
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Nutr. , 28 January 2025
Sec. Clinical Nutrition
Volume 12 - 2025 | https://doi.org/10.3389/fnut.2025.1513747
This article is part of the Research Topic Nutrition Counseling for Non-Communicable Disease Management View all 3 articles
 Magdalena Sevilla-González1,2,3*
Magdalena Sevilla-González1,2,3* Ailema González-Ortiz4,5
Ailema González-Ortiz4,5 María Victoria Landa-Anell6
María Victoria Landa-Anell6 Marco A. Melgarejo-Hernández6,7
Marco A. Melgarejo-Hernández6,7 Ana Teresa Arias-Marroquín8
Ana Teresa Arias-Marroquín8 Fabiola Mabel Del Razo-Olvera7,9
Fabiola Mabel Del Razo-Olvera7,9 Berenice Monserrat Román-Calleja10
Berenice Monserrat Román-Calleja10 Ana Victoria Monreal-Lugo9
Ana Victoria Monreal-Lugo9 Angélica J. Martin-Vences11
Angélica J. Martin-Vences11 Karime Haua-Navarro12
Karime Haua-Navarro12 Angeles Espinosa-Cuevas13
Angeles Espinosa-Cuevas13Background: The Nutrition Care Process (NCP) is a systematic framework designed to enhance the quality of nutrition care. Given the high prevalence of metabolic diseases in Mexican population, there is a critical need for tailored nutrition care strategies.
Objective: We aim to describe the adaptation of the NCP to manage metabolic diseases in Mexican individuals.
Methods: Our adaptation included a comprehensive literature review of clinical nutrition guidelines, by a structured consultation with experts to ensure clinical setting-specific and culturally appropriate modifications. A team of registered dietitians from two tier 3 hospitals, each with over five years of experience in metabolic disease management, customized the NCP’s four core steps—assessment, diagnosis, intervention, and monitoring—to meet the specific needs of the Mexican population.
Results: We adapted the NCP to manage five common metabolic disorders: obesity, type 2 diabetes, kidney disease, metabolic dysfunction-associated steatotic liver disease, and dyslipidemia. Each step of the NCP was complemented by the development of educational materials designed to (1) enhance awareness of disease risk, (2) broaden their knowledge of nutritional management, and (3) provide tailored strategies for developing personalized action plans. The adapted NCP was implemented in clinical and research settings and the materials were documented as an online publication to facilitate widespread dissemination.
Conclusion: Our adaptation represents a significant advancement in the use of structured tools for nutrition care in Mexican populations, who face disproportionately high rates of metabolic diseases. Further research is needed to assess the effectiveness of this approach in clinical settings.
Metabolic diseases, including obesity, Type 2 Diabetes Mellitus (T2DM), chronic kidney disease (CKD), Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), and dyslipidemia, represent a significant global health challenge, particularly for Hispanic populations, where the rates of these disorders are disproportionately high. In Mexico, the 2022 National Health and Nutrition Survey (ENSANUT) indicates that 75.2% of Mexican adults are classified as overweight or obese (1). In 2021, this alarming rate was linked to 118,000 deaths attributable to elevated body mass index (BMI), with elevated BMI accounting for 55% of T2DM-related deaths and 41.1% of deaths from CKD (2). Dyslipidemia also significantly affects the adult population, with approximately 50% presenting some form of lipid disorder (3). Moreover, MASLD (previously known as NAFLD and later as MAFLD), represents a significant and growing public health challenge in Mexico with a prevalence of 17–41.3%, this condition is intricately linked to the country’s rising rates of obesity, T2DM, and metabolic syndrome (4). Despite its impact, accurate diagnosis of MASLD remains limited due to diagnostic challenges (5). In 2021, the prevalence of CKD was reported at 9,184.9 cases per 100,000 inhabitants, largely driven by T2DM, the leading cause of CKD. T2DM contributed to 69,052 deaths (95% CI = 60,412–77,991) across all age groups in Mexico (6). Furthermore, the prevalence of T2DM was estimated at 18.3% among adults aged 20 years and older, equating to around 14.6 million individuals (7).
Unhealthy dietary habits, particularly the consumption of sugary drinks, processed meats, saturated fats, and general caloric imbalance, are the most significant modifiable factors associated with metabolic diseases, contributing to 27.3% of Disability-Adjusted Life Years (DALY) lost (8). Effective management of these diseases requires addressing dietary risk factors. Nutritional Medical Treatment (NMT) is a crucial component emphasized in various consensus statements for its integration into multidisciplinary teams managing metabolic conditions. Guidelines recommend implementing NMT through comprehensive nutritional education programs aimed at promoting self-care. This approach should be consistently reinforced across different life contexts to achieve metabolic control, reduce complications, and improve quality of life (3, 9). International guidelines advocate for nutrition professionals to utilize evidence-based NMT to address nutritional issues at both individual and population levels.
The Nutrition Care Process (NCP), introduced by the Academy of Nutrition and Dietetics in 2003, provides a valuable framework for implementing NMT across various clinical settings (10–13). Despite its potential, the NCP is underutilized in nutrition service centers, primarily due to barriers such as inefficient staffing, limited time for documentation, and the lack of necessary infrastructure, including supportive electronic health record systems (14–17). While the NCP has been shown to enhance nutritional care quality in chronic metabolic diseases (18–20). most studies focus on non-Latin American settings. This gap indicates different health systems, food cultures, accessibilities, and metabolic disease rates, such as those in Mexico. Research supports the effectiveness of culturally adapted programs to improve lifestyle intervention adherence among Latinos in the US (21), underscoring the need for tools that simplify the NCP’s implementation in environments reflecting the unique characteristics of the Mexican population, especially concerning prevalent metabolic disorders, particularities of the health system and food culture. In this study, we aimed to describe the adaptation of the NCP for managing five metabolic diseases— Individuals with Obesity at Risk of Type 2 Diabetes (ORT2D), T2DM, CKD, MASLD, and dyslipidemia—in Mexican individuals. The objectives of the adaptation involved prioritizing specific evaluation items and nutritional diagnoses for each disease, creating educational materials, summarizing clinical guidelines for nutritional management, and recommending tailored monitoring tables for each pathology.
The selection criteria for the adaptation team for each disease included extensive experience in the nutrition care of metabolic diseases and significant research involvement. Seven dietitians from one tier 3 hospital and another from a different tier 3 hospital were selected based on their diverse clinical expertise and perspectives. All chosen dietitians were required to have at least a master’s degree and active participation in research protocols in their field, ensuring a rigorous evaluation of the quality of the evidence presented. Additionally, each dietitian had a minimum of five years of experience and was actively involved in their respective specialty departments. All members had also completed at least one training course on NCP methodology. The teams were organized by disease focus—ORT2D, T2DM, CKD, MASLD, and dyslipidemia—to optimize the adaptation process. The tier 3 hospitals function as referral centers, directing patients from various regions to specialized medical and nutritional care and also offering areas for non-specialized, general treatment. This structure accommodates a broad spectrum of the country’s healthcare needs and ensures a wide representation of the population.
The adaptation was done in three steps: 1.- Literature review, 2.- Adaptation to Mexican population, 3.- Adaptation of NCP to metabolic diseases and development of educational materials (Figure 1).
