 Camila Lima Chagas1
Camila Lima Chagas1 Nadja Fernandes da Silva1Isa Galvão Rodrigues2,3Gabriela Maria Pereira Floro Arcoverde1,3Victoria Domingues Ferraz1Dário Celestino Sobral Filho2,3Alcides da Silva Diniz1
Nadja Fernandes da Silva1Isa Galvão Rodrigues2,3Gabriela Maria Pereira Floro Arcoverde1,3Victoria Domingues Ferraz1Dário Celestino Sobral Filho2,3Alcides da Silva Diniz1 Cláudia Porto Sabino Pinho1,3Poliana Coelho Cabral1Ilma Kruze Grande de Arruda1*
Cláudia Porto Sabino Pinho1,3Poliana Coelho Cabral1Ilma Kruze Grande de Arruda1*- 1Universidade Federal de Pernambuco - UFPE, Recife, Brazil
- 2Universidade de Pernambuco - UPE, Recife, Brazil
- 3Pronto Socorro Universitário Cardiológico de Pernambuco – PROCAPE, Recife, Brazil
Background: Abdominal adipose tissue consists of visceral and subcutaneous fat deposits, each with unique metabolic and functional properties. Identifying the characteristics that influence different obesity phenotypes can support targeted prevention and intervention strategies.
Objective: To identify predictive factors associated with visceral and subcutaneous adipose tissue accumulation.
Methods: This is a cross-sectional study including adults of both sexes aged ≥20 years under outpatient care in a public healthcare service in Northeast Brazil. Visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) were measured via ultrasound. Anthropometric, clinical, sociodemographic, and behavioral variables were incorporated into the predictive model.
Results: A total of 347 individuals were included. They were median age of 47.0 years (interquartile range: 39.0 to 56.0). Visceral obesity was found in 79.3% of the sample. Adjusted analysis demonstrated that physical inactivity (OR 2.3; 95% CI 1.1–4.7; p = 0.023) and elevated waist circumference (WC) (OR 6.4; 95% CI 2.6–15.8 p < 0.001) were associated with VAT accumulation. Alcohol consumption increased the likelihood of SAT accumulation by 2.2 times (95% CI 1.3–3.7; p = 0.005), while elevated WC raised this likelihood by 4.5 times (95% CI 2.1–9.8; p < 0.001). The VAT/SAT ratio was significantly higher in older adults (OR 5.5; 95%CI 2.0–14.8; p = 0.001), among individuals of Mixed Race and Black, those with lower educational levels (OR 2.4; 95%CI 1.1–5.2; p = 0.028), and in diabetics (OR 2.4; 95%CI 1.2–4.9; p = 0.017).
Conclusion: Distinct factors influence visceral and subcutaneous obesity. Sedentary behavior emerged as an independent predictor of visceral obesity, while alcohol consumption was associated with a subcutaneous obesity pattern. Diabetes and sociodemographic factors (older age, non-White race, and lower education) were predictive of an elevated VAT/SAT ratio.
1 Introduction
Obesity is a chronic, complex, and multifactorial condition involving biological, psychosocial, socioeconomic, and environmental factors. Obesity can result from high intake of poor-quality foods combined with low energy expenditure (1). Obesity is a serious public health challenge; in recent decades, its prevalence has tripled worldwide, emerging as a major cause of mortality and disability with significant impact on adult morbidity patterns. According to estimates from the World Health Organization (WHO), 2.5 billion adults were classified as overweight in 2022, and in the previous year, obesity contributed to approximately 2.8 million deaths due to non-communicable diseases (NCDs) (2, 3).
Adipose tissue serves multiple functions, primarily as an energy reservoir (4, 5). However, body fat distribution is an additional crucial predictor of cardiovascular risk (4, 5). Abdominal fat comprises subcutaneous and visceral fat, each of which poses distinct risks for metabolic and hemodynamic changes (6). Roughly 80% of total body fat is located subcutaneously, predominantly in the gluteofemoral region, back, and anterior abdominal wall. Visceral fat, however, constitutes 10–20% of total fat in men and 5–8% in women (7) and is located around the viscera and peritoneum, bordering the dorsal side of the intestine and the ventral surface of the kidney (4).
Subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT) differ in morphology and function. SAT drains venously through the systemic circulation, whereas VAT is perfused by the portal circulation (8, 9), rendering VAT metabolically more active and a greater source of inflammatory cytokines (4, 7, 10). Consequently, the lipolytic activity of abdominal VAT constantly releases free fatty acids, which, drained by the portal vein, accumulate in the liver, leading to alterations in lipid and glucose metabolism (7) and directly contributing to the rise in chronic diseases (6, 11). However, the absolute VAT quantification individually may not fully reflect an individual’s risk for visceral obesity. The VAT/SAT ratio is considered as an alternative and appropriate indicator, as it reflects both visceral fat accumulation and an individual’s predisposition to preferentially store fat viscerally (12, 13). This ratio has also been described as a proxy for cardiometabolic risk (13).
The deleterious effects of excessive body fat are extensive; however, the tendency to store fat in different locations under conditions of excess energy intake varies greatly between individuals (14). Despite this, there remain significant gaps in understanding the profiles of individuals at higher risk of accumulating abdominal fat in either subcutaneous or visceral deposits. Therefore, the objective of this study was to assess the predictive factors influencing the accumulation of subcutaneous and visceral adipose tissue. This approach potentially contributes to identifying characteristics that define subcutaneous and visceral abdominal obesity phenotypes, guiding targeted intervention strategies.
2 Materials and methods
This is a cross-sectional study conducted at a public university hospital specializing in cardiology in Northeastern Brazil. Volunteers of both genders aged ≥20 years, receiving outpatient care at a public university hospital in Northeast Brazil, were included. At this outpatient clinic, the population is predominantly composed of individuals with chronic non-infectious diseases: systemic arterial hypertension, diabetes mellitus, metabolic syndrome, and dyslipidemia.
All patients provided informed consent and the study protocol adhered to ethical standards for research involving human subjects and was approved under protocol number 4.659.262/2021. Exclusion criteria were individuals with hepatomegaly and/or splenomegaly, ascites, recent abdominal surgery, underwent surgical weight loss treatment, pregnancy, or had given birth within 6 months prior to the study screening. Participants with physical limitations precluding anthropometric measurements were also excluded, as these conditions could affect intra-abdominal fat measurement.
Sample size was calculated using the STATCALC module in Epi Info software, version 6.04 [WHO/CDC, Atlanta, GA, United States], based on a visceral obesity prevalence of 68.3%, obtained from a pilot study involving the first 30 patients. A 5.0% standard error and a 95% confidence interval were applied, resulting in a minimum required sample of 333 patients. To account for potential losses, the sample size was increased by 10%, leading to a final sample size of 367 individuals.
VAT and SAT were assessed using ultrasound (US) with a Vivid T8 Pro Color Doppler Ultrasound System (GE, P.O., Asia). All participants were evaluated in the supine position, with the right arm raised and a minimum fasting period of 4 h (15, 16). A 3.5 MHz convex electronic transducer was positioned transversely 1 cm above the umbilical scar. Visceral fat thickness was defined as the greatest distance, in centimeters, between the inner (deep) surface of the rectus abdominis muscle and the anterior wall of the aorta. Subcutaneous fat thickness was measured as the distance, in centimeters, between the skin and the upper surface of the rectus abdominis muscle (16). Measurements were taken with participants exhaling and without abdominal pressure to avoid underestimation. Each measurement was taken twice and repeated if the measurement error exceeded 0.1 cm (16).
