 Sara Shojaei-Zarghani
Sara Shojaei-Zarghani Mohammad Reza Fattahi2†
Mohammad Reza Fattahi2† Asma Kazemi
Asma Kazemi Ali Reza Safarpour
Ali Reza Safarpour
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 25 March 2025
Sec. Nutritional Epidemiology
Volume 12 - 2025 | https://doi.org/10.3389/fnut.2025.1521571
Background: Impaired fasting glucose (IFG) is a precursor to type 2 diabetes and is influenced by dietary factors. This cross-sectional study assessed the association between major dietary patterns and IFG in the baseline phase of PERSIAN Kavar cohort study (PKCS).
Methods: The study included 3,144 participants aged 35–70 years. After assessing dietary intakes by a food frequency questionnaire, principal component analysis was used to identify dietary patterns. Logistic regression model was applied to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for the association between dietary patterns and IFG.
Results: Three major dietary patterns were identified: healthy, Western-like, and CarnFat (Carnivorous-fat). In the fully adjusted model, individuals in the highest tertile of the healthy dietary pattern had a lower likelihood of IFG compared to those in the lowest tertile (OR = 0.68, 95% CI: 0.53–0.88). The second tertile of the healthy pattern was also associated with lower odds of IFG (OR = 0.77, 95% CI: 0.62–0.96). No significant associations were found for the Western-like and CarnFat dietary patterns.
Conclusion: A healthy dietary pattern characterized by high intakes of fruits, vegetables, low-fat dairy, nuts, seeds, olive oil, legumes, fish, and whole grains was associated with a lower risk of IFG. These findings highlight the importance of promoting healthy dietary patterns for the prevention of prediabetes and type 2 diabetes.
Impaired fasting glucose (IFG) refers to a fasting plasma glucose (FPG) level that falls between normal and diabetes cutoff values (1). The expert committee of the American Diabetes Association (ADA) introduced the concept of IFG in 1997, defining it as FPG levels between 110 and 125 mg/dL (2). According to this criterion, the global prevalence of IFG was 5.8% (~298 million individuals) in 2021, and is expected to increase to 6.5% (~414 million individuals) by 2045 (3). However, in 2003, the ADA revised the definition of IFG to encompass FPG levels ranging from 100 to 125 mg/dL (4). Studies utilizing this updated cutoff have reported a higher prevalence of IFG; for instance, nearly one-fourth of adults surveyed in the New York City Health and Nutrition Examination Survey (NYC HANES) were found to have IFG, with the highest prevalence observed among Asians [32.4%; (5)]. Similarly, a population-based study conducted among adults aged 35 to 70 years in Iran reported a prevalence of IFG of 20.61% (6). IFG has been linked with an elevated risk of developing diabetes and experiencing vascular complications (7). Understanding the risk factors associated with IFG and developing individualized management strategies are essential for delaying or preventing its progression and the associated consequences.
Literature suggests the impact of certain dietary patterns on metabolic health, including IFG. A recent cross-sectional study conducted among Chinese men revealed an increased odds of IFG associated with an animal offal-dessert dietary pattern, a decreased likelihood associated with a vegetables-fruits dietary pattern, and no significant association with a white rice-red meat dietary pattern (8). Conversely, another prospective study from the Tehran Lipid and Glucose Study in Iran found no significant association between tertiles of Western, traditional, and healthy dietary patterns and the risk of IFG or prediabetes (9). Given the variations in predominant dietary patterns across different geographical regions and timeframes of investigation, as well as the limited evidence and conflicting findings in the literature, we utilized data of the PERSIAN Kavar cohort study (PKCS) to recognize the major dietary patterns among the included population and to elucidate how these different dietary patterns may influence the odds of IFG.
In this cross-sectional study, we used the baseline data from PKCS, a branch of PERSIAN (Prospective Epidemiological Research Studies in IrAN) cohort study conducted in Kavar city, located in the central region of the Fars province in Iran. The PKCS is conducted on 4,997 participants aged 35–70 years. The detailed protocol has been previously published (10). Written informed consent was signed by all participants. Individuals with pre-existing chronic conditions such as malignancies, hepatitis, renal failure, diabetes, hypertension, cardiac diseases, and hyperlipidemia as well as those with FPG levels higher than 125 mg/dL and pregnant women were excluded from the current analysis. The protocol of this study adhered to the Declaration of Helsinki and was approved by the Ethics Committee of Shiraz University of medical sciences, Shiraz, Iran (Code: IR.SUMS.REC.1399.1092).
The data collection involved the use of validated questionnaires, blood sampling, and physical examinations (10, 11). The socio-economic status of the participants was evaluated by the wealth score index (WSI), which considered the assets of their households (10). The FPG levels were measured using Iranian commercial kits (Pars Azmoon) and an auto-analyzer (model BT3000 Plus, Biotecnica®, Italy). The IFG was defined as FPG value of 100 to 125 mg/dL (1). Dietary intake over the previous year was assessed using a validated food frequency questionnaire (12). Trained nutritionists queried each participant about the frequency of consuming individual food items on a daily, weekly, monthly, or yearly basis, as well as the quantity consumed based on predetermined portion sizes. Then, these values were converted to grams of food intake per day. Out of 118 food items, 29 food groups were derived with similar nutrient profile to identify major dietary patterns.