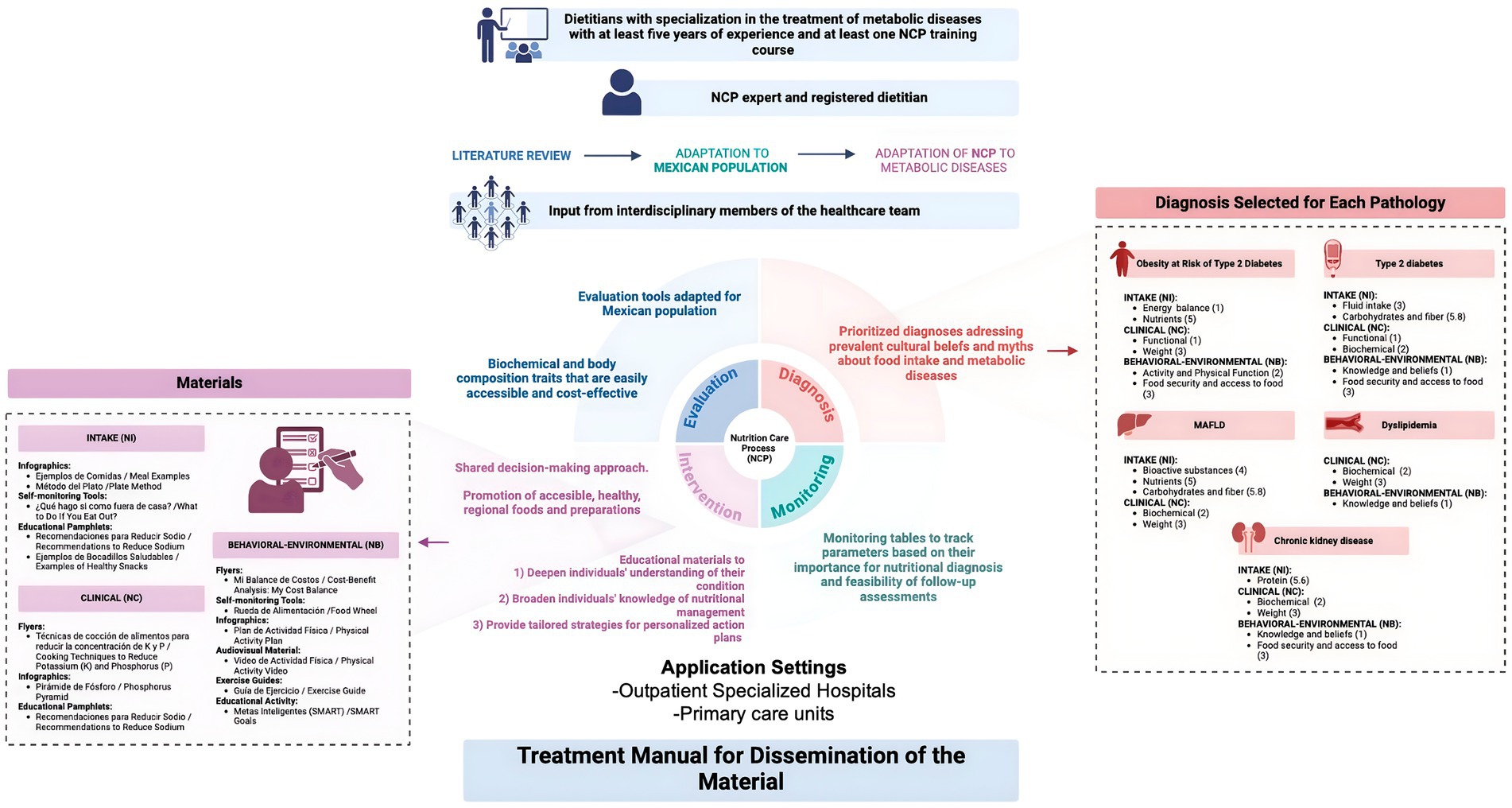
Figure 1. Summary of the adaptation of the nutrition care process in metabolic diseases in Mexican population. Created with BioRender.com.
Each team gathered scientific literature pertinent to their specific pathology. We conducted a literature review to gather the most current information on the epidemiological status and clinical guidelines for the nutritional management of five pathologies. Clinical guidelines were obtained from national and international medical societies, and we accessed relevant information through PubMed database. There was no restriction on the publication year for the literature search, although the most current clinical guidelines and research studies published more than five years ago were included, provided they were highly relevant to the topic. To standardize the literature search, each researcher used keywords and MeSH terms, excluding only reports and case series. We also prioritized studies focusing on the Mexican population.
Each team facilitated discussions with the aim to compare the recommendations outlined in the guidelines with their practical implementation in real clinical settings, identifying any discrepancies or gaps. This approach was designed to reveal potential deficiencies in the application of guidelines within real-world scenarios.
We carefully reviewed the evaluation items, aligning them with relevant literature to include only those pertinent or most used in the treatment of metabolic diseases. Similarly, we prioritized common diagnoses observed in clinical practice for adaptation. Regarding interventions, each team documented guidelines-based suggestions tailored to our population. To facilitate the educational intervention, we assembled a toolbox of educational resources. This helped to simplifying the explanation of nutritional and disease concepts. Some of the adapted materials were piloted implemented in an interdisciplinary program for treating individuals with T2DM, as well as in nutrition clinics for patients with dyslipidemia, MASLD, and renal diseases. This implementation facilitated valuable feedback from both patients and dietitians. Lastly, we developed pathology-specific monitoring tables, incorporating suggested monitoring times from literature and clinical practice.
The implementation of the educational materials was fully approved by the Ethics and Research Committee of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán and was registered at ClinicalTrials.gov (NCT02836808). Written informed consent was obtained from each participant. Research was conducted according to the tenets of the Helsinki Declaration of Human Studies principles.
Following the framework of the NCP methodology, each adaptation team sought input from interdisciplinary team members, all of whom were part of the same clinical team within the institution. These team members offered valuable insights into the patient treatment context and provided tools to identify referral signals. This collaborative approach ensures a comprehensive overview of patient needs for an effective care coordination.
Throughout the adaptation process, our team received invaluable support from an NCP expert—a registered dietitian with over a decade of experience in NCP methodology. With a robust background, including completion of courses at the Academy of Nutrition and Dietetics and years of experience conducting training sessions. Regular meetings were held with the expert to address queries and ensure clarity. The final report was reviewed and edited by the NCP expert, ensuring alignment with NCP standards. We documented our results and process in a document, which was published as a book.
Our literature review encompassed 370 articles, including 25 clinical practice guidelines. Two of these guidelines specifically focused on exercise and physical activity [Guides 1 (22) and 24 (23), as detailed in Table 1] for managing obesity and dyslipidemia. The majority of the guidelines supported the implementation of the NCP across various settings, primarily in primary care for metabolically stable patients. They provided a framework for outpatient management, with limited recommendations for inpatient care [Guides 8 (24) and 15 (25) in Table 1].