Cut-off values for visceral obesity were set at VAT ≥5.39 cm for men and ≥ 4.27 cm for women (17). Subcutaneous obesity was defined by SAT values above the upper tertile for each sex, with thresholds of ≥2.83 cm for men and ≥ 3.68 cm for women (18). The visceral-to-subcutaneous fat ratio (VAT/SAT) was calculated, with values above the highest tertile for each sex (≥3.60 for men and ≥ 2.14 for women) used as indicators of visceral fat accumulation predisposition and as criteria for elevated VAT/SAT ratio. Among anthropometric parameters, body mass index (BMI) was calculated using the equation weight/height2, following WHO classifications (19). Waist circumference (WC) was measured at the narrowest point between the last rib and the iliac crest (20) and classified as WC ≥94 cm for men and ≥ 80 cm for women to indicate higher values (19).
Weight (kg) and height (m) were measured according to techniques recommended by Lohman et al. (20), using an electronic scale (Welmy®, Santa Bárbara d’Oeste, São Paulo, Brazil) with a capacity of 150 kg and an accuracy of 100 g, equipped with an attached stadiometer precise to 1 mm. For WC (cm) measurement, a flexible, non-elastic measuring tape with 0.1 cm accuracy was used. Measurements were collected twice by trained observers, with additional measurements taken if discrepancies greater than 1 cm or 100 g were noted.
Sociodemographic variables included age, sex, self-reported race & ethnicity (categorized as White, Black, and Mixed race), years of education, per capita family income, and socioeconomic status. Clinical variables included hypertension and diabetes mellitus, defined by prior medical diagnosis, use of antihypertensive, oral hypoglycemic, or insulin medications, and recorded in the participant’s medical records. To determine socioeconomic status, the “Brazilian Economic Classification Criteria” established by the Brazilian Association of Anthropology and the Brazilian Association of Research Companies (21) was used. This tool scores household possessions and the education level of the family head, classifying individuals into economic classes A1, A2, B1, B2, C1, C2, D, and E, from highest to lowest purchasing power (21). These economic classes were subsequently recategorized into high (A1 and B1), middle (B2 and C1), and low (C2, D, and E) socioeconomic status (22).
Behavioral variables included alcohol consumption, smoking, and physical activity level. Smoking status was categorized as smoker (individual currently smoking), non-smoker (individual who never smoked or quit over 10 years ago), and former smoker (individual who quit between one and 10 years before the study) (23). Alcohol consumption was recorded as a dichotomous variable (“yes” or “no”). To assess physical activity, the International Physical Activity Questionnaire (IPAQ) short version was used, covering four domains of physical activity: leisure, household activities, occupational activities, and transportation-related activities. A physical activity score in minutes per week was calculated by summing the time spent on all activities, with <150 min per week serving as the cutoff for classifying individuals as insufficiently active or sedentary (24, 25).
Data were analyzed using the Statistical Package for Social Sciences – SPSS version 13.0 (IBM® Inc., Chicago, IL, United States). Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Variables with a normal distribution were described using mean and standard deviation, while non-Gaussian variables were presented as medians and interquartile ranges. Proportions were reported with a 95% confidence interval using a binomial approximation to the normal distribution. Intra- and inter-observer reproducibility of the US measurements was evaluated using the intraclass correlation coefficient and 95% limits of agreement, with triplicate measurements for each anatomical site.
A univariate analysis was conducted between the dependent variables (visceral and subcutaneous obesity) and the independent variables, using the Chi-square test and determining prevalence ratios (PR) with their 95% confidence intervals. To examine the independence of associations between dependent and independent variables, a multivariable binary logistic regression model was developed. Independent variables were tested for multicollinearity using Variance Inflation Factor (VIF) and Tolerance statistics (>0.10 and < 3). Logistic regression was performed using the purposeful selection method, where variables associated with the outcome with p < 0.20 in univariate analysis were included. Equality of hypotheses was rejected for p < 0.05.
3 Results
Intra- and inter-observer calibration evaluation for US procedures demonstrated a high inter-observer reproducibility, with Intraclass Correlation Coefficients (ICC) exceeding 0.97 for VAT and greater than 0.98 for SAT. Intra-observer reproducibility was also high, with ICC values above 0.90 for all VAT and SAT assessments.
A total of 367 patients were initially screened. Following exclusions (data inconsistencies or refusal), the final sample included 347 individuals. They were most women (66.3%), with a median age of 47.0 years (interquartile range: 39.0–56.0). A total of 78.8% of the sample presented with more than 9 years of education, and 62.0% classified as middle to low socioeconomic status. Hypertension and diabetes mellitus was found in 47.3 and 25.1%, respectively. Around 75% of the participants were insufficiently active, and 92.0% were overweight by BMI. The prevalence of visceral obesity was 79.3% (Table 1).
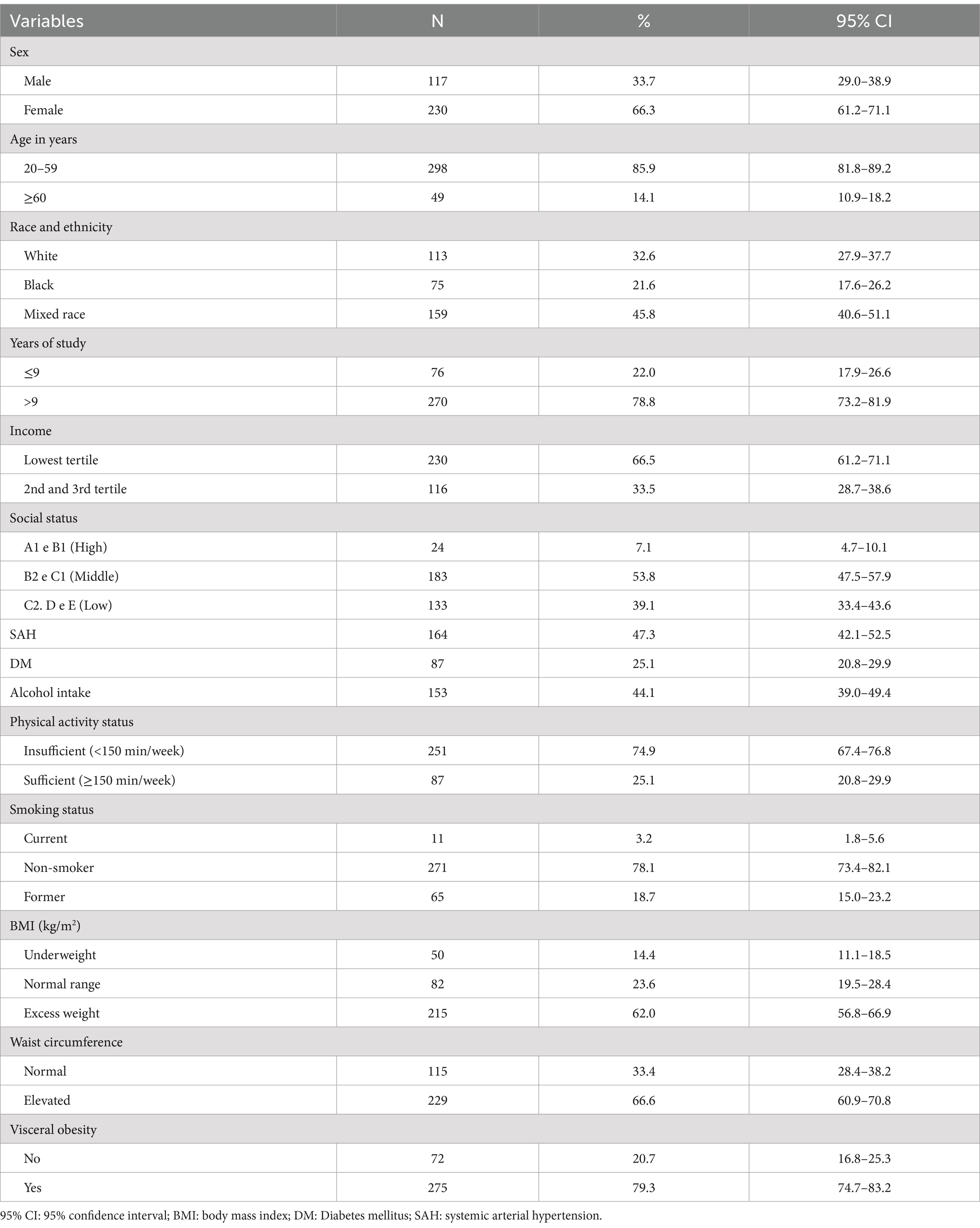
Table 1. Characteristics of the sample (N = 347).
