 Cecilia Arteaga-Pazmiño1*
Cecilia Arteaga-Pazmiño1* Diana Fonseca-Pérez2Manuel Balladares Mazzini3Javier Galvez-Celi1Janet Emén Sánchez3Ludwig Álvarez-Córdova2,4
Diana Fonseca-Pérez2Manuel Balladares Mazzini3Javier Galvez-Celi1Janet Emén Sánchez3Ludwig Álvarez-Córdova2,4- 1Carrera de Nutrición y Dietética, Facultad de Ciencias Médicas, Universidad de Guayaquil, Guayaquil, Ecuador
- 2Carrera de Nutrición y Dietética, Facultad de Ciencias de la Salud, Universidad Católica de Santiago de Guayaquil, Guayaquil, Ecuador
- 3Carrera de Medicina, Facultad de Ciencias Médicas, Universidad de Guayaquil, Guayaquil, Ecuador
- 4Maestría de Nutrición y Dietética, Facultad de Ciencias de la Salud, Universidad de Las Américas (UDLA), Quito, Ecuador
Background: Dynapenic obesity (DO) is the coexistence of excess adipose tissue/body weight and low muscle strength. This condition is associated with an increased risk of suffering from various chronic diseases and physical deterioration in older people.
Aim: To analyze the association between DO phenotypes and physical performance in middle-aged women living in the community.
Methods: This cross-sectional study was conducted on middle-aged and older women (≥50 years) residing in Guayaquil, Ecuador. Dynapenia was diagnosticated by a handgrip strength (HGS) < 16 kg; obesity was determined based on body mass index (BMI) ≥ 30 kg/m2. Participants were categorized into four groups based on their dynapenia and obesity status: non-dynapenic/non-obesity (ND/NO), obesity/non-dynapenic (O/ND), dynapenic/non-obesity (D/NO) and dynapenic/obesity (D/O). Physical performance was assessed by the Short Physical Performance Battery (SPPB).
Results: A total of 171 women were assessed. The median (IQR) age of the sample was 72.0 (17.0) years. Obesity and dynapenia were 35% (n = 60) and 57.8% (n = 99) of the participants, respectively. The prevalence of ND/NO was 25.1% (n = 43), O/ND 17% (n = 29), D/NO 39.8% (n = 68) and DO 18.1% (n = 31). The mean SPPB total score was 6.5 ± 3.2. Participants of D/NO and DO groups presented significantly lower mean SPPB scores (p < 0.001) compared to those of NO/ND and O/ND groups.
Conclusion: Women with DO and D/NO exhibited significantly lower SPPB scores, indicating poorer physical performance. These findings emphasize the importance of incorporating a comprehensive assessment of muscle strength and obesity in middle-aged and older women.
1 Introduction
Obesity is a multifactorial, chronic, progressive disease associated with adverse health outcomes throughout the life course (1, 2). In 2022, an estimated 374 million women were identified with obesity (3), however, data on the prevalence of obesity specifically in women aged 50 and older is lacking.
In middle-aged women, several factors contribute to changes in body composition. These include age-related decline in estrogen levels around menopause (4, 5) and its impact on metabolism and related diseases (6, 7), lifestyle factors (8–10) such as diet (11), anabolic resistance associated with aging (12), among others. As a result, decreasing of muscle mass and strength, which begin to decrease around 30 and accelerate after 40 (13, 14), infiltration of fat within muscle and increasing prevalence of dynapenia (weakness) (15), sarcopenia (weakness and muscle loss), and obesity are common in this aged group (16).
Moreover, a wide range of alterations, including altered immune function, increased systemic inflammation, accumulated intracellular macromolecules, decreased genomic integrity, and changes in tissue and body composition (17), are common to both obesity and aging (18, 19).
In the last few years, the concept of dynapenic obesity (DO) has been used to describe the coexistence of excess adipose tissue/body weight and low muscle strength (20). Different criteria have been used to identify the obesity component, such as body mass index (BMI) (21), abdominal obesity (22), and fat mass percentage (23). DO is not a homogenous condition and different phenotypes might exist based on variations in factors like fat distribution and muscle quality.
Regardless of the criteria to identify obesity, DO has been associated with a higher risk of falls (24), poorer bone health (25), inflammatory biomarkers (26), and an increased risk of chronic diseases (27). Given the independent effect of obesity on muscle function (28, 29), DO could be associated with worse physical performance. In individuals with obesity have been reported impaired functional capacity (30); particularly, women with obesity exhibited slower fast gait speeds, shorter stride lengths, poorer sit-to-stand performance, and endurance (31). Nevertheless, high handgrip strength levels could attenuate the negative effect of adiposity (32).
Moreover, recent studies on the association between DO and physical performance in middle-aged women and older show conflicting results (33, 34), which might be due to population characteristics and heterogeneity in DO definitions. We previously reported the prevalence of sarcopenia and obesity in community-dwelling older adults (35), however, the current prevalence of DO in middle-aged and older women remains unknown.
Understanding different DO phenotypes can provide more specific insights into the relationship with physical performance and ultimately lead to more targeted interventions. Thus, this study aimed to assess the relationship between DO phenotypes and physical performance in middle-aged women living in the community.
2 Materials and methods
2.1 Subjects
This was an observational cross-sectional study carried out in community-dwelling, middle-aged and older women living in urban-marginal areas of Guayaquil, Ecuador from November 2019 to December 2020. The following criteria were used for inclusion: women in the ≥50 years old who agreed to participate voluntarily in the study signing an informant consent. The exclusion criteria were institutionalized individuals, those with known dementia or severe cognitive impairment, functional dependence, current cancer, chronic obstructive pulmonary disease, and musculoskeletal diseases. Figure 1 shows the sample selection flowchart.