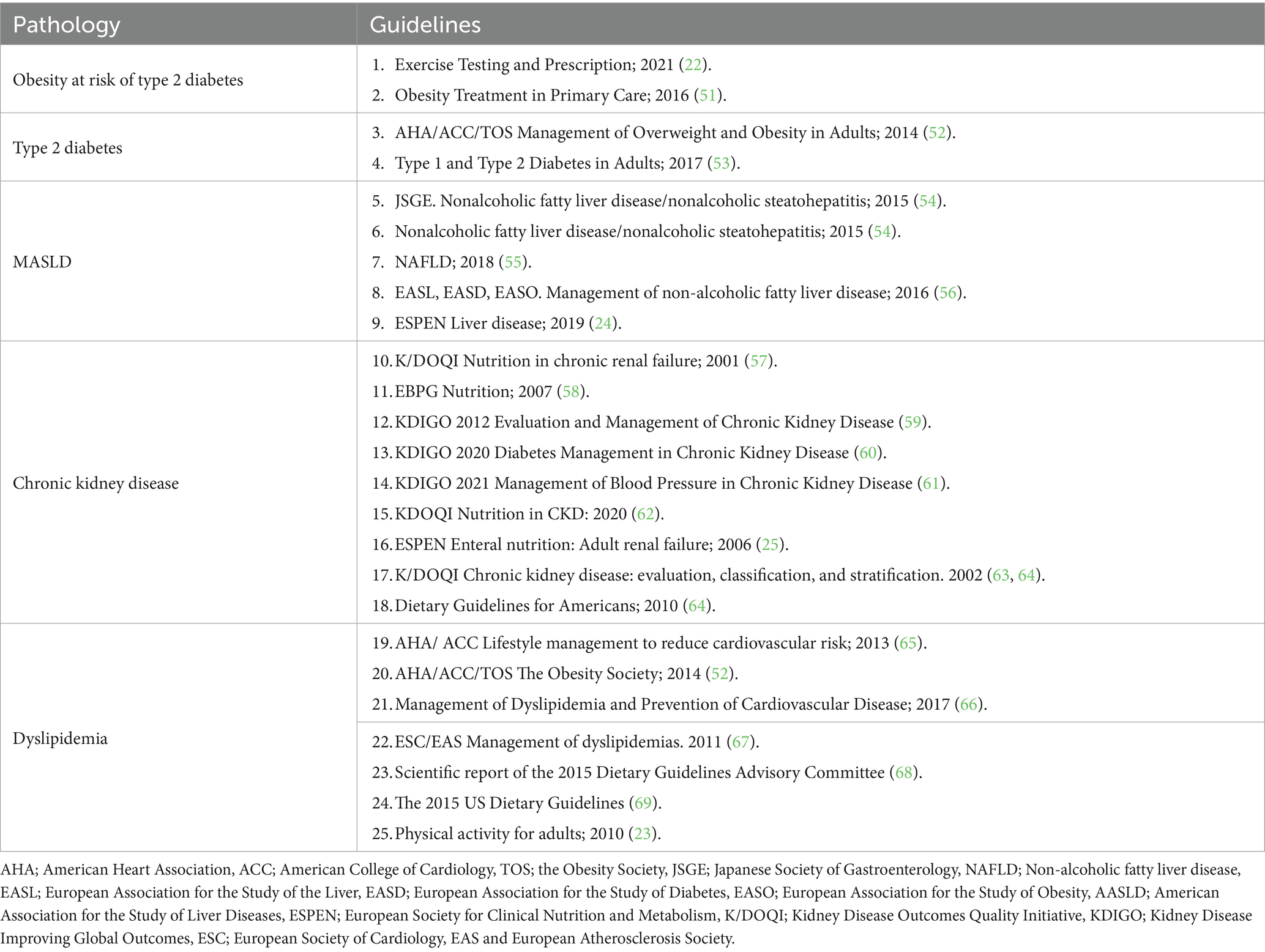
Table 1. Clinical guidelines used in the development of the adaptation of the NCP model in Mexican population.
In selecting evaluation items, we focused on the most commonly used and critical metrics for each pathology, prioritizing biochemical and body composition traits that are accessible and cost-effective. We developed medical histories in two formats—simplified and detailed—to accommodate diverse clinical settings and address the time constraints faced by dietitians in both primary care and tier 3 hospitals within the Mexican health system. Our aim was to streamline the evaluation process, enhancing efficiency and practicality for healthcare professionals. Furthermore, we incorporated Mexican-adapted evaluation tools, such as the Malnutrition Inflammation Score for CKD (26), vector analysis and body composition assessments in hemodialysis patients (27) and two formulas for estimating energy expenditure specific to the Mexican population (28, 29).
For diagnostics, we identified the conditions most commonly observed in individuals with the specified metabolic pathologies. Special attention was given to addressing prevalent cultural beliefs and myths related to food intake that negatively impact the understanding and management of these diseases. Recognizing that individuals in this population can be at risk for metabolic diseases even at lower BMI values (30, 31), we emphasized the importance of considering alternative parameters beyond BMI for diagnosis. Where feasible (in-hospital or clinical research settings), more precise anthropometric and clinical measures like body fat percentage were utilized to provide a better assessment of health status. The most common diagnostics for each pathology are detailed in Table 2.
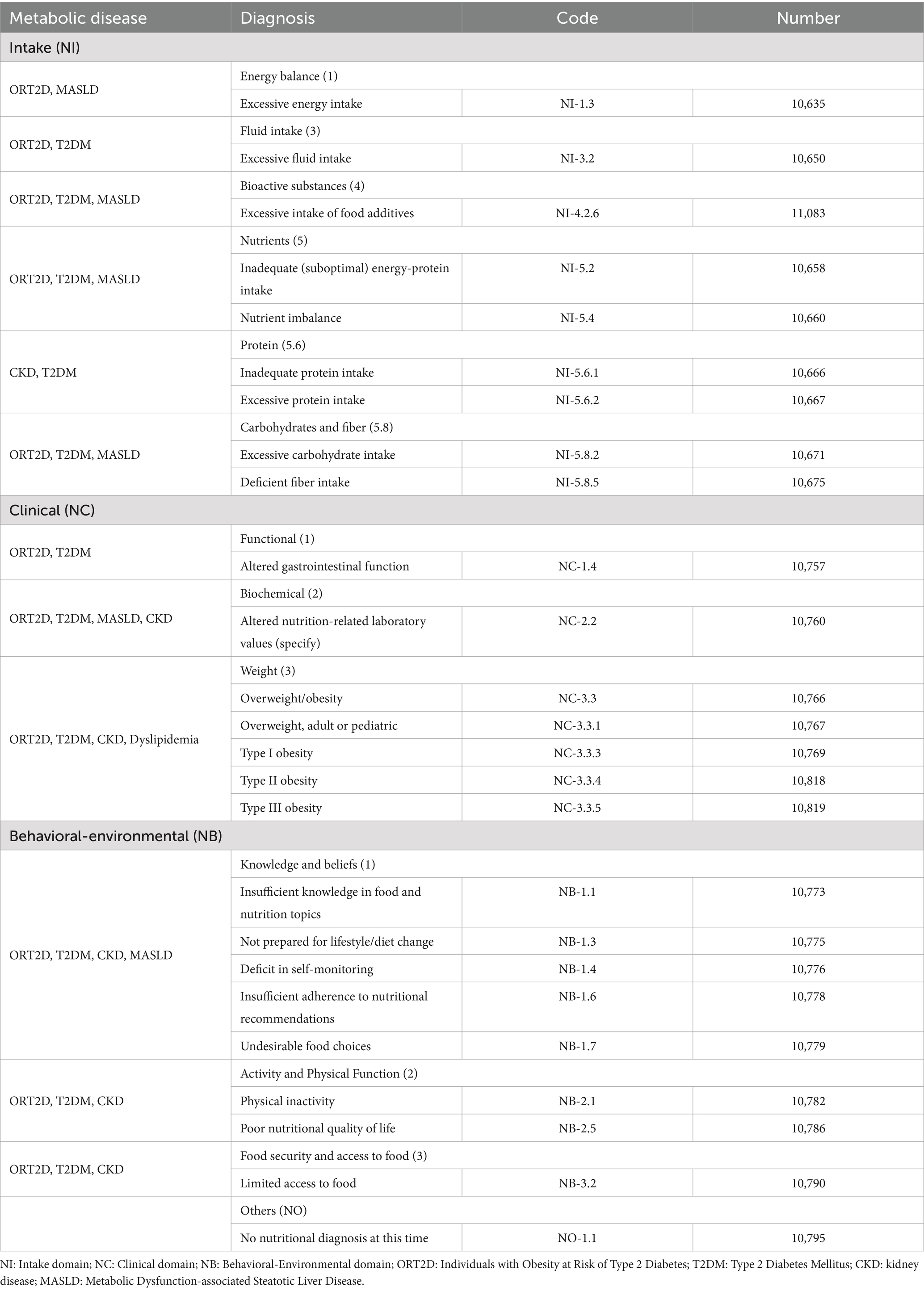
Table 2. Common nutritional care process diagnosis selected for each pathology.