Statistical analyses were conducted using SPSS 26 software. The normality of data was tested using skewness, kurtosis, and standard deviation (SD). Then, normal data was reported as mean ± SD and qualitative data as frequency (percentage). Between-group differences were conducted using ANOVA for quantitative data and chi-square test for qualitatives. For extracting dietary patterns, principal component analysis with varimax rotation was used. Kaiser-Meyer-Olkin (KMO) test and Bartlett's test of sphericity were done for assessing the suitability of the sample size for conducting factor analysis and correlations across food groups, respectively. Major dietary patterns were identified using eigenvalues of > 1.5 (13, 14) and scree plot. For assessing the association between dietary patterns and hyperglycemia, we used multivariable logistic regression, and results are reported as odds ratio (OR) and 95% confidence intervals (CI). Age, sex, ethnicity, marital status, education, socioeconomic status, smoking status, alcohol intake, physical activity, body mass index (BMI), and energy were included in the regression model. A two-sided P < 0.05 was considered significant.
The 29 food groups and their corresponding food items are detailed in Table 1. The suitability of the sample size for conducting factor analysis and inter-item correlations was confirmed by a KMO value of 0.773 and a significant Bartlett's test of sphericity (P < 0.001). Subsequently, three major dietary patterns were identified using eigenvalues of > 1.5 and a scree plot (Figure 1). These three dietary patterns include a healthy pattern with high intakes of fruits, vegetables, low-fat dairy, nuts-seeds, dried fruits, olive, legume, pickle, fish, onion-garlic, fresh juice, potato, and whole grain; a Western-like pattern associated with a higher intake of sweetened beverages, proceed meats, refined grains, mayonnaise, pizza, snacks, confectionary-sugar, eggs, high-fat dairy, poultry, salt, and oil, and a lower intake of whole grain; and a CarnFat (Carnivorous-fat) pattern with high factor loading on animal-hydrogenated fat, organ meat, and red meat, and lower levels of soy and oil (Table 2). These dietary patterns explained 24.85% of total variance.
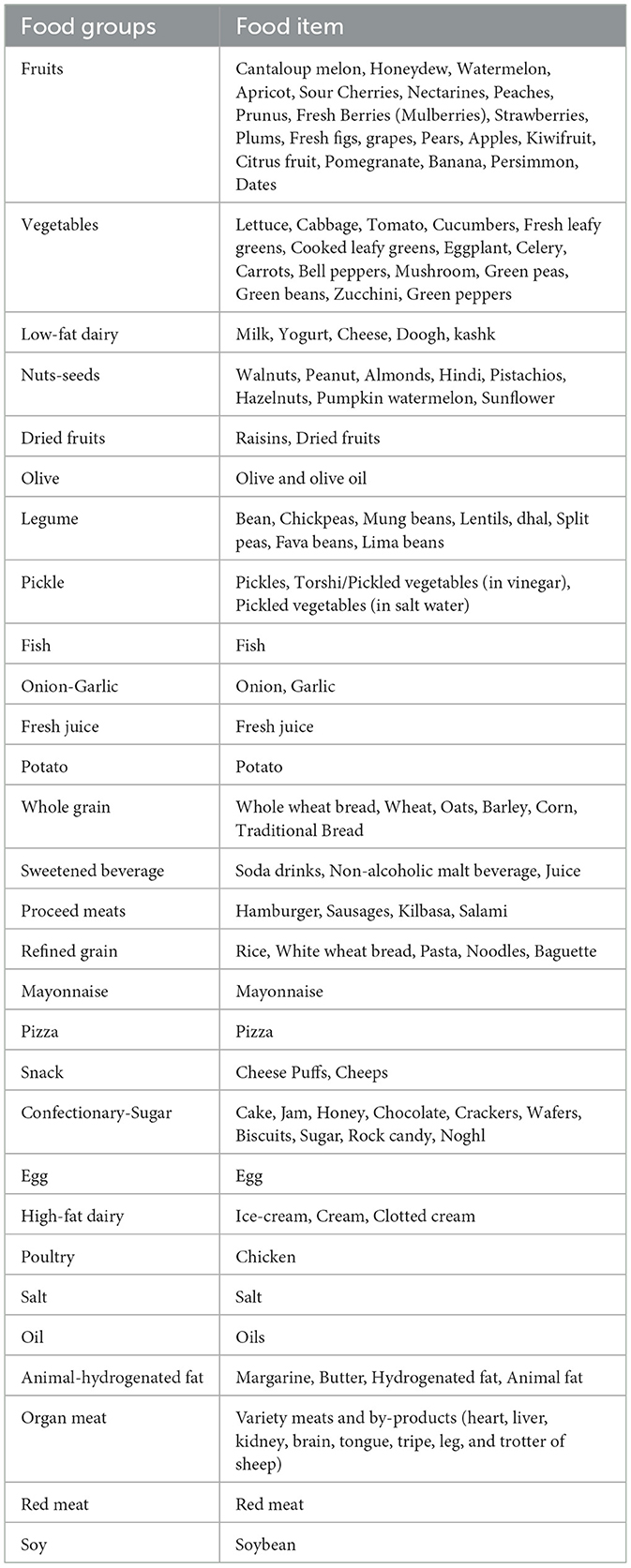
Table 1. Food groups and their related food items for deriving dietary patterns.