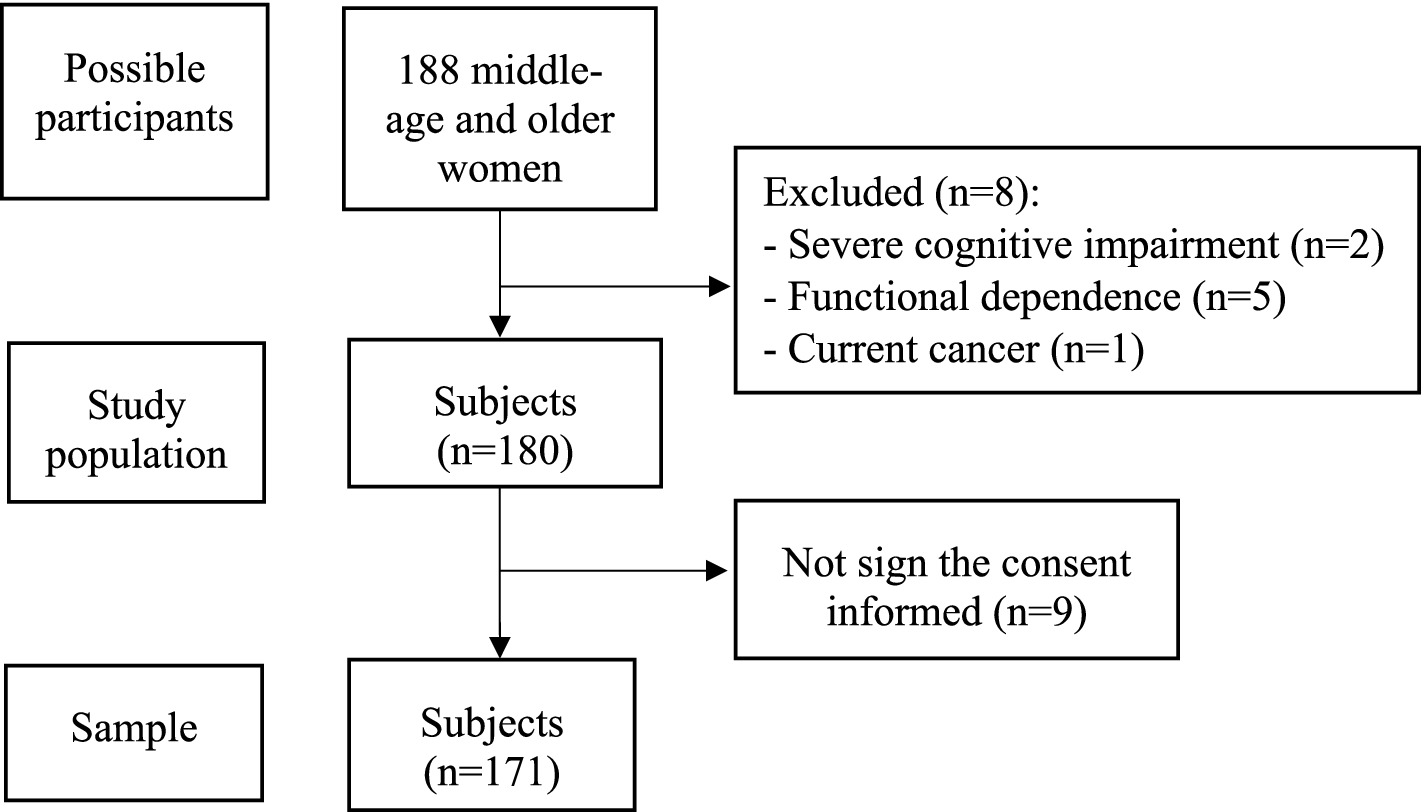
Figure 1. Flowchart of the recruitment process of the participants of the study.
2.2 Sociodemographic and clinical characteristics
Participants filled out a self-reported survey with a standardized questionnaire that assessed their socioeconomic and clinical characteristics. Socioeconomic variables include: age, ethnicity (mestizo, afro-Ecuadorian, Caucasian, indigenous), marital status (single, married, widowed, divorced), education level (none, primary, secondary, tertiary). Clinical characteristics were assessment by prevalent medical conditions such as type 2 diabetes, hypertension, dyslipidemia, gastroesophageal reflux disease, arthritis, constipation.
2.3 Dynapenia measurement
Dynapenia was diagnosticated by handgrip strength (HGS) using a Jamar Plus Hand Dynamometer with an accuracy of over 99% (36). HGS was evaluated in both hands, regardless of the dominant one. Subjects were advised verbally to grip the instrument and perform maximum handgrip strength. All the lectures were carried out standing, with both arms pending sideways and the dynamometer facing the evaluator. The value registered was the higher value realized by side, individuals rest 1 min at least between trials of the same hand. Dynapenia was evaluated by handgrip strength defined as HGS < 16 kg according to the European Working Group on Sarcopenia in Older People (EWGSOP2) (37).
2.4 Obesity measurement
Obesity was identified according to body mass index (BMI), calculated as weight in kilograms divided by height in meters squared (kg/m2). Body mass (weight) was measured on a SECA 700 ® mechanical physical scale and recorded in kilograms (kg) to the nearest 0.1 decimal. Height was recorded on a SECA 213® portable stadiometer. Obesity was determined based on BMI ≥ 30 kg/m2 (38).