We tailored dietary modifications to consider the availability of regional foods and the specific nutritional needs of the Mexican population (32). Additionally, these modifications were integrated into dietary recommendations for outpatient nutritional counseling, ensuring they are practical and applicable in real-world settings. Key macronutrient adjustments were made in sources of carbohydrates, proteins, and fatty acids. In Mexico, corn is a primary carbohydrate source, while chicken, eggs and beans are significant protein sources (33–35). We developed strategies to highlight the availability and accessibility of healthy food options, challenging the prevailing belief that healthy eating is expensive and hard to reach (36). Our objective was to promote healthier versions of regional foods through nutritious preparations, positioning these healthier choices as the most convenient option.
We adopted a shared decision-making framework, wherein health-related decisions are collaboratively made between the patient and a health professional (37, 38). Specifically, treatment options were discussed between dietitians and patients, with a strong emphasis on adapting these options to be more accessible for the patients. This approach enabled patients to choose the treatment strategies they found most suitable. Additionally, when setting goals, we utilized the SMART method (39) to ensure they were specific, measurable, achievable, relevant, and time-bound, thereby enhancing the effectiveness and achievability of the goals set during counseling.
Our educational resources were designed to address three critical areas: healthy eating, physical activity, and disease risk awareness. The materials aimed to enhance individual’s awareness of disease risks, enhance their knowledge of nutritional management, and provide tailored strategies for personalized action plans. We ensured that all materials were written in clear, accessible language and featured engaging designs. They were produced in various formats, including infographics, educational pamphlets, recipes, exercise guides, and self-monitoring tools. Infographics and pamphlets provided concise, clear information on nutrition and health, offering guidelines for balanced diets and disease-specific advice. Interactive educational activities were incorporated to boost participant engagement and understanding of their conditions. Recipe books highlighted practical, balanced meal examples, focusing on regional recipes and locally accessible ingredients. Audiovisual materials were utilized in training sessions and workshops to reinforce learning. A summary of each educational material, its focus area, and its alignment with diagnoses from the NCP is detailed in Table 3.
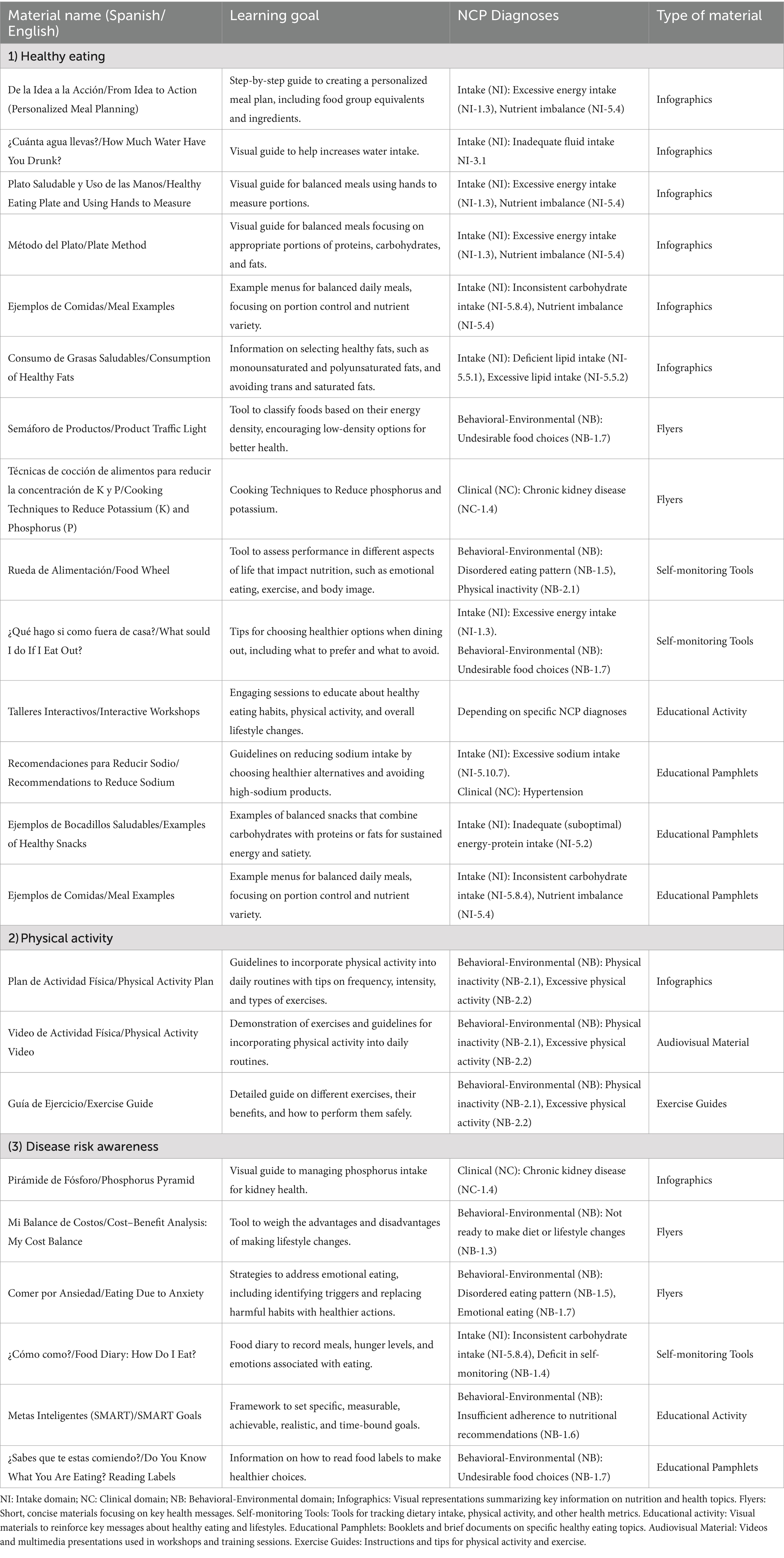
Table 3. Materials, learning goal, NCP diagnoses and type of material.
For the pathologies ORT2D and MASLD, we engaged with physicians specializing in these disorders to gain deeper insights into the integration of nutritional and medical treatments. Specifically, for ORT2D, feedback from a psychology expert was incorporated, detailing tools designed to enhance patient adherence to nutritional treatments. Recognizing the high demand for treatment among these patient populations, we also explored the implementation of electronic tools aimed at improving adherence to dietary recommendations, which could facilitate more efficient patient management and outcome tracking (40).
We developed monitoring tables to systematically track the most relevant clinical and behavioral parameters across subsequent visits. The selection of these parameters was based on their critical role in nutritional diagnosis and their feasibility for follow-up assessments in real world-settings. Given the logistical and economic challenges faced by this population, including limited appointment availability and transportation difficulties, we prioritized parameters that are practical and cost-effective to monitor. Additionally, considering the high costs of clinical tests for patients and institutions, optimizing these parameters is essential for resource management and effective monitoring. To address and mitigate barriers during treatment, we employed strategies derived from documented experiences of individuals with T2DM (41) in similar settings, facilitating improved adherence and outcomes.