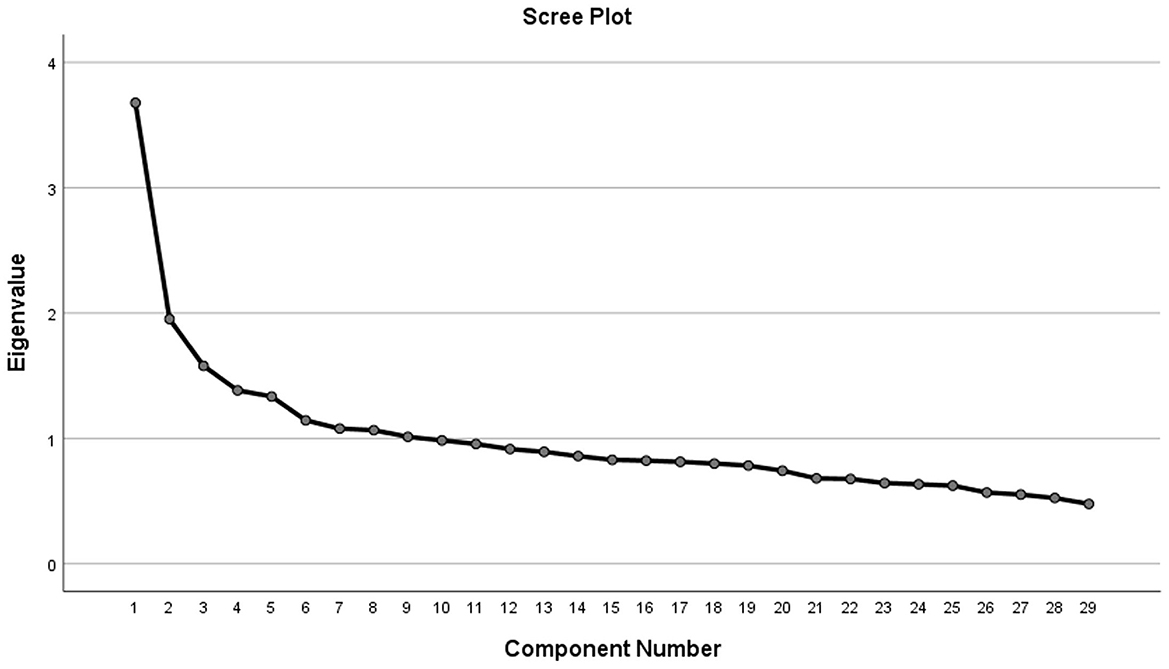
Figure 1. Scree plot from the principal component analysis.
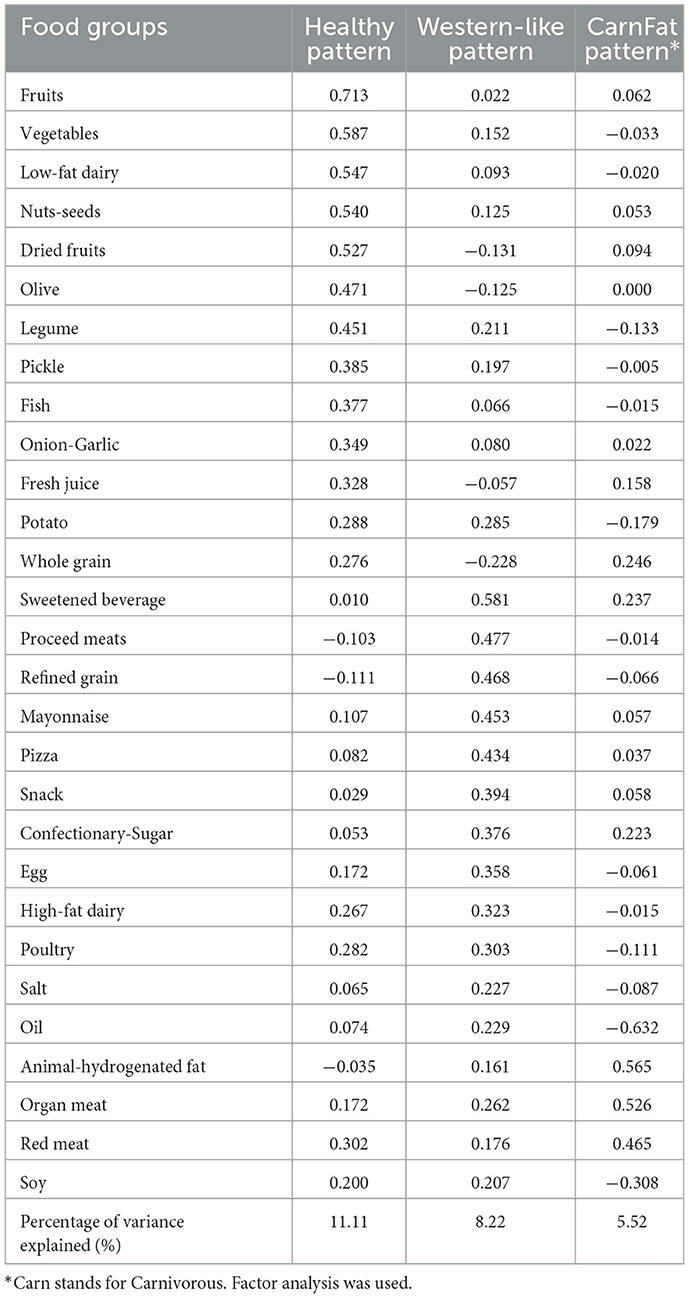
Table 2. Factor loading matrix for dietary patterns.
