 Rosario Suárez1†‡
Rosario Suárez1†‡ Gabriela Cucalon2†‡
Gabriela Cucalon2†‡ Carolina Herrera2‡
Carolina Herrera2‡ Martha Montalvan3‡
Martha Montalvan3‡ Jestin Quiroz2*‡
Jestin Quiroz2*‡ Melissa Moreno2‡
Melissa Moreno2‡ Yoredy Sarmiento-Andrade1‡
Yoredy Sarmiento-Andrade1‡ Luis Cabañas-Alite4‡
Luis Cabañas-Alite4‡- 1School of Medicine, Universidad Técnica Particular del Loja, Loja, Ecuador
- 2Facultad Ciencias de la Vida, ESPOL Polytechnic University, ESPOL, Campus Gustavo Galindo, Guayaquil, Ecuador
- 3Universidad Espíritu Santo, Escuela de Medicina, Samborondón, Ecuador
- 4Faculty of Health Sciences, Miguel de Cervantes European University, Valladolid, Spain
Objective: This study aims to provide rapid and up-to-date evidence on the effectiveness of Health at Every Size (HAES) interventions compared to controls or other conventional approaches in individuals with overweight or obesity, with the goal of developing more effective and body-diverse respectful strategies.
Methods: A review of literature was carried out using the following databases: PubMed, Scopus, Embase, Web of Science, and SciELO. Research articles were selected based on predefined inclusion and exclusion criteria. Extracted data included study characteristics (design, setting, population demographics, sample size, intervention characteristics, study duration, and follow-up period) and health-related outcomes.
Results: The search yielded 324 articles, of which 20 articles met the inclusion and exclusion criteria. The majority of studies focused on lifestyle improvement, particularly in nutrition, body image, and relationships with food, utilizing a HAES approach. Additionally, other studies examined outcomes such as general well-being, body weight, body composition, cardiovascular risk, and changes in physical activity. Long-term results were particularly noted in studies incorporating physical activity interventions.
Conclusion: HAES interventions appear to be a feasible strategy for promoting overall health and wellness, regardless of body size or shape. However, further evaluation is needed to assess the sustainability of these changes and their long-term impact, as current evidence suggest a they may not be maintained over time.
1 Introduction
In both clinical medicine and public health, effective weight management is essential for improving overall health and preventing chronic illnesses (1). Traditional strategies for addressing obesity typically involve weight -reduction methods, such as calorie restriction and increased physical activity (2), which can be implemented through individual or group interventions (3). These methods can offer various health benefits. For example, one study demonstrated that a low-calorie DASH diet can reduce cardiovascular risk factors, as well as lower levels of trimethylamine N-oxide (TMAO), endotoxemia, and chronic inflammation (4). Despite increased attention on obesity treatments, its incidence continues to rise. Several traditional approaches, including diet, exercise, pharmacology, and surgery, have been studied extensively in efforts to address obesity (5).
However, lifestyle change efforts and obesity treatment programs have faced significant challenges, often yielding limited success in sustaining long-term results (4, 6). For instance, while lifestyle interventions have been effective for up to 2 years in individuals with a body mass index (BMI) of under 35 kg/m2, many participants experience weight regain, often returning to their pre-intervention weight within 3–5 years (4). Studies estimate that at least 50% of individuals with obesity will regain in the absence of sustained lifestyle changes. One factor influencing this trend is the brain-gut axis, which affects weight through the secretion of gastrointestinal hormones (7).
Furthermore, several organizations recommend intensive treatments, such as bariatric surgery, over drug therapy or lifestyle modifications for individuals with a BMI exceeding 40 kg/m2 or between 35 and 40 kg/m2 if obesity-related complications are present. However, uncertainties remain regarding the long-term efficacy of surgical procedures (4).
Given the challenges managing obesity, there has been a growing shift in perspective among professionals advocating for a departure from a weight-centric focus. This change has resulted in the rise of Health at Every Size (HAES) movement (8). HAES promotes a nontraditional approach to health and well-being by encouraging individuals to move away from dieting and focus instead on honoring hunger and fullness cues, following a varied, unrestricted diet, and engaging in joyful movement for health promotion—without prioritizing weight loss (9). HAES, which emerged in the early 2000s, also emphasizes mindful and/or intuitive eating, with a focus on body acceptance and overall health rather than weight loss. Key concepts associated with HAES include size acceptance, a non-diet approach, and health-focused behavior changes. The primary goal of HAES is also to reduce weight-based bias and the feelings of guilt often associated with eating and body image. Instead of emphasizing weight loss, HAES focuses on the overall health benefits of behavior changes related to eating and physical activity, highlighting size acceptance and non-dieting.
Studies have shown that implementing the HAES approach can lead to improvements in eating behaviors, such as a decrease in emotional eating, stronger reliance on internal hunger cues, intuitive eating, and improved body satisfaction (9).
Intuitive eating, which is aligned with HAES philosophy, involves responding to internal hunger and satiety cues rather than external signals (10, 11). Studies have found that body acceptance plays a crucial role in this process, with women who perceive body acceptance from others reporting higher self-esteem and better body image. Notably, BMI does not predict a positive body image, but the acceptance of one’s body by significant others and society does (12). Furthermore, greater body acceptance has been linked to enhanced interoceptive awareness, which, in turn, predicts improved body appreciation and success in practicing intuitive eating (12, 13). This approach is particularly important in reducing the risk of eating disorders among adolescents with obesity or weight gain (14). Therefore, this approach can help improve quality of life in the long-term.
Systematic reviews and meta-analyses have reported that HAES interventions can lead to improvements in both total and LDL cholesterol levels in cases of obesity-related malnutrition, as well as psychological benefits like lower depression, enhanced satiety, and a reduction in disordered eating behaviors (15). This review aims to evaluate the effects of HAES intervention on body composition and compare these outcomes with conventional obesity treatments.
Other preventive approaches include the “OPERA Project,” which integrates medical, athletic, gastronomic, and psychological fields to create health promotion interventions in countries with high rates of obesity and overweight (16).