The adapted NCP was implemented across various clinical and research settings, each tailored to meet specific needs and objectives. In research settings, the adaptation was primarily applied within lifestyle intervention protocols for individuals at risk of type 2 diabetes. These protocols utilized the adapted NCP to guide personalized nutritional interventions, emphasizing evaluation, nutrition diagnosis, and rigorous documentation and follow-up, as detailed in our recent studies (40, 42).
In contrast, the clinical implementation focused on comprehensive care programs at the National Institute of Medical Sciences and Nutrition Salvador Zubirán in Mexico City. Here, the adapted NCP was integrated into routine patient care for managing Type 2 Diabetes Mellitus (T2DM), supporting patients in achieving and maintaining health goals through structured nutritional interventions within a multidisciplinary team framework (11, 41, 43–45).
Additionally, departments specializing in dyslipidemia, gastroenterology, and renal diseases at the same institute adopted the adapted NCP materials, including educational resources and nutritional diagnostic processes, into their clinical practices. Evidence indicates feasibility of implementation and differences in the effectiveness of the adapted NCP across clinical and research settings. In research protocols, the adapted approach not only standardized lifestyle interventions among dietitians but also enhanced the monitoring of nutritional care. In clinical settings, the adaptation has contributed to identify the barriers to adherence to a nutritional plan and strategies to overcome them in patients with T2D (41). It also supported the stratification of individuals based on their nutritional diagnosis, enabling more tailored and effective nutritional treatment within an interdisciplinary program (11). These findings suggest that the implementation of culturally and disease-adapted nutritional interventions can significantly improve nutrition practice across diverse settings.
To disseminate our findings, we compiled them into a comprehensive book. The book is structured into six chapters: the first chapter outlines the general principles of the NCP, while the subsequent chapters focus on its implementation for specific pathologies. Where applicable, subchapters on interdisciplinary treatment approaches are also included. Each chapter begins with an introduction to the disease, followed by a presentation of its global and regional epidemiology. The chapters detail how the steps of the NCP—evaluation, diagnosis, intervention, and monitoring—are tailored for each pathology. To enhance clarity and usability, abbreviated tables summarizing the most frequently used NCP terms for each pathology are included. A detailed checklist of the sections for each pathology can be found in Supplementary Table S1. Furthermore, we developed a comprehensive toolbox of educational resources to support the effective implementation of the NCP. Each chapter also features a clinical case example, demonstrating the practical application of the materials in real-world scenarios. The book is available as an online publication at the following link: https://www.amazon.com.mx/proceso-atencion-nutricia-enfermedades-metab%C3%B3licas-ebook/dp/B0BPJKNDHZ. The content of the book was reviewed and subsequently approved by the publications committee of the Mexican Society of Endocrinology and Nutrition, ensuring the integrity and accuracy of the information presented.
We adapted the NCP to address five prevalent metabolic diseases in the Mexican population. The material provides a standardized framework for the various NCP steps—diagnosis, evaluation, nutritional intervention, and monitoring—to ensure consistent care across different settings and providers. Each step of the NCP was meticulously customized to these conditions, including the development of targeted educational materials designed to (1) increasing individuals’ disease risk awareness, (2) broaden their knowledge of nutritional management, and (3) provide tailored strategies for developing personalized action plans. This tailored approach was successfully implemented in both research and clinical environments. The educational materials created are documented in an online book publication, serving as a valuable resource for health professionals.
The NCP has been adapted and successfully implemented in diverse settings and geographical locations, though several barriers to its adoption have been noted. In the Philippines, authors at a level 3 hospital emphasized the need for enhanced support from institutions, professional organizations, and policymakers to facilitate implementation (46). In Saudi Arabia, although most dietitians are familiar with the NCP and confident in its application, it has not yet been adopted as a standard practice in hospitals (47). Australian dietitians, prior to implementation, reported barriers including a lack of knowledge, support, training, and resources, while those already using the NCP identified heavy workloads and work status as obstacles (48). Lövestam et al. stressed the necessity for context-specific strategies to address local challenges and improve dietetic support (16).
The primary barriers to NCP implementation have been identified as inefficient staffing, limited time for completing necessary documentation, and the lack of supportive infrastructure, such as electronic health record systems (16, 17). In Switzerland, the integration of NCP documentation into electronic patient records has helped strengthen the linkage between assessment and nutrition diagnosis, although the frequent selection of similar nutrition problems by dietitians’ points to an ongoing challenge in adopting critical thinking (49). Additionally, Chen et al. explored mobile applications as a means to enhance the efficiency of the nutrition care process, potentially freeing up more time for dietetic counseling (50), found that apps could improve the efficiency of the nutrition care process, allowing more time for dietetic counseling. While these apps show promise in complementing dietetic care, they cannot replace direct practice. In Mexico, where the demand for healthcare services related to metabolic diseases is rapidly increasing, the adoption of electronic systems and tools that streamline healthcare management and reduce commute times to hospitals presents an attractive opportunity for further exploration.
Our study represents a pioneering effort in adapting the NCP for metabolic diseases within a Latin-American context, marking the first such implementation across diverse clinical and research settings in the region. This adaptation not only addresses a significant gap in the literature but also provides a practical framework for healthcare professionals in similar settings. However, several limitations warrant mention. First, the literature review that underpinned the adaptation process was conducted several years ago. While it incorporated the most relevant and up-to-date references available at that time, some of the references may now appear outdated, potentially overlooking recent advances in the management of metabolic diseases. Despite this, we have made efforts to update critical aspects, such as the nomenclature and clinical nutrition management of the diseases, to reflect current standards and practices. Second, the scope of the literature review was primarily confined to PubMed. This decision was made due to PubMed’s comprehensive coverage of biomedical literature, which aligned well with our study’s focus on metabolic diseases. However, this approach, while thorough within its specified domain, inevitably limited the breadth of our review by excluding potentially valuable insights from broader multidisciplinary sources available in other databases such as Web of Science or ScienceDirect. This limitation may have restricted our perspective and lessened the comprehensiveness of the adaptation process.
The effective implementation of the NCP in Mexican healthcare settings demands a well-established set of skills, robust institutional support, and specific practices to ensure its adoption, sustainability, and impact. Dietitians treating metabolic diseases often encounter significant challenges, including high workloads and budget constraints, which can impede the adoption of new strategies requiring additional training or resources. Moreover, the role of dietitians is not consistently defined within institutional decision-making processes, complicating the implementation of standardized care protocols. Successful implementation relies on allocating dedicated time for practitioners to familiarize themselves with the NCP, providing ongoing training to maintain and improve skills, and securing strong support and leadership from management and department leaders. These elements represent both challenges and opportunities for institutions to advocate for programs that demonstrate the benefits of such changes, thereby supporting the sustained impact of the NCP. The adapted NCP discussed in this study marks substantial progress in creating targeted tools to enhance nutritional counseling practices in populations severely affected by metabolic diseases. A standardized NCP framework not only promotes consistent practice but also provides a solid basis for evaluating the effects of nutrition care on patient health outcomes. Achieving this, however, requires active participation and commitment from both institutions and healthcare professionals. Future research should focus on validating the effectiveness of these tools in real-world settings exploring their implementation alongside electronic systems to optimize service delivery.