Among the 4,997 participants in the baseline phase of the PKCS, 3,144 subjects (54% men and 46% women with a mean age of 45.75 years) were included in the final analysis (Figure 2), and their characteristics are reported in Table 3. Upon assessing the subjects' features across tertiles of adherence to dietary patterns, it was observed that individuals with greater adherence to the healthy dietary pattern were more likely to be male (P < 0.001), of Persian ethnicity (P < 0.001), have a higher level of education (P < 0.001), exhibit a higher socio-economic status (P < 0.001), have a higher BMI (P < 0.001), and consume more energy (P < 0.001). Additionally, there were significant differences in sex, education, smoking, alcohol intake, age, BMI, and energy among the tertiles of Western-like and CarnFat dietary patterns (Table 3).

Figure 2. Flowchart of study.
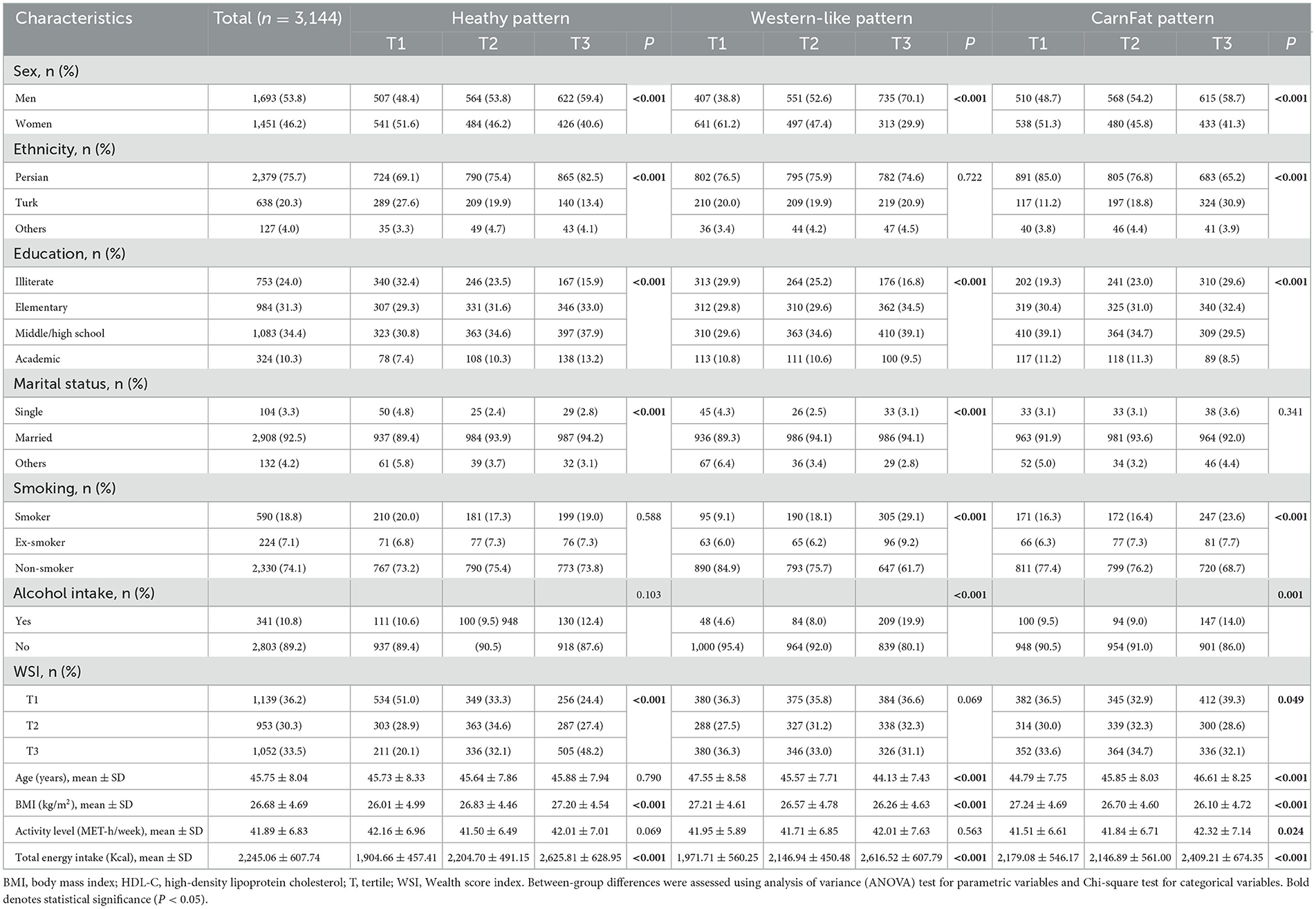
Table 3. Baseline characteristics of the major dietary patterns by factor score tertiles.