On the other hand, intuitive eating has gained increasing recognition as an alternative to traditional weight-focused interventions. This approach emphasizes responding to internal cues of hunger and satiety, encouraging individuals to develop a more positive and mindful relationship with food (17). Recent studies have shown a strong association between intuitive eating and improved psychological outcomes, such as enhanced body image and reduced psychological distress, particularly in populations at risk of developing eating disorders (18) One study demonstrated that women practicing intuitive eating experienced better body image and reduced psychological distress, further supporting its potential as a viable intervention for promoting mental health and overall well-being, regardless of obesity history (19).
Research also emphasizes the interconnectedness between body acceptance, self-esteem, and intuitive eating. Higher levels of body acceptance predict greater success in intuitive eating, creating a positive feedback loop between body positivity and healthy eating behaviors (20). Moreover, individuals who perceive greater acceptance of their bodies—both from themselves and from others—tend to exhibit improved interoceptive awareness, enhanced body appreciation, and a higher likelihood of engaging in intuitive eating practices (21). These results highlight the significance of focusing on body image and self-perception in interventions aimed at promoting intuitive eating.
This review aimed to compare the effects of HAES-based interventions with those of conventional approaches in individuals with overweight or obesity.
2 Methodology
2.1 Literature research
This review was carried out according to the PRISMA 2020 statement guidelines (17). An comprehensive search was performed in PubMed, Scopus, Embase, Web of Science, and SciELO, identifying 324 articles published between January and May 2024. The search strategy was developed using the PICOS method, incorporating key terms such as “Health at Every Size” (HAES), “intuitive eating,” “non-weight-centrism,” “overweight,” “obesity,” and “fat mass.” The search syntax and controlled vocabulary for each database were adjusted accordingly, and the complete search strategy is provided in the Supplementary Table S1. This approach enabled a broad exploration of studies relevant to health and nutrition in populations with overweight and obesity.
2.2 Study eligibility, selection, and data extraction
For inclusion in the review, research articles were selected based on the following criteria: (1) BMI or Waist-Hip Index (WHI) indicative of obesity, (2) study participants over the age of 18, (3) articles written in English, Spanish, or German, (4) original research interventions primarily aimed at improving and reporting on the effects of body composition, health, or behavioral outcomes of individuals, using interventions based on the HAES (Health at Every Size) method. Eligible studies included randomized controlled trials (RCTs), quasi-experimental interventions, pre-post studies, and feasibility trials, and (5) with a publication date between 2013 and 2023.
Exclusion criteria were as follows: (1) studies that did not address the primary objective of the review, (2) articles focusing solely on hospitalized patients, (3) duplicate studies already included in another database, (4) studies using pharmacological or surgical interventions, (5) systematic reviews, narratives, meta-analyses, and protocols, and (6) interventions focused on specific diseases or health behaviors not related to body weight.
From an initial pool of 324 articles, 131 duplicates were identified and removed, along with five entries that were books and did not meet the inclusion criteria for original research. This left 188 articles for further screening. Following an initial screening of titles and abstracts, 97 articles were excluded due to study type (e.g., reviews, editorials, protocols) or lack of originality. This left 91 references for further detailed screening. During this phase, 69 articles were excluded for failing to meet the inclusion criteria: five due to involving participants under 18 years old, eight due to focusing on non-obese populations, 32 because of unsuitable study designs, and 26 because their objectives differed from the review’s scope.
The final selection of articles was carried out through a comprehensive review process conducted by three independent reviewers. All selection discrepancies were addressed through discussion and agreement. Throughout the review, Zotero software was used for reference management. Data extraction was conducted by two reviewers and verified by all authors to ensure consistency and accuracy. The data extracted included study design, population characteristics, intervention details, and health outcomes.
3 Results
Twenty articles that satisfied the inclusion criteria were selected for this report and are shown in Table 1. The screening process is illustrated in Figure 1, which provides a flow diagram of the search strategy.
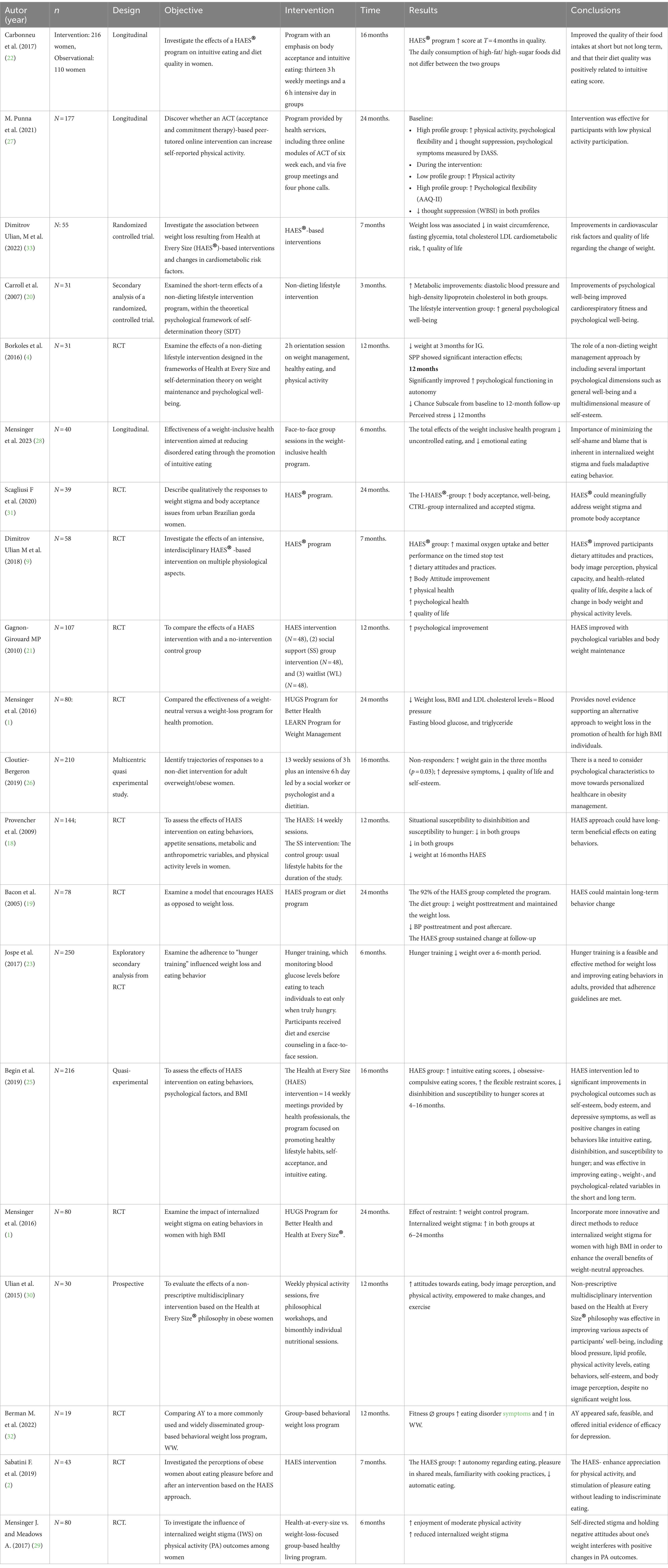
Table 1. Results summary.
