, Lieb, K, Tadic, A, Engelmann, J, Wollschlager, D, and Wagner, S. Body mass index (Bmi) in major depressive disorder and its effects on depressive symptomatology and antidepressant response. J Affect Disord. (2019) 256:524–31. doi: 10.1016/j.jad.2019.06.067
25. Ssy, AL, Natto, ZS, Midle, JB, Gyurko, R, O'Neill, R, and Steffensen, B. Association between time since quitting smoking and periodontitis in former smokers in the National Health and nutrition examination surveys (Nhanes) 2009 to 2012. J Periodontol. (2019) 90:16–25. doi: 10.1002/JPER.18-0183
26. Cleland, CL, Hunter, RF, Kee, F, Cupples, ME, Sallis, JF, and Tully, MA. Validity of the global physical activity questionnaire (Gpaq) in assessing levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health. (2014) 14:1255. doi: 10.1186/1471-2458-14-1255
27. Vilar-Gomez, E, Nephew, LD, Vuppalanchi, R, Gawrieh, S, Mladenovic, A, Pike, F, et al. High-quality diet, physical activity, and college education are associated with low risk of Nafld among the us population. Hepatology. (2022) 75:1491–506. doi: 10.1002/hep.32207
28. De La Cruz, N, Shabaneh, O, and Appiah, D. The Association of Ideal Cardiovascular Health and Ocular Diseases among us adults. Am J Med. (2021) 134:252–259.e1. doi: 10.1016/j.amjmed.2020.06.004
29. Wang, K, Zhao, Y, Nie, J, Xu, H, Yu, C, and Wang, S. Higher Hei-2015 score is associated with reduced risk of depression: result from Nhanes 2005-2016. Nutrients. (2021) 13:348. doi: 10.3390/nu13020348
30. Menke, A, Casagrande, S, Geiss, L, and Cowie, CC. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA. (2015) 314:1021–9. doi: 10.1001/jama.2015.10029
31. Liang, J, Huang, S, Jiang, N, Kakaer, A, Chen, Y, Liu, M, et al. Association between joint physical activity and dietary quality and lower risk of depression symptoms in us adults: cross-sectional Nhanes study. JMIR Public Health Surveill. (2023) 9:e45776. doi: 10.2196/45776
32. Xu, Q, Qian, X, Sun, F, Liu, H, Dou, Z, and Zhang, J. Independent and joint associations of dietary antioxidant intake with risk of post-stroke depression and all-cause mortality. J Affect Disord. (2023) 322:84–90. doi: 10.1016/j.jad.2022.11.013
33. Gomez-Gomez, I, Bellon, JA, Resurreccion, DM, Cuijpers, P, Moreno-Peral, P, Rigabert, A, et al. Effectiveness of universal multiple-risk lifestyle interventions in reducing depressive symptoms: systematic review and Meta-analysis. Prev Med. (2020) 134:106067. doi: 10.1016/j.ypmed.2020.106067
34. Feng, Q, Liu, F, Nie, J, Yang, Y, Li, X, and Wang, S. The associations between dietary flavonoids intake and risk of depressive symptom in diabetic patients: data from Nhanes 2007-2008, 2009-2010, and 2017-2018. J Affect Disord. (2024) 359:226–33. doi: 10.1016/j.jad.2024.05.069
35. Zhang, W, Cheng, Z, Lin, H, Fu, F, and Zhan, Z. Serum carotenoid levels inversely correlate with depressive symptoms among adults: insights from Nhanes data. J Affect Disord. (2024) 362:869–76. doi: 10.1016/j.jad.2024.07.021
36. Payne, ME, Steck, SE, George, RR, and Steffens, DC. Fruit, vegetable, and antioxidant intakes are lower in older adults with depression. J Acad Nutr Diet. (2012) 112:2022–7. doi: 10.1016/j.jand.2012.08.026
37. Milaneschi, Y, Bandinelli, S, Penninx, BW, Corsi, AM, Lauretani, F, Vazzana, R, et al. The relationship between plasma carotenoids and depressive symptoms in older persons. World J Biol Psychiatry. (2012) 13:588–98. doi: 10.3109/15622975.2011.597876