Univariate analyses are detailed in Tables 2–4. Visceral obesity was associated with female sex, age ≥ 60 years, lower education level, higher income, lower social class, hypertension, diabetes, physical inactivity, smoking (current or former), overweight, and elevated waist circumference. Higher subcutaneous fat accumulation was associated with age (more common in individuals aged 20–59), higher education, absence of diabetes, alcohol consumption, normal weight, and elevated WC. An elevated VAT/SAT ratio was associated with older age, lower education level, higher income, hypertension, diabetes, current or former smoking, overweight, elevated waist circumference, and abstention from alcohol consumption.
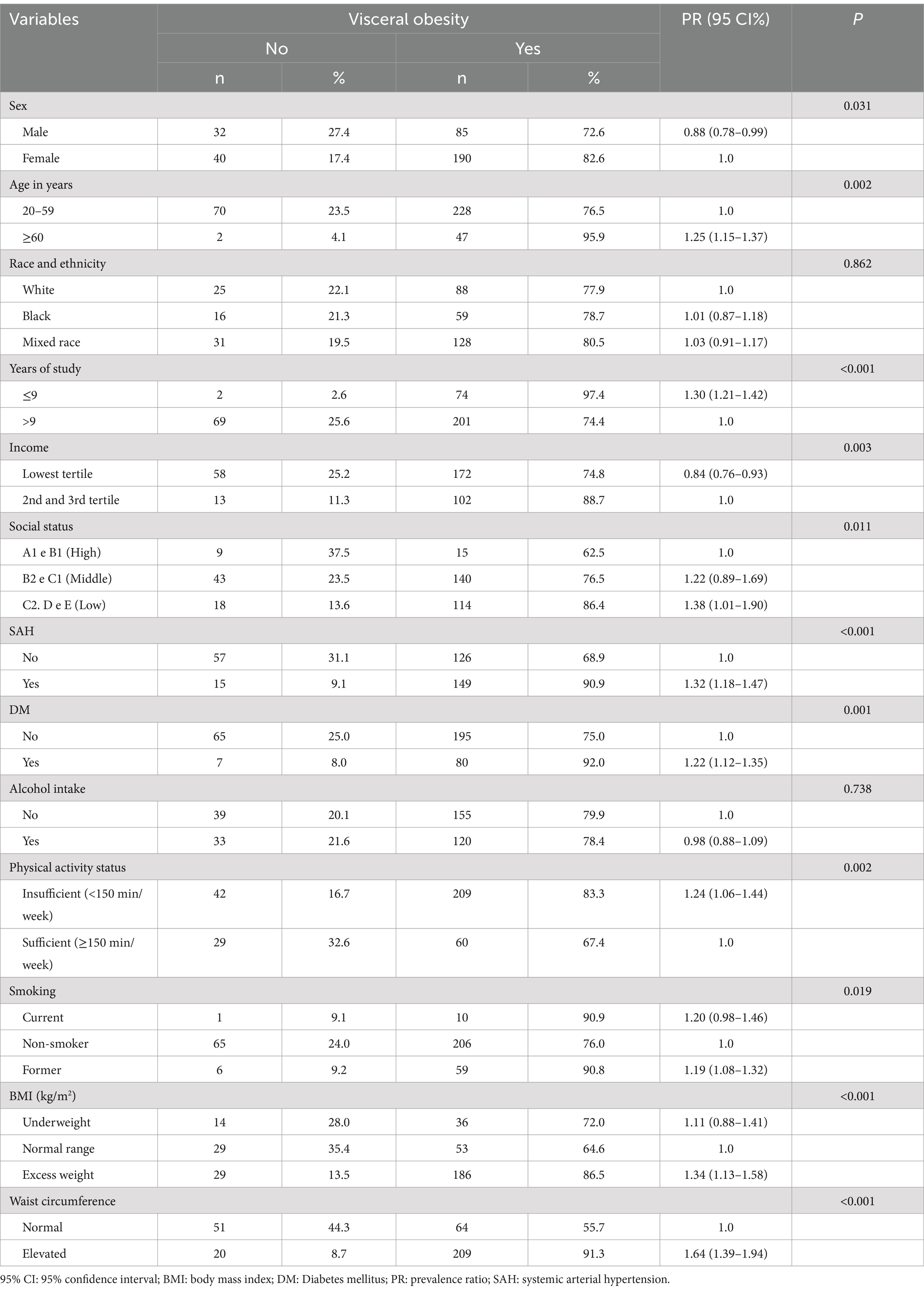
Table 2. Factors associated with visceral adiposity among outpatients from a university cardiology hospital (N = 347).
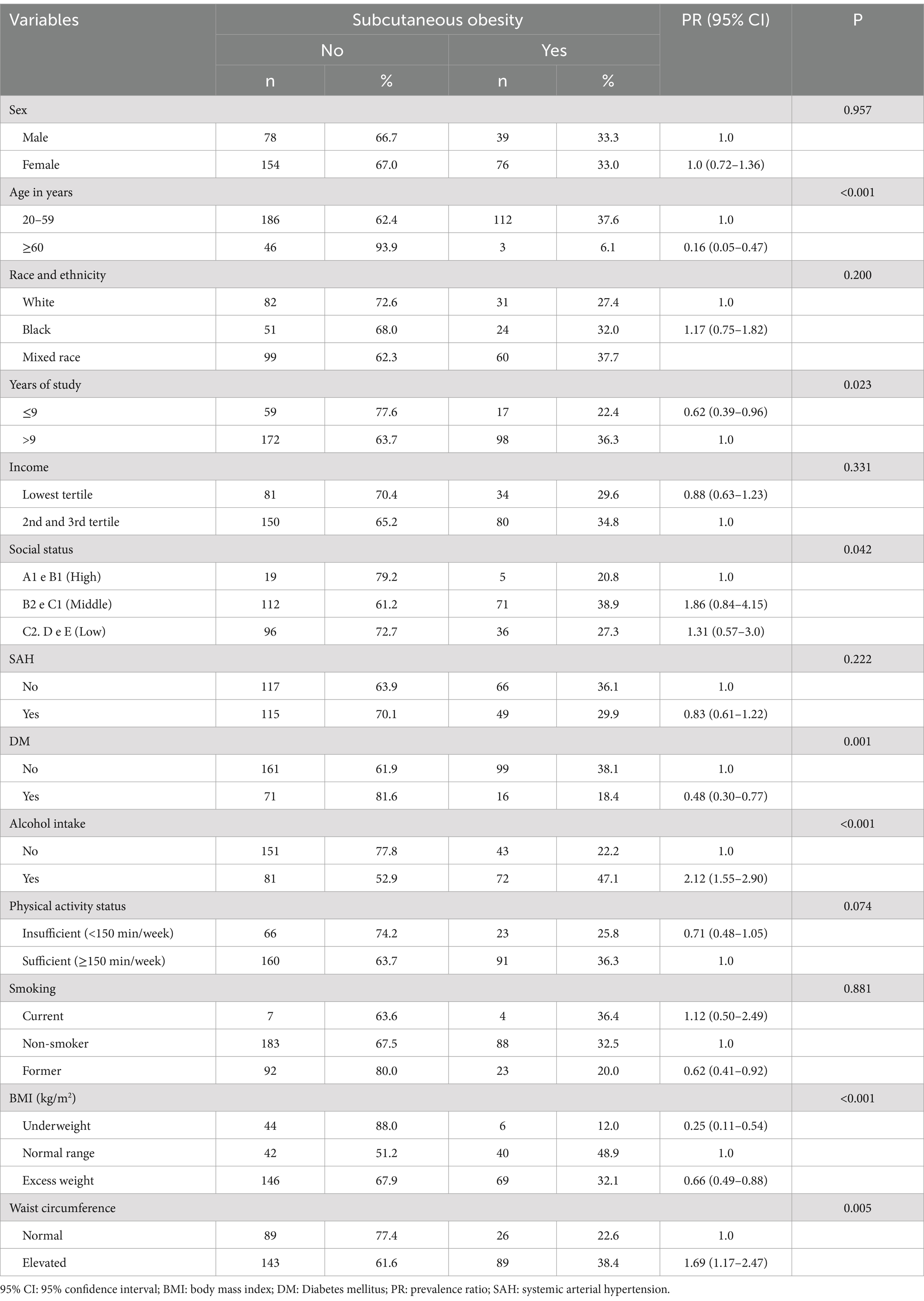
Table 3. Factors associated with subcutaneous adiposity among outpatients from a university cardiology hospital (N = 347).