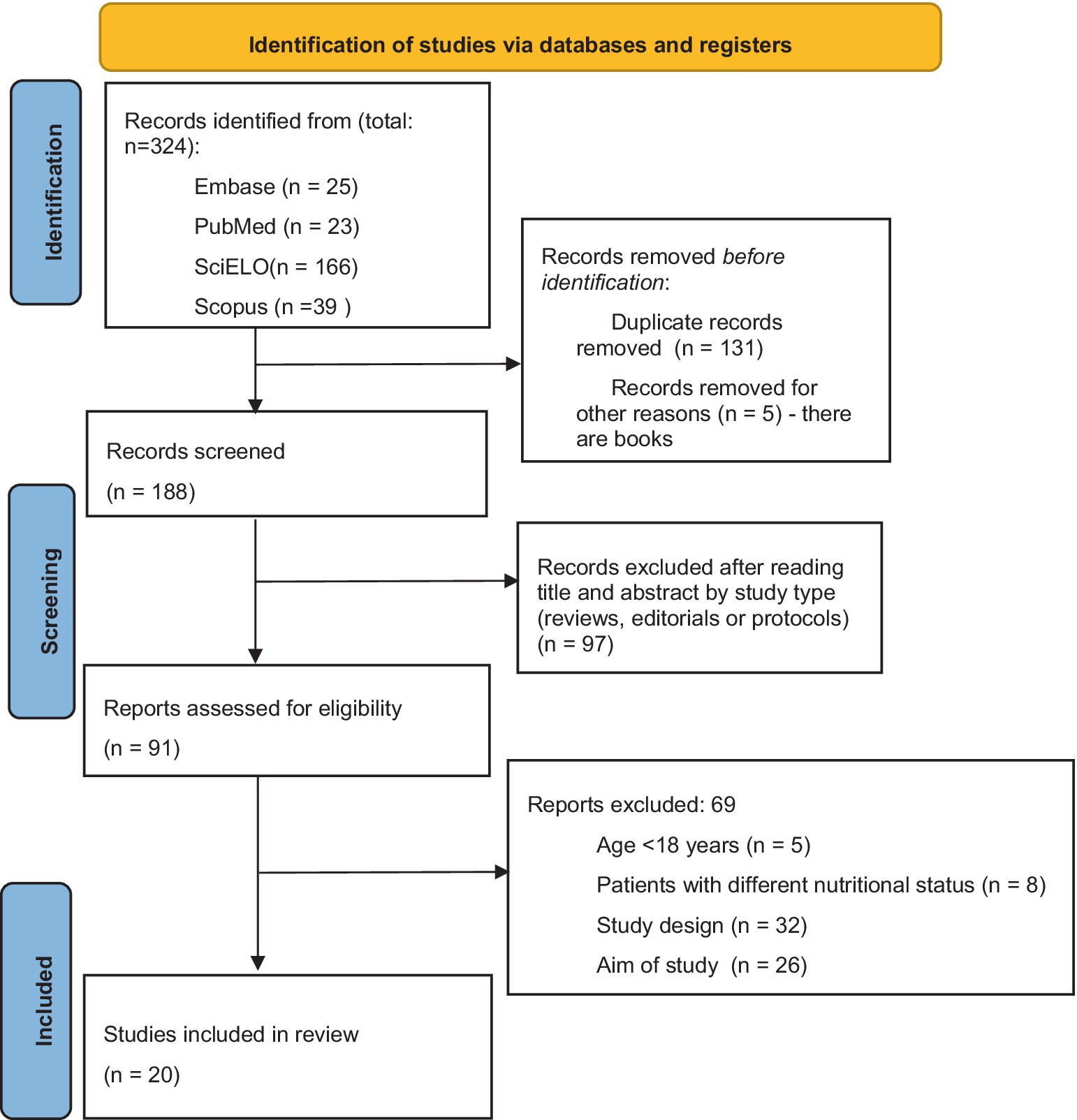
Figure 1. Study data collection: authors’ own creation.
Characteristics of included studies are summarized in Table 1.
Of the final articles included, twelve described programs focused on lifestyle improvements, specifically related to nutrition, body image, or the relationship with food, all framed within a HAES perspective (1, 18–28). Eight studies adopted the same perspective or intervention but included physical activity (2, 4, 9, 29–33). In addition, eight studies investigated overall well-being (1, 2, 4, 9, 20, 21, 31, 33), ten focused on body weight, body composition, and body image (4, 9, 18–21, 29, 33), five examined cardiovascular risk impacts (1, 9, 19, 26, 33), two explored changes in eating behaviors (28, 30) and three analyzed physical activity outcomes (27, 29, 30).