2.5 Dynapenic obesity phenotypes
Participants were categorized into four groups based on their dynapenia and obesity status: non-dynapenic/non-obesity (ND/NO), obesity/non-dynapenic (O/ND), dynapenic/non-obesity (D/NO) and dynapenic/obesity (D/O) (39).
2.6 Physical performance measurement
The Short Physical Performance Battery (SPPB) was used to assess physical performance. The SPPB comprises three physical performance measures: standing balance, repeated chair stands, and gait speed (40). Evaluation of balance involved hierarchical tasks consisting of side-by-side, semi-tandem, and full-tandem stands. During the repeated chair stand test, participants underwent timing while performing five sit-to-stand repetitions. Gait speed assessment was conducted by timing participants as they walked 2.44 meters at their usual pace.
Each assessment is graded on a scale ranging from 0 (indicating an inability to complete the task) to 4 points (representing the highest level of performance) on the test. The overall score for the SPPB falls within the range of 0 (indicating the poorest performance) to 12 points (indicating the best performance) and assesses performance in the various tests based on three or four distinct categories of scores: three categories include 0–6 points (indicating subpar performance), 7–9 points (indicating moderate performance), and 10–12 points (indicating good performance); while four categories consist of 0–3 points (indicating disability/very poor performance), 4–6 points (indicating poor performance), 7–9 points (indicating moderate performance), and 10–12 points (indicating good performance).
2.7 Other variables
The following body composition compartments were also measured, using a Multifrequency Segmental Body Composition Analyzer (InBody 270 DSM-BIA®): muscle mass, fat mass, and body fat percentage, as well as their index. To assess BC, participants were advised not to eat or drink 4 h before the test, consume any caffeine beverage or alcohol within 12 h of the test, use diuretic medication, perform exercise 12 h before the test, and suggest evacuating urine.
2.8 Ethical considerations