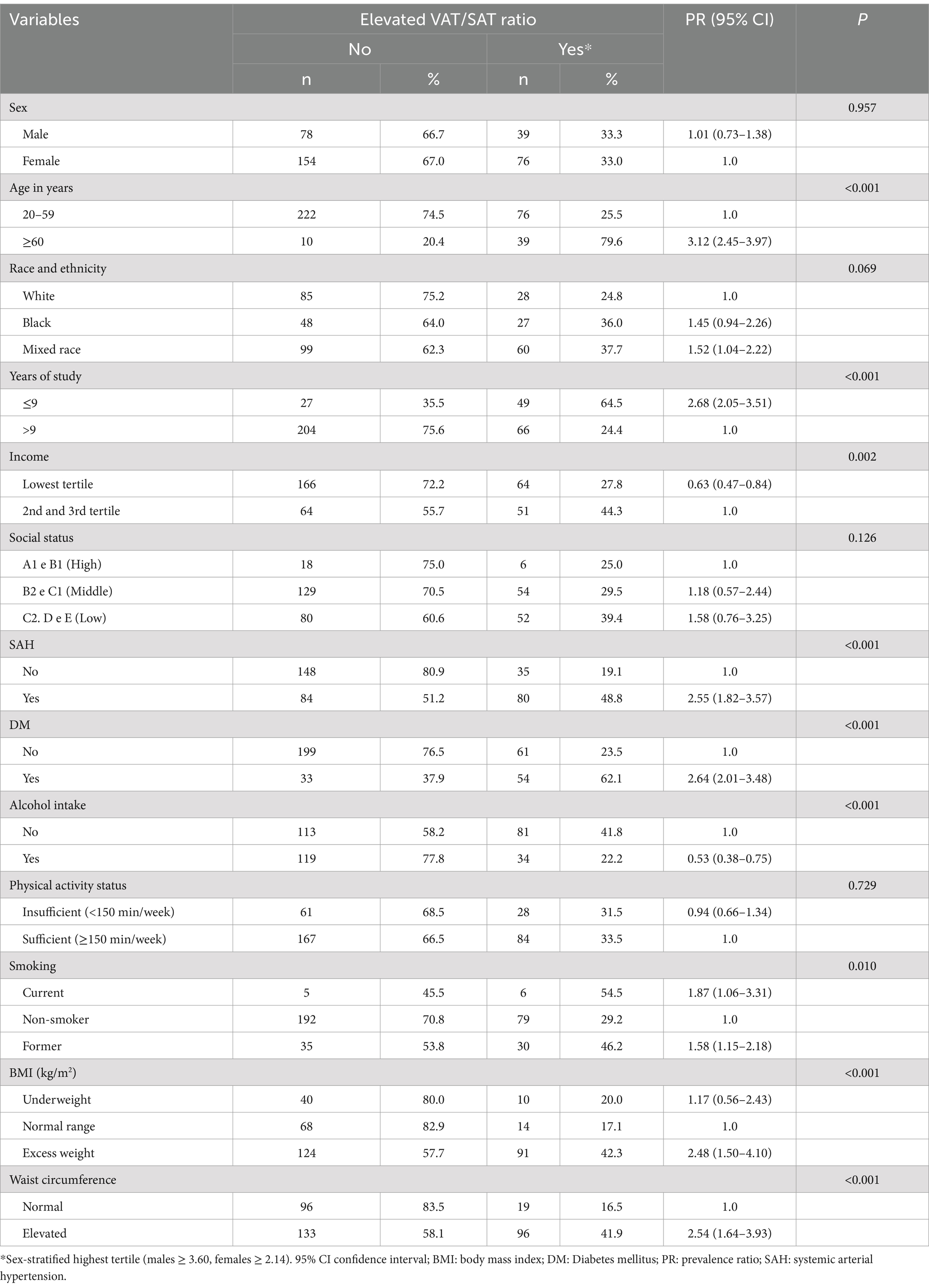
Table 4. Factors associated with elevated VAT/SAT ratio among outpatients from a university cardiology hospital (N = 347).
After adjusting for confounders, only physical inactivity and elevated WC remained associated with VAT accumulation, with an odds ratio of 2.3 (95% CI 1.1–4.7; p = 0.023) for visceral obesity in sedentary individuals and 6.4 (95% CI 2.6–15.8; p < 0.001) for individuals with elevated waist circumference. Regarding subcutaneous obesity, older adults, individuals with malnutrition, and those with BMI >25 kg/m2 were protected against SAT accumulation, while alcohol consumption increased the odds of SAT accumulation by 2.2 times (95% CI 1.3–3.7; p = 0.005), and elevated waist circumference increased this likelihood by 4.5 times (95% CI 2.1–9.8; p < 0.001). An elevated VAT/SAT ratio was more common among older adults (OR 5.5; 95% CI 2.0–14.8; p = 0.001), individuals of Mixed Race and Black, those with lower education (OR 2.4; 95% CI 1.1–5.2; p = 0.028), and diabetics (OR 2.4; 95% CI 1.2–4.9; p = 0.017). Alcohol consumption provided protection against an elevated VAT/SAT ratio (OR 0.5; 95% CI 0.2–0.9; p = 0.015) (Table 5).