Furthermore, eight studies evaluated the long-term effects of lifestyle changes in participants undergoing these interventions (1, 4, 18, 19, 21, 22, 25, 26).
These findings will be analyzed in detail in the following section, comparing them to similar studies for further insights.
4 Discussion
This review aimed to explore the feasibility and effectiveness of HAES interventions for individuals with obesity, focusing on their impact on various health-related outcomes. We reviewed 20 articles; while preliminary findings indicate promising short-term outcomes across various health domains, our analysis focuses on long-term effects.
4.1 Effects on overall well-being
Eight studies evaluated the effects of HAES on quality of life or overall well-being using different tools such as validated instruments, focus groups, and interviews. One consistent finding across these studies is that strategies aimed at enhancing overall well-being can positively affect health outcomes, irrespective of significant weight loss.
In the study by Ulian et al. (9), both the intervention group (I-HAES®) and the control group (CTRL) showed significant improvements in quality-of-life parameters. The I-HAES® group demonstrated increases in the “physical” (p = 0.05), “psychological” (p = 0.03), and “quality of life” (p = 0.02) domains, while the control group improved in the “psychological health” (p = 0.04) and “perception of quality of life” (p = 0.01) domains. These results were achieved as participants worked to change their routines.
In a follow-up study conducted in 2022 with the same population, weight loss was associated with improved quality of life (β = −1.05, p = 0.007), as measured by the World Health Organization Quality of Life—BREF questionnaire (WHOQOL-BREF). This intervention primarily focused on nutritional counseling without a diet prescription (33).
The results suggest that the positive changes in body image observed in the traditional control group were expanded in the interdisciplinary intervention group, which likely fostered an empathetic atmosphere, increased self-esteem, and improvements in body attitudes and perception, all of which contributed to an enhanced quality of life, which might be a result of these improvements. In contrast, Brown et al. (34), highlighted the negative effects of stigma and lack of support in primary care settings on access to healthcare services for patients with obesity, emphasizing the importance of including nutritional counseling in obesity treatment programs.
Scagliusi et al. (31), did not present comparative data due to their study design, which did not account for time effects versus intervention impacts. However, Sabatini et al. using a case–control design and focus groups, found that both intervention groups reported improvements in eating pleasure, a decrease in guilt around eating, and enhanced experiences of commensality. The I-HAES group also reported reductions in emotional eating, greater confidence in food choices, improved cooking skills, and less mindless eating. These studies underscore the need for standardized tools to measure quality-of-life outcomes.
Carroll et al. (20) reported significant improvements in psychological well-being compared to the control group (test for interaction, p = 0.0005) in absence of significant changes in body mass or composition. Similarly, Borkoles et al. (4) assessed well-being using the General Well-Being Schedule (GWB) and found significant improvements across all subscales from baseline to 12-month follow-up, despite the absence of significant weight loss. Similarly, The Healthy Weight in Lesbian and Bisexual Women study (n = 266 LB women age ≥ 40) conducted by Ingraham (35), assessed the effects of mindfulness interventions on health outcomes. Although weight loss was not a primary outcome, increased mindfulness was associated with significant improvements in mental health and quality of life.
Gagnon-Girouard et al. (36) observed no significant short-term changes in well-being but reported that HAES interventions could lead to sustained long-term improvements in mood, self-esteem, quality of life, body dissatisfaction related to appearance, body dissatisfaction—weight, body dissatisfaction—attribution, binge eating, and body weight. These improvements are directly targeted by the HAES intervention, suggesting that achieving self-acceptance, enhanced quality of life, and positive body image may require a longer duration to manifest.
Finally, Mensinger et al. (24) found sustained improvements in psychological well-being, such as enhanced quality of life and self-esteem, over 24 months, though there were not significant differences between the intervention and control groups. Bruce and Ricciardelli (37) reviewed the growing body of literature supporting a positive correlation between intuitive eating and emotional well-being in women. Similarly, Tribole and Resch, in their book on intuitive eating, they associated restrictive eating behaviors with an increase in depressive symptoms and poor emotional regulation (38).
4.2 Effects on body weight, body composition and body image
Several authors have reported the impact of the HAES intervention on body weight after. Ulian et al. (33) noted that after 7 months of intervention, weight loss was significantly related to improvements in waist circumference (β = 0.83, p < 0.001). Similarly, Borkoles et al. (4) also found a modest weight reduction after 3 months of lifestyle intervention.
Other authors reported that improvements in body esteem during the intervention phase suggested the likelihood of maintaining body weight during follow-up phase (p = 0.011) (21). Mensinger et al. (1) observed reductions in weight, BMI, and LDL cholesterol from baseline to post-intervention (p = 0.003), with greater reductions in the weight-neutral program. Provencher et al. (18) found that 63.4% of women in the HAES group maintained a lower weight at 16 months compared to baseline (mean BMI 30.10.4 at baseline vs. 29.50.5 at 16 months; 2% difference from the initial weight).
In contrast, Bacon et al. (39) reported significant weight loss in the diet group post-treatment (−5.2 kg ± 7.3 from baseline), with participants maintaining a 5.2% reduction in weight after follow-up (−5.3 kg ± 6.7 from baseline). However, most studies noted weight maintenance or even weight gain over time (1, 4, 19, 33). Additionally, some authors using HAES methods reported no significant changes in body weight (9, 20, 23, 26, 29).
Despite these findings, several reviews highlight that HAES and other non-weight-centric interventions lead to significant and sustained changes in dietary behaviors and practices (up to 2 years), although these changes are not reflected in anthropometric measurements (9, 40). These results suggest that weight is not the sole indicator of overall well-being.