The study’s approval came from the Ethics Committee for Research in Humans of the “Hospital Clínica Kennedy,” Guayaquil, Ecuador (CEISH No: HCK-CEISH-19-0038, June 21, 2019) and conducted by the guidelines of the Declaration of Helsinki. All participants were informed of the study, its aims, and used instruments, following which they gave written permission to take part.
2.9 Data analysis
Data analysis was performed using IBM SPSS Statistics (version 25.0; IBM, Chicago, IL, EE. UU). Study participants were divided into groups according to DO phenotypes. Continuous variables are reported as mean and standard deviation or median and interquartile range (IQR) in the descriptive analysis, and categorical variables as frequencies and percentages. For the bivariate analysis, the numerical variables with normal distribution were compared using the Anova test; contrary to this, we used the Kruskall-Wallis test. For all analyses, a p value <0.05 was considered statistically significant.
3 Results
A total of 171 middle-aged and older women participated in this study. The median (IQR) age of the sample was 72.0 years (17.0). Obesity and dynapenia were 35.1% (n = 60) and 57.8% (n = 99) of the participants, respectively. The prevalence of ND/NO was 25.1% (n = 43), O/ND 17% (n = 29), D/NO 39.8% (n = 68) and DO 18.1% (n = 31). Subjects with D/NO were older compared with other phenotypes (p < 0.001).
Participants with DO had a higher BMI, waist circumference, fat mass index, and visceral fat compared with the other phenotypes. HGS and phase angel were higher in those with NO/ND and O/ND, compared with the other phenotypes, while skeletal muscle mass was higher in participants with O/ND and D/O phenotypes in contract with others groups. The sociodemographic and clinical characteristics of the participants, according to DO phenotypes, are presented in Table 1.
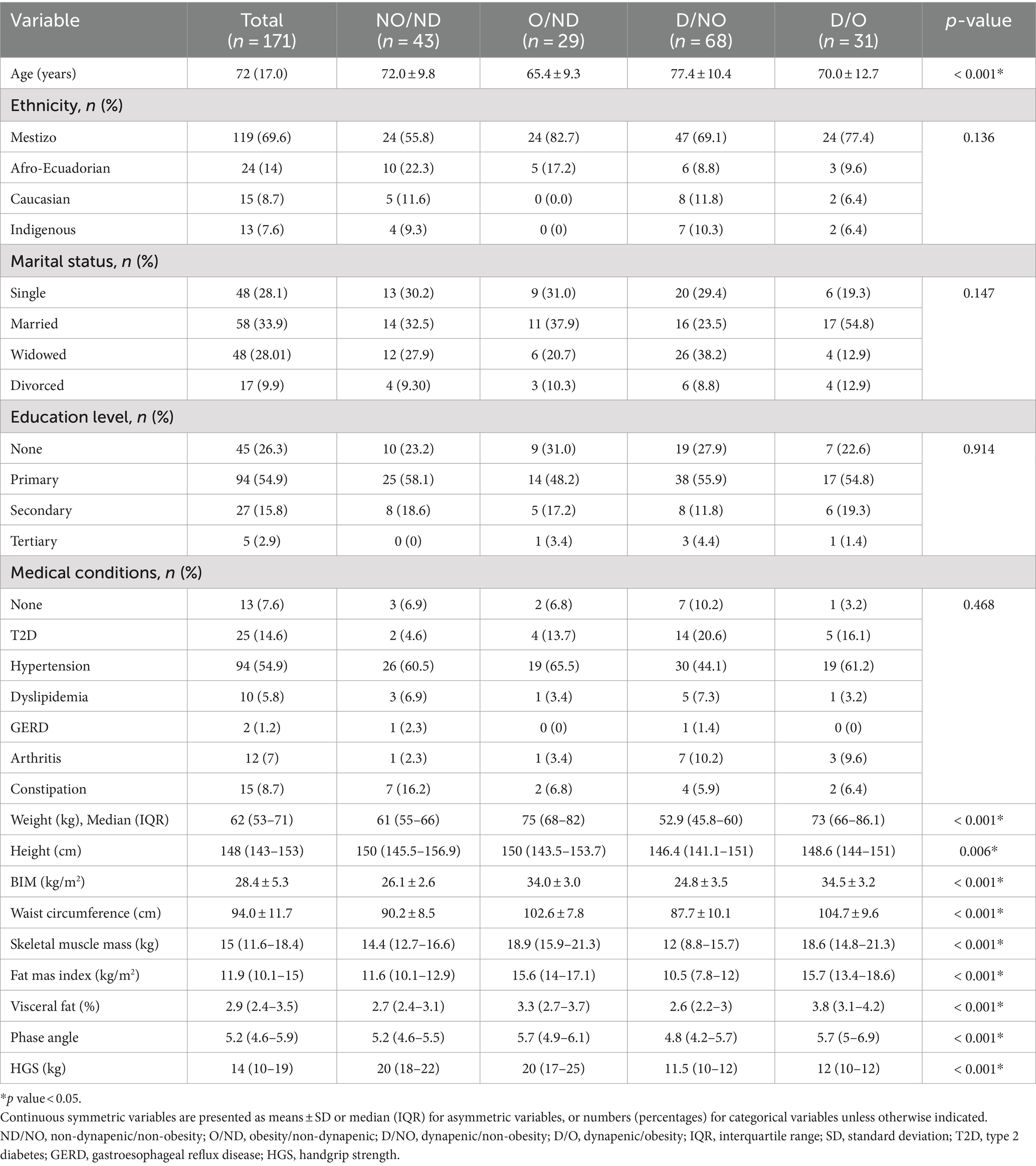
Table 1. Characteristics of the studied population according to dynapenic obesity phenotypes.
The mean SPPB total score was 6.5 ± 3.2 Participants of D/NO and DO groups presented significantly lower mean SPPB scores (p < 0.001) compared to those of NO/ND and O/ND groups (Figure 2).
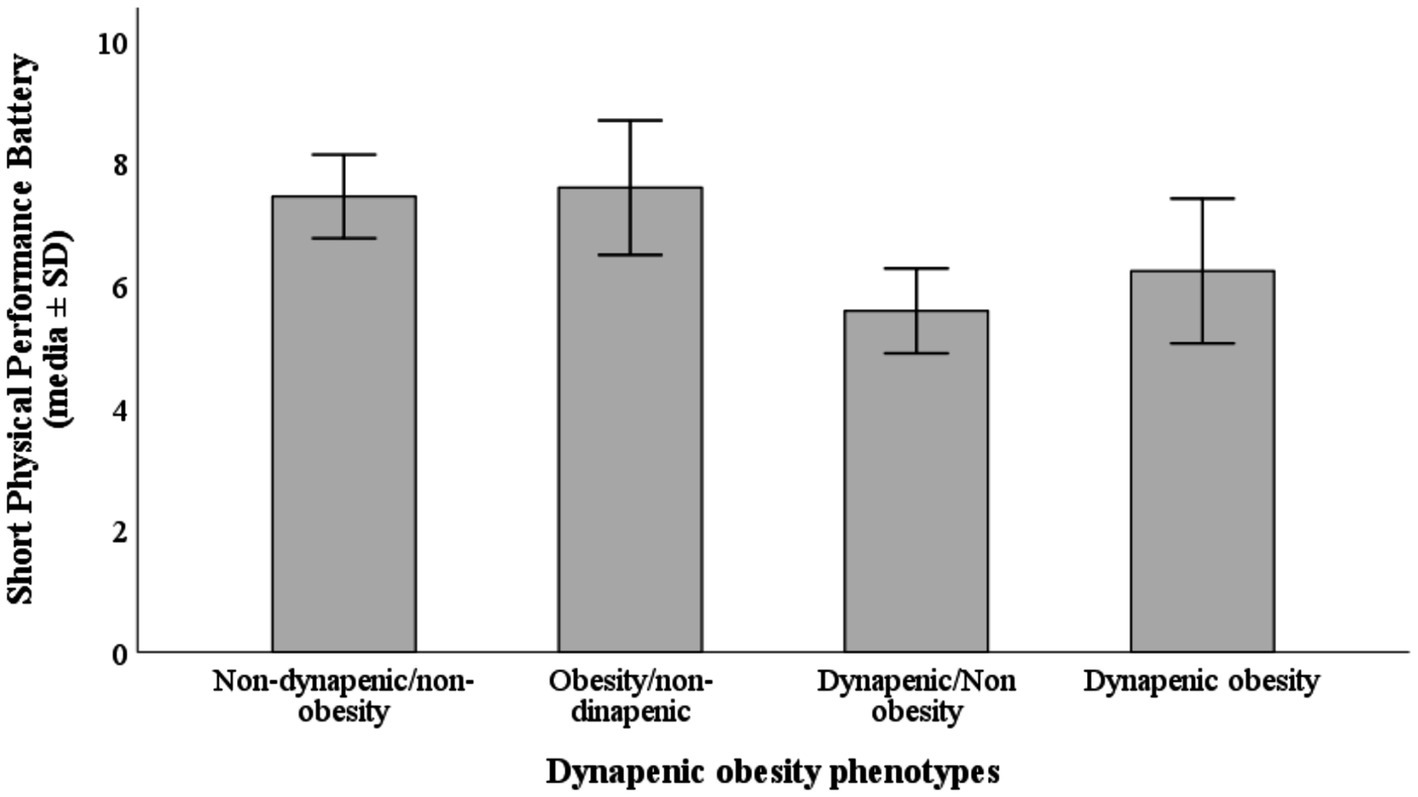
Figure 2. Mean Short Physical Performance Battery (SPPB) total score according to dynapenic obesity phenotypes.