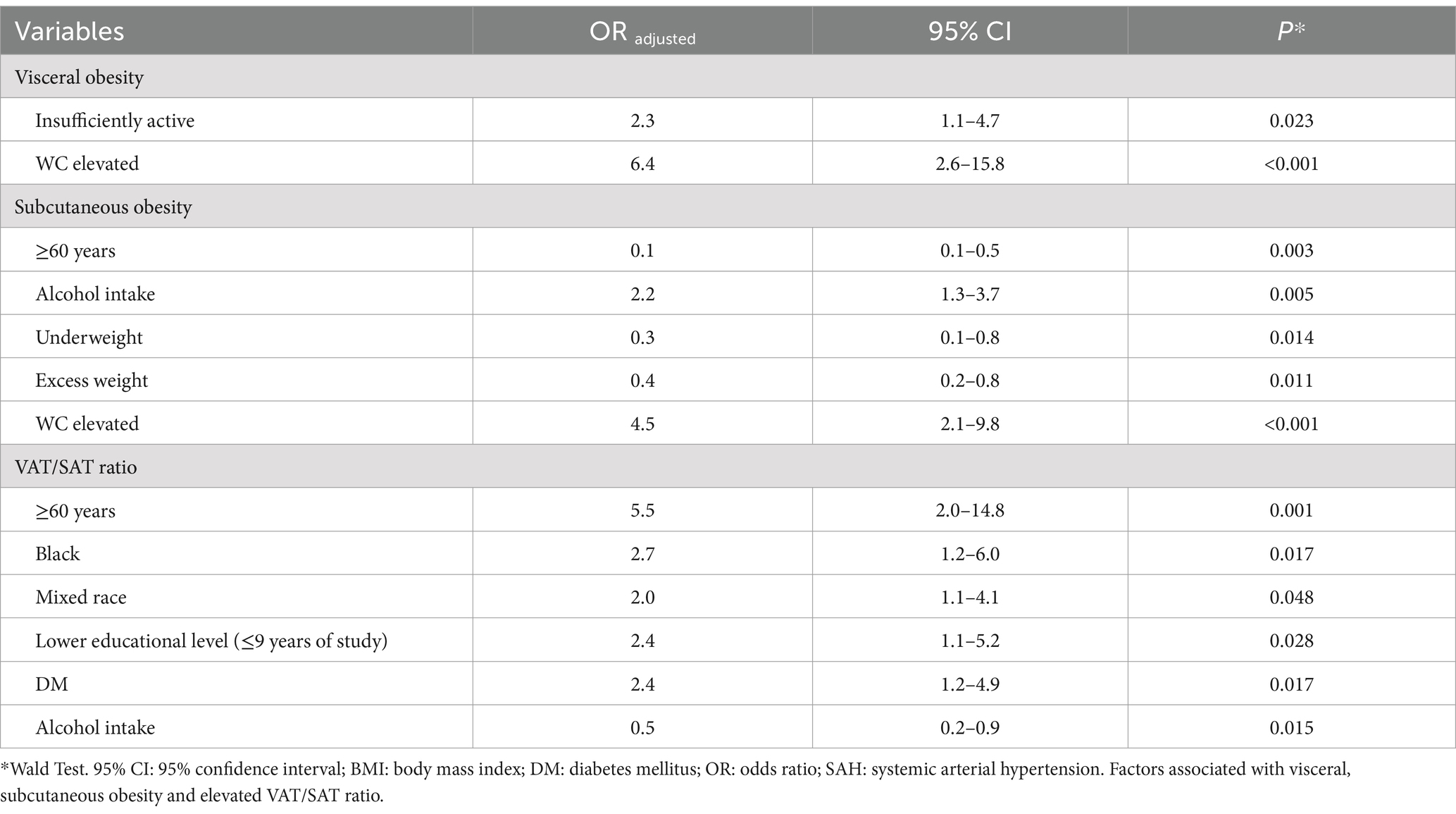
Table 5. Logistic binary regression.
4 Discussion
This study aimed to identify predictive factors for visceral and subcutaneous obesity phenotypes and characteristics associated with an elevated VAT/SAT ratio, demonstrating that distinct factors may influence the accumulation of each abdominal adipose tissue (AAT) component. Our main results demonstrate that physical inactivity was predictor of higher VAT, while older age and alcohol consumption were independently associated with greater SAT accumulation. The predisposition to accumulate VAT, represented by the VAT/SAT ratio, was influenced by sociodemographic factors (older age, non-White race, and lower education) and diabetes. WC was an independent predictor of both VAT and SAT, though not of the ratio between these components.
Studies investigating modulating factors of the abdominal fat distribution across visceral and subcutaneous depots remain underexplored. However, it is known that abdominal fat distribution is influenced by complex interactions among multiple factors, including genetics, sex, race, age, dietary habits, physical activity level, comorbidities, and hormonal factors (23, 26–29). Given the distinct metabolic and functional behaviors of different abdominal fat compartments (30, 31), there is growing global interest in quantifying abdominal adiposity and identifying factors influencing its accumulation (26, 32).
4.1 Behavioral factors
In our study, physical inactivity was a predictor of higher VAT accumulation. This result was also found in previous studies (33, 34). Better physical activity status and reduced sedentary behavior favor a negative energy balance by increasing resting energy expenditure. Although the direct causal relationship between physical activity status and preferential VAT reduction remains unclear, evidence suggests that visceral adipocytes are more sensitive to catecholamine stimulation released during exercise than abdominal subcutaneous adipocytes, resulting in greater lipolytic capacity and attenuation of VAT accumulation (27, 33).
The level of physical activity in our study was assessed using the IPAQ; however, only the total time spent on weekly activities was considered in the analysis, without evaluating exercise intensity or sedentary behavior duration. Future research should delve deeper into the role of physical activity in abdominal adipose composition, incorporating data on the frequency and intensity of physical activity. Understanding how different types of daily activities are linked to different adiposity phenotypes could shed light on the mechanisms by which sedentary time and physical inactivity contribute to multiple adverse health outcomes, including changes in body composition. This knowledge could ultimately inform more targeted guidelines on sedentary behavior and physical activity (34).
Lifestyle factors (i.e., behavioral) evaluated in this study differentially influenced AAT components. While physical inactivity influenced VAT accumulation, alcohol consumption modulated SAT accumulation. The role of alcohol consumption in determining AAT components has not been thoroughly explored, and differing results have been reported (35). Some studies identified alcohol as an independent predictor of VAT accumulation (36, 37). These discrepancies may be related to methodological variations in defining “alcohol consumption” or to synergistic characteristics that could amplify or reduce this association’s effect. It’s relevant noting that we did not assess the frequency and intensity of alcohol consumption, which may limit more definitive interpretations and conclusions.
4.2 VAT/SAT ratio
Elevated WC was predictive of higher VAT and SAT concentrations but not of an elevated VAT/SAT ratio. This finding underscores WC as a useful screening tool to estimate excessive intra-abdominal fat but highlights its limited ability to discriminate a greater predisposition for VAT over SAT accumulation. Evidence suggests that the VAT/SAT ratio may offer a better metric for assessing cardiometabolic risk than absolute quantification of each depot (12, 38). This is because the ratio provides an estimate of the relative contribution of visceral adipose tissue to total abdominal fat (38).
The ectopic fat model, represented by the VAT/SAT ratio, suggests that excess energy resulting from an imbalance between dietary intake and caloric expenditure is initially stored in subcutaneous compartments. When these subcutaneous stores reach their maximum capacity, the excess energy may be redirected to visceral compartments. This overload of fat in adipocytes can lead to reduced subcutaneous fat storage capacity, resulting in visceral fat accumulation (12). Given the variability in body shape and size across populations, the absolute values of VAT may not adequately reflect the risk differences associated with visceral obesity. In this context, assessing the VAT-related risk becomes challenging in individuals with diverse body types. Taken together, the VAT/SAT ratio theoretically provides a more accurate indicator for evaluating an individual’s body composition and associated health risks.