4.3 Impact on cardiovascular risk
Analyzing the results of the aforementioned studies reveals a variety of findings concerning the HAES approach and its impact on cardiovascular health. Ulian et al. (33) found that weight loss was associated with significant improvements in waist circumference (B = 0.83; p < 0.001), fasting blood glucose (B = 0.45; p = 0.036), total cholesterol (B = 1.48; p = 0.024), LDL (B = 1.33; p = 0.012), and pooled cardiometabolic risk (B = 0.18; p = 0.006). In contrast, Mensinger et al. (1) observed no significant changes in systolic or diastolic blood pressure, fasting blood glucose, or triglyceride levels over time. Cloutier-Bergeron et al. (26) identified significant differences when comparing non-responders to other groups, finding higher rates of cardiovascular disease (x2 (1, N = 205) = 6.232, p = 0.013, n2 = 0.03) and dyslipidemia (x2 (1, N = 199) = 5.471, p = 0.019, n2 = 0.028). Bacon et al. (19) reported a significant decrease in systolic blood pressure but no significant changes in diastolic blood pressure. In addition, Ulian et al. (9) showed that although fat-free mass (FFM) increased and waist and hip circumferences slightly decreased, these changes were not statistically significant.
Recent studies support the complexity of the relationship between the HAES approach and cardiovascular risk. For example, Schaefer and Magnuson (41) revealed significant improvements in health-related quality of life (B = 0.72; p = 0.021) and a reduction in anxiety (B = −1.25; p = 0.038) in individuals who adopted a HAES approach. Similarly, Bacon and Aphramor (42) found a significant decrease in perceived stress (B = −0.56; p = 0.017) and improved body image in participants following a health-focused approach rather than a weight-loss-centered one.
Gagnon-Girouard et al. (21) reported that the HAES approach improved self-esteem (B = 0.72; p = 0.021) and reduced depressive symptoms (B = −1.25; p = 0.038) in women with overweight or obesity. Mensinger et al. (1) also found significant improvements in physical activity (B = 0.56; p = 0.017) and life satisfaction in participants following the HAES approach.
These results emphasize the importance of considering comprehensive approaches, such as HAES, to promote cardiovascular health and overall well-being. They highlight the need to personalize health strategies to address cardiovascular risk effectively in diverse populations, focusing on improving health and quality of life rather than just weight loss.
4.4 Impact on eating behaviors
Mensinger et al. (28), provide significant statistical supporting the importance of addressing maladaptive eating patterns in women with high BMI. Their study demonstrated a 25% decrease in emotional eating scores (b = −1.79, SE = 0.34, p < 0.0001), and a 20% reduction in uncontrolled eating behaviors (b = −3.76, SE = 0.64, p < 0.0001), following 6 months of participation in a HAES-based program, showing a statistically significant improvement in dietary patterns (p < 0.05) (28).
Moreover, each reduction in weight stigma was associated with a corresponding 0.75-point increase in intuitive eating behavior score (r = −0.60, p < 0.01), highlighting that reducing weight stigma is crucial for fostering a healthier relationship with food, an essential aspect of the HAES intervention.
Ulian et al. (30) also demonstrated the impact of the HAES approach by showing a 13% decrease in body fat mass, an 11.1% reduction in body fat percentage, a 3.6 kg reduction in weight, and a 3.2 -point reduction in BMI, all of which were statistically significant. Additionally, binge eating behaviors improved; initially, 57.1% of participants exhibited moderate binge eating, but by the end of the study, 78.6% exhibited no binge eating behaviors, while only 14.3% continued to display moderate levels of such behaviors.
Both studies highlight the importance of comprehensive approaches that address both physical and psychological aspects of health during interventions. Mensinger et al. (28) provide evidence of reduced uncontrolled and emotional eating, while Ulian et al. (30) show reductions in binge eating. These findings suggest that reducing weight stigma and promoting intuitive eating can lead to improved health outcomes and greater body acceptance.
4.5 Effects on physical activity
Punna et al. (27) investigated the effects of an online peer-mentored intervention based on acceptance and commitment therapy. The study found that participants with low baseline physical activity levels significantly increased their participation in physical activity, highlighting the importance of personalizing interventions to maximize effectiveness.
Ulian et al. (9) also reported significant improvements in body composition following an exercise program, nutritional counseling, and philosophical workshops. After the intervention, there were significant reductions in weight, BMI, body fat mass, and fat mass percentage (−3.6, −3.2%, −13.0%, and −11.1%, respectively; p ≤ 0.05), all of which positively impacted cardiovascular and metabolic health. Similar findings were reported by Schaefer and Magnuson (41), who found that participants adopting a HAES approach, including physical activity, experienced significant improvements in health-related quality of life (B = 0.72, p = 0.021) and reduced anxiety (B = −1.25, p = 0.038). Bacon and Aphramor (42) similarly found that combining physical activity with nutrition education led to significant reductions in perceived stress (B = −0.56; p = 0.017) and improvements in body image. Gagnon-Girouard et al. (21) also showed that health promotion strategies incorporating physical activity increased self-esteem (B = 0.72; p = 0.021) and reduced depressive symptoms (B = −1.25; p = 0.038) in women with overweight or obesity.
These results highlight the importance of adopting a holistic approach that integrates physical activity with other wellness factors to foster positive changes in health and quality of life. More recently, Mensinger et al. (1) demonstrated that a “weight neutral” approach, which emphasizes physical activity and overall health, was associated with greater body satisfaction (B = 0.72; p = 0.021) and a reduction in eating disorder symptoms (B = −1.25; p = 0.038) in women with overweight or obesity. These findings further support the value of prioritizing health and wellness over weight loss.
Schaefer and Magnuson (41) supported these findings, reporting significant improvements in self-efficacy for exercise (β = 0.72; p = 0.021) and increased physical activity adherence (β = −1.25; p = 0.038). These results underscore the importance of fostering self-efficacy and intrinsic motivation to promote the adoption and long-term maintenance of an active lifestyle.
In contrast, Mensinger and Meadows (29) observed that the effect of internalized weight stigma on moderate-intensity physical activity was not statistically significant (b = 0.22, SE = 0.11, 95% CI, t(132) = 1.89, p = 0.061). However, they noted a significant increase in moderate-intensity physical activity over time (b = 0.80, SE = 0.14, 95% CI [0.51, 1.08], t(71) = 5.54, p < 0.001), emphasizing the importance of considering psychological factors such as weight stigma to promote long-term physical activity adherence.