Among the included population, 689 subjects (21.9%) had IFG. Table 4 presents the odds ratios of IFG based on the tertiles of dietary pattern scores. In the fully adjusted model, a reduced likelihood of IFG was observed in individuals with the highest adherence to the healthy dietary pattern than persons with the lowest adherence (OR = 0.68, 95% CI: 0.53–0.88, P = 0.004). Subjects in the second tertile had also significantly lower odds of IFG compared to the reference (OR = 0.77, 95% CI: 0.62–0.96, P = 0.018).
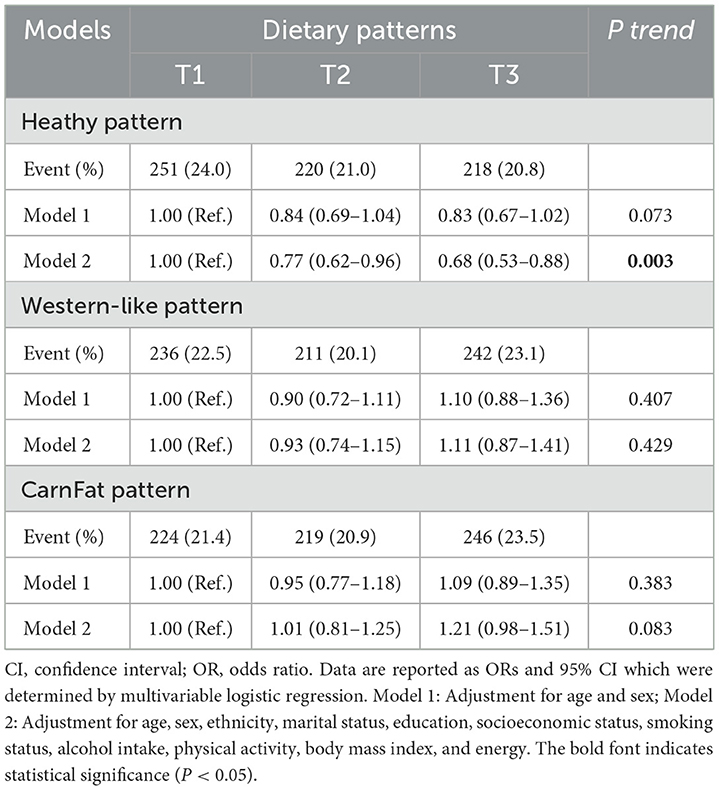
Table 4. Odds of impaired fasting glucose according to the tertiles of dietary pattern's scores.
The three major dietary patterns identified in the current study were categorized as healthy, Western-like, and CarnFat. These dietary patterns were derived from 29 food groups, which is a greater number than those identified in a previous study involving seven centers of the PERSIAN Cohort Study, which derived 23 food groups from the FFQ questionnaire. Notably, this earlier study did not categorize high-fat dairy products, pickles, onions, garlic, potatoes, mayonnaise, organ meats, pizza, and snacks as separate categories, unlike our study (12). The factor loadings for the healthy dietary pattern in this study were largely consistent with those identified in our research; however, the other patterns exhibited significant differences. In another similar study conducted by Zhang et al., three dietary patterns—vegetables-fruits, animal offal-dessert, and white rice-red meat—were extracted from 21 food groups (8). Fast foods, peanuts, alcoholic beverages, seaweeds, mushrooms, tubers, coarse cereals, and condiments were considered as separate categories in that study, whereas they were not distinctly categorized in either our study or the one by Eghtesad et al. (12). A comparison of food groups between the current analysis and these two studies is depicted in Figure 3. Furthermore, our dietary patterns showed considerable alignment with those identified in a previous study by Mirzababaei et al., which examined dietary patterns among overweight and obese Iranian women. This study identified three major patterns: a healthy dietary pattern, including, vegetables, fruits, legumes, nuts, low-fat dairy products, white meat, and olives; a Western-like dietary pattern marked by high levels of fast food, mayonnaise, snacks, high-energy beverages, sweets, cereals, and condiments; and an unhealthy dietary pattern rich in solid fats, high-fat dairy products, red meat, organ meats (such as liver, brain, and kidney), tea and coffee, along with lower consumption of liquid oils (15). The factor loadings in this study across different dietary patterns were largely similar to those observed in our research.