Very poor performance was prevalent in 22.6% (n = 7), while poor performance, moderate performance, and good performance were prevalent in 16.1% (n = 5), 54.8% (n = 17) and 6.4% (n = 2) in the sample, respectively (Table 2).
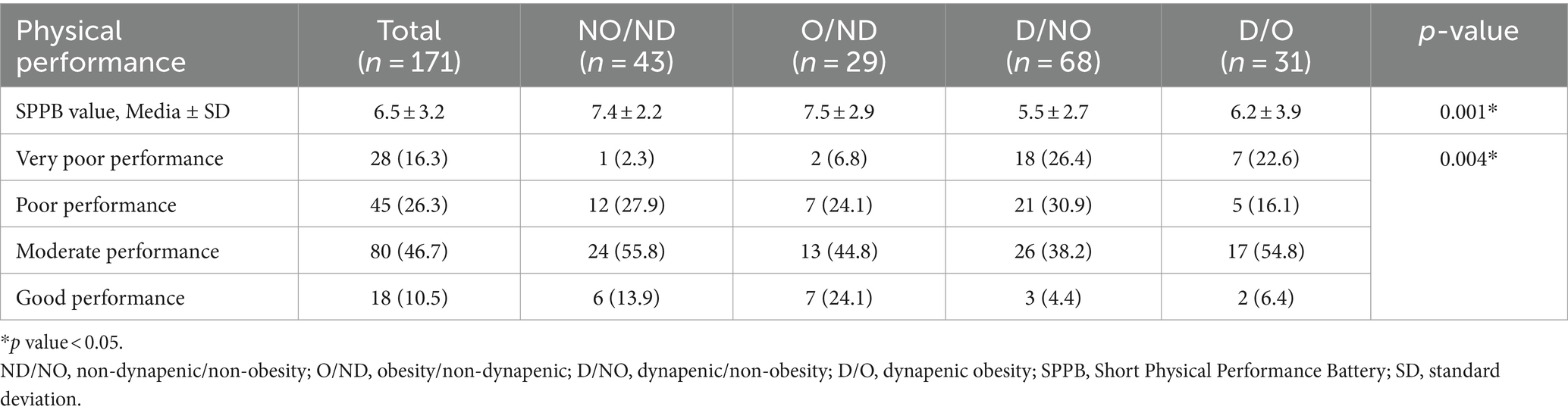
Table 2. Characteristics of the studied population according to dynapenic obesity phenotypes.
4 Discussion
This report aims to enhance understanding of the phenotypes of dynapenia, obesity, and DO in middle-aged and older women living in the community and highlight the detrimental effect of DO on physical function, exceeding the negative effects of either phenotype alone.
To our knowledge, the only report on the prevalence of muscle weakness in older adults was published by Garces, based on the data from the first National Health, Wellbeing, and Aging Survey (21). Later, he reported a lower prevalence of 6.8% phenotype of DO in female older adults, in comparison to 18.1% in our data. This result can be related to a more representative sample size, in contrast with our population of mostly urban-marginal middle-aged women. In other variables, the prevalence of obesity was 35.1% vs. 20%, and the prevalence of only dynapenia was significantly higher in our data with 57.8% vs. 24.7% (39).
Our main findings showed that the D/NO phenotype had the worse scores for physical performance in middle-aged women and older women in the SPPB test, followed by the DO group; we found statistical differences in the SPPB value for the four categories. Anthropometric characteristics of the population related to an increase in fat mass present statistical differences in the four phenotypic groups weight, height, BMI, waist circumference, and visceral fat. Interestingly, skeletal muscle mass was higher in participants with the O/ND phenotype compared to both DO and NO/ND groups. This suggests potential differences in body composition within dynapenic individuals.
Some reports DO have poorer physical function than individuals with obesity alone or dynapenia alone, suggesting a possible independent effect on physical performance measurements, and probably these effects are considered additive and not multiplicative (34, 41). Furthermore, based on cross-sectional and longitudinal studies that have described the mixture effect of obesity and poor muscle strength in older adults, defined as DO, this condition increases the probability of mobility disability, poor functional performance, risk of falls, hospitalization, and higher mortality (41, 42).
Low muscle mass function and obesity affect more than one in ten older adults globally (43). Our data shows that the prevalence of DO in our sample was 18.1%. Stenholm et al. evaluated 930 adults aged 65 and older in a 6-year follow-up period; obesity (cataloged with BMI), and low muscle strength (measured with knee extensor strength) registered a 17% reduction of walking speed, in comparison with 8% counterparts with only obesity and 4% individual with lower strength (44). In another study, with 2,208 adults aged 55 years and older, had been described a prevalence of walking limitations significantly higher 61% than their previous reports when DO was diagnosed (45). Additionally, a recent research suggests that diminished gait speed, an indicator of physical performance, can predict a risk of DO (46).
Regardless the relationship between muscle strength and adiposity is related to the determination of the method to diagnose body fat excess. Reports from Keevil et al. show that a larger BMI was associated with lower HGS, but a high waist circumference value has an opposite association. In addition, they found that a greater value waist circumference HGS was lower in both sexes. These findings proposed that abdominal fat is the most metabolically active tissue with the understanding potential mechanism for the association between skeletal muscle and fat mass (47).