The VAT/SAT ratio, as measured by US scans, is associated with abnormal glucose metabolism and an increased risk of developing type 2 diabetes mellitus (39, 40). In a cohort of 473 female patients, the VAT/SAT ratio was independently linked to clusters of cardiometabolic risk factors (41). Furthermore, it holds prognostic significance as a unique predictor of cardiometabolic risk, independent of age and BMI (42). However, an elevated SAT may lower the absolute value of the VAT/SAT ratio without mitigating the associated risk. In this context, it is evident that abdominal fat accumulation, irrespective of its specific compartment, poses a health risk and should be addressed as a significant cardiometabolic risk factor.
4.3 Biological factors
Notably, aging is associated with changes in body fat distribution, including increases in intra-abdominal fat. Our findings indicated a higher predisposition for VAT accumulation (elevated VAT/SAT ratio) in older individuals (≥60 years). This trend may be explained by age-related body fat redistribution and decreased basal energy expenditure, leading to a greater concentration of visceral abdominal fat, while subcutaneous fat tends to decline (2, 43).
The observation that an elevated VAT/SAT ratio was more common among non-White individuals (Mixed race and Black) may reflect the influence of socioeconomic, biological, environmental, and cultural factors (44), as well as genetic and epigenetic factors (8, 45). However, contrasting with our study, it is generally recognized that African-American men tend to have lower VAT concentrations than White men, whereas VAT levels are more comparable between White and African-American women (46, 47).
The observed differences can be partially attributed to the unique characteristics of our population, including the mixed genetic background of Brazilian individuals, which stems from the integration of Indigenous, European, and African ancestry (48, 49). This high degree of miscegenation presents a challenge when comparing Brazilian individuals with other racial and ethnic groups. Further studies are necessary to investigate the predictive factors of abdominal adipose composition in such a diverse population.
4.4 Clinical factors
Demerath et al. (46) showed that SAT concentration may be higher in Black women compared to White women, a difference not observed among men. The independent association of a higher VAT/SAT ratio with lower educational attainment may reflect risk behaviors associated with limited social conditions. Education is a recognized proxy for socioeconomic status, which is a strong determinant of health behaviors across both sexes and all age groups (28). Furthermore, dietary behaviors are influenced by social and educational status, with low socioeconomic and educational levels being associated with obesity and higher consumption of ultra-processed foods and refined carbohydrates (50, 51). Another study highlighted that higher socioeconomic status was linked to healthier dietary choices, particularly more frequent fruit and vegetable consumption (52), a habit that may support a healthier pattern of intra-abdominal fat distribution (2).
4.5 Sociodemographic factors
Moreover, the quality of self-care and the ability to interpret information related to preventive health behaviors, including abdominal fat accumulation, can also be influenced by educational attainment and socioeconomic factors (44). However, the relationship between the predisposition for VAT accumulation and socioeconomic status requires further investigation due to the complexity of understanding how social factors may impact biological processes. The association between the VAT/SAT ratio and DM may be bidirectional (53). Excess visceral adiposity can precede the development of DM due to the direct supply of free fatty acids and inflammatory adipokines to the liver, which are secreted by visceral adipocytes. Free fatty acids inhibit insulin secretion from pancreatic cells and limit insulin-induced glucose uptake, likely by impairing signaling and transduction mechanisms (6, 8). Conversely, individuals with DM are at increased risk of developing obesity due to insulin resistance, which raises hepatic glucose production and, consequently, insulin levels, further contributing to fat accumulation (53).
4.6 Future perspectives
This study is not without limitations. The sampling method did not allow for a randomized sample, and recruiting individuals from a healthcare setting may limit the generalizability of the findings. The observational design and cross-sectional sample restrict the ability to infer causality from the observed associations. Furthermore, some important variables that influence abdominal adipose tissue composition, such as dietary intake, genetic, and hormonal factors, were not analyzed.
We also acknowledge that the use of more precise instruments could provide more relevant insights into the sociodemographic and behavioral profile of the studied sample; however, this was not feasible in our study. Nonetheless, we emphasize that this limitation reflects the real-world challenges faced in clinical routines within public healthcare settings, where time for detailed investigations is often constrained. Additionally, the absence of analyses using raw/continuous data may limit the modeling effects and the detection of small statistical differences, which we propose as a focus for future investigations.
On a positive note, this study included the use of an imaging technique (i.e., US) for the non-invasive assessment and separate quantification of abdominal fat depots. US has been reported as a useful alternative to reference methods for evaluating different body compartments. Furthermore, we incorporated a wide range of explanatory variables in the conceptual model and assessed the predisposition to accumulate VAT relative to SAT (VAT/SAT ratio). In addition, the intra- and inter-observer calibration evaluation confirmed the adequate reproducibility of the imaging method used, reinforcing the methodological standardization of the study.
It is noteworthy that adipose distribution patterns vary across ethnic groups, highlighting the need for future multicenter, multiethnic studies with large sample sizes. Longitudinal studies are also required to explore the effects of social, biological, and behavioral aspects on adipose characteristics over time. Furthermore, in-depth investigations into the VAT/SAT ratio metric and its metabolic implications should be conducted across different ethnic and social populations.
5 Conclusion