Figure 3. Venn diagram for the comparison of food groups between the current analysis and others.
Our findings indicate that subjects in the second and third tertiles of adherence to the healthy dietary pattern exhibited, respectively, 23 and 32% lower odds of IFG, representing a small effect. Limited studies have investigated the association between dietary patterns and IFG. Consistent with our results, Zhang et al. conducted a cross-sectional study on Chinese men, revealing that a vegetables-fruits dietary pattern, characterized by high intake of vegetables and fruits as well as cereals, refined grain, soybean, peanuts, and dairy products, was negatively associated with the odds of IFG, defined as FPG levels between 110 and 126 mg/dL (8). In another prospective study on 904 Iranian subjects, a healthy dietary pattern (high load of vegetables and their oils, fresh and dried fruits, low-fat dairy, and nuts and seeds) was inversely associated with 3-year changes in FPG, fasting insulin, 2 h-serum glucose, and homeostasis model assessment of insulin resistance in linear regression models. However, no relationship was found between tertile categories of the healthy dietary pattern and IFG (FPG levels of 100–126 mg/dL), impaired glucose tolerance (IGT, 2-h serum glucose levels of 140–199 mg/dL), prediabetes (defined as having either IFG or IGT, or β-cell dysfunction in multivariable logistic regression models. Indeed, while a healthy dietary pattern was associated with reduced FPG levels, it did not significantly diminish the risk of developing IFG (9). This dietary pattern is linked to adequate micronutrient intake (16). The beneficial effects of a healthy dietary pattern on IFG may be attributed to its high content of vitamins, minerals, antioxidants, anti-inflammatory compounds, phytochemicals, fiber, monounsaturated fats, and ω-3 fatty acids, all of which had beneficial effects on IFG (17–20). Discrepancies among studies regarding the effects of healthy patterns on IFG and diabetes prevention may arise from differences in study populations, the specific factors loaded in each study's dietary pattern, and variations in disease threshold definitions.
Here, we did not observe any association between Western-like and CarnFat dietary patterns and the odds of IFG. This finding is consistent with some (9, 21) previous studies but contrasts with a body of literature that establishes links between Western diets and some metabolic disorders, like IFG, insulin resistance, and diabetes (8, 22, 23). In a study by Walsh et al. involving 209 subjects aged 60–65 (28 of whom had IFG), no association was reported between the highest tertile of Western diet score and IFG (21). Similarly, Doostvandi et al. found no association between the Western dietary pattern (fast foods, salty snacks, mayonnaise, soft drinks, confectionary, and organ meats) and FPG in linear model, nor with the incidence of IFG, prediabetes, β-cell dysfunction, and hyperinsulinemia in the logistic models. However, they detected a significant relationship between the Western dietary pattern and IGT development (9). One potential explanation for this observation could be the possibility that the mechanisms underlying the effects of a Western diet on IFG may differ from those related to IGT (21). A previous meta-analysis of randomized controlled trials reported no significant effect of red meat consumption on FPG, fasting insulin, postprandial insulin, insulin sensitivity, homeostatic model assessment of insulin resistance (HOMA-IR), hemoglobin A1c, pancreatic beta-cell function, or glucagon-like peptide-1. The authors suggested that discrepancies among studies regarding the association between red meat and diabetes risk may be attributable to residual confounding factors associated with higher red meat consumption (24). Furthermore, the existing data concerning the role of saturated fatty acids in diabetes remain inconsistent (25, 26). Variations in study design and unadjusted lifestyle factors may contribute to the contradictory findings observed between Western-style and CarnFat dietary patterns in relation to diabetes. Additionally, genetic predisposition and racial ancestry have been reported to interact with the impact of the Western dietary pattern on the risk of diabetes and metabolic syndrome (27, 28). In current study, we were unable to assess the duration of dietary exposure; this limitation should be addressed in future prospective studies aimed at evaluating the effects of dietary patterns on glucose metabolism.
Our study had several limitations. We could not determine the direction of the association due to the cross-sectional design of the current study. Furthermore, data related to insulin levels, hemoglobin A1C, and IGT were not available in our database, preventing us from assessing the effects of dietary patterns on these variables. Additionally, despite adjusting for several confounding factors, some unmeasured or unknown variables may still influence the reported associations. Future prospective longitudinal studies with large sample size are needed to clarify the effects of various dietary patterns on glucose metabolism more comprehensively.