Finally, finding obesity phenotypes (48) could help researchers better understand how DO interacts with physical performance, which will advance the study of DO (49).
This study provides valuable insights into sarcopenia (DO) phenotypes in middle-aged and older women residing in the community. When compared to national reference data (39), our findings reveal a significant increase in the prevalence of obesity, dynapenia, and sarcopenia. This highlights the critical need for public health programs and interventions to prevent and address these conditions. The heightened prevalence of sarcopenia emphasizes the need for further research aimed at identifying associated factors and developing strategies to improve muscle health and physical function in this population.
At the national level, the high prevalence of dynapenia and obesity calls for a comprehensive approach to assessment and intervention. Potential strategies could include programs that promote physical activity through public awareness campaigns, community-based exercise and nutrition initiatives, and training healthcare professionals to manage these conditions effectively. Ensuring equitable access to care will require addressing socioeconomic disparities and improving healthcare accessibility across all sectors.
One key limitation of this study is its cross-sectional design, which does not allow for establishing causal relationships between the variables examined (e.g., obesity and dynapenia with physical performance). Furthermore, the study only included middle-aged and older women, limiting the generalizability of the results to younger populations.
5 Conclusion
In conclusion, the D/NO and D/O groups presented the worst scores in physical performance and were associated with impaired physical function. The DO group had the highest body fat percentage and worst performance on the SPPB. This suggests the DO phenotype is associated with poorer physical health. This link between the DO phenotype and functional limitations is a key finding that can help establish personalized therapeutic strategies to address the coexistence of these health problems.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee for Research in Humans of the “Hospital Clínica Kennedy,” Guayaquil, Ecuador (CEISH No: HCK-CEISH-19-0038, June 21, 2019). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
CA-P: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. DF-P: Writing – original draft, Writing – review & editing. MB: Writing – original draft, Writing – review & editing. JG-C: Writing – original draft, Writing – review & editing. JE: Writing – original draft, Writing – review & editing. LÁ-C: Funding acquisition, Investigation, Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was partially funded by the Universidad Católica de Santiago de Guayaquil.
Acknowledgments
To the students who participated in data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Martin, WP, and le Roux, CW. Obesity is a disease, Bariatric surgery in clinical practice In: D Haslam, A Malhotra, and MS Capehorn, editors. Wellcome Trust–funded monographs and book chapters. Cham (CH): springer (2022)
2. Verde, L, Barrea, L, Vetrani, C, Frias-Toral, E, Chapela, SP, Jayawardena, R, et al. Chronotype and sleep quality in obesity: how do they change after menopause? Curr Obes Rep. (2022) 11:254–62. doi: 10.1007/s13679-022-00479-9
3. Worldwide trends in underweight and obesity from . To 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet. (1990) 403:1027–50. doi: 10.1016/S0140-6736(23)02750-2
4. Palacios, S, Chedraui, P, Sánchez-Borrego, R, Coronado, P, and Nappi, RE. Obesity and menopause. Gynecol Endocrinol. (2024) 40:2312885. doi: 10.1080/09513590.2024.2312885
5. Barrea, L, Verde, L, Auriemma, RS, Vetrani, C, Cataldi, M, Frias-Toral, E, et al. Probiotics and prebiotics: any role in menopause-related diseases? Curr Nutr Rep. (2023) 12:83–97. doi: 10.1007/s13668-023-00462-3
6. Suárez, R, Chapela, SP, Álvarez-Córdova, L, Bautista-Valarezo, E, Sarmiento-Andrade, Y, Verde, L, et al. Epigenetics in obesity and diabetes mellitus: new insights. Nutrients. (2023) 15:811. doi: 10.3390/nu15040811
7. Barrea, L, Frias-Toral, E, Pugliese, G, Garcia-Velasquez, E, de Los Angeles Carignano, M, Savastano, S, et al. Vitamin D in obesity and obesity-related diseases: an overview. Minerva Endocrinol. (2021) 46:177–92. doi: 10.23736/S2724-6507.20.03299-X
8. Verma, A, Malhotra, A, Ranjan, P, Kumari, A, Chopra, S, Khan, MA, et al. A comprehensive evaluation of predictors of obesity in women during the perimenopausal period: a systematic review and narrative synthesis. Diabetes Metab Syndr Clin Res Rev. (2024) 18:102933. doi: 10.1016/j.dsx.2023.102933
9. Silva, FM, Giatti, L, Fonseca, M d JM d, Brant, LCC, Diniz, M d FHS, Molina, M d CB, et al. Consumption of ultra-processed foods and eight-year risk of death from all causes and noncommunicable diseases in the ELSA-Brasil cohort. Int J Food Sci Nutr. (2023) 74:845–54. doi: 10.1080/09637486.2023.2267797