Patterns of adipose tissue distribution across different abdominal fat compartments is influenced by complex interactions among multiple factors. Physical inactivity emerged as an independent predictor of the visceral obesity phenotype, while alcohol consumption was associated with a subcutaneous abdominal obesity pattern. DM and sociodemographic factors, such as older age, non-White race, and lower education, were predictive factors for an elevated VAT/SAT ratio. Our study adds to the growing body of evidence, aiding in identifying characteristics that determine different obesity phenotypes, provide relevant data that can guide strategies aimed at groups at potential risk for complications related to the accumulation of TAV, in addition to signaling indicators that can serve as tools for monitoring and evaluating specific provisions for this audience. However, further evidence from diverse populations is still needed to clarify how sociodemographic and behavioral factors influence the accumulation of different abdominal adipose tissue components, considering additional aspects such as dietary intake, genetic, and hormonal factors.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Comite de Ética e Pesquisa em Seres Humanos HUOC/PROCAPE. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CC: Conceptualization, Investigation, Data curation, Writing – original draft. NS: Conceptualization, Data curation, Investigation, Writing – original draft. IR: Data curation, Investigation, Methodology, Validation, Writing – review & editing. GA: Data curation, Investigation, Validation, Writing – original draft. VF: Data curation, Investigation, Writing – review & editing. DS: Investigation, Supervision, Validation, Writing – review & editing. AD: Investigation, Supervision, Validation, Writing – review & editing. CP: Investigation, Writing – review & editing, Conceptualization, Formal Analysis, Supervision. PC: Investigation, Supervision, Validation, Writing – review & editing. IA: Conceptualization, Investigation, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was partially funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Powell-Wiley, TM, Poirier, P, Burke, LE, Després, JP, Gordon-Larsen, P, Lavie, CJ, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. (2021) 143:e984–e1010. doi: 10.1161/CIR.0000000000000973
2. López-Hernández, L, Pérez-Ros, P, Fargueta, M, Elvira, L, López-Soler, J, and Pablos, A. Identifying predictors of the visceral fat index in the obese and overweight population to manage obesity: a randomized intervention study. Obes Facts. (2020) 13:403–14. doi: 10.1159/000507960
4. Silva, NF, Pinho, CPS, Diniz, AS, Leão, AD, Arruda, IKG, and Rodrigues, IG. The applicability of the visceral adiposity index (VAI) for predicting visceral fat. Rev Bras Cineantropom Desempenho Hum. (2022) 24:e83146. doi: 10.1590/1980-0037.2022v24e83146
5. Silva, NF, Pinho, CPS, and Diniz, AS. Evaluation of ultrasonographic approaches aimed at determining distinct abdominal adipose tissue depots. Arch Endocrinol Metab. (2023) 67:162–71. doi: 10.20945/2359-3997000000584
6. Reyes-Farias, M, Fos-Domenech, J, Serra, D, Herrero, L, and Sánchez-Infantes, D. White adipose tissue dysfunction in obesity and aging. Biochem Pharmacol. (2021) 192:114723. doi: 10.1016/j.bcp.2021.114723
7. Cesaro, A, Michele, G, Fimiani, F, Acerbo, V, Scherillo, G, Signore, G, et al. Visceral adipose tissue and residual cardiovascular risk: a pathological link and new therapeutic options. Front Cardiovasc Med. (2023) 10:1187735. doi: 10.3389/fcvm.2023.1187735
8. Pinho, CPS, Diniz, AS, Arruda, IK, Leite, APDL, and Rodrigues, IG. Effects of weight loss on adipose visceral and subcutaneous tissue in overweight adults. Clin Nutr. (2017) 37:1252–8. doi: 10.1016/j.clnu.2017.05.011
9. Mittal, B. Subcutaneous adipose tissue & visceral adipose tissue. Indian J Med Res. (2019) 149:571–3. doi: 10.4103/ijmr.IJMR_1910_18
10. Kolb, H. Obese visceral fat tissue inflammation: from protective to detrimental? BMC Med. (2022) 20:494. doi: 10.1186/s12916-022-02672-y
11. Lee, YH, Park, J, Min, S, Kang, O, Kwon, H, and Oh, SW. Impact of visceral obesity on the risk of incident metabolic syndrome in metabolically healthy normal weight and overweight groups: a longitudinal cohort study in Korea. Korean J Fam Med. (2020) 41:229–36. doi: 10.4082/kjfm.18.0122
12. Almeida, EP, Pinho, CP, Leão, APD, Rodrigues, IG, Diniz, AS, and Arruda, LKG. Ratio of visceral to subcutaneous fat as a predictor of cardiometabolic risk. Rev Chil Nutr. (2018) 45:28–36. doi: 10.4067/s0717-75182018000100028
13. Storz, C, Heber, SD, Rospleszcz, S, Machann, J, Sellner, S, Nikolaou, K, et al. The role of visceral and subcutaneous adipose tissue measurements and their ratio by magnetic resonance imaging in subjects with prediabetes, diabetes and healthy controls from a general population without cardiovascular disease. Br J Radiol. (2018) 91:20170808. doi: 10.1259/bjr.20170808
14. Tchernof, A, and Després, JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. (2013) 93:359–404. doi: 10.1152/physrev.00033.2011
15. Oh, J, Kim, SK, Shin, DK, Park, KS, Park, SW, and Cho, YW. A simple ultrasound correlate of visceral fat. Ultrasound Med Biol. (2011) 37:1444–51. doi: 10.1016/j.ultrasmedbio.2011.05.844
16. Mauad, FM, Chagas-Neto, FA, Benedeti, ACGS, Nogueira-Barbosa, MH, Muglia, VF, Carneiro, AAO, et al. Reproducibility of abdominal fat assessment by ultrasound and computed tomography. Radiol Bras. (2017) 50:141–7. doi: 10.1590/0100-3984.2016.0023
17. Pimanov, S, Bondarenko, V, and Makarenko, E. Visceral fat in different locations assessed by ultrasound: correlation with computed tomography and cut-off values in patients with metabolic syndrome. Clin Obes. (2020) 10:e12404–9. doi: 10.1111/cob.12404
18. Uchida, K, Sugimoto, T, Tange, C, Nishita, Y, Shimokata, H, Saji, N, et al. Association between abdominal adiposity and cognitive decline in older adults: a 10-year community-based study. J Nutr Health Aging. (2024) 28:100175. doi: 10.1016/j.jnha.2024.100175
19. World Health Organization. Obesity: Preventing and managing the global epidemic. Geneva: WHO (1998).
20. Lohman, TG, Roche, AF, and Martorell, R. Anthropometric standardization reference manual. Champaign: Human Kinetics Pub (1988).
21. Brazilian Association of Research Companies (BARC). Economic classification criteria Brazil-2021. Available at: https://www.abep.org/criterio-brasil/ (Accessed on August 30, 2022).
22. Arcoverde, GF, Prado, L, Burgos, MG, Silva, RL, Andrade, MI, and Cabral, P. Early menarche and its association with anthropometric and body composition variables in young university students. Rev Chil Nutr. (2020) 47:247–54. doi: 10.4067/S0717-75182020000200247
23. Pinho, CPSP, Diniz, AS, Arruda, IKG, Filho, MBF, Coelho, PC, Sequeira, LASS, et al. Prevalence of abdominal obesity andassociated factors among individuals 25 to 59 years of age in Pernambuco state. Brazil Cad Saúde Pública. (2013) 29:313–24. doi: 10.1590/S0102-311X2013000200018
24. International Physical Activity Questionnaire (IPAQ). Disponível em. (2001) Available at: http://www.ipaq.ki.se/ipaq.htm (Accessed on September 20, 2020).
25. Alves, VV, Ribeiro, LFP, Barros, R, Gadelha, SR, and Santos, SC. Circumference measured at different sites of the trunk and cardiometabolic risk factors. Rev Bras Cineantropom Desempenho Hum. (2011) 13:250–6. doi: 10.5007/1980-0037.2011v13n4p250
26. Lumish, HS, O’Reilly, M, and Reilly, MP. Sex differences in genomic drivers of adipose distribution and related cardiometabolic disorders. Arterioscler Thromb Vasc Biol. (2020) 40:45–60. doi: 10.1161/ATVBAHA.119.313154
27. Abe, T, Song, JS, Bell, ZW, Wong, V, Spitz, RW, Yamada, Y, et al. Comparisons of calorie restriction and structured exercise on reductions in visceral and abdominal subcutaneous adipose tissue: a systematic review. Eur J Clin Nutr. (2022) 76:184–95. doi: 10.1038/s41430-021-00942-1