38. Lai, JS, Oldmeadow, C, Hure, AJ, McEvoy, M, Hiles, SA, Boyle, M, et al. Inflammation mediates the association between fatty acid intake and depression in older men and women. Nutr Res. (2016) 36:234–45. doi: 10.1016/j.nutres.2015.11.017
39. Yu, Q, Xue, F, Li, Z, Li, X, Ai, L, Jin, M, et al. Dietary intake of carotenoids and risk of depressive symptoms: a systematic review and Meta-analysis. Antioxidants. (2022) 11:2205. doi: 10.3390/antiox11112205
40. Chen, D, Huang, C, and Chen, Z. A review for the pharmacological effect of lycopene in central nervous system disorders. Biomed Pharmacother. (2019) 111:791–801. doi: 10.1016/j.biopha.2018.12.151
41. Lei, X, Lei, L, Zhang, Z, and Cheng, Y. Neuroprotective effects of lycopene pretreatment on transient global cerebral ischemia-reperfusion in rats: the role of the Nrf 2/ho-1 signaling pathway. Mol Med Rep. (2016) 13:412–8. doi: 10.3892/mmr.2015.4534
42. Prema, A, Janakiraman, U, Manivasagam, T, and Thenmozhi, AJ. Neuroprotective effect of lycopene against Mptp induced experimental Parkinson's disease in mice. Neurosci Lett. (2015) 599:12–9. doi: 10.1016/j.neulet.2015.05.024
43. Niu, K, Guo, H, Kakizaki, M, Cui, Y, Ohmori-Matsuda, K, Guan, L, et al. A tomato-rich diet is related to depressive symptoms among an elderly population aged 70 years and over: a population-based, cross-sectional analysis. J Affect Disord. (2013) 144:165–70. doi: 10.1016/j.jad.2012.04.040
44. Beurel, E, Toups, M, and Nemeroff, CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. (2020) 107:234–56. doi: 10.1016/j.neuron.2020.06.002
45. Colasanto, M, Madigan, S, and Korczak, DJ. Depression and inflammation among children and adolescents: a meta-analysis. J Affect Disord. (2020) 277:940–8. doi: 10.1016/j.jad.2020.09.025
46. Kiecolt-Glaser, JK, Derry, HM, and Fagundes, CP. Inflammation: depression fans the flames and feasts on the heat. Am J Psychiatry. (2015) 172:1075–91. doi: 10.1176/appi.ajp.2015.15020152
47. Kohler, CA, Freitas, TH, Maes, M, de Andrade, NQ, Liu, CS, Fernandes, BS, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. (2017) 135:373–87. doi: 10.1111/acps.12698
48. Wang, YL, Han, QQ, Gong, WQ, Pan, DH, Wang, LZ, Hu, W, et al. Microglial activation mediates chronic mild stress-induced depressive-and anxiety-like behavior in adult rats. J Neuroinflammation. (2018) 15:21. doi: 10.1186/s12974-018-1054-3
49. Zhang, F, Fu, Y, Zhou, X, Pan, W, Shi, Y, Wang, M, et al. Depression-like behaviors and heme oxygenase-1 are regulated by lycopene in lipopolysaccharide-induced neuroinflammation. J Neuroimmunol. (2016) 298:1–8. doi: 10.1016/j.jneuroim.2016.06.001
50. Zhao, B, Wu, J, Li, J, Bai, Y, Luo, Y, Ji, B, et al. Lycopene alleviates Dss-induced colitis and behavioral disorders via mediating microbes-gut-brain Axis balance. J Agric Food Chem. (2020) 68:3963–75. doi: 10.1021/acs.jafc.0c00196
51. Ou, S, Fang, Y, Tang, H, Wu, T, Chen, L, Jiang, M, et al. Lycopene protects neuroblastoma cells against oxidative damage via depression of Er stress. J Food Sci. (2020) 85:3552–61. doi: 10.1111/1750-3841.15419
Keywords: dietary lycopene intake, depression, NHANES, diet, lifestyle
Citation: Li X and Lan Y (2025) Association between higher dietary lycopene intake and reduced depression risk among American adults: evidence from NHANES 2007–2016. Front. Nutr. 12:1538396. doi: 10.3389/fnut.2025.1538396
Edited by:
Samiksha Wasnik, Independent Researcher, Gilroy, CA, United StatesReviewed by:
Smriti Gaur, Jaypee Institute of Information Technology, IndiaCopyright © 2025 Li and Lan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaosong Li, Y2N3c3N5bEAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.