In conclusion, healthy dietary pattern, which was characterized with high intake of fruits, vegetables, low-fat dairy, nuts-seeds, dried fruits, olive, legume, pickle, fish, onion-garlic, fresh juice, potato, and whole grain, was associated with lower odds of IFG. However, no association was found for Western-like and CarnFat dietary patterns.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was approved by the Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
SS-Z: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – review & editing, Writing – original draft. MF: Methodology, Writing – review & editing, Project administration, Supervision, Validation. AK: Methodology, Writing – review & editing, Data curation, Formal analysis, Software. NN: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. AS: Data curation, Formal analysis, Methodology, Software, Writing – review & editing, Conceptualization, Funding acquisition, Project administration, Supervision, Validation.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was funded by Vice-Chancellor for Research and Technology of Shiraz University of Medical Sciences (Code: 21723).
We thank Iranian Ministry of Health and Medical Education for funding the PERSIAN cohort (no 700/534).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American Diabetes Association. Standards of medical care in diabetes–2011. Diabetes Care. (2011) 34:S11–61. doi: 10.2337/dc11-S011
2. Gavin III JR, Alberti K, Davidson MB, DeFronzo RA. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. (1997) 20:1183. doi: 10.2337/diacare.20.7.1183
3. Rooney MR, Fang M, Ogurtsova K, Ozkan B, Echouffo-Tcheugui JB, Boyko EJ, et al. Global prevalence of prediabetes. Diabetes Care. (2023) 46:1388–94. doi: 10.2337/dc22-2376
4. Genuth S, Alberti K, Bennett P, Buse J, DeFronzo R, Kahn R, et al. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care. (2003) 26:3160–8. doi: 10.2337/diacare.26.11.3160
5. Thorpe LE, Upadhyay UD, Chamany S, Garg R, Mandel-Ricci J, Kellerman S, et al. Prevalence and control of diabetes and impaired fasting glucose in New York City. Diabetes Care. (2009) 32:57–62. doi: 10.2337/dc08-0727
6. Ghaemmaghami Z, Eftekhar E, Shahbazi R, Nejatizadeh A, Shahmoradi M, Kheirandish M. Pre-diabetes, diabetes mellitus and related cardio-metabolic risk factors in the southern coastal region of Iran middle-aged and elderly population; Bandare-Kong cohort study. Arch Iran Med. (2022) 25:409–16. doi: 10.34172/aim.2022.68
7. Yu ES, Hong K, Chun BC. Incidence and risk factors of vascular complications in people with impaired fasting glucose: a national cohort study in Korea. Sci Rep. (2020) 10:19504. doi: 10.1038/s41598-020-76661-7
8. Zhang M, Zhu Y, Li P, Chang H, Wang X, Liu W, et al. Associations between dietary patterns and impaired fasting glucose in Chinese men: a cross-sectional study. Nutrients. (2015) 7:8072–89. doi: 10.3390/nu7095382
9. Doostvandi T, Bahadoran Z, Mozaffari-Khosravi H, Mirmiran P, Azizi F. Food intake patterns are associated with the risk of impaired glucose and insulin homeostasis: a prospective approach in the Tehran lipid and glucose study. Public Health Nutr. (2016) 19:2467–74. doi: 10.1017/S1368980016000616
10. Safarpour AR, Fattahi MR, Niknam R, Tarkesh F, Mohammadkarimi V, Boogar SS, et al. Alarm of non-communicable disease in Iran: kavar cohort profile, baseline and 18-month follow up results from a prospective population-based study in urban area. PLoS ONE. (2022) 17:e0260227. doi: 10.1371/journal.pone.0260227
11. Eghtesad S, Hekmatdoost A, Faramarzi E, Homayounfar R, Sharafkhah M, Hakimi H, et al. Validity and reproducibility of a food frequency questionnaire assessing food group intake in the PERSIAN cohort study. Front Nutr. (2023) 10:1059870. doi: 10.3389/fnut.2023.1059870
12. Eghtesad S, Masoudi S, Sharafkhah M, Rashidkhani B, Esmaeili-Nadimi A, Najafi F, et al. Validity and reproducibility of the PERSIAN cohort food frequency questionnaire: assessment of major dietary patterns. Nutr J. (2024) 23:35. doi: 10.1186/s12937-024-00938-0
13. Yong HY, Mohd Shariff Z, Mohd Yusof B-N, Rejali Z, Appannah G, Bindels J, et al. The association between dietary patterns before and in early pregnancy and the risk of gestational diabetes mellitus (GDM): Data from the Malaysian SECOST cohort. PLoS ONE. (2020) 15:e0227246. doi: 10.1371/journal.pone.0227246