10. Mirmiran, P, Moslehi, N, Golzarand, M, and Azizi, F. Ultra-processed foods consumption and the risk of metabolically unhealthy phenotype in normal-weight and overweight/obese adults: a prospective investigation. Int J Food Sci Nutr. (2023) 74:522–31. doi: 10.1080/09637486.2023.2222935
11. Godos, J, Zappalà, G, Mistretta, A, Galvano, F, and Grosso, G. Mediterranean diet, diet quality, and adequacy to Italian dietary recommendations in southern Italian adults. Mediterr J Nutr Metab. (2024) 17:11–14. doi: 10.3233/MNM-240043
12. Frias-Toral, E, Chapela, S, de los Angeles Carignano, M, Moretti, D, Martinuzzi, A, Rodríguez-Veintimilla, D, et al. Mediterranean diet and physical activity for successful aging: an update for nutritionists and endocrinologists. Endocrine. (2021) 2:366–83. doi: 10.3390/endocrines2040034
13. Larsson, L, Degens, H, Li, M, Salviati, L, Lee, Y, Thompson, W, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev. (2019) 99:427–511. doi: 10.1152/physrev.00061.2017
14. Keller, K, and Engelhardt, M. Strength and muscle mass loss with aging process. Age and strength loss. Muscles Ligaments Tendons J. (2013) 3:346–50. doi: 10.32098/mltj.04.2013.17
15. Zadoń, H, Michnik, R, and Nowakowska-Lipiec, K. Exploring the impact of body mass change on fatigue and activity of the muscular system during daily routine. Technol Health Care. (2023) 31:2487–98. doi: 10.3233/THC-235014
16. Zhou, W, Tong, J, Wen, Z, Mao, M, Wei, Y, Li, X, et al. Prevalence and factors associated with dynapenia among middle-aged and elderly people in rural southern China. Prev Med Rep. (2024) 38:102630. doi: 10.1016/j.pmedr.2024.102630
17. Piché, M-E, Tchernof, A, and Després, J-P. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. (2020) 126:1477–500. doi: 10.1161/CIRCRESAHA.120.316101
18. Tam, BT, Morais, JA, and Santosa, S. Obesity and ageing: two sides of the same coin. Obes Rev. (2020) 21:e12991. doi: 10.1111/obr.12991
19. Atkins, JL, and Wannamathee, SG. Sarcopenic obesity in ageing: cardiovascular outcomes and mortality. Br J Nutr. (2020) 124:1102–13. doi: 10.1017/S0007114520002172
20. Pérez-Campos Mayoral, L, Matias-Cervantes, CA, Pérez-Campos, E, Romero Díaz, C, Laguna Barrios, LÁ, Pina Canseco, MS, et al. Associations of Dynapenic obesity and Sarcopenic obesity with the risk of complications in COVID-19. Int J Mol Sci. (2022) 23:8277. doi: 10.3390/ijms23158277
21. Orces, CH . Prevalence of clinically relevant muscle weakness and its association with vitamin D status among older adults in Ecuador. Aging Clin Exp Res. (2017) 29:943–9. doi: 10.1007/s40520-016-0678-3
22. Ramírez, PC, de Oliveira, DC, de Oliveira Máximo, R, de Souza, AF, Luiz, MM, Delinocente, MLB, et al. Is dynapenic abdominal obesity a risk factor for cardiovascular mortality? A competing risk analysis. Age Ageing. (2023) 52:afac301. doi: 10.1093/ageing/afac301
23. Rossi, AP, Urbani, S, Fantin, F, Nori, N, Brandimarte, P, Martini, A, et al. Worsening disability and hospitalization risk in Sarcopenic obese and Dynapenic abdominal obese: a 5.5 years follow-up study in elderly men and women. Front Endocrinol. (2020) 11:314. doi: 10.3389/fendo.2020.00314
24. Gadelha, AB, Neri, SGR, Vainshelboim, B, Ferreira, AP, and Lima, RM. Dynapenic abdominal obesity and the incidence of falls in older women: a prospective study. Aging Clin Exp Res. (2020) 32:1263–70. doi: 10.1007/s40520-019-01318-z
25. Nakano, W, Ozaki, E, Kato, M, Tsukamoto, T, Ono, S, Tomida, S, et al. Association between bone health and dynapenic obesity in postmenopausal women. Geriatr Gerontol Int. (2024) 24:378–84. doi: 10.1111/ggi.14849
26. Corrêa, H d L, Rosa, T d S, Dutra, MT, Sales, MM, Noll, M, Deus, LA, et al. Association between dynapenic abdominal obesity and inflammatory profile in diabetic older community-dwelling patients with end-stage renal disease. Exp Gerontol. (2021) 146:111243. doi: 10.1016/j.exger.2021.111243
27. Choi, Y, Cho, J, Kim, J, Bae, JH, Cho, E-J, Chang, E, et al. Dynapenic-abdominal obesity as an independent risk factor for chronic kidney disease in postmenopausal women: a population-based cohort study. Menopause. (2022) 29:1040–6. doi: 10.1097/GME.0000000000002032
28. Morgan, PT, Smeuninx, B, and Breen, L. Exploring the impact of obesity on skeletal muscle function in older age. Front Nutr. (2020) 7:569904. doi: 10.3389/fnut.2020.569904
29. Maza Moscoso, CP, Calvo Higuera, I, Gómez Carrillo, A, Abril, T, and Frías-Toral, E. Estado nutricional y disminución de fuerza muscular en pacientes hospitalizados. RB. (2023) 8:1–10. doi: 10.21931/RB/2023.08.04.21
30. Roh, E, and Choi, KM. Health consequences of Sarcopenic obesity: a narrative review. Front Endocrinol. (2020) 11:332. doi: 10.3389/fendo.2020.00332
31. Pataky, Z, Armand, S, Müller-Pinget, S, Golay, A, and Allet, L. Effects of obesity on functional capacity. Obesity. (2014) 22:56–62. doi: 10.1002/oby.20514