Bacon et al. (19) further revealed that the HAES approach, which combines physical activity and nutrition education, significantly improved diet quality (B = 0.72; p = 0.021) and reduced cardiometabolic risk (B = −1.25; p = 0.038) in adults with overweight or obesity. These findings highlight the value of adopting a holistic approach to promote cardiovascular and metabolic health.
4.6 Results at long term
A very relevant question regarding health interventions, especially those addressing cardiovascular, metabolic, or nutritional health, is whether the results are maintained in the long term. In other words, do individuals continue adhering to the changes implemented during the intervention? This question has been extensively explored in the articles included in this review, and the findings are discussed below.
The average duration of the interventions analyzed ranges from 4 to 6 months, while long-term analysis typically take place 12 months after the intervention’s completion (4, 18, 22, 25, 26, 36), or in some cases, up to 24 months (1, 19).
Some interventions showed that changes in eating behaviors, dietary quality, or weight were not maintained over the long term (18, 24), or that the differences between control and intervention groups were no longer significant after the intervention period (1, 4, 18). However, results in areas like autonomy and other psychological functions remain significant (p < 0.001) (4), and improvements in depression symptoms were observed (p < 0.05) (25, 26). Additionally, changes in individual’s relationships with food, such as reduced compulsive eating (p < 0.0001), were sustained (25). In contrast, studies focusing on quality-of-life improvements found that these effects were not maintained long-term (30). Cloutier-Bergeron et al. (26) also highlighted the existence of a group classified as “non-responders,” who exhibited worse psychological function, less adaptation to changes in eating behavior, and higher rates of clinical depression. These individuals struggled to adjust to the behavioral changes introduced during the intervention.
While interventions based on this methodology can have a significant effect in the short-term impact, they seem to be less effective in the long term. Research evaluating HAES interventions, which emphasize healthy behaviors, size acceptance, and non-dieting approaches, has demonstrated health benefits regardless of weight loss. Nevertheless, as mentioned in previous sections and corroborated by other literature from the last twenty years (33, 43, 44), the long-term effectiveness of these interventions remains in question. Available data and findings from other authors suggest the long-term (>12 months) may not be sustained (45, 46). More long-term data are needed to support the use of these interventions.
It is important to acknowledge both the strengths and limitations of this review. One limitation is that some studies were carried out by the same research teams, meaning more studies from various regions are needed to strengthen the evidence. While interventions have been carried out in Canada, Brazil, the UK and the USA, which provides some diversity, more information is needed on the application of HAES across different cultural contexts. The increasing number of participants in these studies makes the data more robust, but it should also be noted that the majority of these studies have focused exclusively on women. This gender bias indicates that more research is needed on the effects of these interventions on men. Furthermore, few studies evaluate body composition or weight measurements, aligning with HAES principles of weight-neutrality. Nonetheless, this approach complicates comparisons between clinical outcomes.
Future research should include men and older populations, have longer follow-ups (>12 months), extend the intervention duration (>6 months), and involve larger population groups. Additionally, more detailed data on food intake is needed to understand what nutritional changes lead to improved health outcomes and, where applicable, reduced weight or body fatness in intervention groups. Factors such as energy-balance, food intake, and overall well-being, should be more thoroughly examined.
In conclusion, available data suggest that HAES interventions have positive effects on body composition, cardiovascular health, and psychological factors related to food and well-being. However, these long-term effects (particularly in studies lasting a minimum of 2 years) require further verification, as current evidence suggests that some benefits may not be sustained. More extensive and longer-term studies are needed to clarify these findings.
Author contributions
RS: Writing – review & editing, Writing – original draft. GC: Writing – review & editing, Writing – original draft. CH: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. MaM: Writing – review & editing, Writing – original draft. JQ: Writing – review & editing, Writing – original draft, Software, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. MM: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. YS-A: Writing – review & editing, Writing – original draft. LC-A: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research received funding from the Universidad Técnica Particular de Loja, Ecuador.
Acknowledgments
Many thanks to all authors for their contribution to this Research Topic.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1482854/full#supplementary-material
References
1. Mensinger, JL, Calogero, RM, Stranges, S, and Tylka, TL. A weight-neutral versus weight-loss approach for health promotion in women with high BMI: a randomized-controlled trial. Appetite. (2016) 105:364–74. doi: 10.1016/j.appet.2016.06.006
2. Sabatini, F, Ulian, MD, Perez, I, Pinto, AJ, Vessoni, A, Aburad, L, et al. Eating pleasure in a sample of obese Brazilian women: a qualitative report of an interdisciplinary intervention based on the health at every size approach. J Acad Nutr Diet. (2019) 119:1470–82. doi: 10.1016/j.jand.2019.01.006
3. Canuto, R, Garcez, A, Souza, R, Kac, G, and Olinto, M. Nutritional intervention strategies for the management of overweight and obesity in primary health care: a systematic review with meta-analysis. Obes Rev. (2020) 22:e13143. doi: 10.1111/obr.13143
4. Borkoles, E, Carroll, S, Clough, P, and Polman, RCJ. Effect of a non-dieting lifestyle randomised control trial on psychological well-being and weight management in morbidly obese pre-menopausal women. Maturitas. (2016) 83:51–8. doi: 10.1016/j.maturitas.2015.09.010
5. Diao, Z, Molludi, J, Fateh, HL, and Moradi, S. Comparison of the low-calorie DASH diet and a low-calorie diet on serum TMAO concentrations and gut microbiota composition of adults with overweight/obesity: a randomized control trial. Int J Food Sci Nutr. (2023) 75:207–20. doi: 10.1080/09637486.2023.2294685