We adapted the NCP for five metabolic diseases, incorporating assessment tools, dietary recommendations, and educational materials specifically tailored to the Mexican population. This comprehensive framework is designed to enhance professional nutrition practice. The adaptation is particularly significant for the Mexican population, which faces disproportionately high rates of metabolic diseases and associated treatment challenges. Who face disproportionately high rates of metabolic diseases and related treatment challenges. Future research is needed to evaluate the effectiveness of this adapted NCP in clinical settings and to explore its integration with electronic health records and mobile apps to facilitate implementation within health systems.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics and Research Committee of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AG-O: Investigation, Validation, Writing – original draft. ML-A: Conceptualization, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing. MM-H: Conceptualization, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing. AA-M: Visualization, Writing – review & editing. FDR-O: Investigation, Validation, Writing – original draft, Writing – review & editing. BR-C: Investigation, Validation, Writing – review & editing. AM-L: Validation, Visualization, Writing – review & editing. AM-V: Investigation, Validation, Writing – review & editing. KH-N: Investigation, Validation, Writing – review & editing. AE-C: Investigation, Validation, Writing – review & editing. MS-G: Conceptualization, Supervision, Investigation, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. MSG is supported by the American Diabetes Association grant 9-22-PDFPM-04 and by the NIH NIDDK grant 5U24DK132733-02.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that Gen AI was used in the creation of this manuscript. During the preparation of this work the authors used ChatGPT in order to improve readability. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1513747/full#supplementary-material
1. Campos-Nonato, I, Galván-Valencia, O, Hernández-Barrera, L, Oviedo-Solís, C, and Barquera, S. Prevalencia de obesidad y factores de riesgo asociados en adultos mexicanos: resultados de la Ensanut 2022. Salud Publica de Mexico. (2023) 65:s238–47. doi: 10.21149/14809
2. Arreola-Ornelas, H, Merino-Juárez, GA, Contreras-Loya, D, Méndez-Carniado, O, Morales-Juárez, L, Bernal-Serrano, D, et al. Burden of overweight and obesity in Mexico from 1990 to 2021. Gac Med Mex. (2023) 159:543–56. doi: 10.24875/GMM.M24000836
3. Hernández-Alcaraz, C, Aguilar-Salinas, CA, Mendoza-Herrera, K, Pedroza-Tobías, A, Villalpando, S, Shamah-Levy, T, et al. Dyslipidemia prevalence, awareness, treatment and control in Mexico: results of the Ensanut 2012. Salud Pública de México. (2020) 62:137–46. doi: 10.21149/10520
4. Méndez-Sánchez, N, and Díaz-Orozco, LE. Editorial: international consensus recommendations to replace the terminology of non-alcoholic fatty liver disease (NAFLD) with metabolic-associated fatty liver disease (MAFLD). Med Sci Monitor. (2021) 27:e933860. doi: 10.12659/MSM.933860
5. Sayiner, M, Koenig, A, Henry, L, and Younossi, ZM. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic Steatohepatitis in the United States and the rest of the world. Clin Liver Dis. (2016) 20:205–14. doi: 10.1016/j.cld.2015.10.001
6. Argaiz, ER, Morales-Juárez, L, Razo, C, Ong, L, Rafferty, Q, Rincón-Pedrero, R, et al. The burden of chronic kidney disease in Mexico. Data analysis based on the global burden of disease 2021 study. Gac Med Mex. (2024) 159:487–93. doi: 10.24875/GMM.M24000830
7. Basto-Abreu, A, López-Olmedo, N, Rojas-Martínez, R, Aguilar-Salinas, CA, Moreno-Banda, GL, Carnalla, M, et al. Prevalencia de prediabetes y diabetes en México: Ensanut 2022. Instituto Nacional de Salud Publica. (2023) 65:s163–8. doi: 10.21149/14832
8. Montoya, A, Gallardo-Rincón, H, Silva-Tinoco, R, García-Cerde, R, Razo, C, Ong, L, et al. Type 2 diabetes epidemic in Mexico. Burden of disease 1990-2021 analysis and implications for public policies. Gac Med Mex. (2023) 159:474–86. doi: 10.24875/GMM.M24000835
9. Fajardo Dolci, G.E., Anda, F.J.V.De, Ortiz-Vázquez, P., and Olaiz-Fernández, G. (2023). “The burden of cardiovascular disease in Mexico 1990–2021. Summary of the global burden of disease 2021 study”, Gac Med Mex, 159:557–564, doi: 10.24875/GMM.M24000837
10. Lamers-Johnson, E, Kelley, K, Knippen, KL, Feddersen, K, Sánchez, DM, Parrott, JS, et al. A quasi-experimental study provides evidence that registered dietitian nutritionist care is aligned with the academy of nutrition and dietetics evidence-based nutrition practice guidelines for type 1 and 2 diabetes. Front Nutr. (2022) 9:1–10, doi: 10.3389/FNUT.2022.969360
11. Landa-Anell, MV, Del Razo-Olvera, FM, Bodnar, I, Cordova-Isidro, B, Lagunas-Valdepeña, D, Arias-Marroquín, AT, et al. Nutritional diagnoses in people with type 2 diabetes: association with metabolic, anthropometric, and dietary parameters. Front Nutr. (2024) 11:1473429. doi: 10.3389/FNUT.2024.1473429
12. Lee, SY, Kim, J, Oh, S, Kim, YM, Woo, S, Jang, HB, et al. “A 24-week intervention based on nutrition care process improves diet quality, body mass index, and motivation in children and adolescents with obesity”. Nutr Res. (2020) 84:53–62. doi: 10.1016/J.NUTRES.2020.09.005
13. Rushton, A, Edwards, A, Bauer, J, and Bell, JJ. Dietitian assistant opportunities within the nutrition care process for patients with or at risk of malnutrition: a systematic review. Nutr Diet. (2021) 78:69–85. doi: 10.1111/1747-0080.12651
14. Lacey, K, and Pritchett, E. Nutrition care process and model: ADA adopts road map to quality care and outcomes management. J Am Diet Assoc. (2003) 103:1061–72. doi: 10.1016/S0002-8223(03)00971-4
15. Lewis, S, Miranda, L, Kurtz, J, Brewer, WJ, and Papoutsakis, C. Harnessing the benefits of the nutrition care process quality evaluation and standardization tool: a National Auditing Initiative to improve quality of documentation. J Acad Nutr Diet. (2023) 123:1662–8. doi: 10.1016/J.JAND.2023.07.001
16. Lövestam, E, Boström, AM, and Orrevall, Y. Nutrition care process implementation: experiences in various dietetics environments in Sweden. J Acad Nutr Diet. (2017) 117:1738–48. doi: 10.1016/J.JAND.2017.02.001
17. Maeda, K, Egashira, F, Ueshima, J, Horikoshi, Y, and Kamoshita, S. A survey of the nutrition care process in Japanese acute care hospitals using a nationwide web-based questionnaire. Asia Pac J Clin Nutr. (2024) 33:515–28. doi: 10.6133/APJCN.202412_33(4).0006
18. Lewis, SL, Wright, L, Arikawa, AY, and Papoutsakis, C. Etiology intervention link predicts resolution of nutrition diagnosis: a nutrition care process outcomes study from a veterans’ health care facility. J Acad Nutr Diet. (2021) 121:1831–40. doi: 10.1016/J.JAND.2020.04.015
19. Nutrition care process and model part I: the 2008 update. J Am Diet Assoc. (2008) 108:1113–7. doi: 10.1016/J.JADA.2008.04.027
20. Swan, WI, Vivanti, A, Hakel-Smith, NA, Hotson, B, Orrevall, Y, Trostler, N, et al. Nutrition care process and model update: toward realizing people-centered care and outcomes management. J Acad Nutr Diet. (2017) 117:2003–14. doi: 10.1016/J.JAND.2017.07.015
21. Guirette, M, Sevilla-Gonzalez, M, Balaguera, M, and Caballero, AE. A nutrition-focused review of the interventions in US-living Latino communities with type II diabetes. Front Nutr. (2024) 11:1418683. doi: 10.3389/FNUT.2024.1418683
22. Warburton, DER, Charlesworth, S, Ivey, A, Nettlefold, L, and Bredin, SSD. A systematic review of the evidence for Canada’s physical activity guidelines for adults. Int J Behav Nutr Phys Act. (2010) 7. doi: 10.1186/1479-5868-7-39
23. Britten, P, Cleveland, LE, Koegel, KL, Kuczynski, KJ, and Nickols-Richardson, SM. Updated US Department of Agriculture Food Patterns meet goals of the 2010 dietary guidelines. J Acad Nutr Diet. (2012) 112:1648–55. doi: 10.1016/J.JAND.2012.05.021
24. Plauth, M, Bernal, W, Dasarathy, S, Merli, M, Plank, LD, Schütz, T, et al. “ESPEN guideline on clinical nutrition in liver disease”. Clin Nutr. (2019) 38:485–521. doi: 10.1016/J.CLNU.2018.12.022
25. Cano, N, Fiaccadori, E, Tesinsky, P, Toigo, G, Druml, W, Kuhlmann, M, et al. “ESPEN guidelines on enteral nutrition: adult renal failure”. Clin Nutr. (2006) 25:295–310. doi: 10.1016/J.CLNU.2006.01.023
26. Gonz ález-Ortiz, AJ, Arce-Santander, CV, Vega-Vega, O, Correa-Rotter, R, and Espinosa-Cuevas, MA. Assessment of the reliability and consistency of the ‘malnutrition inflammation score’ (MIS) in Mexican adults with chronic kidney disease for diagnosis of protein-energy wasting syndrome (PEW). Nutr Hosp. (2014) 31:1352–8. doi: 10.3305/NH.2015.31.3.8173
27. “[Bioimpedance vector analysis for body composition in Mexican population]—PubMed”. (n.d.). Available at: https://pubmed-ncbi-nlm-nih-gov.ezp-prod1.hul.harvard.edu/17569296/ (accessed 22 September 2024).