28. Torres-Peña, JD, Arenas-de Larriva, AP, Alcala-Diaz, JF, Lopez-Miranda, J, and Delgado-Lista, J. Different dietary approaches, non-alcoholic fatty liver disease and cardiovascular disease: a literature review. Nutrients. (2023) 15:1483. doi: 10.3390/nu15061483
29. Alsayed, EAA, Fisher, S, Nasser, J, and Sukumar, D. Ethnic differences in the relationship between visceral adiposity and waist circumference in healthy adults. Curr Dev Nutr. (2024) 8:103526. doi: 10.1016/j.cdnut.2024.103526
30. Kahn, D, Macias, E, Zarini, S, Garfield, A, Zemski, BK, MacLean, P, et al. Exploring visceral and subcutaneous adipose tissue secretomes in human obesity: implications for metabolic disease. Endocrinology. (2022) 163:140. doi: 10.1210/endocr/bqac140
31. Kang, PS, and Neeland, IJ. Body fat distribution, diabetes mellitus, and cardiovascular disease: an update. Curr Cardiol Rep. (2023) 25:1555–64. doi: 10.1007/s11886-023-01969-5
32. Zhang, Y, Yang, J, Hou, W, and Arcan, C. Obesity trends and associations with types of physical activity and sedentary behavior in US adults: national health and nutrition examination survey, 2007–2016. Obesity. (2020) 29:240–50. doi: 10.1002/oby.23043
33. Ando, S, Koyama, T, Kuriyama, N, Ozaki, E, and Uehara, R. The association of daily physical activity behaviors with visceral fat. Obes Res Clin Pract. (2020) 14:531–5. doi: 10.1016/j.orcp.2020.10.004
34. Winters-Van Eekelen, E, Van Der Velde, JHPM, Boone, SC, Westgate, K, Brage, S, Lamb, H, et al. Objectively measured physical activity and body fatness: associations with Total body fat, visceral fat, and liver fat. Med Sci Sports Exerc. (2021) 53:2309–17. doi: 10.1249/MSS.0000000000002712
35. Kazibwe, R, Chevli, PA, Evans, JK, Allison, M, Michos, ED, Wood, AC, et al. Association between alcohol consumption and ectopic fat in the multi-ethnic study of atherosclerosis. J Am Heart Assoc. (2023) 12:e030470. doi: 10.1161/JAHA.123.030470
36. Mathur, M, Yeh, YT, Arya, RK, Jiang, L, Pornour, M, Chen, W, et al. Adipose lipolysis is important for ethanol to induce fatty liver in the National Institute on Alcohol Abuse and Alcoholism murine model of chronic and binge ethanol feeding. Hepatology. (2022) 77:1688–701. doi: 10.1002/hep.32675
37. Li, Q, Wang, O, Ji, B, Zhao, L, and Zhao, L. Alcohol, white adipose tissue, and brown adipose tissue: mechanistic links to lipogenesis and lipolysis. Nutrients. (2023) 15:2953. doi: 10.3390/nu15132953
38. Ladeiras-Lopes, R, Sampaio, F, Bettencourt, N, Fontes-Carvalho, R, Ferreira, N, Leite-Moreira, A, et al. The ratio between visceral and subcutaneous abdominal fat assessed by computed tomography is an independent predictor of mortality and cardiac events. Rev Esp Cardiol. (2017) 70:331–7. doi: 10.1016/j.recesp.2016.09.006
39. Philipsen, A, Jørgensen, ME, Vistisen, D, Sandbaek, A, Almdal, TP, Christiansen, JS, et al. Associations between ultrasound measures of abdominal fat distribution and indices of glucose metabolism in a population at high risk of type 2 diabetes: the ADDITION-PRO study. PLoS One. (2015) 10:e0123062. doi: 10.1371/journal.pone.0123062
40. Koda, M, Senda, M, Kamba, M, Kimura, K, and Murawaki, Y. Sonographic subcutaneous and visceral fat indices represent the distribution of body fat volume. Abdom Imaging. (2007) 32:387–92. doi: 10.1007/s00261-006-9082-3
41. He, H, Ni, Y, Chen, J, Zhigang, Z, Jian, Z, Daoyan, L, et al. Sex difference in cardiometabolic risk profile and adiponectin expression in subjects with visceral fat obesity. Transl Res. (2011) 2:24–9. doi: 10.1016/j.trsl.2009.08.003
42. Oh, YH, Moon, JH, and JuKH, KMH. Visceral-to-subcutaneous fat ratio as a predictor of the multiple metabolic risk factors for subjects with normal waist circumference in Korea. Diabetes Metab Syndr Obesity. (2017) 10:505–11. doi: 10.2147/DMSO.S150914
43. Kuk, JL, Saunders, TJ, Davidson, LE, and Ross, R. Age-related changes in total and regional fat distribution. Ageing Res Rev. (2009) 8:339–48. doi: 10.1016/j.arr.2009.06.001
44. Eickemberg, M, Amorim, LDVF, Almeida, MCC, Pitanga, FJG, Aquino, EML, Fonseca, MJM, et al. Obesidade abdominal no ELSA-Brasil: construção de padrão-ouro latente e avaliação da acurácia de indicadores diagnósticos. Ciênc Saúde Coletiva. (2020) 25:2985–98. doi: 10.1590/1413-81232020258.20992018
45. Merritt, MA, Lim, U, Lampe, JW, Kaenkumchorn, T, Boushey, CJ, Wilkens, LR, et al. Dietary intake and visceral adiposity in older adults: the multiethnic cohort adiposity phenotype study. Obesity Sci Pract. (2024) 10:e734. doi: 10.1002/osp4.734
46. Demerath, EW, Sun, SS, Rogers, N, Lee, M, Reed, D, Choh, AC, et al. Anatomical patterning of visceral adipose tissue: race, sex, and age variation. Obesity. (2007) 15:2984–93. doi: 10.1038/oby.2007.356
47. Leone, A, Battezzati, A, Bedogni, G, Vignati, L, Vanzulli, A, De Amicis, R, et al. Sex- and age-related differences in the contribution of ultrasound-measured visceral and subcutaneous abdominal fat to fatty liver index in overweight and obese Caucasian adults. Nutrients. (2019) 11:3008. doi: 10.3390/nu11123008
48. Parra, FC, Amado, RC, Lambertucci, JR, Rocha, J, Antunes, CM, and Pena, SD. Color and genomic ancestry in Brazilians. Proc Natl Acad Sci USA. (2003) 100:177–82. doi: 10.1073/pnas.0126614100
49. Pizarro, MH, Santos, DC, Melo, LGN, Barros, BSV, Muniz, LH, Porto, LC, et al. Influence of genomic ancestry and self-reported color-race in CKD in a nationwide admixed sample of Brazilian patients with type 1 diabetes. Diabetes Metab Syndr Obes. (2019) 12:1831–40. doi: 10.2147/DMSO.S210585
50. Villarreal, VI, Cabral, PC, Batista Filho, M, Sequeira-de-Andrade, LAS, Arruda, IKG, Silva, CS, et al. Obesidad abdominal en adultos del estado de Pernambuco, Brasil: un estudio epidemiológico de tipo transversal. Rev Esp Nutr Hum Diet. (2020) 24:190–202. doi: 10.14306/renhyd.24.3.849
51. Isanejad, M, Steffen, LM, Terry, JG, Shikany, JM, Zhou, X, So-Yun, Y, et al. Diet quality is associated with adipose tissue and muscle mass: the coronary artery risk development in young adults (CARDIA) study. J Cachexia Sarcopenia Muscle. (2023) 15:425–33. doi: 10.1002/jcsm.13399
52. Czarnocinska, J, Wadolowska, L, Lonnie, M, Kowalkowska, J, Jezewska-Zychowicz, M, and Babicz-Zielinska, E. Regional and socioeconomic variations in dietary patterns in a representative sample of young polish females: a cross-sectional study (GEBaHealth project). Nutr J. (2020) 19:26. doi: 10.1186/s12937-020-00546-8
Keywords: abdominal fat, subcutaneous fat, body fat distribution, obesity, body composition
Citation: Chagas CL, da Silva NF, Rodrigues IG, Arcoverde GMPF, Ferraz VD, Sobral Filho DC, Diniz AdS, Pinho CPS, Cabral PC and de Arruda IKG (2025) Different factors modulate visceral and subcutaneous fat accumulation in adults: a single-center study in Brazil. Front. Nutr. 12:1524389. doi: 10.3389/fnut.2025.1524389
Edited by:
Mor Diaw, Cheikh Anta Diop University, SenegalReviewed by:
Yang Liu, Hebei Normal University, ChinaRhonda BeLue, University of Texas at San Antonio, United States
Abdou Khadir Sow, Cheikh Anta Diop University, Senegal
Copyright © 2025 Chagas, da Silva, Rodrigues, Arcoverde, Ferraz, Sobral Filho, Diniz, Pinho, Cabral and de Arruda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ilma Kruze Grande de Arruda, aWxtYS5hcnJ1ZGFAdWZwZS5icg==