6. Kurtgil, S, and Pekcan, AG. Determination of breakfast habits, food pattern and quality among adults. Mediterr J Nutr Metab. (2023) 16:281–91. doi: 10.3233/MNM-230038
7. Barrea, L, Salzano, C, Pugliese, G, Laudisio, D, Frias-Toral, E, Savastano, S, et al. The challenge of weight loss maintenance in obesity: a review of the evidence on the best strategies available. Int J Food Sci Nutr. (2022) 73:1030–46. doi: 10.1080/09637486.2022.2130186
8. Hoare, JK, Lister, NB, Garnett, SP, Baur, LA, and Jebeile, H. Weight-neutral interventions in young people with high body mass index: a systematic review. Nutr Diet. (2023) 80:8–20. doi: 10.1111/1747-0080.12729
9. Ulian, MD, Aburad, L, da Silva Oliveira, MS, Poppe, ACM, Sabatini, F, Perez, I, et al. Effects of health at every size® interventions on health-related outcomes of people with overweight and obesity: a systematic review. Obes Rev. (2018) 19:1659–66. doi: 10.1111/obr.12749
10. Raffoul, A, and Williams, L. Integrating health at every size principles into adolescent care. Curr Opin Pediatr. (2021) 33:361–7. doi: 10.1097/MOP.0000000000001023
11. Miller, WC . Fitness and fatness in relation to health: implications for a paradigm shift. J Soc Issues. (1999) 55:207–19. doi: 10.1111/0022-4537.00113
12. Augustus-Horvath, CL, and Tylka, TL. The acceptance model of intuitive eating: a comparison of women in emerging adulthood, early adulthood, and middle adulthood. J Couns Psychol. (2011) 58:110–25. doi: 10.1037/a0022129
13. Avalos, LC, and Tylka, TL. Exploring a model of intuitive eating with college women. J Couns Psychol. (2006) 53:486–97. doi: 10.1037/0022-0167.53.4.486
14. Tekin, T, and Bağlam, N. Body weight gain in adolescents can increase the risk of developing an eating disorder. Med J Nutrition Metab. (2023) 16:213–22. doi: 10.3233/MNM-230033
15. Dugmore, JA, Winten, CG, Niven, HE, and Bauer, J. Effects of weight-neutral approaches compared with traditional weight-loss approaches on behavioral, physical, and psychological health outcomes: a systematic review and meta-analysis. Nutr Rev. (2020) 78:39–55. doi: 10.1093/nutrit/nuz020
16. Muscogiuri, G, Barrea, L, Laudisio, D, Pugliese, G, Aprano, S, Framondi, L, et al. The Opera prevention project. Int J Food Sci Nutr. (2020) 72:1–3. doi: 10.1080/09637486.2020.1765152
17. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
18. Provencher, V, Bégin, C, Tremblay, A, Mongeau, L, Corneau, L, Dodin, S, et al. Health-at-every-size and eating behaviors: 1-year follow-up results of a size acceptance intervention. J Am Diet Assoc. (2009) 109:1854–61. doi: 10.1016/j.jada.2009.08.017
19. Bacon, L, Stern, JS, Loan, MDV, and Keim, NL. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J Am Diet Assoc. (2005) 105:929–36. doi: 10.1016/j.jada.2005.03.011
20. Carroll, S, Borkoles, E, and Polman, R. Short-term effects of a non-dieting lifestyle intervention program on weight management, fitness, metabolic risk, and psychological wellbeing in obese premenopausal females with the metabolic syndrome. Appl Physiol Nutr Metab. (2007) 32:125–42. doi: 10.1139/h06-093
21. Gagnon-Girouard, MP, Bégin, C, Provencher, V, Tremblay, A, Mongeau, L, Boivin, S, et al. Psychological impact of a “health-at-every-size” intervention on weight-preoccupied overweight/obese women. J Obes. (2010) 2010:928097:1–12. doi: 10.1155/2010/928097
22. Carbonneau, E, Bégin, C, Lemieux, S, Mongeau, L, Paquette, MC, Turcotte, M, et al. A health at every size intervention improves intuitive eating and diet quality in Canadian women. Clin Nutr. (2017) 36:747–54. doi: 10.1016/j.clnu.2016.06.008
23. Jospe, MR, Taylor, RW, Athens, J, Roy, M, and Brown, RC. Adherence to hunger training over 6 months and the effect on weight and eating behaviour: secondary analysis of a randomised controlled trial. Nutrients. (2017) 9:1260. doi: 10.3390/nu9111260
24. Mensinger, JL, Tylka, TL, and Calamari, ME. Mechanisms underlying weight status and healthcare avoidance in women: a study of weight stigma, body-related shame and guilt, and healthcare stress. Body Image. (2018) 25:139–47. doi: 10.1016/j.bodyim.2018.03.001
25. Begin, C, Carbonneau, E, Gagnon-Girouard, MP, Mongeau, L, Paquette, MC, Turcotte, M, et al. Eating-related and psychological outcomes of health at every size intervention in health and social services centers across the province of Quebec. Am J Health Promot. (2019) 33:248–58. doi: 10.1177/0890117118786326
26. Cloutier-Bergeron, A, Provencher, V, Mongeau, L, Paquette, MC, Carbonneau, É, Turcotte, M, et al. Does HealthAtEvery size® fit all? A group-based trajectory modeling of a non-diet intervention. Appetite. (2019) 143:104403. doi: 10.1016/j.appet.2019.104403
27. Punna, M, Lappalainen, R, Kettunen, T, Lappalainen, P, Muotka, J, Kaipainen, K, et al. Can peer-tutored psychological flexibility training facilitate physical activity among adults with overweight? J Context Behav Sci. (2021) 21:1–11. doi: 10.1016/j.jcbs.2021.04.007
28. Mensinger, JL, Shepherd, BF, Schapiro, S, Aware, Y, Brochu, PM, Calogero, RM, et al. Mediating effects of a weight-inclusive health promotion program on maladaptive eating in women with high body mass index. Eat Behav. (2023) 49:101730. doi: 10.1016/j.eatbeh.2023.101730
29. Mensinger, JL, and Meadows, A. Internalized weight stigma mediates and moderates physical activity outcomes during a healthy living program for women with high body mass index. Psychol Sport Exerc. (2017) 30:64–72. doi: 10.1016/j.psychsport.2017.01.010
30. Ulian, MD, Benatti, FB, de Campos-Ferraz, PL, Roble, OJ, Unsain, RF, de Morais, SP, et al. The effects of a “health at every size”-based approach in obese women: a pilot-trial of the “health and wellness in obesity” study. Front Nutr. (2015) 2:34. doi: 10.3389/fnut.2015.00034
31. Scagliusi, FB, Ulian, MD, Gualano, B, Roble, OJ, Unsain, RF, Carriero, MR, et al. Before i saw a gas canister, now i see a person post obesity-intervention body acceptance and responses to weight stigma among urban brazilian gorda women. Hum Organ. (2020) 79:176–91. doi: 10.17730/1938-3525-79.3.176
32. Berman, MI, Park, J, Kragenbrink, ME, and Hegel, MT. Accept yourself! A pilot randomized controlled trial of a self-acceptance-based treatment for large-bodied women with depression. Behav Ther. (2022) 53:913–26. doi: 10.1016/j.beth.2022.03.002
33. Dimitrov Ulian, M, Pinto, AJ, de Morais Sato, P, Benatti, FB, Lopes de Campos-Ferraz, P, Coelho, D, et al. Health at every size®-based interventions may improve Cardiometabolic risk and quality of life even in the absence of weight loss: an ancillary, exploratory analysis of the health and wellness in obesity study. Front Nutr. (2022) 9:598920. doi: 10.3389/fnut.2022.598920
34. Brown, I, Thompson, J, Tod, A, and Jones, G. Primary care support for tackling obesity: a qualitative study of the perceptions of obese patients. Br J Gen Pract. (2006) 56:666–72.