28. “Basal metabolic rate and body fatness of adult men in northern Mexico—PubMed”. (n.d.). Available at: https://pubmed.ncbi.nlm.nih.gov/8194506/ (accessed 2 October 2024).
29. Orozco-Ruiz, X, Pichardo-Ontiveros, E, Tovar, AR, Torres, N, Medina-Vera, I, Prinelli, F, et al. “Development and validation of new predictive equation for resting energy expenditure in adults with overweight and obesity”, clinical nutrition (Edinburgh, Scotland). Clin Nutr. (2018) 37:2198–205. doi: 10.1016/J.CLNU.2017.10.022
30. Williams Amy, AL, Jacobs Suzanne, SBR, Moreno-Macías, H, Huerta-Chagoya, A, Churchhouse, C, Márquez-Luna, C, et al. Sequence variants in SLC16A11 are a common risk factor for type 2 diabetes in Mexico. Nature. (2014) 506:97–101. doi: 10.1038/nature12828
31. Wong, WW, Strizich, G, Heo, M, Heymsfield, SB, Himes, JH, Rock, CL, et al. “Relationship between body fat and BMI in a US Hispanic population-based cohort study: results from HCHS/SOL”. Obesity. (2016) 24:1561–71. doi: 10.1002/OBY.21495
32. Aburto, TC, Pedraza, LS, Sánchez-Pimienta, TG, Batis, C, and Rivera, JA. Discretionary foods have a high contribution and fruit, vegetables, and legumes have a low contribution to the Total energy intake of the Mexican population. J Nutr. (2016) 146:1881S–7S. doi: 10.3945/JN.115.219121
33. Biruete, A, Leal-Escobar, G, Espinosa-Cuevas, Á, Mojica, L, and Kistler, BM. Dieta de la Milpa: a culturally-concordant plant-based dietary pattern for Hispanic/Latine people with chronic kidney disease. Nutrients. (2024) 16:574. doi: 10.3390/NU16050574
34. Rivera, JA, Pedraza, LS, Aburto, TC, Batis, C, Sánchez-Pimienta, TG, de Cosío, TG, et al. Overview of the dietary intakes of the Mexican population: results from the National Health and nutrition survey 2012. J Nutr. (2016) 146:1851S–5S. doi: 10.3945/JN.115.221275
35. Valerino-Perea, S, Lara-Castor, L, Armstrong, MEG, and Papadaki, A. “Definition of the traditional Mexican diet and its role in health: a systematic review”. Nutrients. (2019) 11. doi: 10.3390/NU11112803
36. Clark, P, Mendoza-Gutiérrez, CF, Montiel-Ojeda, D, Denova-Gutiérrez, E, López-González, D, Moreno-Altamirano, L, et al. A healthy diet is not more expensive than less healthy options: cost-analysis of different dietary patterns in mexican children and adolescents. Nutrients. (2021) 13:11. doi: 10.3390/NU13113871/S1
37. Briss, P, Rimer, B, Reilley, B, Coates, RC, Lee, NC, Mullen, P, et al. “Promoting informed decisions about cancer screening in communities and healthcare systems”. Am J Prev Med. (2004) 26:67–80. doi: 10.1016/j.amepre.2003.09.012
38. Charles, C, Gafni, A, and Whelan, T. Shared decision-making in the medical encounter: what does it mean? (or it takes, at least two to tango). Soc Sci Med. (1997) 44:681–92. doi: 10.1016/S0277-9536(96)00221-3
39. Bjerke, MB, and Renger, R. Being SMART about writing SMART objectives. Eval Prog Plan. (2017) 61:125–7. doi: 10.1016/J.EVALPROGPLAN.2016.12.009
40. Del Rocio Sevilla-Gonzalez, M, Bourguet-Ramirez, B, Lazaro-Carrera, LS, Martagon-Rosado, AJ, Gomez-Velasco, DV, and Viveros-Ruiz, TL. “Evaluation of a web platform to record lifestyle habits in subjects at risk of developing type 2 diabetes in a middle-income population: prospective interventional study”. JMIR Diab. (2022) 7:e25105. doi: 10.2196/25105
41. Landa-Anell, MV, Melgarejo-Hernández, MA, García-Ulloa, AC, Del Razo-Olvera, FM, Velázquez-Jurado, HR, and Hernández-Jiménez, S. “Barriers to adherence to a nutritional plan and strategies to overcome them in patients with type 2 diabetes mellitus; results after two years of follow-up”, Endocrinologia, diabetes y Nutricion. Endocrinol Diabetes Nutr (Engl Ed). (2020) 67:4–12. doi: 10.1016/J.ENDINU.2019.05.007
42. Sevilla-Gonzalez, MDR, Manning, AK, Westerman, KE, Aguilar-Salinas, CA, Deik, A, and Clish, CB. Metabolomic markers of glucose regulation after a lifestyle intervention in prediabetes. BMJ Special J. (2022) 10:e003010. doi: 10.1136/BMJDRC-2022-003010
43. Garcia-Ulloa, AC, Landa-Anell, V, Melgarejo-Hernández, M, Villegas-Narvaez, A, Urbina-Arronte, LE, and Hernández-Jimenez, S. Assessment of a multidisciplinary intervention in patients with BMI ≥35 kg/m2 and recently diagnosed type 2 diabetes. J Clin Endocrinol Metab. (2019) 104:2994–3002. doi: 10.1210/JC.2018-01148
44. Hernández-Jiménez, S, García-Ulloa, AC, Bello-Chavolla, OY, Aguilar-Salinas, CA, and Kershenobich-Stalnikowitz, D. Long-term effectiveness of a type 2 diabetes comprehensive care program. The CAIPaDi model. Diabetes Res Clin Pract. (2019) 151:128–37. doi: 10.1016/J.DIABRES.2019.04.009
45. Hernandez-Jimenez, S, Garcia-Ulloa, C, Mehta, R, Aguilar-Salinas, C, and Kershenobich-Stalnikowitz, D. Innovative models for the empowerment of patients with type 2 diabetes: the CAIPaDi program. Recent Pat Endocr Metab Immune Drug Discov. (2014) 8:202–9. doi: 10.2174/1872214808999141110155515
46. Delomen, JI, Bernardo, AKM, and Centeno, EMM. Ascertainment of nutrition care process (NCP) implementation and use of NCP terminologies (NCPT) among hospital dietitians in the Philippines. Acta Medica Philippina. (2024) 58:40–51. doi: 10.47895/AMP.VI0.6697
47. Alkhaldy, AA, Allahyani, MN, Alghamdi, NA, Jeddawi, AK, Malibary, RM, and Al-Othman, AM. Status of nutrition care process implementation in hospitals in Jeddah, Saudi Arabia. Clin Nutr. (2020) 36:53–9. doi: 10.1016/J.CLNESP.2020.02.007
48. Porter, JM, Devine, A, Vivanti, A, Ferguson, M, and O’Sullivan, TA. Development of a nutrition care process implementation package for hospital dietetic departments. Nutrition Dietetic. (2015) 72:205–12. doi: 10.1111/1747-0080.12169