32. Ramírez-Vélez, R, Pérez-Sousa, MÁ, García-Hermoso, A, Zambom-Ferraresi, F, Martínez-Velilla, N, Sáez de Asteasu, ML, et al. Relative handgrip strength diminishes the negative effects of excess adiposity on dependence in older adults: a moderation analysis. J Clin Med. (2020) 9:1152. doi: 10.3390/jcm9041152
33. Zhang, L, Liu, S, Wang, W, Sun, M, Tian, H, Wei, L, et al. Dynapenic abdominal obesity and the effect on long-term gait speed and falls in older adults. Clin Nutr. (2022) 41:91–6. doi: 10.1016/j.clnu.2021.11.011
34. Máximo, R d O, de Oliveira, DC, Ramirez, PC, Luiz, MM, de Souza, AF, Delinocente, MLB, et al. Combination of dynapenia and abdominal obesity affects long-term physical performance trajectories in older adults: sex differences. Am J Clin Nutr. (2022) 115:1290–9. doi: 10.1093/ajcn/nqac023
35. Frias-Toral, E, Alvarez, L, Artacho, R, Arteaga, C, Salcedo, D, Fonseca, D, et al. Prevalence of sarcopenia in community-dwelling older adults of Guayaquil. Clinical Nutrition ESPEN. (2020) 40:473. doi: 10.1016/j.clnesp.2020.09.201
36. Cildan Uysal, S, Tonak, HA, and Kitis, A. Validity, reliability and test-retest study of grip strength measurement in two positions with two dynamometers: Jamar® plus and K-force® grip. Hand Surg Rehabil. (2022) 41:305–10. doi: 10.1016/j.hansur.2022.02.007
37. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
38. Haam, J-H, Kim, BT, Kim, EM, Kwon, H, Kang, J-H, Park, JH, et al. Diagnosis of obesity: 2022 update of clinical practice guidelines for obesity by the Korean Society for the Study of obesity. J Obes Metab Syndr. (2023) 32:121–9. doi: 10.7570/jomes23031
39. Orces, CH, Orces, CH, Weisson, K, and Weisson, K. Vitamin D status of older adults with Dynapenic obesity in Ecuador. J Am Geriatr Soc. (2016) 64:e235–7. doi: 10.1111/jgs.14500
40. Guralnik, JM, Simonsick, EM, Ferrucci, L, Glynn, RJ, Berkman, LF, Blazer, DG, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. (1994) 49:M85–94. doi: 10.1093/geronj/49.2.m85
41. Bouchard, DR, and Janssen, I. Dynapenic-obesity and physical function in older adults. J Gerontol A Biol Sci Med Sci. (2010) 65A:71–7. doi: 10.1093/gerona/glp159
42. da Silva, AT, Scholes, S, Ferreira Santos, JL, de Oliveira Duarte, YA, and de Oliveira, C. Dynapenic abdominal obesity increases mortality risk among English and Brazilian older adults: a 10-year follow-up of the ELSA and SABE studies. J Nutr Health Aging. (2018) 22:138–44. doi: 10.1007/s12603-017-0966-4
43. Gao, Q, Mei, F, Shang, Y, Hu, K, Chen, F, Zhao, L, et al. Global prevalence of sarcopenic obesity in older adults: a systematic review and meta-analysis. Clin Nutr. (2021) 40:4633–41. doi: 10.1016/j.clnu.2021.06.009
44. Stenholm, S, Alley, D, Bandinelli, S, Griswold, ME, Koskinen, S, Rantanen, T, et al. The effect of obesity combined with low muscle strength on decline in mobility in older persons: results from the InCHIANTI study. Int J Obes. (2009) 33:635–44. doi: 10.1038/ijo.2009.62
45. Stenholm, S, Rantanen, T, Alanen, E, Reunanen, A, Sainio, P, and Koskinen, S. Obesity history as a predictor of walking limitation at old age. Obesity. (2007) 15:929–38. doi: 10.1038/oby.2007.583
46. Flores-Pérez, CJ, Flores-Pérez, CJ, Castro-Porras, L, Castro-Porras, LV, López-Rodríguez, G, López-Rodríguez, G, et al. Slow gait speed is associated with dynapenic obesity in Mexican ambulatory older adults. Geriatr Nurs. (2022) 45:125–30. doi: 10.1016/j.gerinurse.2022.03.011
47. Keevil, VL, Luben, R, Dalzell, N, Hayat, S, Sayer, AA, Wareham, NJ, et al. Cross-sectional associations between different measures of obesity and muscle strength in men and women in a British cohort study. J Nutr Health Aging. (2015) 19:3–11. doi: 10.1007/s12603-014-0492-6
48. Barrea, L, Muscogiuri, G, Pugliese, G, de Alteriis, G, Colao, A, and Savastano, S. Metabolically healthy obesity (MHO) vs. metabolically unhealthy obesity (MUO) phenotypes in PCOS: association with endocrine-metabolic profile, adherence to the Mediterranean diet, and body composition. Nutrients. (2021) 13:3925. doi: 10.3390/nu13113925
Keywords: dynapenic obesity, physical performance, middle-age women, community-dwelling, dynapenia
Citation: Arteaga-Pazmiño C, Fonseca-Pérez D, Balladares Mazzini M, Galvez-Celi J, Emén Sánchez J and Álvarez-Córdova L (2024) Association between dynapenic obesity phenotypes and physical performance in middle-age and older women living in community. Front. Nutr. 11:1480284. doi: 10.3389/fnut.2024.1480284
Edited by:
Almino Ramos, Gastro Obeso Center, BrazilReviewed by:
Alexandra Castan, 123 Certification, CanadaJimmy Martin, Junta de Beneficencia de Guayaquil, Ecuador
Copyright © 2024 Arteaga-Pazmiño, Fonseca-Pérez, Balladares Mazzini, Galvez-Celi, Emén Sánchez and Álvarez-Córdova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cecilia Arteaga-Pazmiño, Y2VjaWxpYS5hcnRlYWdhcEBnbWFpbC5jb20=