14. Malekahmadi M, Khayyatzadeh SS, Heshmati J, Alshahrani SH, Oraee N, Ferns GA, et al. The relationship between dietary patterns and aggressive behavior in adolescent girls: a cross-sectional study. Brain Behav. (2022) 12:e2782. doi: 10.1002/brb3.2782
15. Mirzababaei A, Sajjadi SF, Ghodoosi N, Pooyan S, Arghavani H, Yekaninejad MS, et al. Relations of major dietary patterns and metabolically unhealthy overweight/obesity phenotypes among Iranian women. Diabetes Metab Syndr Clin Res Rev. (2019) 13:322–31. doi: 10.1016/j.dsx.2018.09.012
16. Ito T, Tanisawa K, Kawakami R, Usui C, Ishii K, Suzuki K, et al. Micronutrient intake adequacy in men and women with a healthy Japanese dietary pattern. Nutrients. (2019) 12:6. doi: 10.3390/nu12010006
17. Zhang S, Meng G, Zhang Q, Liu L, Yao Z, Wu H, et al. Dietary fibre intake and risk of prediabetes in China: results from the Tianjin chronic low-grade systemic inflammation and health (TCLSIH) cohort study. Br J Nutr. (2022) 128:753–61. doi: 10.1017/S0007114521003779
18. Rizzo MR, Abbatecola AM, Barbieri M, Vietri MT, Cioffi M, Grella R, et al. Evidence for anti-inflammatory effects of combined administration of vitamin E and C in older persons with impaired fasting glucose: impact on insulin action. J Am Coll Nutr. (2008) 27:505–11. doi: 10.1080/07315724.2008.10719732
19. Derosa G, Cicero AF, D'Angelo A, Borghi C, Maffioli P. Effects of n-3 pufas on fasting plasma glucose and insulin resistance in patients with impaired fasting glucose or impaired glucose tolerance. Biofactors. (2016) 42:316–22. doi: 10.1002/biof.1277
20. Abdulai T, Li Y, Zhang H, Tu R, Liu X, Zhang L, et al. Prevalence of impaired fasting glucose, type 2 diabetes and associated risk factors in undiagnosed Chinese rural population: the Henan rural cohort study. BMJ Open. (2019) 9:e029628. doi: 10.1136/bmjopen-2019-029628
21. Walsh EI, Jacka FN, Butterworth P, Anstey KJ, Cherbuin N. The association between Western and Prudent dietary patterns and fasting blood glucose levels in type 2 diabetes and normal glucose metabolism in older Australian adults. Heliyon. (2017) 3:e00315. doi: 10.1016/j.heliyon.2017.e00315
22. Hou Y-C, Feng H-C, Tzeng I-S, Kuo C-Y, Cheng C-F, Wu JH, et al. Dietary patterns and the risk of prediabetes in Taiwan: a cross-sectional study. Nutrients. (2020) 12:3322. doi: 10.3390/nu12113322
23. Ushula TW, Mamun A, Darssan D, Wang WY, Williams GM, Whiting SJ, et al. Dietary patterns and the risks of metabolic syndrome and insulin resistance among young adults: evidence from a longitudinal study. Clin Nutr. (2022) 41:1523–31. doi: 10.1016/j.clnu.2022.05.006
24. Sanders LM, Wilcox ML, Maki KC. Red meat consumption and risk factors for type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Eur J Clin Nutr. (2023) 77:156–65. doi: 10.1038/s41430-022-01150-1
25. Tajadod S, Shekari S, Mohseni GK, Abbasi K, Torki SA, Salimi Z, et al. Association between type 2 diabetes and different types of dietary fats: a case-control study. Clin Nutr ESPEN. (2023) 58:67–72. doi: 10.1016/j.clnesp.2023.08.034
26. von Frankenberg AD, Marina A, Song X, Callahan HS, Kratz M, Utzschneider KM, et al. High-fat, high-saturated fat diet decreases insulin sensitivity without changing intra-abdominal fat in weight-stable overweight and obese adults. Eur J Nutr. (2017) 56:431–43. doi: 10.1007/s00394-015-1108-6
27. Qi L, Cornelis MC, Zhang C, Van Dam RM, Hu FB. Genetic predisposition, western dietary pattern, and the risk of type 2 diabetes in men. Am J Clin Nutr. (2009) 89:1453–8. doi: 10.3945/ajcn.2008.27249
Keywords: glucose intolerance, dietary patterns, healthy diet, Western diet, carnivorous diet
Citation: Shojaei-Zarghani S, Fattahi MR, Kazemi A, Najafi N and Safarpour AR (2025) A cross-sectional study on the association between major dietary pattern and impaired fasting glucose. Front. Nutr. 12:1521571. doi: 10.3389/fnut.2025.1521571
Received: 02 November 2024; Accepted: 10 March 2025;
Published: 25 March 2025.
Edited by:
Lei Zhang, University of Waterloo, CanadaReviewed by:
Xiangtao Liu, The University of Iowa, United StatesCopyright © 2025 Shojaei-Zarghani, Fattahi, Kazemi, Najafi and Safarpour. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ali Reza Safarpour, c2FmYXJwb3VyYXJAZ21haWwuY29t
†ORCID: Sara Shojaei-Zarghani orcid.org/0000-0001-8479-065X
Mohammad Reza Fattahi orcid.org/0000-0001-6160-0403
Asma Kazemi orcid.org/0000-0001-5032-0078
Ali Reza Safarpour orcid.org/0000-0002-9880-0043
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.