49. Aurélien, C, Isabelle, C, and Ludivine, S. Evaluation of the nutrition care process documentation in the patients’ records using the diet-NCP-audit: experience in a medium-sized multi-site Swiss hospital. J Hum Nutr Diet. (2024) 37:593–600. doi: 10.1111/JHN.13283
50. Chen, J, Gemming, L, Hanning, R, and Allman-Farinelli, M. Smartphone apps and the nutrition care process: current perspectives and future considerations. Patient Educ Counsel. (2018) 101:750–7. doi: 10.1016/J.PEC.2017.11.011
51. Thompson, PD, Arena, R, Riebe, D, and Pescatello, LS. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription, ninth edition. Curr Sports Med Rep. (2013) 12:215–7. doi: 10.1249/JSR.0B013E31829A68CF
52. Jensen, MD, Ryan, DH, Apovian, CM, Ard, JD, Comuzzie, AG, Donato, KA, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Obesity Society. Circulation. (2014) 129:2. doi: 10.1161/01.CIR.0000437739.71477.EE
53. Franz, MJ, MacLeod, J, Evert, A, Brown, C, Gradwell, E, Handu, D, et al. Academy of nutrition and dietetics nutrition practice guideline for type 1 and type 2 diabetes in adults: systematic review of evidence for medical nutrition therapy effectiveness and recommendations for integration into the nutrition care process. J Acad Nutr Diet. (2017) 117:1659–79. doi: 10.1016/J.JAND.2017.03.022
54. Watanabe, S, Hashimoto, E, Ikejima, K, Uto, H, Ono, M, Sumida, Y, et al. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. J Gastroenterol. (2015) 50:364–77. doi: 10.1007/S00535-015-1050-7
55. Aller, R, Fernández-Rodríguez, C, Iacono, O, Bañares, R, Abad, J, Carrión, JA, et al. Consensus document. Management of non-alcoholic fatty liver disease (NAFLD). Clinical practice guideline. Gastroenterol Hepatol. (2018) 41:328–49. doi: 10.1016/J.GASTROHEP.2017.12.003
56. Marchesini, G, Day, CP, Dufour, JF, Canbay, A, Nobili, V, Ratziu, V, et al. EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. (2016) 64:1388–402. doi: 10.1016/J.JHEP.2015.11.004
57. Kopple, JD. National kidney foundation K/DOQI clinical practice guidelines for nutrition in chronic renal failure. Am J Kidney Dis. (2001) 37:S66–70. doi: 10.1053/AJKD.2001.20748
58. Fouque, D., Vennegoor, M., Wee, P.Ter, Wanner, C., Basci, A., Canaud, B., et al. (2007). “EBPG Guideline on Nutrition”, Nephrology Dialysis Transpl, 22:ii45, doi: 10.1093/NDT/GFM020
59. “CKD evaluation and management – KDIGO”. (n.d.). Available at: https://kdigo.org/guidelines/ckd-evaluation-and-management/ (accessed 15 August 2024).
60. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney international. Kidney Int. (2020) 98:S1–S115. doi: 10.1016/J.KINT.2020.06.019
61. Cheung, AK, Chang, TI, Cushman, WC, Furth, SL, Hou, FF, Ix, JH, et al. KDIGO 2021 clinical practice guideline for the Management of Blood Pressure in chronic kidney disease. Kidney Int. (2021) 99:S1–S87. doi: 10.1016/J.KINT.2020.11.003
62. Ikizler, TA, Burrowes, JD, Byham-Gray, LD, Campbell, KL, Carrero, JJ, Chan, W, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kidney Dis. (2020) 76:S1–S107. doi: 10.1053/J.AJKD.2020.05.006
63. Levey, AS, Coresh, J, Balk, E, Kausz, AT, Levin, A, Steffes, MW, et al. “National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification”. Ann Intern Med. (2003) 139:137–47. doi: 10.7326/0003-4819-139-2-200307150-00013
64. McGuire, S. “U.S. Department of Agriculture and U.S. Department of Health and Human Services, dietary guidelines for Americans, 2010. 7th edition, Washington, DC: U.S. government printing office, January 2011”. Adv Nutr. (2011) 2:293–4. doi: 10.3945/AN.111.000430
65. Eckel, RH, Jakicic, JM, Ard, JD, de Jesus, JM, Houston Miller, N, Hubbard, VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. (2014) 129:2. doi: 10.1161/01.CIR.0000437740.48606.D1
66. Jellinger, PS, Handelsman, Y, Rosenblit, PD, Bloomgarden, ZT, Fonseca, VA, Garber, AJ, et al. American association of clinical endocrinologists and American college of endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. (2017) 23:1–63. doi: 10.4158/EP171764.APPGL
67. Reiner, Ž, Catapano, AL, De Backer, G, Graham, I, Taskinen, MR, Wiklund, O, et al. ESC/EAS guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European atherosclerosis society (EAS). Eur Heart J. (2011) 32:1769–1818. doi: 10.1093/EURHEARTJ/EHR158
68. Millen, BE, Abrams, S, Adams-Campbell, L, Anderson, CAM, Brenna, JT, Campbell, WW, et al. The 2015 dietary guidelines advisory committee scientific report: development and major conclusions. Adv Nutr. (2016) 7:438–44. doi: 10.3945/AN.116.012120
Keywords: nutrition therapy, educational, diabetes mellitus, obesity, metabolic diseases, population health
Citation: Sevilla-González M, González-Ortiz A, Landa-Anell MV, Melgarejo-Hernández MA, Arias-Marroquín AT, Del Razo-Olvera FM, Román-Calleja BM, Monreal-Lugo AV, Martin-Vences AJ, Haua-Navarro K and Espinosa-Cuevas A (2025) Adaptation of the nutrition care process for metabolic diseases in the Mexican population. Front. Nutr. 12:1513747. doi: 10.3389/fnut.2025.1513747
Edited by:
Jeanette Mary Andrade, University of Florida, United StatesReviewed by:
Lubia Velázquez López, Instituto Mexicano del Seguro Social, MexicoCopyright © 2025 Sevilla-González, González-Ortiz, Landa-Anell, Melgarejo-Hernández, Arias-Marroquín, Del Razo-Olvera, Román-Calleja, Monreal-Lugo, Martin-Vences, Haua-Navarro and Espinosa-Cuevas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magdalena Sevilla-González, bXNldmlsbGFnb256YWxlekBtZ2guaGFydmFyZC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.