35. Ingraham, N, Eliason, MJ, Garbers, S, Harbatkin, D, Minnis, AM, McElroy, JA, et al. Effects of mindfulness interventions on health outcomes in older lesbian/bisexual women. Womens Health Issues. (2016) 26:S53–62. doi: 10.1016/j.whi.2016.04.002
36. Bruce, LJ, and Ricciardelli, LA. A systematic review of the psychosocial correlates of intuitive eating among adult women. Appetite. (2016) 96:454–72. doi: 10.1016/j.appet.2015.10.012
38. Bacon, L . Getting over the obesity paradigm: health solutions that don’t backfire. Obes Res Clin Pract. (2013) 7:e56–7. doi: 10.1186/1475-2891-10-9
39. Lema, R . Intervenciones no pesocentristas y principios de salud en todas las tallas en el abordaje del sobrepeso y la obesidad. Rev Nutr Clin Metab. (2022) 5:47–57. doi: 10.35454/rncm.v5n3.384
40. Schaefer, JT, and Magnuson, AB. A review of interventions that promote eating by internal cues. J Acad Nutr Diet. (2014) 114:734–60. doi: 10.1016/j.jand.2013.12.024
41. Bacon, L, and Aphramor, L. Weight science: evaluating the evidence for a paradigm shift. Nutr J. (2011) 10:9. doi: 10.1186/1475-2891-10-9
42. Bacon, L, Keim, NL, Van Loan, MD, Derricote, M, Gale, B, Kazaks, A, et al. Evaluating a “non-diet” wellness intervention for improvement of metabolic fitness, psychological well-being and eating and activity behaviors. Int J Obes Relat Metab Disord. (2002) 26:854–65. doi: 10.1038/sj.ijo.0802012
43. Cloutier-Bergeron, A, Samson, A, Provencher, V, Mongeau, L, Paquette, MC, Turcotte, M, et al. Health at every size intervention® under real-world conditions: the rights and wrongs of program implementation. Health Psychol Behav Med. (2022) 10:935–55. doi: 10.1080/21642850.2022.2128357
44. Babbott, KM, Cavadino, A, Brenton-Peters, J, Consedine, NS, and Roberts, M. Outcomes of intuitive eating interventions: a systematic review and meta-analysis. Eat Disord. (2023) 31:33–63. doi: 10.1080/10640266.2022.2030124
45. Burnette, CB, and Mazzeo, SE. An uncontrolled pilot feasibility trial of an intuitive eating intervention for college women with disordered eating delivered through group and guided self-help modalities. Int J Eat Disord. (2020) 53:1405–17. doi: 10.1002/eat.23319
Keywords: HAES, nutritional intervention, weight-neutral approach, eating behavior, lifestyle intervention
Citation: Suárez R, Cucalon G, Herrera C, Montalvan M, Quiroz J, Moreno M, Sarmiento-Andrade Y and Cabañas-Alite L (2024) Effects of health at every size based interventions on health-related outcomes and body mass, in a short and a long term. Front. Nutr. 11:1482854. doi: 10.3389/fnut.2024.1482854
Edited by:
Florencia Ceriani, Universidad de la República, UruguayReviewed by:
Andrea Gomez Carrillo, Autonomous University of Baja California, MexicoVictoria Abril-Ulloa, University of Cuenca, Ecuador
Copyright © 2024 Suárez, Cucalon, Herrera, Montalvan, Quiroz, Moreno, Sarmiento-Andrade and Cabañas-Alite. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: J. Quiroz, amFxdWlyb3pAZXNwb2wuZWR1LmVj
†These authors have contributed equally to this work and share first authorship
‡ORCID: Rosario Suárez, https://orcid.org/0000-0003-0419-030X
G. Cucalon, https://orcid.org/0000-0002-6900-5649
C. Herrera, https://orcid.org/0009-0007-9415-6899
Martha Montalvan, https://orcid.org/0000-0001-9550-2772
J. Quiroz, https://orcid.org/0000-0001-6077-564X
M. Moreno, https://orcid.org/0009-0005-6550-5573
Yoredy Sarmiento-Andrade, https://orcid.org/0000-0002-4343-7793
L. Cabañas-Alite, https://orcid.org/0000-0003-3522-5632